Autonomisation médullaire en réanimation Spasticité ... · « Spasticité maligne ......
46
Physiopathologie de la Spasticité musculaire Dr Nicolas Engrand ANARLF 21 novembre 2014
Transcript of Autonomisation médullaire en réanimation Spasticité ... · « Spasticité maligne ......

Physiopathologie de la Spasticité musculaire
Dr Nicolas Engrand
ANARLF21 novembre 2014

Pas de conflit d’intérêt


Hypertonie : augmentation du tonus musculaire
rigide spastique
composante nerveuse composante musculaire(raideur)
Rétractions musculo-tendineuses« contractures »
Spasticité : Définition
• Désordre moteur caractérisé par :
une exagération du tonus musculaire, qui est vitesse-dépendante,associé à des saccades tendineuses, résultant d’une hyperexcitabilité du réflexe d’étirement (composante
tonique)
Lance JW. Symposium synopsis ; 1980. p485-94
• S’intègre dans le syndrome pyramidal
• Pas de modèle expérimental
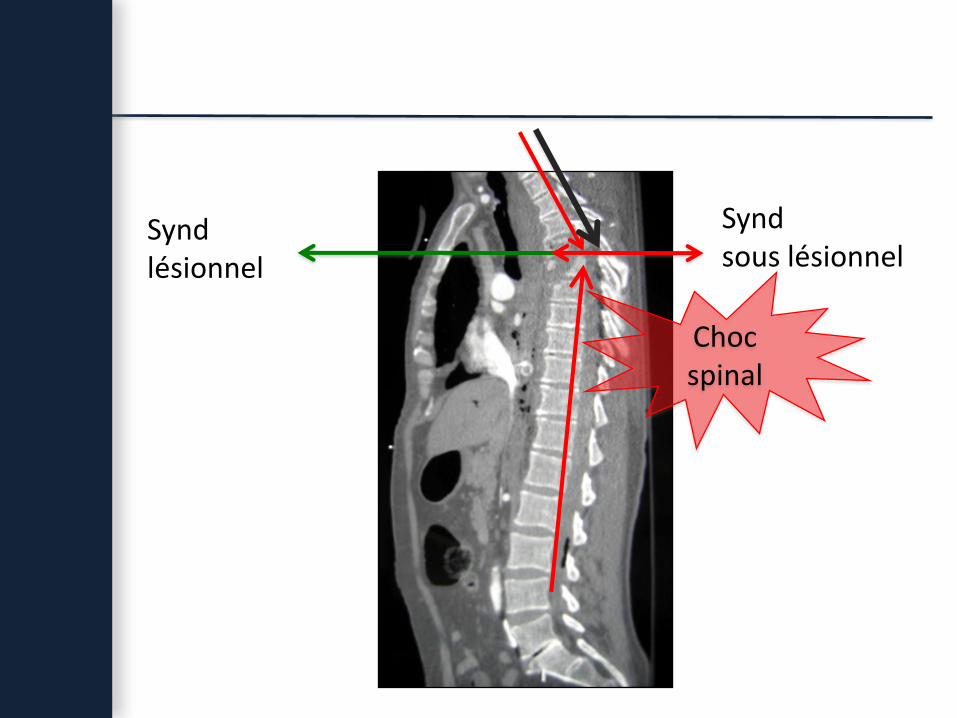
Syndlésionnel
Synd sous lésionnel
Choc spinal

