M2RToxMed octobre 2013 Paris · ECOGENETIQUE (Pharmaco/Toxicogénétique) Principes, applications...
87
ECOGENETIQUE (Pharmaco/Toxicogénétique) Principes, applications et perspectives Vers une Médecine Prédictive du Risque Chimique Pr Franck Broly, MD, PhD Unité de Génopathies, Pharmacogénétique et Toxicogénétique, Centre de Biologie et Pathologie, CHRU Lille. EA4483: « Impact de l’environnement chimique sur la santé » Pôle Recherche, Faculté de Médecine, Lille.
Transcript of M2RToxMed octobre 2013 Paris · ECOGENETIQUE (Pharmaco/Toxicogénétique) Principes, applications...

ECOGENETIQUE (Pharmaco/Toxicogénétique)Principes, applications et perspectives
Vers une Médecine Prédictive du Risque Chimique
Pr Franck Broly, MD, PhDUnité de Génopathies, Pharmacogénétique et Toxicogénétique, Centre de Biologie et Pathologie, CHRU Lille.
EA4483: « Impact de l’environnement chimique sur la santé »Pôle Recherche, Faculté de Médecine, Lille.
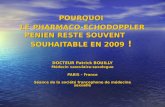
ECOGENETIQUE
COMPRENDRE,PREVOIR et PREVENIR
Les effets de l’environnement chimique
Étude de l’influence de l’hérédité sur notre réponse aux composés chimiques de l’environnement
qui nous sont étrangers (xénobiotiques)
1 Identification des variations de réponse aux xénobiotiquesd'origine génétique
2 Compréhension de leur mécanisme moléculaire
3 Évaluation de leur importance clinique
4 Développement de méthodes d'identification des individusà risque Avant exposition ++++

Days after transplantation
0
300
200
100
Peripheral bloodleucocyte(106/ml)
Azathioprinedose
(mg/day)
0 10 20 30 40 50 60 70 80 90 100
Pneumoniaeand septicemia
Death
0
2
4
6
8
10
12
14
16
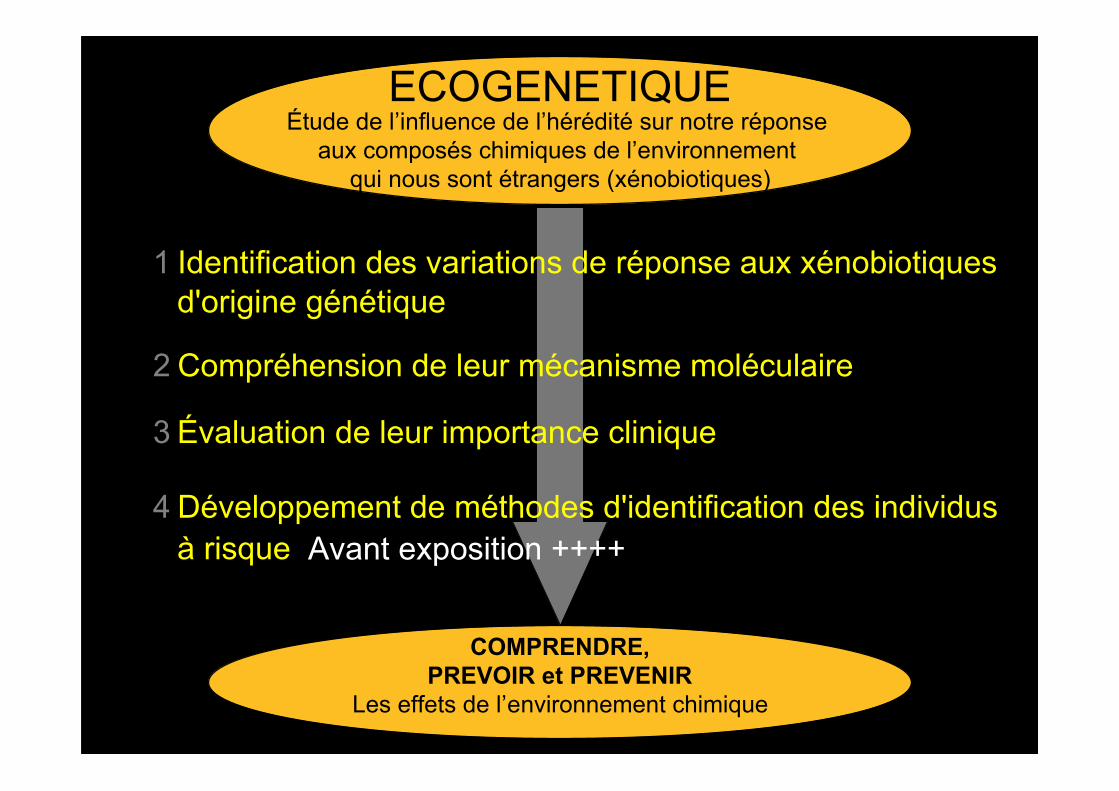
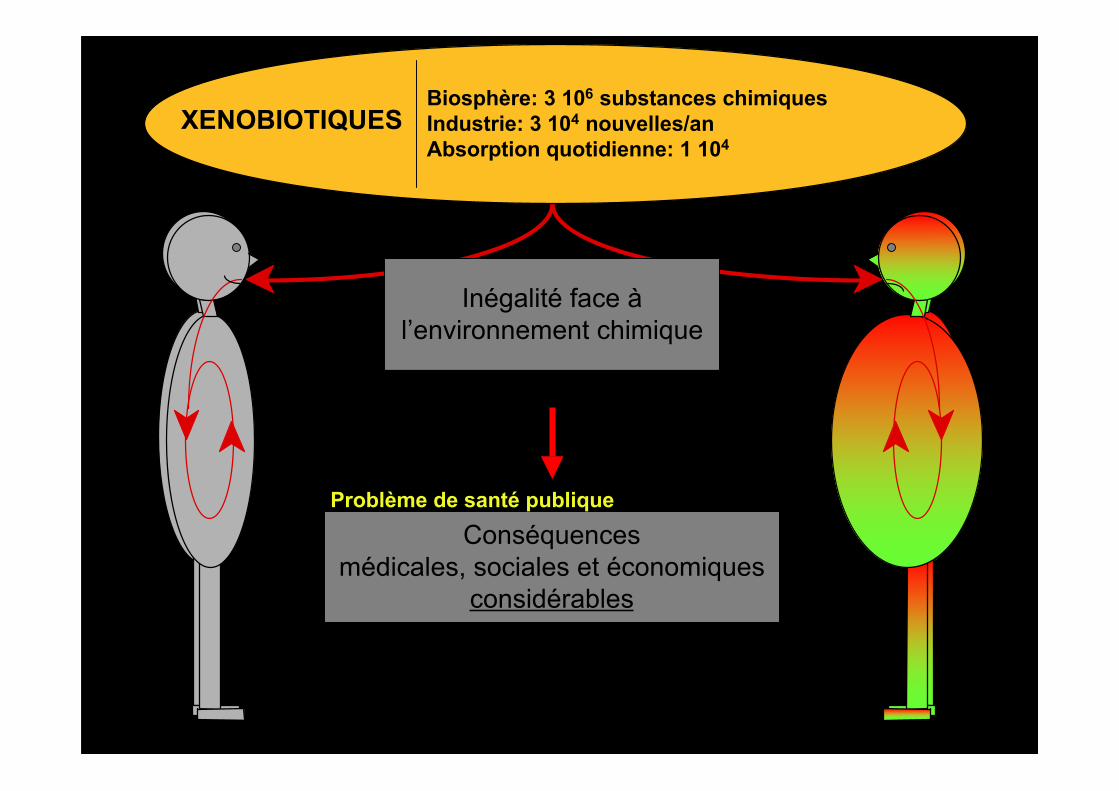
XENOBIOTIQUESBiosphère: 3 106 substances chimiquesIndustrie: 3 104 nouvelles/anAbsorption quotidienne: 1 104
• Multitude• Naturels ou artificiels• Sources multiples et variées
• Additifs alimentaires• Combustibles industriels ou domestiques• Cosmétiques• Pesticides• Médicaments : 6 103
• Etc…
• 1930 à 2004 : 1M ⇒ 400 Millions de tonnes/an• Agents chimiques cancérogènes, mutagènes ou
toxiques pour la reproduction consommés enFrance: 4.5 Millions de tonnes/an
• Modification récente considérable (Ère industrielle)
• Propriétés et risques sanitaires ?
• 3 000 / 100 000 substances recensées dans l’UE
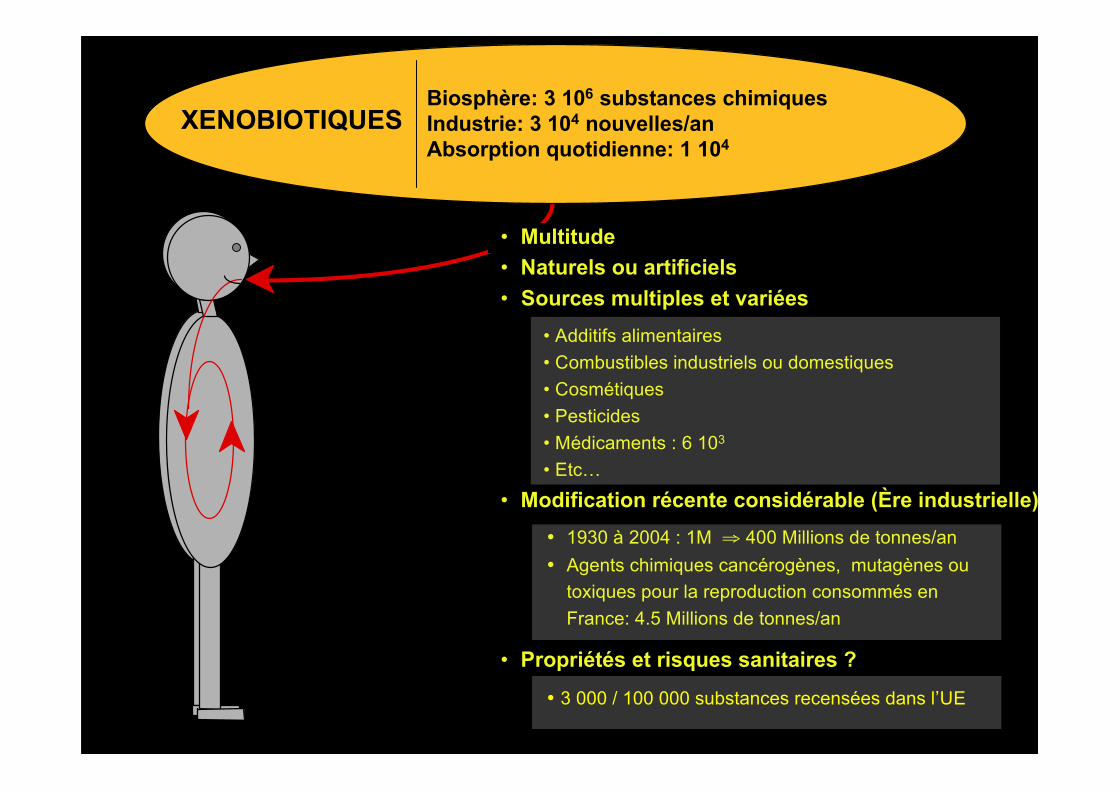
Inégalité face àl’environnement chimique
XENOBIOTIQUESBiosphère: 3 106 substances chimiquesIndustrie: 3 104 nouvelles/anAbsorption quotidienne: 1 104

Inégalité face àl’environnement chimique
Conséquencesmédicales, sociales et économiques
considérables
Problème de santé publique
XENOBIOTIQUESBiosphère: 3 106 substances chimiquesIndustrie: 3 104 nouvelles/anAbsorption quotidienne: 1 104

Overall incidence of ADRs: 6.70 %Incidence of fatal ADRs: 0.32 %
Incidence of Adverse Drug Reactions (ADRs) in Hospitalized Patients
1994 • 2 216 000 hospitalized patients for "serious ADRs"• 106 000 patients with fatal ADRs
ADRs
Leading cause of death in the US
ADRs
Economic burden resultingfrom drug-related morbidity
and mortality136.8 billion $US annually
Resistance to therapy
• 35 % of people do not respond to beta blockers• 50 % do not respond to tricyclic antidepressants• 30 % of schizophrenics do not respond to treatment by antipsychotics••
50-60% do not respond to 5-FU combined with irinotecan and oxaloplatine for colorectal K
...
1 Heart disease 743 4602 Cancer 529 9043 Stroke 150 1084 Pulmonary disease 101 0775 Accidents 90 5236 Pneumonia 75 7197 Diabetes 53 894
The response rates for gefinitib or erolitinib in non-small cell lung cancer patients is 10-20%
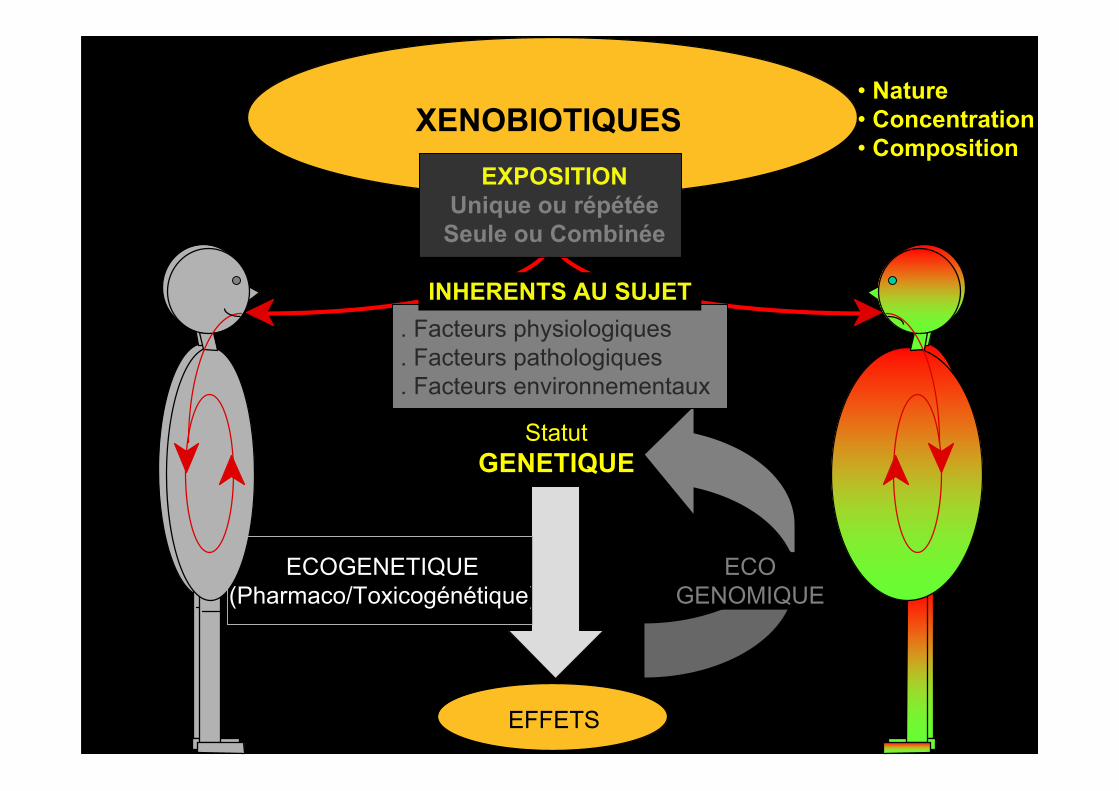
XENOBIOTIQUES
EFFETS
StatutGENETIQUE
ECOGENETIQUE(Pharmaco/Toxicogénétique)
ECOGENOMIQUE
. Facteurs physiologiques
. Facteurs pathologiques
. Facteurs environnementaux
• Nature• Concentration• Composition
EXPOSITIONUnique ou répétée
Seule ou Combinée
INHERENTS AU SUJET

