Echo Pleuro Pulm-2 - SEMINAIRES IRIS · Radio pulmonaire de face, ... Sémiologie basée sur les...
50
L’ÉCHOGRAPHIE L’ÉCHOGRAPHIE PLEURO PLEURO-PULMONAIRE PULMONAIRE PLEURO PLEURO-PULMONAIRE PULMONAIRE Séminaire Séminaire IRIS IRIS Bruxelles Bruxelles – Mars 2010 Mars 2010 D r Ph. PÈS Bruxelles Bruxelles – Mars 2010 Mars 2010 D r Philippe PÈS D r Etienne HINGLAIS D r Tomislav PETROVIC SEMINAIRES IRIS
Transcript of Echo Pleuro Pulm-2 - SEMINAIRES IRIS · Radio pulmonaire de face, ... Sémiologie basée sur les...

L’ÉCHOGRAPHIEL’ÉCHOGRAPHIEPLEUROPLEURO--PULMONAIREPULMONAIREPLEUROPLEURO--PULMONAIREPULMONAIRE
SéminaireSéminaire IRISIRIS
BruxellesBruxelles –– Mars 2010Mars 2010
Dr Ph. PÈS
BruxellesBruxelles –– Mars 2010Mars 2010
Dr Philippe PÈSDr Etienne HINGLAISDr Tomislav PETROVIC
SEMIN
AIRE
S IR
IS

PLANPLAN
Echographie PleuroEchographie Pleuro--PulmonairePulmonaire
Etat des lieuxEtat des lieuxEtat des lieuxEtat des lieuxDescription techniqueDescription techniqueParoi (syndrome pariétal)Paroi (syndrome pariétal) Plèvre (épanchement)Plèvre (épanchement) Poumon (syndrome interstitiel)Poumon (syndrome interstitiel)
Dr Ph. PÈS
Poumon (syndrome interstitiel)Poumon (syndrome interstitiel) Intérêt & conclusionIntérêt & conclusion
SEMIN
AIRE
S IR
IS

��Rien de spécifique pour le Rien de spécifique pour le poumonpoumon
ÉCHOGRAPHIE PAR UN NON ÉCHOGRAPHIE PAR UN NON RADIOLOGUERADIOLOGUE
��Rien de spécifique pour le Rien de spécifique pour le poumonpoumon(jusqu’à (jusqu’à 20092009…)…)
��Durée apprentissage théorique Durée apprentissage théorique variable de variable de 8 8 à à 24 24 heuresheures
��Durée formation pratique variable de Durée formation pratique variable de
Dr Ph. PÈS
��Durée formation pratique variable de Durée formation pratique variable de 5 5 à à 500 500 examens supervisésexamens supervisés
SUSTI University Hospital, Rijeka, Croatia 1999
TSO P. J. Trauma – 1992,
SALEN P. J. Trauma – 1999,
SEMIN
AIRE
S IR
IS

UNE BONNE LECTURE...UNE BONNE LECTURE...
Dr Ph. PÈShttp://chestjournal.chestpubs.org/content/135/4/1050.full.html
SEMIN
AIRE
S IR
IS

ÉTATS DES LIEUXÉTATS DES LIEUX
��Radio pulmonaire de face, au litRadio pulmonaire de face, au lit•• Référence quotidienne aux urgencesRéférence quotidienne aux urgences•• Référence quotidienne aux urgencesRéférence quotidienne aux urgences•• Contrôle des sondes et drains en réa…Contrôle des sondes et drains en réa…
MAISMAIS
•Mouvements du thorax•Rotation du patient
MAUVAISE ÉVALUATIONMAUVAISE ÉVALUATION ::
ÉPANCHEMENTS PLEURAUXÉPANCHEMENTS PLEURAUX
Dr Ph. PÈS
•Rotation du patient•Plaque positionnée en arrière du thorax•Origine antérieure des rayons X•Distance trop faible de la cage thoracique
ÉPANCHEMENTS PLEURAUXÉPANCHEMENTS PLEURAUXCONSOLIDATIONS ALVÉOLAIRESCONSOLIDATIONS ALVÉOLAIRESATTEINTES ALVÉOLOATTEINTES ALVÉOLO--INTERSTITIELLESINTERSTITIELLES
SEMIN
AIRE
S IR
IS
ÉTATS DES LIEUXÉTATS DES LIEUX
��Scanner Scanner thoraciquethoracique spiraléspiralé•• RéférenceRéférence ouou Gold StandardGold Standard•• RéférenceRéférence ouou Gold StandardGold Standard
-- Atélectasies et consolidationsAtélectasies et consolidations-- Syndromes alvéoloSyndromes alvéolo--interstitielsinterstitiels-- Pneumothorax et épanchements pleurauxPneumothorax et épanchements pleuraux-- Morphologie pulmonaireMorphologie pulmonaire
MAIS…MAIS…
--Transport du patient (instable…)Transport du patient (instable…) -Installation du patient (long et risqué) -Irradiation non négligeable
Dr Ph. PÈS
-- Morphologie pulmonaireMorphologie pulmonaire-- Distribution de la perte d’aérationDistribution de la perte d’aération-- Surdistension pulmonaireSurdistension pulmonaire-- Séquelles barotraumatiquesSéquelles barotraumatiques
-Irradiation non négligeable-Disponibilité de l’appareil-Décontamination de la salle
Rendant illusoire son utilisation quotidienneRendant illusoire son utilisation quotidienneSE
MINAI
RES
IRIS
CROYANCES ET IDÉES REÇUESCROYANCES ET IDÉES REÇUES
��L’ennemi c’est l’airL’ennemi c’est l’air !!•• 1992 1992 : «: « Le poumon représente un Le poumon représente un
obstacle majeur à l’utilisation des ultrason obstacle majeur à l’utilisation des ultrason •• 1992 1992 : «: « Le poumon représente un Le poumon représente un
obstacle majeur à l’utilisation des ultrason obstacle majeur à l’utilisation des ultrason au niveau thoraciqueau niveau thoracique » » HARRISSON TR Principles of HARRISSON TR Principles of Internal medicine.Internal medicine.
•• 2001 2001 : «: « L’échographie n’est pas utile L’échographie n’est pas utile pour l’évaluation du parenchyme pour l’évaluation du parenchyme pulmonairepulmonaire » » HARRISSON TR Principles of Internal medicine.HARRISSON TR Principles of Internal medicine.
Dr Ph. PÈS
��L’os est (presque) infranchissableL’os est (presque) infranchissable
SEMIN
AIRE
S IR
IS
MÉTHODEMÉTHODE
��Où mettre la sonde ?Où mettre la sonde ?•• Là ou je met le sthéto…Là ou je met le sthéto…•• Là ou je met le sthéto…Là ou je met le sthéto…•• Méthode des quadrantsMéthode des quadrants
��Position du PatientPosition du Patient
Dr Ph. PÈS
��Syndromes «Syndromes « déclivedéclive »»��Syndrome «Syndrome « culminantsculminants »»
SEMIN
AIRE
S IR
IS

