![1. CONTACTEUR ÉLECTROMAGNÉTIQUE EN TRANSLATIONpsi1montaigne.com/CONVERSION.../cours_conversion_electromecanique... · conversion de puissance 3 [ÉlectromagnÉtisme 10] conversion](https://static.fdocuments.fr/doc/165x107/5c20922309d3f24d208c148b/1-contacteur-electromagnetique-en-tran-conversion-de-puissance-3-electromagnetisme.jpg)
COMPREHENSIVE PERCEPTION OF BURN CONVERSION: A …
8
COMPREHENSIVE PERCEPTION OF BURN CONVERSION: A LITERATURE REVIEW COMPRENDRE L’APPROFONDISSEMENT DES BRÛLURES: REVUE DE LA LITTÉRATURE Wardhana A., 1* Basuki A., 1 Aurora L., 2 Marsigit J. 3 1 Cipto Mangunkusumo Hospital, Jakarta, Indonesia 2 Hermina Sukabumi Hospital, Sukabumi, West Java, Indonesia 3 Kramat 128 Hospital, Central Jakarta, Jakarta, Indonesia SUMMARY. Burn conversion is the conversion of stasis zone into both greater burn area and burn depth. It may hamper the patient’s condition since morbidity and mortality are expected to be higher with the in- crease of burn size. To gain a comprehensive perception of burn conversion, this study aims to collect the latest updates regarding therapy, diagnosis, etiology and prognosis. A literature search was carried out on online databases, namely PubMed, SCOPUS and PROQUEST. The keywords “Burns AND (Conversion OR Progression OR Expansion)” were formulated. The inclusion and exclusion criteria were applied. Twenty-six articles were found, which were divided into diagnosis of burn conversion (11%), etiology of burn conversion (8%), prognosis of burn conversion (0%), and therapy of burn conversion (81%). All of the research was performed on animals. One of the best tools to diagnose burn conversion was the forward- looking infrared (FLIR) imaging, having sensitivity up to 96% and specificity up to 100% to predict scar depth ≥3 mm. The main etiology was ischemia, reactive oxygen species and inflammation. Most of the re- search regarding therapy showed benefit in preventing burn conversion. However, no side effects were in- vestigated and not all of the research was statistically significant. More research on burn conversion prognosis and treatment side effects should be performed. Further research involving trials in humans should be conducted, since animal and human trials may differ. Keywords: burn conversion, burn progression, latest updates RÉSUMÉ. L’approfondissement d’une brûlure est la conversion de la zone d’ischémie en zone nécrosée, résultant en l’extension en profondeur et /ou en surface d’icelle, obérant ainsi les pronostics vital et fonc- tionnel. Cette étude a pour but de faire le point sur les données actuelles de la science pour ce qui en con- cerne l’étiologie, le diagnostic, le traitement et le pronostic. Nous avons exploré la littérature dans Pubmed, Scopus et Proquest, avec les mots clés « burns » AND (conversion OR progression OR expansion), ce qui a ramené 26 articles. Le diagnostic était le sujet de 11% d’entre eux, l’étiologie de 8%, le traitement de 81%. Aucun ne traitait du pronostic. Le meilleur outil diagnostic est l’imagerie Forward Looking InfraRed (FLIR), qui a les meilleures sensibilité (jusqu’à 96%) et spécificité (jusqu’à 100%) pour prédire une atteinte sur plus de 3 mm de profondeur. Les causes principales sont l’ischémie, les radicaux oxygénés réactifs et l’inflammation. Le meilleur traitement est préventif, toutes les recherches ne donnant pas des résultats sig- nificatifs et aucune ne s’intéressant aux effets secondaires des options étudiées. Ainsi, la recherche, en par- ticulier chez l’humain, doit s’intensifier dans ce champ. Mots-clés : brûlure, approfondissement, état de la science ___________ * Corresponding author: Aditya Wardhana, Head of Burn Unit, Plastic Reconstructive and Aesthetic Surgery Division, Department of Surgery, Cipto Mangunkusumo Hospital - Faculty of Medicine, Universitas Indonesia, Diponegoro Road 71, Jakarta 10430, Indonesia. Tel.: +62213146938; email: [email protected] Manuscript: submitted 04/12/2019, accepted 10/03/2020 Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020 89
Transcript of COMPREHENSIVE PERCEPTION OF BURN CONVERSION: A …

COMPREHENSIVE PERCEPTION OF BURN CONVERSION:A LITERATURE REVIEW
COMPRENDRE L’APPROFONDISSEMENT DES BRÛLURES: REVUE DELA LITTÉRATURE
Wardhana A.,1* Basuki A.,1 Aurora L.,2 Marsigit J.3
1 Cipto Mangunkusumo Hospital, Jakarta, Indonesia2 Hermina Sukabumi Hospital, Sukabumi, West Java, Indonesia3 Kramat 128 Hospital, Central Jakarta, Jakarta, Indonesia
