Risques la sant© et maladies professionnelles dans les
258
Risques à la santé et maladies professionnelles dans les industries alimentaires Volume 3 : maladies professionnelles Jacques Binet Janvier 1992 Département de Santé Communautaire de l'hôpital du Haut-Richelieu
Transcript of Risques la sant© et maladies professionnelles dans les

Risques à la santé et maladies professionnelles
dans les industries alimentaires
Volume 3 : maladies professionnelles
Jacques Binet
Janvier 1992
Département de Santé Communautaire de l'hôpital du Haut-Richelieu
CENTRE DE DOCUMENTATION Direction de la Santé publique de la Montérégle \ Complexe Cousineau
Table des matières " ^ ^ r H u ^ QU°-Loc'0" 3°°°
^ ^ _ J3Y6J I
Remerciements
Liste des tableaux
I n t r o d u c t i o n INSTITUT NATIONAL DE SANTÉ PUBLIQUE DU QUÉBEC
CENTRE DE DOCL'MENTATION MONTRÉAL
1 - Surdité et autres effets du bruit
Bibliographie
2 - Contraintes thermiques et santé
2.1 Chaleur
2.2 Froid
2.3 Prévention, contrôle et surveillance médicale
Bibliographie
3 - Travail posté et travail de nuit
Bibliographie v.
4 - Problèmes musculo-squelettiques
Bibliographie
5 - Zoonoses
Bibliographie
6 - Listériose
Bibliographie
Maladies respiratoires
7.1 Asthme professionnel et rhinite allergique
7.1.1 Méthode et dépistage et surveillance
7.1.2 Examens de la fonction respiratoire
7.1.3 Périodicité des examens
7.2 Asthme des boulangers
7.3 Alvéolite allergique
7.3.1 Manifestations cliniques
7.3.2 Examen clinique et laboratoire
7.3.3 Pronostic
7.3.4 Immunologie et pathologie
7.3.5 Dépistage des alvéolites allergiques
7.3.6 Information et prévention
7.4 Syndrome des poussières organiques
7.4.1 Etiologie potentielle
7.4.2 Diagnostic différentiel
7.4.3 Dépistage et prévention
7.5 Bronchite chronique
Bibliographie
Dermatoses
8.1 Dermatites irritatives
8.2 Dermatites de contact
8.2.1 Fruits et légumes
8.2.2 Prévention
8.3 Dermatites infectieuses
8.3.1 Virus
8.3.2 Infections fungiques
8.3.3 Infections bactériennes
8.3.4 Prévention des infections
Bibliographie
9 -
10-
Maladies dentaires d'origine professionnelle
Bibliographie
Risques chimiques
10.1 Asthme des empaqueteurs de viande
10.2 Bioxyde de carbone.
Bibliographie
Liste des tableaux
Tableau I Liste des causes principales d'asthme dans l'industrie alimentaire
Tableau n Synthèse des aspects médicaux à considérer dans l'asthme des boulangers
Tableau n i - Substances associées à l'alvéolite allergique
Tableau IV - Composition des poussières de grain
Tableau V Prévalence des dermatoses spécifiques chez les travailleurs des abattoirs
Tableau VI - Plantes culinaires présentant un risque de dermatite de contact
/
MALADIES RESPIRATOIRES
7.1 - Rhinite allergique et asthme professionnel
L'asthmë est une condition caractérisée par une hyperexcitabilité de la
trachée et des bronches due à des stimuli variés et se manifestant par un
rétrécissement réversible diffus des voies aériennes qui varie en gravité soit
spontanément soit suite à un traitement.
L'asthme professionnel est une forme d'asthme qui se trouve déclenché suite
à des expositions à des aérosols, des poussières, des gaz, des vapeurs, des
filmées etc... dans le milieu de travail (tableau I).
7.1.1 Méthode de dépistage et surveillance
Nous avons inclus en annexe le guide de surveillance pour l'asthme
professionnel préparé pour le territoire du DSC du Haut-Richelieu.
Le guide n'est pas spécifique au domaine dé l'alimentation.
L'utilisation d'un questionnaire de dépistage de l'asthme est un outil
acceptable même s'il n'est pas encore standardisé. Selon Lebowitz
un questionnaire auto-administré peut souvent fournir des résultats
satisfaisants à condition qu'il soit complètement rempli. Il est
recommandé de l'administrer en début d'emploi pour établir une
ligne de base individuelle dans l'évolution des symptômes.
L'examen physique se fait souvent à la suite d'un questionnaire
positif et doit être pratiqué à la période où les symptômes se
présentent. C'est aussi une bonne occasion pour le médecin de
procéder à un questionnaire médical traditionnel, beaucoup plus
précis pour orienter le diagnostic.
Les causes d'asthme les plus importantes dans l'industrie alimentaire
sont principalement reliées au contact avec des animaux, des
produits végétaux, des champignons (tableau I)
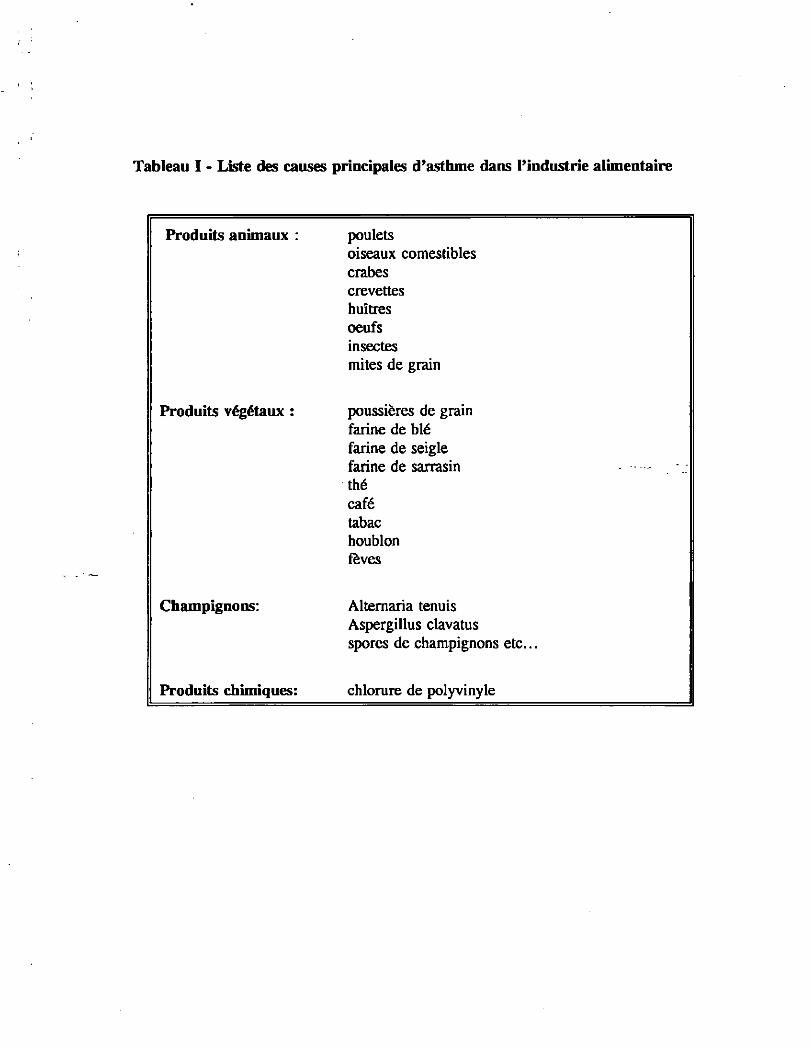
Tableau I - Liste des causes principales d'asthme dans l'industrie alimentaire
Produits animaux : poulets
oiseaux comestibles
crabes
crevettes
huîtres
oeufs
insectes
mites de grain
Produits végétaux : poussières de grain
farine de blé
farine de seigle
farine de sarrasin
thé
café
tabac
houblon
fèves
Champignons: Alternaria tenuis
Aspergillus clavatus
spores de champignons etc...
Produits chimiques: chlorure de polyvinyle
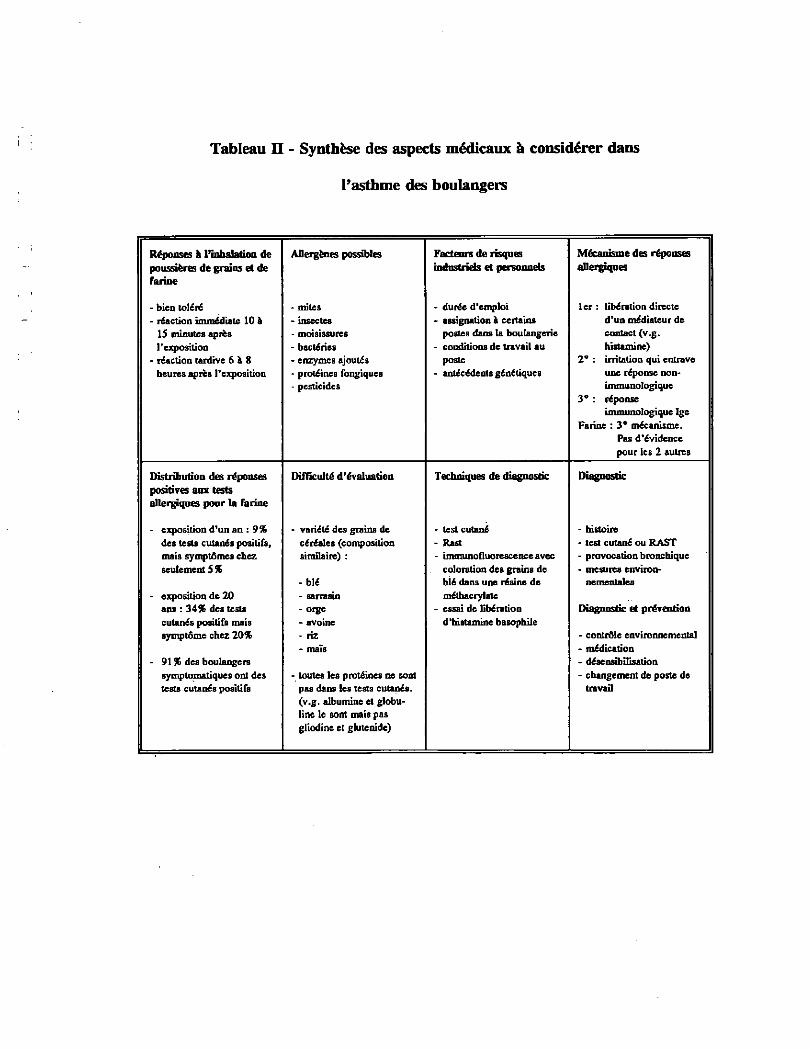
Tableau n - Synthèse des aspects médicaux
l'asthme des boulangers
à considérer dans
Réponses à l'inhalation de Allergèaes possibles Facteurs de risques Mécanisme des réponses poussières de grains et de industriels et personnels allergiques farine
- bien toléré - mites - durée d'emploi 1er : libération directe - réaction immédiate 10 h • insectes - assignation & certains d'un médiateur de
15 minutes après - moisissures postes dans ta boulangerie contact (v.g. l'exposition - bactéries - conditions de travail au histamine)
- réaction tardive 6 à 8 - enzymes ajoutés poste 2° : irritation qui entrave heures après l'exposition - protéines fongiques - antécédents génétiques une réponse non-
- pesticides immunologique 3° : réponse
immunologique Ige Farine : 3° mécanisme.
Pas d'évidence pour les 2 autres
Distribution des réponses Difficulté d'évaluation Techniques de diagnostic Diagnostic positives ans tests allergiques pour la farine
- exposition d'un an : 9% - variété des grains de - test cutané - histoire des tests cutanés positifs, céréales (composition - Rast - test cutané ou RAST mais symptômes chez similaire) : - immunofluorescence avec - provocation bronchique seulement 5 % coloration des grains de - mesures environ-
- blé blé dans une résine de nementales - exposition de 20 - sarrasin méthacrylate
ans : 34% des tests - orge - essai de libération Diagnostic et prévention cutanés positifs mais - avoine d'histamine basophile symptôme chez 20% - riz - contrôle environnemental
- mais - médication - 91 % des boulangers • désensibilisation
symptomaliques ont des - toutes les protéines ne sont - changement de poste de tests cutanés positifs pas dans les tests cutanés. travail
(v.g. albumine et globu-line le sont mais pas gliodine et glutenide)
- Alvéolite allergique ^ ^
Sous ce nom on trouve aussi les maladies suivantes : poumon du fermier,
pneumonite allergique extrinsèque, poumon du champignonniste, pneumonite
granulomateuse, pneumoconiose organique. L'alvéolite allergique est une
maladie granulomateuse interstitielle du poumon qui se manifeste suite à
l'inhalation répétée de particules de matière organique de 1 à 5 microns chez
un sujet prédisposé.
Le prototype de l'alvéolite allergique est le poumon du fermier, mais des
études plus récentes mettent en cause bien d'autres produits et quelques-uns
se retrouvent dans l'industrie alimentaire (tableau III). Pour cette raison nous
avons cru bon d'introduire quelques notions de base qui pourraient servir
plus amplement advenant des interventions en milieu agricole. La différence
entre l'alvéolite du fermier et celle des autres travailleurs vient de la
spécificité des antigènes de chaque produit respiré.
Ces agents partagent cependant en commun une caractéristique qui est la
grosseur des particules inhalées qui varient de 1 à 5 microns. Les particules
de 1 micron présentent la plus grande probabilité d'atteindre les alévoles
pulmonaires. On présente au tableau III une liste des principales activités
reliées directement ou indirectement à l'industrie alimentaire. Les produits
en cause sont réputés causer des alvéolites allergiques. Enfin, on ne peut
ignorer que les mêmes produits peuvent aussi déclencher des réactions
asthmatiques, d'où parfois la confusion au point de vue dépistage et
diagnostic.
7.3.1 Manifestations cliniques
Les diverses manifestations cliniques ont les caractéristiques
suivantes:
- 50% connaissent un début insidieux
- elles varient selon le niveau d'exposition
- souvent, il y a expositon prolongée à des moisissures, des
semaines ou des mois avant la première manifestation
- dyspnée progressive
- 1/3 des attaques sont typiques :
- frisson
- toux irritante et harassante
- dyspnée
- malaise
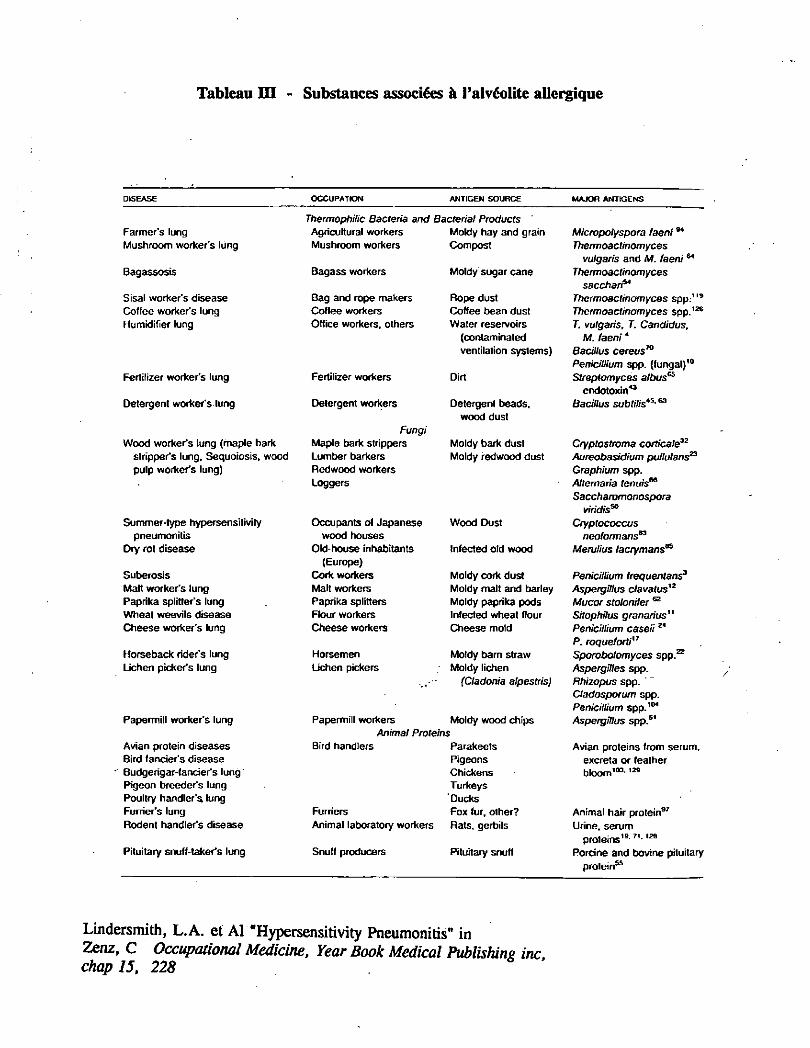
Tableau H I - Substances associées à l'alvéolite allergique
DISEASE OCCUPATION ANTIGEN SOURCE MAJOR ANTIGENS
Thermophilic Bacteria and Bacterial Products
Farmer's lung Agricultural workers Moldy hay and grain Micropotyspora faeni94
Mushroom worker's lung Mushroom workers Compost Thermoactinomyces
vulgaris and M. faeni64
Bagassosis Bagass workers Moldy sugar cane Thermoactinomyces
sacchari*4
Sisal worker's disease Bag and rope makers Rope dust Thermoactinomyces spp.119
Coffee worker's lung Coffee workers Coffee bean dust Thermoactinomyces spp.126
Humidifier lung Office workers, others Water reservoirs T. vulgaris, T. Candidas,
(contaminated M. faeni4
ventilation systems) Bacillus cereus70
Pénicillium spp. (fungal)10
Fertilizer worker's lung Fertilizer workers Dirt Streptomyces a/bus65
endotoxin43
Detergent worker's lung Detergent workers Detergent beads, Bacillus subtilis4S-63
wood dust Fungi
Wood worker's lung (maple bark Maple bark strippers Moldy bark dust Cryptostroma corticale32
stripper's lung, Sequoiosis, wood Lumber barkers Moldy redwood dust Aureobasidium pullulans23
pulp worker's lung) Redwood workers Graphium spp. Loggers Altemaria tenuis66
Saccharomonospora
viridis50
Summer-type hypersensitivity Occupants of Japanese Wood Dust Cryptococcus pneumonitis wood houses neoformans83
Dry rot disease Old-house inhabitants Infected old wood Meruiius lacrymans86
(Europe) Suberosis Cork workers Moldy cork dust Pénicillium frequentans3
Malt worker's lung Malt workers Moldy malt and barley Aspergillus clavatusy2
Paprika splitter's lung Paprika splitters Moldy paprika pods Mucor stolonifer 62
Wheat weevils disease Flour workers Infected wheat flour Sitophilus granarius" Cheese worker's lung Cheese workers Cheese mold Pénicillium caseu 24
P. roqueforti17
Horseback rider's lung Horsemen Moldy barn straw Sporobolomyces spp.22
Lichen picker's lung Uchen pickers Moldy lichen Aspergilles spp. (Cladonia alpestris) Rhizopus spp.
Cladosporum spp. Pénicillium spp. t04
Papermill worker's lung Papermill workers Moldy wood chips Aspergillus spp.6' Animal Proteins
Avian protein diseases Bird handlers Parakeets Avian proteins from serum. Bird fancier's disease Pigeons excreta or feather Budgerigar-fancier's lung ' Chickens b l o o m ' 0 3 - 1 2 9
Pigeon breeder's lung Turkeys Poultry handler's lung 'Ducks Furrier's lung Furriers Fox fur, other? Animal hair protein97
Rodent handler's disease Animal laboratory workers Rats, gerbils Urine, serum proteins'9-7 '-128
Pituitary snuff-taker's lung Snuff producers Pituitary snuff Porcine and bovine pituitary protein"
Lindersmith, L.A. et Al "Hypersensitivity Pneumonitis" in
Zenz, C Occupational Medicine, Year Book Medical Publishing inc chap 15, 228
- céphalée
- fièvre de 100° à 106°F après 4 à 8 heures d'exposition
- hémoptysie légère
- absence de sibilance sauf si l'asthme est concomittant
7.3.2 Examen clinique et laboratoire
A l'examen clinique, on observe :
- des râles basilaires plusieurs jours après le début
- il y a possibilité de cyanose
A l'examen de laboratoire on observe :
- leucocytose et éosinophilie
7.3.3 Pronostic
Si le sujet s'éloigne de l'allergène, dans 10 à 12 heures les
symptômes diminuent graduellement sur une période de 2 semaines.
Occasionnellement la dyspnée persiste plusieurs mois. Si les attaques
sont fréquentes les symptômes augmentent : anorexie, perte de poids
suivi d'un stage irréversible d'insuffisance pulmonaire et du
ventricule droit ou coeur pulmonaire. Dans 1 à 15% des cas, la
maladie est insidieuse avec tendance à développer plus tard des
attaques aiguës typiques.
7.3.4 Immunologie et pathologie
Cette partie du sujet dépasse le besoin du présent document mais
pour ceux qui sont intéressés les références traitent bien ces aspects.
7.3.5 Dépistage des alvéolites allergiques
Il n'y a pas présentement de tests médicaux bien évalués disponibles
pour dépister les alvéolites allergiques. Possiblement, le dosage des
anticorps spécifiques selon les expositions précises pourraient être
envisagé, mais le coût-bénéfice serait la plus grande objection.
7.3.6 Information et prévention
L'information des travailleurs sur ces risques peut permettre un
dépistage plus précoce et le diagnostic des travailleurs déjà atteints.
Une infirmière et un médecin informés des symptômes ou des
maladies pulmonaires chez les travailleurs exposés peuvent les
diriger vers les experts aptes à compléter le diagnostic.
Les mesures préventives recommandées sont les suivantes :
- retrait de l'exposition à l'allergie pour les cas connus
- contrôle des poussières
- information des travailleurs
Syndrome des poussières organiques
Le syndrome des poussières organiques porte aussi le nom de "mycotoxicose
pulmonaire". Les symptômes similaires à l'influenza (grippe) apparaissent
à la suite d'expositions à des concentrations élevées de produits d'agriculture
et ce avec ou sans symptômes respiratoires et habituellement sans évidence
clinique ou radiologique d'alvéolite allergique (parfois l'alvéolite clinique est
présente).
7.4.1 Etiologie potentielle
Le syndrome des poussières organiques origine des poussières
contenant des moisissures, des bactéries ou d'autres agents non
identifiés. On observe 30 à 40% de prévalence chez les personnes
exposées. Les poussières en cause sont :
- l'ensilage, le grain (tableau IV), les copaux de bois, etc. dont la
caractéristique commune est d'être moisis ^ ç f ^ j ^ ^ J j ^ n ^
- la poussière de grain, de cochon, de volaille contaiCin^efSr^e?7
endotoxines.
7.4.2 Diagnostic différentiel
Ce syndrome se différencie de l'alvéolite allergique par les éléments
suivants :
1) une proportion élevée des individus exposés deviennent
symptomatiques
2) les niveaux de concentration environnementale sont toujours très
élevés
3) aucun indice de maladie pulmonaire progressive en dépit
d'expositions répétées
4) dans la plupart des cas les anticorps sériques ne sont pas détectés
5) le lavage alvéolaire pendant la phase aiguë révèle une
prédominance de neutrophiles plutôt que de lymphocytes
6) la biopsie montre des inflammations mais sans granulome.
7.4.3 Dépistage et prévention
Aucun questionnaire ou test n'est valable jusqu'à présent bien que
cela serait probablement utile. L'information aux travailleurs de
l'existence de cette entité pathologique peut aider au dépistage. La
prévention peut se faire par la protection personnelle et le contrôle
de poussières.
Bronchite chronique
Chez presque tous les groupes de travailleurs exposés à des poussières
organiques on peut retrouver des bronchites chroniques. Cependant, comme
pour les soudeurs, établir la relation avec le travail n'est pas toujours facile
en particulier chez les fumeurs. Il existe par contre certaines études qui
tendent à démontrer que pour des groupes de travailleurs précis tels que les
mélangeurs de farine et les boulangers, la prévalence d'une maladie pul-
monaire obstructive serait plus élevé comparée à des groupes de contrôle.
Ces études sont basées sur la présence de symptômes sur des mesures des
fonctions respiratoires.
Dépistage
Le dépistage de la bronchite est complexe vu que ces travailleurs peuvent
présenter aussi de l'asthme. Les questionnaires existants ne couvrent pas
nécessairement les deux pathologies bien que les tests de fonctions
respiratoires s'appliquent bien aux deux. Le médecin responsable devra
choisir les moyens de dépistage aux fins de ce qu'il veut rechercher. Dans
le cas de la bronchite chronique le questionnaire ATS est valable. Le
diagnostic précis se fera avec la connaissance précise du milieu de travail,
de l'histoire du travailleur et des tests pulmonaires.
Tableau IV - Composition des poussières de grain
Grain de céréales (blé, orge, sarrasin, avoine, maïs et produits de
désintégration)
Pesticides (tétraclorure de carbone, malathion, bromure de méthyl,
phosphate d'aluminium, disulfure de carbone)
Débris de mammifère et débris avaires (poids et excréments des
rongeurs, pigeons)
Fungus et leurs métabolites (alfatoxine)
Pollens
Endotoxines bactériennes
Parties d'insectes
Mites
Silices
Maladies respiratoires
Asthme professionnel
Bibliographie
BERITIC-STAHULJAK, D., VALIC, F. et al., "Simultaneous Exposure to Airborne Flour
Particles and Thermal Load as Cause of Respiratory Impairment", Int. Arch. Occup.Environ. Health, vol. 37, pp. 193-203, (1976).
BJÔRKSTÉN, F., BACKMAN, A. et al., "Immunoglobulin E specific to wheat and rye flour
proteins", Clinical Allergy, vol. 7, pp. 473-483, (1977).
BLANDS, J., DIAMANT, B. et al., "Flour Allergy in Bakers", Int. Archs Allergy appl. Immun., vol. 52, pp. 392-406, (1976).
BLOCK, G., TSE K.S. et al., "Baker's asthma" Clinical Allergy, vol. 14, pp. 177 - 185 (1984).
BOURBEAU, J., "Occupational Asthma : A Patient-Oriented Approach", Canadian Journal of CME, (November/December 1990).
CHAN-YEUNG, M. , "State of Art. Occupational Asthma.", Am. Rev. Respir. Dis., vol: 133,
pp. 686-703, (1988).
DSC HAUT-RICHELIEU, Guide de surveillance médicale pour l'asthme professionnel, avril 1991.
HENDRICK, D.J., DAVIES, R.J. et al., "Baker's Asthma", Clinical Allergy , vol. 6, pp. 241-
250, (1976).
HERENG, M. P., DEMARTEAU, S. et al., "Evaluation du degré de sensibilisation aux
allergènes professionnels et de l'incidence de l'asthme dans une population de boulangers d'une
industrie de la région liégeoise", Cahiers de médecine du travail, vol. XXV, no. 4, (1989).
LEHRER, S.B., "Bean Hypersensitivity in Coffee Workers' Asthma : A Clinical and
Immunological Appraisal" Allergy Proceedings, vol. 11, no. 2, pp. 65-66, (1990).
LEHRER, S.B., "Hypersensitivity Reactions in Seafood Workers", Allergy Proceedings, vol.
11, no. 2, pp. 67-68, (1990).
MALO, J.L., "L'asthme professionel - Rapport du comité spécial de la Société de thoracologie
du Canada", Le Clinicien, (mars 1988).
MC NUTT, G.M., "Screening for Occupational Asthma : A Word of Caution", Journal of Occupational Medicine, vol. 33 no. 1, pp. 19-22, (1991).
MUSK, A.W., VENABLES, K.M., "Respiratory Symptoms, Lung Function, and Sensitisation
to Flour in a British Bakery", British Journal of Industrial Medicine, vol. 46, pp. 636-642,
(1989).
"Occupational Disease Surveillance : Occupational Asthma", Morbidity and Mortality Weekly Report, vol. 39, no. 7, pp. 119-123, (23 fév. 1990).
O'NEIL, C., "Occupational Respiratory Diseases Resulting from Exposure to Eggs, Honey,
Spices and Mushrooms", Allergy Proceedings, vol. 11, no. 2, pp. 69-70, (1990).
PRICHARD, M.G., RYAN, G. et al., "Wheat flour sensitisation and airways disease in urban
bakers", British Journal Industrial Medicine, vol. 41, pp. 450-454, (1988).
TSE, K.S., "Grain Dust Asthma" Allergy proceedings, vol. 11, no. 2, pp. 61-62, (1990).
ZUSKIN, E., KANCELJAK, B. et al., "Acute Effects of Herbal Tea Dust Extracts on Lung
Function", Chest, vol. 96/6, (december 1989).
* Articles joints
** Le texte est inclus dans le Guide de surveillance médicale pour l'asthme professionnel (ci-
joint).
64
Int.AVclïioc&p.'ïitoviron**II1 tft" "193-203 ( 197G) •
AILIWS IH <Kl1l|MllhNUll I I IH I l'jllVil*4HIIIN*llltll llcahli . TN SptIIIIVI \»N!.ir
r-
1 ' re
I c
t y
ive
)
and
Simultaneous Exposure to Airborne Flour Particles and Thermal Load as Cause of Respiratory Impairment
DUNJA BERITIÔ-STAHUUAK. F. VAUC. MIRA CIGULA. and D. BUTKOVIÔ
Andrija Stamper School of Public Health, Zagreb University,
Rockefellerova 4, Zagreb, Yugoslavia
Summary. In order to estimate whether only simultaneous exposure to both
airborne flour particles and unfavorable thermal environment alone cause th»
development of nonspecific respiratory disease or whether sole exposure t.-
flour aerosols is likely to cause impairment of the respiratory system, a
group of 80 millers and 130 bakers, all nonsmokers, were examined. Both
millers and bakers were exposed to approximately the same concentration cr
airborne flour particles but the latter worked under considerable thermal
load. It was found that between millers and bakers the difference in the preva-
lence of respiratory symptoms was not statistically significant. Although
the differences between the mean measured and the mean predicted venti-
latory function parameters (FVC, FEVj, PEF, KEF 50*., MEF 75*) were signifi-
cant both in millers and bakers, they did not differ significantly between
these two groups. This finding suggests that exposure to flour dust may
cause the development of chronic nonspecific respiratory disease and a re-
duction of ventilatory lung capacity..irrespective of simultaneous heat
load.
Key words: Flour particles - Thermal load - Respiratory impairment.
! ;
i '
t :
i 5 • s
; Ji f
'c " I N T R O D U C T I O N
R a m a z z i n i , a s e a r l y a s t h e 1 8 t h - c e n t u r y , d e s c r i b e d o c c u p a t i o n a l a s t h m a c a u s e d b y f l o u r p a r t i c l e s [ 2 9 ] . A n u m b e r o f p u b l i c a t i o n s c a n b e f o u n d l a t e r i n t h e l i t e r a t u r e d e s c r i b i n g a l l e r g i c e f f e c t s o f f l o u r i n t h e f o r m o f b r o n c h i a l a s t h m a a n d r h i n i t i s i n b a k e r s a n d m i l l e r s [ l , 6 , 8 , 1 0 - 1 6 , 1 9 - 2 2 , 2 7 , 3 2 , 3 3 ] . I n a p r e v i o u s p u b l i -c a t i o n w e s h o w e d t h a t t h e l o n g - t e r m e x p o s u r e t o f l o u r p a r t i c l e s b r i n g s a b o u t r e s p i r a t o r y s y m p t o m s a n d i m p a i r m e n t o f v e n t i l a t o r y l u n g c a p a c i t y i n b a k e r s [ 3 4 ] . H e s t u d i e d t h e r e l a t i o n s h i p b e -t w e e n h y p e r s e n s i t i v i t y t o f l o u r a n d t h e p r e v a l e n c e o f c h r o n i c b r o n c h i t i s i n b a k e r s [ 4 ] . E x a m i n i n g t h e r o l e o f b a c t e r i a l a n d f u n g a l f l o r a i n t h e d e v e l o p m e n t o f c h r o n i c b r o n c h i t i s i n b a k e r s w e f o u n d n o s i g n i f i c a n t d i f f e r e n c e i n t h e f r e q u e n c y o f p a t h o -g e n i c , a g e n t s i n b a k e r s w i t h a n d w i t h o u t c h r o n i c b r o n c h i t i s . , : , i ••• . ' / K 7;
s : ' 'Cf.,: 193
. ' - T h i s ' o b s e r v a t i o n t o g e t h e r w i t h t h e f i n d i n g t h a t a m o n g t h e b a k e r s ,
. . i n w h o s e e x p e c t o r a t i o n s p r e d o m i n a n t l y p a t h o g e n i c a g e n t s w e r e i s o l a t e d , t h e r e w e r e m a n y w i t h o u t c h r o n i c b r o n c h i t i s ^ h a s g i v e n
- g r o u n d t o t h e a s s u m p t i o n t h a t i n b a k e r s 1 c h r o n i c b r o n c h i t i s i t i s n o t i n f e c t i o n t h a t p l a y s t h e m o s t i m p o r t a n t r o l e [ 5 j . E x a m -i n i n g . a p o s s i b l e d i r e c t p h a r m a c o d y n a m i c e f f e c t o f f l o u r p a r - . ; t i c l e s o n t h e r e s p i r a t o r y s y s t e m we s h o w e d t h e p r e s e n c e o f a g e n t s t h a t c o n t r a c t s m o o t h m u s c l e s [ 3 5 ] .
A l l p r e v i o u s s t u d i e s o f t h e i n f l u e n c e o f f l o u r p a r t i c l e s o n t h e v e n t i l a t o r y l u n g c a p a c i t y a n d t h e d e v e l o p m e n t o f r e s p i r a t o r y s y m p t o m s h a v e b e e n c o n d u c t e d i n b a k e r s . B a k e r s , a s a r u l e , a r e e x p o s e d n o t o n l y t o f l o u r p a r t i c l e s b u t a l s o , s i m u l t a n e o u s l y , t o u n f a v o r a b l e t h e r m a l c o n d i t i o n s . I t i s , t h e r e f o r e , i m p o s s i b l e t o r u l e o u t t h e a d d i t i o n a l i n f l u e n c e o f t h e r m a l f a c t o r s i n t h e d e v e l o p m e n t o f n o n s p e c i f i c l u n g d i s e a s e i n b a k e r s . I n o r d e r t o a s s e s s q u a n t i t a t i v e l y s e p a r a t e c o n t r i b u t i o n s o f e x p o s u r e t o f l o u r d u s t a n d u n f a v o r a b l e t h e r m a l e n v i r o n m e n t , w e s t u d i e d t w o p o p u l a t i o n g r o u p s e x p o s e d t o s i m i l a r a i r b o r n e c o n c e n t r a t i o n s o f f l o u r d u s t b u t w o r k i n g . u n d e r s i g n i f i c a n t l y d i f f e r e n t t h e r m a l c o n d i t i o n : a g r o u p o f m i l l e r s e x p o s e d t o f l o u r p a r t i c l e s u n d e r n o r m a l t h e r m a l - c o n d i t i o n s a n d a g r o u p o f b a k e r s s i m u l t a n e o u s l y e x p o s e d t o f l o u r p a r t i c l e s a n d t o a c o n s i d e r a b l e t h e r m a l l o a d .
P O P U L A T I O N A N D M E T H O D S
Sample. 1 6 3 m i l l e r s a n d 3 2 2 b a k e r s w e r e e x a m i n e d . D a t a , o n 8 0 m i l l e r s a n d 1 3 0 b a k e r s ( n o n s m o k e r s ) w e r e p r o c e s s e d i n d e t a i l i n o r d e r t o e x c l u d e t h e a d d i t i o n a l e f f e c t o f s m o k i n g o n t h e v e n t i -l a t o r y f u n c t i o n a n d t h e d e v e l o p m e n t o f r e s p i r a t o r y s y m p t o m s . T h e a g e d i s t r i b u t i o n o f t h e l a t t e r w a s v e r y s i m i l a r , t h e m e a n a g e o f t h e m i l l e r s b e i n g 3 7 y e a r s , a n d o f t h e b a k e r s 3 7 . 5 y e a r s T h e y d i f f e r e d l i t t l e i n t h e i r a v e r a g e l e n g t h o f s e r v i c e ( m i l -l e r s : 1 6 . 1 y e a r s ; b a k e r s : 1 7 . 5 y e a r s ) .
.tows* I*?*1
v a l u e s Jw c a l c u l a A-• •
C o m m u n i t u s i n g 'W c a l c u l a ; f a c t u r e - v c h a n g e s " c u r v e s t h e m a x 75%) o f • c u r v e s b y P e t e l a t e d u
Respirat
s t a r : d a r
RESULTS
Assessn
The res the wor sented in sev€ mg/m-* ; centrât and the and the The gee m g / m 3 , 1 . 0 9 a r lers at*
E v a l u a t i o n of Hork Environment. H e x h l e t t w o - s t a g e d u s t s a m p l e r s w e r e u s e d f o r t h e s a m p l i n g o f t o t a l a n d r e s p i r a b l e p a r t i c l e s [ 3 8 ] . A i r t e m p e r a t u r e , h u m i d i t y , a i r m o t i o n , a n d r a d i a n t h e a t w e r e m e a s u r e d w i t h s t a n d a r d f i e l d i n s t r u m e n t s . C o r r e c t e d e f f e c t i v e t e m p e r a t u r e (CET) [2] w a s r e a d a n d w e t b u l b g l o b e t e m p e r a t u r e (WBGT) [ 3 8 ] a n d h e a t s t r e s s i n d e x b y B e l d i n g a n d H a t c h ( H S I ) [ 3 ] w e r e c a l c u l a t e d . - . . .
Ventilatory Function. - P u l m o n o r s p i r o m e t e r s V w e r e u s e d f o r t h e m e a s u r e m e n t o f t h e ^ f o r c e d v i t a l c a p a c i t y (FVC). a n d t h e f o r c e d e x p i r a t o r y v o l u m e i n t h e f i r s t - s e c o n d ( F E V ^ ) . F i v e m e a s u r e m e n t s .. w e r e t a k e n i n e a c h s u b j c c t a n d t h e m e a n , o f - t h e t w o h i g h e s t (.
Jones Mtxlic.il Instrument 0»., 2(K> Windsor Br., O.ikbroak, 111'., USA.
Evaluat
T h e r e s a n d t h < s e n t e d a s c o r i a n d a s l a t i o n p r e s s i < w h e r e l
* Enone m»:
b a k e r s ,
c
i v c n
s i t
«ani-
o n
a t o r y a r e
L b l e - h e
r t o
: w o n s o f
\ 1 e r
a s l y Dad.
il in
...n
rears
v a l u e s w a s t a k e n a s - t h o / r c s u l t . j . P r c d i c t e ^ . n o r m a ] v a l u e r , w o r ^ ' c a l c u l a t c d u s i n a t h c t a b l e s b f t h e E u r o p e a n - C o a l a n d M o e ï V C o n u n u n i t y [ 7 ] , T h c p e a k e x p i r a t o r y • f l o w " ( P C F ) w a s m e a s u r e J u s i n g W r i g h t 1 s i n s t r u m e n t * . T h e p r e d i c t e d n o r m a l v a l u e s w e r e
c a l c u l a t e d u s i n g t h c p r e d i c t i o n e q u a t i o n p r o v i d e d b y t h e m a n u -f a c t u r e r [ 3 l ] , F o r t h e d e t e c t i o n o f p o s s i b l e o b s t r u c t i v e c h a n g e s i n s m a l l a i r w a y s . t h e m a x i m u m e x p i r a t o r y f l o w - v o l u m e ~ c u r v e s w e r e r e c o r d e d i n a s m a l l e r q r o u p o f w o r k e r s o n w h i c h t h e m a x i m u m e x p i r a t o r y f l o w a t 50%. (MEF 50V.) a n d a t 7 0 : 0-iKF 75%) o f t h c c o n t r o l v i t a l c a p a c i t y w e r e r e a d . T h c f l e w - v o l u n e c u r v e s w e r e r e c o r d e d b y m e a n s o f t h e f l o w - v o l u m e s p i r o m e t e r ' b y P e t e r s e t a l . [ 2 8 ] . T h c p r e d i c t e d n o r m a l v a l u e s w e r e c a l c u -l a t e d u s i n g t h e e q u a t i o n s b y C h e r n i a k a n d R a b e r [ 9 j .
Respiratory Symptoms. R e s p i r a t o r y s y m p t o m s w e r e r e c o r d e d u s i n g t h e s t a n d a r d B r i t i s h M e d i c a l R e s e a r c h C o u n c i l Q u e s t i o n n a i r e _ 2 4 _ .
RESULTS
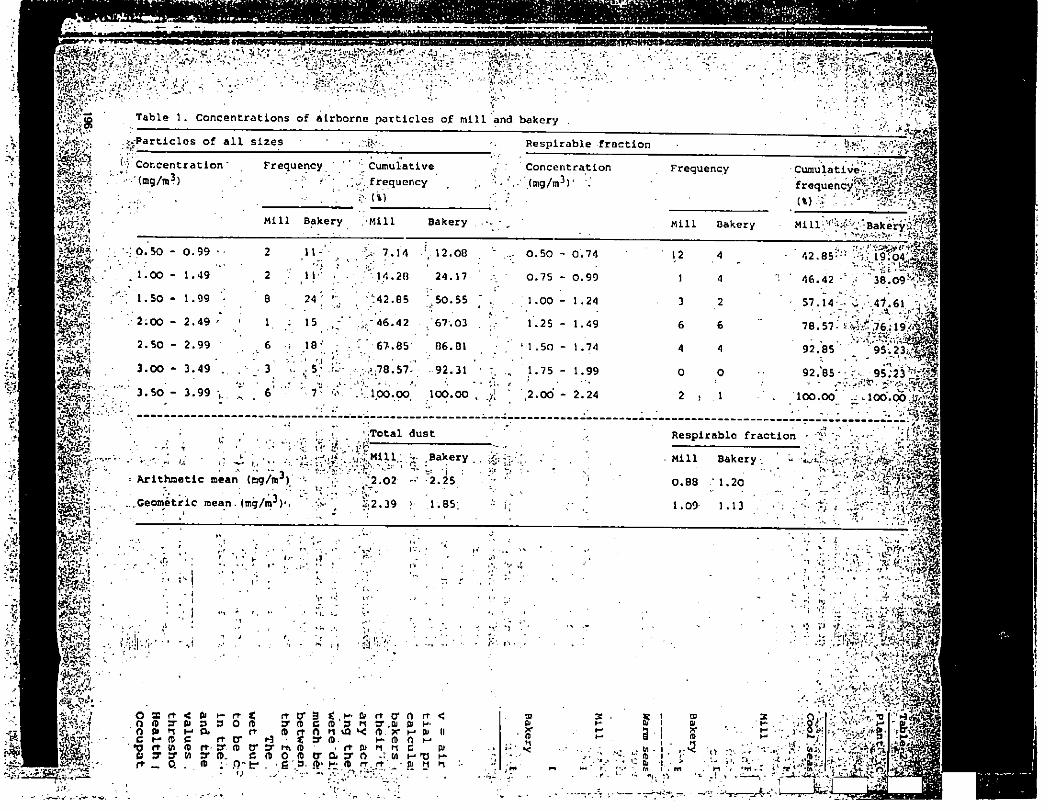
A s s e s s m e n t o f D u s t E x p o s u r e
T h e r e s u l t s o f t h e d e t e r m i n a t i o n o f a i r b o r n e f l o u r p a r t i c l e s i n t h e w o r k i n g e n v i r o n m e n t s o f t h e m i l l a n d t h e b a k e r y a r e p r e -s e n t e d i n T a b l e 1 a s c u m u l a t i v e f r e q u e n c i e s o f c o n c e n t r a t i o n s i n s e v e n c o n c e n t r a t i o n c l a s s e s ( t o t a l p a r t i c l e s : 0 . 5 0 - 3 . 9 9 m g / m 3 ; r e s p i r a b l e p a r t i c l e s : 0 . 5 0 - 2 . 2 4 m g / m 3 ) . T h e m e a n c o n -c e n t r a t i o n s o f t o t a l p a r t i c l e s w e r e 2 . 0 2 m g / m 3 a n d 2 . 2 5 m g / m 3 , a n d t h e m e a n c o n c e n t r a t i o n s o f r e s p i r a b l e p a r t i c l e s i n t h e m i l l a n d t h e b a k e r y w e r e 0 . 8 8 m g / m 3 a n d 1 . 2 0 m g / m 3 , r e s p e c t i v e l y . T h e g e o m e t r i c m e a n s f o r t o t a l p a r t i c l e s w e r e 2 . 3 9 a n d 1 . 8 5 . m g / m 3 , a n d f o r r e s p i r a b l e p a r t i c l e s i n t h e m i l l a n d t h e b a k e r y " 1 . 0 9 a n d 1 . 1 3 m g / m 3 , r e s p e c t i v e l y . T h e e x p o s u r e l e v e l s , c f ' m i l -l e r s a n d b a k e r s w e r e f o u n d t o b e s i m i l a r .
'ere
E v a l u a t i o n o f T h e r m a l E x D O S u r e
.ve
•e
e d
•^nts
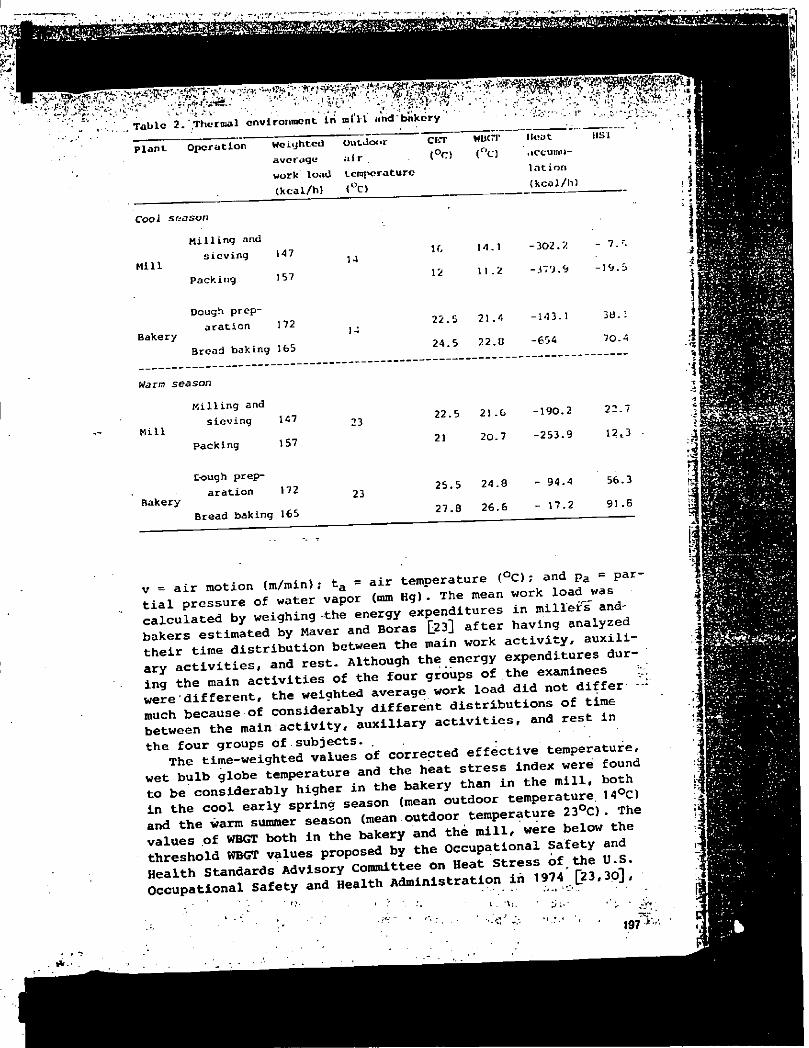
T h e r e s u l t s o f t h e m e a s u r e m e n t s o f t h e r m a l f a c t o r s in t h e m i l l
a n d t h e b a k e r y i n t w o d i f f e r e n t s e a s o n s o f t h e y e a r a r e p r e -
s e n t e d i n T a b l e 2 . T h e l e v e l o f t h e r m a l e x p o s u r e i s e x p r e s s e d
a s c o r r e c t e d e f f e c t i v e t e m p e r a t u r e , w e t b u l b g l o b e t e m p e r a t u r e
a n d a s h e a t s t r e s s i n d e x b y B e l d i n g a n d H a t c h . H e a t a c c u m u -
l a t i o n , e x p r e s s e d i n k c a l / h , w a s c a l c u l a t e d u s i n g t h e e x -
p r e s s i o n [18] : A = M + 6 . 6 ( t r - 3 5 ) + 0 . 6 v 0 - 6 ( t a - 3 5 ) - 1 . 2 v° -6( 4 2 - p a ) ,
w h e r e M » e n e r g y e x p e n d i t u r e ( k c a l / h ) ; t r = g l o b e t e m p e r a t u r e ( ° C ) ;
2A i r m e d Ltd., Edinburgh, Scotland.
3Ensnerson Comp., Ltd., Cambridge, Ha., USA,
195
i l i i | .•v V"
» m*
m
Table 1. Concentrations of airborne particles of mill and bakery
rS'-Tn-.•svr V ^^««Jfc
i ./T» -«SI • M
:<>-Particles of all sizes
1 ? Concentration' '{mg/m
3)
Frequency
Mill Bakery
Cumulative
frequency
(iV
Mil 1 Bakery
50 - 0. 99
1. 00 - 1 . ,49
1. 50 - 1 . ,99
2. 00 - 2. ,49
2. 50 - 2. .99
3. 00 - 3, .49
3. 50 - 3. .99
2 11- 7>: s, 12.08
2 - • • 14.20 24.17
8 24 ; ;':42.85 ;.50.55
1 : 15 .;«' 46.42 . 67.03
6 ; 18; ; 85* 06.01
3 < ' • . • v^;78.57-' 92.31
6 " *-. c.
. -.100.00 100.00
Respirable fraction mm
Concentration
• \ ( m g / m3) ' ','
0.50 - 0.74
0.75 - 0.99
1.00 - 1.24
1.25 - 1.49
'1.50 - 1.74
1.75 - 1.99
.2.00 - 2.24
Frequency Cumulative'" f r e q u e n c V U ^ I ^ I
Mill Oakery Mill Bakery'â?/®'
12
1
3
6
4
O
2
•T .--'V 42.85:
46.42
57.14 V 47.61 ' : „'•" -A..1»
78.57.' ' ."r •'.» "'SV > j V 92.85 9S.23^
92.85- T-.. 95;23^'ip
îoo.oo ^
•Total dust
Arithmetic mean (mg/m3)
.Geometric mean, (mg/rn3)'*
:"JS,!+ - Mill Bakery : : ' "
• fc-.V" /'.•h,' -- "" * "i •: • Tr : • 2.02 . o • -2 • 39
2.25
1.65'
V
Respirable fraction
Mill Bakery
0.88 1.20
1.09 1.13
>n ' -V- . S J ^ m
y
isfes '
te-"
r I S :
A W* -
•
• Sf.'
- y. i. '••Wh'
O a i t < 6 i h f r î n O 7 & 3 3 O rt o a» n m a ft c H» ft c ft CP H •0 rtw <0 ft. 3*. it 0*2P
rr tX 3 t.H-û) r t c o rt< ? H C K ? h ff.Di & K It It 0 H û ^ ll .x H m II • î ff ft. H- ft 0 M rttft i ft Di H h C Ptf
fii ? y w s* o. c f t o f t c r a y o - W H ' O P -ft ^ Q .ft ; .<Vf iî' tt.ft T.-'.rT fil f ^
r-1- f
•-» U Qj •.* • tri
,.•3
r' M; . ""
•ï P y-::-'
Bakery
Packing
Dough prep-
aration 172
Bread baking 165
Warm season
Milling and
sieving Mill
Packing
147
157
23 22.5 21.6
21 20.7
190.2
253.9
22.7
12,3
Bakery
C-ough prep-
aration 172 23 25.5 24.8
27.8 26.6
94.4
17.2
56.3
91.6
V = air motion (m/min); t a = air temperature <°C); and PA= Par-
tial pressure of water vapor (mm Hg) . The mean work load was
r i c u ^ d b y weighing the energy expenditures „ ; «
s ; r r % " :id f s S r u t i r L
at :
ae e r t h : . c ^ y . - n -
a r y a c t i v i t i e s ^ a n d r e s t . A l t h o u g h t h e . e n e r g y « P e n a i t u r e s d u r -i n g t h e m a i n a c t i v i t i e s o f t h e f o u r ^ o u p s o r t h e e x a m i n e e s w e r e d i f f e r e n t , t h e w e i g h t e d a v e r a g e w o r k l o a d d i d n o t d i f f e r m u c h b e c a u s e o f c o n s i d e r a b l y d i f f e r e n t d i s t r i b u t i o n s o f t i m e b e t w e e n t h e m a i n a c t i v i t y , a u x i l i a r y a c t i v i t i e s , a n d r e s t in
t h 6T ^ ° U t i m e - w e i g h t e ^ v a l u e s " o f c o r r e c t e d e f f é c t i v e t e m p e r a t u r e
w e t b u l b g l o b e t e m p e r a t u r e a n d t h e h e a t s t r e s s i n d e x w e r e f o u n d t o b e c o n s i d e r a b l y h i g h e r i n t h e b a k e r y t h a n i n t h e m i l l , b o t h I n t h e c o o l e a r l y s p r i n g s e a s o n ( m e a n o u t d o o r t e m p e r a t u r e AC)
a n d t h e w a r m s u n d e r s e a s o n ( m e a n - t d o o r ^ m p e r a t u r e 2 3 C ) . T h e v a l u e s o f WBGT b o t h i n t h e b a k e r y a n d t h e m i l l , w e r e D e x o
WBGT v a l u e s p r o p o s e d b y ^ O c c u p a t i o n a j a f j t y n d H e a l t h S t a n d a r d s A d v i s o r y C o m m i t t e e o n H e a t S t r e s s o r O c c u p a t i o n a l S a f e t y a n d H e a l t h A d m i n i s t r a t i o n i n 1 9 7 4 ^ 2 3 . 3 0 j ,
Sj|
197 - IV .
I K ' '
Wï:?; «Vi'-.V/i y^'lr-
J* '.V. ' ; V 3FV
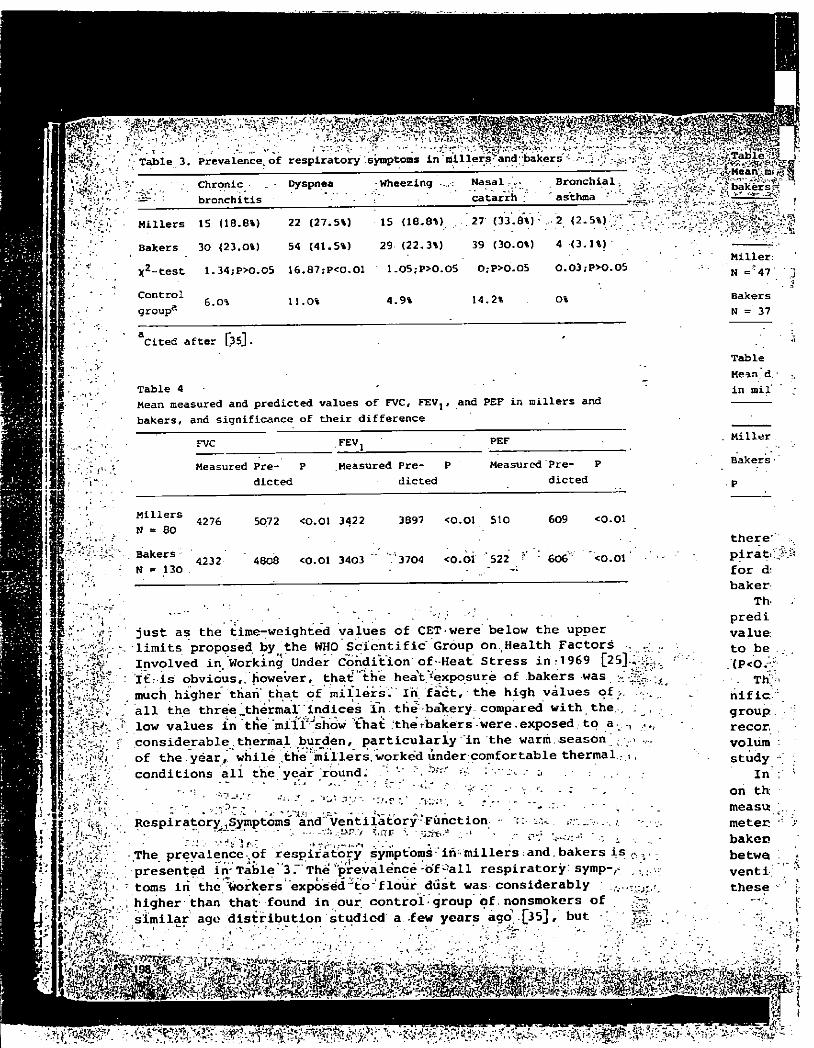
Table 3. Prevalence^of respiratory'.symptoms in m i l l e r s a n d b a k e r s :
f.- T:
J :
. '4
- - '
y1
'..•c'r-.*'-:/.-.
Chronic
bronchitis
Dyspnea Wheezing Nasal
catarrh
Bronchial
asthma
Table
«vMean im S. » -Ï3 v* bakers-
Millers 15 (18.6%) 22 (27.5%) 15 (18.8%) . . 27" (33.8%)• . 2 (2. 5%)
Bakers 30 (23.0%) 54 (41.5%) 29 (22.3%) 39 (30.0%) 4 (3. 1%)
X2- t e s t 1. 34;P>O.OS 16. 87 ?P<0.01 1. 05;P>0.05 0; P>0.05 0.03; P>0.05
Control
group3
6. o% 11. 0% 4. 9% 14. 2% o%
Cited after [35].
Table 4 -
Mean measured and predicted values of FVC, FEVj, and PEF in millers and
j u s t a s t h e t i m e - w e i g h t e d v a l u e s o f CET w e r e b e l o w t h e u p p e r . l i m i t s p r o p o s e d b y t h e WHO S c i e n t i f i c G r o u p o n . , H e a l t h F a c t o r s
I n v o l v e d i n " W o r k i n g U n d e r C o n d i t i o n o f - H e a t S t r e s s i n ' : 1 9 6 9 [ 2 5 ] . . : l € ; i s o b v i o u s h o w e v e r , t h a £ " t h e h e a V ^ ' e x p o s u r e o f . . b a k e r s w a s
m u c h h i g h e r t h a n t h a t o f m i l l e r s - I n f a c t , t h e h i g h v a l u e s o£ a l l t h e t h r e e ^ t h e r m a l i n d i c e s i n t h e - b a T t e r y c o m p a r e d w i t h t h e , l o w v a l u e s £ n ' t l i e ' m i i ï ^ s t i w 7 t h a t : t h e V b a k e ' r s " - w e r e . e x p o s e d . . . . t o a^ . . , c o n s i d e r a b l e t h e r m a l b u r d e n , p a r t i c u l a r l y i n t h e w a r m . s e a s o n . o f t h e y e a r , , w h i l e t h e m i l l e r s , w o r k e d u n d e r c o m f o r t a b l e t h e r m a l : i c o n d i t i o n s a l l t h e y e a r r b u n d : . ; \ - V :
-
R e s p i r a t o r y . S y m p t o m s ' a n d V e n t i l a t o r y ' F u n c t i o n • '5 : u.u . , .
. T h e p r e v a l e n c e , o f r e s p i r a t o r y s y m p t o m s ' i r i - m i l l e r s : a n d . b a k e r s i s p r e s e n t e d i n - T a b l e ' 3 . " T h e ' p r e v a l e n c e o f - a l l r e s p i r a t o r y : s y m p - f -t o m s i n t h e w o r k e r s e x p o s e d J t o " f l o u r d u s t w a s c o n s i d e r a b l y h i g h e r t h a n t h a t f o u n d i n o u r . c o n t r o l - g r o u p o f , n o n s m o k e r s o f s i m i l a r a g o d i s t r i b u t i o n s t u d i e d a f e w y e a r s a g o ' - [ 3 5 ] / b u t ;
> ? " • t rs\
Miller:
N = '47
Bakers
N = 37
Table
Mean, d.
in mil'
FVC FEVj PEF Miller
Measured Pre- P .Measured Pre- P Measured Pre- P Bakers -
dieted dieted dieted P
Millers 4276 5072 <0.01 3422 3897 <0.01 510 609 <0.01
N = 80 N = 80 t h e r e '
Bakers -4232 4808 <0.01 3403 ': 3704 <O.OÏ '522 606"" <0 .01 p i r a t . : j £ j ï
N - 130 4232 4808 <0.01
- • „ f o r d
Th- • p r e d i v a l u e ; t o b e . . . (P<0^ . Tfr;=<
n i f i c " g r o u p . r e c o r . v o l u m : s t u d y 1
I n . o n t h me a su : ... m e t e c • r b a k e c b e t w o . v e n t i ' * t h e s e ' 5
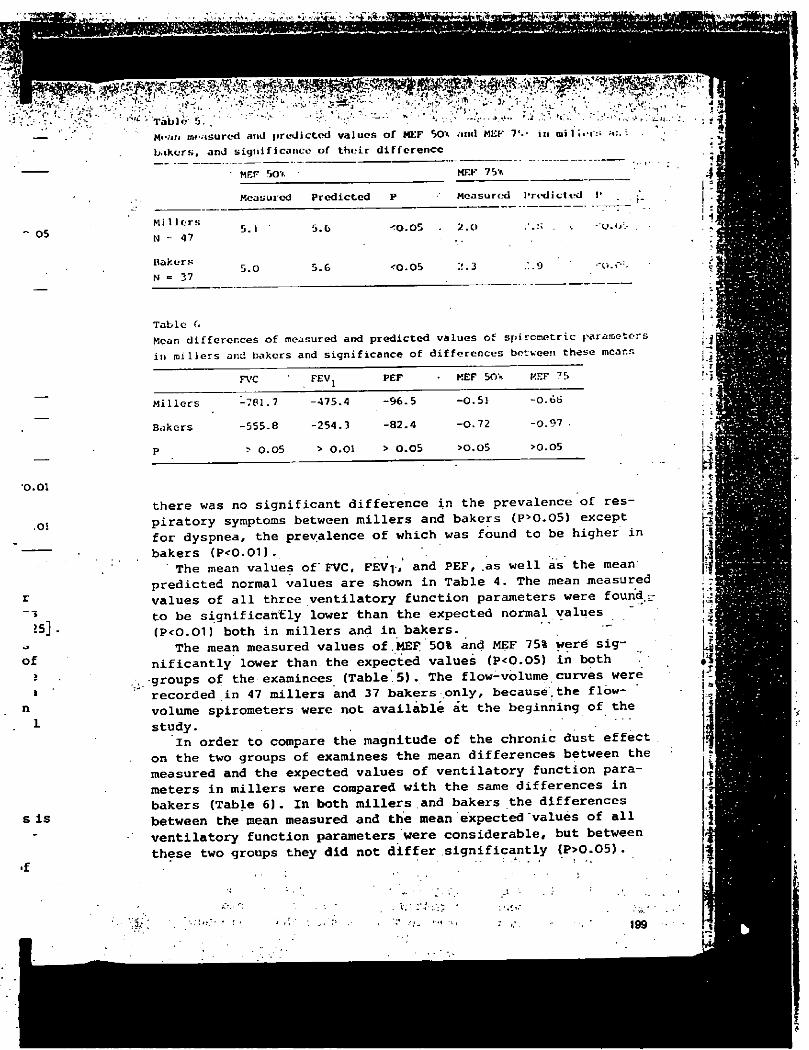
__ M«'.JII ro-'isurod arnJ predicted values of MEF 50* and MEF 7«.- in oiîl'.«i:; \
bakers, and significance of their différence
MEF SO* MF.F 75>.
Measured Predicted P Measured Prodictvd I1
05 Millers
N = 47 5.1 ' 5.G <0.05 . 2.0
Bakers
N = 37 5.0 5.6 <0.05 ?.. 3
. ' . s . \
. 9
• u . < / .
V'.C--
1 : i
1,
0.01
.01
o f
s i s
Table (>
Mean differences of measured and predicted values of spircmetric parameters
in millers and bakers and significance of differences between, these means
FVC FEVj PEF MEF 50\ KEF 75
Millers -781.7 -475.4 -96.5 -0.51 -0.6S
Bakers -555.8 -254.3 -82.4 -0.72 -0.97 .
P > 0.05 > O.Ol > 0.05 >0.05 >0.05
t h e r e w a s n o s i g n i f i c a n t d i f f e r e n c e i n t h e p r e v a l e n c e o f r e s -p i r a t o r y s y m p t o m s b e t w e e n m i l l e r s a n d b a k e r s ( P > 0 - 0 5 ) e x c e p t f o r d y s p n e a , t h e p r e v a l e n c e o f w h i c h w a s f o u n d t o b e h i g h e r i n b a k e r s ( P < 0 . 0 1 ) .
T h e m e a n v a l u e s o f ' FVC, F E V r , ' a n d P E F , . a s w e l l a s t h e m e a n p r e d i c t e d n o r m a l v a l u e s a r e s h o w n i n T a b l e 4 . T h e m e a n m e a s u r e d v a l u e s o f a l l t h r e e v e n t i l a t o r y f u n c t i o n p a r a m e t e r s w e r e f o u n d . -t o b e s i g n i f i c a n t l y l o w e r t h a n t h e e x p e c t e d n o r m a l v a l u e s ( P < O . O D b o t h i n m i l l e r s a n d i n b a k e r s . '
T h e m e a n m e a s u r e d v a l u e s o f . M E F ; 50% a n d MEF 75% w e r e s i g -n i f i c a n t l y l o w e r t h a n - t h e e x p e c t e d v a l u e s ( P < 0 . 0 5 ) i n b o t h
- g r o u p s o f t h e e x a m i n e e s ( T a b l e 5 ) . T h e f l o w - v o l u m e . c u r v e s w e r e r e c o r d e d i n 47 m i l l e r s a n d 3 7 b a k e r s o n l y , b e c a u s e , t h e f l o w -v o l u m e s p i r o m e t e r s w e r e n o t a v a i l a b l e a t t h e b e g i n n i n g o f t h e s t u d y .
I n o r d e r t o c o m p a r e t h e m a g n i t u d e o f t h e c h r o n i c d u s t e f f e c t o n t h e t w o g r o u p s o f e x a m i n e e s t h e m e a n d i f f e r e n c e s b e t w e e n t h e m e a s u r e d a n d t h e e x p e c t e d v a l u e s o f v e n t i l a t o r y f u n c t i o n p a r a -m e t e r s i n m i l l e r s w e r e c o m p a r e d w i t h t h e s a m e d i f f e r e n c e s i n b a k e r s ( T a b l e 6 ) . I n b o t h m i l l e r s a n d b a k e r s t h e d i f f e r e n c e s b e t w e e n t h e m e a n m e a s u r e d a n d t h e m e a n e x p e c t e d " v a l u e s o f a l l v e n t i l a t o r y f u n c t i o n p a r a m e t e r s w e r e c o n s i d e r a b l e , b u t b e t w e e n t h e s e t w o g r o u p s t h e y d i d n o t d i f f e r s i g n i f i c a n t l y < P > 0 . 0 5 ) .
.i
• Ï
: \
ft J ti I 7
i -,
F3
1
> -'j-• • .-*
• M \ , 199
D I S C U S S I O N
• i n a p r e v i o u s - p u b l i c a t i o n , we s h o w e d , t h a t . a l o n g - t e r m e x p o s u r e t o f l o u r p a r t i c l e s i s l i k e l y t o b r i n g a b o u t a h i g h e r p r e v a l e n c e o f r e s p i r a t o r y s y m p t o m s a n d a r e d u c t i o n o f v e n t i l a t o r y l u n g c a -p a c i t y i n b a k e r s [ 3 5 ] . D u r i n g t h a t s t u d y a t t e n t i o n w a s n o t p a i d
. t o a n o t h e r o c c u p a t i o n a l r i s k o f b a k e r s , n a m e l y , t o t h e u n f a v o r -a b l e t h e r m a l c o n d i t i o n s w h i c h m i g h t a l s o c o n t r i b u t e t o t h e i m -p a i r m e n t o f t h e r e s p i r a t o r y s y s t e m . I n t h e p r e s e n t s t u d y , i n o r d e r t o a s s e s s w h e t h e r s o l e e x p o s u r e t o f l o u r p a r t i c l e s c a u s e s i m p a i r m e n t o f t h e r e s p i r a t o r y s y s t e m , w e c o m p a r e d b a k e r s , e x -p o s e d s i m u l t a n e o u s l y t o a i r b o r n e f l o u r p a r t i c l e s a n d u n f a v o r -a b l e t h e r m a l e n v i r o n m e n t a n d m i l l e r s e x p o s e d t o f l o u r p a r t i c l e s o n l y .
E s t i m a t i n g t h e t h e r m a l e n v i r o n m e n t o f m i l l e r s a n d b a k e r s , s i g n i f i c a n t d i f f e r e n c e s w e r e f o u n d i n t h e i r h e a t l o a d ( T a b l e 2 ) . T h e b a k e r s w e r e e x p o s e d t o m u c h h i g h e r t h e r m a l e x p o s u r e t h a n t h e m i l l e r s w h o s e t h e r m a l e n v i r o n m e n t w a s f o u n d t o b e p l e a s a n t b o t h i n t h e c o o l a n d w a r m s e a s o n o f t h e y e a r . M i l l e r s a n d b a k e r s w i t h a n - a p p r o x i m a t e l y e q u a l . l e v e l o f d u s t e x p o s u r e w e r e c h o s e n f o r t h e s t u d y i n o r d e r t o c o m p a r e t w o p o p u l a t i o n s a m p l e s e x -p o s e d t o p r a c t i c a l l y e q u a l a i r b o r n e d u s t c o n c e n t r a t i o n s b u t d i f -f e r i n g i n t h e i r t h e r m a l b u r d e n . O n l y . n o n s m o k e r s w e r e c h o s e n i n o r d e r . t o e l i m i n a t e s m o k i n g , a f a c t o r w h i c h u n d o u b t e d l y c o n t r i b -u t e s t o t h e d e v e l o p m e n t o f c h r o n i c r e s p i r a t o r y s y m p t o m s . T h e a n a l y s i s o f c h r o n i c n o n s p e c i f i c r e s p i r a t o r y s y m p t o m s h a s s h o w n t h a t t h e p r e v a l e n c e o f c h r o n i c b r o n c h i t i s , d y s p n e a , w h e e z i n g , n a s a l c a t a r r h , a n d b r o n c h i a l a s t h m a w a s s i g n i f i c a n t l y h i g h e r i n b o t h m i l l e r s a n d b a k e r s a s c o m p a r e d w i t h t h e c o n t r o l g r o u p , b u t t h a t t h e r e w a s n o s i g n i f i c a n t d i f f e r e n c e b e t w e e n b a k e r s a n d m i l -l e r s , e x c e p t f o r d y s p n e a w h i c h w a s f o u n d t o b e s i g n i f i c a n t l y h i g h e r i n b a k e r s ( T a b l e 3 ) . T h e a n a l y s i s o f v e n t i l a t o r y f u n c t i o n h a s s h o w n " t h a t t h e m e a s u r e d v a l u e s o f a l l v e n t i l a t o r y c a p a c i t y p a r a m e t e r s o f b o t h m i l l e r s a n d b a k e r s w e r e l o w e r t h a n t h e e x -p e c t e d n o r m a l v a l u e s c a l c u l a t e d o n t h e b a s i s o f t h e i r h e i g h t a n d a g e ( T a b l e s 4 a n d 5 ) .
I n o r d e r t o a n s w e r t h e m a i n q u e s t i o n w h e t h e r t h e e x p o s u r e t o a i r b o r n e f l o u r p a r t i c l e s , w i t h o u t s i m u l t a n e o u s h e a t l o a d , • c a u s e s c h a n g e s i n p u l m o n a r y v e n t i l a t i o n , t h e e f f c c t s f o u n d i n m i l l e r s a n d b a k e r s . w e r e c o m p a r e d . A s t h e h e i g h t a n d a g e d i s t r i -b u t i o n s o f m i l l e r s a n d b a k e r s w e r e n o t i d e n t i c a l , i t w a s c o n -s i d e r e d u n j u s t i f i a b l e t o c o m p a r e d i r e c t l y t h e m e a s u r e d v a l u e s o f v e n t i l a t o r y c a p a c i t y i n t h e t w o g r o u p s . T h e e x p e c t e d n o r m a l v a l u e s o f a l l t h e v e n t i l a t o r y f u n c t i o n p a r a m e t e r s w e r e c a l c u -l a t e d f o r e a c h e x a m i n e e , a s w e l l a s t h e d i f f e r e n c e b e t w e e n t h e e x p e c t e d a n d t h e m e a s u r e d v a l u e s . T h e m e a n s o f t h o s e d i f f e r -e n c e s w e r e c a l c u l a t e d s e p a r a t e l y f o r b a k e r s a n d m i l l e r s a n d t h e d i f f e r e n c e o f t h e s e m e a n s w a s t e s t e d b y t h e t - t e s t f o r u n p a i r e d v a r i a b l e s . T h e r e s u l t s p r e s e n t e d i n T a b l e 6 s h o w t h a t t h e r e w a s
no diffe f
t h e ' d u s t ^
measured-
thermal-',
feet .of
T o o u * c o m p a r i n a u t h o r s I t i s mo a
t h e h i g h * t h a n i n t h a n 77% s e r v i c e -a g e o f '4 y e a r s . A m i l l e r s .. l o w e r v a a b l y h i g o n h e i g h
O u r r t h e d e v e a r e d u c t u l t a n e o u
REFERENC
1. Baagoi 2. Bedfoj
Counc.
