Cancer du pancréas opérable ou border-line - ffcd.fr SAUVANET Cancer du... · Lemaire, Br J Surg,...
41
Cancer du pancréas opérable ou border-line A Sauvanet, DHU Unity, Hôpital Beaujon, AP-HP, Université Paris VII Clichy, France
Transcript of Cancer du pancréas opérable ou border-line - ffcd.fr SAUVANET Cancer du... · Lemaire, Br J Surg,...

Cancer du pancréas opérable ou border-line
A Sauvanet,
DHU Unity, Hôpital Beaujon, AP-HP, Université Paris VII
Clichy, France

Les principes
Le bilan d’extension repose principalement sur une TDM
récente et dédiée
Ne proposer une résection que si curative (radicale, ou R0)
La chirurgie peut être « élargie » (veines , organes de
voisinage) dans le but d’obtenir une résection R0.
Un traitement d’induction est indiqué pour augmenter les
possibilités de résection R0

CT scan for pancreatic adenocarcinoma : technique Helical CT with < 2 mm thickness slices, 3 phases
« Water contrast » into the duodenum
Vascular and multiplanar reconstruction
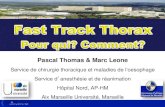
Main limit of CT-scan for staging of pancreatic
adenocarcinoma : detection of metastases
Knueurtz, J Gastrointest Surg 2011 (Baltimore)
31/280 = 11% Liver metastases :
- main cause of absence of resection
- median survival : 5 mo. vs 8 mo. if
locally advanced (p<0.001)
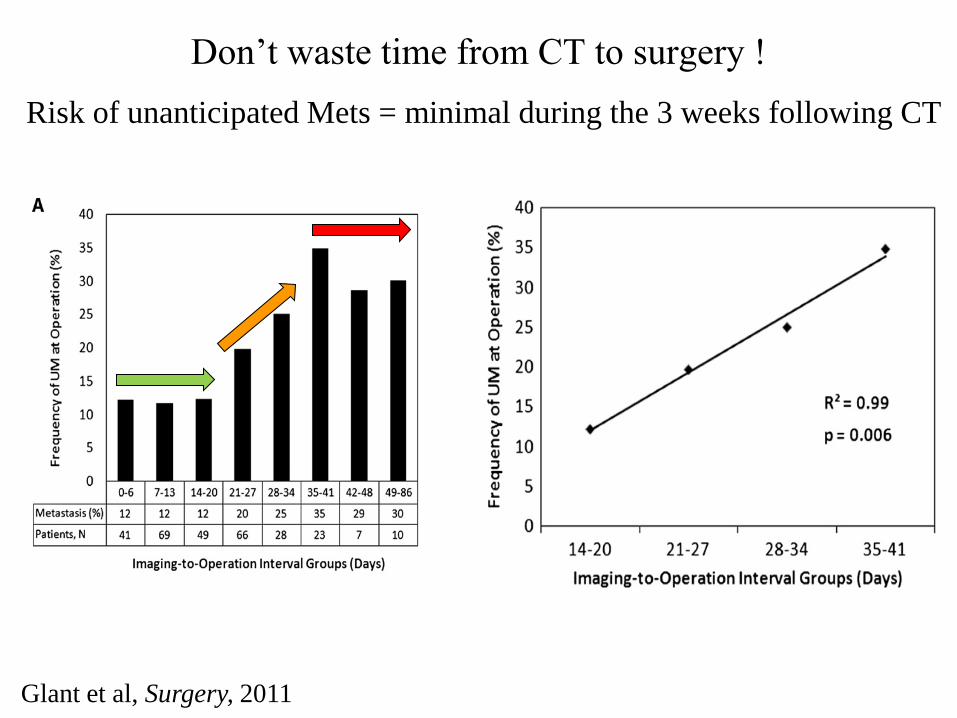
Don’t waste time from CT to surgery !
Glant et al, Surgery, 2011
Risk of unanticipated Mets = minimal during the 3 weeks following CT

Resection has no value in case of liver/peritoneal mets
Shrikhande, Ann Surg Oncol, 2006 Survey French Association Surgery 2010 JR Delpero, F Paye, P Bachellier