PRINCIPES DE BASEPRINCIPES DE BASE
��Air Monte / Liquide descend*Air Monte / Liquide descend*��Air Monte / Liquide descend*Air Monte / Liquide descend*��Coupe longitudinale guidée par les cotesCoupe longitudinale guidée par les cotes��Sémiologie basée sur les artéfactsSémiologie basée sur les artéfacts��Analyse en dynamiqueAnalyse en dynamique��Extension en surface de la majorité des Extension en surface de la majorité des
Dr Ph. PÈS
��Extension en surface de la majorité des Extension en surface de la majorité des pathologies aiguespathologies aigues
* Confucius, y a longtemps…* Confucius, y a longtemps…SE
MINAI
RES
IRIS

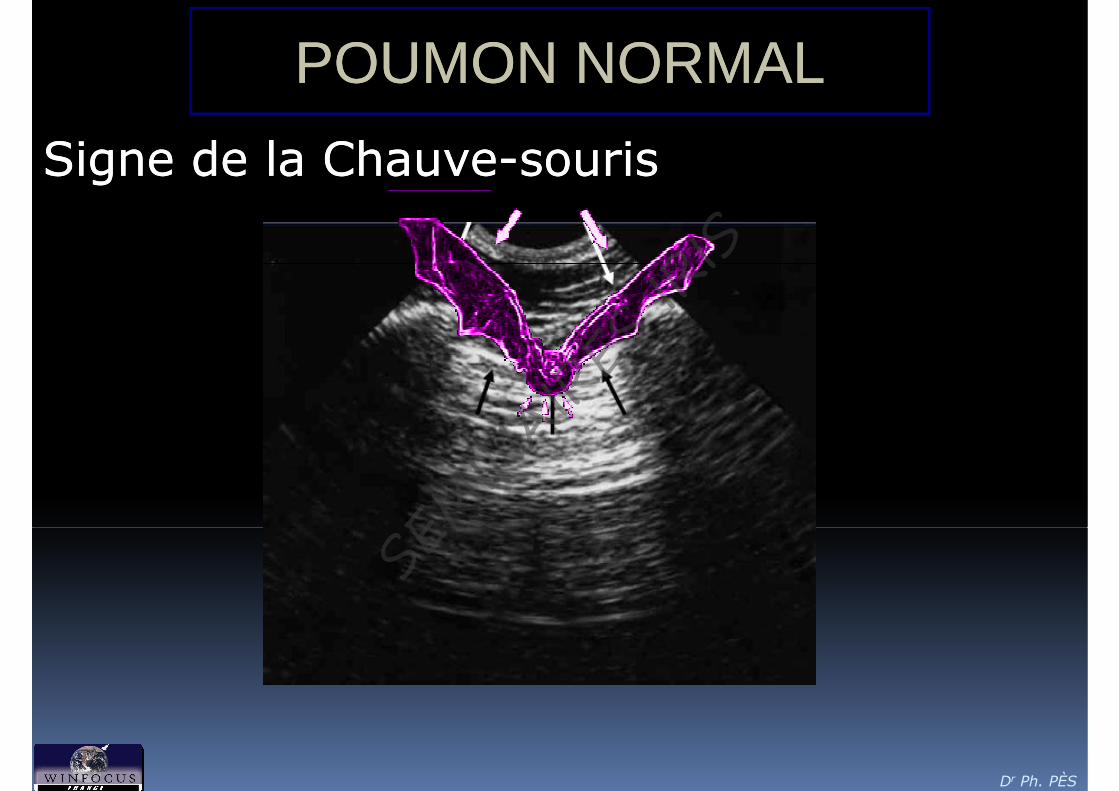
POUMON NORMALPOUMON NORMAL
Signaux StatiquesSignaux Statiques•• Signe de la chauveSigne de la chauve--sourissourissourissouris
•• Ligne A (Artéfacts de Ligne A (Artéfacts de réverbération)réverbération)
•• Ligne B (Artéfacts en Ligne B (Artéfacts en queue de comètes) queue de comètes) Souvent absents chez le Souvent absents chez le sujet sainsujet sain
Dr Ph. PÈS
sujet sainsujet sain
Normalement, les ultrasons sont Normalement, les ultrasons sont arrêtés par le gaz intraarrêtés par le gaz intra--pulmonaire et pulmonaire et le parenchyme pulmonaire n’est pas le parenchyme pulmonaire n’est pas visible auvisible au--delà de la plèvre.delà de la plèvre.
Lichtenstein D. Int.Care. Lichtenstein D. Int.Care. 20012001, , 20042004SE
MINAI
RES
IRIS
POUMON NORMALPOUMON NORMAL
Signe de la ChauveSigne de la Chauve--sourissouris
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