SUMMARY. Burn conversion is the conversion of stasis zone into both greater burn area and burn depth.It may hamper the patient’s condition since morbidity and mortality are expected to be higher with the in-crease of burn size. To gain a comprehensive perception of burn conversion, this study aims to collect thelatest updates regarding therapy, diagnosis, etiology and prognosis. A literature search was carried out ononline databases, namely PubMed, SCOPUS and PROQUEST. The keywords “Burns AND (ConversionOR Progression OR Expansion)” were formulated. The inclusion and exclusion criteria were applied.Twenty-six articles were found, which were divided into diagnosis of burn conversion (11%), etiology ofburn conversion (8%), prognosis of burn conversion (0%), and therapy of burn conversion (81%). All ofthe research was performed on animals. One of the best tools to diagnose burn conversion was the forward-looking infrared (FLIR) imaging, having sensitivity up to 96% and specificity up to 100% to predict scardepth ≥3 mm. The main etiology was ischemia, reactive oxygen species and inflammation. Most of the re-search regarding therapy showed benefit in preventing burn conversion. However, no side effects were in-vestigated and not all of the research was statistically significant. More research on burn conversionprognosis and treatment side effects should be performed. Further research involving trials in humans shouldbe conducted, since animal and human trials may differ.
Keywords: burn conversion, burn progression, latest updates
RÉSUMÉ. L’approfondissement d’une brûlure est la conversion de la zone d’ischémie en zone nécrosée,résultant en l’extension en profondeur et /ou en surface d’icelle, obérant ainsi les pronostics vital et fonc-tionnel. Cette étude a pour but de faire le point sur les données actuelles de la science pour ce qui en con-cerne l’étiologie, le diagnostic, le traitement et le pronostic. Nous avons exploré la littérature dans Pubmed,Scopus et Proquest, avec les mots clés « burns » AND (conversion OR progression OR expansion), ce quia ramené 26 articles. Le diagnostic était le sujet de 11% d’entre eux, l’étiologie de 8%, le traitement de81%. Aucun ne traitait du pronostic. Le meilleur outil diagnostic est l’imagerie Forward Looking InfraRed(FLIR), qui a les meilleures sensibilité (jusqu’à 96%) et spécificité (jusqu’à 100%) pour prédire une atteintesur plus de 3 mm de profondeur. Les causes principales sont l’ischémie, les radicaux oxygénés réactifs etl’inflammation. Le meilleur traitement est préventif, toutes les recherches ne donnant pas des résultats sig-nificatifs et aucune ne s’intéressant aux effets secondaires des options étudiées. Ainsi, la recherche, en par-ticulier chez l’humain, doit s’intensifier dans ce champ.
Mots-clés : brûlure, approfondissement, état de la science___________
* Corresponding author: Aditya Wardhana, Head of Burn Unit, Plastic Reconstructive and Aesthetic Surgery Division, Department of Surgery, Cipto MangunkusumoHospital - Faculty of Medicine, Universitas Indonesia, Diponegoro Road 71, Jakarta 10430, Indonesia. Tel.: +62213146938; email: [email protected]: submitted 04/12/2019, accepted 10/03/2020
Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
89
Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
90
Introduction
The incidence of burn injury is estimated at about180.000 deaths annually, with two-thirds of them oc-curring in Africa and South-East Asia.1 Indonesia isthe most populated country among developing coun-tries in South-East Asia, with an estimated 260 mil-lion citizens.2 Moreover, mortality from burn injuryin Indonesia remains high, at 24% in the Cipto Man-gunkusumo Burn Centre and 14.5% in the Dr. Soe-tomo General Hospital.3,4 The lack of facilities inJakarta’s Burn Unit is also believed to impact thetreatment of patients. As an example, there are only24 beds available for burns patients in Jakarta, whichhas 10.2 million citizens.5 This number is consideredsmall compared to Singapore, which has about 16beds with an estimated 5.7 million citizens.6
The progression of superficial partial-thicknessburns into deep partial-thickness or full-thicknessburns is called burn conversion.7 Each burn injuryhas a stasis zone which is at risk of progressing intoboth greater burn area and burn depth.7,8 The extentof the size and depth of the burn may hamper the pa-tient’s condition since greater morbidity and mortal-ity are expected with the increase in burn size.7,9
Unlike the primary injury zone, burn conversion isexpected to be modifiable with prompt treatment andintervention.8
A lot of research has been conducted to under-stand the management of burn conversion. However,there is no article that collects studies on etiology,diagnosis, prognosis and therapy of burn conversion,and compares studies in animals and in humans.Comprehensive perception regarding burn conver-sion is needed to improve the quality of burn care.This study aims to collect the latest updates on ther-apy, diagnosis, etiology and prognosis in burn con-version.