Shrikhande, Ann Surg Oncol, 2006 Doi, World J Surg, 2007
Nakao, World J Surg, 2006 Shimada Surgery 2006
Resection has no value if distant (para-aortic) metastatic
lymph nodes are present
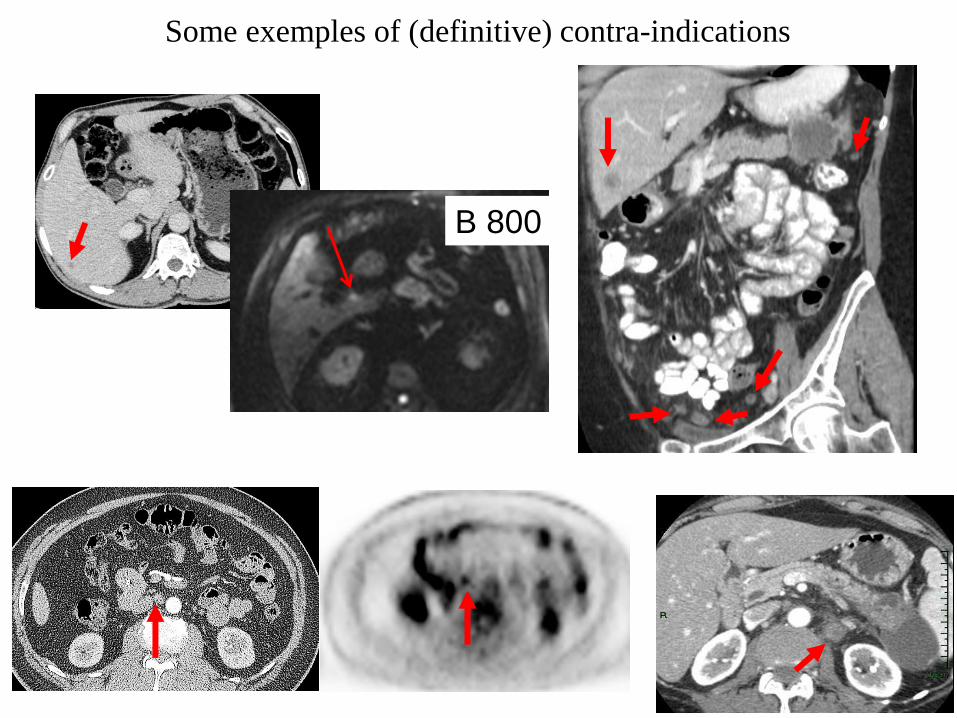
Some exemples of (definitive) contra-indications
B 800
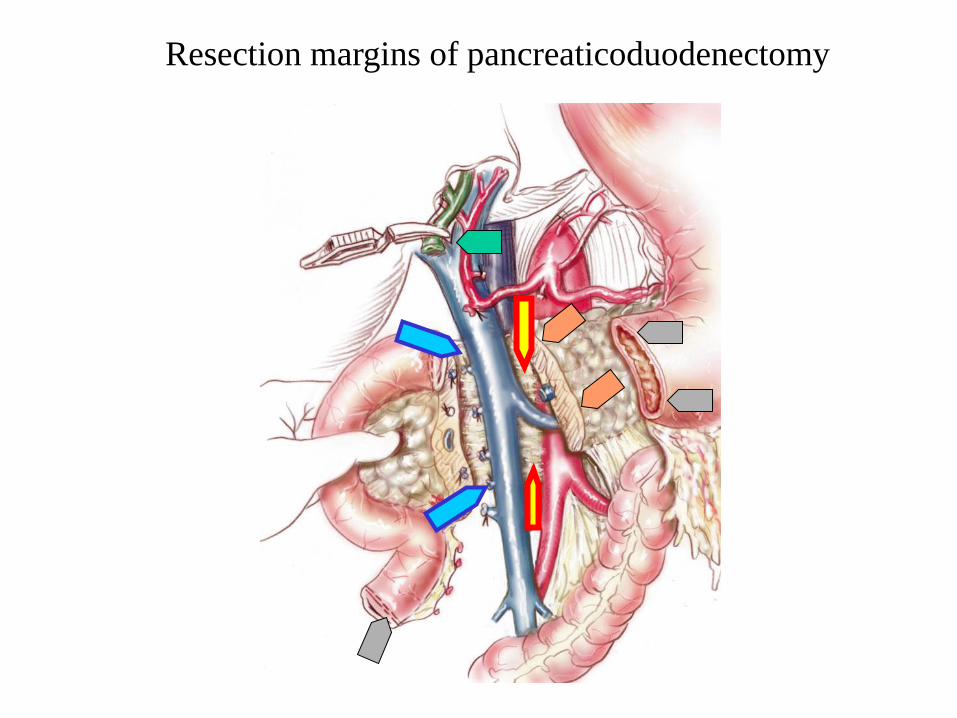
Resection margins of pancreaticoduodenectomy

« Vascular » margins are the most important
Margins DFS OS around SMA p=0.009 p=0.04 around SMV p=0.01 p=0.06 posterior p=0.517 p=0.359 pancreatic neck p=0.372 p=0.448
Pingpank, J Gastrointest Surg 2001
By courtesy of Pr JR Delpero
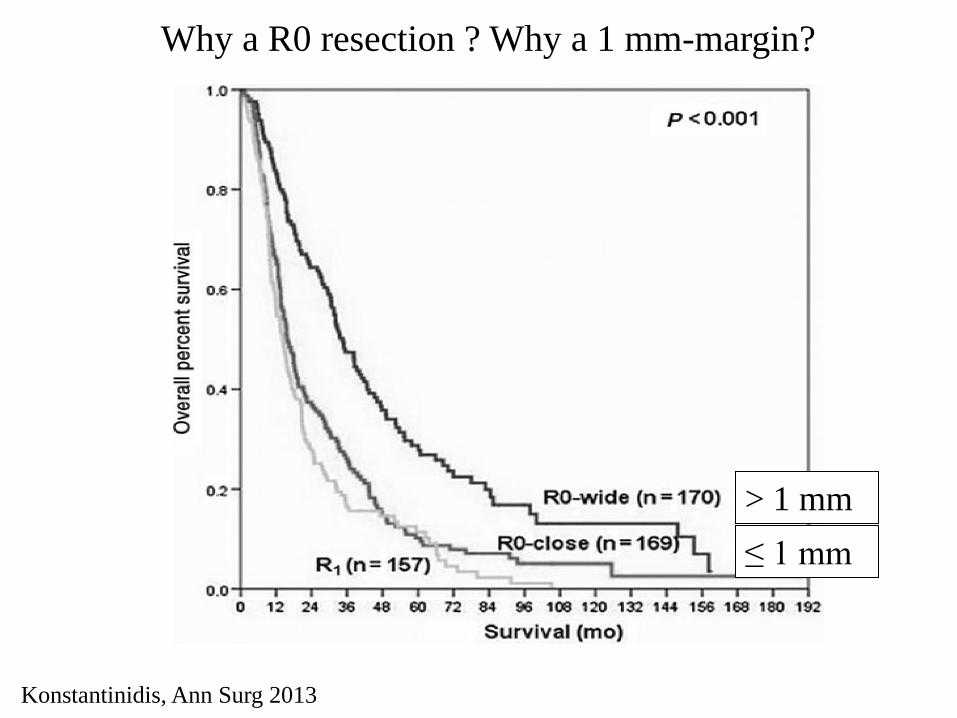
Why a R0 resection ? Why a 1 mm-margin?
> 1 mm
≤ 1 mm
Konstantinidis, Ann Surg 2013

Prediction of R0/R1 resection
• «Naive» patients : prediction of tumor infiltration of retroportal lamina
Mazzeo, Abdom Imaging, 2009
Accuracy ± 80%
Katz Gastrointest Surg 2012
CT overstimates distance between
Ca. and SMA in 73% des cas
• Limits of PDAC are difficult to delineate