phase réflexe
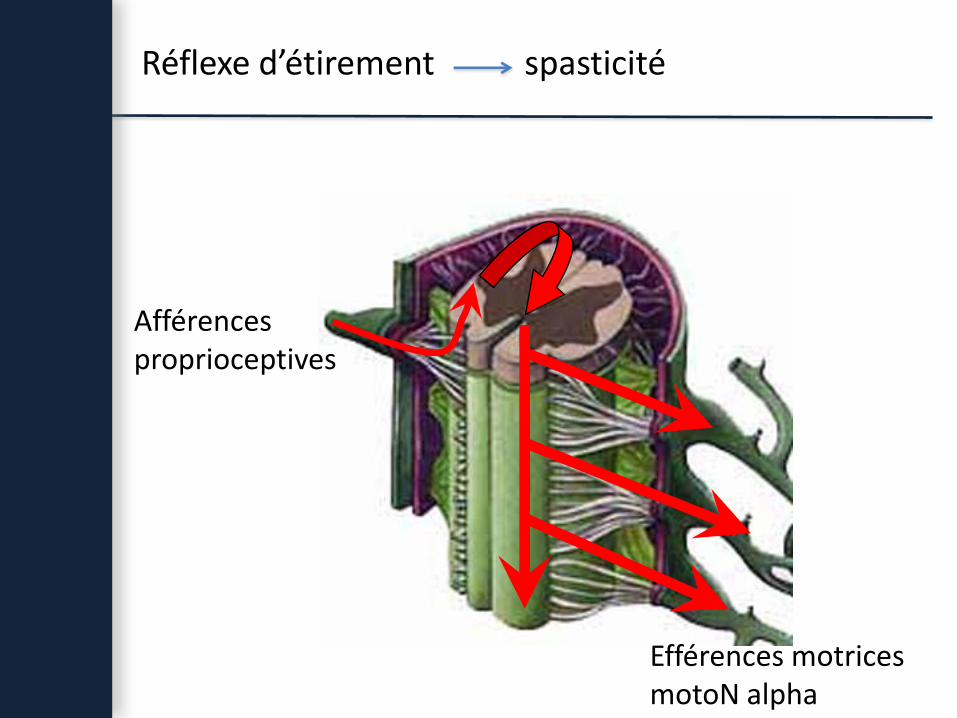
Réflexe d’étirement spasticité
Afférences proprioceptives
Efférences motricesmotoN alpha
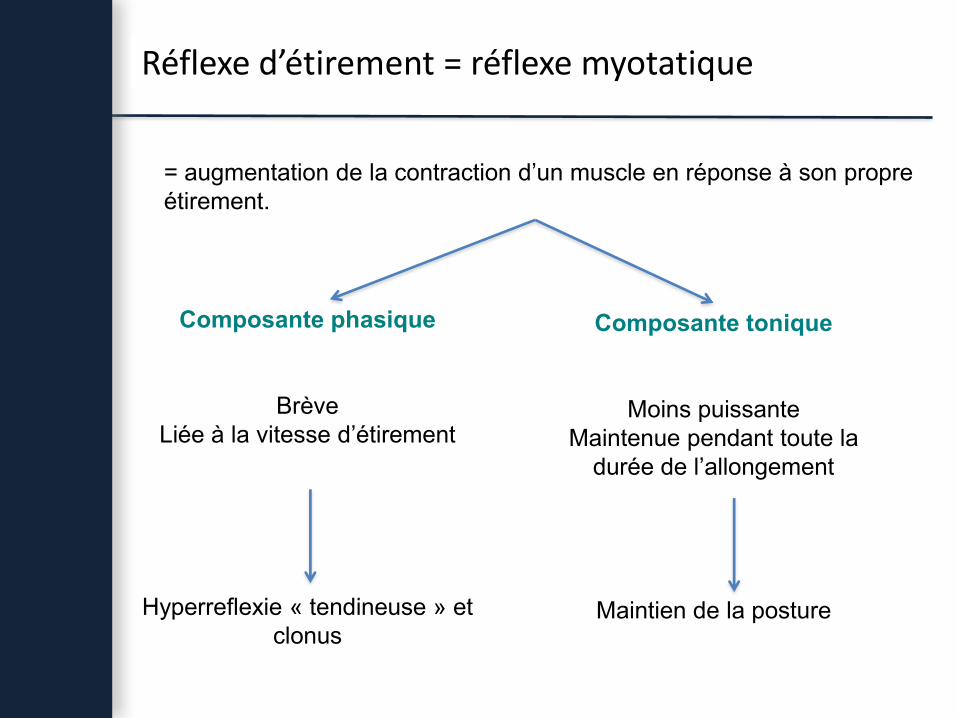
Composante phasique
BrèveLiée à la vitesse d’étirement
Hyperreflexie « tendineuse » et clonus
Composante tonique
Moins puissanteMaintenue pendant toute la
durée de l’allongement
Maintien de la posture
= augmentation de la contraction d’un muscle en réponse à son propre étirement.
Réflexe d’étirement = réflexe myotatique