Materials and methods
This review aims to summarize the latest evi-dence regarding the etiology, prognosis, diagnosisand therapy of burn conversion. To collect compre-hensive knowledge about burn conversion, an exten-sive literature search was performed. The keywords
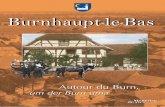
“Burns AND (Conversion OR Progression OR Ex-pansion)” were formulated to each database. The on-line databases used were PubMed, SCOPUS andPROQUEST. The search was conducted between1st - 7th September 2018. The flow chart in Fig. 1 ex-plains search strategy, results and inclusion-exclu-sion criteria. Table I presents a list of abbreviations.
Results
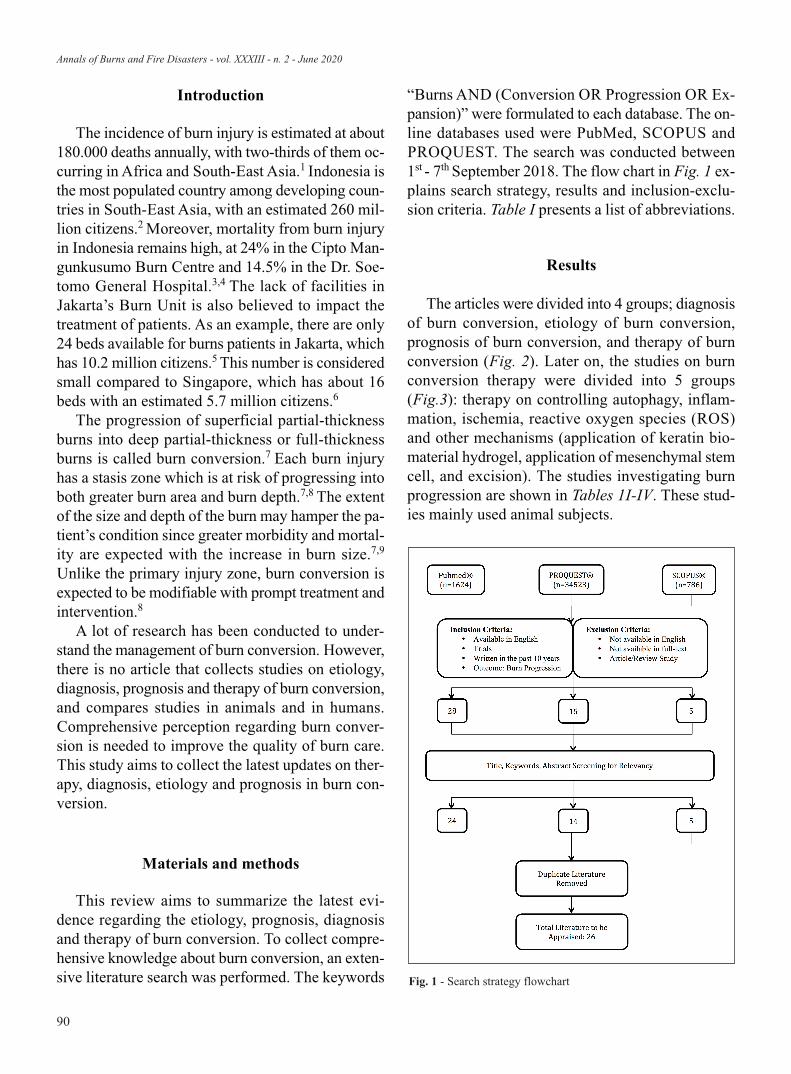
The articles were divided into 4 groups; diagnosisof burn conversion, etiology of burn conversion,prognosis of burn conversion, and therapy of burnconversion (Fig. 2). Later on, the studies on burnconversion therapy were divided into 5 groups(Fig.3): therapy on controlling autophagy, inflam-mation, ischemia, reactive oxygen species (ROS)and other mechanisms (application of keratin bio-material hydrogel, application of mesenchymal stemcell, and excision). The studies investigating burnprogression are shown in Tables 1I-IV. These stud-ies mainly used animal subjects.