No metastases No arterial invasion No SMV-PV invasion
Invasion of SMV-PV Invasion SMA < 180°
Invasion AMS > 180° Invasion of Celiac Axis Thrombosis SMV or PV Invasion IVC or Aorta
Resectable Borderline Locally advanced
Chun et al. Ann Surg Oncol 2010 Survey AFC 2010
http://www.nccn.org/
No R0 resection
R0 resection is possible
Classification of
Pancreatic ductal adenoCa.
No resection
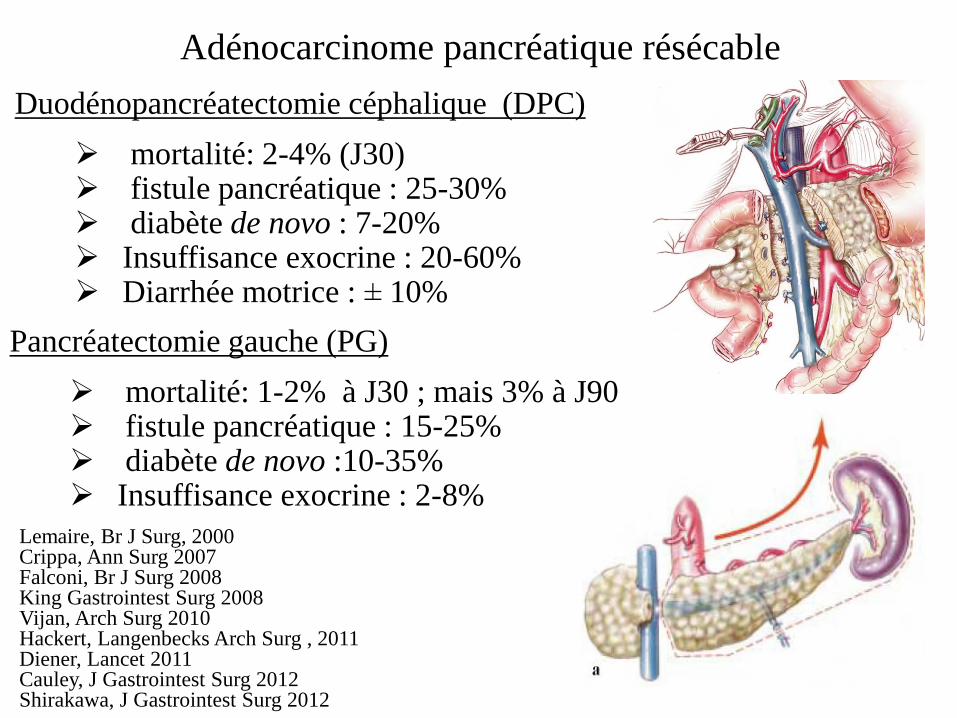
Résultats des pancréatectomies « conventionnelles » Duodénopancréatectomie céphalique (DPC)
mortalité: 2-4% (J30) fistule pancréatique : 25-30% diabète de novo : 7-20% Insuffisance exocrine : 20-60% Diarrhée motrice : ± 10%
Lemaire, Br J Surg, 2000 Crippa, Ann Surg 2007 Falconi, Br J Surg 2008 King Gastrointest Surg 2008 Vijan, Arch Surg 2010 Hackert, Langenbecks Arch Surg , 2011 Diener, Lancet 2011 Cauley, J Gastrointest Surg 2012 Shirakawa, J Gastrointest Surg 2012
Pancréatectomie gauche (PG)
mortalité: 1-2% à J30 ; mais 3% à J90 fistule pancréatique : 15-25% diabète de novo :10-35% Insuffisance exocrine : 2-8%
Adénocarcinome pancréatique résécable

Ca
Routine complete resection of the retroportal lamina
Noto, Am J Surg Pathol 2005 Perineural invasion
Resectable cephalic carcinoma : How to obtain R0 resection ?
Complete resection of the retroportal lamina

Survival after resection has improved
PD with
lymphadenectomy
« standard » PD
Ann Surg 1995 J Gastrointest Surg 2005
John Hopkins (Baltimore) : 5-year survival after pancreaticoduodenectomy
20% 29%

Survival after resection has improved
1992 2010
Two surveys of the French Association of Surgery :
5-year survival after pancreaticoduodenectomy
18% 34%
Coordinators: -1992 : M Huguier, H Baumel -2010: JR Delpero, F Paye, P Bachellier

Prognostic factors after resection are identified
Winter J Gastrointest Surg 2005
Other prognostic factors after resection
Winter J Gastrointest Surg 2005
Gouma Ann Surg 2005
Fong Ann Surg 2005
Tseng Surgery 2007
French Association of Surgery 2010
Limited blood loss / No transfusion
High-volume center
Experienced surgeon
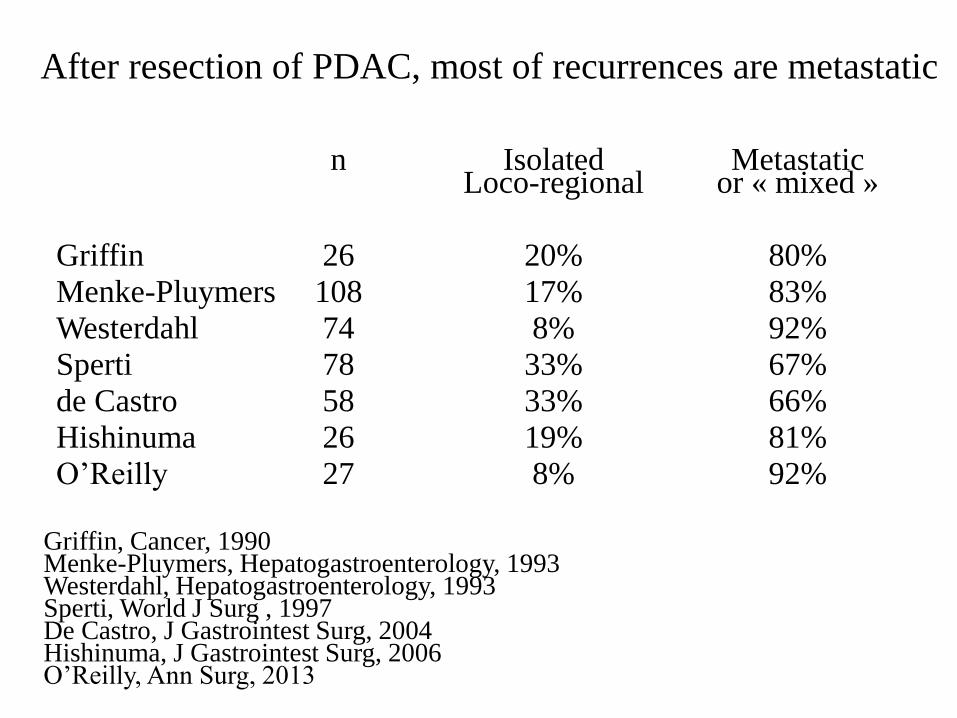
After resection of PDAC, most of recurrences are metastatic
n Isolated Metastatic Loco-regional or « mixed »
Griffin 26 20% 80%
Menke-Pluymers 108 17% 83%
Westerdahl 74 8% 92%
Sperti 78 33% 67%
de Castro 58 33% 66%
Hishinuma 26 19% 81%
O’Reilly 27 8% 92%
Griffin, Cancer, 1990 Menke-Pluymers, Hepatogastroenterology, 1993 Westerdahl, Hepatogastroenterology, 1993 Sperti, World J Surg , 1997 De Castro, J Gastrointest Surg, 2004 Hishinuma, J Gastrointest Surg, 2006 O’Reilly, Ann Surg, 2013
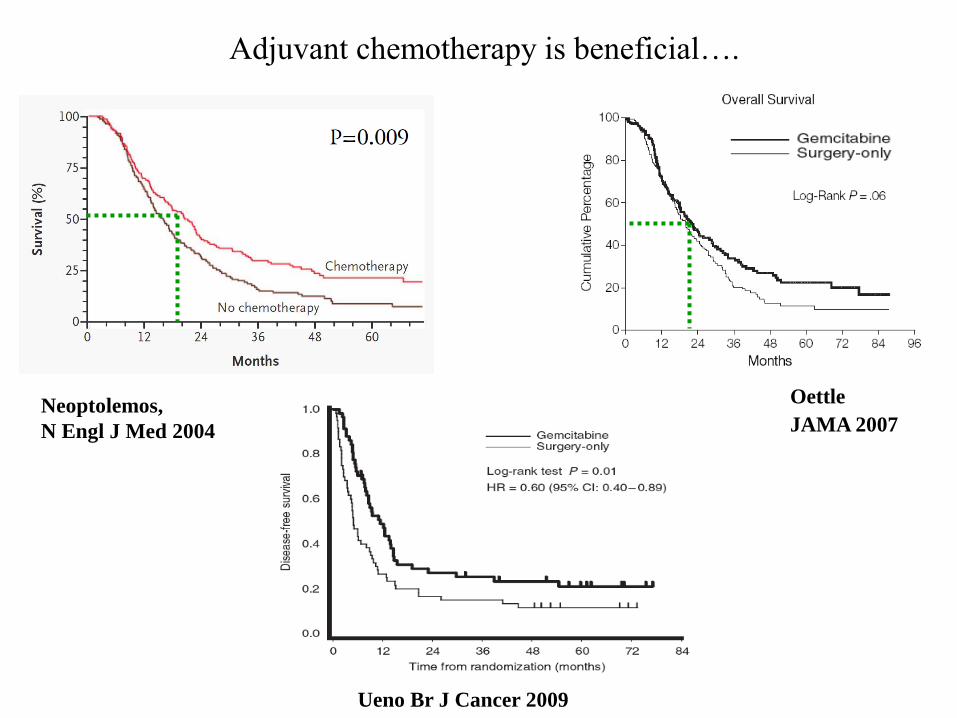
Adjuvant chemotherapy is beneficial….
Ueno Br J Cancer 2009
Neoptolemos,
N Engl J Med 2004
Oettle
JAMA 2007

