Preoperative beta blocker use associated with cerebral ischemia during carotid endarterectomy;...
7
Click here to load reader
Transcript of Preoperative beta blocker use associated with cerebral ischemia during carotid endarterectomy;...

REPORTS OF ORIGINAL INVESTIGATIONS
Preoperative beta blocker use associated with cerebral ischemiaduring carotid endarterectomy
Utilisation preoperatoire d’un beta-bloqueur associee a uneischemie cerebrale au cours d’une endarteriectomie carotidienne
Alexandra Florea, MD • Janet van Vlymen, MD •
Samia Ali, MD • Andrew G. Day, MSc •
Joel Parlow, MD
Received: 3 March 2014 / Accepted: 10 June 2014 / Published online: 2 July 2014
� Canadian Anesthesiologists’ Society 2014
Abstract
Purpose Cerebral ischemia is a known complication of
carotid cross-clamping during carotid endarterectomy.
Selective intraluminal shunting for cerebral protection is
not always effective and carries risks. The purpose of this
study was to identify potentially modifiable risk factors for
intraoperative cerebral ischemia and shunting during
carotid endarterectomy.
Methods We performed an historical case-control chart
review of primary carotid endarterectomies with
electroencephalographic (EEG) monitoring and selective
shunting. Randomized controls and cases that showed
ischemic EEG changes and required shunting were
matched by year of surgery and the presence or absence
of a contralateral carotid occlusion. Detailed perioperative
data were collected for all cases. Results were analyzed
using the Mantel-Haenszel test, analysis of variance, and a
multivariate logistic regression model.
Results Of 523 charts screened, 69 patients had
experienced evidence of cerebral ischemia on clamping
of the carotid and required shunting. These patients were
more likely than their matched controls to have been
receiving regular preoperative beta blockers (33/69 vs 18/
69, respectively; P = 0.01; odds ratio [OR] 2.5; 95%
confidence interval [CI] 1.2 to 5.1). Ipsilateral moderate
carotid stenosis (60-80%) was also associated with
increased risk. An adjusted multivariate regression model
estimated an OR of 3.6 (95% CI 1.5 to 8.9; P = 0.005) for
the association between use of a beta blocker and shunting.
Intraoperative hemodynamic values were similar for the
shunt and control groups as well as for patients receiving
and not receiving preoperative beta blockers.
Conclusion The current study found an association
between regular preoperative use of beta blockers and
intraoperative cerebral ischemia in patients undergoing
carotid endarterectomy. This effect did not relate to
intraoperative hemodynamics.
Resume
Objectif L’ischemie cerebrale est une complication
connue du clampage de la carotide au cours de
l’endarteriectomie carotidienne. Une deviation
endoluminale selective pour la protection cerebrale n’est
pas toujours efficace ni denuee de risques. L’objectif de
cette etude etait d’identifier des facteurs de risque
potentiellement modifiables de l’ischemie cerebrale
peroperatoire et de la deviation endoluminale au cours
de l’endarteriectomie carotidienne.
Methodes Nous avons realise une analyse cas-controles
historiques des endarteriectomies de la carotide primitive
This article is accompanied by an editorial. Please see Can J Anesth
2014; 61: this issue.
Author contributions Samia Ali, Janet van Vlymen, and JoelParlow contributed to the conception of the study. Alexandra Florea,Samia Ali, Janet van Vlymen, and Joel Parlow contributed to thedesign of the study. Alexandra Florea and Samia Ali contributed tothe acquisition of data. Alexandra Florea, Janet van Vlymen, JoelParlow, and Andrew G. Day contributed to the analysis andinterpretation of data and drafting the article. Alexandra Florea,Janet van Vlymen, Joel Parlow, Samia Ali, and Andrew G. Daycontributed to revising the article.
