COMPLICATIONS MÉCANIQUES DE L’INFARCTUS: Qu’est-ce que...
57
Mario Sénéchal, MD, FRCPC Professeur adjoint département de Médecine Institut Universitaire de Cardiologie et de Pneumologie de Québec 22 Novembre 2016 COMPLICATIONS MÉCANIQUES DE L’INFARCTUS: Qu’est-ce que le (la) technicien(ne) et le cardiologue devraient savoir ?
Transcript of COMPLICATIONS MÉCANIQUES DE L’INFARCTUS: Qu’est-ce que...

Mario Sénéchal, MD, FRCPC Professeur adjoint département de Médecine
Institut Universitaire de Cardiologie et de Pneumologie de Québec
22 Novembre 2016
COMPLICATIONS MÉCANIQUES DE L’INFARCTUS: Qu’est-ce que le
(la) technicien(ne) et le cardiologue devraient savoir ?


PLAN
1. Discuter de l’IM organique post infarctus
(rupture de pilier)
2. Discuter de la CIV post infarctus
3. Discuter de la rupture subaiguë post infarctus
fonctionnelle post infarctus
4. Discuter brièvement de l’IM fonctionnelle
post-infarctus

RESEARCH ARTICLE Open Access
Long-term survival after mitral valve surgeryfor post-myocardial infarction papillary muscleruptureWobbe Bouma1,4*, Inez J Wijdh-den Hamer1, Bart M Koene1, Michiel Kuijpers1, Ehsan Natour1, Michiel E Erasmus1,Jayant S Jainandunsing2, Iwan CC van der Horst3, Joseph H Gorman III4, Robert C Gorman4
and Massimo A Mariani1
Abstract
Background: Papillary muscle rupture (PMR) is a rare, but dramatic mechanical complication of myocardialinfarction (MI), which can lead to rapid clinical deterioration and death. Immediate surgical intervention isconsidered the optimal and most rational treatment, despite high risks. In this study we sought to identifyoverall long-term survival and its predictors for patients who underwent mitral valve surgery for post-MI PMR.
Methods: Fifty consecutive patients (mean age 64.7 ± 10.8 years) underwent mitral valve repair (n = 10) orreplacement (n = 40) for post-MI PMR from January 1990 through May 2014. Clinical data, echocardiographicdata, catheterization data, and surgical data were stored in a dedicated database. Follow-up was obtained inJune of 2014; mean follow-up was 7.1 ± 6.8 years (range 0.0-22.2 years). Univariate and multivariate Cox proportionalhazard regression analyses were performed to identify predictors of long-term survival. Kaplan-Meier curves werecompared with the log-rank test.
Results: Kaplan-Meier cumulative survival at 1, 5, 10, 15, and 20 years was 71.9 ± 6.4%, 65.1 ± 6.9%, 49.5 ± 7.6%,36.1 ± 8.0% and 23.7 ± 9.2%, respectively. Univariate and multivariate analyses revealed logistic EuroSCORE ≥40%and EuroSCORE II ≥25% as strong independent predictors of a lower overall long-term survival. After removalof the EuroSCOREs from the model, preoperative inotropic drug support and mitral valve replacement (MVR)without (partial or complete) preservation of the subvalvular apparatus were independent predictors of a loweroverall long-term survival.
Conclusions: Logistic EuroSCORE ≥40%, EuroSCORE II ≥25%, preoperative inotropic drug support and MVRwithout (partial or complete) preservation of the subvalvular apparatus are strong independent predictors of alower overall long-term survival in patients undergoing mitral valve surgery for post-MI PMR. Whenever possible, thesubvalvular apparatus should be preserved in these patients.
Keywords: Myocardial infarction, Papillary muscle (rupture), Mitral regurgitation, Mitral valve repair, Mitral valvereplacement, Outcome
* Correspondence: [email protected] of Cardiothoracic Surgery, University of Groningen, UniversityMedical Center Groningen, Groningen, the Netherlands4Gorman Cardiovascular Research Group, University of Pennsylvania, Hospitalof the University of Pennsylvania, Philadelphia, PA, USAFull list of author information is available at the end of the article
© 2015 Bouma et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Bouma et al. Journal of Cardiothoracic Surgery (2015) 10:11 DOI 10.1186/s13019-015-0213-1
Bouma, Journal of Cardiothoracic Surgery, 2015

INCIDENCE et MORTALITÉ
• ’80-’90: 1-5%
• >2000: <0,5%
• 80% < 7 jours
• † 50% < 24 heures si tx médical .
• 80% 1 er semaine

BackgroundIn the current era of early reperfusion with primary per-cutaneous coronary intervention (PCI) following acuteST-elevation myocardial infarction (STEMI), the inci-dence of post-myocardial infarction papillary musclerupture (post-MI PMR) has dropped from 1-5% in theeighties and early nineties to <0.5% in recent years [1-3].Although rare, PMR is still a dramatic complication,which can lead to rapid clinical deterioration and death[1]. Approximately 80% of ruptures occur within 7 daysafter MI, but a delayed rupture several weeks or monthsafter MI is also possible [1,2,4]. The natural history ofpost-MI PMR is extremely unfavorable and under med-ical treatment alone mortality may be as high as 50% inthe first 24 hours (especially when PMR is complete),and as high as 80% in the first week [4,5].Since the first mitral valve replacement (MVR) for
post-MI PMR in 1965 [6], several reports have empha-sized that immediate surgical intervention is the optimaland most rational treatment for acute PMR, despite highrisks [2,4,7]. Although mitral valve repair may improveoutcome due to a better preservation of postoperativeleft ventricular (LV) function [8-13], MVR is generallypreferred in these haemodynamically unstable, high-riskpatients [7,14-18].In this study we sought to identify overall long-term
survival and its predictors for patients who underwentmitral valve surgery for post-MI PMR.
MethodsThis study was conducted in accordance with the guide-lines of the University Medical Center Groningen Insti-tutional Review Board.
PatientsBetween January 1990 and May 2014, 50 consecutive pa-tients underwent mitral valve surgery for moderate-to-severe (grade 3+) or severe (grade 4+) mitral regurgitation(MR) caused by post-MI PMR. Clinical data, echocardio-graphic data, catheterization data, and surgical data werestored in a dedicated database. Baseline patient characteris-tics are summarized in Table 1. All patients had a docu-mented MI before PMR. Infarct location was determinedelectrocardiographically and echocardiographically (by thedetection of wall motion abnormalities). Four patients (8%)had a history of congestive heart failure, 12 patients (24%)had hypertension, 9 patients (18%) had diabetes mellitus,16 patients (32%) were smokers, 6 patients (12%) hadhypercholesterolemia, 7 patients (14%) were obese (bodymass index > 30 kg/m2), 2 patients (4%) had peripheral vas-cular disease, 7 patients (14%) had a family history ofcoronary artery disease, 1 patient (2%) had chronic renaldisease, 3 patients (6%) had chronic obstructive pulmonarydisease, and 5 patients (10%) had cerebrovascular disease.
Table 1 Preoperative patient data (n = 50)Variablea Value
Age, years 64.7 ± 10.8
Gender
Male 36 (72)
Female 14 (28)
NYHA functional class
Class III 7 (14)
Class IV 43 (86)
EuroSCORE I (logistic), % 29.9 ± 22.6
EuroSCORE II, % 19.6 ± 14.5
Previous myocardial infarction 50 (100)
Inferior and/or posterior 34 (68)
Inferoposterolateral 13 (26)
Anterolateral 9 (18)
Coronary artery disease 50 (100)
Left main stenosis 3 (6)
One-vessel disease 24 (48)
Two-vessel disease 18 (36)
Three-vessel disease 8 (16)
Infarct related artery
Left anterior descending coronary artery 1 (2)
Left circumflex coronary artery 29 (58)
Right coronary artery 20 (40)
Previous percutaneous coronary intervention 14 (28)
Previous cardiac surgery 0 (0)
Preoperative grade of mitral regurgitation
3+ (moderate) 1 (2)
4+ (severe) 49 (98)
Preoperative LV function
Normal (EF >50%) 34 (68)
Moderately impaired (EF 30-50%) 11 (22)
Severely impaired (EF <30%) 5 (10)
Heart rhythm
Sinus rhythm 45 (90)
Atrial fibrillation 5 (10)
Pacemaker 0 (0)
Pulmonary artery pressure
Systolic/diastolic, mmHg 45 ± 13/25 ± 10
Mean, mmHg 32 ± 10
Pulmonary capillary wedge pressure, mmHg 24 ± 14
Mechanical ventilation 23 (46)
Inotropic drug support 28 (56)
Intra-aortic balloon pump 23 (46)
Bouma et al. Journal of Cardiothoracic Surgery (2015) 10:11 Page 2 of 10
Echocardiography and coronary angiographyAll patients underwent preoperative echocardiography(transthoracic (TTE) and/or transesophageal (TEE)) andcoronary angiography. TTE accurately revealed the diag-nosis of PMR in 20 patients (40%). PMR was suspectedin the remaining 30 patients (60%) and confirmed withTEE in 24 patients (48%). In 6 patients (12%) the exactmechanism of MR remained inconclusive. Left ventricularfunction was assessed by echocardiography. In addition,wall motion abnormalities were documented for infarctlocalization.
Surgical techniqueSurgical data is summarized in Table 2.Patients were considered to undergo a salvage operation
when brought to the operating room under cardiopulmo-nary resuscitation, an emergency operation when broughtto the operating room directly from the catheterization labor intensive care unit because of haemodynamic instability,and an urgent operation when operated on during thesame hospitalization as for angiography because their dis-charge was deemed medically unreasonable [19]. Other-wise the operation was considered elective.PMR was confirmed during surgery in all patients.
When a papillary muscle (PM) was divided into severalheads, rupture of a single head was defined as “partial”[11,12]. In case of detachment of the main insertion of ahead which still remained fixed to the remnant PM viamuscular bridges, rupture was defined as “incomplete”[11,12]. Rupture of the whole PM was defined as “totaland complete” [11,12]. Posteromedian papillary musclerupture (PMPMR) occurred in 44 patients (88%), antero-lateral papillary muscle rupture (ALPMR) occurred in 5patients (10%), and combined complete PMPMR andALPMR occurred in 1 patient (2%). Complete PMPMRoccurred in 15 patients (39%), incomplete PMPMR oc-curred in 2 patients (5%), and partial PMPMR occurredin 25 patients (57%). Complete ALPMR occured in 4 pa-tients (80%), incomplete ALPMR did not occur, and partialALPMR occurred in 1 patient (20%). Isolated posterior mi-tral valve leaflet (PMVL) prolapse was found in 15 patients(30%), isolated anterior mitral valve leaflet (AMVL) pro-lapse was found in 12 patients (24%), and combined pro-lapse was found in 23 patients (46%).Myocardial protection was carried out using mod-
erate systemic hypothermia and antegrade or combined
antegrade and retrograde cardioplegia. The mitral valvewas exposed with a left atriotomy (in 36 patients), with atransseptal approach (in 13 patients), or with a leftventriculotomy (in one patient with a ventricular septalrupture). Surgeon’s choice dictated treatment strategy.Ten patients underwent mitral valve repair (20%). Themitral valve was repaired by reimplantation of the PM inthe LV wall combined with an annuloplasty ring in 1 pa-tient, by reimplantation of the PM in the correspondingPM with a sandwiched pledget-reinforced polytetrafluor-ethylene (PTFE) suture combined with an annuloplastyring in 2 patients, by quadrangular resection of P2 com-bined with an annuloplasty ring in 6 patients, and bycommissuroplasty combined with an annuloplasty ring in1 patient. Mitral valve repair with a quadrangular resectionof P2 combined with an annuloplasty ring failed intraoper-atively in 1 patient and resulted in MVR. Concomitant
Table 1 Preoperative patient data (n = 50) (Continued)
Serum creatinine, μmol/L 159 ± 94
Acute renal failure 10 (20)
Cardiogenic shock 33 (66)aData are presented as mean ± standard deviation or number (%).EF = ejection fraction; LV = left ventricle; NYHA = New York Heart Association.
Table 2 Surgical data (n = 50)Variablea Value
Mitral valve surgery
Salvage 2 (4)
Emergent 31 (62)
Urgent 11 (22)
Elective 6 (12)
Timing of mitral valve surgery
Surgery ≤7 days after MI 29 (58)
Surgery >7 days and ≤30 days after MI 9 (18)
Surgery >30 days after MI 12 (24)
Mitral valve replacement 40 (80)
Mechanical prosthesis 36 (90)
Bioprosthesis 4 (10)
Preservation of the SA (partial or complete) 26 (65)
AMVL and attached SA (partial or complete) 5 (19)
PMVL and attached SA (partial or complete) 14 (54)
AMVL and PMVL and attached SA (partial or complete) 7 (27)
Mitral valve repair 10 (20)
Concomitant surgery 28 (56)
Coronary artery bypass grafting 24 (48)
Septal rupture closure 2 (4)
Aortic valve replacement 1 (2)
Tricuspid valve plasty 2 (4)
Duration of surgery, min 278 ± 88
Cardiopulmonary bypass time, min 179 ± 67
Aortic cross-clamp time, min 98 ± 35
Intraoperative IABP requirement 26 (52)aData are presented as mean ± standard deviation or number (%).AMVL = anterior mitral valve leaflet; IABP = intra-aortic balloon pump;MI = myocardial infarction; PMVL = posterior mitral valve leaflet;SA = subvalvular apparatus.
Bouma et al. Journal of Cardiothoracic Surgery (2015) 10:11 Page 3 of 10
Bouma, Journal of Cardiothoracic Surgery, 2015

