Les Hôpitaux Universitaires de STRASBOURG
55
Les Hôpitaux Universitaires de STRASBOURG
Transcript of Les Hôpitaux Universitaires de STRASBOURG

Les Hôpitaux Universitaires de STRASBOURG

1
4

M HASSELMANN SRLF 2011
La nutrition hypocalorique non intentionnelle est courante dans la pratique clinique o erreurs de prescription o erreurs d’administration o fréquentes dysfonctions du tube digestif, o jeûne imposé : procédures diagnostiques ou
thérapeutiques, pratiques de soins.
Apports caloriques reçus : 50% à 70% des besoins calculés
7
M HASSELMANN SRLF 2011
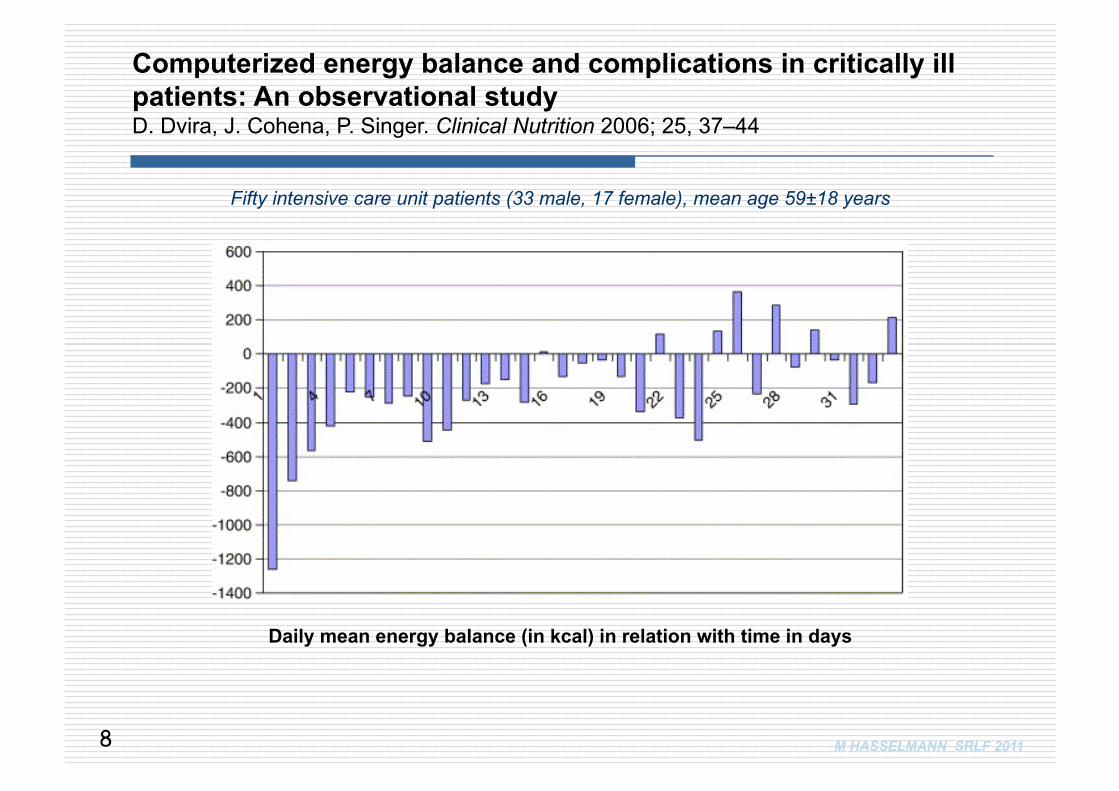
Daily mean energy balance (in kcal) in relation with time in days
Computerized energy balance and complications in critically ill patients: An observational study D. Dvira, J. Cohena, P. Singer. Clinical Nutrition 2006; 25, 37–44
Fifty intensive care unit patients (33 male, 17 female), mean age 59±18 years
8
M HASSELMANN SRLF 2011
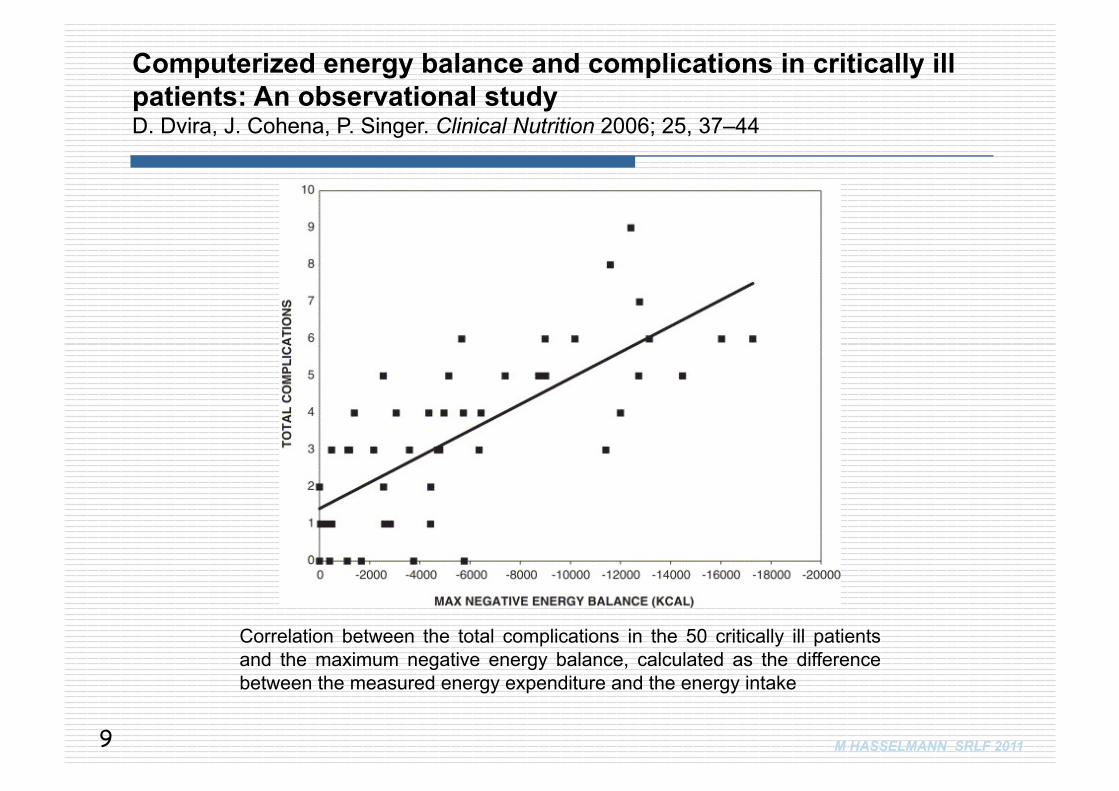
Correlation between the total complications in the 50 critically ill patients and the maximum negative energy balance, calculated as the difference between the measured energy expenditure and the energy intake
Computerized energy balance and complications in critically ill patients: An observational study D. Dvira, J. Cohena, P. Singer. Clinical Nutrition 2006; 25, 37–44
9
M HASSELMANN SRLF 2011
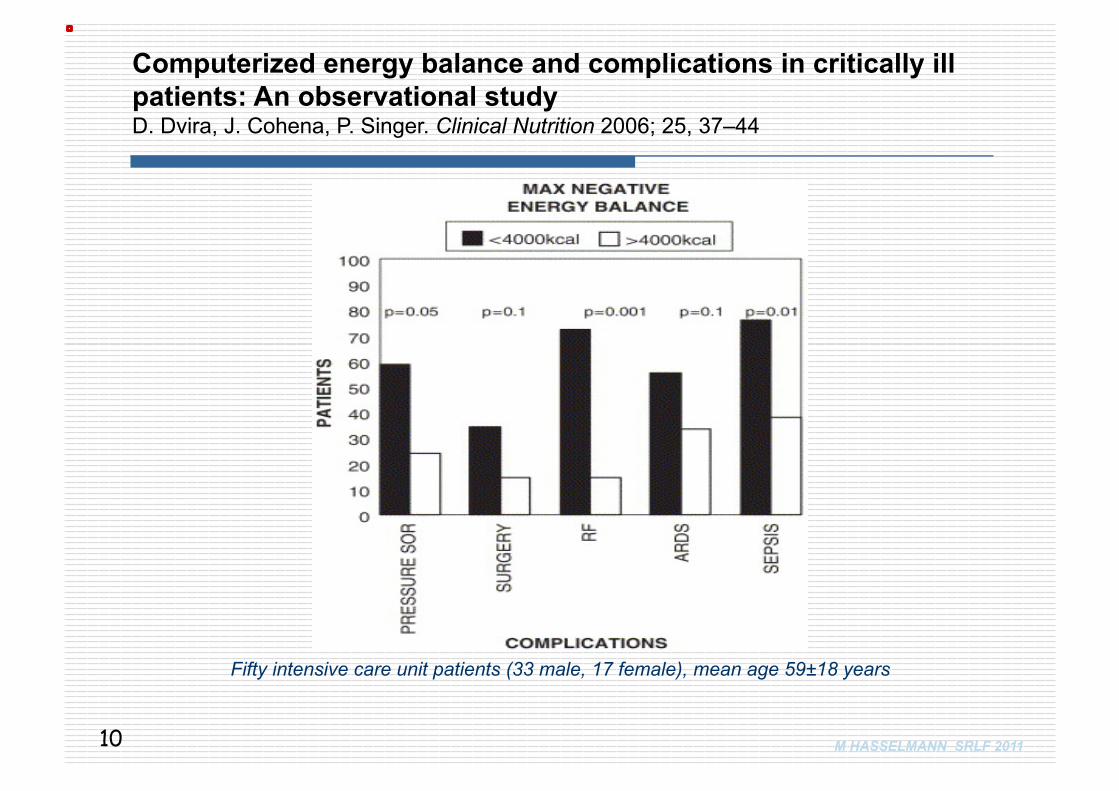
Computerized energy balance and complications in critically ill patients: An observational study D. Dvira, J. Cohena, P. Singer. Clinical Nutrition 2006; 25, 37–44
Fifty intensive care unit patients (33 male, 17 female), mean age 59±18 years
10
M HASSELMANN SRLF 2011
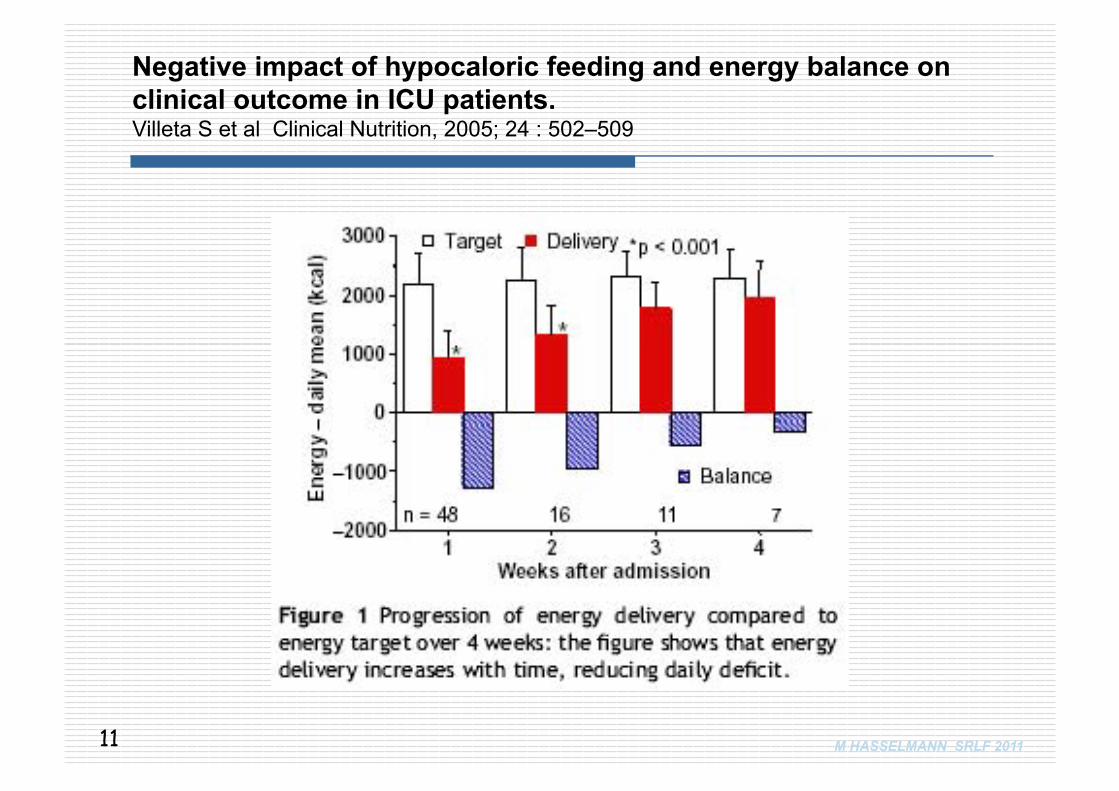
Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Villeta S et al Clinical Nutrition, 2005; 24 : 502–509
11
M HASSELMANN SRLF 2011
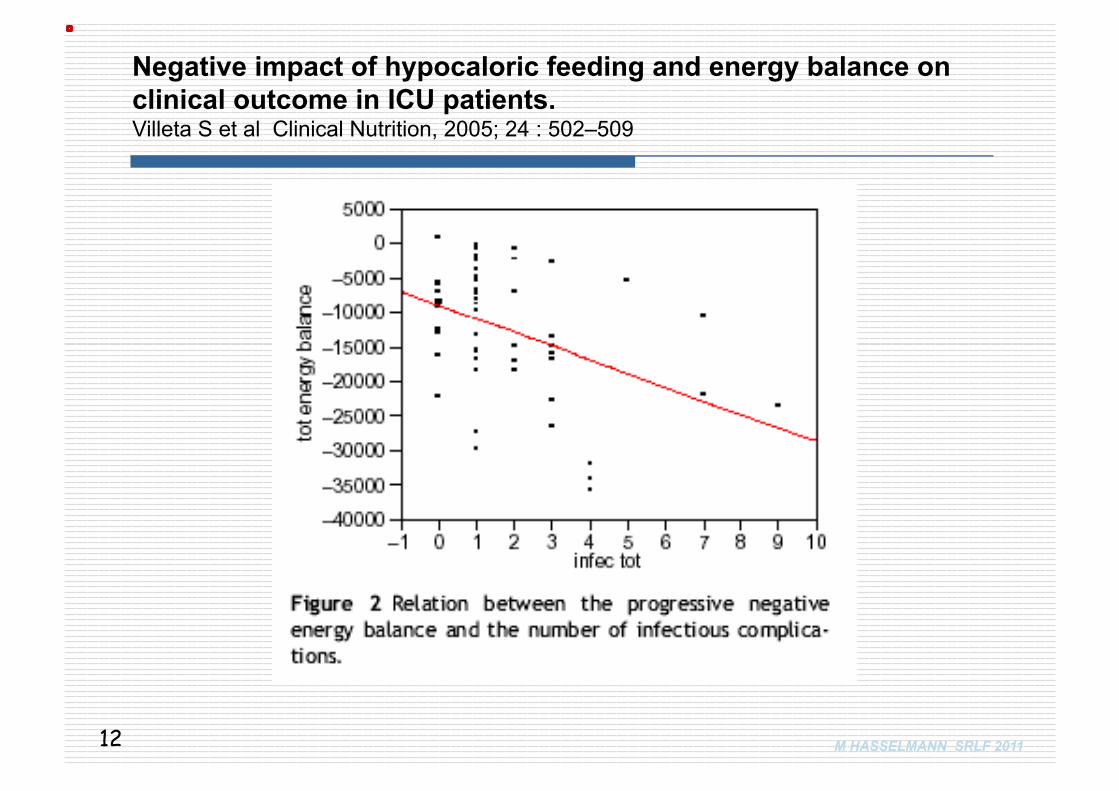
Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Villeta S et al Clinical Nutrition, 2005; 24 : 502–509
12
M HASSELMANN SRLF 2011
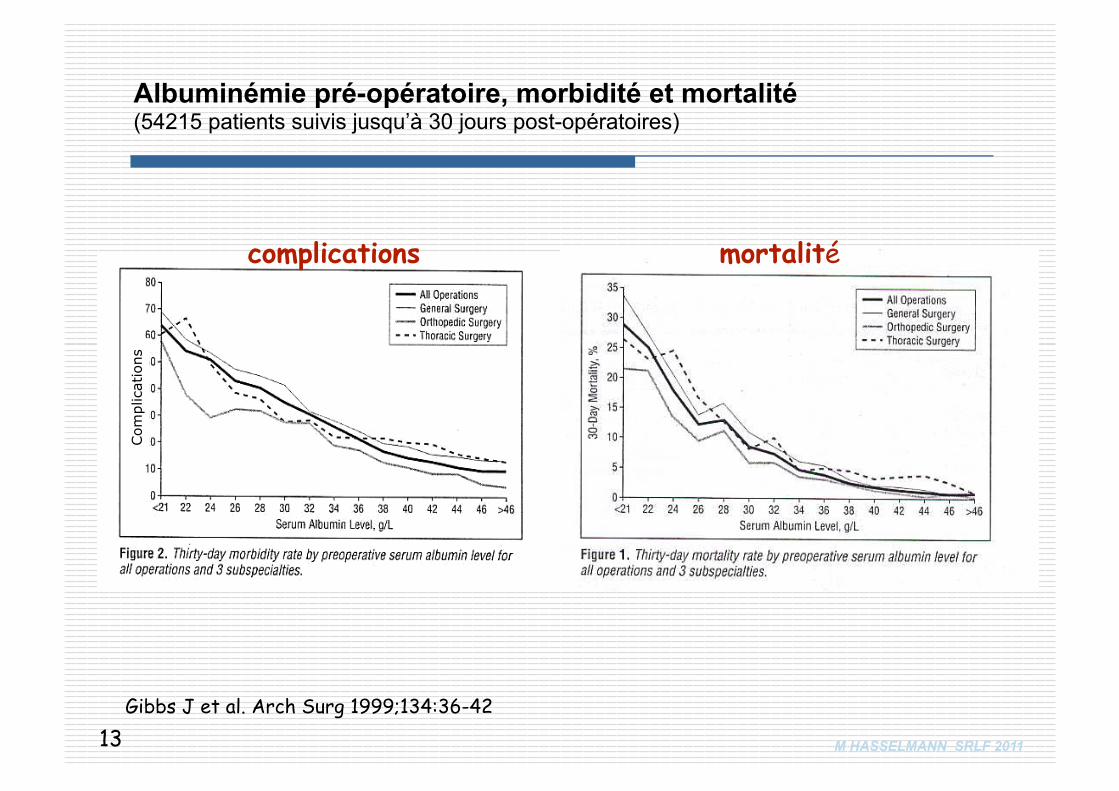
Gibbs J et al. Arch Surg 1999;134:36-42
Albuminémie pré-opératoire, morbidité et mortalité (54215 patients suivis jusqu’à 30 jours post-opératoires)
complications mortalité
13
Com
plic
atio
ns
M HASSELMANN SRLF 2011
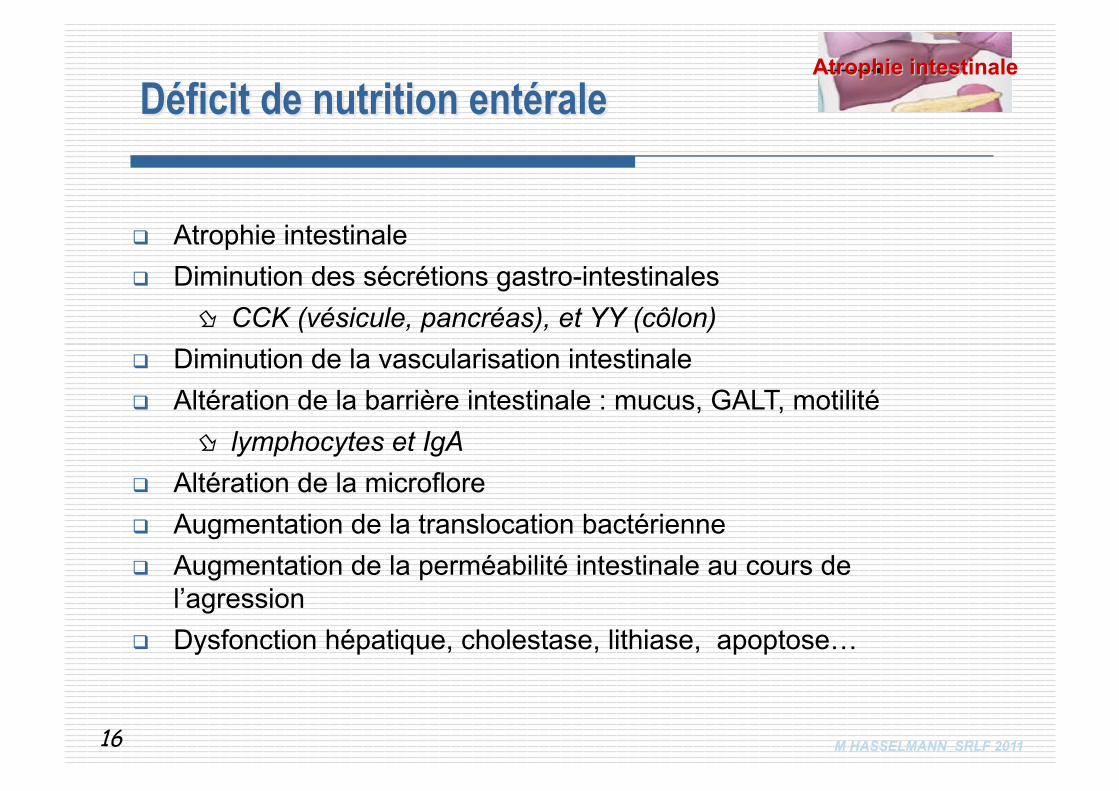
Atrophie intestinale Diminution des sécrétions gastro-intestinales
CCK (vésicule, pancréas), et YY (côlon) Diminution de la vascularisation intestinale Altération de la barrière intestinale : mucus, GALT, motilité
lymphocytes et IgA Altération de la microflore Augmentation de la translocation bactérienne Augmentation de la perméabilité intestinale au cours de
l’agression Dysfonction hépatique, cholestase, lithiase, apoptose…
16
M HASSELMANN SRLF 2011
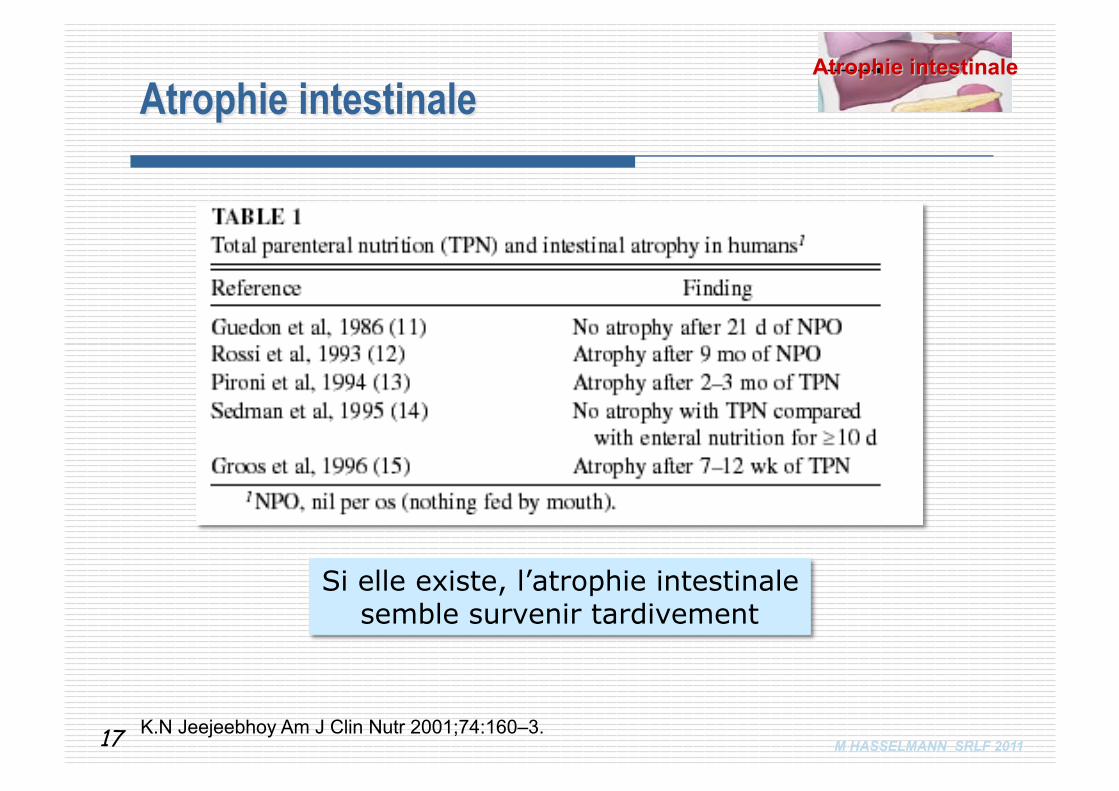
Si elle existe, l’atrophie intestinale semble survenir tardivement
K.N Jeejeebhoy Am J Clin Nutr 2001;74:160–3. 17
M HASSELMANN SRLF 2011
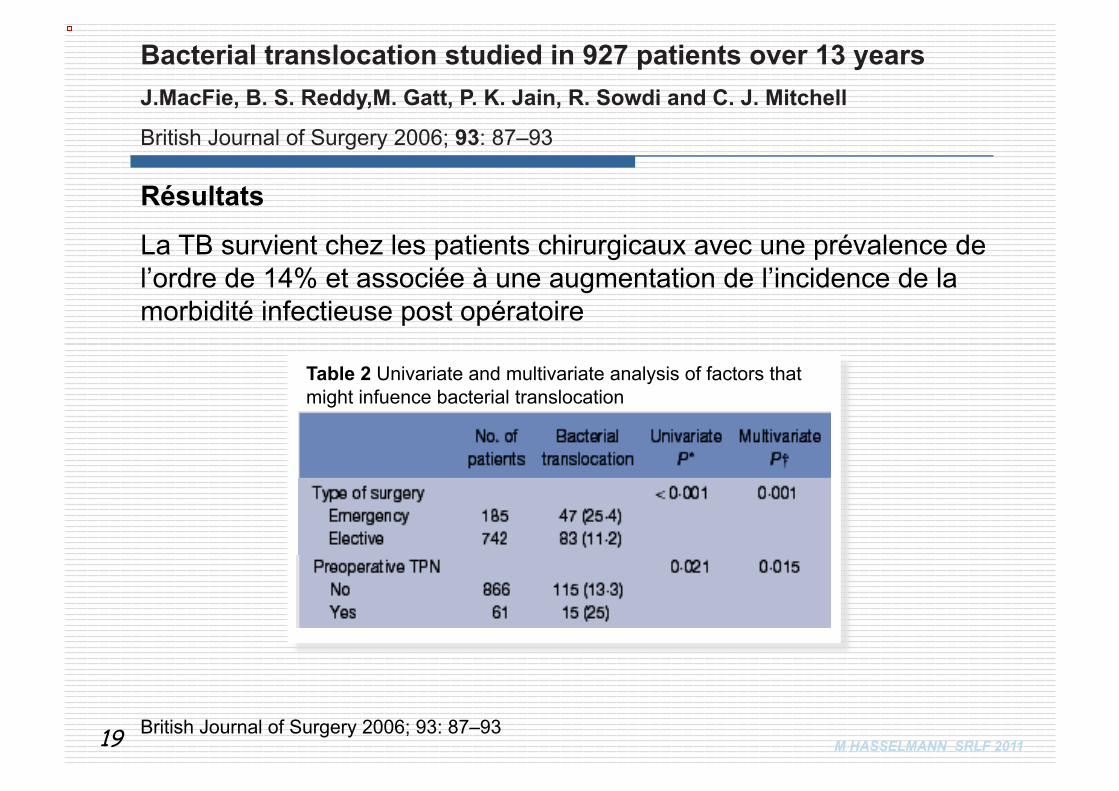
927 patients de chirurgie digestive
Prélèvement per-opératoire et mise en culture de ganglions lymphatiques mésentériques
Analyse uni- et multi-variée par régression logistique des paramètres individuels.
Bacterial translocation studied in 927 patients over 13 years J.MacFie, B. S. Reddy,M. Gatt, P. K. Jain, R. Sowdi and C. J. Mitchell
British Journal of Surgery 2006; 93: 87–93
18
M HASSELMANN SRLF 2011 British Journal of Surgery 2006; 93: 87–93