A. Florea, MD � J. van Vlymen, MD � S. Ali, MD �J. Parlow, MD (&)
Department of Anesthesiology and Perioperative Medicine,
Kingston General Hospital, Queen’s University, 76 Stuart Street,
Kingston, ON K7L 2V7, Canada
e-mail: [email protected]
A. G. Day, MSc
Kingston General Hospital Clinical Research Centre, Kingston,
ON, Canada
123
Can J Anesth/J Can Anesth (2014) 61:819–825
DOI 10.1007/s12630-014-0195-9

avec surveillance electroencephalographique (EEG) et
deviation selective. Les controles et cas randomises qui
presentaient des modifications EEG ischemiques et
necessitaient une deviation ont ete apparies en fonction
de l’annee de l’intervention et de la presence (ou absence)
d’une occlusion de la carotide controlaterale. Des donnees
perioperatoires detaillees ont ete recueillies pour tous les
cas. Les resultats ont ete analyses avec le test de Mantel-
Haenszel, une analyse de la variance et un modele de
regression logistique multifactorielle.
Resultats Parmi les 523 dossiers etudies, 69 patients ont
presente des signes d’ischemie cerebrale au clampage de la
carotide et ont necessite une deviation. Ces patients ont ete
plus susceptibles que leurs controles apparies d’avoir recu
des beta-bloqueurs regulierement en preoperatoire
(respectivement, 33/69 contre 18/69; P = 0,01; rapport
de cotes 2,5; intervalle de confiance a 95 % [IC]: 1,2 a 5,1).
Une stenose carotidienne moderee ipsilaterale (60 a 80 %)
a ete egalement associee a l’augmentation du risque. Un
modele de regression logistique multifactorielle a estime un
rapport de cotes de 3,6 (IC a 95 %: 1,5 a 8,9; P = 0,005)
pour l’association entre l’utilisation d’un beta-bloqueur et
la deviation. Les valeurs hemodynamiques peroperatoires
ont ete identiques dans le groupe deviation et le groupe
temoin ainsi que pour les patients ayant recu ou non des
beta-bloqueurs preoperatoires.
Conclusion La presente etude a constate une association
entre l’utilisation reguliere de beta-bloqueurs
preoperatoires et l’ischemie cerebrale peroperatoire chez
des patients subissant une endarteriectomie carotidienne.
Cet effet est sans rapport avec les parametres
hemodynamiques peroperatoires.