Bouma, Journal of Cardiothoracic Surgery, 2015
procedures were performed in 28 patients (56%) and con-comitant coronary artery bypass grafting (CABG) was per-formed in 24 patients (48%) (Table 2). After weaning fromcardiopulmonary bypass mitral valve competence was con-firmed with TEE.Patients who underwent mitral valve repair or MVR
with a bioprosthesis received acenocoumarol treatmentfor 3 months and patients who underwent MVR with amechanical prosthesis were put on lifelong acenocou-marol treatment. In addition, patients who underwentconcomitant CABG also received lifelong acetylsalicylicacid treatment.
Follow-upFollow-up was obtained in June of 2014 directly fromoutpatient visits or by telephone interview with thepatient and/or the referring physician. No patient waslost to follow-up. Overall long-term mortality was de-fined as death of any cause after surgery (and includedin-hospital deaths).
StatisticsContinuous variables were expressed as mean ± standarddeviation. Categorical variables were expressed aspercentages.Cox proportional-hazard regression analysis was used
to determine univariate predictors and multivariateindependent predictors of overall long-term survival.Univariate variables with P < 0.10 were included in themultivariate analysis. Age and gender were included in allmultivariate models, irrespective of the results of univariateanalysis. Multivariate analysis was performed with the lo-gistic EuroSCORE (continuous variable) (model 1), withthe EuroSCORE II (continuous variable) (model 2), withlogistic EuroSCORE ≥40% (categorical variable) (model 3),with EuroSCORE II ≥25% (categorical variable) (model 4),and without the EuroSCOREs (model 5). Multivariate Coxproportional-hazard regression analysis by means of a for-ward stepwise algorithm (cutoff for entry and removal setat a significance level of 0.05) was performed to identify in-dependent predictors of overall long-term survival. Hazardratios were reported with 95% confidence intervals (CI).Goodness of fit of the final model was assessed withthe Chi square (χ2) goodness-of-fit test (the log likelihoodstatistic).Separate multivariate analyses were performed with a
cutoff value of 40% for the logistic EuroSCORE (model 3)and a cutoff value of 25% for the EuroSCORE II (model 4).We have previously shown that these values were optimalcutoff values in predicting in-hospital mortality [13]. TheEuroSCOREs were included as categorical variables atthese cutoff values to determine if they could also predictoverall long-term survival.
Survival curves were calculated and presented accord-ing to the product-limit method of Kaplan and Meier.Cumulative survival was expressed as percentage ±standard error. Survival was expressed as mean ± standarderror. Differences in survival between groups were com-pared with the log-rank test.All calculations were performed using a commercially
available statistical package (IBM SPSS Statistics 21.0;IBM Corporation, Chicago, IL, USA). Statistically signifi-cant differences were established at P < 0.05.
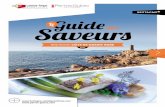
ResultsOverall long-term survivalMean follow up was 7.1 ± 6.8 years (range: 0.0 to22.2 years). Total follow-up was 353.1 patient-years.Actuarial overall long-term survival after mitral valvesurgery for post-MI PMR is shown in Figure 1. Kaplan-Meier cumulative survival at 1, 5, 10, 15, and 20 yearswas 71.9 ± 6.4%, 65.1 ± 6.9%, 49.5 ± 7.6%, 36.1 ± 8.0% and23.7 ± 9.2%, respectively. Causes of death are shown inTable 3. At last follow-up all survivors (n = 21) were inNYHA functional class I or II.
Predictors of overall long-term survivalUnivariate and multivariate Cox regression analyses oflong-term survival are shown in Table 4. Multivariateanalysis was performed with the logistic EuroSCORE(continuous variable) (model 1), with the EuroSCORE II(continuous variable) (model 2), with logistic Euro-SCORE ≥40% (categorical variable) (model 3), withEuroSCORE II ≥25% (categorical variable) (model 4),and without the EuroSCOREs (model 5).
Figure 1 Kaplan-Meier actuarial overall long-term survival aftermitral valve surgery for post-MI PMR. Pts = patients; + = censored.
Bouma et al. Journal of Cardiothoracic Surgery (2015) 10:11 Page 4 of 10

-35% des ruptures de piliers sont partielles et habituellement seulement visible à l’ETO
Moursi et al., Circulation, 1996

-Sensibilité de l’ETT 65 %
-ETO 95%


LVEF pre 53±7 NA LVEF pre 50±13 NA 0.51
LVEF post 46 NA LVEF post 41 NA
PMR PMR Ant 5 28 Ant 3 16 0.45
Post 13 72 Post 16 84 Jet Jet
Excentric 2 11 Excentric 18 95 <0.0001 Central 16 89 Central 1 5
Coanda Effect 0 0
Coanda Effect 10 53 <0.0001
Cordage 0 0 Cordage 10 53 <0.0001
Prolapse 0 0 Prolapse 15 79 <0.0001
TTE 13 72 TTE 6 32 0.0217
TEE 18 100 TEE 19 100 1.0
Données échocardiographiques: ruptures complètes vs. partielles




La règle de 50
1. Les patients avec rupture de pilier ont souvent une FE ≧ 50%;
2. Environ 50% des patients avec une rupture de pilier avaient une rupture partielle;
3. Environ 50% des patients avec rupture partielle de pilier avaient une hémodynamie stable initiallement (pas de choc initiale);
4. Si rupture de pilier documenté et patient stable hémodynamiquement, réfléchir comme si la rupture était complète c’est-à-dire, chirurgie urgente.

Qu’est-ce que le (la) technicien(ne) devrait savoir ? 1. En présence d’un infarctus toujours rechercher
l’insuffisance mitrale (faire doppler couleur dans
toutes les incidences a/n de la valve mitrale);
2. Si IM significative (≧ modérée) s’interroger sur le
mécanisme (tenting ? Restriction feuillet postérieur ?
Rupture de pilier ?);
3. Se méfier du patient stable hémodynamiquement;
4. Si IM significative (≧ modérée) scanner/zoom les piliers
dans toutes les incidences.

Qu’est-ce que le cardiologue devrait savoir ?
1. Avoir la même démarche que le (la) technicien (ne);
2. On ne trouve pas ce que l’on ne cherche pas !!;
3. Se souvenir de la règle de 50%;


Risk factors of mortality after surgical correction of ventricular septaldefect following myocardial infarction: Retrospective analysis andreview of the literature
Alexandre Cinq-Mars a, Pierre Voisine b, François Dagenais b, Éric Charbonneau b, Frédéric Jacques b,Dimitris Kalavrouziotis b, Jean Perron b, SiamakMohammadi b, Michelle Dubois a, Florent Le Ven c, Paul Poirier c,Kim O'Connor c, Mathieu Bernier c, Sébastien Bergeron c, Mario Sénéchal c,⁎a Research Center, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Québec City, Canadab Department of Cardiac Surgery, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Québec City, Canadac Department of Cardiology, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Québec City, Canada
a b s t r a c ta r t i c l e i n f o
Article history:Received 5 October 2015Received in revised form 30 November 2015Accepted 12 December 2015Available online 14 December 2015
Background: Rupture of the ventricular septum following acutemyocardial infarction (AMI) is an uncommon butserious complication, usually leading to congestive heart failure and cardiogenic shock. Surgical repair is the onlydefinitive treatment for this condition.Methods:We reviewour experience of surgical repair of post-infarction ventricular septal defects (VSDs), analyzethe associated risk factors and outcomes, and do a complete review of the literature. A retrospective study wasperformed on 34 consecutive patients who had undergone surgical repair for VSDs following AMI from Decem-ber 1991 to July 2014. Preoperative, clinical and echocardiographic variables were studied by uni-and multivar-iate analyses.Results: Mortality was analyzed for the entire group of patients. Mean age was 69 ± 7 years with 44% women.VSDs were anterior in 11 (32%) and posterior in 23 (68%) patients. A majority, 24 (71%) patients were incardiogenic shock. Median interval frommyocardial infarction to VSDs repair was 7 days. The 30 days operativemortalitywas 65%.Mortalitywithin the posterior VSDs groupwas 74% and the anterior VSDs groupwas 46% (P=0.14). Concomitant coronary artery bypass graft (CABG) did not influence early or late survival.Multivariate anal-ysis identified older age (HR = 1.11, P = 0.0001) and shorter time between AMI and surgery (HR = 0.90, P =0.015) as independent predictors of 30-day and long-term mortality.Conclusion: In conclusion, surgical repair of post-AMI VSDs carries a high operative mortality. An algorithm oftreatment for the management of these patients is suggested.
© 2015 Published by Elsevier Ireland Ltd.
Keywords:Ventricular septal defectMyocardial infarctionRisk factorsOutcomes
1. Introduction
Despite significant improvements in overall mortality for patientswith acute myocardial infarction (AMI) over the last two decades, theoutcome of patients who develop ventricular septal defects (VSDs) re-mains poor. Rupture of the ventricular septum followingmyocardial in-farction is an uncommon complication, with contemporary seriesreporting an incidence ranging between 0.17 and 0.31% of patients pre-sentingwith AMI [1]. Transmural AMI generating a VSDs affects ventric-ular function and has the potential to generate a macro-reentry circuit,inducing congestive heart failure, ventricular tachyarrhythmia and car-diogenic shock. Unpredictable hemodynamic deterioration is the norm
in most patients in the days and weeks following VSDs, and reports oflong-term survival without corrective surgery are extremely rare. Infact, surgical repair is the only definitive treatment for these patientssince medical management has 30-day mortality approaching 100%[2]. However, complex surgical repairs are characterized by mortalitynear 50% inmulticentre reports [3–6].Many risk factors have been iden-tified to explain the poor outcomes of surgical repair for post-AMI VSDs[7]. Cardiogenic shock with hemodynamic instability, emergencysurgery, early repair, right ventricular dysfunction, VSDs of posterior lo-cation, renal impairment and complex VSDs represent common poten-tial risk factors [3]. Under optimal management, 30-day mortality ratesrange from 19 to 54% [2–7].
In this retrospective study,we have analyzed our experience regard-ing the surgical treatment of patients with VSDs following AMI in thepast decades. In addition, a review of the literature has been performedto identify key points in the management of patients with post-AMIVSDs.
International Journal of Cardiology 206 (2016) 27–36
⁎ Corresponding author at: Institut Universitaire de Cardiologie et de Pneumologie deQuébec, 2725, Chemin Sainte-Foy, Quebec, Quebec G1V 4G5, Canada.
E-mail address: [email protected] (M. Sénéchal).
http://dx.doi.org/10.1016/j.ijcard.2015.12.0110167-5273/© 2015 Published by Elsevier Ireland Ltd.
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Multivariate analysis identified older age and shorter time betweenAMI and surgery as independent predictors of 30-day and long-termmortality.
Long-term survival is presented in Fig. 1 and results from the statis-tical analysis are presented in Table 5.
4. Discussion
Post-AMI VSDs is a serious clinical problem with high mortalityrate. In recent years, early and efficient revascularization therapy formyocardial infarction has contributed to a decreased incidence ofVSDs [10]. However, management of patients with post-AMI VSDs re-mains a challenge. Furthermore, the spectrum of surgical patientsseems to switch toward patients with more extensive heart failure, he-modynamic compromise and associated comorbidities. Our experienceregarding mortality and risk factors are in accordance with previouslypublished reports. In the following, we compare our data to the avail-able literature and describe best evidence risk factors. Conventionaland non-conventional management for patients with post-AMI VSDsare also described.
4.1. Risk factors
4.1.1. Cardiogenic shockOur experience identified low diastolic blood pressure as a univari-
ate significant risk factor for operative mortality. Patients with diastolicpressure under 60 mm Hg are in cardiogenic shock, therefore carryingan extensive deleterious condition usually leading to poor survivalrates despite aggressive treatments. In our experience, patients wereoften rushed to surgery under emergency status because of this
complication. In patients developing VSDs following AMI, prognosis isdependent on the degree of hemodynamic compromise. Consequently,many authors have identified the development of cardiogenic shock asthe single most important predictor of mortality [2,3,5,6,11–14] espe-cially if concomitant right ventricular dysfunction develops [15]. Studieshave shown that the most important factor contributing to cardiogenicshock is the typically large infarct present in patients with VSDs. Inpatients with cardiogenic shock and in the absence of surgical interven-tion, death is inevitable. Results of surgical treatment regarding post-AMI VSDs from many series demonstrated the importance of thisparameter on operative mortality [2,3,5,6,8,11,12,14–17]. Cummingset al. revealed an operative mortality ranging from 13% to 42% in ab-sence of cardiogenic shock, compared to a range of 44% to 58% for pa-tients in cardiogenic shock [8]. Others have reported series in whichcardiogenic shock complicated more than 80% of post-AMI VSDs [8].Therefore, it has been suggested that early operative closure of VSDsshould not be conducted in patients with cardiogenic shock but appro-priately delayed until hemodynamic stabilization, whenever possible[15,18].
4.1.2. Early surgeryA recent publication from the Society of Thoracic Surgeons National
Database (STS Database, n = 2876) showed that mortality of patientsvaried significantly depending on timing of surgery. Patients whounderwent surgery within 7 days from the symptoms onset had a 54%mortality compared with 18% mortality if repair was delayed morethan 7 days after VSDs post-AMI initial presentation [11]. Moreover,Serpytis et al. [18] recently exposed early outcomes of 41 patientswith post-AMI VSDs. The report showed a 100% survival rate for all pa-tients (n=33)who underwent surgery after 3–4weeks of stabilizationand a 100% mortality rate when operated within the first 10 days (n =5). Our data confirmed that a shorter time betweenAMI and surgery is asignificant risk factor for 30-day operativemortality. The improved out-comemay be related to evolution of the infarct and improved stability ofthe cardiac tissue allowing amore effective repair in an elective delayedsurgical procedure. However, it may represent a survival bias, as earlysurgery is usually performed in individuals with marked hemodynamicinstability and circulatory compromise, making immediate surgicalmanagement the only viable option for them.
4.1.3. Right ventricular dysfunctionThe importance of right ventricular dysfunction on outcome was
demonstrated by Cummings et al. [8]. A higher proportion of right ven-tricular infarct extension is found in VSDs-generating AMI, independentof their anterior or inferior location. In fact, the incidence of right ven-tricular infarction in the post-AMI VSDs group was 100% vs 28% in thenon-VSDs group (P b 0001). Dysfunction of the right ventricle may bethe consequence of right ventricular infarction, right ventricularischemia, and/or pressure–volume abnormalities. VSDs following AMI
Table 4Outcomes and mortality etiology.
Variables Results
n = 34 (%)
Survival 12 (35)30 day mortality 22 (65)All over hospital mortality 23 (68)
Anterior VSD mortality 5/11 (46)Posterior VSD mortality 17/23 (74)
MortalityCauses: 1: Cardiac 18/22 (82)
2: Multi-organ failure 2/22 (9)3: Infection 1/22 (5)4: Respiratory 1/22 (5)
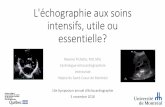
Fig. 1. Kaplan–Meier survival curve.
Table 5Significant predictors of operative mortality in univariate and multiple Cox proportional-hazard regression models.
Univariate Multivariate
HR [95% conf.interval]
P-value HR [95% conf.interval]
P-value
Age 1.10 1.04–1.17 0.002 1.11 1.04–1.18 0.0001BMI 0.88 0.79–0.99 0.04 – – –VSD localization 2.45 0.96–6.25 0.06 – – –BP diastole 0.96 0.94–0.99 0.016 – – –Reoperation 0.28 0.08–0.95 0.042 – – –Bypass time 1.11 1.03–1.19 0.005 – – –Cross-clamp time 1.13 1.00–1.28 0.05 – – –Time between AMIand operation
0.93 0.88–0.99 0.045 0.90 0.83–0.98 0.015
VSD: ventricular septal defect, BP: blood pressure.
29A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