3. Beldii resul'
• 4. Berit: : i
flour--J
(197® j 5. Berit. > .
in th'i
oed. ji
6. Cas tbi . •>
Acta J '
7. CECA:
( 1967 8. Cenoc*
forna
9. Chcrn using
io. Co Irne; f lucn
of 32
't*
; u r o a l c n c c
c a -p a i d
L c a V O r -
o i m -n u s e s
e x -• r -c l e s
e 2 ) .
a s a n t î k e r s s e n
d i f -i n
. . ^ r i b -r h e
own
9» r.or i n
b u t m i l -
- x y m e t i o n
i t y x -
j h t a n d
e ad, a i n ,
t r i -n -
L u e s mal u -
î t h e
t h e p a i r e d
w a s
-a t h e - d u s t e f f e c t s o n a n y . o f t h e v v e n t i l a t o r y . c a p a c i t y p a r a m e t e r s m e a s u r e d . The-, s i m u l t a n e o u s e x p o s u r e . o f b a k e r s t o u n f a v o r a b l e t h e r m a l e n v i r o n m e n t d i d . n o t c o n t r i b u t e ' s i g n i f i c a n t l y t o t h e e f -f e c t o f f l o u r d u s t e x p o s u r e , o n t h e r e s p i r a t o r y s y s t e m .
T o o u r k n o w l e d g e , o n l y o n e p a p e r h a s b e e n , p u b l i s h e d s o f a r . , c o m p a r i n g s p i r o m e t r i c f i n d i n g s i n b a k e r s a n d m i l l e r s [^26^ . T h e a u t h o r s h a v e f o u n d g r e a t e r r e d u c t i o n s o f FEV-j a n d . FVC i n b a k e r y . I t i s m o s t l i k e l y t h a t t h e i r f i n d i n g s a r e t o b e a t t r i b u t e d t o t h e h i g h e r a g e a n d a m u c h l o n g e r l e n g t h o f s e r v i c e i n t h e b a k e r s t h a n i n t h e m i l l e r s e x a m i n e d . Among t h e i r b a k e r s t h e r e w e r e m o r e t h a n 77% a b o v e t h e a g e o f 4 0 a n d m o r e t h a n 71% w i t h a l e n g t h o f s e r v i c e o f o v e r 2 0 y e a r s , c o m p a r e d w i t h 44% o f m i l l e r s a b o v e t h e a g e o f 4 0 a n d o n l y 1 9 . 4 % w i t h t h e l e n g t h o f s e r v i c e o f o v e r 2 0 y e a r s . A s t h e y w e r e c o m p a r i n g t h e m e a n s o f FEV-j a n d FVC b e t w e e n m i l l e r s a n d b a k e r s , w i t h o u t a d j u s t m e n t f o r a g e a n d h e i g h t , t h e l o w e r v a l u e s i n t h e b a k e r s w e r e m o s t l i k e l y d u e t o a c o n s i d e r -a b l y h i g h e r a g e a n d l e n g t h o f s e r v i c e ( t h e y d i d n o t g i v e d a t a o n h e i g h t d i s t r i b u t i o n ) .
O u r r e s u l t s - s u g g e s t t h a t e x p o s u r e t o f l o u r d u s t m a y c a u s e t h e d e v e l o p m e n t o f n o n s p e c i f i c c h r o n i c r e s p i r a t o r y d i s e a s e a n d a r e d u c t i o n o f v e n t i l a t o r y l u n g c a p a c i t y i r r e s p e c t i v e o f s i m -u l t a n e o u s h e a t l o a d .
REFERENCES
1.
2.
3 .
4.
5.
6.
7 .
8.
9 .
10.
Baagoe, K.H.: Mehlidiosynkrasie. Klin.Wschr. U 792 (1933)
Bedford, T.: Environmental warmth and its measurement. Medical Research
Council War Memo, No.17. London:' HMSO 1946
Belding, H.S., Hatch, T.F.: Index for evaluating heat stress ir. terms of
resulting physiological strains. Heat.Pip.Air Condit. 27, 129 (J95S)
.Beritic, D., Valic, F.: On the relationship between hypersensitivity to
flour and chronic bronchitis in bakers [in Croatian^. Lij.vjes. 93^ 991
(1971). , .;-
Beritic, &., Valic, F., Zagar, Z.s Role of bacterial and fungal flora .
in the development of chronic bronchitis in bakers [in.Croatian:. A c t a ,
med.jugosl. 26, 19 (1972) <
Castberg, T., Sorensen, C.M.: Allergic examinations of bakers and millers.
Acta Allerg. U 283 (1948)
CECA: Tables de références pour les examines spirographiques, Luxembourg
(1967)
Cenacchi, G.C., Rosa, L., Bergami, G.: Indagine sulle allergopathie dei
fornai. Folia med. 42, 345 (1959) t
Cherniack, R., Raber, M.B.: Normal standards for ventilatory function
using an automated wedge spirometer. Amer.Rev.resp.Dis. 106, 35 (1972)
Colmes, A . , Guild, T.B., Rackemann, P . M . : •Studies in sensitization; in-
fluence of occupation on sensitization in man as determined in study
of 32 bakers. J.Allergy 6, 358 (1935).
i l
j f i < \V
: l r
H I i t I 'T I rS I rtfj
"I
?l I ' I 1 i i-à| i-i i m **! N.»»f
, v r„y J '«. 201
7£ï
i .......
-v.
-ii
V
,r. ..
•a-.v-,
\ ;
r s c v
e i"
^ 75
D . , Ljaljevic, M . Popovifc, D., Spuzic, I.:
les boulangers et les meuniers. Acta m e d .
J-'jugosi. 13/;;294 (1959) ' ' V-
12. Diedrich, W., Lubbers, P.: Das Mehlasthroa als Berufskrankheit. Z.Ar-
b'eitsmed. Arbèitsschutz 5, 189 (1955)
13. Dishoek, V., Roux, D.J.: Sensitization to flour and respiratory ill-
nesses among flour workers. J.Hyg.(Lond.) 34, 674 (1934)
14. Epstein, U.: Cited in: P. Bonevie, Occupational allergy. Leiden: Sten-
fert 1958
15. Gadborg, S.: Allergy to flour. Doctoral Thesis, Copenhagen (1956).
Cited in: P. Bonnevie, Occupational allergy. Leiden: Stenfert 1958
16. Granati, A . , Capone, C.: Studio sulle condizioni ambientali e sulla
patologia professionale nei laboratori artigani de11a fabbricazione
del pane.'Folia roed. 42, 948 (1959)
17. Health factors involved-in working under conditions of heat stress.
Techn.Rep.Ser., No.412. Geneva: W.H.O. 1969
18. Hertig, B.A.: Thermal standards and measurement techniques. In: The
industrial .environment evaluation and control, p-413. Washington
N.I.O.S.H. 1973
19. Herxheimer, H.: Die Entwicklung von Mehlempfindlichkeit der Haut bei
Bâckerlehrlingen und BSckern. Klin.Wschr. ^ 5 , 481 (1967)
20. Hlavacek, II.A.E. : Allergic symptoms on thc sruccus membrane of the res-
piratory tract of bakers and millers. Acta oto-laryng.(Stockh.) 26,
• 358 (1938)
21. Klùnker, W.: Zur Frage der Aetiologie und Pathogenese des sogenannten
ï C- Bâcker- und Mûllerasthmas. Schweiz.med.Wschr: 8 7 , 714 (1957) . v'
22. Linko, E.: Allergic rhinitis and bronchial asthma in bakers. Ann.Med.
intern.Fenn. 34, 98 (1947)
23. Maver, H.,' Boras, E.: A contribution to the knowledge of energy expen-
ditures in bakers Q.n Croatian^ - Proceedings of the Fourth Congress on
Preventive Medicine, Sarajevo, Yugoslavia (1961)
.24. Medical Research Council Committee on the Aetiology of Chronic Bron-•
chitis: Definition and classification of chronic bronchitis for clini-
\?"cal and epidemiological purposes. Lancet II' 196S,"775 _ **'
25. National Institute of Occupational Safety and Health: Criteria for'a
recommended standard. Occupational exposure to hot environment. HSM -
1.972 - 10269, Cincinnati (1972)
2G. Odavic, M. , Cvotanov, VI. : Incidence of'the allergic manifestations and
phenomena of pulmonary spastic syndrome in the workers exposed to flour
and floury dust. Allergie u . Asthma ^5» 364 (1969)
27. Postallozzi, C., Schnyder, U.W.: Zur Frage'der Bâckerrhinitis und des
Bâckerasthmas. Schweiz.med.Wschr. 496 (1955) '
28. Peters, J.M., Mead, J . , Van Ganse, W.F.: A simple flow-volume dcvice
for measuring ventilatory function in the field. Amor.Rev.resp.Dis. 9 9 ,
617 (19691
2'J. Ramn/.zini, H. : I.e malattie dei lavoratori (de morbis art if i cum diatriba)
•. Torino: Minerva medica 1933
3oi R/imsey,' J . D . : À heat stress standard - How do we face up to it? Prc-
s»«nt<xJ_.to American Society of Safety Engineers Professional Development
' Conf'Toncr-, Pittsburgh, PA. (lrJ74)
w m m ,
-, 31 '. Regreji
' Airaecjf' • • » •• 32 Salêni.^l
" » . ' • '"l-t J
33. Spuzi<}; !
- Nikol: vj •
Petro' ... . r
34. Spuzii'_j j
ratio] ,
niers
35. Valifc. ,. ->-
Lij.v; ,
36. Valifc
terisi
(1972:
37. Vallei
forna^
38. Wrigh-
Med.
39. Vagloi
ing a
Received J, :
•
.V-rM'.
i n . r- 'I -*'.' ' ''.
•I I
m m : r?
W m J
Ar- tor Allergie. Glcichzeitig oinig« GesichtspunkLc uhcr g e w i s s o pi(tv/.i-
piell bcdeutungsvollo Allergieproblcme. Acta rood.scand. Sf ; f>OI>. i|'M!-j ;
33. Spuzifc, B., Bojanic, B . , M i l i j i c , B. , Perisic, S.,-l.jaljevit,
Nikolifc, V.: Allergy in workers employed in steam b a k e r y ' i s i K iiYT'" st-.cn- Potrovac na Mlavi £in Serbian]. Zavod zdrav.zast.SKS 1 / 2 1 (19v3)".
34. Spuzifc, V., Bojanifc, M., S p u z i c , I.V.: La rolo d e la farine dans l'appa-
rations des manifestations allergiques chez les b o u l a n g e r s et les xcu-
3 niers en Yougoslavie. Acta allerg.(Kbh.) Q , 69 (1960)
35. v a l i c , F., Beritic, D. : Chronic bronchitis in bakers [in CroaciarJ .
Lij.vjos. 93, 739 (1971)
30. V a l i c , F., Tudic, C., Beritic, D., G j u r i s , v.: Pharmacodynamic charac-
teristics if flour particles £in Croatian]. Acta m e d . j u g o s l . 2ô, 29
(1972)
3 7- V a l l e r a n i , G., Bonino, R . : Rilievi sulle allergopathie respiratorie nei
fornai. Minerva roed. ^ 4 , 3069 (1963)
38. W r i g h t , B.M.: A size-selecting sampler for a i r b o r n e d u s t . Brit.J.industr.
L M e d . 2 1 , 284 (1954)
—39. Y a g l o u , G.P., Minard, D.: Control of heat casualties at military train-
2S- ing centres. Arch.Industr.Hlth 16, 3o2 (1957)
ten Received December 18, 1975 / Accepted February 13, 1976
In-on
I - ' %
a • .. - -
• ' ". V'V'., • 5 and " " D u r
i c 5
ii,
Lba).
j^nt
203 •
irffli iliinmiiânttr fflmkMbéiiMB
-, ••• • . • - - - - v V •• y . WW*-rM-^feS'
x/ 01
a )
0 1
<f
! Immunoglobulin E-specific to wheat and rye flour proteins ^ -
! I n ' ;
I - . I I J O K K . S T f ' I N . A . I I A C K M A N . K . A . J. J A K V I N I - N . H . I . M I T I . I : . S A V I I . A I I T I . I ' . S Y V A N T - N ami T . K Â K K K Â I N I - N Hospital for Allergic Diseases urn! {'hik/ren's Hospital.
Helsinki University Central Hospital. Helsinki, iinlaml
Summary VVc have used (lie radioallcrgosorhenl test ( KASÏ ) to determine Igli.-antihodics specific to wheal Hour proteins in the sent of seven groups of patients. In some cases rye-specific IgF. was also determined. .Wheal and rye RAST scores showed a good cor-relation. presumably due to cross-reactions. Among bakers with asthma, positive scores. 0-5 3, occurred with a prevalence of 43*V.« *md anion'}* children with cc/ema. scores in the range 0-5-4 were found with a prevalence of54"„. A score of 0*5 was a marginal value which was also occasionally encountered with sera from patient groups with no history of immediate hypersensitivity to wheat or rye. These groups included adults and children with allergic rhinitis and asthma, children from the general population and children with online disease. The RAST appeared useful in the diagnosis of allergy to inhaled Hour dust among bakers. Among children with -cc/ema, positive wheat and rye RAST results were a common finding, which only occasionally could he linked to .strung and unequivocal reactions to the foods in question. Both in bakers and.children with cczcriïâ. wheal and rye RAST results showed good agreement with intracutaneous skin test results. . w , .
Introduction ' " ' Wheal and rye Hour dusts cause asthma ami iliinitisin hakcrs (llcndrick. Da vies & -Pepys, 1976; Naka/itwa <7 a!.% 1976; Wilbur A .Ward. 1976). and immunoglobulin Ii (lgl:.) specific to (lour proteins can frequently he found in the.sera of those affected (IJIands et r/A, 1976). In several studies manifestations of immediate hypersensitivity have been found in some" 20% of the workers exposed (l.inko. 1947; BorcherU'1972; llcrxhcimcr, 1973).
Overt allergy to cereal grains ingested as foods occurs in children and young adults (Hcincr, Goldstein & Rose. 1970: Hoffman & lladdad. 1974; Hoffman. 1975). Also 4hcsc pallie ills usually have circulai int? ly? I- specific to cereal onitfl pn*li*fn< l n «'MiUrm . with ec/.cma, ce real-specific Igl: can frequently he found even in the absence of overt symptoms to the cereals in question (Itollman." 1975; Hoffman et «#/.. 1975).
To obtain further informal ion on the occurrence of wheal- and rye-specific lgl:.,.
Correspondence: l)r l?. tljorkslcn. ItcKpiiat for A11er pic Disses. S1-00250 Helsinki 25. Iinlaml.
473
> ?
I. > .«is
! " t . '-i INi' mê?: "ri- ïù.t
and several hcr prm.,* <.f allergic and Ilor i ,.ionï nï réloV«t i S ^ l h c ^ ' S ? - ^ results have been compared «ith ski,, ind challcn^cM :.nd ttllh da.:, fnYm^ pM.er.ls lnslor.es. I,. particular. «e have tried l.rlU,.,l>"e ,blisl,-||.e ero.ips iii Which ccrc!il-spccil;c lPl- is to he fiwrnl. ami Ihe clinical significance of this liudiiu. ^ «
•• ; • • . t . * . • • . . yuC, .s..'. .
rutiviUs :util nicflioils
hnicntx
W c slmlial seven L'itiups ol'patients. • ^ ,
( iroup (a) included .«ciMy-onc lake* «ill. ..Ml,,,,:,. i«cKc «omen and „i„0 men •
" : ,fC J V 2 < " . MOM palicnls had also rl.i..i.is and .«o had • ' cç/cnia. I hey had »o,Ud i„ k,U-rics for 0 5 l-l years. mean A-7 vears. Sixteen l.ad a 1-story Mippcshnp allerex ... «heat or r>e flour dust. These alleges could ,„., he distinguished by history. Only patients l'.l>. and R.U. had asthma hclore entériné the iniilc.
Group (b) included thirty-nine adults. twenty-live women and fourteen men ' w,l i;Mue;lnn,cnr.m Xye;,rs.n,nKcl5 OS years. Most patients had asthma. and manv - -siillcrctl from „„„ied,;Mc hypersensitivity as ,uggested by history/serum total l B r . levels, blood eosinophil counts and sccrctory eosinophils. In a few cases thc asilimi : could he classilicd as intrinsic. No patient had a history of allergy to wheat or rvc and no-onc was a baker. • - V * *
" Group (c) included forty-onc children, tw^niy j irls ami Vwcntv-onc hovs with ' :i mean age of 31 years (Table 31. All had ce/ema presumably related to immediate hypcrscnsiimty. In addition, eleven bad asthma, three rhinitis and one spastic bron- ' chilis. Seven patients had a history s u i t i n g sensitivity to foods contamine wheat or " i. rye. . •• - V- /•- * t ;
:Group (,|, included H.ïriV-Ù.wr childreiû ei^iteen jiirls and>tticen l^-s, UÏM'I a ^ mean age n| 3-3 yc?rs. Ihe age distribution of the' ^roup was niaielied to thai of ' group |c|. I he patients «c.c being healed lor xarious Mimical. urolo,*-:.! and neuro-logicalconditions. I he group «as assumed to represent the general population as far as immediate hypersensitivity was concerned. "" ' " " ; '
Group (e) included twenty-lour children. Viine ^iK':Vm|;liriecn' lîovx" wi'ih a men ' ' age ol X\S years, range U I I yeais. M<>st-chtjdrcn liadtrhinitisand some asthma No- -one had present serious cc/cma, In all patients symptoms were due lo inimediafe k J hypersensitivity s sug^teil by histijVy. scrum total lçl.;/blood eosinophil counts atul&^ .secretory eosinophils: No patientlutd a history of allergy to'uhrat or"r>-c..";>^- "
Group <f) included ten. children: scvcVpirls nmrihrcc'lHiys. with â mean" a ce of ' 71) years, range 0 5 l(y5 years. All lûd ^psyÂerilîSlTeliae disease. Scrum samplcs^ 1 were taken prior to1'withdrawal of glutenTrom thé diet. ' " - - 7
(îr«»up (g) included I3f. patients, all of uliom had wheat- or rve-specilic I g l i ; ' <»r both, in their serum. I lie group was stmlied to cliicidatc thc correlation b e t -ween wheat- and rye-specilic Igl-: couechtralitms. Some of llie palicnls were also' * include! in gr<»iip (a) or iiM. - ^ -
; ^ ' . ;;
w '
J
Alli*rf*y irsts ; • » * ' ' • 5 '
l-or intracutaneous skin tests I : KHI ulieàt jloi.r and ne Hour cxtn^s in C oca's solution were used. A skin reaction was regarded as positive uhcnlhc area "of"'llie"
«RI
m
n p
v,-». •
A
yn r • r' V-. YC;-
* Il iftcyjr m/ rjrr syir M-'
. v i
iv'a'4; f;
weal c a u s a l by (he allergen was larger than that causa l hy Coca ' s solution a lone! ànd at least half a s large as that c a u s a l by 1(H) m g l histamine d ihydrochlor idcin Coca ' s so lu t ion .
In nasal challenge tests hakcrs sniflcd wheat o r rye flour. I fnasa l . eye or bronchial s y m p t o m s developed within 15 min. the test result was regarded as positive. Test condi t ions were not ideal, since the bakers cont inued working and many had symptoms at the start of the test.
In p repara t ion for an oral challenge, chi ldten were kept on a wheat- or rye-free diet fo r 3 days. They were then given It) g wheat or rye flour, respectively, in the fo rm of a boiled cereal. The test result was considered positive if skin, respiratory, gastr ic or generalized symptoms developed within 24 hr. The test was not repeated.
Serum total Igl: was determined using the Phadcbas Igl; lest kit (Pharmacia Diagnostics) . Results arc given in u/ml (Rowc. G r a b £ Anderson. 1973).
I t
I
I
Determination of wheat- and rye-.yeei/ie /e/;
Specific Igli was determined using the radioallcrgosorbciii test (RAST) (Johansson, lïennich & lïcrg. 1971).
To obtain antigens. Hours were extracted with an acid solvent (to dissolve glindiiis) and with a neutral solvent (to dissolve albumins and globulins). Wheat flour was suspended in the ratio of I g per 3 ml and r\c flour in the ratio of I c per 4 ml of mmol/l sodium acetate buffer, pll 3-8. The suspensions were mixed for 45 min at room temperature, centrifugal, and separated into supernatant and precipitate, which were both saved. The precipitates were homogenized and resuspended using the original volume of I0mniol/l sodium phosphate huflcr. pll 7-0. containing 430 mmol/l sodium chloride. Suspensions were again mixed, centrifuged and separated, and the supernatant was saved. Uoth extraction solvents containal 4 g/l phenol as preservative. All extracts were concentrated ten-fold using ultrafiltration through a Diaflo'UMO membrane (Amîcon Corp.).' ' V- ~- . ' - ' -s
The proteins from fresh flour extracts were coiipled to cyanogen bromide-activated paper discs (Ccska & l.undkvist. 1972). To prepare-wheat flour discs, both acid and. neutral wheat extracts were added in equal volume to the same coupling solution. The volumes 7-5, 25 and 75/d of each extract per disc were trial in experimental runs, and the volume giving the highest count rate in a subsequent determination of specific IgF., in a suitable test serum, was chosen for the preparation of routine assay discs. Volumes chosen varied from lot to lot. Rve flour discs were prepared similarly. Reagents other than discs nealal for the specific Igl: determination were obtained from Phadcbas RAST kits (Pharmacia Diagnostics);
Assay, calibration and result reporting procedures were mainly as described by the manufacturer Tor Phadcbas RAST kits. This includes the use ôf a semi-quantitative, 0-4 RAST score based on the use of a reference serum dilution series and rcfcreiicc allergen discs. Wc modified the system to include the score 0*5, with which we describe the specific IgE concentration in a sample giving a count rate at least twice the back-ground, but less than that required for RAST score I (approximately thrice the background). Our 'background* is the lowest count rate given by a patient sample in a RAST series of at least fifty assays, For the present we will consider a RÂST score of 0-5 or higher as positive. i.c. as an indication of the presence of specific IgF..
*
i'l
Î
t "
i t
' '. *. ; • ' . . .
• - J v
i; V"-.-.,"- V • •
" *•• -J • ,'• •. » '
.V^V.vv-. V '
. - - (• V
«v -
A:-
•, ' • s Table I. Patient *\vup (a); iwemy-one bakers with asthma
\<
ï • Acc
ii ^ V . - A. !•:. It
i -i H v .'il." -A. K ' . -if?
.; - * •:•! -VK- i . - ' H i - " " ' a . I:-. K . ••• .i;D• y,
« ,. S O.S. ;A.:R.:t " ;
,.Serum lilOOil 101.11
.eosinophilic igE t :< 10" 1) iu ml)
-
150 v-'O t* \ TO
; I.MV ? ;vo - :5o 1400
150'' •r .'NO • 440;-: T-.l/O'
'0 IMJ .: : « ) '
440^ r ; •• JO .
-If." : : m • —: ou. -J.-00
150 V >0 • ; -
• • . . . io
History. -Skin test
. Srcc'nk
w I RAST
Rye tlpur^V:^ '•iy
Spcciilc -IsE -
N:,S;|1 • IRAST Na<al
>corci .-hallcntfc Ski::'lose score) hallen e—
; r.. ^ !:.! I.r o U.I
£ T .T . . : 15»!; ^ .10 II» -|V0
'-i ' - Logarithmic m c W • t . ' ;
U < 0 < 0-5 0 II \
- I I) (I 0 I) I) *
II ^
0 () I)
u-5 ' 0
o >
I) f.
'"TT. ' . ,
> 0
'f! T:
. a ' - . r l
3, -
i- \v r •
i/ . J A:
d s ; ri1. - • , tv-P' V
T"! r-• » s
• •< - h-
* V'-1 ' . V r
Results
$
Àihilts '".V '
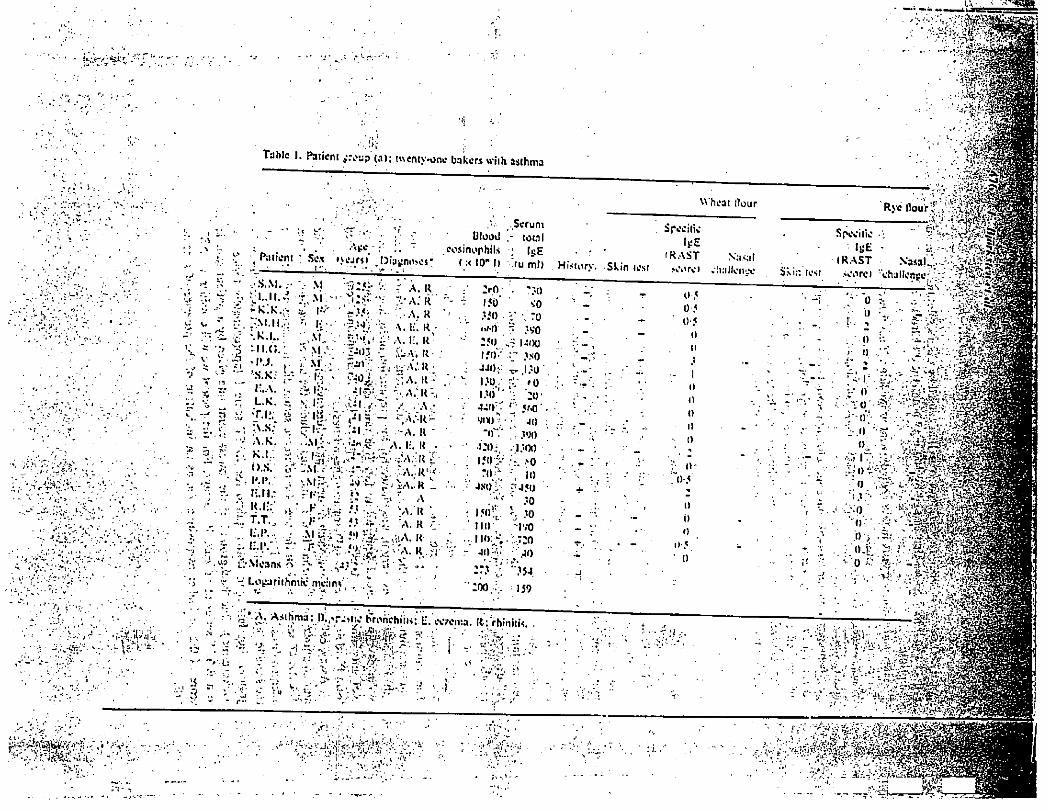
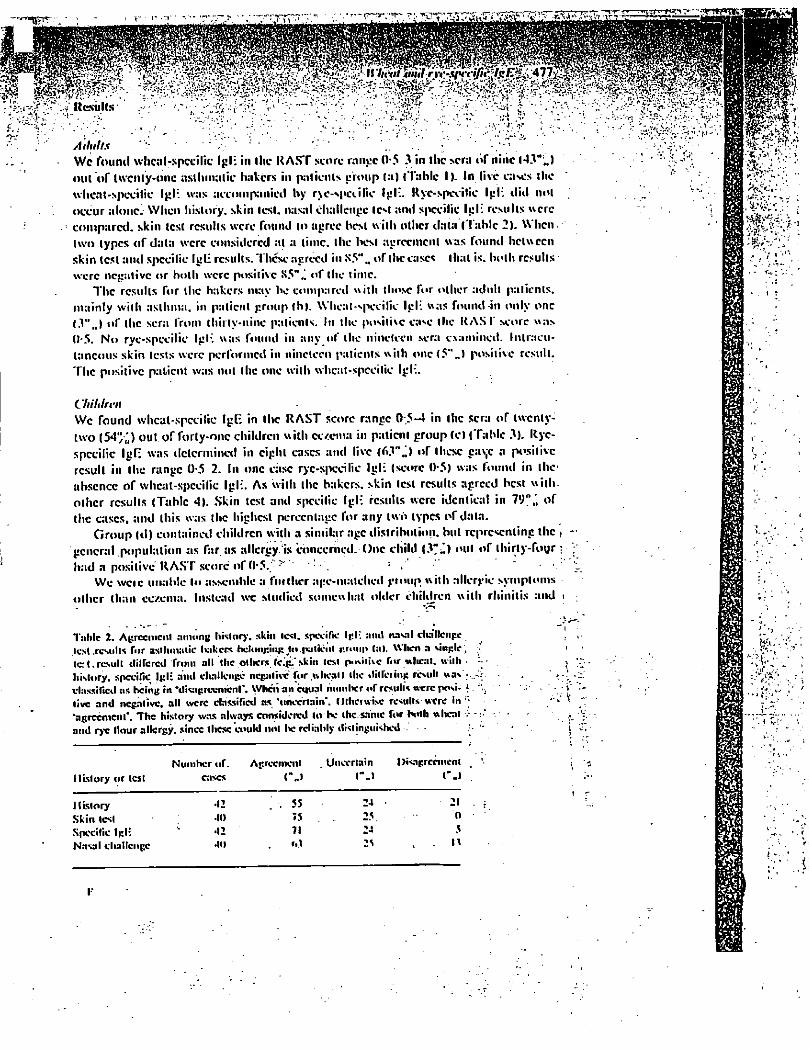
Wc fourni whcal-spccilic Igl: in thc HAST score range 0-5 3 in the sera ôf nine <43"..) out of twenty-one aslhmatic bakers in patients group (a) (Table 1). In live eases the wheat-specific Igl: was accompanied by r\e-specilîc Igl:. Rye-specific lei: did not occur alone! When history, skin test, nasal challenge tcM ami specific Igl: results were compared, skin lest results were found to agree best with other data ( Table 2). When two types of data were considered at a time, the best agreement was found between skin test and specific Igl: results. These agreed in S5"M of the ease* that is. both results were negative or both were positive of the time.
Thc results for the hakcrs may be compared with those for other adult patients, mainly with asthma, in patient group (b). Wheal-vpecilic Igli was found-in only one l.l«J of the sera from thiily-ninc patients. In the positive case the NASI' score was (1-5. No rye-specilic Igl: was found in any of the nineteen .sera examined. Intracu-taneous skin tests were performed in nineteen patients with one (5"J positive result. Thc positive patient was not thc one with wheat-spccilic Igl:.
Children
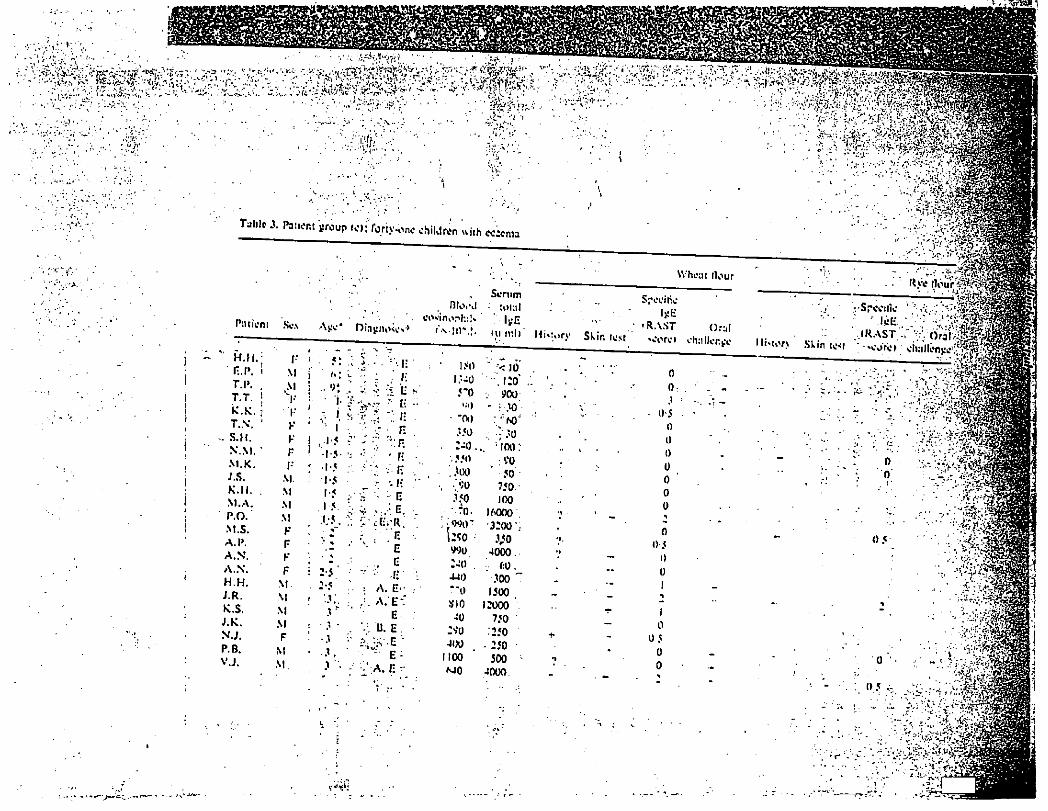
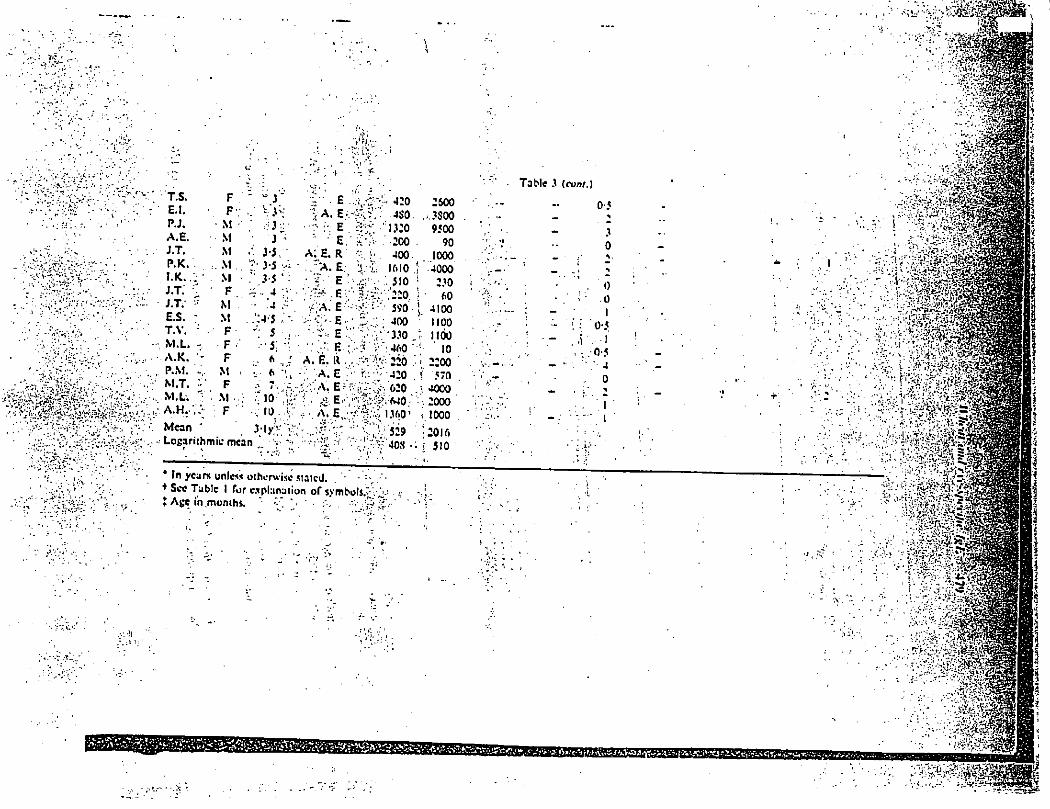
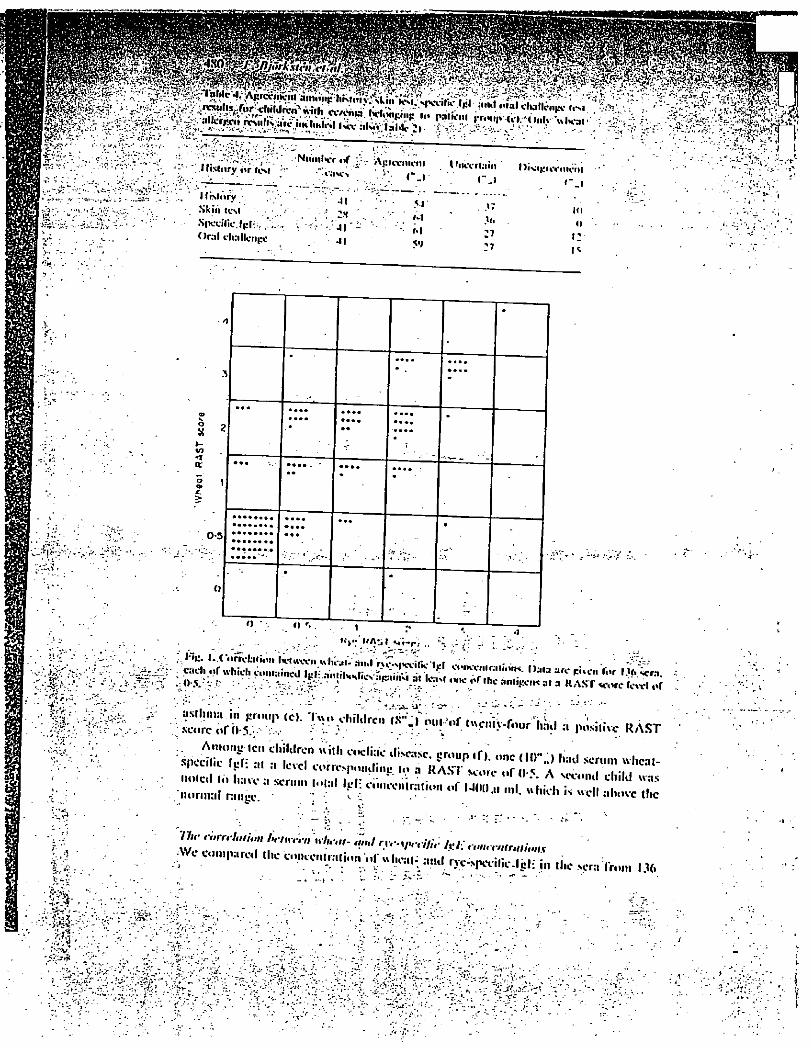
We found whcal-spccilic Igl; in thc RAST score ranee 0.5-4 in thc sera of twenty-two (54";) out of forty-one children with cc/ema in patient group Ccl (Table 3). Rye-specilic IgF. was determined in eight cases and live (f>3"j of these ca\c a positive result in the range 0-5 2. In one case rye-specilic Igl: (score 0-5) was found in the-absence of whcal-spccilic Igl:. As with the hakcrs. skin test results agreed best with other results (Table 4). Skin test and spccilic Igl: results were identical in V)",\ of thc cases, and this was thc highest percentage for any two types of data.
Group (d) contained children with a similar age distribution, hut representing thc , general population as far as allergy, is concerned.One child (J"*) out of tliirty-foyr : had a positive RAST score of 0-5. ^ /
We weie unable to assemble a fut liter age-matched gtoup with allergic symptoms other than eczema. Instead wc studied somewhat older children with rhinitis and i
. ' • V • • * Ï.&
Table 2. Agreement among history, skin lesi. specific Igl- «ml natal clia'Hciige .lest results for asthmatic hakens hehniginj: jto.paticiii r.r«»up Cal. Wltcn a single , let. result diltcred from all the others Ici'.skin test posime for * heat, with . history, spccilic Igl; ami duillenge negative for wheat) the «lillciing resulr was vhssificd as being in 'disagreement*. When an equal mini IK r of result* were posi. { live and negative. all were classified a* ' uncertain*. Otherwise refill* were in 'agreement*. Thc history was always considered to he thesnnte for KM h wheal > and rye Hour allergy, since these could not l»e reliably distinguished - ' [•
Number of. Agreement Uncertain \ )i<agreei»ent History or test cases ("„» r j r.i
History .12 . 55 24 21 Skin lest •to 75 25. 0 Specific Igl: •12 71 24 5 Nasal challenge •til M M
? .v
I-
^ T f c U .
m m
"T. . ' . ' • ' - - " " / '
V J. l ."
•i
Tahle X Pa:icnt group fci: loriy-ono children with cc:cma
Patient Sc.s Diagnose*4
nuvj Scrum total :
History Skin test
rSpecjiic ',\v; ' Mj:E:
0f> tc<t ; .corc) challenge:;
- • n ' , • '.V
y.. G •.
- v o ^
0 5
0
0 5
-
• 'tS-r.y, • -
: v. v - %
•r-T.'.-
i t .
, - . s - ' - . • -
• \ O. ' ( V
T.S. F E.I. F P.J. M A.E. M J.T. M P.K. . M I . K . M J.T. F J.T. ? M E.S. - M T.V. ; F , M.L. - F A.K. ~ F
, P.M. -, M . - M.T. V F . M.L. : M ..;• !.'. A. H.-, ; F Mean
;
- Logarithmic mean
"J - V
3-5, ^
~.. 4 ' . 4 ~
5 •• • 5;
7
. 7. •10 - , 10- î. : V
My 'î';'-
I I ~ ' -1 • •*/ W
V *
.1» i
• a\ -> -, A «
' -r:
V • E. •> A. E
• - R - E E
A; E. R . "A. E
E ..V
E -
E E.;':
A. É. K , . ;; A . E. '.'À. E? K
Table 3
• 4 2 0 2600
•4S0 . , . 3$00
1 3 : 0 9500
A, E •.tr.
200
400 1610 510
;'220
590
400
? V ; 4 6 0 0
rv-'^-AlO
"' '620 MO ' 1360' 529
! V 408 •
90 1000 4000
230 60
4100
iioo ; 1100 : "io 2200
i 570 V 4000
2000
i.!000 |20K> i 510
• <•
0-5
y
0
0 0 I
0-5 , I 0-5
4
0 ^
. I 1
- i;-
• ïn year* unlc« otherwise stated. + See Tabic I fur explanation of symbols. . , t Age in months. • .wS" '
• A-/; . '
; ;
'Il
»•" -T
• •• • ' . ' •: ' • • . . . * s
, ? ; , .
, 1 .
ïiv.
..-^••rtvv ; IliNl.iryor iisi - . ' . I'nccrlain |>i«,.UVl
rO .• . . ' "> ' t -f. "r , a -..'. v-| i.Ti1. ^ --•-•'.oLj'/.v
History • Skin test •SpLX-îlic.lcl-:, .* Oral challenge
41 2H
-41 41
rmt
M M M ?)
r . . i
.w .v. 27
'7
I'moiH ' - . J
in n i: i*
. - .y}:;'*-5'.
T.
s ?.
0-5 • • • • • • • • • • « • • • • «
• • • • • • • •
O r». i
.... '. * ••V: »'A*.i I Mi-r) .. J • -i.
V rl'.à:^ T ^ i °r , l , c
« < A S T ^ o r c icxvi or ;
M J ^ o f f e RAST
... o n ; ; / * normal ^ 'f <" M..,,,, ml. «hiel, i. well al,,,,, ,„e
. ** " ' V* V* Z. - - K 'ii . • • • T' -• '
1 .-•••!»• •
TJr ,;,rr,t,
•"> '•"n l l , ; ,re«l ll.e co.ieiM.tralion ol" «lieal-^aïul rve-specilie-lël: in lîic sera Yr HO • .... - _ . : l. :V • - r
M îvrv;
J .3 J.-
w m m m ;
in groiip (g) (lip. I). In 60"., of the sera .both wheat- ami rye-specific id. às indicated by a RAST score of at least 0-5 for each antigen. In 38%-" v - / J i n r a . n n r i M . r H M ! ! * » . « . . . I I n ! . < < * ' . . . . • • . I . o u t - . ^ ^ . I f ! . ' . I _ IT . . . . . _ I
persons was found, ; of the scrano ryc-spccilic and in 1-5% no wheat-specific Igt was detected. Thc Spearman rank correlation coefficient for thc RAST scores was 0-826 (significantly -different from 0. ^ <0-001 h and Ihe regression equation was:
(wheat score] -• 0-698 |ryc scorc)+0 65l.
Discussion .. "i Wheat and rye flour contain about 10",; protein, also called/gluten/1 his protein includes a large number of separable protein species, which arc Traditionally grouped on the basis of solubility in gliadins. gluteniiis. albumins and globulins (Patcy, 1974). Using crossed imuumoclcctrophorc.sis. HI and s ft ol. ( 1976) demonstrated thc presence of forty protein antigens in a wheat Hour extract. In the sera of thirteen allergic bakers they found Igl: against eighteen of these proteins, which belonged to the gliadin, albumin and globulin groups. Similar experiences in our laboratory led its to couple as many ccrcal proteins as possible to the solid-phase carrier used in our wheat and rye Hour I(AST.
Htands c7 at. (1976) also demonstrated that twenty of the wheat proteins cross-reacted with rye Hour proteins. In analogy with this, we found that the wheat and rye flour RAST usually yielded correlating results. Our wheat RAST was more sensitive and thc rye RAM was positive alone in only two out of 136 cases < l ig. I ). Thus deter-mination of rye Hour-spccific Igl: rarely provided information beyond that obtained by an assay of wheat fiour-spccilic Igl:.
Hour-specific Igl: is frequently found in the sent of bakers with asthma (Table I ) or rhinitis (Hlands et a/., 1976). In our hands, the RAST scorc was frequently only 0*5, but this has, for the present purposes, been considered as a positive test result. In fact, the score 0-5 is a marginal value, which we sometimes also encountered in children and adults with asthma or rhinitis, but with no history of wheat or rye allergy. We conclude that the RAST is useful in the diagnosis of allergy to inhaled wheal or rye Hour dust.
Children with strong and unequivocal food allergies usually have high serum con-centrations of Igl: specific to thc offending food proteins (Aas & Lundkvist, 1973; llolftnan & lladdad, 1974; Schur, llydc & Wypych. 1974; Chiïa et al.. 1976; Dan-nacus et al.. I977J. In our study, child A.K.. 6 years old. had a wheal RAST score of 4 - the highest encountered (Table 3). She had a history of asthma causcd hy flour dust. An oral challenge with wheat causcd diarrhoea and itching within 2 lu. Some years previously she had rcccived a diagnosis of cocliac disease, which was probably erroneous and should have been cereal allergy. Child T.I*., 9 months old, also had a strong and unequivocal réaction urticaria and swelling - upon oral challenge combined witji a wheal RAST scorc of 3. •
On the whole, however, thc diagnosis and treatment of food allergies in children with eczema must be considered an unsolved problem. The RAST has brought only limited aid. Thc presence of food-spccilie Igl: in thc serum can frequently be demons tralcd in thc ahscncc of any obvious sensitivity to thc food in question. This has been shown for many foods, including wheat (llolTman, 1975; llolfman & lladdad, 1975: Dannacus ct aL% 1977), and it is also apparent from our results concerning wheat and rye (Table 3). Specific Igf: to lish is an cuxption; it is rarely, if c\cr. encountered in
i
y f
p.iiucil by sitcli nej::ui\e <l:tl;iL " *
•Six children « i ,h cc /cnw li:ul :, posiuve his.orv. « r positive c ln l lcncc ie<. : - - ' v- •• -
iiiul llic\ n n v !ri\ • l! • ™ « " c enlire.v i lepe.ul.hle. c c Î , , " C r r , , r 5 , , m c ° r , l , C S C « « « • .".pression, lunv-
>cy ; , r , el,m,,,:,.«I l s „ i l l harder. There : ,re. however. M ,n ,e i„ wi,iel,
;
. , iHiuirin u o M aiul 79 agreement respect velv) Simil i r
r r r ™ n,r t,,iv;s ,,,iik- « - - À - & . - , «"orgies .«..IdMein & H e i n e . I<>70,. l-,.r m : , „ v 1 o , H ^ ^ ' V
Uns m:iy IK true ;IIM. for I lie KAST. - 0
^ a ' . r ? i h * 1 * * — r-«-n leu children u i . h H c / ^ disease. )ne liad'^Tuheal KAS'I" mthiv"f 0*5. . «agreement « i , h I l V."'* ^ «mc ludc ihat l.ule or „ „ circulating uhcat-specilic i ! * can be found in such patients. . 1 h
^ i îS»
< f
Acknotv(vif}*iitciifs ,
The s tudy « a s supported hy gram* fro^Alle^
Jtcfcrcnces • 1 '• : " ' " ' v S ' ™ '
,K » £ £ ^ f^nicHifoh.
L L ^ ' r ï r . i n " ,u ,r a n d i^,. mnniatwiMi ,\uh„,-.y„t Alkigy aiul Applied lmmuihit<ic% W»
sm,
M -
. i
2 J 2 gfirf !'» 'W HHl.-1. t.\(iiu.ili(iji of Igcs. IpA ami Igl; « « M » to fond ami-C o n S n -r.."
5hHl a'""
ic 66. .11.
T ^ f r 7.V ' ,ink
*al »"
d ïn'nnmolopîcaf pen^vii^ in food ™iii-iiv.
A review. Journal ttf AlU-rgy. 270. IIMNI;H I ) .C . . C; . I 1 ( K IMN. <;. À R ,» , , ». (IV70I Immuiiochcmicnl ««.lie, ,.r «:kv.c.l s.ihjccK ui.h . wheal mlolcroncc. Journal of All,-rt:v -IS 1U Minjecu lMlh
I h N..KK K. I ) J R j . * |i J . d m , linkers* 3,(1,,,,n. Clmic.,1 MU r,-r. 6.241 1 " " " ' «
1 y ..r talo»" apprend. A final*
I c n n mvcs l i pa i i , , , , . A, l.i ,ill, rv.,l.~-i, 2K.-I* ^
• " . K - . l . c c r c : , . ^ . / , , "'"'T; ^
y," ""
7"
k "
f K-ncinn, r,.,„l : 1>v
niili>iiiuimiiiii:iwiv. Journal ol Allrrgy .m,I f Uni, ,,I Immunol,,gr M | M ' - « « s^nj ^ ..n.n^i^ i., ,
C I / C I I K I . Journal..I .411,-rx, .nuKlini.al Immunol.,Kr « ' V .
ll'NNI' II. II. A lllNfi. T. IIV7II In rilra iliaunii-is ufalupic aHcrgv. Ill <>„:,„-" T w - '•> tlK- r : , . . i . , . . „ , , „ ,>,, „ „ . , „ , ; ,
" " " " " " fi l ial* a\lhma i „ hake,,. . , „ „ „ / „ „ „ , , „ , .
NAKA/AWA. T. Ï I INUIA. T.. I , „,:ka„A. M.. I AVA. I. A K..„AVAM„. S. |IV7>.| l„l,i|.ii..ry clceis
. i t s s z z c : ^ ^ — — l'Aifiv, A.L. (1974) CSIiadin: ihe protein mixture toxic to coeliac palicnls. Umett i 7"
Kmy, ' C " t A n - * ANI»I.H»IN, S.Ci. IIW| An international reference preparation for human . 'mmunoglohului I:, lint ft-/in of the ^ 'oi ltl /It nllh Organization 49
Sc'iiNi RNRKFJHH I l.-W.. SrinnitT, !{.. SitIMIAHSI N*. I'OHCK. (ï. ( l975M)ie Hctlcutiiitp ties Kattio-T n
S V\
VCriî,"
Ch ,,,il 1,C" Jcr niag„o>e aHergischcr l-.rkrankungcn. sU ta ullrrxot.^iat .W 4 M ^
f/VV''
V',"-
J-'- IVs-wliilc scnsiiiviiv and a,.,pic even,a.
/Uh'rgy anil ( lut not hnnumctavr S4 174
f,vVM"'; ,(; W S,m,i" in a «r " -I"-. J-'rnul../ Allergy will < Imirtil Innwautlogy, 58, .W».

Int Archs Allergy appl. Immtm. 52:392-406 (2976)
flour Allergy in Bakers
L Identification of Allergenic fractions in Flour and Comparison of Diagnostic Methods
/. Blonds» B. Diamant, F„ Kallôs, L. Katlâs-Deffner and H. Lfwensteln
Medical Department TA, Rigshospltalet, Department of Pharmacology and Protein Laboratory, University of Copenhagen, Copenhagen
Abstract, Extract of wheat flour obtained by extraction, centrifugation and dialysis was
immunochemically characterized by quantitative Immunoelectrophoresis using rabbit anti-
bodies. Hie analysis revealed wheat flour to be composed o( 40 antigens, some of which were
immunologically partially identical with antigens of rye flour and of common grass pollen.
Furthermore, antigens of the gliadin fraction of wheat flour were identified.
25 bakers with allergic complaints working in and around Copenhagen were clinically
tested with wheat flour and related extracts. Among 13 bakers with respiratory complaints
(asthma and/or rhinitis), 11 showed positive reactions to wheat flour extract when tested in
histamine release from basophil leukocytes radioallergosorbent test and skin test, whereas
further 2 were positive in the basophil test only.
The ability of the IgE of individual sera to adsorb to the individual antigens of wheat
flour was examined by means of crossed radioimmunoelectrûphoresb. On the basis of these
results, individual allergenic components of wheat flour were identified, three of these with
comparatively high affinity and frequency.
Introduction
Bonnevie [1958] pointed out that the
'founder of modern occupational medicine,
Ramazani' as early as in 1700 wrote that
'bakers were often diseased by cough, short-
ness of breath and hoarseness*. Later on,
these respiratory disorders have been diag-
nosed as rhinitis and/or bronchial asthma.
According to Bonnevie, the etiology of
these occupational diseases, allergy to wheat
and/or lye flour, has been established by
Schtoss [1916], who obtained positive im-
mediate skin reactions In asthmatic bakers
with 'ordinary wheat extract'. These early
findings were confirmed and extended for
example by Beagle [1933], Castberg end
Sprensen [1948], van Dtshoeck and Roux
[1939], Schwartz [1952], Gadborg [1956],
Diedrichs and LMbbers [1955], and Pesta-
Received: September 10,1976
id i /D iamant /K f t l l ^ t
JJXZ/ and Schnydei
1929, de Bcsche rej
passive transfer of si
to Prausnltz-KUstne:
isthmatlc bakers ar
fcrgic to wheat floux
that 'these eases art
fcrgic asthma, acquh
the influence of spc
work (i.e. expositioc
ieems to be justified
order as occupation
t^s disease' (transit
From 1952 to 1!
Deffner [1971] bv
Based on anamac
symptoms, the result
sal provocation (
1946] with flour ei
diagnosed in 163 ce
the affectcd cases)
(48Vo) rhinitis and i
tds-Deffner [1971]
without typical clini
a positive skin or pr
extract 85 of the i
krgic to wheat flout
and 37 (23°/o) to be
their occupational (
and asthma due to
rye pollen extract e
this group a posit"
the flour-allergic bai
Other cereal product
zàtion to flour occu;
.within the 1st yea;
•76.7«/o of the case:
between the 2nd aj
aional activity. Thit
^explained [Marsh, 1'
? Rhinitis was in a
i'der, and asthma oc
393
ods
"tory,
i
I
to/ flwrf Schnyder [1955]. As early as
1929, reported on the successful
passive transfer of skin reactivity (according
to Prausnitz-KUstner) with tho serum of 3 tfthmatic bakers and 3 grain workers aU
kigic to wheat flour. De Besche concluded
that 'these cases are to be regarded as al-
lergie asthma, acquired by individuals under
fre influenco of special conditions in their
work (i.e. exposition to flour dust). Thus, it
jeems to be Justified to characterize this dis-
order as occupational disease, namely bak-
er's disease* (translated by us).
From 1952 to 1971, Kallôs and Kallôs-
Deffner [1971] investigated 583 bakers.
Based on anamnesis, clinical signs and
symptoms, the results of skin testing and na-
lal provocation [Urbach and Gottlieb,
1946] with flour extract, flour allergy was
diagnosed in 163 cases (30%). 85 (52% of
(he affected cases) had rhinitis only, 78
(48%) rhinitis and asthma. Kallôs and Kal-
tés-Deffner [1971] obtained in no case
without typical clinical signs and symptoms
ft positive skin or provocation test with flour
«tract 85 of the reactors (53%) were al-
lergic to wheat flour, 41 (25%) to rye flour,
find 37 (23%) to both. 4 cases had, besides
their occupational disease, seasonal rhinitis
and asthma due to grass pollen. Whoat or
tyc pollen extract elicited in no case within
this group a positive skin reaction. AU of
the flour-allergic bakers could eat bread and
other cereal products with impunity. Sensiti-
zation to flour occurred in 38 cases (23.3%)
within the 1st year in the profession. In
76.7% of the cases, sensitization occurred
. between the 2nd and 15th year of profes-
sional activity. This discrepancy cannot be
explained [Marsh, 1975].
Rhinitis was in all cases the initial disor-der, and asthma occurred in about half of
J* I
the cases 6 months to 10 years later. These
observations are in good accordance with
the literature. Continuous exposition to
flour dust leads in individuals with heredi-
tary disposition to sensitization and allergic
disease [Marsh, 1975]. The best prophylac-
tic measure is to diminish or eliminate this
exposition. According to Kallôs and Kallôs-
Deffner [1971], tho frequency of sensitiza-
tion Is clearly decreasing in modem baker-
ies, where flour is handled in a completely
closed system.
KaOâs and Kallôs-Deffner [1971] used
freshly prepared conventional flour extract
(Coca's solution, 1:10 w/v, undiluted for
nasal provocation, appropriately diluted for
skin tests) in their investigations. They
showed that allergenic activity is confined to
the protein fraction of flour extract
In a recent investigation, Hoffmann
[1975] analyzed the inhibitory effect of dif-
ferent protein fractions of whoat and whole
wheat extracts as well as the cross-reaction
between grass pollen and wheat flour by
means of the radioallergosorbent test
(RAST). He found generally a low cross-
reactivity between grass pollen and wheat
flour. Among the wheat protein fractions
studied, the highest reactivities (Le. allcr-
genicity) were found in the most soluble'
fractions.
In the present investigation, we attempt-
ed to evaluate the histamine liberation In-
duced by wheat flour extract from basophil
leukocytes in a group of allergic bakere and
appropriate controls and to correlate the re-
sults to the clinical state of the patients as
well as to their stdn reactivity, and to the re-
sults of In vitro tests such as radioimmuno-
sorbent test (RIST) and RAST with flour
extract. Finally, the protein fraction of flour
extract has been analysed by means of
crossed radioinummoelectrophoresU (CRIE), in an attempt to identify the individual proteins with allergenic activity as well as to compare it with related antigen sources.
Materials and Methods
Patients
25 bakers with allergic complaints working id and around Copenhagen were submitted to the various allergy tests. Contact with the bakere was obtained through a previous questionnaire distrib-uted through the Danish Bakers* Union and vol-untarily answered. All bakers investigated, except patient 1, were, at the time of the Investigation, actively working in their profession in which they had been active between 5 and 50 yean. $kfn tests were performed on the same day as blood was taken for the basophil test, total Igfi (RZST), spé-cifie IgB (RAST), and CRIB. In the CRIB test 5 normal individuals and 4 patients not allergic to flour were Included (controls).
Antigens
Extraction of wheat floor (Kbngstfrnen, Swe-den) was performed by gently agisting g 20% (w/v) suspension at 5 ° C overnight in ammonium acetate (Ionic strength 0.14, pH &2)..The suspen-sion was centrifuged twice at 5 ®G for 120 min at 10.000 g. The supernatant was denoted St MS 74
and was stored cither unchanged or as 0.05 M
phenol solution or as 0.015 M sodium azide solu-tion at - 2 0 °C.
St MS 74 was thawed, centrifuged at 0 °C for 60 min at 50,000;. The supernatant was dialyzed once against a 50-fold volume of 0.025 M ammon-ium bicarbonate, 0.015 M sodium a2ide and then twice against 0.005 ammonium bicarbonate for 24 h at 5 °C. The product was freeze-drled and stored dry at 5 A solution (lOg-i, denoted hereafter St MS 74. DF) of the freeie-dried prod-uct was then made up in 0.1 M sodium bicarbon-ate, 0.015 M sodium azide. Small amounts of the supernatant and the dialyzed extract were stored a t - 2 0 °C as controls.
Extraction of rye flour (Dansk Mel Central, Denmark) was performed essentially as described for St MS 74 D F by agitation of a 10% (w/v) sus-
pension in 0.123 M ammonium bicarbonate. 0.015 M sodium azide at 5 ° C overnight, and suV soquently centrifuged for 60 min at 0 ° C at 50,000 g, dialyzed twice against 50-fold volume of 0.005 M ammonium bicarbonate, 0.015 M sodium azide and once against water for 24 h at 5 °C. Fj. nally, freezc-drylng and storage at 5 ° C . A ]•/• (w/v) solution in 0.1 M sodium bicarbonate denoted St Ru 7S and was stored either un-changed or as 0.015 M sodium azide solution it -20
ÛG
Freeze-dricd extracts of pollen from timothy, rye grass, blue grass, false oat, and orchard were produced as described for rye flour and were uted as 2 % (w/v) solutions In 0.15 M sodium chloride. 0.015 M sodium azide,
Olladln (Sigma Chemical Company, St. Louis, Mo.) 10% (w/v) was suspended in 0.1 M sodium bicarbonate, 0.015 M sodium azide for l h at 20 °C and centrifuged at 0 ° C for 80 mm at 50,000;. The supernatant was denoted glladln 1*U
and stored at - 2 0 °C. H i e protein content of St MS 74, St MS 74
DF, St Ru 75, and glladln was 3.4, 3.9, 3.6, and 1.2 g 1"», respectively. The latter determina-tion Was performed by the method of Lowry et at. £1951] using bovine albumin as standard.
Antibodies
Antibodies against the extract of wheat flour were raised by immunizing 3 rabbits with St MS 74 for 3 months and thereafter with St MS 74 DF for 6 months. The immunization and subsequent purification were performed according to Harboe
and Ingltd [1973], '"I-immufioabsorbed rabbit immunoglobulin*
against human IgB Were prepared as described by Lfwenstetn and Week* [1975].
Immunoelectrophorettc Methods
Equipment and reagents were essentially as de-scribed by Weeke 11973]; The electrophoreses were performed in 1% (w/v) agarose gel» batch 102 Dx (Lltex, Glostrup. Denmark) containing a buffer of 0 .073/ / Tris, 0.024 M barbital, 0.006A/ calcium lactate, and 0.003 M sodium aside (pH 8.6, 25 °C). Crossed Immunoelectrophoresis (ClE) and croBsed-line Immunoelectrophoresis (CUE) were performed as described by AxeUen et ai
11973). Because of the cathodic migration, both an
anodic and cathodic toed (fig. 1). Unless otl coud-dimension electn la a 0.15-cm-thick gel i In 0.10-cm-thick gel at lively. 7 X 5 cm glass p i CUE. The thickness o 0,12 cm. 1% (v/v; retail Of Aprotinin (Novo» h the antibody-contaittinj degradation [Bferrum
«ere pressed, washed stained with Coomassi scribed by Weeke (1973
CRIE
CRIE was perform end Lfiwensteln (1973]. st room temperature follows: (1) Incubation VIS M phosphate biifi serum added to the pi
cover the gel film on being left to react over proteins were removed with 10-20 ml of 0.1 A four times for 10-min 7 ml of incubation bufi er, pH 7 J , containing t
albumin, 0.9% w/v soc sodium azide, and 1% log to 0 3 5 fi Ci and gi 200,000 cpm in our gar Ihe gel and allowed to honbound " 'I-antl-lgE W later experiments; t With 10-20 ml saline s distilled water, the gel * tn hot air and placcd « proof box. The expose day to 2 months, and >lato Was stained for
Brilliant Blue. » *
LAutoradiography
Autoradiography w Lfwenstetn tt ah t
urc time necessary t e various precipitata jmnned days 0-1, 1 -
Ë&rboaatt, ; and sub-
o-c « volume or M sodium 1 Î.°C FJ-C . A I*/,
»nat« w u
fltber to-
DlotiOQ i|
-, timothy,
lard were
"ere used
chloride.
saodic and cathodic second dimension gel was
jjsed (fig. 1). Unless otherwise stated, first- and se-
cond-dimension electrophoreses were performed
fa a 0.15-cm-thick gel at l O V c m-' for 30 min and
b 0.10-cm-ihick get at 2 V c m ~ i for 15 h, respec-
tively. 7 X 3 c m glass plates were used for CIE and
C U E . The thickness of the intermediate gels was
0.12 c m . l*/o (v/v; relative to the antibody volume)
of Aprotinin (Novo, Mainz. B R D ) was added to
(be antibody-containing gels to prevent proteolytic
degradation [Blerrum et at., 1975]. The plates
were pressed, washed, and dried, and Anally
tiained with Coomassie Brilliant Blue R as de-
scribed by Weeke [1973).
CRIE
C R I E was performed as described by Weeke
end Lfwensteln {1973]. T h e procedures performed
tt room temperature (18-r24 °C) were briefly as
follows; (1) Incubation with patient scrum: 7 m l of
î/1 S M phosphate buffer (pH 7 J ) and 0.7 m l of
serum added to the plastic box was sufficient to
cover the gel film on the glass plate; (2) after
being left to react overnight, the non-bound serum
proteins were removed from the gel by washing it
with 10-20 m l of 0.1 M sodium chloride at least
four times for 10-min periods; (3) l U(-antMgE in
7 m l of incubation buffer (0.05 M phosphate buff-
er, p H 7.5. containing 0.3e/o (w/v) of bovine serum
albumin, 0.9% w/v sodium chloridc, ÔÏ1% w/v of
lodium azide» and 1 % w/v of E D T A ) , correspond-
ing to 0.35 jid and givlns rise to approximately
200,000 c p m in our gamma-counter, was added to
the gel and allowed to react for at least 1 day; (4)
£onbound '"I-antl-IgE was recovered and stored
for later experiments; (5) after 4 10-mln washings
With 10-20 mt saline and finally 1 washing with
distilled water, the gel on the glass plate was dried
in hot air and placed on an X-ray film in a light-
proof box. The exposure time was varied from t
day to 2 months, and (6) the gel on the glass
^plate wo* stained for proteins with Coomassie
«Brilliant Blue,
Autoradiography
* Autoradiography was performed- as described
^by Ltwenstrtn et al. J1976) by measuring the ex-
Iposure time necessary for visible radlostaining of
;the various preclpHates. The periods of exposure
^Spanned days 0-1. 1-7, and 8-43, which, after
correcting for the radioactive dccay of l t s
I,
amounted to 1, 6.7 and 26.8 days. T h e activity
bound to the various precipitate* was graded 27,
4, and 1, respectively (normalized reciprocal val-
ues of the corrected exposure times), correspond-
ing to visible radiostaining after 1, 8, and 43 days.
In case of very strong radiostaining, the grading
was multiplied by factor 2. T h e values obtained
were further corrected for the mean unspeclflc
IgE uptake in wheat C R I E performed on 4 non-
allergic aad 5 non-flour-allergic subjects.
RIST
Phadcbas IgE (Pharmacia) was used for the
determination of total IgE In the analyzed sera.
The total IgE concentrations were expressed in
Uml-i by comparison with à W H O standard ser-
u m [Rowe, 1971). 1 U corresponds approximately
to 2.4 ng {Bazaral and Hamburger, 1972). T h e re-
producibility of the determinations was about
1 0 % . W e took a value of 26-630 Urn1" as being a
normal 9 5 % range in adults.
RAST
R A S T was performed with St M S 74, coupled
to activated filter paper discs according to Ceska
et al, (1972). The results were expressed in sor-
bent units (SU) and in allergy classes (class 0, 1,
2, 3, and 4, corresponding to 0-1,2-3, 4-19, 20-99
and 9 X 1 0 0 $ U , respectively), using the reaction of
the serum (diluted X10) from a patient (H. D.) al-
lergic to timothy as a 100 S U reference. T h e grad-
ing system corresponds to that for Phadebas
R A S T (Pharmacia) reference (birch allergen and
birch allergie reference lerum). The determina-
tions were performed in duplicate.
The duplicate determinations were run twice
for each serum and the mean va|uo9 were used.
RAST Inhibition Experiments
They were performed as dcscribcd by Nielsen
et al. (1974) and the concentrations corresponding
to a 5 0 % inhibition (C"V.) were measured.
The inhibition experiments were performed
with gliadin 1 % , having dilutions from 1 to 10~*
in steps of I decade. St M S 74 was used as the al-
lergen reference in the experiments. Sera from the
patients listed in table 1 were used.
Intracutaneous tests (IC)
They were carried out on the volnr «de of the
ri- 11
396 Blands/Diamanl/Kallôs/KaUds-Dcffncr/l wen ftd l i , A U ç f g y in Bakers x
antebrachium. using a histamine ^hydrochloride
solution (0.1 m g ml"») as a reference. St M S 74
(wheat flour) dissolved in 0.9V» sodium chloride,
0.5°/o phenol (w/v) and diluted X l O M O * was used
for the skin testing. The dilutions were carried out
less than 1 month before performing the tests. T h e
area of Ihe urticarial wheal wa« determined by
multiplying the mutually perpendicular diameters
(in millimeters). According to the Scandinavian
Allergy Standard IA at and Bettn, 1972J a 3 +
reactlon corresponds to t histamine equivalent.
In some cases, St R u 75 (ryo flour) was tested
using similar criteria.
IC St M S 74 x I0-4 m m X m m —skin test index
IC histamine, 0.1 m g ml- 1 m m x m m
was used when compared with the various In vitro
tests.
Separation of the Leukocyte Fraction from
Whole Blood
The procedures follow in general the methods
described by Bjyum {1968] and Day [1972]. 9 m l
venous blood was collected In a plastic tube (vol-
u m e 10 ml) containing E D T A (0.5 m l of a 0.2 M
solution). After gentle mixture, 7.5 m l was diluted
with 22.5 m l N a C I (0.9Vs) in a 50 ml plastic tube.
Sodium diatrizoate (10.50/o w/v; Winthrop Labora-
tories Ltd., Surrey, England) or in most experi-
ments sodium metrizoate (10J®/o w/v; Nyegaard
A S , Oslo, Norway) mixed with Flcoll (6.4°/o w/v)
and adjusted with distillod water to a specific
gravity of 1.080 was used as separation fluid.
1 1 m l of the separation fluid was layered bélow
the blood suspension with carc taken to maintain
a sharp interphase. T h e tube was centrifuged at
400 g for 40 min at room temperature. The inter-phase containing leukocytes was harvested by the
use of a Pasteur pipette. The cell suspension was
diluted with 10 mi of a balanced salt solution
(BSS) containing 131 m W NaCI, 2.4 m A f KC1,
E D T A 1 mM and 1 mg/ml h u m a n scrum albumin
buffered to p H 7.0 with S0rensen phosphate buff-
er (6.7 mM). T h c cells were washed twice by cen-
Crifugation for 10 min at 70;. They were finally
diluted in 150//I of the same BSS, except that
E D T A was exchanged for 1.5 mM CaCI,.
incubation Procedures
5 (t\ of the cell suspension was added to 200 u\
prewarmed (37 °C) calcium-BSS containing suiia.
ble dilutions of the antigens. Routinely, the ami-
gens (wheat and rye flour extracts free of azidej
were tested in dilutions 10~*-10~". Each dilution
was run in triplicate.
Incubation was performed in small glass tube*
( O D 7 m m , ID 5 m m , length 50 m m ) for 30 min at 37 °C The tubes were then placed on ice and cen-
trifuged for 10min at.600; at 4 °C T h e supertu.
tant was transferred by-the use of a constriction
pipette to new tubes containing 5 /«I of 3 N HCI.
T h e cell residues were placed on a boiling v.aier
bath for 5 min after the addition of 200 /il.of div
tilled water and 5/<| of 3 /V HCI. In each experi-
ment, the spontaneous histamine release was de-
termined as well as possible blank values for the highest concentration of antigens.
Histamine Determination
T o each supernatant and precipitate 30 «I
1.25 N N a O H was added followed by 10 1 ortho-
phtaldialdehyde (l*/e dissolved in methanol). After
exactly 4 min, 10/il of 3 N H C I was added to the
tubes. Vigorous mixing was performed after' Victi
addition. Following centrifugation for 10 min at
2.500 the fluorescence was read in a Farmnd
Ratio Fluorometer supplied with a Farrand car-
rier and adaptor suitable for the small incubation
tubes used.
Histamine release was determined as a percen-
tage of the total histamine content of each sample.