Carotid endarterectomy (CEA) has been used for decades
as an effective means of preventing stroke in patients with
severe atheromatous disease of the carotid.1-4 Despite
stroke prevention being its ultimate goal, carotid clamping
during CEA may be complicated by intraoperative cerebral
ischemia. In patients who are monitored with
electroencephalography (EEG), 18-27% have been found
to develop ischemic changes during CEA.5-8 Furthermore,
it has been documented that patients who experienced
intraoperative ischemia had a 7% rate of postoperative
stroke and death compared with 1.9% of those who did not
(P \ 0.001).9 A number of strategies have been employed
for cerebral protection, including routine or selective
intraluminal shunting, although conclusive evidence of
benefit is lacking.10 Furthermore, shunt insertion carries its
own procedural risks and has been associated with
complications such as plaque embolism,11 hemorrhage,
carotid re-stenosis, and postoperative neurocognitive
dysfunction.11-13
Recent evidence has linked the use of beta blockers to
an increased risk of perioperative stroke following a variety
of surgical procedures. The POISE study found an
association between perioperative administration of long-
acting metoprolol and postoperative stroke and death
following noncardiac surgery in patients not receiving
regular beta blocker therapy.14 A meta-analysis published
in 2008 evaluating the use of beta blockers in noncardiac
surgery found an increased risk of stroke in patients who
were started on beta blockers perioperatively (odds ratio
[OR] 2.16; number needed to harm 275).15 In addition,
routine use of preoperative metoprolol has been correlated
with a 4.2-fold increase in perioperative stroke after
noncardiac surgery.16 Nevertheless, a recent study
evaluating the correlation between perioperative use of
beta blockers and postoperative stroke in noncardiac
surgery showed no increased risk for those taking chronic
beta blocker treatment.17 Animal studies have also shown a
correlation between acute beta blockade with metoprolol
and decreased cerebral oxygen tension, potentially through
mechanisms of impaired compensatory cardiac output
response or diminished vasodilation in response to beta
agonists.18,19 In a recent study, bisoprolol was found to be
associated with fewer strokes compared with metoprolol or
atenolol, indicating that beta1 (b1) selectivity may be
associated with less risk.20 Regarding CEA procedures,
risk factors previously identified with shunting include
female sex, history of stroke, contralateral carotid
occlusion, and moderate ipsilateral carotid stenosis.6,9
Studies evaluating risk factors for perioperative stroke
have largely identified non-modifiable patient
characteristics, such as advanced age, vascular disease,
and renal insufficiency.21,22 The purpose of this study was
to identify potentially modifiable risk factors for
intraoperative cerebral ischemia and shunting during
CEA. We postulated that the results of this study could
be meaningful in two ways: First, identifying risk factors
for intraoperative ischemia could potentially lead to a
decrease in its incidence. Secondly, gaining insight into the
mechanisms behind intraoperative cerebral ischemia could
shed light on the rare but devastating complication of
perioperative stroke that has been associated with
significant increases in perioperative morbidity and
mortality.21,22
Methods
The study was approved by the local Research Ethics
Board (REB) and was performed in accordance with the
Ethical Principles of Medical Research as outlined in the
820 A. Florea et al.
123

Declaration of Helsinki. Due to the historical anonymized
design, requirement for written informed consent was
waived by the REB. Patient information was available only
to the investigators and was password protected within
electronic sources.
We screened the hospital records of all patients having
primary carotid endarterectomies carried out with 16-lead
bilateral EEG monitoring by a dedicated EEG technologist
over a ten-year period (November 2000 - November 2010).
Cases were performed by two vascular surgeons at a single
institution. None of the selected patients had ever
undergone contralateral carotid surgery. At this
institution, the surgeons practice selective extravascular
shunting in the event of new ischemic changes on EEG
upon carotid cross-clamping. We identified all cases that
required shunt insertion in response to new documented
EEG changes suggesting ischemia. These cases were
confirmed retrospectively by a neurologist according to
standard criteria, including ipsilateral or bilateral reduction
of EEG voltage in all frequencies or focal delta frequency
slow waves. The remaining charts of patients not requiring
shunting were stratified by year and randomized using a
random number generator on Microsoft Excel� (Excel
version 12.0., Microsoft Corp, Redmond, WA, USA). From
the randomly generated lists, an equal number of controls
were matched to the shunt cases by 1) year of surgery and
2) presence or absence of 100% contralateral carotid
occlusion, as determined by carotid angiography.
We then performed a detailed chart review of all cases
and controls. The collected data included preoperative
comorbidities and medications as well as the degree of
carotid stenosis of the operative and contralateral sides.
Hemodynamic information was collected at various time
points, including pre- and postoperatively, pre-and post-
induction of anesthesia, and highest or lowest overall
values. The preoperative values of blood pressure and heart
rate were chosen from the lowest values of those recorded
at the pre-anesthetic clinic appointment, the history and
physical sheet filled out by the patient’s family physician,
and the preoperative blood pressure in the pre-anesthetic
unit on the day of surgery. Data on anesthetic management
as well as postoperative complications, including incidence
of stroke, transient ischemic attack (TIA), and myocardial
infarction (MI) up to 30 days postoperatively, were also
collected.
Preoperative patient characteristics were compared
between the shunt and control groups using the Mantel-
Haenszel test, stratifying for year and contralateral
occlusion for categorical variables, and by analysis of
variance, blocking by year and contralateral occlusion for
continuous variables. Where significance was found for a
modifiable characteristic, a multivariate logistic regression
model, conditioning on year and contralateral occlusion,
was used to determine the odds of requiring a shunt after
adjusting for the other characteristics. The characteristics
chosen as having the potential to be confounders were: sex,
age, ipsilateral carotid stenosis, diabetes, hypertension,
coronary artery disease (CAD), cholesterol-lowering and
antiplatelet drugs, calcium channel blockers (CCB), beta
blockers, angiotensin converting enzyme inhibitors (ACE-
I), angiotensin receptor blocking (ARB) drugs,
hemoglobin, estimated glomerular filtration rate (eGFR),
and surgeon. As there may have been too many predictors
in this full model for the available data, secondary analysis
included an adjusted model stratifying for year and
contralateral occlusion, but it included only additional
covariates retained by backward-stepwise selection with a
retention criterion of P \ 0.2.