…after both R0 and R1 resection
Ueno
Br J Cancer 2009
Oettle
JAMA 2007
…but only 70-80% of patients receive adjuvant treatment
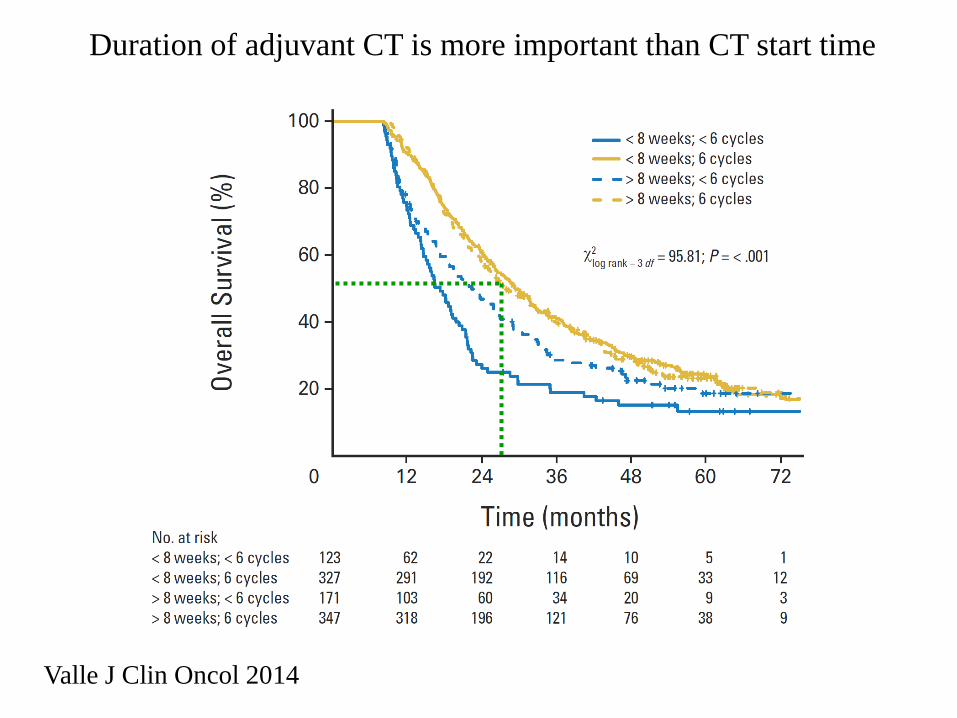
Duration of adjuvant CT is more important than CT start time
Valle J Clin Oncol 2014
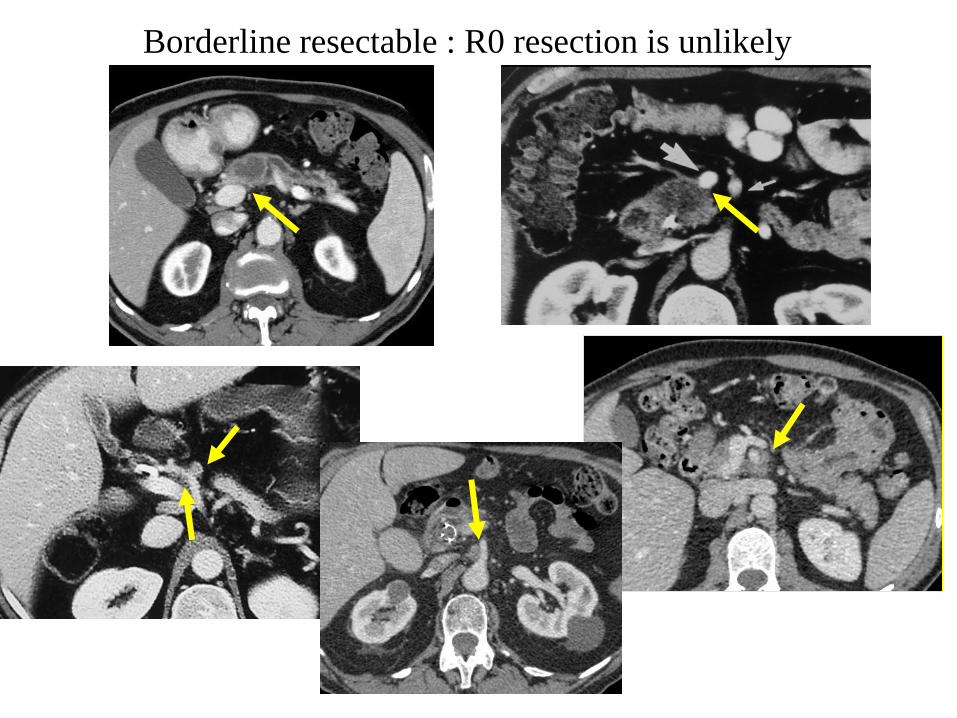
Borderline resectable : R0 resection is unlikely