Xénobiotiques
Absorption
Distribution
Métabolisme
Excrétion
XENOBIOTIQUES
EFFETS
Cinétique
Dynamie
Nature
Intensité
Durée
PROTEINES
GENES
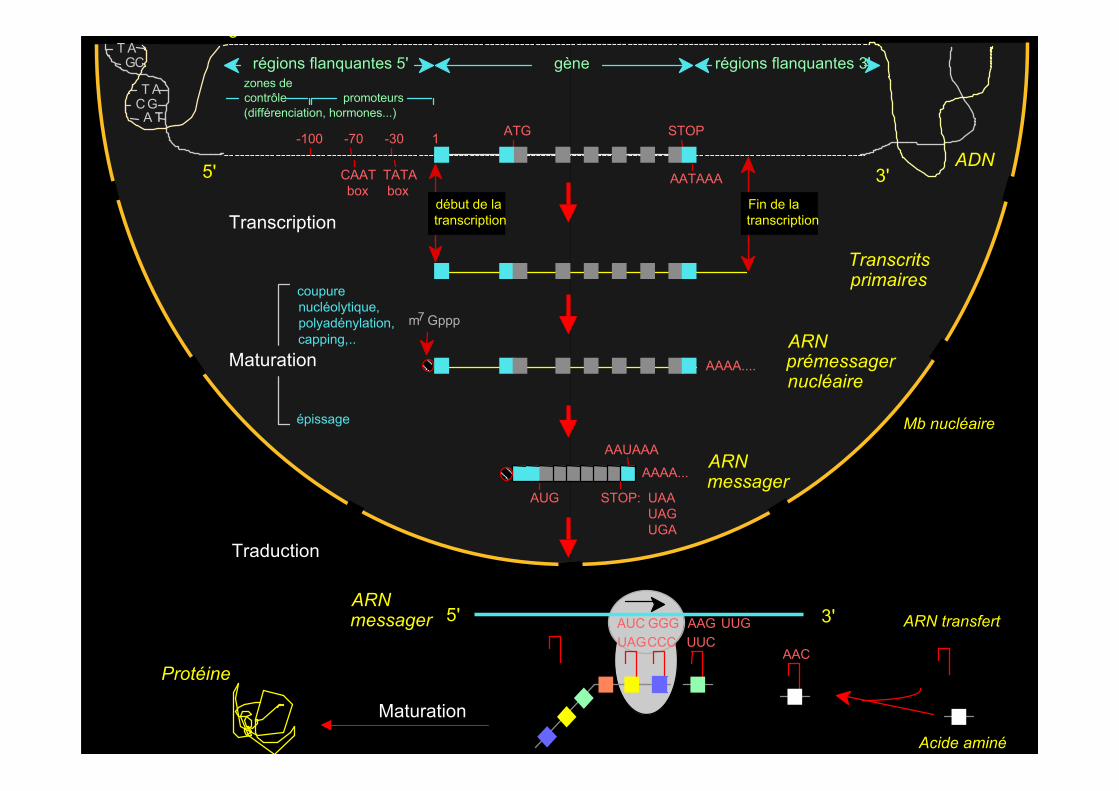
ATG STOP
AATAAA
1-30-70-100
TATAbox
CAATbox
gènerégions flanquantes 5' régions flanquantes 3'
Transcription
Traduction
Maturation
zones decontrôle(différenciation, hormones...)
promoteurs
AAAA...
AUG STOP: UAAUAGUGA
début de latranscription
Fin de latranscription
m7 Gppp
AAAA....
AAUAAA
ARNprémessagernucléaire
Transcritsprimaires
ARNmessager
coupurenucléolytique,polyadénylation,capping,..
épissage
5' 3'
ARN transfert
Acide aminé
ARNmessager 5' 3'
Mb nucléaire
Maturation
Protéine
ADN
AAGUUC
UUG
AAC
AUC GGGUAGCCC
3'
T ACG
A T
GCT A

MICROLESIONS
. Délétion
. Duplication
. Amplification
Recombinaison (crossing-over)
. Fusion de gènes
. Inversion
. Insertions
Mutations ponctuelles
Chromosome A
Chromosome B
(Constitutional) Copy Number Variations (CNV)
MACROLESIONS
Very common phenomenon: 2447 CNV, 660 Mb, 22% of the human genome
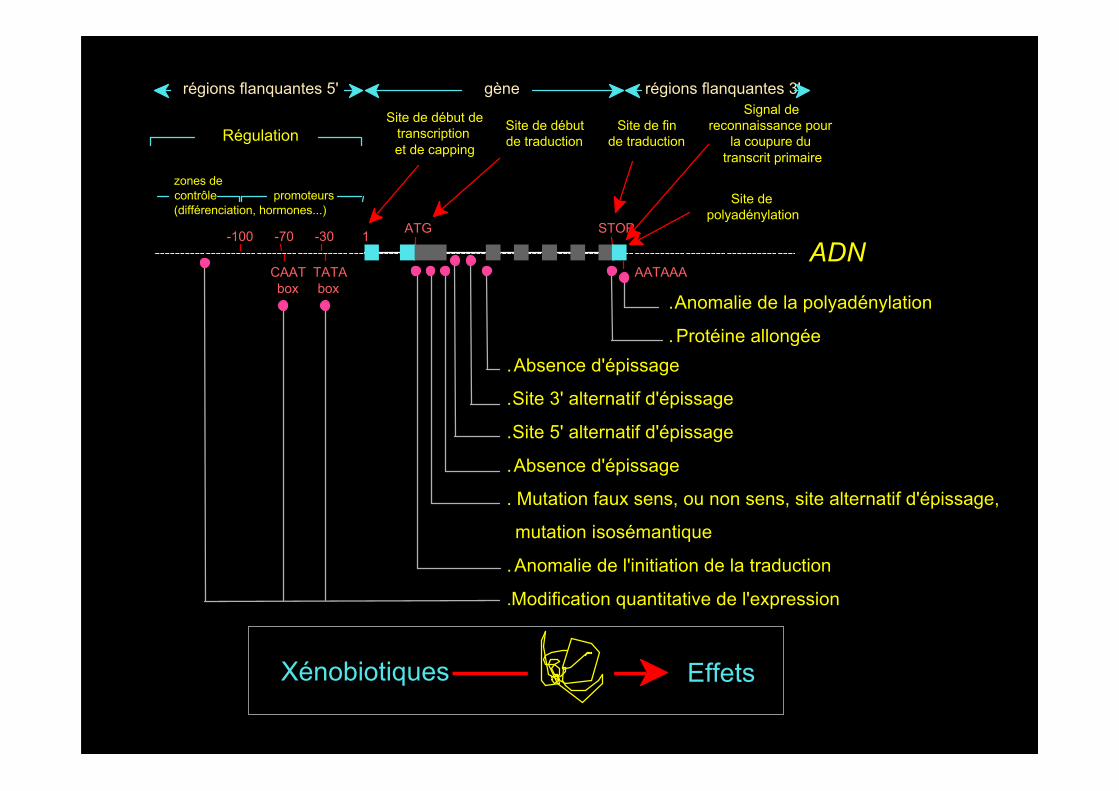
.Absence d'épissage
.Site 3' alternatif d'épissage
.Site 5' alternatif d'épissage
.Absence d'épissage
. Mutation faux sens, ou non sens, site alternatif d'épissage,
mutation isosémantique
.Anomalie de l'initiation de la traduction
.Modification quantitative de l'expression
. Anomalie de la polyadénylation
.Protéine allongée
zones decontrôle(différenciation, hormones...)
ATG STOP
AATAAA
1-30-70-100
TATAbox
CAATbox
gènerégions flanquantes 5' régions flanquantes 3'
promoteurs
ADN
Site de début detranscriptionet de capping
Site de débutde traduction
Signal dereconnaissance pour
la coupure dutranscrit primaire
Site depolyadénylation
RégulationSite de fin
de traduction
Xénobiotiques Effets

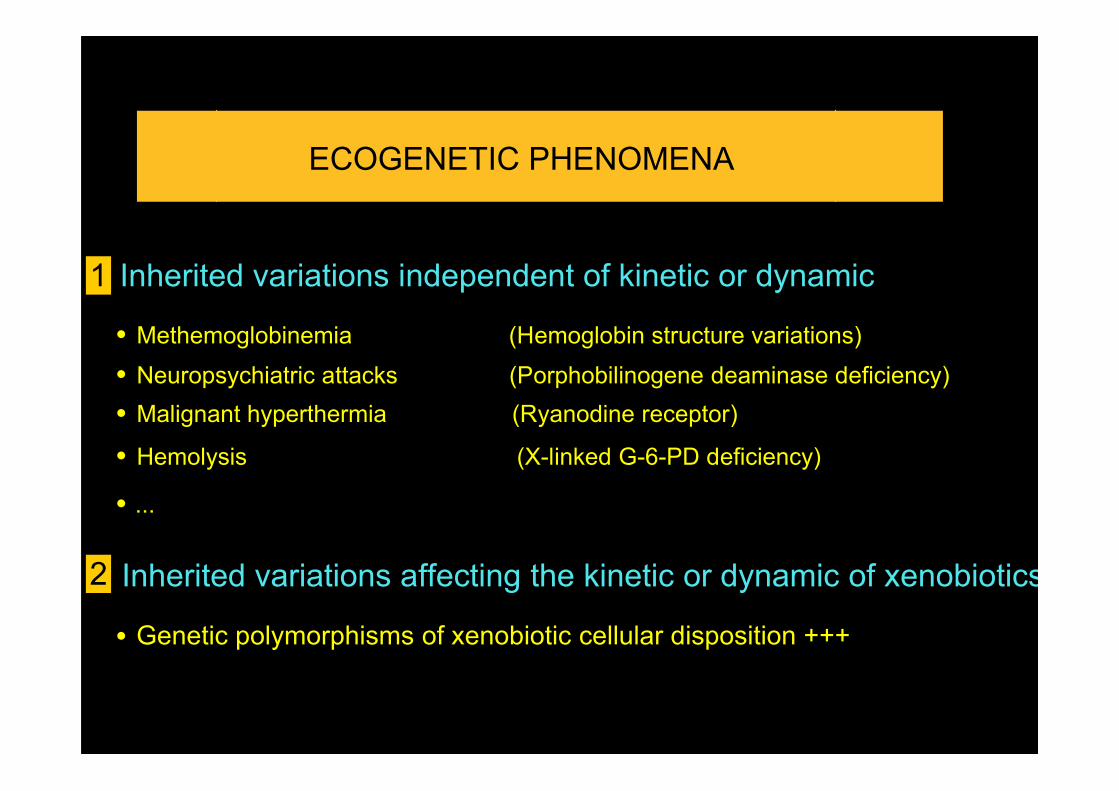
ECOGENETIC PHENOMENA
1 Inherited variations independent of kinetic or dynamic
• Malignant hyperthermia (Ryanodine receptor)
• Hemolysis (X-linked G-6-PD deficiency)
• Neuropsychiatric attacks (Porphobilinogene deaminase deficiency)• Methemoglobinemia (Hemoglobin structure variations)
• ...
Inherited variations affecting the kinetic or dynamic of xenobiotics
• Genetic polymorphism of xenobiotic cellular disposition
2

G6PDH
NADPNADPH
H2O2
H2O
Glutathionperoxydase
• Fèves (vicine et convicine)• Teintures au Henné• Boules de naphtalène• Colorants alimentaires artificiels• Insecticides DDT• Nitrobenzène• Médicaments• …..
Glutathionréductase
Glucose-6-phosphate
Ribulose-5phosphate
2 GSH GSSGO2
peroxydes• Acide pipémidique (pipram®)• Acide nalidixique (négram ®)• Ciprofloxacine (ciflox ®)• Sulfaméthoxazole (bactrim ®)• Dapsone (disulone ®)• Doxorubicine (adriblastine ®)• Flumequine (apurone ®)• …..
AnémieHémolytique
Globule rouge
Glucose-6-PhosphateDéshydrogénase
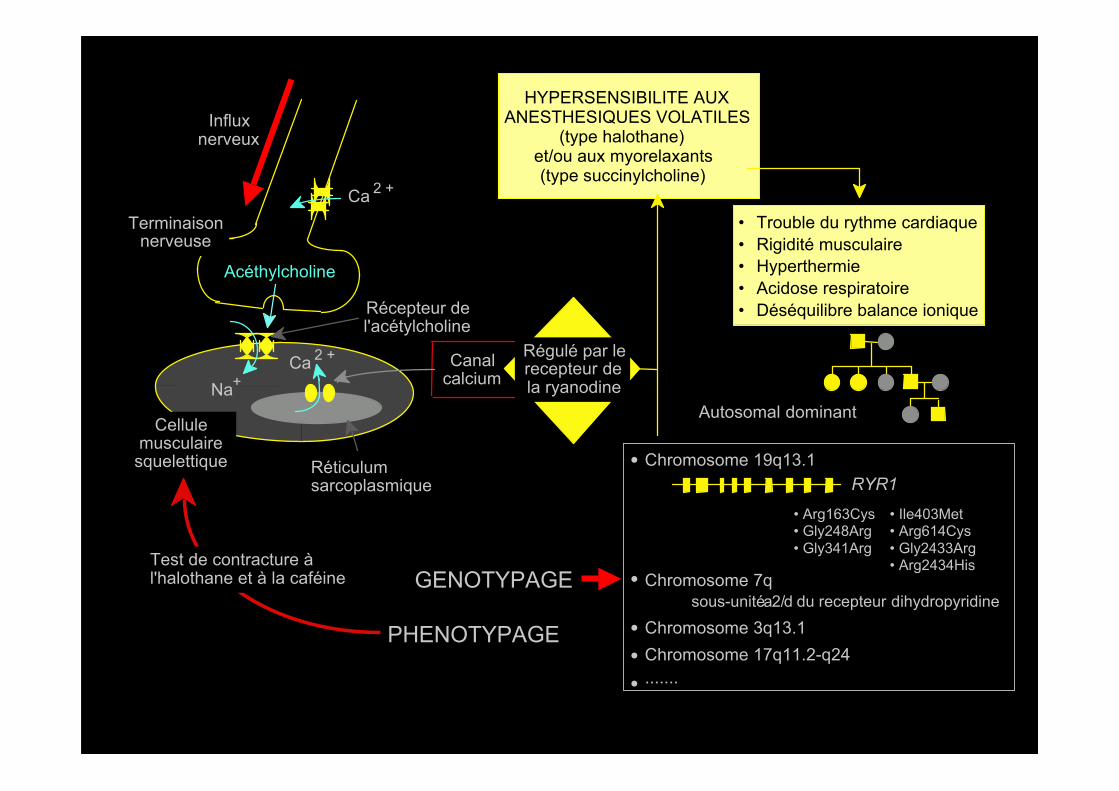
Autosomal dominant
Ca 2 +
Influxnerveux
Acéthylcholine
Na+Ca 2 +
Récepteur del'acétylcholine
Réticulumsarcoplasmique
Cellulemusculairesquelettique
Terminaisonnerveuse
Canalcalcium
Régulé par lerecepteur dela ryanodine
HYPERSENSIBILITE AUXANESTHESIQUES VOLATILES
(type halothane)et/ou aux myorelaxants(type succinylcholine)
• Trouble du rythme cardiaque• Rigidité musculaire• Hyperthermie• Acidose respiratoire• Déséquilibre balance ionique
PHENOTYPAGE
GENOTYPAGE
RYR1
• Arg163Cys• Gly248Arg• Gly341Arg
• Chromosome 19q13.1
Chromosome 17q11.2-q24
• Ile403Met• Arg614Cys• Gly2433Arg• Arg2434His
• Chromosome 7q
•
sous-unité a2/d du recepteur dihydropyridine
Test de contracture àl'halothane et à la caféine
Chromosome 3q13.1•
.......•
ECOGENETIC PHENOMENA
1 Inherited variations independent of kinetic or dynamic
• Malignant hyperthermia (Ryanodine receptor)
• Hemolysis (X-linked G-6-PD deficiency)
• Neuropsychiatric attacks (Porphobilinogene deaminase deficiency)• Methemoglobinemia (Hemoglobin structure variations)
• ...
Inherited variations affecting the kinetic or dynamic of xenobiotics
• Genetic polymorphisms of xenobiotic cellular disposition +++
2