number of patients included in our cohortmay explain the lack of statis-tical significance of the variable in the analysis.
4.2.5. Mechanical assistanceBecause emergency operative repair carries a high mortality, pa-
tients in the acute phase of shock may require aggressive mechanicalsupport in order to delay surgical repair. The use of mechanical circula-tory support allows time for the hemodynamic status to stabilized. Evenif patch closure of the VSDs can effectively repair the defect and elimi-nate the shunt in the acute setting, patients with extensive infarctionand pump failure may need a mechanical support strategy to avoid fur-ther deterioration. Attempts to bridge patients with post-AMI VSDs arecomplicated by technical difficulties such as necrotic muscle at the site
of left ventricular apical cannulation as well as previously placedpatches for VSDs repair [43]. Many strategies have been described tobridge patients from acute phase to destination therapy and decisionsregarding the best therapeutic option.
4.2.6. Percutaneous ventricular assist deviceIntra-aortic balloon pump is used in patients with post-AMI VSDs to
decrease left-to-right shunt and left ventricular afterload. As seen in ourexperience, overall surgical mortality rates remain high despite the useof intra-aortic balloon pump, demonstrating the limit of this approachin patients with extended hemodynamic compromise. The use of a per-cutaneous ventricular assistance device (Impella Recover LP 5.0 SupportSystem, ABIOMED, Danvers, Mass) has proven useful in achieving
Table 6Best evidence studies describing risk factors and operative mortality in patient with surgical repair of VSD post-AMI.
Author, date, journal Patient group Significant risk factors identified Operativemortality(within 30 daysof operation)
Comments
Cardiogenicshocka
Rightventriculardysfunctionb
Earlyrepairc
PosteriorVSD
Huang S.M. et al. (2015), Journalof Cardiothoracic Surgery
Single center cohort study(1995–2013), n = 47
No N/A Yes N/A 36% (n = 17) Overall survival at 6 years was41.1 ± 2.2%
Pang P. Y.k. et al. (2013), Journalof Cardiothoracic Surgery
Single center cohort study(1999–2011), n = 38
Yes Yes Yes No 40% (n = 15) Overall survival at 10 years was44.4 ± 8.4%.
Rohn V. et al. (2013), PragueMedical Report
Single center cohort study(2004–2012), n = 25
Yes No N/A Yes 40% (n = 10) The most common cause of deathwas persistent low cardiac output andmultiorgan failure.
Arnaoutakis G. J. et al. (2012),Annals of Surgery
Database from the Society ofThoracic Surgeons(1999–2010), n = 2800
Yes N/A Yes N/A 43% (n = 1235) Anatomic site of VSD rupture (posteriorvs anterior) is not contained in the STSACSD, and this operative factor was notanalyzed.
Sibal A.K. et al. (2009), Heart,Lung and Circulation
Single center cohort study(1992–2006), n = 36
Yes Yes Yes Yes 53% (n = 19) The subgroup of inferior VSD withshock had mortality rates similar tomedically managed groups publishedin literature (90%).
Coskun O.K. et al. (2009), Journalof Cardiothoracic Surgery
Single center cohort study(1990–2005), n = 41
Yes N/A Yes Yes 34% (n = 14) All patients who underwent the surgicalrepair later than day 36 survived.
Vargas-Barrón J. et al. (2005),The American Journal ofCardiology
Two large teachinginstitutionsstudy, n = 17
N/A Yes N/A No 59% (n = 10) Mortality rate was higher in patientswho had complex rupture (78% vs 38%,P b 0.001) and in those who had RVextension (71% vs 29%, P b 0.001).
Labrousse et al. (2002),European Journal ofCardio-thoracic Surgery
Single center cohort study(1971–2001), n = 85
Yes Yes N/A No 42% (n = 36) The fifteen patients who were operatedon more than 15 days after theoccurrence of the VSD were excluded.
Deja A. et al. (2000), EuropeanJournal of Cardio-thoracicSurgery
Single center cohort study(1986–1998), n = 117
Yes No Yes No 35% (n = 35) Neither did the VSD location, norperioperative factors, like patchmaterial, myocardial protection oroperating surgeon, prove significant.
Dalrymple-Hay M.J. et al. (1998),Seminars in Thoracic andCardiovascular Surgery
Single center cohort study(1972–1995), n = 179
No N/A Yes Yes 27% (n = 48) The study suggests that even the mosthemodynamically unstable patients, ifaggressively managed, have goodlong-term outcomes.
Killen D. A. et al. (1997),Annals of Thoracic Surgery
Single center cohort study(1970–1994), n = 76
No N/A No No 41% (n = 31) The operative mortality rate is highwith early operative repair, thepreoperative presence of cardiogenicshock, and an inferior location of theacute infarction.
Parry G. et al. (1992) EuropeanHeart Journal
Single center cohort study(1980–1989), n = 108
Yes N/A Yes No 47% (n = 38) Posterior VSDs carried a higher operativemortality than anterior (53% vs 43%) butthe difference was not significant.
Cummings R. G. et al. (1989),Annals of Thoracic Surgery
Single center cohort study,n = 42
Yes Yes Yes Yes 42% (n = 14) The higher mortality in patients withinferior infarction may be associatedwith a greater degree of right ventricularinfarction and consequent dysfunction.
Moore C. A. et al. (1986),Circulation
Single center cohort study(1979–1984), n = 25
Yes Yes Yes Yes 56% (n = 14) Cardiogenic shock was more commonin inferior infarction and associatedwith a 91% mortality
a Cardiogenic shock: systolic blood pressure less than 80 mm Hg or mean arterial pressure less than 60 mm Hg, with evidence of end-organ hypoperfusion (obtundation, decreasedurine output, elevated levels of creatine or blood urea nitrogen, or cool, clammy skin), or the requirement formechanical or pharmacological interventions tomaintain blood pressure andend-organ perfusion.
b Right ventricular dysfunction: abnormalities in filling or contracting the right ventricle following myocardial ischemia and/or pressure/volume overload.c Early repair: a significant period of time in the acute setting of VSD post-AMI in which the author suggested surgical management to be delayed.
31A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

2. Methods
A retrospective chart review for presentation,management and out-comes was carried out in a cohort of 34 patients who underwent sur-gery for post-AMI VSDs between December 1991 and July 2014 at the“Institut Universitaire de Cardiologie et de Pneumologie de Quebec”. Pre-and peri-operative variables were collected from the cardiac surgeons'database. Primary outcome was 30-day mortality. Clinical and echocar-diographic data were assessed to identify significant risk factors forearly and late mortality. We certify that the study protocol conformsto the ethical guidelines of the 1975 Declaration of Helsinki as reflectedin a priori approval by the institution's human research committee.
2.1. Definitions
Cardiogenic shock was defined as; 1 — systolic blood pressure≤ 80 mm Hg or mean arterial pressure ≤ 60 mm Hg, with evidence ofend-organ hypoperfusion (obtundation, decreased urine output, elevat-ed creatinine levels or elevated blood urea nitrogen, or cool, clammyskin), or 2 — the requirement for mechanical or pharmacological inter-ventions tomaintain blood pressure and end-organ perfusion [8]. Renalimpairment was defined as reduction in kidney function characterizedby an absolute increase in serum creatinine ≥ 150 μmol/l, or a reductionin urine output (documented oliguria of b0.5 ml/kg/h for N6 h) [9].Pulmonary hypertension was defined as mean pressure ≥ 25 mm Hg.Operative mortality was defined as death within 30 days of surgery,either in hospital or after hospital discharge.
2.2. Statistical analysis
Continuous variableswere tested for distribution normalitywith theShapiro–Wilk test and expressed as mean ± SD or median and inter-quartile range. Differences between groups were assessed using t-testfor continuous variables and χ2 test or Fisher exact test for categoricalvariables. Long-term survival was presented with a Kaplan–Meiercurve. The impact of clinical and Doppler echocardiographic variableson in-hospital and overall mortality was assessed with logistic andCox proportional-hazard regression models, respectively. Clinicallyrelevant variables with a P-value ≤ 0.05 on individual analysis were in-cluded in backward stepwise multivariable models. P-value ≤ 0.05 wasconsidered statistically significant.
3. Results
Patient demographic and clinical characteristics are presented inTables 1 and 2. Mean age was 69 years with 44% women. The VSDswas anterior in 11 (32%) and posterior in 23 (68%) patients. Sixteen(47%) patients had a single vessel coronary artery disease. Mean ejec-tion fraction was 44 ± 14%, and 24 patients (71%) were in cardiogenicshock. Mean systolic blood pressure was 97 ± 19 mm Hg and mean
diastolic blood pressure was 60 ± 13 mm Hg. Pre-operative intra-aortic balloon pump was inserted in 22 patients (65%). Twenty-sevenpatients (79%) were intubated before the operation and 12 (35%) pre-sented with right ventricular dysfunction. Median interval from AMIto VSDs repair was 7 days.
Operative and post-operative data are listed in Table 3. Mean aorticcross clamp and cardiopulmonary bypass times were 94 and 141 min,respectively. Coronary artery bypass grafting (CABG) was performedin 15 patients (44%).
Outcomes are presented in Table 4. Thirty days operative mortalitywas 65%. Mortality for the posterior VSDs group was 74% and the ante-rior VSDs group 46%. Univariate analysis identified age, bodymass index(BMI), diastolic blood pressure, posterior localization of VSDs, bypasstime, cross-clamp time, reoperation during hospitalization and timebetween AMI and surgery as predictors of long-term mortality.
Table 1Patients demographic data.
Variables Survivors Non-survivors Total P
n = 12(%)
n = 22(%)
n = 34(%)
Age 64 ± 8 72 ± 4 69 ± 7 b0.001Gender (Female) 3 (25) 12 (55) 15 (44) 0.152Diabetes 4 (33) 7 (32) 11 (32) 1Arterial hypertension 6 (50) 11 (50) 17 (50) 0.535Smoking 1 (8) 8 (36) 9 (27) 0.113BMI 28 ± 4 25 ± 4 26 ± 4 0.0096History of CAD 9 (75) 20 (91) 29 (85) 0.329History of stroke 1 (8) 1 (5) 2 (6) 1COPD 4 (33) 3 (14) 7 (21) 0.211Renal impairment (Créat N 150) 5 (42) 5 (23) 10 (29) 0.271
Table 2Patients clinical data.
Variables Survivors Non-survivors Total P
n = 12 (%) n = 22 (%) n = 34 (%)
AMI location (inferior) 6 (50) 17 (77) 23 (68) 0.138Thrombolysis 4 (33) 7 (32) 11 (32) 1EF (ejection fraction) 42 ± 11 44 ± 16 44 ± 14 0.572Cardiogenic shock 6 (50) 18 (82) 24 (71) 0.110
Right ventricular failure 3 (25) 9 (41) 12 (35) 0.465Systolic pressure (mm Hg) 99 ± 16 97 ± 21 97 ± 19 0.759Diastolic pressure (mm Hg) 66 ± 12 56 ± 13 60 ± 13 0.027Pulmonary hypertension 3 (25) 7 (32) 10 (29) 1Mitral regurgitation 9 (75) 11 (50) 20 (59) 0.275
Mitral regurgitation ≥ 2/4 2 (17) 3 (14) 5 (15) 1Tricuspid regurgitation 6 (50) 13 (59) 19 (56) 0.724
Tricuspid regurgitation ≥ 2/4 5 (42) 10 (46) 15 (44) 1VSD diameter (mm) 17 ± 10 15 ± 6 16 ± 7 0.765VSD location (posterior) 6 (50) 17 (77) 23 (68) 0.138IABP 10 (83) 20 (91) 30 (88) 0.602
Preoperative IABP 7 (58) 15 (68) 22 (65) 0.711Perioperative IABP 2 (17) 4 (18) 6 (18) 1Postoperative IABP 1 (8) 1 (5) 2 (6) 1
Preoperative intubation 9 (75) 18 (82) 27 (79) 0.677Time interval AMI-VSD (d) 7.21 1.79 3.91 0.014Time interval VSD-OP (d) 4.44 2.74 3.38 0.198Time interval AMI-OP (d) 11.65 4.4 7.03 0.013
Table 3Operative and post-operative data.
Variables Survivors Non-survivors Total P
n = 12(%)
n = 22(%)
n = 34(%)
Cardioplegia vs. perfusedheart
11 (92) 20 (91) 31 (91) 1
Cardioplegia type (blood) 11 (92) 22 (100) 33 (97) 0.353Normothermia vs.hypothermia
7 (58) 14 (64) 21 (62) 1
Concomitant CABG 4 (33) 11 (50) 15 (44) 0.476Concomitant LV repair(aneurysm orpseudoaneurysm repair)
5 (42) 8 (36) 13 (38) 1
Cross clamp time (min) 83 ± 21 100 ± 44 94 ± 38 0.215Bypass time (min) 115 ± 29 156 ± 62 141 ± 56 0.042Cardioplegia volumeuse (ml)
3937 ± 4520 4381 ± 2540 4145 ± 3286 0.722
Glue use 4 (33) 7 (32) 11 (32) 1Low cardiac outputsyndrome (cardiac index,2.0 l/min per m2)
6 (50) 14 (64) 20 (59) 0.487
Residual VSD 3 (25) 6 (27) 9 (27) 1ECMO 0 1 (5) 1 (3) 1Renal failure 6 (50) 11 (50) 17 (50) 1Stroke 1 (8) 2 (9) 3 (9) 1Reoperation 4 (33) 3 (14) 7 (21) 0.211
28 A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