Fig. 1 - Search strategy flowchart
Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
91
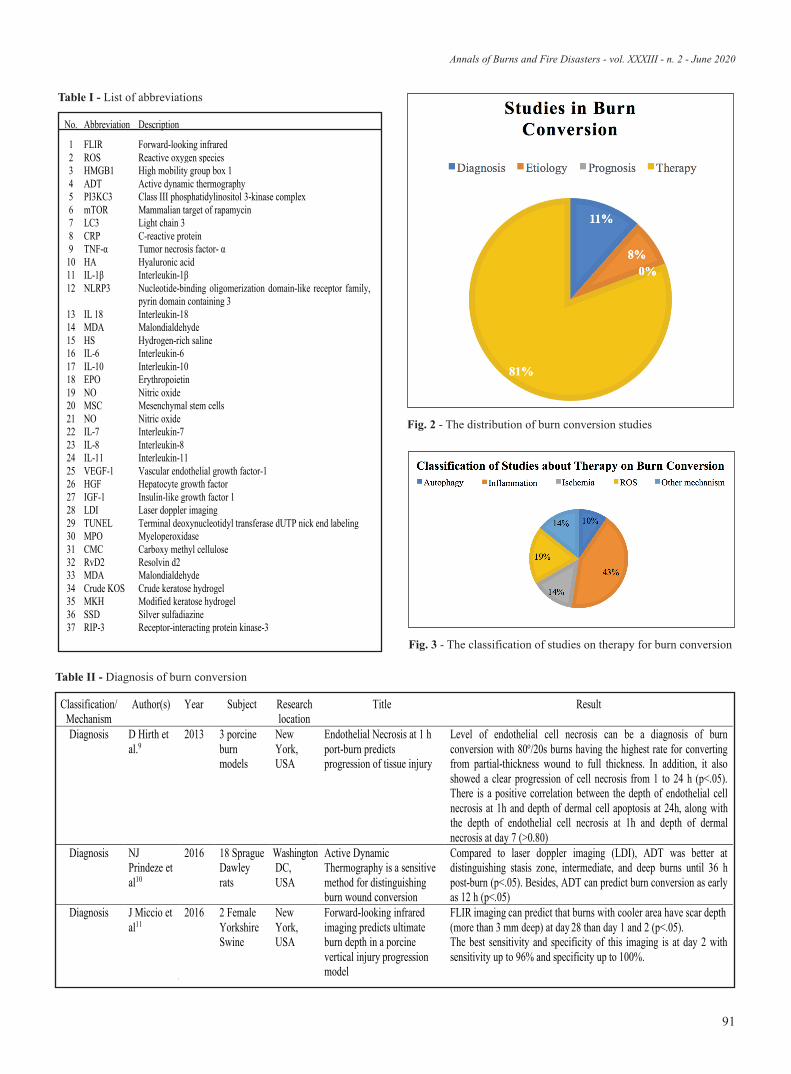
32 RvD2 Resolvin d2 33 MDA Malondialdehyde 34 Crude KOS Crude keratose hydrogel 35 MKH Modified keratose hydrogel 36 SSD Silver sulfadiazine 37 RIP-3 Receptor-interacting protein kinase-3
No. Abbreviation Description
1 FLIR Forward-looking infrared 2 ROS Reactive oxygen species 3 HMGB1 High mobility group box 1 4 ADT Active dynamic thermography 5 PI3KC3 Class III phosphatidylinositol 3-kinase complex 6 mTOR Mammalian target of rapamycin 7 LC3 Light chain 3 8 CRP C-reactive protein 9 TNF- Tumor necrosis factor-
10 HA Hyaluronic acid 11 IL- Interleukin- 12 NLRP3 Nucleotide-binding oligomerization domain-like receptor family,
pyrin domain containing 3 13 IL 18 Interleukin-18 14 MDA Malondialdehyde 15 HS Hydrogen-rich saline 16 IL-6 Interleukin-6 17 IL-10 Interleukin-10 18 EPO Erythropoietin 19 NO Nitric oxide 20 MSC Mesenchymal stem cells 21 NO Nitric oxide 22 IL-7 Interleukin-7 23 IL-8 Interleukin-8 24 IL-11 Interleukin-11 25 VEGF-1 Vascular endothelial growth factor-1 26 HGF Hepatocyte growth factor 27 IGF-1 Insulin-like growth factor 1 28 LDI Laser doppler imaging 29 TUNEL Terminal deoxynucleotidyl transferase dUTP nick end labeling 30 MPO Myeloperoxidase 31 CMC Carboxy methyl cellulose
Table I - List of abbreviations
Fig. 2 - The distribution of burn conversion studies
Fig. 3 - The classification of studies on therapy for burn conversion
Classification/Mechanism
Author(s) Year Subject Research location
Title Result
Diagnosis D Hirth et al.9
2013 3 porcine burn models
New York, USA
Endothelial Necrosis at 1 h port-burn predicts progression of tissue injury
Level of endothelial cell necrosis can be a diagnosis of burn conversion with 80o/20s burns having the highest rate for converting from partial-thickness wound to full thickness. In addition, it also showed a clear progression of cell necrosis from 1 to 24 h (p<.05). There is a positive correlation between the depth of endothelial cell necrosis at 1h and depth of dermal cell apoptosis at 24h, along with the depth of endothelial cell necrosis at 1h and depth of dermal necrosis at day 7 (>0.80)
Diagnosis NJ Prindeze et al10
2016 18 Sprague Dawley rats
WashingtonDC, USA
Active Dynamic Thermography is a sensitive method for distinguishing burn wound conversion
Compared to laser doppler imaging (LDI), ADT was better at distinguishing stasis zone, intermediate, and deep burns until 36 h post-burn (p<.05). Besides, ADT can predict burn conversion as early as 12 h (p<.05)
Diagnosis J Miccio et al11
2016 2 Female Yorkshire Swine
New York, USA
Forward-looking infrared imaging predicts ultimate burn depth in a porcine vertical injury progression model
FLIR imaging can predict that burns with cooler area have scar depth (more than 3 mm deep) at day 28 than day 1 and 2 (p<.05). The best sensitivity and specificity of this imaging is at day 2 with sensitivity up to 96% and specificity up to 100%.