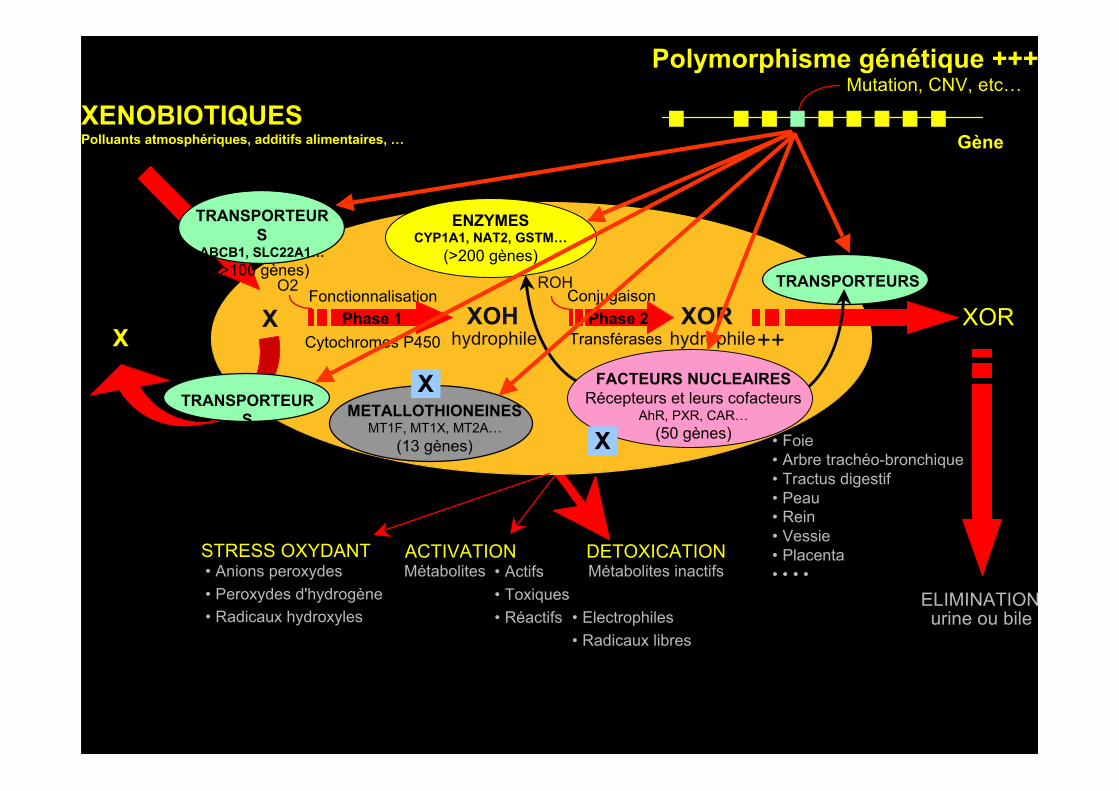
FACTEURS NUCLEAIRESRécepteurs et leurs cofacteurs
AhR, PXR, CAR…(50 gènes)
DETOXICATIONMétabolites • Actifs
• Toxiques • Réactifs
ACTIVATION
ELIMINATIONurine ou bile
XORhydrophile ++
XORX
ENZYMESCYP1A1, NAT2, GSTM…
(>200 gènes)TRANSPORTEURS
TRANSPORTEURS METALLOTHIONEINES
MT1F, MT1X, MT2A…(13 gènes)
TRANSPORTEURS
ABCB1, SLC22A1…(>100 gènes)
Métabolites inactifs
X
X
ConjugaisonXOH
hydrophileX Phase 2
FonctionnalisationPhase 1
• Foie• Arbre trachéo-bronchique• Tractus digestif• Peau• Rein• Vessie• Placenta• • • •
O2 ROH
TransférasesCytochromes P450
• Electrophiles • Radicaux libres
STRESS OXYDANT• Anions peroxydes• Peroxydes d'hydrogène• Radicaux hydroxyles
XENOBIOTIQUESPolluants atmosphériques, additifs alimentaires, …
FACTEURS NUCLEAIRESRécepteurs et leurs cofacteurs
AhR, PXR, CAR…(50 gènes)
DETOXICATIONMétabolites • Actifs
• Toxiques • Réactifs
ACTIVATION
ELIMINATIONurine ou bile
XORhydrophile ++
XORX
ENZYMESCYP1A1, NAT2, GSTM…
(>200 gènes)TRANSPORTEURS
TRANSPORTEURS METALLOTHIONEINES
MT1F, MT1X, MT2A…(13 gènes)
TRANSPORTEURS
ABCB1, SLC22A1…(>100 gènes)
Métabolites inactifs
X
X
ConjugaisonXOH
hydrophileX Phase 2
FonctionnalisationPhase 1
• Foie• Arbre trachéo-bronchique• Tractus digestif• Peau• Rein• Vessie• Placenta• • • •
O2 ROH
TransférasesCytochromes P450
• Electrophiles • Radicaux libres
STRESS OXYDANT• Anions peroxydes• Peroxydes d'hydrogène• Radicaux hydroxyles
Gène
Mutation, CNV, etc…Polymorphisme génétique +++
XENOBIOTIQUESPolluants atmosphériques, additifs alimentaires, …
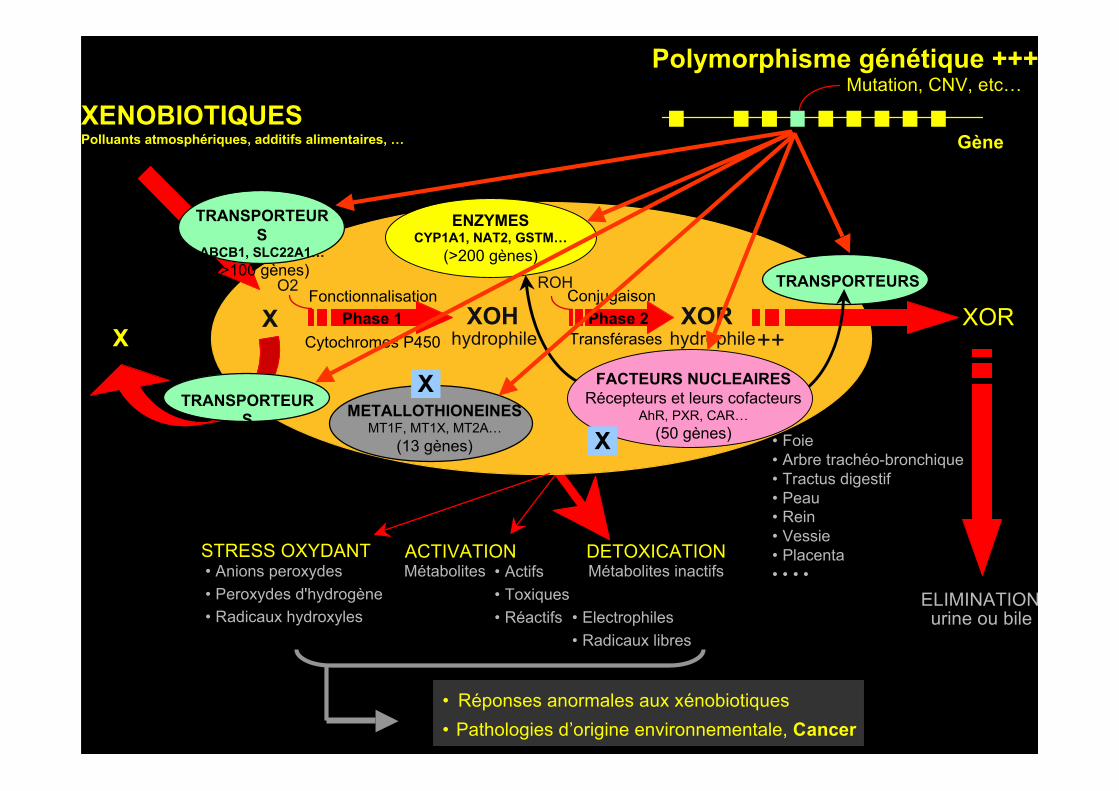
FACTEURS NUCLEAIRESRécepteurs et leurs cofacteurs
AhR, PXR, CAR…(50 gènes)
DETOXICATIONMétabolites • Actifs
• Toxiques • Réactifs
ACTIVATION
ELIMINATIONurine ou bile
XORhydrophile ++
XORX
• Réponses anormales aux xénobiotiques• Pathologies d’origine environnementale, Cancer
ENZYMESCYP1A1, NAT2, GSTM…
(>200 gènes)TRANSPORTEURS
TRANSPORTEURS METALLOTHIONEINES
MT1F, MT1X, MT2A…(13 gènes)
TRANSPORTEURS
ABCB1, SLC22A1…(>100 gènes)
Métabolites inactifs
X
X
ConjugaisonXOH
hydrophileX Phase 2
FonctionnalisationPhase 1
• Foie• Arbre trachéo-bronchique• Tractus digestif• Peau• Rein• Vessie• Placenta• • • •
O2 ROH
TransférasesCytochromes P450
• Electrophiles • Radicaux libres
STRESS OXYDANT• Anions peroxydes• Peroxydes d'hydrogène• Radicaux hydroxyles
Gène
Mutation, CNV, etc…Polymorphisme génétique +++
XENOBIOTIQUESPolluants atmosphériques, additifs alimentaires, …
ECOGENETIQUEApplication: aide à la thérapeutique
PHARMACOGENETIQUE

Lille
Grenoble
Nimes
Montpellier
Paris
Bordeaux
Nancy
Tours
Limoges
CHU Lille, Institut de Biochimie et Biologie Moléculaire ,UF Génopathies et Pharmacogénétique, UF Neurobiologie
CHU de Tours,Laboratoire
d’Immunologie
Hôpital Michallon,Dpt de Biologie et
Pathologie de la Cellule,UF de Pharmacologie
CHU Caremeau,Service deBiochimie
Hôpital Arnaud deVilleneuve, Lab de Biologie
Cellulaire et Hormonale
CHU Pellegrin, Servicede Biochimie
Lyon
Hôpital Herriot, Fédération deBiologie, UF de
Pharmacologie Spécialisée
CHU Dupuytren, Service dePharmacologie et Toxicologie
CHU Nancy Brabois,Service de Biochimie
Hôpital EGP, Service de BiochimieHôpital Bicêtre, Lab de Génétique Moléculaire et PharmacogénétiqueHôpital Robert Debré, Lab de Pharmacologie PédiatriqueHôpital Henri Mondor, Lab de Génétique Moléculaire
AngersCRLCC Paul Papin,
Lab d’Oncopharmacologie etPharmacogénétique
Pharmacogénétique Constitutionnelle
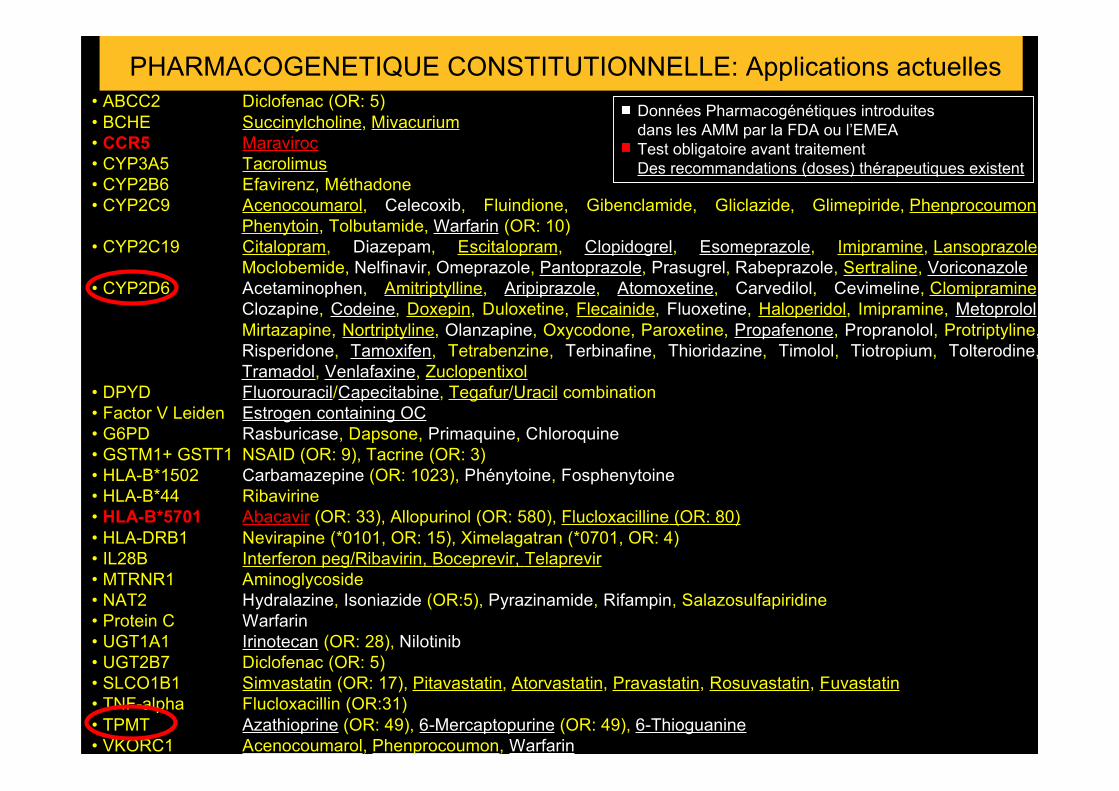
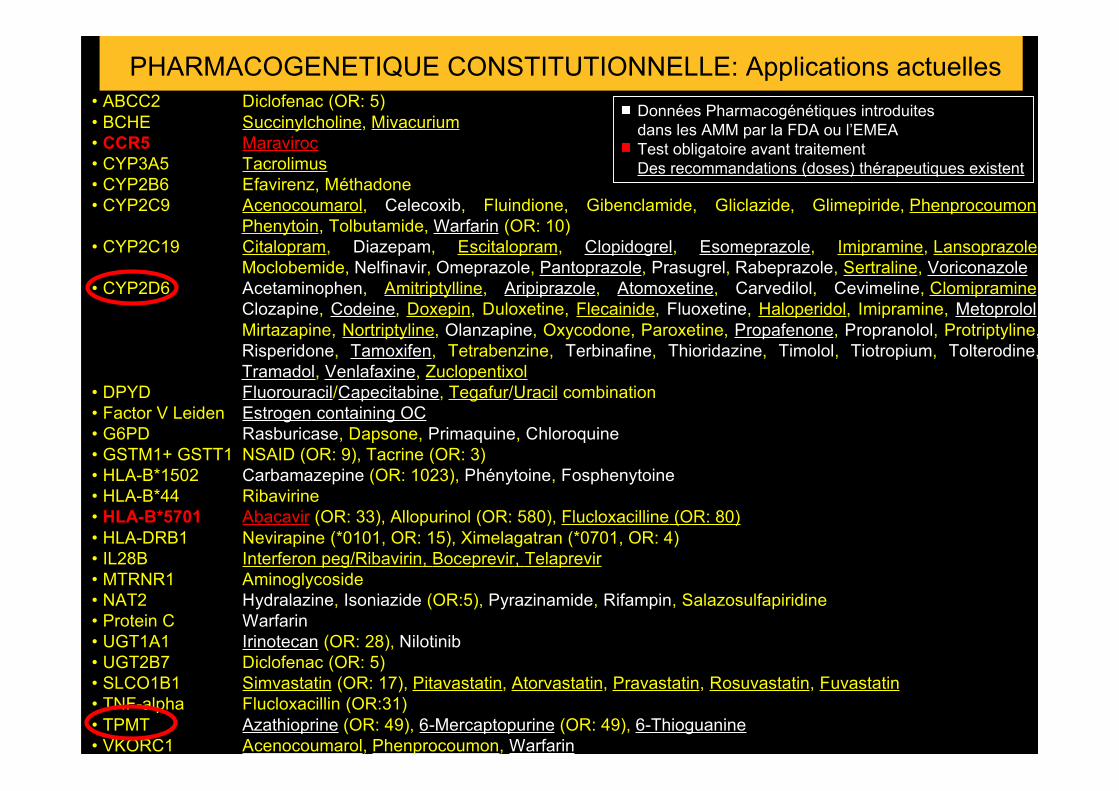
• ABCC2 Diclofenac (OR: 5)• BCHE Succinylcholine, Mivacurium• CCR5 Maraviroc• CYP3A5 Tacrolimus• CYP2B6 Efavirenz, Méthadone• CYP2C9 Acenocoumarol, Celecoxib, Fluindione, Gibenclamide, Gliclazide, Glimepiride, Phenprocoumon,
Phenytoin, Tolbutamide, Warfarin (OR: 10)• CYP2C19 Citalopram, Diazepam, Escitalopram, Clopidogrel, Esomeprazole, Imipramine, Lansoprazole,
Moclobemide, Nelfinavir, Omeprazole, Pantoprazole, Prasugrel, Rabeprazole, Sertraline, Voriconazole• CYP2D6 Acetaminophen, Amitriptylline, Aripiprazole, Atomoxetine, Carvedilol, Cevimeline, Clomipramine,
Clozapine, Codeine, Doxepin, Duloxetine, Flecainide, Fluoxetine, Haloperidol, Imipramine, Metoprolol,Mirtazapine, Nortriptyline, Olanzapine, Oxycodone, Paroxetine, Propafenone, Propranolol, Protriptyline,Risperidone, Tamoxifen, Tetrabenzine, Terbinafine, Thioridazine, Timolol, Tiotropium, Tolterodine,Tramadol, Venlafaxine, Zuclopentixol
• DPYD Fluorouracil/Capecitabine, Tegafur/Uracil combination• Factor V Leiden Estrogen containing OC• G6PD Rasburicase, Dapsone, Primaquine, Chloroquine• GSTM1+ GSTT1 NSAID (OR: 9), Tacrine (OR: 3)• HLA-B*1502 Carbamazepine (OR: 1023), Phénytoine, Fosphenytoine• HLA-B*44 Ribavirine• HLA-B*5701 Abacavir (OR: 33), Allopurinol (OR: 580), Flucloxacilline (OR: 80)• HLA-DRB1 Nevirapine (*0101, OR: 15), Ximelagatran (*0701, OR: 4)• IL28B Interferon peg/Ribavirin, Boceprevir, Telaprevir• MTRNR1 Aminoglycoside• NAT2 Hydralazine, Isoniazide (OR:5), Pyrazinamide, Rifampin, Salazosulfapiridine• Protein C Warfarin• UGT1A1 Irinotecan (OR: 28), Nilotinib• UGT2B7 Diclofenac (OR: 5)• SLCO1B1 Simvastatin (OR: 17), Pitavastatin, Atorvastatin, Pravastatin, Rosuvastatin, Fuvastatin• TNF-alpha Flucloxacillin (OR:31)• TPMT Azathioprine (OR: 49), 6-Mercaptopurine (OR: 49), 6-Thioguanine• VKORC1 Acenocoumarol, Phenprocoumon, Warfarin
PHARMACOGENETIQUE CONSTITUTIONNELLE: Applications actuellesDonnées Pharmacogénétiques introduitesdans les AMM par la FDA ou l’EMEATest obligatoire avant traitementDes recommandations (doses) thérapeutiques existent
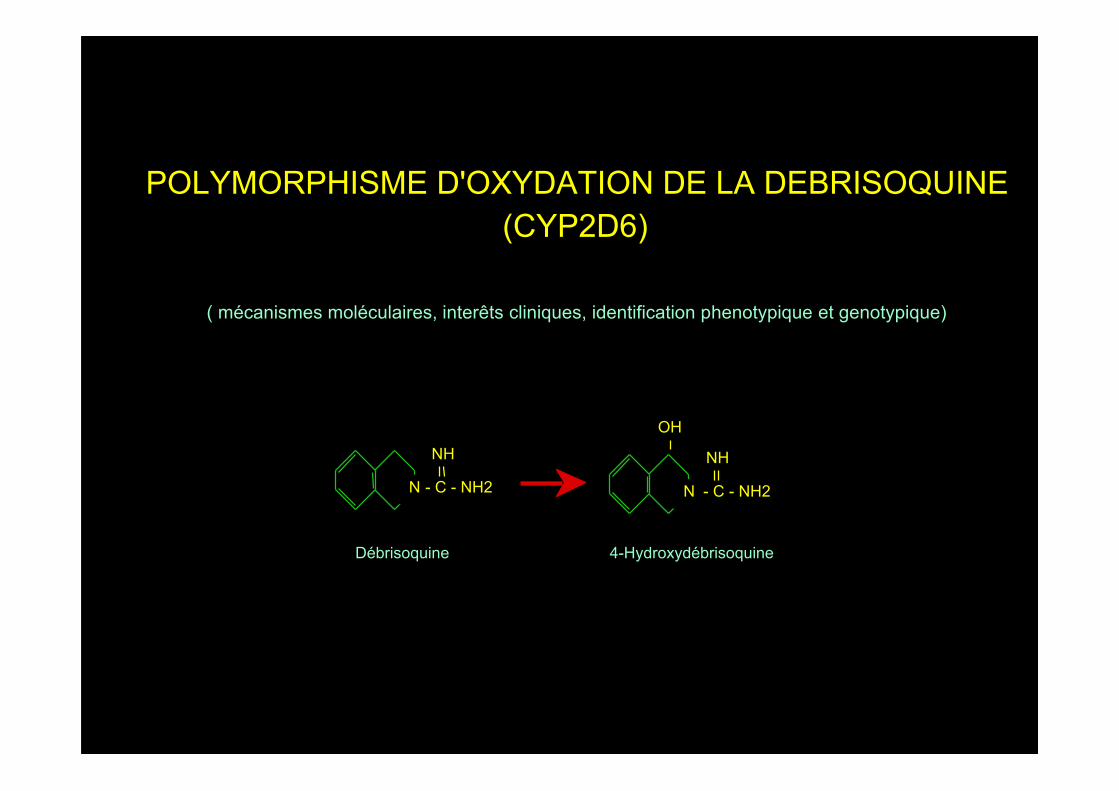
Débrisoquine 4-Hydroxydébrisoquine
NH
N - C - NH2
OH
NH
N - C - NH2
POLYMORPHISME D'OXYDATION DE LA DEBRISOQUINE(CYP2D6)
( mécanismes moléculaires, interêts cliniques, identification phenotypique et genotypique)
HydroxylationDebrisoquine 4-Hydroxydebrisoquine
NH
N - C - NH2
OH
NH
N - C - NH2
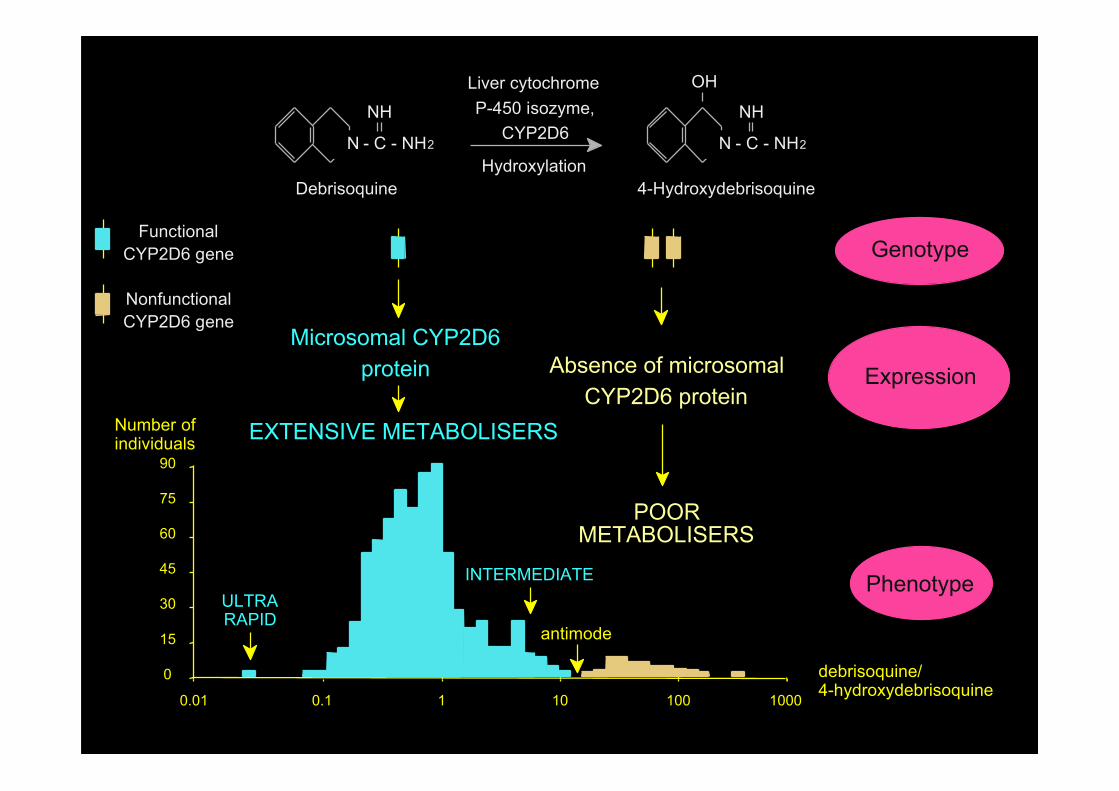
Liver cytochromeP-450 isozyme,
CYP2D6
Genotype
Expression
Phenotype
EXTENSIVE METABOLISERS
POORMETABOLISERS
Microsomal CYP2D6protein Absence of microsomal
CYP2D6 protein
FunctionalCYP2D6 gene
NonfunctionalCYP2D6 gene
0.01
debrisoquine/4-hydroxydebrisoquine0.1 1 10 100 1000
Number ofindividuals
0
90
75
60
45
30
15 antimode
ULTRARAPID
INTERMEDIATE
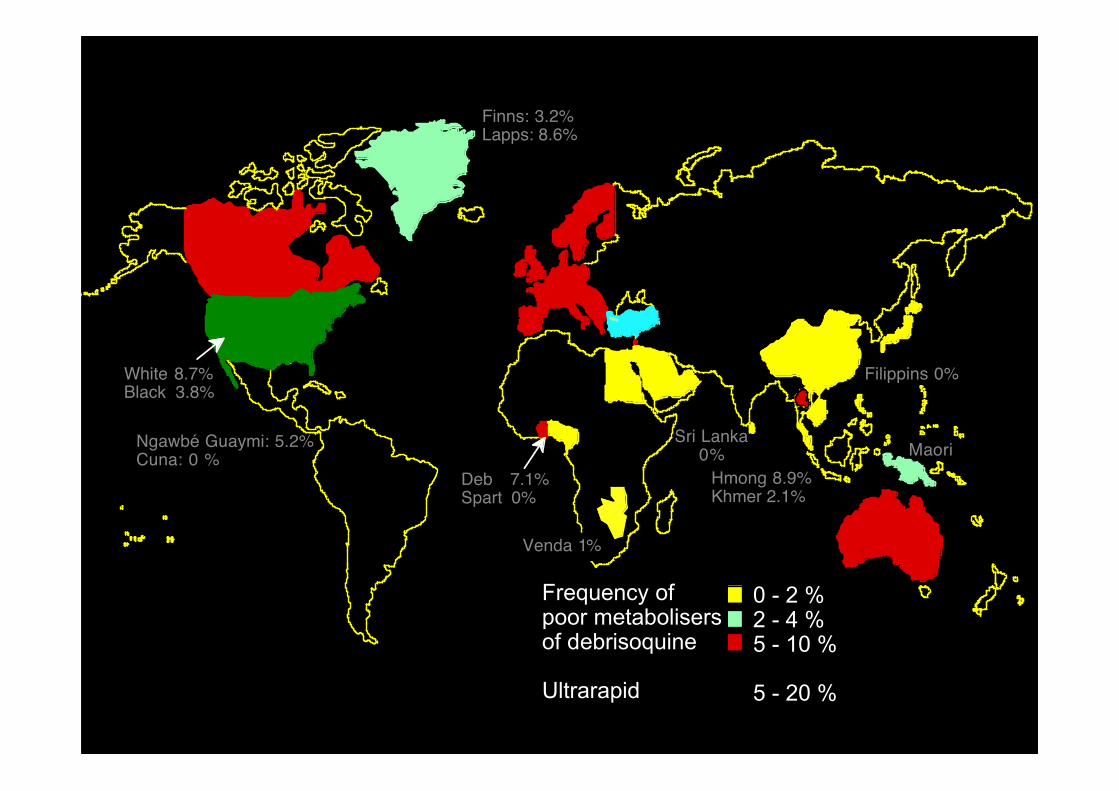
0 - 2 %2 - 4 %5 - 10 %
5 - 20 %
Frequency of poor metabolisersof debrisoquine
Ulrarapid
Deb 7.1%Spart 0%
White 8.7%Black 3.8%
Finns: 3.2%Lapps: 8.6%
Sri Lanka0%
Filippins 0%
MaoriHmong 8.9%Khmer 2.1%
Ngawbé Guaymi: 5.2%Cuna: 0 %
Venda 1%
0 - 2 %2 - 4 %5 - 10 %
5 - 20 %
Frequency of poor metabolisersof debrisoquine
Ultrarapid

