Tout ce que vous devez savoir sur l’intubation en …€¦ · OXYGENATION Doit toujours être la...
77
Tout ce que vous devez savoir Tout ce que vous devez savoir sur l sur l ’ ’ intubation en r intubation en r é é animation animation NANCY, mercredi 25 novembre 2009 Pr Samir JABER Service d’Anesthésie-Réanimation B (SAR B) INSERM ERI 25 – Université Montpellier I Hôpital Saint-Eloi; CHU Montpellier 34295
Transcript of Tout ce que vous devez savoir sur l’intubation en …€¦ · OXYGENATION Doit toujours être la...
Tout ce que vous devez savoir Tout ce que vous devez savoir sur lsur l’’intubation en rintubation en rééanimationanimation
NANCY, mercredi 25 novembre 2009
Pr Samir JABERService d’Anesthésie-Réanimation B (SAR B)
INSERM ERI 25 – Université Montpellier IHôpital Saint-Eloi; CHU Montpellier 34295
Question 1 (en réanimation)
Est-ce que l’intubation est plus difficile ou est-ce le patient qui
est difficile ? Ou les deux ?
Question 2
Comment amComment amééliorer les liorer les conditions de lconditions de l’’intubation intubation
en ren rééanimation ?animation ?
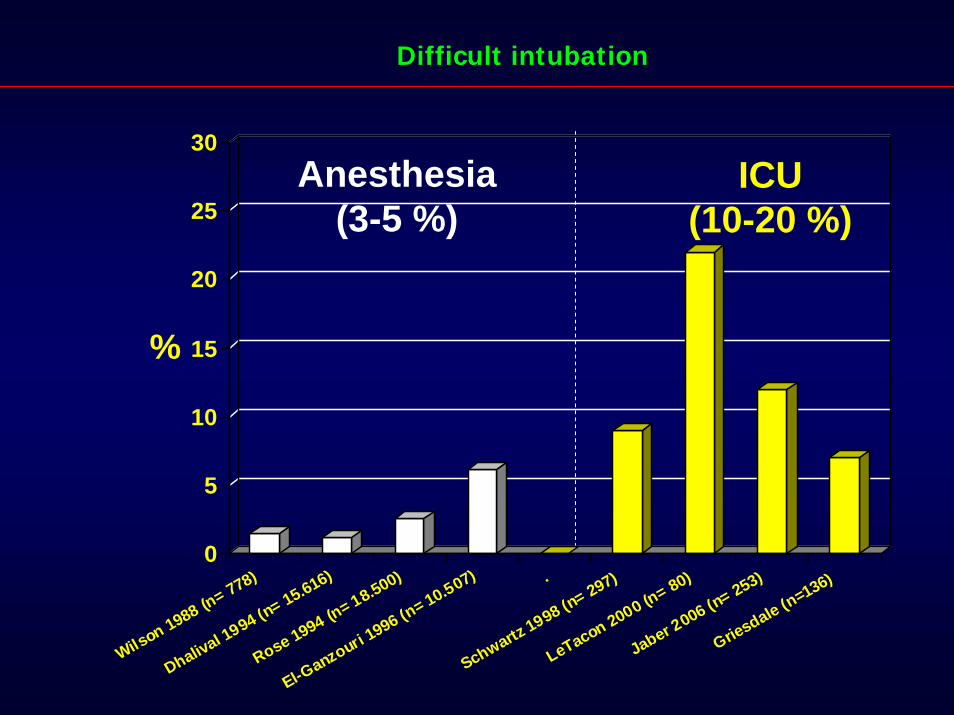
Difficult intubation
ICU(10-20 %)
Anesthesia(3-5 %)
0
5
10
15
20
25
30
%
Wilson 1988 (n= 778)
Dhalival 1994 (n= 15.616)
Rose 1994 (n= 18.500)
El-Ganzouri 1
996 (n= 10.507) .
Schwartz 1998 (n= 297)
LeTacon 2000 (n= 80)
Jaber 2006 (n= 253)
Griesdale (n=136)

Difficult Intubation
intubation difficile (can not intubate)
Ventilation difficile(can not ventilate)
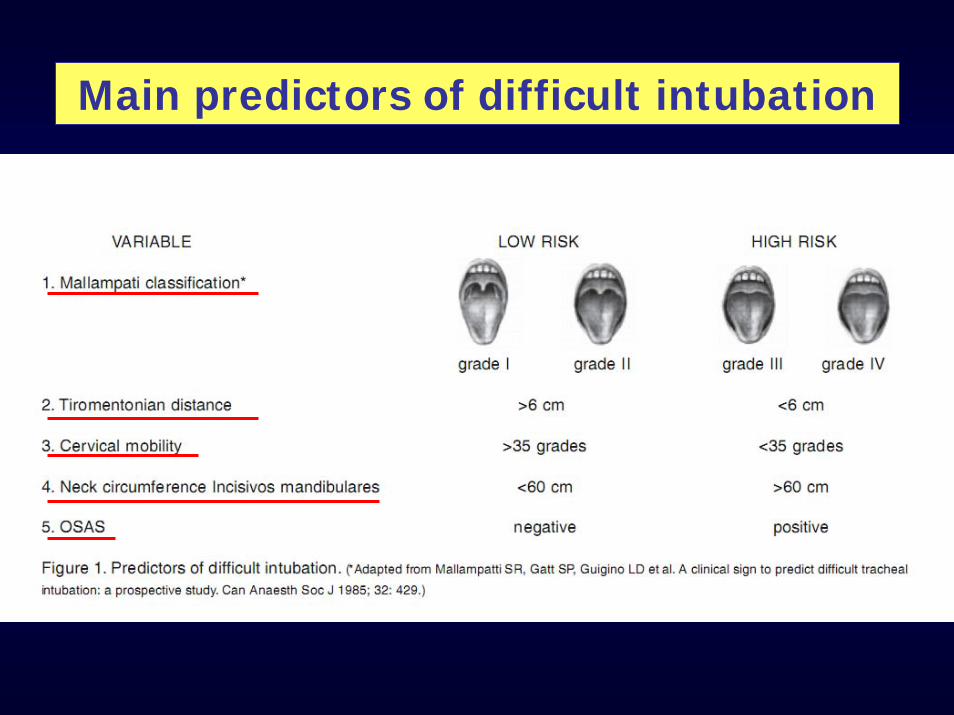
Main predictors of difficult intubation
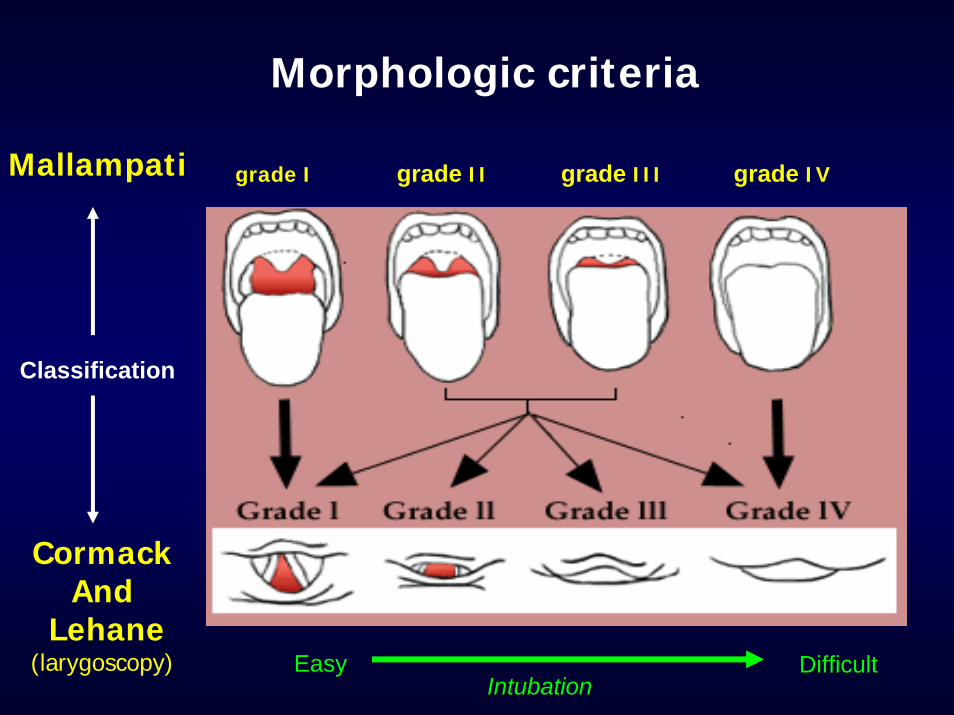
grade I grade II grade III grade IVMallampati
Cormack And
Lehane(larygoscopy)
Morphologic criteria
Classification
Easy DifficultIntubationIntubation
1. Assurer une bonneOXYGENATION OXYGENATION
Doit toujours être la priorité
2. Appeler de l’aide +++
En cas D’intubation difficile
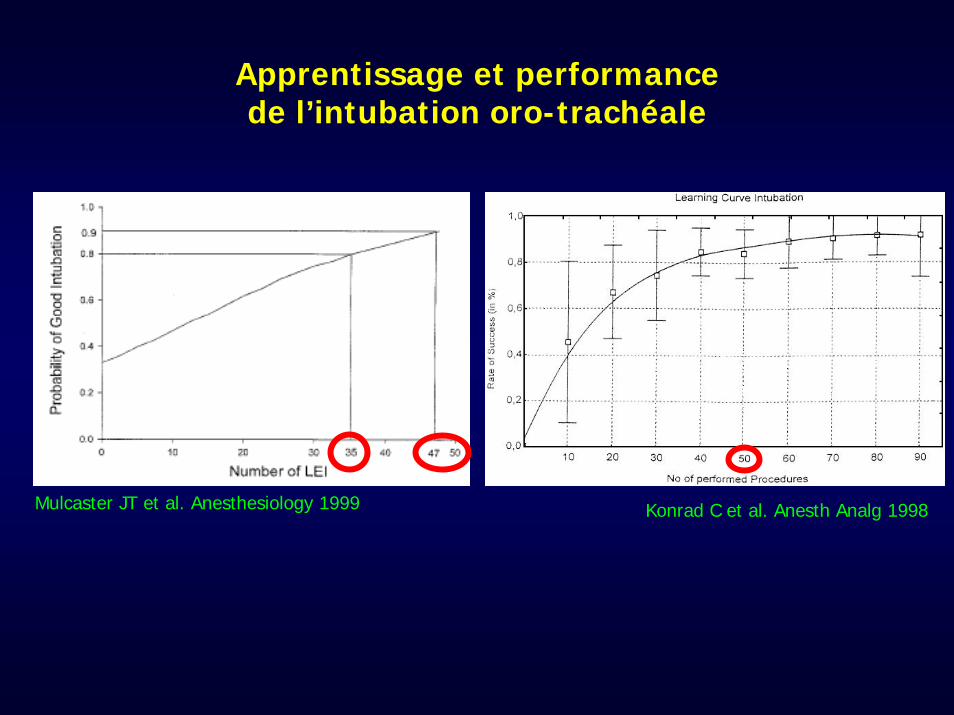
Apprentissage et performance de l’intubation oro-trachéale
Mulcaster JT et al. Anesthesiology 1999 Konrad C et al. Anesth Analg 1998
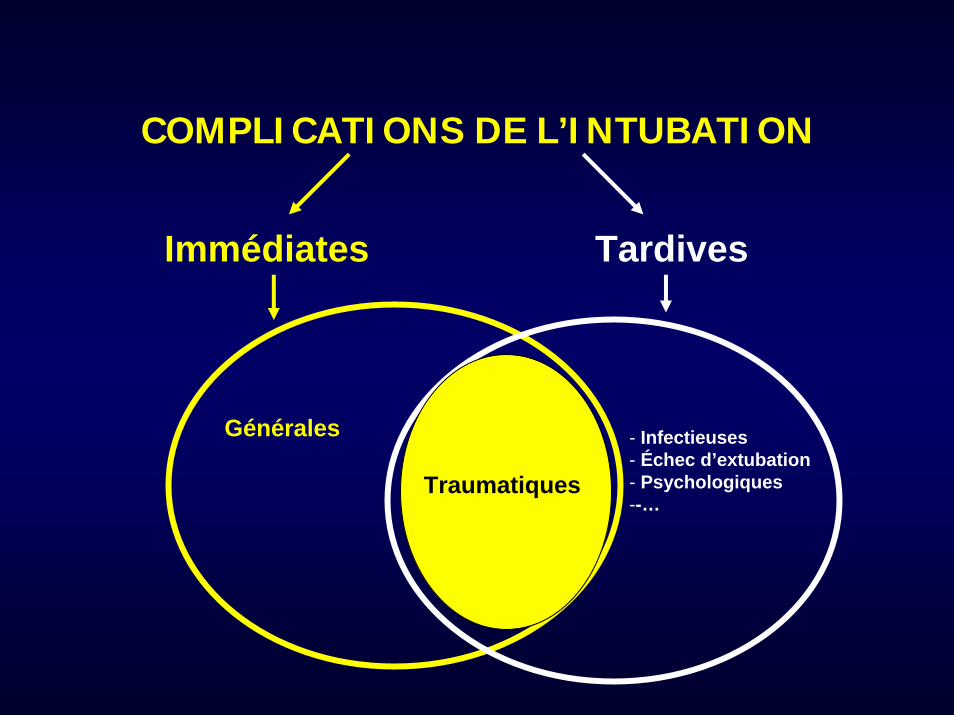
COMPLICATIONS DE L’INTUBATION
- Infectieuses- Échec d’extubation- Psychologiques--…
TardivesImmédiates
Générales
Traumatiques
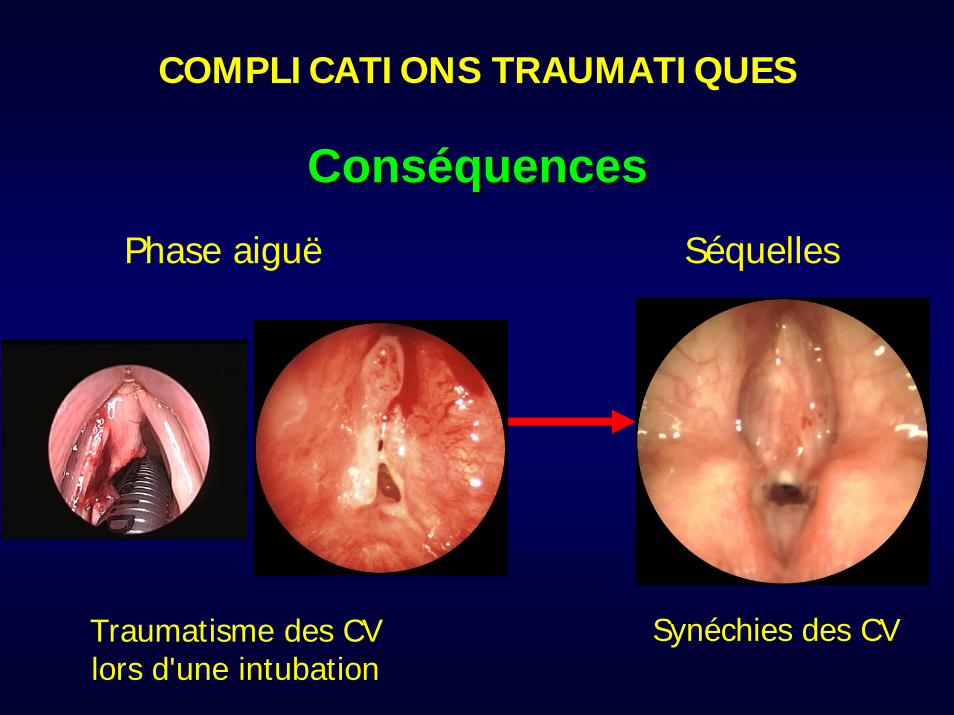
ConsConsééquencesquencesSéquelles
Synéchies des CV
Phase aiguë
Traumatisme des CV lors d'une intubation
COMPLICATIONS TRAUMATIQUES
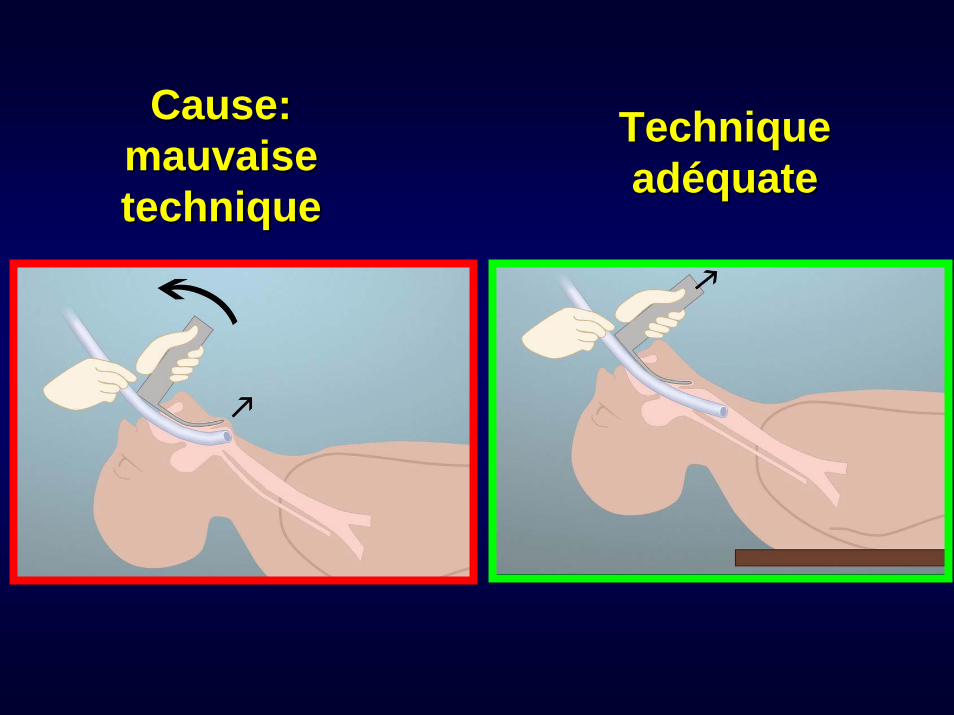
Cause: Cause: mauvaise mauvaise techniquetechnique
Technique Technique adadééquatequate

LLéésions lors de la phase aigusions lors de la phase aiguëë
Œdème Granulations
Dyspnée
Pas de séquelles
Dyspnée
AdhérencesInter-aryténoidiennes
Ulcérations
Pas de dyspnée
Sténose glottique postérieure
Schwartz DE et al. Anesthesiology 1995
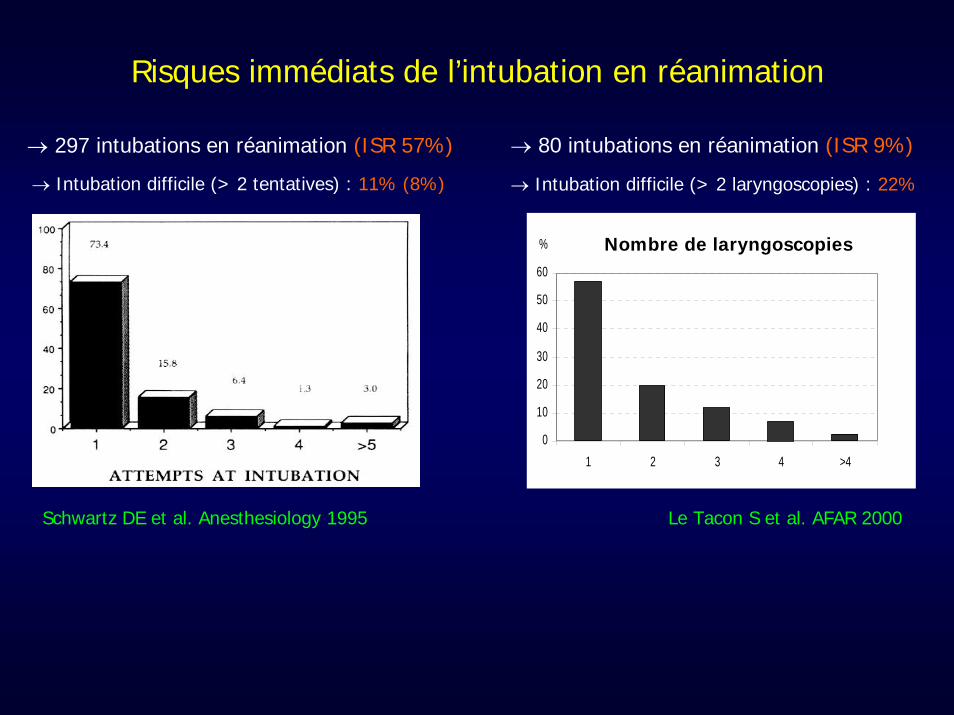
→ 297 intubations en réanimation (ISR 57%) → 80 intubations en réanimation (ISR 9%)
→ Intubation difficile (> 2 tentatives) : 11% (8%)
