Cardiomyopathie du péripartum - anesth-chips.franesth-chips.fr/IMG/pdf/cardiomyopathie.pdf ·...
40
Cardiomyopathie du péripartum Staff d’Anesthésie du Lundi 20 Avril 2015 CHI Poissy St-Germain Sarah Féray – Interne
Transcript of Cardiomyopathie du péripartum - anesth-chips.franesth-chips.fr/IMG/pdf/cardiomyopathie.pdf ·...

Cardiomyopathie du péripartum
Staff d’Anesthésie du Lundi 20 Avril 2015
CHI Poissy St-Germain Sarah Féray – Interne

Cas clinique Madame TK, 36 ans, origine africaine • Antécédents médicaux :
– Obésité IMC = 33 – Aucun FdR cardiovasculaire
• Antécédents obstétricaux : – G3P3 :
– AVB en 2007 (4250g) – AVB en 2009 (4950g) – AVB en 2011 (5120g)
• Antécédents chirurgicaux : aucun • Allergie : non connue

Histoire de la maladie • Hospitalisé à 10 mois de sa dernière grossesse pour
décompensation cardiaque globale • Se plaint depuis 2 mois d’une dyspnée d’effort
Examen clinique initial : • Etat général conservé, apyrétique, TA 120/70, FC 90/min • Dyspnée NYHA III • Bruit du Coeur régulier, souffle systolique de 3/6ème mitral • Signes d’insuffisance cardiaque gauche : crépitants aux
bases pulmonaires • Signes d’insuffisance cardiaque droite : OMI,
hepatomegalie, reflux hépato-jugulaire

Examens complémentaires • ECG : ryhtme sinusal à 90/min, trouble de la repolarisation non
spécifique • Radio thorax : cardiomégalie, syndrome interstitiel accentué au
hile • Biologie : normale sauf NTproBNP 2000 pg/ml, troponine
négative • ETT :
VG dilaté - parois normotrophiques avec hypokinésie globale FEVG = 33% OG dilatée Cavités droites non dilatés, pas d’HTAP Fuite mitrale modérée

Diagnostic et PEC • Insuffisance cardiaque globale sur cardiomyopathie
dilatée, hypokinétique, non connue auparavant chez une patiente de 36 ans
• Hypothèse : cardiomyopathie dilatée liée à la grossesse à Coroscanner : normal à IRM cardiaque : cardiomyopathie dilatée non ischémique,
VG dilaté, FE à 33%. Pas d’étiologie spécifique retrouvée = élimination diagnostic
différentiel • Traitement médical débuté : Triatec, Bisoprolol, Lasilix,
Kardégic

Evolution • Suivi régulier, tous les 6 mois :
– Persistance d’une fonction VG altérée (FEVG = 40%) à 2 ans de l’épisode initial mais stabilité
– Asymptomatique dans la vie quotidienne, pas de dyspnée au repos ou à l’effort modérée
• Discussion de la mise en place d’une DAI
• CAT en cas de nouvelle grossesse?

Nouvelle grossesse • Se présente en février 2015, enceinte à 7 SA
+2 jour • Staff pluridisciplinaire DAN : demande d’ITG
d’indication maternelle • Consultation d’anesthésie : insuffisance
cardiaque à Aspiration sous AL potentialisée plutôt qu’AG
• Réalisation de l’Aspiration le 27/02/15 sous AL + Propofol en titration (total = 80 mg). Stabilité tensionnelle per et post opératoire

Définition CMP-PP • Cardiomyopathie idiopathique : – signes cliniques d’IC secondaire à dysfonction VG au
3ème trimestre ou dans les mois suivant l’accouchement à pic dans le premier mois post accouchement
– Absence de cause identifiable à l’insuffisance
cardiaque = dg d’élimination – Absence de cardiopathie pré-existante – Altération Echocardiographique de la fonction
systolique du VG, FEVG < 45% (+/- dilatation ventriculaire)

Pic de fréquence des cardiomyopathie au cours du péri-‐partum

Epidémiologie • Incidence très variable de 1/1000 à 1/4000
naissances • Facteurs de risque :
– Age maternel > 30 ans – Multiparité – Grossesses gémellaires – Origine Africaine – Obésité – Pré-eclempsie et HTA gravidique – Tocolyse prolongée (> 4 semaines)

Physiopathologie
La dyspnée est le maître symptôme, d’abord à type de poly-pnée superficielle d’effort, puis s’aggravant rapidement. Unoedème aigu pulmonaire inaugural peut être la première ma-nifestation la CMP-PP. Cette dyspnée pose un problème dediagnostic différentiel dans ce contexte avec la survenue d’uned’embolie pulmonaire grave. Elle est accompagnée dans prèsde deux tiers des cas d’une toux, volontiers nocturne, majoréepar le décubitus et en rapport avec l’insuffisance ventriculairegauche.Des précordialgies atypiques peuvent être présentes et neprennent qu’exceptionnellement une allure angineuse [3].En cas de scène infarctoïde et/ou d’électrocardiogramme évo-cateur (sus-décalage du segment ST, bloc de branche gauchenon connu antérieurement), il faut discuter la réalisation d’unecoronarographie en urgence afin d’éliminer un infarctus pardissection coronaire, autre maladie rare mais particulièrementpréoccupante pouvant survenir au décours de l’accouchement[13].On note aussi des signes cliniques classiques d’insuffisancecardiaque gauche : tachycardie sinusale, galop présystolique,assourdissement des bruits du coeur, souffle d’insuffisancemitrale fonctionnelle, râles crépitants pulmonaires. Une
insuffisance cardiaque droite associée est souvent présente,avec la classique triade syndrome oedémateux – hépatomégalie– reflux hépatojugulaire. Un tableau de choc cardiogénique peuts’installer en quelques heures, avec une hypotension artérielle,des signes d’hypoperfusion périphérique et une oligo-anurie.
Examens complémentaires
Radiographie thoraciqueLa radiographie thoracique est non spécifique, montrant dessignes d’insuffisance cardiaque et une cardiomégalie quasiconstante [4]. Les cliches successifs vont permettre de suivrel’évolution des signes congestifs.
ÉlectrocardiogrammeLe tracé est le plus souvent assez banal dans ce contexted’insuffisance cardiaque : tachycardie sinusale, possibles trou-bles du rythme supra-ventriculaire (fibrillation atriale notam-ment), voire ventriculaires (extrasystolie, salves de tachycardieventriculaire), anomalies non spécifiques de la repolarisation,pouvant parfois prendre le masque d’une cardiopathie isché-miques avec des modifications systématisées du segment ST àtype de sus ou sous-décalage.
616
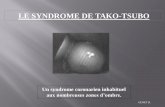
Figure 1Ensemble des mécanismes physiopathologiques supposés ou démontrés contribuant à la survenue d’une cardiomyopathie dupéripartumIL : interleukynes ; HTA : hypertension artérielle ; TNF : tumor necrosing factor.
D’après [14]
G Vanzetto, A Martin, H Bouvaist, S Marlière, M Durand, O Chavanon
tome 41 > n86 > juin 2012

Changements physiologiques
• 50% d’augmentation du volume intravasculaire : pic au début/milieu du 3ème trimestre
• Diminution progressive des résistances vasculaires systémiques et Augmentation DC (30-40%) à PAM conservée, augmentation 15% FC
• Variations importantes DC durant le travail avec tachycardie et augmentation ~ 500 ml de volume sanguin dans la circulation à chaque contraction
• Etat d’hypercoagulabilité • Diminution de la CRF

Physiopathologie
• Hypothèse inflammatoire : – Biopsies myocardique : lésion « myocardite aigue » – Perturbation réponse inflammatoire au cours de la grossesse – Facteur infectieux initiant/aggravant cette réaction
inflammatoire inappropriée : virus • Hypothèse Auto-immune :
– Ac anti actine, anti myosine utérins libérés – Modification immunitaire de fin de grossesse (perte de la
tolérance immunologique du fœtus / persistance Ag fœtaux circulant)
• Hypothèse Hormonale : élévation stress oxydatif à activation cathepsine D à clivage en la prolactine en 16kDAProlactine à dysfonction cardiomyocytes, endothéliales

