A new flow model for prosthetic heart valves · l ~a boratoire de génie biomédical, IRCM,...
11
A New Flow Mode1 for Doppler Ultrasound Study of Prosthetic Heart Va Louis-Gilles ~ u r a n d l , Damien Garcia1, Frederic Sakrl, Herkole Sava1, Richard Cimon1, Philippe ~ibarotl.~, Aaron ~enster~, Jean G. ~urnesnil~ l ~a boratoire de génie biomédical, IRCM, Université de Mon tréal, p épar te men t de Cardiologie, Institut de Cardiologie de Quebec, Quebec and 31maging Research Laboratory, The John P. Robarts Research Institute, London, Ontario, Canada Background and aim of the study: Steady and pulsatile flow models used to assess the hydrodynamic aspects of prosthetic heart valves are generally made of Plex- iglas and Lucite tubing. They often allow continuous- wave and pulsed-wave Doppler ultrasound velocity measurements to be made parallel to the flow, but cannot be used as such for ultrasound scanning of valve inflow and outflow velocities because of ultra- sonic reverberation and refraction by the tubing. The aim of the study was to develop a new flow model which allowed ultrasonic scanning of the prosthetic valve flow for three-dimensional(3D) reconstruction of color Doppler flow distributions. Metkods: The flow model, designed with left ventric- ular and aortic chambers composed of agar gel which mimics the ultrasound characteristics of biological tissues, was developed and tested for comparative in vitro hydrodynamic and Doppler ultrasonic studies of aortic prosthetic valves. An electromagnetic flowmeter and a pressure monitor provided the flow and pressure signals for the hydrodynamic tests. The Doppler ultrasonic evaluation was performed with an Ultramark 9 HDI ultrasound system and a 3D The non-invasive clinical assessrnent of prosthetic heart valve function is mostly based on valve inflow and outflow velocity measurements by Doppler echocardiography to estimate the transvalvular pres- sure gradient (TPG) with the Bernoulli equation, and the valve effective orifice area (EOA) with the continu- ity equation (1-8). This approach, which is relatively accurate for the assessment of native and bioprosthetic heart valves, shows significant variability when used for mechanical valves, because of their complex flow velocity distributions and different valve designs. Sev- eral studies (4,9-17) showed that, in mechanical pros- Address for correspondence: Louis-Gilles Durand MD, IRCM, 110 Avenue des Pins Ouest, Mon- treal, Quebec, Canada, H2W 17R ultrasound imaging system. The model was designed to enable assessment of prosthetic valve performance by pulsed-wave and continuous-wave Doppler veloc- ity measurements, as well as by 3D color Doppler velocity measurements obtained by ultrasonic scan- ning of the left ventricle or aortic chamber with an ultrasound probe mounted on a motorized transla- tion assembly. Results: The study results showed that this new flow model can provide 3D color Doppler velocity distrib- utions as well as accurate comparisons of hydrody- namic parameters of mechanical and bioprssthetic heart valves derived from Doppler and catheter mea- surements, both under steady and pulsatile flow con- ditions. Conclusion: This new flow model can be used to eval- uate the usefulness of hydrodynamic parameters for the assessment of prosthetic heart valves using both conventional Doppler echocardiography, as currently used in patients, and 3D color Doppler ultrasonic imaging. The Journal of Heart Valve Disease 1999;8:85-95 theses, the Doppler-derived TPG may substantially overestimate the catheter-derived TPG. This is due to the fact that the Doppler technique measures the maxi- mal velocity of the valve jet(s), and thus provides an estimate of maximal value of TPG (TPG,,,) rather than the net TPG. On the other hand, the catheter technique is generally used to record the net TPG, which takes into consideration the phenomenon of pressure recov- ery downstream of the valve (since net TPG = TPG,,, - pressure recovery) (14,16,18). The presence of multi- ple jets of different velocities downstream of mechani- cal valves also complicates the Doppler estimation of TPG, as the recording of the maximal velocity repre- sents only a part of total flow in the multiple jets. Doppler ultrasound assessrnent of the TPG and EOA of prosthetic valves is based on continuous-wave (CW) O Copyright by ICR Publishers 1999
Transcript of A new flow model for prosthetic heart valves · l ~a boratoire de génie biomédical, IRCM,...

