Pr FaiçalJARRAYA, MD - Promotion de l’épidémiologie...
73
Pr Faiçal JARRAYA, MD Néphrologue ESH Clinical Hypertension Specialist Service de Néphrologie, CHU Hédi Chaker, Sfax, Tunisie Unité de Recherche 12ES14 Pathologie rénale, Faculté de médecine, Sfax Nouakchott, le 15 Novembre 2015
-
Upload
nguyenmien -
Category
Documents
-
view
214 -
download
0
Transcript of Pr FaiçalJARRAYA, MD - Promotion de l’épidémiologie...
Pr Faiçal JARRAYA, MDNéphrologue
ESH Clinical Hypertension SpecialistService de Néphrologie, CHU Hédi Chaker, Sfax, Tunisie
Unité de Recherche 12ES14 Pathologie rénale, Faculté de médecine, Sfax
Nouakchott, le 15 Novembre 2015

Global maps for level 3 risk factors in 2013 of attributable DALYs for females (B)
DALYs=disability-adjusted life-years / années de vie ajustées sur l'incapacité
Global, regional and national comparative risk assessment of 79 behavioural, environmental
and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a
systematic analysis for the Global Burden of Disease Study 2013.
GBD 2013 Risk Factors Collaborations
Lancet. Published Online September 11, 2015

Global maps for level 3 risk factors in 2013 of attributable DALYs for males (A)
DALYs=disability-adjusted life-years / années de vie ajustées sur l'incapacité
Global, regional and national comparative risk assessment of 79 behavioural, environmental
and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a
systematic analysis for the Global Burden of Disease Study 2013.
GBD 2013 Risk Factors Collaborations
Lancet. Published Online September 11, 2015
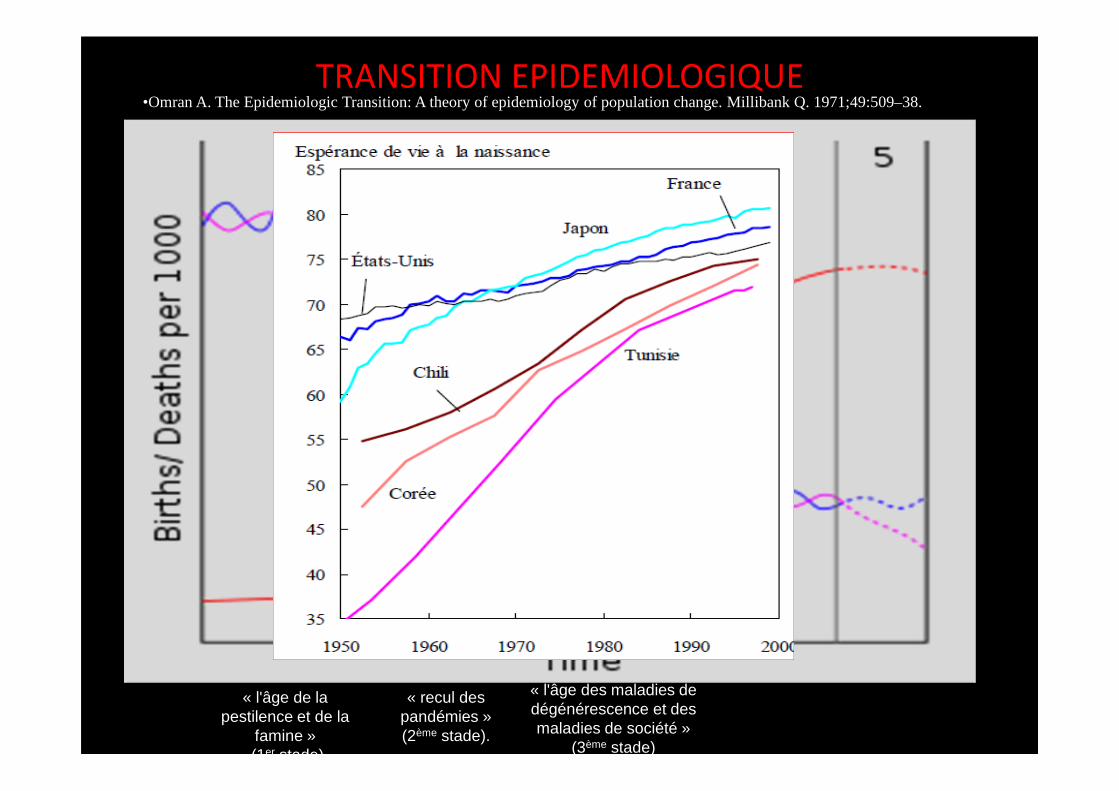
TRANSITION EPIDEMIOLOGIQUE
« l'âge de la pestilence et de la
famine »(1er stade)
« recul des pandémies » (2ème stade).
« l'âge des maladies de dégénérescence et des maladies de société »
(3ème stade)
•Omran A. The Epidemiologic Transition: A theory of epidemiology of population change. Millibank Q. 1971;49:509–38.

PRINCIPAUX GROUPES DE MALADIES OU CAUSES EXTERIEURES
2009
N %MALADIES DU SYSTEME CIRCULATOIRE 6461 28.9TUMEURS MALIGNES 3599 16.1
MALADIES ENDOCRINIENNES, NUTRITIONNELLES ET METABOLIQUES 2289 10.2
MALADIES DE L’APPAREIL RESPIRATOIRE 2502 11.2
AFFECTIONS DONT L’ORIGINE SE SITUE DANS LA PERIODE PERINATALE 1480 6.6
CAUSES EXTERIEURES DE MORTALITE (ACCIDENTS, CHUTES,…) 648 2.9
MALADIES DE L’APPAREIL GENITO-URINAIRE 674 3.0MALADIES DE L’APPAREIL DIGESTIF 683 3.1
LESIONS TRAUMATIQUES ET EMPOISONNEMENTS 795 3.6
MALADIES DU SYSTEME NERVEUX ET DES ORGANES DES SENS 623 2.8
MALADIES INFECTIEUSES ET PARASITAIRES 674 3.0
MALFORMATIONS CONGENITALES ET ANOMALIES CHROMOSOMIQUES 424 1.9
MALADIES DU SANG ET DES ORGANES HEMATOPOIETIQUES 151 0.7
AUTRES CAUSES 1355 6.0TOTAL 22358 100.0
Janvier 2013
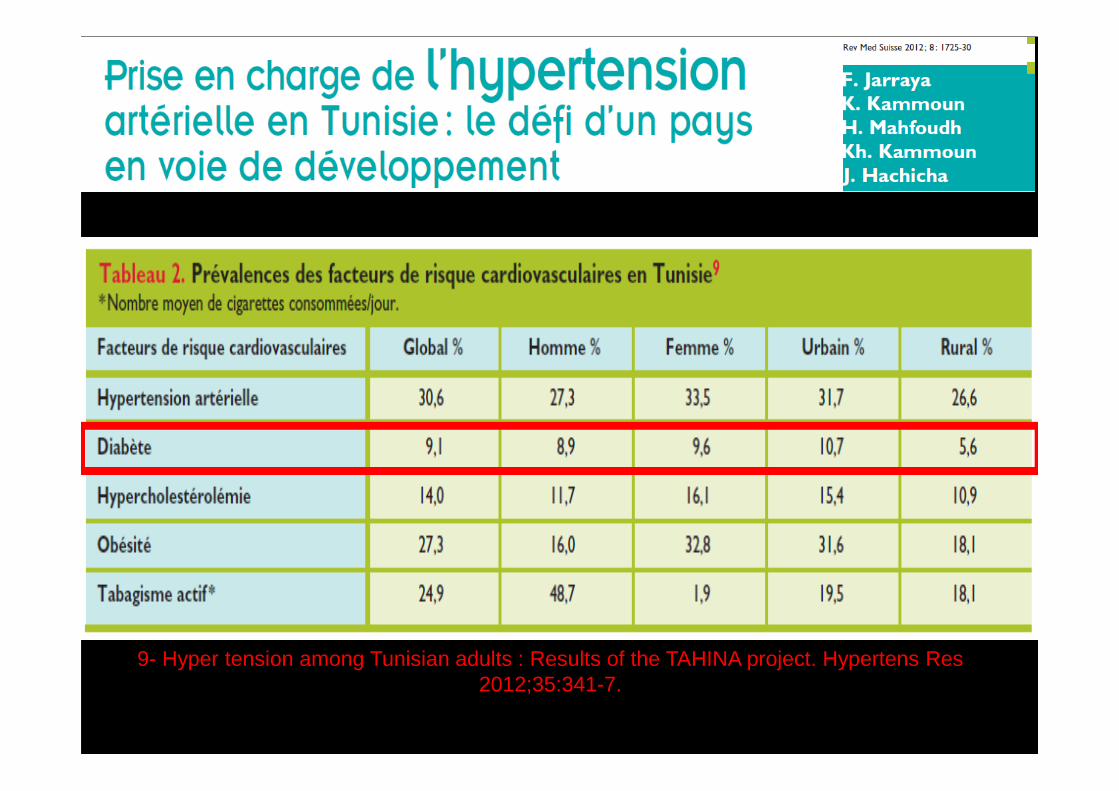
9- Hyper tension among Tunisian adults : Results of the TAHINA project. Hypertens Res 2012;35:341-7.

http://www.era-edta-reg.org

INCIDENCE: 2008 = 135 pmpDiabetes 29pmp

PREVALENCE: 2008 = 750pmpDiabetes: 154pmp

Tunisie 2010
NEPHROPATHIES CODES EFFECTIF %Glomérulosclérose Diabétique / Néphropathies Diabétiques
80 1 786 21. 0 %
Néphropathie Vasculaire due à une HTA / HTA Maligne
72 - 71 1 157 13. 6 %
Glomérulonéphrite sans Preuve Histologique 10 715 8. 4 %
Pyélonéphrite de Cause Non Précisée 20 459 5. 4%
Polykystoses de l’Adulte /Polyk. Non Précisées 40 - 41 289 3. 4 %
Pyélonéphrite due à une Lithiase Rénale / Urinaire ou uropathie
25 - 23 230 2. 7 %
Néphropathie Vasculaire Cause Non Précisée 70 170 2. 0 %
Néphropathie Interstitielle Autre ou de Cause Non Précisée
30 127 1. 5 %
Amylose Rénale 83 85 1. 0 %
Pyélonéphrite due à une Uropathie Obstructive Congénitale avec ou sans Réflux Vésico-Urétéral
22 68 0. 8 %
Incidence : 133 patients par million d’habitants.
Prévalence : 806 patients par million d’habitants.
Dr C Mahjoubi, Registre de dialyse, MSP