POUMON NORMALPOUMON NORMAL
��Ligne B Ligne B ��Ligne B Ligne B (Artéfacts en (Artéfacts en queue de queue de comètes)comètes)
Dr Ph. PÈS
Targhetta R. J. Clin. Ultrasound, Targhetta R. J. Clin. Ultrasound, 19931993SE
MINAI
RES
IRIS

POUMON NORMALPOUMON NORMAL
Dr Ph. PÈS
Ligne B (Artéfacts en Ligne B (Artéfacts en queue de comètes)queue de comètes)
Targhetta R. J. Clin. Ultrasound, Targhetta R. J. Clin. Ultrasound, 19931993SE
MINAI
RES
IRIS

POUMON NORMALPOUMON NORMAL
Glissement présent
Lichtenstein D. CHEST. Lichtenstein D. CHEST. 19951995
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

LE MODE TMLE MODE TM
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

LES GRANDS SYNDROMESLES GRANDS SYNDROMES
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

FUMER TUEFUMER TUE
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

SYNDROME PARIÉTALSYNDROME PARIÉTAL
��S’il n’existe pas d’air entre la sonde et S’il n’existe pas d’air entre la sonde et la masse à étudier…la masse à étudier…la masse à étudier…la masse à étudier…
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

SYNDROME PARIÉTALSYNDROME PARIÉTAL
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

SYNDROME PARIÉTALSYNDROME PARIÉTAL
ATTENTION À LA SOUS ÉVALUATIONATTENTION À LA SOUS ÉVALUATION
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

CINÉTIQUE DIAPHRAGMATIQUECINÉTIQUE DIAPHRAGMATIQUE
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PLÈVRE (ÉPANCHEMENT)PLÈVRE (ÉPANCHEMENT)
��Épanchement pleural liquidienÉpanchement pleural liquidien
•• Abord exclusivement interAbord exclusivement inter--costalcostal
•• Aspect hypoAspect hypo--échogèneéchogène
•• La plèvre, hyperLa plèvre, hyper--échogène est bordanteéchogène est bordante
•• Signe de la sinusoïde en mode TMSigne de la sinusoïde en mode TM
Dr Ph. PÈS
•• Signe de la sinusoïde en mode TMSigne de la sinusoïde en mode TM
Lichtenstein Ann. Fr. Anesth Reanim 1998Sensibilité : 86 à 97 %Spécificité : 94 %
SEMIN
AIRE
S IR
IS

�� Epaisseur liquidienne Epaisseur liquidienne augmente à l’inspirationaugmente à l’inspiration
PLÈVRE (ÉPANCHEMENT)PLÈVRE (ÉPANCHEMENT)
Signe de la SinusoïdeSigne de la Sinusoïde
Dr Ph. PÈS
Lichtenstein Intensive Care Med 1999Image D. LichtensteinImage D. Lichtenstein
SEMIN
AIRE
S IR
IS
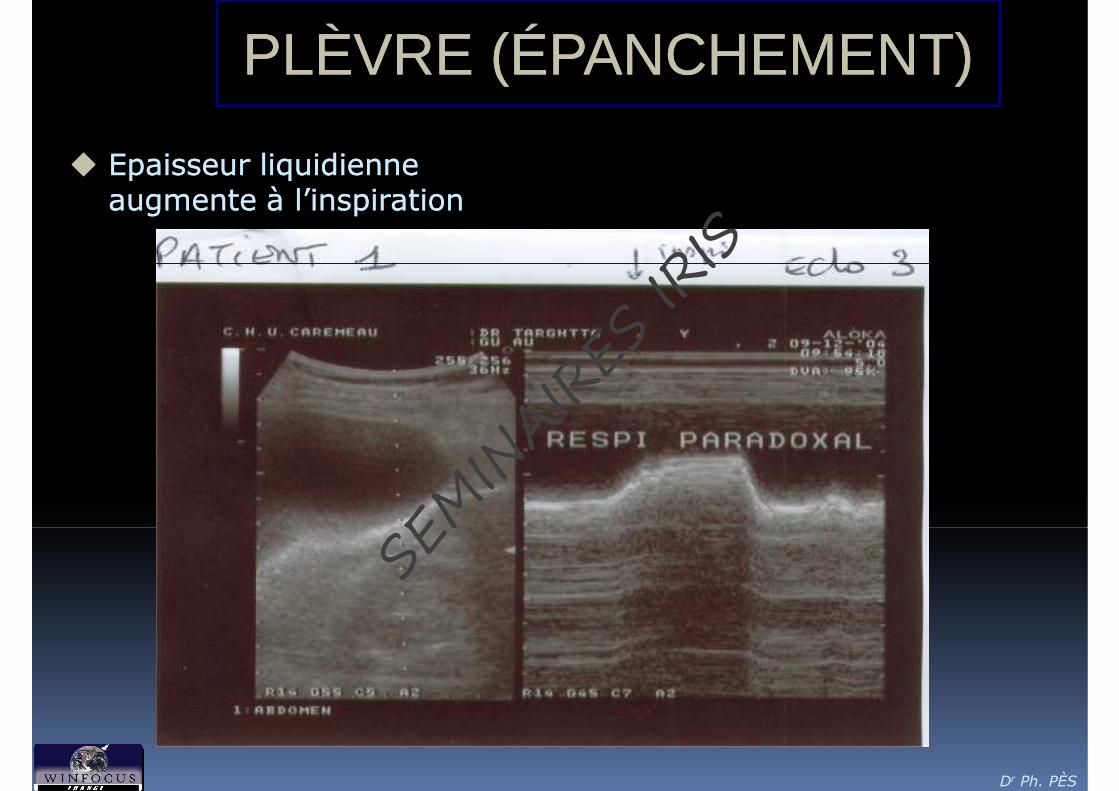
�� Epaisseur liquidienne Epaisseur liquidienne augmente à l’inspirationaugmente à l’inspiration
PLÈVRE (ÉPANCHEMENT)PLÈVRE (ÉPANCHEMENT)
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS
PLÈVRE (ÉPANCHEMENT)PLÈVRE (ÉPANCHEMENT)
��PneumothoraxPneumothorax
•• Abord exclusivement interAbord exclusivement inter--costalcostal
•• Absence de signe du glissementAbsence de signe du glissement ((se se 100100%, sp %, sp 9191%%))
•• Absence de lignes B Absence de lignes B ((se se 6060%, sp %, sp 100100%%))
•• Signe du point poumon en mode TMSigne du point poumon en mode TM
Dr Ph. PÈS
•• Signe du point poumon en mode TMSigne du point poumon en mode TM
Lichtenstein Chest 1995SE
MINAI
RES
IRIS