Pancreatectomy with vascular resection : Indications
1) Arterial involvement : NO !!
Author year nb mortality survival (months)
Takahashi 1994 13 57% < 24 mo. Tseng-Evans 2004 17* 6% ? Allendorf 2008 11 82% ? Stitzenberg 2008 12 17% < 40 mo. Gigot 2010 11 13% < 20 mo. Delpero AFC 2010 37 8% < 30 mo Bockhorn 2010 29 14% 10% at 24 mo.. Bachellier 2011 26 8% < 36 mo.
* Hepatic artery only
2) Venous involvement in adenoCa. and PNET: OK but 2 conditions
- a R0 resection can be achieved
- operative risk is « acceptable » (mortality < 5%??)
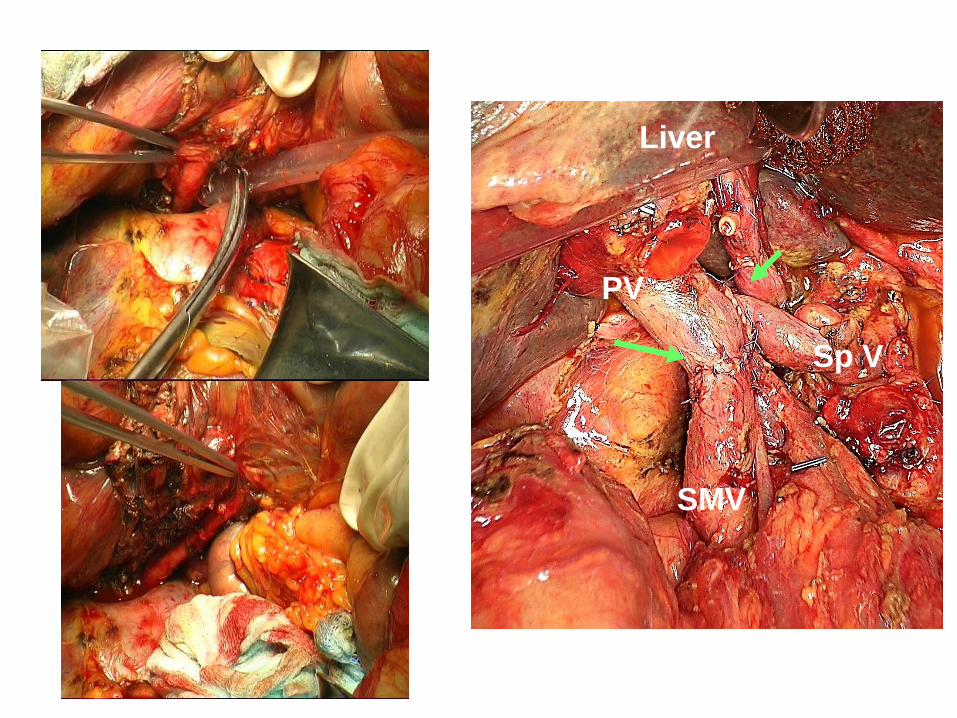
PV
SMV
Sp V
Liver
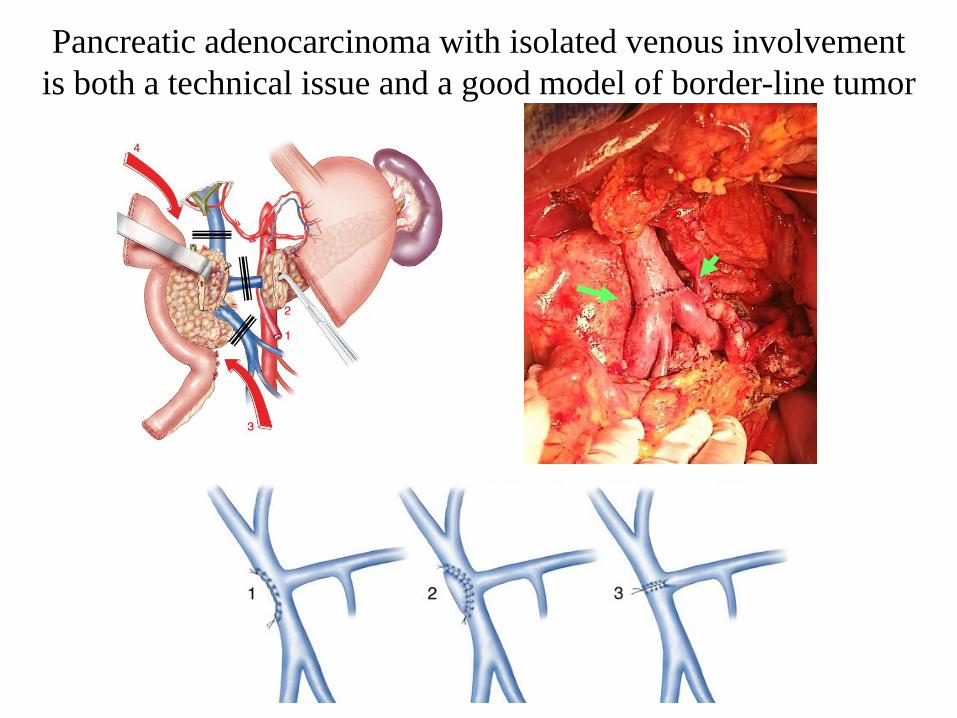
Pancreatic adenocarcinoma with isolated venous involvement
is both a technical issue and a good model of border-line tumor