Diagnostic différentiel
• Eliminer une cardiopathie préalable à la grossesse (interrogatoire) : – Cardiomyopathie dilatée familiale – Antécédents de cardiopathies hypertrophiques – Prise anthracyclines
• Eliminer une cause aigue de dysfonction systolique ventriculaire gauche : – Infarctus du myocarde ( ECG +++ et coronarographie si besoin) – Myopéricardite (Fièvre, syndrome inflammatoire +/- douleurs
thoraciques, ETT, IRM si diagnostic très suspect) – Valvulopathies (ETT)

Diagnostic différentiel • Atteinte cardiaque de la pré-éclampsie
– dysfonction diastolique – Pression remplissage élevée MAIS fonction systolique
normale • Pré-eclampsie et CMP-PP partagent certains mécanismes
physiopathologiques (lésions endothélium)
• Plusieurs cohortes de patiente avec CMP PP : grande prévalence d’HTA/pré-éclampsie à pré-éclempsie prédispose à CMP-PP ?
• Résolution rapide après l’accouchement Versus traitement et suivi de plusieurs mois

Diagnostic
• Clinique : – Typique d’insuffisance cardiaque :
• DYSPNEE (superficielle à l’effort puis d’aggrave rapidement)
• OAP inaugurale, toux nocturne, majorée par décubitus • Signes Insuffisance cardiaque gauche et droite
– Signes non spécifiques : • Douleur thoracique, palpitations • Embolies systémiques ou pulmonaires

Diagnostic • Paraclinique :
– ECG : non spécifique, tachycardie, trouble du rythme, trouble repolarisation à type ondes T négatives
– Radio de Thorax : cardiomégalie – ETT : examen clé = dysfonction systolique ventriculaire
gauche et dilatation ventriculaire +/- sévère

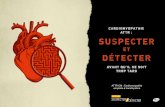
Diagnostic IRM cardiaque: éliminer diagnostic différentiel
• Fibroses myocardique : hypersignal, rehaussement tardif = absente à élimine myocardite
• Eliminer ischémie (dissection coronaire au cours effort acchmt) • Estimation fonction VG, volume • Détection thrombi
PAS DE REHAUSSEMENT TARDIF APRES GADOLINIUM ICI SUR VG MODEREMENT DILATE

Pronostic • Favorable dans 50% des cas : récupération complète de la
fonction systolique VG • Amélioration partielle de la fonction systolique dans la majeur
partie autres cas • Rare cas de défaillance myocardique sévère pouvant aboutir à la
nécessité d’un support HD (ECMO) voir d’une greffe (<10%) à Mortalité : 1 à 2%
• Facteur de mauvais pronostic : – Gravité de la défaillance HD initiale et sa réponse au ttt – Complications emboliques – Existence d’une cardiopathie séquellaire au delà du 6ème mois après
diagnostic

Prise en charge initiale • Traitement conventionnel :
– Restriction hydro-sodée – Diurétique de l’anse, dérivés nitrés si signes congestifs – IEC dans le post partum (Teratogène + IRA) – ß bloquant cardiosélectif – +/- antialdostérone
• Traitement anticoagulant : Héparinothérapie dose curative phase aigue – thrombus à l’écho – passage en ACFA
• Si HD instable : inotrope positif (dobutamine)
• Assistance circulatoire • Transplantation cardiaque

Prise en charge obstétricale (CMP 3ème trimestre)
• Collaboration multidisciplinaire (GO,AR,Cardio,Néonat) • Planifier un déclenchement ou une extraction
Pas de recommandations • Césarienne = risque hémorragique, thrombo-embolique,
infectieux si FEVG < 35% ? VERSUS • Voie basse = augmentation du débit cardiaque
Eviter épreuve d’effort, travail long, douloureux Abréger l’expulsion : forceps Possible si état cardiaque stable (FEVG > 35% ?)

Prise en charge anesthésique
Pas de consensus : idem insuffisant cardiaque
Voie basse Analgésie péridurale
– Titration des AL pour éviter modification HD – Association AL faible dose/concentration + morphinique = Bloc d’installation très progressive – Traitement de l’hypotension artérielle : phényléphrine ou
ephédrine-phényléphrine à éviter tachycardie maternelle /maintien perfusion utérine
– Proclive latéralisée à gauche

Prise en charge anesthésique Pas de consensus : idem insuffisant cardiaque
Césarienne APD seule /APD-Rachi / Rachianesthésie continue AG : à éviter
• IOT séquence rapide : etomidate, celocurine, morphinique • Stabilité hémodynamique (monitorage ++)
– Induction lente, dosage réduit – Pré-charge : monitorer le remplissage, peu de précharge-
dépendance. – Post-charge : maintenir basse à pression perfusion coronnaire – Correction HD avec vasoconstricteurs, inotropes, sans modifier
profondeur anesthésie – Halogénés : Sevoflurane

Prise en charge anesthésique
Abaisser la postcharge Favoriser la contractilité
Apport d’oxygène
Monitorage fonction cardiaque remplissage
Ocytocine CI relative Nalador
Normothermie Analgésie
✔Surveillance post op continue USI

Rappels • Péridurale lombaire : – VasodilataJon veineuse, baisse du retour veineux, bradycardie
• Rachianesthésie : sympathicolyse brutale
• AG : – VenJlaJon mécanique en pression posiJve : diminuJon pré-‐charge, augmentaJon post charge
– Agents anesthésiques

Prise en charge au long cours • IEC • B bloquant • Diurétique si nécessaire (Pression remplissage élevées) • Aldactone si NYHA ≥ II - III • Surveillance régulière : clinique + ETT • Si persistance FEVG ≤ 35% : discussion DAI en
prévention primaire de TdR ventriculaire +/- stimulation multi-sites si présence BBG complet
• Transplantation cardiaque
Traitements spécifiques sans preuves : Immunoglobuline IV , Immunosupresseur
Bromocriptine (en cours d’étude)