Sub saharian AfricaNorth AfricaMiddle EastEuropeCentral / South AsiaEast AsiaOceaniaAmerica
80
60
40
20
0
Freq
uenc
y (%
)
Ultra rapid Extensive Intermediate Poor
PHENOTYPE CLASSES
North Africa
100Central / South Asia
America
East Asia
Europe
Europe and North America~ 7 % Poor~ 8 % Intermediate~ 81 % Extensive~ 4 % Ultra-rapid
Oceania

MEDICAMENTS DONT LE MÉTABOLISME EST AFFECTÉPAR LE POLYMORPHISME DE TYPE DÉBRISOQUINE
ß-bloqueursalprénololbufuralolbunitrololbupranololcarvédilolmétoprololpropranololtimolol
Antidépresseursamineptineamitriptylinecitalopramclomipraminedésipraminefluoxetinefluvoxamineimipraminelofepraminemaprotilinemiansérinenéfazodonenortriptylineparoxetinetomoxetinetrazodonetrimipraminevenlafaxine
Diverscinnarizinechloroquinedexfenfluramineflunarizinehalofantrine4-hydroxyamphét.lidocaïneloratadine4-méthoxyamph.minaprinenicergolineondansetronperhexilinephénacetinephenformineprométhazineritonavirsinvastatinetamoxifènethébaïnetropisetronzolpidem
AntiarythmiquesaprindineencainideflécainidemexilétinepropafénoneN-propylajmalinespartéine
Neuroleptiquesclopenthixolclozapinefluperlapinefluphénazinehalopéridollévomépromazineloxapineolanzapineperphénazineremoxipriderispéridonethioridazinetriflupéridolzuclopenthixol
Opiacés et dérivéscodéinedextrométorphanedihydrocodéineéthylmorphinedextrométhorphanehydrocodoneoxycodonetramadol
IMAOamiflaminebrofarominedeprenylméthoxyphénamine
Psychostimulantminaprine
Antihypertenseursdébrisoquinecaptoprilguanoxanindoramine
atomoxetine

METABOLISEUR LIMITE• Effet thérapeutique exagéré antidépresseurs,..• Réduction de l'effet thérapeutique codéine,..• Toxicité accrue du médicament perhexiline,..• Toxicité accrue d'un métabolite phénacétine,..• Réduction de la toxicité encaïnide,..
METABOLISEUR EXTENSIF/ULTRA-RAPIDE
• Inefficacité thérapeutique antidépresseurs,..• Toxicité accrue d'un métabolite métiamide,..• Intéractions médicamenteuses Inhibiteurs compétitifs • substrats
• non substrats quinidine,...Inhibiteurs non compétitifs cimetidine,...
METABOLISEUR EXTENSIF ou LIMITE• Voie métabolique accessoire propranolol,..• Précurseur et métabolite(s) actifs propafénone,..• Index thérapeutique large tropisetron,..

TRICYCLICANTIDEPRESSANTS
DRUG PM (%) IM (%) EM (%) UM (%)amitryptiline 73 92 111 130clomipramine 60 87 121 155desipramine 42 83 125 167doxepin 36 82 127 172imipramine 28 79 131 183nortriptyline 53 96 119 142trimipramine 32 76 141 206
SSRIS citalopram 98 100 101 102fluoxetine 78 94 107 120fluvoxamine 69 93 112 131paroxetine 66 90 114 138sertraline 99 100 100 100
OTHER ANTIDEPRESSANTS buproprion 90 97 104 111maprotiline 36 82 127 172mianserin 74 90 114 138mirtazapine 102 101 99 97moclobemide 121 107 92 77nefazadone 90 97 105 113trazadone 80 93 110 127venlafaxine 68 86 109 132
ANTIPSYCHOTICS aripiprazole 70 92 113 134flupentixol 74 86 116 146haloperidol 76 97 107 126olanzapine 61 105 122 139perazine 86 91 110 117perphenazine 31 80 129 178risperidone 87 96 106 116thioridazine 40 85 126 140zuclopenthixol 63 90 116 142
DOSING ADJUSTEMENT ACCORDING TO CYP2D6 PHENOTYPE
Doses are in mg/day
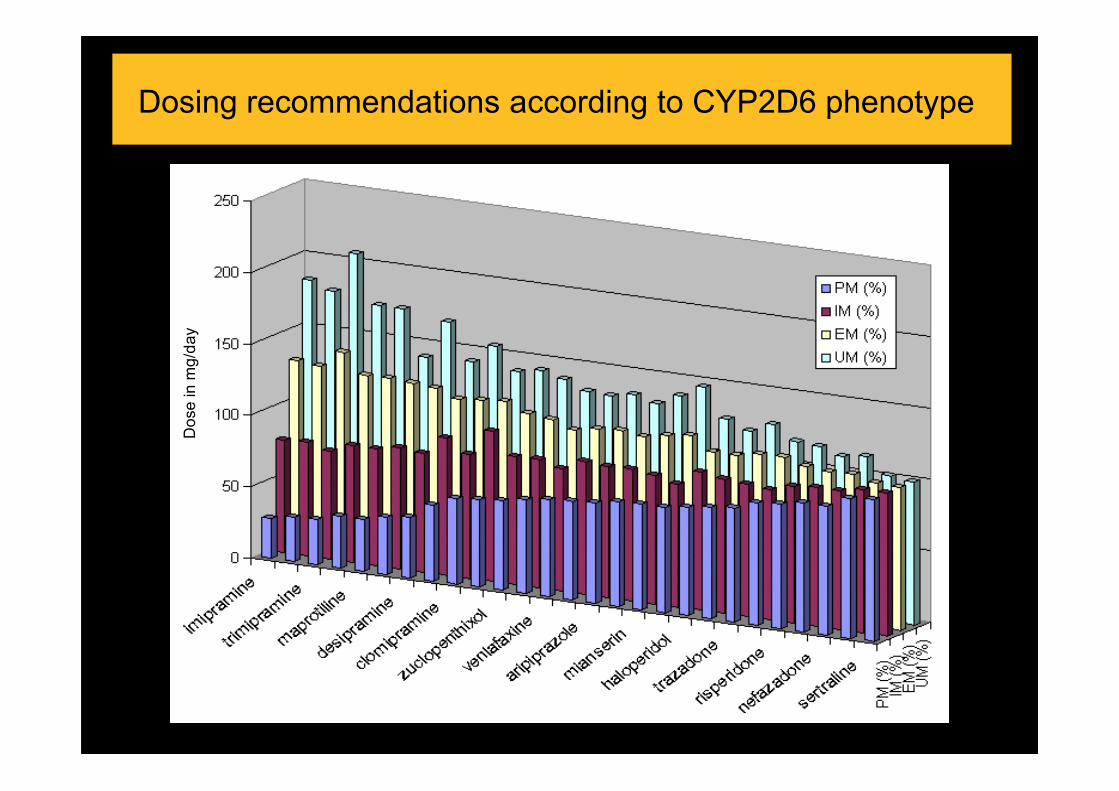
Dosing recommendations according to CYP2D6 phenotype
Dos
e in
mg/
day
INTERETS POUR LE POLYMORPHISME DU CYP2D6dans l'industrie pharmaceutique
Développement de nouveaux médicaments
- Etudes in vitroModélisationPréparation subcellulaireExpression de cDNA
- Essais cliniques
AUTRES INTERETS POUR LE POLYMORPHISME DUCYP2D6
• Association du phénotype et de :- Personnalité- Préférence alimentaire- Dépendance aux opiacés- Variables biologiques- Sensibilité à la douleur- Plaisir du tabac
• Anticorps anti LKM1
• CYP2D6 dans le cerveau