Nb PD Mortality Morbidity
V- / V+ V- / V+ V- / V+
Author
Delpero 2010 (AFC) 1325 / 360 2,5% / 4,60% # 54% / 53%
Castleberry 2012 (ACS) 3301 / 281 2,9% / 5,7% # 33% / 40% #
# : p<0,05
In recent large multicentric series,
Venous resection (V+) increases morbi-mortality of PD

Venous involvement is also related with extension (including.
perineural and lymphatic involvement) into the retroportal lamina,
particularly if the left border of the venous axis is involved.
Wang, J Am Coll Surg 2013

PD with venous resection is associated with a poorer survival
particularly in case of circumferential involvement
and need for a troncular resection
Circumferential
Lateral
Absent
3 year survival p Lateral resection 46% versus Troncular resection < 2cm : 30% versus Troncular resection > 2cm 18% 0.001
Delpero JR, Association Française de Chirurgie 2010
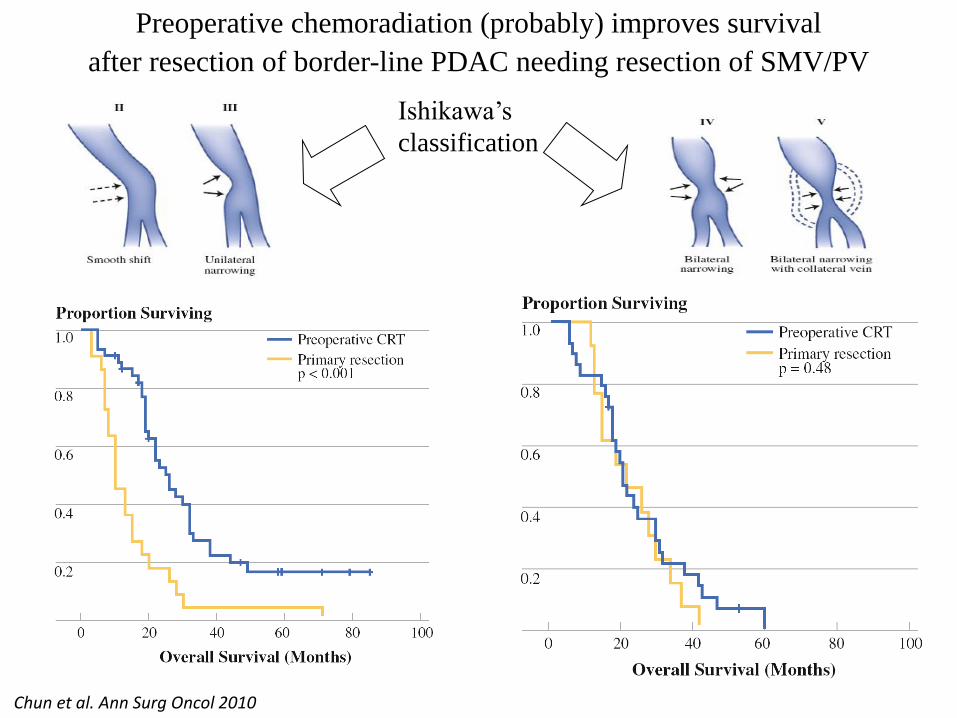
Preoperative chemoradiation (probably) improves survival
after resection of border-line PDAC needing resection of SMV/PV
Chun et al. Ann Surg Oncol 2010
Ishikawa’s
classification

Resectability for BL / LA after induction CT/CRT
1 Sa Cunha et al. J Am Coll Surg 2005
2 White R et al. Ann Surg Oncol 1999
3 Bettini N et al. Gastroenterol Clin Biol 2005
4 Morgan DE, et al. AJR 2010
5 Katz et al. Cancer 2012
6 Cassinotto et al. Eur J Radiol 2012
7 Dudeja, HPB (Oxford) 2013
• After CRT, CT and EUS do not evaluate accurately
resectability. 1-7
• Different for BL and LA
Resection rate
Borderline Locally advanced
Turrini et al. EJSO 2009 16% 7%
Katz et al. JACS 2008 38%
Katz et al. Cancer 2012 66%
Denost et al. HPB 2013 71% 18%
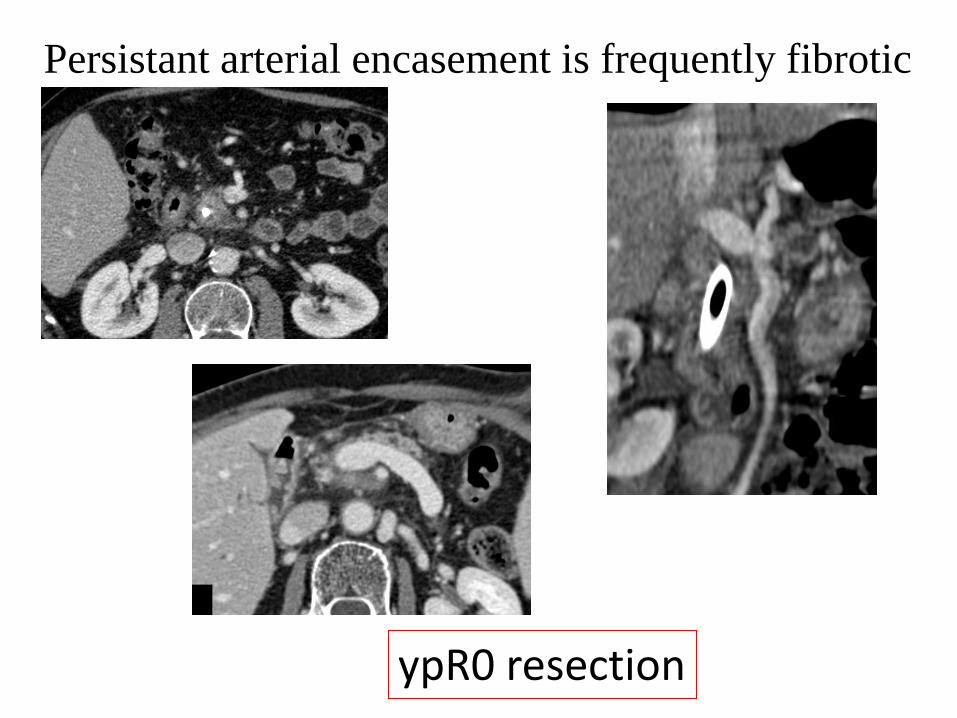
Persistant arterial encasement is frequently fibrotic
ypR0 resection