La TB survient chez les patients chirurgicaux avec une prévalence de l’ordre de 14% et associée à une augmentation de l’incidence de la morbidité infectieuse post opératoire
Table 2 Univariate and multivariate analysis of factors that might infuence bacterial translocation
Résultats
Bacterial translocation studied in 927 patients over 13 years J.MacFie, B. S. Reddy,M. Gatt, P. K. Jain, R. Sowdi and C. J. Mitchell
British Journal of Surgery 2006; 93: 87–93
19

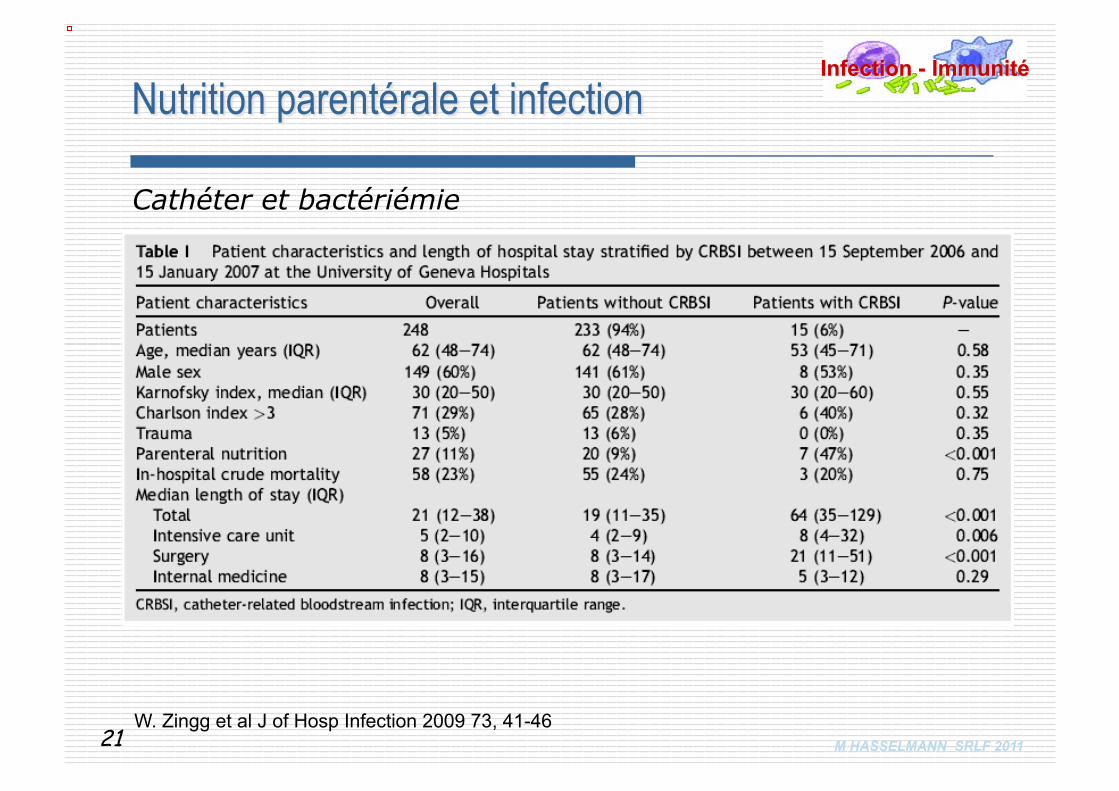
M HASSELMANN SRLF 2011 W. Zingg et al J of Hosp Infection 2009 73, 41-46
Cathéter et bactériémie
21
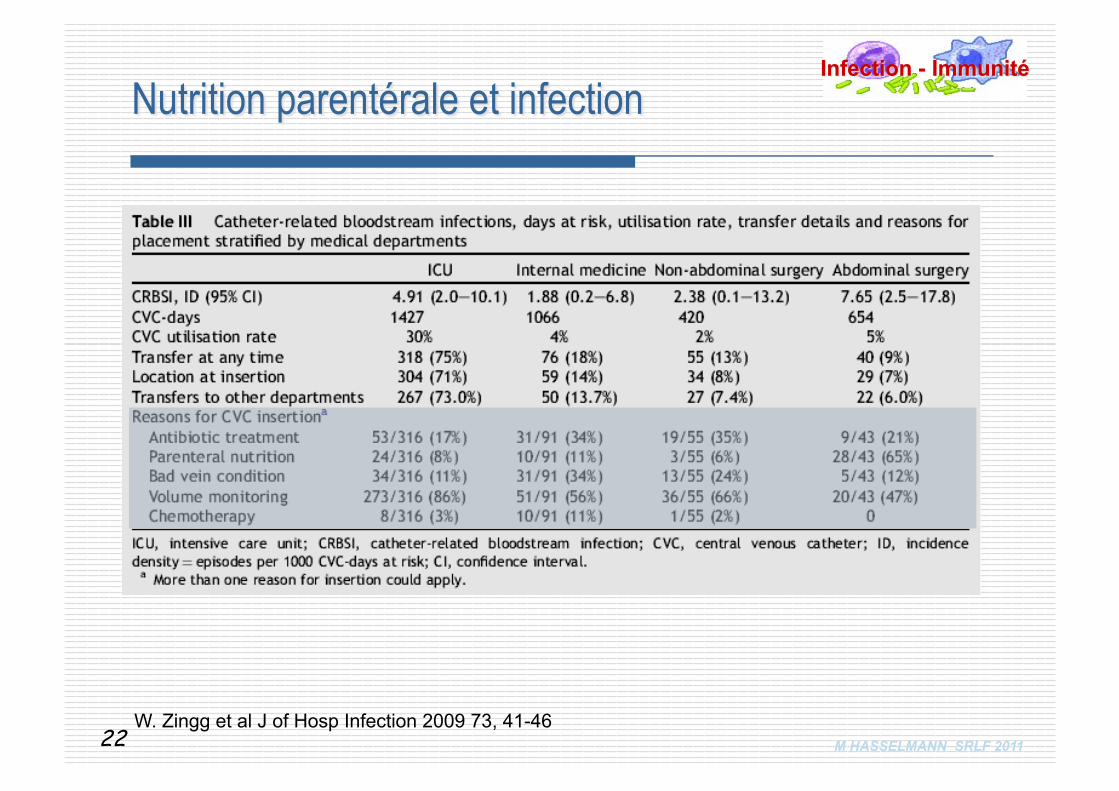
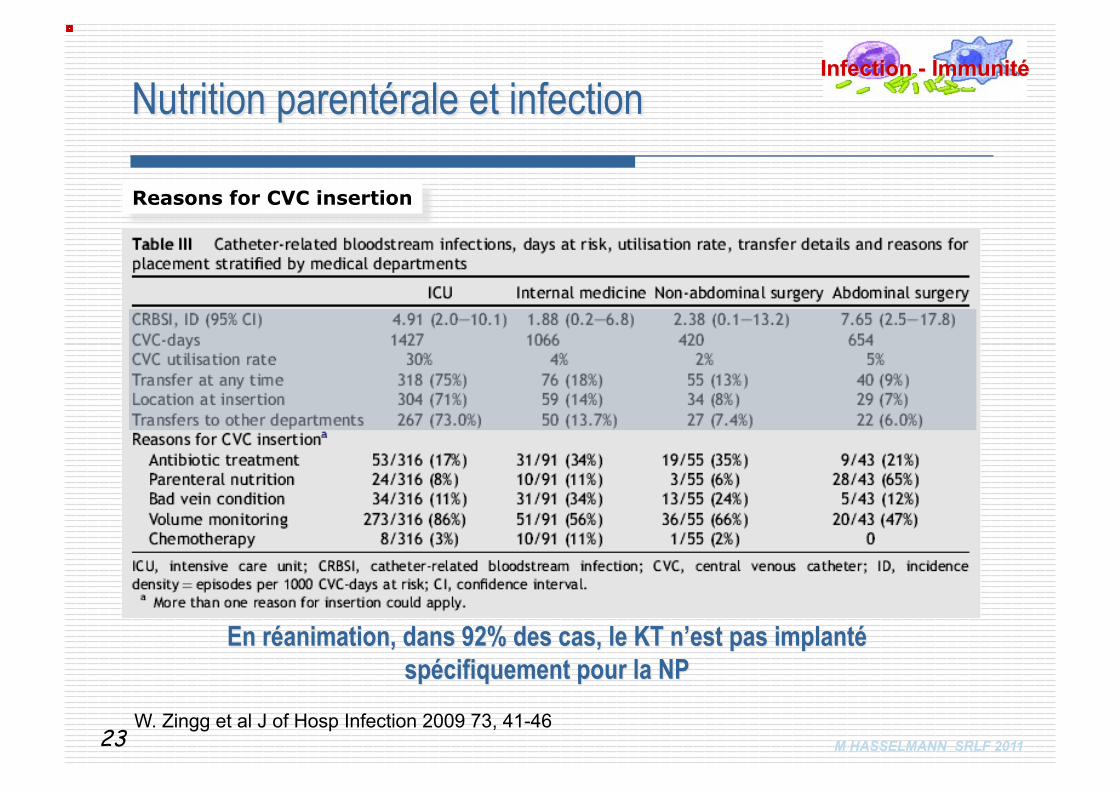
M HASSELMANN SRLF 2011 W. Zingg et al J of Hosp Infection 2009 73, 41-46
22
M HASSELMANN SRLF 2011 W. Zingg et al J of Hosp Infection 2009 73, 41-46
Reasons for CVC insertion
23
M HASSELMANN SRLF 2011
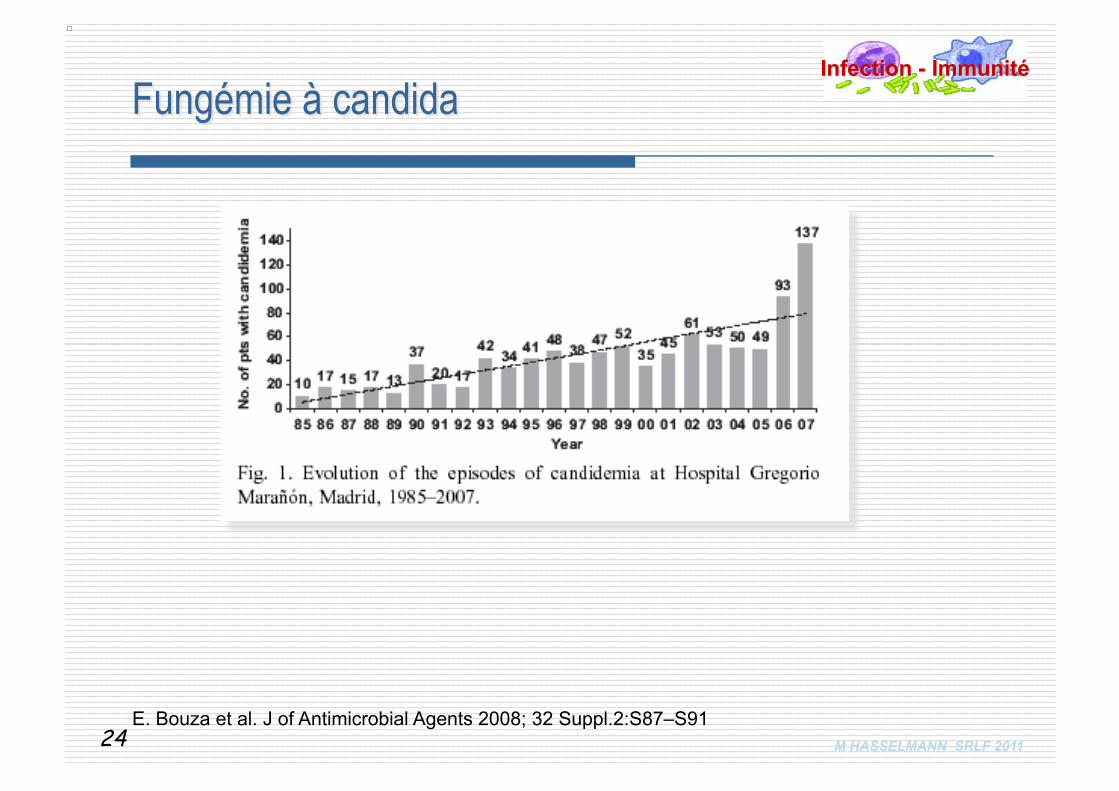
E. Bouza et al. J of Antimicrobial Agents 2008; 32 Suppl.2:S87–S91 24
M HASSELMANN SRLF 2011
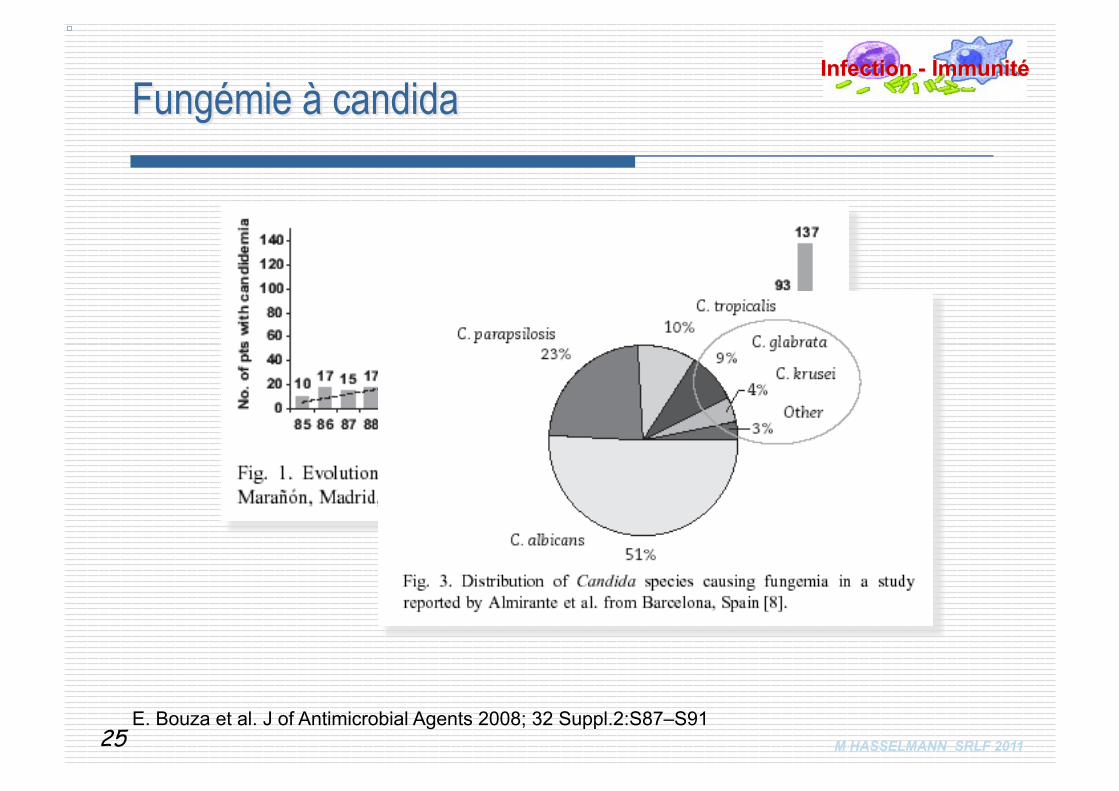
E. Bouza et al. J of Antimicrobial Agents 2008; 32 Suppl.2:S87–S91 25
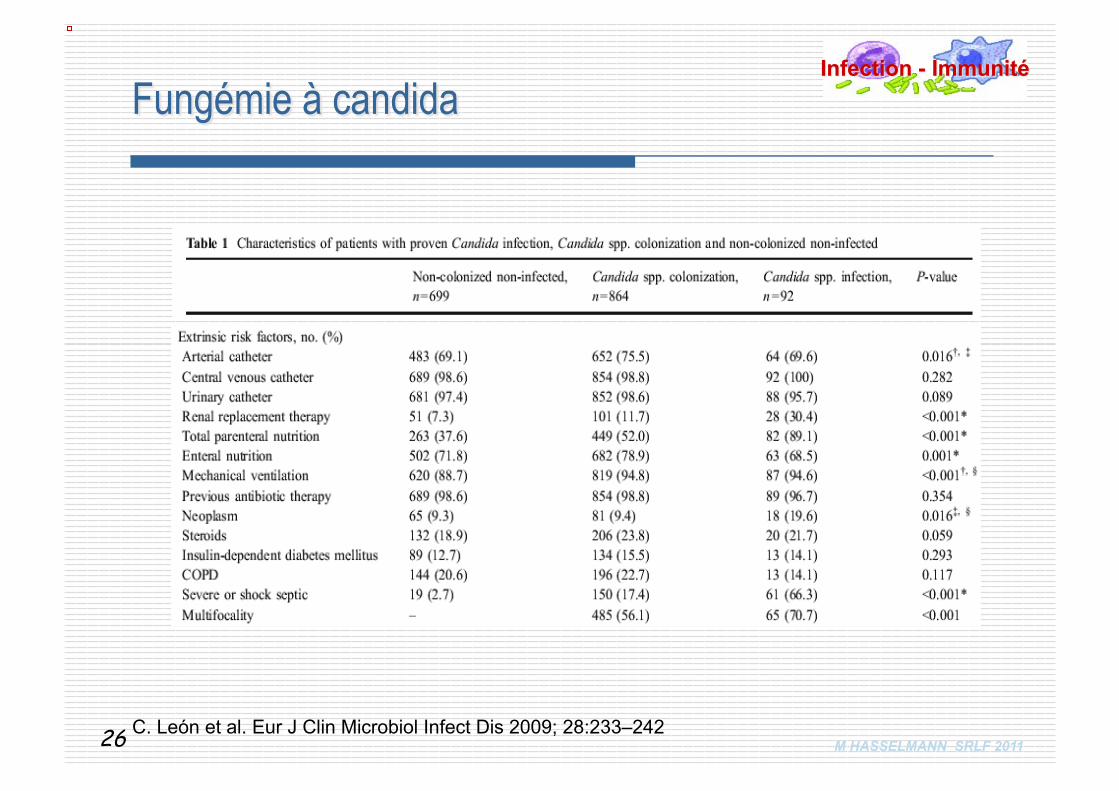
M HASSELMANN SRLF 2011 C. León et al. Eur J Clin Microbiol Infect Dis 2009; 28:233–242 26
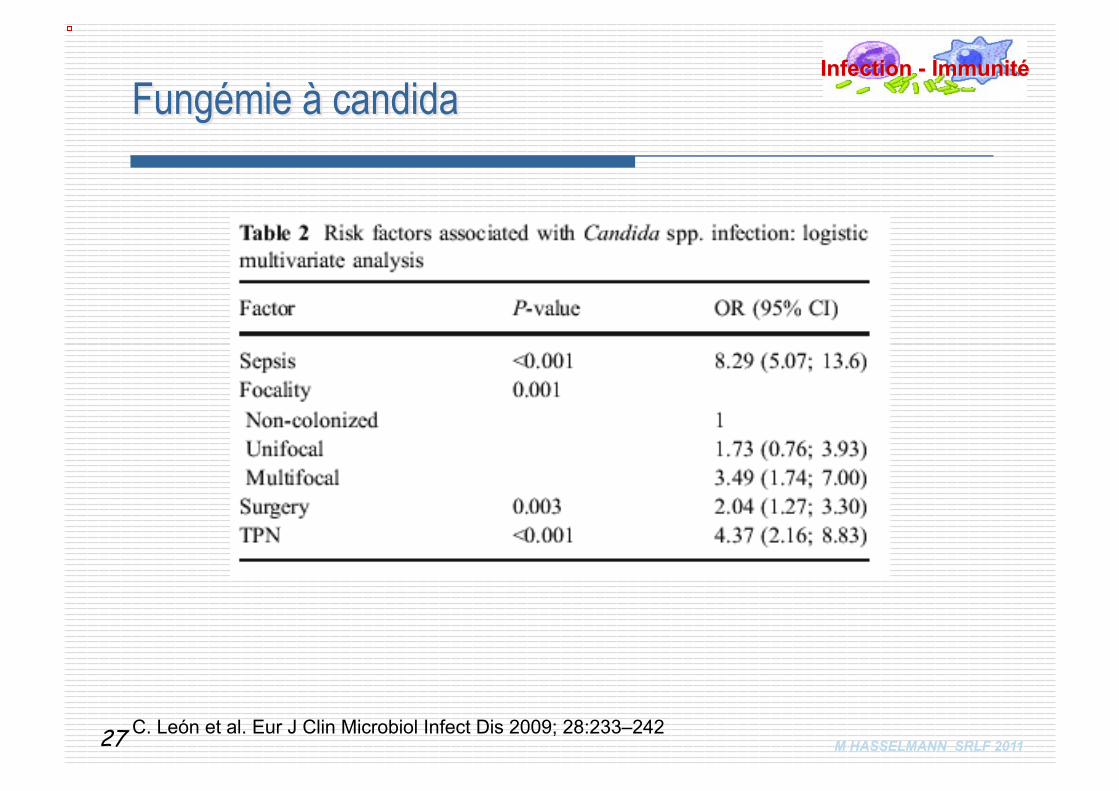
M HASSELMANN SRLF 2011 C. León et al. Eur J Clin Microbiol Infect Dis 2009; 28:233–242 27
M HASSELMANN SRLF 2011 J K. Chow et al., Clinical Infectious Diseases 2008; 46:1206–13
« For critically ill patients in an ICU who are exposed to TPN, it is reasonable to note that the use of TPN is associated with an
increased risk of C. albicans BSI, compared with candidemia due to non-albicans Candida species. »
28