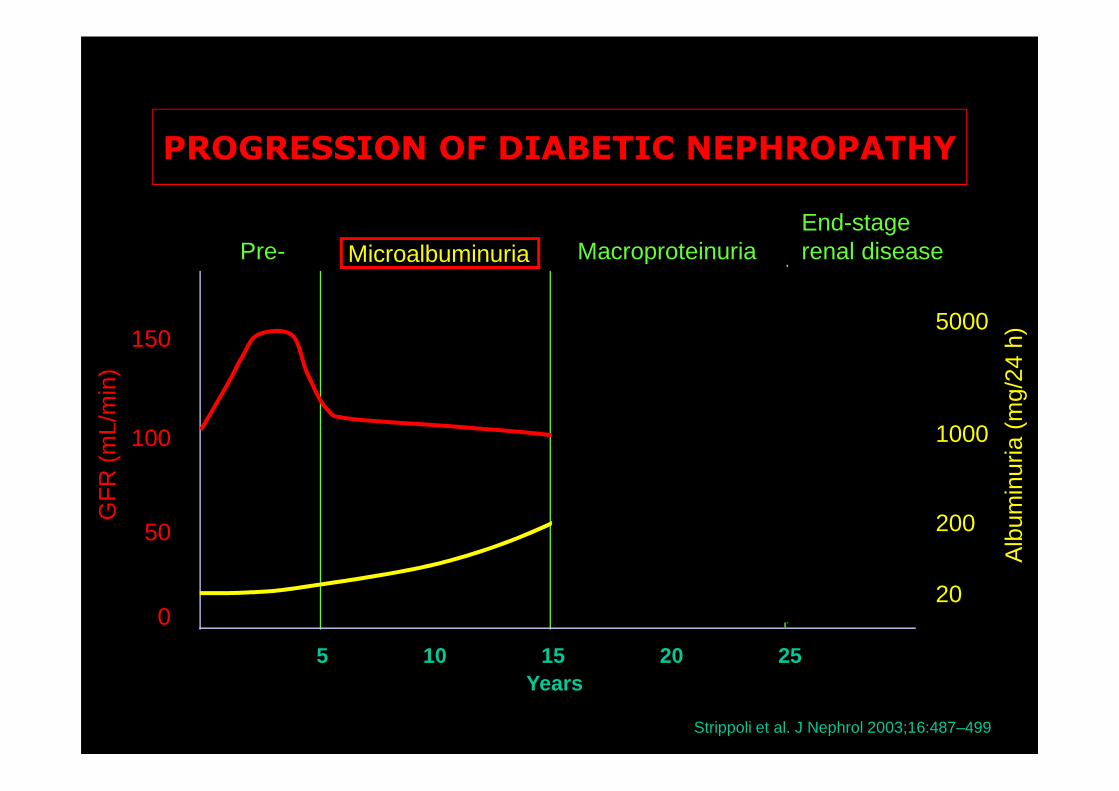
PROGRESSION OF DIABETIC NEPHROPATHY
Microalbuminuria
150
100
50
0
GF
R (
mL/
min
)
5000
1000
200
20
Alb
umin
uria
(m
g/24
h)
5 10 15 20 25Years
Pre- MacroproteinuriaEnd-stagerenal disease
Strippoli et al. J Nephrol 2003;16:487–499

Baseline proteinuria as a determinant for renal eventsin type 2 diabetes
De Zeeuw et al; Kidney Int 2004
Primary composite Endpoint
0
10
15
5
Ha
zard
ra
tio
<.5 2.0 2.95 4.4 ≥5.25≥≥≥≥≥≥≥
Baseline Albuminuria (g/g) Baseline Albuminuria (g/g)
0
<.5 2.0 2.95 4.4 5.25
ESRD
10
20
30
≥H
aza
rd r
atio
F. JARRAYA 17-3-09
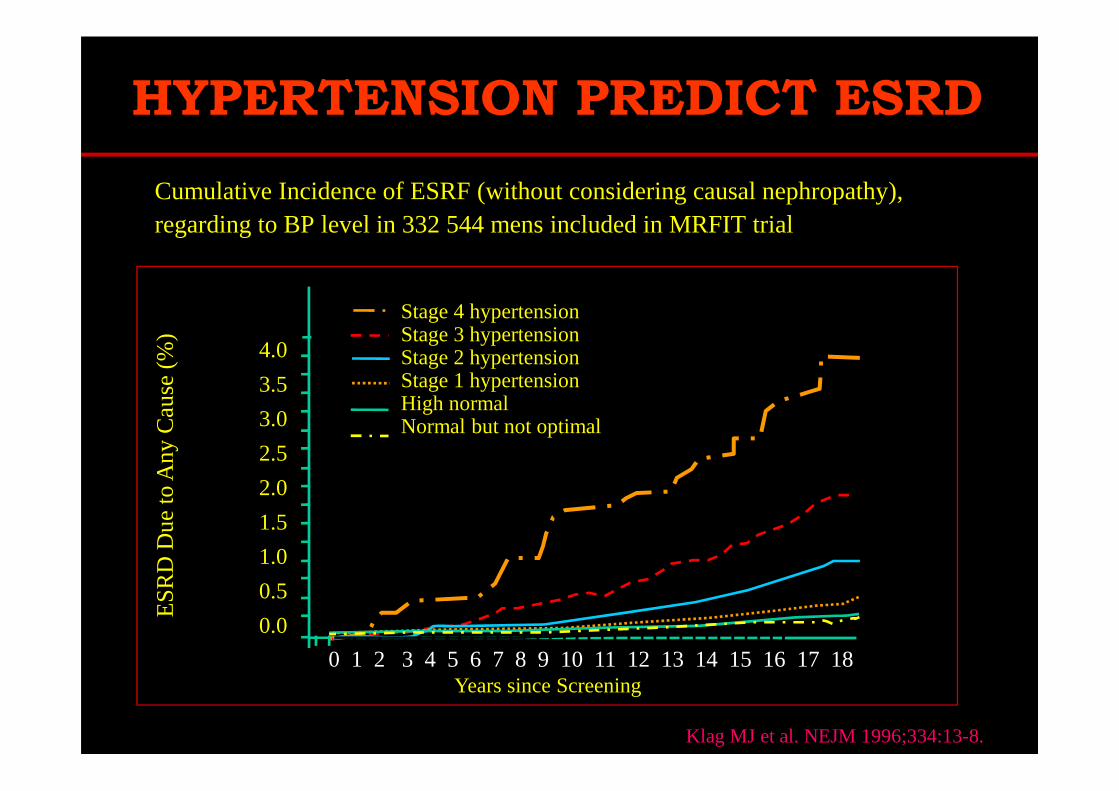
HYPERTENSION PREDICT ESRD
Cumulative Incidence of ESRF (without considering causal nephropathy), regarding to BP level in 332 544 mens included in MRFIT trial
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Years since Screening
Klag MJ et al. NEJM 1996;334:13-8.
Stage 4 hypertensionStage 3 hypertensionStage 2 hypertensionStage 1 hypertensionHigh normalNormal but not optimal
ES
RD
Due
to A
ny C
aus
e (
%)

1/creatinin x 103
T1 DM + NPDIRCT après 7 ans (5 - 15 ans) RH Jones et al. Lancet 1979
Evolution Spontanée
de la Fonction
Rénale chez les Patients Atteint de
Néphropathie Diabétique
Si on ne fait rien…..!!!

PREVENIR, RALENTIR LA PROGRESSION…
1. HTA2. Prot-urie3. Lipides4. Néphro
toxicité5. Tabac,
protides
Temps (an)2 4 6 8 10 12 14
-4ml/min/anralentissement-12ml/min/an
Ccr (ml/min)
100
50
Dialyse10
60
Intervention
rémission
Facteurs
de progression :

PROGRESSION OF DIABETIC NEPHROPATHY
Microalbuminuria
150
100
50
0
GF
R (
mL/
min
)
5000
1000
200
20
Alb
umin
uria
(m
g/24
h)
5 10 15 20 25Years
Pre- MacroproteinuriaEnd-stagerenal disease
Strippoli et al. J Nephrol 2003;16:487–499
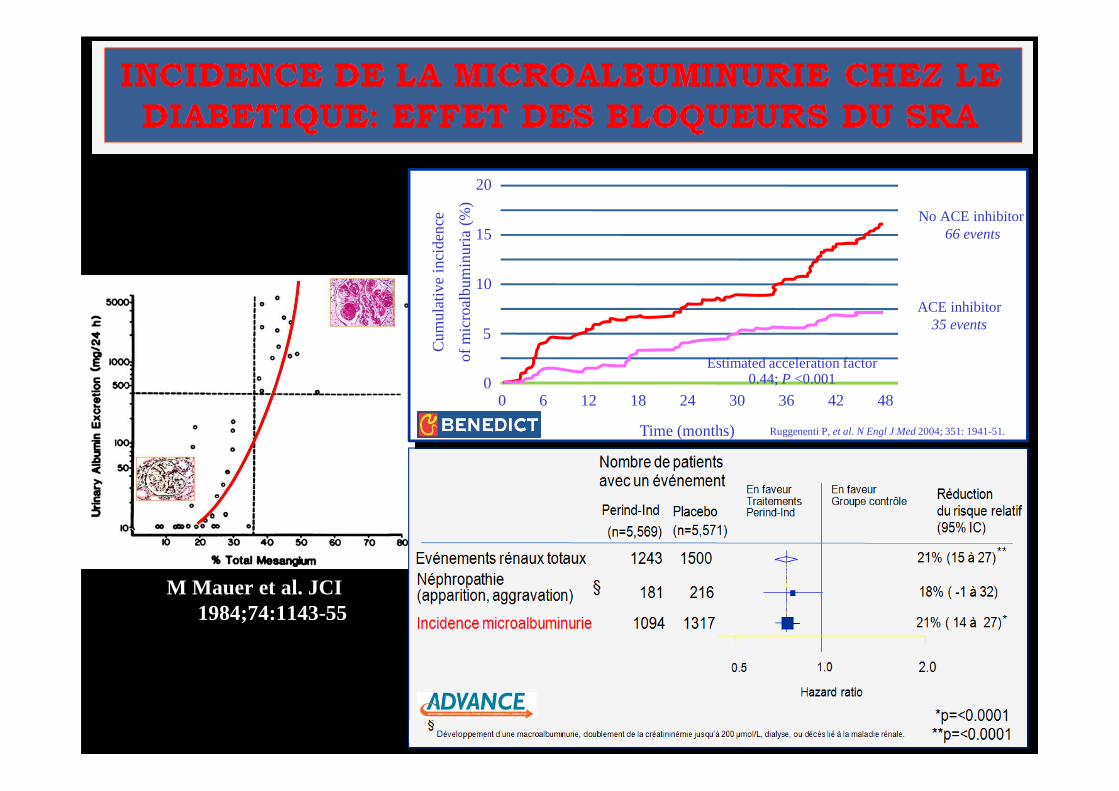
M Mauer et al. JCI 1984;74:1143-55
0
10
20
0 6 12 18 24 30 36 42 48
5
Cum
ulat
ive
inci
denc
e
of m
icro
albu
min
uria
(%
)
Time (months)
ACE inhibitor35 events
No ACE inhibitor66 events15
Estimated acceleration factor 0.44; P <0.001
Ruggenenti P, et al. N Engl J Med2004; 351: 1941-51.