Prise en charge obstétricale
C-I de la contraception oestro-progestative Récidive grossesse ultérieure : 25 à 100%
- Contre indiqué si FEVG < 50% - Déconseiller même si récupération complète (info patiente ++) - IMG en cas dégradation de FEVG au cours 1 ou 2ème trimestre - Intérêt ETT dépistage ?
IEC, et les bêtabloquants est introduit après quelques jours, unefois la patiente stable. Si la cardiomyopathie se déclare avantl’accouchement, les IEC sont contre-indiqués en raison de leurrisque tératogène. En revanche, il n’y pas de contre-indication àl’allaitement, et les IEC pourront donc être débutés rapidementaprès la délivrance (tableau II).Selon la sévérité de la dysfonction ventriculaire initiale, uneanticoagulation peut être débutée, car des complicationsthrombo-emboliques artérielles ont été rapportées [24], etl’évolution de la fonction systolique à court et moyen termene peut être prédite. Certaines équipes recommandent doncla mise en place d’une anticoagulation efficace systématique sila fonction systolique est inférieure à 35 % [25]. Commepour les IEC, les antivitamines-K (AVK) sont contre-indiquéesdurant le dernier trimestre de la grossesse, et ne devrontdonc pas être prescrits en cas de décompensation avant l’ac-couchement. Dans ces conditions, la patiente est traitée parhéparine.
Perspectives thérapeutiques
D’autres approches, telles que l’administration d’immuno-globulines IV, seraient à évaluer de manière prospective[26]. De même, l’ajout d’un traitement anti-TNF-alpha (lapentoxifylline) au traitement conventionnel semble améliorerles chances de normalisation de la fonction systolique [27]. Demanière plus récente, l’équipe de Hilfiker-Kleiner, en se fon-dant sur les données de leur modèle expérimental murinimpliquant un produit issu de la dégradation de la prolactinedans la dysfonction systolique ventriculaire au cours de la CPP(cf chapitre Physiopathologie), a testé l’intérêt potentiel d’untraitement par bromocriptine dans un essai de phase I nonrandomisé sur 12 patientes gravides ayant des antécédents deCPP. Les 6 patientes traitées par bromocriptine ont eu unpronostic favorable et sont demeurées asymptomatiques, alorsque 3 des 6 patientes non traitées par bromocriptine sontdécédées, tandis que les 3 autres ont eu une altération sig-nificative de leur fonction cardiaque. Ces premiers résultatspourraient conduire à la mise en place d’un essai multicentriquerandomisé [28].
Prise en charge obstétricale
Il n’y a pas de recommandations systématiques pour la gestionobstétricale des patientes ayant un tableau de CPP avant leterme de la grossesse. La décision d’un accouchement préma-turé est discutée au cas par cas en fonction de la sévérité de ladysfonction ventriculaire gauche, de l’évolution initiale soustraitement, et d’une éventuelle souffrance foetale.
Prise en charge au long coursElle repose, à nouveau, sur le traitement classique de l’insuffi-sance cardiaque chronique, avec l’association bêtabloquant,IEC, et des diurétiques de l’anse selon l’importance de ladysfonction ventriculaire gauche et les signes éventuels derétention hydrosodée. L’interruption du traitement après récu-pération ad integrum de la fonction systolique ne semble pass’accompagner d’une nouvelle dégradation de fonction [19].Cependant, la poursuite des traitements reste recommandéeau long cours. Étant donné la prescription chronique d’IEC, lespatientes doivent être sous contraception. Cette contraceptiondoit être revue et prescrite par le gynécologue de la patiente,en rappelant la contre-indication de principe des oestroproges-tatifs dans le cadre de l’insuffisance cardiaque. En cas denouvelle grossesse, les IEC doivent être immédiatement inter-rompus.Enfin, en absence de récupération de la fonction cardiaque, etselon l’évolution clinique, les patientes sont éventuellementinscrites sur liste de transplantation cardiaque.
Conduite à tenir en cas de nouvelle grossesse
Une contraception efficace est essentielle chez ces femmesjeunes dans les suites d’un premier épisode de CPP. En cas denouvelle grossesse, le suivi obstétrical doit être organisé dans
999
Mis
eau
poin
t
Tableau IITraitements de l’insuffisance cardiaque autorisés ou contre-indiqués durant la grossesse
Traitements autorisés Traitements contre-indiqués
Digoxine IEC/ARA-II
Dérivés nitrés Amiodarone
Héparine AVK
Diurétiques
Bêtabloquants
Dobutamine
Dopamine
(AVK : Antivitamine K ; ARA-II : antagonistes des récepteurs de l’angiotensine-II ; IEC :inhibiteur de l’enzyme de conversion).
Tableau IÉvolution en cas de nouvelle grossesse (d’après [23])
Fonctionsystoliquenormalisée
Persistanced’une dysfonction
systolique
Risque d’insuffisance cardiaque 26 % 50 %
Dégradation de la FEVG > 20 % 17 % 33 %
Risque d’accouchement prématuré 13 % 50 %
Risque de décès de la patiente 0 % 25 %
Retour à la fonction systoliqueinitiale (avant la seconde grossesse)
90 % 60 %
(FEVG : fraction d’éjection ventriculaire gauche).
Cardiomyopathie du péripartum
Journees europeennes de la Societ e française de cardiologie
tome 38 > n86 > juin 2009

Conclusion • Cause rare d’insuffisance cardiaque • Physiopathologie incertaine • Pas de traitement spécifique pour l’instant • Evolution favorable dans majorité des cas sous
traitement médical simple • Rare cas de défaillance cardiaque sévère =
transplantation, décès • Suivi au long cours si récupération incomplète • Risque lors nouvelle grossesse ++ • PEC Multidisciplinaire

CASE REPORTS / CASE SERIES
Anesthetic management and outcomes of parturients with dilatedcardiomyopathy in an academic centre
Gestion anesthesique et evolution de parturientes atteintes decardiomyopathie dilatee dans un centre universitaire
Unyime S. Ituk, MBBS • Ashraf S. Habib, MBBCh •
Carrie M. Polin, MD • Terrence K. Allen, MBBS
Received: 22 January 2014 / Accepted: 2 December 2014 / Published online: 11 December 2014! Canadian Anesthesiologists’ Society 2014
AbstractPurpose This study examines the peripartum anesthetic
management and outcomes of women with dilated
cardiomyopathy in a large university medical centre overa seven-year period.
Principal findings Twenty-five women were included in
this series, 18 with a new diagnosis of cardiomyopathy andseven with a history of cardiomyopathy. Sixteen patients
(64%) identified themselves as African American, seven
(28%) were Caucasian, and two patients (8%) wereHispanic. The median (range) gestational age at the time
of a new diagnosis of cardiomyopathy was 29 (7-38) weeks.
Eight women (32%) had New York Heart Association classIII/IV symptoms at the time of delivery or in the immediate
postpartum period. A multidisciplinary team of
obstetricians, anesthesiologists, cardiologists, andpediatricians were involved in the care of these women.
The median (range) gestational age at the time of delivery
was 33.5 (30-40) weeks. There were nine vaginal deliveries
and 15 operative deliveries. One patient had fetal loss at19 weeks gestation. Twelve women had labour induced
with an intravenous infusion of oxytocin at a rate of 0.001-
0.02 IU!min-1. An oxytocin infusion at a variable rate witha maximum dose of 0.05 IU!min-1 was administered after
vaginal delivery to maintain uterine tone. Epidural
analgesia was initiated prior to induction of labour or inthe latent phase of labour. Seven Cesarean deliveries were
performed under combined spinal-epidural anesthesia, five
were performed under epidural anesthesia, and threewomen had general anesthesia. Oxytocin was administered
via an intravenous infusion at a rate of 0.05-0.2 IU!min-1
after operative delivery. One patient had a cardiac arreston induction of general anesthesia and was successfully
resuscitated. There were no maternal or neonatal deaths.
Ten women were followed up at our institution and at sixmonths postpartum; 50% of these patients were still
symptomatic.
Conclusion We report favourable outcomes in 25pregnant women with dilated cardiomyopathy who were
managed by a multidisciplinary team.
ResumeObjectif Cette etude examine la gestion anesthesiqueperipartum et l’evolution des femmes atteintes de
cardiomyopathie dilatee dans un grand centre medical
universitaire sur une periode de sept ans.Constatations principales Vingt-cinq femmes ont ete
incluses dans cette serie: 18 avec un diagnostic recent de
cardiomyopathie et 7 avec une anamnese decardiomyopathie. Seize patientes (64 %) s’identifiaient
comme Afro-americaines, sept (28 %) etaient
caucasiennes et deux (8 %) etaient hispaniques. L’agegestationnel median (ecart) au moment du nouveau
diagnostic de cardiomyopathie etait de 29 (7 a
This article is accompanied by an editorial. Please see Can J Anesth2015; 62: this issue.
Author contributions Unyime S. Ituk and Ashraf S. Habibparticipated in the study design. Unyime S. Ituk, Ashraf S. Habib,Carrie Polin, and Terrence K. Allen contributed to data collection,data interpretation, and writing of the manuscript.
U. S. Ituk, MBBS ! A. S. Habib, MBBCh !C. M. Polin, MD ! T. K. Allen, MBBSDepartment of Anesthesiology, Duke University Medical Center,Durham, NC, USA
U. S. Ituk, MBBS (&)Department of Anesthesia, Carver College of Medicine,University of Iowa, 200 Hawkins Drive, 6JCP, Iowa City,IA 52242, USAe-mail: [email protected]
123
Can J Anesth/J Can Anesth (2015) 62:278–288
DOI 10.1007/s12630-014-0290-y