M HASSELMANN SRLF 2011 K.H. Polderman, A.R.J. Girbes. Intensive Care Med 2002;28:18–28
Parenteral feeding is a significant risk factor probably because it can lead to precipitation of feed in stopcocks, valves, and in the line itself…
Parenteral feed is an excellent culture medium for bacteria. In addition, use of the CVC for parenteral feeding may lead to increased use and decreased hygiene during CVC manipulation.
29

2
En chirurgie
31
M HASSELMANN SRLF 2011 32
M HASSELMANN SRLF 2011
Guidelines ESPEN 2009 Nutrition Péri-opératoire
L'immunonutrition est indiquée chez les patients bénéficiant d'une intervention chirurgicale digestive majeure, notamment en cancérologie.
Différer l’intervention si dénutrition La nutrition entérale doit être préférée et administrée avant
l’admission à l’hôpital Les patients cancéreux doivent recevoir une phramaconutrition 5-7 j
avant une chirurgie abdominale majeure
33

En réanimation
M HASSELMANN SRLF 2011
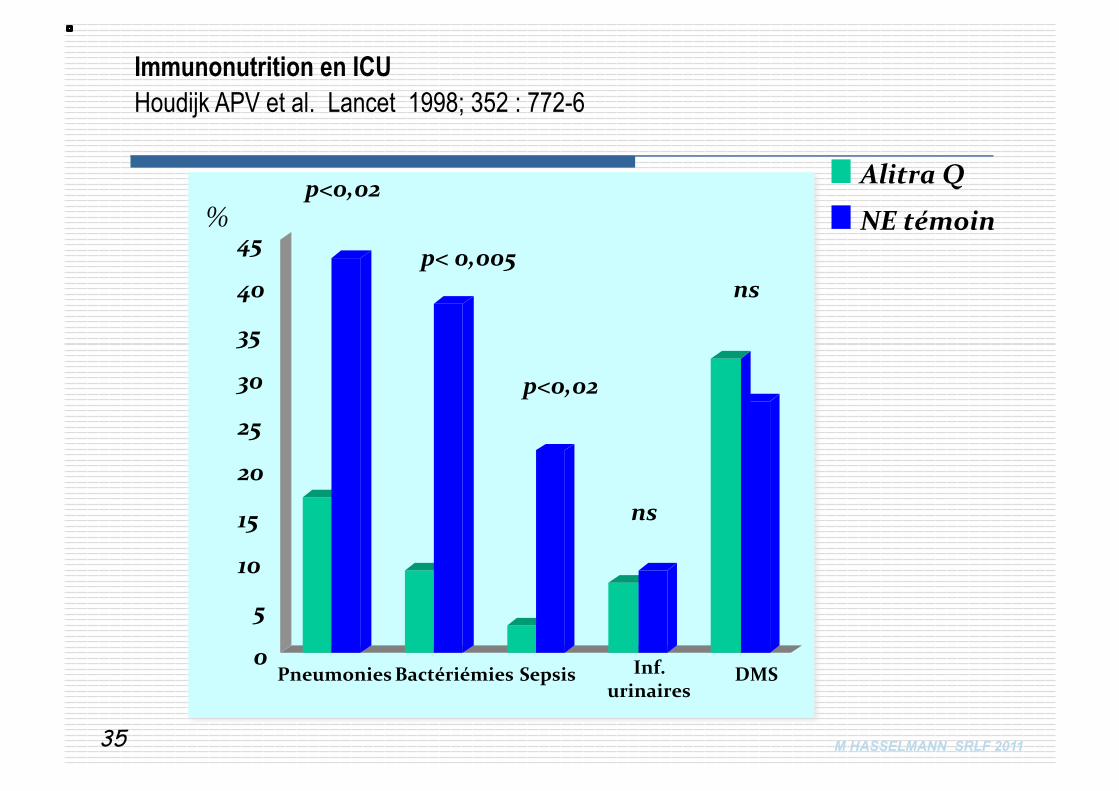
Alitra Q
NE témoin
0
5
10
15
20
25
30
35
40
45 %
Pneumonies Sepsis Bactériémies
p<0,02
p< 0,005
p<0,02
Inf. urinaires
ns
DMS
ns
Immunonutrition en ICU Houdijk APV et al. Lancet 1998; 352 : 772-6
35
M HASSELMANN SRLF 2011
12 études prospectives randomisées (10 de Heys) 1482 patients (analyse en IT) , sponsoring labo. Résultats : Diminution des infections: RR = 0.6 [ 0.42-0.86] Diminution du séjour hospitalier: RR = 2.9 [ 1.4-4.4] Diminution durée de VM ; RR = 2.6 [ 0.5-5] Pas d’effet sur la mortalité : RR = 1.05 [0.78-1.41]
Immunonutrition in the critically ill: a systematic review of clinical outcome. Beale et al Crit. Care Med. 1999; 27 : 2799-2805
36
M HASSELMANN SRLF 2011