Table II - Diagnosis of burn conversion

Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
92
Classification/Mechanism
Author(s) Year Subject Research location
Title Result
Etiology JQ Tan et al14
2013 15 adult male
Sprague Dawley
rats
Xi’an, China
The roles of autophagy and apoptosis in burn wound progression in rats.
The number of autophagy cells (Beclin1 as the marker) was significantly higher in 6h post-burn compared to control (p<.05). The terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) staining revealed that the apoptotic cell was significantly higher after 24h post-burn compared to control (p<.05). Bax protein expression was significantly higher after 24h post-burn while Bcl-2 was significantly lower (p<.05).
Etiology Xiao et al15 2014 56 male Wistar rats
Beijing, China
Role of autophagy and apoptosis in wound tissue of deep second-degree burn in rats
Beclin-1 was decreased significantly at 24h post-burn compared to control (p<.01) TUNEL assay, which showed more cells undergoing apoptosis compared to control (p<.05 at 6 hours and p<.01 at 24, 48, and 72 hours). Myeloperoxidase (MPO) as the inflammatory marker, increased 5.3-fold over the 48 hours (p <.01)
Table III - Etiology of burn conversion
Table IV - Research on animals for burn conversion therapy

Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
93

Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
94
Discussion
Diagnosis of burn conversionMicroscopic view of high mobility group box 1
(HMGB1) and Caspase 3a staining were capable ofgiving the picture of adnexal necrosis progressionand apoptosis in this type of burn injury over 24hours post-burn in the 80°/20s burn type becausethere were still viable tissues over 24 hours follow-ing injury. Moreover, the upper subzones turned intofull-thickness burn as there was subsequent vesselplugging, making the cells undergo the necroticprocess. The lower subzones were the zones thatcould still be salvageable depending on cytokine dif-fusion from the upper subzones.9 Active dynamicthermography (ADT) was proven to be significantlybetter at detecting the progression of stasis zone on12 hour post-burn.10 Another diagnostic tool wasFLIR to detect temperature of the affected tissue. Itwas found that the cooler the area, the deeper thescar found on day 28 post-injury (compared to day1 and 2). Day 2 had the strongest correlation, sensi-tivity and specificity with scar depth on day 28.
Based on the result given, only FLIR had sensi-tivity up to 96% and specificity up to 100% to detectdeeper scar 28 days after burn injury.11 WhileHMGB1 and Caspase 3a seem promising, ADT andFLIR are easier in daily clinical use.
Etiology of burn conversionAutophagy is a catabolic process involving the
engulfment of proteins including the organellewhich are then delivered to lysosomes to be brokendown into the basic form of biomolecules.12 Au-tophagy occurs in dying cells to maintain cellularhomeostasis, however when the stress persists,apoptosis may be activated. Beclin-1 and Bax wereoriginally identified as the interaction partner of theanti-apoptotic protein called BCL2. Through class IIIphosphatidylinositol 3-kinase complex (PI3KC3),Beclin-1 can induce autophagy, while Bax can in-duce apoptosis. BCL2 can inhibit both of theseprocesses. It is known that the reduced level of Be-clin-1 can prevent the turnover of damaged mito-chondria, leading to a decrease in the production ofROS.12,13 Beclin-1 was significantly higher in 6h
post-burn compared to control,14 however not after24h post-burn.15 Bax protein was also significantlyhigher in 24h post-burn with significantly lowerBCL-2 protein expression.14 Studies showed that theapoptotic cells were significantly higher from 6huntil 72h post-burn compared to controls.14,15 Thereis a contradiction within these studies which may beexplained by the fact that different burn-type sub-jects were used in the studies. Further research isneeded regarding the etiology of burn conversion in-volving Bcl-2 protein family.