Although the maximal release could vary between
different individuals, the concentration of the »n-
tigen solution which released 50°/o of the maxi-
m u m values was determined.after graphic registra-
tion of the results. In some cases, it was necessary
to decrease the antigen concentration below !•' '*
lo obtain this value.
Storage, of Blood Samples
For convenience it was of interest lo determine
if blood camples could be stored 12-24 h before
separation of the leukocytes without loss of reac-tivity or cells. This was determined In 5 cases. Du-
plicate blood samples* were stored overnight w
4 °C before separation and incubation. In 4 ca*e<«
identical release values and similar histamine ex-
tent of the separated cells were found for stored
blood as compared to blood immediately used
Fig-1* Extract of wheal fit
ClE In l°/o (w/v) agarose gel c> fris, 0.024 M barbital, 0.006 Ai
ind 0.0003 M sodium azide (p!
15 °C. a Antigens: 10 fA of Si fpplied. First dimension: 10 V c:
thick gel for 25 min. A n o d e to li les: 20 cm"', rabbit antibodi.
of wheat flour. Second dimens
0.10-cm-thtck anodic ( + ) and
separation and study of the rcac
pie reason why one of the blood
plvc similar results after storage
tabllshed. At present, however,
tannot be excluded.
Statistical E vat tuition of Corr
Rank difference coefficient c
letermlned between I he results o
eat testa and is given in the text.
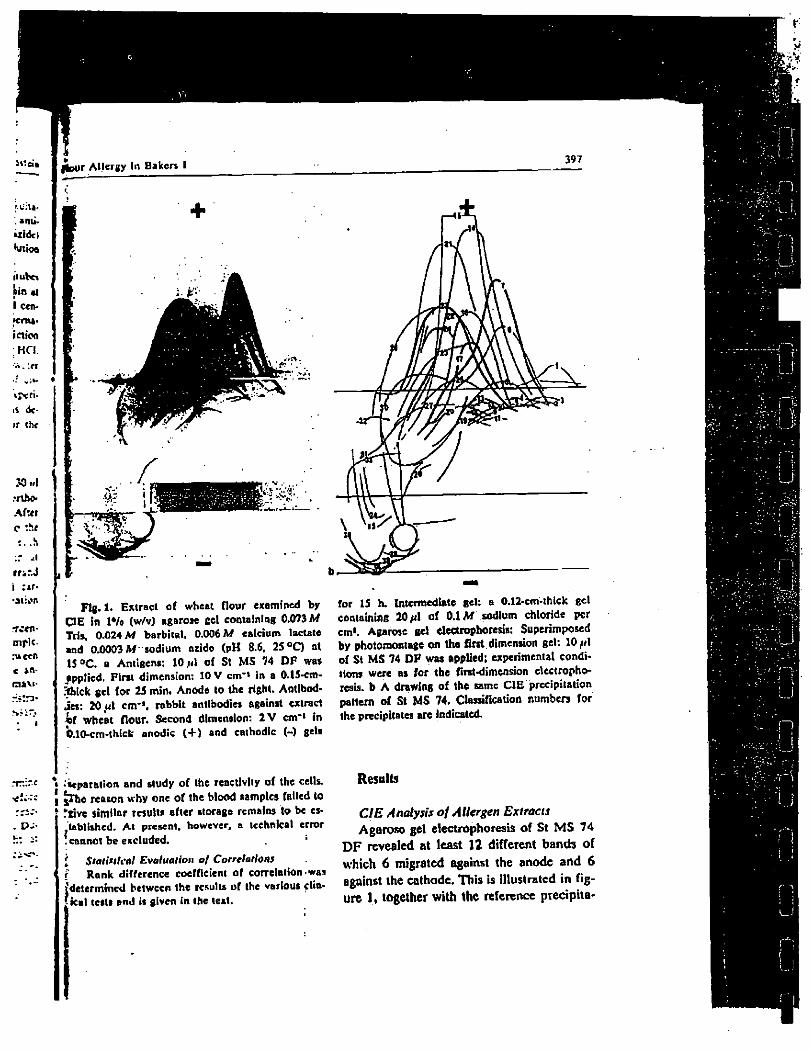
jfeur Allergy In Bakers I 397
Fig. 1. Extract of wheat flour examined by
CIE in !*/• (w/v) agarose gel containing 0.073 M
Tris, 0.024 M barbital. 0.006 M calcium lactate
and 0.0003 M sodium oxide (pH 8.6, 25 °C) at
15 °C. a Antigens: 10/<1 of St M S 74 D F was
applied. First dimension: 10 V cm"» In a 0.15-cm-
Shlck gel for 25 mïn. Anode to the right. Antibod-
ies: 20 ut cm*1, rabbit antibodies against extract
if wheat flour. Second dimension: 2 V cm"» in
b.lO-cm-thlck anodic (+) and cathodic (-) gets
for 15 h. Intermediate gel: a 0.12-cm-thlck gel
containing 20 /il of 0.1 M sodium chloride per
cm1. Agarose gel electrophoresis: Superimposed
by photomontage on the first dimension gel: 10/fi
of St M S 74 D P was applied; experimental condi-
tions were as for the first-dimension electropho-
resis. b A drawing of the same CIE précipitation
pattern of St M S 74. Classification numbers for
the precipitates are Indicated. . n
• • separation and study of the reactivity of the cells.
[ Jrh« reason why one of the blood samples failed to
îgive similar results after storage remains to be es-
tablished. At present, however, a technical error
'cannot be excluded.
I Statistical Evaluation of Correlations
f Rank difference coefficient of correlation was determined between the results of the various clin-ical tests and is given in the text.
Results
CIE Analysis of Allergen Extracts
Agaroso gel electrophoresis of St MS 74 D F revealed at least 12 different bands of which 6 migrated against the anode and 6 against the cathode. This is Illustrated in fig-ure 1, together with the reference précipita-
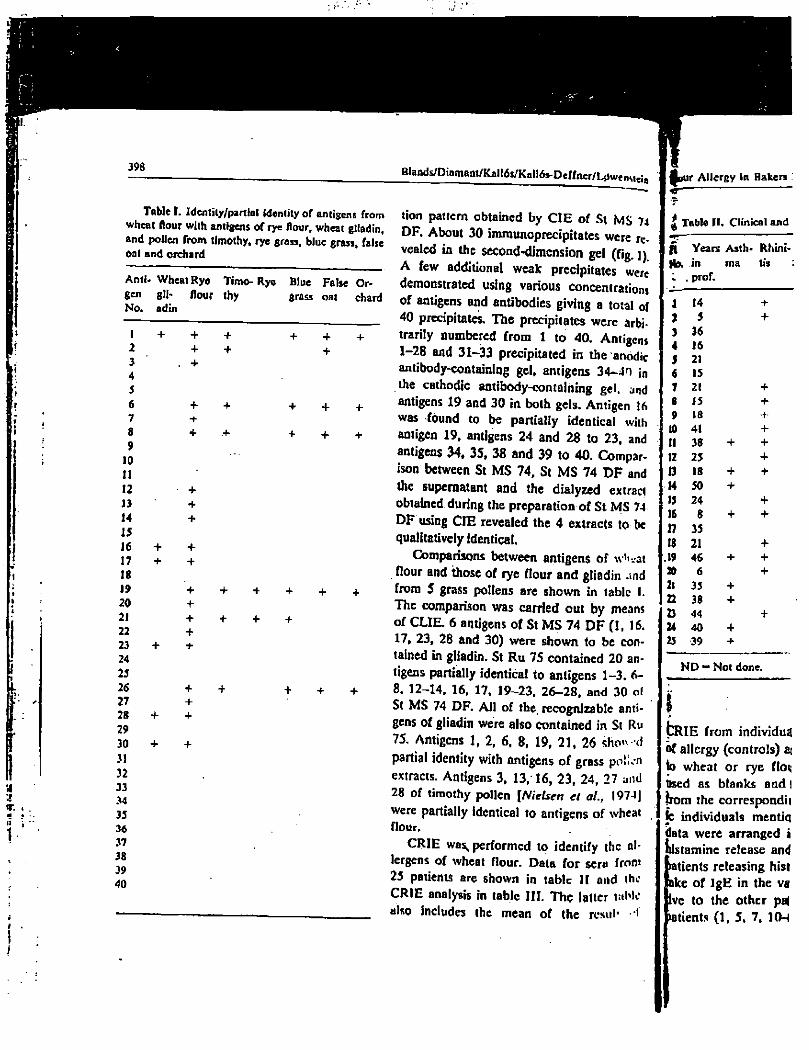
398
Table I. Identity/partial Identity of antigens from wheat flour with antigens of rye flour, wheat gliadin, and pollen from timothy, rye grass, blue grass, false oat and orchard
Anti* Wheat Rye gen gtl- flour No. adin
Timo- Rye
thy Blue grass
False Cr-oat chard
I + + 2 + 3 . + 4 5 6 + 7 8 + 9
10 11 12 • +
13 + 14 + 15 16 + + 17 + + 18 19 + 20 + 21 + 22 + 23 + 24 25 26 + 27 + 28 + + 29 30 + + 31 32 33 34 35 36 37 38 39 40
+ + + +
+ + + +
+ + +
Blands/Dinmant/Kali6s/KaH6s-Deffner/L0wenMg;a f f u r Allergy in Bakers «
| Table II. Clinical and tion pattern obtained by CIE of St M S 74
DF. About 30 immunoprecipitates were re-vealed in the second-dimension gel (fig. ]) A few additional weak precipitates were demonstrated using various concentration» of antigens and antibodies giving a total of 40 precipitates. The precipitates were arbi-trarily numbered from I to 40. Antigens 1 -28 and 31-33 precipitated in the anodic antibody-containing gel, antigens 34-40 in the cathodic antibody-containing gel. and antigens 19 and 30 in both gels. Antigen 16 was found to be partially identical with antigen 19, antigens 24 and 28 to 23, and antigens 34, 35, 38 and 39 to 40. Compar-ison between St MS 74, St MS 74 D F and the supernatant and the dialyzed extract obtained during the preparation of St MS 74 DF using CIE revealed the 4 extracts to be qualitatively identical.
Comparisons between antigens of wh.at flour and those of rye flour and gliadin and from 5 grass pollens are shown in table I. The comparison was carried out by means of CUE. 6 antigens of St MS 74 DF (1,16. 17, 23, 28 and 30) were shown to be con-tained in gliadin. St Ru 75 contained 20 an-tigens partially identical to antigens 1-3. 6-8, 12-14, 16, 17. 19-23, 26-28, and 30 of St MS 74 DF. All of the. recognizable anti-gens of gliadin were also contained in St Ru 75. Antigens 1, 2, 6, 8, 19, 21, 26 ifom-d partial identity with antigens of grass poîi.n extracts. Antigens 3, 13, 16, 23, 24, 27 and 28 of timothy pollen [Nielsen et al., I974| were partially identical to antigens of wheat flour.
CRIE was, performed to identify the al-lergens of wheat flour. Data for sera from 25 patients are shown in tabic I I and the CRIE analysis in table I I I . The latter uiMo also includes the mean of the rcsul1 •'<
n Years Asth- Rhini-in ma tis prof.
i 14 +
2 5 + 3 36 4 16 5 21 6 15 7 21 + 8 15 + 9 18 +
10 41 + 11 38 + + 12 25 + 13 18 + + 14 50 + 15 24 + 16 8 + + 17 35 18 21 +
.19 46 + + 20 6 + 2! 35 + n 38 + 23 44 + 24 40 4 25 39 +
N D - Not done.
I >
fcRIE from individu^ ôf allergy (controls) ai to wheat or rye floç Used as blanks and I from the correspondit le individuals mentiq data were arranged i histamine release and
tients releasing hist ke of IgE in the vg ve to the other pal tients (1, 5. 7, 10H
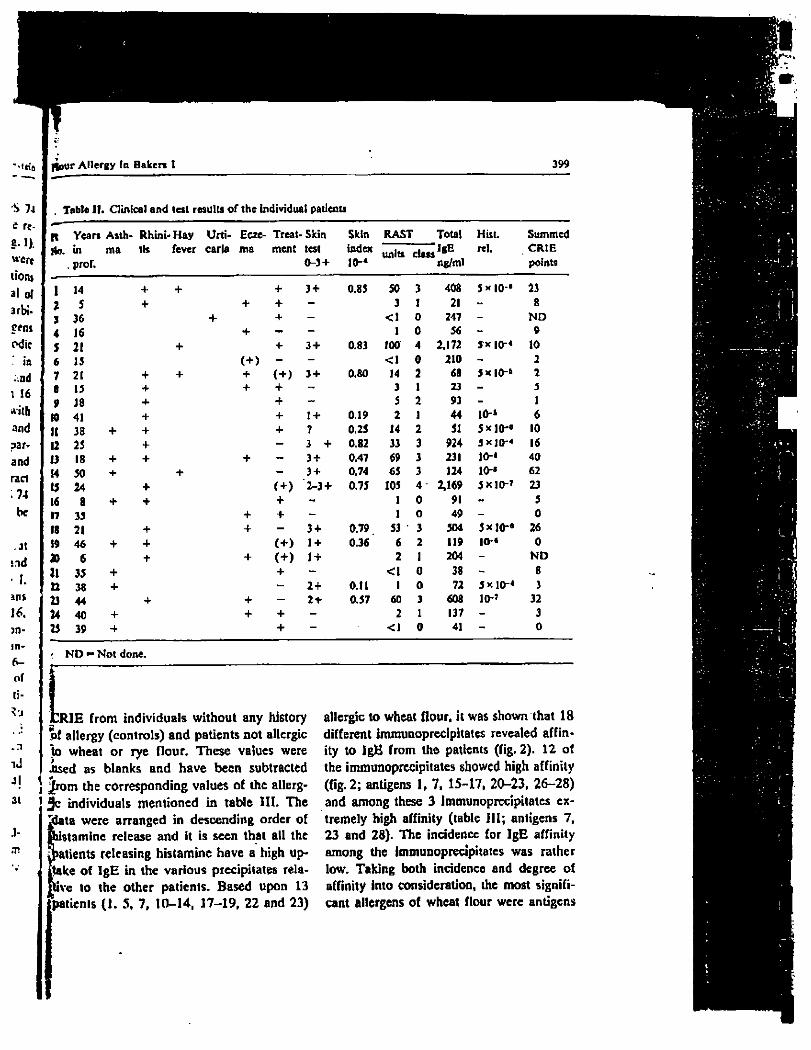
Itour Allergy (n Bakers 1 399
Table II. Clinical and lest results of the individual patients
R Years Asth* Rhini- Hay Urti- Ecze- Treat--Skin Skin R A S T Total Hist. S u m m e d
Ko. in m a tls fever caria m a ment test index units class IgE rcl. C R I E
prof. 0-3 + 10-* units class
ng/ml points
1 14 + + + 3 + 0.83 50 3 408 5*10-* 23
2 5 + + + - 3 1 21 - 8
3 36 + + - < 1 0 247 - N D
4 16 + - - 1 0 56 - 9
S 21 + + 3 + 0.83 100 4 2.172 3 x 10-4 10
6 15 - - < 1 0 210 - 2
7 21 + + + 3 + 0.8O 14 2 68 5x10-® 2
B 15 + + + - 3 1 23 - 5
9 18 + + 5 2 93 - 1
to 41 + + 1 + 0.19 2 1 44 10-4 6
II 38 + + ? 0.25 14 2 51 5 * 10-» 10
12 25 + - 3 + 0.82 33 3 924 JXJQ-4 16
U 18 + + + - 3 + 0.47 69 3 231 io-« 40
14 50 + - 3 + 0.74 65 3 124 10-® 62
15 24 + 2-3 + 0.75 105 4" 2,169 5*10-* 23
16 8 + + + - 1 0 91 - 5
n 35 + + - 1 0 49 - 0
18 21 + + - 3 + 0.79 53 3 504 5xl0-« 26
19 46 + + (+) 1 + 0.36 6 2 119 10-« 0
20 6 + + (+) 1 + 2 1 204 - N D
21 35 + + - < 1 0 38 - 8
22 38 + - 2 + 0.11 1 0 72 5x10-* 3
23 44 + + - 2 + 0.57 60 3 608 10-' 32
24 40 + + + - 2 1 137 - 3
25 39 + - < 1 0 41 - 0
. n
iJ
N D - Not done.
I RIE from individuals without any history allergic to wheat flour, it was shown that 18 of allergy (controls) and patients not allergic different immunoprecipitates revealed affin-to wheat or rye flour. These values were ity to IgB from the patients (fig. 2). 12 of ised as blanks and have been subtracted the immunoprecipitates showed high affinity
J ^rom the corresponding values of the allerg- (fig. 2; antigens 1, 7, 15-17, 20-23, 26-28) 31 3c individuals mentioned in table I I I . The and among these 3 immunoprecipitates ex-
[data were arranged in descending order of tremely high affinity (table I I I ; antigens 7, staminé release and it is seen that all the 23 and 28). The incidence for IgE affinity tients releasing histamine have a high up- among the Immunoprecipitates was rather
take of IgE in the various precipitates rela- low. Taking both incidence and degree of ive to the other patients. Based upon 13 affinity Into consideration, the most signifi-
patienis (J. 5, 7, 10-14, 17-19, 22 and 23) cant allergens of wheat flour were antigens
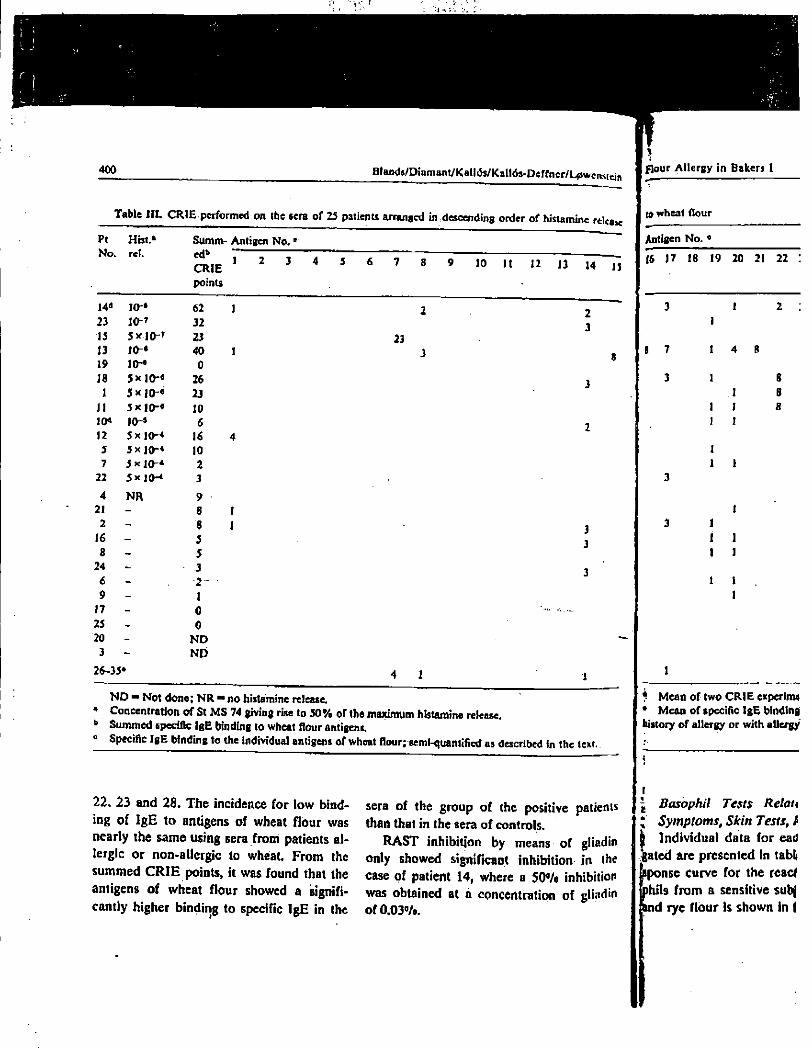
400 Btand$/D»amant/KaUOj/KaH6s-Peffncf/L0wcnstein
} flour Allergy in Bakers I
Table III C R I E performed on the sera of 25 patients arranged in descending order, of histamine release
S u m m - Antigen No.0
Pt Hist.*
N o . ret. ed*
C R I E
points
10 It 12 n u
14 d IO-* 62
23 10-7
32
15 5XJO-T 23
13 I0-* 40 19 io-« 0
IS 5*10-« 26
1 5xiO-« 23
11 5xj0-« 10 10* IO-* 6 12 5x|0-« 16 5 5x]0-« 10 7 5*10"* 2
22 5 * 10-* 3
4 N R 9 21 - 8 2 - 8 16 - 5 8 - 5
24 - 3
6 - 2 -9 - I 17 - 0
25 - 0 20 - N D 3 - N D
26-33*
23
4 1
N D - Not done; N R - no histamine release.
Concentration of St M S 74 giving rise to 5 0 % of the maximum histamine release.
S u m m e d specific IgE binding to wheat flour antigens.
Specific IgE binding to the individual antigens of wheat flour; semi-quantified as described in the text..
M
22. 23 and 28. The incidence for low bind-
ing of IgE to antigens of wheat flour was
nearly the same using sera from patients al-
lergic or non-allergic to wheat. From the
summed CRIE points, it was found that the
antigens of wheat flour showed a signifi-
cantly higher binding to specific IgE in the
sera of the group of the positive patients
than that in the sera of controls.
RAST inhibition by means of gliadin
only showed significant inhibition in the
case of patient 14, where a .50% inhibition
was obtained at â concentration of gliadin
of 0.03°/o.
to wheat flour
Antigen N o . 4
16 17 18 19 20 21 22
I 7
3
I 4
1 1
1 I
1 I
I
1 1
I
1 1 1 I 1
1 I 1
? M e a n of two C R I E cxperinM
* M e a n of specific IgE binding
history of allergy or with allergy
I Basophil Tests Relau
; Symptoms, Skin Tests, /
| Individual data for ead
gated are presented in tablj
sponse curve for the read
phils from a sensitive subj
and rye flour Is shown In f
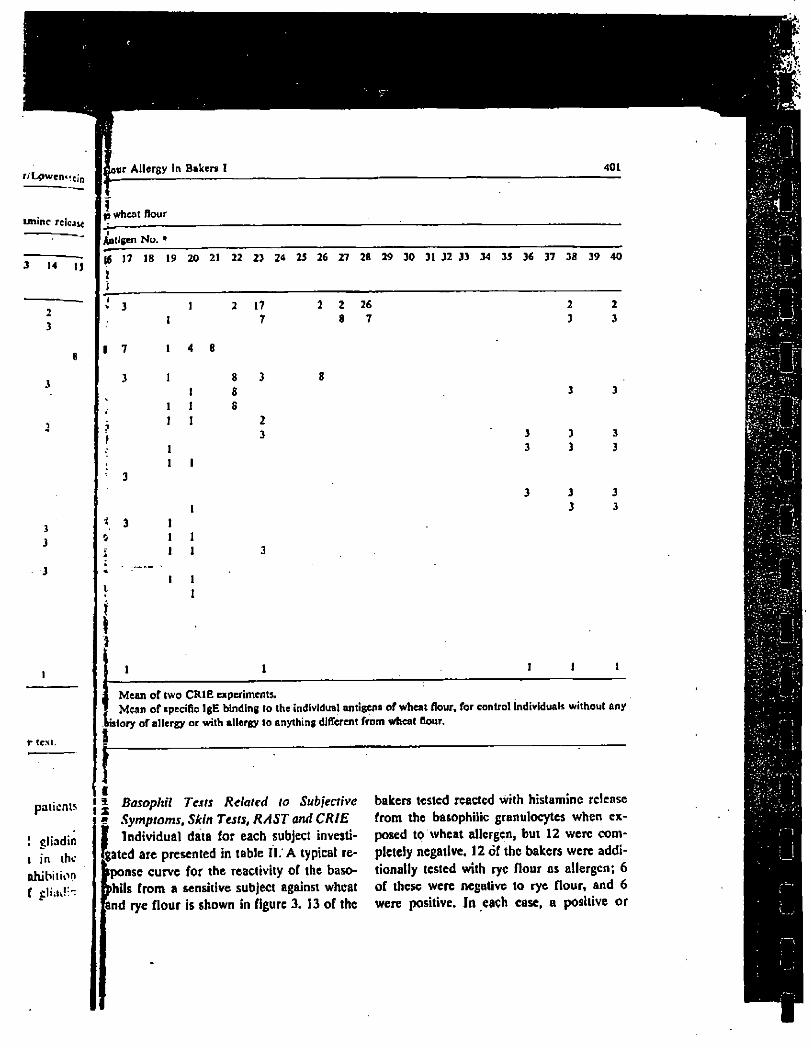
r/L0wen<«cin »ur Allergy In Bakers I 401
tminc re leak
M Ij
t (ext.
! gliadin I in thc ohihition f
ID wheat flour
Antigen No. 4
|6 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
j
3
I 7
3
2 17 7
2 2 26 8 7
* 3 0
1 4 8
1 1
1 1 1 I
1 1 1
1 1 1
1 1 1
I . Mean of two C R I B experiments.
Mean of specific IgE binding to the individual antigens of wheal flour, for control individuals without any
ristory of allergy or with allergy to anything different from wheat flour.
i patients { | Basophil Tests Related to Subjective
Symptoms, Skin Tests, RAST and CRIE
Individual data for each subject investi-gated are presented in table II. A typical re-sponse curve for the reactivity of the baso-phils from a sensitive subject against wheat ind rye flour is shown in figure 3. 13 of the
bakers tested reacted with histamine release from the basophilic granulocytes when ex-posed to wheat allergen, but 12 were com-pletely negative. 12 of thc bakers were addi-tionally tested with rye flour as allergen; 6 of these were negative to rye flour, and 6 were positive. In each case, a positive or
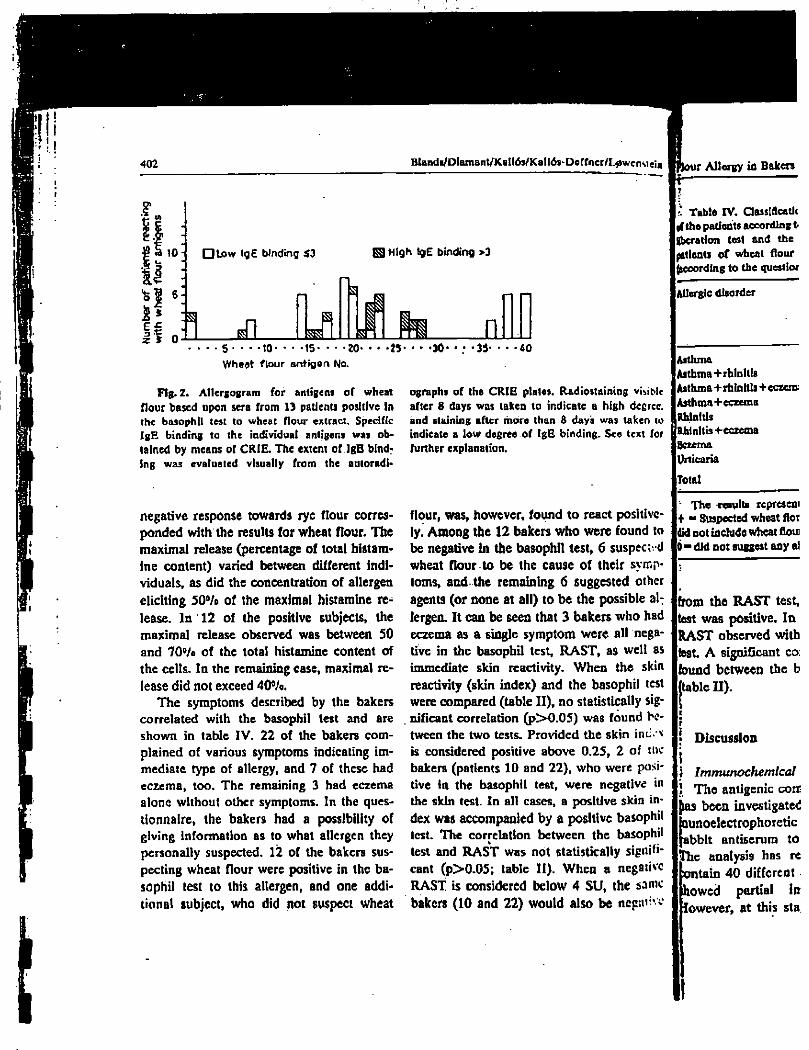
10
i l i 6-J
• Low IgE binding $3 0 High IgE binding >3
A j i n 5 10 15- • • • 20*
Wheat flour antigen No.
M- •30 33« 40
Fig. 2. All ergo gram for antigens of wheat
flour based upon sera from 13 patients positive In
the basophil test to wheat flour extract. Specific
IgE binding to the individual antigens was ob-
tained by means or CRIE. The extent of IgE bind-ing was evaluated visually from the autoradl-
negative response towards rye flour corres-ponded with the results for wheat flour. The maximal release (percentage of total histam-ine content) varied between different indi-viduals, as did the concentration of allergen eliciting 50% of the maximal histamine re-lease. In 12 of the positive subjects, the maximal release observed was between 50 and 70% of the total histamine content of the celts. In the remaining case, maximal re-lease did not exceed 40%.
The symptoms described by the bakers correlated with the basophil test and are shown in table IV. 22 of the bakers com-plained of various symptoms indicating im-mediate type of allergy, and 7 of these had eczema, too. The remaining 3 had eczema alone without other symptoms. In the ques-tionnaire, the bakers had a possibility of giving information as to what allergen they personally suspected. 12 of the bakers sus-pecting wheat flour were positive in the ba-sophil test to this allergen, and one addi-tional subject, who did not suspcct wheat
ographs of the C R I E plates. Radiostaining visible
after 8 days was taken to indicate a high degree,
and staining after more than 8 days was taken IO indicate a low degree of IgE binding. See text for
further explanation.
flour, was, however, found to react positive-ly. Among the 12 bakers who were found to be negative In the basophil test, 6 suspen d wheat flour to be the cause of their symp-toms, and the remaining 6 suggested other agents (or none at all) to be the possible al:
lergen. It can be seen that 3 bakers who had eczema as a single symptom were all nega-tive in the basophil test, RAST, as well as immediate skin reactivity. When the skin reactivity (skin index) and the basophil test were compared (table I I) , no statistically sig-nificant correlation (p>0.05) was found be-tween the two tests. Provided the skin inti is considered positive above 0.25, 2 of we bakers (patients 10 and 22), who were posi-tive In the basophil tent, were negative in the skin test. In all cases, a positive skin in-dex was accompanied by a positive basophil
test. The correlation between the basophil test and RAST was not statistically signifi-cant (p>0.05; table I I) . When a negative RAST is considered below 4 SU, the same bakers (10 and 22) would also be ncpaiiv*
Table IV. Classlftcatlc
if the patients according t
gbcration test and the
patients of wheat flour
(according to the questlor
Allergic disorder
Asthma
Asthma+rblnltls
Asthma+rhinitis+eczenx
Asthma+eczema
Rhinitis
gRJhinltis+eczema
Bczema
Urticaria
Total
The results represent
+ •> Suspected wheat flot
did not include wheat flou
did not suggest any al
from the RAST test, test was positive. In RAST observed with test A significant co: found between the b table D).
Discussion
Immunochemical
The antigenic coir {las been investigated {nunoelectrophoretic fabblt antiserum to ]The analysis has re
tain 40 different owed partial in owever, at this sta
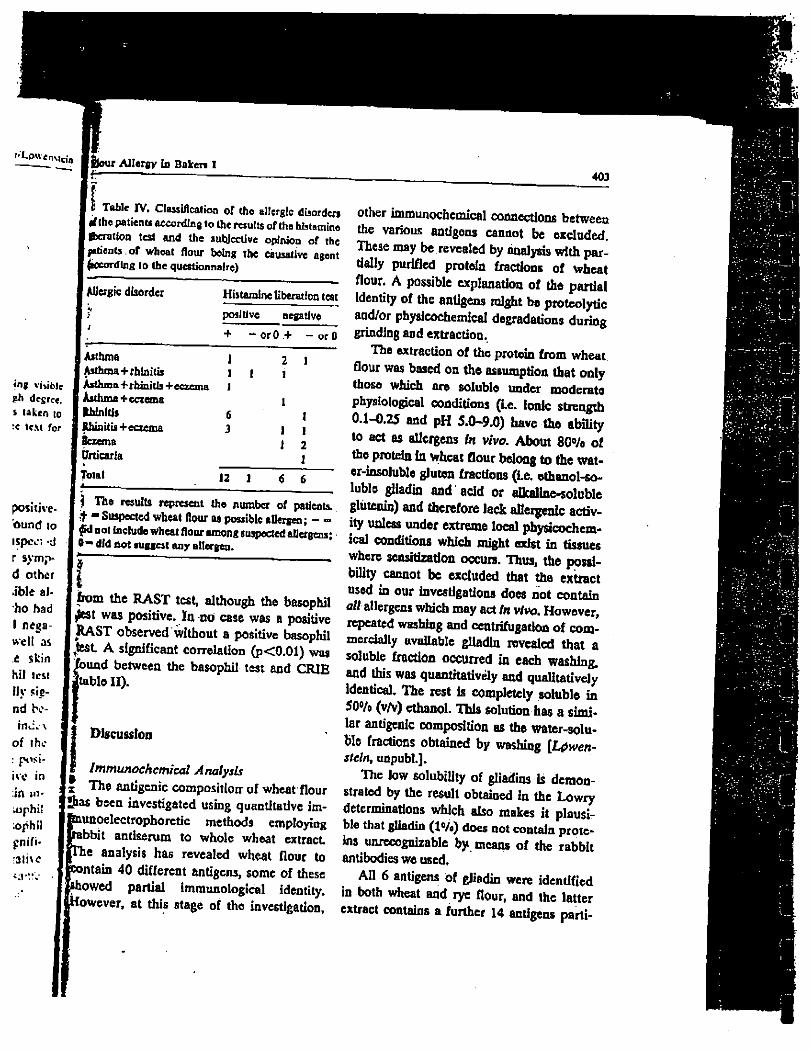
Ifeour Allergy to Baker, 1 — •
403
Table IV. Classification of the allergie disorders i d the patients according to the results ofthe histamine deration test and the subjective opinion of the patients.of wheat flour being the causative agent
| According to the questionnaire)
Allergic disorder Histamine liberation test positive negative + - orO + or 0
•ng visible gh degree. * taken to :< text for
Asthma Asthma+rhinitis Asthma+rhinitis+eczema Asthma+eczema IhlnltJs JUunitis+eczema Bcxema Urticaria Total 12 1 6 6
tnti»-\ of thc : posi-
) The results represent the number of patients. It - Suspected wheat flour as possible allergen; - -^d not include wheat flour among suspected allergens ; O-dld not suggest any allergen. r bom the RAST test, although the basophil £st was positive. In no case was a positive RAST observed without a positive basophil
ftest A significant correlation (p<0.01) was found between the basophil test and CRIE [tablo II).
Discussion
^ Immunochemical Analysis
x The antigenic composition of wheat flour
Sias been investigated using quantitative im-
~ îunoelectrophoretic methods employing
ibbit antiserum to whole wheat extract
ie analysis ha6 revealed wheat flour to
mtain 40 different antigens, some of these
showed partial immunological identity.
Towever, at this stage of the investigation.
other immunochemical connections between
the various antigens cannot be excluded.
These may be revealed by analysis with par-
tially purified protein fractions of wheat
flour. A possible explanation of the partial
identity of the antigens might be proteolytic
and/or physlcochemical degradations during
grinding and extraction.
The extraction of the protein from wheat
flour was based on the assumption that only
those which are soluble under moderate
physiological conditions (i.e. ionic strength
0.1-0.25 and pH 5.0-9.0) have the ability
to act as allergens In vivo. About 80% of
the protein In wheat flour belong to the wat-
er-insoluble gluten fractions (i.e. ethanol-so-
luble gliadin and add or alkaline-soluble
glutenin) and therefore lack allergenic activ-
ity unless under extreme local physicochem-
ical conditions which might exist in tissues
where sensitization occurs. Thus, the possi-
bility cannot be excluded that the extract
used in our investigations does not contain
«// allergens which may act in vivo. However,
repeated washing and centrifugatlon of com-
mercially available gliadin revealed that a
soluble fraction occurred in each washing,
and this was quantitatively and qualitatively
Identical The rest is completely soluble in
50®/o (v/v) ethanol. TTiis solution hag a simi-
lar antigenic composition as the water-solu-
ble fractions obtained by washing [L^wen-
stein, unpubl.].
The low solubility of gliadins is demon-strated by the result obtained in the Lovvry determinations which also makes it plausi-ble that gliadin (W0) does not contain prote-ins unrecognizable by means of the rabbit antibodies we used.
All 6 antigens of gliadin were identified
in both wheat and rye flour, and thc latter
extract contains a further 14 antigens parti-
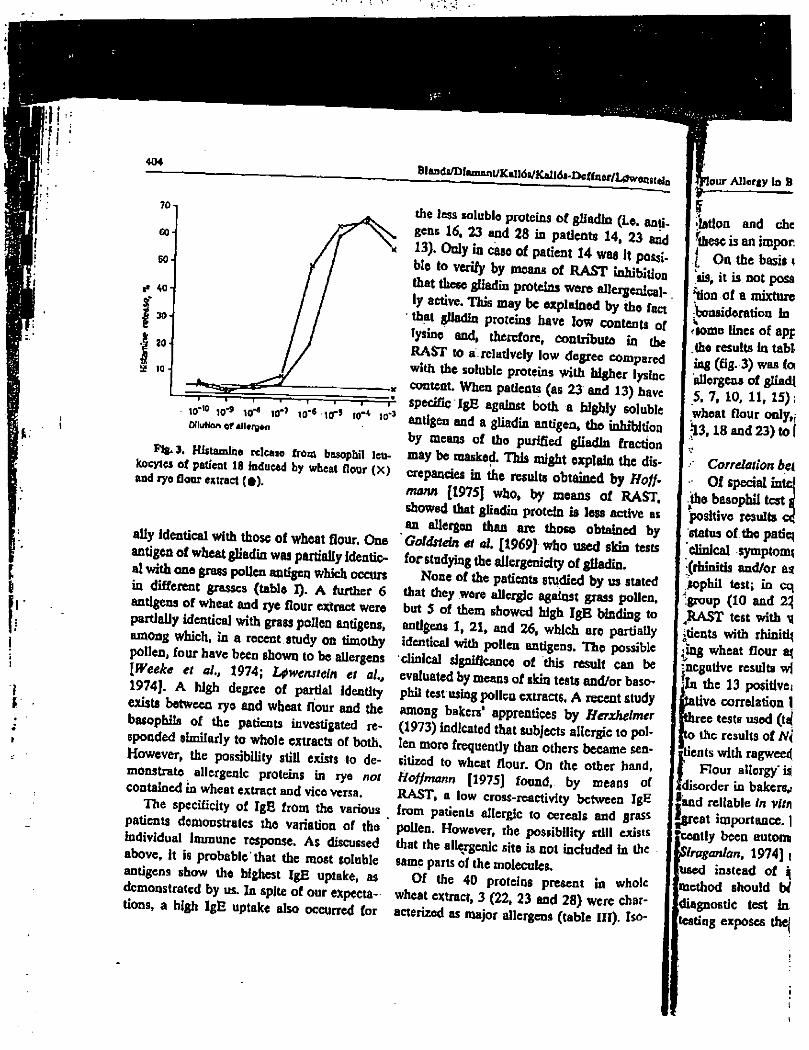
S!M 404
70
GO
60
«• 40-
| 30
l 20 2 10
n » 1 1 , ,
• 10"10 le"
9 M* 10"' Ï0"
5 1(T« tO
_i JO'»
Wluttôn of âlUrgfto
Pig. J. Histamine release from basophil leu-kocytes of patient 18 induced by wheat flour (X) and rye flour extract (*).
ally Identical with those of wheat flour. One
antigen of wheat gliadin was partially identic-
al with one grass pollen antigen which occurs
in different grasses (table I). A further 6
antigens of wheat and rye flour extract were
partially identical with grass pollen antigens,
among which, in a recent study on timothy
pollen, four have been shown to be allergens
[Week* et al, 1974; Lfwensieln et ai,
1974], A high degree of partial Identity
exists between ryo and wheat flour and the
basophils of the patients investigated re-
sponded similarly to whole extracts of both.
However, the possibility still exists to de-
monstrate allergenic proteins in rye not
contained in wheat extract and vico versa.
The specificity of IgE from the various
patients demonstrates tho variation of the *
individual immune response. As discussed
above, it is probable that the most soluble
antigens show the highest IgE uptake, as
demonstrated by us. In spite of our expecta-
tions, a high IgE uptake also occurred for
Blands/Dlammt/Kallds/Kall s-Dcffner/LtSwent u
the less soluble proteins of gliadin (Le. anti-
gens 16, 23 and 28 in patients 14, 23 and
13). Only in case of patient 14 wag it possi-
ble to verify by means of RAST inhibition
that these gliadin proteins wore alleigenlcal-
1y active. This may be explained by tho fact
that glJadln proteins have low contenu of
lysine and, therefore, contribute In the
RAST to a. relatively low degree compared
with the soluble proteins with higher lysine
content. When patients (as 23 and 13) have
specific IgE against both a highly soluble
antigen and a gliadin antigen, tho inhibition
by means of tho purified gliadin fraction
may be masked. TOs might explain the dis-
crepancies in the results obtained by Hoff-
mann [1975] who, by means of RAST.
showed that gliadin protein is less active as
an allergen than are those obtained by
Goldstein et al. [1969] who used skin tests
forstudying the aliergenicity of gliadin.
None of the patients studied by us stated
that they were allergic against grass pollen,
but 5 of them showed high IgB binding to
antigens 1, 21, and 26, which are partially
identical with pollen antigens. The possible
clinical significance of this result can be
evaluated by means of skin tests and/or baso-
phil test using pollen extracts, A recent study
among bakers' apprentices by Herxhelmer
(1973) indicated that subjects allergic to pol-
len more frequently than others became sen-
sitized to wheat flour. On the other hand,
Hoffmann [1975] found, by means of
RAST, a low cross-reactivity between IgE
from patients allergic to cereals and grass
pollen. However, the possibility still exists
that the allergenic site is not included in the
same parts of the molecules.
Of the 40 proteins present in whole
wheat extract, 3 (22, 23 and 28) were char-
acterized as major allergens (table III). Iso-
tour Allergy In B
•lation and che
'these is an impor
I On the basis <
"lis, it is not posa
[ lion of a mixture
iVonsideration In
<tomo lines of apj
.the results In tabl-
ing (fig. 3) was foi
alleigeas of gliadj
5. 7, 10, 11, 15);
wheat flour only,;
;13,18 and 23) to I
Correlation bei
Of special inte
iho basophil test \
positive results oc
status of tho patiq
clinical symptom*
(rhinitis and/or as
jkophil test; in cq
group (10 and 2%
4RAST test with \(
itients with rhiniti^
;îng wheat flour aj
^negative results wi
jln the 13 positive]
Jtative correlation 1
fthree tests used (tcj
fto the results of N(
gtients with ragweed
Flour allergy' is!
«disorder in bakers,!
land reliable In vitr\
•great importance. 1
cently been eutonn
Siraganlan, 1974] i
used instead of q
method should tW
diagnostic test in
testing exposes the|
i i »
Flow Allergy la Bakers I 2411
lation and chemical characterization of
these is an important future aim.
; On the basis of thc present CRIE analy-
sis, it is not possiblo to define the composi-
tion of a mixture of allergens prcferablo for
bonsideratxon in immunotherapy. However,
-iome lines of approach can be derived from
the results in table i n . Thus, high IgE-bind-
Ing (fig. 3) was found (a) in 1 patient (14) to
allergens of gliadin only; (b) in 6 patients (1,
5, 7, 10, 11, 15) to the soluble allergens of
wheat flour only, and (c) in 4 patients (12,
13,18 and 23) to both fractions.
Correlation between Diagnostic Tests
I Of special interest is the observation that
the basophil test gave the highest number of
positive results correlating with the clinical
ttotus of the patients. Thus, 13 patients with
clinical symptoms of wheat flour allergy
(rhinitis and/or asthma) gave a positive ba-
sophil test; in contrast, 2 patients of this
group (10 and 22) gave negative skin and
,RAST test with wheat flour extract 5 pa-
rents with rhinitis and/or asthma, suspect-
Jug wheat flour as allergen, gave, however,
negative results with all three test methods.
In the 13 positive cases, there is no quanti-
tative correlation between the results of the
jthrcc tests used (table II). This Is in contrast
rto the results of Norman et ai [1973] in pa-
rents with ragweed hay fever.
£ Flour allergy is a common occupational
^disorder in bakers, and therefore, a sensitive
tand reliable in vitro diagnostic method is of
"great importance. The basophil test has re-
Icently been automatized [Ruff et al.t 1967;
Itoraganian, 1974] and whole blood can be
jused instead of isolated leukocytes. This
[method should be explored as a routine
[diagnostic test in allege subjects. Skin
testing exposes the patient to some discom-
fort and risks and an in vitro substitute is highly desirable.
Acknowledgements
W d t e r a 0 d L«
M r t Hewelman
Foundation for Scientific Research (Stockholm)
and Robert Koch Foundation (Bonn) » gratefully
aclmowledged. W e are indebted to M n . Kirs ten
Eobestn, M n . Eva Haardtng-Larsen and M r s
iben Hfort for expert technical assistance.
References
Aas, K , and Belin, L.; Standardisation of dlagnos-Z " °
T k « « « W . Acta aUcrg, 27: 43<M69
(1972).
Axelsen, N . M.; Krtfli, J , and Weeke, B.: A man-
ual of quantitative Immunoelectrophoresis.
Method* and applications. Scand. I. Immunol.
2: suppL 1(1973).
Baag0e, K . H.: Mcltiidiosynkrasie als Ursache von
vasomotoria cher Rhinitis und Asthma. Klin
Wschr. 293$ 1:792.
Bazaral, M . O . and Hamburger, R . N J Standard!.
zaUon and stability of immunoglobulin E (IgE).
J. Allergy din. Immunol. 49: 18ÎM91 (1972).
B esche, A . de: Serologische Untersuchungen Ober
aUergiicbe Krankfaeiten. Acta path, microblol
«cand. 6:115 (1929).
Bjernun, O . J.; Ramlau, d e m m e s e n , L; IngUd,
A., and Btfg-Hanscn, T . C.i A n artefact In
quantitative Immunoelectrophoresis of spectra
caused by proteolytic activity in antibody prep-
arations. Scand. J. Immunol. 4: suppl 2
PP. 81-48 (1975). * '
Bonnevie, P.: Occupational allergy m bakery; in
Stenfert-Kroese Occupational allergy, p 161
(Leiden 1958).
Btfyum, A ; Separation of leucocytes from blood
and bone marrow. Scand. J. clin. Lab. Invest.
2i: suppl 97 (1968).
Caatberg. T . and Sprenscn, C . M.i Allergic exami-nation of bakers and millers. Acta allers, i-283(1948). '
406
Ccska, M.; Ericson, R , and Varga, J. M.: Ra-
dioimmunosorbent assay of allergens. J, Aller-
gy clin. Immunol. 49:1-9 (1972).
Day, R . p.: Basophil leucocyte separation from
h u m a n peripheral blood: a tochnlquo for their
isolation in hlgh-purlty and high yield. Clin.
Allergy 2:205-212 (1972).
Dlcdrichs. W . und LUbbers, P.: Das Mehlasthma
als Berufskrankheit. Zentbl. ArbMed. Arb-
Schutl 5: 189 (1955). -
Dlshoeck, H . A . E . van and Roux, D . J.: Sensiti-
zation to flour. J. H y g . 39; 674 (1939).
Gadborg, E.: O m molallergi (Thesis In Danish).
Christrcus, Copenhagen 1956 (oxtensively re-
viewed by Bonnevie).
Goldstein, E. D.; Helner, D . C., and Rose, B.:
Studies of reagents to alfa-gliadin via paUent
with wheat hypersensitivity. J. Allergy 44*
37-50 (1969).
Harboe, N . H . G . and IngUd, A.: Immunization,
isolation of Immunoglobulins, estimation of
antibody titre, Scand. J. Immunol. 2: snppl 1,
pp. 161-164 (1973).
Herxhelmer, H.: T h e skin sensitivity to flour of
bailors* apprentices. A final report of a long-
term investigation. Acte allerg. 28: 42-49
(1973).
Hoffmann, D . R.: T h e specificities of human IgE
antibodies combining with cereal grain. Immu-
nochemistry 12: 535-538 (1975). Kallôs, P. and KalWs-Deffner, L : Flour allergy in
bakers. 75th Congr. Trade Union of Swedish
Food Workers, Stockholm 1971, p. 182.
Lowry, O . H.; Roscbrough, N . J.; Far!. A . L , and
Randall, R . J.: Protein measurement with the
fotin phenol reagent. J. bio!. C h e m . 193:
265-275 (1951).
L0wensteln, H.; Markusen, B., and Weeke, B.:
Identification of allergens In extract of b o n e
hair and dandruff by moans of crossed ra-
dioimmunoelectrophoresis. Int. Archs Allergy
ftppl. I m m u n . 51: 38-47 (1976).
Lpwenstcin, H.; Niolsen, L., and Weeke, B.: Frac-
tionation of allergen extracts using timothy
(PhUum pretense) pollen extracts as a model.
Acta allerg. 29:418-432 (1974);
Biands/Diaroant/KaU6s/KalMs-Dcffner/L0wemtein
Lpwenstcin, H . and Weeke, B ^ Purification of hu-
m a n IgE and rabbit antlhuman IgE. Scand. J.
Immunol. 4: suppl, 3, pp. 459-466 (1975).
Marsh, D . O.: Allergens and the genetics of aller-
gy; Antigens $; 271 (1975).
Nielsen, L ; L^wensteln, H., and Wecko, B.: Quan-
titative Immunoelectrophoresis used in analysis
of the antigen in timothy pollen extract. Acta
allerg. 29:385-401 (1974).
Norman, P. S.; Liechtenstein, L . M., end Ishizaka,
K.: Diagnostic teats In ragweed hay fevêr. I.
Allergy din. Immunol. 32: 210-224 (1973).
Pestalorzi, C . und Schnyder, U . W.: Zur Frage
der Backerrhinitis und des BSckerasthmas.
Schwelz. m e d . Wschr. 1933 /; 498,
Rowe, D . S.: Measurements of concentrations of
h u m a n serum immunoglobulins. Clin. exp. Im-
m u n o l 9: 695-697 (1971).
Ruff, F.; Saindelle, A.; Dutripon, E., and Parrot,
J.-L.: Continuous automatic fluorometric eval-
uation of total blood histamine. Nature, Lond.
214:279-281 (1967).
Schwaru, M ^ Horldity in bronchial asthma; thesis
(Munksgaand, Copenhagen 1952).
Siraganlan, R . P.: A n automated continuous-flow
system for the extraction and fluorometric
analysis of histamine. Analyt. Biocfiera. 57:
383-394 (1974).
Urbach, E . and Gottlieb, P. M ^ Allergy; 2nd ed.,
p. 183 (Gruno St, Stratton, N e w York 1946).
Weeke, B.: Crossed Immunoelectrophoresis,
Scand. J. I m m u n o l 2: suppl. 1; pp. 47-56
(1973).
Weeke, B. and Ltfwenstein, H.: Allergens identi-fied In crossed radioimmunoclèctrophoresis. Scand. J. Immunol. 2: suppl. 1. pp. 149-15.1 (1973).
Weeke. B.; L0wcnstein, H., and Nielsen. L.: Aller-
gens In timothy pollen identified by crossed-ra-
dio-immunoelectrophorcsis (CRIE). Acta al-
lerg. 29:402-417 (1974).
Correspondence to; Dr. Bertil Diamant, Depart-
ment of Pharmacology, 20, Juliane Maries Vcj,
DK-2100 Copenhagen 0 (Denmark)
Short Communie
Int Archs Allergy appL Im
Anaphylactoid Re
Dt Harper and <?. B. We,
Department of Applied Biolc
Abstract When the bloi anaphylactoid reaction in q:
action in the other hindpawi raised after alloxan pretreati reaction is inhibited. The rej effects by involving different
Most rats respond to iij traperitoneal injections of (molecular weight 44,000-1 anaphylactoid reaction co oedema of the extremity pruritus. These have beeni tor or R rats. A few do not
|breeding Harris et al. [196^ «ure to an inherited auta "gene, and a pure line of t clinical dextran has been a
fftre termed non-reactor or ?NR rats are relatively mora 5 shock, tourniquet shock, I shock [Ankier et al.. 1967), ftamine and 5-hydroxytry( only with difficulty when d bjccted.
Freeman and West [1Î
Roceived: February 12, 1976.
•finical Allers 1 9 8 4 . V o l u m e 1 4 . p a g e s 1 7 7 - 1 8 5
Baker 's asthma
S t u d i e s o f t h e c r o s s - a n t i g e n i c i t y b e t w e e n
i i i V e r e n t c e r c a l g r a i n s
G . B L O C K * . K . S . T S E , K . K I J E K . . H . C H A N and M . C H A N - Y E U N G
U n i v e r s i t y of British Columbia. Vancouver. Canada
, Rrccireti 2> October 1982: accepted for publication 19 February 1983,
n ° U r S ^ o m e ' o f t h e b a k e r s Ï u Î n T h e R A S T i n h i b i t i o n t e s t s , c r o s s - a n t i g e n i c t y w a s n e e m s o m e o f t h e b a k e r s . ^ o f c r o s s . r e a c l l v l l y c l o s e l y
s h o w n t o e x i s t b e t w e e n d i f f e r e n t c e r e a l r a i n s ^ I f o l i o w j n e o r d e r o f
p a r a l l e l e d t h e i r , a x o n o m , c r e a n o n s h , p a n d a p p e a r e d • o b t j c
S » — - I . d i s t r i b u t e d a m o n g v a r i o u s
f r a c t i o n s o f d i f f e r e n t m o l e c u l a r w e i g h t s .
, h a l b ; ' k C r " S " . B l o c k r ; 9 A l h w h e a l a n d r y e a r e t h e m o r e c o m m o n c e r e a l a n u g e n s ( B l o c k < / • . 9 8 3 ) . . A ^ e x p o s u r e t o f l o u r s I r o m
flours t h a t t h e y w o r k s i g n i f i c a n c e . t h e r e f o r e , t o d e , e r m i n e
' he d e g r e e o f c r o s s - r e a c t i v i t y b e t w e e n i n d i v i d u a l c e r e a l g r a n t s .
M a t e r i a l s and Me thods
S i ' r a , i - . . v „ , I m i I ; C ( J s e v e n s y m p t o m a t i c b a k e r s i n d e t a i l a n d h a v e
between the level o f se rum I g E
• Or „ „ * , « « the rccipicm of .be B r i u * Colun.bia Chrisu»» Seal, F««o«hip.
Corrirsptiiulcnce: Dr Moin, Chan-Y tu„S . . IS-2775 H«*hcr S u e , . Vuncou. r . B.C.. Canada ^
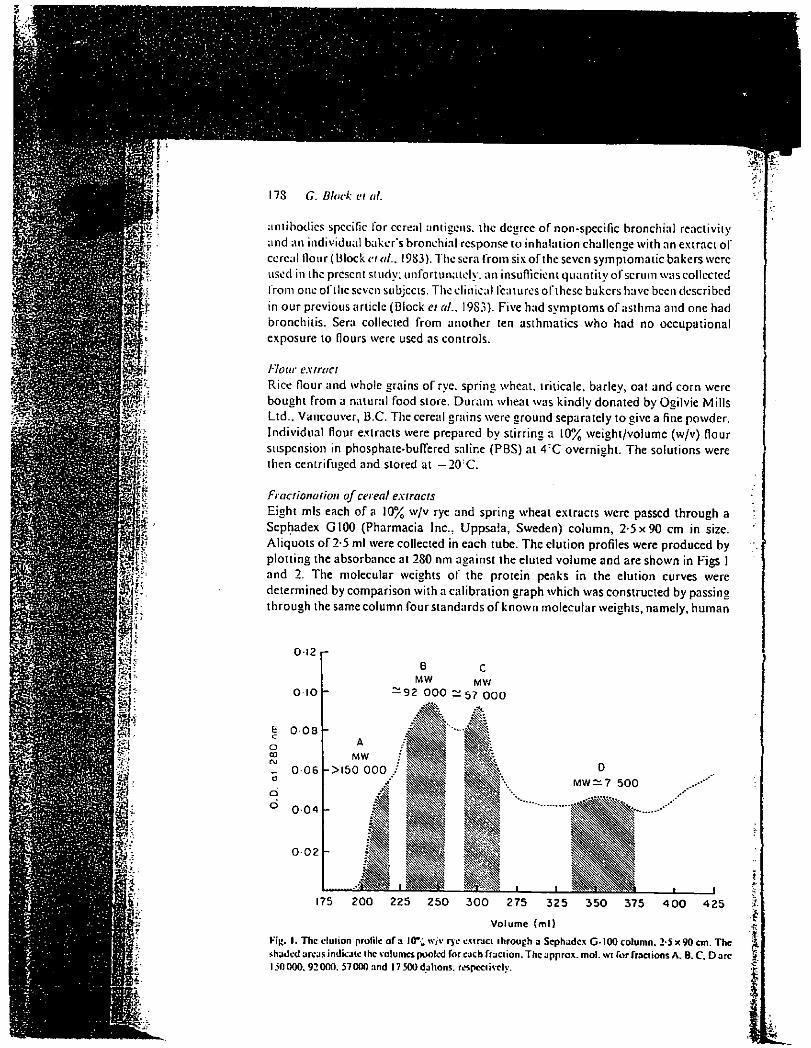
17S G Block cl til.
ÉS' Ki:
antibodies specific for cereal antigens, the degree of non-specific bronchial reactivity
and an individual baker's bronchial response to inhalation challenge with an extract of
cereal Hour ( Block et «/.. 1983). The sera from six of the seven symptomatic bakers were
used in the present study; unfortunately, an insufficient quantity of scrum was collected
from one of the seven subjects. The clinical features of these bakers have been described
in our previous article (Block et al., I9S3). Five had symptoms of asthma and one had
bronchitis. Sera collected from another ten asthmatics who had no occupational
exposure to flours were used as controls.
Flour extract Rice flour and whole grains of rye. spring wheat, triticale. barley, oat and corn were
bought from a natural food store. Du ram wheat was kindly donated by Ogilvie Mills
Ltd.. Vancouver, B.C. The cereal grains were ground separately to give a fine powder.
Individual flour extracts were prepared by stirring a 10% weight/volume (w/v) flour
suspension in phosphate-buffered saline (PBS) at 4 : C overnight. The solutions were
then centrifuged and stored at — 20:C.
Fractionation of cereal extracts Eight mis each of a 10% w/v rye and spring wheat extracts were passed through a
Sephadex G100 (Pharmacia Inc., Uppsala, Sweden) column, 2-5x90 cm in size.
Aliquots of 2-5 ml were collected in each tube. The elution profiles were produced by
plotting the absorbance at 280 nm against the eluted volume and are shown in Figs 1
and 2. The molecular weights of the protein peaks in the elution curves were
determined by comparison with a calibration graph which was constructed by passing
through the same column four standards of known molecular weights, namely, human
OI2
3 0 0 275 3 2 5
Volume (ml )
3 5 0 375 4 0 0 4 2 5
Kij». 1. The cluiion profile of a 10"; w/v rye cxtraci through u Sephadex G-100 column. 2-5 x 90 cm. The shaded Jreus indicate the volumes pooled for each fraction. The appro*, mol. wt Tor fractions A. B. C. D arc 150000.92000. 57000 and 17 500 dallons. respectively.
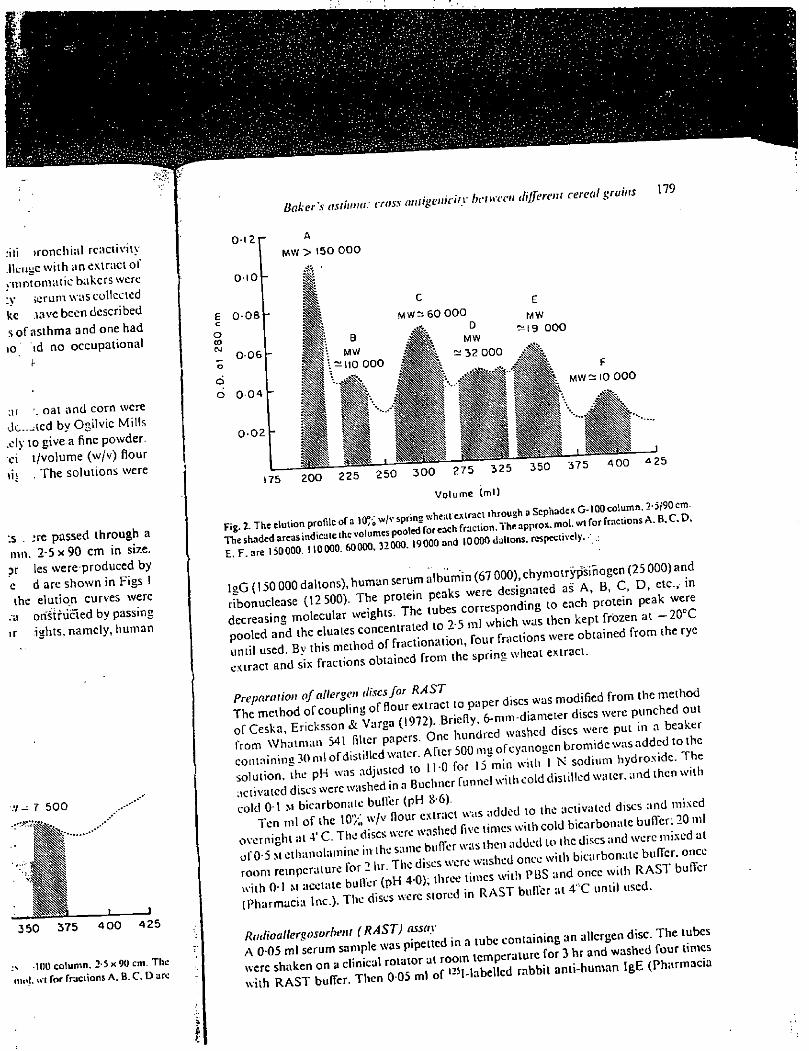
:iti >ronchiul rcactiviiy .Heuuewiih an extract of . mmomatic bakers were •y icrum wascollccied ke ,iave been described s of asthma and one had 10 »d no occupational
ar oat and corn were
Uc.-^ied by OgiWic Mills
.cly to give a fine powder,
ci t/volume (w/v) flour
m . The solutions were
:s .. -*re passed through a
mn. 2-5x90 cm in size,
pr les w e r e produced by
c d are shown in Figs I
the elulion curves were
.-a on^triicted by passing
ir ights, namely, human
3 5 0 3 7 5 4 0 0 4 2 5
100 column. 2-5 x 90 cm. Thc m«l. wi for frac i ion s A. B. C. D arc
0l2r
0-10
£ 0 -08 c
O 00
Z 0-06 o
o
o 0 0 4
0 - 0 2
Baker's asthma.
M W > 1 5 0 0 0 0
<r,*s aniigeniciiy br„rcn différent cereal grains 179
MW ^19 000
175 2 0 0 2 2 5 2 5 0 3 0 0 2 7 5 3 2 5
Volume (ml )
350
Fig. 2- The elution profile of a
lgG ( 150 000 dallons), human serum ^ j e s ^ ' ^ a ^ ^ ' a ^ ^ " B ^ C . ^ D ^ e^c.^in
ribonuclease (12500). The protein P ^ o Z p Z U to each protein peak were
decreasing molecular weights. Th tubes c o r s p o B ^ ^ k ^ a i _ 2 0 X
L - r ^ t ^ ^ r r r i ^ f o n / l r rracnons «re obtained from the rye obtained from the spring wheat extract.
preparation of allergen dises for RAST fied frQm (he me(hod
The'method ofcouplmgof flour exa e t d , s c s w e r c p l i n c hed out orCeska, Ericksson & Varga (1.)72).Bnelly o w c r e u l i n a beaker ,-rom Whatman 541 fiUcr papers. One ° ; „Q,,cn b r o m i d c was added .o the containing 30 ml of dialed water Af cr 500 ^ N ^ ^ ) i y d r 0 N i d c. The
1
cold 01 M bicarbonate bufler (pH 8-6). activated discs and mixed
Ten ml of the 10% w/v flour ex ac b i < a r b 0„ a.e bufler; 20 ml
overnight a, 4" C. The discs were wa 1 ed fi m c ^ ^ ^ ^ m l x c d a l
o,-0-5 M ethanolaniine ,n the s ' « e b t ^ r w^*.hen. b i c i i r b o n : l l c bu fTer. once
room remperature for 2 and once wi.h RAST buffer î p r a c ; r ; e Ï S ^ r d i n R A S T b u f l , r a t 4 X .used.
S S Ï S Ï i - 2 3 £
130 G. Block Cl ai
I M
m
,§3 M Si? m
f ! :
-i ç'i
I
Inc.) was added to each tube and the tubes were again shaken on the rotator at room
temperature overnight. The tubes were washed four times with RAST buffer and the
radioactivity was measured by a gamma counter. The uptake of radioactivity of the
a lergend.scs was expressed as the RAST value which wasthe ratio of the radioactivity
ol the baker s scrum sample to that of normal control.
Radioallergosorhent (RAST) inhibition tests
The antigen specificity of the scrum RAST activity was determined by the dearee of
inhibition of serum RAST values by prior absorption of the serum sample witlTa flour
extract. Ahquots of a serum sample in 015 ml were mixed with different amounts of a
1 H o u r extract and left at room temperature for 3 hr. Then 005 ml of the sample was
used for the RASTassay, using an allergen disc containing the same cereal antigen The
results were expressed as:
% inhibition = (B)-(A)
(B) x 100%,
where (B) represents the serum RAST value before incubation with flour extracts and
(A) represents the serum RAST value after incubation with flour extracts. Similarly
the antigenicity of the four fractions of the rye flour extract and the six fractions of the
wheat flour extract obtained by fractionation through a Sephadex G-100 column was
also measured by the ability of each fraction to inhibit the RAST value of a given serum sample.
The degree of cross-reactivity between differential cereal flours was also determined
by the RAST inhibition test. In this case, 015 ml of the serum sample was
pre-mcubated with 0 05 ml of the cereal extract to be tested and then the RAST assay
was carried out using rye or wheat allergen discs.
Results
Serum RAST values against different cereal flours
These resultsareshown in Table I. Incomparison with the ten asthmaliccontrols who
had no occupational exposure to flours, each of the six symptomatic bakers was found
to have elevated serum RAST values for several of the cereal flours. As reported in our
earlier article (Block « „/., 1983). four of six symptomatic bakers (bakers 1-4) had
positive reactions while the remaining two had negative reactions to antigenic
bronchoprovocation with rye or wheal flour extracts. The sera from bakers 1-4 were
lound to have considerably higher RAST values than the sera from bakers 5 and 6
These subjects not only had elevated serum RAST values for several 0 r the
taxonomically closely related cereals such as rye. wheat, durum wheat and triticale Oi
hybrid specics between rye and wheat), but several of them also had very hi»h values
lor barley (bakers 3.4). corn (bakers 3,4). oat (baker 3) and rice (baker 4) The latter
lour cereal grams have a much more distant taxonomic relationship with rye and
wheat. The taxonomic chart of different cereal grains has been published previously by
Haldo. Krilis & Wriglcy (1980). '
Antigenic specificity of the serum RAST activity
The results of the RAST inhibition tests arc shown in Fig. 3. Addition of increasing
amounts of a particular flour extract to a scrum sample from a baker prior to the RAST
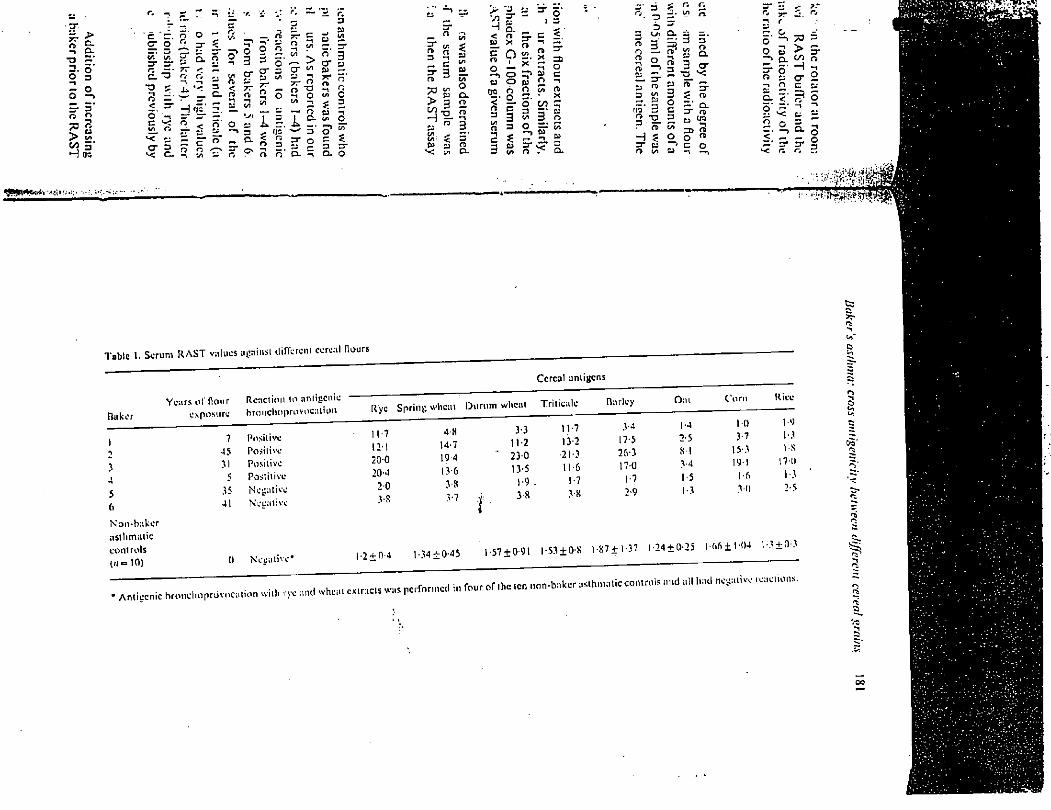
•CP-
s-i - i Q. •3 ~ 5" g -n - O O -> H ' > fe
H oc
- - . j •t. V. •j J*', i-IT O
5' n" rv o 3" ?
& v> •V
n r» 7T fS -n V) to
3 ? O o o -1 -n V)
a 1/5 5. O ? 3 3 2 > cr • ?r M CT o* a
1 to o r i ,, c/1 CT £3 i/i to ?r ? Xh 3 < r 7T 7T
O o 73 ro . c . n n> o -1 o t/>
y H •i i CI VI tst
n ? to </> o < o' O
'_/»
I X T a ? to </>
< u 5 fie' 5 ' a and o -1 n irt cT
?C o. 9s
< n ^ n
Q 3 O
r r a .
o c r" 5 o.
ti —t
3 to </>
3 5* n> 3
S (A o
</) ? to
to c c/i — . 3 to o o o * to o CL 3 > 3 fï o
00 H nT —1
c/> to n> §. $ c/v t/i s 5* 3* to to o O a.
'J y j y -15 » ^ Q-
s 9 2,5 to
g* 5 n « a. x * =: r» »
o c/i rc x oo = ' to 3 o ST " ? 5; »
=r C< = rs . Q-
3 o O 3
3 rt 3 o o «i o a> to 3* to 3 en to no' 3 o 3 • H £ 3* to n> t/i
^ r. r.
I 3 3" s.
S 3 cr to rt C. 3 s ? O = =T o S « c« o o «
o
3" J. r. 7T o r O
c — » 73 3 O to > 5" —^ CL 00 a
o o' H c O o to
Q. < " o o' o O
-1 to
™ > o < ft 3* a r. 3
''jWH1^'»"!''''-':
• ' *''I . ' ••A-NMJjt
Cereal aniigens
Baker Years ol' Hour
exposure Reaction lo antigenic bronchnprovocaium Rye Spring wheat Durum wheal Tritieale Barley Oat Corn Rice
1 ^
5 4 5 6
7 45 31 5
41
Positive Positive Positive Posliiive Negative Negative
11-7 12-1 200 20-4 20 3-R
4-S 14-7 19-4 13-6 3-8 3-7
3-3 11-2
* 230 13-5 1-9 .
J 38 Ï
11-7 13-2 21-3 11-6 1-7 3-S
3-4 17-5 26-3 17-0 1-7 2-9
1-4 2-5 SI 3-4 1-5 1-3
1-0 3-7 15-3 iyi
3-D
!•') 1-3 IS 170 1-3 2-5
Non-baker asthmatic controls (/» =10) 0 Negative* 1-2 + 0-4 1-34 ±0-45 1-57 ±091 1-53 ± OS 1-87+1-37 1 -24 + 0-25 106 ± 104 1-3+0-3
• Anliecnic bronelmprdvncn nion willi rye ami wheat extracts was performed in four of the ten non-baker a: slhnuitic controls and all had negative reactions.