Results
Five hundred and thirty-three records of patients
undergoing primary CEA with scheduled EEG
monitoring were identified at our institution over the ten-
year period. Ten charts were excluded from the study for
the following reasons: four had insufficient information to
determine whether ischemia or shunting occurred, two
operations were aborted due to inoperable anatomy, and
four procedures did not use intraoperative EEG monitoring
because it was not available. Sixty-nine of the remaining
523 patients experienced ischemic changes on EEG at the
time of carotid clamping and underwent shunting, giving
an overall shunt rate of 13%.
Sixty-nine controls were matched to the 69 shunt cases
by year of surgery and presence or absence of contralateral
carotid occlusion, giving a total study population of 138
cases and controls. The preoperative characteristics of
these patients are listed in the Table. The two groups had
similar rates of symptoms (TIA, stroke) at presentation.
Moderate (60-80%) but not severe ([ 80%) carotid
stenosis on the operative side was found to correlate
significantly with intraoperative ischemia and shunting
(P = 0.01). The only other significantly different
preoperative variable between the two groups was the
regular use of preoperative beta blockers, with patients
undergoing shunting for cerebral ischemia more likely to
have received beta blockers (P = 0.01; odds ratio [OR]
2.5; 95% confidence interval [CI] 1.2 to 5.1). All patients
who were receiving regular preoperative beta blocker
therapy, regardless of drug or dose, were considered in the
analysis. All other preoperative patient characteristics
(comorbid conditions and preoperative medications) were
similar (Table).
A multivariate logistic regression model, conditioning
on year of surgery and contralateral carotid occlusion, was
Beta blockers associated with cerebral ischemia 821
123

used to assess the effect of beta blockers on the odds of
requiring a shunt after adjusting for sex, age, degree of
ipsilateral carotid stenosis, diabetes, hypertension, CAD,
cholesterol-lowering medication, antiplatelet medication,
CCB medication, ACE-I/ARB medication, hemoglobin,
eGFR, and surgeon. The full multivariable logistic
regression model estimates an OR of 3.7 (95% CI 1.4 to
9.6; P = 0.01). Accounting for the fact that the full model
may have too many predictors for the available data, we
also include the adjusted model with CAD, ACE-I/ARB,
degree of ipsilateral carotid stenosis, history of stroke,
history of TIA, hemoglobin, and surgeon as covariates for
adjustment. This model estimated an OR of 3.6 (95% CI
1.5 to 8.9; P = 0.005) for the association between regular
use of preoperative beta blockers and the requirement for
shunting.
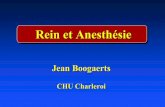
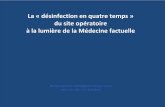
The mean values for heart rate and systolic blood
pressure were similar between the shunt and non-shunt
groups at four time periods (Fig. 1). Systolic blood
pressure was similar and heart rate was significantly
lower in patients who were receiving beta blockers
(P = 0.001) (Fig. 2).
All patients had general anesthesia, with exact
techniques used at the discretion of the specific
anesthesiologists. Patients were induced with propofol or
sodium thiopental, and anesthesia was maintained with
desflurane or sevoflurane and a short-acting opioid.
Hypotension was treated with intravenous fluid and
phenylephrine or ephedrine where appropriate.
Five patients in our study population experienced
perioperative strokes; all had exhibited intraoperative
cerebral ischemia and had undergone shunting. No
strokes occurred in the non-shunted control group. One
of these patients had a hemoglobin value of 90 mg�L-1 on
the day the stroke occurred, while the other four had
hemoglobin values [ 110 mg�L-1. Three of the patients
had watershed strokes; only one of these patients was
taking beta blockers and died from the stroke two days
postoperatively. The remaining two patients, neither of
whom was receiving beta blockers, had strokes caused by
thromboembolism in the immediate postoperative period.
They both returned to the operating room for internal
carotid artery thrombectomy procedures. In addition, four
patients experienced a perioperative MI; all of these
occurred in the shunt group, and three of the four had
been receiving perioperative beta blockers (not significant
between groups).