Risques immédiats de l’intubation en réanimation
Le Tacon S et al. AFAR 2000
→ Intubation difficile (> 2 laryngoscopies) : 22%
%
0
10
20
30
40
50
60
1 2 3 4 >4
Nombre de laryngoscopies
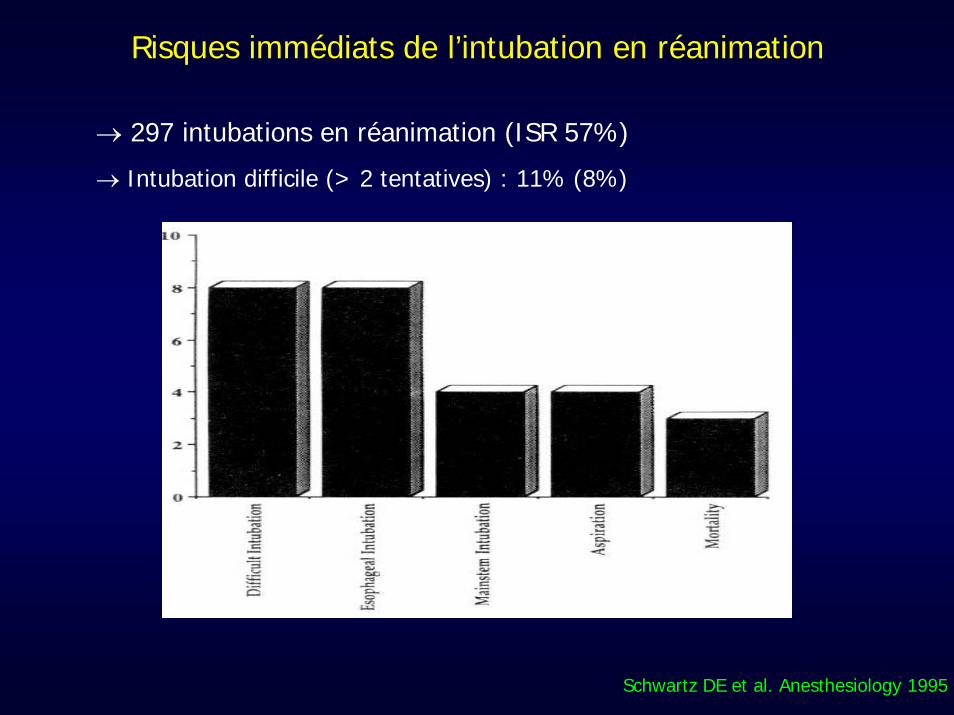
Schwartz DE et al. Anesthesiology 1995
→ 297 intubations en réanimation (ISR 57%)
→ Intubation difficile (> 2 tentatives) : 11% (8%)
Risques immédiats de l’intubation en réanimation
0%
5%
10%
15%
20%
25%
30%
Severe
hypoxe
mia
Severe
colla
pseCard
iac ar
rest
Death
Difficu
lt intubati
on
Cardiac
arrh
ythmia
Esophgea
l intubati
onAgita
tion
Inhalatio
nDen
tal in
jury
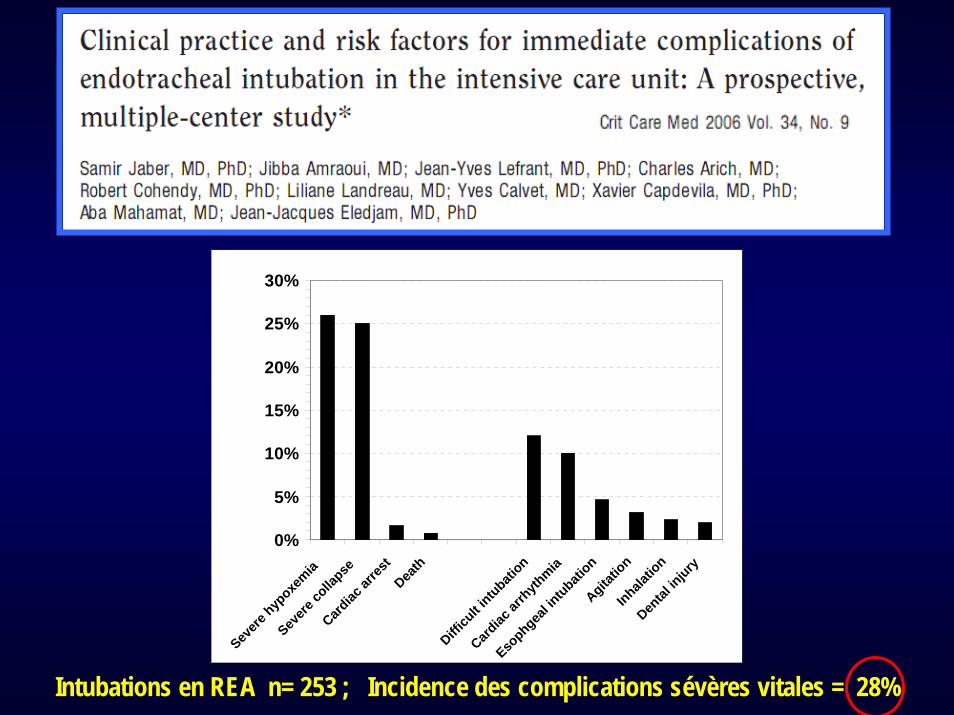
Intubations en REA n= 253 ; Incidence des complications sévères vitales = 28%
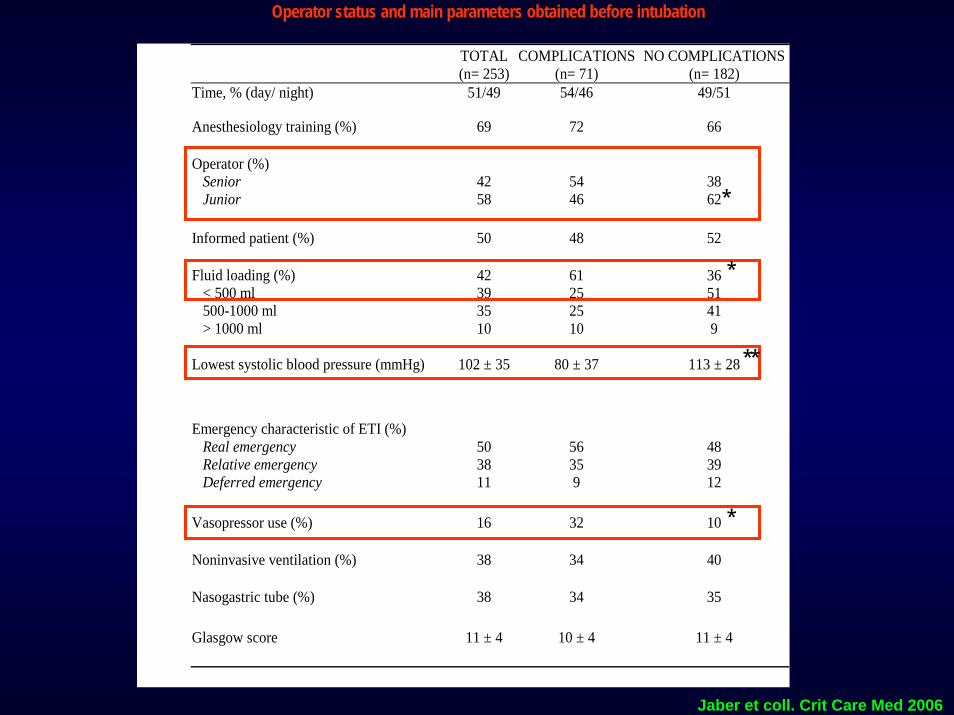
TOTAL(n= 253)
COMPLICATIONS(n= 71)
NO COMPLICATIONS(n= 182)
Time, % (day/ night) 51/49 54/46 49/51
Anesthesiology training (%) 69 72 66
Operator (%) Senior Junior
42 58
54 46
38 62
Informed patient (%) 50 48 52
Fluid loading (%) < 500 ml 500-1000 ml > 1000 ml
42 39 35 10
61 25 25 10
36 51 41 9
Lowest systolic blood pressure (mmHg) 102 ± 35 80 ± 37 113 ± 28
Emergency characteristic of ETI (%) Real emergency Relative emergency Deferred emergency
50 38 11
56 35 9
48 39 12
Vasopressor use (%) 16 32 10
Noninvasive ventilation (%) 38 34 40
Nasogastric tube (%) 38 34 35
Glasgow score 11 ± 4 10 ± 4 11 ± 4
Operator status and main parameters obtained before intubation
*
*
**
*
Jaber et coll. Crit Care Med 2006
Multivariate logistic regression analysis to assess independent risk factors
for development of ETI complications
Predictive risk factor Odds ratio 95% Confidence interval
Acute respiratory failure 3.04 1.08 8.75
Lowest systolic blood pressure 0.98 0.98 0.99
Junior operator 0.42 0.22 0.78
Seul facteur protecteur
Jaber et coll. Crit Care Med 2006
JUNIOR
SENIOR
A deuxC’est mieux…
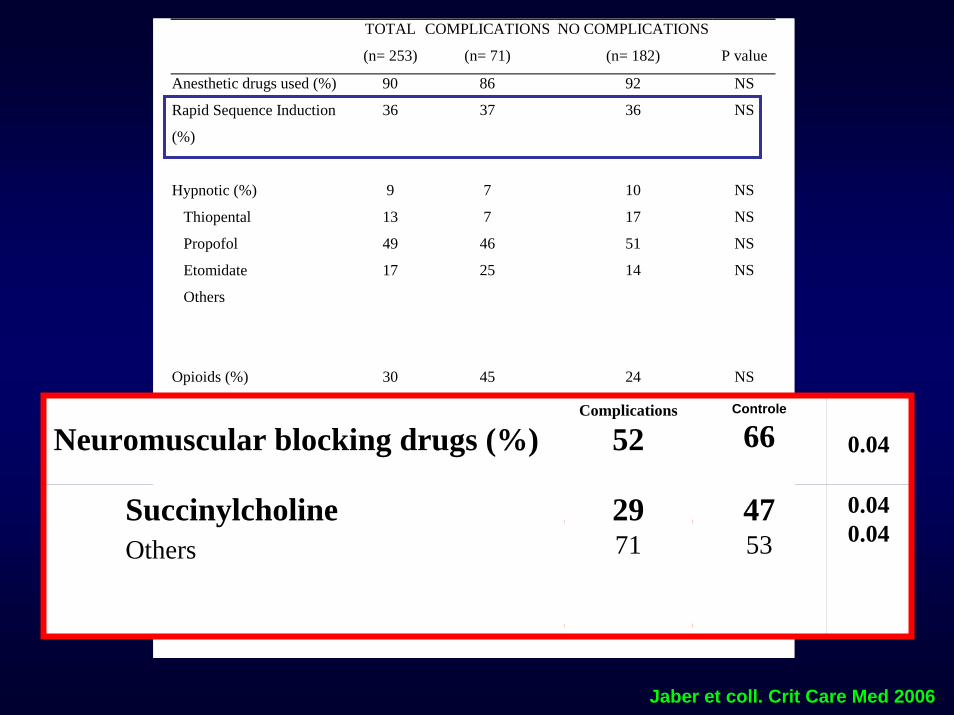
TOTAL
(n= 253)
COMPLICATIONS
(n= 71)
NO COMPLICATIONS
(n= 182)
P value
Anesthetic drugs used (%) 90 86 92 NS
Rapid Sequence Induction
(%)
Hypnotic (%)
Thiopental
Propofol
Etomidate
Others
36
9
13
49
17
37
7
7
46
25
36
10
17
51
14
NS
NS
NS
NS
NS
Opioids (%)
30
45
24
NS
Fentanyl
Sufentanyl
Others
41
18
41
32
27
41
46
14
40
NS
NS
NS
Neuromuscular blocking
drugs (%)
62
52
66
0.04
Succinylcholine
Others
69
31
29
71
47
53
0.04
0.04
Jaber et coll. Crit Care Med 2006
Neuromuscular blocking drugs (%) Complications
52Controle
66 0.04
SuccinylcholineOthers
2971
4753
0.040.04
Comment améliorer les conditions d’intubations
et diminuer ses complications ?
1.1. Induction SInduction Sééquence Rapide (ISR) quence Rapide (ISR) –– CurareCurare
2. Améliorer les conditions d’oxygénation: utilisation de la VNI ?
3. Détection précoce de l’intubation oesophagienne
4. Recommandations locales !
ViteVite, , vitevite ilil fautfaut faire faire uneuneintubation en rintubation en rééanimationanimation
Take time to go fast !
Intubation en réanimation….
