L’anthropologie de la maladie d’Alzheimer: le cas des ... Leibing.pdf · L’anthropologie de...
29
L’anthropologie de la maladie d’Alzheimer: le cas des médicaments Annette Leibing Professor, medical anthropology Faculty of Nursing Université de Montréal www.meos.qc.ca
Transcript of L’anthropologie de la maladie d’Alzheimer: le cas des ... Leibing.pdf · L’anthropologie de...
L’anthropologie de la maladie d’Alzheimer: le cas
des médicaments
Annette Leibing
Professor, medical anthropology
Faculty of NursingUniversité de Montréal
www.meos.qc.ca
Auguste Deters et Alois Alzheimer
Problème de départ
• Le statut controversé des médicaments pour l’Alzheimer
- observé dans l’équipe (par les non-MDs principalement);- dans la littérature
Deux groupes de médicaments pour l’Alzheimer
• 1. Renforceurs de mémoire- Reminyl / galantamine- Aricept / donezipil - Tacrine- Exelon / rivastigmine- Ebixa(Namenda) / memantine
• 2. Psychiatriques- antidepressants, (atypical) antipsychotics etc.
Renforceurs de m. (« ça marche »)
• “The conclusion is clear: stabilizing or slowing the progression of symptoms of AD using these drugs is a clinically meaningful therapeutic goal”(Gauthier 2006)
• “There is substantial evidence that available treatments for AD are effective in improving or reducing deterioration in behavior, ADLs [activities of daily living], and cognition.”(Geldmacher et al. 2006)
Renforceurs.. (« ça ne marche pas »)
• “… trial reports tend to exaggerate beneficial effects and underestimate adverse effects. This is due to incomplete follow-up and the bias introduced by more early withdrawals from the active-treatment groups in a progressively deteriorating disease” (Therapeutics Initiative 2005)
Médicaments psychiatriques (« ça marche »)
• « Atypical or novel antipsychotic drugs represent the reference drugs for treating BPSD. Among these, risperidone is considered as a drug of choice. Also, selective serotonin reuptake inhibitors (SSRIs) are useful in the treatment of BPSD. »(Parnetti et al. 2001)
Médicaments psychiatriques(« ça ne marche pas »)
• “pharmacological therapies are not particularly effective for the management of neuropsychiatric symptoms of dementia” (Sink et al. 2005: 596)
• “… the overall evidence base for the use of psychotropic medication remains poor”(Treloar et al. 2001: 445)
???• Comment les médecins peuvent prescrire des
médicaments sans être certains?
– Les médicaments: le traitement centrale d’une démence, parce qu’ils agissent sur le cerveau. (prévention: exercice du cerveau)
- paradigme cognitive (German Berrios):“…the view that dementia is an irreversible disorder (mainly in the elderly) of intellectual functions (particularly memory).”
- en train de changer
Entrevues exploratoires (avec des psychogériatriciens à RJ, qui sont « bien informés »)
• 3 questions principales:1. S’il y avait un changement dans la
conception de la maladie d’Alzheimer;2. a Comment ils/elles traitent ces patients et b. la différence entre traitement publique et privé; 3. Leurs formations en psychogériatrie et sources d’actualisation
• 2005 and 2006; n=25
• “As to the general population, Alzheimer’s disease is more being discussed in the public, because the number of older people keeps growing … The media has contributed to this a lot,... Health professionals, especially the doctors, also changed their mentality. It was an incredible step, the acquisition of a conscience that, although there is no cure for a dementia, that with the right care the older person can still have a good quality of life. … I know that there is still a long way to go, but we have now access to all updates about inter- and multidisciplinary care, so that patients are handled with more efficacy. Medical technologies have advanced immensely. The choice in pharmaceuticals for treatment and symptom control is augmenting all the time. And I have to emphasize also the non-pharmacological interventions, which are extremely important…The goal is to maintain a certain functional capacity and to slow down the progression of the disease.”
(gériatre fém., no.2)
• “You give the medications to everybody until you find one that works for that person. You can the observe a stabilization of the patient for one, two or three years and afterwards a slower decline when compared to patients without medications or to those with medications, but which do not work.”(psychiatre masc., producteur des connaissances; no. 19)
• “My most important criterion is socio-economic. These medications are quite expensive and not accessible for the poorer people. Afterwards I evaluate the side effects. And finally, if the person with the disease has someone to help her or him to take the medication correctly, so it won’t be forgotten. Every patient is different. The only difference is that poorer people have the choice (sic) of only one medication, but the clinical treatment is the same for everybody.”(gériatre fém., no. 18)
• “The family tells me about the efficacy. They observe that the person is getting more independent, more active, more connected with things out there, more active in the family life. One lady, for example, who started the medication [renforceur de m.], she went back to reading the newspaper, reading magazines, something she had stopped doing. Another one told me that she went back to watching the soap opera she liked…”(psychiatre fém., aussi psychanaliste, no. 20)
Résumé des entrevues• 1. pas de doutes concernant l’efficacité des
médicaments, même s’il faut changer parfois le médicament (au Brésil pour les plus riches, les pauvres reçoivent Exelon)
• 2. Des soins sont multidisciplinaires• 3. La cognition n’est plus le symptôme central du
syndrome. (fonctionnalité, qualité de vie)
• Comment on peut expliquer la certitude des médecins?