afférence Ia
antagoniste
agoniste
Physiologie du réflexe d’étirement

Interneurone inhibiteur sur le motoneurone α antagoniste
Contrôle de l’activité du motoneurone alphaInhibition réciproque Ia
afférence Ia
antagoniste
agoniste
INI
Mukherjee. Frontiers in Neurol, 2010 ; 149 : 1-10

Contrôle de l’activité du motoneurone alphaInhibition récurrente (Renschaw)
afférence Ia
antagoniste
agoniste
R
Mukherjee. Frontiers in Neurol, 2010 ; 149 : 1-10

Contrôle de l’activité du motoneurone alphaInhibition autogénique Ib
fonction de protection du muscle en cas d’étirement trop intense
afférence Ib
agoniste
IN Ib
Mukherjee. Frontiers in Neurol, 2010 ; 149 : 1-10

fibre Ia
motoneurone
fibre Ia
acide aminé excitateur
GABA
Contrôle de l’activité du motoneurone alphaInhibition pré-synaptique
synapse axono-axonale
__
_
+ ++ +

Voie pyramidale : - activité volontaire- innervation réciproque
Fx : - cortico-spinaux- réticulo spinal latéral
Fx : - réticulo-spinaux- vestibulo-spinal- système monoaminergique (voie coeruleo-spinale,
noyau du raphé)
Inhibition RenshawInhibition Ib
Voies descendantes des systèmes Inhibiteurs supra-spinaux :
Voie finale commune

Renforcement des boucles réflexes spinales
Libération des voies segmentaires
Hyperexcitabilité réflexes spinaux

Inhibition présynaptique
Inhibition Ib
MS : FlexionMI : Extension
ParésieSpasticité - prononcée
Inhibition présynaptique
Inhibition récurrente
MS : FlexionMI : Flexion
Paralysie + complèteSpasticité sévèreSpasmes spontanés ou provoqués
Decq. Neurochirurgie, 2003 ; 49 :163-84Marra. Acta Neurochir Suppl, 2007 ; 97 (Pt 1) : 173-80Dietz. Handb Clin Neurol, 2012 ; 109 : 197-211

TC, HSA, HTIC (agression cérébrale moins systématisée)
- MS en F ou E- MI en F ou E- torticolis- rigidité axiale en extension
« Spasticité maligne »± troubles neurovégétatifs (« diencephalic seizure »
jeunes, anoxie, LAD, lésions diencéphale)Zafonte. J Head Trauma Rehabil. 2004 ; 19 : 89-100Cuny. Neurochirurgie, 2003 ; 49 : 289-92Becker. J Neurol Neurosurg Psychiatry. 1999 ; 66 : 114

Groupes musculaires les + fréquemment atteints
• MS : palmairesfléchisseurs doigtsbiceps brachialgrand pectoral
• MI : adducteurs de la cuissequadricepstriceps sural
• Cou : trapèzesSCM

Echelle de spasmes de Penn
0 : absence de spasme.
1 : spasmes modérés induits par des stimulations sensorielles ou la mobilisation passive.
2 : spasmes spontanés < 1 / heure.
3 : spasmes spontanés entre 1 et 10 / heure.
4 : plus de 10 spasmes / heure.
Penn. N Engl J Med. 1989 ; 320 : 1517-21
Spasmes spontanés