induction of labour or in the latent phase of labour. The
standard mixture for epidural analgesia infusion at ourinstitution is 0.1% bupivacaine with fentanyl 2 lg!mL-1.
Epidural analgesia was initiated with a 15-20 mL bolus of
0.1% isobaric bupivacaine given in divided doses andfentanyl 50 lg. Patient-controlled epidural analgesia was
maintained with 0.125% bupivacaine with fentanyl
2 lg!mL-1 using a bolus of 5 mL with an eight-minutelockout period and a continuous infusion of 5 mL!hr-1.
Intra-arterial blood pressure monitoring was initiated priorto epidural catheter placement in six women, and two
women had a central venous catheter placed for central
venous pressure monitoring in labour. All labouringpatients except one (patient #9) had pulse oximetry and
electrocardiographic telemetry monitoring. Table 3
summarizes the mode of delivery and anestheticmanagement of the included patients.
Seven Cesarean deliveries were performed under
combined spinal-epidural (CSE), and in five patients,epidural anesthesia was used for Cesarean delivery. The
spinal component of the CSE was used to deliver 0.75%
hyperbaric bupivacaine 7.5 mg, fentanyl 15-20 lg, andpreservative-free morphine 150 lg for postoperative
analgesia. Two percent lidocaine with epinephrine
1:200,000 was administered via the epidural to augmentor prolong surgical anesthesia in all patients who had a
CSE. If the patient did not receive intrathecal morphine,preservative-free morphine 3 mg was administered via the
epidural catheter for postoperative analgesia.
Two women (patients #14 and 19) had generalanesthesia for Cesarean delivery because of failure of the
neuraxial anesthesia technique to establish adequate
surgical anesthesia. A third woman (patient #12) receivedgeneral anesthesia for cardioversion of refractory
Table 1 Patient characteristics
Patient Age (yr) BMI(kg!m-2)
Gravidity/Parity
Gestational ageat diagnosis(weeks)
LVEF (%) Interval betweenLVEF measurementand delivery (weeks)
NYHA class Other Medical history
1 43 28 G1P0 31 35 \ 1 III HTN
2 26 38 G1P0 28 15 2 IV GDM
3 34 50 G6P4 29 30 7 II HTN, GDM
4 37 42 G6P2 19 15 \ 1 II HTN
5 34 37 G11P0 30 35 1 II HTN, DM
6 30 36 G4P1 29 35 3 II AICD
7 32 27 G4P1 25 40 7 I -
8 30 28 G5P4 Pre-existing 30 3 II Congenitalendocardiofibroelastosis
9 39 40 G12P8 31 25 \ 1 II HTN
10 28 26 G7P2 38 35 \ 1 II -
11 40 28 G1P0 35 35 \ 1 III DM, HTN, CAD
12 29 40 G1P0 34 15 \ 1 IV DM, HTN
13 32 50 G4P2 18 40 4 III Sleep apnea
14 29 43 G3P2 36 35 \ 1 III Preeclampsia
15 28 29 G4P2 24 20 2 III -
16 27 44 G5P3 Pre-existing 40 4 I HTN
17 33 27 G1P0 Pre-existing 35 7 I A-V block, pacemaker
18 29 28 G2P1 7 40 9 II -
19 36 60 G6P3 Pre-existing 45 6 II HTN, Preeclampsia
20 37 48 G3P2 Pre-existing 20 2 III DM
21 34 48 G11P0 29 35 5 II HTN, DM
22 24 28 G2P1 Pre-existing 40 2 II -
23 25 50 G8P4 22 35 4 II HTN, DM
24 32 38 G4P3 8 40 8 II ASD
25 31 43 G4P2 Pre-existing 40 2 II Atrial fibrillation
BMI = body mass index; A-V block = atrioventricular block; LVEF = left ventricular ejection fraction; NYHA = New York HeartAssociation; HTN = hypertension; GDM = gestational diabetes mellitus; DM = diabetes mellitus; AICD = automatic implantablecardioverter–defibrillator; CAD = coronary artery disease; ASD = atrial septal defect
Cardiomyopathy in pregnancy 281
123

Table 3 Mode of delivery and anesthetic management
Patient Gestation(weeks) atdelivery
Mode ofdelivery
Urgency ofdelivery
Indication for Cesareandelivery
Type of Anesthesia InvasiveMonitoring
Neonatal weight(grams)/APGARscore
Peripartum Complications
1 31 Cesarean Scheduled Breech presentation CSE ABP 1,860/6,1 -
2 31 Cesarean Scheduled Breech presentation CSE ABP, PAC 1,865/8,9 Cardiogenic shock, LV clot
3 36 Cesarean Scheduled Breech presentation CSE ABP 3,875/9,9 -
4 19 D & E (IUFD) - - CSE ABP - -
5 32 Cesarean Scheduled Breech presentation CSE ABP 1,560/9,9 Wound sepsis
6 32 FAVD - - Epidural ABP 1,420/3,6 -
7 37 FAVD - - Epidural ABP 2,480/8,9 -
8 31 FAVD - - Epidural ABP 1,780/4,8 -
9 31 SVD - - None None 1,820/8,9 1,730/4,8 Precipitous labour
10 38 Cesarean Emergent NRFHT* Epidural ABP, CVC 3,645/9,9 Uterine atony
11 35 Cesarean Urgent Deteriorating cardiac function Epidural ABP 2,250/7,8 -
12 34 Cesarean Urgent Deteriorating cardiac function General ABP, PAC 2,080/9,9 SVT requiring cardioversion
13 39 FAVD - - Epidural None 3,070/8,9 -
14 36 Cesarean Urgent Deteriorating cardiac function General (Failedepidural)
ABP, CVC 2,800/5,8 Pulmonary edema
15 34 FAVD - Epidural ABP, CVC 2,620/8,9 -
16 33 Cesarean Urgent Placenta previa CSE CVC 2,030/6,7 -
17 40 Cesarean Scheduled Breech presentation CSE None 3,905/8,9 -
18 38 FAVD - - Epidural None 3,150/9,9 -
19 38 Cesarean Emergent Severe Preeclampsia* General (Failedepidural)
ABP, CVC 3,120/1,5 Cardiac Arrest
20 32 Cesarean Emergent NRFHT* Epidural ABP, CVC 1,890/8,9 PVC, atrial fibrillation
21 32 Cesarean Emergent NRFHT* Epidural None 1,560/9,9 Wound sepsis
22 33 Cesarean Urgent Deteriorating cardiac function Epidural None 2,080/9,9 -
23 32 Cesarean Urgent Previous Cesarean x3 CSE None 1,760/6,7 -
24 39 FAVD - - Epidural None 3,070/8,9 -
25 30 FAVD - - Epidural None 3,785/8,9 SVT
CSE = combined spinal-epidural; ABP = intra-arterial blood pressure; PAC = pulmonary artery catheter; LV = left ventricle; D & E = dilatation and evacuation; IUFD = intrauterine fetaldemise; FAVD = forceps-assisted vaginal delivery; SVD = spontaneous vaginal delivery; NRFHT = non-reassuring fetal heart tone; CVC = central venous catheter; SVT = supraventriculartachycardia; PVC = premature ventricular contraction. APGAR scores were measured at one and five minutes. *Labouring prior to Cesarean delivery
Card
iom
yo
path
yin
preg
nan
cy2
83
123

Bibliographie • Mise au point 2012 - Journées Européennes de la SFC -
Cardiomyopathie du péripartum - Gérald Vanzetto, Alix Martin, Hélène Bouvaist, Stéphanie Marlière, Michel Durand, Olivier Chavanon
• Cardiopathies et grossesse – SFAR – Vincent Laudenbach • Précis d’anesthésie cardiaque – Chapitre 13 Anesthésie et
cardiomyopathie • Pregnancy and non-valvular heart disease--anesthetic
considerations – Annals of cardiac anesthesia 2010 • Peripartum cardiomyopathy : current management and future
perspectives – European Heart Journal, 2015
Remerciement • Docteur David Berville, Cardiologue, CHI de Poissy