A New Flow Mode1 for Doppler Ultrasound Study of Prosthetic Heart Va Louis-Gilles ~ u r a n d l , Damien Garcia1, Frederic Sakrl, Herkole Sava1, Richard Cimon1, Philippe ~ibarot l .~ , Aaron ~ e n s t e r ~ , Jean G. ~ u r n e s n i l ~
l ~a boratoire de génie biomédical, IRCM, Université de Mon tréal, p épar te men t de Cardiologie, Institut de Cardiologie de Quebec, Quebec and 31maging Research Laboratory, The John P. Robarts Research Institute, London, Ontario, Canada
Background and aim of the study: Steady and pulsatile flow models used to assess the hydrodynamic aspects of prosthetic heart valves are generally made of Plex- iglas and Lucite tubing. They often allow continuous- wave and pulsed-wave Doppler ultrasound velocity measurements to be made parallel to the flow, but cannot be used as such for ultrasound scanning of valve inflow and outflow velocities because of ultra- sonic reverberation and refraction by the tubing. The aim of the study was to develop a new flow model which allowed ultrasonic scanning of the prosthetic valve flow for three-dimensional(3D) reconstruction of color Doppler flow distributions. Metkods: The flow model, designed with left ventric- ular and aortic chambers composed of agar gel which mimics the ultrasound characteristics of biological tissues, was developed and tested for comparative in vitro hydrodynamic and Doppler ultrasonic studies of aortic prosthetic valves. An electromagnetic flowmeter and a pressure monitor provided the flow and pressure signals for the hydrodynamic tests. The Doppler ultrasonic evaluation was performed with an Ultramark 9 HDI ultrasound system and a 3D
The non-invasive clinical assessrnent of prosthetic heart valve function is mostly based on valve inflow and outflow velocity measurements by Doppler echocardiography to estimate the transvalvular pres- sure gradient (TPG) with the Bernoulli equation, and the valve effective orifice area (EOA) with the continu- ity equation (1-8). This approach, which is relatively accurate for the assessment of native and bioprosthetic heart valves, shows significant variability when used for mechanical valves, because of their complex flow velocity distributions and different valve designs. Sev- eral studies (4,9-17) showed that, in mechanical pros-
Address for correspondence: Louis-Gilles Durand MD, IRCM, 110 Avenue des Pins Ouest, Mon- treal, Quebec, Canada, H2W 17R
ultrasound imaging system. The model was designed to enable assessment of prosthetic valve performance by pulsed-wave and continuous-wave Doppler veloc- ity measurements, as well as by 3D color Doppler velocity measurements obtained by ultrasonic scan- ning of the left ventricle or aortic chamber with an ultrasound probe mounted on a motorized transla- tion assembly. Results: The study results showed that this new flow model can provide 3D color Doppler velocity distrib- utions as well as accurate comparisons of hydrody- namic parameters of mechanical and bioprssthetic heart valves derived from Doppler and catheter mea- surements, both under steady and pulsatile flow con- ditions. Conclusion: This new flow model can be used to eval- uate the usefulness of hydrodynamic parameters for the assessment of prosthetic heart valves using both conventional Doppler echocardiography, as currently used in patients, and 3D color Doppler ultrasonic imaging.
The Journal of Heart Valve Disease 1999;8:85-95
theses, the Doppler-derived TPG may substantially overestimate the catheter-derived TPG. This is due to the fact that the Doppler technique measures the maxi- mal velocity of the valve jet(s), and thus provides an estimate of maximal value of TPG (TPG,,,) rather than the net TPG. On the other hand, the catheter technique is generally used to record the net TPG, which takes into consideration the phenomenon of pressure recov- ery downstream of the valve (since net TPG = TPG,,, - pressure recovery) (14,16,18). The presence of multi- ple jets of different velocities downstream of mechani- cal valves also complicates the Doppler estimation of TPG, as the recording of the maximal velocity repre- sents only a part of total flow in the multiple jets.
Doppler ultrasound assessrnent of the TPG and EOA of prosthetic valves is based on continuous-wave (CW)
O Copyright by ICR Publishers 1999

86 L.-G. Durand et al. A new flow mode1 for prosthetic heart valves
J Heart Valve Dis Vol. 8. No. 1
January 1999
1 Pulsatile pump
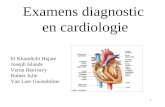
Figure 1: Schematic illustration of the flow mode1 system including the data acquisition system. The dashed lines represent the cable connections between the ultrasound probes (UP) and the Doppler ultrasound system, and between the motorized translation assem- bly W T A ) and the 3 0 ultrasound imaging system. Only one electromagnetic probe (probe #1 or probe #2) is connected to the elec-
tromagnetic flowmeter at a given time.
Doppler measurement of the maximal velocity in the prosthesis jet, pulsed-wave (PW) measurement of the left ventricular outflow tract (LVOT) velocity, and the estimation of the LVOT diameter using B-mode echocardiography (19). One of the main difficulties with this approach is that the velocity distribution is assumed to be spatially uniform in the LVOT and in the prosthesis jet, and that there is no pressure recovery downstream of the valve. These assumptions are not valid for mechanical prosthetic heart valves, as well as for stenotic native and bioprosthetic heart valves (10,19-21). The development of color Doppler echocar- diography has provided a new approach to obtain the velocity distributions in the cardiac chambers and ves- sels. However, few studies have been performed to determine the velocity distributions of the aortic valve by color Doppler ultrasound. For instance, the clinical studies of Zhou et al. (19), Rossvoll et al. (22) and Wiseth et al. (23) showed that it is possible to measure
the spatial velocity distributions across the LVOT in healthy individuals and in patients before and after aortic valve replacement. These three studies demon- strated that the flow velocity distributions in the LVOT were not uniform, but skewed, with the highest veloc- ity most often found near the anterior wall or the sep- ta1 section of the LVOT. In addition, the study of Wiseth et al. (23) showed that aortic valve replacement with a mechanical or bioprosthetic heart valve in patients with aortic stenosis does not change the veloc- ity profiles in the LVOT.
On the other hand, the in vitro study of Shandas et al. (24) was designed to evaluate the utility of 3D recon- struction of color Doppler images for accurate evalua- tion of the EOAs of valve orifices with various shapes and sizes under steady and pulsatile flows. The probe was aligned parallel to the flow and the 3D images were obtained by mechanical rotation of the ultrasonic probe along its central axis. The study showed that the

J Heart Valve Dis Vol. 8. No. 1 January 1999
La-G. Durand et al. 87 A new filow model for prosthetic heart valves
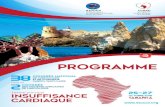
Figure 2: Photograph of the flow mode1 system, including the ATL ultrasound system (middle left) and the 3 0 Life lmaging system (far left). From left to right on the bench can be seen the reservoir, the Harvard pump, the flow model with the 3D positioning sys-
tem, the linear motor and the ultrasound transducer, and the aortic compliance. The electromagnetic flowmeter and the three-channel physiological monitor are on the top section of the bench, near the flow model. The computer is not shown in the picture.