An immune-enhancing enteral diet reduces mortality rate and episodes of bacteremia in septic intensive care unit patients. Galban C et al. Crit Care Med 2000; 28: 643-8
• Etude multicentrique prospective, randomisée en réanimation polyvalente • 181 malades :
- APACHE II > 10 ; états septiques (pneumonies n=121) • Randomisation dans les 36 h après le diagnostic de sepsis
- immunonutrition entérale (Impact®) - ou NE témoin non isocalorique non isoazotée (Precitene HPt®)
• Résultats : gp traité n = 89 ; gp témoin n = 87 - Réduction de mortalité :
o 17(19%) vs 28 (32%) p< 0.05 ; plus prononcé pour APACHE II entre 10 et 15 - Moins de bactériémies et d’infections nosocomiales
o 7 (7,8%) vs 19 (21,8%) p = 0.01 o 5 (5,6%) vs 17 (19,5%) p = 0.01
37
M HASSELMANN SRLF 2011
Etude multicentrique simple aveugle - 15 ICU Espagnoles, 220 patients patients répartis en :
Nutrison® ( 62,5 g protéines/l pas de MCT, pas de fibre ) vs
Streson® ( 75 g protéines/l + arginine, MCT et fibres) Résultats
• Réduction des ILC (0.4 episodes/1000 jours ICU vs 5.5 episodes/1000 jours ICU ; RR : 0.07 (95% IC : 0.01 à 0.54, p < .001)
• Pas de différence pour les autres infections • Pas de différence de mortalité en ICU et à 6 mois, • Tendance pour les patients traités plus de 2 jours
Early enteral nutrition in critically ill patients with a high-protein diet enriched with arginine, fiber, and antioxidants compared with a standard high-protein diet. The effect on nosocomial infections and outcome Caparrós T et al. JPEN 2001 ; 25 : 299-308
38
M HASSELMANN SRLF 2011
Should immunonutrition become routine in critically ill patients? A systematic review of the evidence Heyland et coll. JAMA 2001 ; 286 : 944-953
• 22 études prospectives randomisées • 2419 patients de chirurgie et de réanimation.