Premier argument:le déclin du paradigme cognitif
• 1. Les médecins acceptent les médicaments pour AD, parce qu’une nouvelle efficacité a été montré.
• Avant: la cognition était central pour définir la démence.
• Maintenant: un diagnostique plus inclusif et une nouvelle efficacité
La création du BPSD (Behavioral and psychological symptoms of dementia)
• Risperidone –Janssen Pharmaceuticals a organisé (avec IPA) la première conférence de consensus où la catégorie “BPSD” a été créée (à Landsdowne, VA en 1996); financement illimité par Janssen.
• "Symptoms of disturbed perception, thought content, mood, behavior frequently occurring in patients with dementia".Anxiety, Aggression, Depressed mood, Screaming, Hallucinations, Restlessness, Delusions, Agitation, Wandering, Culturally-inappropriate behaviors, Sexual disinhibition, Hoarding, Cursing, Shadowing
• “The development of the Consensus Statement on Behavioral and Psychological Symptoms of Dementia (BPSD) represents a first step towards recognizing that these are core symptoms of dementia and that it is as essential to study and treat them as it is to study and treat any other aspects of dementing disorders.” (Finkel 1996)
Critiques à BPSD• McShane and Gormley (2002): “[d]rugs are widely and
often excessively used to manage BPSD. The placebo response rate is high in randomized studies. This may be because of the increased attention of triallists and the natural tendency of BPSD to resolve” (p. 241).
• Ballard and Cream (2005) : “the results [of studies on treating BPSD] are almost impossible to interpret, as the studies group together a range of dissimilar behavioral and psychiatric symptoms, which probably have different etiologies” (p. 6).
• van Iersel et al. (2004): “The term ‘BPSD’ served its goal by marketing the relevant problem of psychiatric co-morbidity and behavioural problems in dementia among scientists, clinicians and industry.”
Renforceurs de mémoire (« ça marche »), 2ième regard
• “The conclusion is clear: stabilizing or slowing the progression of symptoms of AD using these drugs is a clinically meaningful therapeutic goal”(Gauthier 2006)
• “There is substantial evidence that available treatments for AD are effective in improving or reducing deterioration in behavior, ADLs [activities of daily living], and cognition.”(Geldmacher et al. 2006)
BPSD• Dans un article publié dans un journal de l’IPA :
AD is "... characterized by deterioration in the ability to perform activities of daily living (ADL) in addition to loss of cognitive function and behavioral changes" (Potkin 2002)
• 2007 BPSD vanishing (ADI), but the shift occurred
• Voir: A. Leibing, Tense prescriptions? Alzheimer medications and the anthropology of uncertainty – Part I, Transcultural Psychiatry, sous presse.
• A. Leibing - From the Periphery to the Center: Treating behavioural and psychological symptoms in dementia. Dans: Do we have a pill for that? Interdisciplinary perspectives on the development, use and evaluation of drugs in the treatment of dementia. Jesse Ballenger et al. (dir.). The Johns Hopkins University Press, sous presse.