EOAs estimated with 3D color Doppler ultrasound ventricular and aortic sections of the flow mode1 were were in good agreement with, but overestimated, the designed also to allow conventional CW and PW areas of the vena contracta as measured by laser flow Doppler velocity measurements parallel to the valve visualization. It was concluded that 3D Doppler ultra- flow. Examples of the results obtained from the testing sonic flow images can provide a superior format to of prosthetic heart valves in steady and pulsatile flows two-dimensional (2D) Doppler for quantitative and are presented. qualitative appreciation of the shape and dimensions of valve orifice jets.
The accuracy of the Doppler ultrasound technique used to assess the functionality of prosthetic heart valves, using parameters such as TPG and EOA, is gen- erally determined by comparison with the same para- meters derived from pressure and flow rate measure- ments. Most of these comparative studies are performed in steady flow models (25-27) and in pulse duplicator models able to simulate the physiological conditions of blood flow in the left ventricle and aorta (9,14,18,26,28,29). These steady and pulsatile flow models, which are generally made of Plexiglas and Lucite tubing, can be adapted to allow CW and PW Doppler velocity measurements. However, they often cannot be used as such for scanning of the valve inflow and outflow velocities by Doppler ultrasound because of ultrasonic reverberation and refraction due to the tubing.
The objective of the present project was to develop a left heart flow model allowing computer-controlled, motorized ultrasound scanning of the LVOT and aortic chamber with a 2D phase array or linear probe for 3D reconstruction of color Doppler inflow and outflow distributions of the prosthetic heart valves. The left
Materials and methods
Flow mode1 As shown in Figure 1, the flow model is composed of
a fluid reservoir, a modified pulsatile pump (Harvard, model 1421), an adjustable left ventricular compliance, a left ventricular chamber, an aortic prosthetic valve, an aortic chamber, a variable compliance chamber and an adjustable peripheral resistance. For steady flow studies, a variable speed, magnetically coupled cen- trifugal pump (Micropump Inc., model 75225-10) was used instead of the pulsatile pump. The blood-mimick- ing fluid was a solution of 10 1 of 70% saline and 30% glycerol (viscosity about 3.5 cP) to which 1 g/l of sodi- um azide (as fungicidal agent) and 10 g/l of cornstarch particles (the ultrasound scatterers) were added. The flow resistance and chamber compliances can be adjusted to simulate the flow waveform observed in the left ventricle and the aorta at physiologic pressures. Figure 2 illustrates the flow model, including the ATL ultrasound system (middle left) and the 3D ultrasound imaging system (far left).
The ventricular and aortic chambers of the left heart model are each composed of a Plexiglas box containing

88 L.-G. Durand et al. A new flow model for prosthetic k a r t valves
LEFT HEART MODEL
TOP VIEW
LEFT VENTRICLE AORTA
Figure 3: Top view of the structure of the left heart model. A W: Acoustic window for pulsed-wave and continuous-wave
Doppler measurements parallel to the valve axial flow; IC: Inflow connector; LVOT: Left ventricular outflow tract; OC:
Outflow connector. I an agar gel which mimics the ultrasound acoustic
properties of biological tissues. This gel was composed of 86% distilled water, 8% glycerol, 3% agar, 3% 50 Fm cellulose and 1 g/l sodium azide. The inner chambers of the left ventricle and aorta were formed by inserting a Plexiglas mold in the center of each box and by pour- ing the molten agar gel around the molds, which were removed after about 12 h, when the gel had set (30,31). To protect the structural integrity of the agar gel and enable 3D Doppler ultrasound scanning of the prosthe- sis inflow and outflow over a long distance, a high-den- sity polyethylene plate (McMaster-Carr) was used to make the top wall of each chamber. High-density poly-
1 ethylene was used because it had an acoustic imped- I
ance similar to that of the agar gel and did not produce signifiant refraction or reverberation of the ultra- sound beam. The left ventricular section was similar to the aortic section but had a shorter length. Each mold was made of a cylindrical tube and trapezoidal block of Plexiglas.
The LVOT and ascending aorta were modeled with cylindrical chambers each having a diameter of 2.54 cm. The trapezoidal blocks were used to allow splitting of the left ventricular and aortic flows on the lateral sides of two central acoustic windows (one for the left ventricular section and one for the aortic section). This allowed PW and CW Doppler flow velocity measure- ments parallel to the central flow axis of the model. The central acoustic window of the aortic section is the white rectangle between the outflow tubes of the model in Figure 2. Figure 3 is a top view of the left heart model showing more clearly the geometry of its inflow and outflow sections. The Doppler acoustic windows of the left ventricular and aortic sections were made by cutting a rectangular aperture in the Plexiglas wall
J Heart Valve Dis Vol. 8. No. 1
January 1999
St-Jude HP 2 1 mm
Distance from the valve ring (mm)
Figure 4: Example of the distribution of the transvalvular pressure gradient (TPG) as a function of the flow rate and the axial position of the catheter measurement downstream of a 21-mm St. Jude Medical bileaflet valve. The measurements
were repeated three times for each of the following steady flow rates: 5.4,8.8,12.2,15.6,19.0,22.4 and 25.8 llmin. (lower curve to upper curve). The symbol 'x' represents the mean
value; the vertical bar represents the SD of each measurement.
between the two flow connectors of each section, which were then replaced by polyethylene plates. The centers of both windows were aligned with the longitudinal axis of the flow model. A set of two hard rubber mount- ing plates cut to fit the sewing ring of each prosthetic valve tested was used to insert a prosthesis between the left ventricular and aortic chambers.