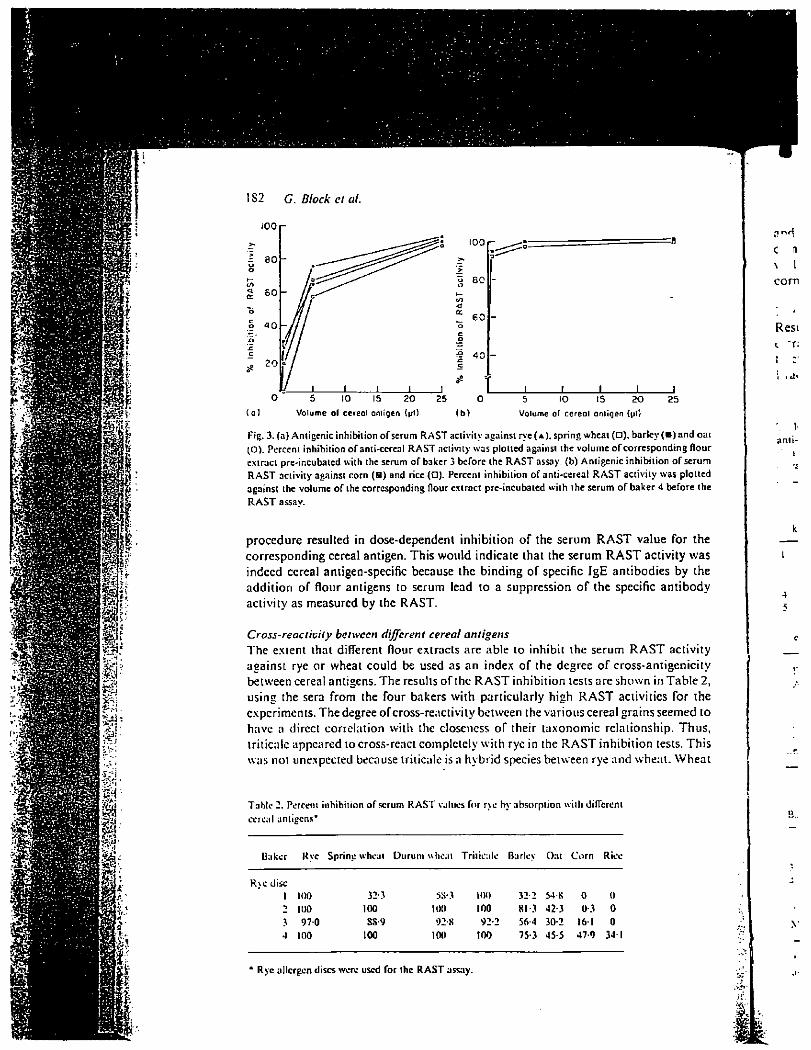
i t m
P I f
§ i •*->
i i feiî
m 1 ir'
•J . s
1 Si! Wl
lïi
*
i ii U'
fiVt
IS2 G. Block ci ai
100 r
100
80
60
40
5 10 IS 20 Volume of ce rea l antigen (pi) ( b )
5 10 15 20 Volume of ce rea l ant igen (pi)
25
Fig. 3. (a) Antigenic inhibition of serum RAST activity against rye( A), spring wheat (O). barley ( • ) and oat (O). Percent inhibition of anti-cereal RAST activity was plotted against the volume of corresponding flour extract pre-incubated with the serum of baker 3 before the RAST assay, (b) Antigenic inhibition of serum RAST activity against corn (H) and rice ( • ) . Percent inhibition of anti-cereal RAST activity was plotted against the volume ofthe corresponding flour extract pre-incubated with the serum of baker 4 before the RAST assav.
procedure resulted in dose-dependent inhibition of the serum RAST value for the
corresponding cereal antigen. This would indicate that the serum RAST activity was
indeed cereal antigen-specific because thc binding of specific IgE antibodies by the
addition of flour antigens to serum lead to a suppression of the specific antibody
activity as measured by the RAST.
Cross-reactivity between different cereal antigens The extent that different flour extracts are able to inhibit the serum RAST activity
against rye or wheat could be used as an index of the degree of cross-antigenicity
between cereal antigens. The results of the RAST inhibition tests are shown in Table 2,
using the sera from the four bakers with particularly high RAST activities for the
experiments. The degree ofcross-reactivity between the various cereal grains seemed to
have a direct correlation with thc closencss of their taxonomic relationship. Thus,
triticalc appeared to cross-react completely with rye in the RAST inhibition tests. This
was not unexpected because triticalc is a hybrid species between rye and wheat. Wheat
Table 2. Percent inhibition of scrum RAST values for rye by absorption with different ccrcal anliecns*
Baker Rye Spring wheat Durum wheat Triticalc Barley Oat Corn Rice
R\c disc 1 KM) 32-3 5S-3 too 32-2 54-K 0 0 •» 100 100 too 100 81-3 42 3 03 0 3 970 SS-9 92 K 92 2 56-4 30-2 16 1 0 4 100 100 100 100 75-3 45-5 47-9 34 1
C (1
\ 1 com
Resi
anti-i
* Rye allergen discs wore used for thc RAST assay.
' i . •à;'
«a
m y." -
15 20
in (pt)
25
:cu« v û ) . bar ley ( B ) and ou i une o f c o r r e s p o n d i n g f lour t i j c i n h i b i t i o n o f serum
' ac t i v i t y was p lo t ted :ru... o f bake r 4 before the
R. .ST value for the n R A S T activity was ï l ntibodies by the h ;pecific antibody
iiuui R A S T activity of cross-antigenicity ir hown in Table 2, S activities for the real grains seemed to
uionship. Thus, ii bition tests. This .e and wheat. Wheat
1
Baker's asthma: cross antigenicity between different cereal grains 183
.ind barlev were also found to have a high degree of cross-reactivity with rye as compared with oat, com and rice in the RAST inhibition tests. Again, this finding fits well with the fact that wheat and barley are more close to rye taxonomicallv than oat, corn and rice.
The antigenicity of various fractions of rye and wheat extracts Results of the RAST inhibition tests using the various fractions of rye and wheat extracts are shown in Tables 3 and 4 and indicate that the lower molecular-weight fractions are relatively more antigenic than the higher molecular weight fractions, -raclions C and D of the rye extract (approx. mol. wt 57 000 and 17 500 dallons.
' f ab le 3. Percent i nh i b i t i on o f serum
an t i - r ye R A S T values by p r i o r absorp-
t i o n w i t h d i f fe ren t f rac t ions o f a rye
ex t rac t *
Frac t ions
• Rye a l lergen discs were used for the
R A S T assay.
Tab le 4. Percent i nh i b i t i on o f serum ant i -wheat R A S T
values by p r i o r abso rp t i on w i t h d i f ferent f ract ions o f a
wheat ex t rac t *
Fract ions
Baker A B C D F. F
I i.s-s 23-4 % » 5S-I 4S-4 250
0 0 2I-: 32-9 4S4 32-4 » : . v i 406 41II 27-1 20 1 71
J 3-S" 79 16 5 33-3 54-3 6.V6
5 37-6 37-4 50-1 42-S S40 5.V7 6 52 6 3S9 78-6 K2-X 70S 51-5
Mean 230 24-7 43-3 46-2 54-3 3S-9
• Sp r ing wheat al lergen discs were used for the R A S T
assays.
Baker A B C D ?
1 23-4 62-5 72-9 88-5 - f 2 6-3 15 0 15-7 80-3
3 16 2 21 4 75-1 19-7
4 4-1 0 15-4 79-3
5 12-7 2S-2 73-3 82-4
6 23-6 48-7 68-6 86-7
Mean 15-2 29-3 53-5 72-8
I m || p|
I l
184 G. Block et al.
IP
#
•C: i
m
i .1'
Ï
T '
it
Qnnn r y ) f r a C l ' ° n S ° a " d E ° f , h e w h e a t c * , r a « & P P ™ - w. 32000 and 19000 dallons, respectively) induced a higher degree or R A S T inhibition than other tract,ons. It was evident, however, that the major antigenic component of the rye and
^ n h ! r , r r l m n U l d , n 0 1 * i S ° l a , C d b y r r : , c l i ° n a l i ° " molecular sieving using a Sephad,x G-100 column because the results of the R A S T inhibition tests clearly >howed that the antigenic activity was identifiable throughout the various fractions of the flour extracts.
Discussion
The results of this study have clearly demonstrated the presence of cross-react,vitv between different cereal flours. The degree of cross-antigenicity between different cereal grams as determined by the R A S T inhibition assay closely parallels their taxonomic relationship. The order oHaxonomic relationship in decreasing closeness is as follows: wheat, tnticale, rye, barley, oat, rice, corn (Baldo, Krilis & Wrigley 1980) Closely related species such as wheat, rye and tnticale were found to have a very high degree of cross-antigenicity. Even comparing more distantly related species such as rye, barley and oat, the degree of cross-reactivity between them was still remarkable Our results are in agreement with those of other investigators who also reported the
WrLTev6 . t r S S ~ r e M C t iT b e t W e e " ^ W h e a l ' b a H e y a n d 0 a t ( B a l d ° . Krilis &
m , h i ? n ^ T ™ * " C O r " 3 n d r i C C < H o f f m a " . '975). By employing the method of two-dimensional cross-immunoelectrophoresis between an extract of wheat or rye flour and the corresponding anti-serum raised in rabbits, Blands et al (1976) were able to ,dent,fy about forty antigenic components (as distinguished by different bands of .mmunoprecipitates) in the wheat extract and some of the components were partially .demical to that in the rye extract. The existence of cross-reactivity between different cereal flours has important clinical implications. It would mean that bakers once they are sensmzed from occupational exposures, are likely to develop allergies to multiple cereal grains. The present study has indeed confirmed this point. We found that symptomatic bakers commonly developed specific IgE antibodies to a wide ran-e of cereal grains (see Table I). For sensitized bakers to avoid further o c c u p a t i o n a l
: r , dh : e T r a l r y , S y r n P l 0 T ' , h e y W O U l d h a v e 1 0 in «he bakery
Jô?,M K ^ C h a n g , n g , h C , r W O r k e x P ° s u r e f r o m o n e 'ype o f nour to another wou ld be an ineffective way to manage the problem
The allergenic activity of rye and wheat does no. appear l 0 be confined to a simile component but rather it is distributed among various fractions ofdilTeren. molecular weights of the rye and wheat flour extracts (see Tables 3 and 4). In general, the low n olecular-weight r a d o n s seem to be more allergenic, wi.h respect to .heir rcactivitv
rennried ' 7 ® i ' Z ' ^ a " C r s i c b : , k e r S - ° " , C r " ^ s . i g a . o r s have also epor ted similar results W h e n the water-soluble pro.eins of wheat were fractionated
m to albumin and globulin fractions by sal. precipi.a.ion, bo.h fractions were reactive ,'h t h c
fs p c a f i c ® antibodies from subjects wi.h baker's asthma al.hough .he
Ibumm fracnon was found .o have a higher degree of rcacivi.y (Baldo & Wrigley. S m" ; . ' r l y - ' ^ / ' " " S o n i c i . y of rice was also found to be distributed ; „
various fractions of rice proteins (Shibasaki el at., 1979).
References
BALDO. B.A. & W K I ( W Y C .w . (1978, IgE anybodies to wheat Hour components. C / , W 8, .09. BALDO B . A . . KRILIS S. & WR.CLEY C . W . (1980) Hype rsens i t i v i t y l o i nha led
flour ant igens. Allergy, 35 , 45.
£ .Ti.
:p mol. w i 32000 and A inhibition than other ; component of thc rye and :h — olecular sieving using a S" nhibition tests clearly oui the various fractions of
Baker'* as.luna: cross an,iSenicin- be^een ^eren, eerea, grains 185
-, „ KMUKP KALLOS-Orri-'NEK. L.& Lowi:ssTi:is. H. ( 1976)Flour allergy in bakers.
" -vr't c Z " ' v ^ 5M <••«»*"
anj
III<K'K G TW.. K.S.. KIJUK. K.. CHAN. H. A. \-»»A. ' immuno log ic R i B l i o , n m . » n o » r h c n . assay o f al lergens. Jnun.u, of
t-,:SK.\ M • UKU KSSOS. K . & VAIU.A. J.1M. V»
- m b i m n s sri,ins-« ' " T M L ™ S NUNUITO. H. & KUROUMI:. T . ( 1979) A l lc rgenie i ly and lymphocy le -s i i l a . n g
^ ' o f ^ P^i". •"< ' W """ -59'
presence of cross-reactivity iu icity between different ss closely parallels their lip in decreasing closeness is do Krilis & Wrigley, 1980). e jnd to have a very high n related species such as \ them was still remarkable, at ; who also reported the • : i oat (Baldo, Kril is & in. 1975). By employing the t r"veen an extract of wheat
ra its, Blands et al. (1976) ;is «.stinguished by different >me of the components were ; . :ross-reactivity between . 1 /ould mean that bakers, likely to develop allergies to ii ed this point. We found E itibodies to a wide range IVUIU further occupationally juit working in the bakery j i type of flour to another
car to be confined to a single e ns of different molecular 3 d 4). In general, the low ilii respect to their reactivity th-"- investigators have also s wheat were fractionated . _. ih fractions were réactive akcr's asthma although the r Mivity (Baldo & Wrigley, n to be distributed among
.1 , oncnts. Clinical A livre r, 8, 109. uilcU Hour antigens. Allergy. 35, 45.
Focus on CME at Université Laval
By Jean Bourbeau, MD
DR. BOURBEAU is professor of medicine, Université Lavai and active staff member. Centra Hospitalier Universitaire du Saint-Sacrement, Quebec, Quebec.
OCCUPATIONAL ASTHMA: A PATIENT-ORIENTED APPROACH Occupational asthma is an important health problem as long-term exposure may result in persistent disease even when the patient leaves the offending work environment. Increased awareness among physicians should improve the recognition of this underestimated health problem in Canada.
In the past few years occupa-tional asthma has attracted considerable medical attention. It is now known that the disor-der can be caused by a large number of organic and inorgan-ic compounds. As new materi-als are introduced into industry, the list of compounds will increase. While the develop-ment of new investigative tech-niques has and will continue to assist the diagnosis of this dis-ease, an increased awareness among physicians is still of con-siderable importance.
PREVALENCE OF OCCUPATIONAL ASTHMA The overall prevalence of occupational asthma in Canada is unknown. In the last few years, however, there has been an increase in Workers' Com-
pensation Board claims for occupational asthma as com-pared to the traditional pneumo-conioses. The prevalence of occupational asthma seems to vary depending on the industrial agent, exposure, and specific working conditions. As many as 30% of animal handlers, 5% of workers exposed to volatile iso-cyanate and 4% of workers exposed to western red cedar dust develop asthma. Proper epidemiologic assessment, especially prospective studies, are needed to clarify the extent of the problem in relation to specif ic agents or the work environment.
DEFINING THE DISEASE Airway diseases related to the work environment. As recently recommended by the
The Canadian Journal of CME November/December 1990 19
Occupational Asthma
The prevalence of occupational asthma seems to vary depending on the industrial agent, exposure, and specific working conditions.
Proper epidemiologic assessment, especially
prospective studies, are needed to clarify the extent of the
! problem in relation to specific agents or the work environment
Dr. Jean Bourbeau
Canadian Thoracic Society, the diagnosis of occupational asth-ma is usually restricted to patients with variable airway narrowing induced by sensitiz-ing agents in the work environ-ment. Other airway diseases, however, can be related to the work environment: * Byssinosis due to cotton, flax and jute exposure is recognized as work-related and character-ized by "Monday symptoms" with improvement during the week; * Reactive Airways Dysfunction Syndrome (RADS) due to high level exposure of irritating fumes, smoke or gases may be work-related and is character-ized by airway hyperactivity of variable duration with or without airway obstruction.
In practice, the distinction
between an occupational exac-erbation of pre-existing asthma and the induction of a new state of airway reactivity may be diffi-cult to make, especially in work-ers with persistent symptoms who have been exposed to the
In practice, the distinction between an occupational exacerbation of pre-existing asthma and the induction of a new state of airway reactivity may be difficult to make.
compound(s) for a long period. Causes. There are a large
number of agents known to cause occupational asthma. The majority have been report-ed through single case or case series and less often from epi-demiologic studies. There are two distinct classes of sub-
stances which provoke occupa-tional asthma (Table 1). One comprises materials of high molecular weight such as ani-mal products, grain, flour, bio-logic enzymes and crab. The second group includes materi-als of low molecular weight such as isocyanates, anhy-drides from epoxy resins, exotic wood dust, persulfate and henna .used in hairdressing products, and certain fluxes from soldering.
Mechanisms and patterns of asthmatic reactions. Dif-ferent patterns of asthmatic reactions have been document-ed in the workplace and should be differentiated by the clini-cian. These are known as immediate, late and dual reac-tion.
An immediate reaction occurs within minutes of exposure, with recovery within two hours. It is induced by either nonailergic or allergic stimuli. Nonailergic stimuli such as cold air, exer-cise and nonspecific irritants induce bronchoconstr ict ion through reflex mechanisms in patients who have pre-existing bronchial hyperreactivity. Al-lergic stimuli in patients with positive immediate wheal reac-tions are likely mediated by immunoglobulin antibodies (IgE) and may be associated with a late phase reaction. This type of reaction usually is seen
20 The Canadian Journal of C M E November/December 1990
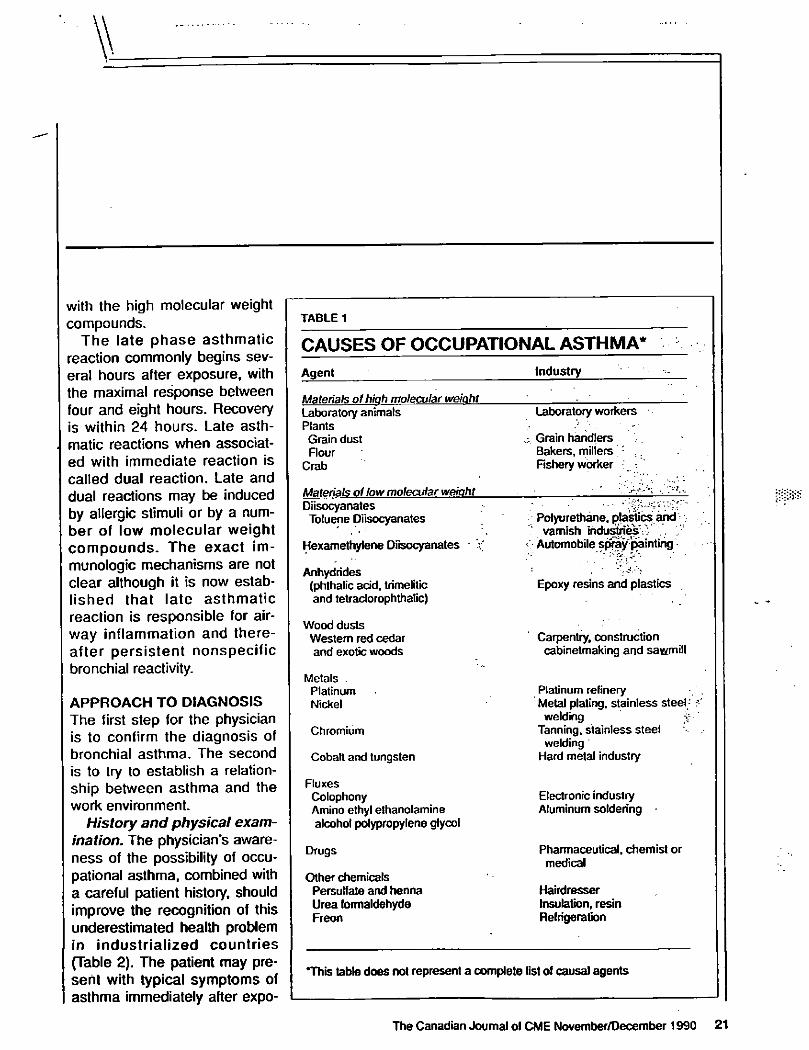
with the high molecular weight compounds.
The late phase asthmatic reaction commonly begins sev-eral hours after exposure, with the maximal response between four and eight hours. Recovery is within 24 hours. Late asth-matic reactions when associat-ed with immediate reaction is called dual reaction. Late and dual reactions may be induced by allergic stimuli or by a num-ber of low molecular weight compounds. The exact im-munologic mechanisms are not clear although it is now estab-lished that late asthmatic reaction is responsible for air-way inflammation and there-after persistent nonspecific bronchial reactivity.
APPROACH TO DIAGNOSIS The first step for the physician is to confirm the diagnosis of bronchial asthma. The second is to try to establish a relation-ship between asthma and the work environment.
History and physical exam-ination. The physician's aware-ness of the possibility of occu-pational asthma, combined with a careful patient history, should improve the recognition of this underestimated health problem in industrialized countries (Table 2). The patient may pre-sent with typical symptoms of asthma immediately after expo-
TABLE 1
CAUSES OF OCCUPATIONAL ASTHMA* Agent Industry
Materials of hiah molecular weiaht Laboratory animals Plants Grain dust Flour
Crab
Laboratory workers
Grain handlers Bakers, millers : . . Fishery worker •;
Materials of low molecular weiaht Diisocyanates Toluene Diisocyanates
Hexamethylene Diisocyanates
Polyurethane, plastics' and ' varnish industries;-/V .
v Automobile spray painting
Anhydrides (phthalic add, trimelitic and tetraclorophthalic)
Epoxy resins and plastics
Wood dusts Western red cedar and exotic woods
Carpentry, construction cabinetmaking and sawmill
Metals . Platinum Nickel
Chromium
Cobalt and tungsten
Platinum refinery Metal plating, stainless steel; welding £
Tanning, stainless steel welding
Hard metal industry
Fluxes Colophony Amino ethyl ethanolamine alcohol polypropylene glycol
Electronic industry Aluminum soldering
Drugs
Other chemicals Persulfate and henna Urea formaldehyde Freon
Pharmaceutical, chemist or medical
Hairdresser Insulation, resin Refrigeration
'This table does not represent a complete list of causal agents
The Canadian Journal of CME November/December 1990 21
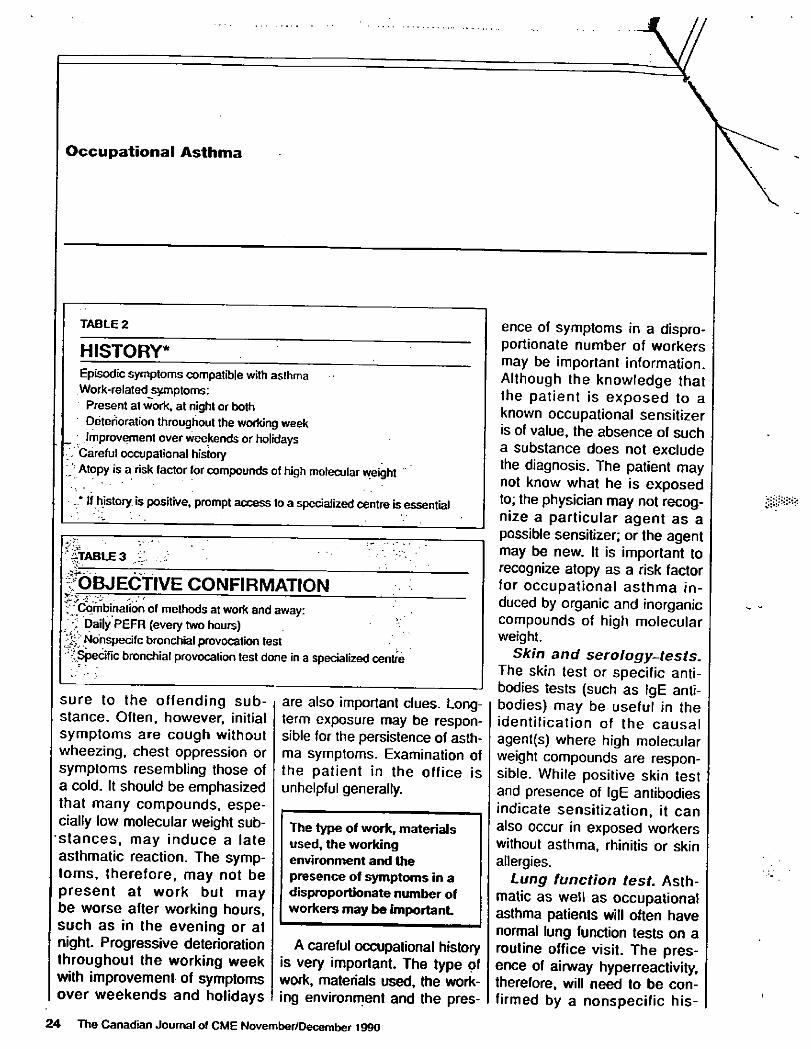
Occupational Asthma
\
TABLE 2
HISTORY* Episodic symptoms compatible with asthma Work-related symptoms:
Present at work, at night or both Deterioration throughout the working week Improvement over weekends or holidays
Careful occupational history / Atopy is a risk factor for compounds of high molecular weight
. * If history, is positive, prompt access to a specialized centre is essential
"Stable3 :.,'•
^OBJECTIVE CONFIRMATION ^
; J Combination of methods at work and away: Daily PEFR (every two hours)
i-' Nohspecifc bronchial provocation test " Specific bronchial provocation test done in a specialized centre
sure to the offending sub-stance. Often, however, initial symptoms are cough without wheezing, chest oppression or symptoms resembling those of a cold. It should be emphasized that many compounds, espe-cially low molecular weight sub-stances, may induce a late asthmatic reaction. The symp-toms, therefore, may not be present at work but may be worse after working hours, such as in the evening or at night. Progressive deterioration throughout the working week with improvement of symptoms over weekends and holidays
are also important clues. Long-term exposure may be respon-sible for the persistence of asth-ma symptoms. Examination of the patient in the office is unhelpful generally.
The type of work, materials used, the working environment and the presence of symptoms in a disproportionate number of workers may be impor tant
A careful occupational history is very important. The type of work, materials used, the work-ing environment and the pres-
ence of symptoms in a dispro-portionate number of workers may be important information. Although the knowledge that the patient is exposed to a known occupational sensitizer is of value, the absence of such a substance does not exclude the diagnosis. The patient may not know what he is exposed to; the physician may not recog-nize a particular agent as a possible sensitizer; or the agent may be new. It is important to recognize atopy as a risk factor for occupational asthma in-duced by organic and inorganic compounds of high molecular weight.
Skin and serology-tests. The skin test or specific anti-bodies tests (such as IgE anti-bodies) may be useful in the identification of the causal agent(s) where high molecular weight compounds are respon-sible. While positive skin test and presence of IgE antibodies indicate sensitization, it can also occur in exposed workers without asthma, rhinitis or skin allergies.
Lung function test. Asth-matic as well as occupational asthma patients will often have normal lung function tests on a routine office visit. The pres-ence of airway hyperreactivity, therefore, will need to be con-firmed by a nonspecific his-
2 4 The Canadian Journal of CME November/December 1990
tamine test or a methacholine bronchial provocation test.
It is necessary to obtain objective confirmation of a rela-tionshipJbetween asthma and the work environment (Table 3). It is common practice to have a peak expiratory flow rate (PEFR) recorded by the patient every two hours both at work and at home over a two week period. The demonstration of increased bronchial reactivity on returning to work, together with appropriate changes in PEFR, suggests a relationship between a sensitizing com-pound and the presence of asthma. Although it is easy to perform, the PEFR has recog-nized limitations such as when exposure to an agent is inter-mittent, persistence of asthma even after removal from expo-sure and potential falsifying of the results by the patient. Bronchial reactivity is nonspe-cific and may be increased by viral infection, exposure to acetylsalicylic acid (ASA), sul fites, allergens and even certain irritants such as ozone.
Bronchial reactivity may be decreased by the treatmen therapy of oral and topical corti-costeroids. Specific bronchial provocation tests are often required to complete the inves-tigation and to establish the relationship between a com-
TABLE 4
MANAGEMENT AND TREATMENT
Avoidance of exposure by change of location or change ot work
Usual approach with anti-asthma agents: Beta 2 adrenergic
. Inhaled or oral corticosteroids Theophylline
pound to which the patient is exposed at work and the pres-ence of asthma: These tests should be performed by experi-enced personnel under the supervision of a specialist in a hospital. Testing is indicated in a situation w h e r e , occupational asthma is suspected but a spe-cific compound is unrecog-
Treatment w i t h ora l a n d topical cor t icostero ids m a y d e c r e a s e bronchia l reactivity.
nized, when an evaluation at work is tor any reason difficult, or if there is a need to confirm the diagnosis for medical/legal purposes.
M A N A G E M E N T A N D
T R E A T M E N T
The worker who is suspected of having occupational asthma should not resign from his job until a firm diagnosis has been made, or a compensation claim has been decided. If the asth ma is disabling, the patient
should be taken off work duties and, where possible, put on sick benefits. A claim may be made to the provincial compen sation board for financial loss, disability and, where possible, enrollment in a program for retraining.
When the relationship be tween asthma and the work place or a specific agent has been established, the therapeu tic approach includes two major steps (Table 4). First, the patient should avoid exposure to the offending substance by changing location of work or the work itself. The use of masks and respirators should be regarded as temporary protec-tion and cannot usually control occupational asthma. It is well known that long-term exposure is associated with persistent asthma. Secondly, the treat-ment approach regarding anti-asthma agents is the same in occupational compared to non-occupational asthma. Long-term treatment is sometimes
The Canadian Journal ol CME November/December 1990 2 5
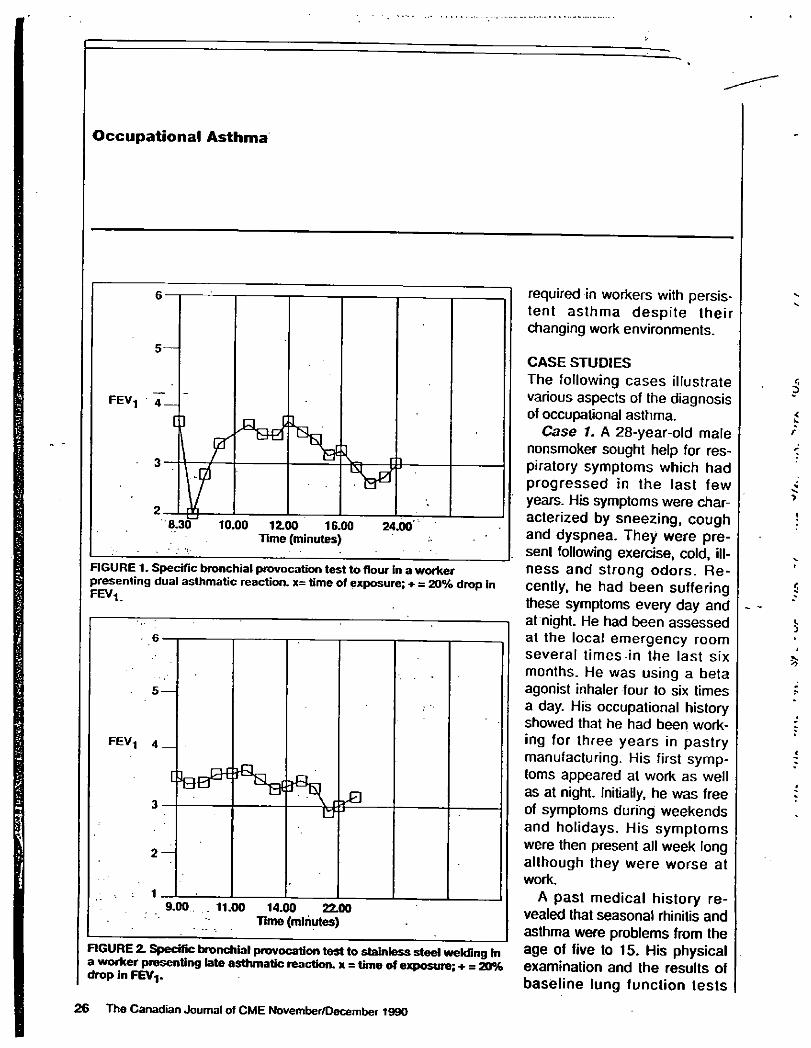
Occupational Asthma
6
FIGURE 1. Specific bronchial provocation test to flour in a worker presenting dual asthmatic reaction. x= time of exposure; + a 20% drop in FEV1
5 —
FEV! 4
[
3 r 0
5 —
FEV! 4
[
3 r 0
2 —
: 1
a J
9.00 11.00 14.00 22.00 Time (minutes)
FIGURE 2. Specific bronchial provocation test to stainless steel welding In a worker presenting late asthmatic reaction, x = time of exposure; + = 20% drop in FEV-j.
required in workers with persis-tent asthma despite their changing work environments.
CASE STUDIES The following cases illustrate various aspects of the diagnosis of occupational asthma.
Case 1. A 28-year-old male nonsmoker sought help for res-piratory symptoms which had progressed in the last few years. His symptoms were char-acterized by sneezing, cough and dyspnea. They were pre-sent following exercise, cold, ill-ness and strong odors. Re-cently, he had been suffering these symptoms every day and at night. He had been assessed at the local emergency room several times-in the last six months. He was using a beta agonist inhaler four to six times a day. His occupational history showed that he had been work-ing for three years in pastry manufacturing. His first symp-toms appeared at work as well as at night. Initially, he was free of symptoms during weekends and holidays. His symptoms were then present all week long although they were worse at work.
A past medical history re-vealed that seasonal rhinitis and asthma were problems from the age of five to 15. His physical examination and the results of baseline lung function tests
26 The Canadian Journal of CME November/December 1990
were normal. The PEFR showed a major decline at work but also during the weekend. His allergy skin tests were sig-nificant for different pollens and flour. A claim to-the-compensa-tion board was made and the patient was referred to a spe-
cialized centre. Analysis. Despite the pa-
tient's atopy and past history of rhinitis and asthma, it is still important to exclude the diag-nosis of occupational asthma in this case. Further investigation, including a nonspecific his-tamine bronchial provocation test showed a change in bronchial reactivity. Before exposure to flour, the PC20 was at 2 mg/mL and after exposure the FEVi dropped 35% follow-ing inhalation of physiologic serum. A specific provocation test with flour showed a dual asthmatic reaction, confirming the diagnosis of occupational asthma (Figure 1).
Case 2. A 35-year-old non-smoking male was seen for coughing spells. His respiratory symptoms began a year previ-ously, specifically during the working week and at night. He was very athletic but had to stop participating in sports because of respiratory symp-toms when he exercised.
For the past three years he was employed soldering greasy and sometimes galvanized and
Effective ulcer therapy with a cytoprotective, non-systemic safety profile -
NOTHING WORKS LIKE
N O N - S Y S T E M I C
sucra (fate/NORDIC
Sulcrate® can 'protect the gastric mucosa against various irritants
... alcohol, ASA, acid../ Product Monograph . September 14.1989
Tablets 1 g and Suspension 500 mg/5 mL
(ympnimivr 1 [ 'Su lcrate
B.I.D. dosage convenience j'sj. . ;
FOR PRESCRIBING INFORMATION, PLEASE SEE PAGE 10
The Canadian Journal of CME November/December 1990 2428
Occupational Asthma
stainless steel. Other workers had also complained of respira-tory symptoms. The work in-volved inhaling a significant amount of fumes; the ventilation systems often malfunctioned and he was not using the mask provided by the employer. . The patient's past medical his-
tory was non-contributory and the physical examination was unremarkable. His baseline lung function and his PEFR at work and home were normal. He stat-ed, however, that his employer assigned him to do work with low fume exposure during the time he was assessing his PEFR at work. The patient was referred to a specialized centre.
Analysis. Further investiga-tion included a nonspecific his-tamine bronchial provocation test which shows a PC20 at 16 mg/mL. It was impossible to organize a test at work since the relationship between the worker and his manager was not ami-cable. A specific provocation test was done in the laboratory in which the worker used the same equipment with different steels on different days. A late asth-matic reaction was shown follow-ing stainless steel welding, con-firming the diagnosis of occupa-tional asthma (Figure 2).
CONCLUSION Occupational asthma is under-
diagnosed in Canada. It is an important health problem as long-term exposure may result in persistent asthma despite removal from the work environ-ment. Although recognition of an occupational , sensitizer is valu-able, the diagnostic approach should involve starting with the symptoms of the patient instead of the specific agent. Definitive objective confirmation of a rela-tionship between asthma and the work environment will often need to be done with specific bronchial provocation tests. Any worker suspected of having occupational asthma should make a claim to the provincial workers' compensation board. If the condition is disabling, the worker should be enrolled for sick benefits. In occupational asthma, treatment is the same as for any asthmatic patient. It is important, however, that the worker avoids exposure by changing the location of the work or the work itself.
SUGGESTED READING 1. Brooks. SM. Weiss. MA. Bernstein. IL:
Reactive airways dysfunction syndrome (RAOS). Persistent airway hyperreactivi-ty after high level irritant exposure. Chest 88:376.1985.
2 Butcher. BT, O'Neil, CE. Jones. RN: The Respiratory Effects ol Cotton Dust —Cfinics in Chest Medicine. Saivaggio. JE. Stankus. RP. eds. W B Saunders. Philadelphia. 1983. p.63.
3. Chan-Yeung, M. Lam. S: Occupational asthma. A m Rev Respir Ois 133:687. 1986.
T H E C A N A D I A N J O U R N A L O F
C O N T I N U I N G M E D I C A L E D U C A T I O N
Publishing schedule 1991
January/February McMastër University
March
University of British Columbia
April
University of Western Ontario
May University of Calgary
June/July Queen's University
August /September University of Alberta
October University of Toronto
November /December McGill University
28 The Canadian Journal of CME November/December 1990
Occupational Respiratory Diseases Resulting From Exposure to Eggs, Honey, Spices, and Mushrooms
Presented by Carol O'Neil, Ph.D.
ore than 200 agents encountered in thc workplace have been found to induce occupational asthma
and hypersensitivity pneumonitis in susceptible indi-viduals. O'Nei l commented that her presentation was ntended to be illustrative rather than comprehensive.
Common methods for evaluating allergic reactions include pulmonary function testing, questionnaire ad-ninistration. both individual and environmental dust evel monitoring, skin testing, and radioallergosorbent
testing (RAST) . Two studies of occupational allergy esulting from inhalation of egg were reviewed. The irst study, which involved 25 employees of an egg-
processing factory, found occupational asthma in five workers. Positive skin reactivity to one or more egg illergens was found in eight workers, including the five vith occupational asthma. The study showed that skin tests are the best clinical predictor of reactivity.
The second study tested 13 bakery workers using an :gg and water solution to glaze rolls with a spray gun. While eight o f t h e 13 workers reported symptoms to ?ggs. there was no consistency of symptoms. Six of 13 iubjects were classified as atopic, and two of these were jkin test positive to egg (only one of these was symp-tomatic). Failure to use purified egg fractions may have iccounied for the low number of positive skin tests, O ' N e i l noted. The dose and length of exposure may explain the failure to demonstrate occupational expo-sure leading to respiratory symptoms. Alternately, the powdered egg or powdered egg yolk may be a more
Clinical Immunology Section, Tulane Medical Center
potent allergen than aerosolized egg. Comparison of subjects in this study, whose main route of administra-tion of egg allergen is inhalation, with 267 subjects whose sole route of administration was ingestion, sug-gests that egg allergy may be an indicator of a high degree of atopy. Respiratory sensitivity to inhaled egg is not related to the atopic state.
O'Nei l > presented a case report of a 31-year-old woman who was a breeder of birds. The woman devel-oped respiratory symptoms to birds along with a G1 sensitivity to ingested eggs. She showed little reactivity to egg white. In patients with known exposure to birds, it is clinically important to test for allergy to egg yolk as well as to the more common allergen egg white.
There are over 1,600 commercial beekeepers in the United States and 30 companies that process honey on a year-round basis. This number does not include thou-sands of hobbyists. Cases of occupational asthma have been reported in workers in honey-processing plants. O'Nei l presented a case report of a 48-year-old woman who was asymptomatic until her ninth year of employ-ment. Her symptoms were seasonal coughing and wheezing. The subject underwent skin testing, R A S T testing, and provocative inhalation challenge. She had no reactivity to honey ingestion and bee stings, and skin test results were negative for common inhalant allergens and honeybee venom. However, skin lest and R A S T for whole body extracts were positive. After rechallenge using an extract obtained from a personal monitor worn by the patient at work and at home, the allergen was determined to be body parts of honeybees. O'Nei l emphasized the importance of challenging non-sensitive asthmatics in order to confirm the specificity of the reaction.
Allergy Proc. 69
Occupational exposure to garlic may induce asthma in sensitive individuals. O f the five reported cases, two were farm workers w ho harvested garlic bulbs, and three were workers in a spice factory. A iopv may be an undcrKing risk factor in garlic sensitivity. O ' N e i l pre-sented a case report o f an electrician employed in a spice factory. After S years on the job. he developed severe asthma, and he also noted the immediate onset of wheezing after ingesting garlic. Inhalation challenge showed an immediate reaction: however, ingestion symptoms peaked at 2 hours after challenge.
Un l ike occupational asthma, which usuallv strikes individuals, outbreaks o f "mushroom workers* lung." a hypersensitivity pneumonit is, have been reported. U n -dcrKing host risk factors remain unknown. Rout ine clinical immunology laboratory tests are less useful than in the diagnosis o f occupational asthma. Antigens de-rive f rom two primary sources: microorganisms and mushroom spores. However, workers can be exposed to a variety o f antigens, and individual responses vary widely. In a ease o f 17 workers reporting systemic and respiratory symptoms, there was no c o m m o n precipi-tant l inking these workers. Occupational asthma has occurred in mushroom growers and soup processors. In growers, the allergen is mushroom spores, whi le in soup processors, the allergen is dried mushroom pow-der.
As in the major i ty o f food-handling and -processing industries, prevalence or incidence studies o f occupa-tional respiratory diseases are lacking. In some cases, the causative agent may not be the food itself (e.g.. poultry miles). T h e role of atopy is unclear in occupa-tional respiratory diseases. Symptoms of food allergy-may also occur in sensitive workers, but this is not universal.
Discussion
Feinberg questioned whether studies had been done
on the allergenicity of the polysaccharides and glu-cosamines in crustacea. Lehrer noted that R A S T reac-tions are due to glycoproteins. High R A S T values f rom the preparations with the water and the meat were a result of proteins. Tests on shell products have not shown any reactivity.
A question f rom the audience concerned the level o f awareness a m o n g manufacturers and their responses to the cases and studies that had been discussed. Lehrer said that the two plants in the snowcrab study had made efforts in envi ronmenta l control, including changes in construction and improved ventilation. In a study o f an indoor mushroom-growing plant specializing in shi-itake. a species that sporulates throughout its lifecycle. high levels o f spores were found, even in the hallways and office areas, according to Lehrer. H e added that, while this large company was making serious envi ron-mental control efforts, the smaller " m o m - a n d - p o p "
70
operations will be more likely to have occupational allergy problems.
REFERENCES 1. Edwards JH. McConnoehic K. Trotman DM. Collins G.
Saunders MJ. Latham SM. Allergy to inhaled egg material. Clin Allergy 13:427-432. 1983.
2. Bernstein Dl . Smith AO. Mollcr DR. ci al. Clinical and immunologic studios among egg-processing workers with oc-cupational asthma. J Allcrgv Clin Immunol 80791-797 1987.
3. Rcisman RE. Hale R. Wypvch J|. Allergy lo honeybee bodv components: distinction from bee venom sensitivity. J AI le ray Clin Immunol 71:18-20. 1983.
J. Bousquet J. Dhivcrt I t . Clauzel A-M. Hewitt B. Michel F-B. Occupational allergy to sunflower pollen. J Allergy Clin Im-munol 75:70-74. 1985.
5. Lybarger JA. Gallagher JS. PuUcr DW. Litwin A. Brooks S. Bernstein IL. Occupational asthma induced by inhalation and ingestion of garlic. J Allergy Clin Immunol 69:448-454. 1982.
6. van Toorcnenbcrgcn AW. Dicges PH. Immunoglobulin E antibodies against coriandcr and other spiccs. J Allergy Clin Immunol 76:477-81. 1985.
7. Jackson E. Welch K M A. Mushroom worker's lung. Thorax j 25:25-30. 1970.
8. Symington IS. Kerr JW. McLean DA. Type I allergy in I mushroom soup processors. Clin Allergy 11:43-7. 1981. O |
l
A D D I T I O N A L REFERENCES j 1. Smith AB. Bernstein D l . A w T - C . et al. Occupational asthma
from inhaled egg protein. A m J Ind Med 12:205-218. 1987. j 2. Lutsk y I. Teichtahl H. Bar-Sela S. Occupational asthma due j
to poultry mites. J Allergy Clin Immunol 73:56-60. 1984. i 3. Bar-Sela S. Teichtahl H. Lutsky I. Occupational asthma in j
poultry workers. J Allergy Cl in Immunol 73:271-275. 1984. j 4. Edwards JH. McConnochie K. Da vies BH. Skin-test reactivity I
to egg protein—exposure by inhalation compared with inges- ' t ion.Cl in Allergy 15:147-150. 1985. i
5. Hoflman DR. Guenther D M . Occupational allergy to avian j proteins presenting as allergy to ingestion of egg yolk. J Allcrgv Clin Immunol 81:484-488. 1988. !
6. Paggiero PL. Loi A M . Toma G. Bronchial asthma and der- j matitis due to spiramycin in a chick breeder. Cl in Altergv I 9:571-574. 1979. * 3
7. Bousquet J. Campos J. Michel F-B. Food" intolerance to ; honey. Allergy 39:73-75. 1984.
8. Cohen SH. Yunginger JW, Rosenberg N. Fink JN. Acute allergic reaction after composite pollen ingestion. J Allergy Clin Immunol 64:270-274. 1979. c
9. Ostrom NK. Swanson MC. Agarwal MIC Yunginger JW. Occupational allergy to honeybee-body dust in a honey proc-essing plant. J Allergy Cl in Immunol 77:736-740. 1986. ,
10. Fallcroni AE. Zeiss CR. Leviiz D. Occupational asthma sec-ondary to inhalation of garlic dust. J Allergv Cl in Immunol 68:156-160. 1981.
11. Couturier P. Bousquet J. Occupational allergy secondary to , garlic dust. J Allergy Cl in Immunol 70:145. 1982. j
12. van Toorcnenbcrgcn AW. Huijskes-Heins MIE. Leijnsc R. Dicges PH. Immunoblot analysis of IgE-binding antigens in spices, lnt Arch Allergy Appl Immunol 86:117-120. 1988.
13. Uragoda ÇG. Asthma and other symptoms in cinnamon workers. Br J Ind Med 41:224-227. 1984.
14. Zuskin E. Skuric Z. Respiratory function in tea workers. Br J Ind Med 41:88-93. 1984.
15. Stewart CJ. Mushroom worker's lung—two outbreaks. Thorax 29:252-257. 1974. •
March-April 1990, Vol. 11. No. 2
-ij'.'innMimg.tf- iiimuuj H mwB—roai mmmmmBBi ammmtmmmmmm
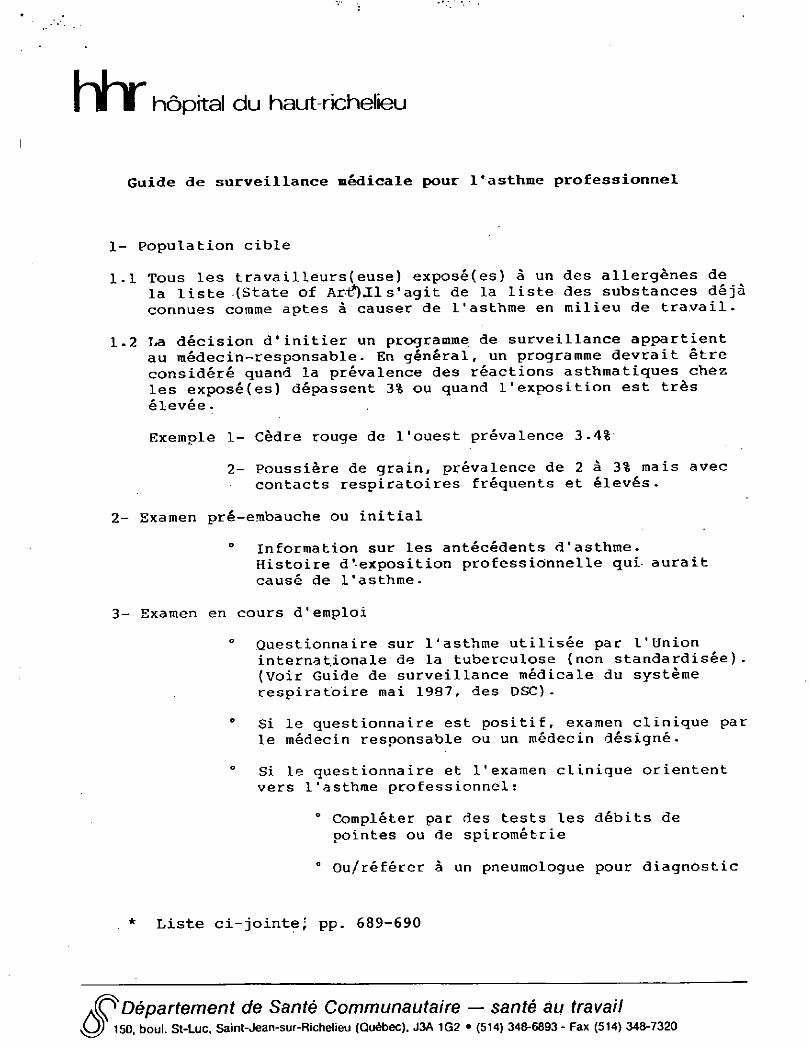
h h r hôpital du haut-richelieu
Guide de surveillance médicale pour l'asthme professionnel
1- population cible
1.1 Tous les travailleurs(euse) exposé(es) à un des allergènes de la liste (State of Artb.Il s'agit de la liste des substances déjà connues comme aptes à causer de l'asthme en milieu de travail.
1.2 La décision d'initier un programme de surveillance appartient au médecin-responsable. En général, un programme devrait être considéré quand la prévalence des réactions asthmatiques chez les exposé(es) dépassent 3% ou quand l'exposition est très élevée.
Exemple 1- Cèdre rouge de l'ouest prévalence 3.4%
2- Poussière de grain, prévalence de 2 â 3% mais avec contacts respiratoires fréquents et élevés.
2- Examen pré-embauche ou initial
° Information sur les antécédents d'asthme.
Histoire d'exposition professionnelle qui aurait causé de l'asthme.
3- Examen en cours d'emploi
° Questionnaire sur 1'asthme utilisée par l'Union
internationale de la tuberculose (non standardisée). (Voir Guide de surveillance médicale du système respiratoire mai 1987, des DSC).
° Si le questionnaire est positif, examen clinique par le médecin responsable ou un médecin désigné.
° Si Le questionnaire et l'examen clinique orientent vers 1'asthme professionnel :
° Compléter par des tests les débits de pointes ou de spirométrie
° Ou/référer à un pneumologue pour diagnostic
Liste ci-jointe; pp. 689-690
Département de Santé Communautaire — santé au travail 150 boul. St-Luc, Saint-Jean-sur-Richelieu (Québec). J3A 1G2 • (514) 348 -6893- Fax (514) 348-7320
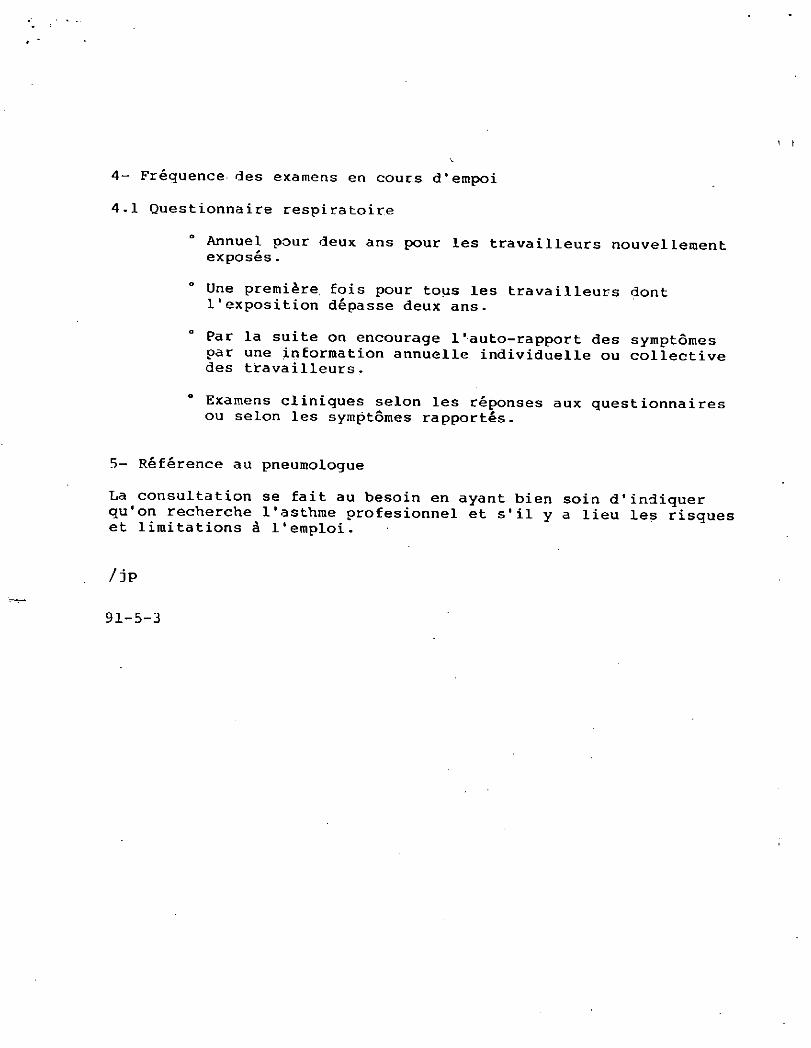
4- Fréquence des examens en cours d'empoi
4 -1 Questionna ire respira toire
Annuel pour deux ans pour les travailleurs n o u v e l l e m e n t e x p o s é s .
Une première fois pour tous les travailleurs dont l'exposition dépasse deux a n s .
Par la suite on encourage l'auto-rapport des symptômes par une information annuelle individuelle ou c o l l e c t i v e des travailleurs.
Examens cliniques selon les réponses aux q u e s t i o n n a i r e s ou selon les symptômes rapportés.
5- Référence au pneumologue
La consultation se fait au besoin en ayant bien soin d'indiquer qu'on recherche l'asthme profesionnel et s'il y a lieu les risques et limitations à l'emploi.
/ jp
91-5-3
( à
State of Art
)| Occupational Asthma1-
MOIRA CHAN-YEUNG and STEPHEN LAM
CONTENTS
Historical Perspective Definition Causes of Occupational Asthma
Reflex Bronchoconstriction Inflammatory Bronchoconstriction Pharmacologic Bronchoconstriction Allergic Bronchoconstriction
Diagnosis History Skin and Serologic Tfcsts. Lung Function Tests Nonspecific Bronchial Provocation Tests Specific Bronchia] Provocation Tests
Mechanisms of Different Patterns of Asthmatic Reactions Induced by Bron-
choprovocation Tests Epidemiologic Studies of Occupational
Asthma Predisposing Host Factors
Prognosis Management Prevention Summary and Future Research
Historical Perspective
A s t h m a caused by occupational haz-
ards has been recognized for a long time.
In 1713, Ramazzini (1), "father of Indus-
trial Medicine/* described grain dust
asthma in an article entitled "Diseases
of Sifters and Measurers of Grain": "the
men who sift and measure are so plagued
by this kind of dust that when the work
is finished they heap a thousand curses
on their calling. The throat, lungs and
eyes are keenly aware of serious damage;
the throat is choken and dried up with
dust,, the pulmonary passages become
coated with crust formed by.dust, and
the result is a dry and obstinate cough.
The eyes aremuph inflamed and watery
and almost all who make a living by sift-
ing or measuring grain are short of breath
and cachectic and rarely reach old age."
The term bysinnosis was first used in
7877 for breathlessness among cotton
workers (2). As early as I9H, asthma
caused by platinum salt exposure was rec-
ognized among photographic workers
(3). However, the interest in occupation
as a cause of asthma and hypersensitiv-
ity pneumonitis vns only revived in the
late 1960*$, particularly through the work
of Pepys in London, England. Since then
a number of distinguished researchers
have also contributed significantly to our
understanding of occupational lung dis-
eases.
Definition Occupational asthma has been defined
as variable airway narrowing causally
related to exposure in the working envi-
ronment to airborne dusts, gases, vapors
orXumeai4). Although the definition ap-
pears to be straightforward, it is not uni-
formly accepted, possibly because it is
too general. For example, in Britain, the
Industrial Injuries Advisory Council de-
fined occupational asthma as "asthma
which develops after a variable period
of symptomless exposure to a sensitiz-
ing agent at work" (5). The Council de-
scribed only 7 groups of industrial
agents: platinum salts, isocyanates, epoxy
resins, colophony fumes, proteolytic en-
zymes, laboratory animals and insects,
and grain (or flour)dust. This definition
is perhaps too restrictive, and this may
have considerable medicolegal implica-
tions. Other definitions include agents
that induce bronchoconstriction by
mechanisms other than sensitization in
the working environment as causes of oc-
cupational asthma (6-8). This diversity
of opinion reflects both the difficulty in
defining asthma in general and the fact
that there are different pathogenetic
mechanisms in occupational asthma.
Causes of Occupational Asthma
Many agents in the working environment
can give rise to asthma. In 1980, their
number was reported to exceed 200 (4).
With the introduction of new materials
into the industry and the increased aware-
ness among physicians, the list will grow
with time.
Gandevia (6) first introduced the class-
ification of occupational asthma accord-
ing to pathophysiologic mechanisms:
reflex, acute inflammatory, pharma-
cologic, and immunologic bronchocon-
striction. In using such a classification,
it should be borne in mind that the mech-
anism responsible for bronchoconstric-
tion in many instances of occupational
asthma is unknown. At times, possibly
more than one ofthe above mechanisms
may be involved for the single occupa-
tional agent.
Reflex Bronchoconstriction Cold air, inhalation of inert particles, or
noxious gases or fumes cause bron-
choconstriction by direct effect on the
irritant receptors in the wall (9-12). Re-
flex bronchoconstriction usually occurs
in subjects with pre-existing bronchial
asthma rather than in normal healthy
subjects. Because the reaction is non-
specific and acts as a temporary aggravat-
ing factor, it is not often accepted as a
cause of occupational asthma.
(Inflammatory Bronchoconstriction In 1970, Gandevia (6) described acute in-
flammatory bronchoconstriction caused
by accidental exposure to high concen-
trations of irritant gases and vapors such
as hydrogen sulphide, diethylene diamine,
fume from over-heated plastics, or smoke
and fume from combustion of a variety
of materials. The air-now obstruction
usually developed within hours, reached
a maximum in a week, and stabilized or
resolved within 3 to 4 months (13-18).
* From the Respiratory Division, Department o f Medtdne, Vancouver General Hospital, University o f Brit ish Columbia, Vancouver, Brit ish Colum-bia, Canada.
' Requests for reprints should be addressed to Dr. Moira Chan-Yeung, Department o f Medicine. Vancouver General Hospital. 2775 Heather Street, Vancouver. & C , VSZ 3J5 Canada.
• 686 AM REV RESPIft DIS 1M0; 13):M*-703
«pçirc or, ART: OCCUPATIONAL. ASTHMA 987
Pathologic studies of patients who died after exposure showed extensive damage and sloughing of the mucosa of the large and small airways along with hemor-
./ rhagic pulmonary edema (13). Dense in-flammatory eel! infiltration, hyperplasia ofthe bronchial submucosal glands, and terminal bronchiolar fibrosis in addition
• to destruction of thc bronchial epithe-lium were also observed in one study (19). Lung function studies of patients after acute inhalation injury showed the pres-ence of reversible air-flow obstruction or bronchial hyperreactivity in some pa-tients (14, 15. 20).
In 1981, Brooks and Lockey (21) de-
scribed "reactive airway disease syn-
drome" in 13 workers who developed
cough, shortness of breath, and wheeze
after short, accidental exposures to high
levels of irritating fumes, smoke, or gases
such as chlorine and ammonia. Typically,
the symptoms occurred within hours of
initial exposure and generally resolved
within several weeks (but they can per-
sist for years after exposure). Nonspecific
bronchial hyperreactivity as determined
by methacholine challenge test was pres-
ent in 5 of 6 patients tested. These pa-
tients did not have any preexisting respi-
ratory symptoms. In a subsequent study
;J (22), Brooks and coworkers carried out
' bronchial biopsies on 2 such patients who
showed bronchial/bronchiolar epithelial
desquamation and mucus cell hyperpla-
sia together with mild infiltration of the
bronchial wall by plasma cells and lym-
phocytes. Changes consistent with bron-
chial asthma, such as eosinophil infiltra-
tion, mucous gland hyperplasia, base-
ment membrane thickening, or smooth
muscle hypertrophy were not found in the
biopsies. They postulated that the cause
of reversible air-fiow obstruction and air-
way hyperreactivity in these patients was
due to extensive inflammatory response;
subsequent re-epithelialization and prob-
able reservation ofthe bronchial mucosa
might have altered the threshold of the
receptors. Another possibility for the
presence of bronchial hyperreactivity is
the increase in epithelial permeability
from the inhalation injury (23, 24).
Whether "reactive airway disease syn-
drome" should be used to describe the
clinical picture presented by these pa-
tients is still uncertain.
i (Pharmacologic Bronchoconstriction V Some ofthe agents in the working envi-
ronment induce asthma by effects simi-
lar to those of pharmacologic agonists.
In these situations, it is expected that
there should be a dose-response relation-ship between exposure and response When the dose is high enough, all'tot-posed subjects are expected to develop bronchoconstriction. There is consider-able controversy as to whether these agents, by causing reversible air-flow ob-struction, really give rise to "asthma" in the usual sense because they do not give rise to eosinophilia or nonspecific bron-chial hyperreactivity.'
Byssinosis. Byssinosis occurs in textile workers exposed to dust of cotton, flax, hemp, or jute The characteristic symp-toms are chest tightness, cough, and la-bored breathing several hours after the patient returns to work on Monday. The symptoms usually disappear overnight, and if they recur on Hiesday, they tend to be milder. Later in the work week the worker usually becomes asymptomatic. The symptoms on Mondays are often as-sociated with a postshift fall in lung func-tion.
The prevalence of byssinosis is higher
among workers with the most exposure,
such as during ginning, opening, or card-
ing, and lowest in those with the least ex-
posure, such as during slashing or weav-
ing (26-31). The prevalence of byssino-
sis increases with the duration of
exposure. Although byssinosis has been
known since 1877, the pathogenetic
mechanisms underlying the disease re-
main unclear. Several nonimmunologic
mechanisms have been postulated:
(1) Release of chemical mediators. Cot-
ton dust extracts were found to induce
histamine release from isolated human,
pig, cow, and sheep lungs but not from
the lungs of other species such as rat,
mouse, guinea pig, or cat. Cotton dust
extracts were also found to contain hista-
mine (32). However, it is thought that the
amount of histamine present in cotton
dust extracts is too small to induce bron-
choconstriction in vivo (33). The levels
of histamine were found to be elevated
in the blood of both cotton and flax
workers. Levels were significantly higher
on Mondays after the weekend. In
asymptomatic workers, the levels of
histamine were lower (34). These find-
ings suggest that histamine release is
likely to play a role in causing acute bron-
choconstriction in these workers. It is
quite possible that other chemical medi-
ators, such as prostaglandins or leu-
kotrienes, may be responsible for bron-
choconstriction in cotton workers.
(2) Endotoxin. Another popular the-
ory for the mechanism of disease in bys-
sinosis is the presence of endotoxin in cot-
ton dust. Cotton dust is known to be con-
taminated with bacteria and fungi (35).
Rylander and coworkers (36) reported
that acute FEV, decrements on M o n d a y
among card room workers correlated beiT
ter with an exposure index incorporat-
ing the number of gram-negative bacte-
ria contaminating bale cotton than with
•the levels of vertical elutriated cotton dust
alone: More recently. Castellan and co-
workers (37) found that after.6 h of ex-
posure of human volunteers in the labo-
ratory to cotton dust, the levels of en-
dotoxin in the dust were highly correlated
with acute changes in forced expiratory
volume in one second (FEV,).
When endotoxins were given to labo-
ratory animals by aerosol, fever and dysp-
nea occurred after inhalation. When they
were given on 2 consecutive days, the sec-
ond inhalation had no effect—simulating
the "Monday tightness" characteristic of
byssinosis (38). The endotoxin was found
to activate the complement system (39),
with subsequent generation of anaphylo-
toxins and release of histamine and leu-
kotactic substances. Evidence against en-
dotoxin playing a major role was the find-
ing of Buck and coworkers (40), who
demonstrated acute decline in lung func-
tion in normal volunteers after exposure^-
to cotton bract extracts even when en f
dotoxin was virtually removed.
Studies of immunologic mechanism in
byssinosis have also yielded controversial
results. Aqueous extracts of cotton dust
have been shown to contain at least 40
separate antigens (41). Dust-specific IgE
antibodies were found in the serum of
some workers in a cottonseed crushing
mill, and a correlation was shown be-
tween the presence of specific IgE anti-
bodies and the postshift decline in FEV,
(42). However, specific IgE antibodies
were also found in the serum of 6 of 11
unexposed control subjects. The sig-
nificance of the dust-specific IgE anti-
bodies has yet to be determined. The fact
that most healthy subjects challenged
with cotton bract extract demonstrate
some degree of bronchoconstriction is
against the hypothesis that an immuno-
logic mechanism is present in byssinosis.
Organophosphate insecticide. Acute
asthma has been described in farm work-
ers spraying crops with organophosphate
insecticides, which act as an anticholi-
nesterase and probably precipitate air-
flow obstruction on a pharmacologic ba(
sis (43). v
Isocyanates and plicatic acid. The
pathogenesis of occupational asthma
caused by isocyanates and western red ce-
686 CMAM-VEUHQ AND LAM
dar {Thujapticafa) is still controversial.
The role of immunologic mechanisms
wi!! be discussed later. The pharmaco-
n • v logic effects of diisocyanate compounds
J J were explored using in vitro techniques.
Ibluene diisocyanate (TDI) was found to
compete with isoproterenol-induced
production of intracellular cyclic AMP
in peripheral blood lymphocytes (44).
The effect appears to be dose-dependent
(45). This antagonistic property of TDI
fror* classic beta-adrenergic
blockade because it also affects prosta-
glandin E» (44) and glucagon receptors
(46). It should be noted that these prop-
erties occurred only in relatively high con-
centrations of TDI. Moreover, in these
in vitro experiments, 10% dimethyl sul-
phoxide was used as the solvent for TDI.
Dimethyl sulphoxide may alter the phos-
pholipid mobility and render the mem-
branous receptors more vulnerable to
TDI. In reviewing all the recent experi-
mental data, Bernstein (47) concluded
that isocyanates probably cause non-
specific inhibition of a variety of mem-
brane receptors and enzyme systems, ef-
fects that are consistent with the highly
reactive properties of these substances.
Plicatic acid, the chemical compound
responsible for western red cedar asthma,
4 ) was found to activate the classic complè-
t e m e n t pathway with generation of medi-
ators of anaphylaxis (48). However, in
both isocyanate- and plicatic-acid-.
induced asthma, pharmacologic action
alone cannot explain why only 5% of the
exposed population develop asthma. It
is possible that the pharmacologic prop-
erties of these compounds may interact
and potentiate the immunologic re-
sponse.
Allergic Bronchoconstriction
By far the greatest number of occupa-
tional agents causing asthma have known
or suspected allergic properties.
Organic high molecular weight com-
pounds, such as proteins, polysaccha-
rides, glycoproteins, and peptides, can in-
duce allergic response by producing spe-
cific IgE antibodies and sometimes
specific IgG antibodies. Some of the
causes of occupational asthma arising-
from exposure to animal-products, in-
sects, plants^ and biological enzymes are
shown in table I. In most instances, posi-
tive immediate skin test reactions can be
lirited with extracts of the offending
agents, and specific IgE antibodies to
these antigens can be detected. Atopic
subjects are much more frequently af-
fected than nonatopic subjects.
Animât handlers. Recent prevalence
studies have shown that asthma occurs
in 3 to 3070 of workers handling labora-
tory animals (49-53). The 4 small mam-
mals (rat, mouse, guinea pig, and rab-
bit) commonly used for laboratory work
have all been reported to cause asthma.
The major source of allergens was found
to be in the proteins in the pelt or urine
or these animals; these proteins have a
relatively low molecular weight (between
10,000 and 38,000 daltons) (54,55). There
appears to be a considerable cross-reac-
tivity between allergens derived from
these animals (55). Rhinitis is commonly
present and usually precedes or coincides
with the onset of asthma. The symptoms
usually occur within a few months after
exposure, with the majority appearing
within 4 yr. Most studies indicate that
atopic subjects are more prone to develop
asthma than nonatopic subjects (50-54).
Greater than 80% of patients with
asthma had positive skin tests to animal
antigens (50-53, 55). Specific IgE anti-
bodies were detected (54) but precipitins
or specific IgG antibodies were not de-
tected (51, 54).
Grain dust. Grain dust is composed of
many materials, including various types
of grain and their disintegration prod-
ucts, as well as pollens, fungi, insects, and
mites. It also contains silicon dioxide in
amounts varying from 5 to 15% of the
total dust and is contaminated by excreta
of rodents and pigeons. Because of the
complex composition of the dust, several
clinical syndromes have been attributed
to grain dust exposure: asthma, chronic
obstructive pulmonary disease, grain fe-
ver, and extrinsic allergic alveolitis.
Several studies (67-69) in grain han-
dlers have demonstrated specific bron-
chial reactions to inhalation challenge
with grain dust or grain dust extract. The
bronchial reactions usually occurred im-
mediately after challenge; in some work-
ers, the immediate reaction was followed
by a late reaction several hours later. Fe-
ver, malaise, and leukocytosis sometimes
accompanied the late asthmatic reaction
(70,71). Results of investigations into al-
lergic mechanisms in grain-dust:induced
bronchoconstriction have been inconclu-
sive. Although Warren and coworkers
(67) found good correlation between
positive skin reaction to grain dust ex-
tract and bronchial reactions, others (68,
69) have failed to do sa Very little infor-
mation is available as to which are the
likely allergens in the grain dust. In 1 case
report, recurrent nocturnal asthma was
shown to be due to exposure to the grain
mite Glycyphagus destructor (59). In an-
other study, durum wheat was found to
contain the responsible allergen (69).
Between 4 and 11% of grain workers
showed a post shift fall in FEV, of greater
than 10% (72, 73). The acute effects on
lung function were found to be dose-
related, the higher the respirable or total
dust level, the greater the acute changes
in lung function (73, 74). There is now
evidence to suggest that the acute revers-
ible changes in lung function from grain
dust exposure may be due to nonimmun-
ologic mechanisms. Extracts of grain
dust have been shown to activate both
the alternative and classic complement
pathways in vitro (75). More recently, ex-
tracts of grain and grain dust were found
tô induce direct release of histamine from
peritoneal mast cells of rats (76). Further
studies are required to elucidate the
mechanism of grain dust asthma and
other clinical syndromes induced by grain
dust exposure.
Baker's asthma. For a long time,
Baker's asthma was thought to be iden-
tical with the asthma experienced by
grain workers. It is, however, becoming
clear that the 2 conditions are distinct.
Most published reports (77,78) have im-
plicated cereal flours as the responsible
allergens for baker's asthma. Affected
bakers develop immediate positive skin
reactions to extracts of cereal flour, and
specific IgE antibodies were found by the
radioallergosorbent test (RAST) (78-82).
Considerable cross-antigenicity was
found between different cereal grains
such as wheat, rye, triticale, barley, and
oat (79, 83).
There are no prevalence studies of
asthma among bakers in Britain or in
North America, but there are good
studies on flour allergy from the Federal
Republic of Germany. Herxheimer (84)
skin tested all baker's apprentices in West
Berlin and found a progressive increase
in the number showing sensitivity to
flour, exceeding 20% by the fifth year
of apprenticeship. Seven percent devel-
oped skin, nasal or bronchial symptoms.
A more recent study by Thiel and Ulmer
(85).showed allergic symptoms in almost
20% of.established bakers; all of them
had rhinitis and most had asthma as well.
It is interesting to note that each year in
West Germany approximately 300 bakers
claim industrial injury compensation and
approximately a quarter receive it (85).