Discussion
This study aimed to identify preoperative patient
characteristics that are associated with EEG changes
during CEA which are indicative of cerebral ischemia at
the time of carotid clamping and the subsequent need for
shunting. This novel study determined that regular
preoperative use of beta blockers was associated with
intraoperative ischemia and shunting. Secondly, as
previously reported by Ballotta et al.,6 moderate carotid
stenosis on the ipsilateral side was also predictive of
ischemia. This suggests that there may be a greater relative
drop in ipsilateral blood flow with a moderately diseased
artery, whereas the development of collateral circulation in
Table Preoperative characteristics and results of univariate analysis
Shunt
(n = 69)
No shunt
(n = 69)
P
value
Mean (SD) age 70 (8) 70 (9) 0.62
Sex
Male 44 (64) 50 (72) 0.27
Female 25 (36) 19 (28)
Hypertension 59 (86) 53 (77) 0.20
Coronary artery disease 23 (33) 27 (39) 0.40
Diabetes 20 (29) 14 (20) 0.23
Cholesterol-lowering drug 50 (72) 49 (71) 0.92
Antiplatelet drug 66 (96) 67 (97) 0.76
Calcium channel blocker 28 (41) 19 (28) 0.10
ACE-I/ARB 43 (62) 39 (57) 0.41
Beta blocker 33 (48) 18 (26) 0.01
Previous TIA/stroke
Asymptomatic 7 (10) 4 (6)
TIA 30 (43) 39 (57) 0.25
Stroke 32 (46) 26 (38)
Smoking
Prior 33 (48) 38 (55) 0.57
Current 23 (33) 17 (25)
Ipsilateral stenosis
60-80% 48 (70) 31 (45) 0.01
C 80% 21 (30) 38 (55)
Contralateral stenosis
\ 60% 42 (61) 41 (59) N/A
60-99% 10 (14) 11 (16)
100% 17 (25) 17 (25)
Mean (SD) preoperative
hemoglobin
131 (16) 136 (18) 0.12
Mean (SD) preoperative
eGFR
67 (26) 72 (20) 0.22
Surgeon
A 31 (45) 42 (61) 0.07
B 38 (55) 27 (39)
Data expressed as number of patients (percent) unless otherwise
indicated. TIA = transient ischemic attack; ACE-I = angiotensin
converting enzyme inhibitors; ARB = angiotensin receptor blocking;
eGFR = estimated glomerular filtration rate; N/A = not applicable;
TIA = transient ischemic attack
822 A. Florea et al.
123

patients with severe carotid occlusion may be protective
against perioperative ischemia.6 A number of clinical
investigations have suggested a link between use of beta
blockers and stroke in a variety of perioperative settings. A
recent study by Mashour et al. found that preoperative use
of metoprolol was associated with an increased risk of
perioperative stroke.16 The POISE study showed a higher
incidence of perioperative stroke and death related to
stroke in patients undergoing noncardiac surgery who were
randomized to receive perioperative long-acting
metoprolol.14 Unlike the current study, these patients had
not been taking beta blockers preoperatively, and the dose
of metoprolol had not been fully titrated and optimized.
The POISE study also found a strong association between
postoperative hypotension – which was more common in
patients receiving the study drug – and stroke. This
suggests the possible mechanism that beta blockers may
cause clinically significant hypotension, which in turn may
lead to cerebral hypoperfusion.14,23
The current study compared intraoperative
hemodynamic data between patients who developed
cerebral ischemia and those who did not. There were no
differences in heart rate or systolic blood pressure between
these groups. In addition, there was no difference in blood
pressure between those receiving beta blockers and the
control group. Therefore, our study found neither that
clinically significant hypotension was related to the
development of cerebral ischemia, nor that the
mechanism of the higher frequency of ischemia in beta
blocked patients was related to hypotension.
Another potential mechanism for intraoperative
ischemia related to beta blockers could be an alteration
in cerebral blood flow caused by impaired autoregulation.