Résultat • Réduction des infections (plaies, abcès intra abdominal pneumonies)
RR = 0.66 [ 0.33 – 1.31] p< 0.0001 • Pas d’effet sur la mortalité ; RR = 1.1 [ 0.93- 1.10] • REMARQUES : en réanimation, la réduction du nombre d’infection est
plus grande (RR = 0.4] . • Cependant la mortalité est augmentée particulièrement chez le patient
septique (RR = 2,5]
39
M HASSELMANN SRLF 2011
Immunonutrition in the intensive care unit. A systematic review and consensus statement. Montejo JC et colll. Clin. Nutr. 2003 ; 22: 221-233
• Méthodologie de conférence de consensus • 26 études prospectives randomisées de bonnes qualités • 2816 patients de chirurgie et de réanimation Résultats • Diminution des infections : RR = 0.41 [0.31 1] p = 0.0001
• plaies opératoires : RR = 0.46 [ 0.3-0.69] p = 0.003 • abcès intra abdominal; RR = 0.26 [ 0.12-0.58] p = 0.0005 • pneumopathies : RR = 0.54 [0.35-0.84] p = 0.0007 • infection urinaire : RR = 0.66 [0.43-1] p= 0.002 • bactériémie : RR = 0.45 [ 0.29-0.69] p = 0.002 • choc septique : RR = 1.1 [ 0.9 – 2.4] p = 0.12
40
M HASSELMANN SRLF 2011
Immunonutrition et Sepsis Dent et coll. Crit. Care Med. 2003 ; 30 : A17
• 170 patients de réanimation / Impact ® versus contrôle • Mortalité : 26% GR Impact ® / 9.6% GR contrôle • APACHE II est comparable (25) • Les patients du groupe Impact ® ont fait plus de pneumopathie.
41
Premiers doutes…
M HASSELMANN SRLF 2011
• Etude prospective randomisée multicentrique • 237 patients de réanimation • Comparaison : NPT vs immunonutrition entérale • 36 patients ont un sepsis grave. • 19 patients (NPT) et 17 patients (Immunonutrtition) • Mortalité: 14.3 % (NPT) / 44.4 % (immunonutrition) : p < 0.0001
Early enteral immunonutrition in patients with severe sepsis: results of an interim analysis of a randomized multicentre clinical trial Bertolini et coll. Int. Care Med. 2003;29:834-840
Développement d’une controverse sur l’utilisation des diètes immunomodulatrices chez les patients septiques
42
La suite…
M HASSELMANN SRLF 2011
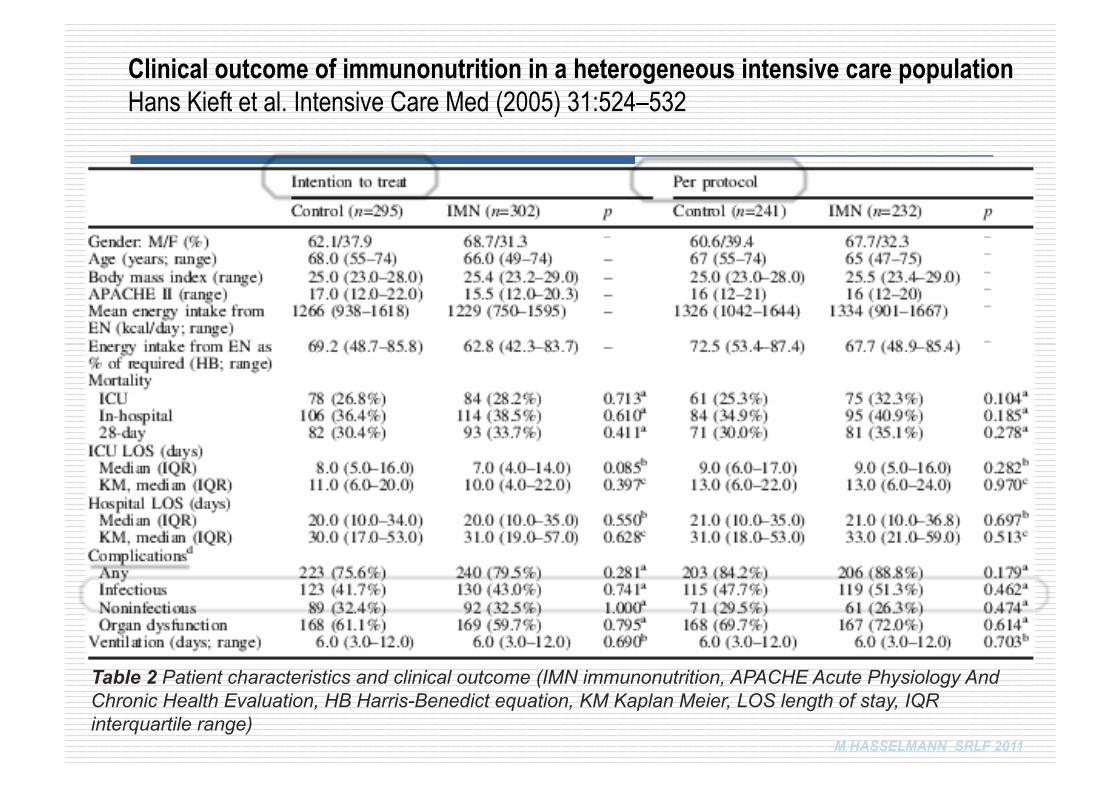
Clinical outcome of immunonutrition in a heterogeneous intensive care population Hans Kieft et al. Intensive Care Med (2005) 31:524–532
Table 2 Patient characteristics and clinical outcome (IMN immunonutrition, APACHE Acute Physiology And Chronic Health Evaluation, HB Harris-Benedict equation, KM Kaplan Meier, LOS length of stay, IQR interquartile range)
M HASSELMANN SRLF 2011
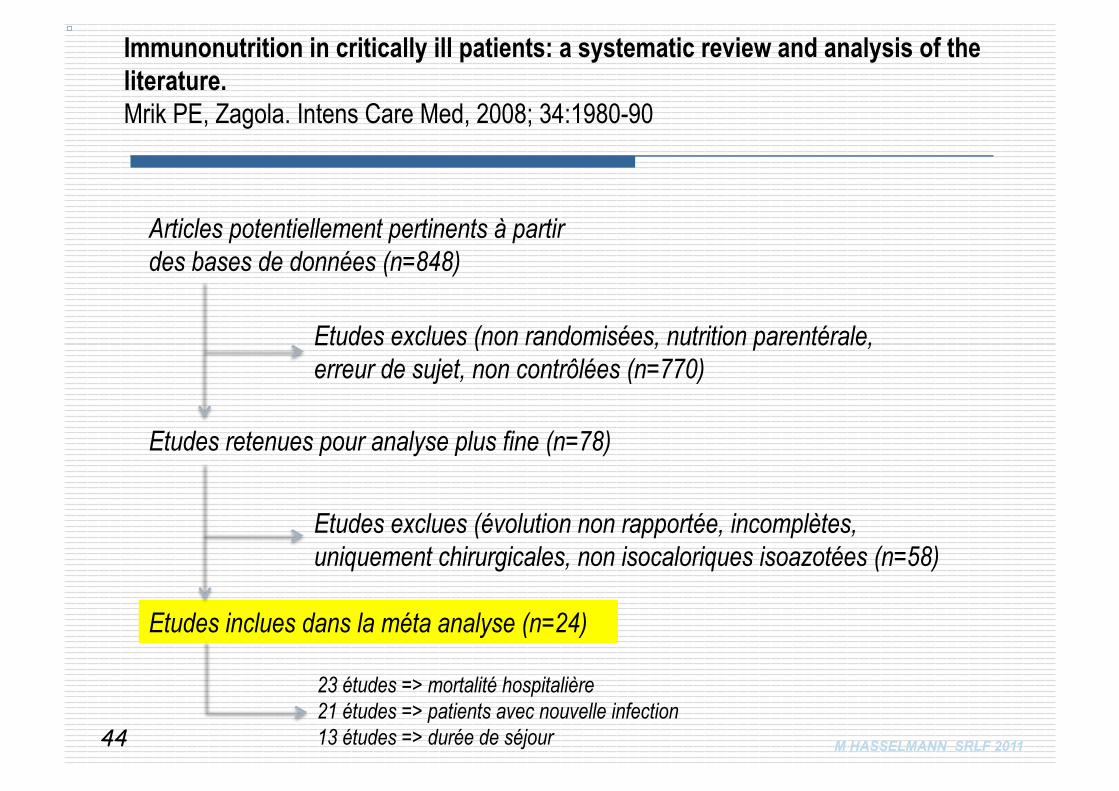
Articles potentiellement pertinents à partir des bases de données (n=848)
Etudes retenues pour analyse plus fine (n=78)
Etudes exclues (non randomisées, nutrition parentérale, erreur de sujet, non contrôlées (n=770)
Etudes exclues (évolution non rapportée, incomplètes, uniquement chirurgicales, non isocaloriques isoazotées (n=58)
Etudes inclues dans la méta analyse (n=24)
23 études => mortalité hospitalière 21 études => patients avec nouvelle infection 13 études => durée de séjour 44
Immunonutrition in critically ill patients: a systematic review and analysis of the literature. Mrik PE, Zagola. Intens Care Med, 2008; 34:1980-90
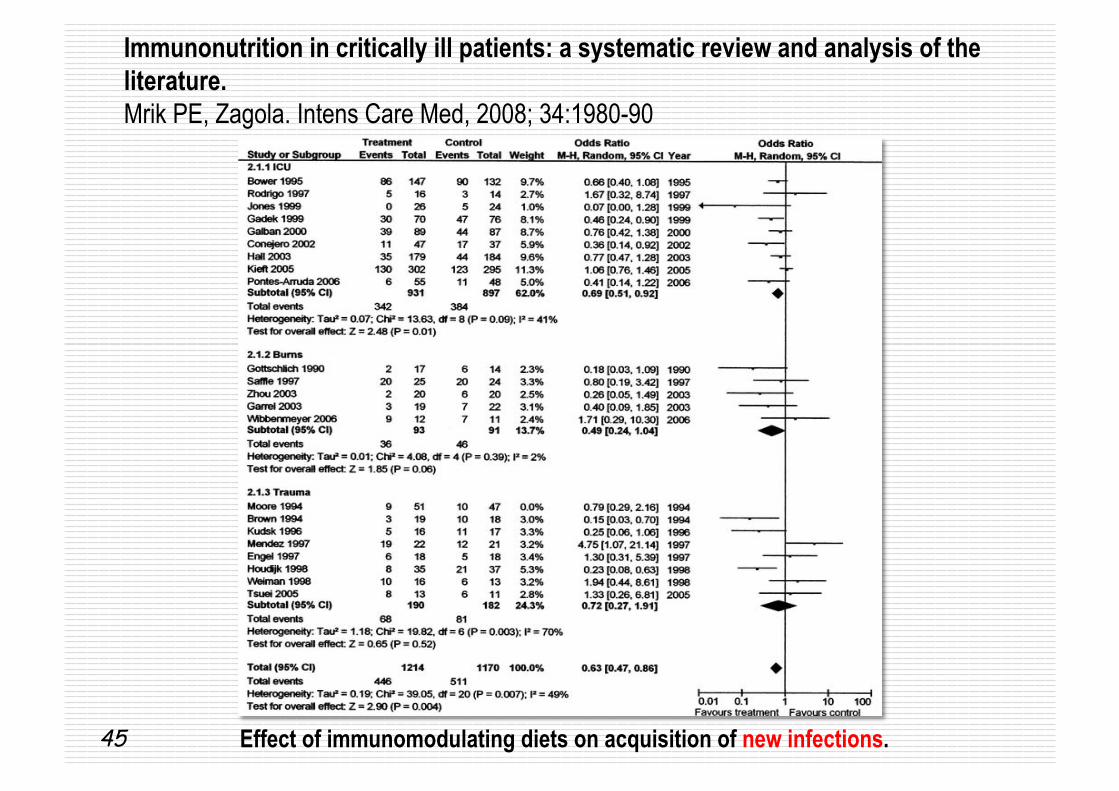
Immunonutrition in critically ill patients: a systematic review and analysis of the literature. Mrik PE, Zagola. Intens Care Med, 2008; 34:1980-90
Effect of immunomodulating diets on acquisition of new infections. 45
M HASSELMANN SRLF 2011
• Current evidence suggests that a fish oil IMD without added arginine reduces mortality, secondary infections and LOS in patients with sepsis, SIRS and ARDS
• Glutamine supplementation may be beneficial in burn patients. • Arginine containing IMDs appear to have a limited role in trauma
patients. • The role of a high omega-3 IMD in trauma patients has yet to be
determined.