POLYMORPHISMEgénétique d'hydroxylation de la débrisoquine
(CYP2D6)
PHENOTYPES
- Phénotypage- Génotypage
Capacité métaboliquenombreux médicaments
. Surdosage
. Inefficacité thérapeutique
. Interactions médicamenteuses
Prévisions de risques
Associations pathologiques
Pathologies

POORMETABOLISERS
CALCUL DU RAPPORTMETABOLIQUE
Substancetest
EXTENSIVE METABOLISERS
0.01 0.1 1 10 100 1000
Number ofindividuals
0
90
75
60
45
30
15 antimode
ULTRARAPID
INTERMEDIATE
[substrat][métabolite(s)]
MESURE DE LACONCENTRATION
[substrat] [métabolite(s)]HPLC, CPG, ...
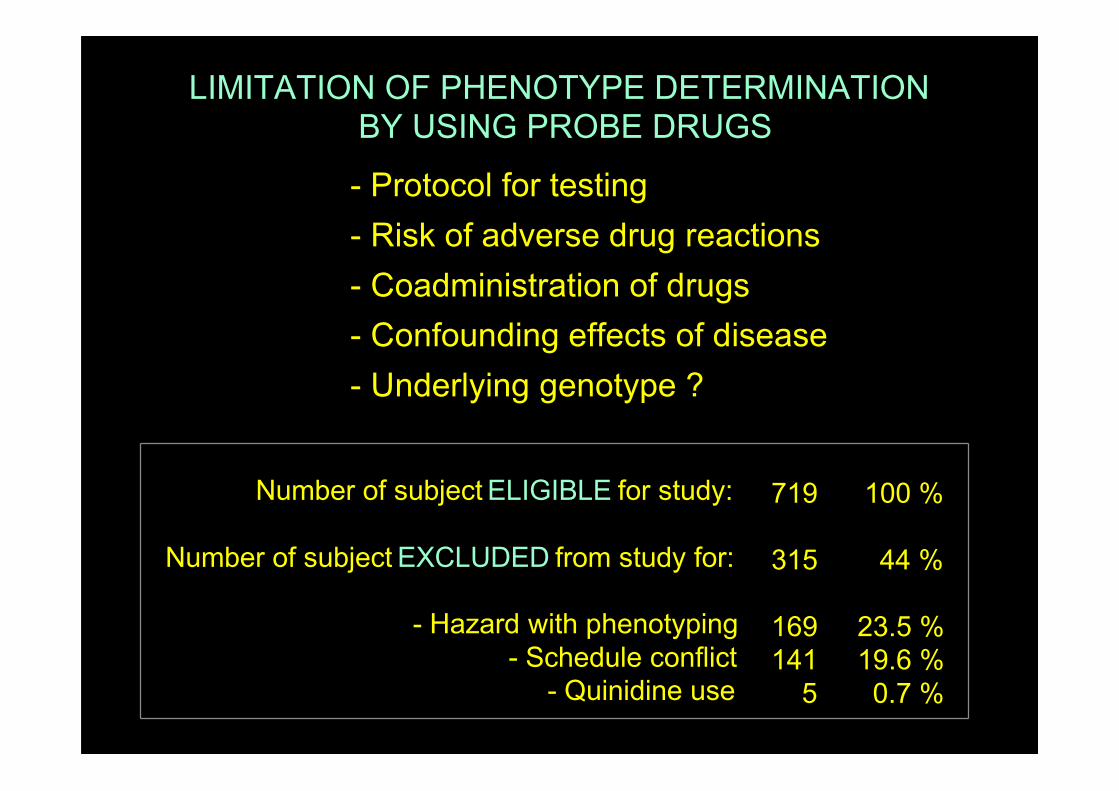
- Protocol for testing- Risk of adverse drug reactions- Coadministration of drugs- Confounding effects of disease- Underlying genotype ?
LIMITATION OF PHENOTYPE DETERMINATION BY USING PROBE DRUGS
Number of subject ELIGIBLE for study:
Number of subject EXCLUDED from study for:
- Hazard with phenotyping- Schedule conflict
- Quinidine use
100 %
44 %
23.5 %19.6 %0.7 %
719
315
169141
5

Génotype
Expression
Phénotype
METABOLISEURSEXTENSIFS
METABOLISEURSLIMITES
Protéine CYP2D6Absence de la protéine
CYP2D6
gène CYP2D6fonctionnel
gène CYP2D6non fonctionnel
debrisoquine/4-hydroxydebrisoquine
Identification directe des anomalies génétiques responsables du polymorphisme d'activité du CYP2D6GENOTYPAGE
0.01 0.1 1 10 100 1000
Nombre desujets
0
90
75
60
45
30
15
ULTRARAPIDES
INTERMEDIAIRES

E 1 25 9
867
X X XX
E E1 2 4 6 83 5 7 9
1 2 4 6 83 5 7 9
43
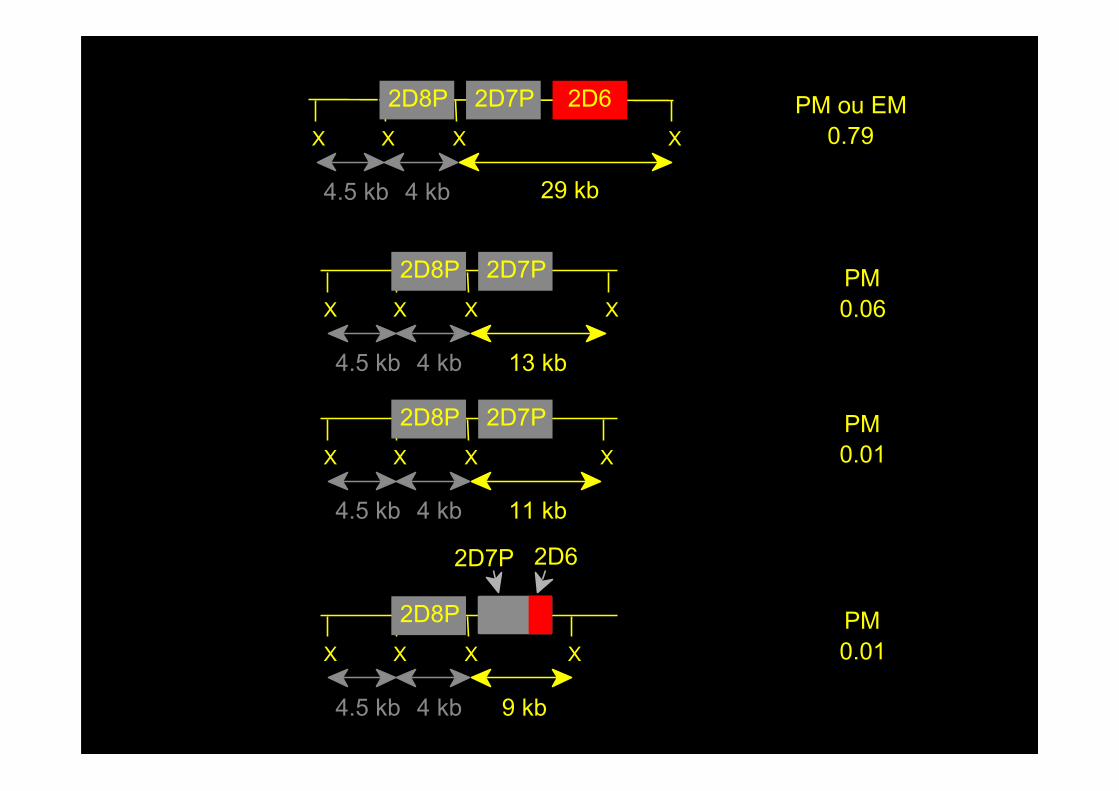
CYP2D8P CYP2D6CYP2D7P
4.5 kb 29 kb4 kb
Humanchromosome 22
(22q13.1)X: XbaI siteE: Eco RI site
CYP LTRCYP-REP
E
8.8 kb 9.4 kb15.1 kb
X X
4.5 kb 4 kb
X
29 kb
2D7P 2D6X
2D8P PM ou EM0.79
X X
4.5 kb 4 kb
X
13 kb
2D8P 2D7PX
PM0.06
X X
4.5 kb 4 kb
X
11 kb
2D8P 2D7PX
PM0.01
X X
4.5 kb 4 kb
X
9 kb
2D8PX
2D7P 2D6
PM0.01

X: XbaI siteE: Eco RI site
X
4.5 kb 4 kb
X
29 kb
2D8P 2D7P 2D6LX
E E E E
8.8 kb 15.1 kb 9.4 kb
X
4.5 kb 4 kb
X
42 kb
2D8P 2D7P 2D6L 2D6LX
E E E E E
8.8 kb 15.1 kb 12.1 kb 9.4 kb
X
4.5 kb 4 kb 175 kb
2D8P 2D7P 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6LX
E E E E E E E E E E E E E E E E
8.8 kb 15.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 12.1 kb 9.4 kb
X
4.5 kb 4 kb
X
55 kb
2D8P 2D7P 2D6L 2D6LX
E E E E E
8.8 kb 15.1 kb 12.1 kb 12.1 kb
E
9.4 kb
2D6LX X
4.5 kb 4 kb
X
78 kb
2D8P 2D7P 2D6L 2D6LX
E E E E E
8.8 kb 15.1 kb 12.1 kb 12.1 kb
2D6L 2D6L
E E
12.1 kb 12.1 kb
E
9.4 kb
2D6L
X X
4.5 kb 4 kb
X
66 kb
2D8P 2D7P 2D6L 2D6LX
E E E E E
8.8 kb 15.1 kb 12.1 kb 12.1 kb
2D6L
E E
12.1 kb 9.4 kb
2D6L
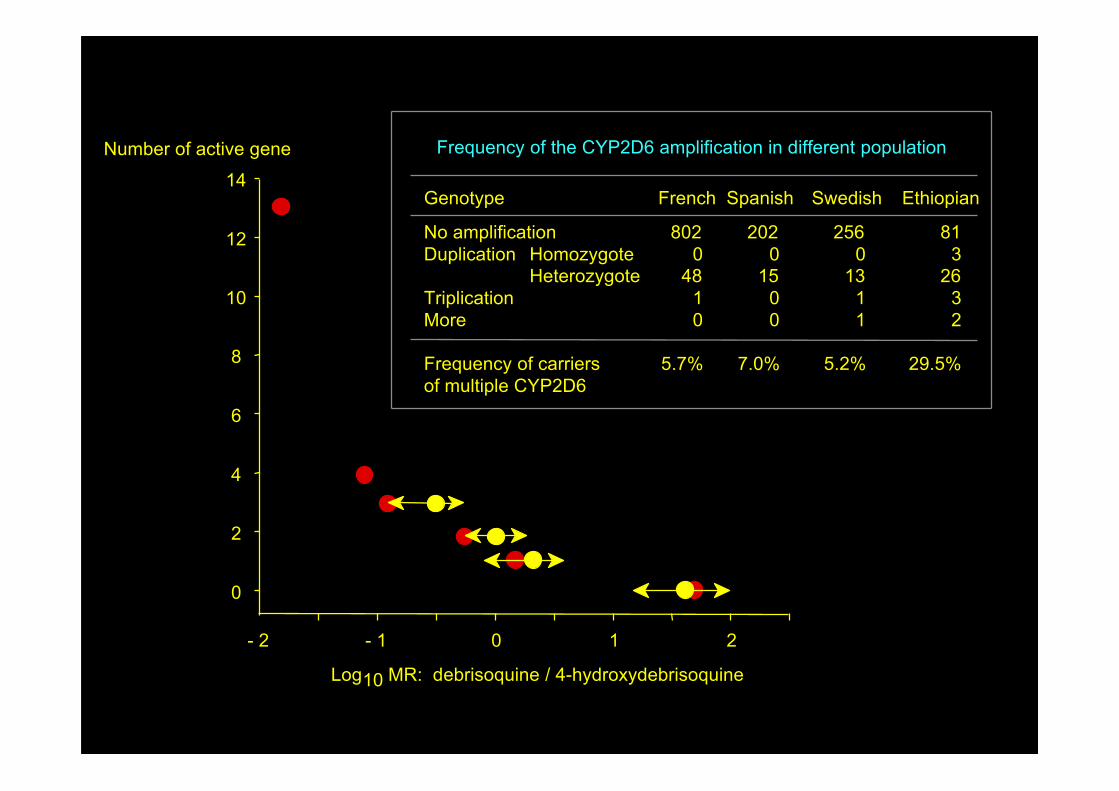
Log10 MR: debrisoquine / 4-hydroxydebrisoquine
14
12
10
8
6
4
2
0
- 2 - 1 0 1 2
Number of active gene Frequency of the CYP2D6 amplification in different population
No amplificationDuplication
TriplicationMore
Frequency of carriersof multiple CYP2D6
HomozygoteHeterozygote
8020
4810
5.7%
2020
1500
7.0%
Genotype French Spanish
2560
1311
5.2%
Swedish
813
2632
29.5%
Ethiopian

G ins
G C G T
Frame shift
3023971
1934D6-B
CYP2D6 inactivatingmutations
1 4 6 7 8 92
2637D6-A
A del
5
Frame shiftT del
3
1795D6-T 1846
Stop codongeneration
Splice sitedisappearance
Splice sitedisappearance
C A
Missense
212
G A
Missense
2627-30
Frame shift
1943-51
G A
AACT del
9 bp rep3 AA repeat
2061
Frame shift

Genotype
Expression
normal geneCYP2D6
Defective mutantCYP2D6
Entire CYP2D6deletion
Mutant CYP2D6reduce activity
CYP2D6amplification
Phenotype
EXTENSIVE METABOLISERS
POORMETABOLISERS
CYP2D6protein Absence of microsomal
CYP2D6 protein
0.01
debrisoquine/4-hydroxydebrisoquine
0.1 1 10 100 1000
Number ofindividuals
0
90
75
60
45
30
15 antimode
ULTRARAPID
INTERMEDIATE
• ABCC2 Diclofenac (OR: 5)• BCHE Succinylcholine, Mivacurium• CCR5 Maraviroc• CYP3A5 Tacrolimus• CYP2B6 Efavirenz, Méthadone• CYP2C9 Acenocoumarol, Celecoxib, Fluindione, Gibenclamide, Gliclazide, Glimepiride, Phenprocoumon,
Phenytoin, Tolbutamide, Warfarin (OR: 10)• CYP2C19 Citalopram, Diazepam, Escitalopram, Clopidogrel, Esomeprazole, Imipramine, Lansoprazole,
Moclobemide, Nelfinavir, Omeprazole, Pantoprazole, Prasugrel, Rabeprazole, Sertraline, Voriconazole• CYP2D6 Acetaminophen, Amitriptylline, Aripiprazole, Atomoxetine, Carvedilol, Cevimeline, Clomipramine,
Clozapine, Codeine, Doxepin, Duloxetine, Flecainide, Fluoxetine, Haloperidol, Imipramine, Metoprolol,Mirtazapine, Nortriptyline, Olanzapine, Oxycodone, Paroxetine, Propafenone, Propranolol, Protriptyline,Risperidone, Tamoxifen, Tetrabenzine, Terbinafine, Thioridazine, Timolol, Tiotropium, Tolterodine,Tramadol, Venlafaxine, Zuclopentixol
• DPYD Fluorouracil/Capecitabine, Tegafur/Uracil combination• Factor V Leiden Estrogen containing OC• G6PD Rasburicase, Dapsone, Primaquine, Chloroquine• GSTM1+ GSTT1 NSAID (OR: 9), Tacrine (OR: 3)• HLA-B*1502 Carbamazepine (OR: 1023), Phénytoine, Fosphenytoine• HLA-B*44 Ribavirine• HLA-B*5701 Abacavir (OR: 33), Allopurinol (OR: 580), Flucloxacilline (OR: 80)• HLA-DRB1 Nevirapine (*0101, OR: 15), Ximelagatran (*0701, OR: 4)• IL28B Interferon peg/Ribavirin, Boceprevir, Telaprevir• MTRNR1 Aminoglycoside• NAT2 Hydralazine, Isoniazide (OR:5), Pyrazinamide, Rifampin, Salazosulfapiridine• Protein C Warfarin• UGT1A1 Irinotecan (OR: 28), Nilotinib• UGT2B7 Diclofenac (OR: 5)• SLCO1B1 Simvastatin (OR: 17), Pitavastatin, Atorvastatin, Pravastatin, Rosuvastatin, Fuvastatin• TNF-alpha Flucloxacillin (OR:31)• TPMT Azathioprine (OR: 49), 6-Mercaptopurine (OR: 49), 6-Thioguanine• VKORC1 Acenocoumarol, Phenprocoumon, Warfarin
PHARMACOGENETIQUE CONSTITUTIONNELLE: Applications actuellesDonnées Pharmacogénétiques introduitesdans les AMM par la FDA ou l’EMEATest obligatoire avant traitementDes recommandations (doses) thérapeutiques existent