Evaluation of vascular involvement by CT
after induction treatment
Specificity False positive
Accuracy
Resectable at presentation (n=42)
88% 10% 83%
After Induction treatment (n=38)
52% 39% 58%
p 0.003 0.005 0.039
Cassinotto et al. Eur J Radiol 2012
Surgical exploration, including « artery-first » approach and
frozen section is needed

Value of induction CT/CRT
in borderline/locally advanced PDAC ?
Denot, HPB (Oxford) 2013 , retrospective study , only responders to CRT were
operated and compared with pts with initially resectable PDAC

Staging CT
Classification Borderline - LA
GEMOX ( gemcitabine –
oxaliplatine)
Surgery
CRT Capecitabine
Restaging CT
Restaging CT
Treatment phase 3 months D
éla
i 4
-6 S
em
ain
es
4 cures ( 2 months)
54 Gy (1 month)
5-6 months
Preoperative CT/CRT in borderline/locally advanced PDAC
Our experience with Gemox + CRT: 2005-2012
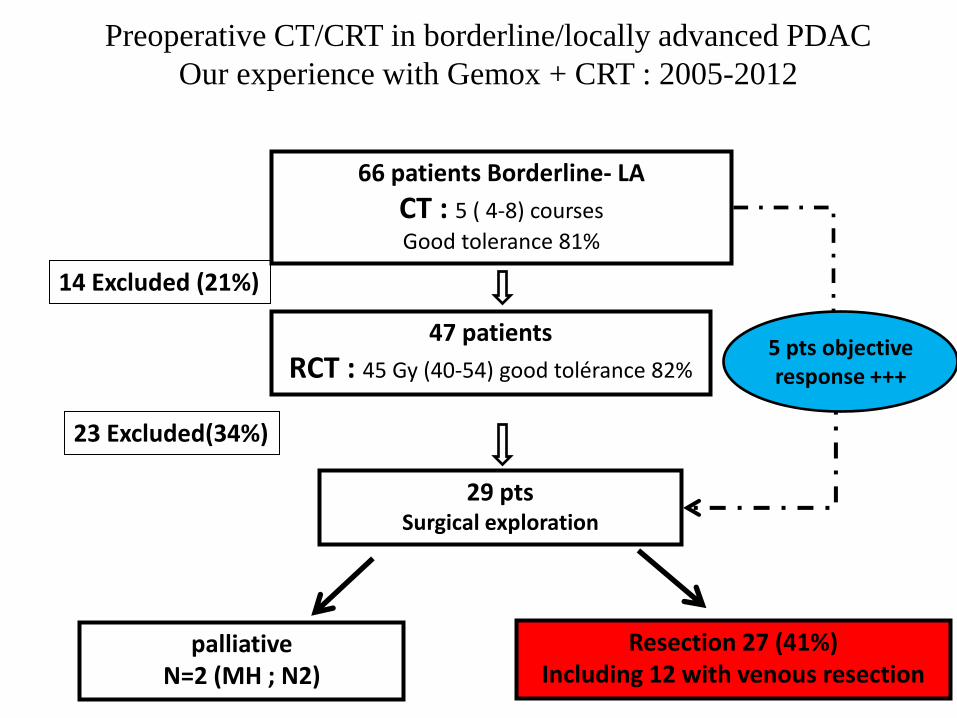
66 patients Borderline- LA
CT : 5 ( 4-8) courses
Good tolerance 81%
Resection 27 (41%) Including 12 with venous resection
29 pts Surgical exploration
47 patients
RCT : 45 Gy (40-54) good tolérance 82%
14 Excluded (21%)
23 Excluded(34%)
5 pts objective response +++
palliative N=2 (MH ; N2)
Preoperative CT/CRT in borderline/locally advanced PDAC
Our experience with Gemox + CRT : 2005-2012