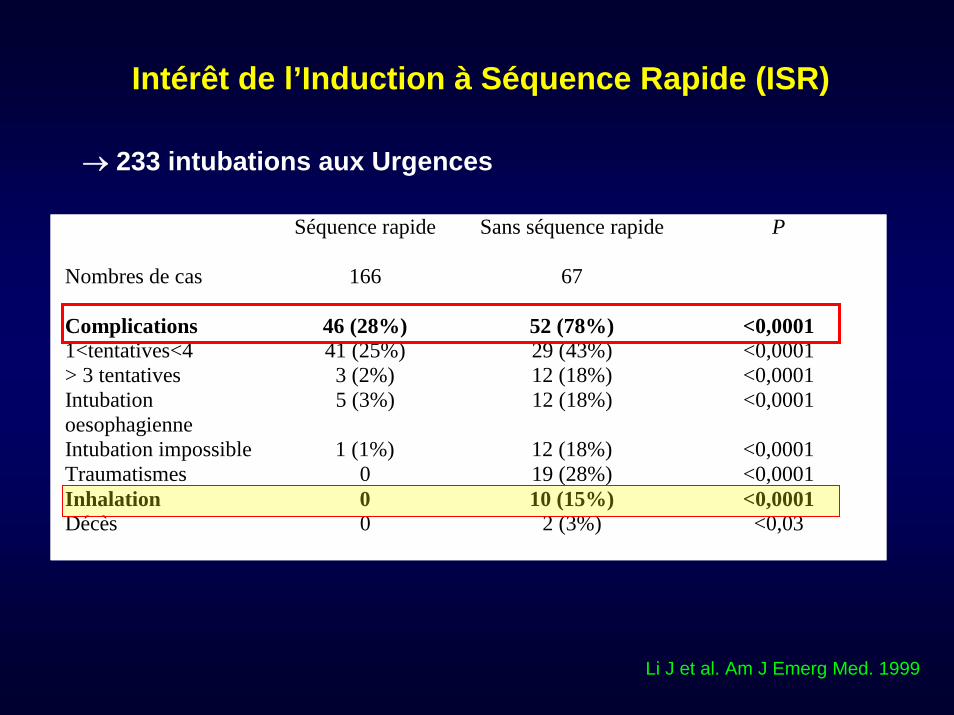
Intérêt de l’Induction à Séquence Rapide (ISR)
Li J et al. Am J Emerg Med. 1999
→ 233 intubations aux Urgences
Séquence rapide Sans séquence rapide P
Nombres de cas 166 67
Complications 46 (28%) 52 (78%) <0,0001 1<tentatives<4 41 (25%) 29 (43%) <0,0001 > 3 tentatives 3 (2%) 12 (18%) <0,0001 Intubation oesophagienne
5 (3%) 12 (18%) <0,0001
Intubation impossible 1 (1%) 12 (18%) <0,0001 Traumatismes 0 19 (28%) <0,0001 Inhalation 0 10 (15%) <0,0001 Décès 0 2 (3%) <0,03
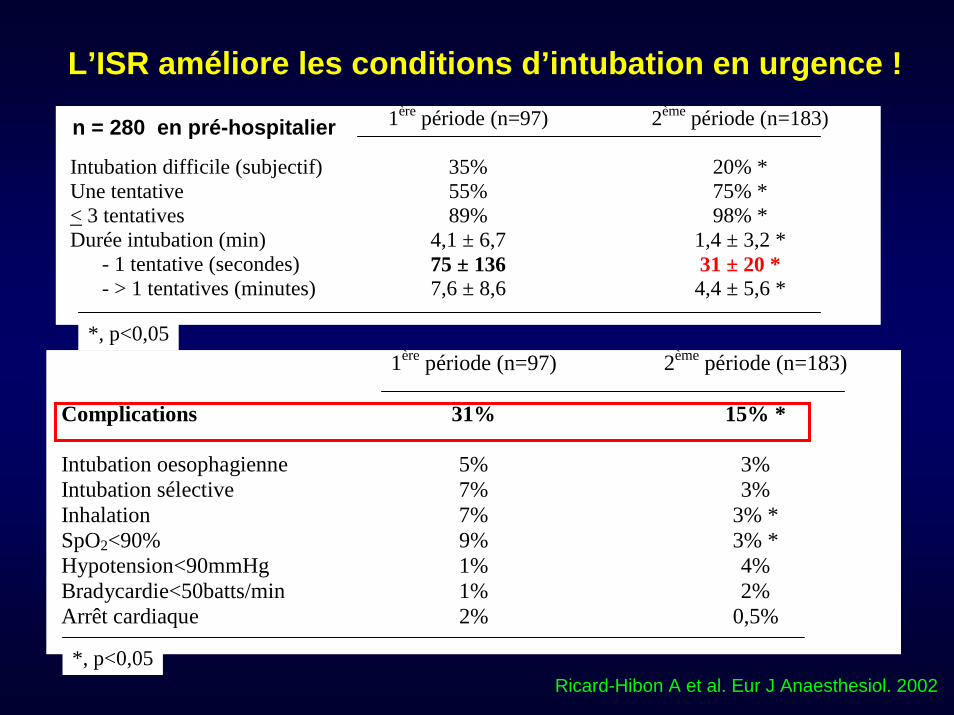
Ricard-Hibon A et al. Eur J Anaesthesiol. 2002
1ère période (n=97)
2ème période (n=183)
Intubation difficile (subjectif) 35% 20% * Une tentative 55% 75% * < 3 tentatives 89% 98% * Durée intubation (min) 4,1 ± 6,7 1,4 ± 3,2 * - 1 tentative (secondes) 75 ± 136 31 ± 20 * - > 1 tentatives (minutes) 7,6 ± 8,6 4,4 ± 5,6 *
*, p<0,05 1ère période (n=97) 2ème période (n=183)
Complications 31% 15% *
Intubation oesophagienne 5% 3% Intubation sélective 7% 3% Inhalation 7% 3% * SpO2<90% 9% 3% * Hypotension<90mmHg 1% 4% Bradycardie<50batts/min 1% 2% Arrêt cardiaque 2% 0,5%
*, p<0,05
L’ISR améliore les conditions d’intubation en urgence !
n = 280 en pré-hospitalier
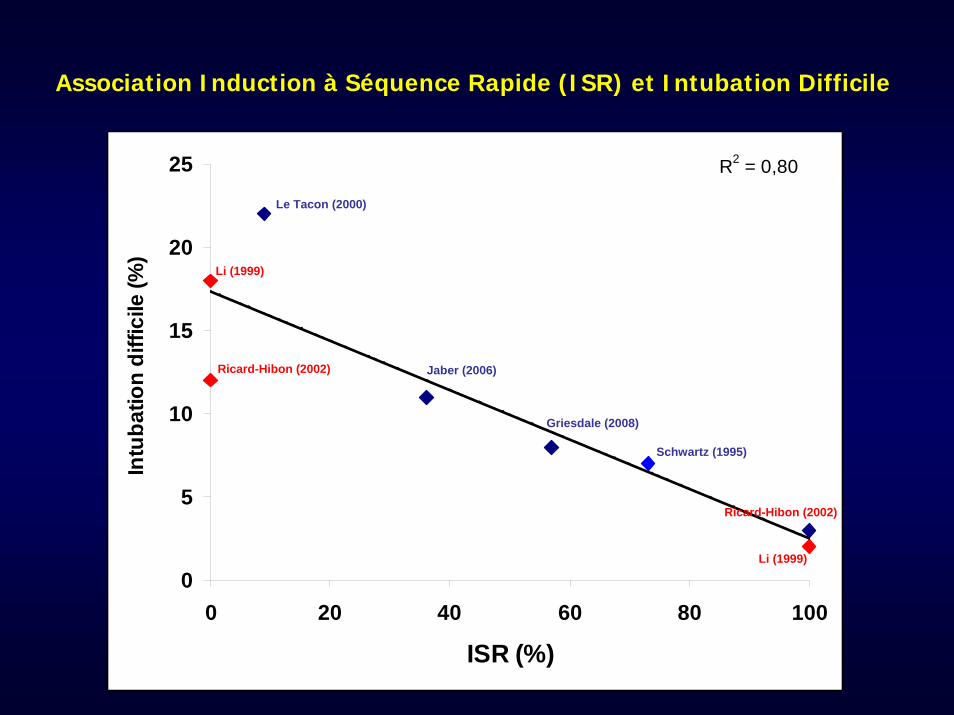
R2 = 0,80
0
5
10
15
20
25
0 20 40 60 80 100
ISR (%)
Intu
batio
n di
ffici
le (%
)
Le Tacon (2000)
Jaber (2006)
Griesdale (2008)
Li (1999)
Li (1999)
Ricard-Hibon (2002)
Ricard-Hibon (2002)
Schwartz (1995)
Association Induction à Séquence Rapide (ISR) et Intubation Difficile
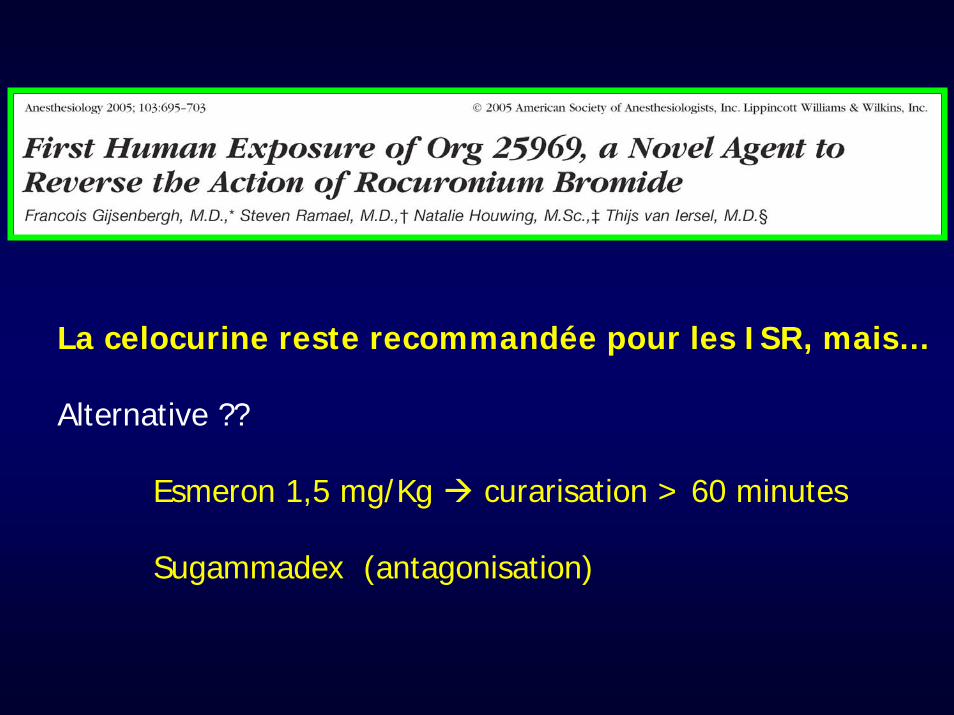
La celocurine reste recommandée pour les ISR, mais…
Alternative ??
Esmeron 1,5 mg/Kg curarisation > 60 minutes
Sugammadex (antagonisation)
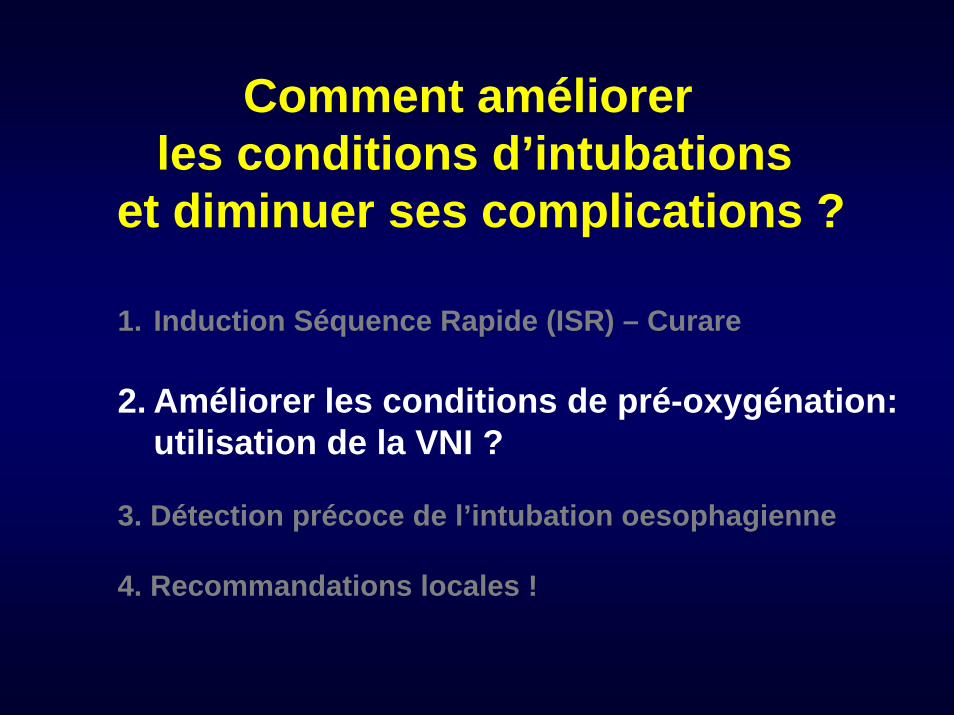
Comment améliorer les conditions d’intubations
et diminuer ses complications ?
1. Induction Séquence Rapide (ISR) – Curare
2. Améliorer les conditions de pré-oxygénation: utilisation de la VNI ?
3. Détection précoce de l’intubation oesophagienne
4. Recommandations locales !
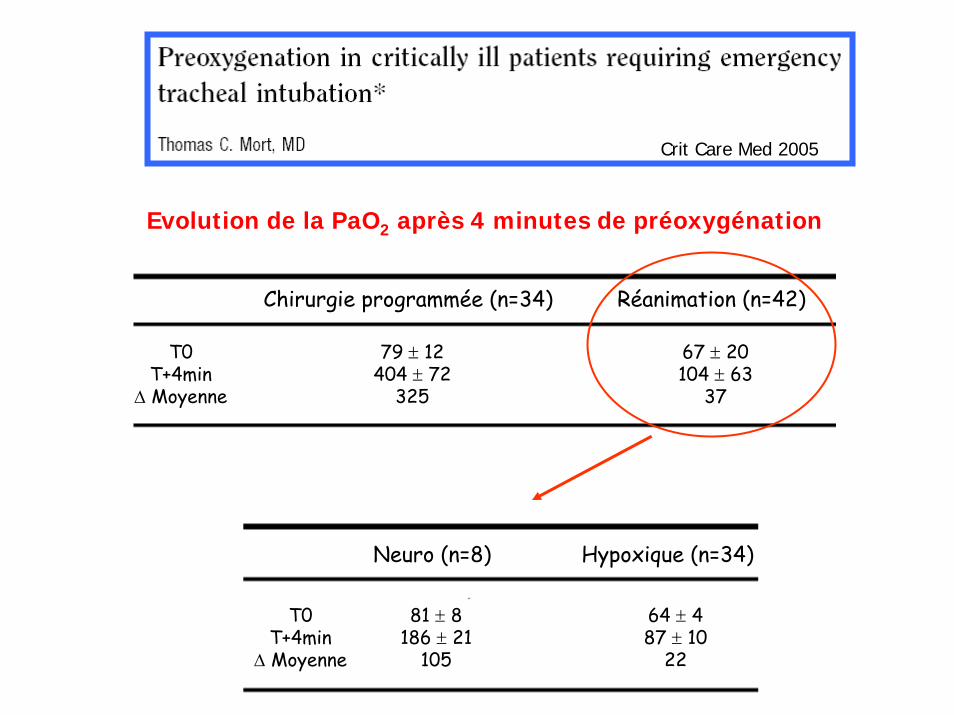
Chirurgie programmée (n=34) Réanimation (n=42)
79 ± 12404 ± 72
325
67 ± 20104 ± 63
37
T0T+4min
Δ Moyenne
Neuro (n=8) Hypoxique (n=34)
T0T+4min
Δ Moyenne
81 ± 8186 ± 21
105
64 ± 487 ± 10
22
Crit Care Med 2005
Evolution de la PaO2 après 4 minutes de préoxygénation
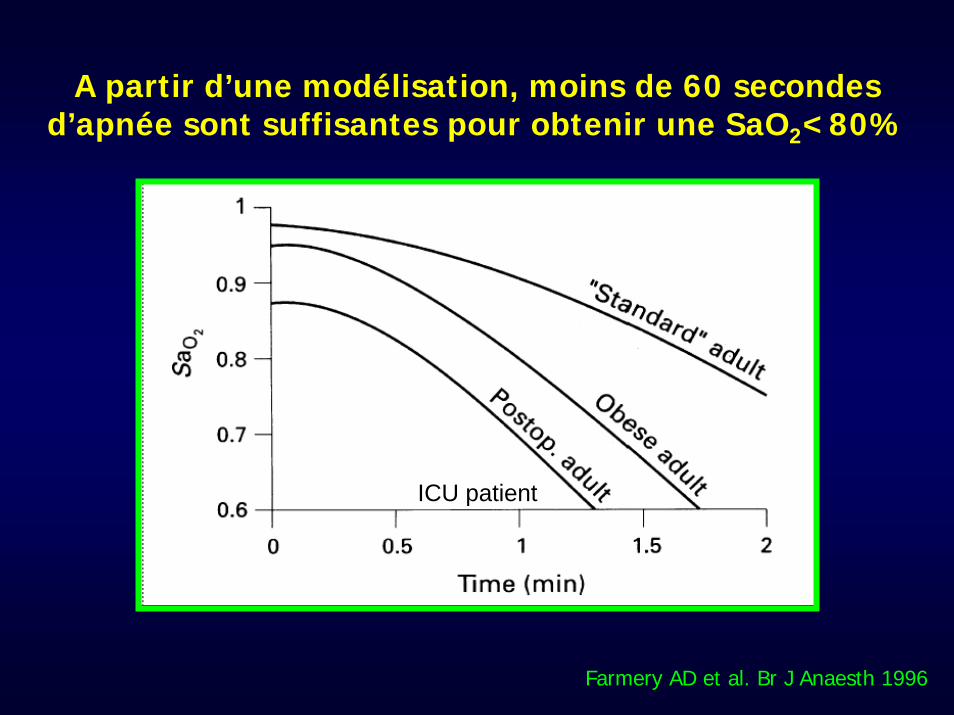
A partir d’une modélisation, moins de 60 secondes d’apnée sont suffisantes pour obtenir une SaO2<80%
Farmery AD et al. Br J Anaesth 1996
ICU patient
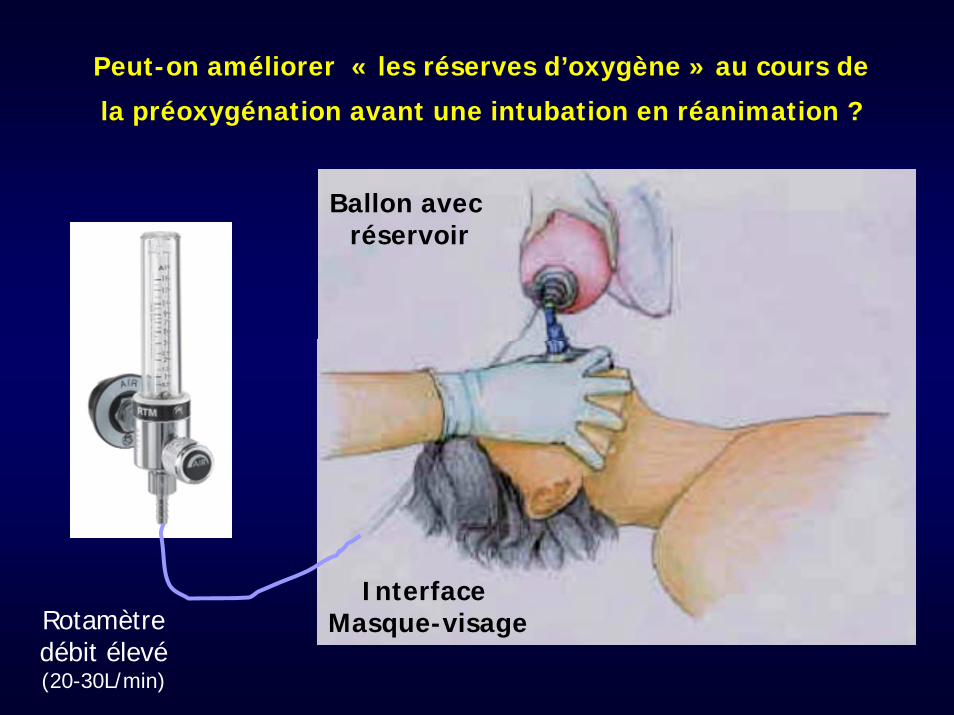
Peut-on améliorer « les réserves d’oxygène » au cours de
la préoxygénation avant une intubation en réanimation ?