Two studies examining the relationship between stump
pressure at carotid clamping and ipsilateral middle cerebral
artery (MCA) blood velocities determined that MCA blood
velocity after carotid clamping depends on collateral blood
flow as well as autoregulation.24,25 Collateral blood flow
determines the initial drop in MCA velocity, and
autoregulation is responsible for the changes that occur in
the following 10-15 sec.25 Beta blockers could act to
reduce cerebral blood flow autoregulation by inhibiting
vasodilation through blockade of vascular beta2-
adrenoreceptors. This theory is supported by recent
evidence from a mouse model, where it was found that
metoprolol inhibited both isoproterenol (a b1 and b2 non-
specific receptor agonist) and clenbuterol (a b2 specific
agonist) mediated vasodilation in the mesenteric artery and
the posterior communicating artery.19 On a background of
reduced cerebral blood flow caused by carotid clamping,
even a minor inhibition of autoregulation through beta
blockade could potentially lead to cerebral ischemia. A
large study has found that selective b1 antagonism with
bisoprolol is associated with fewer postoperative strokes
compared with the less selective metoprolol and atenolol.20
Another recent study found that preoperative metoprolol,
but not atenolol, was associated with postoperative stroke
after noncardiac surgery.16 Thus, in the current study, the
type of beta blocker may have rendered certain patients
more likely to experience ischemia upon cross-clamping.
Nevertheless, the limited sample size and variety of beta
blockers used in these patients precluded testing for this
hypothesis.
An association between anemia in beta blocked subjects
and cerebral ischemia has been shown in animal and
human models.18,20,26 In the current study, preoperative
hemoglobin was factored into the multivariate model and
showed no effect on episodes of cerebral ischemia. As
opposed to previous work,20 however, this was not an
anemic population (only one patient had a preoperative
hemoglobin \ 90 mg�L-1), and the carotid cross-clamping
event typically takes place before any significant bleeding
occurs.
All five patients in this study who suffered perioperative
strokes had undergone shunting procedures, and three of
these had postoperative complications related to their
operative site (i.e., hemorrhage, thrombus formation).
Nevertheless, no patient had a hemoglobin
60
80
100
120
140
160
180
200
(a)
(b)
Preoperative Post-induction Highest Lowest
30
40
50
60
70
80
90
100
Preoperative Post-induction Highest Lowest
Fig. 1 Hemodynamics for shunted and non-shunted patients. Systolic
blood pressure (a, mmHg) and heart rate (b, beats�min-1) for patients
who underwent shunting (n = 69, blue) and no-shunt controls
(n = 69, red). Preoperative values represent the lowest values
recorded prior to surgery. Post-induction values were the lowest
documented values within 10 minutes of induction. Highest and
lowest values represent range of intraoperative data points. Data
represent mean ± standard deviation (Color figure online)
Beta blockers associated with cerebral ischemia 823
123

value \ 90 mg�L-1 at the time of the stroke. While
shunting is a valuable tool for restoring blood flow to
ischemic areas during carotid clamping, increased
manipulation of the carotid artery can lead to
complications at the operative site.10 Regarding the
postoperative strokes, it is not possible to confirm
whether factors predisposing to ischemia, or the shunts
themselves, contributed to the development of permanent
deficits. This highlights the importance of identifying
potential risk factors for ischemia to avoid unnecessary
shunt procedures in the first place. Additionally,
postoperative MIs were also identified only in patients
who underwent shunting. It must be emphasized that no
routine screening with biomarkers for MI was carried out
in this population, so the true incidence of perioperative MI
is not known.
Limitations of the current study relate primarily to the
retrospective design. In particular, documentation of
hemodynamic changes and treatment of these events may
be unreliable or lacking. Nevertheless, the expected
significantly lower heart rate in beta blocked patients
adds validity to the data. Although 523 documented
procedures were performed during the ten-year period,
the overall event rate was only 13%. A larger sample size
may have allowed the identification of other risk factors
that were not shown in this study, e.g., those related to
anesthetic drugs or different types of beta blockers.
Furthermore, the incidence of some secondary findings,
such as postoperative stroke and MI, was too low to form
conclusions about associated factors. There was limited
availability of control cases matched for both year and
presence or absence of 100% contralateral occlusion;
therefore, only 1:1 case to control matching could be
accomplished. Although use of beta blockers was identified
as a risk factor for cerebral ischemia during CEA, it is
critical to point out that a conclusion cannot be drawn that
stopping beta blockers perioperatively would reduce this
complication, and in fact, it could potentially lead to
adverse cardiac outcomes. Finally, although careful
analysis revealed no differences in comorbid medical
conditions between the patients receiving or not receiving
preoperative beta blocker therapy, it remains possible that
use of beta blockers represents a marker for other
characteristics that predisposed those patients to
intraoperative cerebral ischemia, rather than an indicator
for a cause and effect relationship.