Burn conversion therapyTherapy for controlling autophagy. Rapamycin is
known as an autophagy inducer, suppressing mam-malian target of rapamycin (mTOR) kinase activityand enhancing clearance of aggregate-prone proteinsthat reduce cell toxicity, while light chain 3 (LC3) andBeclin-1 reflect the autophagy level in burns, meas-ured using Western Blot analysis. One study indicatedthat rapamycin increased LC3 and beclin- 1, thus itincreased the autophagy process. The rapamycingroup also has more superficial burn depth, moreresidual hair follicles, and less collagen denaturationcompared to the control group. However, the functionof autophagy, whether it hinders or arbitrates celldeath (resulting in apoptosis), remains controversial,as the number of studies on autophagy and deepeningof burn wounds is still limited. It also must be notedthat Xiao’s study has a small sample size, short fol-low-up period, and is limited to rats.16
Therapy for controlling inflammation. Ab-normal inflammatory response, caused by a higher-than-normal inflammatory mediator, is believed to bean important factor in wound conversion pathogene-sis.17 One study stated that inflammation in burnwound is preserved, especially complement and C re-active protein (CRP) with increased infiltration ofneutrophils and macrophages, which happens up to46 days after the insult.18 Along with this fact, fewstudies have been conducted on attenuating inflam-mation in burn wounds, where mainly well-knownanti–inflammatory agents are used. Several anti-in-flammatory agents were tested in rats to see if theycan significantly reduce burn progression. Two stud-ies used (anti-tumor necrosis factor- α)-hyaluronicacid ((anti-TNF- α )-HA) conjugates resulting in

Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
95
promising anti- inflammatory effects as it decreasedinflammatory markers, such as interleukin-1β (IL-1β)and macrophages.19,20 However, the clinical outcomeis not statistically significant in one of the studies.20
Macrophage count was also lowered in burned ratstreated with Resolvin D2.21 Another study measuresthe effect of 3,4- Methylenedioxy-β nitrostyrene toinhibit nucleotide-binding oligomerization domain-like receptor family, pyrin domain containing 3(NLRP3) inflammasome, which is the precursor ofinflammatory markers, such as IL 1β and interleukin-18 (IL 18). The result is promising as there were sig-nificantly lower inflammatory markers.22 A studyconducted in Korea showed that giving Nicorandil, avasodilator drug that activates Potassium channels,can also significantly reduce both IL-1β and tumornecrosis factor- α (TNF-α).23
Therapy for controlling ROS. Other studies meas-ured Malondialdehyde (MDA), which is a marker foroxidative stress, in order to see whether the treatmentscan reduce burn progression or not, such as by usingHydrogen-rich Saline (HS),24 Astaxanthin,25 andmethylene blue injection.26 However, the resultsshowed that only HS and the use of Astaxanthinmedium-high dose significantly reduced MDA. Inaddition, HS can significantly lower inflammatorymarkers, such as TNF-α, IL-1β, and interleukin-6(IL-6) in the zone of stasis while augmenting inter-leukin-10 (IL- 10).24 HS acted by inhibiting mem-brane lipid peroxidation and enhancing endogenousantioxidant enzyme system activity. Hydrogen hasbeen reported to alleviate injury triggered by is-chemia/reperfusion and burns in various organs by se-lectively quenching oxygen-free radicals.
Therapy for controlling ischemia. Erythropoietin(EPO) is believed to have tissue-protective effects bymediating nitric oxide (NO)-mediated arterial vesselrelaxation, inducing angiogenesis, preventing apop-tosis caused by ischemia, and preventing inflamma-tion. There were two studies found: one involvedtime-dependent administration of EPO and the sec-ond involved the dosage-dependent administration ofEPO. The results showed that EPO administration,when given at a low dose (500 IU/kg body weight)within 45 minutes after burn, can significantly reduceinterspace necrosis, which results in faster burnwound healing.27-29 Dressing could also impact the
perfusion. The modified keratose hydrogel (Coto-plast) showed the least burn progression compared tosilver sulfadiazine dressing, even with no statisticallysignificant result. This is probably due to the fact thatkeratin has vasodilator properties topically.30
Therapy for controlling other mechanisms. Onlymesenchymal stem cells (MSC) have been knownto significantly reduce necrotic area by 20%throughout, secreting a large number of cytokines;interleukin-7 (IL-7), interleukin-8 (IL-8), inter-leukin-11 (IL-11) and cell mediators, such as vascu-lar endothelial growth factor- 1 (VEGF-1),hepatocyte growth factor (HGF), and insulin-likegrowth factor-1 (IGF- 1).31 Other studies involvingimmediate burn excision and giving Necrostatin-1did not give successful results.32,33 The interestingfact is that this result suggests that burn interspaceprogression is not dependent on the “passive” re-lease of bioactive molecules from necrotic cells.However, the mechanism of how it could happen isnot clearly understood. Necrostatin-1 also failed toprevent burn progression in rat burn models. Thismay be due to the necroptosis role in burn progres-sion or inactivity of necrostatin-1.