Biologic enzymes. Shortly after the in-
troduction of proteolytic enzymes of Ba-cillus subtilis in detergent production in
the United Kingdom in 19Ô6, Flindt (92)
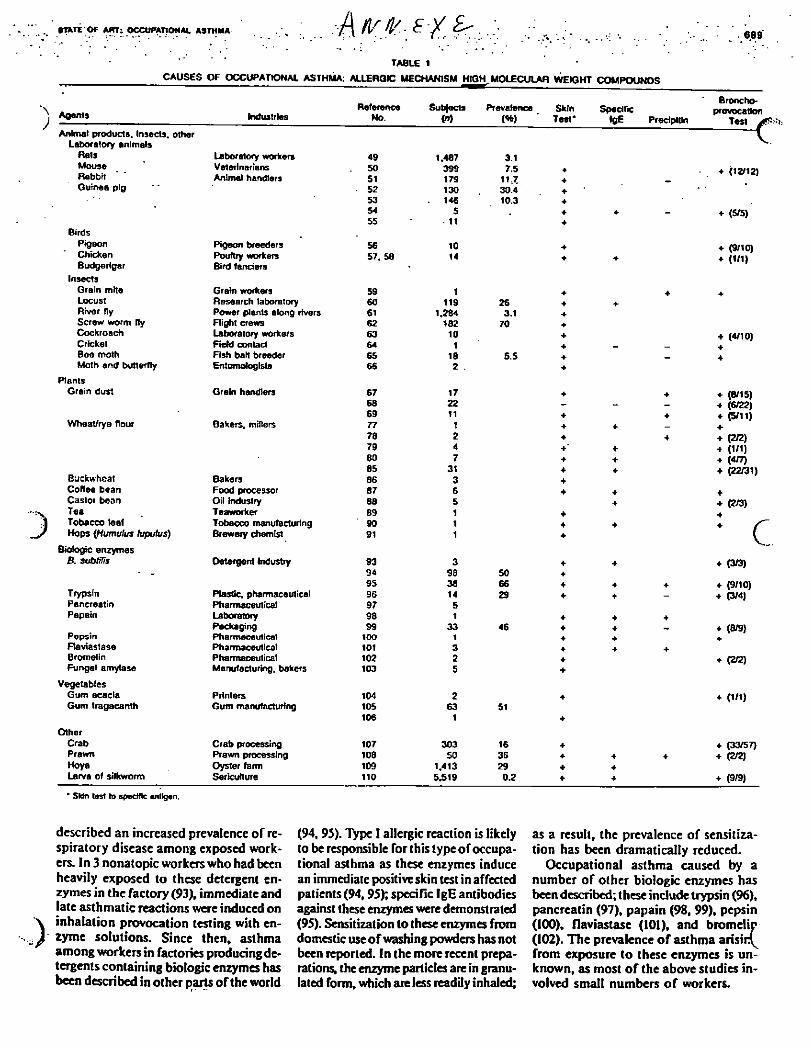
•rare-of Ami occupational asthma A vfc- ^ 6 8 9
TABLE 1 CAUSES OF OCCUPATIONAL ASTHMA: ALLERQtC MECHANISM HIGH MOLECULAR WEIGHT COMPOUNDS
Agents Industries Reference
No. Subjects
(n) Prevalence
(4b) Skin
Test* Spedftc
»0E Precipitin
Broncho-provocation
Test / Animal products. Insects, other
Laboratory animals V
Rats Laboratory workers 49 1.487 3.1 Mouse Veterinarians 50 399 7.5 • Rabbit Animal handlers 51 179 11.7 4
4 (12/12)
Guinea pig 52 130 30.4 • 53 146 10.3 4 54 5 . 4 4 - + (5/5) 55 - 11 4
+ (5/5)
Birds Pigeon Pigeon breeders 56 10 4 4 (9/10) Chicken Poultry workers 57. SO 14 4 4 4 (1/1) Budgerigar Bird fanciers •
Insects Grain mHe Grain workers 59 1 • 4 4 Locust Research laboratory 60 119 26 4 4 River fly Power plants along rivers 61 1.284 3.1 4 Screw worm fly Flight crews 62 182 70 4 Cockroach Laboratory workers 63 10 4 + (4/10) Cricket Field contact 64 1 4 _ _ 4 Bee moth Fish bait breeder 65 18 5.5 4 _ 4 Moth and butterfly Entomologists 66 2 . 4
Plants Grain dust Grain handlers 67 17 4 4 • (8/15)
68 22 - - «• (6/22) 69 11 4 4 4 (5/11)
Wheat/rye flour Bakers, miners 77 1 4 4 _ 4 78 2 4 4 4 (2/2) 79 4 4' + 4 (1/1) 60 7 4 4 4 (4/7) 85 31 4 4 + (22/31)
Buckwheat Bakers 86 3 4
+ (22/31)
Coffee bean Food processor 87 6 4 4 <f Castor bean Oil industry 88 5 4 • (2/3) Tea Teaworker 89 1 4 4 Tobacco leaf Tobacco manufacturing 90 1 • 4 • S Hops (Humuius tuputus) Brewery chemist 91 1 4 c
Biologic enzymes V
B. subtifis Detergent industry 93 3 • 4 4 (3/3) - - 94 98 50 4
4 (3/3)
95 38 66 • 4 4 4 (9/10) Trypsin Plastic, pharmaceutical 96 14 29 4 4 _ 4 (3/4) Pancreatin Pharmaceutical 97 5
4 (3/4)
Papain Laboratory 98 1 4 4 4 Packaging 99 33 46 4 4 _ 4 (8/9)
Pepsin Pharmaceutical 100 1 4 4 4 Flaviastase Pharmaceutical 101 3 4 4 4 Bromelin Pharmaceutical 102 2 4 4 (2/2) Fungal amylase Manufacturing, bakers 103 5 4
4 (2/2)
Vegetables Gum acacia Printers 104 2 4 4 (1/1) Gum tragacanth Gum manufacturing 105 63 51
4 (1/1)
106 1 4
Other Crab Crab processing 107 303 16 4 4 (33/57) Prawn Prawn processing 108 50 36 4 4 4 4 (2/2) Hoya Oyster farm 109 1.413 29 4 4 Larva of silkworm Sericulture 110 5.519 0.2 + 4 4 (9/9)
' SUn tost to Bpectflc antigen.
described an increased prevalence of re-spiratory disease among exposed work-ers. In 3 nonatopic workers who had been heavily exposed to these detergent en-zymes in the factory (93), immediate and late asthmatic reactions were induced on inhalation provocation testing with en-zyme solutions. Since then, asthma among workers in factories producing de-tergents containing biologic enzymes has been described in other parts ofthe world
(94,95). Type I allergic reaction is likely to be responsible for this type of occupa-tional asthma as these enzymes induce an immediate positive skin test in affected patients (94,95); specific IgE antibodies against these enzymes were demonstrated (95). Sensitization to these enzymes from domestic use of washing powders has not been reported. In the more recent prepa-rations, the enzyme particles are in granu-lated form, which are less readily inhaled;
as a result, the prevalence of sensitiza-tion has been dramatically reduced.
Occupational asthma caused by a number of other biologic enzymes has been described; these include trypsin (96), pancreatin (97), papain (98, 99), pepsin (100), flaviastase (101), and bromelir (102). The prevalence of asthma arising from exposure to these enzymes is un-known, as most of the above studies in-volved small numbers of workers.
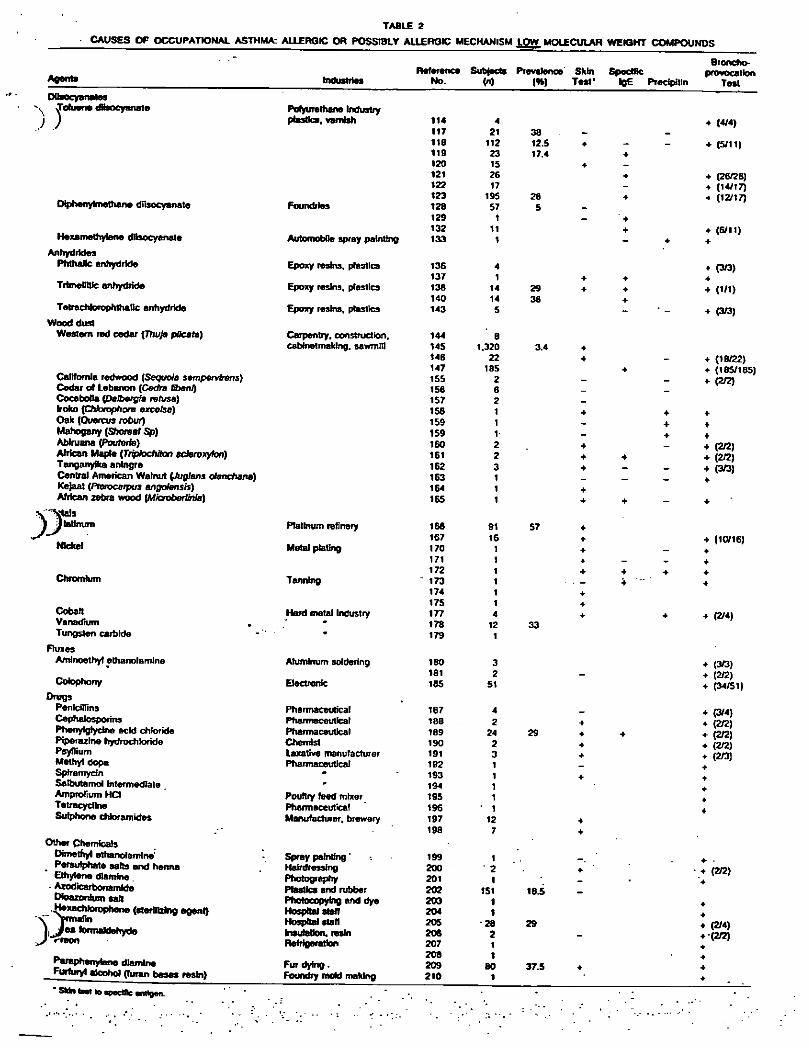
TABLE 2
Agents Reference Subjects Prevalence' Skin Specific
Industries No. W (9») Test' IgE Precipitin
Potyurethane Industry plastics, varnish 114 4
117 21 38 _ 116 112 12.5 4 _ 119 23 17.4 4
120 15 4 _ 121 26 4
122 17 _ 123 195 28 4
Foundries 128 57 5 129 1 _ ' 4
132 11 4 Automobile spray painting 133 1 - 4
Epoxy resins, plastics 136 4 137 1 4 4
Epoxy resins, plastics 138 14 29 4 4
140 14 36 4 Epoxy resins, plastics 143 5 -
Carpentry, construction. 144 6 caMnetmafclng. sawmill 145 1.320 3.4 +
146 22 4 _ 147 185 4
155 2 _ _ 156 6 _ _ 157 2 _ 158 1 4 4
159 1 _ 4 159 1 _ 4
160 2 _ 161 2 4 4
162 3 4 _ _ 163 1 _ _ 164 1 4
165 1 4 4 -
Platinum refinery 166 91 57 + 167 16 4
Metal plating 170 1 4 _ 171 1 4 _ _ 172 1 + 4 •
Tanning ~ 173 1 4 174 1 4
175 1 4 Hard metal Industry 177 4 4 4
• 178 12 33 179 1
Aluminum soldering 180 3 181 2 _
Electronic 165 51
Pharmaceutical 167 4 Pharmaceutical 188 2 4 Pharmaceutical 189 24 29 4 4 Chemist 190 2 4 Laxative manufacturer 191 3 4 Pharmaceutical 192 1 _
• 193 1 4 * 194 1
Poultry feed mixer 195 1 Pharmaceutical 196 ' 1 Manufacturer, brewery 197 12 4
198 7 4
Spray painting ' 199 1 Hair dressing 200 2 4 Photography 201 1 _ Plastics and rubber 202 151 16.5 Photocopying and dye 203 1 Hospital staff 204 1 Hospital stall 205 • 28 29 Insulation, resin 206 2 _ Refrigeration 207 1
208 1 Fur dying. 209 BO 37.5 4 Foundry mold making 210 1
Broncho-provocation
Test DQsocyanates
^ Toluene tfèsocyanate
Dlphenyfmethane diisocyanate
Hexamethytene diisocyanate Anhydrides
PhthaJIc anhydride
TrtmeRtttc anhydride
TetrachkxophthaDc anhydride Wood dust
Western red cedar (Thuja pHcata)
California redwood (Sequoia sempervbens) Cedar of Lebanon (Cerfra Ebanfj CocaboOa (Dafrergfe refusa) Iroto (CMbrqpftore excelse) Oak (Ouercus robur) Mahogany {Shoreat Sp) Abfruana (Poc/ferfe) African Maple (TriplochHon sderoxyfon) Tanganyika aningre Central American Walnut (A/g/ans danctiana) Kejaat (Pterocerpus angohnsis) African zebra wood {Microbertinla)
(tals tatimrm
Nickel
Chromium
Cobalt VanadHim Tungsten carbide
Fluxes Amlnoethyt ethanolamfne
Colophony
Drugs Penicillins Cephalosporins Phenytgfydne acid chloride Piperazine hydrochloride Psyllium Methyl dopa Spiramycin Salbutemol Intermediate Amprofium HCt Tetracycline Sulphone cMoramides
Other Chemicals Dimethyl ethanolemtne:
. Persulphate salts and henna Ethylene diamine.
• Azodicartoonamlde Dtoaxortfum sail -iJ^cWoropheoe (sterilizing agent)
• (4/4)
• (5/11)
4 (26/26) • (14/17) •* (12/17)
4 (6/11) 4
4 (3/3) 4
4 (1/1)
4 (3/3)
4 (16/22)
4 (185/185) 4 (2/2)
4
4
4
4 (2/2) + (2/2) 4 <3/3)
(10/16)
(2/4)
4 (3/3) 4 (2/2) 4 (34/51)
4 (3/4) 4 (2/2) 4 (2/2) 4 (2/2) 4 (2/3)
Paraphenylane diamine Furfuryl alcohol (Turan bases resin)
(2/2)
(2/4) (2/2)
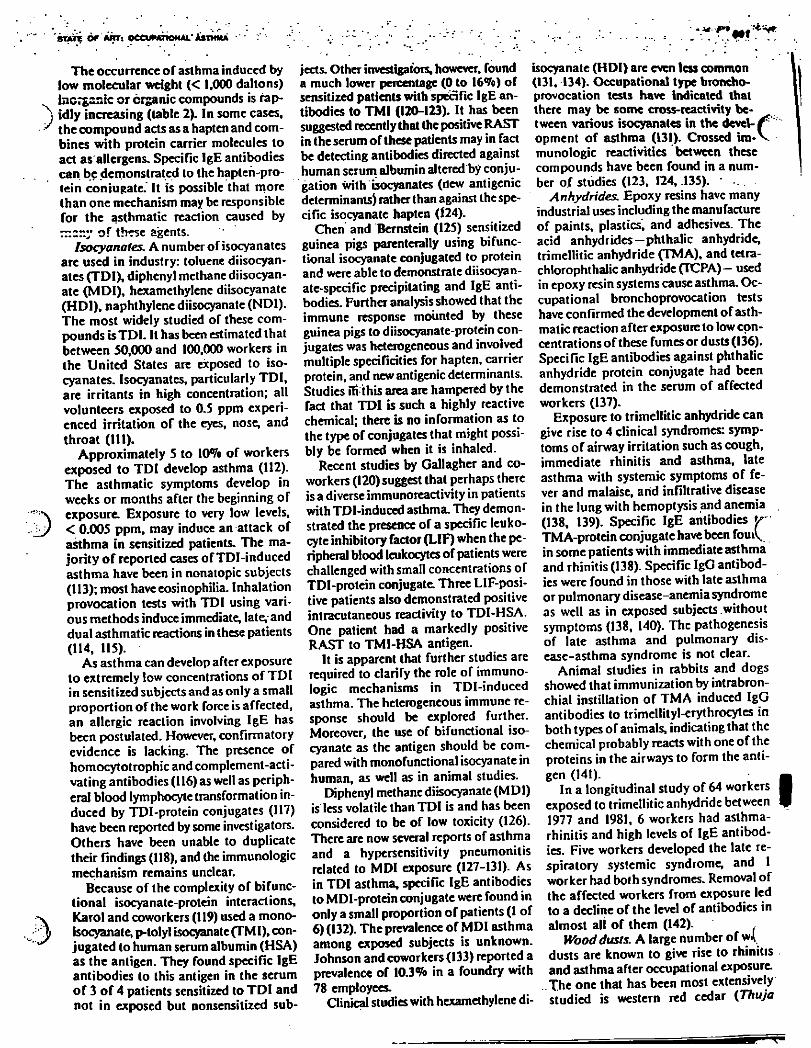
'STATE Of AWT: OCCUMTiOMAL' iSTKMA - •
The occurrence of asthma induced by
low molecular weight (< 1,000 daltons)
inorganic or organic compounds is rap-
idly increasing (table 2). In some cases,
the compound acts as a hapten and com-
bines with protein carrier molecules to
act as allergens. Specific IgE antibodies
can be demonstrated to the hapten-pro-
tein conjugate.' It is possible that more
than one mechanism may be responsible
for the asthmatic reaction caused by
rr.zr.y of these agents.
Isocyanates. A number of isocyanates
are used in industry: toluene diisocyan-
ates (TDI), diphenyl methane diisocyan-
ate (MDI) , hexamethylene diisocyanate
(HDI), naphthylene diisocyanate (NDI).
The most widely studied of these com-
pounds is TDI. It has been estimated that
between 50,000 and 100,000 workers in
the United States are exposed to iso-
cyanates. Isocyanates, particularly TDI,
are irritants in high concentration; all
volunteers exposed to 0.5 ppm experi-
enced irritation of the eyes, nose, and
throat (111).
Approximately 5 to 10<7o of workers
exposed to TDI develop asthma (112).
The asthmatic symptoms develop in
weeks or months after the beginning of
exposure. Exposure to very low levels,
< 0.005 ppm, may induce an attack of
asthma in sensitized patients. The ma-
jority o f reported cases of TDl-induced
asthma have been in nonatopic subjects
(113); most have eosinophilia. Inhalation
provocation tests with TDI using vari-
ous methods induce immediate, late, and
dual asthmatic reactions in these patients
(114, 115).
As asthma can develop after exposure
to extremely low concentrations of TDI
in sensitized subjects and as only a small
proportion of the work force is affected,
an allergic reaction involving IgE has
been postulated. However, confirmatory
evidence is lacking. The presence of
homocytotrophic and complement-acti-
vating antibodies (116) as well as periph-
eral blood lymphocyte transformation in-
duced by TDI-protein conjugates (117)
have been reported by some investigators.
Others have been unable to duplicate
their findings (118), and the immunologic
mechanism remains unclear.
Because of the complexity of Afunc-
tional isocyanate-protein interactions,
Karol and coworkers (119) used a mono-
isocyanate, p-tolyl isocyanate (TMI), con-
jugated to human serum albumin (HSA)
as the antigen. They found specific IgE
antibodies to this antigen in the serum
of 3 of 4 patients sensitized to TDI and
not in exposed but nonsensitized sub-
jects. Other investigators, however, found
a much lower percentage (0 to 16%) of
sensitized patients with specific IgE an-
tibodies to TMI (120-123). It has been
suggested recently that the positive RAST
in the serum of these patients may in fact
be detecting antibodies directed against
human serum albumin altered by conju-
gation with isocyanates (ilew antigenic
determinants) rather than against the spe-
cific isocyanate hapten (f24).
Chen and Bernstein (125) sensitized
guinea pigs parenterally using Afunc-
tional isocyanate conjugated to protein
and were able to demonstrate diisocyan-
ate-specific precipitating and IgE anti-
bodies. Further analysis showed that the
immune response mounted by these
guinea pigs to diisocyanate-protein con-
jugates was heterogeneous and involved
multiple specificities for hapten, carrier
protein, and new antigenic determinants.
Studies lfi this area are hampered by the
fact that TDI is such a highly reactive
chemical; there is no information as to
the type of conjugates that might possi-
bly be formed when it is inhaled.
Recent studies by Gallagher and co-
workers (120) suggest that perhaps there
is a diverse immunoreactivity in patients
with TDI-induced asthma. They demon-
strated the presence of a specific leuko-
cyte inhibitory factor (LIF) when the pe-
ripheral blood leukocytes of patients were
challenged with small concentrations of
TDI-protein conjugate. Three LIF-posi-
tive patients also demonstrated positive
intracutaneous reactivity to TDI-HSA.
One patient had a markedly positive
RAST to TMI-HSA antigen.
It is apparent that further studies are
required to clarify the role of immuno-
logic mechanisms in TDI-induced
asthma. The heterogeneous immune re-
sponse should be explored further.
Moreover, the use of Afunctional iso-
cyanate as the antigen should be com-
pared with monofunctional isocyanate in
human, as well as in animal studies.
Diphenyl methane diisocyanate (MDI)
is less volatile than TDI is and has been
considered to be of low toxicity (126).
There are now several reports of asthma
and a hypersensitivity pneumonitis
related to MDI exposure (127-131). As
in TDI asthma, specific IgE antibodies
to MDI-protein conjugate were found in
only a small proportion of patients (1 of
6) (132). The prevalence of MDI asthma
among exposed subjects is unknown.
Johnson and coworkers (133) reported a
prevalence of 10.3% in a foundry with
78 employees.
Clinical studies with hexamethylene di-
4. . ^ r ' m * ' *
isocyanate (HDI) are even less common (131, 134). Occupational type broncho-provocation tests have indicated that there may be some cross-reactivity be-tween various isocyanates in the devel- Z7 ' opment of asthma (131). Crossed im-V munologic reactivities between these compounds have been found in a num-ber of studies (123, 124, .135). •
Anhydrides. Epoxy resins have many industrial uses including the manufacture of paints, plastics, and adhesives. The acid anhydrides—phthalic anhydride, trimellitic anhydride (TMA), and tetra-chlorophthalic anhydride (TCPA)- used in epoxy resin systems cause asthma. Oc-cupational bronchoprovocation tests have confirmed the development of asth-matic reaction after exposure to low con-centrations of these fumes or dusts (136). Specific IgE antibodies against phthalic anhydride protein conjugate had been demonstrated in the serum of affected workers (137).
Exposure to trimellitic anhydride can give rise to 4 clinical syndromes: symp-toms of airway irritation such as cough, immediate rhinitis and asthma, late asthma with systemic symptoms of fe-ver and malaise, arid infiltrative disease in the lung with hemoptysis and anemia (138, 139). Specific IgE antibodies */" TM A-protein conjugate have been fornV,. in some patients with immediate asthma and rhinitis (138). Specific IgG antibod-ies were found in those with late asthma or pulmonary disease-anemia syndrome as well as in exposed subjects without symptoms (138, 140). The pathogenesis of late asthma and pulmonary dis-ease-asthma syndrome is not clear.
Animal studies in rabbits and dogs showed that immunization by intrabron-chial instillation of TMA induced IgG antibodies to trimellityl-erythrocytes in both types of animals, indicating that the chemical probably reacts with one of the proteins in the airways to form the anti-gen (141).
In a longitudinal study of 64 workers exposed to trimellitic anhydride between 1977 and 1981, 6 workers had asthma-rhinitis and high levels of IgE antibod-ies. Five workers developed the late re-spiratory systemic syndrome, and 1 worker had both syndromes. Removal of the affected workers from exposure led to a decline of the level of antibodies in almost all of them (142).
Wood dusts. A large number of w<\ dusts are known to give rise to rhinitis and asthma after occupational exposure. The one that has been most extensively studied is western red cedar (T h u j a
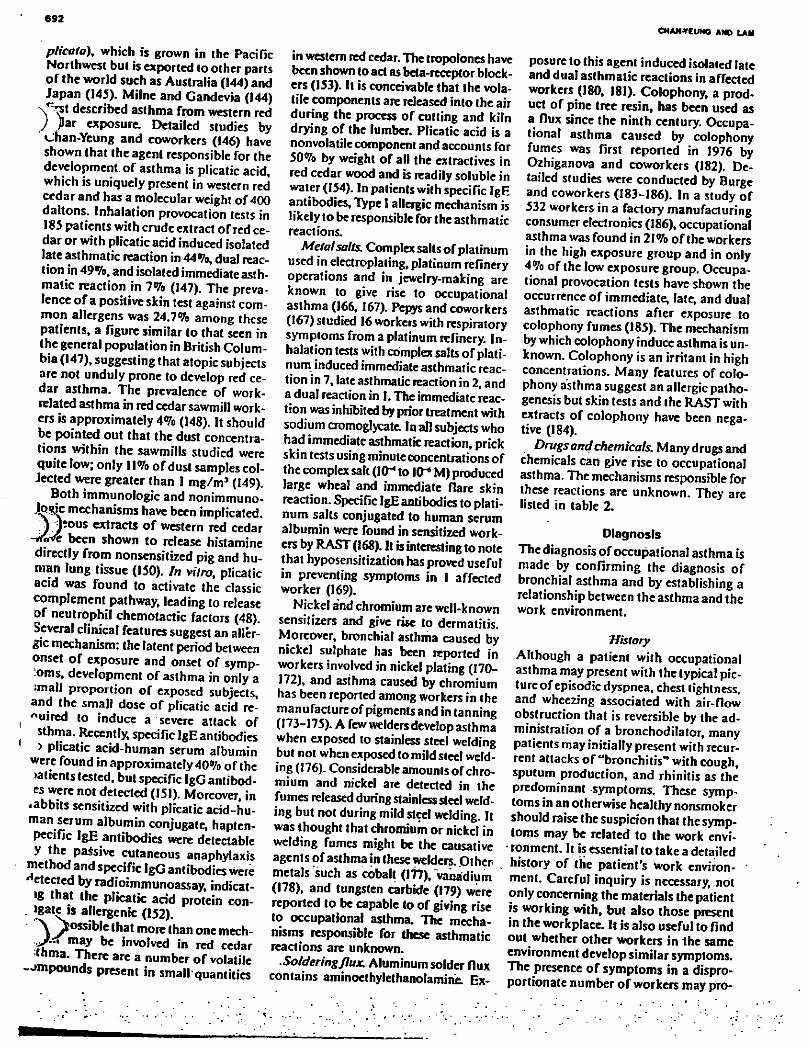
692
plicata), which is grown in thc Pacific
Northwest but is exported to other parts
of the world such as Australia (144) and
Japan (145). Milne and Gandevia (144)
described asthma from western red
J Jlar exposure: Detailed studies by
Chan-Yeung and coworkers (146) have
shown that the agent responsible for the
development of asthma is plicatic acid,
which is uniquely present in western red
cedar and has a molecular weight of 400
daltons. Inhalation provocation tests in
185 patients with crude extract of red ce-
dar or with plicatic acid induced isolated
late asthmatic reaction in 44%, dual reac-
tion in 49%, and isolated immediate asth-
matic reaction in 7% (147). The preva-
lence of a positive skin test against com-
mon allergens was 24.7% among these
patients, a figure similar to that seen in
the general population in British Colum-
bia (147), suggesting that atopic subjects
are not unduly prone to develop red ce-
dar asthma. Thc prevalence of work-
related asthma in red cedar sawmill work-
ers is approximately 4% (148). It should
be pointed out that the dust concentra-
tions within the sawmills studied were
quite low; only 11% of dust samples col-
Jected were greater than I mg/m3 (149).
Both immunologic and nonimmuno-
J-gSfc mechanisms have been implicated.
J JÎOUS extracts of western red cedar
- X f t been shown to release histamine
directly from nonsensitized pig and hu-
man lung tissue (150). In vitro, plicatic
acid was found to activate the classic
complement pathway, leading to release
of neutrophil chemotactic factors (48).
Several clinical features suggest an aller-
gic mechanism: the latent period between
onset of exposure and onset of symp-
:oms, development of asthma in only a
:mall proportion of exposed subjects,
and the small dose of plicatic acid re-
quired to induce a severe attack of
sthma. Recently, specific IgE antibodies
> plicatic acid-human serum albumin
were found in approximately 40% ofthe
>atients tested, but specific IgG antibod-
es were not detected (151). Moreover, in
•abbits sensitized with plicatic acid-hu-
man serum albumin conjugate, hapten-
Pccific IgE antibodies were detectable
y the passive cutaneous anaphylaxis
method and specific IgG antibodies were
etected by radioimmunoassay, indicat-
»g that the plicatic add protein con-
nate is allergenic (152).
\ possible that more than one mech-m a y be involved in red cedar
m a- T h c r e are a number of volatile
i m p o u n d s present in small quantities
in western red cedar. The tropolones have been shown to act as beta-receptor block-ers (153). It is conceivable that the vola-tile components are released into the air during the process of cutting and kiln drying of the lumber. Plicatic acid is a nonvolatile component and accounts for 50% by weight of all the extractives in red cedar wood and is readily soluble in water (154). In patients with specific IgE antibodies. Type I allergic mechanism is likely to be responsible for the asthmatic reactions.
Metalsalts. Complex salts of platinum
used in electroplating, platinum refinery
operations and in jewelry-making are
known to give rise to occupational
asthma (166, 167). Pepys and coworkers
(167) studied 16 workers with respiratory
symptoms from a platinum refinery. In-
halation tests with complex salts of plati-
num induced immediate asthmatic reac-
tion in 7, late asthmatic reaction in 2, and
a dual reaction in I. The immediate reac-
tion was inhibited by prior treatment with
sodium cromoglycate. In all subjects who
had immediate asthmatic reaction, prick
skin tests using minute concentrations of
the complex salt (10^ to 10^ M) produced
large wheal and immediate flare skin
reaction. Specific IgE antibodies to plati-
num salts conjugated to human serum
albumin were found in sensitized work-
ers by RAST (168). It is interesting to note
that hyposensitization has proved useful
in preventing symptoms in 1 affected
worker (169).
Nickel and chromium are well-known
sensitizers and give rise to dermatitis.
Moreover, bronchial asthma caused by
nickel sulphate has been reported in
workers involved in nickel plating (170-
172), and asthma caused by chromium
has been reported among workers in the
manu facture of pigments and in tanning
(173-175). A few welders develop asthma
when exposed to stainless steel welding
but not when exposed to mild steel weld-
ing (176). Considerable amounts of chro-
mium and nickel are detected in the
fumes released during stainless steel weld-
ing but not during mild steel welding. It
was thought that chromium or nickel in
welding fumes might be the causative
agents of asthma in these welders. Other
metals such as cobalt (177), vanadium
(178), and tungsten carbide (179) were
reported to be capable to of giving rise
to occupational asthma. The mecha-
nisms responsible for these asthmatic
reactions are unknown.
•Sofderingjlux. Aluminum solder flux contains aminoethylethanolamine. Ex-
CHAN-VEUMQ AND LAM
posure to this agent induced isolated late and dual asthmatic reactions in affected workers (180, 181). Colophony, a prod-uct of pine tree resin, has been used as a flux since the ninth century. Occupa-tional asthma caused by colophony fumes was first reported in 1976 by Ozhiganova and coworkers (182). De-tailed studies were conducted by Burge and coworkers (183-186). In a study of 532 workers in a factory manufacturing consumer electronics (186), occupational asthma was found in 21% ofthe workers in the high exposure group and in only 4% of the low exposure group. Occupa-tional provocation tests have shown the occurrence of immediate, late, and dual asthmatic reactions after exposure to colophony fumes (185). The mechanism by which colophony induce asthma is un-known. Colophony is an irritant in high concentrations. Many features of colo-phony asthma suggest an allergic patho-genesis but skin tests and the RAST with extracts of colophony have been nega-tive (184).
Drugs and chemicals. Many drugs and chemicals can give rise to occupational asthma. The mechanisms responsible for these reactions are unknown. They are listed in table 2.
Diagnosis The diagnosis of occupational asthma is made by confirming the diagnosis of bronchial asthma and by establishing a relationship between the asthma and the work environment.
;History
Although a patient with occupational
asthma may present with the typical pic-
ture of episodic dyspnea, chest tightness,
and wheezing associated with air-flow
obstruction that is reversible by the ad-
ministration of a bronchodilator, many
patients may initially present with recur-
rent attacks of "bronchitis" with cough,
sputum production, and rhinitis as the
predominant symptoms. These symp-
toms in an otherwise healthy nonsmoker
should raise the suspicion that the symp-
toms may be related to the work envi-
• ronment. It is essential to take a detailed
history of the patient's work environ-
ment. Careful inquiry is necessary, not
only concerning the materials the patient
is working with, but also those present
in the workplace. It is also useful to find
out whether other workers in the same
environment develop similar symptoms.
The presence of symptoms in a dispro-
portionate number of workers may pro-
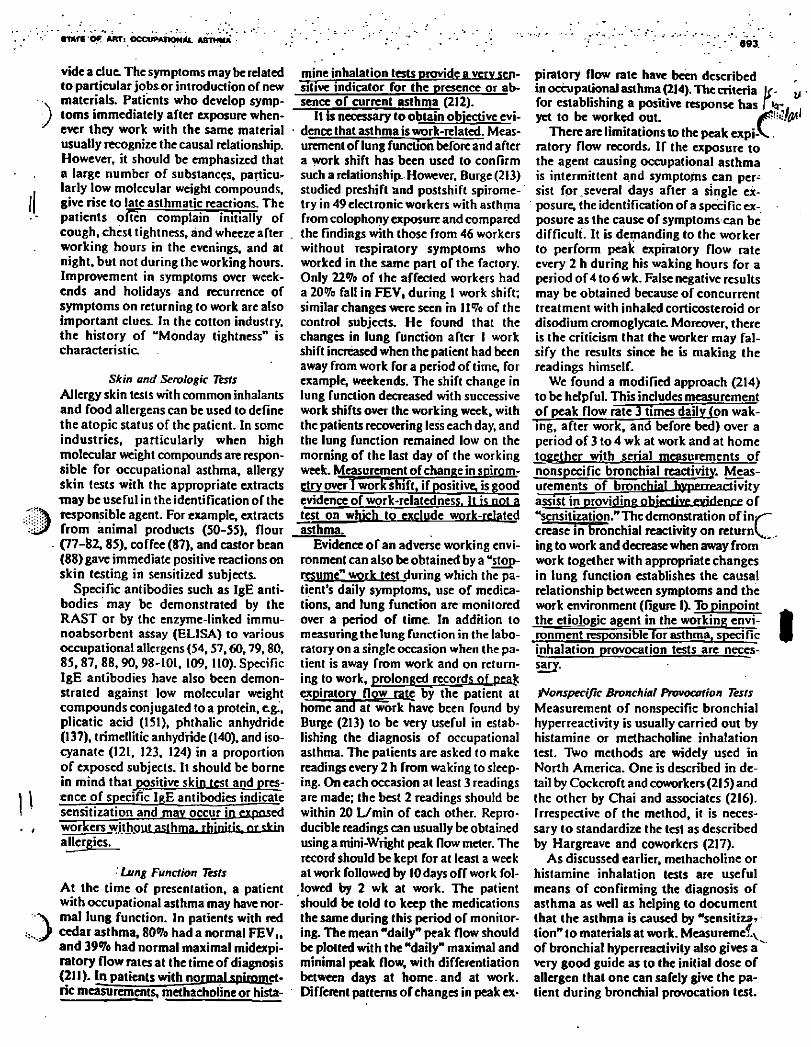
«art Of ART: OCCUPATION*. ASTHMA 693.
)
3
vide a due. The symptoms may be related to particular jobs.or introduction of new materials. Patients who develop symp-toms immediately after exposure when-ever they work with the same material usually recognize the causal relationship. However, it should be emphasized that a large number of substances, particu-larly low molecular weight compounds, give rise to late asthmatic reactions. The patients often complain initially of cough, chest tightness, and wheeze after working hours in the evenings, and at night, but not during the working hours. Improvement in symptoms over week-ends and holidays and recurrence of symptoms on returning to work are also important clues. In the cotton industry, the history of "Monday tightness" is characteristic.
Skin and Serologic Tests Allergy skin tests with common inhalants
and food allergens can be used to define
the atopic status of the patient. In some
industries, particularly when high
molecular weight compounds are respon-
sible for occupational asthma, allergy
skin tests with the appropriate extracts
may be useful in the identification of the
responsible agent. For example, extracts
from animal products (50-55), flour
(77-82,85), coffee (87), and castor bean
(88) gave immediate positive reactions on
skin testing in sensitized subjects.
Specific antibodies such as IgE anti-
bodies may be demonstrated by the
RAST or by the enzyme-linked immu-
noabsorbent assay (ELISA) to various
occupational allergens (54,57,60,79,80,
85,87, 88, 90, 98-101, 109,110). Specific
IgE antibodies have also been demon-
strated against low molecular weight
compounds conjugated to a protein, e.g.,
plicatic acid (151), phthalic anhydride
(137), trimellitic anhydride (140), and iso-
cyanate (121, 123, 124) in a proportion
of exposed subjects. It should be borne
in mind that positive skin test and pres-
ence of specific IgE antibodies indicate
sensitization and may occur ig p»pn*ed
workers without asthma. rhiPifîg. Pr gWïn
allergies.
Lung Function Tests At the time of presentation, a patient
with occupational asthma may have nor-
mal lung function. In patients with red
cedar asthma, 80% had a normal FEV„
and 39% had normal maximal midexpi-
ratory flow rates at the time of diagnosis
(211). In patients with normal spimmet-
ric measurements, methacholine or hista-
mine inhalation tests provide a very sen-
sitive indicator for the presence or ab-
sence of current asthma (212).
It is necessary to obtain objective evi-
dence that asthma is work-related. Meas-
urement of lung function before and after
a work shift has been used to confirm
such a relationship However, Burge (213)
studied preshift and post shift spirome-
try in 49 electronic workers with asthma
from colophony exposure and compared
the findings with those from 46 workers
without respiratory symptoms who
worked in the same part of the factory.
Only 22% of the affected workers had
a 20% fall in FEV, during 1 work shift;
similar changes were seen in 11% of the
control subjects. He found that the
changes in lung function after I work
shift increased when the patient had been
away from work for a period of time, for
example, weekends. The shift change in
lung function decreased with successive
work shifts over the working week, with
the patients recovering less each day, and
the lung function remained low on the
morning of the last day of the working
week. Measurement of change in spirom-
etry over j work shift, if positive, is good
evidence of work-relatedness. It is not a
test on which to exclude work-related
asthma.
Evidence of an adverse working envi-
ronment can also be obtained by a "stop-
resume" work test during which the pa-
tient's daily symptoms, use of medica-
tions, and lung function are monitored
over a period of time. In addition to
measuring the lung function in the labo-
ratory on a single occasion when the pa-
tient is away from work and on return-
ing to work, prolonged records nf peak
expiratory flow rate by the patient at
home and at work have been found by
Burge (213) to be very useful in estab-
lishing the diagnosis of occupational
asthma. The patients are asked to make
readings every 2 h from waking to sleep-
ing. On each occasion at least 3 readings
are made; the best 2 readings should be
within 20 L/min of each other. Repro-
ducible readings can usually be obtained
using a mini-Wright peak flow meter. The
record should be kept for at least a week
at work followed by 10 days off work fol-
lowed by 2 wk at work. The patient
should be told to keep the medications
the same during this period of monitor-
ing. The mean "daily" peak flow should
be plotted with the "daily" maximal and
minimal peak flow, with differentiation
between days at home, and at work.
Different patterns of changes in peak ex-
piratory flow rate have been described in occupational asthma (214). The criteria u
for establishing a positive response has l k r g
yet to be worked out. J&'-u-ffi/li There are limitations to the peak expi-V
ratory flow records, If the exposure to the agent causing occupational asthma is intermittent and symptoms can per-sist for.several days after a single ex-posure, the identification of a specific ex-posure as the cause of symptoms can be difficult. It is demanding to the worker to perform peak expiratory flow rate every 2 h during his waking hours for a period of 4 to 6 wk. False negative results may be obtained because of concurrent treatment with inhaled corticosteroid or disodium cromoglycate. Moreover, there is the criticism that the worker may fal-sify the results since he is making the readings himself.
We found a modified approach (214) to be helpful. This includes measurement of peak flow rate 3 times daily (on wak-ing, after work, and before bed) over a period of 3 to 4 wk at work and at home together with serial measurements of nonspecific bronchial reactivity. Meas-urements of bronchi?! hypMTffartivîfy assist in providing ofrjfcfive evidence of "sensitization." The demonstration of inx"~ crease in bronchial reactivity on returnV^. ing to work and decrease when away from work together with appropriate changes in lung function establishes the causal relationship between symptoms and the work environment (figure 1). To pinpoint the etiologic agent in the working envi- • ronment responsible for asthma, specific ^ inhalation provocation tests are neces-sary.
iNonspecific Bronchial Provocation Tests Measurement of nonspecific bronchial
hyperreactivity is usually carried out by
histamine or methacholine inhalation
test. Two methods are widely used in
North America. One is described in de-
tail by Cockcroft and coworkers (215) and
the other by Chai and associates (216).
Irrespective of the method, it is neces-
sary to standardize the test as described
by Hargreave and coworkers (217).
As discussed earlier, methacholine or
histamine inhalation tests are useful
means of confirming the diagnosis of
asthma as well as helping to document
that the asthma is caused by "sensitiza?
tion" to materials at work. Measuremef.y
of bronchia] hyperreactivity also gives a "
very good guide as to the initial dose of
allergen that one can safely give the pa-
tient during bronchial provocation test.
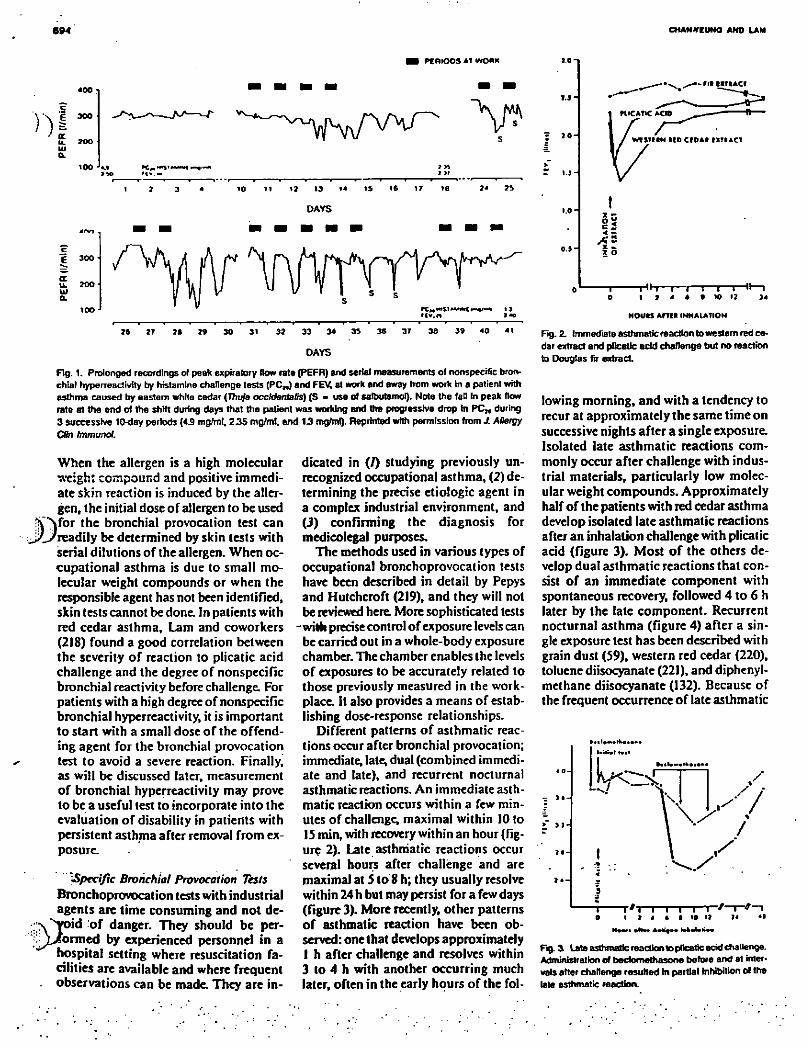
694 CHANJTEUMO ANO LAM
PC mOOS Ai WORK
' rr
300
100
«2 13
0AYS
4<V)
c E 300 ^
a u. ?oo ui Q.
too
76 27 76 23 30 3» 32 33 34 35
DAYS
37 36 39 40 41
Fig. 1. Prolonged recordings of peak expiratory Row rate (PEFR) and serial measurements ol nonspecific bron-chial hyperreactivity by histamine challenge tests (PC») and FEV, at work and away from work in a patient with asthma caused by eastern white cedar {Thuja occIdentafis) (S - use of satbutamol). Note the fat] In peak flow rate at the end of the shift during days that the patient was working and the progressive drop in PC„ during 3 successive ItMJay periods (43 mg/m!, 235 mg/mt, end 13 mgfrnl). Reprinted with permission from J. ABergy
CBn Immunol.
When the allergen is a high molecular
weight compound and positive immedi-
ate skin reaction is induced by the aller-
gen, the initial dose of allergen to be used
for the bronchial provocation test can
readily be determined by skin tests with
serial dilutions of the allergen. When oc-
cupational asthma is due to small mo-
lecular weight compounds or when the
responsible agent has not been identified,
skin tests cannot be done In patients with
red cedar asthma, Lam and coworkers
(218) found a good correlation between
the severity of reaction to plicatic acid
challenge and the degree of nonspecific
bronchial reactivity before challenge. For
patients with a high degree of nonspecific
bronchial hyperreactivity, it is important
to start with a small dose of the offend-
ing agent for the bronchial provocation
test to avoid a severe reaction. Finally,
as will be discussed later, measurement
of bronchial hyperreactivity may prove
to be a useful test to incorporate into the
evaluation of disability in patients with
persistent asthma after removal from ex-
posure.
]SpeciJic Brorichiol Provocation Tests Bronchoprovocation tests with industrial
agents are time consuming and not de-
x'^void o f danger. They should be per-
^Y-/ormed by experienced personnel in a
hospital setting where resuscitation fa-
cilities are available and where frequent
observations can be made. They are in-
dicated in (/) studying previously un-
recognized occupational asthma, (2) de-
termining the precise etiologic agent in
a complex industrial environment, and
(3) confirming the diagnosis for
medicolegal purposes.
The methods used in various types of
occupational bronchoprovocation tests
have been described in detail by Pepys
and Hutchcroft (219), and they will not
be reviewed here. More sophisticated tests
with precise control of exposure levels can
be carried out in a whole-body exposure
chamber. The chamber enables the levels
of exposures to be accurately related to
those previously measured in the work-
place. It also provides a means of estab-
lishing dose-response relationships.
Different patterns of asthmatic reac-
tions occur after bronchial provocation;
immediate, late, dual (combined immedi-
ate and late), and recurrent nocturnal
asthmatic reactions. An immediate asth-
matic reaction occurs within a few min-
utes of challenge, maximal within 10 to
15 min, with recovery within an hour (fig-
ure 2). Late asthmatic reactions occur
several hourç after challenge and are
maxima) at 5 to 8 h; they usually resolve
within 24 h but may persist for a few days
(figure 3). More recently, other patterns
of asthmatic reaction have been ob-
served: one that develops approximately
1 h after challenge and resolves within
3 to 4 h with another occurring much
later, often in the early hours of the fol-
z o
•Hh—i—i—i—I—I—11—i
HOUtS Ami INHALATION
Fig. 2. Immediate asthmatic reaction to western red ce-dar extract and pfcatlc add challenge but no reaction to Douglas fir extract.
lowing morning, and with a tendency to
recur at approximately the same time on
successive nights after a single exposure.
Isolated late asthmatic reactions com-
monly occur after challenge with indus-
trial materials, particularly low molec-
ular weight compounds. Approximately
half of the patients with red cedar asthma
develop isolated late asthmatic reactions
after an inhalation challenge with plicatic
acid (figure 3). Most of the others de-
velop dual asthmatic reactions that con-
sist of an immediate component with
spontaneous recovery, followed 4 to 6 h
later by the late component. Recurrent
nocturnal asthma (figure 4) after a sin-
gle exposure test has been described with
grain dust (59), western red cedar (220),
toluene diisocyanate (221), and diphenyl-
methane diisocyanate (132). Because of
the frequent occurrence of late asthmatic
Iftill H|f
Jy^
I i i /—r-*—i T ' T i j * t i to » i*
Fig. & Late asthmatic reaction to plicatic acid challenge. Administration of bedomethasone before and at inter-vals after challenge resulted in partial inhibition of the late asthmatic reaction.
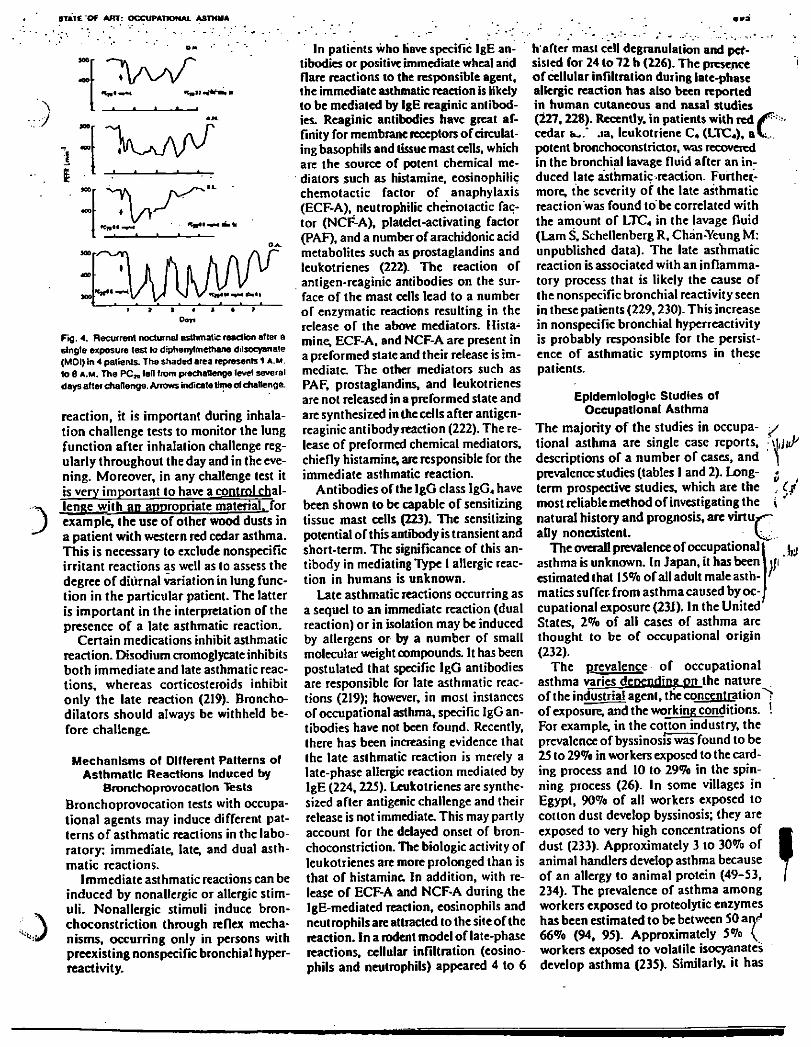
STATE O f AITT: OCCUPATIONAL ASTHMA
• «
« » » ' *
v K n l N ^ M C a t l
Dap
Fig. 4. Recurrent nocturnal asthmatic reaction alter a 6ingte exposure test to diphenylmethane diisocyanate (MOI) in 4 patients. The shaded area represents 1 A.M. to 6 A.M. The P C „ fen Irom prechallenge level several days after challenge. Arrows indicate time of challenge.
reaction, it is important during inhala-
tion challenge tests to monitor the lung
function after inhalation challenge reg-
ularly throughout the day and in the eve-
ning. Moreover, in any challenge test it
is very important to have acontrol chal-
lenge with an appropriate material. for
example, the use of other wood dusts in
a patient with western red cedar asthma.
This is necessary to exclude nonspecific
irritant reactions as well as to assess the
degree of diurnal variation in lung func-
tion in the particular patient. The latter
is important in the interpretation of the
presence of a late asthmatic reaction.
Certain medications inhibit asthmatic
reaction. Disodium cromoglycate inhibits
both immediate and late asthmatic reac-
tions, whereas corticosteroids inhibit
only the late reaction (219). Broncho-
dilators should always be withheld be-
fore challenge.
Mechanisms of Different Patterns of Asthmatic Reactions Induced by
Bronchoprovocation Tests Bronchoprovocation tests with occupa-
tional agents may induce different pat-
terns of asthmatic reactions in the labo-
ratory: immediate, late, and dual asth-
matic reactions. Immediate asthmatic reactions can be
induced by nonallergic or allergic stim-
uli. Nonallergic stimuli induce bron-
choconstriction through reflex mecha-
nisms, occurring only in persons with
preexisting nonspecific bronchial hyper-
reactivity.
In patients who Have specific IgE an-
tibodies or positive immediate wheal and
flare reactions to the responsible agent,
the immediate asthmatic reaction is likely
to be mediated by IgE reaginic antibod-
ies. Reaginic antibodies have great af-
finity for membrane receptors of circulat-
ing basophils and tissue mast cells, which
are the source of potent chemical me-
diators such as histamine, eosinophilic
chemotactic factor of anaphylaxis
(ECF-A), neutrophilic chemotactic fac-
tor (NCF-A), platdet-activating factor
(PAF), and a number of arachidonic acid
metabolites such as prostaglandins and
leukotrienes (222). The reaction of
antigen-reaginic antibodies on the sur-
face of the mast cells lead to a number
of enzymatic reactions resulting in the
release of the above mediators. Hista-
mine, ECF-A, and NCF-A are present in
a preformed state and their release is im-
mediate. The other mediators such as
PAF, prostaglandins, and leukotrienes
are not released in a preformed stale and
are synthesized in the cells after antigen-
reaginic antibody reaction (222). The re-
lease of preformed chemical mediators,
chiefly histamine, are responsible for the
immediate asthmatic reaction.
Antibodies of the IgG class IgG, have
been shown to be capable of sensitizing
tissue mast cells (223). The sensitizing
potential of this antibody is transient and
short-term. The significance of this an-
tibody in mediating Type 1 allergic reac-
tion in humans is unknown.
Late asthmatic reactions occurring as
a sequel to an immediate reaction (dual
reaction) or in isolation may be induced
by allergens or by a number of small
molecular weight compounds. It has been
postulated that specific IgG antibodies
are responsible for late asthmatic reac-
tions (219); however, in most instances
of occupational asthma, specific IgG an-
tibodies have not been found. Recently,
there has been increasing evidence that
the late asthmatic reaction is merely a
late-phase allergic reaction mediated by
IgE (224,225). Leukotrienes are synthe-
sized after antigenic challenge and their
release is not immediate. This may partly
account for the delayed onset of bron-
choconstriction. The biologic activity of
leukotrienes are more prolonged than is
that of histamine. In addition, with re-
lease of ECF-A and NCF-A during the
IgE-mediated reaction, eosinophils and
neutrophils are attracted to the site of the
reaction. In a rodent model of late-phase
reactions, cellular infiltration (eosino-
phils and neutrophils) appeared 4 to 6
h'after mast cell degranulation and per-sisted for 24 to 72 h (226). The presence of cellular infiltration during late-phase allergic reaction has also been reported in human cutaneous and nasal studies (227,228). Recently, in patients with red cedar fc-.* .ia, leukotriene C4 (LTC„), a V . potent bronchoconstrictor, was recovered in the bronchial lavage fluid after an in-duced late asthmatic reaction. Further-more, the severity of the late asthmatic reaction was found to be correlated with the amount of LTC4 in the lavage fluid (Lam S, Schellenberg R, Chàn-Yeung M: unpublished data). The late asthmatic reaction is associated with an inflamma-tory process that is likely the cause of the nonspecific bronchial reactivity seen in these patients (229,230). This increase in nonspecific bronchial hyperreactivity is probably responsible for the persist-ence of asthmatic symptoms in these patients.
Epidemiologic Studies of Occupational Asthma
The majority of the studies in occupa-
tional asthma are single case reports,
descriptions of a number of cases, and
prevalence studies (tables 1 and 2). Long-
term prospective studies, which are the
most reliable method of investigating the
natural history and prognosis, are virtu
ally nonexistent.
The overall prevalence of occupational
asthma is unknown. In Japan, it has been
estimated that 15% of all adult male asth-
matics suffer- from asthma caused by oc-
cupational exposure (23J). In the United
States, 2% of all cases of asthma are
thought to be of occupational origin
(232).
The prevalence of occupational
asthma varies depending on the nature
of the industrial agent, the concentration
of exposure, and the working conditions.
For example, in the cotton industry, the
prevalence of byssinosis was found to be
25 to 29% in workers exposed to the card-
ing process and 10 to 29% in the spin-
ning process (26). In some villages in
Egypt, 90% of all workers exposed to
cotton dust develop byssinosis; they are
exposed to very high concentrations of
dust (233). Approximately 3 to 30% of
animal handlers develop asthma because
of an allergy to animal protein (49-53,
234). The prevalence of asthma among
workers exposed to proteolytic enzymes
has been estimated to be between 50 anr1
66% (94, 95). Approximately 5% {
workers exposed to volatile isocyanates
develop asthma (235). Similarly, it has
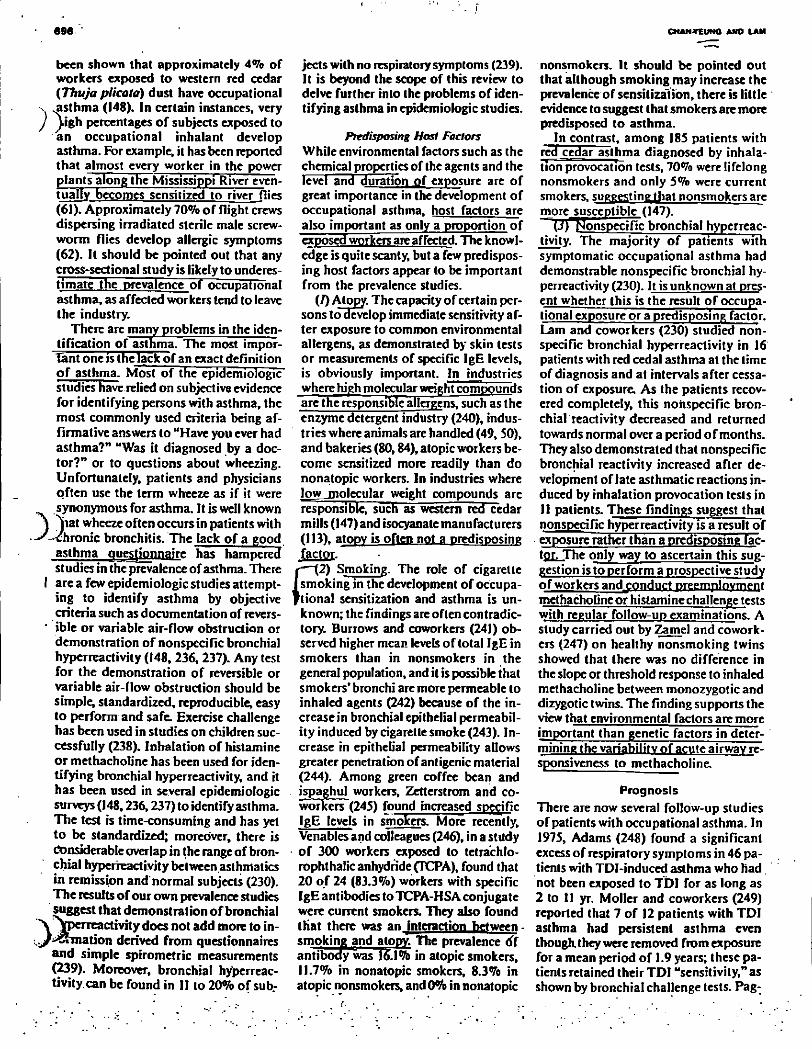
696 CHAN4TEUN0 AND LAM
been shown that approximately 4% of
workers exposed to western red cedar
(Thuja plicata) dust have occupational
v .asthma (148). In certain instances, very
J \igh percentages of subjects exposed to
an occupational inhalant develop
asthma. For example, it has been reported
that almost every worker in the power
plants along the Mississippi River even-
tually becomes sensitized to river flies
(61). Approximately 70% of flight crews
dispersing irradiated sterile male screw-
worm flies develop allergic symptoms
(62). It should be pointed out that any
cross-sectional study is likely to underes-
timate the prevalence of occupational
asthma, as affected workers tend to leave
the industry.
There are many problems in the iden-
tification of asthma. The most impor-
Tant one is the lack of an exact definition
of asthma. Most of the epidemiologic
studies have relied on subjective evidence
for identifying persons with asthma, the
most commonly used criteria being af-
firmative answers to "Have you ever had
asthma?" "Was it diagnosed by a doc-
tor?" or to questions about wheezing.
Unfortunately, patients and physicians
often use the term wheeze as if it were
synonymous for asthma. It is well known
) ^jiat wheeze often occurs in patients with
-'-chronic bronchitis. The lack of a good
asthma questionnaire has hampered
studies in the prevalence of asthma. There
I are a few epidemiologic studies attempt-
ing to identify asthma by objective
criteria such as documentation of revers-
' ible or variable air-flow obstruction or
demonstration of nonspecific bronchial
hyperreactivity (148, 236, 237). Any test
for the demonstration of reversible or
variable air-flow obstruction should be
simple; standardized, reproducible, easy
to perform and safe: Exercise challenge
has been used in studies on children suc-
cessfully (238). Inhalation of histamine
or methacholine has been used for iden-
tifying bronchial hyperreactivity, and it
has been used in several epidemiologic
surveys (148,236,237) to identify asthma.
The test is time-consuming and has yet
to be standardized; moreover, there is
Considerable overlap in the range of bron-
chial hyperreactivity between asthmatics
in remission and'normal subjects (230).
The results of our own prevalence studies
suggest that demonstration of bronchial
" V jpcireactivity does not add more to in-
! > ; / ^ m a t i o n derived from questionnaires
and simple spirometric measurements
(239). Moreover, bronchial hyperreac-
tivity, can be found in II to 20% of sub-
jects with no respiratory symptoms (239). It is beyond the scope of this review to delve further into the problems of iden-tifying asthma in epidemiologic studies.
Predisposing Host Factors White environmental factors such as the
chemical properties of the agents and the
level and duration of exposure are of
great importance in the development of
occupational asthma, host factors are
also important as only a proportion of
exposed workers are affected. The knowl-
edge is quite scanty, but a few predispos-
ing host factors appear to be important
from the prevalence studies.
(I) Atopy. The capacity of certain per-
sons to develop immediate sensitivity af-
ter exposure to common environmental
allergens, as demonstrated by skin tests
or measurements of specific IgE levels,
is obviously important. In industries
where hiph molecular weight compounds
are the responsible allergens, such as the
enzyme detergent industry (240), indus-
tries where animals are handled (49, SO),
and bakeries (80,84), atopic workers be-
come sensitized more readily than do
nonatopic workers. In industries where
low _Diolecular weight compounds are
responsible, such as western red cedar
mills (147) and isocyanate manufacturers
(113), atopy is often not a predisposing
factor.
r—(2) Smoking. The role of cigarette
I smoking in the development of occupa-
t i o n a l sensitization and asthma is un-
known; the findings are often contradic-
tory. Burrows and coworkers (241) ob-
served higher mean levels of total IgE in
smokers than in nonsmokers in the
general population, and it is possible that
smokers' bronchi are more permeable to
inhaled agents (242) because of the in-
crease in bronchial epithelial permeabil-
ity induced by cigarette smoke (243). In-
crease in epithelial permeability allows
greater penetration of antigenic material
(244). Among green coffee bean and
ispaghul workers, Zetterstrom and co-
workers (245) found increased specific
IgE levels in smokers. More recently.
Venables and colleagues (246), in a study
• of 300 workers exposed to tetra'chlo-
rophthalic anhydride (TCPA), found that
20 of 24 (83.3%) workers with specific
IgE antibodies to TCPA-HSA conjugate
were current smokers. They also found
that there was an jnteraction between •
smoking and atopy. The prevalence df
antibody was 16.1% in atopic smokers,
11.7% in nonatopic smokers, 8.3% in
atopic nonsmokers, and 0% in nonatopic
nonsmokers. It should be pointed out
that although smoking may increase the
prevalence of sensitization, there is little
evidence to suggest that smokers are more
predisposed to asthma.
In contrast, among 185 patients with
red cedar asthma diagnosed by inhala-
tion provocation tests, 70% were lifelong
nonsmokers and only 5% were current
smokers, su^g^ting tfiat nonsmokers are
more susceptible ( 147).
(J)T^onspecific bronchial hyperreac-
tivity. The majority of patients with
symptomatic occupational asthma had
demonstrable nonspecific bronchial hy-
perreactivity (230). It is unknown at pres-
ent whether this is the result of occupa-
tional exposure or a predisposing factor.
Lam and coworkers (230) studied non-
specific bronchial hyperreactivity in 16
patients with red cedal asthma at the time
of diagnosis and at intervals after cessa-
tion of exposure. As the patients recov-
ered completely, this nonspecific bron-
chiaLreactivity decreased and returned
towards normal overa period of months.
They also demonstrated that nonspecific
bronchial reactivity increased after de-
velopment of late asthmatic reactions in-
duced by inhalation provocation tests in
11 patients. These findings suggest that
nonspecific hyperreactivity is a result of
exposure rather than a predisposing fac-
tpr. The only way to ascertain this sug-
gestion is to perform a prospective study
of workers andjonduct preemplnvmpqt methacholine or histamine challenge tests
with regular follow-up examinations. A
study carried out by Zamel and cowork-
ers (247) on healthy nonsmoking twins
showed that there was no difference in
the slope or threshold response to inhaled
methacholine between monozygotic and
dizygotic twins. The finding supports the
view that environmental factors are more
important than genetic factors in deter-
mining the variability of acute airway re-
sponsiveness to methacholine.
Prognosis There are now several follow-up studies
of patients with occupational asthma. In
1975, Adams (248) found a significant
excess of respiratory symptoms in 46 pa-
tients with TDI-induced asthma who had
not been exposed to TDI for as long as
2 to II yr. Moller and coworkers (249)
reported that 7 of 12 patients with TDI
asthma had persistent asthma even
though they were removed from exposure
for a mean period of 1.9 years; these pa-
tients retained their TDI "sensitivity," as
shown by bronchial challenge tests. Pag-
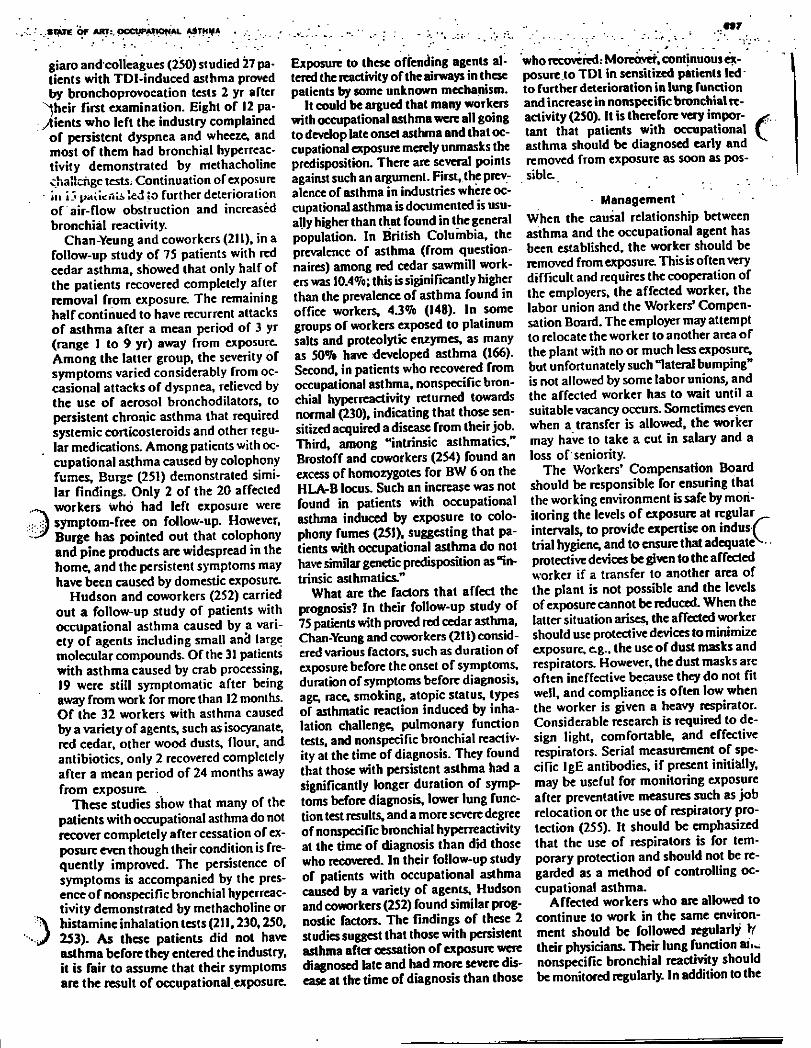
.SIXTE OF ART:. pCCUPApOff AL AATM* A 97
giaro andcolleagues (250) studied 27 pa-
tients with TDI-induced asthma proved
by bronchoprovocation tests 2 yr after
^heir first examination. Eight of 12 pa-
yments who left the industry complained
of persistent dyspnea and wheeze, and
most of them had bronchial hyperreac-
tivity demonstrated by methacholine
challenge tests. Continuation of exposure
' 111 i-t prtilCMU» led to further deterioration
of air-flow obstruction and increased
bronchial reactivity.
Chan-Yeung and coworkers (211), in a
follow-up study of 75 patients with red
cedar asthma, showed that only half of
the patients recovered completely after
removal from exposure The remaining
half continued to have recurrent attacks
of asthma after a mean period of 3 yr
(range 1 to 9 yr) away from exposure.
Among the latter group, the severity of
symptoms varied considerably from oc-
casional attacks of dyspnea, relieved by
the use of aerosol bronchodilators, to
persistent chronic asthma that required
systemic corticosteroids and other regu-
lar medications. Among patients with oc-
cupational asthma caused by colophony
fumes, Burge (251) demonstrated simi-
lar findings. Only 2 of the 20 affected
workers who had left exposure were
; J symptom-free on follow-up. However,
Burge has pointed out that colophony
and pine products are widespread in the
home, and the persistent symptoms may
have been caused by domestic exposure.
Hudson and coworkers (252) carried
out a follow-up study of patients with
occupational asthma caused by a vari-
ety of agents including small ancl large
molecular compounds. Of the 31 patients
with asthma caused by crab processing,
19 were still symptomatic after being
away from work for more than 12 months.
O f the 32 workers with asthma caused
by a variety of agents, such as isocyanate,
red cedar, other wood dusts, flour, and
antibiotics, only 2 recovered completely
after a mean period of 24 months away
from exposure. .
These studies show that many of the
patients with occupational asthma do not
recover completely after cessation of ex-
posure even though their condition is fre-
quently improved. The persistence of
symptoms is accompanied by the pres-
ence of nonspecific bronchial hyperreac-
tivity demonstrated by methacholine or
) histamine inhalation tests (211,230,250,
253). As these patients did not have
asthma before they entered the industry,
it is fair to assume that their symptoms
are the result of occupational exposure.
Exposure to these offending agents al-
tered the reactivity of thc airways in these
patients by some unknown mechanism.
It could be argued that many workers
with occupational asthma were all going
to develop late onset asthma and that oc-
cupational exposure merely unmasks the
predisposition. There are several points
against such an argument. First, the prev-
alence of asthma in industries where oc-
cupational asthma is documented is usu-
ally higher than that found in the general
population. In British Columbia, the
prevalence of asthma (from question-
naires) among red cedar sawmill work-
ers was 10.4%; this is sigjnificantly higher
than the prevalence of asthma found in
office workers, 43% (148). In some
groups of workers exposed to platinum
salts and proteolytic enzymes, as many
as 50% have developed asthma (166).
Second, in patients who recovered from
occupational asthma, nonspecific bron-
chial hyperreactivity returned towards
normal (230), indicating that those sen-
sitized acquired a disease from their job.
Third, among "intrinsic asthmatics,"
Brostoff and coworkers (254) found an
excess of homozygotes for BW 6 on the
HLA-B locus. Such an increase was not
found in patients with occupational
asthma induced by exposure to colo-
phony fumes (251), suggesting that pa-
tients with occupational asthma do not
have similar genetic predisposition as "in-
trinsic asthmatics."
What are the factors that affect the
prognosis? In their follow-up study of
75 patients with proved red cedar asthma,
Chan-Yeung and coworkers (211) consid-
ered various factors, such as duration of
exposure before the onset of symptoms,
duration of symptoms before diagnosis,
age, race, smoking, atopic status, types
of asthmatic reaction induced by inha-
lation challenge, pulmonary function
tests, and nonspecific bronchial reactiv-
ity at the time of diagnosis. They found
that those with persistent asthma had a
significantly longer duration of symp-
toms before diagnosis, lower lung func-
tion test results, and a more severe degree
of nonspecific bronchial hyperreactivity
at the time of diagnosis than did those
who recovered. In their follow-up study
of patients with occupational asthma
caused by a variety of agents, Hudson
and coworkers (252) found similar prog-
nostic factors. The findings of these 2
studies suggest that those with persistent
asthma after cessation of exposure were
diagnosed late and had more severe dis-
ease at the time of diagnosis than those
who recovered: Moreover, continuous ex-posure to TDI in sensitized patients led' to further deterioration in lung function and increase in nonspecific bronchial re-activity (250). It is therefore very impor- > tant that patients with occupational ( asthma should be diagnosed early and removed from exposure as soon as pos-sible.