In summary, this novel study reports an association
between regular preoperative use of beta blockers and
intraoperative ischemia with EEG changes that
necessitated shunt placement during CEA. This adds to a
growing body of literature suggesting a relationship
between beta blockers and the potential for cerebral
ischemia in other clinical situations. As this effect did
not relate to intraoperative hemodynamics in the current
study, it is postulated that this observation could be caused
by impaired vasodilation and autoregulation of cerebral
blood flow in response to carotid clamping. While use of
beta blockers was identified as a potential risk factor for
cerebral ischemia during CEA, we do not advocate abrupt
discontinuation of beta blockers. Further research and
larger scale studies are required to establish the further role
of beta blockers in cerebral ischemia and perioperative
stroke as well as any therapeutic implications of this
relationship.
Acknowledgements The authors sincerely thank Dr. Gregory Hare,
University of Toronto, for his insightful editorial comments and Dr.
Donald Brunet, Queen’s University, for contributing his neurologic
expertise and EEG interpretation.
Funding No funding sources were used in the performance of this
study.
Conflict of interest All authors deny any conflict of interest related
to this study.
60
80
100
120
140
160
180
200
Preoperative Post-induction Highest Lowest
30
40
50
60
70
80
90
100
Preoperative Post-induction Highest Lowest
(a)
(b)
Fig. 2 Hemodynamics for beta blocked and non-beta blocked
patients. Systolic blood pressure (a, mmHg) and heart rate (b,
beats�min-1) for patients receiving beta blockers preoperatively (blue)
and patients not receiving beta blockers (red), in the 138 cases and
matched controls. Preoperative values represent the lowest values
recorded prior to surgery. Post-induction values were the lowest
documented values within 10 minutes of induction. Highest and
lowest values represent range of intraoperative data points. Data
represent mean ± standard deviation (Color figure online)
824 A. Florea et al.
123

References
1. North American Symptomatic Carotid Endarterectomy Trial
Collaborators. Beneficial effect of carotid endarterectomy in
symptomatic patients with high grade carotid stenosis. N Engl J
Med 1991; 325: 445-53.
2. European Carotid Surgery Trialists’ Collaborative Group.
Randomised trial of endarterectomy for recently symptomatic
carotid stenosis: final results of the MRC European Carotid
Surgery Trial (ECST). Lancet 1998; 351: 1379-87.
3. Executive Committee for the Asymptomatic Carotid
Atherosclerosis Study. Endarterectomy for asymptomatic carotid
artery stenosis. JAMA 1995; 273: 1421-8.
4. Mohammed N, Anand SS. Prevention of disabling and fatal
strokes by successful carotid endarterectomy in patients without
recent neurological symptoms: randomized controlled trial. MRC
asymptomatic carotid surgery trial (ACST) collaborative group.
Lancet 2004; 363: 1491-502.
5. Schneider JR, Droste JS, Schindler N, Golan JF, Bernstein LP,
Rosenberg RS. Carotid endarterectomy with routine
electroencephalography and selective shunting: influence of
contralateral internal carotid artery occlusion and utility in
prevention of perioperative strokes. J Vasc Surg 2002; 35:
1114-22.
6. Ballotta E, Saladini M, Gruppo M, Mazzalai F, Da Giau G,
Baracchini C. Predictors of electroencephalographic changes
needing shunting during carotid endarterectomy. Ann Vasc Surg
2010; 24: 1045-52.
7. Rijsdijk M, Ferrier C, Laman M, Kesecioglu J, Stam K, Slooter A.
Detection of ischemic electroencephalography changes during
carotid endarterectomy using synchronization likelihood analysis.
J Neurosurg Anesthesiol 2009; 21: 302-6.
8. Woodworth GF, McGirt MJ, Than KD, Huang J, Perler BA,
Tamargo RJ. Selective versus routine intraoperative shunting
during carotid endarterectomy: a multivariate outcome analysis.