Hasslacher, Nephrol Dial Transpl (1989) 4: 859

Diabète Type 2
� 50% vont présenter une microalbuminurie au moment du diagnostic (probablement secondaire (?) à l’HTA)
� 20% avec µ-albuminurie vont progresser à une NPD protéinurique
� Près de 100% avec une ‘‘macro' protéinurie vont progresser à une IRCT
Diabète Type 1
� 25 - 45% développeront une NPD
� 80-90% avec µ-albuminurie vont progresser à une NPD protéinurique dans 5 - 10 ans
� Près de 100% avec une ‘‘macro' protéinurie vont progresser à une IRCT dans 7 - 10 ans
Epidemiologie de la néphropathie diabétique


Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
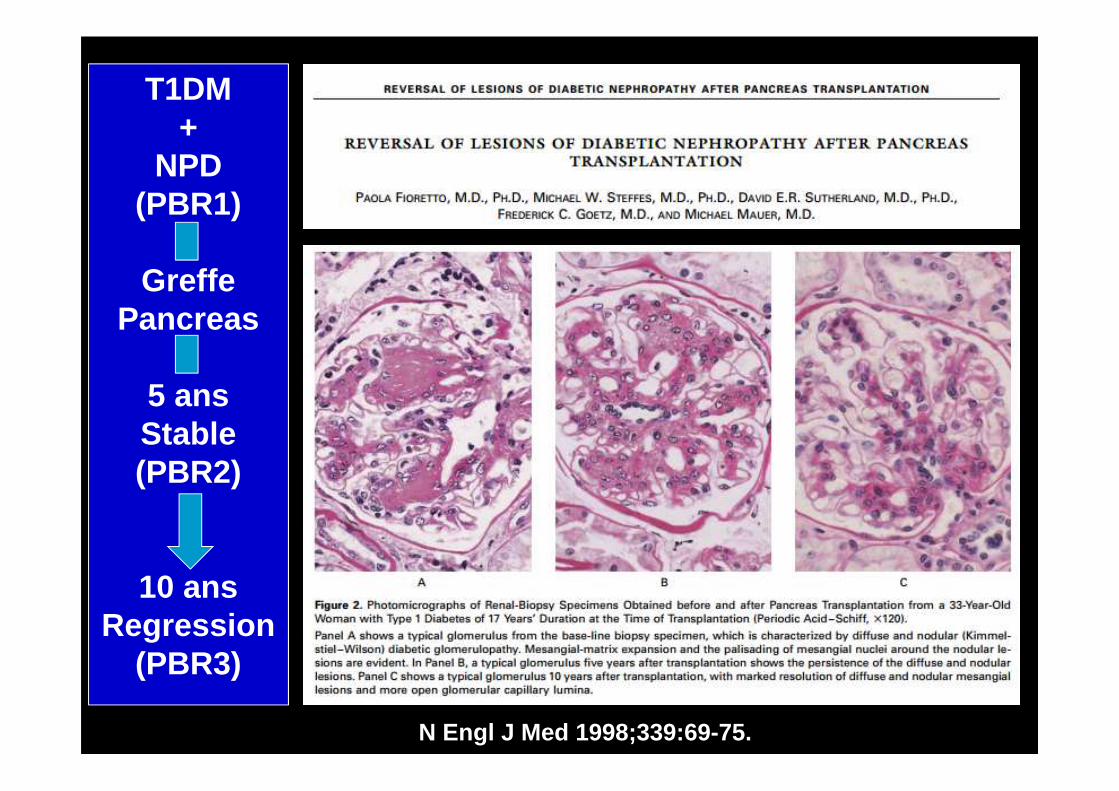
N Engl J Med 1998;339:69-75.
T1DM+
NPD(PBR1)
Greffe Pancreas
5 ansStable(PBR2)
10 ansRegression
(PBR3)

P=0.04
PROGRESSION OF DIABETIC NEPHROPATHY
Microalbuminuria
150
100
50
0
GF
R (
mL/
min
)
5000
1000
200
20
Alb
umin
uria
(m
g/24
h)
5 10 15 20 25Years
Pre- MacroproteinuriaEnd-stagerenal disease
Strippoli et al. J Nephrol 2003;16:487–499

Conditions: Repetition de la mesureAbsence d’infection uro-génitaleAbsence de fiévre et d’état inflammatoireNon précédée d’un effort
Kidney International Suppl. (2013) 3, 19–62

Le continuum réno-cardio-vasculaire
Dyslipidémie
Diabètes
Hypertension
S Métabolique
Facteurs de risques
Atheroscleroses
& HVG
microalbuminurie
Syndrome
Coronarien
Aigu--------
AIT-AVC
IC Congestive
IC terminale
Décès
modified from Ungur et al
Am J Cardiol 2002;89
Normo Albu µ Albu ↓ Cl. Créatinine IRCT DécèsAlbu - SN
CONTROVERSE
!!!!

Nephroprotection
FDR
renaux
Diabète
HTA
Micro
albuminurie
Proteinure
↑Crea>nine
↓eGFR
↓eGFR
IRC
x2 Creatinine
IRCT
Décès
Critères
intermédiaires
Critères
Hard End Point
F. JARRAYA 2015

*p <0.01 vs placebo.Parving H-H et al. N Engl J Med. 2001; 345: 870–8
0
5
10
15
20
0 6 12 18 22 24
Follow-up (months)
Incidence of diabeticnephropathy (%)
Placebo
Irbesartan(150 mg/d)
Irbesartan (300 mg/d) *
RR = 70%
THE EFFECT OF IRBESARTAN ON MICRO-ALBUMINURIA IN HYPERTENSIVE PATIENTS WITH TYPE 2 DIABETES « IRMA2 »
31
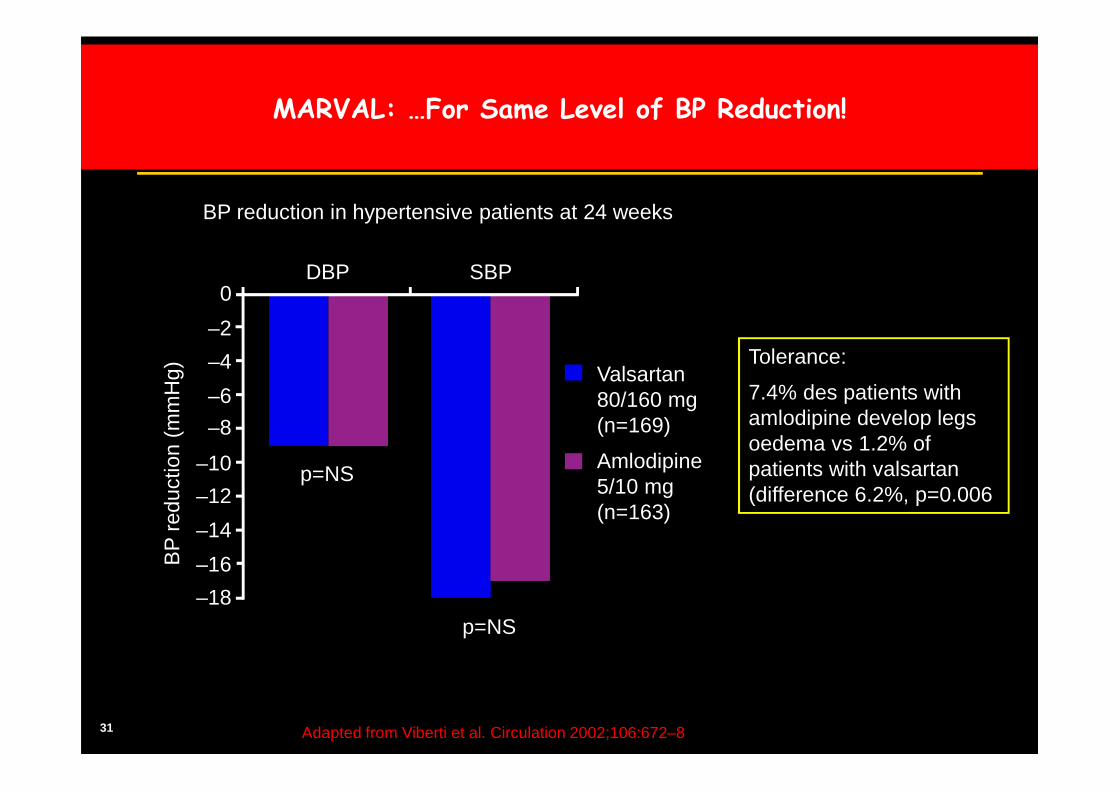
MARVAL: …For Same Level of BP Reduction!
BP reduction in hypertensive patients at 24 weeks
Adapted from Viberti et al. Circulation 2002;106:672–8
Valsartan 80/160 mg(n=169)
Amlodipine 5/10 mg(n=163)
Tolerance:
7.4% des patients with amlodipine develop legs oedema vs 1.2% of patients with valsartan(difference 6.2%, p=0.006
DBP SBP
BP
red
uctio
n (m
mH
g)
p=NS
p=NS
–8
–6
–4
–2
0
–10
–12
–14
–16
–18

32 Viberti et al. Circulation 2002;106:672–8
MARVAL: Valsartan is Significantly More Effective Than Amlod ipine in Reducing UAER in Type 2 Diabetes Patients With Micr oalbuminuria …
**p<0.001 vs amlodipine Time (week)
Cha
nge
in u
rinar
y al
bum
inex
cret
ion
rate
(%)
20
10
0
–10
–20
–30
–40
–500 4 8 12 18 24
Valsartan-based Tx (n=146)
Amlodipine-based Tx (n=145)
–8%
–44%**
Results from a 24-week study in 291 patients† with type 2 diabetes and microalbuminuria‡ (MARVAL study )

33
MARVAL: Valsartan Provides Regression to Normo-albuminuria
in T2DM Patients vs. Amlodipine
0
5
10
15
20
25
30
35
14.5
29.9*
Valsartan 80/160 mg Amlodipine 5/10 mg
Viberti et al. Circulation 2002;106:672–8
Results from a 24-week study in 291 patients† with type 2 diabetes and microalbuminuria‡
†Patients completing the study; ‡Median UAER 20-200 µg/min; *p<0.001 vs. amlodipine; # DIOVAN 80 mg and amlodipine 5 mg doses doubled at 4 weeks if BP uncontrolled (BP >135/85 mmHg); bendrofluazide 12.5 mg and doxazosin added as needed at 8 and 12 weeks, respectively, if BP still uncontrolled; UAER=Urinary albumin excretion rate
Pat
ient
s re
gres
sing
to
norm
oalb
umin
uria
(%)
34
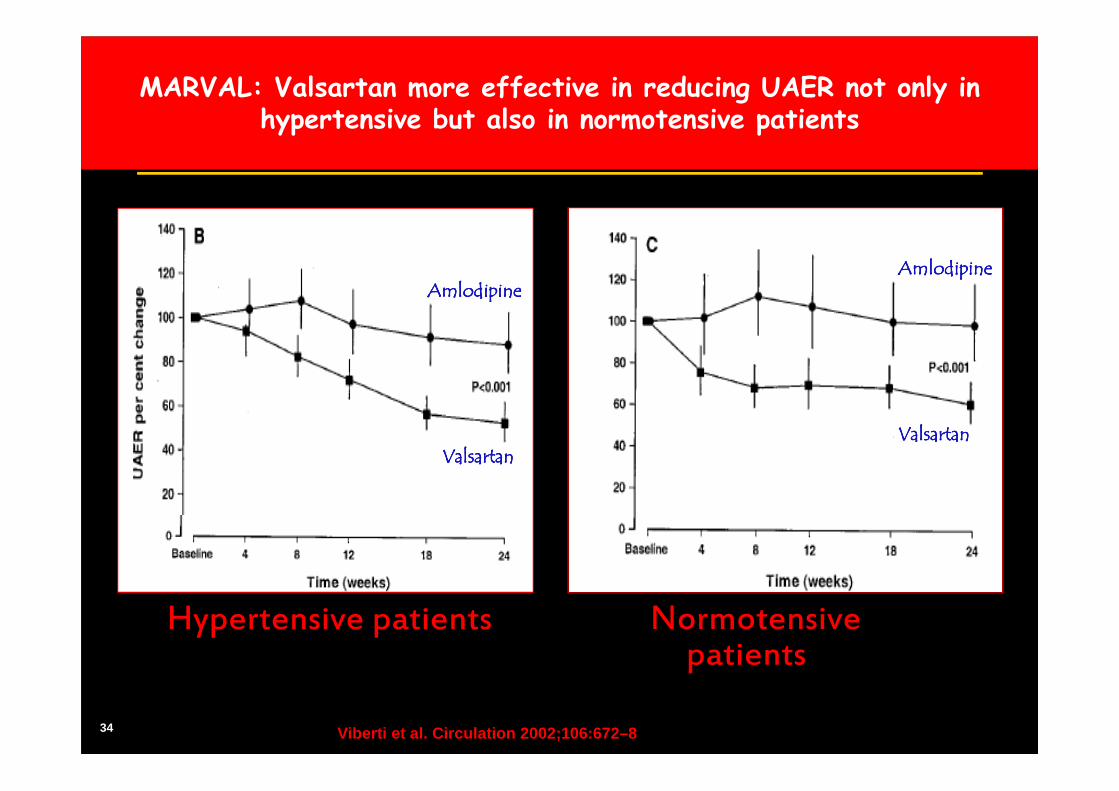
Hypertensive patients Normotensivepatients
AmlodipineAmlodipineAmlodipineAmlodipine
ValsartanValsartanValsartanValsartan
AmlodipineAmlodipineAmlodipineAmlodipine
ValsartanValsartanValsartanValsartan
MARVAL: Valsartan more effective in reducing UAER not only in hypertensive but also in normotensive patients
Viberti et al. Circulation 2002;106:672–8