Management When the causal relationship between
asthma and the occupational agent has
been established, the worker should be
removed from exposure. This is often very
difficult and requires the cooperation of
the employers, the affected worker, the
labor union and the Workers' Compen-
sation Board. The employer may attempt
lo relocate the worker to another area of
the plant with no or much less exposure,
but unfortunately such "lateral bumping"
is not allowed by some labor unions, and
the affected worker has to wait until a
suitable vacancy occurs. Sometimes even
when a transfer is allowed, the worker
may have to take a cut in salary and a
loss of seniority.
The Workers' Compensation Board
should be responsible for ensuring that
the working environment is safe by mon-
itoring the levels of exposure at regular
intervals, to provide expertise on indus/
trial hygiene, and to ensure that adequate^
protective devices be given to the affected
worker if a transfer to another area of
the plant is not possible and the levels
of exposure cannot be reduced. When the
latter situation arises, the affected worker
should use protective devices to minimize
exposure, e.g., the use of dust masks and
respirators. However, the dust masks are
often ineffective because they do not fit
well, and compliance is often low when
the worker is given a heavy respirator.
Considerable research is required to de-
sign light, comfortable, and effective
respirators. Serial measurement of spe-
cific IgE antibodies, if present initially,
may be useful for monitoring exposure
after preventative measures such as job
relocation or the use of respiratory pro-
tection (255). It should be emphasized
that the use of respirators is for tem-
porary protection and should not be re-
garded as a method of controlling oc-
cupational asthma.
Affected workers who arc allowed to
continue to work in the same environ-
ment should be followed regularly ff
their physicians. Their lung function ai...
nonspecific bronchial reactivity should
be monitored regularly. In addition to the
698 CMAN-VCUNQ AMD LAM
use of respirators, they may require the use of prophylactic medications such as disodium cromoglycate, beclomcthasone dipropionate, and beta-adrenergic agon--
\ « t . However, at the present time, there / ) no data to show that prophylactic medi-
cations prevent the development of chronic persistent asthma.
Treatment of acute episodes of occupa-tional asthma does not differ from that of any acute attack of asthma. Sympto-matic relief of mild attacks is often pro-duced by beta-adrenergic agonists in aerosol form. Xanthine derivatives such as theophylline may be added. In severe and prolonged attacks, systemic corti-costeroids may be necessary. Whenever possible; topical steroids such as be-clomethasone should be substituted for systemic corticosteroids.
Hyposensitization has been attempted with certain occupational allergens, eg., complex salts of platinum, which was successful in preventing asthmatic reac-tions in a chemist (169). Such an ap-proach is not feasible when allergic fac-tors are not involved in the pathogenesis.
Prevention There are a number of considerations in the prevention of occupational asthma.
«.•^Efficient environmental control of pro-J Jsses involving sensitization materials
is the most important one It has been documented that the initial development of asthma among workers exposed to TDI is often associated with accidents.
I in which the workers may be exposed to relatively hiflh concentrations of the
• chemical. Institution of safety measures t concerning handling procedures, avoid-
ance of spills, good housekeeping, and education of the workers about these measures are important. There are very few studies relating to the level of ex- | posure to sensitizing materials and sub-sequent development of occupational asthma. This is the most urgent area re-quiring research.
Consideration should be given to
I changes in product formulation when-ever possible. For example, in the deter-gent enzyme industry, encapsulation of the proteolytic enzyme portion of the product reduced the exposure of the
• . workers. Reduction of exposure has dra-matically reduced the proportion of workers becoming sensitized in the en-« m e detergent industry (256). J Substitution of a harmful material by
«/ 'an innocuous one should be considered. This has not been successful in the use
of MDI in replacing TDI, as MDI also causes occupational asthma (132).
Identifigtfion of susceptible workers is another way of preventing occupa-tional asthma. Unfortunately, as dis-cussed earlier, very little is known in this area. Atopy may be an important pre-disposing factor in occupational asthma caused by high molecular weight com-pounds but not in occupational asthma caused by low molecular weight com-pounds. The role of cigarette smoking and nonspecific brpnchial hyperreac-tivity is still uncertain.
Summary and Future Research More than 200 organic and inorganic compounds are known to cause occupa-tional asthma. With the introduction of new materials into the industry, the list will continue to grow. Although consid-erable advances have been made in the last 3 decades, especially in the area of diagnosis of occupational asthma, there are considerable gaps in our knowledge that require further investigation.
The prevalence of asthma in various occupational settings is largely unknown.
. Proper epidemiologic assessment of oc-cupational asthma requires a multidis-ciplinary approach that combines the ef-forts of epidemiologists, immunologists, pulmonary physicians, industrial hygien-ists, chemists, and toxicologists. More-over, occupational epidemiologic studies require the cooperation of management, labor, and governmental regulatory agen-cies.
^TThe techniques currently availablein identifying subjects with asthma in epi-demiologic studies are not satisfactory. There is no validated oiipstinnnaire tor eyaluaiiDK-asthma or occupational asth-ma, although such a questionnaire is pre-sently being validated {257). Cross-sectional prevalence studies are lively to underestimate the true prevalence of oc-cupational asthma as workers who de-velop asthma tend to leave the industry. Prospective studies should be designed «to answer the following questions. (/) 'What is the incidence of occupational asthma in the industry? (2) Is there a dose relationship in sensitization? Can one de-termine the level of exposure below which no one becomes sensitized? (J) Whqt are the predisposing host factors? {4) Can affected workers return to the same job with reduced levels of exposure without detriment to their health?
The use of methacholine or histamine challenge tests in the field to identify sub-
jects with asthma should be properly as-sessed. Preliminary data from our studies indicate that it may not add further in-formation to a well-designed question-naire (239). Whether nonspecific bron-chial hyperreactivity is a predisposing host factor in occupational asthma can only be answered by a prospective study with preemployment examination.
The methods used in confirmation of the diagnosis of occupational asthma are also unsatisfactory. Specific provocation tests are time-consuming and not with-out discomfort to the patients. The use of peak expiratory flow rates 3 to 4 times a day in addition to recording of symp-toms and serial measurements of non-specific bronchial reactivity in establish-ing the work relationship needs to be studied more vigorously to determine the criteria of positive response and to com-pare the results with specific bronchial provocation tests. Research should be carried out to develop immunologic means of confirming sensitization to oc-cupational agents.
There is at present a lack of criteria for assessment of functional impairment caused by occupational asthma. The rec-ommendation for evaluation of impair-ment/disability secondary to respiratory disease is applicable only to patients with pneumoconiosis with a restrictive ventila-tory defect such as asbestosis or silicosis or irreversible chronic obstructive lung disease. This set of criteria is inappropri-ate for a patient with asthma who has variable air-flow obstruction and may have relatively normal lung function while taking a number of medications in-cluding systemic corticosteroids. In es-tablishing such criteria, it is important to take into consideration not only lung function but also the degree of non-specific bronchial hyperreactivity and tlie amount of medications necessary lor the control of asthma even when the patient is no longer cxposea to the etiofogic agent.
The pathogenetic mechanisms under-lying many causes of asthma and occupa-tional asthma are unknown. The mech-anism of the late asthmatic reaction and nonspecific bronchial hyperreactivity are not well understood. More direct means of examining the processes that initiate the asthmatic reaction and nonspecific bronchial reactivity are necessary.. One approach is the use of bronchial lavage and bronchial biopsy to study the mor-phologic changes in the bronchial mu- -cosa and submucosa, and the release of
' " " ' t l A T f ÔF « P T : OCCUPATIONAL'ASTHMA '*'
chemical mediators as well as the func-tional activity of the celts involved in the
^asthmatic reaction. These methods of 'lotudy can also be applied to investigate
J why certain patients with occupational asthma recover, whereas others have per-sistent symptoms after removal from ex-
. - posure. Detailed study of these patients will enhance our .understanding of. the
. basic mechanism of occupational asthma as well as bronchial asthma in general.
blad I. Long term effects of exposure to sulphur dioxide lung function four years after a pyrite dust explosion. A m Rev Respir Dis 1983; 128:890-3. 15. F1uryKE,DinesDE,RodarleJR,RodgersR. Airway obstruction due lo Inhalation of ammo-nia. Mayo Clin Proc 1983; $8:389-93. 16. HasanFM,GchshanA.FulechanFJD. Reso-lution of pulmonary dysfunction following acute chlorine exposure. Arch Environ Health 1983; 38:76-80. 17. Kaufman J, Bur Icons' D. Clinical roentgeno-logic and physiologic effects of acute chlorine ex-posure. Arch Environ Health 1971; 23:29-34. . 18. Whitencr DR, Whïtener L M , Robertson KJ, Baxter CR, Pierce AK. Pulmonary function meas-urements in patients with thermal injury and smoke inhalation. Am Rev Respir Dis 1980; 122:731-9. 19. Galea M. Fatal sulfur dioxide inhalation. Can Med Assoc J 1964; 91345. 20. El wood RK, Johnson AJ, Abboud RT. Hung J, Snelling CFT. Pulmonary function and bron-chial reactivity in survivors of smoke inhalation (abstract). Am Rev Respir Dis 1981; !23(SuppkA77). 21. Brooks SM, Lockey J. Reactive airways dys-function syndrome (RADS). A newly defined oc-cupational disease (abstract). Am Rev Respir Dis 1981; 123(Suppl:AI33).
22. Brooks SM, Weiss MA, Bernstein IL. Reac-tive airways dysfunction syndrome (RADS). Per-sistent airways hyperreactivity after high level irri-tant exposure. Chest 1985; 88:376-84. 23. Diamond JM. Channels in epithelial cell mem-branes and junctions. Fed Proc 1978; 34:2639-44. 24. Simani AS, Inoue S, Hogg JC. Penetration o f the respiratory epithelium of guinea pigs fol-lowing exposure to cigarette smoke. Lab Invest 1974; 31:75-81. 25. Boushcy HA, Hohzman MJ, Shdkr J R, Nadd JA. Bronchial hyperreactivity (State of Art) . Am Rev Respir Dis 1980; 121:389-414. 26. Zuskin E, Wolfson R U Harpel G. Welborn JW, Bouhuys A. Byssinosis in carding and spin-ning workers. Arch Environ Hcahh 1969; 19tf66-75. 27. Fox J J, Tombleson JBL, Watt A , Wilkie AG. A survey of respiratory disease in cotton operatives. Part 1. Symptoms and ventilation (est results. Br J Ind Med 1973; 30:42-8. 28. Fox J J, Tombleson JBL, Watt A, Wilkie AG. A survey of respiratory disease in cotton operatives. Part 11. Symptoms, dust estimations and the effect of smoking habit. Br J tnd Med 1973; 30:48-53.
29. Imbus HR, Suh MW. Byssinosis. A study of 10.133 textile workers. Arch Environ Health 1973; 26:183-91. 30. Jones RN, Diem JE, Glindmeyer H. et ai Mi l l effect and dose-response relationships in byssino-sis. Br J tnd Med 1979; 36:305-13. 31. Merchant JA. Lumsden JC, Kilburn KH. et al. Dose response studies in cotton textile workers. J Occup Med 1973; 15:222-30. 32. Butcher BT, 0*NeiI CE, Jones RN. The respi-ratory effects of cotton dust. In: Salvaggio JE. Stankus RP, eds. Clinics in chest medicine. Vol. 4.1.
, Philadelphia: W. B. Saunders, 1983; 63-70.
33. Edwards J. International conference on bys-sinosis. Mechanisms of disease induction. Chest 1981; 79(Suppl:38-43). 34. Noweir M H . Highlights of broad-spectrum industrial-hygiene research activities in a develop-ing country-Egypt. Am Ind Hyg Assoc J 1979; 40:839-59.
" " - - ' - • • -'-699.' '
35. Prindle B. The microbiology of textile Fibers (cotton). Tbxtile Res 1934; 5:11-3. 36. RylandcT RK, ImbusHR, Suh MW. Bacterial contamination of cotton as an indicator of respi-ratory effecu among cardroom workers. Br J Ind Med 1979; 36:299-304. 37. Castellan RM. Olenchock SA, Hankinson JL, et at. Acute bronchoconstriction induced by cot-ton-dust: dose-related response to endotoxin and other 'dust factors. - Ann Intern Med 1984;-101:157-63.
38. Pernis B. Vigliani EC, Cavagna C. Finulli M . The role of bacterial endotoxins in occupational diseases caused by inhalating vegetable dusts. Br J Ind Med 1961; 18:120-9. 39. Wilson MR. Sekul A . O r y R , Salvaggio JE. Lehrer SB. Activation of the alternative comple-ment pathway by extracts of cotton dust. Clin Al-lergy 1980; 10:303-6.
40. Buck M a Schachtcr EN, Wall JH. Partial composition of a low molecular weight cotton bract extract which induces acute airway constriction in humans. In: Wakekyn PE, ed. Proceedings of the Sixth Cotton Dust Research Conference. Memphis, TN: National Cotton Council, 1982; 19-23. 41. 0*Neil CE. Butcher BT, Hughes JM. Studies of total and specific antibodies in workers employed in cottonseed crushing mills. In: Wakekyn PJ, ed. Proceedings of the Fifth Cotton Dust Research Con-ference. Memphis, TN: National Cotton Council, 1981; 3-6. 42. Jones RN. Butcher BT, Hammand YY. et al.
Interaction of atopy and exposure to cotton dust in the bronchodilator response. Br J Ind Med 1980; 37:141-6. 43.. Weiner' A. Bronchial asthma due to organic phosphate insecticide. Ann Allergy 1961; 19397-401. 44. Davies RJ, Butcher BT, CVNeil CE, Salvaggio JE. The in vitro effect of toluene diisocyanate on lymphocyte cyclic adenosine monophosphate production by isoproterenol, prostaglandin and histamine. A possible mode of action. J Allergy Clin Immunol 1977; 6(h223-9.
45. Butcher BT. Salvaggio JE. O'Neil CE, Weill H. Garg O. Toluene diisocyanate pulmonary dis-ease. Immunopharmacologic and Mecholyl chal-lenge studies. J Allergy Clin Immunol 1977; 59:223-7. 46. VanErt M. Battigeli C. Mechanism of respi-ratory injury by TDI (toluene diisocyanate). Ann Allergy 1975; 35:142-7. 47. Bernstein IL. Isocyanate-induced pulmonary disease: a current perspective. J Allergy Cl in Im-munol. 1982; 70(Suppt:24-3l).
48. Chan-Yeung M. Giclas P, Henson P. Activa-tion of the complement by plicatic acid: the chem-ical compound responsible for asthma due to west-ern red cedar (Thuja plica ta). J Allergy Clin Im-munol 1980; 65:333-7.
49. Davies GE, McArdlc LA. Allergy to labora-tory animals: a survey by questionnaire. Int Arch Allergy Appl Immunol 1981; 64:302-7. 50. Gross NJ. Allergy to laboratory animals: epidemiologic, clinical, and physiologic aspects and a trial of cromolyn in its management. J Allergy G i n Immunol 1980; 66:158-65.
51. Cockcroft A. Edwards J. McCarthy P, Anders-son N. Allcrgv in laboratory animal workers. Lan-cet 1981; 1:827-30. 52. Hook WA, Powers K. Siraganian RP. Skin tests, blood leukocytes, histamine release of patients
A cknowledgment The writers wish to thank the Workers* Com-pensation Board of British Columbia for its continuous support of research in occupa-tional asthma in British Columbia over the years. They also thank Miss Elaine Dorken for her assistance in compiling the tables and references, and Mrs. Ellen Wong and Miss Alice Fong for their secretariat assistance.
References 1. Ramazzini B. De Morbus Art i f icum Diatriba (Wright WC, TVans. Disease of workers). Chicago: University of Chicago Press, 1940. 2. Proust A . TVaité d'Hygiène, Publique et privée. Paris: Masson, 1877; 171-4. 3. Karasek SR, Karasek M . Preliminary report on the injurious effects of metal platinum, chromâtes, cyanides, hydrofluoric acid and of material used by silver miners. Report o f the Illinois State Com-
1 mission on Occupational Disease, 1911; 97. 4. Newman Taylor AJ. Occupational asthma. Tho-rax 1980; 35:241-3. 5. Department of Health and Social Security. Oc-cupational asthma. Report o f the Industrial Inju-ries Advisory Council. London: Her Majesty's Sta-tionery Office, 1981.
6. Gandevia B. Occupational asthma I. Med J Aust 1970; 2:332-5. 7. Murphy R L H Jr. Industrial disease with asthma. In: Weiss EB, Segal MS, eds. Bronchial asthma: mechanisms and therapeutics. Boston: Lit-tle. Brown, 1976; 517-36.
8. Bernstein L . Occupational asthma in occupa-tional lung disease I. In: Brooks SM. Lockey JG, Harber P, eds. Clinics in chest medicine. Vol. 2.2. Philadelphia: W. B. Saunders, 1981; 255-72. 9. Horton DJ. Chen WY. Effects of breathing warm humidified air on bronchoconstriction in-duced by body cooling and by inhalation of methacholine. Chest 1979; 75:24-8. 10. Widdicombe JT. Kent DC. Nadcl JA. Mech-anisms of bronchoconstriction during inhalation of dust. J App l Physiol 1962; 17:613-6. 11. Frank NR. Amdur MO. Worcester J, Whit-tenberger JL. Effects of acute controlled exposure to SOi on respiratory mechanics in healthy male adults. J App l Physiol 1962; 17:252-8. 12. Brooks SM, Mintz S, Weiss E. Changes oc-curring after freon inhalation. Am Rev Respir Dis 1972; 105:640-3.
)13. Charan NB, Myers CG. La k sh mina raya n S, SpenceT T M . Pulmonary injuries associated with acute sulphur dioxide inhalation. Am Rev Respir Dis 1979; 119:555-60. 14. Harkonen H. Nordman H. Korhonen Q. Win-
700 '
with atlcrgies to laboratory animals. J Allergy Clin Immunol 1984; 73:457-63. 53. Slovak A J M , H i l l RN. Laboratory animal al-Ic ig j : m citait*» survey of an exposed population.
" y . B r J Ind Med 1981; 38:38-41. i J4. Newman Tbylor AJ , Longbottom JL, Ptpys
J. Respiratory allergy to urine proteins of rats and mice. Lancet 1977; 2:847-9.
55. Ohman JL Jr, Lowell FC. Bloch KJ. Aller-gens of mammalian origin. I I : Characterization of ait».**.** mt%wTtrtorf from rats, mouse, guinea pig. rabbit pelts. J Allergy Clin Immunol 1975; 55:16-24. 56. H a rg reave FE, Pepys J. Allergic respiratory reaction? in bird-fanciers, provoked by allergen in-halation provocation tests. J Allergy Clin Immunol 1972; 50:157-73. 57. Bar-Sela S. Teichtahl H . Lutsk y I. Occupa-tional asthma in poultry workers. J Allergy Clin Immunol 1984; 73:271-5. 58. Lutsky I» Teichtahl H , Bar-Sela S. Occupa-
• J ion a I asthma due to poultry mites. J Allergy Clin Immunol 1984; 73:56-60. 59. DaviesRJ, Green M . McSchofîdd NM. Recur-rent nocturnal asthma after exposure to grain dust. A m Rev Respir Dis 1976; 114:1011-9. 60. Burge PS. Edge G. O'Brien M . Harries MG. Hawkins R. Pepys J. Occupational asthma in a re-search centre breeding locusts. G i n Allergy 1980; 10355-63. 61. Fîgley KD. Mayfly (Ephemerida) hypersensi-tivity. J Allergy 1940; 11:376-87. 62. Gibbons H L , Dille JR. Cowley RG. Inhalant sUs.-gy to scnrjrccrm fly. Arch Environ Health 1965; 10:424-30. 63. Bemton HS, McMahon TF, Brown H. Cock-
-v-sxoach asthma. Br J Dis Chest 1972; 66:61-6. .: J \JU. Har f i H A . Immediate hypersensitivity to ^ c r i c k e t . Ann Allergy 1980; 44:162-3.
65. Stevenson DD, Mathews KP. Occupational asthma following inhalation of moth particles. J Allergy 1967; 39:274-83. 66. Randolph H . Allergic response to dust of in-sect origin. J A M A 1934; 103:560-2. 67. Warren P, Cherniack RM, Tie KS. Hypersen-sitivity reactions in grain dust. J Allergy Clin Im-munol 1974; 53:139-49. 68. Chan-Yeung M, Wong R, Mac Lean L. Respi-ratory abnormalities among grain elevator work-ers. Chest 1979; 72:461-7.
69. doPico GA, Jacobs S, Flaherty D. Rankin J. Pulmonary reaction to durum wheat; a constitu-ent of grain dust. Chest 1982; 81:55-61. 70. Tie KS. Warren P. Janusz M , McCarthy DS. Cherniack RM. Respiratory abnormalities in work-ers exposed to grain dust. Arch Environ Health 1973; 27:74-7. 71. doPico GA. Flaherty D, Bhansali P, Chavaje
. N . Grain fever syndrome induced by airborne grain dust. J Allergy Cl in Immunol 1982; 69:435-42. 72. Chan-Yeung M.SchulzerM.MacLeanL, Dor-ken E, Grzybowski S Epidemiologic health'sur-vey of grain elevator workers in British Columbia. A m Rev Respir D » 1980; 121:329-37. 73. doPico GA. Reddan W, Anderson S, Flaherty D, Smallcy E. Acute effects of grain dusl exposure during a work shift. A m Rev Respir Dis 1983;
>•>128:399-404. 1 / 4 . Corey P. Hutcheon M. Broder I, MintzS. Grain
elevator workers show work-related pulmonary function change and dose effect relationships with dusl exposure. Br J Ind Med 1982; 39:330-7. 75. Olenchock SA. M u l l J C , Major P. Extracts
V'
of airborne grain dust activate alternative and clas-sical complement pathway». Ann Allergy 1980; 44:23-8. 76. Warren P, Holford-Strevcns V. Induction of histamine release in vitro from rat peritoneal mast cells by extracts of grain and grain dust. Presented in the New Orleans Conference on Agricultural Dusts 1984. 77. Wilbur RD, Ward GW. Immunological studies in a case of baker's asthma. J Allergy Clin Immunol 1976; 38:366-72. 78. Hendrick DJ, Davies RJ, Pepys J. Baker's asthma. Clin Allergy 1976; 6:241-50. 79. Baldo BA. Krilis S. Wrigley CW. Hypersensi-tivity to inhaled flour allergens. Allergy 1980; 35:45-56. 80. Block GL "Be KS, Kijek K, Chan H, Chan-Yeung M. Baker's asthma: clinical and immunological studies. Clin Allergy 1983; 13:359-70. 81. Blands J. Diamant B, Kallos P, Kallos-Deffner L, Lowenstein H . Flour allergy in bakers. Int Arch Allergy Appl Immunol 1976; 52:392-409. 82. Bjorksten F, Backman A , Jarvinen K, et al.
IgE specific to wheat and rye f lour protein. Clin Allergy 1977; 7:473-83. 83. Block G, "Be ICS, Kijek K. Chan H, Chan-Yeung M. Baker's asthma: studies of cross-ant igenicity be-tween different cereal grains. Cl in Allergy 1984; 14:177-85. 84. Herxheimer H . The skin sensitivity to flour of bakers'apprentices. Acta Allergol 1973; 28:42-9. 85. Thiel H, Ulmer WNT. Baker's asthma: devel-opment and possibility of treatment. Chest 1980; 78(Suppl:400-5). 86. Ordman D. Buckwheat allergy. S Af r Med J 1947; 21:737-9. 87. Kan RM. Bronchoprovocation studies in coffee worker's asthma. J Allergy Cl in Immunol 1979; 64:650-4. 88. Davison AG. Britton MG. Forrester JA. Da-vies RJ, Hughes DTD. Asthma in merchant sea-men and laboratory workers caused by allergy lo castor oil beans: analysis of allergens. Clin Allergy 1983; 13:553-61. 89. Uragoda CG. Teamaker's asthma. Br J Ind Med 1970; 27:181-2. 90. Gleich GJ. Welsh PW, Yunginger JW, Hyatt RE, Catlett JB. Allergy to tobacco: an occupational hazard. N Eng J Med 1980; 302:617-9. 91. Newmark FM. Hops allergy and lerpcnc sen-sitivity an occupational disease Ann Allergy 1978; 41:311-2. 92. Flindt MLH. Pulmonary disease due to inha-lation of derivatives of Bacillus subtilis containing proteolytic enzyme. Lancet 1969; 1:1177-81. 93. Pepys J, Hargreave FE. Longbotton JL, Faux J. Allergic reactions of the lungs to enzymes of Ba-cillus subtilis. Lancet 1969; 1:1181-4. 94. Mitchell CA, Gandevia B. Respiratory symp-toms and skin sensitivity in workers exposed to pro-teolytic enzyme in detergent industry. Am Rev Respir Dis 1971; 104:1-12.
"95.- Franz T, McMurrain KD, Brooks S, Bernstein IL. Ginical immunologic and physiologic obser-vations in factory workers exposed to B subtilis en-zyme dust. J Allergy 1971; 42:170-80.
96. Colten HR, Polakoff P U Weinstein SF. Striedcr DJ. Immediate hypersensitivity to hog tryp-sin resulting from industrial exposure. N Engl J Med 1975; 292:1030-3. 97. Dolan TP, Meyers A . Bronchial aslhma and allergic rhinitis associated with inhalation of pan-
CHANJreUNQ AND LAM
creatic extracts. Am Rev Respir Dis 1974; 110:812-3. 98. Ib r lo SM, Shaikh W. Bell B. et al. Pa pain-induced allergic reactions. G i n Allergy 1978; 8:207-13. . 99. Baur X , Konig G, Bencze K. Fruhmann G. Ginical symptoms and results of skin test, RAST and bronchoprovocation test in thirty-three papain workers: evidence for strong immunogenic potency and clinically relevant "proteolytic effects of air-borne papain. G i n Allergy 1982; 12:9-17. 100. Cartier A . Malo JL, Pineau L, Dolovich J. Occupational asthma due to pepsin. J Allergy G i n Immunol 1984; 73:574-7. 101. Pauwels R. Devos M. Callens L , van der Straeten M. Respiratory hazards from proteolytic enzymes. Lancet 1978; 1:669. 102. Galleguillos F, Rodriguez JC. Asthma caused by bromelin inhalation. G i n Allergy 1978; 8:21-4. 103. Flindt M L H . Allergy to alpha-amylase and papain. Lancet 1979; 1:1407-8. 104. Bohner CB, Sheldon JM, "IVenis JW. Sensi-tivity to gum acacia with a report o f ten cases of asthma in printers. J Allergy 1940; 12:290-4. 105. 'Fowler PBS. Printer's asthma. Lancet 1952; 2:755-7. 106. Gelfand H H . The allergenic properties of vegetable gums. A case of asthma due to tragacanth. J Allergy 1943; 14:203-17. 107. Cartier A , Malo JL, Forest F. Lafrance M , etal. Occupational asthma in snow crab process-ing workers. J Allergy G i n Immunol 1984; 74:261-9. 108. Gaddie J. Legge JS, Friend JAR, Reid TMS. Pulmonary hypersensitivity in prawn workers. Lan-cet 1980; 2:1350-3. 109. Jyo T, Kohmoto K, Katsutani T, et al. Hoya (sea-squirt) aslhma). In: Frazier C A , ed. Occupa-tional asthma. New York: Van Nostrand Reinhold Company. 1980; 209-29. 110. Kobayashi S. Different aspects of occupa-tional asthma in Japan. In: Frazier CA, ed. Oc-cupational aslhma. New York: Van Nostrand Rein-hold Company, 1980; 229-44. 111. Henschler D. Assman W.Meyer KO. ThVtox-icology of the toluene diisocyanates. Arch Toxicol 1962; 19:364-87. 112. Brooks SM. Bronchial asthma of occupa-tional origin. Scand J Work Environ Health 1977; 3:53-72. 113. Brugsch HG, Elkins HD. Toluene diisocyanate (TDI) toxicity. N Engl J Med 1963; 268:333-7. 114. Pepys J. Pickering CAC. Brcslin ABX. Terry DJ. Asthma due to mhalcd chemicat agents: tolu-ene diisocyanate. Cl in Allergy 1972; 2:225-36. 115. Butcher BT. Inhalation challenge testing with toluene diisocyanate. J Allergy G i n Immunol 1979; 64:655-7. 116. Taylor G. Immune response to tolylene di-isocyanate (TDI) exposure in man. Proc R Soc Med 1970; 63:379-80. 117. Avery SB. Stetson DM. Pan PM. Mathews KP. Immunological investigation of individuals with toluene diisocyanate asthma. Cl in Exp Immunol 1969; 4:585-96. 118. Butcher BT. Salvaggio JE. Weill H . Ziskind M M . Toluene diisocyanate (TDI) pulmonary dis-ease immunologic and inhalation challenge studies. J Allergy G i n Immunol 1970; 58:89-100.
119. Karol M H , losei H H , Alarie YC. Tolyl-sperifte IgE antibodies in workers with hypersen-sitivity to toluene diisocyanate. A m Ind Hyg As-soc J 1978; 39:454-8. 120. Gallagher JS, Tse CST, Brooks SM, Bern-
e .«TATC .Of >RT: OCCÙMTVONAl.. ASTHMA .
i tc in IL . Diverse profiles of immunoreaeiivity in toluene diisocyanate (TDI) asthma. J Occup Med 1981; 23410-16.
^.121. Butcher BT, 0*NeiI CE. Reed M A . Salvag-Igio JE. Radtoallergosorbent testing of toluene
y diisocyanate-reactivt individuals using /Molyl isocyanate antigen. J Allergy Clin Immunol 1980; 66:213-6.
122. Danks JM, Crornwell O. Buckingham JA. Newman-Taylor AJ , Davies RJ. Toluene-diisocyanate induced asthma: evaluation of anti-bodies in the serum of affected workers against a tolyl mono-isocyanate protein conjugate. G i n Al-lergy. 1981; 11:161-8. 123. Baur X . Fruhmann G. Specific IgE antibod-ies in patients with isocyanate asthma. Chest. 1981; 80(Supp1:73-6). 124. Butcher BT, Mapp C, Reed M A . O'Neill CE, Salvaggio JE. Evidence for carrier specificity of IgE antibodies detected in sera of isocyanate ex-posed workers (abstract). J Allergy G i n Immunol, 1982; 69(Suppl:I23).
123. Chen SE, Bernstein IL. The guinea pig model o f diisocyanate sensitization I : immunological studies. J Allergy G i n Immunol 1982; 70:383-92.
126. Munn A . Hazards of isocyanates. Ann Oc-cup Hyg 1965; 6:163-9. 127. Konzen RB, Craft BF, Sched ID, Gorski CH. Human response to low concentrations of P,P-diphenylmethane diisocyanate. A m Ind Hyg As-soc 1966; 27:121-7. 128. "linser AR. Bourke MP. Blandford AG. . Isocyanate asthma: respiratory symptoms caused by diphenyl-methane diisocyanate. Thorax 1973; 28:596-600.
"•"v 129. Zeiss CR, Kanellakes TM, Bellone JD, Leviiz J D. Pruzansky JJ, Patterson R. Immunoglobulin
E mediated asthma and hypersensitivity pneumo-nitis with precipitating anti-hapten antibodies due to diphenylmethane diisocyanate (MD1) exposure. J Allergy G i n Immunol 1980; 65:347-52.
130. Malo JL. Zeiss CR. Occupational hypersen-sitivity pneumonitis after exposure to diphenyl-methane diisocyanate A m Rev Respir Dis 1982; 125:113-6. 131. O'Brien IM . Harries MG, Burge PS, Pepys J. Toluene diisocyanate-induced asthma. Reactions to T D I , M D I , H D I and histamine. G i n Allergy 1979; 9:1-6. 132. Zammit-Tabona M, Sherkin M , Kijek K. Chan H , Chan-Yeung M. Asthma caused by dimethyl methane diisocyanate in foundry work-ers. G inka l , bronchoprovocation and immunologic studies. A m Rev Respir Dis 1983; 128:226-30.
133. Johnson A . Chan-Yeung M, Mac Lean L, et at. Respiratory abnormalities among workers in an iron and steel foundry in Vancouver. Br J Ind Med 1985; 42:94-100.
134. Malo JL, Ouimet G, Cartier A, Leviiz D, Zeiss CR. Combined alveolitis and asthma due to hex-amethylene diisocyanate (HDI) with demonstration o f cross reactivity and immunologic reactivities to diphenyl methane diisocyanate (MDI) . J Allergy G i n Immunol 1983; 72:413-9.
135. Baur X . Immunologic cross-reactivity be-tween different albumin bound isocyanates. J Al-lergy G i n Immunol 1983; 71:197-205. 136. Fawcett IW, Newman-Taylor AJ, Pepys J. Asthma due to inhaled chemical agents. Epoxy resin systems containing phthalic add anhydride, t r imd-Utic acid anhydride and triethylene tetramine. Clin Allergy 1977; 7:1-14. 137. Maccia C A , Bemstan I L , Emmet I EA,
Brooks SM. In vitro demonstration of sped He IgE in phthalic anhydride hypersensitivity. Am Rev Respir Dis 1976; 113:701-4. 138. Zeiss CR, Patterson R, Pruzansky J J, Miller M, Rosenberg M, Levhz Dl I t ime l l i t k anhydride-Induced airway syndromes: dinical and immuno-logic studies. J Allergy G i n Immunol 1977; 60:96-103.
139. Patterson R, Addington W, Banner A. et al. Anti-hapten antibodies in workers exposed to trimellitic anhydride fumes: a potential im-munopathogenetic mechanisrrt for the trimellitic anhydride pulmonary-disease-anemia syndrome: Am Rev Respir Dis 1979; 120:1259-67. .
140. Patterson R, Zeiss CR, Roberts M, Pruzansky JJ. Wolkonsky P. Chacon R. Human antihapten antibodies in trimellitic anhydride inhalation reac-tions: immunoglobufm dasscs of anti-trimellitic an-hydride antibodies and hapten inhibition studies. J G i n Invest 1978; 62.-97I-8.
141. Sale SR. Patterson R t Zeiss CR. Flore M. Harris KE, lbwn D. Immune response of dogs and rabbits to intiabronchial t r imdl i t ic anhydride. Int Arch Allergy Appl Immunol 1982; 67:329-34.
142. Zdss CR, Wolkonsky P, Chacon R, et of. Syn-dromes in workers exposed to trimellitic anhydride: a longitudinal dinical and immunologic study. Ann Intern Med 1983; 98:8-12. 143. Schlueter DP. Banaszak EF. Fink JN, Bar-boriak J. Occupational asthma due to tetrach-lorophthalic anhydride. J Occup Med 1978; 20:183-7. 144. Milne J, Gandevia E Occupational asthma and rhinitis due to western red cedar (Thuja plicota).
Med J Aust 1967; 2:741-4. 145. IshizakiT.ShidaT,MiyamotoT,Matsumara Y, Mizuno K, Tomaru M. Occupational asthma from western red cedar dust (Thujaplicota) in fur-niture factory workers. J Occup Med 1973; 15:580-5. 146. Chan-Yeung M. Barton GM. Mac Lean L. Grzybowski S. Occupational asthma and rhinitis due to western red cedar (Thuja plicata). Am Rev Respir Dis 1973; 108:1094-102. 147. Chan-Yeung M. Immunologic and nonim-munologic mechanisms in asthma due to western red cedar (Thujaplicata). J Allergy G i n Immunol 1982; 70:32-7.
148. Chan-Yeung M, Vedal S, Kus J. MacLean L. Enarson D, Tse K. Symptoms, pulmonary func-tion and bronchial hyperreactivity in western red cedar compared to those in the office workers. Am Rev Respir Dis 1984; 130:1038-41.
149. Veda! S. Enarson Q, Kus J. McCormack G. MacLean L, Chan-Yeung M. Symptoms and pul-monary function in western red cedar workers related to duration of employment and dust ex-posure (abstract). A m Rev Respir Dis 1984; !29(SuppLAI52).
150. Evans '£. Nicholls RJ. Histamine release by western red cedar (Thujaplicata) from lung tissue
. in v i t ra Br J Ind Med 1974; 31:28-30. 151. Tie KS, Chan H. Chan-Yeung M. Specific IgE antibodies in workers with occupational asthma due to western red cedar. G i n Allergy 1982; 12349-58. 152. Oosfdam JV, Moreno R, Chan H. Paré PD, Schdlenberg RR, Chan-Yeung M. Animal models of western red cedar asthma (abstract). Am Rev Respir Dis 1985; l31(Supp!:A9). 153. Belleau B, Burba J. Occupancy of adrener-gic receptors and inhibition of catechol-o-melhyl transferase by tropolones. J Med Chem 1963; 6:735-9.
• •701
134. Banon GM. Macbonald BF. The chemistry and utilization of western red cedar. Dept of Fish-eries and Forestry, Canadian Forestry Service. Pub-lication No. 1023. Ottawa: Information Canada, 1971.
155. Chan-Yeung M, Abboud R. Occupational asthma due to California redwood (Sequoia sem-pervirens) dust. A m Rev Respir Dis 1976; 114:1027-31. 156. Green berg M. Respiratory symptoms follow-ing brief 'exposure to cedar of Lebanon (Cedra tiboni) dust. Clin Allergy 1972; 2319-24. 157. EatonKK. Respiratory allergy to exotk wood dust. G i n Allergy 1973; 3307-10. 158. Pickering CAC, Batten JC. Pepys J. Asthma due to inhaled wood dust-western red cedar and iroko. Clin Allergy 1972; 2313-8. 159. Sosman AJ, Schlueter DP, Fink JN. Barbo-riak JJ. Hypersensitivity to wood dust. N Engl J Med 1969; 281:977-80. 160. Booth BH, LeFoIdt RH. Mof f i t t EM. Wood dust hypersensitivity. J Allergy G i n Immunol 1976; 57352-7. 161. Hinojosa M, Moneo I, Dominguez J, Del-gado E, Losada E, Alcovtr R. Asthma caused by African maple (THplochiton scheroxyton) wood dust. J Allergy G i n Immunol 1984; 74:782-6. 162. Paggiaro PL, Cantalupi R. Filîert M . et al.
Bronchial asthma due to inhaled wood dust: Tan-
ganyika oningre. Clin Allergy 1980; 11:605-10. 163. Bush RK, Gayton D. Asthma due to Cen-tral American walnut (Jugions olanchana) dust. G i n Allergy 1983; 13:389-94. 164. Ordman D. Wood dust as an inhalant aller-gen. Bronchial asthma caused by kejaat wood (Pterocarpus angolensis). S A f r Med 1949; 23:973-5. 165. Bush RK, Yunginger JW, Reed CE. Asthma due to African zebrawood (Microberlinia) dust. A m Rev Respir Dis 1978; 117:601-3. 166. Hunter D, Mi l ton R, Perry K M A . Asthma caused by the complex salts of platinum. Br J Ind Med 1945; 2.-92-S. 167. Pepys J, Pickering CAC, Hughes E G Asthma due to inhaled chemical agents: complex salts o f platinum. G i n Allergy 1972; 2:391-6. 168. Cromwell O, Pepys J, Parish WE, Hughes EG. Spedfic IgE antibodies to platinum salts in sensitized workers. G i n Allergy 1979; 9:109-17.
169. Levene GM, Calnan CD. Platinum sensitiv-ity treatment by spedfic hyposensitization. G i n Al-lergy 1971; 1:75-82. 170. McConnell L H , Fink JN. Schlueter DP. Schmidt MG. Asthma caused by nickel sensitivity. Ann Intern Med 1973; 78:888-90. 171. Block G. Chan-Yeung M. Asthma induced by nickel. JAMA 1982; 247:1600-2. 172. Malo JL, Cartier A , Dœpner M. Nieboer E. Evans S, Dolovkh J. Occupational asthma caused by nickel sulphate J Allergy G i n Immunol 1982; 69:55-9. 173. Novey HS,Habib M . Wells ID. Asthma and IgE antibodies induced by chromium and nickel salts. J Allergy G i n Immunol 1983: 72:407-12. 174. Joules H. Asthma from sensitization to chro-mium. Lancel 1932; 2:182-3.
175. Smith AR. Chrome poisoning with manifesta-tions of sensitization. J A M A 1931; 97:95-8. ( 176. Keskinen H, Kalliomaki PL. Alanko K. Oc-cupational asthma due to stainless steel welding fumes. G i n Allergy 1980; 10:151-9. 177. Hartmann A , Wulhrich B, Bolognini G.
CHAM4CUMO AND LAM
Benifsbcdingte lungcnkrankherten bet der hart-metallproduktion und bearbcittmg ein allergische geschehen? Schwdz Med Wochenschr 1982; 112:1137-41. 178. Browne R C Vanadium poisoning from gas
.•jirbine. Br J Ind Med 1933; 12J7-9. J ^p. Bruckner HC. Extrinsic asthma in a tung-
,<en carbide worker. J Occup Med 1967; 9:518-9. 180. Pepys J, Pickering CAS. Aslhma due lo in-haled chemical fumes: amino ethyl ethanolamine in aluminum soldering flux. Clin Allergy 1972; 2:197-204.
181. Sterling GM. Asthma due to aluminum sol-dering f lux. Thorax 1967; 22J33-7. 182. Ozhiganova VN. Ivanova IS, Dueva LA. Bronchial asthma in radio equipment assemblers. Sov Med 1977; 4:139-41. 183. Burse PS, Perks W. O'Brien IM. Hawkins R, Green M . Occupational asthma in an electronics factory. Thorax 1979; 34:13-8. 184. Burge PS, Perks W H . O'Brien IM. et ai Oc-cupational asthma in an electronics factory. A case control study lo evaluate aetiologies! factors. Tho-rax 1979; 34:300-7.
185. Burge PS, Harries MG. O'Brien IM. Pepys J. Bronchial provocation studies in workers exposed to the fumes o f electronic soldering fluxes. Clin Allergy 1980; 10:137-49.
186. Burge PS, Edge a Hawkins R. White V, New-man Taylor AJ. Occupational asthma in a factory making flux-cored solder containing colophony. Thorax 1981; 36:828-34.
187. Davies RJ, Hendrick DJ, Pepys J. Aslhma due to inhaled chemical agents: ampicillin, ben-zylpeniri l l in, 6-aminopeniciIlanic arid and related substances. Cl in Allergy 1974; 4:227-47.
Coutts I I , Dally MB, Newman-Taylor AJ , J jlcering CAC, Horsfield N. Asthma in workers
-^-- '•anu factoring cephalosporins. Br Med J 1981; 283.-950.
189. Kammermeyer JK, Mathews KP. Hypersen-sitivity to phenyl glycine and chlpride. J Allergy Cl in Immunol 1973; 52:73-84.
190. Pepys J, Pickering CAC, Loudon HWG. Asthma due to inhaled chemical agent: piperazine di hydrochloride. Cl in Allergy 1972; 2:189-96.
191. Busse WW. SchoenwetterWF. Asthma from psyllium in laxative manufacture. Ann Intern Med 1975; 83:361-2.
192. Harries MG. Newman Tbylor A . Wooden J, MacAuslan A . Bronchial asthma due to alpha-methyldopa. Br Med J 1979; 1:1461. 193. Davies RJ, Pepys J. Asthma due to inhaled chemicals: the macrolide antibiotic spiramycin Clin Allergy 1975; 5:99-107. 194. Fawcett IW. Pepys J, Erooga MA. Asthma due to gtycyl compound powder an intermediate in production of salbutamo!. Cl in Allergy 1976* 6:405-9.
195. Greene SA. Freedman S. Asthma due to in-haled chemical agents: amprolium hydrochloride. Cl in Allergy 1976; 6:105-8. 196. Fawcett IW, Pepys J. Allergy to a tetracycline preparation. Cl in Allergy 1976; 6:301-3. 197. Fcinbcrg SM, Watrous RM. Atopy to simple chemical compounds: sulphonechloramides. J Al-lergy 1945; 16:209-20.
O y Bourne MS, Flindt M L H , Walker JM. 1 / n a due to industrial use of chloramine. Br Med
J A 7 9 ; 2:10-2. W . Vallieres M , Coclccroft DW. Tiylor DM, Dolovich J. Hargreave FE. Dimethyl ethanolamine-
induced asthma. Am Rev Respir Dis 1977; 115:867-71.
200. Pepys J, Hutchcroft BJ. Bresfin ABX. Asth-ma due to inhaled chemical agents: persulphate sahs and henna in hairdressers. Cl in Allergy 1976; 6:399-404.
201. Lam S, Chan-Yeung M. Ethylenediamine-induced asthma. Am Rev Respir Dis 1980; 121:151-5. 202. Slovak AJM. Occupational aslhma caused by plastics blowing agent, azodicarbonamide. Tho-rax 1981; 36:906-9.
203. Graham V. Coe MSS, Davies RJ. Occupa-tional asthma after exposure to a diazonium salt. Thorax 1981; 36:950-1. 204. Nagy L. Orosz M. Occupational asthma due to hexachlorophcnc. Thorax 1984; 39:630-1.
205. Hendrick DJ, Lane DJ. Formalin asthma in hospital staff. Br Med J 1975; 1:607-8. 206. Cockcroft DW, Hoeppner VH, Dolovich J. Occupational asthma caused by cedar urea form-aldehyde particle board. Chest 1982; 82:49-53. 207. Frigas E. Filley WV. Rod C Asthma induced by dusl f rom urea formaldehyde foam insulating material. Chest 1981; 79:706-7. 208. Malo JL,GagnonG. Cartier A . Occupational aslhma due to heated freon. Thorax 1984; 39:628-9. 209. Silberman DE, SorreO A H . Allergy in fur workers with special reference to paraphenylene diamine. J Allergy 1959; 30:11-8.
210. Cockcroft DW, Cartier A , Jones G,T&rloSM, Dolovich J, Hargreave FE. Asthma caused by oc-cupational exposure to a furan-based binder sys-tem. J Allergy Clin Immunol 1980; 66:458-63.
211. Chan-Yeung M. Lam S» Koerner & Clinical features and natural history of occupational asthma due to western red cedar (Thuja pGcoto). Am J Med 1982; 72:411-5.
212. Ramsdale EH, Morris M, Hargreave FE. The diagnostic significance of increased bronchial re-sponsiveness to methacholine m subjects with rhi-nitis (abstract). J Allergy Clin Immunol 1983; 7l(Suppl:l43A).
213. Burge PS. Single and serial measurements of lung function in the diagnosis o f occupational asthma. Eur J Respir Dis 1982; 63(Supp! 123:47-59). 214. Carrier A. Pineau L, Malo JL. Monitoring o f maximum expiratory peak flow rates and hista-mine inhalation lests in the investigation of occupa-tional asthma. Clin Allergy 1984; 14:193-6.
215. Cockcroft DW, Killan DN. Mellon JJA, Har-grcave FE. Bronchial reactivity to inhaled hista-mine. A method and clinical survey. Clin Allergy 1977; 7:235-43.
216. Chai H . Farr RS, Foehlich L A . et al. Stan-dardization of bronchia] inhalation challenge proce-dures. J Allergy Clin Immunol 1975; 56:323-7.
217. Hargreave FE, Dolovich FE, Boulet LP. In-halation provocation lests. In: Petty TL . Cherniack RM, eds. Seminars in Respiratory Medicine. Vol IV. 1983; 224-36.
218. Lam S. "fan F, Chan H, Chan-Yeung M. Rela-tionship between types of asthmatic reaction, non-specific bronchial reactivity and specific IgE anti-bodies in patients with red cedar asthma. J Allergy Cl in Immunol 1983; 72:134-9.
219. Pepys J, Hutchcroft BJ. Bronchial provoca-tion lest in etiology diagnosis end analysis of aslhma. A m Rev Respir Dis 1975; 112329-59. 220. Cockcroft DW, Cotton IM. Mink JT. Non-specific bronchial hyperreactivity after exposure to western red cedar. Am Rev Respir Dis 1979; 119:505-10.
221. Siracusa A . Curradi F, Abr i t t i G. Recurrent nocturnal asthma due to tolylene diisocyanate: a case report. Clin Allergy 1978; 8:195-201.
222. WassermanS. Mediators of immediate hyper-sensitivity. J Allergy Clin Immunol 1983; 72:101-13. 223. Parish WE. Short term anaphylactic IgG an-tibodies in human sera. Lancet 1970; 2:591-4. 224. Dolovich J, Hargreave FE. Chalmers R. Shier KJ, Gauldie J, Bienenstock J. Late cutaneous al-lergic responses in isolated IgE dependent reactions. J Allergy Clin Immunol 1973; 52:38-46.
225.. Solley G. Gleich G. Jordan R, Schrocter A . The late phase of the immediate wheal and flare skin reaction. Its dependence on IgE antibodies. J Cl in Invest 1976; 58:408-20.
226. Tbnncnbaum S. Oretel H . Henderson W, Kaliner M. Thc biologic activity o f mast cell gran-ules. I. Eîicitation of inf lammatory response in rat skin. J Immunol 1980; 125:325-35. 227. DeShazo RD, Levinson A L , Dvorak HF. Da-vies RW. The late phase skin reaction: evidence for activation of Ihe coagulation system in an IgE-dependent reaction in man. J Immunol 1979; 122:692-8.
228. Dvoracek JE, Yungingcr JE, Kern E & Hyatt RE, Gleich GJ. Induction of nasal late-phase reac-tions by insufflation of ragweed pollen extract. J Allergy Clin Immunol 1984; 73:363-8.
229. Lam S, Chan-Yeung M, LeRiche J, Kijek K, Phillips D. Cellular changes in bronchial lavage fluids following late asthmatic reaction in patients with red cedar asthma (abstract). A m Rev Respir Dis 1985; l31(Suppl:A42).
230. Lam S, Wong R, Chan-Yeung M. Nonspecific bronchial reactivity in occupational asthma. J A l -lergy Clin Immunol 1979; 63:28-34.
231. Kobayashi S Different aspects of occupa-tional asthma in Japan. In: Frazier CA, ed. 1980. Occupational asthma. New York: Van Nostrand Reinhold, 1980; 229-44.
232. Salvaggio J, ed. Occupational and environ-mental respiratory disease in N I A I D task force re-port: asthma and other allergic disease Washing-ton, D.CJ U.S. Department of Health, Education and Welfare, May 1979 ( N I H Publication No. 79-387).
233. Karr RM. David RJ, Butcher BT. et at. Oc-cupational aslhma. J Allergy Cl in Immunol 1978; 61:54-64.
234. Newman Taylor AJ. Laboratory animal al-lergy. Eur J Respir Dis 1982; 123(Suppl:60-4).
235. NIOSH criteria for a recommended standard. Occupational exposure to diisocyanate. Washing-ton. D.CJ U.S. Dept of Health. Education and Wel-fare, Sept. 1978 (NIOSH Publication No. 78-215).
236. Woolcock AJ. Colman M H . Jones MW. Atopy and bronchial reactivity in Australian and Melanesian populations. Clin Allergy 1978; 8:155-64.
237. Cockcroft DW, Berscheid BA. Murdock KY. Unimodal distribution of bronchial responsiveness to inhaled histamine in a random human popula-tion. Chest 1983; 83:751-4.
238. Balfour-Lynn L, Tooley M , Godfrey S. Rela- • lionship of exercise-induced asthma lo clinical asthma in childhood. Arch Dis Child 1981; 56:450-4.
239. Enarson DA. Chan-Yeung M, Lam S, Veda I S. McCormack G. Does determination of bronchial reactivity add anything to prevalence studies of re-spiratory disease in their occupational setting (ab-stract). A m Rev Respir Dis 1984; I29:A160.
rr*R£ of AM:. OCCUPATIONAL ASTHMA '
240. Ncwhousc M U Ibgg B. Popock SL, McEwa'n AC. A n epidemiologic study of workers produc-ing enzyme washing powders. Lancet 1970; 1*89-93. 241. Burrows B. Hakmen M. Barbee RA, Lebowitz
/ M D . The relationship of serum immunoglobulin • E to cigarette smoking. A m Rev Respir Dis 1981;
124:523-5. 242. Jones JG, Minty BD. Royston D, Royston JP. Car box y haemoglobin and pulmonary epithe-lial permeability in man. Thorax 1983; 38:129-33. 243. Hulbert WC. Walker DC. Jackson A , Hogg JC. Airway permeability to horseradish peroxidase in guinea pigs: the repair phase after injury by cig-arette smoke. A m Rev Respir Dis 1981; 123:320-6. 244. Leskowitz S, Salvaggio JE, Schwarz HJ. An hypothesis for the development o f atopic allergy in man. Cl in Allergy 1972; 2:237-46. 245. Zctterstrom O. Osterman K, Machado L, Jo-hansson S GO. Another smoking hazard: revised serum IgE concentration and increased risk of oc-cupational allergy. Br Med J 1981; 283:1215-7. 246. Venablcs K M . Topping MD, Howe W.Luc-zynska C M , Hawkins R, Newman Tfeylor AJ. In-
teraction of smoking and atopy in the production of specific IgE antibodies against a hapten protein conjugate. Br Med J (in press). 247. Zamd N. Leroux M, Vanderdoelen JL. Air-way response to inhaled methacholine In healthy nonsmoking twins. J Appl Physiol 1984; 56:936-9. 248. Adams WG. Long term effects on the health of men engaged in (he manufacture of toluene di-isocyanate Br J Ind Med 1975; 32:72-8. 249. Moller DR. McKay RTK. Bernstein IL . Brooks S Long term follow-up of-worken with TDI asthma (abstract). Am Rev Respir Dis 1984; 129:AI59. 250. Paggiaro PL, Loi AM, Rosso O, et at. Follow, up study of patients with respiratory disease due to toluene diisocyanate (TDI). Clin Allergy 1984; 14:463-9. 251. Burge PS. Occupational asthma in electronic workers caused by colophony fumes: follow-up of affected workers. Thorax 1982; 37:348-53. 252. Hudson P. Pineau L, Cartier A, Malo JL. Follow-up of occupational asthma due to various agents (abstract). J Allergy Cl in Immunol 1984;
' 73:174A.
703
253. Simonsson B. Haeger-Aronsen B, Sjoberg A , Rolf Ç. Bronchial reactivity after ceased occupa-tional exposure in aluminum-salt asthma in occupa-tional lung disease. Eur J Respir Dis 1981; 62(Suppl:l-2).
254. Brostoff J. Mowbray JF, Kapoor A , Ho i l i lowell SJ, Rudolf M . Saunders KB. 80% of patients with intrinsic asthma are homozygous for H L A -BW6. Lancet 1976; 2:872-3.
255. ^enables VM, Topping MD. Npnn AJ, Howe W, Newman Thylor AJ. Follow-up of ast h ma caused byletrachlorophthalic anhydride (abstract). Am Rev Respir Dis 1985; 13t:AI73.
256. Juniper CP, How MJ. Goodwin BFJ, Kin-shot I A IC. Bacillus subtilis enzymes: a 7 year clin-ical, epidemiological and immunological study of an industrial allergen. J Soc Occup Med 1977; 27:3-12.
257. Bumey P, Chinn S. Defining asthma. A prog-ress report. Paper presented at International Epidemiology Assodation Sdentific Meeting. Van-couver, British Columbia, 1984. (Personal commu-nication.)
Clinical Allergy. 1976. Volume ft. pages 241 250
Bakers' asthma
D . J. H E N D R I C K V R. J. D A V l E S f am! J. P E P Y S *
* Chest Department, Churchill Hospital. Oxford, f Department of Medicine, 5 / Thomas' Hospital, London anil * Department of Clinical Immunology, Cardio-thoracic Institute. Brampton Hospital. London
Summary Bronchial provocation tests by 'occupational* exposure lo dour provoked dual asthmatic reactions accompanied by rhinitis in two atopic bakers engaged in the manufacture of bread and pies. Ingestion tests with uncooked Hour produced no rcaciions.
Skin prick tests with aqueous extracts of fiour produced positive immediate reac-tions in both bakers, and negative reactions in nine of ten atopic asthmatic control subjects with no occupational exposure to flour. Intracutaneous tests, performed in one precipitin negative baker, gave dual responses. Precipitating antibodies to an aqueous extract of flour were found in the unconcentrated serum of the other baker, and not in ten control subjects.
In t roduct ion
In recent years, bronchial provocation tests have been increasingly employed in the investigation of extrinsic asthma, both in the identification of relevant allergens and in the elucidation of underlying immunological mechanisms. Siresemann (1967) and Popa, George & Gâvànescu (1970) demonstrated immediate asthmatic reactions in a number of flour workers following inhalation tests with nebulized extracts o f flour and/or arthropod contaminants, and Lunn & Hughes (1967). using a nebulized grain weevi l extract, noted a dual reaction in a laboratory worker. The immediate reaction was asthmatic, the late reaction chiefly 'alveolar*. More recently Warren, Cherniak & Tsc (1974) observed dual respiratory réactions tonebulized extracts o f grain dust in crain workers. The exact nature of the late responses was unclear.
This paper described two bakers and reports for the first time dual asthmatic rcaciions lo bronchial provocation tests with flour.
Mate r ia l s and methods
Flour Samples were obtained of the wheat and rye flours used by both bakers together with a sample of another wheat flour from a different source. Correspondence : Or D. J. Hcndrick. Chest Department. Churchill Hospital. Oxford.
241
242 />. J. l/endriek. R. J. Dorics am! J. Pepys
Skin tests Modified prick tests were carried out with aqueous extracts of Hour which had been freeze dried and reconstituted in concentrations of I mg/ml and 10 mg/ml in cnrbol-saline/glycerol (50/50, V/V) .
Intracutaneous tests were carricd out with 0 0 2 ml o f t h e flour extracts prepared in the same concentrations in carbol-saline without glycerol.
Precipitin tests Aqueous extracts ofcach flour sample, prepared in a concentration of 30 mg/ml , were used in agar gel double diffusion tests against the unconcentrated sera of both patients and control subjects.
Control subjects Ten adult asthmatic subjects, who were not exposed to flour occupationally, but who were atopic (positive reactions had been obtained on routine skin prick testing to one or more of twenty-three common allergens), were selected at random f rom patients attending the out-patients department of the Brompton Hospital, London. Skin prick tests with the wheat and rye flour extracts were negative in all but one, and precipitin tests were negative in all ten. Intracutaneous tests were not performed.
Inhalation tests The patients were admitted to hospital for bronchial provocation tests which were carried out in thc mornings using thc 'occupational' method previously described (Pickering, Batten & Pepys, 1972). The flour sample under investigation, like the lac-tose control, was heated overnight at 40°C to remove moisture and so create a finer dust. When coolcd, the patients shook 250 g test samples o f flour from one tray to another for up to 30 min in a con fined environment. The exposures were supervised throughout and could have been terminated at once and appropriate treatment instituted had any untoward reaction occurrcd. Baseline readings of F E V , were taken during the hour preceding the exposure and at 10-min intervals during thc following hour. Thereafter hourly readings were recorded until laic evening. Blood total white cc!l counts and absolute eosinophil counts were measured before and 24 hr after thc lests.
Ingestion tests Capsules containing I g of flour were ingested. These tests were otherwise conducted in thc same way as the inhalation tests.
Case reports
Cose I Patient U.H.. male, 33 years, first developed asthma and rhinitis at the age o f 8 years, fhe symptoms were perennial, hut worse in the summer and alter exposure to house
dusl. In l % 2 he began working in the family bakery, and in 1967 he first presented for allergy assessment. He was advised regarding environmental control of house and wheat dusts and given hyposensitization treatment with extracts of house dusl and mixed cereal dusts with some relief. In 1%') he commenced using sodium cromoglycatc ami received a further hyposensitization course with a house dust mile preparation.
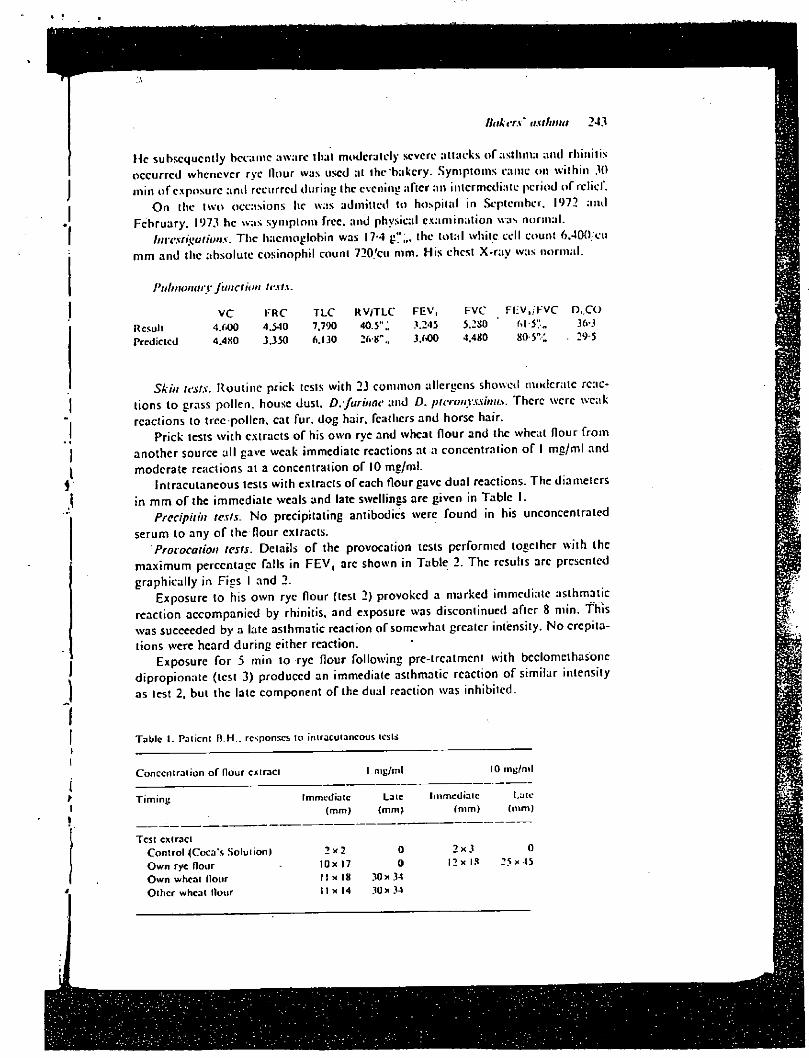
/hikers' asI/mut 243
H e subsequently became aware i l ial moderately severe attacks o f astluna ami rhinitis occurred whenever rye Hour was used at the bakery. Symptoms came on wi th in .10 m in o f exposure ani l recurred during the evening after an intermediate period o f relief.
O n the t w o occasions he was admitted to hospital in September, 1972 and February . 197.1 he was symptom free, and physical examina t ion was normal .
Investigations. T h e haemoglobin was 17-4 g",,, the total white cell count 6 .400/cu m m and the absolute eosinophil count 720/cu mm. His chest X - ray was normal .
Pulmonary function tests.
VC KRC Result 4/tOO 4.540 Predicted 4.4H0 3.350
TLC RV/TLC FEV, 7.790 40.5" „ 3.245 6.130 3.600
FVC FI:V,/> 'VC D..CO 5.2SO ' M 5V„ 36-3 4.480 8 0 5 " ; 29-5
Skin tests. Rout ine prick tests with 23 common allergens showed moderate réac-tions to grass pol len, house dust, D. furinae and 0 . pteronyssinus. There were weak reactions to tree pollen, cat fur, dog hair, feathers and horse hair.
Prick tests w i t h extracts o f his own rye and wheat f lour and the wheat Hour f r o m another source all gave weak immediate reactions at a concentration o f 1 m g / m l and moderate reactions at a concentration o f 10 mg/ml .
Intracutaneous tests wi th extracts o f each flour gave dual reactions. T h e diameters in m m o f the immedia te weals and late swellings are given in Table 1.
Precipitin tests. N o precipitating antibodies were found in his unconcentrated
serum to any o f the flour extracts.
Provocation tests. Details o f the provocation tests performed together w i th the
m a x i m u m percentage falls in F E V , arc shown in Tab le 2. The results are presented
graphical ly in Figs I and 2. Exposure to his o w n rye flour (test 2) provoked a marked immediate asthmatic
reaction accompanied by rhinitis, and exposure was discontinued after 8 nun. This was succeeded by a late asthmatic reaction o f somewhat greater intensity. N o crepita-tions were heard dur ing either reaction.
Exposure for 5 min to rye flour following pre-trcalmcnt with beclomeihasone d ipropionate (test 3) produced an immediate asthmatic reaction o f similar intensity as test 2, but the late component o f the dual reaction was inhibited.
Table I . Patient D.H.. responses to intracutaneous tests
Concentration of flour cxtraci I mg/ml 10 nig/ml
T iming Immediate Late Immediaic Lute (mm) (mm) (mm) (mm)
Test extract Control (Coca's Solution) Own rye flour Own wheat Hour Other wheat flour
2 x 2 0 2 x 3 0 10x 17 0 12x18 25x45 11x18 30x34 I I x 14 .10x 34
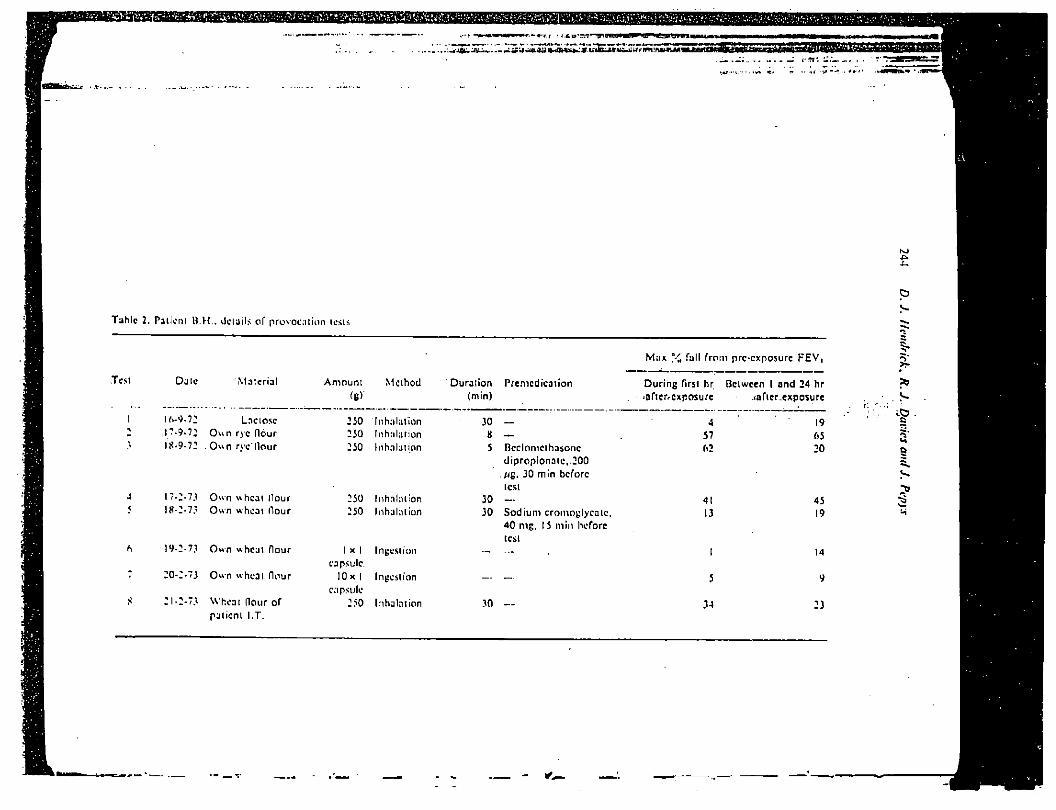
Ï 3h lc 2. Patient B.H.. details of provocation tests
Mux y „ Tall f rom preexposure FEV,
Test Date M a t e r i a l Amount
W Method Duration Premedication
(min)
16-9.72 Laclose ,17-9.7: Own rye flour 18-9-72 , Own rve l l ou r
17-2-73 Own wheat l lour 18-2-7.' Own wheat (lour
i 9-2-73 Own wheat flour
20-2-7J Own wheat Hour
21-2-73 Wheat flour of patient I .T.
250 Inhalation 250 Inhalation 250 Inhalation
250 Inhalation 250 Inhalation
I x I Ingestion capsule.
10x1 Ingestion capsule
250 Inhalation
30 — 8 —
5 Bcclomethasone dipropionatc.,200 //g, 30 min before icsi
30 — 30 Sodium cromoylycatc.
40 nig, 15 min before test
30
Dur ing first hr. Between I and 24 hr jQften-cxposure .tofter.exposure
A 57 62
4! 13
19 65 20
45 19
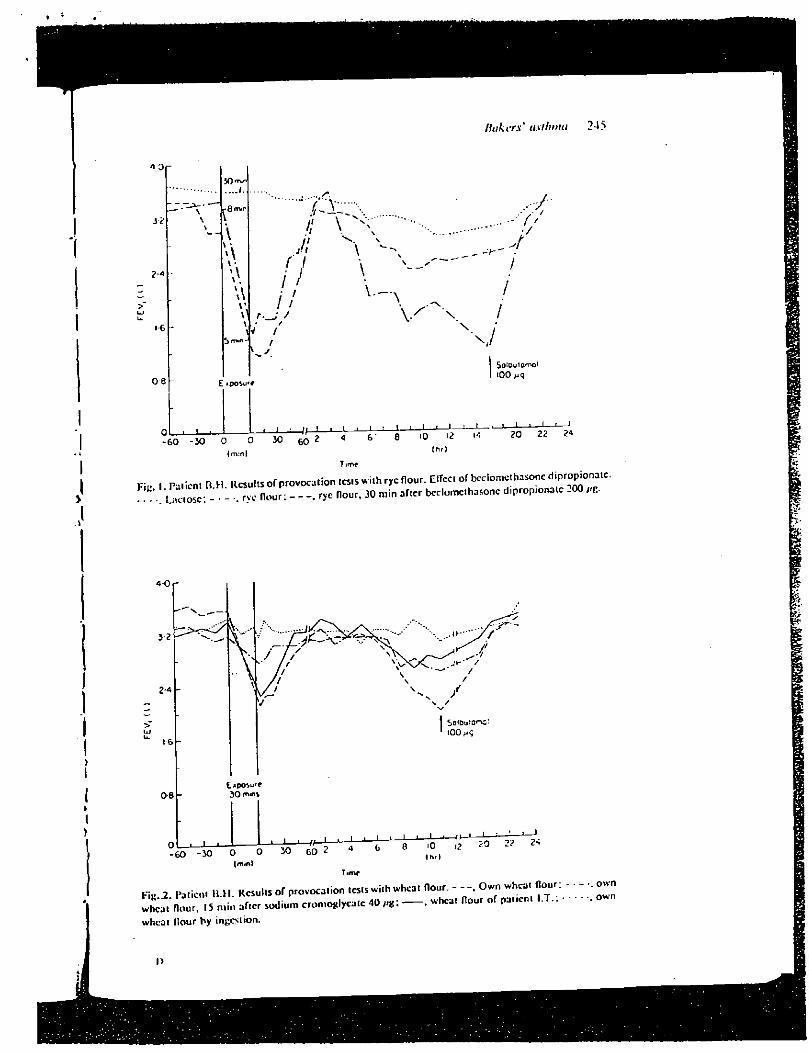
Hakcrs' aslhnui 245
n o
s?.
2 A
16
o-e
Qrmr
w
\ 1
... / * .
,7 // y
, • / V / v . y
" ... // s \ \
\ V—•
J: -r
•7/
i
\ V X /
N/
Eiposu'f
SO'OuiotvjI tOO
(nvn)
- i i I i — I — : — > — i — ' — 1 — 1 — 1
(hr) SO -30 o 0 ' 30 * « 8 .0 « - » 22 2<
T irrvf F i , 1 Patient B H Results of provocation tests with rye flour. ElTcc. of bcclomethasonc diprop.onaic.
-! LKiot,: - - Vryc flour: - - rye flour, 30 min after bcclomcthasonc d.prop.onatc 200 „g .
Q IO I2 ? ? 2* thf I
Time
Fig 2 . Patient 11.11. Results of provocation tests with wheat flour. - Own wheat (lour: wheal flour, .5 min after sodium cromoglyeate 40 — . wheat flour of pat,en, I .T. . wheat Hour by ingestion.