Merci de votre attention

kinetic pattern throughout pregnancy and postpartum (Table 1). Sofar, NT-proBNP, an unspecific marker for pregnancy complicationssuch as preeclampsia as well as for heart failure and other diseases,is markedly elevated in most PPCM patients with little overlap tohealthy peripartum women (Table 1).23,39,40 MiR-146a is specificallyincreased in the serum of PPCM patients compared with healthypostpartum women and patients with DCM (Table 1).23,38 sFlt1, abiomarker for preeclampsia that is supposed to clear rapidly after de-livery, is significantly increased in PPCM patients as are asymmetricdimethyl arginine and Cathepsin D activity (Table 1).23,33 Failure tonormalize a biomarker profile including NT-proBNP, oxLDL,interferon-g, and prolactin is associated with adverse outcome inPPCM patients.39 In turn, creatine-kinase and C-reactive proteinare increased by delivery stress in healthy postpartum women andtroponin T, a marker for cardiac injury, is often within normalranges in PPCM patients (Table 1) and therefore less suited as bio-markers for PPCM.11
Taken together, currently NT-proBNP is the only commerciallyavailable marker for efficient screening of peripartum heart failure(Table 1). However, it is not specific for PPCM and may be elevatedin other conditions such as preeclampsia and pulmonary embolism.MiR-146a is a disease specific potential candidate, but overall thereis an urgent need for better diagnostic and prognostic biomarkersfor PPCM.
Therapeutic concepts andmanagement for peripartumcardiomyopathyHeart failure around pregnancy provides a challenge for the treatingphysician especially due to a lack of evidence-based clinical data.
Currently, PPCM is treated according to the ESC guidelines forheart failure in pregnancy.1 In brief, late in pregnancy, therapeuticinterventions need to consider the health of the mother and thefoetus. Beta-blocker, thiazide diuretics, or furosemide treatmentcan be necessary in some patients with PPCM before delivery,however, as diuretic therapy may impair perfusion of the placentawith potential harm to the foetus, the lowest dosages possible of di-uretic therapy have to be used. After delivery, standard therapy forheart failure is recommended in PPCM including beta-blockers,ACE-inhibitors/AT1-blockers, mineralocorticoid receptor antago-nists (MRA), and diuretics. As no data on the use of inotropes existin patients with PPCM and catecholamines may aggravate myocardialdamage, an i.v. infusion of an inotrope (e.g. dobutamine) should onlybe considered in patients with severe hypotension and/or signs ofcardiogenic shock. As soon as haemodynamic stability is achieved,inotropes should be tapered and general recommendations forpatients with heart failure in pregnancy should be followed.1 Earlytreatment with beta-blockers started at very low dosages appearsto be protective even in patients with severely depressed ejectionfraction. In patients with persistent sinus tachycardia, in whomuptitration of beta-blocker dose was not feasible due to hypotensionor heart failure, we also have good experience with the use ofivabradine.
A South African study reports improved outcome in PPCMpatients with elevated serum markers of inflammation (C-reactive
protein and tumour necrosis factor-a, TNF-a) after treatmentwith pentoxifylline on top of conventional heart failure therapy sug-gesting a potential benefit of anti-TNF-a treatment.41
A pilot study in South Africa reported highly beneficial effect of theprolactin-blocker bromocriptine on top of heart failure medication inpatients with acute onset PPCM.3,42 Likewise, the majority of patientsin the German PPCM registry (96%) who had obtained this therapyconcept improved their condition.23 Currently, the efficacy ofbromocriptine on top of heart failure medication is investigated in alarger randomized multicentre trial in Germany (ClinicalTrials.gov,study number: NCT00998556). Importantly, a recent statementfromthe European Medicines Agency (EMA) recommends restricteduse of bromocriptine for women to stop breast milk production dueto adverse effects on blood pressure and thrombosis. To our knowl-edge, noadverseeffectswereobservedwith low dosebromocriptine(2–5 mg/day) in 57 PPCM patients from the German PPCM registryor in the 44 patients currently enrolled in the German bromocriptinetrial. Moreover, no adverse event related to bromocriptine wasreported from the 75 PPCM patients listed in the internationalPPCM registry of the ESC EURObservational Research Programme.Results from larger studies are awaited for to be more conclusive onthis therapy concept.
PPCM patients have an increased risk for sudden death and seemto benefit from implantable cardioverter defibrillator (ICD) andcardiac resynchronization therapy (CRT).39,43,44 As many PPCMpatients recover from the disease or display at least marked improve-ment of systolic LV function, a wearable cardioverter/defibrillatorwould be an alternative option vs. operative ICD or CRT-D implant-ation for primary prophylaxis. We recommend the use of a wearable
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Overview of biomarkers analysed inperipartum cardiomyopathy patients
Biomarker Relevance for PPCM
NT-proBNP Not specific for PPCM, but goodsensitivity for heart failure.23,39
16-kDa Prolactin Pathophysiological factor of PPCM, hightechnical effort for measurement,diagnostic accuracy needs to beevaluated.37,42
Interferon-g Elevated plasma levels in PPCM patients,diagnostic accuracy needs to beevaluated.39,49
AsymmetricDimethylarginine(ADMA)
Marker for endothelial dysfunction andcardiovascular risk, diagnosticaccuracy needs to be evaluated.23
Cathepsin D Activity elevated in plasma of PPCMpatients, diagnostic accuracy needs tobe further evaluated.23,37
Soluble fms-like tyrosinekinase-1 (sFlt-1)
Elevated plasma levels in PPCM patients,diagnostic accuracy needs to befurther evaluated.33
microRNA-146a Pathophysiological factor of PPCM, hightechnical effort for measurement,diagnostic accuracy needs to befurther evaluated.23,38
PPCM, peripartum cardiomyopathy.
D. Hilfiker-Kleiner et al.Page 4 of 8
by guest on April 11, 2015D
ownloaded from

and when no other cause for these changes is identifiedthe diagnosis of peripartum cardiomyopathy is made.Even amongst pathologists there is a lack of familiarityregarding this specific definition and the criteria for diag-nosing peripartum cardiomyopathy which leads to incor-rect classification of the heart failure.1
Recent work in healthy term pregnant women hasfound reductions in systolic function and impairmentof diastolic function quantified by a reduction in cardiacoutput to pre-pregnancy values and increased mitralvalve E/e0 in some asymptomatic women.9,12,37 Thissuggests that asymptomatic heart dysfunction may bemore common than previously thought and it may bethat these women are at greater risk of developing heartfailure with reduced ejection fraction (i.e. peripartumcardiomyopathy) with a longer pregnancy or in thepostpartum period.9 Large longitudinal serial studiesusing TTE are needed in healthy women to explore thishypothesis.
PreeclampsiaPreeclampsia, without heart failure, classically presentsas diastolic dysfunction with raised filling pressuresand a preserved ejection fraction (Table 1). Haemody-namic variables have been extensively studied in pre-eclampsia.12,14,15,32,38–47 Cardiac output is maintainedin uncomplicated, untreated disease and the ventriclesare of normal size. Left ventricular remodelling and leftventricular hypertrophy are common findings.12,14,15
There are no reports of involvement of the rightventricle.
Early important work by Visser and Wallenburghighlighted the finding of increased left ventricularstroke work index in women with preeclampsia and sug-gested that contractility was increased in these women.43
Subsequent echocardiographic work in women withuntreated disease characterised the diastolic changes inwomen with preeclampsia and confirmed preservationof systolic function.12 This diastolic impairment coupled
Table 1 Comparison of heart failure in peripartum cardiomyopathy and heart failure in preeclampsia
Peripartum cardiomyopathy Preeclampsia
Pathological mechanism Systolic dysfunction Diastolic dysfunctionAdditional features
Hypertension No YesProteinuria No Often
Associated featuresHaemolysis No YesAbnormal liver function No YesThrombocytopenia No YesSeizures No YesRenal dysfunction No Yes (proteinuria)Vascular thrombus Yes* Not reportedArrhythmia Yes^ Not reportedMitral regurgitation Yes Not reported
Echocardiography featuresCardiac volumes and structure
Left atrium volume Dilated NormalLeft ventricular volume Dilated NormalRight ventricular volume Dilated NormalPericardial effusions Infrequent and small Frequent and largerLeft ventricular hypertrophy No! Frequent
Cardiac functionLeft ventricular systolic function Reduced Preserved–
Contractility Reduced PreservedCardiac output Reduced Preserved/increasedMyocardial tissue Doppler systolic velocities Reduced Normal range–
Ejection fraction Reduced Preserved–
Right ventricular systolic function Reduced Not affectedDiastolic function Normal! Abnormal/reduced
Initial pharmacological treatmentInotropic agents Commonly used Uncommonly usedSystemic anticoagulation Yes Uncommonly usedAntihypertensive agents No YesParenteral magnesium sulphate No Yes
*Reported with severe ventricular dysfunction; ^Atrial fibrillation, ventricular tachycardia and ectopics reported; !Unless hypertension presentbefore pregnancy; –Systolic function may be reduced in the presence of malignant hypertension.
A.T. Dennis, J.M. Castro 263