35
P=0.02

PROGRESSION OF DIABETIC NEPHROPATHY
Microalbuminuria
150
100
50
0
GF
R (
mL/
min
)
5000
1000
200
20
Alb
umin
uria
(m
g/24
h)
5 10 15 20 25Years
Pre- MacroproteinuriaEnd-stagerenal disease
Strippoli et al. J Nephrol 2003;16:487–499

Col IV
Fibronecti
ne
Laminine
RANDOMIZED EVALUATION OF NONINSULIN DEPENDENT DIABETES MELLITUS WITH THE ANGIOTENSIN-II ANTAGONIST LOSARTAN
« RENAAL »
CJP composite de 16%. p: 0.02taux de la protéinurie de 35% p: <0,001
incidence de dédoublement de créatinine de 25% p: 0.006
incidence d’IRCT de 28%. p: 0.002
BM Brenner et al. NEJM 2001
Créat x 2Proteinurie IRCT
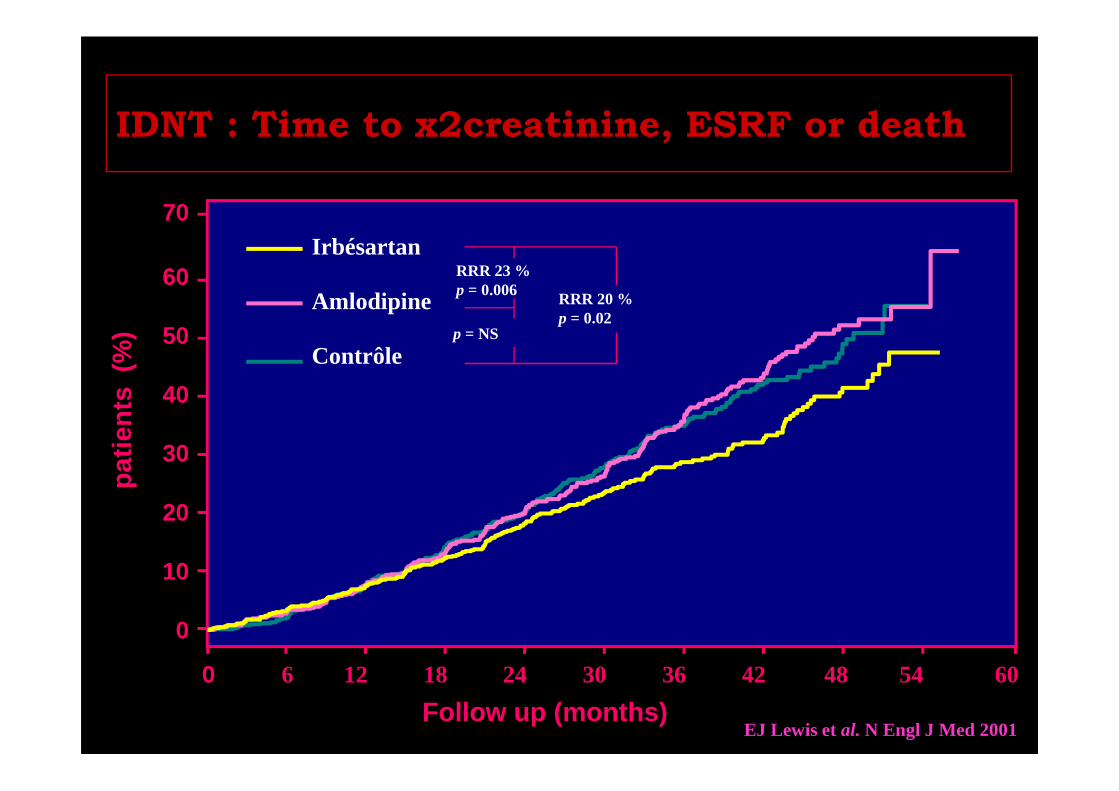
IDNT : Time to x2creatinine, ESRF or deathpa
tient
s (
%)
0 6 12 18 24 30 36 42 48 54
Follow up (months)60
0
10
20
30
40
50
60
70Irbésartan
Amlodipine
Contrôle
RRR 20 %p = 0.02
p = NS
RRR 23 %p = 0.006
EJ Lewis et al. N Engl J Med 2001
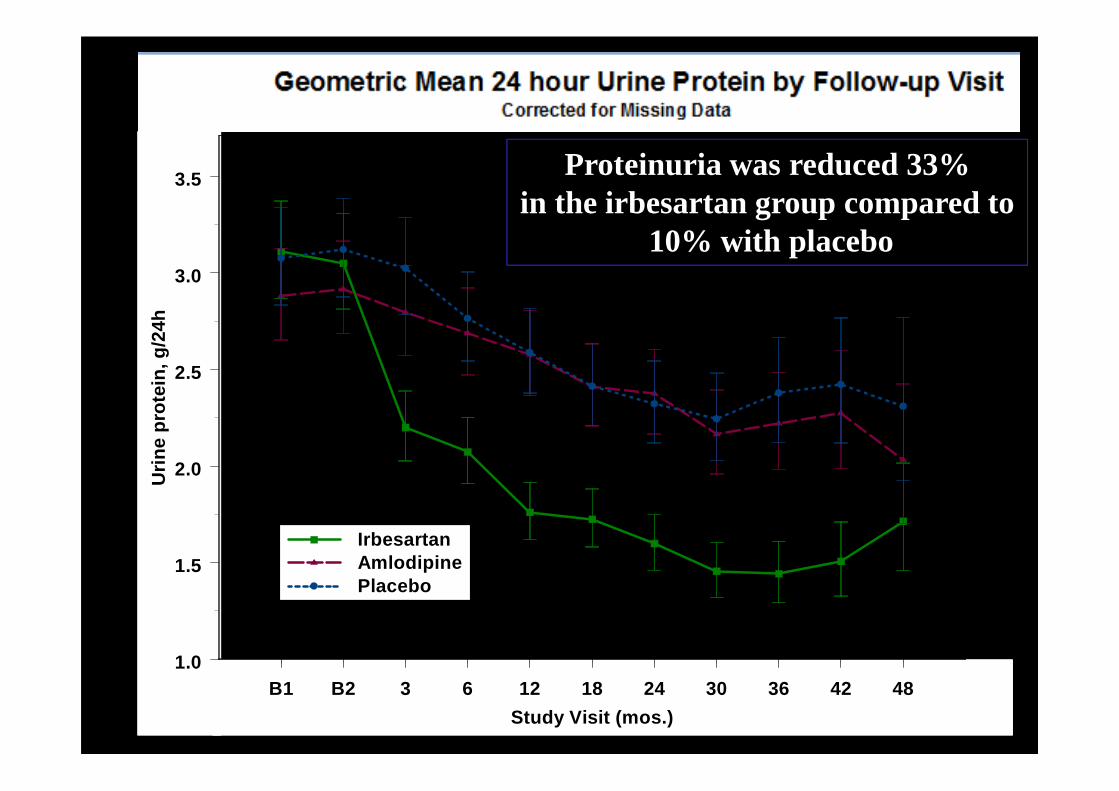
B1 B2 3 6 12 18 24 30 36 42 48
Study Visit (mos.)
1.0
1.5
2.0
2.5
3.0
3.5U
rine
prot
ein,
g/2
4h
Geometric Mean 24 hour Urine Protein by Follow-up V isitCorrected for Missing Data
IrbesartanAmlodipinePlacebo
Proteinuria was reduced 33% in the irbesartan group compared to
10% with placebo

Albumin Glycation in diabetes render UAE more toxic for nephron
ML. Gross et al, Kidney Int, Vol. 62 (2002), pp. 51–59 and unpublished data
More renal scarring by glycated albumin
ScoresProtein Peritubular
droplets fibrosis
NaCl 1.23±0.5 0.40±0.05
Albumin 2.74±0.4 2.87±0.7
Glycated albumin 3.70±0.4 3.3±0.6

†UAER 20-700 µg/min; *p<0.001 vs.160 mg (30 weeks vs. 4 weeks); **p<0.05 vs. 160 mg; T2D=Type 2 diabetes mellitus; UAER=Urinary albumin excretion rate
Valsartan160 mg(n=130)
Valsartan320 mg(n=130)
Valsartan640 mg(n=131)
Cha
nge
in U
AE
R fr
om
base
line
(%)
-25%
-51%*-49%*
-55
-45
-35
-25
-15
-5
12%
19%
24%**
0
5
10
15
20
25
Valsartan160 mg(n=130)
Valsartan320 mg(n=130)
Valsartan640 mg(n=131)
Pat
ient
s re
gres
sing
tono
rmoa
lbum
inur
ia(%
)
DROP Study: Valsartan Reduces UAER in Patients withT2D, HTN and Albuminuria
Hollenberg et al J Hypertens 2007,25:1921-1926
Results from a 30-week study in 391 patients with T2D, HTN and albuminuria† (DROP study)
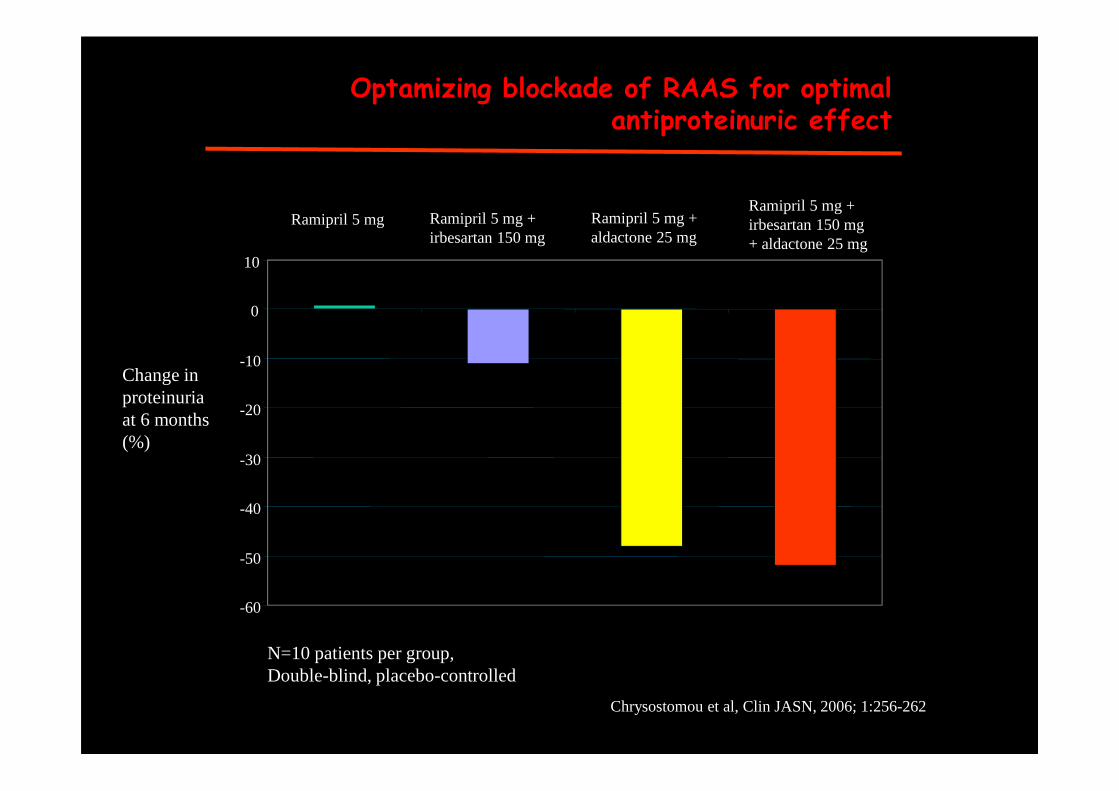
-60
-50
-40
-30
-20
-10
0
10
Change inproteinuriaat 6 months(%)
Ramipril 5 mg Ramipril 5 mg +irbesartan 150 mg
Ramipril 5 mg +aldactone 25 mg
Ramipril 5 mg +irbesartan 150 mg+ aldactone 25 mg
Optamizing blockade of RAAS for optimal antiproteinuric effect
N=10 patients per group,Double-blind, placebo-controlled
Chrysostomou et al, Clin JASN, 2006; 1:256-262