POUMONPOUMON NORMALNORMAL
Dr Ph. PÈSPour rappel et se le remettre dans l’œil…Pour rappel et se le remettre dans l’œil…
SEMIN
AIRE
S IR
IS

PNEUMOTHORAXPNEUMOTHORAX
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PNEUMOTHORAXPNEUMOTHORAX
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

LE LE PNOPNO en MODE TMen MODE TM
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PNEUMOTHORAXPNEUMOTHORAX
Dr Ph. PÈS
PNEUMO…PAS PNEUMO…
Image D. LichtensteinImage D. LichtensteinSE
MINAI
RES
IRIS

PNEUMOTHORAXPNEUMOTHORAX
POINT POINT POUMONPOUMONPOINT POINT POUMONPOUMONdu du PNEUMOTHORAXPNEUMOTHORAX PARTIELPARTIEL
Inspiration Expiration
Dr Ph. PÈS
Image D. LichtensteinImage D. LichtensteinSE
MINAI
RES
IRIS
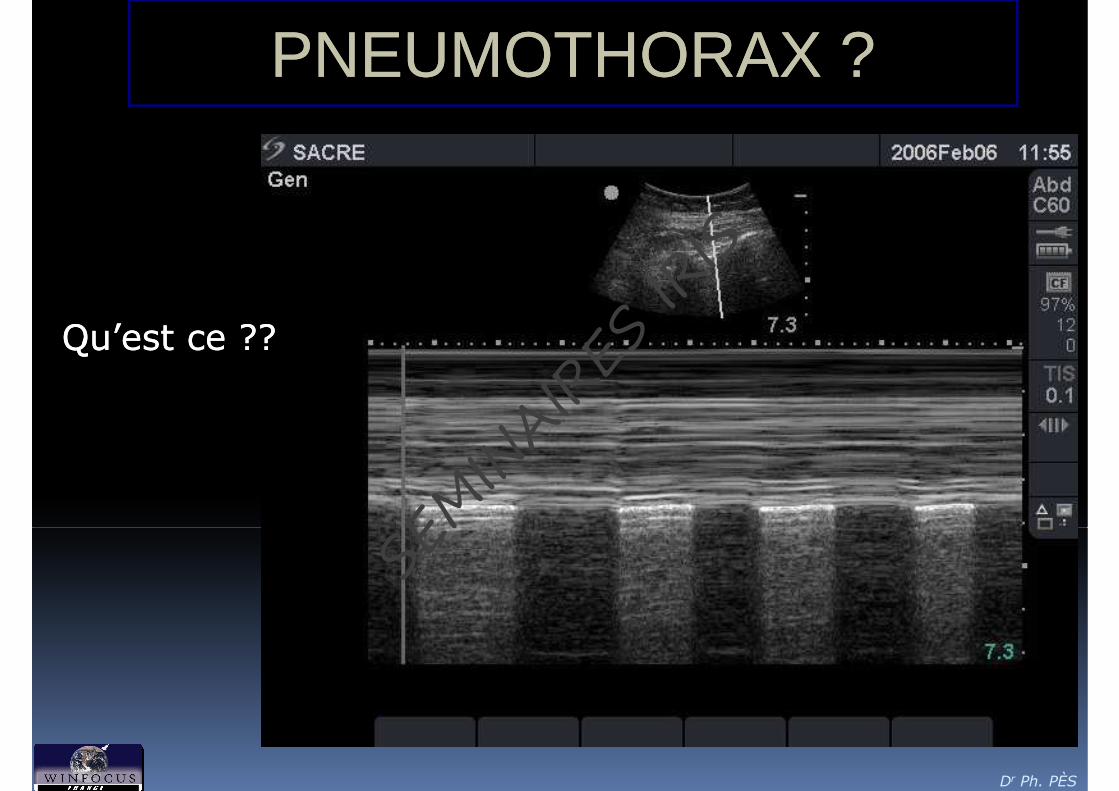
PNEUMOTHORAXPNEUMOTHORAX ??
Qu’est ce ??Qu’est ce ??
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PITFALL…PITFALL…
Mauvais placementMauvais placementde la mire TMde la mire TM
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