Conclusion
All of the studies above represent a huge step for-ward in perceiving burn conversion, particularly itstreatment. Most of the studies on diagnosis focus onidentifying temperature changes to distinguish burnwound conversion. While the etiology of burn con-version mainly discusses apoptosis process, the au-tophagy process remains unclear since resultsremain conflicting. Wide varieties of treatmentsadapted from other diseases mostly show some pos-itive results in reducing burn conversion clinicallyand statistically. Each treatment has its own aims,such as reducing inflammation and ROS, increasingperfusion, and others. Future research related toprognosis and pathophysiology, particularly regard-ing the weight and timeline of each factor, whichcontributes to burn conversion, should be conducted.Moreover, the side effects and efficacy of burn con-version treatment should also be investigated inorder to create safe and optimal therapy.

Annals of Burns and Fire Disasters - vol. XXXIII - n. 2 - June 2020
96
BIBLIOGRAPHY
Anenden H: Burns, 2018 [Updated: 6 March 2018; cited: Sep-1tember 2018]. Available from: http://www.who.int/en/news-room/fact-sheets/detail/burns.The World Factbook, 2017 [Cited: September 2018]. Available2from: https://www.cia.gov/library/publications/the-world-fact-book/rankorder/2119rank.html. Wardhana A, Basuki A, Prameswara AD, Rizkita DN et al.: The3epidemiology of burns in Indonesia’s national referral burn cen-ter from 2013 to 2015. Burns Open, 1(2): 67-73, 2017.Hidayat T, Noer M, Saputro I: Five years retrospective study of4burns in DR Soetomo General Hospital Surabaya. Folia MedicaIndones, 50: 123-30, 2014.Statistics Indonesia – DKI Jakarta Province. Total population5and population growth rate in the regency or city of JakartaProvince 2010, 2014, and 2015. 2017 [updated: 30 January 2017;cited: September 2018]. Available from: https://jakarta.bps.go.id/statictable/2017/01/30/136/jumlah-penduduk-dan-laju-pertum-buhan-penduduk-menurut-kabupaten-kota-di-provinsi-dki-jakarta-2010-2014-dan-2015.html.Burns Centre, Singapore General Hospital: 2017 [cited August62017]. Available from: https://Centers/Burns-Centre/Pages/burns-centre.aspx.Salibian AA, Del Rosario AT, Severo LD, Nguyen L et al.: Cur-7rent concepts on burn wound conversion - a review of recent ad-vances in understanding the secondary progressions of burns.Burns, 42(5): 1025-35, 2016.Jackson DM: The diagnosis of the depth of burning. Br Jr Surg,840: 588, 1953.Hirth D, McClain SA, Singer AJ, Clark RA: Endothelial necro-9sis at 1 hour postburn predicts progression of tissue injury.Wound Repair Regen, 21(4): 563-70, 2013.Prindeze NJ, Hoffman HA, Ardanuy JG, Zhang J et al.: Active10dynamic thermography is a sensitive method for distinguishingburn wound conversion. J Burn Care Res, 37(6): 559-568, 2016.Miccio J, Parikh S, Marinaro X et al.: Forward-looking infrared11imaging predicts ultimate burn depth in a porcine vertical injuryprogression model. Burns, 42(2): 397-404, 2016.Rubinstein AD, Kimchi A: Life in the balance – a mechanistic12view of the crosstalk between autophagy and apoptosis. J CellSci, 125: 5259-5268, 2012.Menon MB, Dhamija S: Beclin 1 phosphorylation - at the center13of autophagy regulation. Front Cell Dev Biol, 6: 137, 2018.Tan JQ, Zhang HH, Lei ZJ, Ren P et al.: The roles of autophagy14and apoptosis in burn wound progression in rats. Burns, 39(8):1551-6, 2013.Xiao M, Li L, Li C, Zhang P et al.: Role of autophagy and apop-15tosis in wound tissue of deep second-degree burn in rats. AcadEmerg Med, 21(4): 383-91, 2014.Xiao M, Li L, Hu Q, Ma L et al.: Rapamycin reduces burn16wound progression by enhancing autophagy in deep second-de-gree burn in rats. Wound Rep Reg, 21: 852-9, 2013.Taira BR, Singer AJ, McClain SA, Lin F et al.: Rosiglitazone,17a PPAR-γ ligand, reduces burn progression in rats. J Burn CareRes, 30(3): 499-504, 2009.Rizzo JA, Burgess P, Cartie RJ, Prasad BM: Moderate systemic18hypothermia decreases burn depth progression. Burns, 39(3):436-44, 2013.Sun LT, Friedrich E, Heuslein JL, Pferdehirt RE et al.: Reduc-19tion of burn progression with topical delivery of (antitumor