43
Bakris GL et al. Am J Kidney Dis 2000; 36(3): 646-661
95 98 101 104 107 110 113 116 119
r = 0.69;P < 0.05
MBP1 (mmHg)
130/85
1Mean Blood Pressure
140/90
Untreated HT
0
-2
-4
-6
-8
-10
-12
-14
Meta-analysis: relation between BP reduction and GFR in Type 2 diabetic patients with proteinuric DPN
Normal GFR 120ml/mn/1.73m²

Objectifs tensionnels changent selon les recommandations…
(American Diabetes Association.Clinical Practice Recommendations 2013.Diabetes Care 2013;36(Suppl.1):S109-S110.)
Chez le diabétique: PA<140/80mmHg
Chez l’hypertendus: PA<140/80mmHg
Chez le ccoronarien: PA<140/90mmHg
Chez le patient atteint de MRC ND:
Non Diabétique +Albu <30mg/24h: PA<140/90mmHgNon Diabétique +Albu 30-300mg/24h: PA<130/80mmHgNon Diabétique +Albu >300mg/24h: PA<130/80mmHg
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease. J Am Coll Cardiol.2012Dec 18;60(24):e44-e164
2012 KDIGO Clinical Practice Guideline for management of Blood Pressure in CKD . Kidney Int 2012
Diabétique +Albu <30mg/24h: PA<140/90mmHgDiabétique +Albu 30-300mg/24h: PA<130/80mmHgDiabétique+ Albu >300mg/24h: PA<130/80mmHg
HTA>130/80
HTA>130/80
2013 ESH/ESC Guidelines for themanagement of arterial hypertension. Journal of Hypertension 2013, 31:1281–1357 2014 JNC 8
F Jarraya 2013
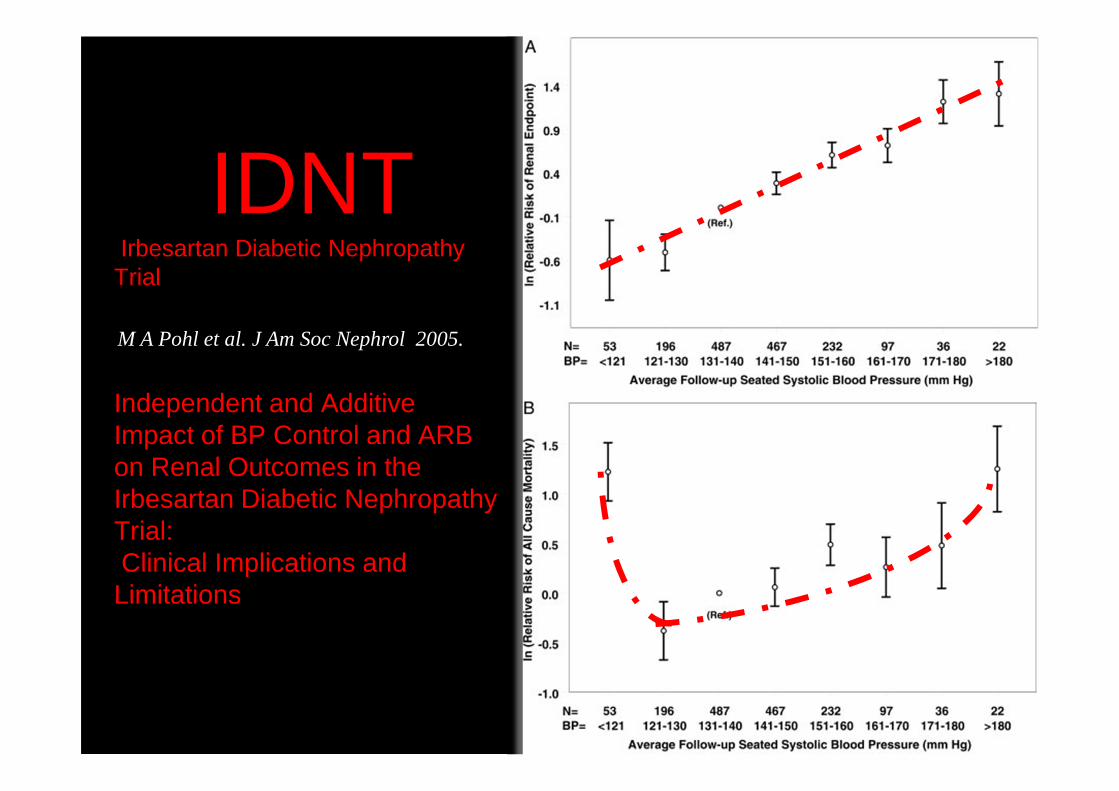
IDNTIrbesartan Diabetic Nephropathy
Trial
Independent and Additive Impact of BP Control and ARB on Renal Outcomes in the Irbesartan Diabetic Nephropathy Trial:Clinical Implications and Limitations
M A Pohl et al. J Am Soc Nephrol 2005.
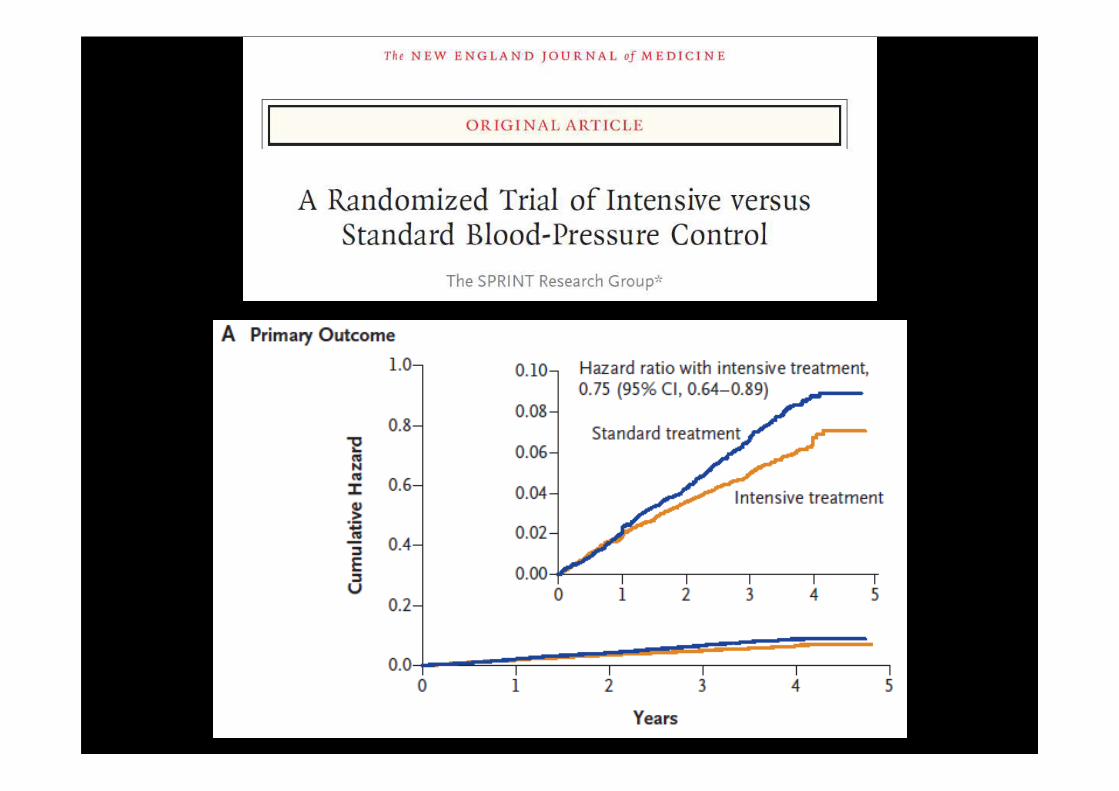
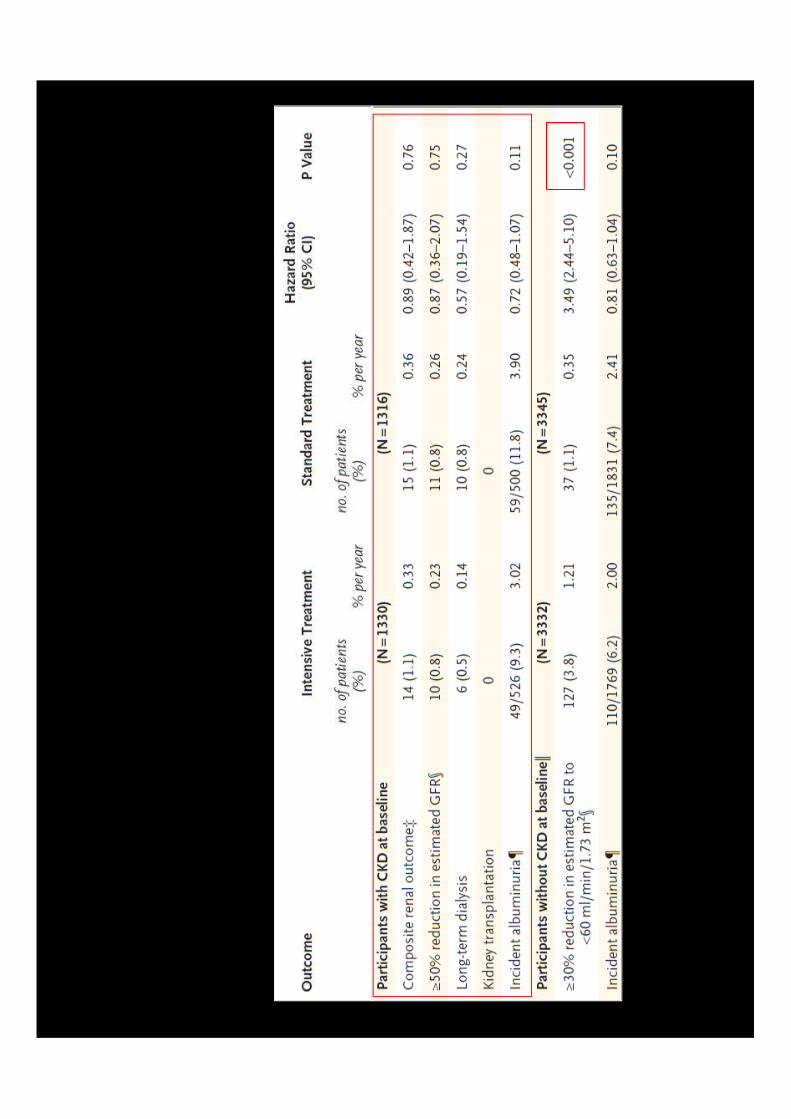
SPRINT
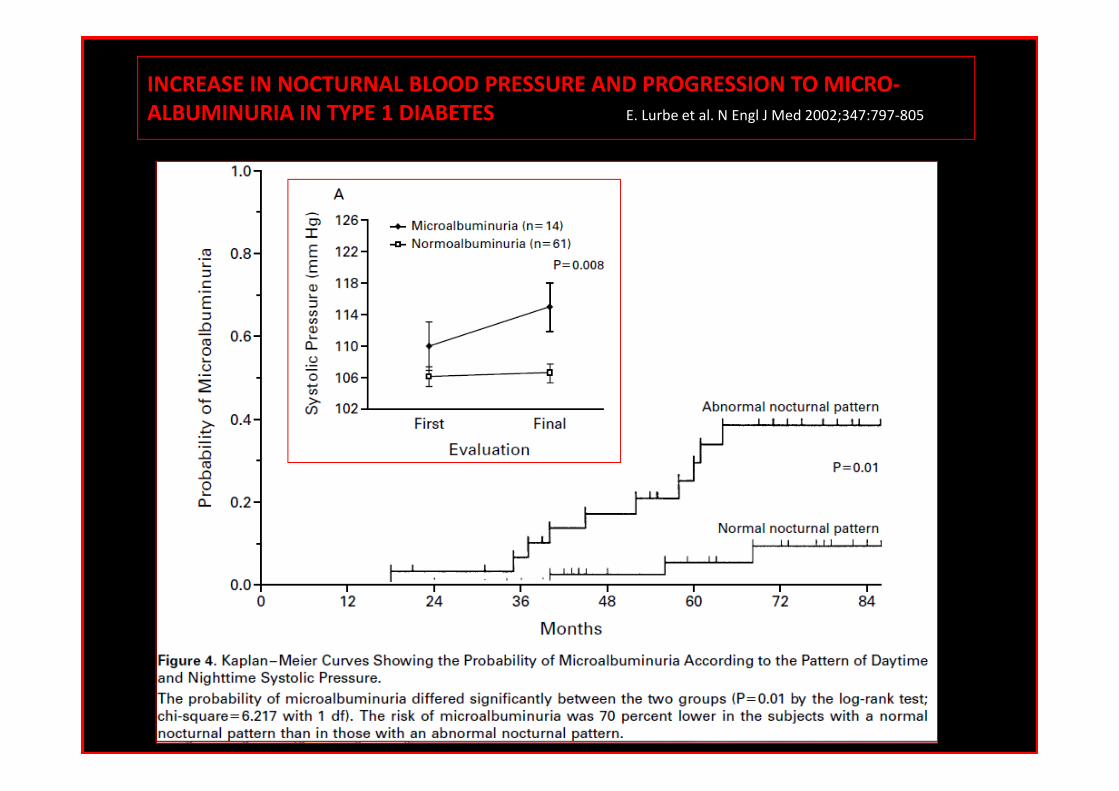
INCREASE IN NOCTURNAL BLOOD PRESSURE AND PROGRESSION TO MICRO-
ALBUMINURIA IN TYPE 1 DIABETES E. Lurbe et al. N Engl J Med 2002;347:797-805.)