Log Rank = 12.9
Overall survival (t0 = diagnosis)
in resected and non resected patients
Op. mortality = 0, N0 =54% , R0 (0 mm) =94%,
median FU = 18 [3-75] mo.
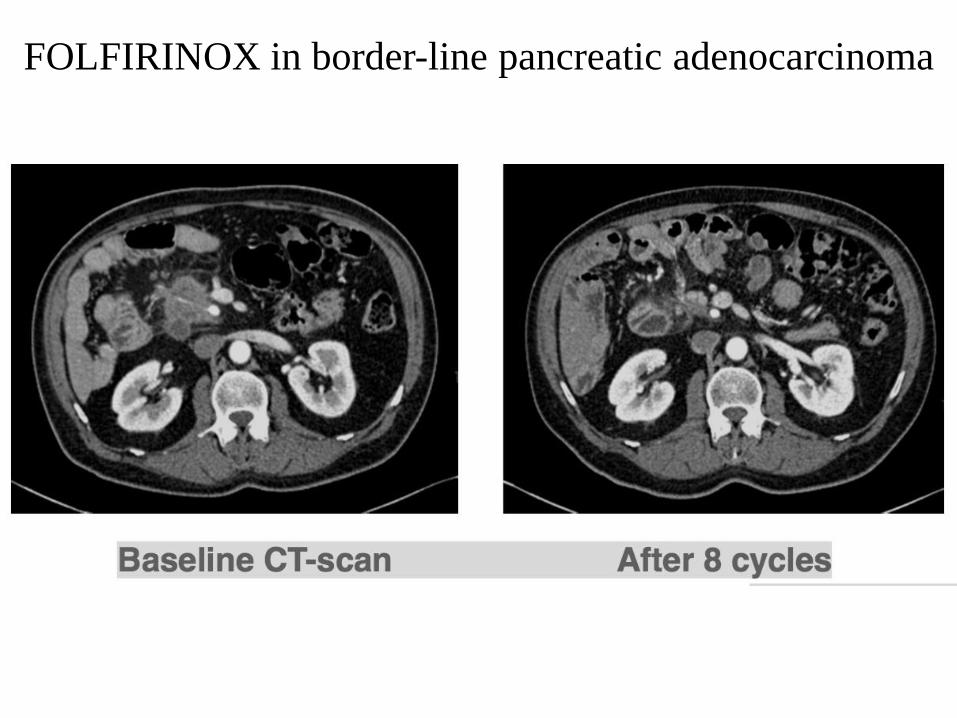
FOLFIRINOX in border-line pancreatic adenocarcinoma
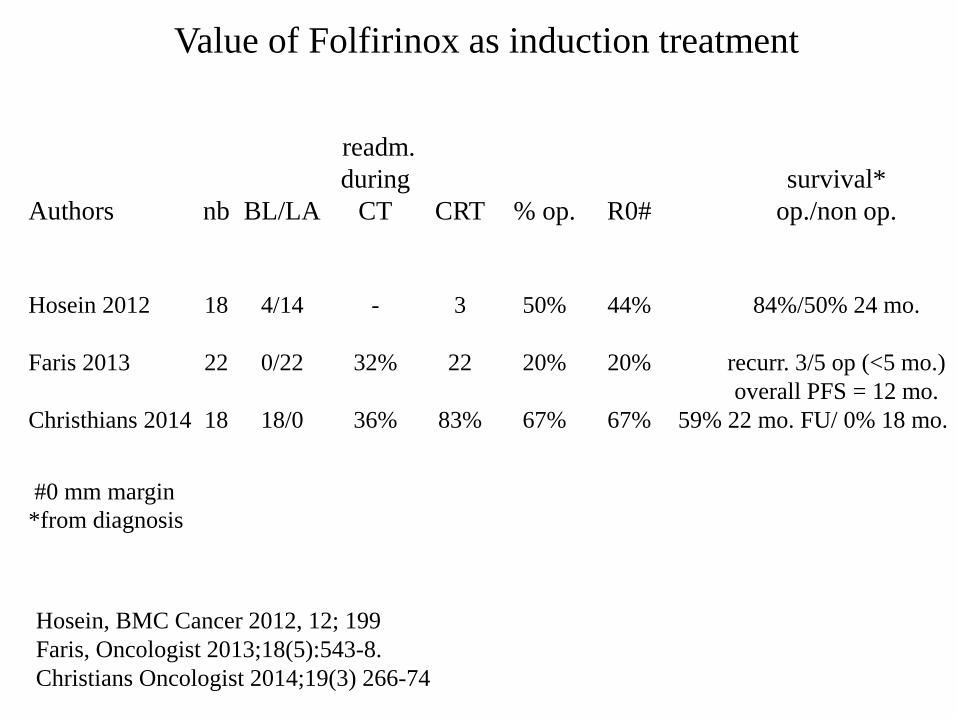
Value of Folfirinox as induction treatment
readm.
during survival*
Authors nb BL/LA CT CRT % op. R0# op./non op.
Hosein 2012 18 4/14 - 3 50% 44% 84%/50% 24 mo.
Faris 2013 22 0/22 32% 22 20% 20% recurr. 3/5 op (<5 mo.)
overall PFS = 12 mo.
Christhians 2014 18 18/0 36% 83% 67% 67% 59% 22 mo. FU/ 0% 18 mo.
#0 mm margin
*from diagnosis
Hosein, BMC Cancer 2012, 12; 199
Faris, Oncologist 2013;18(5):543-8.
Christians Oncologist 2014;19(3) 266-74
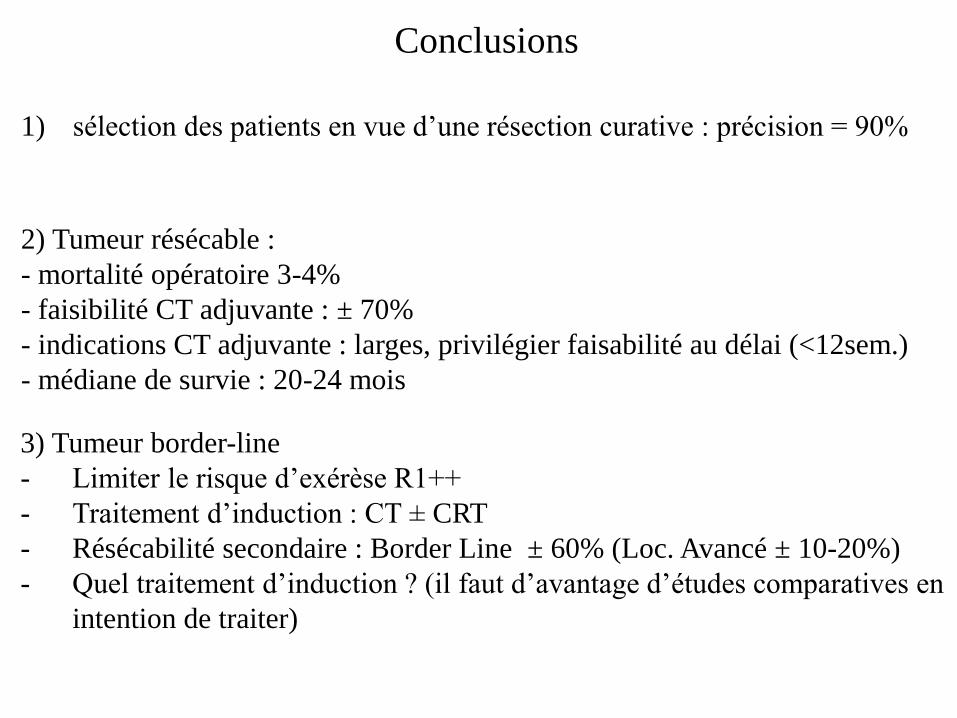
Conclusions
1) sélection des patients en vue d’une résection curative : précision = 90%
2) Tumeur résécable :
- mortalité opératoire 3-4%
- faisibilité CT adjuvante : ± 70%
- indications CT adjuvante : larges, privilégier faisabilité au délai (<12sem.)
- médiane de survie : 20-24 mois
3) Tumeur border-line
- Limiter le risque d’exérèse R1++
- Traitement d’induction : CT ± CRT
- Résécabilité secondaire : Border Line ± 60% (Loc. Avancé ± 10-20%)
- Quel traitement d’induction ? (il faut d’avantage d’études comparatives en
intention de traiter)
![Mémoire, y compris stage professionnalisant[BR ......Mémoire, y compris stage professionnalisant[BR]- Séminaires méthodologiques intégratifs[BR]- Mémoire : Estimation de la consommation](https://static.fdocuments.fr/doc/165x107/5f3ebc954f8adf284e6e5192/mmoire-y-compris-stage-professionnalisantbr-mmoire-y-compris-stage.jpg)