Rôle de la douleur
Mertens. Neurochirurgie, 2003 ; 49 : 154-62Kakinohana. Br J Anaesth. 2006 ; 96 : 88-94
Interneuroneenképhalinergique
spasticité
Afférences extrinsèques
fibres Ad et C
d
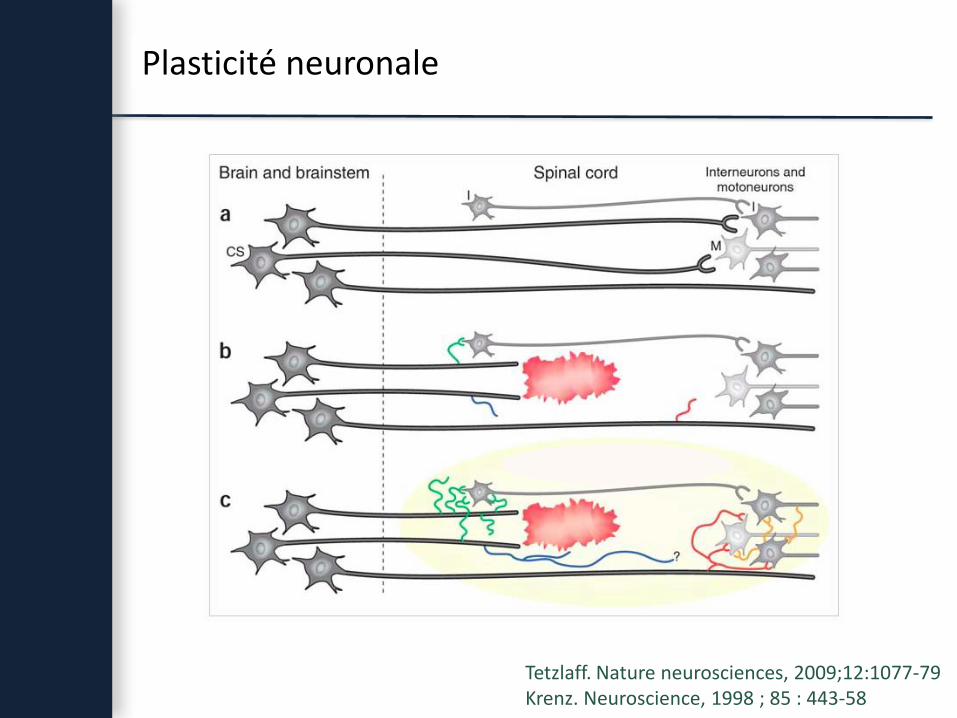
Plasticité neuronale
Tetzlaff. Nature neurosciences, 2009;12:1077-79Krenz. Neuroscience, 1998 ; 85 : 443-58

Hyperexcitabilité neuronale
Plasticité neuronale
Création de contacts par les interneurones
Phase initiale
Phase tardive Up regulationrécepteurs post-synaptiques
Down regulationrécepteurs post-synaptiques
Renforcement des circuits existants
Hypersensibilité des récepteurs aux neurotransmetteurs
Hyperexcitabilité neuronale
Deck. Neurochirurgie, 2003 ; 49 : 163-84Bach-y-Rita. Paraplegia, 1993 ; 31 : 82-7

Résistance musculaire passive
O'Dwyer. Brain, 1996 ;119 : 1737-49Salazar-Torres. Disabil Rehabil, 2004 ; 26 : 756-60Dietz. Handb Clin Neurol, 2012 ; 109 : 197-211
Etirementdu muscle
Reflexemyotatique
Dépend de la vitesse d’étirement
Résistance élastique passive
Dépend de l’étirement, mais pas de la vitesse
Raideur musculaire
spasticité
Distinction entre ces deux composantes : EMG