Interface Masque-visage
Ballon avec réservoir
Rotamètredébit élevé(20-30L/min)
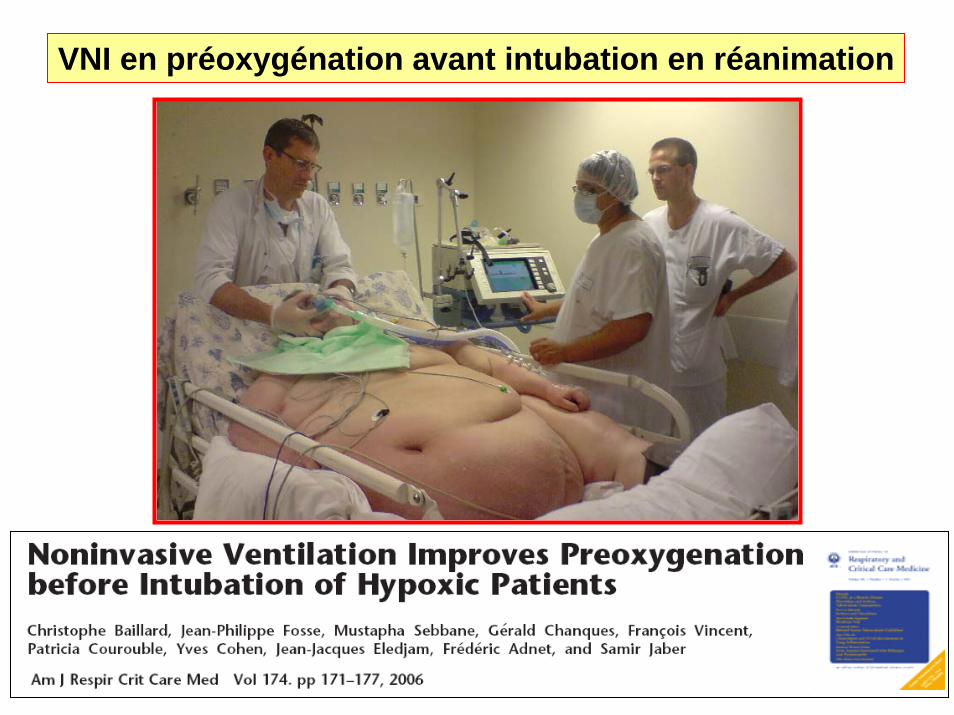
VNI en préoxygénation avant intubation en réanimation
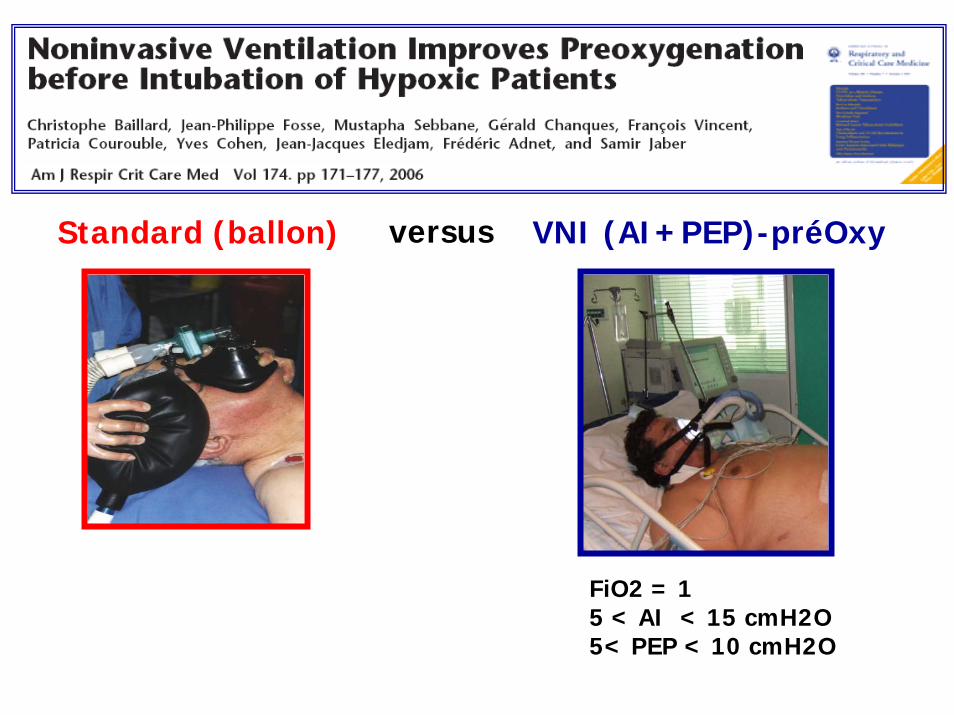
Standard (ballon) VNI (AI+PEP)-préOxyversus
FiO2 = 15 < AI < 15 cmH2O5< PEP < 10 cmH2O
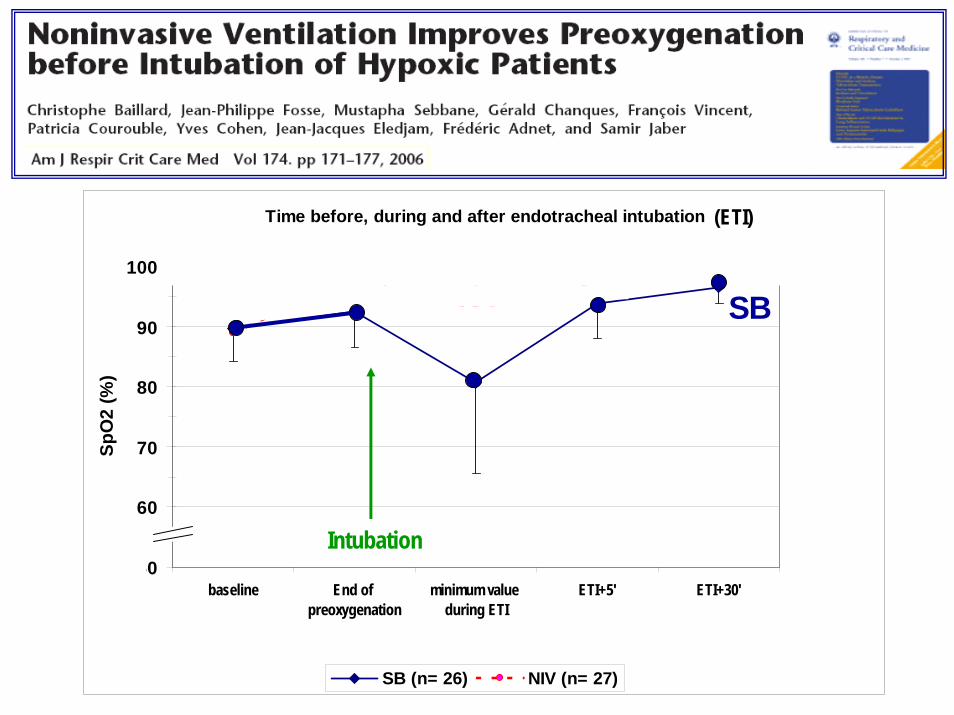
Time before, during and after endotracheal intubation
50
60
70
80
90
100
baseline End of preoxygenation
minimum value during ETI
ETI+5' ETI+30'
SpO
2 (%
)
SB (n= 26) NIV (n= 27)
Intubation
(ETI)
* ** *NS NSNIVSB
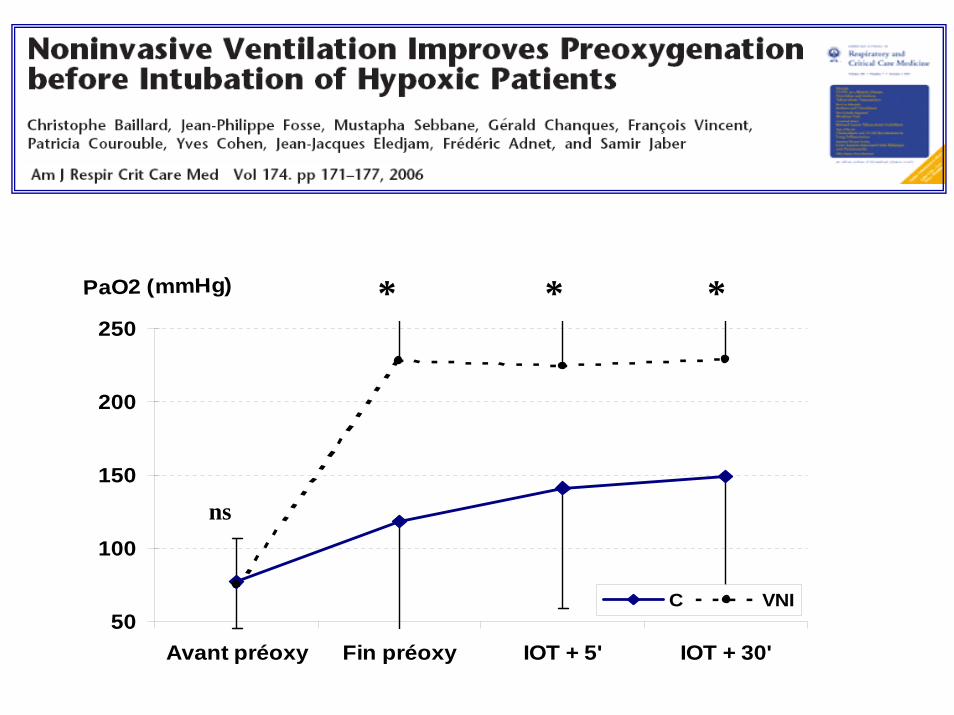
50
100
150
200
250
Avant préoxy Fin préoxy IOT + 5' IOT + 30'
PaO2 (mmHg)
C VNI
* *
ns
*
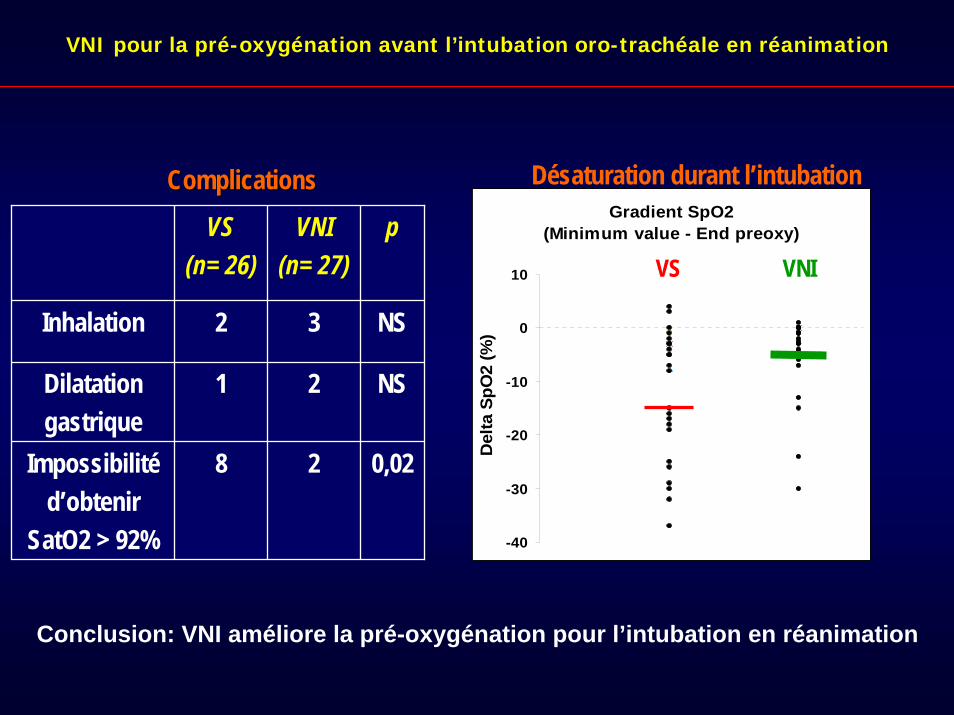
VS(n= 26)
VNI(n= 27)
p
Inhalation 2 3 NS
Dilatationgastrique
1 2 NS
Impossibilitéd’obtenir
SatO2 > 92%
8 2 0,02
Gradient SpO2 (Minimum value - End preoxy)
-40
-30
-20
-10
0
10
Del
ta S
pO2
(%)
Désaturation durant l’intubation
VS VNI
ComplicationsComplications
VNI pour la pré-oxygénation avant l’intubation oro-trachéale en réanimation
Conclusion: VNI améliore la pré-oxygénation pour l’intubation en réanimation
Préoxygénation avant intubation en réanimation
Ventilation non invasive (VNI) en préoxygénation :
Les référentiels
La VNI peut être utilisée
pour la pré-oxygénation
avant intubation pour insuffisance
respiratoire aiguë (Il faut probablement faire)
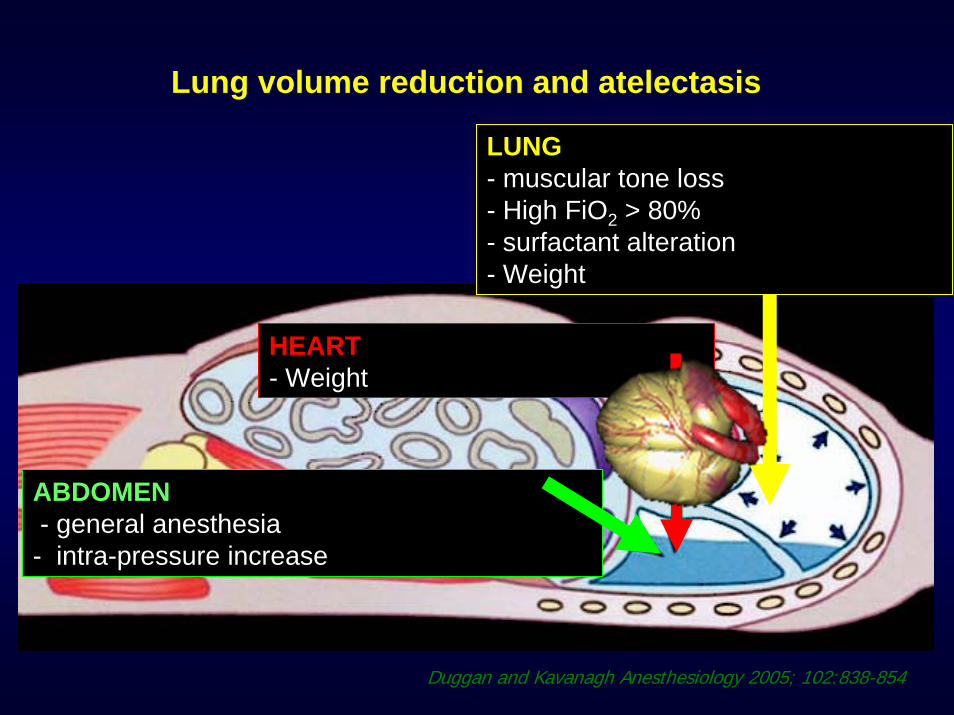
Lung volume reduction and atelectasis
ABDOMEN- general anesthesia- intra-pressure increase
HEART- Weight
LUNG- muscular tone loss- High FiO2 > 80%- surfactant alteration- Weight
Duggan and Kavanagh Anesthesiology 2005; 102:838-854
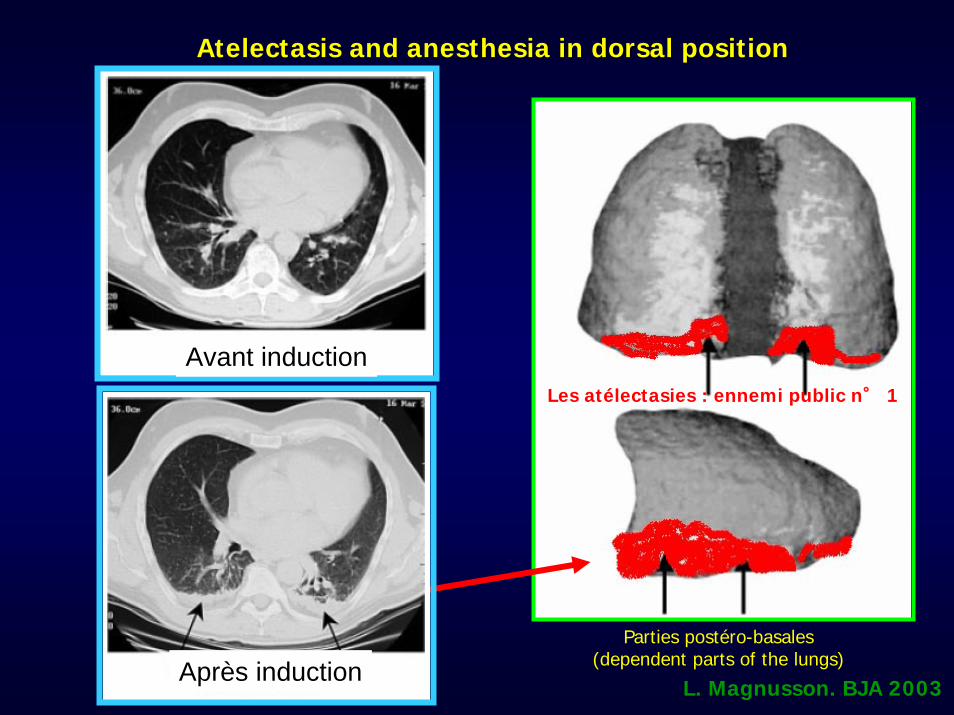
L. Magnusson. BJA 2003
Atelectasis and anesthesia in dorsal positionAtelectasis and anesthesia in dorsal position
Avant induction
Parties postéro-basales(dependent parts of the lungs)
Les atélectasies : ennemi public n° 1
Après induction
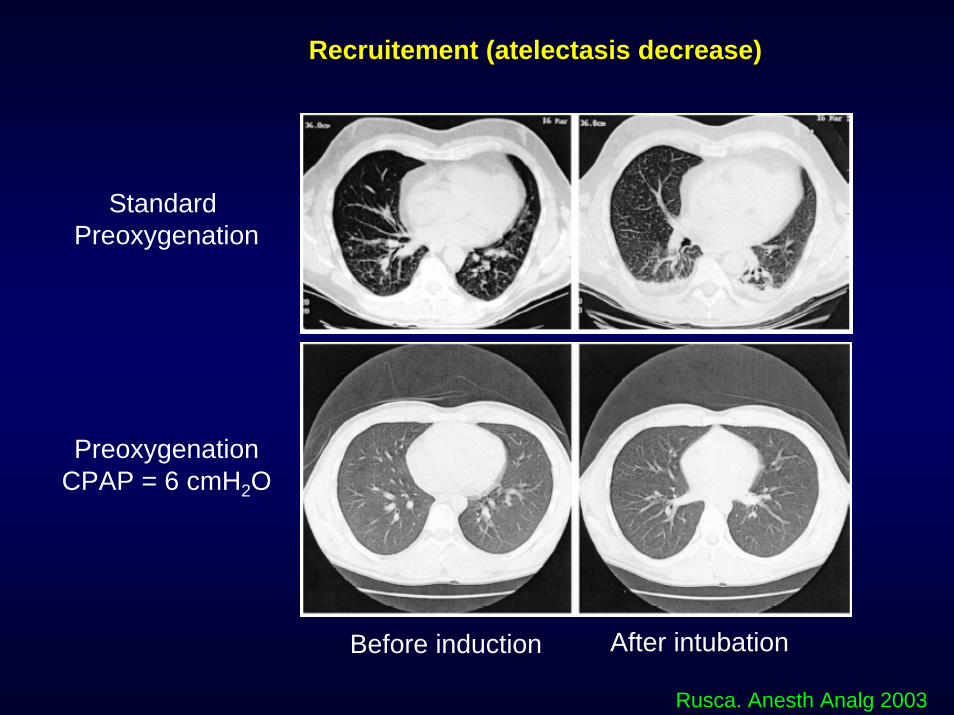
Before induction After intubation
Standard Preoxygenation
PreoxygenationCPAP = 6 cmH2O
Rusca. Anesth Analg 2003
Recruitement (atelectasis decrease)
ConclusionConclusion : The most recent anesthesia ventilators have : The most recent anesthesia ventilators have comparable performances of recent generation ICU ventilators.comparable performances of recent generation ICU ventilators.