Multivariate analysis identified older age and shorter time betweenAMI and surgery as independent predictors of 30-day and long-termmortality.
Long-term survival is presented in Fig. 1 and results from the statis-tical analysis are presented in Table 5.
4. Discussion
Post-AMI VSDs is a serious clinical problem with high mortalityrate. In recent years, early and efficient revascularization therapy formyocardial infarction has contributed to a decreased incidence ofVSDs [10]. However, management of patients with post-AMI VSDs re-mains a challenge. Furthermore, the spectrum of surgical patientsseems to switch toward patients with more extensive heart failure, he-modynamic compromise and associated comorbidities. Our experienceregarding mortality and risk factors are in accordance with previouslypublished reports. In the following, we compare our data to the avail-able literature and describe best evidence risk factors. Conventionaland non-conventional management for patients with post-AMI VSDsare also described.
4.1. Risk factors
4.1.1. Cardiogenic shockOur experience identified low diastolic blood pressure as a univari-
ate significant risk factor for operative mortality. Patients with diastolicpressure under 60 mm Hg are in cardiogenic shock, therefore carryingan extensive deleterious condition usually leading to poor survivalrates despite aggressive treatments. In our experience, patients wereoften rushed to surgery under emergency status because of this
complication. In patients developing VSDs following AMI, prognosis isdependent on the degree of hemodynamic compromise. Consequently,many authors have identified the development of cardiogenic shock asthe single most important predictor of mortality [2,3,5,6,11–14] espe-cially if concomitant right ventricular dysfunction develops [15]. Studieshave shown that the most important factor contributing to cardiogenicshock is the typically large infarct present in patients with VSDs. Inpatients with cardiogenic shock and in the absence of surgical interven-tion, death is inevitable. Results of surgical treatment regarding post-AMI VSDs from many series demonstrated the importance of thisparameter on operative mortality [2,3,5,6,8,11,12,14–17]. Cummingset al. revealed an operative mortality ranging from 13% to 42% in ab-sence of cardiogenic shock, compared to a range of 44% to 58% for pa-tients in cardiogenic shock [8]. Others have reported series in whichcardiogenic shock complicated more than 80% of post-AMI VSDs [8].Therefore, it has been suggested that early operative closure of VSDsshould not be conducted in patients with cardiogenic shock but appro-priately delayed until hemodynamic stabilization, whenever possible[15,18].
4.1.2. Early surgeryA recent publication from the Society of Thoracic Surgeons National
Database (STS Database, n = 2876) showed that mortality of patientsvaried significantly depending on timing of surgery. Patients whounderwent surgery within 7 days from the symptoms onset had a 54%mortality compared with 18% mortality if repair was delayed morethan 7 days after VSDs post-AMI initial presentation [11]. Moreover,Serpytis et al. [18] recently exposed early outcomes of 41 patientswith post-AMI VSDs. The report showed a 100% survival rate for all pa-tients (n=33)who underwent surgery after 3–4weeks of stabilizationand a 100% mortality rate when operated within the first 10 days (n =5). Our data confirmed that a shorter time betweenAMI and surgery is asignificant risk factor for 30-day operativemortality. The improved out-comemay be related to evolution of the infarct and improved stability ofthe cardiac tissue allowing amore effective repair in an elective delayedsurgical procedure. However, it may represent a survival bias, as earlysurgery is usually performed in individuals with marked hemodynamicinstability and circulatory compromise, making immediate surgicalmanagement the only viable option for them.
4.1.3. Right ventricular dysfunctionThe importance of right ventricular dysfunction on outcome was
demonstrated by Cummings et al. [8]. A higher proportion of right ven-tricular infarct extension is found in VSDs-generating AMI, independentof their anterior or inferior location. In fact, the incidence of right ven-tricular infarction in the post-AMI VSDs group was 100% vs 28% in thenon-VSDs group (P b 0001). Dysfunction of the right ventricle may bethe consequence of right ventricular infarction, right ventricularischemia, and/or pressure–volume abnormalities. VSDs following AMI
Table 4Outcomes and mortality etiology.
Variables Results
n = 34 (%)
Survival 12 (35)30 day mortality 22 (65)All over hospital mortality 23 (68)
Anterior VSD mortality 5/11 (46)Posterior VSD mortality 17/23 (74)
MortalityCauses: 1: Cardiac 18/22 (82)
2: Multi-organ failure 2/22 (9)3: Infection 1/22 (5)4: Respiratory 1/22 (5)
Fig. 1. Kaplan–Meier survival curve.
Table 5Significant predictors of operative mortality in univariate and multiple Cox proportional-hazard regression models.
Univariate Multivariate
HR [95% conf.interval]
P-value HR [95% conf.interval]
P-value
Age 1.10 1.04–1.17 0.002 1.11 1.04–1.18 0.0001BMI 0.88 0.79–0.99 0.04 – – –VSD localization 2.45 0.96–6.25 0.06 – – –BP diastole 0.96 0.94–0.99 0.016 – – –Reoperation 0.28 0.08–0.95 0.042 – – –Bypass time 1.11 1.03–1.19 0.005 – – –Cross-clamp time 1.13 1.00–1.28 0.05 – – –Time between AMIand operation
0.93 0.88–0.99 0.045 0.90 0.83–0.98 0.015
VSD: ventricular septal defect, BP: blood pressure.
29A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

hemodynamic stability and delaying surgical repair [44]. This small in-tracardiac axial flow left ventricular device can be inserted throughthe femoral or axillary artery and provides a 4–5 L/min of continuousblood flow. A successful course of events, in which the implantation ofan Impella 5.0 help improving the hemodynamic condition of a patientby decreasing the left-to-right shunt and right ventricular overload, hasbeen reported [44]. After a two-week stabilization period, CABG and clo-sure of the defect were performed successfully. Fibrous tissue had de-veloped around the VSDs, providing easier and stronger anchoring forthe surgical repair. La Torre et al. [45] also implanted the device in a se-ries of patients (n= 5) in cardiogenic shock as a consequence of a pos-terior VSDs post-AMI. The mean duration of support by the leftventricular assist devicewas14.4±6days,withoutmortality during as-sistance. Some have suggest that when surgical closure of the defectmay not be possible because of its location and/or the serious impair-ment in left ventricular function, the Impella 5.0 could be use as a bridgeto heart transplantation [46]. Maintenance of a stable hemodynamicstatus for 10 days using a TandemHeart (CardiacAssist, Inc.; Pittsburgh,PA) followed by a successful closure of VSDs has also been reported [47].The first series of 11 cases treatedwith the TandemHeart was publishedin 2014 [48]. Results showed an overall survival rate of 75% at 6 monthswith a significant trend toward better survival after immediate percuta-neous ventricular assist device placement to stabilize the patient andallow for myocardial healing before surgical VSDs repair.
4.2.7. Left ventricular assist deviceThe use of left ventricular assist devices (LVAD) reduces interven-
tricular shunt and ensures an adequate cardiac output, allowing timefor clinical stabilization before further treatment. Initially, patientswith AMI were not thought to be good candidates for implantableLVAD insertion because of the technical problems in securing the inflowcannula to the necrotic infarcted myocardium. Indeed, right ventricularfunction must be intact to allow hemodynamic stabilization underLVAD, therefore making this procedure possible only in a selectedgroup of patients. Faber et al. [43] described their experience withLVAD in patients with post-AMI VSDs, successfully maintaining
physiologic hemodynamic with minimum doses of drugs until electivesurgery or transplant was contemplated. LVAD was also used in orderto improve clinical status of a post-AMI VSDs patient in cardiogenicshock [49]. After four days, the patient underwent VSDs repair by an in-farct exclusion technique and tolerated the procedure well. The patientremained well at 1 year follow-up, establishing the importance of clini-cal status improvement before surgical repair to optimize patients'prognosis. Finally, a successful placement of the HeartMate (ThoratecCorporation, Pleasanton, CA, USA) LVAD and velour patch closure ofan apical VSDswas described [50]. Unfortunately, the patient developeda secondVSDs in the followingdays,which created a high-flow right-to-left shunt and caused irreversible hypoxic brain injury. The authors sug-gest that the use of a LVAD as a bridge to destination treatmentmust beapproached with extreme precaution for patients developing post-AMIVSDs [50].
4.2.8. Bi-ventricular assist deviceSignificant proportions of patients are in a state of impending or
manifest cardiogenic shock and require immediate surgical treatmentbefore multiple organ failure becomes irreversible. Inflow to the VADcan be accomplished at the atrial level, making this procedure an idealcannulation strategy for VSDs, in which it is important to avoid ashunt at the ventricular level. Recent series demonstrated the useful-ness of bi-VAD as a bridge to surgery or transplant [51–53]. In thepresence of persistent VSDs, Samuels et al. [52] used biventricular me-chanical cardiac support to successfully restore hemodynamic stabilityand reverse multi-organ failure as a bridge to transplantation. The au-thors suggested that bi-VAD implantation could minimize the impactof a massive myocardial infarction and associated heart failure inpatientswith post-AMI VSDs. Reichenspurner et al. [53] described a suc-cessful intervention using bi-VAD to restore peripheral organ perfusion,allowing time for recovery andmaturation of the infarctedmyocardiumbefore surgical correction of the VSDs. Sai-Sudhakar Chittoor B. et al.[51] also described a successful course of events with the use of bi-VAD as a bridge to surgery in a patient with post-AMI VSDs.
Table 7Best evidence studies describing operative mortality and major outcomes in patient with percutaneous repair of VSD post-AMI.
Author, date, journal Patient group Patients characteristics Operativemortality(within30 days ofoperation)
Outcomes Comments
Cardiogenicshock
Percutaneousrepair onlya
Zhu X-Y et al. (2013),EuroIntervention
Multicenter study(2001–2011),n = 35
n = 13 (37%) n = 35 (100%) 14% (n = 5) The long-term overallmortality rate was 20%.
In-hospital mortality was significantlyhigher in patients who presented withcardiogenic shock.
Assenza GE et al. (2013),Circulation: CardiovascularInterventions
Single center cohortstudy (1988–2008),n = 30
n = 17 (57%) n = 9 (30%) 23% (n = 7) Long-term follow-upunavailable
Cardiogenic shock was significantlyassociated with an increased risk of 30-daymortality.
Sathananthan J et al. (2013),Journal of InvasiveCardiology
Single center cohortstudy (1992–2012),n = 9
n = 4 (44%) n = 7 (78%) 33% (n = 3) The long-term overallmortality rate was 44%.
Mortality was higher for cardiogenic shock(75%, n = 3) in comparison to non-shockpatients (20%, n = 1).
Maltais S. et al. (2009),Annals of Thoracic Surgery
Single center cohortstudy (1995–2007),n = 12
n = 9 (75%) n = 12 (100%) 42% (n = 5) Long-term follow-upunavailable
Short time between VSD diagnosis andpercutaneous closure was the mostsignificant predictors of 30-day mortality
Thiele H. et al. (2008),European Heart Journal
Single center cohortstudy (2003–2008),n = 29
n = 16 (55%) n = 29 (100%) 66% (n = 19) The long-term overallmortality rate was 69%.
Mortality was higher for cardiogenic shock(88%, n = 14) in comparison to non-shockpatients (38%, n = 5).
Demkow M. et al. (2005),EuroIntervention
Single center cohortstudy (1999–2005),n = 11
n = 3 (27%) n = 10 (90%) 27% (n = 3) The long-term overallmortality rate was 27%.
All survivors (n = 8) underwent delayedprocedure (4–56 weeks after the infarctiononset) and were hemodynamically stable(in a chronic infarction phase)
Holzer R. et al. (2004),Catheterization andCardiovascularInterventions
Multicenter study,(2000–2003),n = 18
n = 10 (56%) n = 8 (44%) 28% (n = 5) The long-term overallmortality was 41%.
Most patients in cardiogenic shock had agrave postprocedural course and diedwithin the first 6 days of the procedure.
a Without conventional surgical repair attempt neither before nor after percutaneous closure.
32 A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