46
Immunonutrition in critically ill patients: a systematic review and analysis of the literature. Mrik PE, Zagola. Intens Care Med, 2008; 34:1980-90
Glutamine
M HASSELMANN SRLF 2011
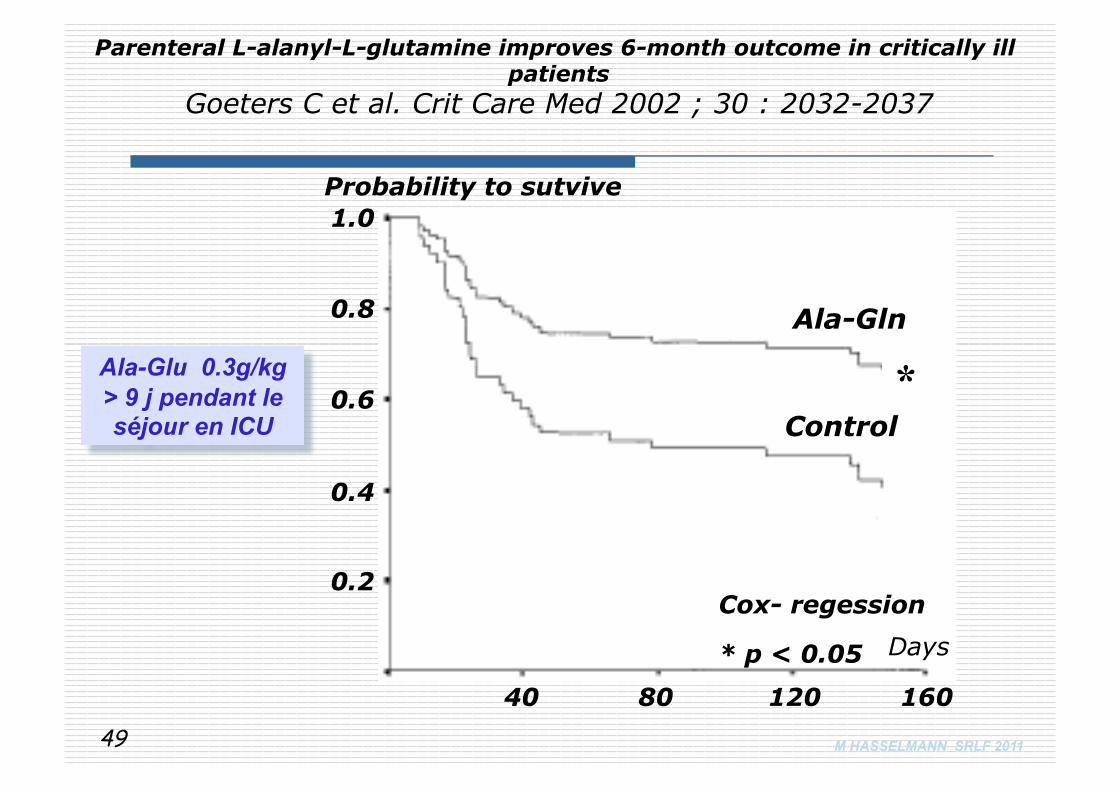
Parenteral L-alanyl-L-glutamine improves 6-month outcome in critically ill patients
Goeters C et al. Crit Care Med 2002 ; 30 : 2032-2037
0.2
0.4
0.6
0.8
1.0
40 80 120 160
Probability to sutvive
Ala-Gln
Control *
Cox- regession
* p < 0.05 Days
Ala-Glu 0.3g/kg > 9 j pendant le séjour en ICU
49
M HASSELMANN SRLF 2011
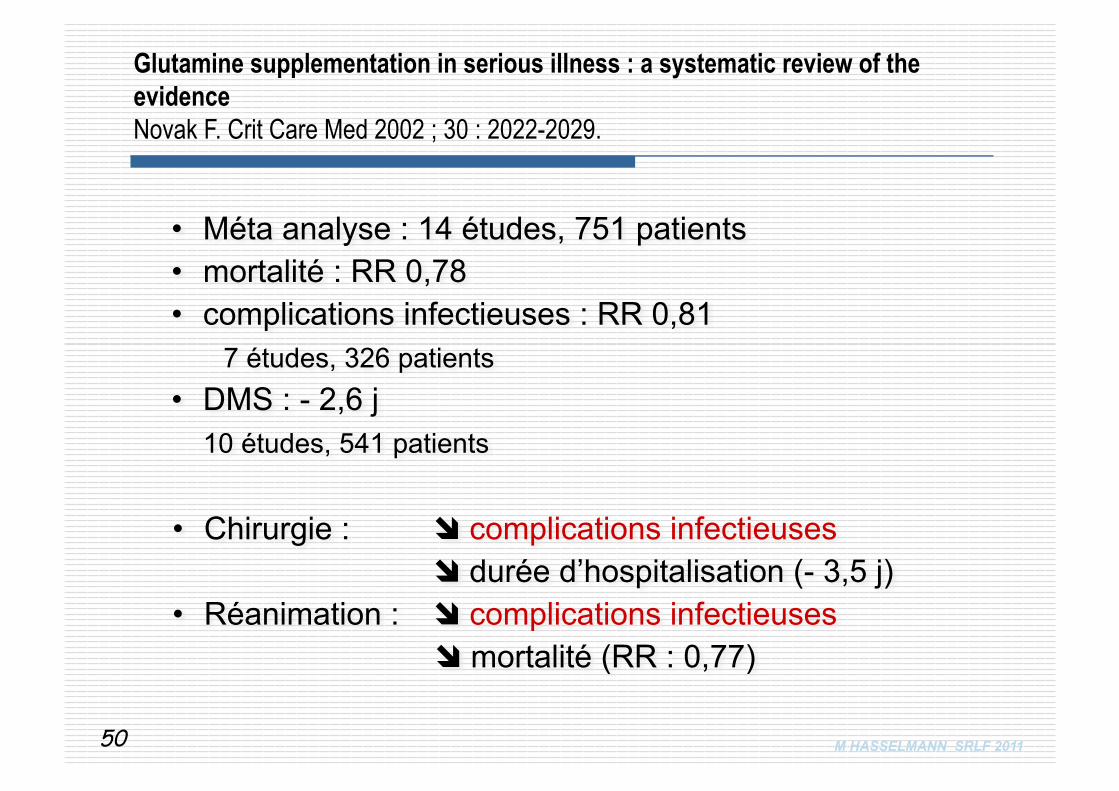
• Méta analyse : 14 études, 751 patients
• mortalité : RR 0,78 • complications infectieuses : RR 0,81
7 études, 326 patients • DMS : - 2,6 j 10 études, 541 patients
Glutamine supplementation in serious illness : a systematic review of the evidence Novak F. Crit Care Med 2002 ; 30 : 2022-2029.
• Chirurgie : complications infectieuses durée d’hospitalisation (- 3,5 j) • Réanimation : complications infectieuses
mortalité (RR : 0,77)
50
M HASSELMANN SRLF 2011
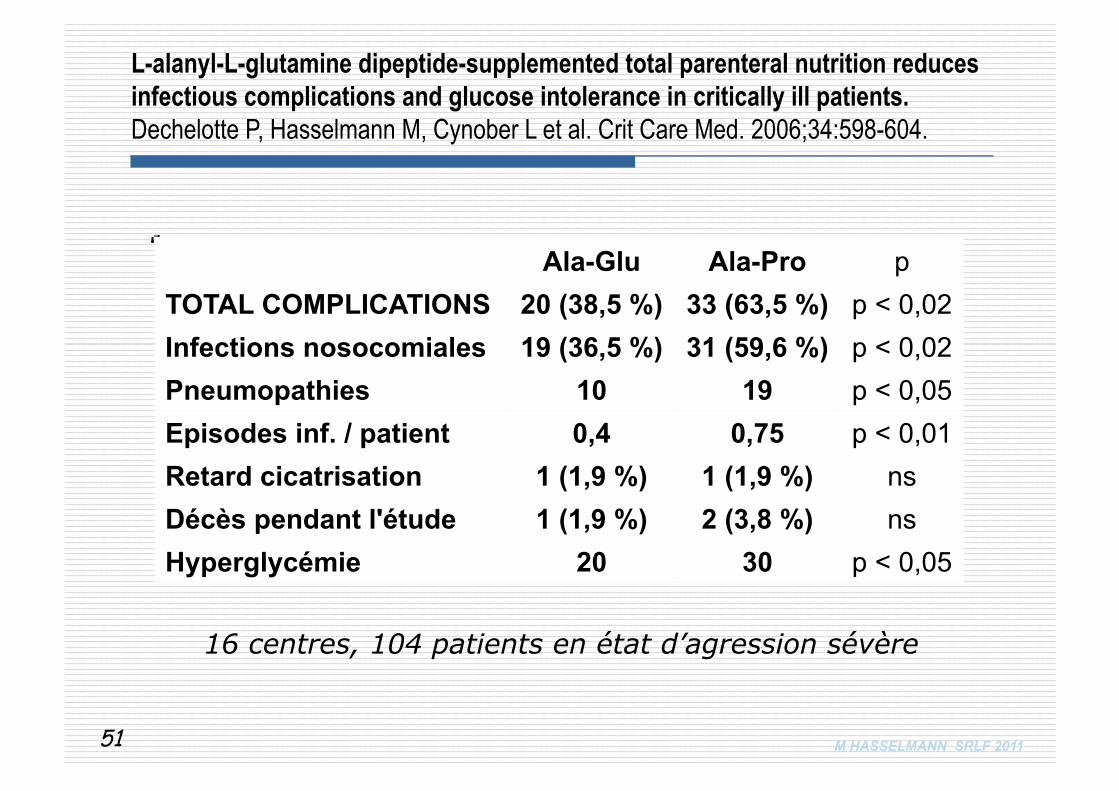
Ala-Glu Ala-Pro p TOTAL COMPLICATIONS 20 (38,5 %) 33 (63,5 %) p < 0,02 Infections nosocomiales 19 (36,5 %) 31 (59,6 %) p < 0,02 Pneumopathies 10 19 p < 0,05 Episodes inf. / patient 0,4 0,75 p < 0,01 Retard cicatrisation 1 (1,9 %) 1 (1,9 %) ns Décès pendant l'étude 1 (1,9 %) 2 (3,8 %) ns Hyperglycémie 20 30 p < 0,05
L-alanyl-L-glutamine dipeptide-supplemented total parenteral nutrition reduces infectious complications and glucose intolerance in critically ill patients. Dechelotte P, Hasselmann M, Cynober L et al. Crit Care Med. 2006;34:598-604.