The New England
Journal
of
Medicine
Copyr ight © 2001 by the Massachusett s Medical Society
VOLUME 344
M
AY
24, 2001
NUMBER 21
N Engl J Med, Vol. 344, No. 21
·
May 24, 2001
·
www.nejm.org
·
1567
MATERNAL AND FETAL OUTCOMES OF SUBSEQUENT PREGNANCIES IN WOMEN WITH PERIPARTUM CARDIOMYOPATHY
U
RI
E
LKAYAM
, M.D., P
ADMINI
P. T
UMMALA
, M.D., K
ALPANA
R
AO
, M.D., M
OHAMMED
W. A
KHTER
, M.D., I
LYAS
S. K
ARAALP
, M.D., O
MAR
R. W
ANI
, M.D., A
FSHAN
H
AMEED
, M.D., I
SRAEL
G
VIAZDA
, B.S.,
AND
A
VRAHAM
S
HOTAN
, M.D.
A
BSTRACT
Background
Peripartum cardiomyopathy is a rarebut sometimes fatal form of heart failure. Little isknown about the outcomes of subsequent pregnan-cies in women who have had the disorder.
Methods
Through a survey of members of theAmerican College of Cardiology, we identified 44women who had had peripartum cardiomyopathy andhad a total of 60 subsequent pregnancies. We thenreviewed the medical records of these women andinterviewed the women or their physicians.
Results
Among the first subsequent pregnanciesin the 44 women, 28 occurred in women in whomleft ventricular function had returned to normal (group1) and 16 occurred in women with persistent left ven-tricular dysfunction (group 2). The pregnancies wereassociated with a reduction in the mean (±SD) leftventricular ejection fraction both in the total cohort(from 49±12 percent to 42±13 percent, P<0.001) andin each group separately (from 56±7 percent to 49±10percent in group 1, P=0.002; and from 36±9 percentto 32±11 percent in group 2, P=0.08). During thesepregnancies, symptoms of heart failure occurred in21 percent of the women in group 1 and 44 percent ofthose in group 2. The mortality rate was 0 percent ingroup 1 and 19 percent in group 2 (P=0.06). In addi-tion, the frequency of premature delivery was higherin group 2 (37 percent vs. 11 percent), as was that oftherapeutic abortions (25 percent vs. 4 percent).
Conclusions
Subsequent pregnancy in women witha history of peripartum cardiomyopathy is associatedwith a significant decrease in left ventricular functionand can result in clinical deterioration and even death.(N Engl J Med 2001;344:1567-71.)
Copyright © 2001 Massachusetts Medical Society.
From the Section of Heart Failure, Division of Cardiology, Departmentof Medicine (U.E., P.P.T., K.R., M.W.A., I.S.K., O.R.W., I.G., A.S.), andthe Department of Obstetrics and Gynecology (A.H.), University ofSouthern California School of Medicine, Los Angeles. Address reprint re-quests to Dr. Elkayam at the Section of Heart Failure, Division of Cardi-ology, University of Southern California School of Medicine, LAC/USCMedical Center, 2025 Zonal Ave., Rm. 7621, Los Angeles, CA 90033, orat [email protected].
ERIPARTUM cardiomyopathy is a rare formof heart failure of unknown cause that occursduring pregnancy or during the postpartumperiod.
1-3
Although approximately 20 percentof women with the disorder either die or survive onlybecause they receive cardiac transplants, the majorityrecover partially or completely. Although the womenwho recover may desire to become pregnant again,there is a concern that such pregnancies may be asso-ciated with an increased risk of recurrence of cardio-myopathy.
1-4
Information about the outcome of ad-ditional pregnancies, however, is limited.
4-8
There istherefore no consensus regarding recommendationsfor future pregnancies in women who have had peri-partum cardiomyopathy.
3
We undertook a study to de-termine maternal and fetal outcomes of subsequentpregnancy among women with a history of peripar-tum cardiomyopathy.
METHODS
We obtained information about subsequent pregnancies in wom-en who had had peripartum cardiomyopathy by sending a question-naire in 1997 and 1998 to all members of the American College ofCardiology in the United States (approximately 15,000 persons)and to 2 members of one cardiology group in South Africa, seek-ing information about women with peripartum cardiomyopathywho had subsequent pregnancies. The physicians who respondedwere asked to obtain from their patients written informed consentto participate in the study and to release their medical records tothe investigators. Data were then collected by the investigatorsthrough the review of medical records and supplemented, if nec-essary, by information elicited in telephone interviews of the refer-ring physicians or the patients. The study protocol and the con-sent form were approved by the institutional review board of theUniversity of Southern California.
P
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on April 11, 2015. For personal use only. No other uses without permission.
Copyright © 2001 Massachusetts Medical Society. All rights reserved.

THE OUTCOMES OF SUBSEQUENT PREGNANCIES IN WOMEN WITH PERIPARTUM CARDIOMYOPATHY
N Engl J Med, Vol. 344, No. 21
·
May 24, 2001
·
www.nejm.org
·
1569
Fetal Outcome
Among the 35 women who had a subsequent preg-nancy and did not have an abortion, 21 had a normalvaginal delivery, and 14 delivered by cesarean section.Premature delivery (defined as delivery at less than 37weeks’ gestation) occurred in three women (13 per-cent of the subgroup) in group 1 (at 30, 32, and 36weeks) and in six women (50 percent of the subgroup)in group 2 (two women at 30 weeks, one at 34 weeks,one at 35 weeks, and two at 36 weeks). There was noperinatal mortality. Of the nine abortions, five weretherapeutic; one of these occurred in group 1 (4 per-cent of the first subsequent pregnancies) and the oth-er four in group 2 (25 percent of the first subsequentpregnancies).
Additional Pregnancies
Eleven of the women had 16 additional pregnan-cies. Of the women in group 1, five women had oneadditional pregnancy each and four women had twoadditional pregnancies each; of those in group 2, one
Figure 1.
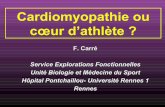
Mean (±SD) Left Ventricular Ejection Fraction in 44 Women at the Time of the Diagnosis of Peripartum Cardiomyopathy(Index Pregnancy), at Postpartum Follow-up, during the First Subsequent Pregnancy, and at the Last Follow-up a Mean of 72Months after the First Subsequent Pregnancy.Group 1 included all the women with a left ventricular ejection fraction of 50 percent or higher before subsequent pregnancies, andgroup 2 included all those with a left ventricular ejection fraction of less than 50 percent before subsequent pregnancies. For thetotal cohort (all women), P<0.001 for the comparison between postpartum follow-up and the index pregnancy, P<0.001 for thecomparison between subsequent pregnancy and postpartum follow up, and P=0.06 for the comparison between last follow-up andsubsequent pregnancy. For group 1, P<0.001 for the comparison between postpartum follow-up and the index pregnancy, P=0.002for the comparison between subsequent pregnancy and postpartum follow-up, and P=0.06 for the comparison between last follow-up and subsequent pregnancy. For group 2, P=0.05 for the comparison between postpartum follow-up and the index pregnancyand P=0.08 for the comparison between subsequent pregnancy and postpartum follow-up.
0
60
32±11
All women!Group 1!Group 2
34±11
28±12
49±12
56±7
36±9
42±13
49±10
32±11
45±13
52±9
36±13
50
40
30
20
10
IndexŁPregnancy
PostpartumŁFollow-up
SubsequentŁPregnancy
LastŁFollow-up
Perc
enta
ge o
f Wom
en
*Group 1 consisted of women with recovered left ventricular function,defined as a left ventricular ejection fraction (LVEF) of 50 percent or high-er, before the subsequent pregnancy; group 2 consisted of women withpersistent left ventricular dysfunction (an LVEF of less than 50 percent).
†P=0.06 for the comparison with group 1.‡P=0.05 for the comparison with group 1.
T
ABLE
1.
I
NCIDENCE
OF
M
ATERNAL
C
OMPLICATIONS
DURING
THE
F
IRST
S
UBSEQUENT
P
REGNANCY
IN
W
OMEN
W
HO
H
AD
H
AD
P
ERIPARTUM
C
ARDIOMYOPATHY
.*
G
ROUP
N
O
.
OF
W
OMEN
S
YMPTOMSOF
H
EART
F
AILURE
>20% D
ECREASEIN
LVEF
D
ECREASED
LVEF
AT
F
OLLOW
-
UP
D
EATH
no. of women (%)
All women 44Group 1 28 6 (21) 6 (21) 4 (14) 0 Group 2 16 7 (44) 4 (25) 5 (31) 3 (19)†
Women who did not have abortions
35
Group 1 23 6 (26) 4 (17) 2 (9) 0 Group 2 12 6 (50) 4 (33) 5 (42) 3 (25)‡
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on April 11, 2015. For personal use only. No other uses without permission.
Copyright © 2001 Massachusetts Medical Society. All rights reserved.