LE PULSE LUNGLE PULSE LUNG
Le Pulse LungRespiration Apnée
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

LE PULSE LUNGLE PULSE LUNG
�La présence du Pulse lung signe la présence du
poumon à la paroi...
�Il n'y a donc pas de pneumothorax en regard de la
sonde
Dr Ph. PÈS
sonde SEMIN
AIRE
S IR
IS

PARENCHYMEPARENCHYME
��CONDENSATION ALVÉOLAIRECONDENSATION ALVÉOLAIRE•• Présence d’image de type tissulairePrésence d’image de type tissulaire•• Présence d’image de type tissulairePrésence d’image de type tissulaire
��Hépatisation pulmonaireHépatisation pulmonaire
•• Images punctiforme hyperImages punctiforme hyper--échogèneéchogène��Bronchogramme aériqueBronchogramme aérique
•• Flux doppler vasculaire conservéFlux doppler vasculaire conservé•• Sec ou humide (si liquide associé, facilite Sec ou humide (si liquide associé, facilite
Dr Ph. PÈS
•• Sec ou humide (si liquide associé, facilite Sec ou humide (si liquide associé, facilite la visualisation)la visualisation)
Targhetta R. J. Ultrasound Med. 1992SE
MINAI
RES
IRIS

PARENCHYMEPARENCHYME
��SYNDROME SYNDROME ALVÉOLAIREALVÉOLAIRE
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PARENCHYMEPARENCHYME��CONDENSATION CONDENSATION -- BRONCHOGRAMMEBRONCHOGRAMME
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PARENCHYMEPARENCHYME��CONDENSATION CONDENSATION –– DOPPLERDOPPLER
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PARENCHYMEPARENCHYME��CONDENSATION CONDENSATION -- ÉTIOLOGIEÉTIOLOGIE
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

PARENCHYMEPARENCHYME
��SYNDROME ALVÉOLOSYNDROME ALVÉOLO--INTERSTITIELINTERSTITIEL•• Lignes B (Fusées pleurale)Lignes B (Fusées pleurale) •• Lignes B (Fusées pleurale)Lignes B (Fusées pleurale) •• Nombreuses à très nombreuseNombreuses à très nombreuse•• Réalisant alors l’aspect «Réalisant alors l’aspect « en rideauen rideau »»
Dr Ph. PÈSLichtenstein D. Am. J. Respir. Crit. Care Med., 1997
Image D. LichtensteinImage D. LichtensteinSE
MINAI
RES
IRIS

INTÉRÊTSINTÉRÊTS
Prise en charge de la Dyspnée aiguePrise en charge de la Dyspnée aiguePrise en charge de la Dyspnée aiguePrise en charge de la Dyspnée aigue
* Blue Protocol : D. Lichtenstein CHEST 2008 ; 134:117-125
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

INTÉRÊTSINTÉRÊTS
BLUE ProtocolBLUE Protocol
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

INTÉRÊTSINTÉRÊTS
��Prise en charge de la Dyspnée aigue*Prise en charge de la Dyspnée aigue*��Suivi quotidiens au litSuivi quotidiens au lit��Suivi quotidiens au litSuivi quotidiens au lit��Interventionnel (Interventionnel (AirwayAirway, ponctions), ponctions)
��Ne pas y croireNe pas y croire
ATTENTION…ATTENTION…
Dr Ph. PÈS
��Trop y croireTrop y croire��La Formation…La Formation…
* Blue Protocol : D. Lichtenstein CHEST 2008 ; 134:117-125SE
MINAI
RES
IRIS
CONCLUSIONCONCLUSION
Échographie pleuroÉchographie pleuro--Échographie pleuroÉchographie pleuro--pulmonaire, le nouveau pulmonaire, le nouveau stéthoscope autour du stéthoscope autour du cou des urgentistes…cou des urgentistes…
non... d'aujourd'hui car non... d'aujourd'hui car "Sthetos" veut dire "Sthetos" veut dire paroi et "scopein" voir a paroi et "scopein" voir a travers...travers...
Stéthoscope de demain ?Stéthoscope de demain ?
Dr Ph. PÈS
SEMIN
AIRE
S IR
IS