- .. own • own
l>
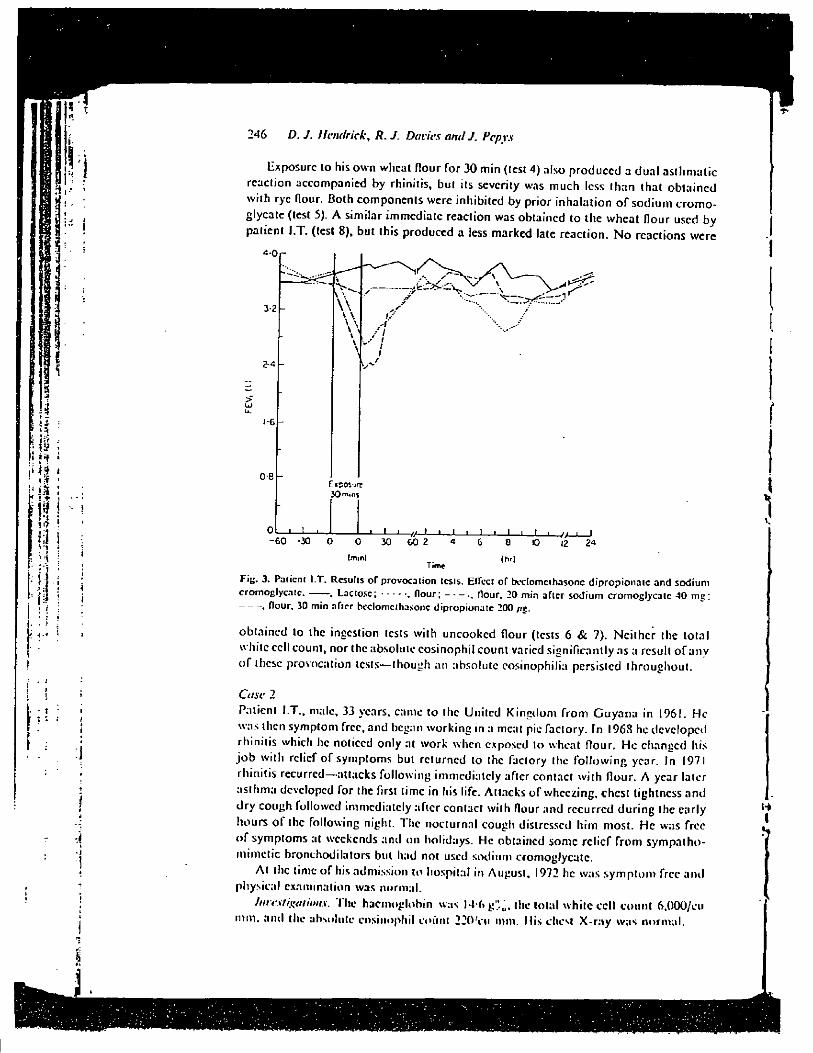
246 D. J. llcnrfrick, R. J. Davies and J. Pepys
Exposure to his own wheat flour for 30 min (test 4) also produced a dua l asthmatic reaction accompanied by rhinitis, but its severity was much less than that obta ined with rye flour. Both components were inhibited by prior inhalat ion o f sodium c romo-glycate (test 5). A similar immediate reaction was obtained to the wheat flour used by patient I .T . (test 8), but this produced a less marked late reaction. N o reactions were
4-0 r
3-2 -
2-4 -
> UJ u. 1 - 6 -
o-e -
V t • . . • . . . i 1 I I I L. 1 1 1 I / / I I - 6 0 -30 0 0 30 6 0 2 4 6 8 10 I2 24
(•Tim) (hr) Time Fi«. 3. Pa lient I.T. Results of provocation tests. ElTect of beclomcthasonc dipropionaic and sodium cromoglycatc. , Laciosc; f lour; Hour. 20 min after sodium cromoglycatc 40 mg;
, flour, 30 min after beclomcthasonc dipropionatc 200 //g.
obtained to the ingestion tests with uncooked flour (tests 6 & 7). Ne i ther the total white cell count, nor the absolute eosinophil count varied significantly as a result o f any o f these provocation tests—though an absolute eosinophil]';» persisted throughout .
Case 2
Patient I .T . , male, 33 years, came to the United K ingdom f r o m G u y a n a in 1961. H e was then symptom free, and began work ing in a meat pie faclory. In 1968 he developed rhinitis which he noticed only at work when exposed to wheat flour. H e changed his j o b with relief o f symptoms but returned lo the faclory the fo l lowing year. In 1971 rhinitis recurred—attacks fol lowing immediately afler conlac! w i th flour. A year later asthma developed for the first l ime in his life. Attacks o f wheezing, chcsl tightness and dry cough followed immediately after contacl with flour and recurred dur ing the early hours o f the following night. The nocturnal cough distressed h im most. H e was free o f symptoms at weekends and on holidays. He obtained some rel ief f rom sympatho-mimetic bronchodilators but had noi used sodium cromoglycatc.
A t the time o f his admission lo hospital in August. 1972 he was s y m p t o m free ami physical examination was normal.
InrcstRations. The haemoglobin was 14-6 g':,u. the total white cell count 6.000/ou m m . and the absolute eosinophil count 2 2 0 V u mm. His cheM X - r a y was normal .
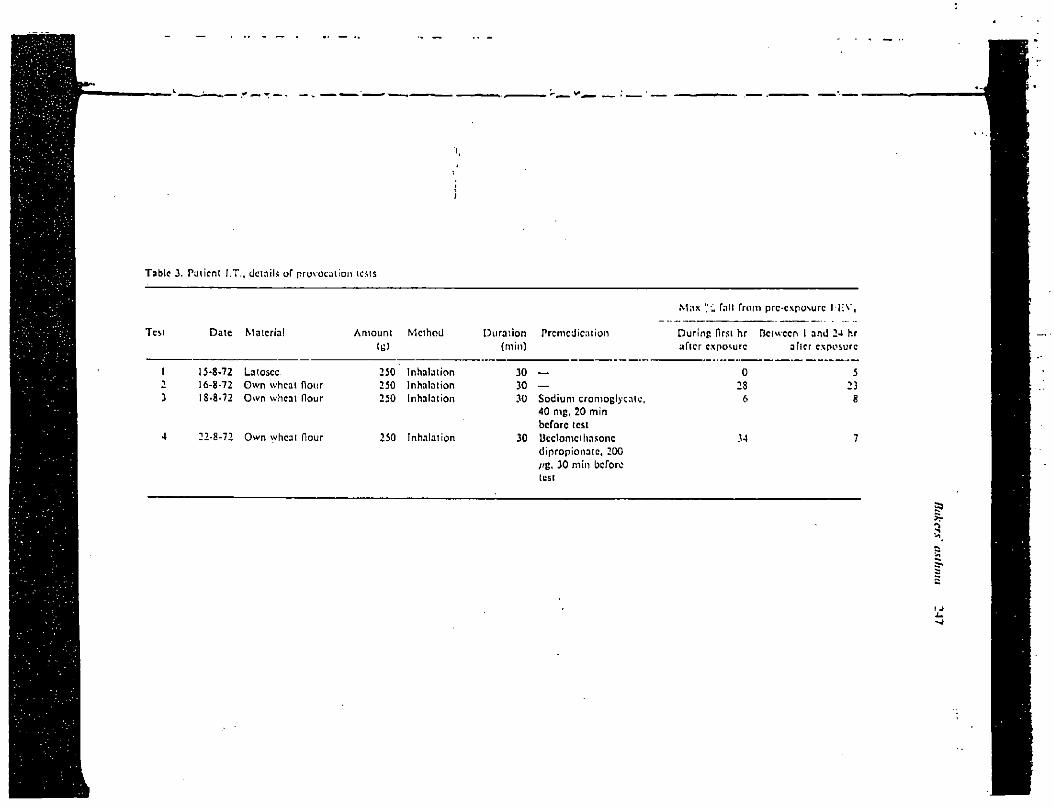
Tabic 3. Patient I.T., details of provocation tests
Test Date Material Amount Method
1 15-8-72 Latosec 250 Inhalation 2 16-8-72 Own wheat Hour 250 Inhalation 3 18-8-72 Own wheat flour 250 Inhalation
4 22-8-72 Own wheat flour 250 Inhalation
Durat ion Premedication (min)
30 — 30 — 30 Sodium cromoglycatc,
40 nig, 20 min before test
30 Ucdomcthnsonc dipropionalc, 200 //g, 30 min before test
Max '".'. fall f rom prc-cxposurc I l ;V ,
Dur ing first hr Between I and 24 hr after exposure after exposure
0 5 28 23
6 8
34 7
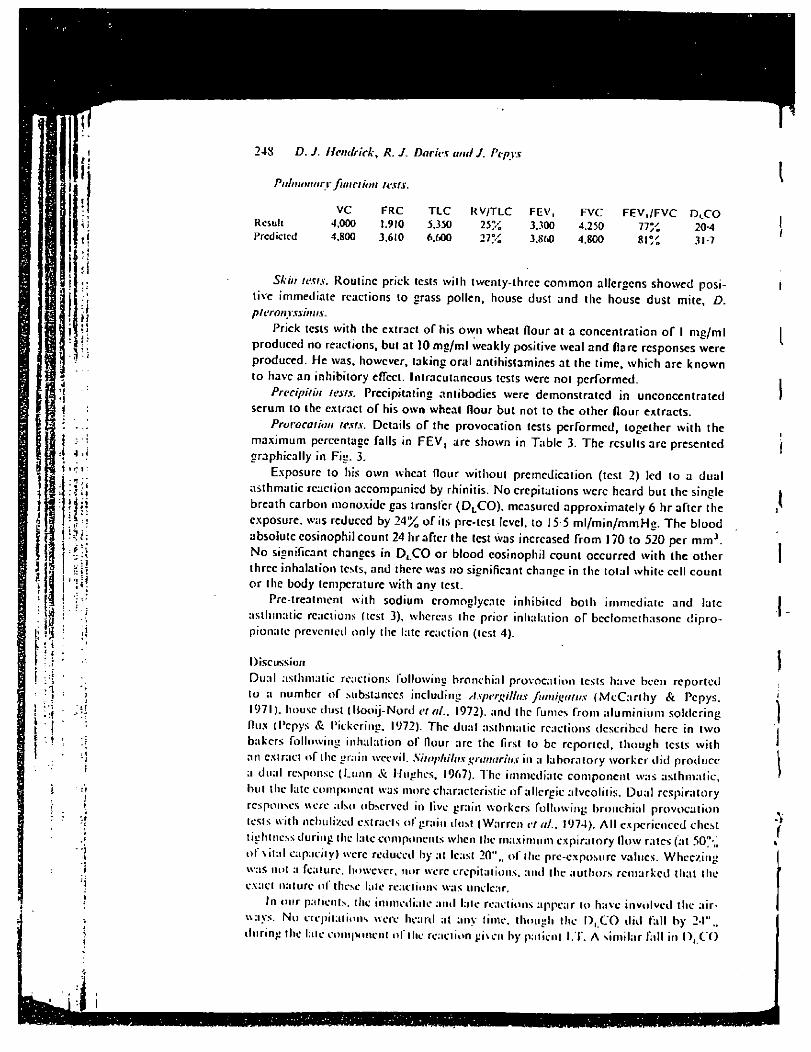
248 D. J. l l cnr f r ick , R. J. Davies and J. Pepys
Pulmonary fund ion lests.
VC FRC Result 4.000 1.910 Predicted 4.800 3.610
TLC RV/TLC FEV, 5.350 25% 3.300 6,600 27% 3.860
FVC FEV./FVC DLCO 4.250 77% 20-4 4.800 81% 31-7
Skin tests. Routine prick tests with twenty-three common allergens showed posi-tive immediate reactions to crass pollen, house dust and thc house dust mite, D. pferonyssinus.
Prick tests with the extract of his own wheat flour at a concentration of I mg/ml produced no reactions, but at 10 mg/ml weakly positive weal and flare responses were produced. He was, however, taking oral antihistamines at thc time, which are known to have an inhibitory eflect. Intracutaneous tests were not performed.
Precipitin tests. Precipitating antibodies were demonstrated in unconcentrated serum to the extract of his own wheat flour but not to the other flour extracts.
Provocation tests. Details of the provocation tests performed, together with the maximum percentage falls in F E V , are shown in Table 3. The results arc presented graphically in Fig. 3.
Exposure to his own wheat flour without premedication (test 2) led to a dual asthmatic reaction accompanicd by rhinitis. No crepitations were heard but the single breath carbon monoxide gas transfer ( D L C O ) , measured approximately 6 hr after the exposure, was reduccd by 24% of its pre-tcst level, to 15-5 m l /m in /mmHc. The blood absolute eosinophil count 24 hr after the test was increased from 170 to 520 per m m J
N o significant chances in D L C O or blood eosinophil count occurred with the other three inhalation tests, and there was no significant chance in thc total white cell count or thc body temperature with any lest.
Pre-treatment with sodium cromoglycatc inhibited both immediate and late asthmatic réactions (test 3). whereas thc prior inhalation of bcclomcthasonc dipro-pionate prevented only the late réaction (test 4).
Discussion
Dual asthmatic reactions following bronchial provocation tests have been reported to a number of substances including Aspergillus fumigutus (McCar thy & Pepys. 1971). house dust ( l looi j -Nord <•/«/., 1972). and thc fumes from aluminium soldering flux (Pepys & Pickering, 1972). Thc dual asthmatic réactions described here in two bakers following inhalation of flour arc thc first to be reported, though tests with an extract of the grain weevil. Sitophilus gratmrius in a laboratory worker did producc a dual response (Lunn & Hughes. 1967). The immediate component was asthmatic, but the late component was more characteristic of allergie alveolitis. Dual respiratory responses were also observed in live grain workers following bronchial provocation tests with nebulized extracts of grain dusl (Warren et ai., 1974). Al l cxpcrienccd chcst tightness during the late components when the maximum expiratory flow rates (at 50/ , , of vital capacity) were reduced by at least 20"., ol" the prc-cxposurc values. Wheezing was not a feature, however, nor were crepitations, and the authors remarked that the exact nature of these laic reactions was unclear.
In our paltcnts. thc immediate and late réactions appear to have involved the air-ways. No crépitations were heard at any time, though Ihe D, C O did fall by 24"., during the late component of the reaction given by palicnt I .T . A similar fall in O, C O
/takers' asthma 249
was observed durini! a laic aslhmalic rcaclion to inhaled benzyl penicillin in a peni-cil l in worker ( Davies. I lciulrick & Pepys. 1974) bul Ihc I ) , C O did nol aller during laic aslhmal ic rcaciions of similar magnitude to wood dusts (Pickering <•/ a l . . 1972). soldering flux fumes (Pepys & Pickering. 1972). or pipcrazinc (Pepys. Pickering & L o u d o n . 1972). T h e significance o f this finding is. at present, unclear.
A l t h o u g h wc have shown previously that sensitized workers engaged in the pro-duct ion o f ampici l l in f rom benzyl penicillin may give similar laic aslhmalic réactions to ihe relevant ant ibiot ic whether inhaled or ingested, the ingestion lests in these bakers w i th up to 10 g o f uncooked flour produced no reactions. This is possibly attr ibutable lo loss o f antigenicity bv digestion, though, in Japan, where buckwheat is widely used in food and ils chaff in padding pillows, asthmatic reactions lo both inhaled and ingested buckwheat-have been described ( M a t s u m u r a et ai. 1964; N a k a m u r a . 1972).
In both patients, prc-ireatment with sodiumcromoglycale inhibi tcd both immediate and late components o f the dual reactions. By contrast, prc-trcatmcnt with the corti-costeroid aerosol, beclomcthasonc dipropionate. had no effect on the immédiate responses though ihc late responses were inhibited. These cffects arc characteristic and
have been reported previously (Pepys et aL 1974). Both patients were atopic subjects in thai both gave immediate skin prick lest
r e a c t i o n s t o a number o f common allergens on routine testing. Positive prick tests were also obtained to extracts o f ihc flour samples studied. These, together with the im-mediate asthmatic and nasal reactions fol lowing the inhalation provocation lests, are suggestive o f l e E mediated type I hypersensitivity (Ce l l & Coombs, 1968). T h e mechanism underlying late asthmatic r e a c t i o n s is controversial. Type 3 hypersensitivity, mediated by complement activating immune complexes o f antigen and precipitating an t ibody has been favoured for some vears but correlations between precipitin levels and disease have proved poor, and Hargreave ct at. ( 1974) have recently suggested that non -prec ip i ta i inc I c E antibodies alone may mediate boih immediate and laic com-ponents o f dual asthmatic reactions. One o f the two bakers described here d.d show a positive precipit in tesi to flour, but ihc other, who was clinically the more sensitive.
d i d n o l . , . . A s a resul t o f these inves t iga t ions the rc lcvance o f inha led flour t o ihe d e v e l o p m e n t
o f asthma and rhinitis was confirmed in both bakers, and the potential protective value o f sodium cromoslycatc was established. By subsequently avoiding undue exposure and by taking.sodium cromoglycatc regularly, both bakers were able to cont inue wi th their occupations.
A c k n o w l e d g m e n t s W c arc nratcful to Miss J. Mitchel l for preparing the flour extracts and for carrying out ihc precipitin tests, IO Miss R. Hawkins , S . R . N . . for performing skin prick tests on the cont ro l subjects and to the Clinical Research Board o f the Brompton Hospital for f inancial support ( D . J . H . ) . The illustrations were kindly prepared by the Medica l I l lustrat ion Department o f the Radclilfc Inf i rmary, Oxford.
References I1OOIJ-NOI>KI>, H.. DIL VKH.S. K.. SLUHM.. H J . & 0«..:, N .G.M. (1972) Laic bronchi:,! o b s t r u c t s
réaction lo experimental inhalation of house dust extract. Chmrut Allerny. 2, 43. OAV.I S K J H I ^I>UH'K.T)J. & LF:»VS. J- (1974) Asthma due lo inhaled chcm.cal ngcnis: anipicil lm.
benzyl penicillin. amino pcnicillanic acid and related substances. Ctinkat Athvxy. 4, 2-7.
250 D. J. l l c n r f r i c k , R. J. Davies and J. Pepys
CELL, P.G.H. & COOMBS. R.R.A. (1968) Clinical Aspects of Immunology. Wackwcll Scientific Publica-tions, Oxford.
HARGREAVE. F . E . , DOLOVICH. J., ROBERTSON. D . G . & KERRIGAN, A . T . ( 1 9 7 4 ) T h c l a t e a s i h m a l i c responses. Canadian Medical Association Journal, 110,415.
L U N N , J . A . & HUGHES, D . T . D . (1967) P u l m o n a r y h y p e r s e n s i t i v i t y t o t h c g r a i n w e e v i l . British Journal
of huiustriaiial Medicine, 24, 158. MATSUMURA, T . , TATENO, K . . Y U G A M I , S. & KUROUME. T . ( 1 9 6 4 ) S i x cases OR b u c k w h e a t a s t h m a
induccd by buckwheat flour attached to buckwheat chaff in pillows. Journal of Asthma Research
1 , 2 1 9 .
MCCARTHY, D.S. & PEPYS, J. (1971) Allergic bronchopulmonary aspergillosis. Clinical immunology: (2) skin, nasal and bronchial tests. Clinical Allergy, 1,415.
NAKAMURA. S. (1972) On occupational allergic asthma of different kinds newly found in our allergy clinic. Journal of Asthma Research, 10, 37.
PEPYS, J . , DAVIES. R J . , BRESUN, A . B . X . , HENDRICK, D . J . & HUTCHCROFT. B .J . ( 1 9 7 4 ) T h e e f f c c i s o f inhaled beclomethasone dipropionate (Becotide) and sodium cromoglycatc on asthmatic reac-tions to provocation tests. Clinical Allergy, 4, 13.
PEPYS. J. & PICKERING, C.A.C. (1972) Asthma due to inhaled chcmical fumes—amino-cthyl ethanola-mine in aluminium soldering flux. Clinical Allergy, 2, 197.
PEPYS, J . . PICKERING. C . A . C . & LOUDON, H . W . G . ( 1 9 7 2 ) A s l h m a d u e t o i n h a l e d c l i n i c a l a g e n t s — piperazinc dihydrochloride. Clinical Allergy, 2, 189.
PICKERING, C . A . C . , BATTEN, J . C . & PEPYS, J . ( 1972 ) A s t h m a d u e t o i n h a l e d w o o d d u s t s — W e s t e r n R e d Cedar and Iroko. Clinical Allergy, 2, 213.
POP A, V.. GEORGE, S.A. & GÂVÂNESCU, O. (1970) Occupational and non-occupational respiratory allergy in bakers. Acta allergotogica, 25, 159.
STRESEMAXN, E. (1967) Results of bronchial testing in bakers. Acta aUcrgologica. 11 (Suppl. 8). 99. WARREN, P., CHER NIA K, R.M. & TSE, K.S. (1974) Hypersensitivity reactions to grain dust. Journal of
Allergy ami Clinical Immunology, 53, 139.
. " ' l ' M I M M l H < \ \l| . \ I »i I \1|- \ \ \ , S 1 . |-lyj
i MIII.Ks Mli IK AHKI IDMil-.M | >KI S |» | . il \ \ | > \ . \ \ . N, 4 .
Evaluation du degré de sensibilisation
aux allergènes professionnels et de l'incidence de l 'asthme
dans une population de boulangers
d 'une industrie de la région liégeoise (*)
M.l\ H K K K I J K M A K T K A U2, J. LAMOTTK', I». ItARTSUl'
Institut E. Malvoz de lu Province de Licgc - Physiopathologie du Travail Ouai du Barbou, Liège
- Se rvicc Médical Intcrcnlreprises - Dir . L. Schillings Bd. de la Sauvenière. Lieue
R E S U M E
Nous avons réalise dans celle élude une évaluation allergologique de boulangers d'une boulangerie industrielle (anamncsc. tests" cutanés, dosages san-guins. épreuves respiratoires avec tests de provoca-tion bronchique à la farine) versus 24 sujets témoins.
Ouinze boulangers étaient exempts de toute symp-tomatologie. Huit sujets souffrant de rhino-conjonc-tivite en relation avec leur travail n'ont présenté aucun test positif, on observe cependant comme chez les boulangers asymptomati'ques. cl plus fréquem-ment que chez les témoins, des réactions douteuses pour le Dermatophagoides Farinac.
Chez les 3 boulangers souffrant d'asthme au con-tact de la farine, les tests cutanés furent positifs au blé et/ou au seigle alors que le R A S T ne l'était que chez l'un d'enire eux. Ils présentèrent tous trois un syndrome obstruciif sévère immédiatement après le test de provocation bronchique spécifique.
D'une façon générale, les tests cuianés se sont révélés plus sensibles que le R A S T . cl le test de provocation bronchique à la farine s'est avéré haute-ment spécifique pour la recherche d'asthme par sensibilisation à la farine.
S A M E N V A T l'I N C
In deze studie. hebben we cen alleruoloeische cviiluatie vcrrichi bij 26 bakkers van cen industr iel bakkcrij (anamncsc. huidiesten. blocddoscringen. ademhalingsproeven hevattend hronchialc provoka-iietest met bloem) versus 24 amiiolcpcrsonen.
y i j l l ien bakkers waicn vrij van aile svniptoniato-logie. Aclu pcrsnnen lijdend aan rhinocônjunclivitis m verband met hun werk hebben ueen positieve test venoond: men merkt nieiieniin \ i p . zoals bij de asynipiomaiisehe bakkers en vaker dan bij de contrô-les. twijfelachtige realties vonr de Derniaiopha«'oï-des Farinae.
Bij de 3 bakkers lijdend aan asima door coniaci met bloc m. werden de huidtesten voor tarwe en/of voor roggc posilief. terwijl de R A S T slechis bij cen van hen postliel was. Zc vertoonden aile drie ecn
ernstig obsiruetief syndroom onmiddeli jk na de spe-eilieke branchiale provokatietest.
Over het algemecn. zijn de huidtesten gevoeliger gebleken dan de R A S T en de bronchiale provokatie-test met bloem is ten zeersie specifiek gebleken voor bel onderzoek van astma door sensibilisatie voor bloem.
I. Introduction — Epidemiologic
Le premier cas d'asthme chez un boulanger fut décrit par Bernardo Ramazzini en 1700.
L'asthme allergique du boulanger, communément appelé farinose, représente une proportion impor-tante des allergies respiratoires professionnelles. Celle sensibilisation semble toutefois diminuer avec les moyens modernes de production (Sutton et coll 19X4. Popa ci coll.. 1970). La prevalence d'allergie respiratoire chez les boulangers varie selon les éludes de 3.1 à 2S % (Thiel. H . . 1983).
En Belgique, depuis 25 ans, 1.073 cas furent reconnus au F .M.P . dont 700 depuis 1981 .soit 1.2 % des maladies professionnelles respiratoires (y com-pris la silicose). Chaque année, en- moyenne 87 nouvelles demandes d'indemnisation sont introdui-tes. le pourcentage de reconnaissance s'élève à 75 % . Parmi ces 1.073 cas reconnus on dénombre 816 boulangers: 934 sujels proviennent de la boulangerie industrielle, les autres cas émanant du secteur agri-cole. d institutions hospitalières, de grandes surfa-ces....
I.e F .M.P . continue acluellemem à indemniser 879 maladies professionnelles chez des boulangers dont M b pour raison d'asthme ei 8 pour autres affections respiratoires. Par comparaison, en R . F . A . , 369 nou-veaux cas sont introduits par an dont 20 % seulement sont indemnisés. En effet. la législation allemande ne prévoit indemnisation que lorsque l'invalidité at-teint 0 M au moins et oblige l'ouvrier a quitter son emploi. Ce second critère est fortement dissuasif
( ' ) ( onnnuniciitmn donnée le «J octobre l')N7 :. la Société M u e de Mi_dtunc et i l Hyp,.,,,, «lu travail d'expression française.
195
I \ : M H IS 11l HI I.l:l ni M NMI'.II |\ \ 11» «S \l \ \IIIKMNh PIO ».SM« INM I s I * \N\ I \l |i HI | \ ||i >\ |i| llli|s| ,\K<il US
compte tenu dos désavantages sociaux cl financiers qu'une reconversion occasionne chez ces travailleurs issus, pour K(l '? des cas. tic petites entreprises familiales (Thiol H . . 1983).
Le taux d'affection respiratoire atteint, selon Thiol. S.4 r/( parmi les apprentis. 12.4 '.v- chez les boulangers ayant moins do 15 ans d'ancienneté ot 23.4 ('/i chez ceux qui ont plus de 15 uns d'ancienneté.
l.o délai d'apparition do la rhino-conjonctivitc varie fortement, la moyenne étant de 9 ans. Pour l'asthme, celte movenne so siluo entre 10 et 14 ans (Popa ot coll.. 1970).
2. Kthiopalholouic
A l'origine dos symptômes respiratoires se re-trouve un mécanisme d'hypersensibilité immédiate de ivpe I à médiation IgE. Los réactions asthmati-ques tardives ne sont cependant pas rares, se dérou-lant 4 à 6 heures après le premier contact allergéni-quo. Le stimulus initial est formé par la liaison entre l'allergène ci les anticorps IgE. Ceci provoque une activation des mastocytes. Los médiateurs broncho-actifs libérés par les cellules (leucotricncs. histamine, prostaglandines) provoquent une bronchoeonstno-tion immédiate. Les médiateurs ohiniiotaetiques qui se libèrent du masiocyto (ECK. N C F — 11MW. P A F . . . . ) entraînent un apport de leucocytes, neutro-p h i l s et éosinophiles. Cos leucocytes sont activés et secrciem à leur tour des médiateurs broncho-actifs qui provoquent la bronchoconstriction tardive (Pau-wels R. . in AUcreolquic Clinique. 19X5).
D'un point de vue clinique, on observe de la toux, dos expectorations accompagnant une dyspnée as-thmatiforme à prédominance hivernale lorsque l'aé-ration du local do travail est plus mauvaise, les svmptômcs apparaissent immédiatement • après le contact mais surtout en fin de travail, c'est-à-dire le malin chez ces travailleurs nocturnes. S'y associent fréquemment rhinite ct/ou conjonctivite (Charpin J.. 1VS6J.
Les allcrgencs en cause connus de longue date appartiennent essentiellement aux protéines des grains do céréales ot dos farines qui en sont extraites. D'autres pneumallergèncs. d'ordre différent, sont à l'origine de certaines sensibilisations. Diverses élu-des ont mis en évidence lo rôle des contaminants de la farine tels les arthropodes (Thiol 11.. 1983. Manis N. . 1954. Neuwell I:, ol C.oo D . . 1936. Loschiavo S.. 197U. Sutton et coll.. 1984). les bactéries et moisissu-res (Klaustennoyer el coll.. 1977).
Antigènes les plus fréquemment rapportés dans la littérature :
a) Les arthropodes
Le rôle des teignes de la farine du genre liphostia appartenant à l'ordre des lépidoptères esl bien connu. A l'ordre des coléoptères appartient le cha-rançon du blé. il esl responsable de sensibilisations de type réaginique ou plus rarement d'alvéolites
I9r>
allergiques extrinsèques de type I I I chez les travail-leurs de la farine (Morichcau-Beauehant cl coll . , 1964). Il est encore appelé communément «punaise de son»», «charançon rouge», «colcoptèrc de la farine ». «colcoptèrc confus de la farine», il s'agit des Tribolium Confusum cl Castancum. La plupart des espèces Tribolium sont sauvages et localisés principa-lement dans les régions intortropieales.
Trois d'entre, elles sont devenues synanthropes cl à peu près cosmopolites : Tribolium Confusum. Cas-tancum et Doslructor. Ces insectes sont très résis-tants et capables de survivre sur une grande variété de matières alimentaires dont le transport commer-cial intercontinental leur a permis d'atteindre des régions qu'elles n'auraient jamais colonisées autre-ment. Omnivores, on les retrouve dans plus de 100 types d'entrepôts. Les farines sont cependant le plus fréquemment infestées, elles prennent alors une coloration grisâtre et parfois une odeur désagréable. Vivant lo plus souvent en lieu clos et chauffé, on n'observe pas de variation saisonnière de leur acti-vité. Celle-ci diminue cependant avec la tempéra-ture. les adultes survivent durant l'hiver dans un état «d'hibernation» relatif. Leur longévité varie de 3 mois à 3 ans (Magis N . . 1954. "Neuwell et G o o . 1936).
Les mesures d'éviction et d'élimination compren-nent la fumigation à l'aide d'insecticides, lo surchauf-fage (une température inférieure à 70" n'altère pas la farine ni les céréales), l'utilisation de sachets élan-ches : sacs de Polyethylene fermés à chaud (Los-chiavo S.. 1970).
A côté de ces espèces décrites plus longuement, les dermatophago'idcs fariuac et tyrophagus putreseen-tiae. acariens domestiques, sont connus pour donner des sensibilisations plus fréquentes et/ou plus impor-tantes chez les boulangers (IJaklo el col.. 19X0. Popa el coll.. 1970. Sullou el coll.. 1984).
b) I.es protéines de céréales
La diversité des allcrgencs provient du nombre de protéines présentes dans chaque type de grains et de la variété dos céréales susceptibles de provoquer line sensibilisation (SutIon el coll.. 1984). Parmi ces céréales figurent essentiellement le froment et le seigle mais aussi l'orge qui leur est apparenté, le riz, l'avoine et le mais, bien que ces derniers soient phylogénétiquement différents cl non utilisés par le secteur qui nous occupe.
Blands ol coll. (1976) démunirent 10 antigènes différents dans un extrait de farine do blé.
Sutton et coll. (1984) isolent et purifient par méthode éloctrophorétique 3 protéines tie la farine do blé présentant une haute spécificité vis-à-vis des lu H issues de sérum de patients sensibilisés à cctlc céréale. Ils observent toutefois une grande diversité d'anticorps d'un sérum à l'autre. Ils déterminent également la nature de ces protéines, la plus grande partie appartenant au groupe des albumines et globu-linos plutôt qu'au groupe gliadine et glulénine moins solubles.
R.v AI. I ^ i II»N M n i . c i u i : ni- SI.NSIHÎI.INA IK»N A I X AI I I-UCKNJ.S I-KOHÎSSIOSNIXλ DANS UNI: I ' (H 'ULATUIN DI: aouï-ANCII-US
Objectifs
Cette etude poursuit deux buts :
Evaluer le degré de sensibilisation aux allcrgencs auxquels les boulangers sont professionnellement exposés en comparaison avec une population témoin professionnellement non exposée.
Objectiver l'incidence d'asthme extrinsèque parmi les boulangers-pâtissiers d'une boulangerie industrielle.
4. Matériel el méthodes
L'entreprise concernée est une boulangerie-pâtis-serie industrielle de la région liégeoise occupant 36 boulangers. 19 briochers!" 14 pâtissiers. 20 expédi-teurs. 3 mécaniciens. 55 camioncurs et 22 employés. Le bâtiment de production renferme deux halls de boulangerie et la pâtisserie, disposés parallèlement. Des dosages atmosphériques de farine furent réalisés durant X heures, le long de ces lignes de fabrication allant du pétrin à l'emballage.
Les endroits particulièrement enfarinés sont : — Le pétrissage où la farine stockée en cuve est
déversée par commande manuelle au-dessus du pétrin.
— Les lignes où se déroulent différents stades de la fabrication du pain : pesage, façonnage.
— Le feuilletage où. dans un local isolé, un condi-tionnement d'air maintient une température con-stante. mais également une grande quantité de farine en suspension.
— L'enfournement. — Le ramassage.
La population témoin comporte 24 sujets dépour-vus d'antécédents héréditaire et personnel d'allergie, non exposés professionnellement à la farine.
Les 26 boulangers et pâtissiers ou briochers consti-tuant le groupe étudié appartiennent aux différents points de production de l'entreprise, qu'ils soient symptomatiques d'allergie ou non. Ils seront par la suite confondus dans le terme «boulanccrs».
Furent pris en compte l'âge des sujets (entre 20 et 60 ans), le tabagisme, les antécédents allergiques et autres, la durée d'exposition professionnelle, le type
line i-
de symptômes manifestés. Chaque sujet a subi un anamnèse médicale et professionnelle, des tests cul; nés (prick-tests Uencaul) à l'aide de pneumallergè-ncs courants : poussière de maison, derniatophacoï-des pteronyssinus. dermatophasoïdes farinac. epi-tlïélia de chiens, de chais, pollens de graminées, el d'allergcnes professionnels: urains dc^ froment de seigle, d'orge, d'avoine, de riz et de maïs, farines mélangées, farine de blé entier, farine de seiyle. Tribolium confusum. ' *
Nous avons systématiquement mesuré I eosinophi-lic sanguine relative et absolue, les luE totales el spécifiques (Prist cl Rasl de Pharmacia) reprenant quelques pneumallergènes courants (dermatophagoï-des pteronyssinus el dermatophaiioïdes farinae pol-
lens de graminées, mixture d'épilhélia) el des aller-gènes professionnels (froment, seigle, orge, avoine, riz. levure, gluten).
Une spiromctric fui enfin réalisée chez chaque personne lors du test de provocation bronchique spécifique à la farine avec enregistrement des C V , V E M S . M E F 50. capacilc synchrone avant l'épreuve el I min puis 15 min après. Le lest de provocation bronchique spécifique consistait à faire inhaler, via un embout buccal, de l'air chargé des farines utilisées dans l'entreprise pendant 3 fois 1 min. Un contrôle du tracé d'asvnchronisme ventilaloire enregistré par la méthode de l'interruption du courant aérien (Petit J .M. cl coll., 1971) fut réalisé avant le lest, entre chaque période d'inhalation et 15 min après, en complément des mesures précédentes. 24 sujets té-moins furent complètement invesligués de même que 26 boulangers (Tableau I ) . Les moyennes d'âge de ces deux populations sont respectivement de 36,3 ans et 34,7 ans.
Tableau I Symptômes rapportés
l | Nombre
| Açc
! TJIIMC
Durée d'exposition
Aniëcedents allergiques
Symptômes j
24
23 — 5X (m = -V..3)
12 NF y F 3 AF
lU»nl:ingci s-Pâtissiers
26
2 2 - 5 1 (m - 34.7)
L(>NF IDF
IX mois —» 39 ans (m » 15.5 ans)
fi 7 rhinite I prurit oculaire 3 asllune + U.C.
Parmi les témoins on dénombre 12 non-fumeurs, 9 fumeurs cl 3 anciens fumeurs, parmi les boulangers 16 non-fumeurs et 10 fumeurs. Dans ce dernier groupe, la durée d'exposition varie de 18 mois à 39 ans. avec une moyenne de 15,5 ans.
Les témoins sont bien entendu asymptomatiques alors qu'on relève parmi les boulangers, lorsqu'ils sont au contact de la farine : 1 cas de rhinite. I prurit oculaire. 3 cas d'asthme avec rhino-coiijoncliviie.
Les tests statistiques appliqués furent ceux du X : , du X- corrigé, du i de Student et le test d'indépen-dance.
5. Résultats
L lests cutanés : ils furent exprimés en scores allant de 0 a + + . Le test est considéré comme positif s i esl supérieur à (Thiel I L , 1983. Stevens E. in Allergologie Clinique. 19K5, IJouiin et coll. in Aller-gology. 1986).
IV M I.XII'-MU \: S Al 1 I l<t <LSI S l'IC >1 I.WH 'NM I N I i.\N\ l'Sl m m A | |l .N 1.1; |l« Il i|.ANI ll-.KS
Les allcrgènes soni séparés eu 2 croupes :
1) allcrgènes courants
poussière tic maison ( H d ) . dcrmatophagnïdes pteronyssinus ( D t Pt). dermatophagoïdes farinae ( D t K a ). pollens de graminées (Ci), epithelium de chiens ( D g ) . epithelium de chats (C l ) :
2) allcrgènes professionnels
grains de froment ( F ) , grains de seigle (S), grains d'orge ( 0 ) . grains d'avoine ( A ) , grains de ri/. ( K ) . grains de maïs ( M ) , farines mélangées (F in) , farine de hlé entier (Fb ) . farine de seigle (Fs) . Tr ibo l ium Confusum (Te) .
Le tableau 11 nous montre le nombre de sujets ayant au moins une réponse positive pour chaque groupe d'allergènes. Concernant les allergenes cou-rants. on observe 25 c/c de réactions positives chez les témoins ci 30.7 chez les boulangers, sans diffé-rence statistiquement significative "entre les deux populations. Concenam les allcrgènes profession-nels. on observe un sujet témoin réagissant a l'en-semble des pneumallergènes. en le réinterrogeant, nous apprendrons qu'i l présente-une urticaire au contaci des foins. Parmi les boulangers. 3 d'entre-eux réagissent j i l'un ou l'autre allergèiîe professionnel, i! s'agii des 3 asthmatiques.
Tableau I I Tests cutanés : sujets ayant au moins une réponse
positive par groupe d'allergènes
i T c n i o i n s n s : U l l i u i l n n p c t ? » n » 2 6
Allcrycnes
courants n = fi
; n
-i i i i I ;
6 I ; i l
professionnels n = m J.2
30.7
11.5
Lorsque l'on compare, la sensibilisation cutanée pour des acariens domestiques et des contaminants de la farine (Tableau I I I ) , on n'observe pas de différence statistiquement significative entre les deux populations.
Lorsque l'on scinde la population de boulangers en 3 groupes en fonction des symptômes, on observe au table au I V que la majorité îles boulangers réagissant aux allcrgènes courants sont asymptoinaliques. que 2 boulangers asthmatiques sont sensibilisés pour ces allcrgènes courants, qu'aucun sujet présentant de la rhino-conjonclivite ne réagit ni aux allcrgènes cou-rants ni aux allcrgènes professionnels.
Tableau I V '/c.vr.v cutanés : résultais positifs pour au moins un allcrgène du groupe eu fonction des symptômes chez
les boulangers
A s y m p i o . K h i n o - c o u j . A s t h m e
n - 1 5 n « S i» * 3
A I l e f y e n e s
n n % n n/ m
c o u r a n t s
n = 6 *
•ai n (l t ) ) 6 6 . 6 %
prolcSNHMinclN n - I I )
0 (i n % 3 K M ) %
A u tableau V . on note à nouveau la grande majorité des réactions positives pour les acariens et les contaminants de la farine chez les boulangers asymptomatiques.
Tableau V
7>i7.v cutanés : résultats positifs aux D t Pt, D t Fa . T.c . en fonction des symptômes chez les boulangers
A lté rue ucs
i Dt Pt
r ! Dt Fa
T.c.
- • • • •
Asytnpto. Rluno-conj. Asthme n = 15 11 = = K n » 3
j 26/» r'o 0 t) r/b 1 33.3 %
5 33.3 rr (1 (1 % (l t)
T 13.3 % (I (I % u o %
Tableau I I I Tests attunes : sujets positifs au D i Pt. Dt Fa. T.c .
Aller tenes
. Dt Pt i Dt Fa T.c.
198
"I éinoins n • 2-1
i n • ;
I :n.s i s.3 '
iloulunucrs n i. 2i>
t • ! iv.: iy.2 n
7.7 '; ;
En ce qui concerne ces 3 derniers allcrgènes. on observe généralement chez un même individu, des réactions positives aux 3 arthropodes, les personnes sensibilisées au Tr ibol ium Confusum le soul tou-jours. et de façon plus importante, aux dermatopha-goides pteronyssinus. qu'il s'agisse de témoins ou de boulangers exposés.
2. Dusages sanguins: au tableau V I . les valeurs deosinophil ic relative cl absolue sont en moyenne basses dans les deux populations, sans relation avec la présence de symptôme chez les boulangers. Les valeurs moyennes d ' IgE totales sont également géné-ralement basses, les plus élevées étant observées
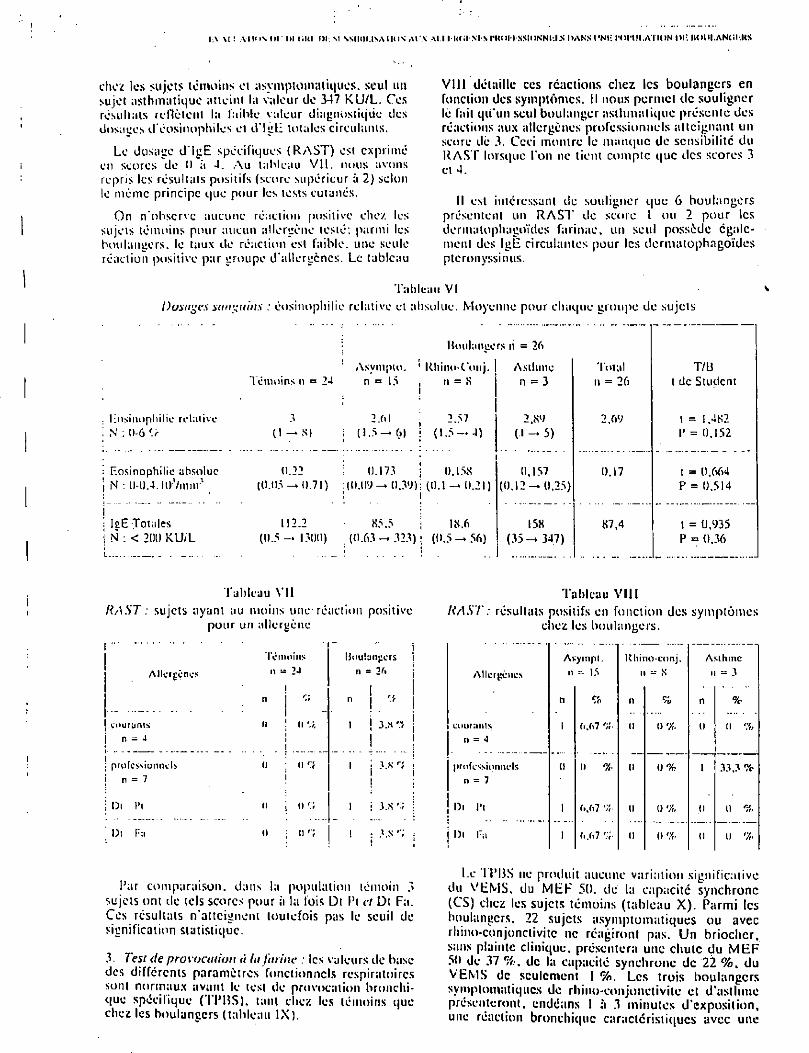
I.\ M '. AII<|\ or III OKI IH-. M NSIHH.JSAIM1S AtX Al l I IMil Nl N PUOI I SSIONNIJ.S DANS I'NIi I'OrtJI.AMON l»l:. IIOIM.ANCI.KS
chez les sujets témoins et asymptomatiques. seul un sujet asthmatique atteint la valeur de 347 K U / L . Ces résultats reflètent la faible valeur diagnostique des dosages d'éosinophiles et d ' IgE totales circulants.
Le dosage d ' IgE spécifiques ( R A S T ) est exprimé en scores de 0 à 4. A u tableau V I L nous avons repris les résultats positifs (score supérieur à 2) selon le même principe que pour les tests cutanés.
On n'observe aucune réaction positive chez les sujets témoins-pour aucun allergène testé: parmi les boulangers, le taux de réaction est faible, une seule réaction positive par groupe d'allergènes. Le tableau
V I I I détaille ces réactions chez les boulangers en fonction des symptômes. Il nous permet de souligner le fait qu'un seul boulanger asthmatique présente des réactions aux allergènes professionnels atteignant un score dè 3. Ceci montre le manque de sensibilité du R A S T lorsque l'on ne tient compte que des scores 3 et 4.
Il esl intéressant de souligner que 6 boulangers présentent un R A S T de score l ou 2 pour les dermalophagoïdos farinae. un seul possède égale-ment des IgE circulâmes pour les dermalophagoïdes pteronyssinus.
Tableau VI Dosages sanguins : éosinophilie relative et absolue. Moyenne pour chaque groupe de sujets
. Eos inoph i l i c re la t ive i N : 0-6
: Eosinophilic absolue j N : 0-0.4. loVmnv
; I2E Totales j N : < 2(H) K U / L
Hinilaneers ri = 26
Asvmpio. ' Rhino-Conj. I Asthme Témoins n = 24 n = 15 i n = S
l
2.fil 2.57 ( I —-NI i (1.5-6) i (1.5— A) 1 •
0.22 0.173 | IÏ.15S (0.05 — 0.71) :(tuiy — 0.39); (O.i — 0.21)
! i
112.2 85.5 I 1S.6 (11.5 — 1300) {0.63 323) ; (0.5 — 56)
n = 3
2.«y (•1-5)
0,157 (0.12 — 0.25)
158 (35 —* 347)
Toi al n = 26
2,69
0.17
87,4
T/L3 l de Student
1 = 1.482 I' = 0.152
t = 0,664 P = 0,514
t = 0,935 P = 0,36
Tableau V I I RAST : sujets ayant au moins une-réaction positive
pour un allergène
Allerpcncs
courants n = 4
professionnels n = 7
l)t Pi
l)t Fa
Témoins
n 24 1
n
n J ( 1
S
0 : n "t i
n j u ;
n ; n
Tableau V I I I RAST : résultais positifs en fonction des symptômes
chez les boulangers.
j IJoubnj:crs ; 11 = j Allcrgencs
Avyinpl. n s. 15
Uhino-conj. n X
Asthme n => 3
n ! . "' ! n e/o 11 % n %
1 j 3.x'.i j ! !
courants il = 4
l (i.67 % U (1% U Il %
i : professionnels 11 = 7
1) 11 % (1 0 % 1 33.3 %
l i 3.S j l)t l'i 1 (1 u % 0 (1 %
l : 3.s'1; : » j l)t l:a 1 M»7 (1 u % 0 () %
Par comparaison, dans la population témoin 3 sujets ont de tels scores pour à la fois D l Pt et Dt Fa. Ces résultats n'atteignent toutefois pas le seuil de signification statistique.
3. Test de prov ocation la farine : les valeurs de base des différents paramètres fonctionnels respiratoires sont normaux avant le lest de provocation bronchi-que spécifique (TPIJS). tant chez les témoins que chez les boulangers (tableau I X ) .
Le I PUS ne produit aucune variation significative du V E M S . du M E F 50. de la capacité synchrone (CS) chez les sujets témoins (tableau X ) . Parmi les boulangers, 22 sujets asymptomatiques ou avec rhino-conjonclivitc ne réagiront pas. Un briochcr. sans plainte clinique, présentera une chute du M E F 50 de 37 de la capacité synchrone de 22 % . du V E M S de seulement I % . Les trois boulangers sympiomatiqucs de rhino-eonjonctivitc el d'aslhme présenteront, endéans I à 3 minutes d'exposition, une réaction bronchique caractéristiques avec une
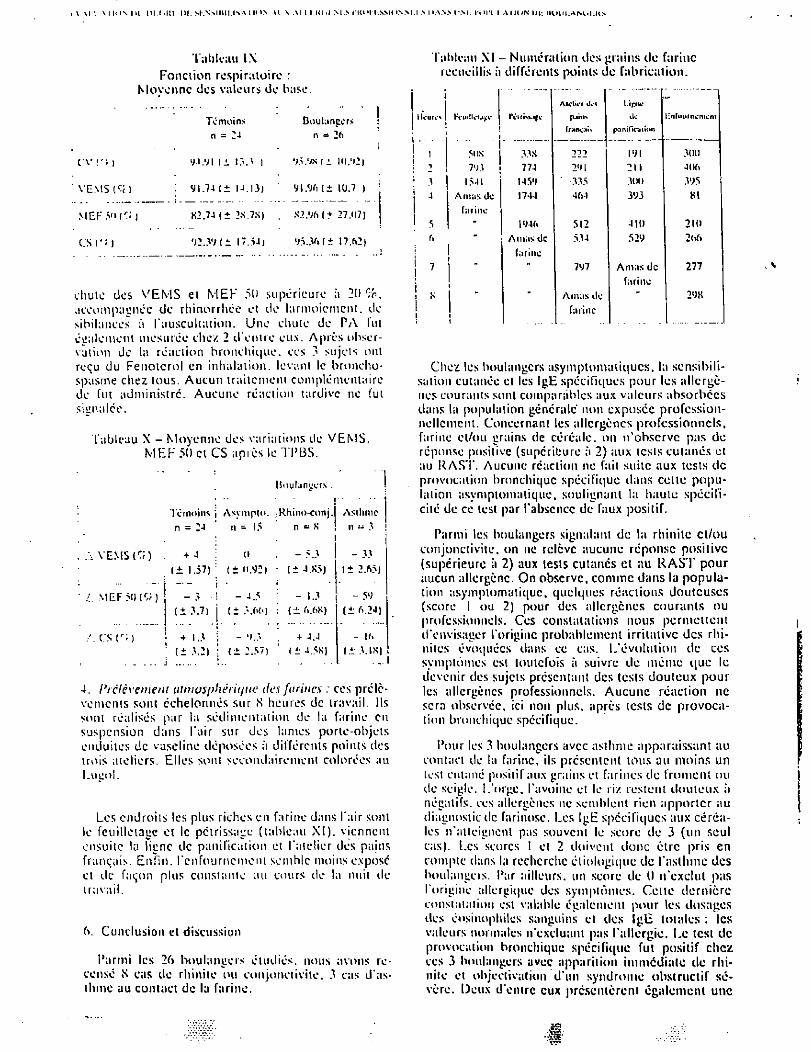
I \ M V 11< I >t IKI IM. M'.SMWUW IH'S Al \ .\l I I Kl >1 M S IIU 'I I.NMUNM.I .S 1I.A.N.N IM; RUN I,A I H IN I)I: HlitU.AMil'.HN
Tableau l \ Fonction respiratoire :
Nlovennc des valeurs de base
Tableau XI - Numération des grains de farine recueillis à différents points de fabrication.
c\-1"> )
VEMS C* I
MEK SUC:; »
es c ; i
Témoins n = :J
V-».VI li I.».* )
91.74 (± N.I3)
82.74 I ± 2S.7SJ
V2.3V(± 17.>4)
Douhtnpcrs n = 26
VxVxii Hl.«i>j
Vl.% (± 10.7 )
S2.%(± 27.U7)
V5.36(± 17.62)
n = 24 n 15 n « K n 3
+ 4 t» - 5.3 - 33 ± 1.57)
: (± n.92) -(± 4.X5) if
tj b»
v«
- ;> ! -4.5 -(± 3.7) j ( ± 3 . 6 6 ) : ( ± 6.68) ( ± 6.2J)
+ 1.3 î - •).;, + 4.4 - 16
(± 3.2) ; t± 2.57» (± 4.5*) f.i 3.IX)
chute des V E M S et M E F 51» supérieure à 2(1%. accompagnée de rhinorrhée et de larmoiement, de sibilances à l'auscultation. Une chute de PA fut également mesurée chez 2 d'entre eux. Après obser-vation de la réaction bronchique, ces 3 sujels ont reçu du Fenotcrol en inhalation, levant le broncho-spasme citez tous. Aucun traitement complémentaire de fut administre. Aucune réaction tardive ne fut signalée.
Tableau X - Moyenne des variations de V E M S . M E F 50 et CS après le TPBS.
Boulangers . |
Témoins j Asympto. -Rhino-conj. Asthme
. VENISE)
: M E F (Cr )
;\c/sr;)
4. Prélèvement atmosphérique des farines : ces prélè-vements sont échelonnés sur S heures de travail. Ils sont réalisés par la sédimentat ion de la farine en suspension dans l 'air sur des lames porte-objets enduites de vaseline déposées ft différents points des trois ateliers. Elles sont secondairement colorées au Lueol .
Les endroits les plus riches en farine dans l'air sont le feuilletage et le pétrissage (tableau X I ) . viennent ensuite la ligne de panification et l'atelier des pains français. Enfin, l'enfournement semble moins expose et de façon plus constante au cours tie la nuit de travail.
Conclusion et discussion
Parmi les 26 boulangers étudiés, nous avons re-censé S cas de rhinite ou conjonctivite. 3 cas d'as-thme au contact de la farine.
| Heure* | K*uitk'M|:c
i S
jus 7VJ 1541
Amas Oc fiirinc
T
Alclii'l îles l.ipilC (uin> ik- tvnfouincniont fiMn<;ii\ pa ni (Va lion
33.X 222 IVI 300 774 2'M 211 406 145V ' 335 3(H) 3V5 1744 464 3V3 81
IV46 512 410 210 Amas de 534 52V 2(>6 fiirinc
•• 7V7 Amas de 277 fiirinc
• Amiis île - 2V8 farine
Chez les boulangers asymptomatiques, la sensibili-sation cutanée el les IgE spécifiques pour les allcrgè-nes courants sont comparables aux valeurs absorbées dans la population générale non exposée profession-nellement. Concernant les allcrgènes professionnels, farine et/ou grains de céréale, on n'observe pas de réponse positive (supérieure à 2) aux tcsls cutanés el au RAST. Aucune réaction ne fait suite aux tesls de provocation bronchique spécifique dans celte popu-lation asymptomatique, soulignant la haute spécifi-cité de ce lesi par l'absence de faux positif.
Parmi les boulangers signalait! de la rhinite et/ou conjonctivite, on ne relève aucune réponse positive (supérieure à 2) aux tesls cutanés et au R A S T pour aucun allergènc. On observe, comme dans la popula-tion asymptomatique, quelques réactions douteuses (score l ou 2) pour des allcrgènes courants ou professionnels. Ces constalations nous permettent d'envisager l'origine probablement irritative des rhi-nites évoquées dans ce cas. L'évolution de ces symptômes esi toutefois à suivre de même que le devenir des sujets présentant des lests douteux pour les allcrgènes professionnels. Aucune réaction ne sera observée, ici non plus, après tcsls de provoca-tion bronchique spécifique.
Pour les 3 boulangers avec asthme apparaissant au contact de la farine, ils présentent tous au moins un te si cutané positif aux grains et farines de froment ou de seigle. L'orge, l'avoine el le riz restent douteux à négatifs, ces allcrgènes ne semblent rien apporter au diagnostic de farinose. Les IgE spécifiques aux céréa-les n'atteignent pas souvent le score de 3 (un seul cas). Les scores I el 2 doivent donc être pris en compte dans la recherche éliologique de l'asthme des boulangers. Par ailleurs, un score de 0 n'exclut pas l'origine allergique des symptômes. Celle dernière constatation est valable également pour les dosages des eosinophils sanguins el des IgE totales : les valeurs normales n'excluant pas l'allergie. Le test de provocation bronchique spécifique fut positif chez ces 3 boulangers avec apparition immédiate de rhi-nite et objcclivalion d'un syndrome obstructif sé-vère. Deux d'entre eux présentèrent également une
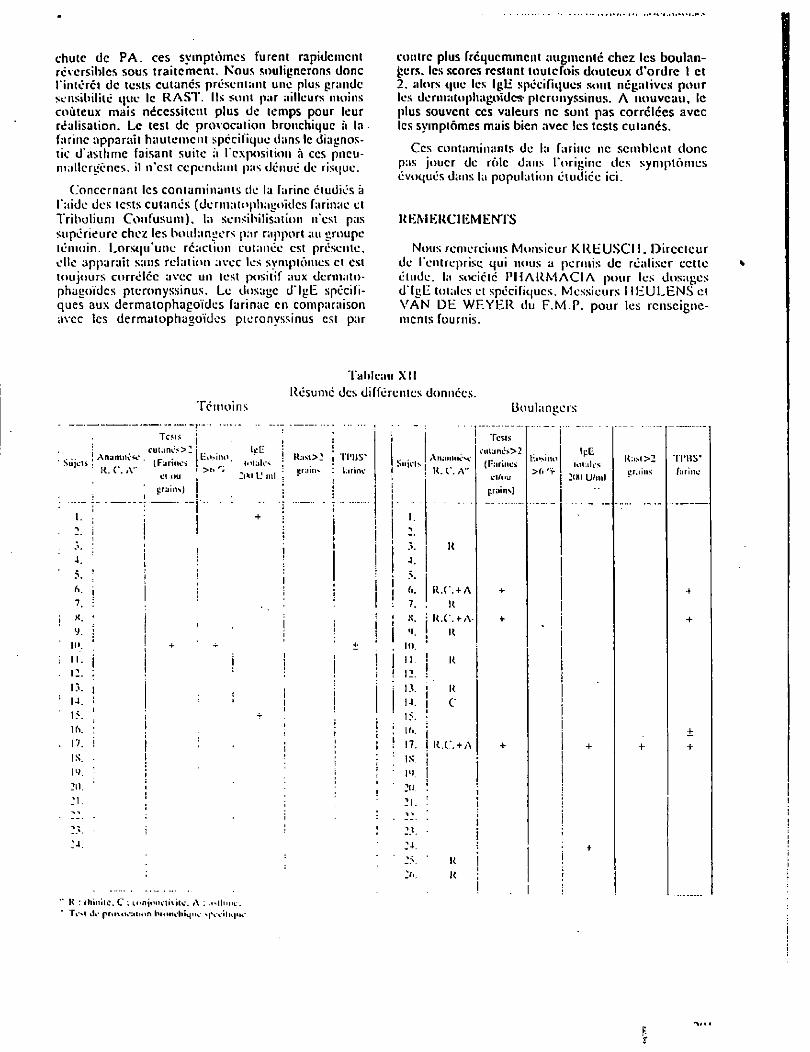
chute de P A . ces symptômes furent rapidement réversibles sous traitement. Nous soulignerons donc l'intérêt de tests cutanés présentant une plus grande sensibilité que le R A S T . Ils sont par ailleurs moins coûteux mais nécessitent plus de temps pour leur réalisation. Le test de provocation bronchique à la farine apparaît hautement spécifique dans le diagnos-tic d'asthme faisant suite à l'exposition à ces pneu-mallcrgènes. il n'est cependant pas dénué de risque.
Concernant les contaminants de la farine étudiés à l'aide des tests cutanés (dermatophagoïdes farinae et Tribol ium Confusum), la sensibilisation n'est pas supérieure chez les boulangers par rapport au groupe témoin. Lorsqu'une réaction cutanée est présente, elle apparaît sans relation avec les symptômes et est toujours corréléc avec un test positif aux dermato-phagoïdes pteronyssinus. Le dosage d' IgE spécifi-ques aux dermatophagoïdes farinae en comparaison avec les dermatophagoïdes pteronyssinus est par
contre plus fréquemment augmente chez les boulan-gers. les scores restant toutefois douteux d'ordre 1 et 2. alors que les Ig l i spécifiques sont négatives pour les dermatophagoldcif pteronyssinus. A nouveau, le plus souvent ces valeurs ne sont pas correlées avec les symptômes mais bien avec les tests cutanés.
Ces contaminants de la farine ne semblent donc pas jouer de rôle dans l'origine des symptômes évoqués dans la population étudiée ici.
REMERCIEMENTS
Nous remercions Monsieur K R E U S C I 1 . Directeur de l'entreprise, qui nous a permis de réaliser cctte élude, la société P H A R M A C I A pour les dosages d ' IuE totales el spécifiques. Messieurs I l l i U L E N S cl V A N D E W E Y E R du F . M . P . pour les renseigne-ments fournis.
Témoins
Tableau X I ! Résumé des différentes données.
Boulaneers
Sujets ! i Anamnësc K. C. A"
6. 7. X.
y. 10. n. 12. 13. u. 15. 16.
17. 1S. N . 20.
2 1 .
M.
Tots cutancs>2 (Farine»
ci nu train-»)
lîo>ino IcU
L' ml
K : ttiiniic. C : lonjunetititc. A : .«-tlimc. rvl île prmtuMlmn bronchique »[Veilk|tie
Rast>: i>r;iinx
TI'BS* farine Su jet
I !
AltilMtMlSc U. C. A"
R.C. + A K
R.C.+A-K
K
4.
5. fi. 7. X. «J.
in. 11.
i:. : 13. j R N. I C 15. ! i*. j 17. I K.C. + A IS. j 1". I 2 u . i
|4.
u X K
Tests eutanes>2 (Farines et/ou grains)
Ht «si HO >6
rf
IpE loi aies :m U/ml
K:isi >2 crains
TIMIS* farine
> - — 'N Dl: | l ( ) | >| A N l i l . l i s
KEFKRKNCES
UAL'lt x.. DOKSdl \V\. VON I ll lil- v
Î ^ U m ^ m : , n d l U n - , , a s l h m :»- Z-Hnuikrs
"Al.DO 11.A.. KRILIS S.. WKICM FY C w i, - M , inhaled Hour ^ ^ a l ^ S ^
V I S * " ! * K " - CHAN-
C I I A ^ J" - Edition Flammarion. 7-1.1. 7JX.
. ' w ' w . ' : m d r h m , , , $ - V ™ - Kl in - P,WU,,«. .SV I 'OI 'A v . . ( i A V A N P W A «
M < m ^ ; m r T A l T " A N T , , l ( I S O N J - " A i E A N r
NI:W.HMi,!m us° I' ~
l1,>: "f »>'
Klin — pneuntol .Vi'v.
D K H U E T M. . SAHUAII A. , I . , SCI.I.IN J.. HONNEAU J R - • I » I.m«,, and :, l l ,.,,v », Ho,,, i „ N,, j i ^ Alleru — Immunol 17-^. \ *» trai l .
I».. I'JËFLOIUN - STOLZ
Acia-iillcrgulitgica 2K, 1 4 2 . V V , , ' " n g l c , m " " ' « "Sanon.
| yx : J m l n J - r j x — Min — I'ncumol .lft/7. .11X0:2.
KENTNER M H A R T U N G M. . T I I U R A U F j.. KOSTIER .o Z ïh 7"
UC 1,f'mr,,,,ll,
!:ic:i1
inh.lminn h-, W ï«pi/ « r y ^ S T " : ^ ! ? , 'r ' ' ^ W - r f T -I«;n: < f.t.x — Kim __ I'ncuimil Mt/4. ISj.lsv.
I -OSCHIAVO S R — j - i «• , , acelanilidc l o p r o l y l i ^ Z ^ ^ Ï 1 ~ ' ~ , r i » « » l duet-; insects. F ^ d i ï c h ^ ^
I 'OI 'A V.. ( ÎAVANCSCA G ... n n
I ' l t K - I I A R U M . o . . R Y A N Ci.. MUSK A W - W h , „ n
I ' l 'O l . l l iS I : S.. ( . 'ORSI fn it rv .• treatment TT, cromoglycatc in [he
SCHULTZC-WCRNINGHAUS G.. SCWARTING H M
surroN R.. SKLRR,,-, J.M.. I I A L I 3 0 u.a.. W K l c ; L 1, Y
VwlàngcS'S;»1-- - KMn -
I I I I E I I I . — CJccup:iii.„1:i(ly inducal ..bsiruclivc -,irw,v . Ik.- ,
I R l l i H K i ( ; . . T I I U E R A U F j . . m n i - R A . , w r i r i P O
U'lll. 2.12-2.15 IV7(i Arhci[-S(izi;i| - l'r;,vcnliv M,-d U ' < A I I I I !>..(;. C-UNNINCiTON A .M. . S E Y M O U R W I I
1979. environments. Clinical allergy 9. MJ-SfiJ,
WOlTOUïTZ U J _ i>..i. . .. ki:mkt I l / l 1 l^NS. d ,SC; ,>C" - lun^en-
pean Hypersensitivity in Coffee Workers' Asthma: A Clinical and "mmunological Appraisal
°resented by Samuel B. Lehrer, Ph.D.
More than 20 mill ion people are employed by the coffee industry. The Uni ted States is the major
nporter ol' codec. Recent years have seen a gradual ecline in the number of coffee manufacturers and
employees in the United Stales because of consolidation rends and increasing mechanization. In 1982, there /ere 150 coffee companies in the United States with a
total of 11.800 workers. Numerous reports of allergic reactions among coffee
corkers were made in the 1950s and 1960s. Coffee .ndustrv workers develop occupational asthma, rhinitis, or dermatitis. The nature of coffee bean allergen was
onflictingly reported to be chlorogenic acid in green •offee beans or protein in castor and green coft'ee beans
by different investigators in the early 1960s. Lehrer loted that the role of chlorogenic acid as an allergen low is doubtful.
Dur ing the last 20 years, there have been nine reports of occupational allergic reactions in the coffee industry, exclusively in coffee workers during manufacturing rather than in growers. Most of these cited the green coffee bean or the castor bean as the causative agent. Symptoms included wheezing and shortness of breath, rhinitis, and conjunctivitis.
Lehrer presented data from his studies of coffee work-ers. The symptomatic coffee workers had positive skin test reactions to extracts of green coffee bean and coffee dusl. The asymptomatic coffee workers and the control group did not demonstrate sénsitivity by skin testing.
Research Professor of Medicine. Tulane Medical Center
The hypothesis that coffee allergen was active in sensi-tive individuals was supported by the fact that specific IgE antibodies were detected in the serum of sympto-matic workers that were not present in the other groups.
A study of two coffee manufacturing plants was conducted. CoITee dust concentrations were measured in milligrams per cubic meter. N o significant difference in quantity was found among the three work areas— the green coffee bean area, the mixed area, and the roasted coffee bean area. However, a qualitative differ-ence was suspected. A study that tested mice with various extracts found that coffee dust and green coffee beans contained potent allergens. Castor bean and green coffee bean demonstrated no cross-reactivity in this animal model.
An epidemiologic survey was conducted for the prev-alence of pulmonary symptoms, atopic disease, x-ray and pulmonary function abnormalities, and skin tests. A standardized questionnaire, chest x-ravs. and skin tests were conducted in 372 workers. Skin testing de-lected 11 to 15% atopic individuals among the subjects. Lower respiratory symptoms, including wheezing and coughing, were reported in 32 to 37%. Upper respira-tory symptoms, such as hayfever or sinus problems, were reported in 42 to 43%. Chronic bronchitis was found in 3 to 7%. Occupational aslhma was not found in the two plants studied. Symptom prevalence did not differ significantly among various exposure areas. Only the castor bean radioallergosorbent test ( R A S T ) test was significant to the exposure area, with the highest positive reactions among workers in the green coffee bean exposure area.
Thus, castor bean appears to be the most potent
Allergy Proc. 65
a l le rgen, because t h e greatest n u m b e r o f coffee w o r k e r s h a d hypersens i t i v i t y responses to it. R A S T i n h i b i t i o n studies o f ext racts o f sack samples suppor t the h y p o t h -esis that cofTcc w o r k e r s arc exposed to castor b e a n a l lergen t h r o u g h h a n d l i n g c o n t a m i n a t e d sacks.
I n c o n c l u s i o n . L e h r e r no ted that the po ten t ia l for o c c u p a t i o n a l e x p o s u r e to al lergens in the co(Tcc indus-t ry is cons iderab ly l o w e r t h a n in o t h e r industr ies that arc less m e c h a n i z e d .
R E F E R E N C E S 1. ColVce—The Wor ld Cup. Prepared by thc promotion fund o f
the International Coffee Organization. Samuel E. Siravisky and Associates. Inc. Public Relations International. Washing-ton. DC.
2. Dcrnton IIS. Occupational sensitization—a hazard to thc cofVee industry. J A M A 223:1146-1147. 1973.
3. Karr RM. Lehrer SB. Butcher BT. Salvaggio JE. Coffee work-ers asthma: a clinical appraisal using the radioallcrgosorbent lest. J Allergy Cl in Immunol 62:143-148. 1978.
4. Jones RN. Hughes JM. Lehrer SB. et al. Lung function consequences o f exposure and hypersensitivity in workers
who process green coffee beans. A m Rev Respir Dis 125:199-202. 1982.
5. Zuskind E. Kanceljak B. Skuric Z. Buikovic D. Bronchial reactivity in green cotTee exposure. Br J Ind Met! 42:415-20. 1985.
6. Van Toom DW. CofTcc workers lung. A new example of extrinsic allergic alveolitis. Thorax 25:399-405. 1970.
7. Vandcrbosch JM. Van Toom DW. Wagcnaar SS. CotTee workers lung: reconsideration of a case report. Thorav38:720. 198.1.
8. Freed man.SO. S idd iq iQl . Krupcy J. Schon A H . identification of a simple chemical compound (chlorogenic acid) as an allergen in plant materials causing human atopic disease. Trans Assoc A m Physicians 75:99-106. 1962.
9. Layton LL. Green FC. Corse JW. Panzani R. Pure chlorogcnic acid not allergenic in atopy to green coffee: a specific protein probably is involved. Nature 203:188-189. 1964.
10. Layton LL. Green FC. Panzani R. Allergy to green coffee: failure of patients allergic to green cofTcc to react to chloro-genic acid, roasted colTec or orange. J Allergy Cl in Immunol 36:84-91. 1965.
11. Figlcy KD, Rawlings FFA. Castor bean: an industrial hazard as a contaminant of green colTce dusl and used burlap bags. J Allergy Cl in Immunol 21:545-553. 1950. •
6 6 M a r c h - A p r i l 1 9 9 0 , Vo l . 11 . No . 2
Hypersensitivity Reactions in Seafood Workers
Presented by Samuel B Lehrer, Ph.D.
"seafood is a major industry in the United Stales, employing a total of 350,000 workers as of 1986.
f n view of ihe known allergenicity of seafood in con-umers. the large number of allergic reactions reported
_mong seafood workers is not surprising. Allergenic agents include snowcrabs. shrimp, oysters, shell prod-
cts. rubber boots, and fishing nets. Allergic reactions ave been reported among fishermen, seafood proces-
sors. oyster shuckers, caterers, and restaurant chefs. Allergic reactions to seafood can be divided into two
ategories: respiratory (including asthma, pulmonary hypersensitivity, and respiratory allergy) and dermato-logical (including dermatitis, contact urticaria, skin dis-
ases. and eczema). Lehrer explained that this presen-it ion would focus on respiratory reactions, which oc-
cur more frequently in seafood workers and have been tudied more thoroughly.
A study of snowcrab processing workers examined uccupational exposure at two processing plants. Large amounts of steam and water vapor released by the
oi l ing process were seen, and ventilation was insuffi-ient. After cooking and cooling the crabs, workers
remove the meat from the legs and claws, thereby scorning exposed to steam, meat, and shell panicles, "here can be as many as 300 workers in one room.
The purpose o f the epidemiologic study was to deter-mine the prevalence of respiratory symptoms, atopic raits, and skin reactivity to snowcrab among the 303 .vorkers. According to the histories obtained, the work-ers were divided into three groups: 1) no symptoms of espiratory allergy: 2) symptoms of dyspnea and/or :ough and phlegm production, but no bronchospasms
Research Pro fessor of Medicine. Tulane Medical Center
and no relationship of symptoms to work; and 3) symptoms of aslhma. The latter group was then divided into subgroups, depending on whether their asthma was thought to be related to work exposure (e.g., symptoms occurred mostly at work). The diagnosis of occupa-tional asthma was confirmed in 15.6% o f the workforce studied. O f t h e occupational reactions reported, asthma was reported by 34%, rhinitis and/or conjunctivitis by 18%, and skin rash by 24%. A n association between allergic reactions, such as asthma, rhinitis, and skin rash, and positive skin test results was shown.
These results suggested an IgE sensitization to crab in these workers. In 1984, a group o f workers was restudied using different snowcrab extracts for skin tests and specific IgE antibody measurements. The results of this study suggested a highly significant relationship between the presence of immediate skin test reactivity, or increased serum IgE antibodies, and the occurrence of occupaiional asthma. Other studies using the West-ern blot or immunoprint method have revealed a num-ber of important allergens in snowcrab extracts.