En résumé
Interruption des voies descendantes inhibitrices
Hyperexcitabiliténeuronale
Plasticité neuronale Up régulation des rcp post-synaptiques
Renforcement des circuits existants
Afférences normales
Hyperactivité motoN a
spasticité
Raideur musculaire passive
Épines irritatives
Dietz. Handb Clin Neurol, 2012 ; 109 : 197-211Deck. Neurochirurgie, 2003 ; 49 : 163-84
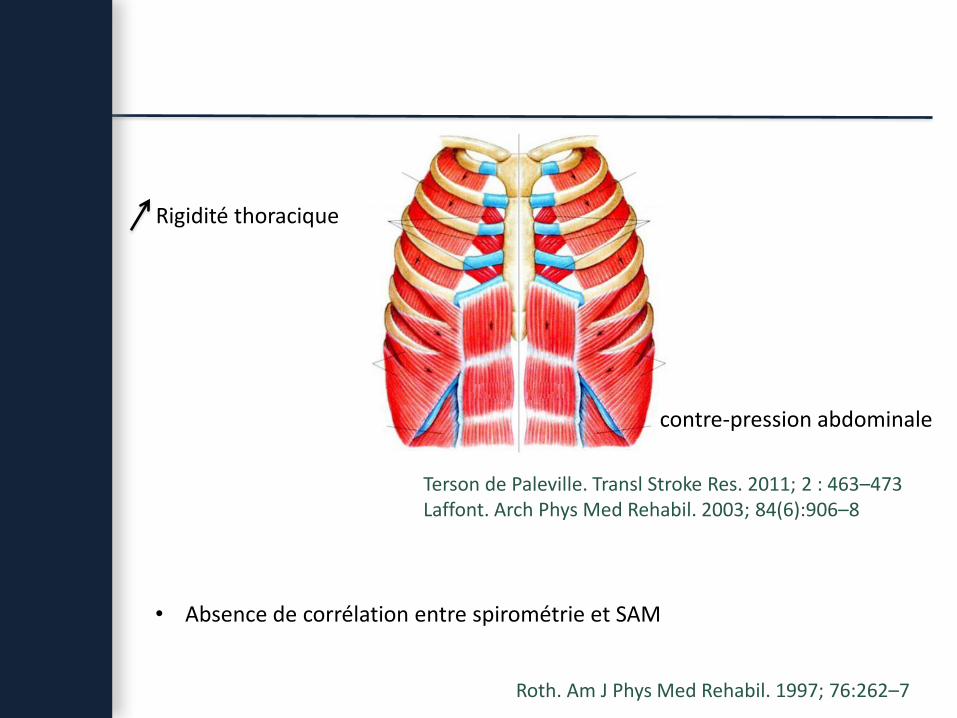
Terson de Paleville. Transl Stroke Res. 2011; 2 : 463–473Laffont. Arch Phys Med Rehabil. 2003; 84(6):906–8
Roth. Am J Phys Med Rehabil. 1997; 76:262–7
Rigidité thoracique
contre-pression abdominale
• Absence de corrélation entre spirométrie et SAM