Quelle stratégie devant uneHTA – Proteinurie ?Associer un diurétique vs Amlodipine :
diurétique > Amlodipine sur l’excretion urinaire d’album ine
� MRC non diabétique, protéinurie >1g/j, lisinopril 40 mg/j
� Restriction sodée + BSRA >> BSRA + BSRA
Slagman M. BMJ 2011
IEC
PuPAS
IEC
+
A
R
A
2IEC
IEC
+
ARA
2
IEC IEC
+
A
R
A
2
IEC IEC
+
ARA2

Hypertension Treatment: Compelling indications
2013 ESH Guidelines2013

Valsartan in Combination with ACEIis more effective in Reducing Proteinuria
†SBP/DBP >140/90 mmHg, proteinuria >1.5 g/day while on therapy with an ACEi alone or in combination with other antihypertensive drugs for at least 3 months, creatinine clearance values >30 mL/min; *p<0.05 vs. benazepril group; Therapy doses are per daily doses; UPER=Urinary protein excretion rateSegura et al. J Renin Angiotensin Aldosterone Syst 2003;4:43-47.
Results from a 6-month study in 36 patients with primary renal disease,†
assessing the change in proteinuria
Mea
n re
duct
ion
in U
PE
R(g
/day
)
-1.0
-2.0
Combination(n=12)
0
Benazepril 10-20 mg(n=12)
Valsartan 80-160 mg(n=12)
-0.5
-1.2
-2.5*-2.5
-0.5
-1.5

1- Controler l’HyperTension Artérielle (IEC, ARA2)<130/80mmHgSauf si pathologie coronarienne 130<PAS<140mmHg
2- Réduire la Proteinurie (IEC,ARA2)Microalbuminurie <30mg/gcreatinine (<30mg/24h) chez le T1DMRegression ou non-progression de la Microalbuminurie chez le T2DM et/ou HTAProtéinurie <0,5g/24h
3- Adapter le régimeProtéines: environs 0,8g/kg/jSel 3à 5 g/j
4- Traiter le diabète (Adapter les antidiabétiques selon le DFG)HbA1C<7%
5- corriger la dyslipidémie (Statine)LDL Ct < 1g/l (2,5mmo/l)
6- Corriger l’anémie (EPO)Hb: 11-13g/dl
7- Prescrire un antiagrégant plaquettaire8- Arrêter le tabac9- Favoriser l’exercice physique10- Eviter les médicaments/produits néphrotoxiques
NEPHROPATHIE DIABETIQUENouveautés en 2015?
NPD
Perspectives!!!!
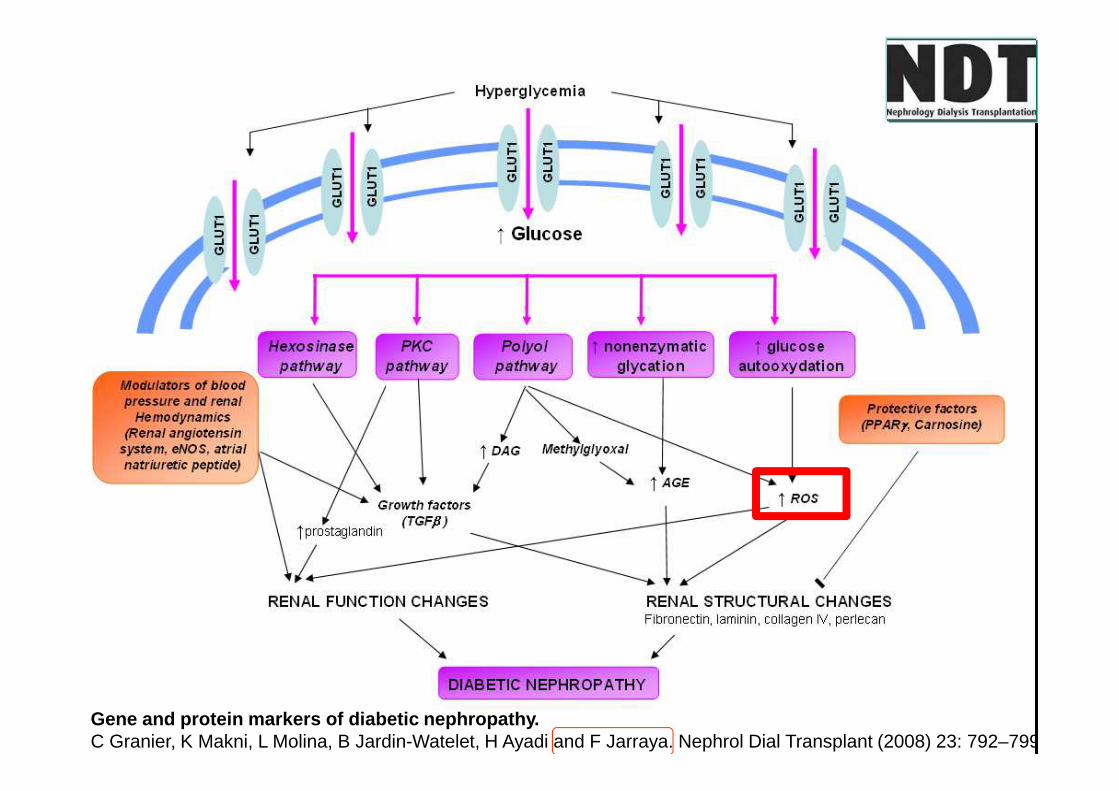
Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
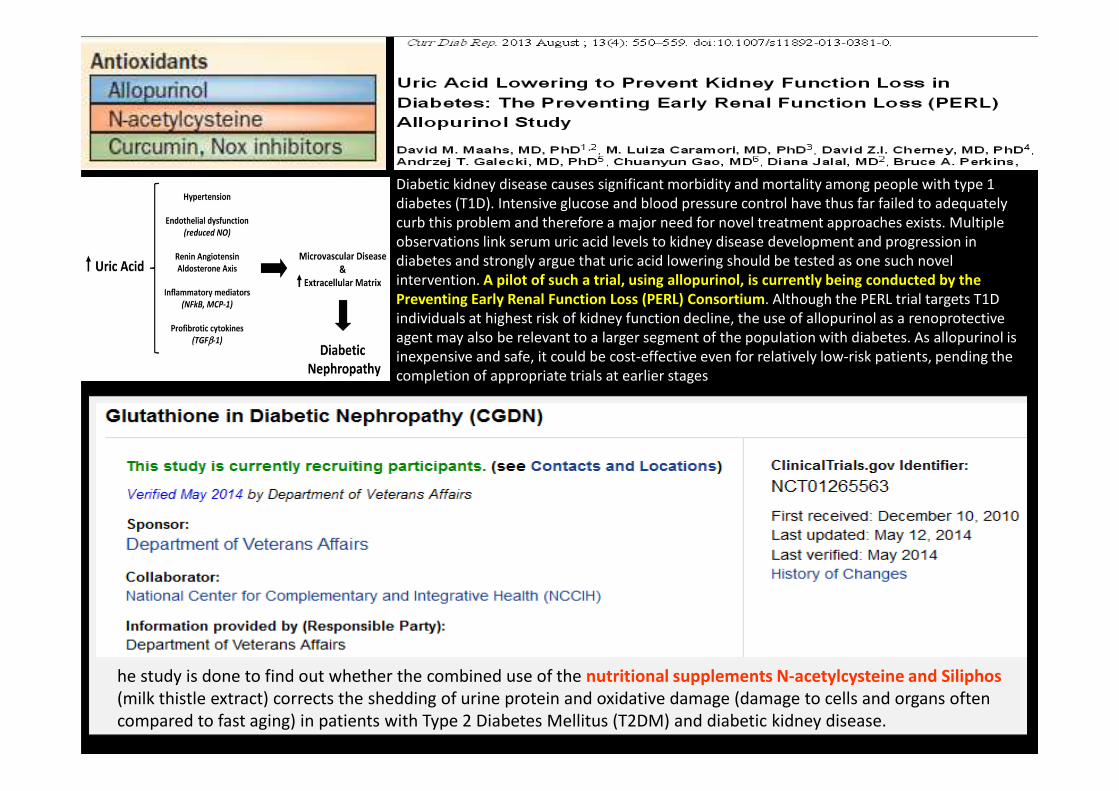
Diabetic kidney disease causes significant morbidity and mortality among people with type 1
diabetes (T1D). Intensive glucose and blood pressure control have thus far failed to adequately
curb this problem and therefore a major need for novel treatment approaches exists. Multiple
observations link serum uric acid levels to kidney disease development and progression in
diabetes and strongly argue that uric acid lowering should be tested as one such novel
intervention. A pilot of such a trial, using allopurinol, is currently being conducted by the
Preventing Early Renal Function Loss (PERL) Consortium. Although the PERL trial targets T1D
individuals at highest risk of kidney function decline, the use of allopurinol as a renoprotective
agent may also be relevant to a larger segment of the population with diabetes. As allopurinol is
inexpensive and safe, it could be cost-effective even for relatively low-risk patients, pending the
completion of appropriate trials at earlier stages
he study is done to find out whether the combined use of the nutritional supplements N-acetylcysteine and Siliphos
(milk thistle extract) corrects the shedding of urine protein and oxidative damage (damage to cells and organs often
compared to fast aging) in patients with Type 2 Diabetes Mellitus (T2DM) and diabetic kidney disease.

Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
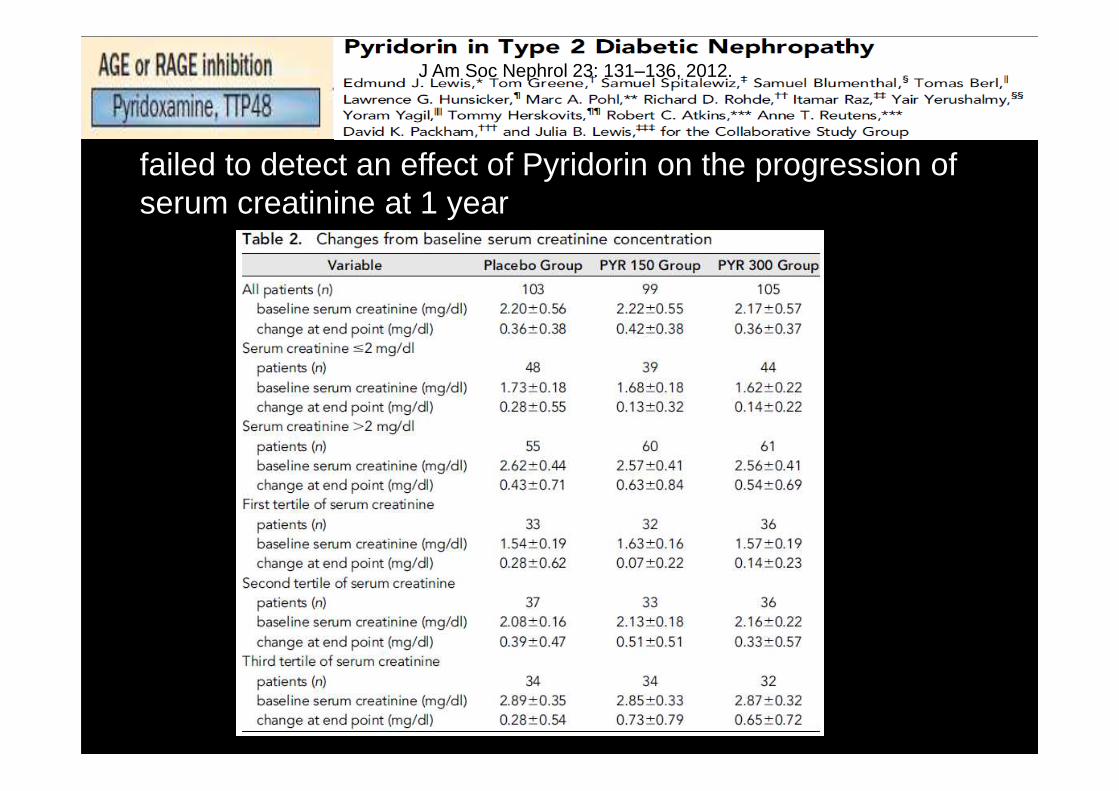
failed to detect an effect of Pyridorin on the progression of serum creatinine at 1 year
J Am Soc Nephrol 23: 131–136, 2012.

Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
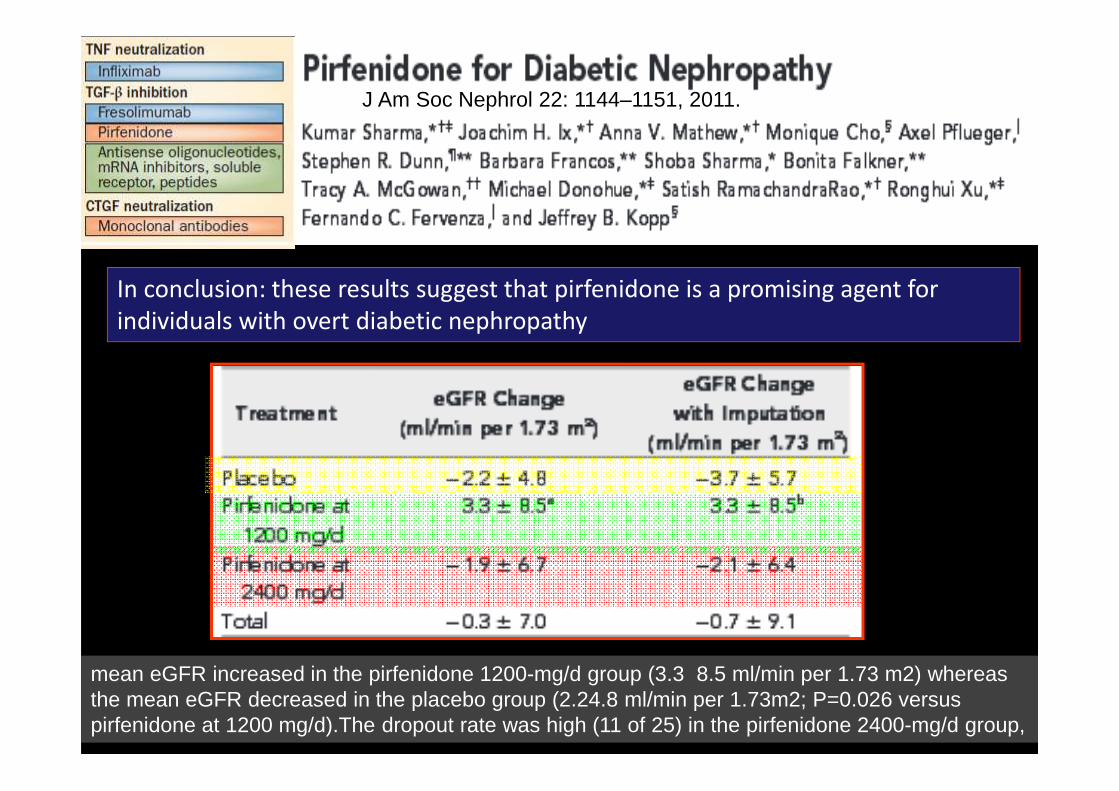
J Am Soc Nephrol22: 1144–1151, 2011In conclusion: these results suggest that pirfenidone is a promising agent for
individuals with overt diabetic nephropathy
mean eGFR increased in the pirfenidone 1200-mg/d group (3.3 8.5 ml/min per 1.73 m2) whereas the mean eGFR decreased in the placebo group (2.24.8 ml/min per 1.73m2; P=0.026 versus pirfenidone at 1200 mg/d).The dropout rate was high (11 of 25) in the pirfenidone 2400-mg/d group,
J Am Soc Nephrol 22: 1144–1151, 2011.
Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
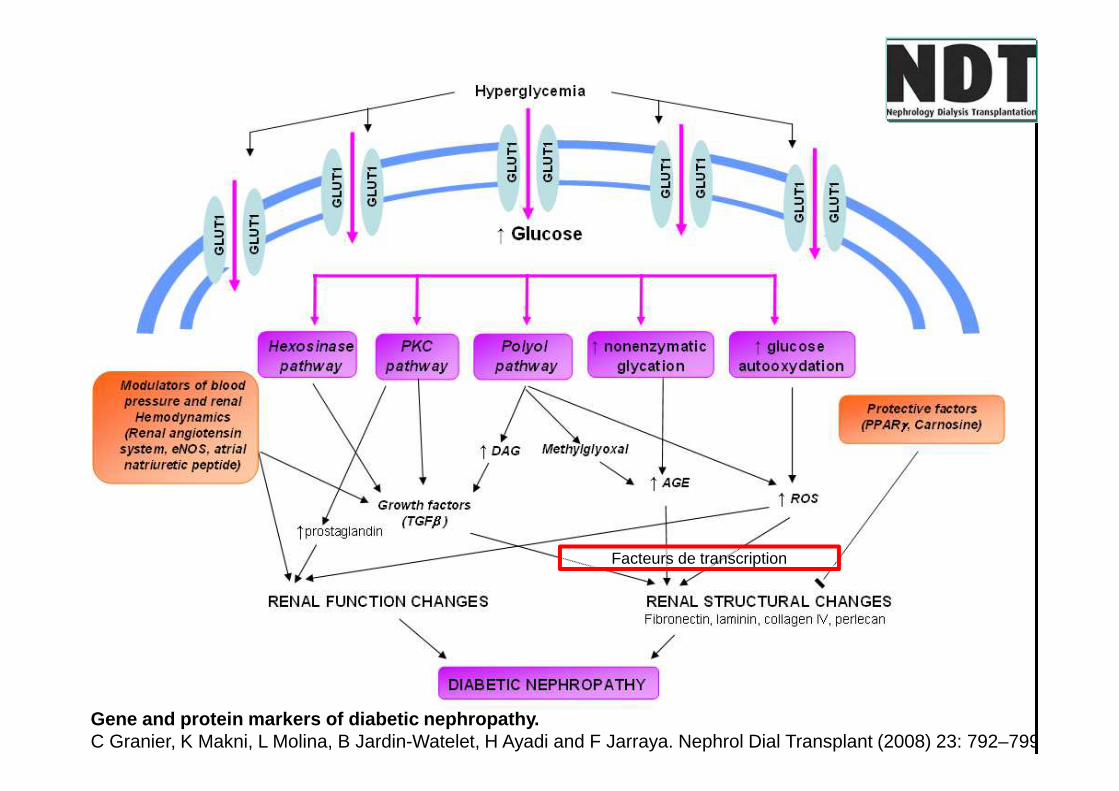
Facteurs de transcription