4.2.9. ECMOVeno-arterial (VA) extra-corporeal membrane oxygenation (ECMO)
may be an interesting option for temporary assistance in patients withpost-AMI VSDs. It has been suggested that when usual treatment failsto stabilize patients in cardiogenic shock, peripheral VA ECMO couldbe the quickest, easiest, and least invasive biventricular support device.Hobbs [54] described three patients with post-AMI VSDs treated withperipherally cannulated ECMO prior to definitive repair. Prior toHobbs' publication, three case reports described the use of VA ECMOfor the preoperative support of patients with post-AMI VSDs. All pa-tients demonstrated an uneventful course with a survival rate of 100%
[55–57]. Further studies will be needed to assess the usefulness ofECMO in this particular group of patients.
4.2.10. TAH-tImplantation of the TAH-t (CardioWest Total Artificial Heart,
SynCardia Systems, Tucson, AZ) has been shown to improve outcomesin unstable patients in end-stage cardiogenic shock by providing imme-diate hemodynamic stabilization and end-organ perfusion until cardiactransplant can occur. Patients with post-AMI VSDs do not typically havea dilated heart, making proper fitting of the TAH-t more challenging[58]. The TAH-t requires the removal of both native ventricles to
Table 8Best evidence case reports describing outcomes and long-term follow-up of alternative treatment for patients with VSD post-AMI.
Author, date, journal Mechanical device used Outcomes Long-term follow-up
pVADa • Gregoric I.D. (2014), AmericanSociety for Artificial InternalOrgans Journal
TandemHeart (CardiacAssist Inc.,Pittsburgh, PA)
Successfully bridge 8 patients tosurgery or recovery (14 ± 4 days)/Unsuccessfully bridge to recovery3 patients (5 ± 2 days)
Postoperatively, all 8 patients survived30 days. At 6 months follow-up, overallsurvival was 75%.
• Patanè F. (2010), InternationalJournal of Cardiology
Impella Recover (Abiomed Inc., USA) Successfully bridge to transplantation(2 weeks)
The patient was discharged andremained alive and well.
LVADb • Pitsis A.A. (2007), The Journalof Thoracic and CardiovascularSurgery
The Levitronix Centrimag (Zurich,Switzerland)
Successfully bridge to surgery (4 days) At 1 year, the patient remained aliveand well.
• Faber C. (2002), The Journal ofThoracic and CardiovascularSurgery
HeartMate (Thermo CardiosystemsInc., Woburn, Mass)/Novacor LVAD(World Heart Corp, Ontario, Canada)
Successfully bridge two patients totransplantation (73 and 91 daysrespectively)
Respectively 5 and 3 years after theoperation, both patients are alive andwell.
• Kshettry V.R. (1997), Journal ofCardiac Surgery
HeartMate (Thermo CardiosystemsInc., Woburn, MA, USA)
Unsuccessful attempt to bridge totransplantation
The patient died in the acute phasefollowing implantation of the LVAD
Bi-VADc • Conradi L. (2009), Annals ofThoracic Surgery
Abiomed AB 5000 (Abiomed Inc.,Danvers, MA)
Successfully bridge to surgery(2 weeks)
4 months after surgery, the patientremains alive and in excellentcondition.
• Sai-Sudhakar C.B. (2006), TheJournal of Thoracic andCardiovascular Surgery
Abiomed AB 5000 (Abiomed Inc.,Danvers, Mass)
Successfully bridge to recovery(several months)
At 18 months, the patient remainedalive and well.
• Samuels L.E. (2003), The Journalof Thoracic and CardiovascularSurgery
Abiomed AB 5000 (Abiomed, Inc.,Danvers, Mass)
Successfully bridge to transplantation(8 weeks)
At 1 year, the patient remained aliveand well.
ECMOd • Hobbs R. (2015), The Journal ofCardiac Surgery
n/a Successfully bridge 2 patients tosurgery (7 and 4 daysrespectively)/Unsuccessful attempt tobridge to transplantation
Respectively 2 and 3 years after theoperation, both patients are alive andwell./The patient died from a stroke onpostoperative day 11
• Neragi-Miandoab S. (2013),The Journal of Cardiac Surgery
Centrifugal pump, Biomedicus PumpConsule-540, Medtronic,Minneapolis, MN, USA
Successfully bridge to surgery (6 days) At 6 months, the patient remained aliveand well.
• Tsai M.T. (2012), AmericanSociety for Artificial InternalOrgans Journal
Rotaflow centrifugal pump: Maquet,Hirrlingen, Germany; Hilite-7000-LTOxygenator: Medos, Stolberg,Germany
Successfully bridge to re-op (4 days)for a recurrent shunt after the initialpatch repair
At 1 year, the patient remained aliveand well.
• Rohn V. (2008), The Journal ofCardiac Surgery
Rotaflow, Maquet, Germany Successfully bridge to surgery (3 days) At 6 months, the patient remained aliveand well.
TAH-te • Arabia F.A. (2013), The Journalof Thoracic and CardiovascularSurgery
Syncardia Temporary CardioWestTotal Artificial Heart
Successfully bridge a patient totransplantation (76 days)/Unsuccessfulattempt to bridge to transplantation
At 3 years, the first patient remainedalive and well./The second patient died9 days after TAH-t implantation.
• Knezevic I. (2013), HeartSurgery Forum
Syncardia Temporary CardioWestTotal Artificial Heart
Successfully bridge to transplantation No follow-up available
HeartTransplant
• Knezevic, Arabia, Samuels,Faber, Patanè
Six patients went through hearttransplant as a definitive treatmentafter hemodynamical stabilization withmechanical support devices (asdescribed above)
All of them followed an uneventfulcourses and long-term follow-upshowed a great trend with a survivalrates of 100%.
• Baldasare Maria D. (2014),Texas Heart Institute Journal
Successfully conduct heart transplant1 year after percutaneous closure ofrecurrent shunt after initialconventional surgical repair ofpost-AMI VSD
No follow-up available
• Sénéchal M. (2014), CanadianJournal of Cardiology
Successfully conduct heart transplant9 days after VSD post-AMI without theuse of a mechanical support device
At 1 year, the patient remained aliveand well.
a pVAD: percutaneous ventricular assist device.b LVAD: left ventricular assist device.c Bi-VAD: bi-ventricular assist device.d ECMO: Extracorporeal Membrane Oxygenation.e TAH-t: Total Artificial Heart.
33A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

connect the mechanical ventricles to the tricuspid and mitral annulusrespectively and therefore abolishes the VSDs. Nevertheless, two suc-cessful reports have been published [58–59], which highlight this ap-proach as an interesting option.
4.2.11. Heart transplantLiterature reported only few patients with post-AMI VSDs who
underwent heart transplantation as a final destination treatment [40,41,43,46,52,58]. Ashfaq et al. [58] successfully proceeded to heart trans-plantation after using the TAH-t as a bridge to surgery. Others [33] con-cluded that when the position of the VSDs is unseemly and there iscoexistence of a widespread coronaropathy not eligible for revasculari-zation, heart transplantation may represent an efficacious alternative.Samuels et al. [52] also performed successful heart transplantation in apatient with a post-AMI VSDs and persistent bi-ventricular failureafter 8 weeks of clinical stabilization with a bi-VAD. Indeed, in the pres-ence of a massive initial AMI, surgical repair of the interventricular sep-tum may not provide long-term optimal survival rates, making hearttransplantation an interesting option. We believe that patients withknown risk factors (posterior VSDs, right ventricular dysfunction, car-diogenic shock) for surgical repair for post-AMI VSDs and significantco-morbidities such as ischemic moderate-to-severe mitral regurgita-tion and/or pseudoaneurysm, should be considered potential hearttransplant candidates. Best evidence case reports describing outcomesand long-term follow-up of alternative treatment for patients withpost-AMI VSDs are shown in Table 8 [43,44,46–60].
4.2.12. Current perspectivesIn the last decades, reports on the management of patients with
post-AMI VSDs have been consistently relying on individuals' experi-ences and despite major improvement in techniques and equipment,mortality remains high. However, interest in finding new treatment
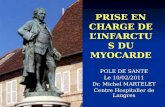
options has led to many unconventional successful experiences. Identi-fication of significant risk factors and growing experience with the useof circulatory support devices have been used to help clinicians guidetheir decision making process for patients with post-AMI VSDs. In addi-tion, recent descriptions of successful heart transplantations in patientswith difficult course of events may lead to further consideration of thisoption as a definitive treatment. We present an algorithm of treatmentdescribing optimal management of patients with post-AMI VSDs con-sidering risk factors and including mechanical assistance devices astemporary treatment and heart transplantation as a potential definitiveoption (Fig. 2).
5. Limitations
The main limitation of this study is the retrospective nature of ourexperience. In addition, incidence of post-AMI VSDs being very low,our study population is relatively small and extends on a large periodwith variable management and operative strategies. However, our re-sults are in accordance with previous contemporary series as a highmortality rate in this particular group of patients was observed. More-over, we reviewed the literature in order to assess the best approachto this population.
6. Conclusion
In conclusion, age aswell as time between AMI and operation are in-dependent predictors of 30-day and long-termmortality. The improvedoutcome with delayed surgery may be related to improved stability ofthe cardiac tissue allowing amore effective repair. It may also representa survival bias as early surgery is usually performed in individuals withmarked hemodynamic instability and circulatory compromise. Afterconfirming diagnosis, when possible prompt attempts should be made
Fig. 2. Algorithm of treatment suggesting optimal management of patients with post-AMI VSDs.
34 A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

connect the mechanical ventricles to the tricuspid and mitral annulusrespectively and therefore abolishes the VSDs. Nevertheless, two suc-cessful reports have been published [58–59], which highlight this ap-proach as an interesting option.
4.2.11. Heart transplantLiterature reported only few patients with post-AMI VSDs who
underwent heart transplantation as a final destination treatment [40,41,43,46,52,58]. Ashfaq et al. [58] successfully proceeded to heart trans-plantation after using the TAH-t as a bridge to surgery. Others [33] con-cluded that when the position of the VSDs is unseemly and there iscoexistence of a widespread coronaropathy not eligible for revasculari-zation, heart transplantation may represent an efficacious alternative.Samuels et al. [52] also performed successful heart transplantation in apatient with a post-AMI VSDs and persistent bi-ventricular failureafter 8 weeks of clinical stabilization with a bi-VAD. Indeed, in the pres-ence of a massive initial AMI, surgical repair of the interventricular sep-tum may not provide long-term optimal survival rates, making hearttransplantation an interesting option. We believe that patients withknown risk factors (posterior VSDs, right ventricular dysfunction, car-diogenic shock) for surgical repair for post-AMI VSDs and significantco-morbidities such as ischemic moderate-to-severe mitral regurgita-tion and/or pseudoaneurysm, should be considered potential hearttransplant candidates. Best evidence case reports describing outcomesand long-term follow-up of alternative treatment for patients withpost-AMI VSDs are shown in Table 8 [43,44,46–60].
4.2.12. Current perspectivesIn the last decades, reports on the management of patients with
post-AMI VSDs have been consistently relying on individuals' experi-ences and despite major improvement in techniques and equipment,mortality remains high. However, interest in finding new treatment
options has led to many unconventional successful experiences. Identi-fication of significant risk factors and growing experience with the useof circulatory support devices have been used to help clinicians guidetheir decision making process for patients with post-AMI VSDs. In addi-tion, recent descriptions of successful heart transplantations in patientswith difficult course of events may lead to further consideration of thisoption as a definitive treatment. We present an algorithm of treatmentdescribing optimal management of patients with post-AMI VSDs con-sidering risk factors and including mechanical assistance devices astemporary treatment and heart transplantation as a potential definitiveoption (Fig. 2).
5. Limitations
The main limitation of this study is the retrospective nature of ourexperience. In addition, incidence of post-AMI VSDs being very low,our study population is relatively small and extends on a large periodwith variable management and operative strategies. However, our re-sults are in accordance with previous contemporary series as a highmortality rate in this particular group of patients was observed. More-over, we reviewed the literature in order to assess the best approachto this population.
6. Conclusion
In conclusion, age aswell as time between AMI and operation are in-dependent predictors of 30-day and long-termmortality. The improvedoutcome with delayed surgery may be related to improved stability ofthe cardiac tissue allowing amore effective repair. It may also representa survival bias as early surgery is usually performed in individuals withmarked hemodynamic instability and circulatory compromise. Afterconfirming diagnosis, when possible prompt attempts should be made
Fig. 2. Algorithm of treatment suggesting optimal management of patients with post-AMI VSDs.
34 A. Cinq-Mars et al. / International Journal of Cardiology 206 (2016) 27–36
Sénéchal, International Journal of Cardiology , 2016

ON RETIENT 1) Mortalité élevée même avec chirurgie
(≥50%)
2) Attendre le plus longtemps possible (≥ 1
semaine)
3) Si impossible, considérer ECMO > device
+/- transplantation selon l’évaluation globale
du patient (type CIV/CHOC/âge/
comorbidité)

Qu’est-ce que le (la) technicien(ne) devrait savoir ?
1. En présence d’un infarctus toujours rechercher une
CIV (faire doppler couleur dans toutes les incidences a/
n milieu du septum);
2. Si CIV suspectée, se demander s’il s’agit d’une CIV
postérieure ou d’une CIV antérieure
3. Se méfier du patient stable hémodynamiquement;

Qu’est-ce que le cardiologue devrait savoir ?
1. Avoir la même démarche que le (la) technicien (ne);
2. Si CIV démontrée, avoir une ouverture à réfléchir
autrement !!;
3. En résumé, envisager d’attendre/ECMO/greffe !