necrosis factor-α)-hyaluronic acid conjugates. Wound RepairRegen, 20(4): 563-72, 2012.Friedrich EE, Sun LT, Natesan S, Zamora DO et al.: Effects of20hyaluronic acid conjugation on anti-TNF-α inhibition of inflam-mation in burns. J Biomed Mater Res A, 102(5): 1527-36, 2014.Inoue Y, Liu YM, Otawara M, Chico Calero I et al.: Resolvin21D2 limits secondary tissue necrosis after burn wounds in rats. JBurn Care Res, 39(3): 423-32, 2018.Xiao M, Li L, Li C, Liu L et al.: 3, 4-methylenedioxy-β-ni-22trostyrene ameliorates experimental burn wound progression byinhibiting the NLRP3 inflammasome activation. Plast ReconstrSurg, 137(3): 566e-75e, 2016.Choi J, Kim R, Kim J, Jeong W et al.: Nicorandil reduces burn23wound progression by enhancing skin blood flow. J Plast Re-constr Aesthet Surg, 71(8): 1196-206, 2018.Guo SX, Jin YY, Fang Q, You CG et al.: Beneficial effects of24hydrogen-rich saline on early burn-wound progression in rats.PLoS ONE, 10(4): 1-15, 2015.Fang Q, Guo S, Zhou H, Han R et al.: Astaxanthin protects25against early burn- wound progression in rats by attenuating ox-idative stress-induced inflammation and mitochondria-relatedapoptosis. Nature, 2017: 1-11, 2017.Rosique MJ, Rosique RG, Faria FM, Oliveira CC et al.: Meth-26ylene blue reduces progression of burn and increases skin sur-vival in an experimental rat model. Burns, 43(8): 1702-1708,2017.Tobalem M, Harder Y, Schuster T, Rezaeian F et al.: Erythro-27poietin in the prevention of experimental burn progression. Br JSurg, 99(9): 1295-303, 2012.Tobalem M, Harder Y, Rezaeian F, Wettsein R: Secondary burn28progression decreased by erythropoietin. Crit Care Med, 41(4):963-70, 2013.Tobalem M, Harder Y, Tschanz E, Speidel V et al.: First-aid with29warm water delays burn progression and increases skin survival.JPRA Surg, 66: 260-6, 2013.Poranki D, Goodwin C, Van Dyke M: Assessment of deep par-30tial thickness burn treatment with keratin biomaterial hydrogelsin a swine model. BioMed Res Int, October: 1-9, 2016.Singer DD, Singer AJ, Gordon C, Brink P: The effects of rat31mesenchymal stem cells on injury progression in a rat model.Acad Emerg Med, 20(4): 398- 402, 2013.Macri LK, Singer AJ, Taira BR, McClain SA et al.: Immediate32burn excision fails to reduce injury progression. J Burn Care Res,34(3): e153-60, 2013.Reddy AS, Abraham A, McClain SA et al.: The role of necrop-33tosis in burn injury progression in a rat comb burn model. AcadEmerg Med, 22(10): 1181- 6, 2015.Bhatia A, O’Brien K, Chen M, Wong A et al.: Dual therapeutic34functions of F- 5 fragment in burn wounds: preventing woundprogression and promoting wound healing in pigs. Mol Ther-Meth Clinic Dev, 3: 16041, 2016.Sadeghipour H, Torabi R, Gottschall J, Lujan-Hernandez J et35al.: Blockade of IgM-mediated inflammation alters wound pro-gression in a swine model of partial-thickness burn. J Burn CareRes, 38(3): 148-60, 2017.Singer AJ, Taira BR, Lin F, Lim T et al.: Curcumin reduces in-36jury progression in a rat comb burn model. J Burn Care Res, 32:135-42, 2011.
Conflict of interest. We would like to state that no financial relationshipwith other people or institutions exist for any of the authors.