Facteurs de transcription
BEACON Trial
N Engl J Med 2013;369:2492-503.
Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
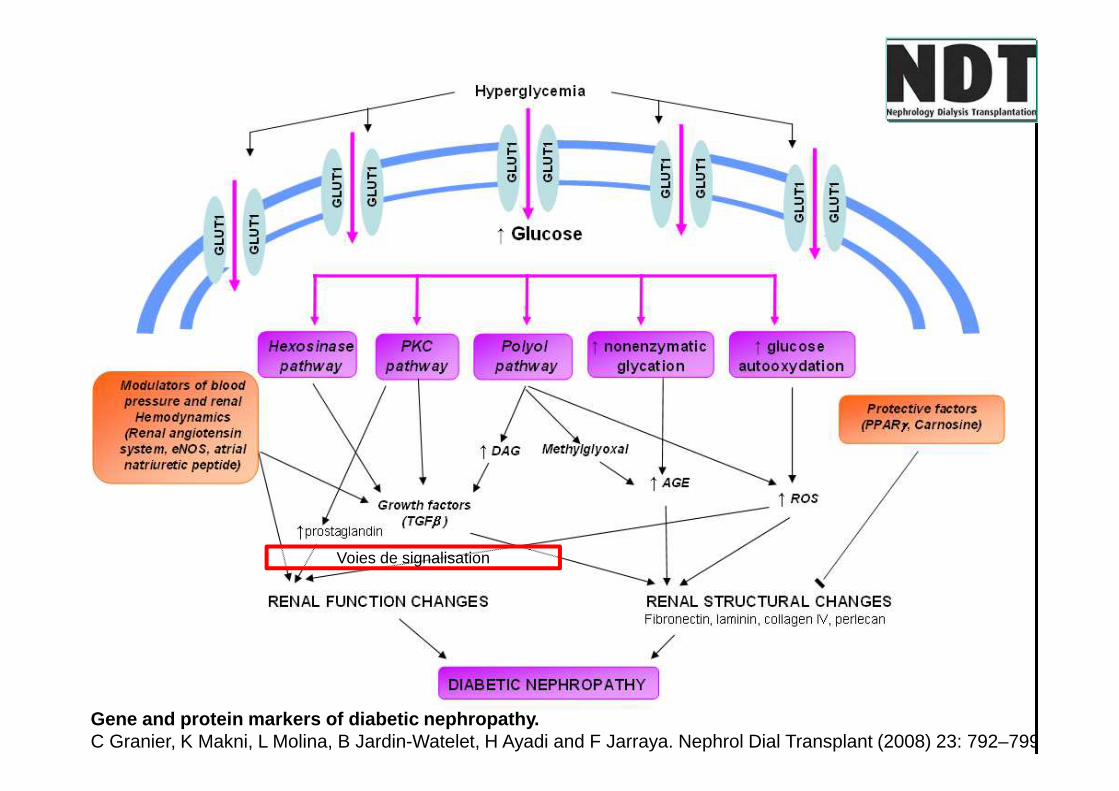
Voies de signalisation

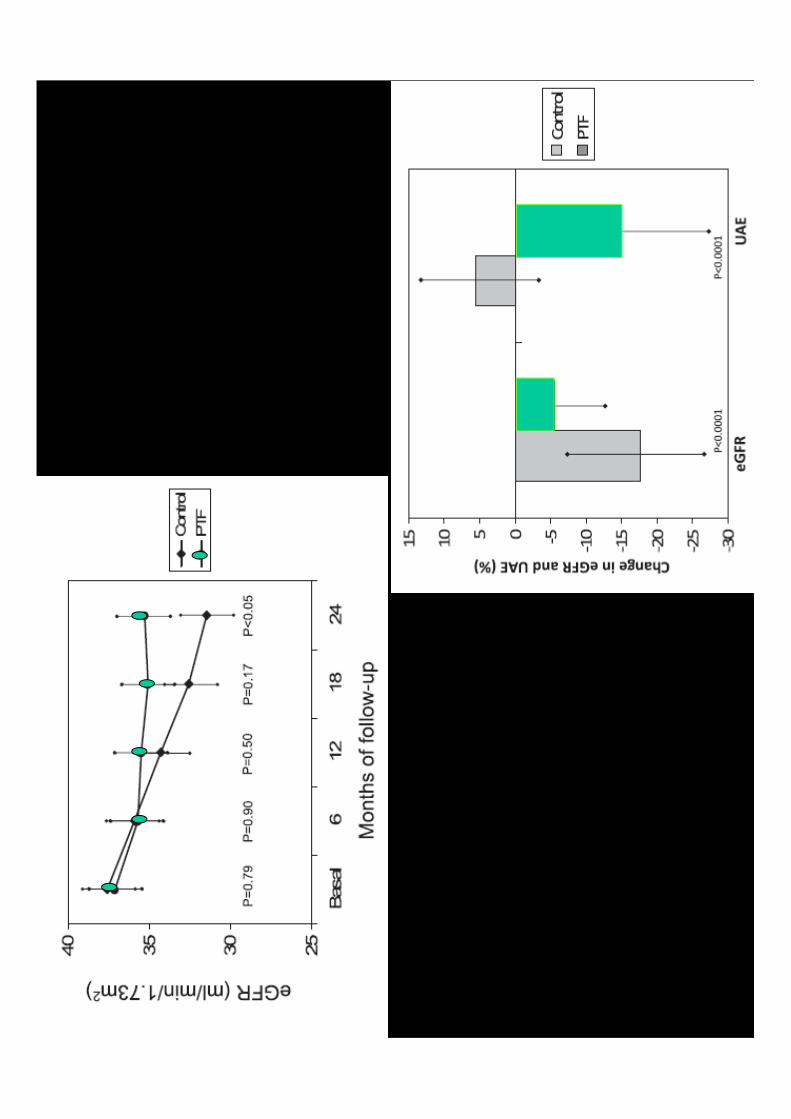
Pentoxifylline for renoprotection in Diabetic
Nephropathy: the PREDIAN study. Rationale and
basal results
Juan F. Navarro-González, et al. Journal of Diabetes
and its Complications, 2011;25:314-319
Conclusions :The PREDIAN study will provide evidence on the renoprotective benefit of PTF in addition to interventions of proven efficacy (RAS blockade) in DN.
Activation des voies signalisation

Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799

ASCEND Study. Avosentan for overt diabetic nephropathy. Mann, J. F. et al. J. Am. Soc. Nephrol. 21, 527–535 (2010).
X2creat, IRCT, décèsN= 1392
the median
reduction
(%) in ACR
Av.44.3%,
Av. 49.3,
Pc. 9.7%
Survie

Gene and protein markers of diabetic nephropathy. C Granier, K Makni, L Molina, B Jardin-Watelet, H Ayadi and F Jarraya. Nephrol Dial Transplant (2008) 23: 792–799
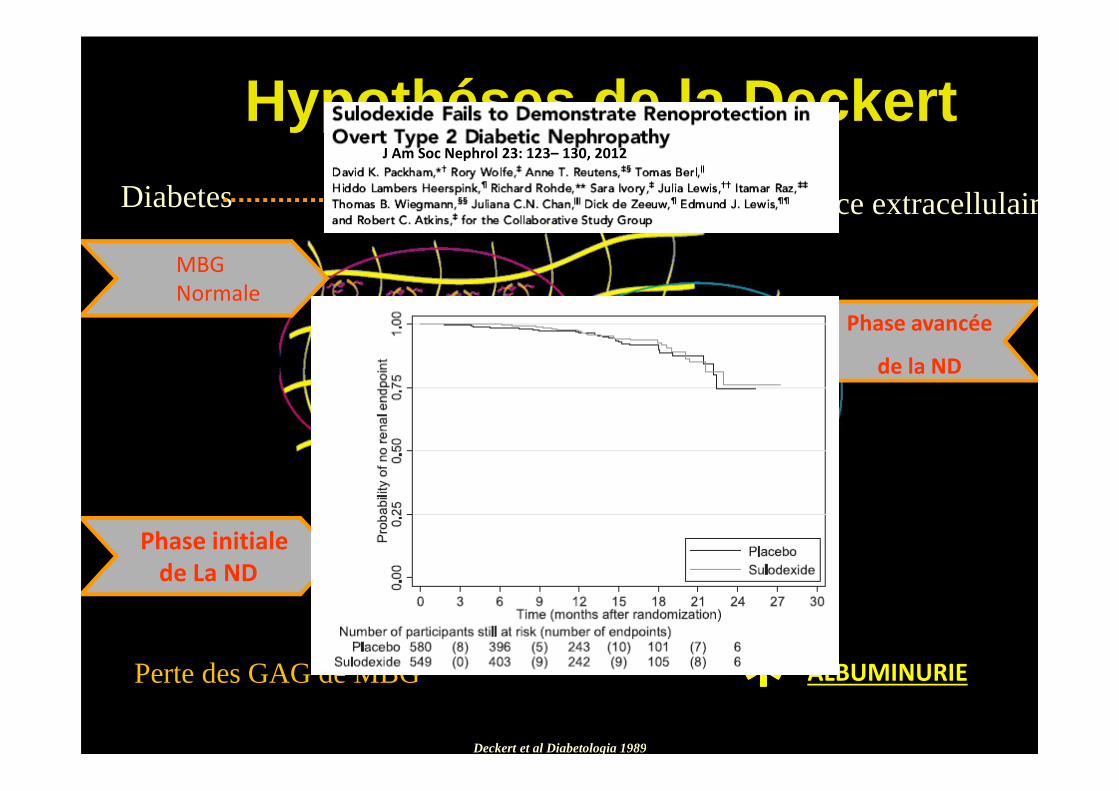
Diabetes perte de la charge negative de la matice extracellulaire
MBG
Normale
Perte des GAG de MBG ALBUMINURIE����
Phase initiale
de La ND
Phase avancée
de la ND
Deckert et al Diabetologia 1989
Hypothéses de la DeckertJ Am Soc Nephrol 23: 123– 130, 2012


Faut pas réver!!!
Nat. Rev. Nephrol. 10, 325–346 (2014)


1- Controler l’HyperTension Artérielle (IEC, ARA2)<130/80mmHgSauf si pathologie coronarienne 130<PAS<140mmHg
2- Réduire la Proteinurie (IEC,ARA2)Microalbuminurie <30mg/gcreatinine (<30mg/24h) chez le T1DMRegression ou non-progression de la Microalbuminurie chez le T2DM et/ou HTAProtéinurie <0,5g/24h
3- Adapter le régimeProtéines: environs 0,8g/kg/jSel 3à 5 g/j
4- Traiter le diabète (Adapter les antidiabétiques selon le DFG)HbA1C<7%
5- corriger la dyslipidémie (Statine)LDL Ct < 1g/l (2,5mmo/l)
6- Corriger l’anémie (EPO)Hb: 11-13g/dl
7- Prescrire un antiagrégant plaquettaire8- Arrêter le tabac9- Favoriser l’exercice physique10- Eviter les médicaments/produits néphrotoxiques
Take Home Messages:Les 10 Commandements du traitement néphroprotecteur
heinn!!!!

Ruggenenti, P. et al. Clin J Am Soc Nephrol 2007;2:146-150
Annual ESRD incidence in the United States from 1980 to 2004 according to the Annual ESRD incidence in the United States from 1980 to 2004 according to the Annual ESRD incidence in the United States from 1980 to 2004 according to the Annual ESRD incidence in the United States from 1980 to 2004 according to the publication of randomized clinical trials providing the evidence of a protective publication of randomized clinical trials providing the evidence of a protective publication of randomized clinical trials providing the evidence of a protective publication of randomized clinical trials providing the evidence of a protective
effect of RAS inhibitor therapy against the development of ESRDeffect of RAS inhibitor therapy against the development of ESRDeffect of RAS inhibitor therapy against the development of ESRDeffect of RAS inhibitor therapy against the development of ESRD
Lewis REIN RENAAL-IRMA2- IDNT-

Merci pour votre attention
Agissons ensemble pour préserver les
néphrons de diabétiques