IN-HOSPITAL COURSE OF THE PATIENTS WITH SUB-ACUTE VENTRICULAR FREE WALL RUPTURE: Clinical fea-tures of the patients with this complication are sum-marized in Table II. When the blood was expandedwith fluid infusion, some patients responded favor-ably. Hemodynamic recovery was complete in patient8, who had refused surgical intervention. In this case,cardiac tamponade dramatically relapsed 5 days later.At surgery, 2 large clots, old and new, respectively,surrounded the heart, whereas 2 tears were recogniz-able at the site of infarct expansion.As a therapeutic measure, percutaneous pericardio-
centesis was performed in 6 patients. In 4 of them thesuccess of the procedure was limited by rapid clottingof blood into the set for pericardial drainage. Twopatients died of further tamponade after initial im-provement following pericardiocentesis (patients 12and 22). Emergency cardiac catheterization was per-formed in 2 subjects with concomitant ventricularseptal defect (patients 14 and 23). Four patients diedof electromechanical dissociation while awaiting sur-
gery (patients 6, 12, 21, and 22). These deaths oc-curred between 50 minutes and 6 hours after the firstclinical signs of rupture.
In-hospital mortality due to acute myocardial infarc-tion: Among the patients directly admitted to the cor-onary care unit during the study period, 77 (12.7%)died in hospital from various complications of acutemyocardial infarction. Necropsy was performed in89% of all cases. Clinicopathologic correlations re-vealed that the death was most frequently due tocardiogenic shock (7.5%), followed by acute ventric-ular free wall rupture (4.1%), subacute rupture (0.3%),and arrhythmias (0.8%).
Surgical treatment: Twenty-four of the 28 patientswith subacute ventricular free wall rupture were takento surgery (6 from group A, 7 from group B, and 11from group C). The time lapse from the first clinicalindication of rupture to intervention ranged from 1 to16 hours (median, 5 h).Five patients experienced cardiac arrest on arrival
in the cardiac surgery unit or during induction of
TABLE II Clinical Characteristics of 28 Patients With Subacute Ventricular Free Wall Rupture
PatientsAge (yr)& Sex
Infarct Siteon ECG
ConductionDisturbance
DuringAMI
Timing ofRupture (d) Clinical Features
Physical Findings*
HR(beats/min)
SBP(mm Hg)
RAP(cm H2O)
ArterialPulse
Group A1 68/F Anterior RBBB, LAH 1 Syncope 3 shock 130 70 28 P2 58/M Inferior � 1 Pain, shock 85 80 30 P3 66/M Inferior � 1 Syncope 3 shock 130 60 20 P4 75/M Inferior � 1 Syncope 3 shock 105 80 24 P5 82/M Inferior � 7 Pain, syncope 100 90 18 �6 79/M Anterior � 1 Pain, syncope 3 shock 3
EMD100 60 23 �
7 74/M Inferior � 6 3 7 Hosp. Pain, dyspnea 100 140 12 �Group B
8 66/F Posterior � 4 Pain, syncope 3 shock 3Regr§
150 60 23 P
9 70/M Inferior � 4 Syncope 3 shock 120 60 30 P10 76/M Anterior � 1 Shock 130 80 22 A11 63/F Inferior � 1 Shock 120 70 29 A12 72/M Anterior RBBB 3 Syncope 3 shock 3 EMD 130 70 22 P13 85/F Inferior AVB 1 Pain, syncope† 50 80 22 �14 70/M Inferior AVB 3 Shock‡ 105 70 18 �15 67/M Anterior � 1 Shock 50 60 22 P
Group C16 48/F Lateral � 2 Pain, shock 125 70 27 P17 82/F Anterior � 1 Pain, syncope 3 shock 100 90 20 �18 62/M Inferior � 2 Shock 115 90 20 P19 60/M Posterior RBBB 1 Pain, syncope 125 120 30 P20 77/M Inferior � 1 Pain, syncope 70 120 5 �21 67/F Posterior � 1 Shock 3 regr 3 EMD 120 120 25 �22 62/M Inferior � 5 Pain, shock 3 EMD 60 70 25 �23 69/F Inferior RBBB 1 3 2 Hosp. Pain, syncope 3 shock 3
regr‡130 100 18 �
24 75/M Inferior � 12 Syncope 3 shock 3 regr 140 120 18 P25 75/M Inferior � 4 Syncope 100 140 16 �26 65/F Lateral � 1 Syncope 3 shock 100 60 23 �27 75/M Anterior � 2 Not significant 90 90 13 �28 71/M Inferior RBBB 3 Syncope 3 shock 107 70 30 P
* Physical findings were recorded on arrival of the patient into the coronary care unit of Lancisi Hospital (groups A and C) or at the onset of critical event (groupB); †Pacemaker rhythm; ‡Holosystolic murmur (ventricular septal defect); §Relapse of tamponade 5 days later.
A ⇥ alternans; AVB ⇥ atrioventricular block; ECG ⇥ electrocardiogram; EMD ⇥ electromechanical dissociation; Hosp. ⇥ hospital admission; HR ⇥ heart rate;LAH ⇥ left anterior hemiblock; P ⇥ paradoxus; RAP ⇥ right atrial pressure; RBBB ⇥ right bundle branch block; Regr ⇥ regression; RV ⇥ right ventricle; SBP ⇥ systolicblood pressure; � ⇥ absent.
CORONARY ARTERY DISEASE/MANAGEMENT OF VENTRICULAR FREE WALL RUPTURE 401
Purcaro , American Journal of Cardiology, 1997
Diagnostic Criteria and Management
of Subacute Ventricular Free Wall
Rupture Complicating Acute
Myocardial Infarction
Augusto Purcaro, MD, Carlo Costantini, MD, Nino Ciampani, MD,Marco Mazzanti, MD, Carla Silenzi, MD, Alberto Gili, MD, Romualdo Belardinelli, MD,
and Daniel Astolfi, MD
In this prospective study we evaluated the value of themain diagnostic criteria for postinfarction subacute rup-ture of the ventricular free wall. Two-dimensional echo-cardiograms and recordings of right atrial pressure andwaveform were immediately obtained in every patientexhibiting rapid clinical and/or hemodynamic compro-mise in the acute infarction setting. The same protocolwas applied to patients referred from other hospitals forsuspected myocardial rupture. In 28 cases a subacutefree wall rupture was identified. In most of the patientsthe diagnosis was based on the demonstration of hemo-pericardium and cardiac tamponade by echocardiogra-phy, cardiac catheterization and, occasionally, by peri-cardiocentesis. In 2 instances, the identification ofintrapericardial echo densities suggesting clots, in the
absence of cardiac tamponade, allowed a diagnosis ofsubacute rupture. Direct, but indistinct visualization ofmyocardial rupture was obtained in 4 cases. Among the28 patients with this complication, 4 died while awaitingsurgery and 24 underwent surgical repair (mortalityrate 33%). Long-term outcome of survivors was favor-able. Various myocardial lesions underlie postinfarctionsubacute free wall rupture. Clinical presentation variedwidely. The diagnosis was based, usually but not al-ways, on the association of hemopericardium and signsof cardiac tamponade. An organized approach to man-agement of this complication of acute myocardial infarc-tion was suggested. �1997 by Excerpta Medica, Inc.
(Am J Cardiol 1997;80:397–405)
A
fter cardiogenic shock, myocardial rupture is theleading cause of in-hospital death from acute
myocardial infarction. Clinical and pathologic studieshave demonstrated that ventricular free wall rupturesmay take an acute, subacute, or chronic course.1–5 Inthe first instance, a transmural tear produces a cardiactamponade that is rapidly fatal. In contrast, in subacuteclinical presentation, cardiac tamponade is less rapidand less severe.6 If the diagnosis is made early, long-term prognosis after successful surgical repair may beexcellent. Unfortunately, the recognition of subacutefree wall rupture remains a challenging problem afteracute myocardial infarction.The purpose of this study was to evalute: (1) the
incidence of subacute ventricular free wall rupture inan unselected population of patients with acute myo-cardial infarction; (2) the possibility of early diag-noses of this condition in a coronary care unit utilizingan appropriate algorithm; (3) the effectiveness ofemergency surgery, once the diagnosis is made; and(4) long-term outcome of survivors of intervention.
METHODSStudy patients: Between January 1990 and May
1995, 608 consecutive patients were directly admitted
to the Lancisi coronary care unit with a diagnosis ofacute myocardial infarction and were prospectivelyevaluated for inclusion in the study. Diagnosis ofacute myocardial infarction was made according toNew York Heart Association criteria.7 Patients withprimary valvular heart disease, cardiomyopathy, peri-cardial disease, or previous cardiac surgery were ex-cluded.During the study period all patients with acute
myocardial infarction were managed according touniform criteria. A 12-lead electrocardiogram and2-dimensional echocardiogram were recorded in ev-ery patient at admission to the coronary care unit.Additionally, a polyethylene catheter was insertedinto the right atrium from the antecubital vein forrecording intracavitary pressure in case of hemody-namic compromise. Serial electrocardiograms and2-dimensional echocardiograms were obtaineddaily during the first week and every 2 days there-after, before discharge, and promptly if hemody-namic deterioration occurred.Early thrombolytic therapy (within 6 hours from
symptom onset) was used in this patient population.Intravenous heparin, unassociated with thrombolysis,and early intravenous � blockade were administered atthe discretion of the participating physician. Oral�-blocking agents were strongly recommended. All pa-tients without contraindication received aspirin 160 mg/day. Steroids and nonsteroidal anti-inflammatory drugswere not utilized.Cardiac catheterization was usually performed in
From the Division of Cardiology and Division of Cardiac Surgery,Ospedale cardiologico ‘‘G.M. Lancisi,’’ Ancona, Italy. Manuscriptreceived November 12, 1996; revised manuscript received andaccepted April 17, 1997.
Address for reprints: Augusto Purcaro, MD, Via Toti, 1, 60100Ancona, Italy.
©1997 by Excerpta Medica, Inc. 0002-9149/97/$17.00 397All rights reserved. PII S0002-9149(97)00385-8

anesthesia or ventilatory support. Immediate resusci-tative efforts were undertaken.During surgery a free wall rupture (complete or
incomplete) was identified in every case. Cardiopul-monary bypass and total body hypotermia was per-formed in 18 patients. During the period of 1990 to1994, the ventricular tear was closed in 2 layers withsutures backed with 2 strips of felt. A sutureless tech-nique was used in the presence of epicardial hema-
toma or bleeding infarct and, re-cently, in patients with a well-defined myocardial rupture.In patients 14 and 23 the closure
of a concomitant septal defect wasperformed according to standardtechniques and was accompanied bycoronary revascularization in case14. Weaning from cardiopulmonarybypass was difficult in 5 patients andrequired left ventricular support withintraaortic balloon pumping.Among the 24 patients undergo-
ing surgery, 16 survived and 8 diedperioperatively (mortality rate 33%).The causes of death were electrome-chanical dissociation (2 cases), in-cessant hemorrhage (3 cases), andcardiogenic shock (3 cases). Thenonsurviving population includedthe patients who had experiencedcardiac arrest before the implemen-tation of cardiopulmonary bypassand the 2 patients with combinedfree wall and septal rupture.The average hospital stay was 15
days, ranging from 8 to 33. At dis-charge the survivors had a fairlygood left ventricular function at rest.
Pathologic features: The variousventricular free wall ruptures ob-served in this study are shown inFigure 4. Coronary anatomy was de-fined at autopsy or by angiography in
13 patients. One- or 2-vessel coronary disease waspresent in 9 cases and 3-vessel disease in 4. In everypatient a new thrombotic occlusion of the infarct-related artery was observed.
Postoperative follow-up: Patients were followed-upto 5 years and 5 months (mean, 30). One patient died4 months after surgery following a femoral arteryrupture due to the detrimental effects of a circulatorysupport device. Another died of reinfarction 5 yearsafter cardiac rupture. One patient died of intracranialneoplasm 3 months after surgery. Two subjects expe-rienced exertional angina and underwent coronary an-giography. In patient 4 a permanent pacemaker wasimplanted 2 years after cardiac rupture because ofintermittent third-degree atrioventricular block. At theend of follow-up 11 patients continued to be asymp-tomatic at moderate levels of physical activity.
DISCUSSIONIncidence and pathologic features of subacute ven-
tricular free wall rupture: In our department, whichserves as both a primary care base for the local pop-ulation and a tertiary care center for a large geographicregion, a subacute free wall rupture was observed in2.46% of all patients with acute myocardial infarctiondirectly admitted to the coronary care unit. In 4.10%the myocardial rupture took an acute course. Duringthe study period no case of left ventricular false an-
TABLE III. Sensitivity, Specificity, and Predictive Value of Different Variables, UsedIndependently and in Combination, for Diagnosing a Postinfarction ExternalCardiac Rupture
Sensitivity (%) Specificity (%)Positive Predictive
Value (%)
Infarct siteAnterior 25 70 3.9Inferior 68 54 6.7Lateral 7.1 90 3.3
Prior myocardial infarction 3.5 75 0.6Bundle branch block 32 74 5.7Pulsus paradoxus 46 99 72ST-T-wave deviations 32 85 10Syncope 64 91 26Shock 78 83 19Hemodynamic signs of
cardiac tamponade(CTH)*
85 99 0.9
Pericardial effusion (PE) 100 77 17Intrapericardial echoes (IE) 93 99 81Echocardiographic signs
of cardiac tamponade(CTE)
93 99 93
Hemopericardium (Hp) 21 99 85PE � bandlike
intrapericardial echoes7.1 99 28
Syncope or shock � PE �type II � IE � CTE�H
53 100 100
Syncope or shock � PE �type I � IE � CTE�H
32 100 100
Syncope or shock � PE �Hp � CTE�H
7.1 100 100
* Hemodynamic diagnosis of cardiac tamponade was considered in the presence, at least, of thefollowing: an increase of right atrial pressure and characteristic profile of right atrial pressure waveform(deep x descent and blunted y descent).
FIGURE 3. Time distribution of subacute ventricular free wall rup-ture in 28 patients.
402 THE AMERICAN JOURNAL OF CARDIOLOGY⇥ VOL. 80 AUGUST 15, 1997
Purcaro , American Journal of Cardiology, 1997

Qu’est-ce que le cardiologue devrait savoir ? 1. Avoir la même démarche que le (la) technicien
(ne);
2. On ne trouve pas ce que l’on ne cherche pas !!
3. Utilité IRM ❤/TACO devant un diagnostic de
rupture colmaté est douteux/n’est pas démontré;
4. Travail d’équipe/collaboration rapide du
cardiologue et du chirurgien cardiaque est
importante/capitale

L’IM survenant > 16 jours après un infarctus du myocarde (feuillets mitraux normaux)
L’IM chronique secondaire à une MCAS

Dysfonction VG / Remodeling Local
⇡ Forces de Tethering
⇡ Modification de la Géométrie Mitrale
Insuffisance mitrale
Dysynchronie
⇣ Forces de fermeture
Dysfonction Annulaire