Conclusions:Conclusions: Anaesthesia machines have benefited from considerable Anaesthesia machines have benefited from considerable advances in design and technology. advances in design and technology. The most recent workstations were more appreciated by users thanThe most recent workstations were more appreciated by users thanthe first generation of anaesthesia workstations.the first generation of anaesthesia workstations.
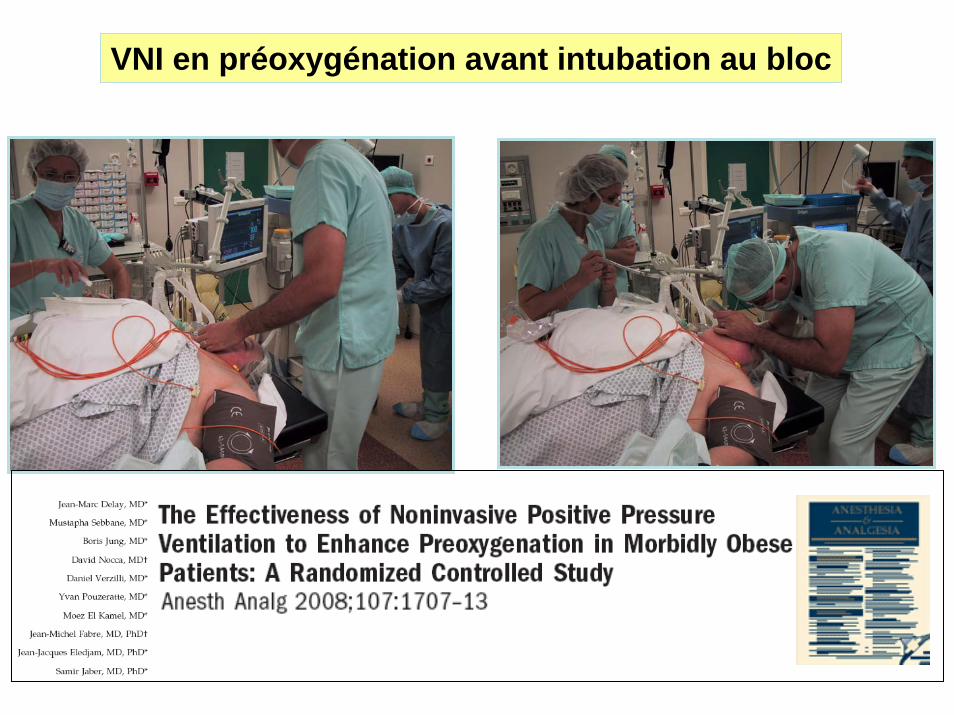
VNI en préoxygénation avant intubation au bloc
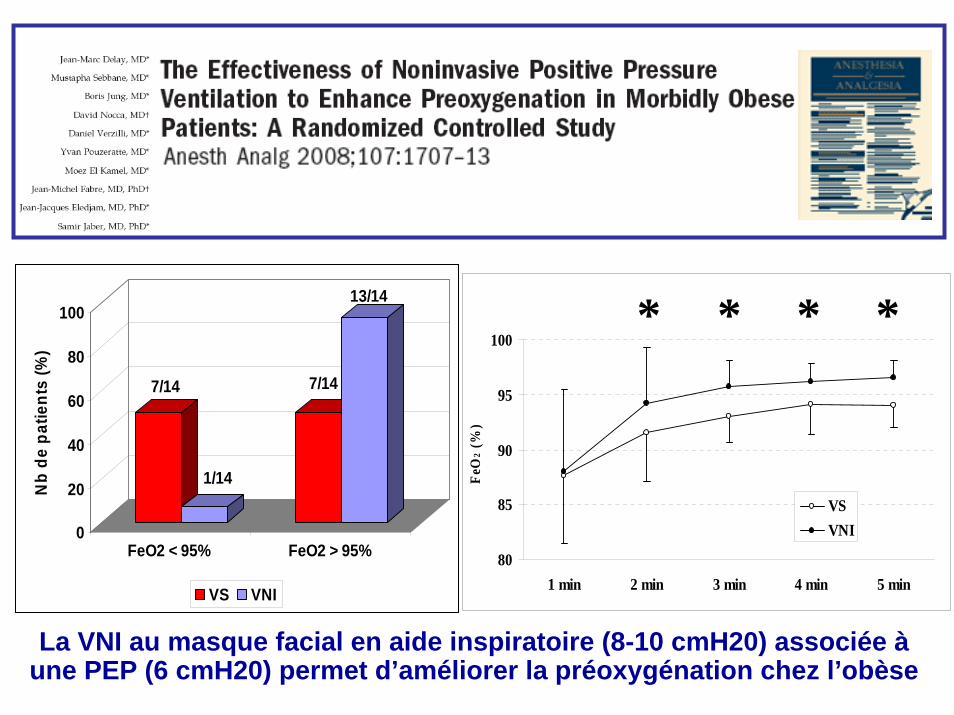
7/14
1/14
7/14
13/14
0
20
40
60
80
100
Nb
de p
atie
nts
(%)
FeO2 < 95% FeO2 > 95%
VS VNI
80
85
90
95
100
1 min 2 min 3 min 4 min 5 min
FeO
2 (%
)
VSVNI
* * * *
La VNI au masque facial en aide inspiratoire (8-10 cmH20) associée àune PEP (6 cmH20) permet d’améliorer la préoxygénation chez l’obèse

Parfois, la VNI peut être difficile à utiliser !
Tu vas la faire ta VNI !
Pour l’intubation
quelques recommandations…
pour diminuer les complications liées
à l’intubation
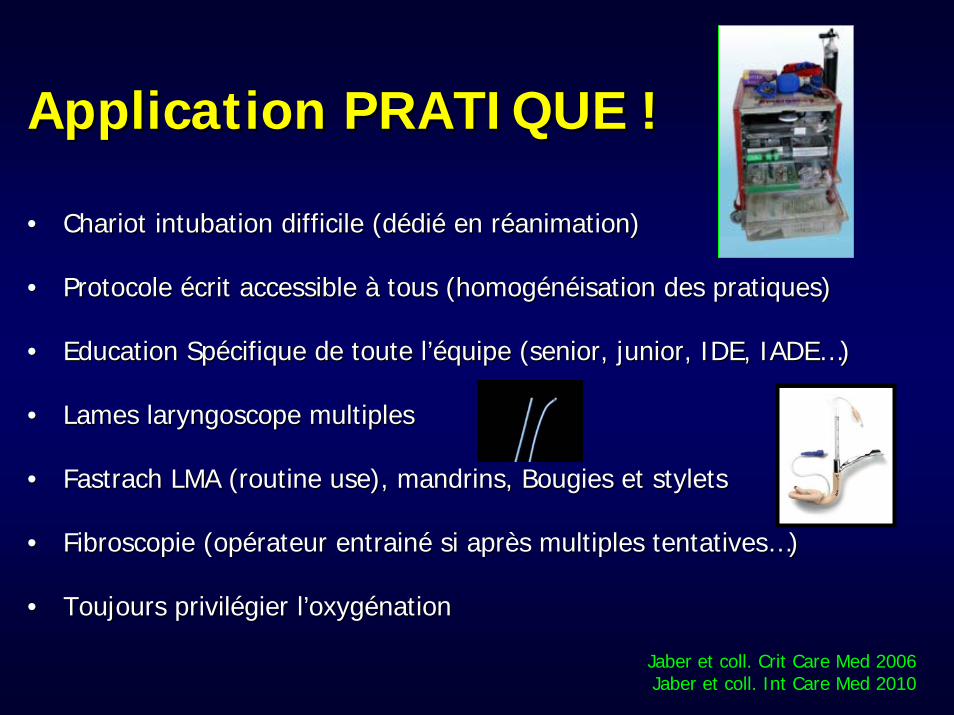
Application PRATIQUE !Application PRATIQUE !
•• Chariot intubation difficile (dChariot intubation difficile (déédidiéé en ren rééanimation)animation)
•• Protocole Protocole éécrit accessible crit accessible àà tous (homogtous (homogéénnééisation des pratiques)isation des pratiques)
•• Education SpEducation Spéécifique de toute lcifique de toute l’é’équipe (senior, junior, IDE, IADEquipe (senior, junior, IDE, IADE……) )
•• Lames laryngoscope multiplesLames laryngoscope multiples
•• FastrachFastrach LMA (routine use), mandrins, Bougies et stylets LMA (routine use), mandrins, Bougies et stylets
•• Fibroscopie (opFibroscopie (opéérateur entrainrateur entrainéé si aprsi aprèès multiples tentativess multiples tentatives……))
•• Toujours privilToujours priviléégier lgier l’’oxygoxygéénationnation
Jaber et coll. Crit Care Med 2006Jaber et coll. Int Care Med 2010
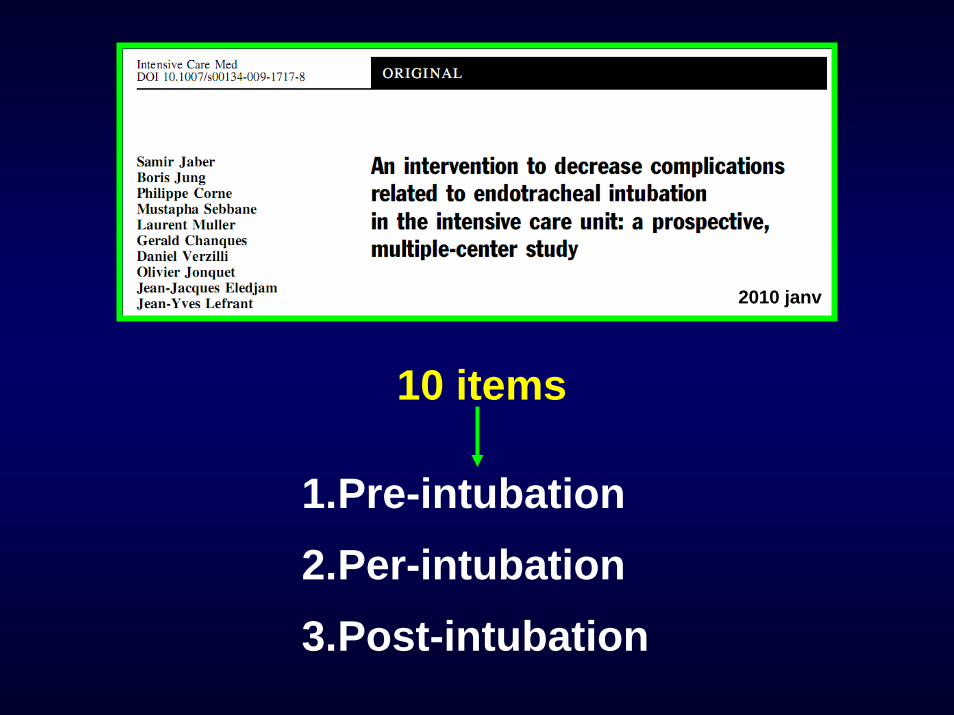
10 items
1.Pre-intubation2.Per-intubation3.Post-intubation
2010 janv
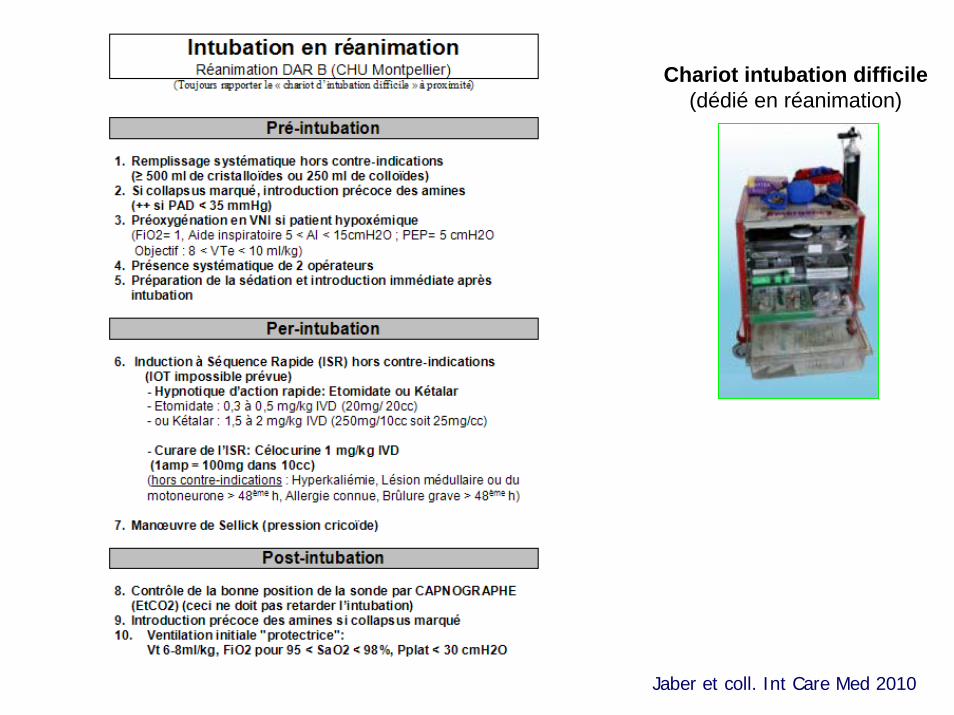
Chariot intubation difficile(dédié en réanimation)