16 centres, 104 patients en état d’agression sévère
51
Huiles de poissons
M HASSELMANN SRLF 2011
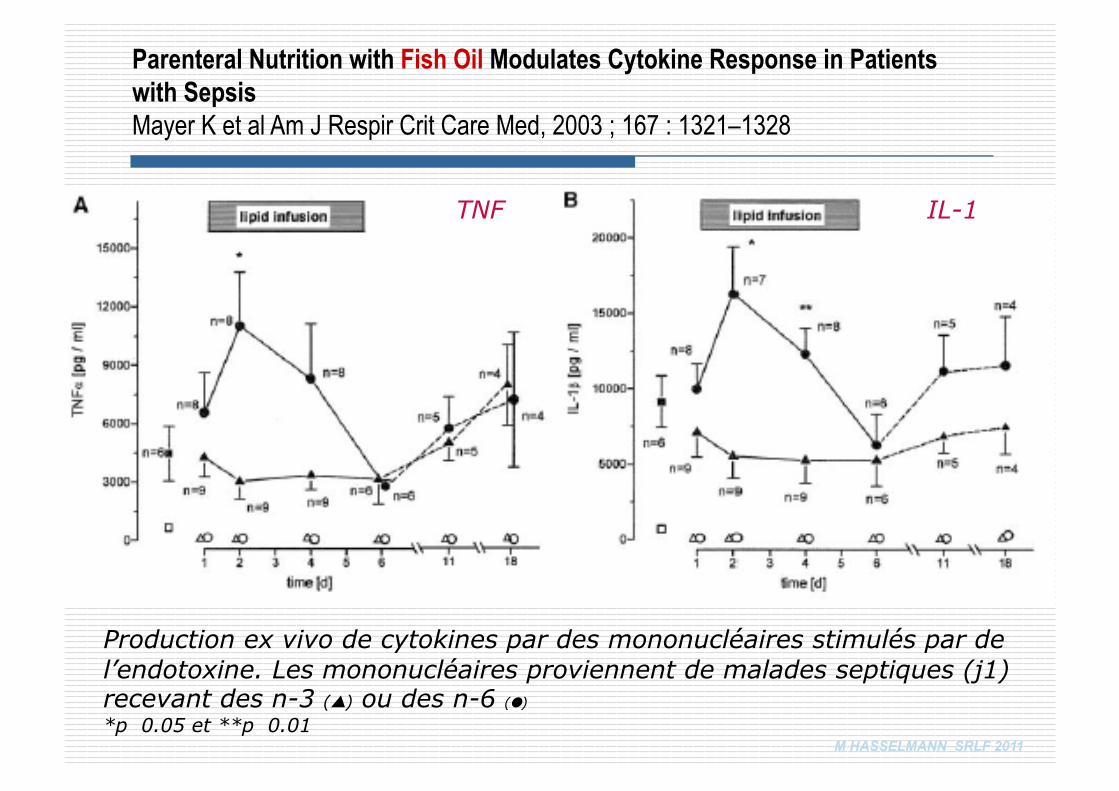
TNF IL-1
Production ex vivo de cytokines par des mononucléaires stimulés par de l’endotoxine. Les mononucléaires proviennent de malades septiques (j1) recevant des n-3 () ou des n-6 () *p 0.05 et **p 0.01
Parenteral Nutrition with Fish Oil Modulates Cytokine Response in Patients with Sepsis Mayer K et al Am J Respir Crit Care Med, 2003 ; 167 : 1321–1328
M HASSELMANN SRLF 2011
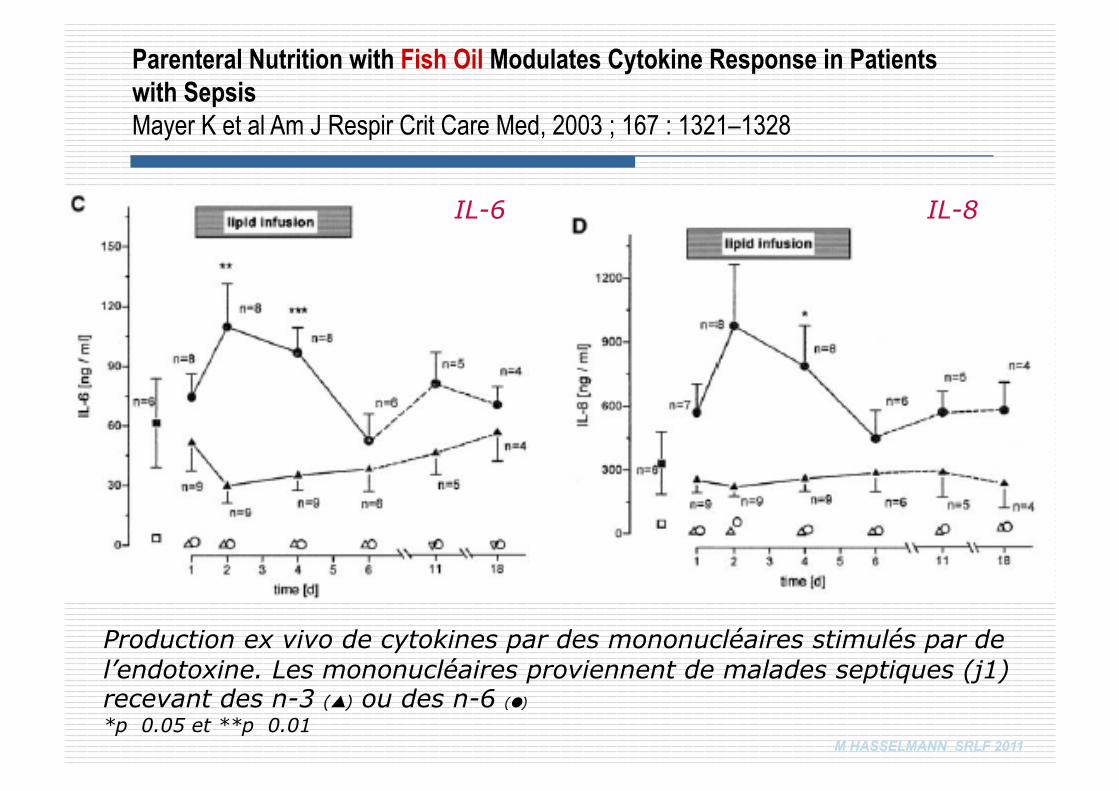
Production ex vivo de cytokines par des mononucléaires stimulés par de l’endotoxine. Les mononucléaires proviennent de malades septiques (j1) recevant des n-3 () ou des n-6 () *p 0.05 et **p 0.01
IL-6 IL-8
Parenteral Nutrition with Fish Oil Modulates Cytokine Response in Patients with Sepsis Mayer K et al Am J Respir Crit Care Med, 2003 ; 167 : 1321–1328
M HASSELMANN SRLF 2011
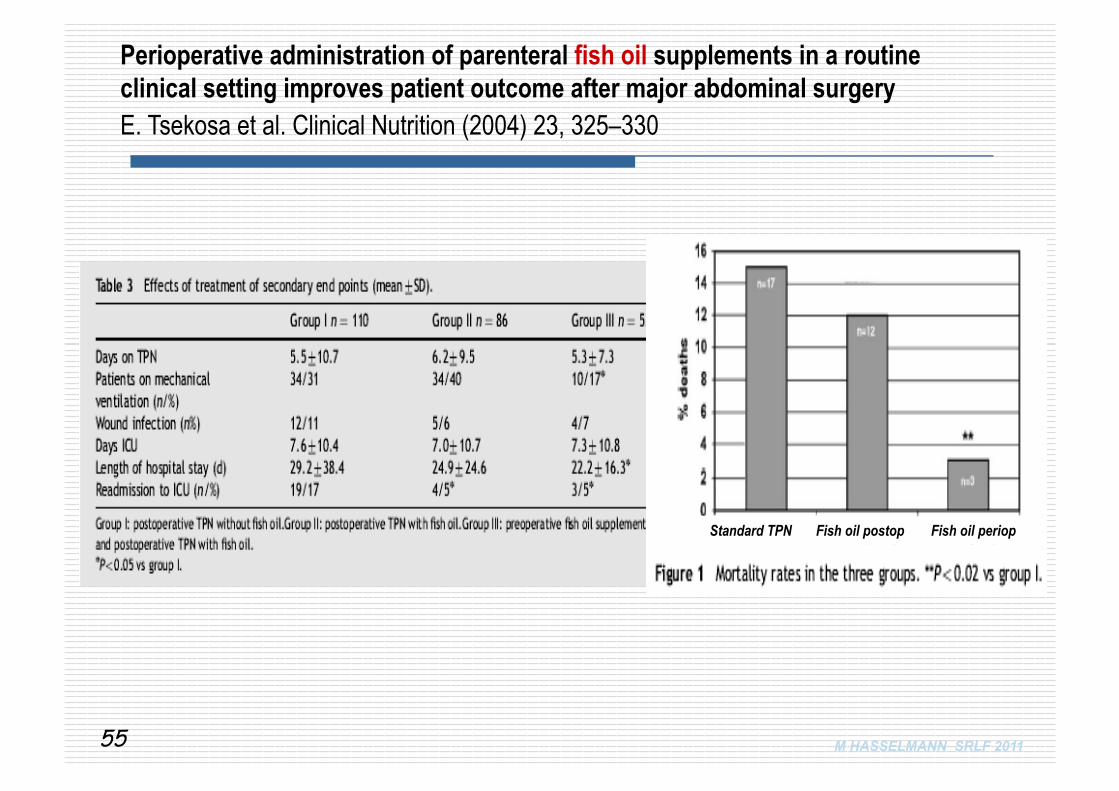
Perioperative administration of parenteral fish oil supplements in a routine clinical setting improves patient outcome after major abdominal surgery E. Tsekosa et al. Clinical Nutrition (2004) 23, 325–330
55
Fish oil periop Fish oil postop Standard TPN