Table 5 Comparison between echocardiographic studies examining the prevalence of ischemic mitral regurgitation in STEMI populationAuthor (Enrollmentyears)
N MR prevalence(%)
Moderate or severeMR (%)
Treatment strategy STEMI F/U Death (%) Other Mitral surgicalcorrection (%)
Barzilai et al. [31](1985-1986)
59 39 NR NR 59% 14 m MR (+): 48%, MR (0):11%
NR NR
Bursi et al. [2](1988-1998)
773 50 12 NR 59% 5 y None: 28%, Mild: 38%,M-S: 60%
CHF Adm NR
None: 16%, Mild: 26%,M-S: 65%
Grigioni et al. [6](1990-1997)
303 64 NR NR 100% 5 y MR (+): 62%,MR (0): 39%
Card Death NR
MR (+): 50%,MR (0): 30%
Amigoni et al. (Valiantstudy) [1](1998-2001)
496 53 13 Thrombolytic (40%),PCI (19%)
63% 20 m None: 10%, Mild: 21%,M-S: 30%
NR NR
Feinberg et al. [5](1996)
417 35 6 Thrombolytic (42%),PTCA / CABG (41%)
100% 1 y None: 4.8%, Mild: 12.4%,M-S: 24%
NR NR
Van Dantzig et al. [33](1991-1993)
188 NR 13 Thrombolytic (55%) 62% NR NR NR NR
Leor et al. [32] (N/A) 104 33 11 Thrombolytic (100%) 100% 1 m NR NR NR
Aronson et al. [30](2000-2005)
1190 46 6 PCI (30%) 100% 2 y None: 8%, Mild: 15%,M-S: 38%
CHF Adm NR
None: 0.6%, Mild: 3.6%,M-S: 4%
Barra et al. [16](2006-2008)
796 45 15 PCI (56%) 45% 2 y None: 12%, Mild: 22%,M-S: 39%
CHF Adm NR
None: 11%, Mild: 24%,M-S: 20%
Chung et al. [4](2000-2002)
519 56 15 PCI (81%) 86% 6 m None - Mild: 10%,M-S: 19%
NR NR
Chua et al. [3](2000-2004)
318 17 NR PCI (100%) 100% 7 y MR (+): 49%,MR (0): 26%
NR NR
Wita et al. [15] (N/A) 83 42 NR PCI (100%) 100% 6 m NR NR NR
Uddin et al. [18](2003-2007)
888 47 11 PCI (100%) 100% 5 y None: 13%, Mild: 18%,M-S: 34%
NR None: 0%, Mild: 0%,M-S: 4%
MacHaalany et al.(2006–2012)
174 44 11 PCI (100%) 100% 1 y None: 0%, Mild: 2%,M-S: 5%
CHF Adm None: 0%, Mild: 0%,M-S: 26%
None: 0%, Mild: 2%,M-S: 5%
MR: Mitral Regurgitation; STEMI: ST elevation Myocardial Infarction; F/U: follow-up; PTCA: Percutaneous transluminal coronary angioplasty; PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery BypassGrafting; M-S: moderate to severe MR; Card Death: Cardiovascular Death; CHF Adm: Congestive Heart Failure Admission; NR: Not Reported.
MacH
aalanyet
al.CardiovascularUltrasound
2014,12:14Page
8of
10http://w
ww.cardiovascularultrasound.com
/content/12/1/14
MacHaalany et al. Cardiovasc Ultrasound, 2014

higher rates of surgical mitral valve revascularizationwith concurrent valvular correction.Functional IMR has an important prognostic impact
after myocardial infarction. It is generated by papillarymuscles displacement secondary to the infarcted LV
[26]. Due to the non-extensibility of the chordae, pa-pillary muscle translation exerts traction on leafletsthrough strut chordae implanted on the leaflets body[27,28]. This produces tethering with apical and lateralleaflets displacement [26,29], annular flattening and
Table 3 Echocardiographic characteristics at baseline and follow-upVariable ALL (n = 174; 100%) No MR (n = 95; 55%) Mild MR (n = 60; 34%) Moderate or severe MR
(n = 19; 11%)P value
Baseline (POST-PCI)
LVEDD (mm) 47 ± 6 46 ± 1 47 ± 1 48 ± 1 0.40
LVESD (mm) 35 ± 7 34 ± 1 36 ± 1 38 ± 2 0.02
LVESD >40 mm 39 (22%) 15 (16%) 18 (30%) 6 (32%) 0.07
LVEDV (ml) 102 ± 35 100 ± 4 104 ± 5 107 ± 8 0.68
LVESV (ml) 57 ± 29 53 ± 3 59 ± 4 66 ± 7 0.16
LVEF (%) 46 ± 12 48 ± 1* 45 ± 2* 41 ± 3 0.03
LV sphericity – diastole (%) 0.55 ± 0.07 0.54 ± 0.01 0.56 ± 0.01 0.56 ± 0.02* 0.29
LA volume - indexed (ml/m2) 26 ± 9 23 ± 1* 28 ± 1 36 ± 2 <0.0001
MR – Vena Contracta (cm) 0 [0 – 0.23] 0 [0 – 0]* 0.19 [0.10 – 0.27] 0.62 [0.53 – 0.7]* <0.0001
PASP (mmHg) 29 ± 10 26 ± 1 29 ± 1 43 ± 3 <0.0001
Long-term follow-up
LVEDD (mm) 48 ± 9 48 ± 1 48 ± 1 51 ± 2 0.34
LVESD (mm) 35 ± 10 34 ± 1 35 ± 1 39 ± 2 0.11
LVEDV (ml) 114 ± 47 111 ± 5 116 ± 6 120 ± 10 0.71
LVESV (ml) 59 ± 40 56 ± 4 60 ± 5 72 ± 9 0.27
LVEF (%) 52 ± 13 53 ± 1* 52 ± 2* 44 ± 3 0.02
LV sphericity – diastole (%) 0.57 ± 0.09 0.55 ± 0.01 0.57 ± 0.01 0.61 ± 0.02* 0.01
LA size - indexed (ml/m2) 30 ± 12 27 ± 1* 30 ± 2 41 ± 3 <0.0001
MR – Vena Contracta (cm) 0.1 [0 – 0.23] 0 [0 – 0.19]* 0.12 [0 – 0.24] 0.54 [0.44 – 0.6]* <0.0001
PASP (mmHg) 28 ± 10 26 ± 1 27 ± 1 36 ± 2 0.001
*Difference between baseline and long-term follow-up values is statistically significant; (all p-values ≤ 0.03).LVEDD – Left ventricular end-diastolic diameter; LVESD – Left ventricular end-systolic diameter; LVEDV – Left ventricular end-diastolic volume; LVESV – Leftventricular end-systolic volume; LVEF – Left Ventricular Ejection Fraction; LA – Left atrium; MR- Mitral regurgitation; PASP – Pulmonary artery systolic pressure.
Figure 1 Distribution of ischemic functional mitral regurgitation (MR) over time according to baseline MR grade.
MacHaalany et al. Cardiovascular Ultrasound 2014, 12:14 Page 5 of 10http://www.cardiovascularultrasound.com/content/12/1/14
MacHaalany et al. Cardiovasc Ultrasound, 2014

enlargement, all elements that converge to yield func-tional IMR. The prevalence has been variable (Table 5)as it is dependent on the detection technique utilized. Itranges from <20% in angiographic studies [10-14] to ashigh as 60% in echocardiographic studies [1-8,15,30-33],with moderate or severe IMR accounting for <5% and10-15% of cases, respectively. This discrepancy reflectsthe selection biases inherent to most studies, as most in-volved a heterogeneous sample size that included a mix-ture of STEMI and NSTEMI patients. Some wereexposed to selection bias as they were based on sub-analysis of larger randomized trials [1,10,12,13] whileothers were samples of patients admitted to the coronarycare unit. Furthermore, various studies were solely basedon thrombolytic therapy [1,10,12-14,32,33], which is rec-ognized as a less effective treatment in STEMIs vs. pri-mary PCI [34], and ultimately not everyone excluded
patients with previous MI [2-4,32]. Our study attemptedto take into consideration most of these issues by select-ing a homogenous sample population composed of all-comers presenting to the catheterization laboratory inthe setting of primary PCI setting, and in the first12 hours of symptoms onset. Additionally, these patientswere all treated within today’s standard of care.In accordance to previous studies [1,7,9,13,30], our data
indicate that female gender is an important determinant inthe severity of early IMR. This finding may partly providean explanation for the higher incidence of post-STEMImortality seen in females [35-37]. We have also found thatlonger ischemic time prior to PCI is an important deter-minant in the severity of IMR. This finding once again em-phasizes the notion of early opening of the infarcted-arterywith the aim of salvaging as much muscle mass as possible;therefore reducing the rate of IMR occurrence.
Table 4 Cumulative clinical outcomes according to early ischemic MR severityVariable All (n = 174; 100%) No MR (n = 95; 55%) Mild MR (n = 60; 34%) Moderate or severe MR
(n = 19; 11%)P value
Death 2 (1%) 0 (0%) 1 (2%) 1 (5%) 0.13
Stroke 3 (2%) 2 (2%) 1 (2%) 0 (0%) 0.81
Re-infarction 13 (8%) 10 (11%) 2 (3%) 1 (5%) 0.23
Re-Hospitalization for CHF 2 (1%) 0 (0%) 1 (2%) 1 (5%) 0.13
Percutaneous coronary intervention 9 (5%) 6 (6%) 2 (3%) 1 (5%) 0.72
Coronary artery bypass grafting 14 (8%) 5 (6%) 4 (7%) 5 (26%) 0.008
Annuloplasty or mitral valve surgery 5 (3%) 0 (0%) 0 (0%) 5 (26%) <0.0001
MACE* 33 (19%) 15 (16%) 10 (17%) 8 (42%) 0.02
*Major adverse cardiac events (MACE): defined as a combined endpoint of death, MI, stroke, re-hospitalization for congestive heart failure, PCI or CABG and mitralrepair or replacement.MR: Mitral Regurgitation; CHF: Congestive Heart Failure; MACE: Major Adverse Cardiovascular Event.
Figure 2 Kaplan-Meier curves for the combined endpoint of MACE (death, MI, stroke, re-hospitalization for congestive heart failure,PCI or CABG and mitral repair or replacement).
MacHaalany et al. Cardiovascular Ultrasound 2014, 12:14 Page 6 of 10http://www.cardiovascularultrasound.com/content/12/1/14
MacHaalany et al. Cardiovasc Ultrasound, 2014

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 374;4 nejm.org January 28, 2016344
The authors’ full names, academic de-grees, and affiliations are listed in the Appendix. Address reprint requests to Dr. Gelijns at the Department of Popula-tion Health Science and Policy, Icahn School of Medicine at Mount Sinai, 1 Gus-tave L. Levy Pl., Box 1077, New York, NY 10029, or at annetine . gelijns@ mssm . edu.
* A complete list of members of the Cardio-thoracic Surgical Trials Network (CTSN) is provided in the Supplementary Appen-dix, available at NEJM.org.
This article was published on November 9, 2015, at NEJM.org.
N Engl J Med 2016;374:344-53.DOI: 10.1056/NEJMoa1512913Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDIn a randomized trial comparing mitral-valve repair with mitral-valve replacement in patients with severe ischemic mitral regurgitation, we found no significant difference in the left ventricular end-systolic volume index (LVESVI), survival, or adverse events at 1 year after surgery. However, patients in the repair group had significantly more recurrences of moderate or severe mitral regurgitation. We now report the 2-year out-comes of this trial.
METHODSWe randomly assigned 251 patients to mitral-valve repair or replacement. Patients were followed for 2 years, and clinical and echocardiographic outcomes were assessed.
RESULTSAmong surviving patients, the mean (±SD) 2-year LVESVI was 52.6±27.7 ml per square meter of body-surface area with mitral-valve repair and 60.6±39.0 ml per square meter with mitral-valve replacement (mean changes from baseline, −9.0 ml per square meter and −6.5 ml per square meter, respectively). Two-year mortality was 19.0% in the re-pair group and 23.2% in the replacement group (hazard ratio in the repair group, 0.79; 95% confidence interval, 0.46 to 1.35; P = 0.39). The rank-based assessment of LVESVI at 2 years (incorporating deaths) showed no significant between-group difference (z score = −1.32, P = 0.19). The rate of recurrence of moderate or severe mitral regurgi-tation over 2 years was higher in the repair group than in the replacement group (58.8% vs. 3.8%, P<0.001). There were no significant between-group differences in rates of serious adverse events and overall readmissions, but patients in the repair group had more serious adverse events related to heart failure (P = 0.05) and cardiovas-cular readmissions (P = 0.01). On the Minnesota Living with Heart Failure question-naire, there was a trend toward greater improvement in the replacement group (P = 0.07).
CONCLUSIONSIn patients undergoing mitral-valve repair or replacement for severe ischemic mitral regurgitation, we observed no significant between-group difference in left ventricular reverse remodeling or survival at 2 years. Mitral regurgitation recurred more fre-quently in the repair group, resulting in more heart-failure–related adverse events and cardiovascular admissions. (Funded by the National Institutes of Health and Canadian Institutes of Health Research; ClinicalTrials.gov number, NCT00807040.)
A BS TR AC T
Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation
D. Goldstein, A.J. Moskowitz, A.C. Gelijns, G. Ailawadi, M.K. Parides, L.P. Perrault, J.W. Hung, P. Voisine, F. Dagenais, A.M. Gillinov, V. Thourani,
M. Argenziano, J.S. Gammie, M. Mack, P. Demers, P. Atluri, E.A. Rose, K. O’Sullivan, D.L. Williams, E. Bagiella, R.E. Michler, R.D. Weisel, M.A. Miller, N.L. Geller, W.C. Taddei-Peters, P.K. Smith, E. Moquete, J.R. Overbey, I.L. Kron,
P.T. O’Gara, and M.A. Acker, for the CTSN*
Original Article
The New England Journal of Medicine Downloaded from nejm.org at BIBLIOTHEQUE UNIV LAVAL SEC ACQ on July 11, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
RÉSULTATS:
Récurrence d’une IM modérée à sévère à 2
ans 58,8% vs. 3,8% (plastie vs RVM ) .
Goldstein, NEJM, 2015