Neurosurgery 2007; 61: 1170-6; discussion 1176-7.
9. Mayer RC, Bingley J, Westcott MJ, et al. Intraoperative
neurological changes in 1665 regional anaesthetic carotid
endarterectomies predicts postoperative stroke. ANZ J Surg
2007; 77: 49-53.
10. Rerkasem K, Rothwell PM. Routine or selective carotid artery
shunting for carotid endarterectomy (and different methods of
monitoring in selective shunting). Cochrane Database Syst Rev
2009; 4: CD000190.
11. Ott DA, Cooley DA, Chapa L, Coelho A. Carotid endarterectomy
without temporary intraluminal shunt. Study of 309 consecutive
operations. Ann Surg 1980; 191: 708-14.
12. Hudorovic N, Lovricevic I, Hajnic H, Ahel Z. Postoperative
internal carotid artery restenosis after local anesthesia: presence
of risk factors versus intraoperative shunt. Interact Cardiovasc
Thorac Surg 2010; 11: 182-4.
13. Mazul-Sunko B, Hromatko I, Tadinac M, et al. Subclinical
neurocognitive dysfunction after carotid endarterectomy – the
impact of shunting. J Neurosurg Anesthesiol 2010; 22: 195-201.
14. POISE Study Group; Devereaux PJ, Yang H, Yusuf S, et al.
Effects of extended-release metoprolol succinate in patients
undergoing non-cardiac surgery (POISE trial): a randomised
controlled trial. Lancet 2008; 371: 1839-47.
15. Bangalore S, Wetterslev J, Pranesh S, Sawhney S, Gluud C,
Messerli FH. Perioperative beta blockers in patients having non-
cardiac surgery: a meta-analysis. Lancet 2008; 372: 1962-76;
Erratum in Lancet 2009; 373: 1764.
16. Mashour GA, Sharifpour M, Freundlich RE, et al. Perioperative
metoprolol and risk of stroke after noncardiac surgery.
Anesthesiology 2013; 119: 1340-6.
17. van Lier F, Schouten O, van Domburg RT, et al. Effect of chronic
beta-blocker use on stroke after noncardiac surgery. Am J Cardiol
2009; 104: 429-33.
18. Ragoonanan TE, Beattie WS, Mazer CD, et al. Metoprolol
reduces cerebral tissue oxygen tension after acute hemodilution
in rats. Anesthesiology 2009; 111: 998-1000.
19. El Beheiry MH, Heximer SP, Voigtlaender-Bolz J, et al.
Metoprolol impairs resistance artery function in mice. J Appl
Physiol 1985; 2011(111): 1125-33.
20. Ashes C, Judelman S, Wijeysundera DN, et al. Selective b1-
antagonism with bisoprolol is associated with fewer postoperative
strokes than atenolol or metoprolol: a single-center cohort study of
44,092 consecutive patients. Anesthesiology 2013; 119: 777-87.
21. Mashour GA, Shanks AM, Kheterpal S. Perioperative stroke and
associated mortality after noncardiac, nonneurologic surgery.
Anesthesiology 2011; 114: 1289-96.
22. Sharifpour M, Moore LE, Shanks AM, Didier TJ, Kheterpal S,
Mashour GA. Incidence, predictors, and outcomes of
perioperative stroke in noncarotid major vascular surgery.
Anesth Analg 2013; 116: 424-34.
23. Bijker JB, Gelb AW. Review article: The role of hypotension in
perioperative stroke. Can J Anesth 2013; 60: 159-67.
24. Zachrisson H, Jatuzis D, Blomstrand C, Holm J, Volkmann R.
Middle cerebral artery circulation during carotid surgery. A
transcranial Doppler study. Scand Cardiovasc J 2000; 34: 597-
602.
25. Spencer MP, Thomas GI, Moehring MA. Relation between
middle cerebral artery blood flow velocity and stump pressure
during carotid endarterectomy. Stroke 1992; 23: 1439-45.
26. Hu T, Beattie WS, Mazer CD, et al. Treatment with a highly
selective b1 antagonist causes dose-dependent impairment of
cerebral perfusion after hemodilution in rats. Anesth Analg 2013;
116: 649-62.
Beta blockers associated with cerebral ischemia 825
123