Jaber et coll. Int Care Med 2010
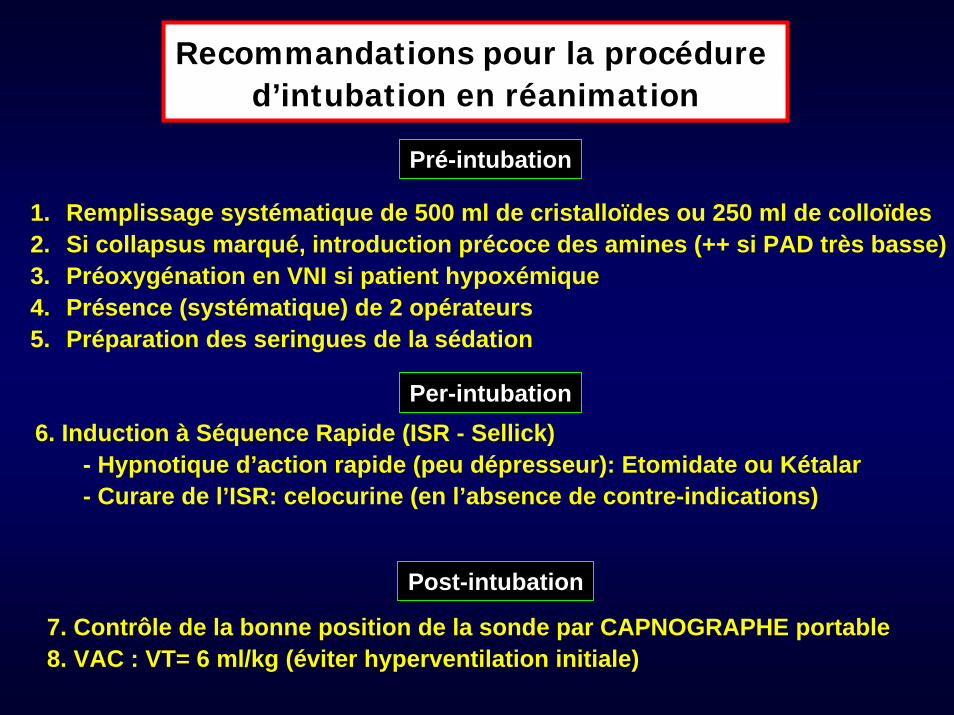
Recommandations pour la procédure d’intubation en réanimation
1. Remplissage systématique de 500 ml de cristalloïdes ou 250 ml de colloïdes2. Si collapsus marqué, introduction précoce des amines (++ si PAD très basse)3. Préoxygénation en VNI si patient hypoxémique4. Présence (systématique) de 2 opérateurs5. Préparation des seringues de la sédation
Pré-intubation
6. Induction à Séquence Rapide (ISR - Sellick)- Hypnotique d’action rapide (peu dépresseur): Etomidate ou Kétalar- Curare de l’ISR: celocurine (en l’absence de contre-indications)
Per-intubation
7. Contrôle de la bonne position de la sonde par CAPNOGRAPHE portable8. VAC : VT= 6 ml/kg (éviter hyperventilation initiale)
Post-intubation
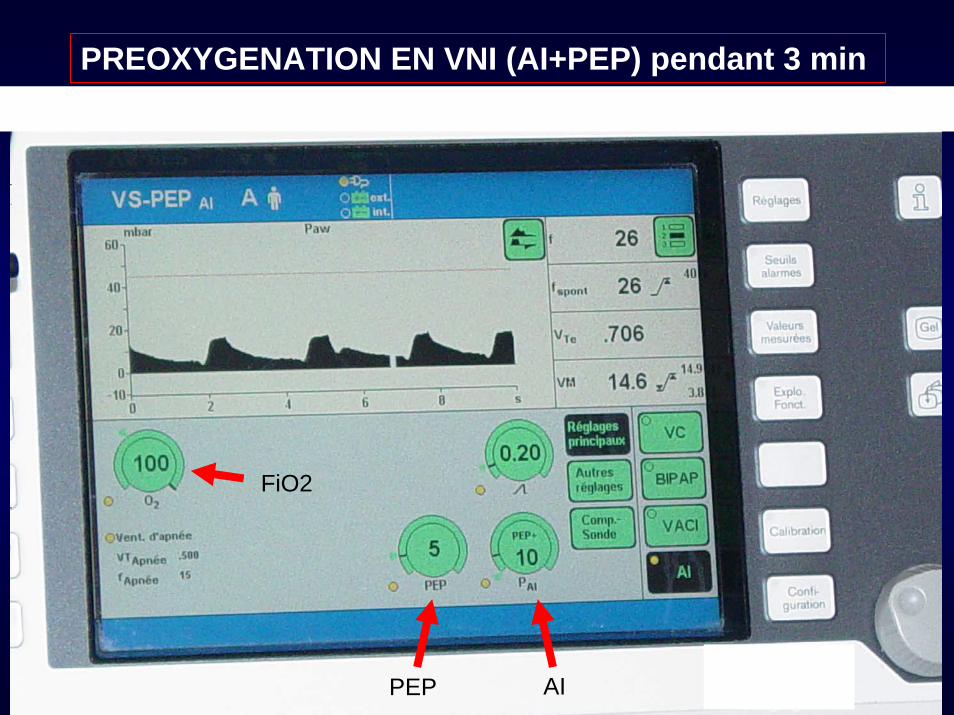
PREOXYGENATION EN VNI (AI+PEP) pendant 3 min
AIPEP
FiO2
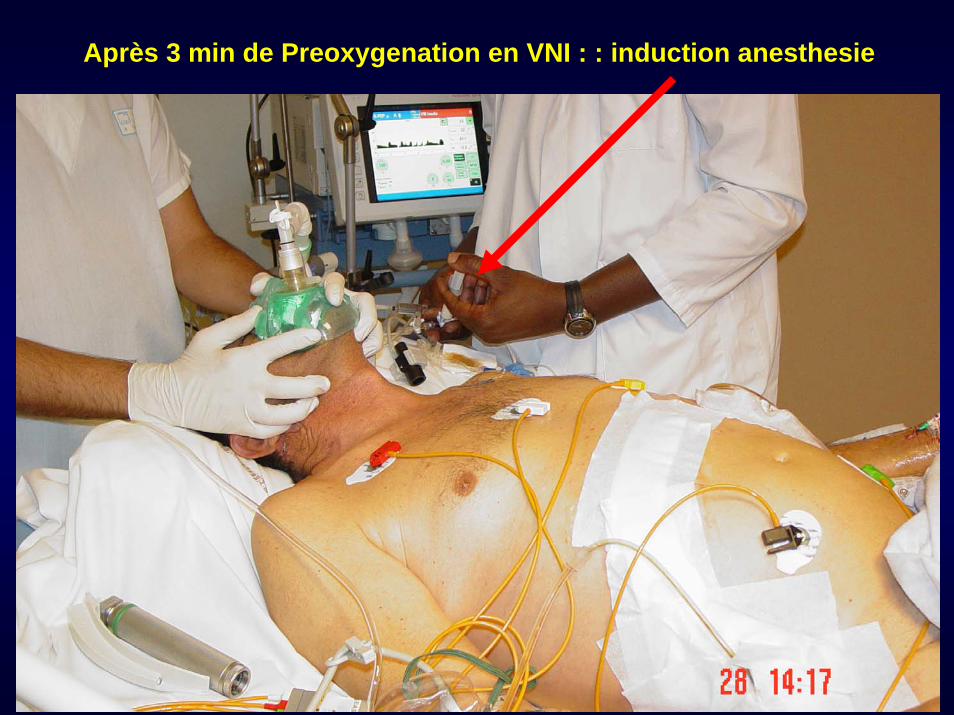
Après 3 min de Preoxygenation en VNI : : induction anesthesie

Attendre l’apnée ….(30-60 s)
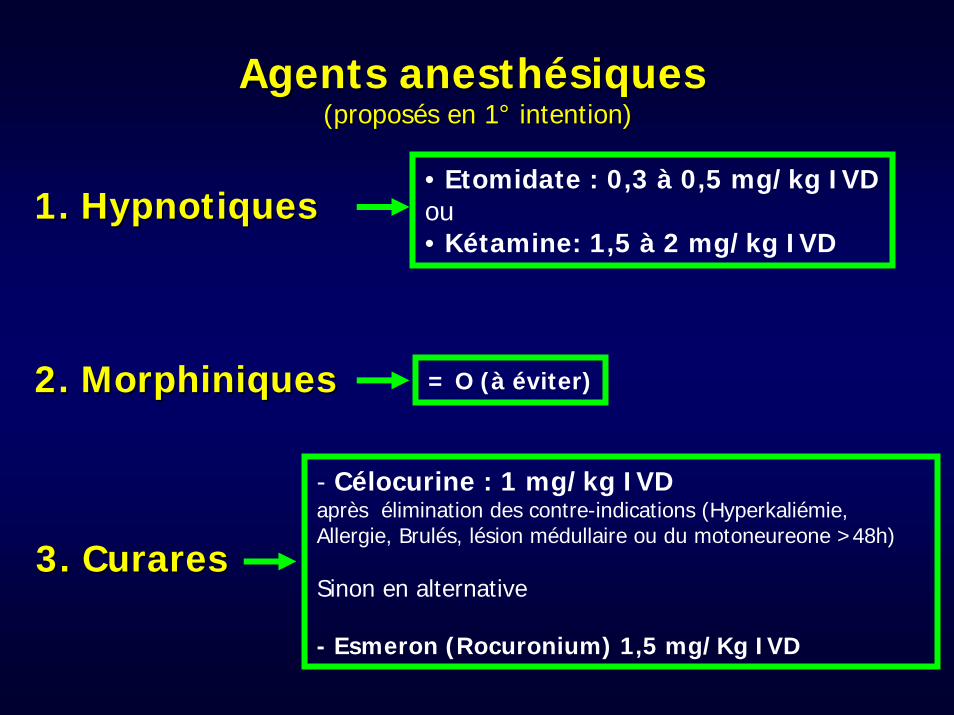
Agents anesthAgents anesthéésiques siques (propos(proposéés en 1s en 1°° intention)intention)
1. 1. HypnotiquesHypnotiques
2. 2. MorphiniquesMorphiniques
3. 3. CuraresCurares
• Etomidate : 0,3 à 0,5 mg/kg IVDou• Kétamine: 1,5 à 2 mg/kg IVD
= O (à éviter)
- Célocurine : 1 mg/kg IVDaprès élimination des contre-indications (Hyperkaliémie, Allergie, Brulés, lésion médullaire ou du motoneureone >48h)
Sinon en alternative
- Esmeron (Rocuronium) 1,5 mg/Kg IVD
Agents anesthAgents anesthéésiques siques
« Peu, c’est déjà trop …. »
Surtout si curare utilisé et patient très fragile (hémodynamique précaire !)
C Morris & C McAllister
Chest, 2005
Crit Care, 2006
ETOMIDATE : ETOMIDATE : stop stop ou encore ?ou encore ?
Murray, Chest 2005
Crit Care 2007
ETOMIDATE : ETOMIDATE : stop ou ou encoreencore ??
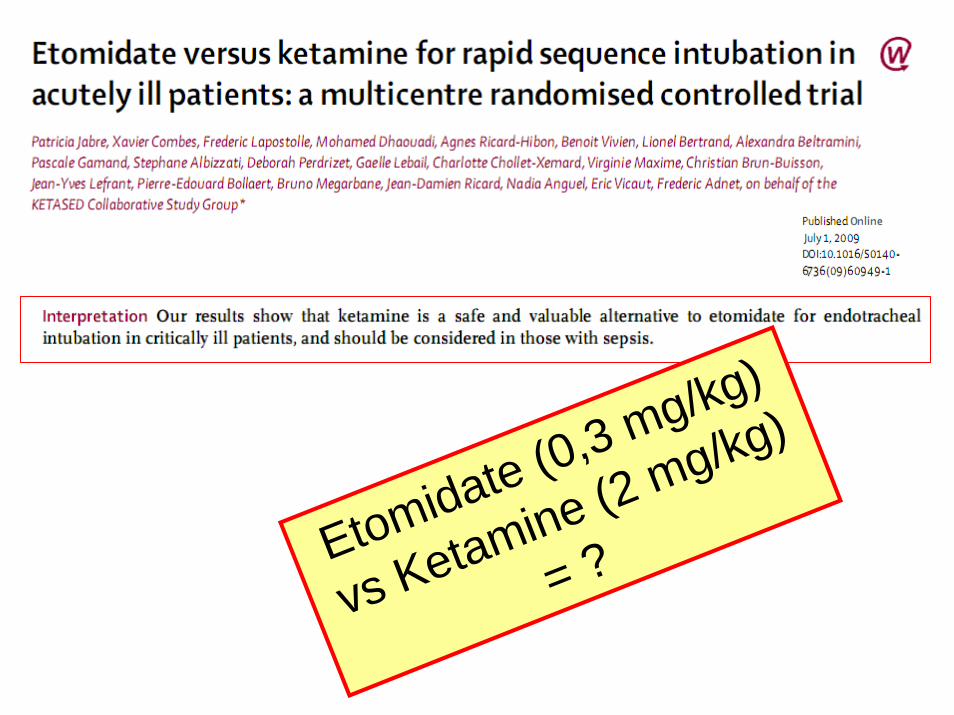
Etomidate (0,3 mg/kg)
vs Ketamine (2 mg/kg)
= ?
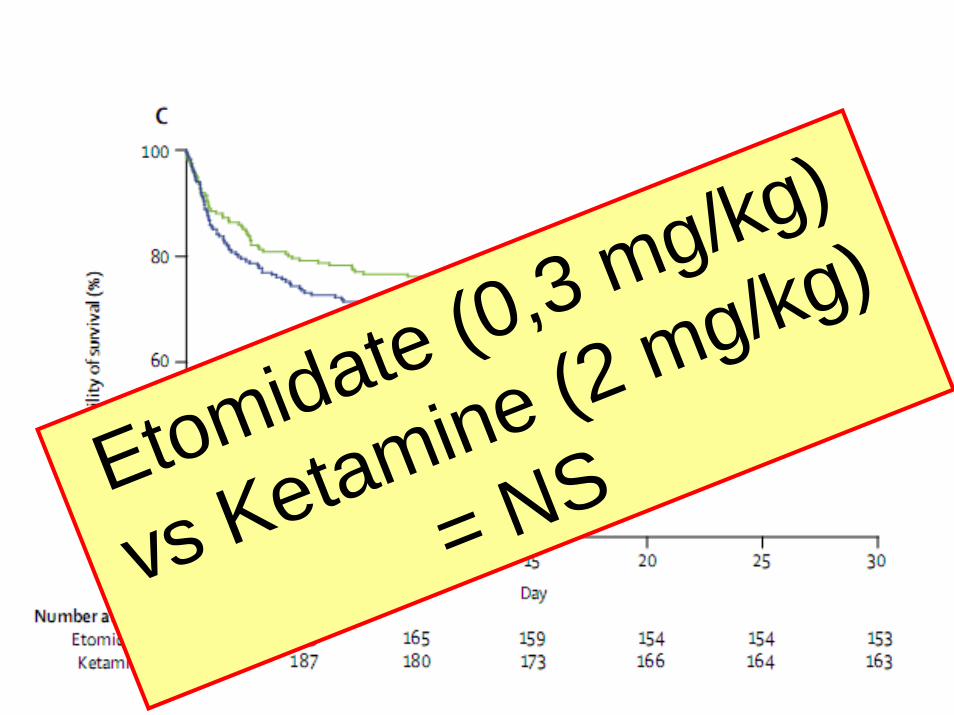
Etomidate (0,3 mg/kg)
vs Ketamine (2 mg/kg)
= NS
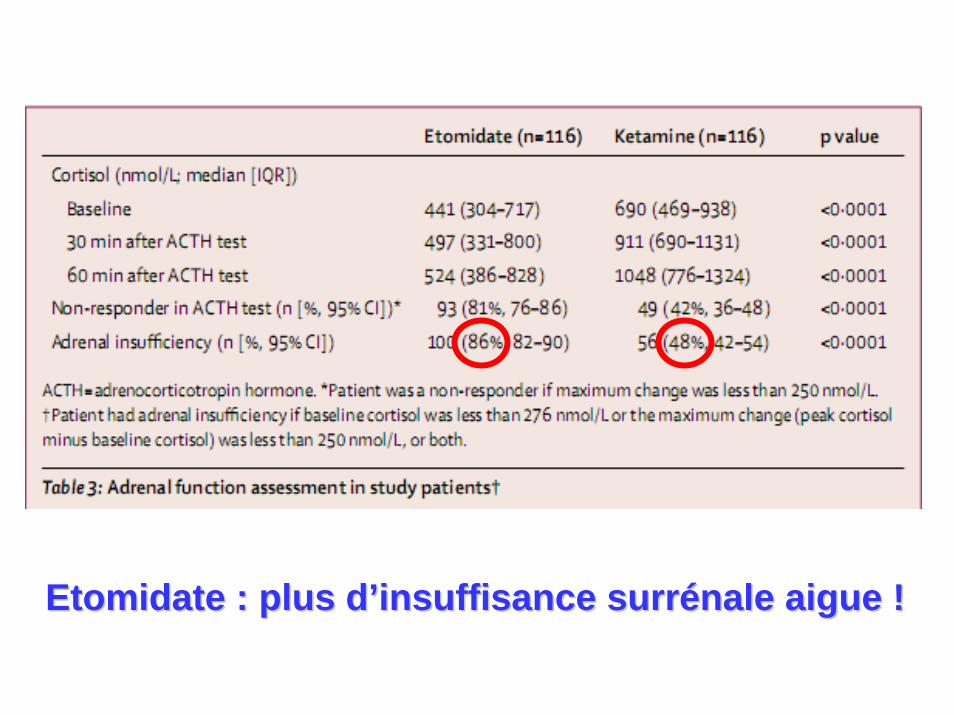
Etomidate : plus Etomidate : plus dd’’insuffisanceinsuffisance surrsurréénale aigue !nale aigue !