CASE REPORTBaclofen Pump Int ervent ion for Spast icit y Af fect ingPulmonary Funct ion
Deanna Britton, MS, CCC-SLP, BC-NCD1; Barry Goldstein, MD, PhD1–3; Jill Jones-Redmond, MS, CCC-SLP1,4;Peter Esselman, MD1,2
1Harborview Medical Center, Seattle, Washington; 2Department of Rehabilitation Medicine, University ofWashington, Seattle, Washington; 3Spinal Cord Injury & Disorders Strategic Health Care Group, VeteransAdministration Puget Sound Health Care System, Seattle, Washington; 4Overlake Medical Center,Bellevue, Washington
Received August 5, 2004; accepted June 2, 2005
Abst r actInt roduct ion: Muscle spasticity may adversely affect pulmonary function after spinal cord injury (SCI).However, there is limited information regarding the treatment of spasticity as a determinant of pulmonaryfunction. This study presents the case of a man with C4 tetraplegia who had severe spasticity and difficultyweaning from ventilatory support.Met hods: Case presentation.
Result s: Severe spasticity likely contributed to respiratory compromise in this patient. Successful and rapidweaning from the ventilator occurred within 3 weeks of baclofen pump placement.Conclusions: Randomized clinical trials among SCI patients with significant spasticity are needed todetermine whether intervention with a baclofen pump facilitates earlier ventilatory weaning.
J Spinal Cord Med. 2005;28:343–347
Key Words: Spinal cord injuries; Spasticity; Ventilator weaning; Baclofen pump; Respiratory impairment;Tetraplegia
INTRODUCTIONDespite the overall decline in mortality for patients withspinal cord injury (SCI), pulmonary complications area leading cause of mortality in patients in the acute andchronic phase after tetraplegia (1). Respiratory impair-ments after cervical SCI are caused by compromise of therespiratory muscles, such as the diaphragm, abdominal,and intercostal muscles. These changes result in de-creased vital capacity, diminished cough strength, andincreased risk of atelectasis, pneumonia, hypoxemia, andsleep disorders. Skeletal deformities and autonomicchanges also contribute to a decline in pulmonaryfunction after SCI (2).
Spasticity may also adversely affect pulmonaryfunction. Silver & Lehr (3) described 3 patients with C4and C5 SCI who experienced dyspnea associated withdiaphragmatic spasticity. Spasticity of truncal muscles(intercostals and abdominals) has been reported to
impair pulmonary function. For instance, Laffront et al(4) described a patient with a C4 American Spinal InjuryAssociat ion (ASIA) grade A SCI whose breathlessness wasattributed to spastic abdominal contractions. However,there is little informat ion regarding the treatment ofspasticity as a determinant of pulmonary function afterSCI. Treatment of spasticity with enteral medicationsmayhave limited effectiveness and may have side effects nottolerated by patients (5). The use of intrathecal baclofenisoften an effective alternative to oral medications for thetreatment of severe spasticity (6,7).
Ventilator weaning is often challenging for personswith high-level tetraplegia because of mult iple factors.Respiratory failure results from decreased vital capacity,arterial hypoxemia and hypercarbia, pneumonia, atelec-tasis, and sleep disorders, and may present acutely aftera SCI, but may also present years after the injury (8,9).
We describe a patient with C4 tetraplegia who hadsevere spasticity and difficulty weaning from ventilatorysupport until a baclofen pump was implanted fortreatment of spasticity.
CASE REPORTA 55-year-old man was injured in an accident resulting inC4 ASIA grade A tetraplegia, requiring ventilatory
Please address correspondence to Deanna Britton, MS, CCC-SLP, BC-NCD, Speech-Language Pathology Clinical Specialist,Harborview Medical Center, 325 Ninth Avenue, Box 359819,Seattle, WA 98104; phone: 206.731.2409 (e-mail: [email protected]).
Baclofen Pum p Int ervent ion 343
#9
Heures sans VM Capacité vitale
Homme 55 ans,Tétraplégie C4 traumatique avec dépendance ventilatoire.Echec TTT médical po (baclofène, valium, tizanidine)
6 mois : pompe ITB, niveau T6-T7 (introduction L4-L5), 240 μg/j

Dyssynergie vésico-sphinctérienne
Distension vésicale
Fibres groupe II
détrusor
sphincter
Pont : noyaux régulateurs