To simulate the cardiac output generally observed in patients at rest and during exercise, the 30-ml head assembly of the Harvard pump model 1421, which has a maximum rate of 200 strokes/min, was replaced by the 100-ml pumping head assembly of the Harvard pump model 1423, which has a maximum rate of 100 strokes/min. In addition, the restrictive inflow ball valve of the head assembly was replaced by a 27-mm bileaflet valve (model 27A-101, St. Jude Medical) and the outflow ball valve was removed. The cross-section- al areas of the input and output flow connectors of the transparent acrylic head chamber of the pump were increased from 1.27 cm2 (diameter 1.27 cm) to 4.12 cm2 (diameter 2.29 cm) to reduce significantly the flow resistance within the pump head assembly at high flow rates. This modified pump can thus provide a stroke volume which is adjustable between 15 and 100 ml, a rate adjustable between 20 and 200 beats/min, and a systole/diastole ratio variable between 35% and 50%. The theoretical maximum blood flow volume capacity of the pump is thus 20 l/rnin.

J Heart Valve Dis Vol. 8. No. 1 January 1999
L.-G. Durand et al. 89 A newjlow model for prosthetic heart valves
y = 0.06 + 0.94 x
SEE = 0.06 cm2
TPG,,, Catheter (mmHg) EOA Catheter (cm2)
Figure 5: Xelationship between Doppler-derived and catheter-derived TPG,,,,, ( a ) and EOA (b) obtained for three Medtronic Mosaic (21 -25mm), four Medtronic Intact (19-25 mm), and four S t . Jude Medical bileaflet (19-25 mm) valves. The study was performed
under continuousflow. The symbols A, U and @ represent values corresponding to the Medtronic Mosaic, Medtronic Intact and S t . Jude Medical valves, respectively. EOA: Eflective orifice area; TPG,,,: Maximal value of transvalvular pressure gradient.
Hydrodynamic measurements An electromagnetic flowmeter (Cliniflow II, Caroli-
na Medical Electronics, Inc.) coupled to a physiologic monitor (Escort E102, Medical Data Electronics) served to monitor the left ventricular or aortic flow waveform and display the mean flow rate in l / min. An electro- magnetic probe (model ÇF-680), calibrated for a range of O to 20 l/min, was used for pulsatile-flow measure- ments, while a second one, calibrated for a range of O to 40 l/min, was used for steady-flow measurements. Two fluid-filled, side-hole catheters were inserted through ports in the left ventricular and aortic cham- bers to record simultaneously the pressure on each side of the valve, using disposable transducers (Namic, model Perceptor DT)(14). The physiologic monitor was modified to transfer the output signals of the left ven- tricular and aortic pressures to a computer. The two pressure signals and electromagnetic flowmeter signal were digitized with 12-bit resolution by a 4-channel data acquisition board (Data Translation DT2828A) installed in the computer. A C-language program was written to digitize, average and display the signals; the digitized signals were then processed by Matlab soft- ware (Math Works, Inc.). For steady flow experiments, the program computed estimates of the mean values of the flow rate, left ventricular and aortic pressures and TPG over a period of 5 S. For pulsatile flow experi- ments, the program performed a coherent averaging of the signals for 10 cycles and computed the systolic, mean and diastolic pressures in the left ventricle and in the aorta, and the peak and mean values of TPG and flow rate.
The sensitivity of each pressure transducer was ini- tially pre-calibrated using a standard mercury sphyg-
momanometer and the resulting value (0.0190 + 0.0003 V/mmHg) entered into the computer program. The catheters were then inserted into the flow model, with both side-hole catheters positioned at the same location within the left ventricular chamber. The magnetically coupled centrifuga1 pump was then started while the valve of the flow resistance of the model was closed, and the pressure increased to 100 mmHg at zero flow. The value of the sensitivity of the aortic pressure trans- ducer was then slightly increased or decreased (<0.0003 VlmmHg) until the difference between the two catheter pressure measurements displayed by the computer program was <+.0.25 mmHg. This fine-tun- ing procedure ensured that the sensitivities of the two pressure transducers were optimally matched.
Doppler dtrasound and 3D volumetrie imaging In the present study, the Doppler velocity measure-
ments were performed by using an ATL (Advanced Technology Laboratories) Ultramark 9 HDI system. For CW Doppler measurements parallel to the flow, a 2-MHz phase array transducer (model P3-2) was mounted on a manually adjustable horizontal assem- bly aligned with the valve flow. The maximal jet veloc- ity downstream of the valve was found by aligning the beam of the CW Doppler transducer with the aortic flow axis until the highest Doppler frequency was recorded. Ultrasound gel was used to couple the trans- ducer to the central acoustic window of the aortic chamber.
The 3D reconstruction of the Doppler velocity profile in the aortic chamber under steady flow was per- formed with a 3D ultrasound imaging system (Life Imaging Çystems Inc., London, Ontario, Canada)

90 La-G. Durand et al. A new flow model for prosthetic heart valves
J Heart Valve Dis Vol. 8. No. 1
January 1999
Time (s)
O 0. 5 1 1.5 2 2.5 Time ( s )
Figure 6: Examples of left ventricular (LVP) and aortic (AP) pressures, transvalvular pressure gradient (TPG), and flow
rate recorded in the flow model under pulsatile flow. A Medtronic Intact bioprosthesis was used. The stroke rate was 72 beatslmin, stroke volume 75 ml, systolic flow rate 230 mlls, mean flow rate 5.5 Ilmin and mean systolic TPG 32 mmHg.
developed by one of the authors (A.F.) using a Macin- tosh computer (Mode1 7500). A 4-MHz linear array transducer (model L4-7) was mounted on a computer- ized motor-driven translation assembly with an angle of 70" with the flow axis. This translation assembly was fixed to a 3D (x, y, z) manual positioning system using linear unislide assemblies (Velmex, Inc.) which was itself fixed to the Plexiglas base of the aortic section (see Figs. 1 and 2). This manual positioning system allowed accurate positioning of the ultrasound transducer above the top acoustic window of the aortic section. Acquisition of 150-200 parallel 2D color Doppler images transverse to the aortic flow was then per- formed by translating the probe over a distance of 7.5- 10 cm on the top acoustic window of the aortic section, using a displacement of 0.50 mm between each image acquisition. Water was used to couple the transducer to the top acoustic window. Scanning began approxi- mately 1 cm downstream of the valve ring position. For each flow rate tested, a 3D flow image was captured by the 3D ultrasound imaging system using an $-bit ana- log-to-digital converter. The angle was then compen- sated to recover the correct geometry and flow veloci- ty. Then, the 3D volume was rescaled using the pre-calibrated voxel dimensions of the specific zoom and focus distance utilized. The time required to per- form data acquisition and 3D reconstruction of each flow volume was about 3 min.