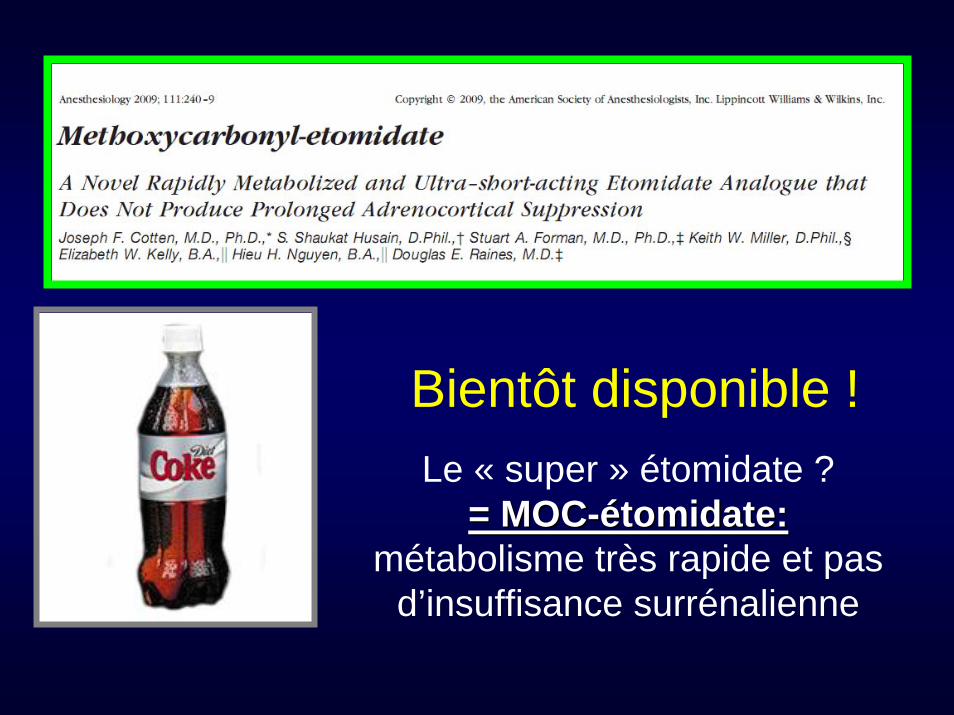
Bientôt disponible !Le « super » étomidate ?
= MOC= MOC--éétomidate: tomidate: métabolisme très rapide et pas
d’insuffisance surrénalienne
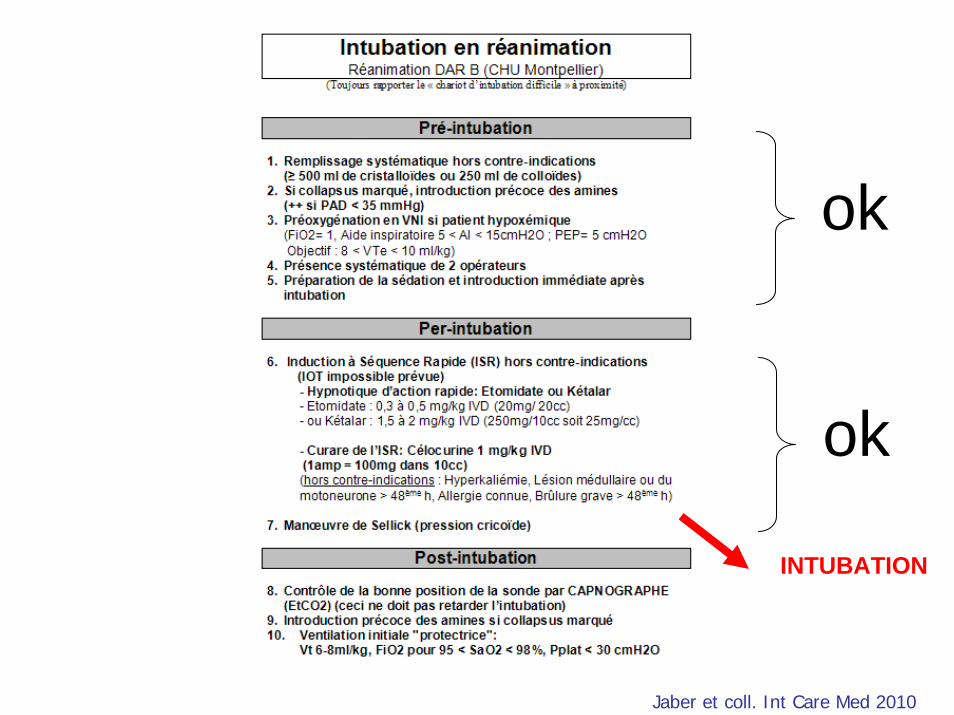
Jaber et coll. Int Care Med 2010
ok
ok
INTUBATION
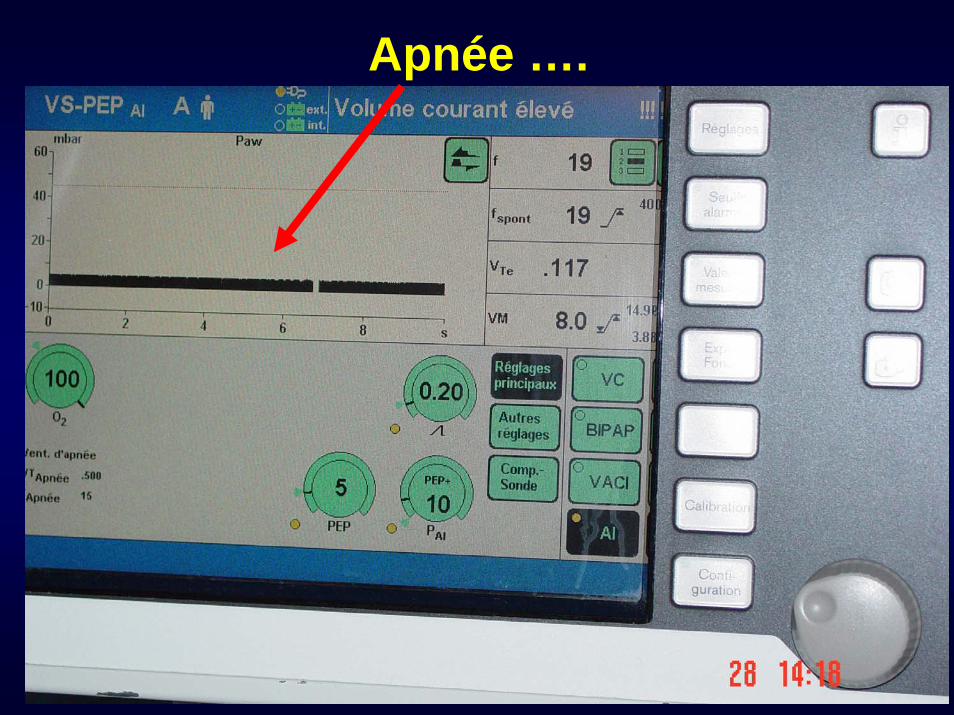
Apnée ….
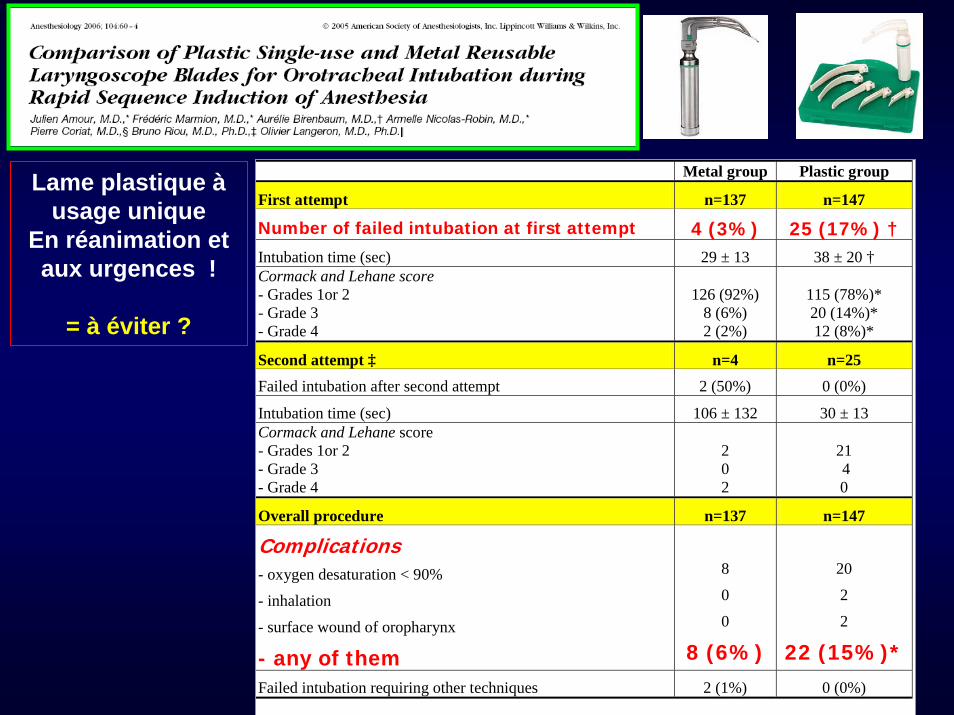
Metal group Plastic group
First attempt n=137 n=147
Number of failed intubation at first attempt 4 (3%) 25 (17%) † Intubation time (sec) 29 ± 13 38 ± 20 † Cormack and Lehane score - Grades 1or 2 - Grade 3 - Grade 4
126 (92%)
8 (6%) 2 (2%)
115 (78%)* 20 (14%)* 12 (8%)*
Second attempt ‡ n=4 n=25
Failed intubation after second attempt 2 (50%) 0 (0%)
Intubation time (sec) 106 ± 132 30 ± 13 Cormack and Lehane score - Grades 1or 2 - Grade 3 - Grade 4
2 0 2
21 4 0
Overall procedure n=137 n=147
Complications - oxygen desaturation < 90%
- inhalation
- surface wound of oropharynx
- any of them
8
0
0
8 (6%)
20
2
2
22 (15%)*Failed intubation requiring other techniques 2 (1%) 0 (0%)
Lame plastique àusage unique
En réanimation et aux urgences !
= à éviter ?
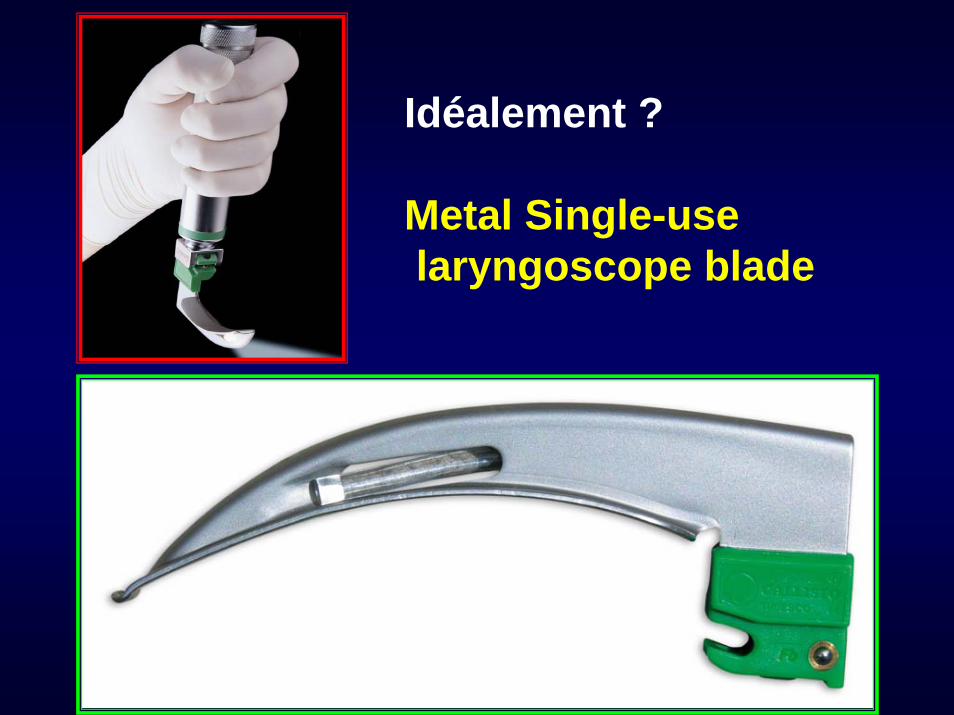
Idéalement ?
Metal Single-uselaryngoscope blade

Intubation….
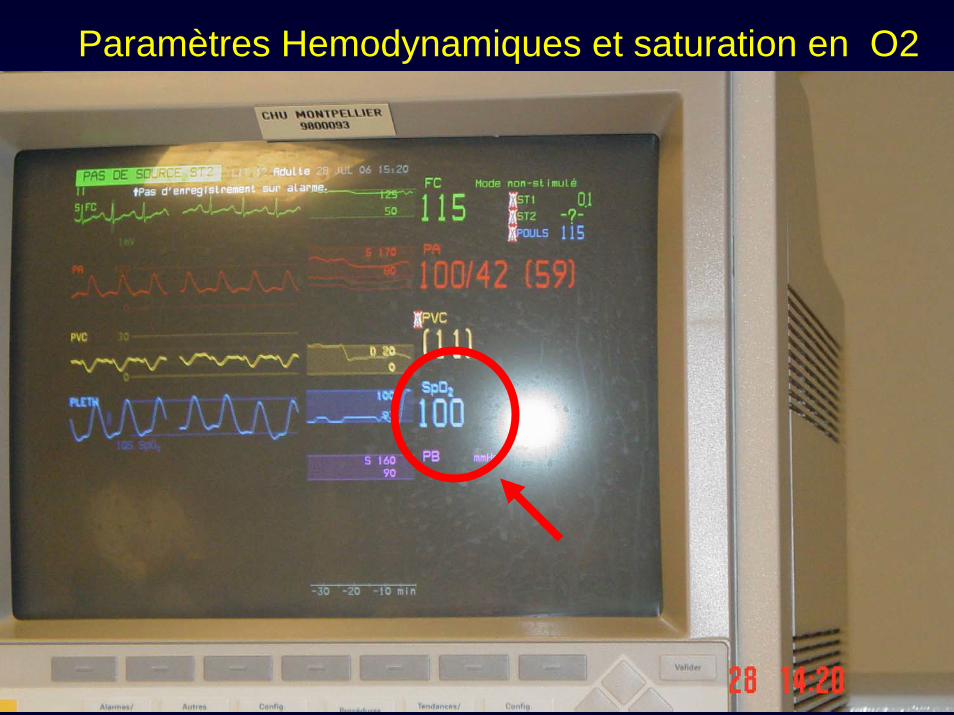
Paramètres Hemodynamiques et saturation en O2
Intubation
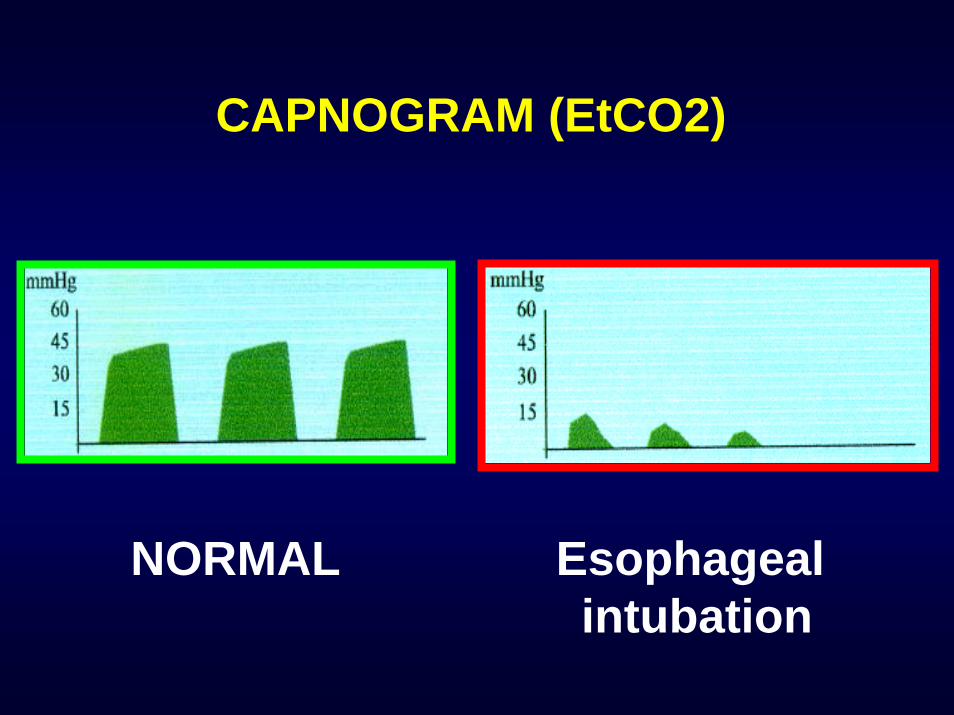
CAPNOGRAM (EtCO2)
NORMAL Esophageal intubation
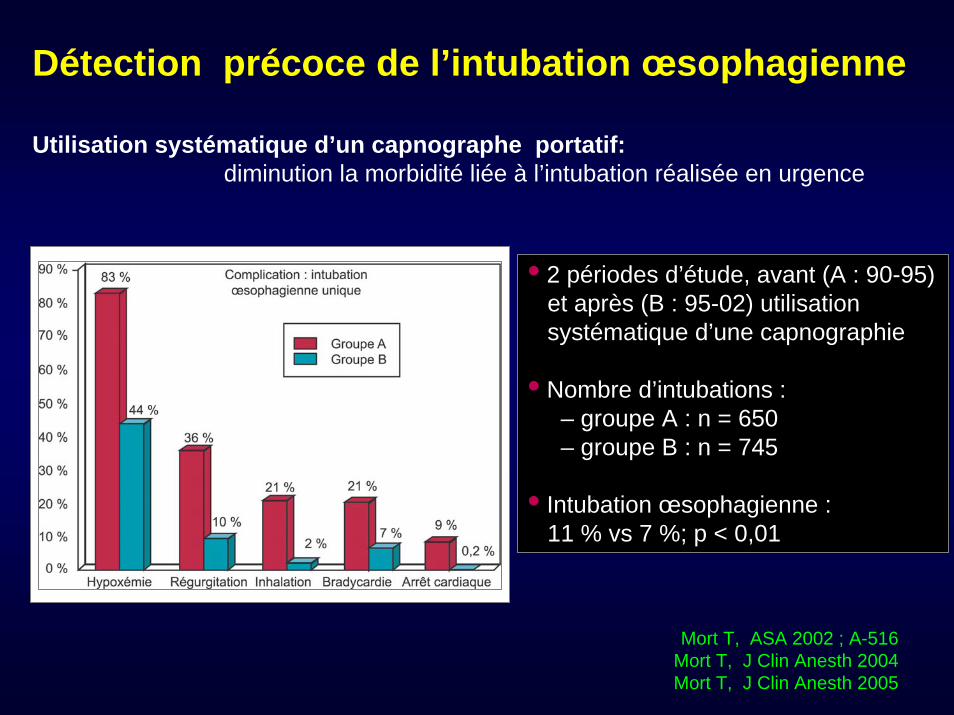
Détection précoce de l’intubation œsophagienne
Utilisation systématique d’un capnographe portatif:diminution la morbidité liée à l’intubation réalisée en urgence
Mort T, ASA 2002 ; A-516Mort T, J Clin Anesth 2004Mort T, J Clin Anesth 2005
• 2 périodes d’étude, avant (A : 90-95) et après (B : 95-02) utilisation systématique d’une capnographie
• Nombre d’intubations :– groupe A : n = 650– groupe B : n = 745
• Intubation œsophagienne :11 % vs 7 %; p < 0,01
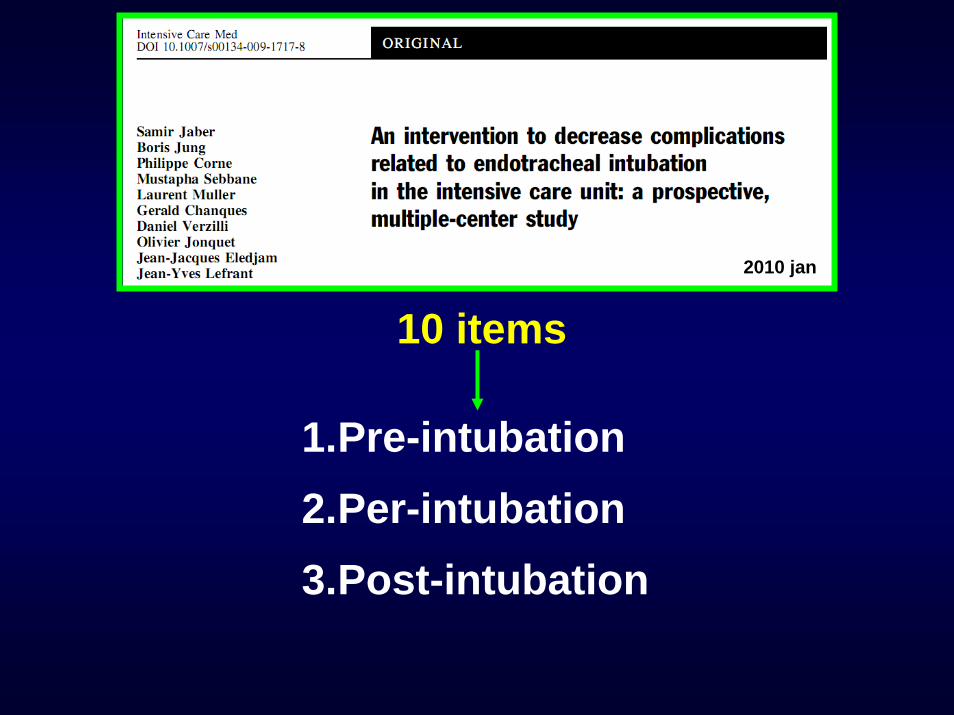
10 items
1.Pre-intubation2.Per-intubation3.Post-intubation
2010 jan
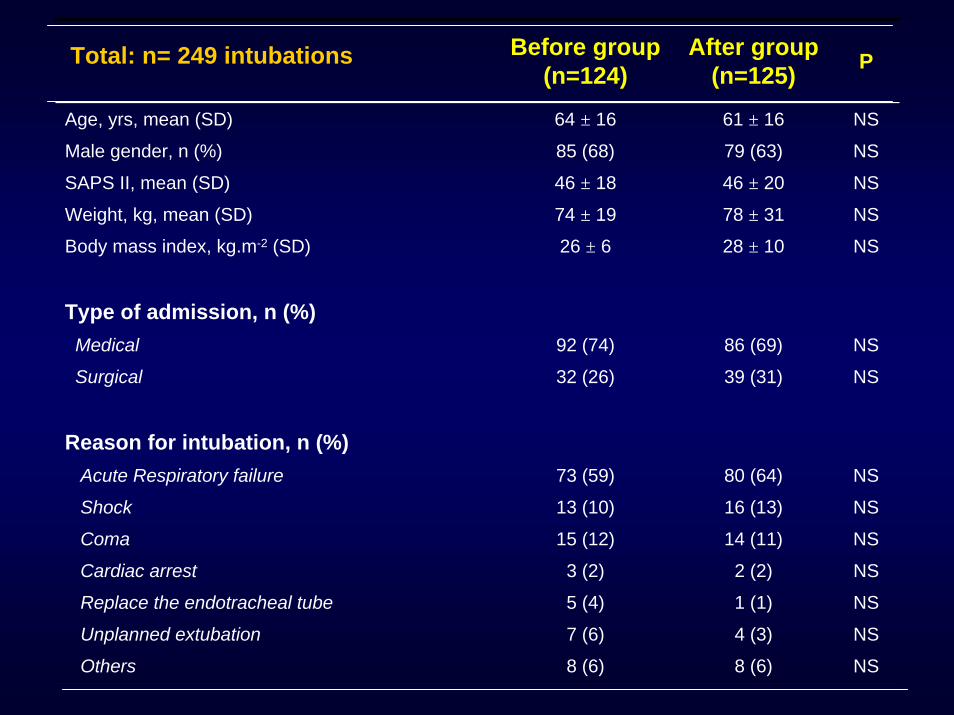
Before group(n=124)
After group(n=125) P
Age, yrs, mean (SD) 64 ± 16 61 ± 16 NS
Male gender, n (%) 85 (68) 79 (63) NS
SAPS II, mean (SD) 46 ± 18 46 ± 20 NS
Weight, kg, mean (SD) 74 ± 19 78 ± 31 NS
Body mass index, kg.m-2 (SD) 26 ± 6 28 ± 10 NS
Type of admission, n (%)Medical 92 (74) 86 (69) NS
Surgical 32 (26) 39 (31) NS