Dyssynergie vésico-sphinctérienne
Distension vésicale
Fibres groupe II
détrusorRéflexes A delta et C- centres sacrés- stimulation pΣ
sphincter
Pont : noyaux régulateurs
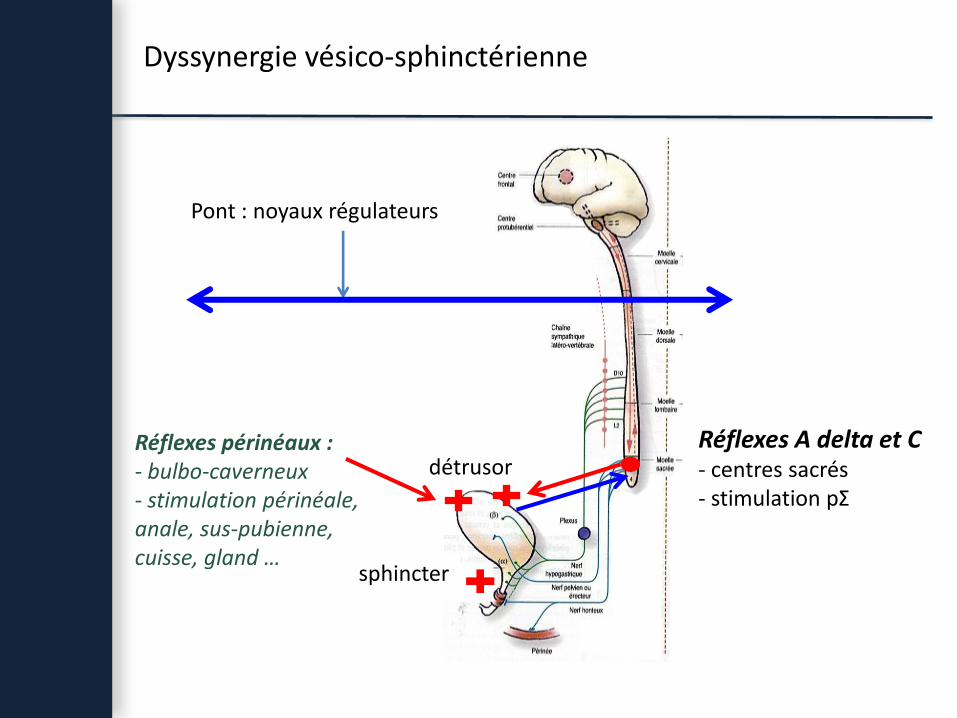
Dyssynergie vésico-sphinctérienne
détrusor
sphincter
Réflexes périnéaux :- bulbo-caverneux- stimulation périnéale, anale, sus-pubienne, cuisse, gland …
Pont : noyaux régulateurs
Réflexes A delta et C- centres sacrés- stimulation pΣ

Nociception Hyperréflexie sympathique
- Récepteurs thermo-algiques- Récepteurs viscéraux sensibles à la distention
Fibres nociceptives de type C
Efférences sympathiques (T5-L2)

Physiopathologie HRS
Gao. Clin Auton Res. 2002 ; 12 : 457-64Hambly. Anaesthesia. 1998;53:273-89
Stimulation nociceptive
Activation Σ exagérée V/C, HTA
Baroréflexe préservé bradycardie
Atteinte > T5
NAd plasmatique modérée Se à la NAd
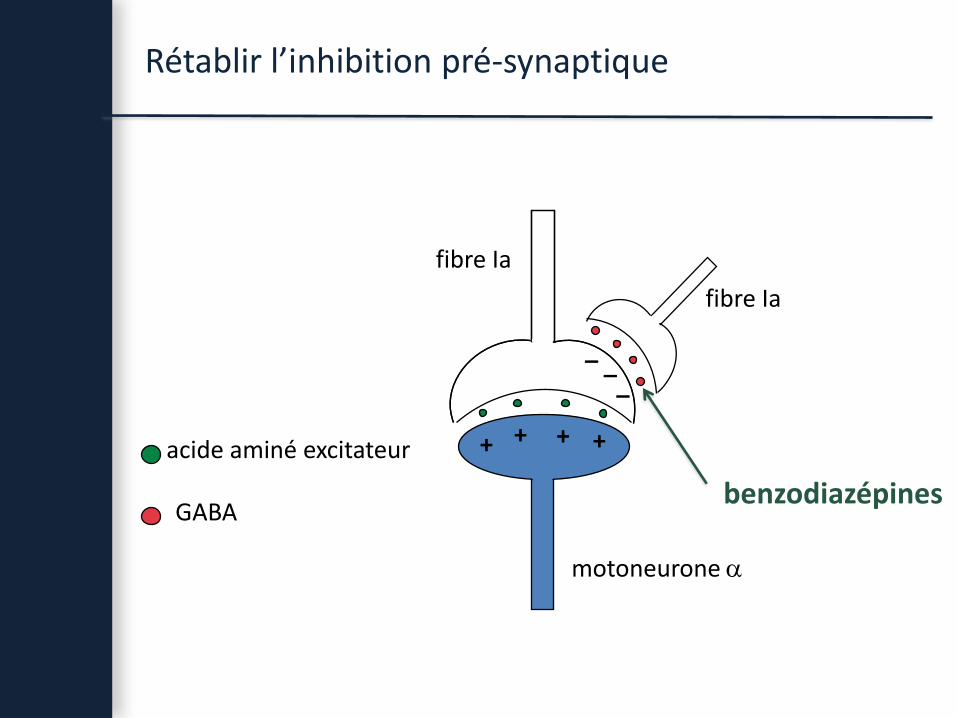
fibre Ia
motoneurone
fibre Ia
Rétablir l’inhibition pré-synaptique
acide aminé excitateur
GABAbenzodiazépines
__
_
+ ++ +