Génotype
Expression
Phénotype
Proportion desujet (%) par0.5 Unité/ml
d'activité TPMT
ACTIVITEINDETECTABLE
(1/300)
ACTIVITE ELEVEE(89 %)
TPMTcytoplasmique
déficitaire
TPMTcytoplasmiquefonctionnelle
Gène TPMT fonctionnel
Gène TPMT non fonctionnel
0
10
5
0 Activité TPMT(Unités/ml)
5 10 15 20
ThiopurineS-méthyltransférase
(TPMT)N
N NH
NSH
N
N NH
NS
CH3
S-adénosyl-L-méthionine
S-adénosyl-L-homocystéine
ACTIVITEINTERMEDIAIRE
(11 %)
6-mercaptopurine 6-méthylmercaptopurine
Polymorphisme génétique de la thiopurine S-methyl transferase (TPMT)
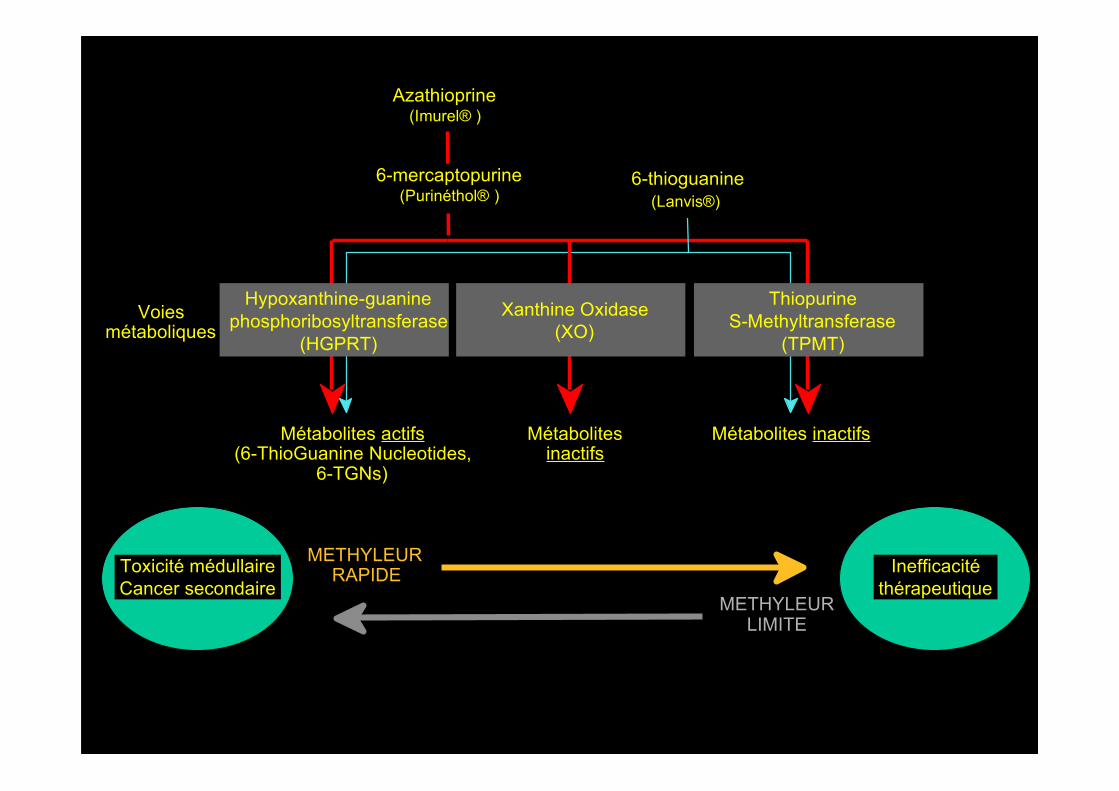
Azathioprine(Imurel® )
6-thioguanine(Lanvis®)
Voiesmétaboliques
Métabolites actifs(6-ThioGuanine Nucleotides,
6-TGNs)
Métabolitesinactifs
Métabolites inactifs
Hypoxanthine-guaninephosphoribosyltransferase
(HGPRT)
Xanthine Oxidase(XO)
ThiopurineS-Methyltransferase
(TPMT)
6-mercaptopurine(Purinéthol® )
METHYLEURRAPIDE
METHYLEURLIMITE
Toxicité médullaire Cancer secondaire
Inefficacité thérapeutique

LeukopeniaGood responsePoor response
TPMT level (U/ml RBCs)10 15 20 25
Dose ofAzathioprine
(mg/kg per Day)
3.0
2.5
2.0
1.5
1.0
0.5
0.0
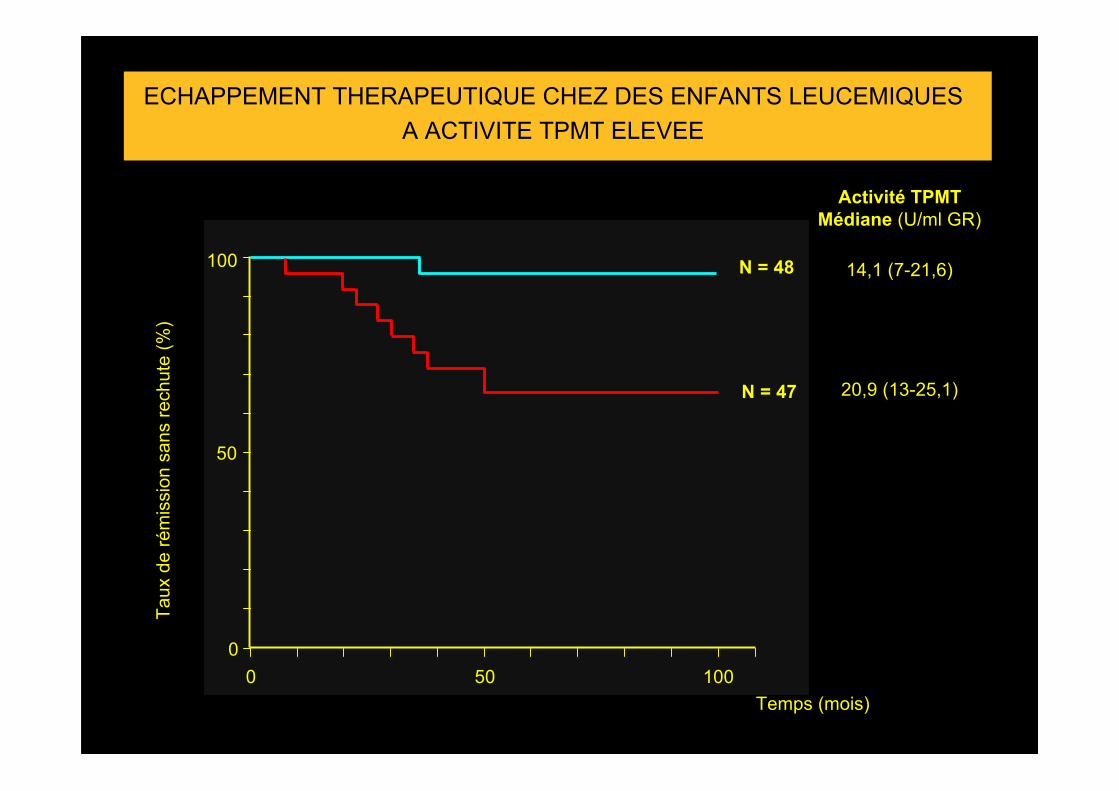
ECHAPPEMENT THERAPEUTIQUE CHEZ DES ENFANTS LEUCEMIQUESA ACTIVITE TPMT ELEVEE
Taux
de
rém
issi
on s
ans
rech
ute
(%)
Temps (mois)
0
50
100
0 50 100
Activité TPMTMédiane (U/ml GR)
14,1 (7-21,6)
20,9 (13-25,1)
N = 48
N = 47
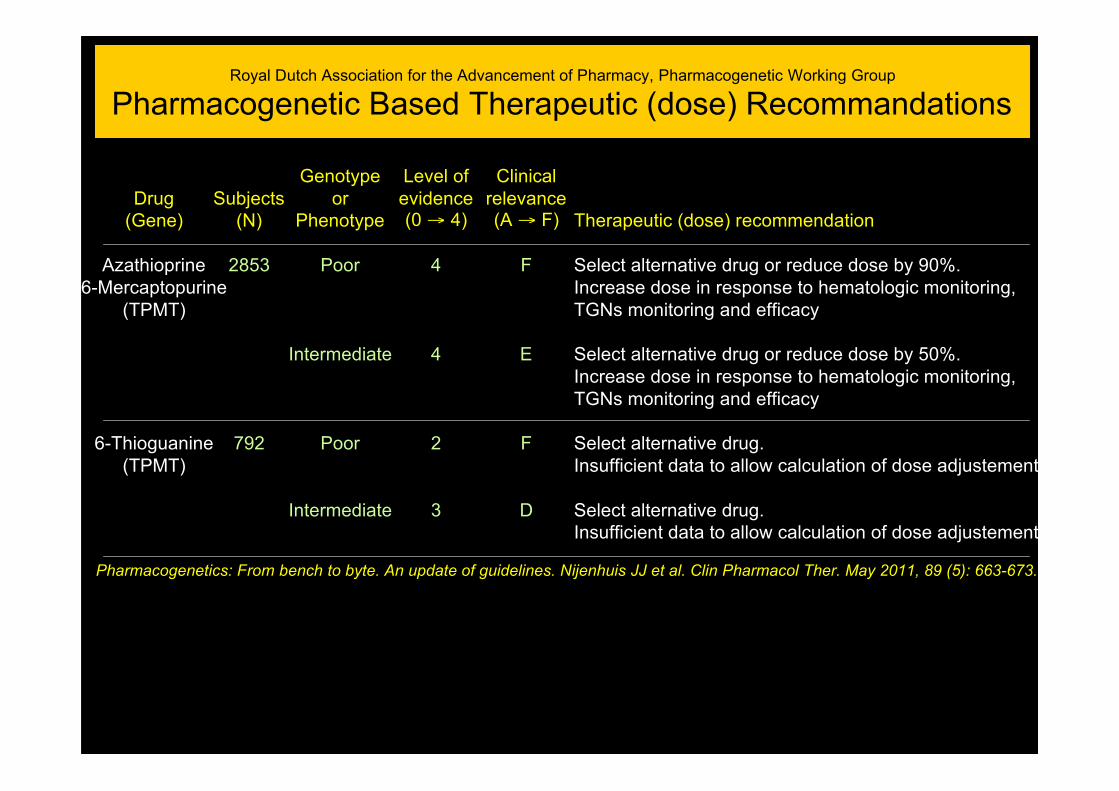
Royal Dutch Association for the Advancement of Pharmacy, Pharmacogenetic Working Group
Pharmacogenetic Based Therapeutic (dose) Recommandations
Drug(Gene)
Azathioprine6-Mercaptopurine
(TPMT)
6-Thioguanine(TPMT)
Pharmacogenetics: From bench to byte. An update of guidelines. Nijenhuis JJ et al. Clin Pharmacol Ther. May 2011, 89 (5): 663-673.
Subjects(N)
2853
792
Genotypeor
Phenotype
Poor
Intermediate
Poor
Intermediate
Level ofevidence(0 → 4)
4
4
2
3
Clinicalrelevance(A → F)
F
E
F
D
Therapeutic (dose) recommendation
Select alternative drug or reduce dose by 90%.Increase dose in response to hematologic monitoring,TGNs monitoring and efficacy
Select alternative drug or reduce dose by 50%.Increase dose in response to hematologic monitoring,TGNs monitoring and efficacy
Select alternative drug.Insufficient data to allow calculation of dose adjustement.
Select alternative drug.Insufficient data to allow calculation of dose adjustement
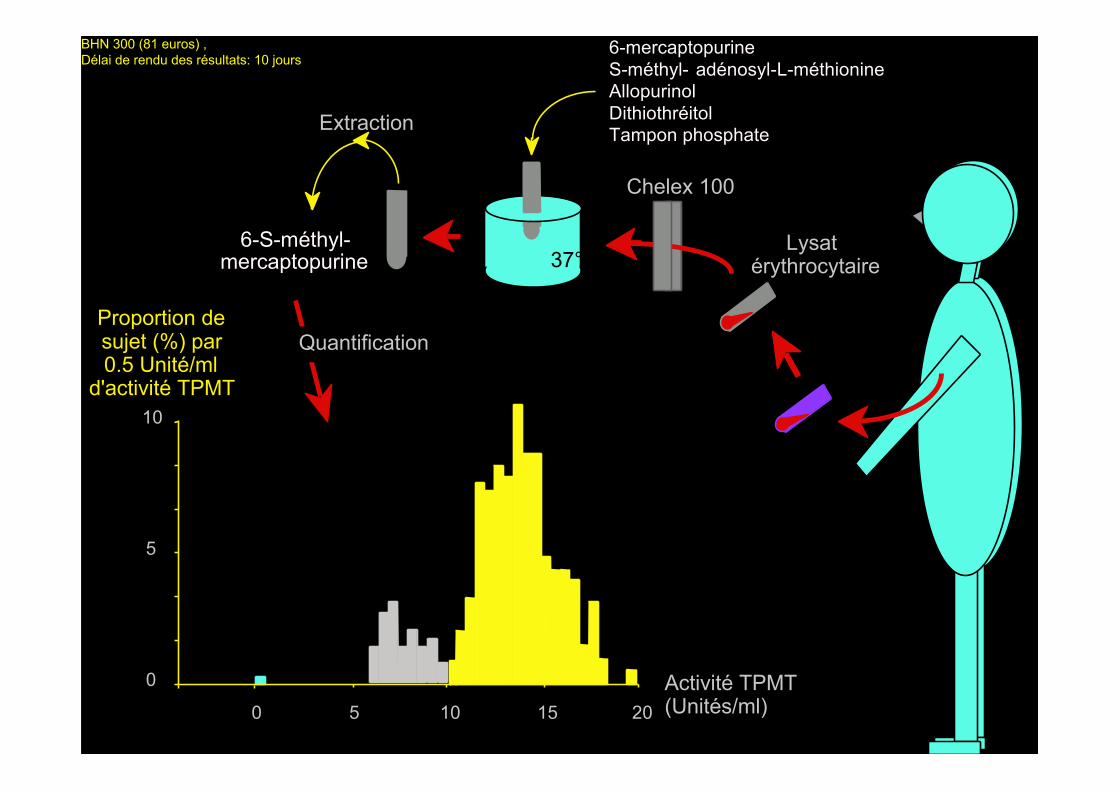
Lysatérythrocytaire
Chelex 100
0
10
5
0 5 10 15 20
37°
6-mercaptopurineS-méthyl- adénosyl-L-méthionineAllopurinolDithiothréitolTampon phosphateExtraction
6-S-méthyl-mercaptopurine
QuantificationProportion desujet (%) par0.5 Unité/ml
d'activité TPMT
Activité TPMT(Unités/ml)
BHN 300 (81 euros) , Délai de rendu des résultats: 10 jours

G238C
Ala80→ Pro
A719G
Tyr240→ Cys
G460A
Ala154→ Thr
Chromosome 6(6p22.3)
MUTATIONS DU GENE TPMT
I II III IV V VI VII VIII IX X
5' 3'
G292T
Glu98→ Stop
G → AT146C
Leu49→ Ser
A539T
Tyr180→ Phe
C474T
Ile158→ Ile
C339T
Thr113→ Thr
T-30AcT114A
T35CC58TG96T
Génotypage prospectif des 3 mutations inactivatrices les plus fréquentes: 48 hrs, BHN 500 (135 euros)
Splice site
T681G
His227→ Gln
G644A
Arg215→ His
A356C
Lys119→ Tyr
G430C
Gly144→ Arg
C374T
Ser125→ Leu
A83T
Glu28→ Val
A1G
Met1→ Val
G → ASplice site
G488A
Arg163→ HisC124G
Gln42→ Glu
G211A
Gly71→ Arg
A365C
Lys122→ Thr
VNTRMotif de 17/18pb répété 4 à 8 fois
Séquençage rétrospectif des 10 exons du gène et de son extrémité 5’: 1 semaine, BHN 2500 (675 euros)

Days after transplantation
0
300
200
100
Peripheral bloodleucocyte(106/ml)
Azathioprinedose
(mg/day)
0 10 20 30 40 50 60 70 80 90 100
Pneumoniaeand septicemia
Death
0
2
4
6
8
10
12
14
16