Test protoc~l To provide examples of the results obtained with this
new flow model system, a series of Medtronic Intact
l y = -0.52 + 1 .O6 x r = 0.99 SEE = 1.90 mmHg
O 1 O 20 30 40 50 60
TPG,,, Catheter (mmHg)
Figure 7: Relationship between Doppler-derived and catheter- derived TPG,,, obtained under pulsatile flow for three
Medtronic Mosaic (21 -25mm) and four Medtronic Intact (1 9- 25 mm) valves. The symbols A and LI represent values corre- sponding to the Medtronic Mosaic and Intact valves, respec-
tively. TPG,,,: Maximal value of transvalvular pressure gradient.
and Mosaic bioprosthetic valves and St. Jude Medical bileaflet prosthetic valves (19-25 mm) were tested in the aortic position of the left heart model. The bileaflet valves were inserted such that the two leaflets were aligned parallel to gravity. A reference procedure allowing determination of the relative position of the two side-holes of each catheter upstream or down- stream of the prosthetic heart valve was irnplemented before performing the hydrodynamic tests. For each valve tested, the left ventricular catheter was posi- tioned so that its two side-holes were located in a region of uniform pressure, between 1 and 2 cm before the valve (before the region of flow convergence). To obtain an estimate of the distribution of the TPG of the valve as a function of the recording position down- stream of the valve, the aortic catheter was positioned at 12 different locations distal to the entrance of the valve, to cover a distance of 100 mm. The first pressure measurement location (distance 0) corresponde~,to the plane parallel to the inflow surface of the prosthesis. The 11 other measurement locations were at 2.5, 5.0, 7.5,10,15,20,30,40,60,80 and 100 mm downstream of the first.
In steady flow, the measurements were performed under the following flow rates: 5.4,8.8,12.2,15.6, 19.0, 22.4 and 25.8 l/min. In pulsatile flow, the measure- ments were performed under the following stroke vol- umes: 55, 65 and 75 ml. The pulse rate was approxi- mately 72 beats/min and the ejection time ranged from 250 to 350 ms. Cardiac output ranged from 3.7 to 5.6 l/min. For each experiment, the left ventricular and aortic pressure signals, and the instantaneous and

J Heart Valve Dis Vol. 8. No. 1 January 1999
L.-G. Durand et al. 93 A n e w flow model for prosthetic heart valves
mean electromagnetic flow rate signals were recorded simultaneously by the computer. Each experiment was repeated three times and the mean and SD of the pres- sure and flow measurements were computed. In steady flow, the aortic pressure was maintained between 50 and 120 mmHg. In pulsatile flow, the sys- tolic aortic pressure was maintained between 80 and 180 mmHg and the diastolic pressure between 50 and 120 mmHg. Since the pressure and flow rate measure- ments were reproducible, the recordings of the CW Doppler signals or sets of 2D color Doppler images were not performed simultaneously with the hydrody- namic measurements.
The digitized signals of the left ventricular and aortic pressures, flow rate and CW Doppler velocity were analyzed numerically to obtain the catheter-derived estimates of TPG,,, and EOA, as well as the Doppler- derived estimates of these parameters. The catheter- derived TPG signals were obtained by subtracting the aortic pressure signal from the left ventricular pressure signal. For steady flow, averaging was performed over 5 s, while for pulsatile flow the averaged TPG signal of 10 cycles was computed. For steady flow, TPG,,, was defined as the maximal value of the averaged TPG, while for pulsatile flow it was defined as the maximal value of the peak systolic TPG, both recorded down- stream of the valve. The Doppler-derived values of TPG,,, were obtained using the Bernoulli equation with the inclusion of the inflow velocity: TPG,,, = 4.0 (V2,, - V2,), where V,, and V, are the velocities record- ed in the central jet (the vena contracta) and in the LVOT, respectively. For steady flow, the CW Doppler signal was processed by a fast Fourier transform algo- rithm to generate the flow velocity distribution from which Vvc was extracted by the computer program and averaged over an interval of 5 S. V, was obtained by dividing the mean flow rate in ml/s (measured by the electromagnetic flowmeter) by the cross-sectional area
of the LVOT. For pulsatile flow, TPG,,, was computed using Vvc and V, measured at peak systole, since flow acceleration can be assumed to be negligible.
In the present study, the EOA was computed only for steady flow using averaged values obtained over 5 S. The Doppler-derived values of EOA were estimated using the continuity equation: EOA = A,V,/V,,, where A, is the cross-sectional area of the LVOT. In a previous study, we demonstrated that the continuity equation was more accurate than the Gorlin equation in deter- mining the catheter-derived values of EOA of aortic prosthetic valves (5). Consequently, catheter-derived values of the valve EOA were obtained by processing the TPG, the cross-sectional area of the LVOT (A,) and the flow rate (Q) with a combination of the continuity and Bernoulli equations:
where K = 2540. When Q2 << K A2, TPG,,,, this equation is reduced
to: EOA = Q/50.4 (TPGm,x)0.5 (5). Since one important objective of this study was to
demonstrate the validity and usefulness of the flow model, the test protocol was designed to measure valve parameters that can be accurately estimated by both Doppler and catheter: TPG,,, and EOA based on TPG,,, for the catheter estimate. The relationships between the Doppler and catheter estimates of TPG,,, and EOA were then determined by using a linear regression analysis.