Reason for intubation, n (%)Acute Respiratory failure 73 (59) 80 (64) NS
Shock 13 (10) 16 (13) NS
Coma 15 (12) 14 (11) NS
Cardiac arrest 3 (2) 2 (2) NS
Replace the endotracheal tube 5 (4) 1 (1) NS
Unplanned extubation 7 (6) 4 (3) NS
Others 8 (6) 8 (6) NS
Total: n= 249 intubations
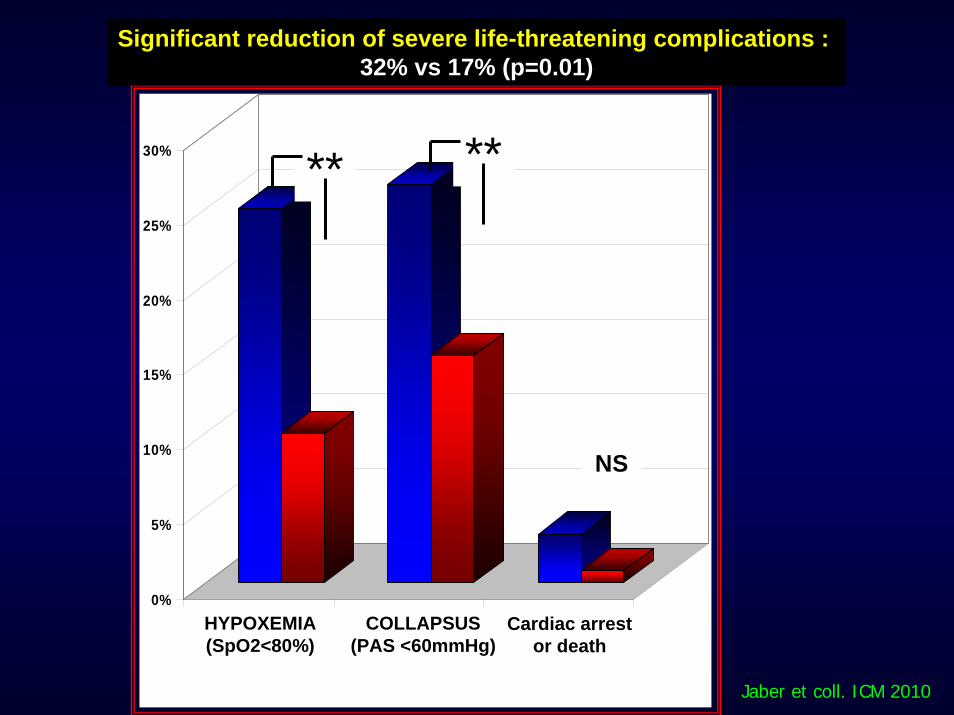
0%
5%
10%
15%
20%
25%
30%
Hypoxémie sévère Collapsus sévère Arrêt cardiaque oudécès
Stratégie libérale(n= 124)
Stratégie guidée par le protocole (n= 125)
****
NS
Significant reduction of severe life-threatening complications : 32% vs 17% (p=0.01)
HYPOXEMIA(SpO2<80%)
Cardiac arrestor death
COLLAPSUS(PAS <60mmHg)
Jaber et coll. ICM 2010
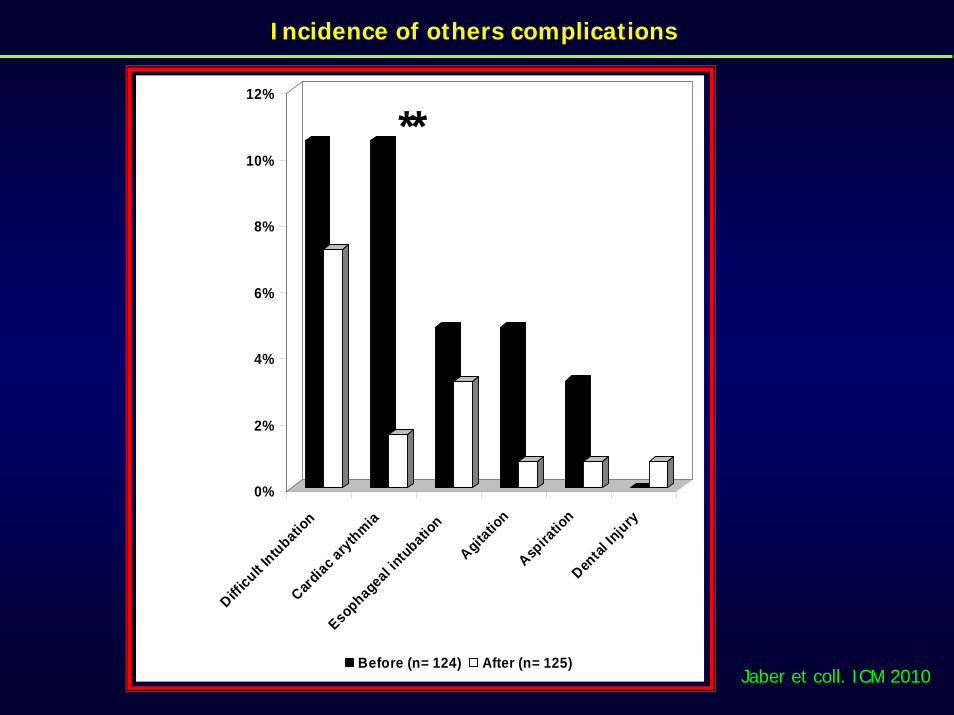
Incidence of others complications
0%
2%
4%
6%
8%
10%
12%
Difficult I
ntubation
Cardiac arythmia
Esophageal intubatio
n
Agitatio
nAsp
iratio
nDen
tal In
jury
Before (n= 124) After (n= 125)
**
0%
2%
4%
6%
8%
10%
12%
Difficult I
ntubation
Cardiac arythmia
Esophageal intubatio
n
Agitatio
nAsp
iratio
nDen
tal In
jury
Before (n= 124) After (n= 125)
**
Jaber et coll. ICM 2010
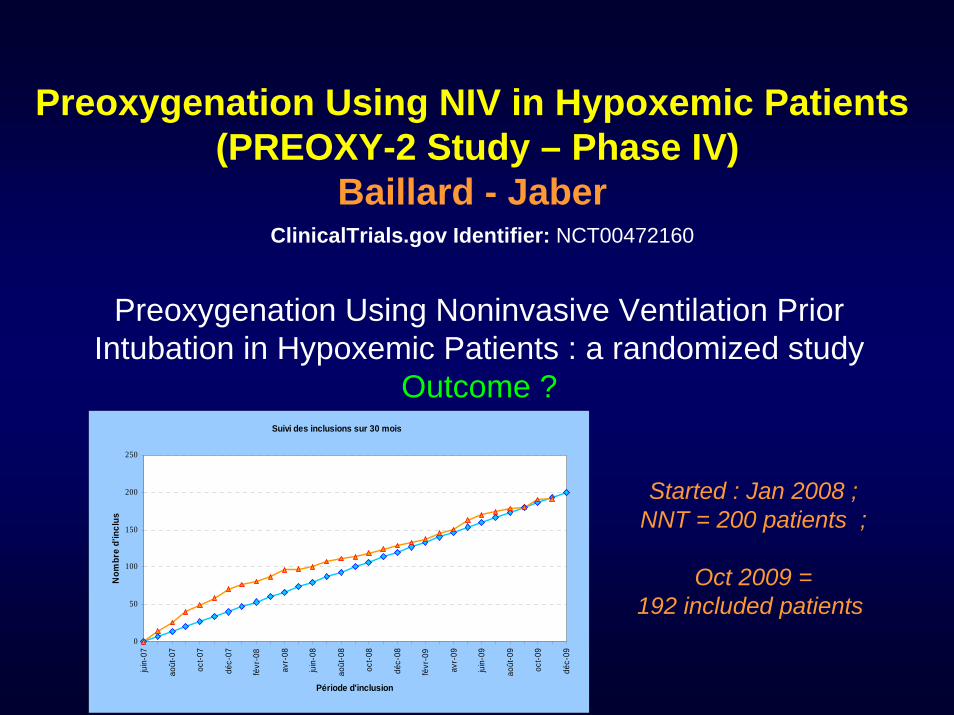
Preoxygenation Using NIV in Hypoxemic Patients (PREOXY-2 Study – Phase IV)
Baillard - JaberClinicalTrials.gov Identifier: NCT00472160
Preoxygenation Using Noninvasive Ventilation Prior Intubation in Hypoxemic Patients : a randomized study
Outcome ?
Started : Jan 2008 ; NNT = 200 patients ;
Oct 2009 = 192 included patients
Suivi des inclusions sur 30 mois
0
50
100
150
200
250
juin
-07
août
-07
oct-0
7
déc-
07
févr
-08
avr-
08
juin
-08
août
-08
oct-0
8
déc-
08
févr
-09
avr-
09
juin
-09
août
-09
oct-0
9
déc-
09
Période d'inclusion
Nom
bre
d'in
clus
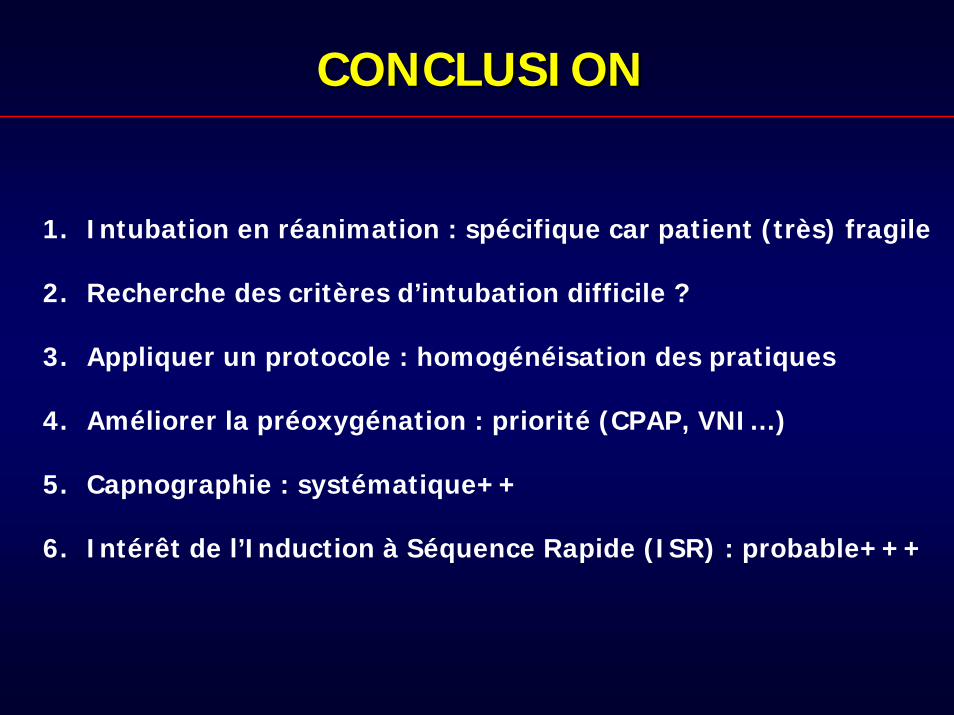
CONCLUSIONCONCLUSION
1. Intubation en réanimation : spécifique car patient (très) fragile
2. Recherche des critères d’intubation difficile ?
3. Appliquer un protocole : homogénéisation des pratiques
4. Améliorer la préoxygénation : priorité (CPAP, VNI…)
5. Capnographie : systématique++
6. Intérêt de l’Induction à Séquence Rapide (ISR) : probable+++
Many thanks…


![Traumatismes médullaires - sofia.medicalistes.fr · musculaire est en effet constante à partir de la 48e heure jusqu’à 6 à 12 mois après le traumatisme [11]. L’intubation](https://static.fdocuments.fr/doc/165x107/5e0f7ce8d458680f3759f707/traumatismes-mdullaires-sofia-musculaire-est-en-effet-constante-partir-de.jpg)