PRETREATMENT COUNSELLING AND TPMT SCREENING
In the context of the information presented, it is recommended that safety and efficacy issuesrelating to azathioprine are discussed fully with patients before treatment with azathioprine isstarted. The obvious concern is the one in 300 chance of an absolute deficiency in TPMT whichwould predispose a patient to a serious risk of early and severe pancytopenia. Both patients andtheir physicians will have different responses to such a risk which will be influenced by cultural,educational and emotional factors in addition to the medical indication for its usage. What iscertain is that it is no longer adequate for the physician to recommend azathioprine on the basisof their personal experience of the efficacy and safety of the drug without more detaileddiscussion concerning possible risks of therapy than has hitherto been the case. Patients in theUK will need to be informed that susceptibility to the risk of severe toxicity with azathioprinewhilst rare, is not yet detectable by pretreatment screening. Neither TPMT assay nor themeasurement of 6-TGNs is currently routinely available in the UK and until they are, safetymonitoring for azathioprine will continue to follow the manufacturer’s guidelines. These are beingamended to highlight concerns about the genetically determined susceptibility of someindividuals to azathioprine toxicity. The gold standard for TPMT assay is the radiochemicalassay of Weinshilboum et al., although work from several groups to assess an HPLC techniquehas recently been completed. The cDNA for TPMT has recently been cloned, sequenced andexpressed and this opens up the possibility of a genotyping test which, if successful, promises tohave the potential for usage in routine TPMT monitoring. Until such a test becomes widelyavailable in the UK an element of Russian roulette will continue to characterise azathioprineusage.
Anstey A. Journal of the Royal Society of Medicine, 1995, 88: 155-160.
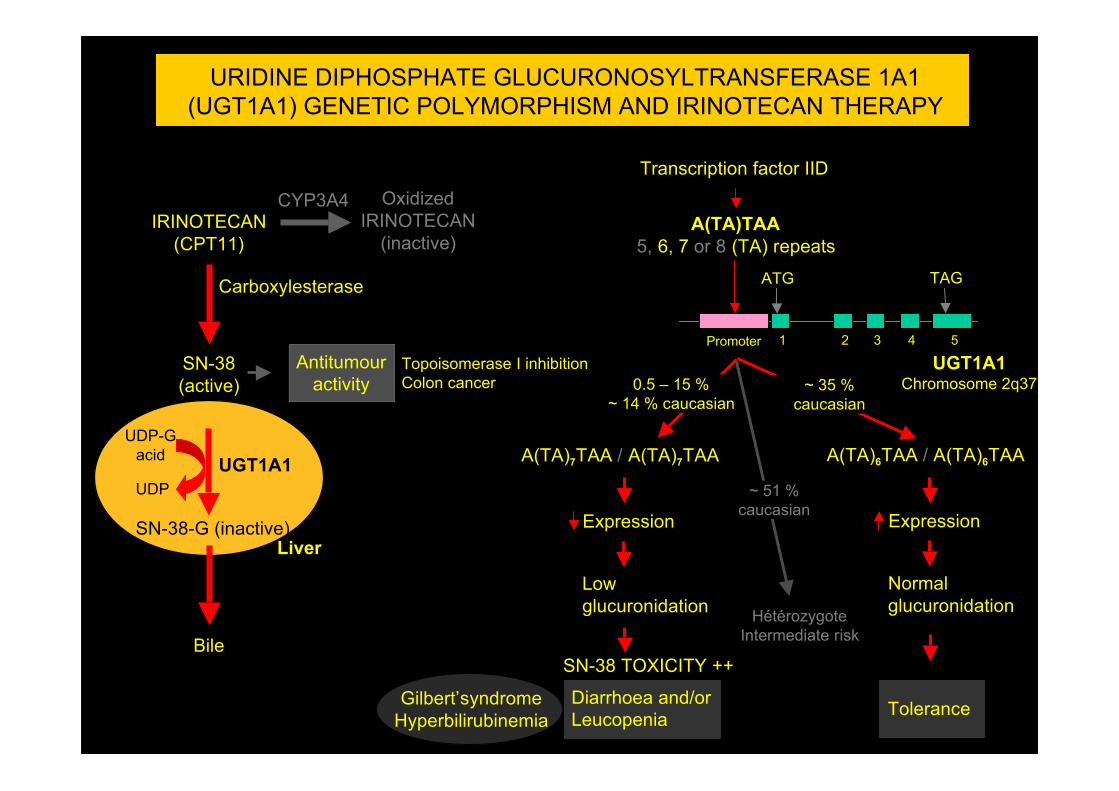
IRINOTECAN(CPT11)
Transcription factor IID
ATG TAG
A(TA)TAA5, 6, 7 or 8 (TA) repeats
Promoter 1 2 3 4 5
OxidizedIRINOTECAN
(inactive)
SN-38(active)
SN-38-G (inactive)
Bile
Antitumouractivity
Liver
UGT1A1
Carboxylesterase
UGT1A1Chromosome 2q37
CYP3A4
A(TA)7TAA / A(TA)7TAA
Expression
Lowglucuronidation
Diarrhoea and/orLeucopenia
Expression
Normalglucuronidation
Tolerance
URIDINE DIPHOSPHATE GLUCURONOSYLTRANSFERASE 1A1(UGT1A1) GENETIC POLYMORPHISM AND IRINOTECAN THERAPY
0.5 – 15 %~ 14 % caucasian
Topoisomerase I inhibitionColon cancer
UDP-Gacid
UDP
Gilbert’syndromeHyperbilirubinemia
SN-38 TOXICITY ++
A(TA)6TAA / A(TA)6TAA
HétérozygoteIntermediate risk
~ 35 %caucasian
~ 51 %caucasian
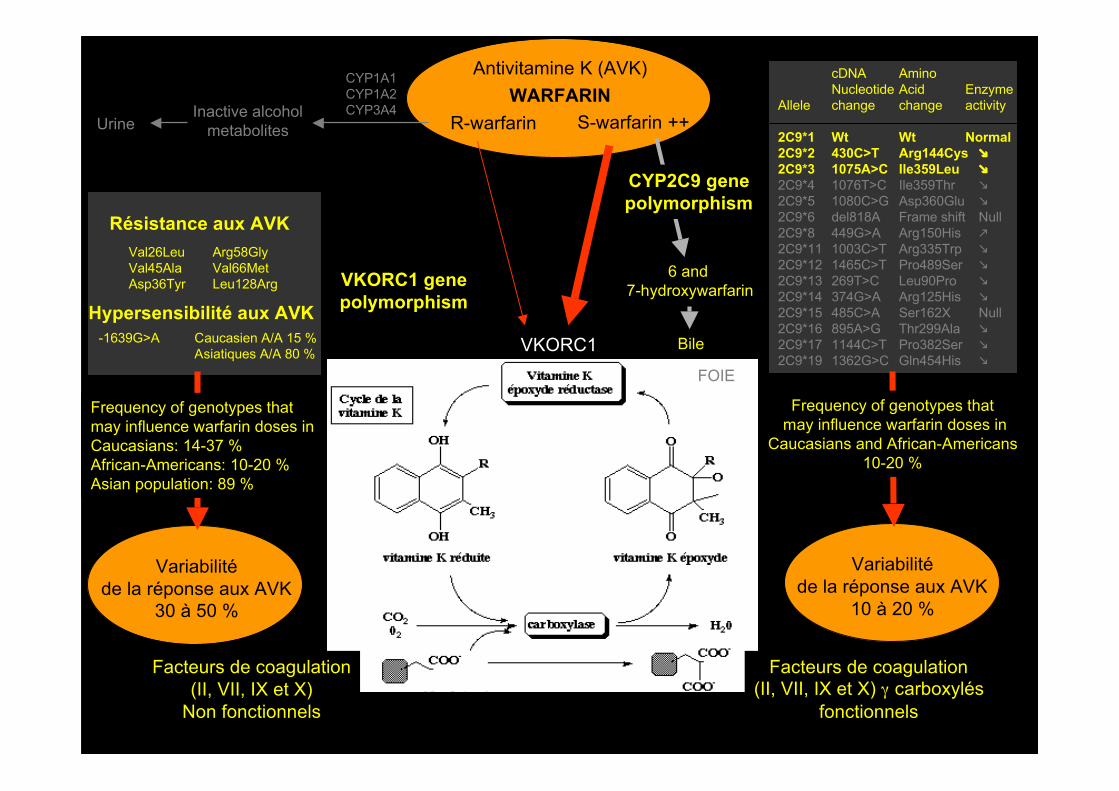
Antivitamine K (AVK)WARFARIN
R-warfarin S-warfarin ++
CYP1A1CYP1A2CYP3A4Inactive alcohol
metabolites
6 and 7-hydroxywarfarin
Urine
Bile
Allele
2C9*12C9*22C9*32C9*42C9*52C9*62C9*82C9*112C9*122C9*132C9*142C9*152C9*162C9*172C9*19
cDNA Nucleotide change
Wt430C>T1075A>C1076T>C1080C>Gdel818A449G>A1003C>T1465C>T269T>C374G>A485C>A895A>G1144C>T1362G>C
AminoAcid change
WtArg144CysIle359LeuIle359ThrAsp360GluFrame shiftArg150HisArg335TrpPro489SerLeu90ProArg125HisSer162XThr299AlaPro382SerGln454His
Enzyme activity
Normal Null Null
Val26LeuVal45AlaAsp36Tyr
Résistance aux AVK
-1639G>A Caucasien A/A 15 %Asiatiques A/A 80 %
Hypersensibilité aux AVK
Arg58GlyVal66MetLeu128Arg
Variabilitéde la réponse aux AVK
30 à 50 %
VKORC1 genepolymorphism
VKORC1
Variabilitéde la réponse aux AVK
10 à 20 %
Facteurs de coagulation(II, VII, IX et X)
Non fonctionnels
Facteurs de coagulation(II, VII, IX et X) γ carboxylés
fonctionnels
CYP2C9 genepolymorphism
FOIE
Frequency of genotypes that may influence warfarin doses in
Caucasians and African-Americans10-20 %
Frequency of genotypes thatmay influence warfarin doses inCaucasians: 14-37 %African-Americans: 10-20 %Asian population: 89 %

Capecitabine (Xeloda® )(5’deoxy-5-fluorouridine)
ProdrugMutation
IVS14+1G>A5’splice site
consensus sequenceGT → AT
Exon 13
5-FU
Antitumour activityCytotoxic effect
Thymidinephosphorylase
DYPD950 kb 23 exons
Chromosome 1p22
AT / AT
DiarrhoeaLeucopenia
Functional protein
Normal 5-FUTolerance
DIHYDROPYRIMIDINE DEHYDROGENASE (DYPD) GENETICPOLYMORPHISM AND 5-FLUOROURACIL (5-FU) THERAPY
~ 4 %caucasian
Head, neack, cervix, breast andgastrointestinal tract cancers
Pyrimidine catabolismdeficiency
Uraciluria/ThyminuriaMental retardation
5-FU TOXICITY +++
~ 96 %caucasian
Dihydro 5-FU(inactive)
DYPD
GTAG
Exon 14
GTAG
Exon 15
GTAG
GT / GTAT / GT
13 14 15
13 14 15
13 14 15
13 Exon1415
13 Exon1415
13 Exon1415
Very rare
Normal DYPDactivity
NON functionalprotein
↓↓ DYPDactivityPaediatric patients
> 80%
Thymidylatesynthase
dTMP de novosynthesis
5-FdUMP
Complex withand inhibits
Liver
LiverBowel
Tumour
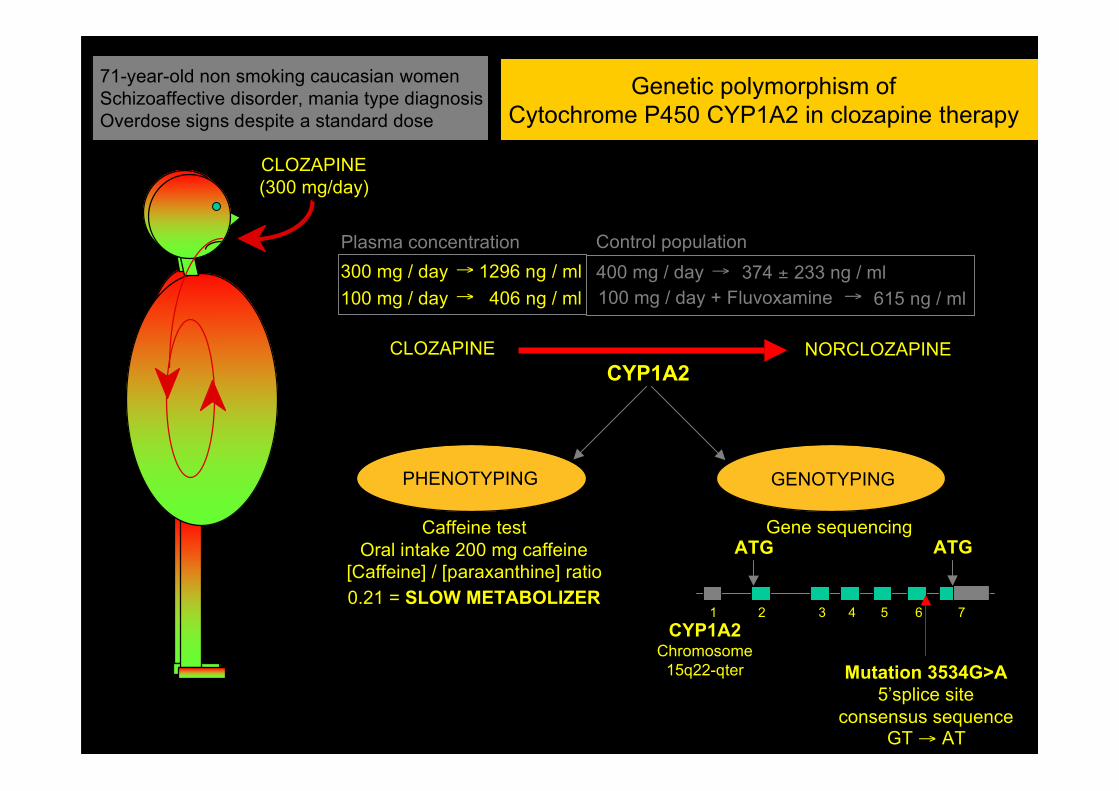
71-year-old non smoking caucasian womenSchizoaffective disorder, mania type diagnosisOverdose signs despite a standard dose
CLOZAPINE(300 mg/day)
CLOZAPINE NORCLOZAPINE
300 mg / day100 mg / day
→
→1296 ng / ml
406 ng / ml
CYP1A2
PHENOTYPING GENOTYPING
Caffeine testOral intake 200 mg caffeine
[Caffeine] / [paraxanthine] ratio0.21 = SLOW METABOLIZER
Gene sequencingATG ATG
Mutation 3534G>A5’splice site
consensus sequenceGT → AT
1 2 3 4 5 6 7
Plasma concentration400 mg / day → 374 ± 233 ng / mlControl population
100 mg / day + Fluvoxamine → 615 ng / ml
CYP1A2Chromosome
15q22-qter
Genetic polymorphism ofCytochrome P450 CYP1A2 in clozapine therapy

ECOGENETIQUEApplications en Médecine Légale
Genetic tests to prevent adversedrug reactions may save tens ofthousands of lives a year, but fora troubled boy named mickaelthey came too late
Forbes Magazine
…While recuperating from what seemed to be flu, Michael went into a prolonged grand mal seizure and died. His grievingparents, Jayne and Neil, soon got another shock: an autopsy showed a massive overdose of Prozac in Michael's blood andtissues, raising the specter of a murder charge against them …Thus began the Adams-Conroys' painful pilgrimage to a medical frontier known as pharmacogenetics, the study of howgenetic influences responses to drugs…”
A DNA tragedy FLUOXETINE: DEATH IN A CHILD WITHPOLYMORPHISME OF CYTOCHROMEP450 2D6
A 9-year-old died due to fluoxetinetoxicity. Genetic tests confirmed that hehad a gene defect at the CYP2D6 locus,which made him a poor metabolizer offluoxetine.
Sallee et al. J Child Adolesc Psychopharmacol. 2000;10:27-34The death of nine-year-old Michael Adams-Conroy didn'tseem at first like a signal event in medicine.It seemed like homicide.
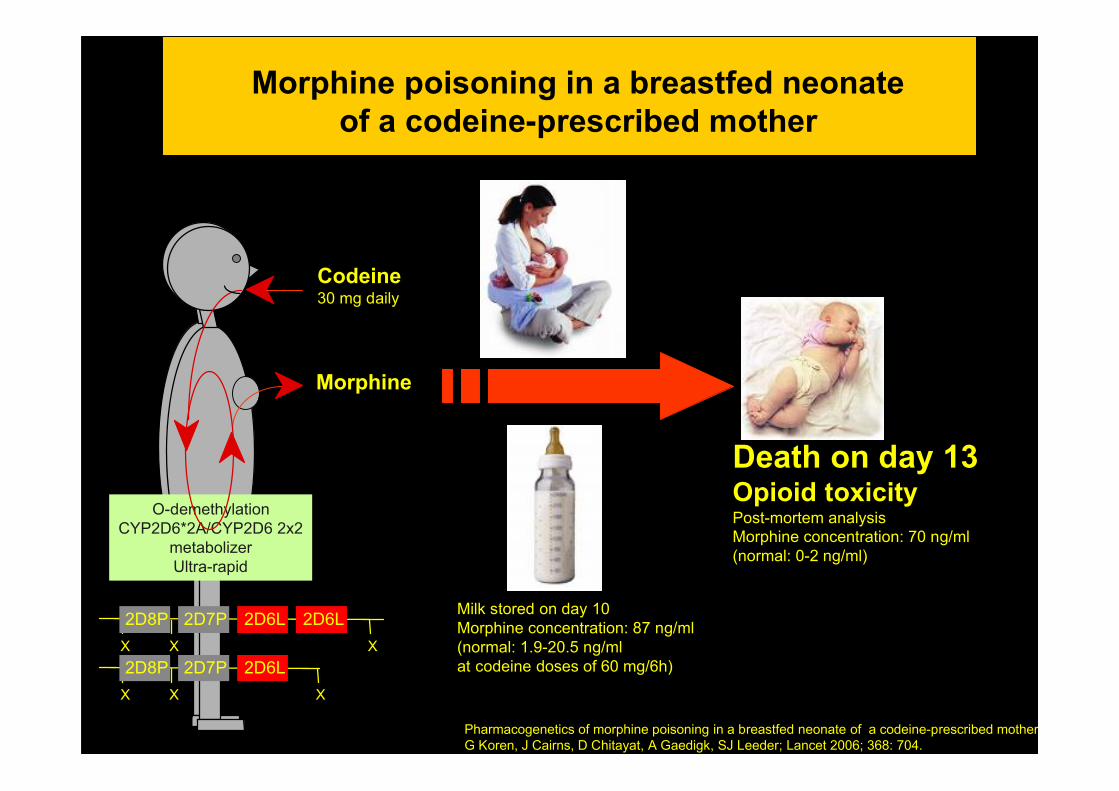
Pharmacogenetics of morphine poisoning in a breastfed neonate of a codeine-prescribed mother.G Koren, J Cairns, D Chitayat, A Gaedigk, SJ Leeder; Lancet 2006; 368: 704.
Morphine poisoning in a breastfed neonateof a codeine-prescribed mother
Codeine30 mg daily
O-demethylationCYP2D6*2A/CYP2D6 2x2
metabolizerUltra-rapid
Morphine
Milk stored on day 10Morphine concentration: 87 ng/ml(normal: 1.9-20.5 ng/ml at codeine doses of 60 mg/6h)
Death on day 13 Opioid toxicityPost-mortem analysisMorphine concentration: 70 ng/ml(normal: 0-2 ng/ml)
X X
2D8P 2D7P 2D6L 2D6LX
X X
2D8P 2D7P 2D6LX