For 3D color Doppler volumetric imaging, the main difficulty encountered was the optimal setting of the ultrasound instrument. Since the maximal flow velocities are generated very close to the valve, the first 2D color image obtained when the ultrasound transducer was located at the nearest position downstream of the valve was used to determine the maximum velocity scale of the
Table 1: Reproducibility of the flow ~ a t e and pyessure measurements for different flow rates.'
Flow rate Left ventricular pressure Aortic pressure Transvalvular pressure gradient (1 /min) (mmHg) (mrnHg) (mmHg)
Mean values 91.1 + 0.28 67.9 + 0.26 23.2 + 0.21 --
Values are expressed as mean + SD from 12 consecutive measurements.

92 L.-G. Durand et al. A new flow model for prosthetic heart valves
J Heart Valve Dis Vol. 8. No. 1
January 1999
Figure 8: Example of the average 3 0 color velocity distribu- tion obtained from a 23-mm St. Jude Medical bileaflet valve at a steady flow rate of 19 llmin. The dimensions of the 3 D vol- ume are 3 x 3 x 7.5 cm and the maximal velocity (bright yel-
low jets) is 2 mls.
color map. The maximal velocities determined by CW Doppler measurements were also utilized during this step. The optimal adjustment of the color gain was per- formed with the ultrasound transducer located at the far- thest position from the valve. During this step, the color gain was adjusted such that the forward flow color image corresponded to the full cross-sectional area of the aortic flow section. Since the 3D ultrasound imaging system was designed to grab black-and-white images, the B- mode was turned off and a gray-scale velocity map used to digitize the 2D color flow images. This calibration pro- cedure was repeated for each valve and for each flow rate tested in order to avoid color aliasing and to optimize the setting of the ultrasound instrument. More details on the optimal setting of the ultrasound instrument are avail- able elsewhere (32).
Table I shows the reproducibility of the catheter mea- surements of the TPG, left ventricular and aortic pres- sures and electromagnetic flow rate, as a function of steady flow rate. The reproducibility was expressed by computing the standard deviation (ÇD) of the mean values of the flow and pressure measurements obtained from 12 consecutive recordings, each having a duration of 20 S. The procedure was repeated for eight different flow rates, as shown in Sable I. A 25-mm aortic Medtronic Intact bioprosthetic heart valve was inserted in the left heart model. The aortic measure-
Figure 9: Examples of the averaging of the first 50 2 0 color images recorded downstream of ( a ) a 23-mm St. Jude Medical valve and (b) a 25 mm Medtronic Intact bioprosthesis. Verti-
cal (velocity) scale is in cmls; dimension scales are in mm.
ment was performed 30 mm downstream of the entrance of the Intact prosthesis. The results show that both the flow and pressure measurements were highly reproducible, the ÇD being very srnall compared with the mean values. They were independent of the pres- sure level with a mean value of 0.28 mmHg for left ven- tricular pressure, 0.26 mxnHg for aortic pressure and 0.21 mmHg for the TPG. The ÇD of the flow rate mea- surements was proportional to the flow rate with a mean normalized value (ÇD/mean) of 0.40%.
An example of the distribution of TPG as a function of steady flow rate and the axial position of the catheter

J Heart Valve Dis Vol. 8. No. 1 January 1999
L.-G. Durand et al. 93 A new flow model for prosthetic heart valves
measurement downstream of a 21-mm St. Jude Medical bileaflet valve is shown in Figure 4. This figure demon- strates that TPG,, was recorded within the first 10 mm of the entrance plane of the valve ring (distance O). Fur- ther downstream, the pressure decreases rapidly, as an important part of the kinetic energy of the central jet is converted into potential energy, thus increasing the downstream pressure and decreasing the TPG. This is a typical example of the phenomenon of pressure recov- ery. The valve's net TPG can be observed at 60 mm.
The relationships obtained between the Doppler- derived and catheter-derived TPG,,, and EOA for the Medtronic and St. Jude Medical valves tested are shown in Figure 5a and b, respectively. It is clear from this figure that the Doppler-derived TPG,,, and EOA under steady flow are in very good agreement with those derived by catheter (r >O.99). According to Figure 4, the Doppler-derived values of TPG,,, significantly overestimate the net TPG recorded by catheter 260 mm downstream of the bileaflet valve.
Figure 6 demonstrates that the flow model can also provide pressure and flow signals similar to those found in humans at a mean flow rate of 5.5 l/min. The TPG was computed only when the left ventricular pres- sure was higher than the aortic pressure. The negative left ventricular pressure observed in early diastole is due to the vacuum produced by the Harvard pump during filling of its piston chamber. Figure 7 shows the relationships obtained between the Doppler-derived and catheter-derived TPG,,, under pulsatile flow. The data were obtained for Medtronic Intact and Mosaic bioprosthetic heart valves.