2ième argument:(BPSD et) le besoin urgent de traiter les
symptômes non-cognitifs
• There’s still a person in there (Castleman et al. 1999)
• Hearing the Voice of People with Dementia (Goldsmith 1996)
• The Person with AD, Pathways to understanding the experience (Harris 2002)
• Speaking our Minds, Personal reflections from individuals with AD (Snyder, eds. 1999)
Alzheimer 1980 et 2000
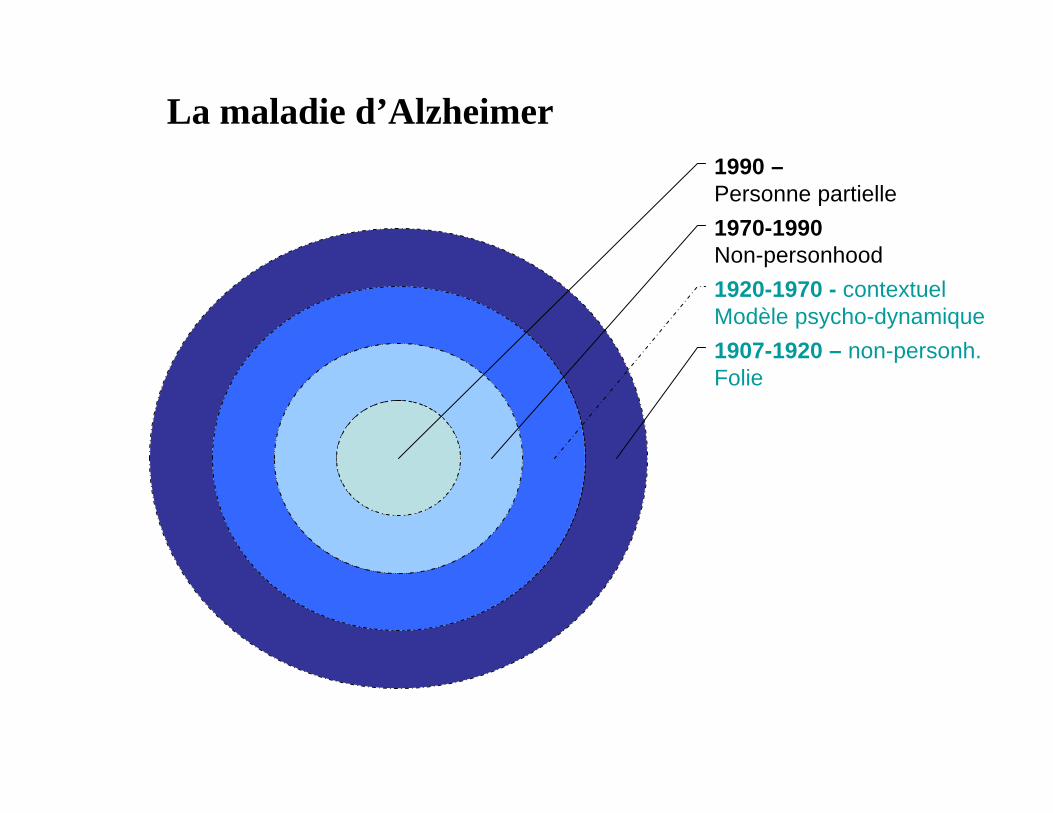
1907-1920 – non-personh.Folie
1920-1970 - contextuelModèle psycho-dynamique
1970-1990Non-personhood
1990 –Personne partielle
La maladie d’Alzheimer
« Avec la maladie d’Alzheimer, le défi des soignants est d’échapper aux limites
médicales de la maladie et de ressembler une nouvelle humanité dans la perte. »
Thomas Schenk, The Forgetting, 2002.
Voir: A. Leibing - Divided Gazes: Alzheimer’s disease, the Person Within, and Death in Life. Dans: Thinking about Dementia – Culture, loss, and the anthropology of senility. A. Leibing et Lawrence Cohen (dir.), Rutgers University Press, p. 240-268, 2006.
1 et 2: Le même vocabulaire (pharma et « mouvement du personhood »)
• Data published in the July issue of the Journal of the American Geriatrics Society suggest that treatment with Reminyl® (galantamine hydrobromide) may help to maintain the ability of patients with mild to moderate Alzheimer's disease to perform certain activities of daily living (ADLs), such as grooming, walking and being aware of current events.(…) (Janssen website)
3ième argument:la spécificité de gériatrie et gérontologie
• Geriatrics, like pediatrics, is often called a holistic science, since the biological processes of a patient group “in need of protection” are linked to psychosocial factors. Since aging cannot be cured, much of geriatric thinking aims to promote positive aging, through: 1. slowing down biological aging processes; 2. developing positive social relations and 3. overcoming negative aging stereotypes. (Leibing in press)
Trois lignes d’argumenter pour expliquer la certitude des médecins• 1. La production de BPSD qui crée une nouvelle
efficacité pour les médicaments (forte influence de l’industrie pharmaceutique)
• 2. L’acceptation de BPSD par les autres professionnels de la santé à cause du besoin depuis longtemps de traiter les symptômes non cognitifs et de reconnaître « la personne » dans la démence;
• 3. La « culture » spécifique en gériatrie et gérontologie qui a comme des concepts centraux la qualité de vie etc.
Résultats possibles
• La dynamique dans l’équipe change et les membres donne plus d’importance aux interventions non-médicamenteux;
• Empowerment des professionnels non-MD;
• Empowerment des familles et leurs observations;
• Un regard plus critique sur les publications