Baclofène (1965)
agoniste GABA B
BaclofèneΘ
__
_
+ ++ +
fibre Ia
fibre Ia
motoneurone
acide aminé excitateur
GABA

Arnon. 2001, JAMA 285 ; 1059-1070

Faut-il traiter la spasticité en réanimation ?

52 patients varus équinAVC, TC, Encéphalopathie post anoxique10 sem (± 3 sem) : Botox IM vs placébo IM, randomisé double aveugle
+/- 2è injection optionnelle à + 12 semaines
A + 12 semaines
Botox IM (n=26)
☐ placébo IM (n=26)

Après 12 semaines
Botox IM (n=25)
☐ placébo IM (n=26)
Injection optionnelle à 12 Sem : groupe botox initial : 10 / 26groupe placébo initial : 15 / 26 (p=0,26)

27 patients ITB depuis 5 ans±1 an ½
n Durée tttpréalable (mois)
Dose moyen fin 1ère
année
répartition
Groupe 1Arrêt ITB
7 60 ± 15 189 γ /j 5 SEP2 trau medull
Groupe 2diminution ITB de 40 %
10 65 ± 23 290 ± 200 8 SEP1 AVC1 trau medull
Groupe 3Maintien ITB
10 290 7 SEP1 AVC1 trau medull1 TC

Gassmann. Nature review Neuroscience. 2012;13:380-94
Early gene protein (fos, jun, krox24)


Coma recovery scale-revised
Délai depuis lésion (mois) Dose baclofène (µg/j)
HSA 10 200
HIP 11 249
TC 12 399
TC 7 300
Enceph post anoxique 6 325

Garçon 8 ans, TC grave, LADSpasticité sévèreITB à 2,5 moisPL quotidiennes
Homme 18 ans, TC grave, HSA+ LADSpasticité sévèreITB à 1,5 moisPL quotidiennes

Hypothèses physiopathologiques
Margetis. Neuromodulation, 2013Pistoia. CNS Drugs, 2010;24:625-38Sara. Arch Phys Med Rehabil, 2009;90:1245-9Taira. Prog Brain Res, 2009;177;317-28
• Réduction des informations proprioceptives : qui pourraient interférer avec lemaintien de l’attention
• Réduction de l’activité sérotoninergique : modulation des cycles veille/sommeil
• Amélioration de la conduction axonale des neurones lésés
• Stimulation des neurones à oréxine de l’hypothalamus (régulation des étatsveille /sommeil)
• Restauration de la fonction du noyau réticulaire thalamique (TRN)
• Reconnexion de boucles cortico-thalamo-corticales
• Restauration de la transmission gabaergique intra-corticale : lutte contrel’hyperexcitabilité des réseaux corticaux

Hypothèses physiopathologiques
Concentration de baclofène dans le cerveau ?
ITB serait-il efficace chez les patients non spastiques ?

A retenir
1. Les troubles apparaissent en réanimation
2. Mécanismes adaptatifs
(interruptions des voies inhibitrices descendantes, plasticité neuronale,
up régulation des récepteurs post-synaptiques, modifications musculaires propres)
3. Thérapeutiques faciles à mettre en œuvre en réanimation
4. Intérêt des traitements précoces ?