Lehrer also discussed some of his crustacea studies. Although not in an occupational setting, the studies revealed a variety of antigens and allergens present in the extracts and showed that a number of allergens are still present after boiling. In addition, significant cross-reactivity was found.among shrimp, crawfish, crab, and lobster antigens. Following boiling, the fluid was found to contain equal or greater amounts o f antigen as the seafood meat.
In contrast to coffee industry workers, little is known about allergic reactions among seafood workers because of an insufficient number o f studies, Lehrer concluded. The seafood industry has been difficult to study for a number of reasons; for example, smaller plant sizes and seasonal operations make access for researchers more difficult.
Allergy Proc. 67
REFERENCES
I . O'lfciunitn OK. ed. Fisheries or thc United States. 1987. U.S. Department of Commerce. Ma> CD. Bock SA. A modern clinical approach to food h\perv.-n'.iti\ it;.. -Mlcuy 33:166-1X8. 1078. f ie t i ie J. I.ecue JS. Friend JA. Rcid T M . Pulmonary hyper-scnsiiivn\ i» prawn workers. Lancet 8208-9. 1350-1353. I9WI.
J. Carino M. fc'lia CJ. Mol in in i R. Nuzzaco A. Androsi L. Shrimp-meal asthma in thc aquaculture industry. Med Lav 7(\ :J-|_4 75. 1985.
5. I f i o i i h N. Rood-Peterson J. Occupational protein contact dermatitis in food handlers. Contact Derm 2:28-42. 1976. Meek I I I . Nisscn UK. Contact urticaria to commercial fish in atopic persons. Acta Derm Vencreol (Stockh) 63:257-260.
1983. 7. Cartier A. Malo JL. Forest F. et al. Occupational asthma in
snow crab processing workers. J Allergy C l in Immunol 74:261-269. 1984.
K. Cartier A. Malo JL. Ghezzo H. McCants M. Lehrer SB. IgE sensitization in snow crab processing workers. J Allergy Clin Immunol 78:344-348. 1986.
9. Bush RK. Meier-Davis S. Lehrer SB. Cartier A. Snow crab asthma: identification o f allergens by immunoblott ing. Sub-mitted for publication.
10. Lehrer SB. The complex nature of food allergens: studies of cross-reacting crustacca allergens. Ann Allergy 57:267-272. 1986.
11. Halmcpuro L. Salvaggio J. Lehrer SB. Studies o f allergens present in crawfish and lobsters. Int Arch Allergy Appl Im-munol (Basel) 84:165-172. 1987. •
68 March-April 1990, Vol. 11. No. 2
L'asthme professionnel: Rapport du comité spécial de la Société de thoracologie du Canada
par Jean-Luc Malo, m.d.
De plus en plus de travailleurs entrent en contact avec des substances qui causent de l'asthme professionnel. Cette situation a des répercussions sociales et économiques significatives. La Société de thoracologie du Canada (section médicale de l'Association pulmonaire du Canada) s'y est intéressée.
M M asthme professionnel est
9 w une cause de déficit fonc-
H H tionnel respiratoire de plus
en plus fréquente. On attribue
l'accroissement de son incidence et
de sa prévalence à une utilisation
plus répandue des agents étiologi-
ques, à l'augmentation du nombre
de ces agents et à de meilleures
méthodes diagnost iques. O n
estime aujourd'hui qu'il existe
environ 120 causes possibles
d'asthme professionnel.
La maladie est source de nou-
veaux problèmes pour les autorités
canadiennes de santé et de sécurité
responsables de la prévention des
maladies professionnelles et pour
les commissions de la santé et de
Dr MALO est professeur agrégé, faculté de médecine de l'Université de Montréal, et pneumologue. Hôpital du Sacré-Coeur. Montréal.
Ont également participé à la rédaction du Rapport les docteurs L.P. Boulet. I. Bro-der, A. Cartier, M. Chan-Yeung. D. Cock-croft. F.E. Hargreave, W.K.C. Morgan. S. Tarlo et P. Warren (président).
la sécurité du travail dont le man-
dat comprend la réduction des con-
séquences financières et sociales
des maladies professionnelles. Là
Société de thoracologie du Canada
(section médicale de l'Association
pulmonaire du Canada) a établi
des recommandations destinées
aux responsables qui allouent des
compensations aux travailleurs
atteints de maladies professionnel-
les (voir "Recommandations de la
Société de thoracologie du
Canada" p. 58). La Société a éga-
lement dressé une liste de problè-
mes reliés à l'asthme professionnel
que des études devront éclaircir
(voir "Besoins de recherche"
p. 63) .
Obstruction des voies aériennes en milieu de travail Les conditions respiratoires carac-
térisées par de l'obstruction bron-
chique peuvent être produites sur
les lieux du travail par l'exposition
à des poussières, des émanations
ou des gaz. L'obstruction des voies
aériennes peut être variable
(asthme) ou fixe (obstruction chro-
nique des voies aériennes).
La définition de l'asthme propo-
sée par le comité conjoint de l'Ame-
rican Thoracic Society et de
l'American College of Chest Physi-
cians est généralement acceptée:
"L'asthme est une condition carac-
térisée par une hyperexcitabilité
de la trachée et des bronches à des
stimuli variés et se manifestant
par un rétrécissement diffus des
voies aériennes qui varie en gra-
vité soit spontanément soit suite à
un traitement."
On a décrit quatre conditions
caractérisées par l'obstruction des
voies aériennes. Pour chacune de
ces conditions, la variabilité du
calibre bronchique est reconnue et
l'on retrouve une hyperexcitabilité
bronchique suite à l'exposition aux
poussières, aux émanations et aux
gaz dans le milieu de travail. Il
s'agit de:
• L'asthme professionnel dû à la
sensibilisation à des substances
spécifiques;
• La byssinose due à l'exposition
au coton et au lin, entre autres:
• Le Reactive Airways Dysfunc-
tion Syndrome (RADS) dû à l'expo-
sition intense à des substances
toxiques;
• L'obstruction bronchique varia-
ble due à l'exposition à des subs-
tances irritantes non spécifiques.
Ce rapport se limite à l'asthme
professionnel, une condition récem-
le clinicien mars 1988 57
L'asthme professionnel est une obstruction variable des voies aériennes causée par une substance sensibilisante rencontrée sur les lieux du travail.
Recommandations
Que le terme "asthme professionnel" soit réservé à une obstruction des voies aériennes variable accompagnee d hyperexcitabilité bronchique due à une sensibilisation à une substance rencontrée spécifiquement au travail.
Q U , e ' e S ^ e ! P O n S a b ' e S 5 e ' a 8 3 0 1 6 e t d e 13 ^ ^ P^essionnelles identifient à travers le pays les médecins considérés c o m m e des experts dans le diagnostic et l'évaluation de l'asthme professionnel o Z c e n S Z régionaux d'expertise pourraient être établis. e**w»nei . ues centres
^ i ^ r 5 3 ^ d G 1 3 ^ ®î' i ,a a u t r a v a i l au Canada identifient les industries qui exposent des travailleurs à des causes connues d'asthme professionnel et les informent des risques de la matedie.
Que les commissions de santé et de sécurité du travail au Canada acceptent la nature" de I 'as thmW ' :
pro essionne et développent des échelles .'d'invalidité qui sont vraiment applicables >à l'asthme '» - , prof^sionnel tel que recommandé dans ce rapport. Ces commissions devraient obtenir l'expertisé de. ' ! membres ou de consultants aptes à diagnostiquer et à traiter l'asthme professionnel.' . '. ,
Q U 2 ^ t r T i , , e U r S C rJf ! f q u e l S o n « W * » te présence d'asthme professionnel soient référés à des experts régionaux Un diagnostic objectif d'asthme doit êjre établi et le lien de l 'asthmeavec l'exposition à
^ t J f T T S U r , 6 S " e U X d r t r a v a i ' d 0 i t ê t r e c o n n r m é a v a n t 'e travailleur ne soit avisé de quitter ^ ^ f t r l m 6 3 ^ ^ ° ° n f i m i e r 16 I i e n r e xPûsil ion à l'agent responsable sur les lieux du trava.1 et l asthme les c o m m u o n s de santé et de sécurité du travail devraient permettre aux travailleurs d e recevoir des prestations pour les périodes d'absence au travail. (Ces périodes sont nécessaires pour déterminer s» l amélioration des symptômes de l'asthme est suivie d'une récidive au retour autravail .)
Que le diagnostic d'asthme professionnel d é p ë r t e de la corrélation des changements de I n s t r u c t i o n bronchique et de I hyperexcitabilité bronchique avec une exposition variable à la cause Lés tests'de provocation en laboratoire pour prouver les causes d'asthme professionnel ne font plus partie de I investigation habituelle. -
Que l'évaluation du déficit fonctionnel et de l'invalidité pour les travailleurs atteints d'asthme professionnel inclue une mesure de l'hyperexcitabilité bronchique. Les échelles d'invalidité doivent tenir compte d e la onction pulmonaire de base, de ('hyperexcitabilité bronchique et du besoin en médicaments du travailleur
La médication est évaluée par la quantité minimale nécessaire pour soulager les symptômes de façon régulière sur une période d'un mois. Les échelles de base sont fondées sur la gravité d e l'obstruction bronchique avant bronchodilatateur (le VEMS). Ces mesures sont modifiées par le deqré de l hyperexcitabilité bronchique et le besoin en médication.
Le déficit fonctionnel et l'invalidité doivent être évalués tous les deux ans avant que l'on décide de leur permanence.
Une procédure devrait être instaurée pour diagnostiquer et évaluer le travailleur atteint d'asthme professionnel
T d e S 5 ^ s , 0 n s d ? c o m P e n s a t i o n puissent être prises rapidement et que le travailleur puisse ' réintégrer le marché du travail aussi tôt que possible. . H
le clinicien mars 1988 58
•
ment reconnue par la communauté
scientifique médicale et qui pose de
nouveaux problèmes pour les ser-
vices professionnels de santé et les
comités de compensation finan-
cière.
La byssinose est une condition
bien établie. Les médecins oeu-
vrant dans le domaine des mala-
dies professionnelles et les comités
de compensation traitent souvent
cette affection. Des mesures pré-
ventives ont été instituées dans les
industries du coton et du lin.
Le RADS a été rapporté seule-
ment par un auteur. L'obstruction
aiguë post-inflammatoire des voies
aériennes après une exposition à
des concentrations toxiques de pro-
duits chimiques comme le chlore,
le fluor, les acides forts, l'oxyde sul-
fureux, l'oxyde nitreux, l'ammo-
niaque et des solvants était connue
antérieurement. Cependant, la
reconnaissance d'une hyperexcita-
bilité bronchique chez ces sujets est
plus récente. La fréquence de cet
état, son histoire naturelle et le
degré de déficit fonctionnel qu'elle
engendre n'ont pas été établis.
L'obstruction variable des voies
aériennes due à une exposition à
des irritants est répertoriée dans les
mises à jour sur l'asthme mais sa
nature n'a pas été établie. Les cau-
ses incluses dans ces listes sont le
SCX2), l'ozone, entre autres agents.
Ces agents ne sont ni sensibilisants
ni allergéniques. Ils agissent par
voie d'une bronchoconstriction
réflexe et le relâchement direct de
médiateurs. Cette condition est
probablement associée à une expo-
sition chronique au produit irri-
tant au-delà de ce que l'on désigne
comme le Threshold Limit Value
(TLV). Le rôle d'une hyperexcita-
bil ité bronchique préexistante
dans la réponse aux irritants n'est
pas clair, mais elle pourrait y con-
tribuer directement. L'interaction
avec le tabagisme et des conditions
pulmonaires pré-existantes ainsi
que l'histoire naturelle de l'obs-
truction bronchique due à des irri-
tants n'ont pas été établies.
La compensation pour byssinose
est acceptée. Le RADS et l'obstruc-
tion spécifique variable due à des ir-
ritants sur les lieux du travail res-
tent trop vagues pour faire l'objet
de recommandations spécifiques.
La nécessité d'une compensation
doit être décidée après l'analyse
individuelle des cas. L'aggravation
de l'asthme par des causes non sen-
sibilisantes devrait être compensée
seulement si des niveaux excessifs
de l'agent causal sont présents.
Définition L'asthme professionnel est une
obstruction variable des voies aé-
riennes causée par une substance
présente sur les lieux du travail.
La substance causale a sensibilisé
la personne au travail. Bien que la
substance sensibilisante puisse ne
pas être spécifiquement identifiée,
ses effets peuvent être démontrés.
Pour des substances de grand poids
moléculaire, la sensibilisation a
habituellement une base immuno-
logique, médiée par les immuno-
globu l ins E (IgE), mais la base de
la sensibilisation aux substances
de faible poids molécu la i re
demeure incertaine.
Cause s Un grand nombre de substances
pouvant causer l'asthme ont été
identifiées. Certaines l'ont été grâce
à des données épidémiologiques et
à des tests de provocation bronchi-
que, d'autres grâce à des rapports
de cas cliniques. Une liste de réfé-
rences pour ces agents est disponi-
ble sur demande. Le tableau 1
présente une liste des causes
d'asthme professionnel.
Les seules causes qui devraient
être considérées comme confirmées
sont celles dont on a prouvé l'effet
sur Thyperexcitabilité bronchique
et l'obstruction des voies aérien-
nes. Les autres substances
devraient être considérées comme
des causes possibles d'asthme pro-
fessionnel.
Quand une substance répertoriée
est soupçonnée dans un cas
d'asthme professionnel, les docu-
ments pertinents devraient être
étudiés afin de déterminer s'il
s'agit d'une cause reconnue. La
liste des agents déclencheurs
le clinicien mars 1988 59
Des symptômes qui s'aggravent en soirée et durant les jours de travail, mais diminuent au cours de la
fin de semaine ou en période de vacances suggèrent que l'asthme est relié au travail.
Besoins de recherche
Établissement ou rejet des causes possibles d'asthme professionnel Détermination de la prévalence et de l'incidence de l'asthme professionnel chez des travailleurs exposés à des
.causes connues. •"v Détermination que différents types d'exposition et que l'exécution de tâches différentes produisent de l'asthme au
^ même degré. Examen de la relation entre les changements d'hyperexcitabilité bronchique à des agents spécifiques et non ^spécifiques tels que lès poussières inertes, les émanations et l'air froid.
• Meilleure définition du "Reactive Airways Disease Syndrome" et de l'obstruction bronchique secondaire à • ; ; J l'exposition chronique à des irritants. " Évaluation des conséquences du diagnostic précoce de l'asthme professionnel et du retrait précoce d'un travailleur
à l'exposition à l'agent responsable de son affection
Établissement et évaluation prospective d'échelles d'invalidité chez les travailleurs. Identification des facteurs de risque personnels qui contribuent au développement de l'asthme professionnel. Élucidation des mécanismes de sensibilisation, particulièrement aux agents de faible poids moléculaire. Établissement de méthodes de contrôle de l'environnement qui préviendraient l'asthme professionnel. Évaluation du dépistage médical avant l'embauche et du dépistage périodique qui pourraient contribuer au contrôle
de l'asthme professionnel et au développement de méthodes de prévention.
devrait être utilisée par des méde-
cins connaissant le problème, des
comités de santé et de sécurité et
d'autres intervenants intéressés à l'évaluation de l'asthme en tant
que maladie professionnelle. Cette
liste ne doit pas être utilisée pour
établir un diagnostic d'asthme pro-
fessionnel chez un travailleur qui
développe un trouble respiratoire
et est exposé à une substance qui
se trouve sur la liste. Le médecin
doit confirmer le diagnostic sur
une base individuelle et selon les
étapes recommandées. Il ne doit
pas présumer que le sujet présente
de l'asthme professionnel par expo-
sition à un agent causal présent
sur la liste.
Diagnostic Le diagnostic de l'asthrrie profes-
sionnel doit être établi aussi rigou-
reusement que celui des pneumoco-
nioses traditionnelles. Cependant,
les procédures diagnostiques sont
différentes de celles des pneumoco-
nioses. Chez ces dernières, les cau-
ses environnementales sont con-
nues et peuvent être surveillées
dans le milieu de travail, des chan-
gements radiologiques se produi-
sent, le lavage bronchoalvéolaire
et les biopsies pulmonaires sont
disponibles et les changements de
la fonction pulmonaire sont cons-
tants ou progressent lentement.
Dans l'asthme professionnel, les
causes sont multiples, l'environne-
ment de travail est moins bien
défini, il n'existe pas de change-
ments radiologiques et la fonction
pulmonaire est variable.
Les autorités provinciales res-
ponsables de la santé et de la sécu-
le clinicien mars 1988 6 3
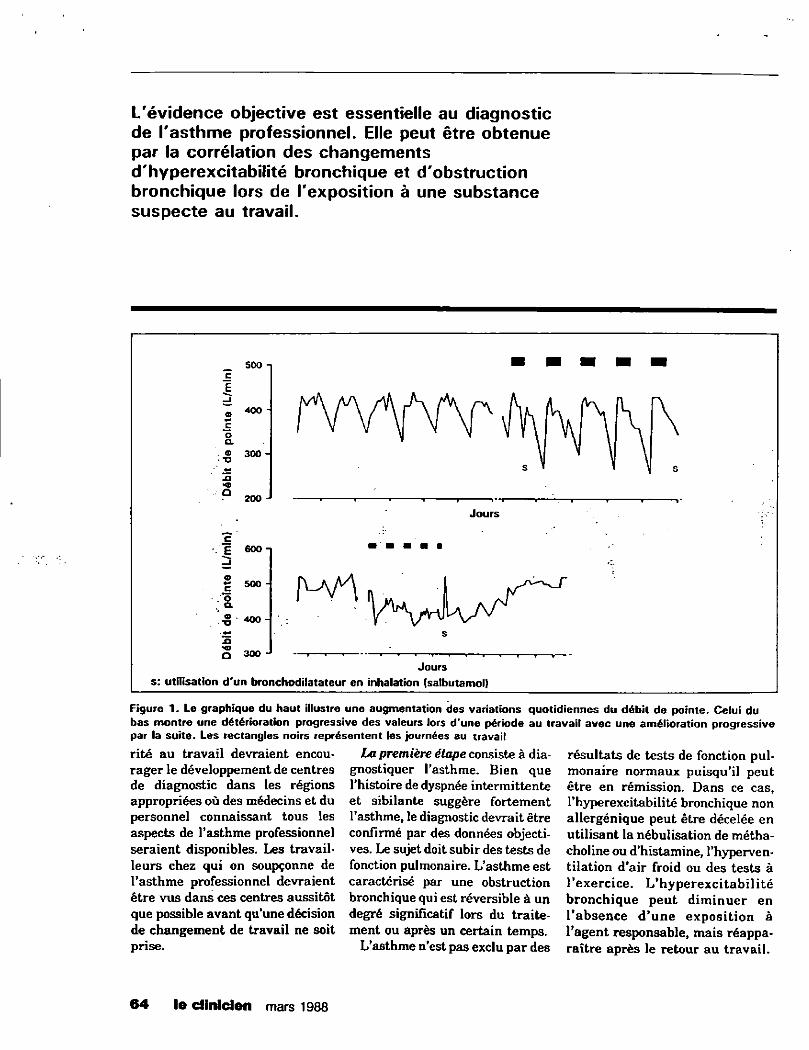
L'évidence objective est essentielle au diagnostic de l'asthme professionnel. Elle peut être obtenue par la corrélation des changements d'hyperexcitabilité bronchique et d'obstruction bronchique lors de l'exposition à une substance suspecte au travail.
_ soo -c E
O 400 - V V Y V \ r \ f u s K r \ \ \ S / V v m v V n Vv \ s \ o a.
y \ \ \ \ ® 300 - \ > \ \
s " » y s i) HD •
p 200 -p 200 - " • • •• . i .i »• i 1 1
r Jours
"c . £ 600-J o c 5 0 0 " . o a -§ 400- Y \fr\yAyv
J3 s
S 300 -J Jours
s: utilisation d'un bronchodilatateur en inhalation (salbutamol)
Figure 1. Le graphique du haut illustre une augmentation des variations quotidiennes du débit de pointe. Celui du bas montre une détérioration progressive des valeurs lors d'une période au travail avec une amélioration progressive par la suite. Les rectangles noirs représentent les journées au travail
rité au travail devraient encou-
rager le développement de centres
de diagnostic dans les régions
appropriées où des médecins et du
personnel connaissant tous les
aspects de l'asthme professionnel
seraient disponibles. Les travail-
leurs chez qui on soupçonne de
l'asthme professionnel devraient
être vus dans ces centres aussitôt
que possible avant qu'une décision
de changement de travail ne soit
prise.
La première étape consiste à dia-
gnostiquer l'asthme. Bien que
l'histoire de dyspnée intermittente
et sibilante suggère fortement
l'asthme, le diagnostic devrait être
confirmé par des données objecti-
ves. Le sujet doit subir des tests de
fonction pulmonaire. L'asthme est
caractérisé par une obstruction
bronchique qui est réversible à un
degré significatif lors du traite-
ment ou après un certain temps.
L'asthme n'est pas exclu par des
résultats de tests de fonction pul-
monaire normaux puisqu'il peut
être en rémission. Dans ce cas,
l'hyperexcitabilité bronchique non
allergénique peut être décelée en
utilisant la nébulisation de métha-
choline ou d'histamine, l'hyperven-
tilation d'air froid ou des tests à
l'exercice. L'hyperexcitabilité
bronchique peut diminuer en
l'absence d'une exposition à l'agent responsable, mais réappa-
raître après le retour au travail.
6 4 le dinlden mars 1988
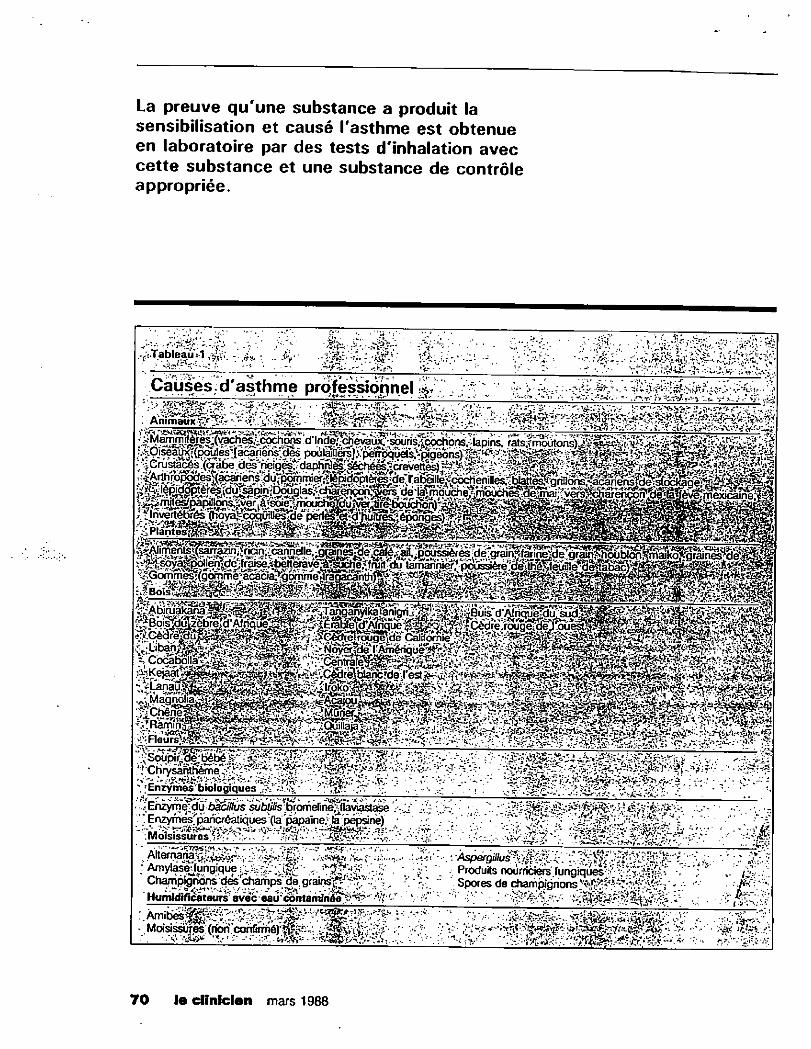
La preuve qu'une substance a produit la sensibilisation et causé l'asthme est obtenue en laboratoire par des tests d'inhalation avec cette substance et une substance de contrôle appropriée.
; A m y l ^ e j u n g i q ù e ' • " v ' - • Produits nourriciers i u r ^ k ^ ^ ^ ^ -Champignons des champs de.grair»?tJ ^rr / . - -v • ' Spores de chamoianons • -Humidificateurs' aveceaûcontamfriée
\£ î " • Spores de champignons • • -f&î
sissuresïffon.confirméy^?^;: ^^.VH' i j 'V^' - F- i ^ s t â t â t * ^ . ^ - - . •>• JÇ&V/' Moisissures
70 le diniclen mars 1988
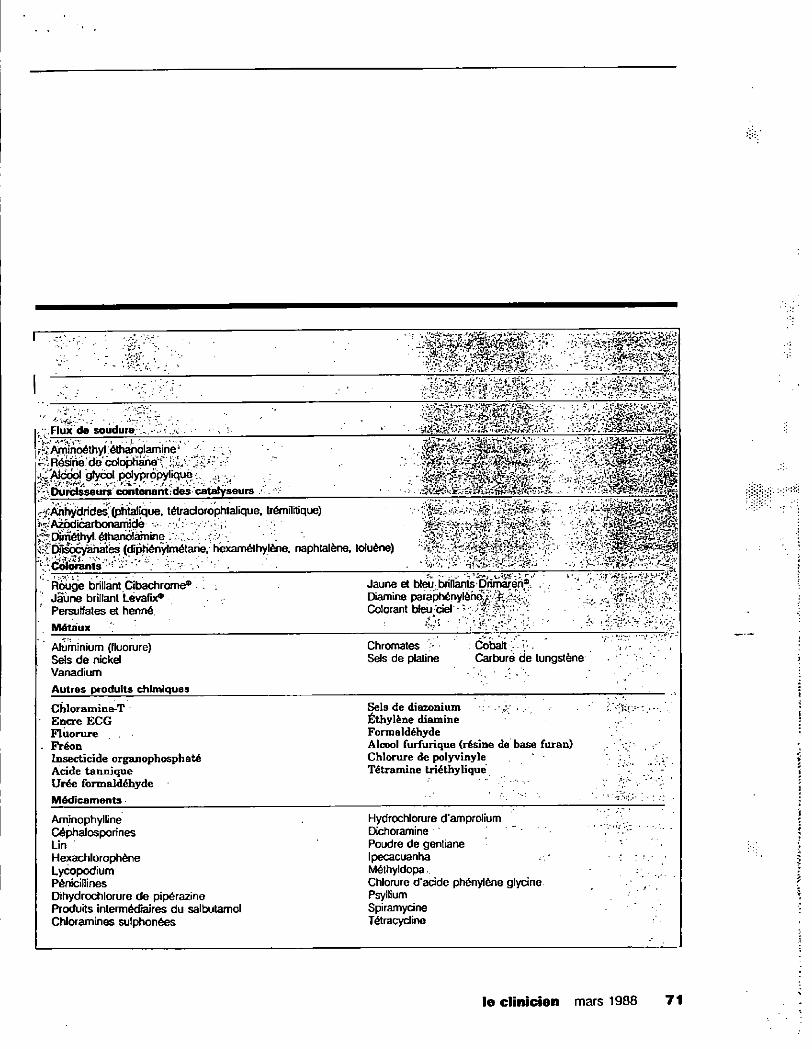
• - ; -
. , - - - 5»i.* •„ • • ^
. v ^ /
* * r '
, Flux de soudure ... w ..<•;/.. é&s i
^/ynin^thylétha^olarnine1 - ;
Résiné de c o l o p l ^ ^ f ;
^Alppol "gfyœlpdypropylique , .. . ; " \Dur t5^urs conti0nant des catalyseurs /-'.
j ^ f ?
f^:/&hydrides,' (phtalique, tétraclorophtalique. trémilitique) * * > '^AaKlicarbonamide- v-. ":/•''•:;»• • ks v ^ p;Diméthyl. éthariolàmine i;---r..- • { ' V'. - <• r ^ ^ ^ DHsocyahates (rîpHénylmétane. hexaméthylène. naphlalène, toluène) * * * ^Colorants • • - -F
f" • r ; ' . • . . • • ' • ' •
. Rouge brillant Cibachrome* • ! \ Jaune brillant Lévafix®
Persulfates et henné
Jaune et bleu brillants Dnmaren® . Diamine paraphénylène^ u Colorant bleu ciel • •<• m*r. -
. • v . • • • ï,-
f o
Métaux ?
Aluminium (fluorure) Sels de nickel Vanadium
Chromâtes ; Cobalt Sels de platine Carburé de tungstène
. ; •' • • i
Autres produits chimiques
Chloramine-T " Encre ECG Fluorure
. Fréon Insecticide organophosphaté Acide tannique Urée formaldéhyde
Sels de diazonium • Éthylène diamine Formaldéhyde Alcool furfurique (résine de base furan) Chlorure de polyvinyle Tétramine triéthylique
ïy^iy-.--.
Médicaments • . : ::
Aminophylline Céphalospo rines Lin Hexachlorophène Lycopodium Pénicillines Dihydrochlorure de pipérazine Produits intermédiaires du salbutamol Chloramines sulphonées
Hydrochlorure d'amprolium Dichoramine Poudre de gentiane Ipecacuanha Méthyldopa , Chlorure d'acide phénylène glycine Psyllium Spiramycine Tétracycline
le clinicien mars 1988 7 1
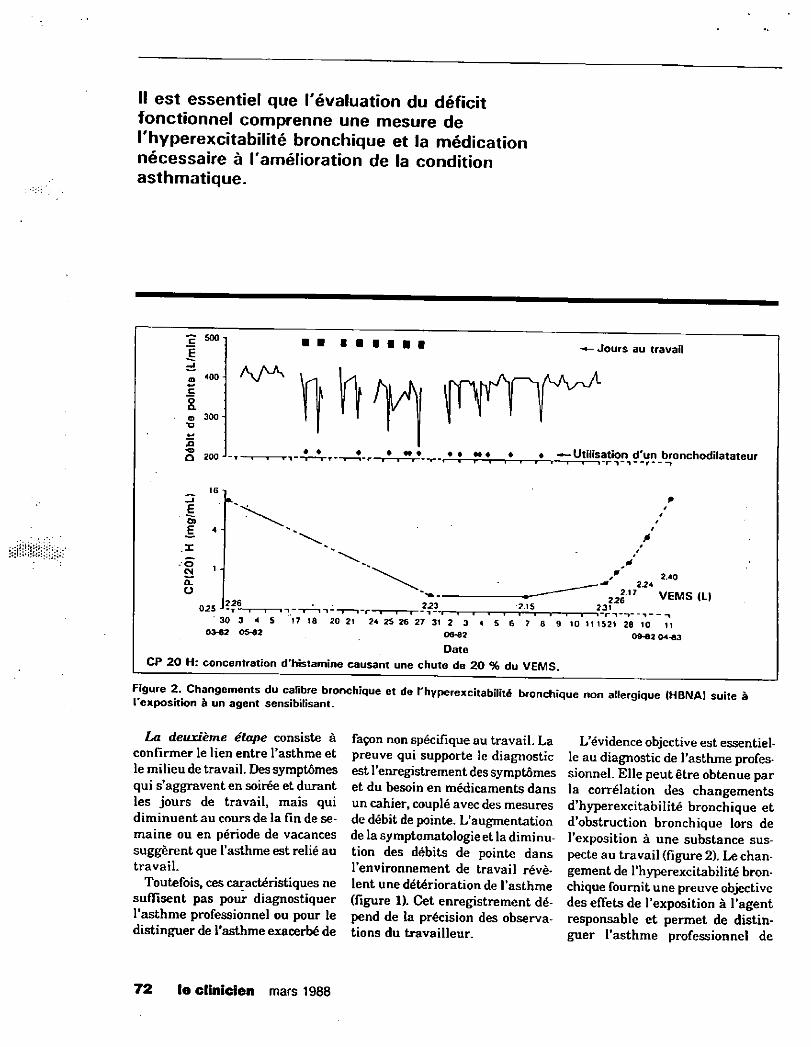
Il est essentiel que l'évaluation du déficit fonctionnel comprenne une mesure de l'hyperexcitabilité bronchique et la médication nécessaire à l'amélioration de la condition asthmatique.
500
o <00-
o a. o 300 "O
O 200 J
Jours au travail
• • • • —Utilisation d'un bronchodilatateur « i i i i ? i i i | i - | - 1 - 1 — r »
O) £ <
025 226 T " 1 I I ' 223 T—"I I 1-1 — 2.15 i »•
. 2.40 ' 224 2 2 l A 1 VEMS (L)
2.31 « "i 1 1 i~r i - 1 — 30 3 4 5 17 18 20 21 24 25 26 27 31 2 3 4 5 6 7 8 9 10 11 1521 28 10 11
<*"« 06-62 09-62 04-63 Date
CP 20 H: concentration d'histamine causant une chute de 20 % du VEMS.
Figure 2. Changements du calibre bronchique et de l'hyperexcitabilité bronchique non allergique (HBNA) suite à I exposition à un agent sensibilisant.
La deuxième étape consiste à
confirmer le lien entre l'asthme et
le milieu de travail. Des symptômes
qui s'aggravent en soirée et durant
les jours de travail, mais qui
diminuent au cours de la fin de se-
maine ou en période de vacances
suggèrent que l'asthme est relié au
travail.
Toutefois, ces caractéristiques ne
suffisent pas pour diagnostiquer
l'asthme professionnel ou pour le
distinguer de l'asthme exacerbé de
façon non spécifique au travail. La
preuve qui supporte le diagnostic
est l'enregistrement des symptômes
et du besoin en médicaments dans
un cahier, couplé avec des mesures
de débit de pointe. L'augmentation
de la symptomatologieet la diminu-
tion des débits de pointe dans
l'environnement de travail révè-
lent une détérioration de l'asthme
(figure 1). Cet enregistrement dé-
pend de la précision des observa-
tions du travailleur.
L'évidence objective est essentiel-
le au diagnostic de l'asthme profes-
sionnel. Elle peut être obtenue par
la corrélation des changements
d'hyperexcitabilité bronchique et
d'obstruction bronchique lors de
l'exposition à une substance sus-
pecte au travail (figure 2). Le chan-
gement de l'hyperexcitabilité bron-
chique fournit une preuve objective
des effets de l'exposition à l'agent
responsable et permet de distin-
guer l'asthme professionnel de
76 le clinicien mars 1988 72
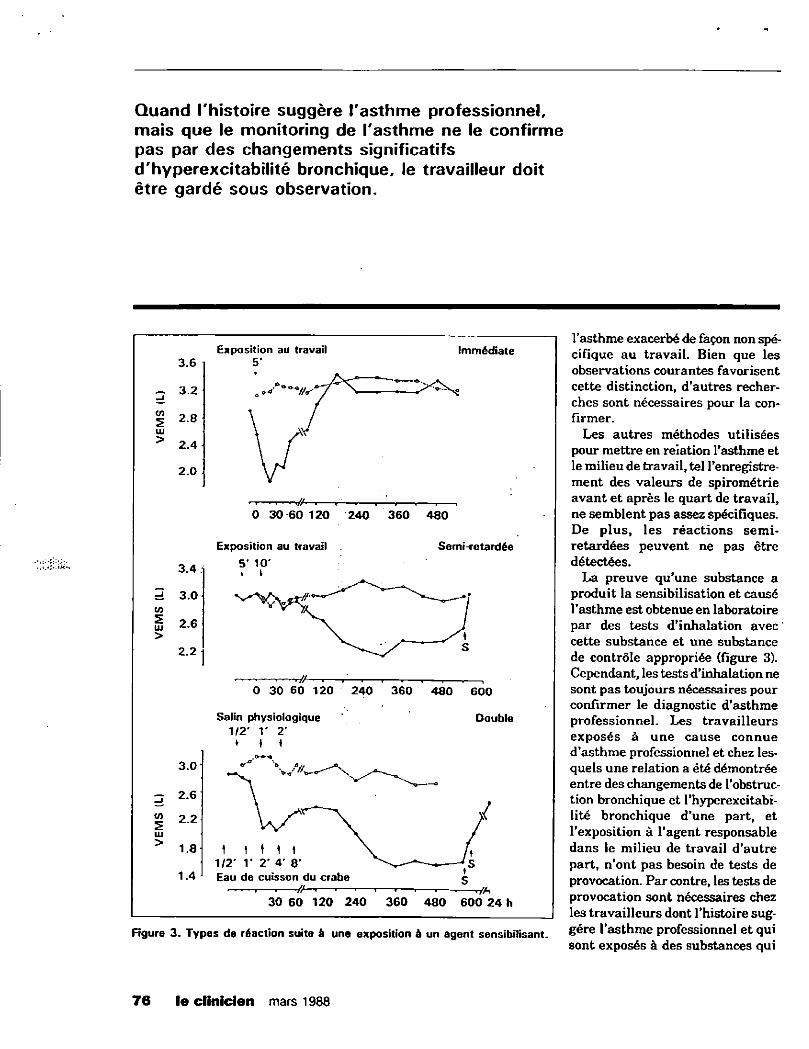
Quand l'histoire suggère l'asthme professionnel, mais que le monitoring de l'asthme ne le confirme pas par des changements significatifs d'hyperexcitabilité bronchique, le travailleur doit être gardé sous observation.
l'asthme exacerbé de façon non spé-
cifique au travail. Bien que les
observations courantes favorisent
cette distinction, d'autres recher-
ches sont nécessaires pour la con-
firmer.
Les autres méthodes utilisées
pour mettre en relation l'asthme et
le milieu de travail, tel l'enregistre-
m e n t des valeurs de spirométrie
avant et après le quart de travail,
ne semblent pas assez spécifiques.
D e plus, les réactions semi-
retardées peuvent ne pas être
détectées.
La preuve qu'une substance a
produit la sensibilisation et causé
l'asthme est obtenue en laboratoire
par des tests d'inhalation avec
cette substance et une substance
de contrôle appropriée (figure 3).
Cependant, les tests d'inhalation ne
sont pas toujours nécessaires pour
confirmer le diagnostic d'asthme
professionnel. Les travailleurs
exposés à u n e cause connue
d'asthme professionnel et chez les-
quels une relation a été démontrée
entre des changements de l'obstruc-
tion bronchique et l'hyperexcitabi-
lité bronchique d'une part, et
l'exposition à l'agent responsable
dans le milieu de travail d'autre
part, n'ont pas besoin de tests de
provocation. Par contre, les tests de
provocation sont nécessaires chez
les travailleurs dont l'histoire sug-
Figure 3 . T y p e s de réaction suite à une exposition à un agent sensibilisant. S é r e l ' a s t h m e p r o f e s s i o n n e l e t qu i sont exposés à des substances qui
Exposition au travail Immédiate 3.6
3.2
2.8
2.4
2.0
3.4
3.0
2.6
2.2
3.0
2.6
2.2
1.8
1.4
VA 0 30 60 120 240 360 480
Exposition au travail 5* 10* « r
Semi-retardée
0 30 60 120 240 360 480 600
Double Salin physiologique 1/2' 1' 2' • • \
\ I • \ \ 1/2' r 2' 4' 8* Eau de cuisson du crabe
30 60 120 240 360 480 600 24 b
7 6 le cl inicien mars 1988 76
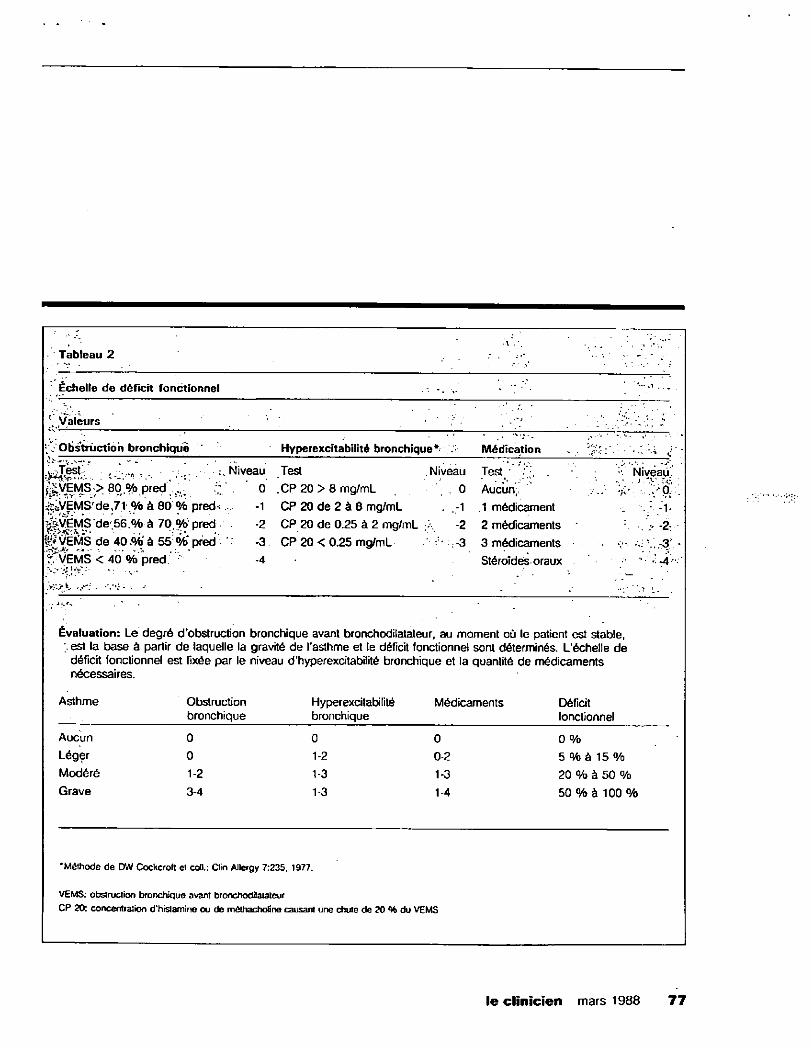
Tableau 2 - . - .
" Échelle de déficit fonctionnel v
V Valeurs ' ' ' - l7 ' ' ;''. v-.:;
Obstruction bronchique ' Hyperexcitabilité bronchique* . Médication . ' : • ' i C
. : •. - . v .Niveau Test Niveau Test / .? ; . . Mi veau. ^ V E M S ; > 80, % pred r 0 CP 20 > 8 mg/mL 0 Aucun,, > a V . f<VEMS f de , 7 1 % à 80 % p r e d * . -1 CP 20 de 2 à 8 mg/mL -1 . 1 médicament -1. 0-VËMS de.56.% à 70.%' pred • . -2 CP 20 de 0.25 à 2 mg/mL -2 2 médicaments v - 2
g£VÉWs de 4 0 à 55: %* pred * -3 CP 20 < 0.25 mg/mL -3 3 médicaments v-ÎVVEMS < 40 % pred ' -4
2 «y.-- v . - v • -.''i - . •• •
StéroTdés oraux
Évaluation: Le degré d'obstruction bronchique avant bronchodilatateur, au moment où le patient est stable, ;. est la base à partir de laquelle la gravité de l'asthme et le déficit fonctionnel sont déterminés. L'échelle de
déficit fonctionnel est fixée par le niveau d'hyperexcitabilité bronchique et la quantité de médicaments nécessaires.
Asthme Obstruction bronchique
Hyperexcitabilité Médicaments Déficit bronchique fonctionnel
Aucun 0 0 0 0 % •
Léger 0 1-2 0-2 5 % à 1 5 % Modéré 1-2 1-3 1-3 20 % à 50 % Grave 3-4 1-3 1-4 50 % à 100 'o
•Méthode de DW Cockcroft et coll.: Clin Allergy 7:235, 1977.
VEMS: obstruction bronchique avant bronchodilatateur CP 20: concentration d'hrstamine ou de méthachotine causant une chute de 20 % du VEMS
76 le clinicien mars 1988 7 7
Après avoir confirmé objectivement l'asthme professionnel, la première étape consiste à
retirer le patient du milieu de travail.
ne sont pas encore reconnues comme causes d'asthme profession-nel, ou lorsque le monitoring de l'hyperexcitabilité bronchique est équivoque. Les tests de provocation doivent
être effectués en laboratoire par des médecins et un personnel expéri-mentés. Ces laboratoires doivent être accrédités par les autorités pro-vinciales responsables de la prati-que médicale dans la communauté. Quand l'histoire suggère l'asthme
professionnel, mais que le monito-ring de l'asthme ne le confirme pas par des changements significatifs d'hyperexcitabilité bronchique, le travailleur doit être gardé sous observation. Si le diagnostic est confirmé lors des mois qui suivent, le travailleur pourra recevoir les conseils pertinents.
T e s t s démontrant la sensibi l i sat ion Les tests cutanés et les tests in vitro de mesure d'anticorps de type IgE aux nombreuses causes d'asthme professionnel sont rarement dispo-nibles. Plusieurs de ces tests n'ont été effectués que lors de recherche. Les travailleurs atteints d'asthme professionnel confirmé n'ont pas toujours une sensibilisation dé-montrable par des tests cutanés ou in vitro. Bien qu'un résultat de test positif témoigne de la sensibilisa-tion à une substance, il est possi-ble que le travailleur ne souffre pas
d'asthme si on l'expose à cette substance sur les lieux de travail. La nécessité pour les travailleurs sensibilisés et sans asthme d'évi-ter l'exposition éventuelle à l'agent responsable reste incer-taine, mais ces personnes doivent être gardées sous surveillance.
Démarche Après avoir confirmé objectivement l'asthme professionnel, la première étape consiste à retirer le patient du milieu de travail. Sans cela, l'asthme persistera, pourra au-gmenter et devenir permanent. Une fois que le travailleur est sensi-bilisé et atteint d'asthme, il est extrêmement improbable que des mesures préventives (telles la ven-tilation du milieu de travail ou l'utilisation de masques) prévien-dront des attaques ultérieures. Ainsi, des expositions inférieures à 0,001 partie par million peuvent être suffisantes pour provoquer de l'asthme chez certains employés sensibilisés aux isocyanates. Les employés sensibilisés qui ne chan-gent pas de travail devraient être gardés sous surveillance médicale.
Que la cause soit professionnelle ou non, la médication anti-asthma-tique est la m ê m e . Les symptômes requièrent un traitement avec des médications sympathomimétiques et de la théophylline tel qu'indi-qué. L'inflammation bronchique peut nécessiter un traitement aux
stéroïdes systémiques ou inhalés. Les autres médicaments peuvent être utilisés selon les indications. Le soulagement symptomatique peut masquer les effets de la sensi-bilisation et inciter le travailleur à continuer à travailler alors qu'il est encore atteint. Les travailleurs avec une hyperexcitabilité bronchique résiduelle devraient être informés des conséquences possibles de l'ex-position aux substances irritantes.
Évaluation du déficit fonctionnel et de l ' invalidité Le déficit fonctionnel dans les maladies pulmonaires est évalué par le degré d'anomalie de la fonc-tion pulmonaire qui est établi en fonction des anomalies de la méca-nique pulmonaire et de la réponse respiratoire à l'exercice. Puisque la nature m ê m e de l'asthme comprend des inconstances, le degré de déficit fonctionnel changera dans le temps selon l'exposition à la cause ou le traitement. Dans l'asthme profes-sionnel, la présence d'hyperexcita-bilité bronchique est très utile pour évaluer le déficit fonctionnel (vu 2a nature variable de la maladie). L'hyperexcitabilité bronchique n'a pas été utilisée pour l'évaluation du déficit fonctionnel dans les maladies pulmonaires profession-nelles. Cependant, son importance dans l'asthme professionnel devrait en faire un critère d'éva-luation de cette maladie.
76 le clinicien mars 1988 7 9
BREFS RENSEIGNEMENTS THÉRAPEUTIQUES
Lopïd I ^ B igmttml)
Capsules à 300 mg
Agent antihyperfipidémjque
MODE D'ACTION Le L0P1D abaisse les concentrations élevées de fipides dans le sérum en diminuant les triglycérides sériques avec réduc-tion variable du cholestérol sérique total. L'ette! inhibiteur se marque sur les tractions de Spoprotéines à (aible densité (LOI) et très faible (VLDL). Oe pfus. le LÛPID peut augmenter la frac-tion de cholestérol des lipoprotéines à forte densité (HDL). U mécanisme par lequel agit le L0PID n'est pas encore définitivement établi. Chez l'homme, il a été démontré que le LOPID provoquait l'inhibition de ta fipotyse périphérique et ta diminution de l'extraction hépatique des acides gras libres, réduisant ainsi la production de triglycérides hépatiques. Le LOPID inhibe également la synthèse des apoprotéines qui transportent les lipoprotéinesàtrèsfaibledensité(VLDL)résul-tant en une diminution des lipoprotéines à très faible densité (VLOL).
INDICATIONS Le LOPID est indiqué comme adjuvant au régime alimentaire et aux autres mesures thérapeutiques dans le traitement des patients affectés dTiypertipidémie de Type IV. et pour qui le risque de séquelles et de complications est très élevé. Le traitement initial de Itiyperlipidémie devrait inclure un ré-gime spécifique, une réduction de poids et un programme d'exercices et. pour les patients diabétiques, un bon équilibre du diabète.
CONTRE-INDICATfONS 1. Dérèglement hépatique ou rénal, incluant la cirriiose triliaire
primaire. 2. Maladie de la vésicule biliaire (voir mises en garde). 3 . Hypersensibilité au gemfibrozil. 4. Ne pas administrer aux femmes enceintes ou aux mères
qui aflaitent.
MISES EN GARDE 1. Anticoagulants concomitants. Faire preuve de prudence en
administrant des anticoagulants en même temps que le LOPIQ. Réduire la dose d'anticoagulant afin de maintenir le temps de prothrombine au niveau désiré afin d'éviter les complications hémorragiques.
2. Des études à long terme sur le gemfibrozil ont été réalisées sur les rats et les souris avec des doses une à dix (ois su-périeures à celles administrées à l'homme. La fréquence de nodules bénins et de cancers du foie a augmenté de manière significative chez les rats mâles soumis à de fortes doses. La fréquence de cancers du (oie a également augmenté chez les rats mâles soumis à de faibles doses, mais cette augmentation n'était pas statistiquement sig-nificative ( P > 0,05). Aucune différence statistiquement significative n'a été observée chez les sujets témoins en ce qui concerne ta fréquencede tumeurs du foie des ratesou des souris mâles et femelles. Le nombre de tumeurs hépa-tiques et test'rculaires a augmenté chez les rats mâles.
3. Calculs biliaires. Le LOPID peut augmenter l'excrétion de cholestérol dans la bile, résultant en la formation de calculs bifiaires. Si descalculs biliaires sont soupçonnés, un exa-men de la vésicule biliaire est recommandé. Interrompre le traitement au LOPIO en présence de calculs biliaires.
4. Puisque les effets du médicament sur la réduction de la mortalité due aux maladies coronaires n'ont pas été démontrés, n'administrer le LOPID qu'aux patients décrits dans la section "indications". Si une réduction significative des lipides dans le sérum n'est pas obtenue dans les 3 pre-miers mois, arrêter le traitement au LOPID.
5. Sa sécurité et son efficacité n'ont pas encore été établisdans le cas des entants.
6. Les femmes fertiles ont à prendre des mesures anticoncep-tionnelles strictes. Si une grossesse survenait malgré ces précautions, arrêter le traitement au LOPID.
7. Les femmes qui envisagent d'avoir un enlani devraient in-terrompre l'usage du LOPID plusieurs mois avant la con-ception.
PRÉCAUTIONS 1. Traitement Initial. Avant d'établir le traitement au LOPID.
essayer de maîtriser les lipides sériques par des mesures diététiques appropriées, des exercices, une perte de poids chez les patients obèses et le contrôle de réquiftre du dia-bète sucré.
2. traitement} long terme. Comme l'administration i long terme du LOPtO est recommandée, effectuer des études chimiques avant de commencer le traitement, afin de s'as-surer que le patient est effectivement atteirë (Tun taux élevé de lipides sériques ou d'un niveau bas de cholestérol de Gpoprotéines à (one densité (HDL). Déterminer le niveau des Gp'rdes sériques à intervalles réguliers au cours du traitement au LOPID.
3. Affaiblissement de la fertilité. L'administration pendant 10 semaines à des rats mâles de doses de trois i dix fois su-périeures aux doses normales pour l'homme, a résulté en une diminution de la fertilité Des études ultérieures ont montré que ces effets s'inversaient après une période de 8 semaines de suspension du traitement et n'étaient pas transmis à leur progéniture.
4. Modifications de l'hémoglobine. Une taible réduction de l'hémoglobine ou de lîiématocrite a été observéeoccasion-neflement chez des patients au stade initial du traitement au LOPID. Les niveaux se stabilisera par la suite durant 1e traitement à long terme. De ce fait, une numération globulaire est recommandée tous lesdeux mois durant la première armée du traitement au LOPID.
5. Fonction hépatique. Des résultats anormaux detests sur la fonction hépatique ont été observés occasionnellement au cours du traitement au LOPID: ce sont notamment des augmentations des transaminases (SGOT, SGPT). des phosphatases alcalines etdelDH. Ces phénomènes sont généralement réversibtesà Tarrèt du traitement au LOPID. De ce fait, des etamens pérkxfiques du système hépatique sont recommandés et le traitement au LOPID devrait être interrompu si tes anomalies persistent.
6. Mrràiistrer le UDP1D avec prudence chez tes patients ayant des antécédents d'ictère ou de maladie hépatique.
7. Arythmie cardiaque. Bien qu'aucune anomalie cfinique-ment significative, qui puisse être attribuée au LOPID, n'ait été rapportée, cette possibilité pourrait toutefois oistet
EFFETS SECONDAIRES Le gemfibrozil a été soigneusement mis à l'épreuve sur plus de 3 000 patients au cours d'études contrôlées en cfinique. Les symptômes rapportés pendant la phase de contrôle de l'étude de 606 sujets, ont été évalués selon leur gravité. Les symp-tômes qui figurent sur la liste se sont présentés chez au moins cinq patients: toutes les réactions cutanées ont été rapportées
•quelle que soit leur frequence. Les principaux symptômes, dont la ftêquencea été plus forte avec gemfibrozil par rapport àceDede placebo, touchent l'appareil digestif. La nausée et le vomissement, tes douleurs abdominales et éptgastriques sont apparus plus fréquemment dans le groupe gemfibrozil que dans le groupe placebo. Toutefois, la fréquence était très fai-ble: la nausée. 4 3 % avec gemfibrozil par rapport à 3.8% avec placebo: le vomissement. 2.3% par rapport à 0 3 % : les douleurs abdominales. 6.4% par rapport à4 .2% et la douleur épigastrique. 3.4% par rapport â 1.7%.
SYMPTÔMES ET TRAITEMENT DU SURDOSACE Aucun cas de surdosage n'a été rapporté: si te cas se présen-tait. des mesuresde soutien devraient être prises en fonction des symptômes.
POSOLOGIE La dose recommandée pour les adultes est de 1200 mg et doit être administrée en deux doses fractionnées, une demi-heure avant les repas du malin et du soie. La dose maximale recom-mandée est de 1500 mg.
PRÉSENTATION La couleur des capsules de LOPID est blanche et marron. Chaque capsule contient 300 mgde gemfibrozil. Flacons de 100.
Monographie du produit disponible sur demande.
PAAB
CCPP
PARKEDAVIS Parhe-OavisCanada Inc. Scarborough.Ontario
'M. dêp. de F"arke. Davis & Company. Parke-Davis Canada Inc. usager aut.
Le travailleur devrait être évalué rapidement après le retrait de l'exposition à l'agent causal et à des intervalles de deux ans pour déter-miner les effets chroniques.
L'invalidité est déterminée par le degré d'atteinte fonctionnelle et les exigences du travail. Les besoins énergétiques requis pour l'exécu-tion de la tâche doivent être consi-dérés dans l'établissement du degré d'invalidité. Tout déficit fonction-nel dans les pneumoconioses est constant et il existe une relation entre les tests à l'exercice et ce déficit fonctionnel.
L'asthme professionnel a des traits uniques: premièrement, la spécificité de la cause de l'asthme; deuxièmement, la variabilité des symptômes asthmatiques et, troi-sièmement, l'hyperexcitabilité des bronches à des stimuli non spécifi-ques. U n e fois sensibilisé, un tra-vailleur asthmatique soumis à une exposition continuelle peut dévelop-per un asthme qui continue après l'exposition à l'agent causal. Le tra-vailleur devient alors incapable d'effectuer le travail qui a causé son asthme. II est préférable de re-connaître l'incapacité du travail-leur à accomplir ses tâches le plus rapidement possible. Une fois que l'exposition à l'agent causal a cessé, le degré du déficit fonctionnel relié à l'invalidité peut être évalué. Pour déterminer cette invalidité, il est essentiel que l'évaluation du
76 le clinicien mars 1988 8 3
déficit fonctionnel comprenne une mesure de l'hyperexcitabilité bron-chique et la médication nécessaire à l'amélioration de la condition asthmatique. Puisque l'asthme est variable, des évaluations répétées seront nécessaires.
Le tableau 2 présente une mé-thode d'évaluation du déficit fonc-tionnel et de l'invalidité. Ce schéma est basé sur celui qui est utilisé par la Commission de santé et de sécu-rité du travail du Québec. Il est ce-pendant moins détaillé et présente uniquement les principes de base de l'évaluation du déficit fonctionnel.
Le diagnostic précoce de l'asthme professionnel et la cessation rapide de l'exposition à l'agent causal faci-litent la disparition ou le contrôle de l'asthme, permettant ainsi au travailleur de reprendre rapide-ment un autre travail. Cependant, le déficit fonctionnel résiduel et l'invalidité peuvent se produire plus fréquemment et à des intervalles plus longs que prévus. Le travail-leur doit être évalué à nouveau à des intervalles de deux ans pour permettre d'établir l'invalidité per-manente.
Hand i cap s Les conséquences financières et so-ciales de Pasthme professionnel doivent être réduites au minimum. Le travailleur a droit à une consul-tation auprès d'un médecin apte à poser un diagnostic précis et à éva-
luer la nécessité d'un changement de travail. Le travailleur doit rece-voir l'assurance qu'une compensa-tion financière lui sera versée et que les comités de compensation vont amorcer les démarches néces-saires pour lui trouver un nouvel emploi. Quand ils évaluent de tels cas, les comités de compensation doivent compter sur les services d'un médecin qui connaît l'asthme professionnel. Ces comités doivent travailler rapidement afin que les travailleurs puissent décider plus facilement s'ils doivent changer de travail pour améliorer leur condi-tion asthmatique et éviter des dé-lais inutiles.
Prévention Les autorités provinciales et fédé-rales responsables de la santé et de la sécurité des travailleurs doivent identifier les industries utilisant des agents qui causent l'asthme et aviser les personnes concernées des risques qu'encourent leurs em-ployés. Les industries qui exposent des travailleurs à des causes con-firmées d'asthme professionnel doi-vent s'assurer que les concentra-tions de ces substances sont rédui-tes et que tous les efforts sont faits pour prévenir des déversements qui pourraient déclencher la sen-sibilisation. Bien qu'il faille aviser les tra-
vailleurs qu'ils courent des risques de développer l'asthme et qu'ils
peuvent obtenir de l'aide médicale, rien ne prouve qu'un programme médical de dépistage périodique soit utile. Le dépistage avant l'embauche est une mesure ten-tante puisqu'elle permet d'identi-fier les travailleurs susceptibles de développer l'asthme professionnel. Il y a peu de preuve que les sujets qui souffrent déjà d'asthme soient à plus grand risque de développer de l'asthme professionnel. Cepen-dant, puisque le diagnostic d'asthme professionnel peut être compliqué par l'existence anté-rieure de la maladie, ces sujets ne devraient probablement pas être mis en contact avec un agent cau-sal connu.
Bien que les travailleurs atopi-ques aient un plus grand risque de sensibilisation à des agents de hauts poids moléculaires que les sujets non atopiques, le risque n'est pas suffisant pour justifier le dépistage et l'élimination avant l'embauche. Le recours à des mesu-res d'hyperexcitabilité bronchique avant l'embauche pour déterminer la capacité d'effectuer un emploi n'est pas justifié.
Les figures contenues dans cet article ont été ajoutées par le docteur Malo et n'engagent pas la responsabilité de la Société de thoracologie du Canada.
Nous tenons à remercier Colette Ques-nel d'avoir relu la traduction de ce document.
76 le clinicien mars 1988 84
Screening For Occupational Asthma: A Word of Caution
Gail M. McNutt, MD; Donald P. Schlueter, MD; and Jordan N. Fink. MD
The diagnosis of occupational asthma may be difficult duo
to the complex mochanisms inducing the disorder. Identifica-
tion of the offending agent after historical documentation may
be difficult without bronchial challenge. The hallmark of
asthma is bronchial hyperreactivity as detected by methacho-
line challenge, and this test could be considered as a screening
test for asthma in the workplace. Four cases are presented
that document changes in methacholine airway reactivity
dependent on temporal association with exposure to the work-
place or to the specific offending agent. This indicates a need
for a careful evaluation of symptoms relative to exposure in
patients suspected of workplace asthma as well as serial
determinations of methacholine response to detect potential
variability in the airway reactivity.
The most f requent ly diagnosed occupationally related diseases involve the respiratory system because it is
a portal of en t ry for i r r i t an t , sensitizing, or toxic agents in the work environment.1 A variety of chemicals and organic dusts encountered in the workplace can induce pulmonary responses,0 '3 but fortunately the number of individuals affected is usually small. Although both a s t h m a and hypersensit ivity pneumonitis have been as-sociated with these exposures, occupational asthma ap-pears to be the most prevelant disorder." The recogni-tion of occupational as thma can be difficult because of the la rge number of potential offending agents, the ext remely diverse r ange of materials and processes tha t a r e involved in the workplace, and the variability in the
F r o m t h o D e p o r t m e n t of M e d i c i n e . M é d i c a l C o l l e g e of W i s c o n s i n .
M i l w a u k e e . W i s ( D r M c N u t t . F e l l o w , A l l e r g y - I m m u n o l o g y D i v i s i o n :
D r S c h l u e t e r . P r o f e s s o r of M e d i c i n e . P u l m o n a r y a n d C r i t i c a l C u r e
D i v i s i o n : D r F i n k , P r o f e s s o r of M e d i c i n c . C h i e f . A l l e r g y - I m m u n o l o g y
D i v i s i o n ) .
A d d r e s s c o r r e s p o n d e n c e t o J o r d a n N . F i n k . M D . 0 7 0 0 W W i s c o n s i n
A v e . M i l w a u k e e . W I 5 3 2 2 6 .
0 0 9 6 - 1 7 3 6 / e 1 / 3 3 0 > - 0 0 1 9 S 0 3 . 0 0 / 0 Copyright © by American College of Occupational Medicine
temporal relationship of the pulmonary response and the workers exposure.6
The diagnosis of occupational a s thma is f requent ly complex, requir ing evidence of sensitization to the sus-pected causative agent , as well as evidence t h a t t he agent can provoke the clinical manifesta t ions of the disease. Sensitization by immunoglobulin E-mast cell mediator release mechanisms may be demonst ra ted in vivo by using skin tests or in vi t ro with radioal lergosor-bent or enzyme-linked immunoassays o r ant igen-s t imu-lated histamine release from basophils. Confirmation of a causal relationship between the workplace and occu-pational as thma has been based on inhalation challenge, ei ther by removal from and r e t u r n to the work environ-ment, or, where a specific agen t has been identified, controlled challenge in the laboratory.6"7 Reproduction of the clinical symptoms^and physiologic changes t h u s identifies the sensitized individual. This type of tes t ing can be uncomfortable for the pat ient , a t t imes insensitive8 and expensive. Therefore , it is advantageous to have some type of prel iminary screening t e s t for evaluating a patient suspected of having occupational as thma.
The hallmark of as thma regard less of etiology is bronchial hyperreactivity. The hyperreact ivi ty can usu-ally be demonstrated in individuals with occupational as thma by using methacholine inhalation challenge. However, a number of factors may influence the resu l t s of this testing and thus obscure its in terpre ta t ion . Stud-ies of nonspecific airway hyperreact ivi ty in response to methacholine have demonstrated variabili ty with st im-uli such as inhaled aeroallergen,® respi ra tory infection, ozone,11 chemicals,1® and immunizations.1 3 Recognition of the variability in nonspecific a irway hyperreact ivi ty can be important in the diagnosis of and screening for occupational asthma. The following cases (summarized in the Table) i l lustrate the need for careful temporal evaluation of some patients with suspected occupational asthma, as the associated airway hyperreact ivi ty may vary in relation to exposure to the inciting agent .
Journal of Occupational Medicine/Volume 33 No. 1/January 1991 19
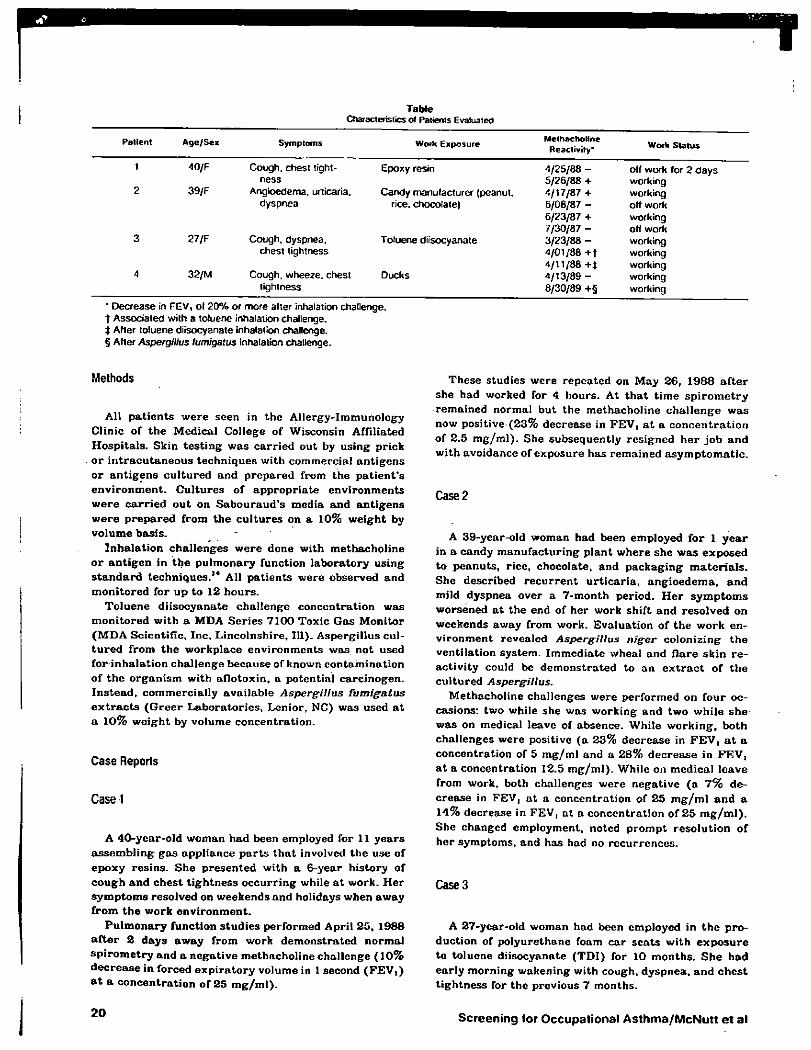
Table Characteristics of Patients Evaluated
Patient Age/Sei Symptoms Work Exposure Methacholine Reactivity* Wort Status
1 40/F Cough, chest tight- Epoxy resin 4/25/88 - off work for 2 days
39/F ness 5/26/88 + working
2 39/F Angioedema, urticaria. Candy manufacturer (peanut. 4/17/87 + working dyspnea rice, chocolate) 6/08/87 - off work
6/23/87 + working 7/30/87 - off work
3 27/F Cough, dyspnea. Toluene diisocyanate 3/23/88 - working chest tightness 4/01/88 + t working
4/11/88 +t working 4 32/M Cough, wheeze, chest Ducks 4/13/89 - working
tightness 8/30/89 +§ working
* Decrease in FEV, of 20% or more alter inhalation challenge, f Associated with a toluene inhalation challenge. Î After toluene diisocyanate inhalation challenge. § After Aspergillus fumigatus inhalation challenge.
Methods
All p a t i e n t s w e r e seen in t h c Al lergy-Immunology Clinic of t h e Medical College of Wisconsin Affi l iated Hosp i t a l s . Skin t e s t i n g w a s c a r r i e d out by us ing pr ick o r i n t r a c u t a n e o u s t echn iques with commercia l a n t i g e n s o r a n t i g e n s c u l t u r e d and p r e p a r e d f rom t h e p a t i e n t ' s e n v i r o n m e n t . C u l t u r e s of a p p r o p r i a t e e n v i r o n m e n t s w e r e c a r r i e d o u t on S a b o u r a u d ' s media a n d a n t i g e n s w e r e p r e p a r e d f rom t h e c u l t u r e s on a 10% w e i g h t by vo lume basis .
I n h a l a t i o n cha l l enges w e r e done with methachol ine o r a n t i g e n in t h e p u l m o n a r y funct ion l abora to ry us ing s t a n d a r d techniques . 1 4 All p a t i e n t s were observed and mon i to r ed for u p to 12 hou r s .
To luene d i i socyana te cha l l enge concen t ra t ion was mon i to r ed wi th a MDA Se r i e s 7100 Toxic Gas Moni to r ( M D A Scient i f ic , Inc . Lincolnshi re , 111). Asperg i l lus cul-t u r e d f rom t h e workp lace env i ronmen t s was not used fo r inha la t ion cha l lenge because of known con tamina t ion of t h e o r g a n i s m with a f lo toxin , a potent ia l ca rc inogen . I n s t e a d , commerc ia l ly ava i lab le Aspergillus fumigatus
e x t r a c t s ( G r e e r Labo ra to r i e s , Lenior , NC) was used a t a 10% w e i g h t by volume concen t ra t ion .
Case Reports
Case 1
A 40-year -o ld woman had been employed for 11 y e a r s a s s e m b l i n g g a s app l iance p a r t s t h a t involved t h e use of e p o x y res ins . S h e p re sen t ed with a 6-year h is tory of c o u g h a n d ches t t i gh tne s s o c c u r r i n g while a t work . H e r s y m p t o m s resolved on weekends and holidays when away f r o m t h e work e n v i r o n m e n t .
P u l m o n a r y func t ion s t u d i e s pe r fo rmed April 25, 1988 a f t e r 2 d a y s a w a y f rom work d e m o n s t r a t e d normal s p i r o m e t r y a n d a nega t i ve methachol ine cha l lenge ( 1 0 % d e c r e a s e in forced e x p i r a t o r y volume in 1 second ( F E V , ) a t a c o n c e n t r a t i o n of 25 m g / m l ) .
These s tudies were r epea ted on May 26, 1988 a f t e r she had worked for 4 hours . At t h a t t ime s p i r o m e t r y remained normal but the methachol ine c h a l l e n g e w a s now positive ( 2 3 % dec rease in FEV, a t a c o n c e n t r a t i o n of 2 .5 m g / m l ) . She subsequent ly res igned h e r j o b a n d wi th avoidance of exposu re has remained a s y m p t o m a t i c .
Case 2
A 39-year-old woman had been employed fo r 1 y e a r in a candy m a n u f a c t u r i n g p lan t w h e r e s h e w a s exposed to peanu t s , r ice, chocolate , and p a c k a g i n g m a t e r i a l s . She described r e c u r r e n t u r t i c a r i a , a n g i o e d e m a , a n d mild dyspnea over a 7 -month per iod. H e r s y m p t o m s worsened a t the end of he r work sh i f t and reso lved on weekends away f rom work. Evalua t ion of t h e work en-v i ronmen t revealed Aspergillus niger coloniz ing t h e vent i la t ion system. I m m e d i a t e wheal and f l a r e skin r e -ac t iv i ty could be d e m o n s t r a t e d to an e x t r a c t of t h e c u l t u r e d Aspergillus.
Methachol ine chal lenges were pe r fo rmed on fou r oc-casions: two while she was working and two whi le she-was on medical leave of absence. While w o r k i n g , bo th chal lenges were positive ( a 23% decrease in F E V , a t a concent ra t ion of 5 m g / m l and a 28% d e c r e a s e in F E V , a t a concent ra t ion 12.5 m g / m l ) . While on medica l l eave f rom work, both chal lenges w e r e nega t ive ( a 7 % de-c rease in FEV, a t a concen t ra t ion of 2 5 m g / m l a n d a 14% decrease in FEV, a t a concen t ra t ion of 2 5 m g / m l ) . She changed employment , noted p r o m p t reso lu t ion of he r symptoms, and has had no r e c u r r e n c e s .
Case 3
A 27-year-old woman had been employed in t h e p ro-duct ion of po lyure thane foam c a r s e a t s wi th e x p o s u r e to to luene di isocyanate ( T D I ) for 10 months . S h e h a d ea r ly morn ing wakening with cough, dyspnea , a n d c h e s t t i g h tn e s s for t h e previous 7 months .
20 Screening for Occupational Asthma/McNutt et al