An example of the 3D color flow velocity distribution obtained from a 19-mm bileaflet St. Jude Medical aortic valve at a steady flow rate of 19 l/min is shown in Figure 8. The transvalvular pressure gradient measured between the ventricular pressure recorded 2 cm upstream of the valve and the aortic pressure recorded 2 cm downstream of the valve was 15 mmHg. This 3D volumetric image was obtained by averaging five 3D color flow velocity dis- tributions generated by repeating the scanning of the aor- tic section of the flow model five times. The 3D imaging software allows the user to rotate interactively the 3D image and cut it in any arbitrary plane. Figure 8 shows a longitudinal cut in a plane located slightly inside the right lateral jet of the valve. The two lateral velocity jets at the beginning of the 3D image can be clearly seen. The central jet is not visible on this image since it had probably diverged and merged with one of the two lateral jets at this level. The longitudinal cut shows that the lateral jet velocity decreases in the distal region of the aorta such that the flow velocity becomes much more uniform towards the end of the 3D flow volume.
Figure 9a and b are examples of the velocity distrib- utions obtained by averaging the first 50 2D color
images recorded downstream of a 23-mm Çt, Jude Medical bileaflet valve (flow 15.6 l/min) and a 25-mm Intact bioprosthesis (flow 8.8 l/min), respectively. The flow distribution of the bileaflet valve shows that, at this position, the central jet has diverged and is com- bined with the two lateral jets. The flow distribution of the bioprosthesis has the basic characteristics (central flow with a triangular configuration) of the flow distri- bution observed in a native aortic valve.
Discussion
In the present study we have shown that it is possible to design a left heart flow model made of an ultrasound tissue mimic (agar gel), Plexiglas and polyethylene that can be used to perform studies of prosthetic heart valves under both steady and pulsatile flows. Results obtained with this new flow model, as shown in Fig- ures 5-9, demonstrate that it can provide 31) color Doppler flow velocity distributions as well as accurate comparisons of hydrodynamic parameters of prosthet- ic heart valve such as TPG,,, and EOA derived from Doppler and catheter measurements. This flow model is different and more versatile than the model of valvu- lar disease developed by Shandas et al. (24) for in vitro flow studies of various shapes and sizes of aortic steno- sis since it can be used for linear, fan and rotational scannings of the aortic valve inflow and outflow, as described previously (33).
This flow model is presently used to evaluate the usefulness of more appropriate hydrodynamic para- meters of bileaflet mechanical heart valves (such as the net TPG) that can be directly and accurately estimated by Doppler ultrasound measurements. We hope that it will also allow a better understanding of the relation- ships between the parameters used to assess prosthetic valve function non-invasively, and those used for the in vitro hydrodynamic evaluation of the valves, and subsequently provide new information allowing a more accurate Doppler ultrasound assessrnent of pros- thetic heart valves implanted in patients.
The main limitation found with this flow model was the difficulty in the adjustment of compliances of the left ventricular and aortic sections in order to obtain physiologic waveforms at high flow rates (>6 l/min). One approach to reduce this limitation would be to develop a compter-based servo-control of the left ven- tricular pressure using a digitized left ventricular pres- sure template and a linear power driver for the pump. Similarly, the aortic pressure of the model could be servo-controlled using a computer-driven electro- mechanical piston in the aortic section and a digitized aortic pressure ternplate. Acknowledgements
The authors are indebted to the Medical Research

94 L. -6 . Durand et al. A new flow model for prosthetic heart valves
J Heart Valve Dis Vol. 8. No. 1
January 1999
Council of Canada which supported this work (MA- 10929). Many thanks also to Dr. Helen Routh, Advanced Technology Laboratories for loaning the Ultramark 9 HDI system, to Life Imaging Systems Inc. for providing a free copy of the 3D ultrasound imaging software, and to St. Jude Medical and Medtronic for providing the replacement heart valves.
References 1. Hatle L, Angelsen BAJ, Tromsd A. Non-invasive
assessment of aortic stenosis by Doppler ultrasound. Br Heart J 1980;43:284-292
2. Skjaerpe T, Hegrenaes L, Hatle L. Noninvasive esti- mation of valve area in patients with aortic stenosis by Doppler ultrasound and two-dimensional echocar- diography. Circulation 1985;7:810-818
3. Rothbart RM, Castriz JL, Harding LV, Russo CD, Teague SM. Determination of aortic valve area by two-dimensional and Doppler echocardiography in patients with normal and stenotic bioprosthetic valves. J Am Coll Cardiol 1990;15:817-824
4. Chafizadeh ER, Zoghbi WA. Doppler echocardio- graphic assessment of the St. Jude Medical prosthetic valve in the aortic position using the continuity equa- tion. Circulation 1991;83:213-223
5. Dumesnil JG, Yoganathan AP. Theoretical and practi- cal differences between the Gorlin formula and the continuity equation for calculating aortic and mitral valve areas. Am J Cardiol1991;67:1268-1272
6. Dumesnil JG, Honos GN, Lemieux M, Beauchemin J. Validation and applications of indexed aortic pros- thetic valve areas calculated by Doppler echocardiog- raphy. J Am Coll Cardiol1990;16:637-643