THE OUTCOMES OF SUBSEQUENT PREGNANCIES IN WOMEN WITH PERIPARTUM CARDIOMYOPATHY
N Engl J Med, Vol. 344, No. 21
·
May 24, 2001
·
www.nejm.org
·
1569
Fetal Outcome
Among the 35 women who had a subsequent preg-nancy and did not have an abortion, 21 had a normalvaginal delivery, and 14 delivered by cesarean section.Premature delivery (defined as delivery at less than 37weeks’ gestation) occurred in three women (13 per-cent of the subgroup) in group 1 (at 30, 32, and 36weeks) and in six women (50 percent of the subgroup)in group 2 (two women at 30 weeks, one at 34 weeks,one at 35 weeks, and two at 36 weeks). There was noperinatal mortality. Of the nine abortions, five weretherapeutic; one of these occurred in group 1 (4 per-cent of the first subsequent pregnancies) and the oth-er four in group 2 (25 percent of the first subsequentpregnancies).
Additional Pregnancies
Eleven of the women had 16 additional pregnan-cies. Of the women in group 1, five women had oneadditional pregnancy each and four women had twoadditional pregnancies each; of those in group 2, one
Figure 1.
Mean (±SD) Left Ventricular Ejection Fraction in 44 Women at the Time of the Diagnosis of Peripartum Cardiomyopathy(Index Pregnancy), at Postpartum Follow-up, during the First Subsequent Pregnancy, and at the Last Follow-up a Mean of 72Months after the First Subsequent Pregnancy.Group 1 included all the women with a left ventricular ejection fraction of 50 percent or higher before subsequent pregnancies, andgroup 2 included all those with a left ventricular ejection fraction of less than 50 percent before subsequent pregnancies. For thetotal cohort (all women), P<0.001 for the comparison between postpartum follow-up and the index pregnancy, P<0.001 for thecomparison between subsequent pregnancy and postpartum follow up, and P=0.06 for the comparison between last follow-up andsubsequent pregnancy. For group 1, P<0.001 for the comparison between postpartum follow-up and the index pregnancy, P=0.002for the comparison between subsequent pregnancy and postpartum follow-up, and P=0.06 for the comparison between last follow-up and subsequent pregnancy. For group 2, P=0.05 for the comparison between postpartum follow-up and the index pregnancyand P=0.08 for the comparison between subsequent pregnancy and postpartum follow-up.
0
60
32±11
All women!Group 1!Group 2
34±11
28±12
49±12
56±7
36±9
42±13
49±10
32±11
45±13
52±9
36±13
50
40
30
20
10
IndexŁPregnancy
PostpartumŁFollow-up
SubsequentŁPregnancy
LastŁFollow-up
Perc
enta
ge o
f Wom
en
*Group 1 consisted of women with recovered left ventricular function,defined as a left ventricular ejection fraction (LVEF) of 50 percent or high-er, before the subsequent pregnancy; group 2 consisted of women withpersistent left ventricular dysfunction (an LVEF of less than 50 percent).
†P=0.06 for the comparison with group 1.‡P=0.05 for the comparison with group 1.
T
ABLE
1.
I
NCIDENCE
OF
M
ATERNAL
C
OMPLICATIONS
DURING
THE
F
IRST
S
UBSEQUENT
P
REGNANCY
IN
W
OMEN
W
HO
H
AD
H
AD
P
ERIPARTUM
C
ARDIOMYOPATHY
.*
G
ROUP
N
O
.
OF
W
OMEN
S
YMPTOMSOF
H
EART
F
AILURE
>20% D
ECREASEIN
LVEF
D
ECREASED
LVEF
AT
F
OLLOW
-
UP
D
EATH
no. of women (%)
All women 44Group 1 28 6 (21) 6 (21) 4 (14) 0 Group 2 16 7 (44) 4 (25) 5 (31) 3 (19)†
Women who did not have abortions
35
Group 1 23 6 (26) 4 (17) 2 (9) 0 Group 2 12 6 (50) 4 (33) 5 (42) 3 (25)‡
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on April 11, 2015. For personal use only. No other uses without permission.
Copyright © 2001 Massachusetts Medical Society. All rights reserved.

Journal of Anaesthesiology Clinical Pharmacology | July-September 2014 | Vol 30 | Issue 3 427
Peripartum cardiomyopathy is a relatively rare but life threatening disease. The etiology and pathogenesis of peripartum cardiomyopathy is generally centered upon viral and autoimmune mechanism. This case report describes the anesthetic management of a patient with term pregnancy suffering from dilated peripartum cardiomyopathy planned for cesarean section , successfully managed with epidural anesthesia after precipitate labour.
Key words: Epidural anesthesia, peripartum dilated cardiomyopathy, precipitate labor
Importance of transesophageal echocardiography in peripartum cardiomyopathy undergoing lower section cesarean section under regional anesthesia
Poonam Malhotra Kapoor, Sameer Goyal, Kalpana Irpachi, Barya Smita1
Department of Cardiac Anaesthesia, CTC, AIIMS, 1Department of Obstetrics and Gynaecology, Pt. Madam Mohan Malviya Hospital, New Delhi, India
Introduction
Peripartum cardiomyopathy (PPC) is a relatively rare form of acute heart failure (HF) associated with pregnancy. The diagnosis presents a challenge as many full term parturients experience dyspnea, fatigue, and peripheral edema. Pearson et al.[1] published data on 27 patients with pregnancy-associated cardiomyopathy who presented in the peripartum period. These investigators coined the term “PPC” and defined diagnostic criteria on the basis of their patient’s characteristics and available diagnostic tools at the time. These criteria included:1. The development of HF in the last month of pregnancy
or within 5 months of delivery;2. The absence of a determinable etiology for HF; and3. The absence of demonstrable heart disease before the last
month of pregnancy.
A workshop organized by the National Heart, Lung, and Blood Institute and the Office of Rare Diseases Research in 1997 added an additional criterion proposed by Hibbard et al.[2] of left ventricular (LV) systolic dysfunction demonstrated by echocardiography with LV ejection fraction (LVEF) 45%, fractional shortening 30%, or both.
As there is paucity in literature to emphasize, the role of transesophageal echocardiography (TEE) being a mandatory diagnostic tool in such cases under regional anesthesia, we report a case of PPC in which TEE was used judiciously to optimize the fetal and maternal outcome.
Case Report
A 22-year-old woman, presented as gravida 1, para 0, at 37 weeks of gestation, with pregnancy induced hypertension and symptoms of cardiac failure. At 36th week of pregnancy, the patient had developed shortness of breath on mild exertion, chest pain and cough with mucoid sputum and pedal edema. At the time of admission, her heart rate was 112/min and blood pressure was 160/100 mmHg in right upper limb supine position. On auscultation of chest, there were bilateral coarse crackles along with a systolic murmur heard over mitral area. Her hemoglobin was 8.9 g/dl, with a normal blood profile. A transthoracic echocardiography revealed generalized hypokinesia, increased LV dimensions, moderate mitral regurgitation and mild tricuspid regurgitation, with an ejection fraction (EF) of 35%. A cardiologist opinion was sought, which led to the diagnosis of peripartum dilated
Case ReportCase Report
Abstract
Address for correspondence: Dr. Poonam Malhotra Kapoor,Cardiac Anaesthesia, Room No-8, 7th Floor, CNC, AIIMS, New Delhi - 110 029, India. Email - [email protected]
Access this article onlineQuick Response Code:
Website:www.joacp.org
DOI: 10.4103/0970-9185.137287
>'RZQORDGHG�IUHH�IURP�KWWS���ZZZ�MRDFS�RUJ�RQ�0RQGD\��0DUFK�����������,3���������������@��__��&OLFN�KHUH�WR�GRZQORDG�IUHH�$QGURLG�DSSOLFDWLRQ�IRU�WKLV�MRXUQDO
Journal of Anaesthesiology Clinical Pharmacology | July-‐September 2014
Letters to the Editor
Journal of Anaesthesiology Clinical Pharmacology | October-December 2011 | Vol 27 | Issue 4 567
Low dose spinalanesthesia for peripartum cardiomyopathy
Sir, Peripartum cardiomyopathy [1] is a dilated cardiomyopathy associated with cardiac failure in the last month of pregnancy or within five months of delivery. There is no identifiable cause of cardiac failure, no heart disease prior to the last month of pregnancy, and left ventricular systolic dysfunction. It has
which were not there and then slightly pulled the catheter which also didn’t help. Finally thinking that there is a blood clot at the tip or some other sort of blockade we pulled out the catheter, but to our surprise, it was clear. We rechecked the catheter and found that the catheter tip connecter (click and ready type) [Figure 1] once placed and clicked for fixing, occluded the lumen and if loosely fixed the drug spilled by its sides. We then attached another connector over the same catheter which functioned well after clicking.
Failure to inject drugs through malfunctioning epidural catheter has been reported,[1,2] but blockade caused by malfunctioning click and ready connector has not been reported in literature. The connector (click and ready) has two parts. One is the base (Lemon yellow) through which the catheter passes and the other is the flap (Transparent) on top which on closure clicks and holds the catheter in place. The click and ready apparatus is an easy and convenient way of fixing the epidural catheter to the syringe prior to the filter and known to have increased grip strength and providing
Figure 1: Complete epidural set with polyamide catheter, click and ready connector and filter (0.2�m)
Figure 2: Click ready connector showing the arch in the midline on the undersurface of the transparent flap
more secure catheter connection. The transparent upper flap also has a small arch of around 1mm on the midline inner surface which actually holds the catheter at the site [Figure 2]. The arch of the catheter was the site of malfunction in our case as we checked 10 more catheter connectors of the same type and company. The arch was slightly larger in our case and hence was completely occluding the catheter lumen.
Before taking out the catheter, one should check the connector in click and ready technique for any manufacturing defects. Only changing the connector (from another sterile set) might overcome the problem and will not deprive the patient of postoperative analgesia. Pre-insertion check of the complete set needs to be emphasized.
Devalina Goswami, Aruna Jain, Homay VajifdarDepartment of Anaesthesiology, Lady Hardinge
Medical College, New Delhi, India
Address for correspondence: Dr. Devalina Goswami, Type V, Block 3, Quarter No 17, Lodhi Road Complex Govt Quarters, New Delhi-110
003, India. E-mail: [email protected]
References
1. Gupta S, Singh B, Kachru N. "Blocked" epidural catheter: Another cause. Anesth Analg 2001;92:1617-8.
2. Arnaoutoglou HM, Tzimas PG, Papadopoulos GS. Knotting of an epidural catheter: A rare complication. Acta Anaesthesiol Belg 2007;58:55-7.
Access this article onlineQuick Response Code:
Website:www.joacp.org
DOI: 10.4103/0970-9185.86614
>'RZQORDGHG�IUHH�IURP�KWWS���ZZZ�MRDFS�RUJ�RQ�0RQGD\��0DUFK�����������,3���������������@��__��&OLFN�KHUH�WR�GRZQORDG�IUHH�$QGURLG�DSSOLFDWLRQ�IRU�WKLV�MRXUQDO
Journal of Anaesthesiology Clinical Pharmacology | October-‐December 2011 | Vol 27 | Issue 4