Dr Ph. PÈS
www.winfocus-france.org
www.winfocus.orgSE
MINAI
RES
IRIS

RESSOURCES INTERNETRESSOURCES INTERNET
�� http://www.winfocushttp://www.winfocus--france.org/france.org/ (Le site de (Le site de WinfocusWinfocus--France)France) �� http://www.ceurf.net/http://www.ceurf.net/ (Le site du (Le site du CercleCercle des des EchographistesEchographistes d’Urgenced’Urgence et de et de RéanimationRéanimation
FrancophonesFrancophones)) �� http://www.ceus.ca/http://www.ceus.ca/ (Le site de la (Le site de la SociétéSociété CanadienneCanadienne d’Echographied’Echographie au au DépartementDépartement de de l’Urgencel’Urgence)) �� http://www.samuhttp://www.samu--dede--france.com/france.com/ (Le site de SAMU de France)(Le site de SAMU de France) �� http://www.samuhttp://www.samu--dede--france.com/france.com/ (Le site de SAMU de France)(Le site de SAMU de France) �� http://www.sfar.org/s/http://www.sfar.org/s/ (Le Site de la (Le Site de la SociétéSociété FrançaiseFrançaise d’Anesthésied’Anesthésie RéanimationRéanimation)) �� http://www.sfaumb.org/http://www.sfaumb.org/ ((SociétéSociété Francophone pour Francophone pour l’Applicationl’Application des des UltrasonsUltrasons en en MédecineMédecine et en et en
BiologieBiologie)) �� http://www.sfmu.org/http://www.sfmu.org/ (Le site de la (Le site de la SociétéSociété Francophone de Francophone de MédecineMédecine d’Urgenced’Urgence)) �� http://www.srlf.org/http://www.srlf.org/ (Le site de la (Le site de la SociétéSociété de de RéanimationRéanimation de Langue de Langue FrançaiseFrançaise)) �� http://www.trauma.org/http://www.trauma.org/ (Site de (Site de ressourcesressources en en TraumatologieTraumatologie)) �� www.ultrason.comwww.ultrason.com (Le site du Centre Francophone de Formation en (Le site du Centre Francophone de Formation en EchographieEchographie))
Dr Ph. PÈS
www.winfocus-france.org
www.winfocus.orgSE
MINAI
RES
IRIS