n engl j med 374;4 nejm.org January 28, 2016 349
Surgical Treatment of Severe Ischemic Mitr al Regurgitation
VariableRepair
(N = 126)Replacement
(N = 125) P Value*
no./total no. of patients (%)
Clinical end point
Death 24/126 (19.0) 29/125 (23.2) 0.42
Stroke 10/126 (7.9) 7/125 (5.6) 0.46
Worsening New York Heart Association class† 5/85 (5.9) 5/84 (6.0) 1.0
Rehospitalization for heart failure 27/126 (21.4) 22/125 (17.6) 0.44
Failed index mitral-valve procedure 6/126 (4.8) 0 0.03
Mitral-valve reoperation 4/126 (3.2) 1/125 (0.8) 0.37
Moderate or severe recurrent mitral regurgitation 57/97 (58.8) 3/79 (3.8) <0.001
MACCE‡ 53/126 (42.1) 53/125 (42.4) 0.96
Canadian Cardiovascular Society class III or IV 4/82 (4.9) 0/80 0.19
no. of events (rate/100 patient-yr)
Serious adverse event
Any event 291 (145.6) 247 (129.8) 0.18
Heart failure 48 (24.0) 29 (15.2) 0.05
Neurologic dysfunction 19 (9.5) 10 (5.3) 0.12
Stroke 12 (6.0) 6 (3.2) 0.19
Other condition 7 (3.5) 4 (2.1) 0.41
Myocardial infarction
Nonperioperative 5 (2.5) 1 (0.5) 0.11
Perioperative 0 2 (1.1) 0.16
Renal failure 6 (3.0) 11 (5.8) 0.19
Bleeding 7 (3.5) 10 (5.3) 0.41
Arrhythmia
Supraventricular 26 (13.0) 19 (10.0) 0.38
Ventricular 12 (6.0) 17 (8.9) 0.29
Localized infection 25 (12.5) 29 (15.2) 0.47
Endocarditis 0 2 (1.1) 0.16
Sepsis 12 (6.0) 6 (3.2) 0.19
Respiratory failure 14 (7.0) 19 (10.0) 0.31
Hospitalization
Rehospitalization 152 (78.9) 121 (66.0) 0.14
Readmission for cardiovascular event 93 (48.3) 59 (32.2) 0.01
* P values were calculated by means of the chi-square test or Fisher’s exact test for the clinical end points and Poisson regression for serious adverse events and hospitalizations.
† Worsening of New York Heart Association class was defined as an increase of one grade or more.‡ A major adverse cardiac or cerebrovascular event (MACCE) was defined as death, stroke, hospitalization for heart fail-
ure, worsening heart failure, or mitral-valve reintervention.
Table 1. Clinical End Points, Serious Adverse Events, and Hospitalizations at 2 Years.
The New England Journal of Medicine Downloaded from nejm.org at BIBLIOTHEQUE UNIV LAVAL SEC ACQ on July 11, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
Goldstein, NEJM, 2015

n engl j med 374;4 nejm.org January 28, 2016 347
Surgical Treatment of Severe Ischemic Mitr al Regurgitation
Rates of Death, Reoperation, and RecurrenceOutcomes at 30 days and 1 year have been de-scribed previously.1 At 2 years, we observed no significant difference in cumulative mortality between treatment groups, with a rate of 19.0% in the repair group and 23.2% in the replacement group (Table 1), for a hazard ratio with mitral-valve repair of 0.79 (95% confidence interval [CI], 0.46 to 1.35; P = 0.39 by the log-rank test) (Fig. 1).
Six patients who were assigned to the repair group were converted to valve replacement be-fore leaving the operating room because the re-pair procedure did not sufficiently correct the mitral regurgitation, and 4 patients in the repair group underwent mitral-valve reoperation at a later date (at 10, 41, 268, and 434 days after the procedure). One recipient of a bioprosthesis in the replacement group underwent a mechanical replacement at 18 months to correct leaflet im-mobility and severe mitral regurgitation. Three patients in the replacement group had a paraval-vular leak of mild severity but did not require intervention.
The proportion of patients with recurrent moderate or severe mitral regurgitation at some point during the 2-year period was significantly higher in the repair group than in the replace-ment group (58.8% vs. 3.8%, P<0.001). Severe mitral regurgitation was present in 14% of the patients with recurrence in the repair group and in none of the patients in the replacement group. In the repair group, patients without recurrent moderate or severe mitral regurgitation within 2 years had a greater degree of reverse remodel-ing than did patients who had such regurgita-tion (LVESVI, 62.6±26.9 and 42.7±26.4, respec-tively; P<0.001).
At 2 years, 75 of 111 patients (67.6%) who underwent mitral annuloplasty died, had moder-ate or severe mitral regurgitation, or underwent mitral-valve reoperation, as compared with 31 of 107 patients (29.0%) in the replacement group (relative risk, 2.3; 95% CI, 1.69 to 3.22; P<0.001). Rates of the composite end point over time are provided in Fig. 2.
Composite Cardiac End Point, Adverse Events, and Hospitalization
At 2 years, the rates of major adverse cardiac or cerebrovascular events did not differ significantly
between the treatment groups (42.1% in the re-pair group and 42.4% in the replacement group) (Table 1), for a hazard ratio of 0.97 (95% CI, 0.66 to 1.42; P = 0.88 by the log-rank test) (Fig. 3). There also was no significant difference in the rate of the individual components of the primary end point (Table 1). The repair group had signifi-cantly more serious heart-failure events at 2 years (24.0 per 100 patient-years vs. 15.2 per 100 pa-tient-years, P = 0.05), although the rates of other serious adverse events were not significantly different between groups. Overall readmission rates did not differ between groups, but patients in the repair group had a significantly higher rate of readmission for cardiovascular causes (48.3 vs. 32.2 per 100 patient-years, P = 0.01). This difference was largely driven by rehospital-ization for heart failure and the need for an implantable cardioverter–defibrillator or perma-nent pacemaker (59 readmissions in the repair group and 38 in the replacement group, for rates of 30.6 vs. 20.7 per 100 patient-years; P = 0.06).
Quality of LifeThe pattern of change in quality-of-life measures over the duration of follow-up was similar in the two groups, with most improvement occurring in the first 6 months after surgery. There were
Figure 1. Time-to-Event Curves for Death.
Shown are the proportions of patients who died in the mitral-valve (MV) repair group and the mitral-valve replacement group at 2 years. The most frequent underlying causes of death were multisystem organ failure (in 20.8% of patients), heart failure (in 17.0%), and sepsis (in 13.2%). The tick marks indicate censored data.
Dea
th (%
)
100
80
90
70
60
40
30
10
50
20
00 6 12 18 24
Month
Hazard ratio, 0.79 (95% CI, 0.46–1.35)P=0.39
No. at RiskMV repairMV replacement
126125
113103
104100
9792
6465
MV repair
MV replacement
The New England Journal of Medicine Downloaded from nejm.org at BIBLIOTHEQUE UNIV LAVAL SEC ACQ on July 11, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
Goldstein, NEJM, 2015

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 374;20 nejm.org May 19, 20161932
The authors’ full names, academic de-grees, and affiliations are listed in the Ap-pendix. Address reprint requests to Dr. Gelijns at the Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai, 1 Gustave L. Levy Pl., Box 1077, New York, NY 10029, or at annetine . gelijns@ mountsinai . org.
* A list of members of the Cardiothoracic Surgical Trials Network (CTSN) is pro-vided in the Supplementary Appendix, available at NEJM.org
Drs. Michler and Smith contributed equal-ly to this article.
This article was published on April 3, 2016, at NEJM.org.
N Engl J Med 2016;374:1932-41.DOI: 10.1056/NEJMoa1602003Copyright © 2016 Massachusetts Medical Society.
BACKGROUNDIn a trial comparing coronary-artery bypass grafting (CABG) alone with CABG plus mitral-valve repair in patients with moderate ischemic mitral regurgitation, we found no significant difference in the left ventricular end-systolic volume index (LVESVI) or survival after 1 year. Concomitant mitral-valve repair was associated with a reduced prevalence of moderate or severe mitral regurgitation, but patients had more adverse events. We now report 2-year outcomes.
METHODSWe randomly assigned 301 patients to undergo either CABG alone or the com-bined procedure. Patients were followed for 2 years for clinical and echocardio-graphic outcomes.
RESULTSAt 2 years, the mean (±SD) LVESVI was 41.2±20.0 ml per square meter of body-surface area in the CABG-alone group and 43.2±20.6 ml per square meter in the combined-procedure group (mean improvement over baseline, −14.1 ml per square meter and −14.6 ml per square meter, respectively). The rate of death was 10.6% in the CABG-alone group and 10.0% in the combined-procedure group (hazard ratio in the combined-procedure group, 0.90; 95% confidence interval, 0.45 to 1.83; P = 0.78). There was no significant between-group difference in the rank-based assessment of the LVESVI (including death) at 2 years (z score, 0.38; P = 0.71). The 2-year rate of moderate or severe residual mitral regurgitation was higher in the CABG-alone group than in the combined-procedure group (32.3% vs. 11.2%, P<0.001). Overall rates of hospital readmission and serious adverse events were similar in the two groups, but neurologic events and supraventricular arrhythmias remained more frequent in the combined-procedure group.
CONCLUSIONSIn patients with moderate ischemic mitral regurgitation undergoing CABG, the ad-dition of mitral-valve repair did not lead to significant differences in left ventricular reverse remodeling at 2 years. Mitral-valve repair provided a more durable correction of mitral regurgitation but did not significantly improve survival or reduce overall adverse events or readmissions and was associated with an early hazard of increased neurologic events and supraventricular arrhythmias. (Funded by the National Insti-tutes of Health and Canadian Institutes of Health Research; ClinicalTrials.gov number, NCT00806988.)
A BS TR AC T
Two-Year Outcomes of Surgical Treatment of Moderate Ischemic Mitral Regurgitation
R.E. Michler, P.K. Smith, M.K. Parides, G. Ailawadi, V. Thourani, A.J. Moskowitz, M.A. Acker, J.W. Hung, H.L. Chang, L.P. Perrault, A.M. Gillinov, M. Argenziano,
E. Bagiella, J.R. Overbey, E.G. Moquete, L.N. Gupta, M.A. Miller, W.C. Taddei-Peters, N. Jeffries, R.D. Weisel, E.A. Rose, J.S. Gammie,
J.J. DeRose, Jr., J.D. Puskas, F. Dagenais, S.G. Burks, I. El-Hamamsy, C.A. Milano, P. Atluri, P. Voisine, P.T. O’Gara, and A.C. Gelijns, for the CTSN*
Original Article
The New England Journal of Medicine Downloaded from nejm.org at BIBLIOTHEQUE UNIV LAVAL SEC ACQ on July 11, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
Michler et al. ,NEJM, 2016
RÉSULTATS:
Récurrence d’une IM modérée à sévère à 2
ans 32,3% vs. 11,2% ( pontages vs
plastie ) .

ON RETIENT
IM modérée à sévère 15 fois plus fréquent
post annuloplastie vs RVM
IM modérée à sévère 3 fois plus fréquent en
absence d’annuloplastie

SOLUTION SIMPLE …
Pas d’intervention nécessaire si IM
modérée/sévère car:
1. Mortalité idem
2. Remodeling similaire
3. Géométrie mitrale pré-op. pas utile

Pas d’intervention nécessaire si IM
modérée/sévère car:
4. Classe III et IV similaires
5. Diminution marginale des hospitalisations
pour insuffisance cardiaque si intervention
sur la mitrale
SOLUTION SIMPLE …

CRITIQUE CAR …
1. Suivi limite de 2 ans
2. La qualité de la vie c’est important ! � hospitalisations cardiaques + épisodes
d’insuffisance cardiaque
3. Classe II + ?

RÉCIDIVE IM post op multifactorielles …
1. Déformation de la géométrie mitrale pré-
opératoire ( mesure complexe ! ) .
2. Remodeling post opératoire .
3. Viabilité ( force de fermeture ) .
4. Trouble de conduction ?

LA RÉCIDIVE DE L’INSUFFISANCE MITRALE EST EXPLIQUÉE PAR LE
TENTING (TETHERING POST OPÉRATOIRE!)

CE QU’IL FAUT RETENIR 2 Types de géométrie mitrale post IM ischémique
FAVORABLE
Distance de tenting <1cm + *surface de tenting <2,5cm² *angle postérieur < 45°
DÉFAVORABLE
a) Symétrique Distance de tenting >10cm
+ *surface de tenting
>2,5cm² * angle postérieur > 45°
b) Asymétrique * angle postérieur > 45°

1. Si IM sévère préopératoire et tenting important: RVM > annuloplastie
2. Si IM modérée préopératoire:
a) Est-elle vraiment modérée? b) Tenting important ? /mesure de la
dimension de l’anneau > 35mm c) FE< 35%?

SI OUI À CES 3 QUESTIONS…
Plutôt favorable à un geste sur la valve
mitrale

Sénéchal et al. Am J Cardiol 2010;106:31-37

² Le traitement de l’IM ischémique n’est pas exclusivement chirurgical (PAC/annuloplastie/RVM)
On retient
² La thérapie de resynchronisation peut faire diminuer « l’IM ischémique » si QRS ≥ 130 ms + viabilité a/n de la sonde

Qu’est-ce que le (la) technicien(ne) devrait savoir ?
1. Évaluer la sévérité et le mécanisme de l’IM en
préparatoire est important
2. Évaluer la sévérité de l’IM ischémique de manière
minutieuse (VC/ERO)
3. Si IM ≧ modérée se demander le mécanisme principal
(tenting/restriction feuillet postérieur)

Qu’est-ce que le cardiologue devrait savoir ? 1. Avoir la même démarche que le (la) technicien
(ne);
2. En présence d’une IM ischémique, toujours
regarder l’ECG (BBG ?)
3. Le mécanisme de l’IM ischémique/fonctionnel
peut être mixte (déformation géométrie mitrale/
asynchronie).

CONCLUSION 1) La rupture de pilier post infarctus est rare (≤
1%); elle peut être partielle et difficile à
reconnaître
2) La CIV post infarctus est rare et associée à
une mortalité opératoire très élevée (≥50%);
lorsque possible attendre; considérer ECMO/
device/transplantation

3) La rupture myocardique subaiguë peut
être associée à un survie acceptable si
reconnue précocement

4) Le choix du meilleure traitement de l’IM
ischémique demeure difficile; toutes les
options se doivent d’être considérées en
s’aidant de la sévérité de l’IM, de la
géométrie de l’appareil mitrale et de l’ECG.