7. Pibarot P, Honos GN, Durand LG, Dumesnil JG. Sub- stitution of left ventricular outflow tract diameter with prosthesis size is inadequate for calculation of the aortic prosthetic valve area by the continuity equation. J Am Soc Echocardiogr 1995;8:511-17
8. Dumesnil JG, Honos GN, Lemieux M, Beauchemin J. Validation and applications of mitral prosthetic valvular areas calculated by Doppler echocardiogra- phy. Am J Cardiol1990;65:1443-1448
9. Walker PG, Yoganathan AP. In vitro pulsatile flow hemodynamics of five mechanical aortic heart valve prostheses. Eur J Cardiothorac Surg 1992;6(suppl.I):S113-SI23
10. Khan SS. Assessment of prosthetic valve hemody- namics by Doppler: Lessons from in vitro studies of the St. Jude valve. J Heart Valve Dis 1993;2:183-193
11. Flachskampf FA, Weyman AE, Guerrero JL, Thomas JD. Influence of orifice geometry and flow rate on effective valve area: An in vitro study. J Am Coll Car- di01 1990;15:1173-1180
12. Baumgartner H, Khan SS, DeRobertis M, Czer LS, Maurer G. Effect of prosthetic aortic valve design on
the Doppler-catheter gradient correlation: An in vitro study of normal St. Jude, Medtronic-Hall, Starr- Edwards and Hancock valves. J Am Coll Cardiol 1992;19:324-332
13. Voelker W, Reul H, Stelzer T, Schmidt A, Karsch KR. Pressure recovery in aortic stenosis: An in vitro study in a pulsatile flow model. J Am Coll Cardiol 1992;20:1585-1593
14. Baumgartner H, Khan SS, DeRobertis M, Czer LS, Maurer G. Discrepancies between Doppler and catheter gradients in aortic prosthetic valves in vitro. A manifestation of localized gradients and pressure recovery. Circulation 1990;82:1467-1475
15. Baumgartner H, Khan SS, DeRobertis M, Czer LS, Maurer G. Doppler assessment of prosthetic valve ori- fice area. An in vitro study. Circulation 1992;85:2275- 2283
16. Vandervoort PM, Greenberg NL, Pu M, Powell KA, Cosgrove DM, Thomas JD. Pressure recovery in bileaflet heart valve prostheses. Localized high veloc- ities and gradients in central and side orifices with implications for Doppler-catheter gradient relation in aortic and mitral position. Circulation 1995;92:3464- 3472
17. Geibel A, Kasper W, Fraedrich G, Konstantinides S, Schollhorn J, Tiede N, Just H. Limitation der Doppler- echokardiographie in der Beurteilung von aorten- klappenprothesen. Z Kardiol1993;82:175-180
18. Niederberger J, Schima H, Maurer G, Baumgartner H. Importance of pressure recovery for the assessment of aortic stenosis by Doppler Ultrasound. Role of aortic size, aortic valve area, and direction of the stenotic jet in vitro. Circulation 1996;94:1934-1940
19. Zhou YQ, Faerestrand S, Matre K, Birkeland S. Veloc- ity distributions in the left ventricular outflow tract and the aortic anulus measured with Doppler colour flow mapping in normal subjects. Eur Heart J 1993;14:1179-1188
20. Gutfinger D, Sklansky J. Robust classifiers by mixed adaptation. IEEE Trans Pattern Analysis Machine Intelligence 1991;13:552-567
21. Henneke KH, Pongratz G, Bachmann K. Limitations of Doppler echocardiography in the assessment of prosthetic valve hemodynamics. J Heart Valve Dis 1995;4: 18-25
22. Rossvoll O, Samstad S, Torp HG, Linker DT, Skjaerpe T, Angelsen BAJ, Hatle L. The velocity distribution in the aortic anulus in normal subjects: A quantitative analysis of two-dimensional Doppler flow maps. J Am Soc Echocardiogr 1991;4:367-378
23. Wiseth R, Samstad S, Rossvoll O, Torp HG, Skjaerpe T, Hatle L. Cross-sectional left ventricular outflow tract velocities before and after aortic valve replace- ment: A comparative study with two-dimensional Doppler ultrasound. J Am Soc Echocardiogr

J Heart Valve Dis Vol. 8. No. 1 January 1999
1993;6:279-285 24. Shandas R, DeGroff CG, Kwon J, Trujillo N, Gill EA,
Valdes-Cruz L. Utility of three-dimensional ultra- sound Doppler flow reconstruction of the proximal jet to quantify effective orifice area: In vitro steady and pulsatile flow studies. J Am Soc Echocardiogr 1998;11:313-321
25. Law YF, Johnston KW, Routh HF, Cobbold RÇC. On the design and evaluation of a steady flow mode1 for Doppler ultrasound studies. Ultrasound Med Biol 1989;15:505-516
26. Yoganathan AP, Corcoran WH, Harrison EC. Pres- sure drops across prosthetic aortic heart valves under steady and pulsatile flow. In vitro measurements. J Biomech 1979;12:153-164
27. Liu H, Winoto SH, Shah DA. Velocity measurements within confined turbulent jets: Application to cardio- vascular regurgitation. Ann Biomed Eng 1997;22:939- 948
28. Arabia FA, Talbot TL, Stewart SFC, Nast EP, Clark RE. A computerized physiologic pulse duplicator for in vitro hydrodynamic and ultrasonic studies of pros-
L.-G. Durand et al. 95 A new flow mode1 for prosthetic heart valves
thetic heart valves. Biomed Instrument Technol 1989;23:205-215
29. Schima H, Baumgartner H, Spitaler F, Kuhn P, Wolner E. A modular mock circulation for hydrornechanical studies on valves, stenoses, vascular grafts and car- diac assist devices. Int J Artif Organs 1992;15:417-421
30. Guo Z, Durand LG, Allard L, Cloutier G, Fenster A. In vitro evaluation of multiple arterial stenoses using three-dimensional power Doppler angiography. J Vasc Surg 1998;27:681-688
31. Guo Z, Boughner DR, Dietrich JM, Pflugfelder PW, Durand LG, Fenster A. Quantitative assessment of in vitro jets based on three-dimensional color Doppler reconstruction. Ultrasound Med Biol 1998; xxxxx
32. Sava H, Pibarot P, Dumesnil JG, Fenster A, Durand LG. A 3D colour Doppler ultrasound imaging system for in vitro estimation of flow parameters down- stream of prosthetic heart valves. 20th Annual Inter- national Conference IEEE-EMBS 1998. In press
33. Fenster A, Downey DB. 3-D ultrasound imaging: A review. IEEE Eng Med Biol Magazine 1996;15:41-51