BIBLIOGRAPHIEBIBLIOGRAPHIELichtenstein D. Lichtenstein D. -- L'échographie générale en réanimation. L'échographie générale en réanimation. 22ème ème Edition Paris, SpringerEdition Paris, Springer--Verlag, Verlag, 20022002..
Lichtenstein D. "Applications nouvelles de l'échographie en Lichtenstein D. "Applications nouvelles de l'échographie en réanimation" MAPAR réanimation" MAPAR 20012001
ACEP Emergency Ultrasound Guidelines ACEP Emergency Ultrasound Guidelines 20012001
Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part
Michael Blaivas, MD and John Christian Fox, MD "Outcome in Michael Blaivas, MD and John Christian Fox, MD "Outcome in Cardiac Arrest Patients Found to Have Cardiac Standstill on the Cardiac Arrest Patients Found to Have Cardiac Standstill on the Bedside Emergency Department Echocardiogram" © Bedside Emergency Department Echocardiogram" © 2001 2001 Academic Emergency Medicine Volume Academic Emergency Medicine Volume 88, Number , Number 6 6166 616--621621
Diku P. Mandavia, MD, Jodi Aragona, MD, Linda Chan, Ph.D., Diku P. Mandavia, MD, Jodi Aragona, MD, Linda Chan, Ph.D., Dennis Chan, MD, et Sean O. Henderson, MD. Ultrasound training Dennis Chan, MD, et Sean O. Henderson, MD. Ultrasound training for emergency physicians. A prospective study.for emergency physicians. A prospective study.Acad Emerg Med, septembre Acad Emerg Med, septembre 2000 2000 ; ; 7 7 : : 10081008--1414..Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part
11." Chest. ." Chest. 2005 2005 Aug;Aug;128128((22):):881881--9595
Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part Beaulieu Y, Marik PE. "Bedside ultrasonography in the ICU: part 22." Chest. ." Chest. 2005 2005 Sep;Sep;128128((33):):17661766--8181..
Targhetta R., Chavagneux R., Bourgeois J.M., Dauzat M., Balmes Targhetta R., Chavagneux R., Bourgeois J.M., Dauzat M., Balmes P., Pourcelot L. P., Pourcelot L. -- Sonographic approach to diagnosing pulmonary Sonographic approach to diagnosing pulmonary consolidation. J. Ultrasound Med., consolidation. J. Ultrasound Med., 1992 1992 ; ; 11 11 : : 667667--672672..
Joyner C.R. Jr., Herman R.J., Reid J.M. Joyner C.R. Jr., Herman R.J., Reid J.M. -- Reflected ultrasound in Reflected ultrasound in the detection and localization of pleural effusion. JAMA, the detection and localization of pleural effusion. JAMA, 1967 1967 ; ; 200 200 : : 399399--402402..
Lichtenstein D., Hulot J.S., Rabiller A., Tostivint I., Meziere G. Lichtenstein D., Hulot J.S., Rabiller A., Tostivint I., Meziere G. --Feasibility and safety of ultrasoundFeasibility and safety of ultrasound--aided thoracentesis in aided thoracentesis in
Acad Emerg Med, septembre Acad Emerg Med, septembre 2000 2000 ; ; 7 7 : : 10081008--1414..
Lichtenstein D., Cluzel P., Grenier P., Coriat P., Rouby J. Lichtenstein D., Cluzel P., Grenier P., Coriat P., Rouby J. -- Apport Apport de l'échographiede l'échographiepulmonaire dans le SDRA. Réanim. Urg., pulmonaire dans le SDRA. Réanim. Urg., 1997 1997 ; ; 6 6 : : 780780..
Chun R, Kirkpatrick AW, Sirois M, Sargasyn AE, Melton S, Hamilton Chun R, Kirkpatrick AW, Sirois M, Sargasyn AE, Melton S, Hamilton DR, Dulchavsky S. “ Where's the tube? Evaluation of handDR, Dulchavsky S. “ Where's the tube? Evaluation of hand--held held ultrasound in confirming endotracheal tube placement.” ultrasound in confirming endotracheal tube placement.” Prehospital Disaster Med. Prehospital Disaster Med. 2004 2004 OctOct--Dec;Dec;1919((44):):366366--99..
Hsieh KS, Lee CL, Lin CC, Huang TC, Weng KP, Lu WH. "Secondary confirmation of endotracheal tube position by ultrasound image." Crit Care Med. 2004 Sep;32(9 Suppl):S374-7.
Raphael DT, Conard FU 3rd. "Ultrasound confirmation of
Dr Ph. PÈS
Feasibility and safety of ultrasoundFeasibility and safety of ultrasound--aided thoracentesis in aided thoracentesis in mechanically ventilated patients. Intens. Care Med., mechanically ventilated patients. Intens. Care Med., 1999 1999 ; ; 25 25 : : 955955--958958..
Lichtenstein D., Meziere G., Biderman P., Gepner A. Lichtenstein D., Meziere G., Biderman P., Gepner A. -- The “lung The “lung point”: an ultrasound sign specific to pneumothorax. Intens. Care point”: an ultrasound sign specific to pneumothorax. Intens. Care Med., Med., 2000 2000 ; ; 26 26 : : 14341434--14401440..
Targhetta R., Bourgeois J.M., Chavagneux R., Coste E., Amy D., Targhetta R., Bourgeois J.M., Chavagneux R., Coste E., Amy D., Balmes P., Pourcelot L. Balmes P., Pourcelot L. -- Ultrasonic signs of pneumothorax: Ultrasonic signs of pneumothorax: preliminary work. J. Clin. Ultrasound, preliminary work. J. Clin. Ultrasound, 1993 1993 ; ; 21 21 : : 245245--250250..
Raphael DT, Conard FU 3rd. "Ultrasound confirmation of endotracheal tube placement." J Clin Ultrasound. 1987 Sep;15(7):459-62.
Schlager D. "Ultrasound detection of foreign bodies and procedure guidance." Emerg Med Clin North Am. 1997 Nov;15(4):895-912. Review.
Atkinson P, Boyle A, Robinson S, Campbell-Hewson G. "Should ultrasound guidance be used for central venous catheterisation in the emergency department?" Emerg Med J. 2005 Mar;22(3):158-64.SE
MINAI
RES
IRIS
BIBLIOGRAPHIEBIBLIOGRAPHIEAzoulayAzoulay E. "Diagnosis and management of pleural effusions in E. "Diagnosis and management of pleural effusions in critically critically iIIiII patients" Rev Mal patients" Rev Mal RespirRespir. . 2005 2005 Feb;Feb;2222((1 1 Pt Pt 11):):7171--99
Jones AE, Kline JA. "Pleural effusions in the critically ill: the Jones AE, Kline JA. "Pleural effusions in the critically ill: the evolving role of bedside ultrasound." evolving role of bedside ultrasound." CritCrit Care Med. Care Med. 2005 2005 Aug;Aug;3333((88):):17571757--6363..
VignonVignon P, P, ChastagnerChastagner C, C, BerkaneBerkane V, V, ChardacChardac E, Francois B, E, Francois B, Normand S, Normand S, BonnivardBonnivard M, M, ClavelClavel M, M, PichonPichon N, N, PreuxPreux PM, PM, MaubonMaubonA, A, GastinneGastinne H. "Quantitative assessment of pleural effusion in H. "Quantitative assessment of pleural effusion in critically ill patients by means of critically ill patients by means of ultrasonographyultrasonography." ." CritCrit Care Med. Care Med. 2005 2005 Aug;Aug;3333((88):):17571757--6363