Peripartum CardiomyopathyPredictors of Recovery and Current State ofImplantable Cardioverter-Defibrillator Use
Jayasree Pillarisetti, MD, MSC,* Ashok Kondur, MD,y Anas Alani, MD,yMadhu Reddy, MD,* Madhuri Reddy, MD,z James Vacek, MD, MSC,* Carl P. Weiner, MD,zEdward Ellerbeck, MD, MPH,x Theodore Schreiber, MD,y Dhanunjaya Lakkireddy, MD*
Kansas City, Kansas; and Detroit, Michigan
Objectives The purpose of this study was to identify the predictors of left ventricular (LV) recovery in patients with peripartumcardiomyopathy (PPCM) and to record rates of implantable cardioverter-defibrillator (ICD) use.
Background PPCM is a rare, life-threatening disease. The use of ICDs has not been clearly understood in this patient group.Identification of the predictors of persistent LV dysfunction can help select patients at risk for sudden cardiac death.
Methods A retrospective study was conducted at 2 academic centers between January 1, 1999, and December 31, 2012.Clinical and demographic variables and delivery records of patients with a diagnosis of PPCM (InternationalClassification of Diseases, 9th Revision code 674.5) were reviewed. Improvement in LV function was noted fromechocardiography reports.
Results The total sample comprised 100 patients, of whom 55% were African Americans, 39% were Caucasians, and6% were Hispanic, with a mean age of 30 ! 6 years. Mean left ventricular ejection fraction (LVEF) at diagnosis was28 ! 9%. Forty-two percent of patients showed improvement in LVEF over a mean duration of 33 ! 21 months.Postpartum diagnosis (hazard ratio: 3.0; p ¼ 0.01) and Caucasian/Hispanic race (hazard ratio: 2.2; p ¼ 0.01) werepredictors of improvement in LVEF. Only 7 of the 58 patients (12%) who did not have improvement in their LVEF hadan ICD implanted. There were 11 deaths, with a trend toward higher mortality in those who did not display improvedLV function (15% vs. 5%; p ¼ 0.1).
Conclusions More than one-third of women with PPCM improve LV function with delayed recovery noted in the majority of thesepatients. Caucasians and those diagnosed in the postpartum period appear to be the most likely to recover. The rateof ICD implantation for primary prevention of sudden cardiac death in this patient group is low. (J Am Coll Cardiol2014;63:2831–9) ª 2014 by the American College of Cardiology Foundation
Peripartum cardiomyopathy (PPCM) is a rare, idiopathiccardiomyopathy characterized by the development of systolicheart failure toward the end of pregnancy or in the monthsafter delivery (1,2). The reported incidence shows signifi-cant geodemographic variation, from 1 in 500 live birthsin Haiti to 1 in 4000 live births in the United States (3–6).Identified risk factors for PPCM include multiparity, advanced
maternal age, twins, preeclampsia, gestational hypertension,and African-American race (1,2,7–9).
Despite the recognition of this disease as a separate entity in1937, the mortality rates are not yet well characterized (8–19),ranging from 4% to 50% (2,8–19). At least one-fourth ofdeaths in PPCM are sudden cardiac deaths presumed to becaused by ventricular tachyarrhythmias (16). Sudden cardiacdeath in these young women could potentially be averted byinsertion of an implantable cardioverter-defibrillator (ICD),and cardiac resynchronization therapy devices (CRTDs) mayreduce progression to end-stage myocardial dysfunction. TheAmerican College of Cardiology Foundation/AmericanHeart Association 2009 guidelines recommend implantationof an ICD for primary prevention of sudden cardiac death inall patients with ischemic and nonischemic cardiomyopathywith ejection fraction (EF) #35% in patients with New YorkHeart Association (NYHA) functional class II and III andEF <30% in patients with NYHA class I if there is noimprovement in EF after 3 to 6 months of guideline-directed
From the *Division of Cardiovascular Diseases, Cardiovascular Research Institute,Mid America Cardiology, University of Kansas Hospital and Medical Center, KansasCity, Kansas; yDetroit Medical Center, Wayne State University, Detroit, Michigan;zDepartment of Obstetrics & Gynecology, University of Kansas Hospital and MedicalCenter, Kansas City, Kansas; and the xDepartment of Epidemiology, University ofKansas Hospital and Medical Center, Kansas City, Kansas. Dr. Lakkireddy hasreceived speaker honoraria from St. Jude Medical, Inc., Janssen Pharmaceuticals, Inc.,Pfizer Inc., and SentreHEART, Inc.; and has received consulting fees from St. JudeMedical, Inc. All other authors have reported that they have no relationships relevantto the contents of this paper to disclose.Manuscript received August 5, 2013; revised manuscript received March 8, 2014,
accepted April 8, 2014.
Journal of the American College of Cardiology Vol. 63, No. 25, 2014! 2014 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2014.04.014