AzoulayAzoulay E. "Pleural effusions in the intensive care unit." E. "Pleural effusions in the intensive care unit." CurrCurr OpinOpinPulmPulm Med. Med. 2003 2003 Jul;Jul;99((44):):291291--77
GironGiron J, Sans N, J, Sans N, FajadetFajadet P, P, BauninBaunin C "Thoracic ultrasound" Rev C "Thoracic ultrasound" Rev PneumolPneumol ClinClin. . 2000 2000 Apr;Apr;5656((22):):103103--1313
Lichtenstein D, Lichtenstein D, HulotHulot JS, JS, RabillerRabiller A, A, TostivintTostivint I, I, MeziereMeziere G G "Feasibility and safety of ultrasound"Feasibility and safety of ultrasound--aided aided thoracentesisthoracentesis in in mechanically ventilated patients." Intensive Care Med. mechanically ventilated patients." Intensive Care Med. 1999 1999 Sep;Sep;2525((99):):955955--88
Lichtenstein D, Lichtenstein D, MeziereMeziere G, G, BidermanBiderman P, P, GepnerGepner A "The cometA "The comet--tail tail artifactartifact: an ultrasound sign ruling out : an ultrasound sign ruling out pneumothoraxpneumothorax." Intensive ." Intensive
2005 2005 Aug;Aug;3333((88):):17571757--6363
BalikBalik M, M, PlasilPlasil P, P, WaldaufWaldauf P, P, PazoutPazout J, J, FricFric M, M, OtahalOtahal M, M, PachlPachl J. J. "Ultrasound estimation of volume of pleural fluid in mechanically "Ultrasound estimation of volume of pleural fluid in mechanically ventilated patients." Intensive Care Med. ventilated patients." Intensive Care Med. 2006 2006 Feb;Feb;3232((22):):318318--2121
SpronkSpronk PE, ten Hove W, Schultz MJ. "Draining all pleural effusions PE, ten Hove W, Schultz MJ. "Draining all pleural effusions in the intensive care unit?" in the intensive care unit?" CritCrit Care Med. Care Med. 2006 2006 Jan;Jan;3434((11):):269 269 RéponseRéponse aux aux lettreslettres : : CritCrit Care Med. Care Med. 1999 1999 Mar;Mar;2727((33):):583583--77. . CritCritCare Med. Care Med. 2005 2005 Aug;Aug;3333((88):):17571757--6363..
WahidiWahidi MM, Ernst A. "Role of the interventional pulmonologist in MM, Ernst A. "Role of the interventional pulmonologist in the intensive care unit." J Intensive Care Med. the intensive care unit." J Intensive Care Med. 2005 2005 MayMay--Jun;Jun;2020((33):):141141--66..
TuTu CY, Hsu WH, Hsia TC, Chen HJ, Tsai KD, Hung CW, Shih CM CY, Hsu WH, Hsia TC, Chen HJ, Tsai KD, Hung CW, Shih CM
artifactartifact: an ultrasound sign ruling out : an ultrasound sign ruling out pneumothoraxpneumothorax." Intensive ." Intensive Care Med. Care Med. 1999 1999 Apr;Apr;2525((44):):383383--88
Lichtenstein D, Lichtenstein D, MeziereMeziere G, G, BidermanBiderman P, P, GepnerGepner A, A, BarreBarre O. "The O. "The cometcomet--tail tail artifactartifact. An ultrasound sign of alveolar. An ultrasound sign of alveolar--interstitial interstitial syndrome." Am J syndrome." Am J RespirRespir CritCrit Care Med. Care Med. 1997 1997 Nov;Nov;156156((55):):16401640--66
Mayo P. “Safety of UltrasoundMayo P. “Safety of Ultrasound--Guided Guided ThoracentesisThoracentesis in Patients in Patients Receiving Mechanical Ventilation.” Receiving Mechanical Ventilation.” CHEST CHEST 20042004; ; 125125::10591059--10621062
RochRoch A, A, BojanBojan M, Michelet P, M, Michelet P, RomainRomain F, F, BregeonBregeon F, F, PapazianPapazian F, F, AuffrayAuffray J.P «J.P « Usefulness of Usefulness of UltrasonographyUltrasonography in Predicting Pleural in Predicting Pleural Effusions > Effusions > 500 500 mLmL in Patients Receiving Mechanical Ventilation” in Patients Receiving Mechanical Ventilation” Chest Chest 20052005;;127127;;224224--232 232 March March 20052005..
Gann M Gann M JrJr, , SardiSardi A. "Improved results using ultrasound guidance A. "Improved results using ultrasound guidance
Dr Ph. PÈS
TuTu CY, Hsu WH, Hsia TC, Chen HJ, Tsai KD, Hung CW, Shih CM CY, Hsu WH, Hsia TC, Chen HJ, Tsai KD, Hung CW, Shih CM "Pleural effusions in febrile medical ICU patients: chest ultrasound "Pleural effusions in febrile medical ICU patients: chest ultrasound study." Chest. study." Chest. 2004 2004 Oct;Oct;126126((44):):12741274--8080
Lichtenstein DA, Lichtenstein DA, LascolsLascols N, N, PrinPrin S, S, MeziereMeziere G. "The "lung pulse": G. "The "lung pulse": an early ultrasound sign of complete an early ultrasound sign of complete atelectasisatelectasis." Intensive Care ." Intensive Care Med. Med. 2003 2003 Dec;Dec;2929((1212):):21872187--9292..
AA--lines and Blines and B--lines: lung ultrasound as a bedside tool for lines: lung ultrasound as a bedside tool for predicting pulmonary artery occlusion pressure in the critically ill. predicting pulmonary artery occlusion pressure in the critically ill. Lichtenstein DA, Lichtenstein DA, MezièreMezière GA, GA, LagoueyteLagoueyte JF, JF, BidermanBiderman P, Goldstein P, Goldstein I, I, GepnerGepner A. Chest. A. Chest. 2009 2009 Oct;Oct;136136((44):):10141014--2020..
Gann M Gann M JrJr, , SardiSardi A. "Improved results using ultrasound guidance A. "Improved results using ultrasound guidance for central venous access." Am Surg. for central venous access." Am Surg. 2003 2003 Dec;Dec;6969((1212):):11041104--77..
Miller AH, Roth BA, Mills TJ, Woody JR, Miller AH, Roth BA, Mills TJ, Woody JR, LongmoorLongmoor CE, Foster B. CE, Foster B. "Ultrasound guidance versus the landmark technique for the "Ultrasound guidance versus the landmark technique for the placement of central venous catheters in the emergency placement of central venous catheters in the emergency department." department." AcadAcad EmergEmerg Med. Med. 2002 2002 Aug;Aug;99((88):):800800--55..
Confirmation of Confirmation of endotrachealendotracheal intubation by combined intubation by combined ultrasonographicultrasonographic methods in the Emergency Department.methods in the Emergency Department.Park SC, Park SC, RyuRyu JH, JH, YeomYeom SR, SR, JeongJeong JW, Cho SJ JW, Cho SJ EmergEmerg Med Med AustralasAustralas. . 2009 2009 Aug;Aug;2121((44):):293293--77..SE
MINAI
RES
IRIS
MERCI DE VOTRE ATTENTIONMERCI DE VOTRE ATTENTION
Dr Ph. PÈSMerciMerci à Daniel, Jeanà Daniel, Jean--mariemarie et Ray pour et Ray pour leurleur aide et aide et leursleurs imagesimages
Des questions ?Des questions ?SE
MINAI
RES
IRIS