Patient dépendant aux opiacésTraité par méthadone à doses standardMort subite
(R, S) -méthadone(60 mg/day)
S-METHADONE
S-EDDP(2-éthylidene-1,5-diméthyl-3,
3-diphénylpyrrolidine)inactif
821 ng / ml209 ng / ml612 ng / ml
CYP2B6
PHENOTYPING GENOTYPING
Gene sequencingATG ATG
Mutation 785A>G (Lys262Arg)Genotype *6/*6
METABOLISEUR LIMITE(~ 6 % Caucasiens)
1 2 3 4 5 6 7
Concentration plasmatique420 ng / ml210 ng / ml205 ng / ml
Control population(R, S)-methadone
(R)-methadone(S)-methadone
KCNH2Canal potassique
cardiaque
Anomalie duRythme cardiaqueRepolarisation et durée du
potentiel d’actionLong QT
Torsade de pointe etMort subite
R-METHADONE
R-EDDP(2-éthylidene-1,5-diméthyl-3,
3-diphénylpyrrolidine)inactif
CYP3A4
Recepteurs µaux opiacés
Inhibition
CYP2B6Chromosome
19q13.2
ECOGENETIQUEApplications en Nutrigénétique

We are Antiaging Group BarcelonaDr. Laura Salvador, responsible for the nutrigenetic/nutrigenomic studies will offer you to design a type of highlypersonalized diet, based on your genetic profile.The nutrigenetic study is carried out in a very simple way. After the first consultation with our specialist, when theindividual characteristics, the lifestyle and the pathological antecedents will be gauged, |he|she will take a sampleof saliva that will be sent to the laboratory. 13 polymorphisms associated with the nutrition are evaluated. With theobtained results we will carry out a series of recommendations highly personalized, indicating which foodsincrease or reduce the risk of developing certain illnesses related with the different diets; that will allow us toprevent different types of illnesses related with the environment.

• Fèves (vicine et convicine)• Teintures au Henné• Boules de naphtaline• Colorants alimentaires artificiels• Insecticides DDT• Nitrobenzène• Médicaments• …..
G6PDH
NADPNADPH
H2O2
H2O
Glutathionperoxydase
Glutathionréductase
Glucose-6-phosphate
Ribulose-5phosphate
2 GSH GSSGO2
peroxydes
AnémieHémolytique
Globule rougeGlobule rouge
Glucose-6-PhosphateDéshydrogénase

Aflatoxine B1
Mutation
Desactivation
Aflatoxine (G)-ADN adduit
EPOXYDE
GSTM1, EPHX1
In vivo, P53: 249
Adduits protéines:Témoin d’exposition
CYP3A4
HEPATOCARCINOME
GSTM1, EPHX1
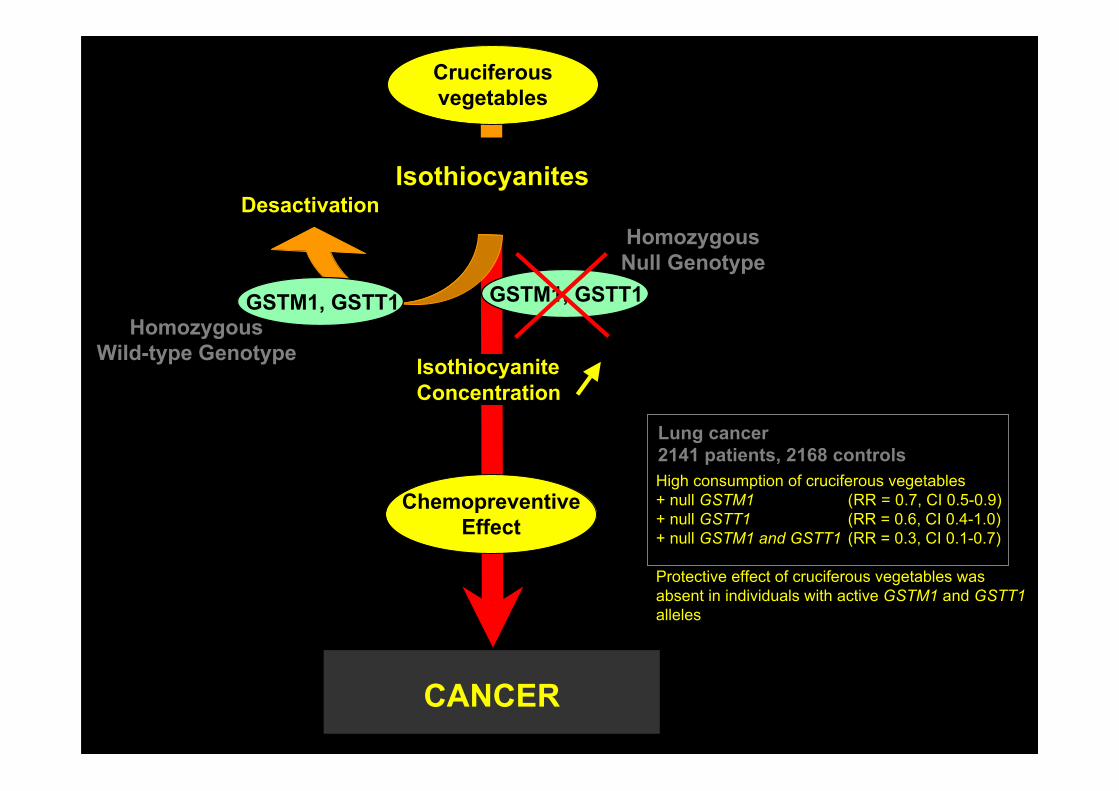
Cruciferousvegetables
ChemopreventiveEffect
Desactivation
IsothiocyaniteConcentration
Isothiocyanites
GSTM1, GSTT1
HomozygousNull Genotype
GSTM1, GSTT1Homozygous
Wild-type Genotype
Lung cancer2141 patients, 2168 controlsHigh consumption of cruciferous vegetables+ null GSTM1 (RR = 0.7, CI 0.5-0.9)+ null GSTT1 (RR = 0.6, CI 0.4-1.0)+ null GSTM1 and GSTT1 (RR = 0.3, CI 0.1-0.7)
Protective effect of cruciferous vegetables wasabsent in individuals with active GSTM1 and GSTT1alleles
CANCER

William Shakespeare,The Tempest, Act 2. Scene 2. (Trinculo's monologue)"What have we here? a man or a fish? dead or alive? A fish: he smells like a fish; a very ancient and fish-like smell; a kind of not ofthe newest Poor-John. A strange fish! Were I in England now, as once I was, and had but this fish painted, not a holiday fool therebut would give a piece of silver: there would this monster make a man; any strange beast there makes a man: when they will notgive a doit to relieve a lame beggar, they will lazy out ten to see a dead Indian. Legged like a man and his fins like arms! Warm o'my troth! I do now let loose my opinion; hold it no longer: this is no fish, but an islander, that hath lately suffered by a thunderbolt.«
• Embarrassment,• Ridicule,• Low self-esteem,• Social exclusion,• Isolation,• Anxiety,• Depression
• and SUICIDE….
Sea products: Marine fish (deap-sea), cephalopods, crustaceans …Legumes: Soya, bean products, peas, peanuts….Offals: Liver, kidney…Eggs…..
TRIMETHYLAMINURIA(Fish odour syndrome)

GUT
Eggs
LIVERDIET
Liverand other offals
Legumes
Fish(Salt water or marine)
CholineHOCH2CH2N+(CH3)
3
Trimethylamine-N-oxide(CH3)3 N+ O-
Bacteria
Dimethylamine
Methylamine
CO2 + NH3
TRIMETHYLAMINEN-OXIDE
Sweat, UrineBreath, Saliva
FMO3FMO3 deficiency
(ODOURLESS)LecithinCarnitineOther bétaïnes
TRIMETHYLAMINEN-OXIDE
TRIMETHYLAMINE
TRIMETHYLAMINE

mm
oles
/mol
cre
atin
ine
MESURE DE LA CONCENTRATION[Trimethylamine][Trimethylamine-N-oxide]
6000500040003000200010000
6050403020100
-------
------- R
atio
TM
A/T
MA
O
0 12 24 36 48 60 72Time (hours)
6000500040003000200010000
0.060.050.040.030.020.010
-------
-------
0 12 24 36 48 60 72Time (hours)
Patient with FMO3 deficiency
Control
mm
oles
/mol
cre
atin
ine
Rat
io T
MA
/TM
AO
Trimethylamine Marine fish meal
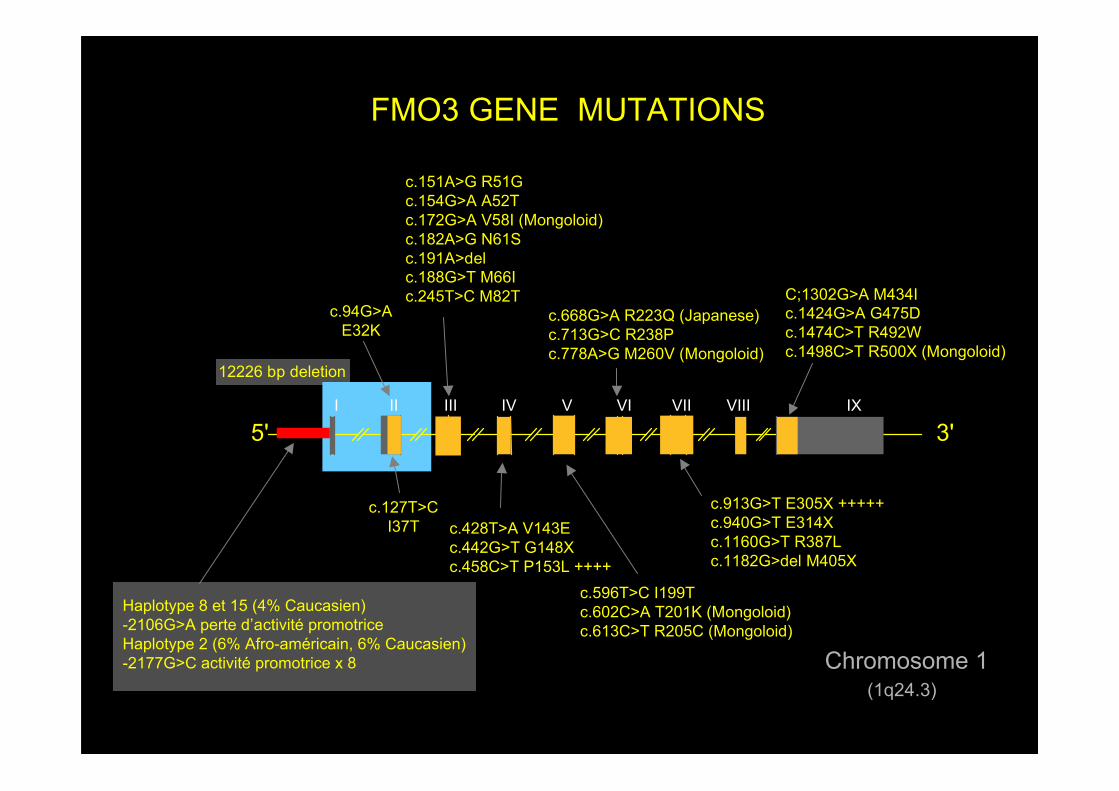
Chromosome 1(1q24.3)
I II III IV V VI VII VIII IX
5' 3'
c.94G>AE32K
FMO3 GENE MUTATIONS
c.127T>CI37T
c.151A>G R51Gc.154G>A A52Tc.172G>A V58I (Mongoloid)c.182A>G N61Sc.191A>delc.188G>T M66Ic.245T>C M82T
c.428T>A V143Ec.442G>T G148Xc.458C>T P153L ++++
c.596T>C I199Tc.602C>A T201K (Mongoloid)c.613C>T R205C (Mongoloid)
c.668G>A R223Q (Japanese)c.713G>C R238Pc.778A>G M260V (Mongoloid)
c.913G>T E305X +++++c.940G>T E314Xc.1160G>T R387Lc.1182G>del M405X
C;1302G>A M434Ic.1424G>A G475Dc.1474C>T R492Wc.1498C>T R500X (Mongoloid)
12226 bp deletion
Haplotype 8 et 15 (4% Caucasien)-2106G>A perte d’activité promotriceHaplotype 2 (6% Afro-américain, 6% Caucasien)-2177G>C activité promotrice x 8
ECOGENETIQUEApplications en Médecine du travail
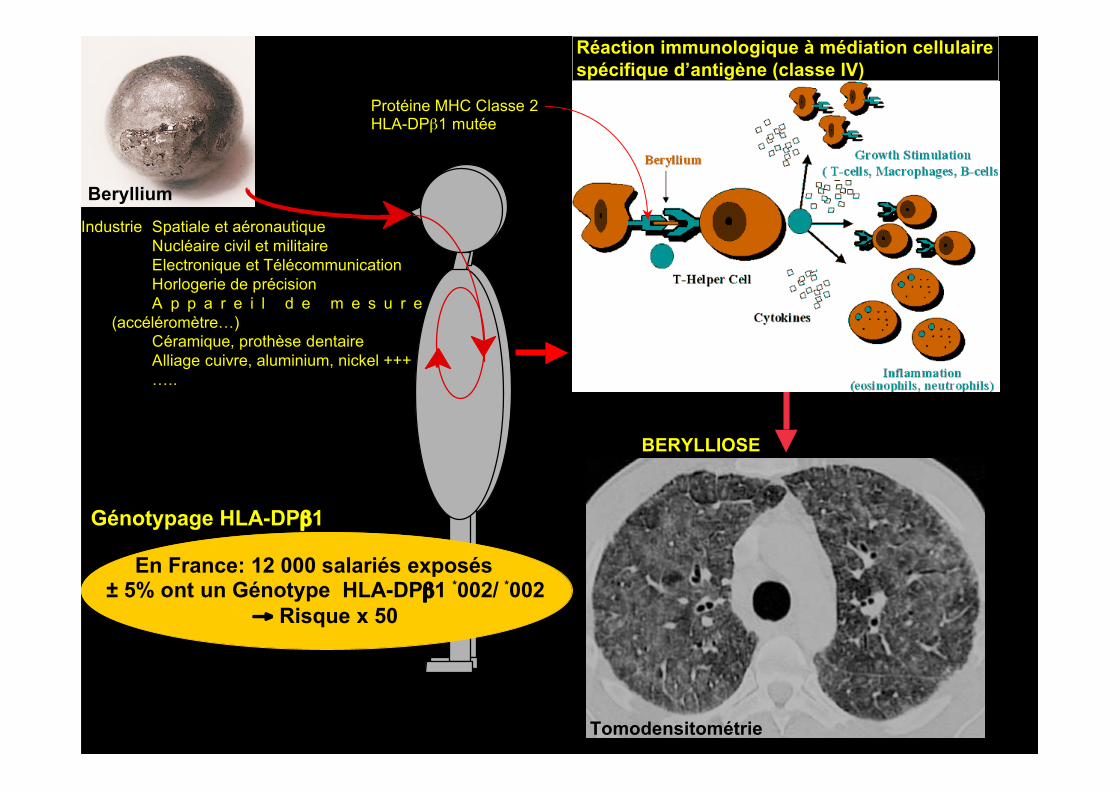
BerylliumIndustrie Spatiale et aéronautique
Nucléaire civil et militaireElectronique et TélécommunicationHorlogerie de précisionA p p a r e i l d e m e s u r e
(accéléromètre…)Céramique, prothèse dentaireAlliage cuivre, aluminium, nickel +++…..
BERYLLIOSE
Réaction immunologique à médiation cellulairespécifique d’antigène (classe IV)
Tomodensitométrie
Protéine MHC Classe 2HLA-DPβ1 mutée
En France: 12 000 salariés exposés ± 5% ont un Génotype HLA-DPβ1 *002/ *002
→ Risque x 50
Génotypage HLA-DPβ1
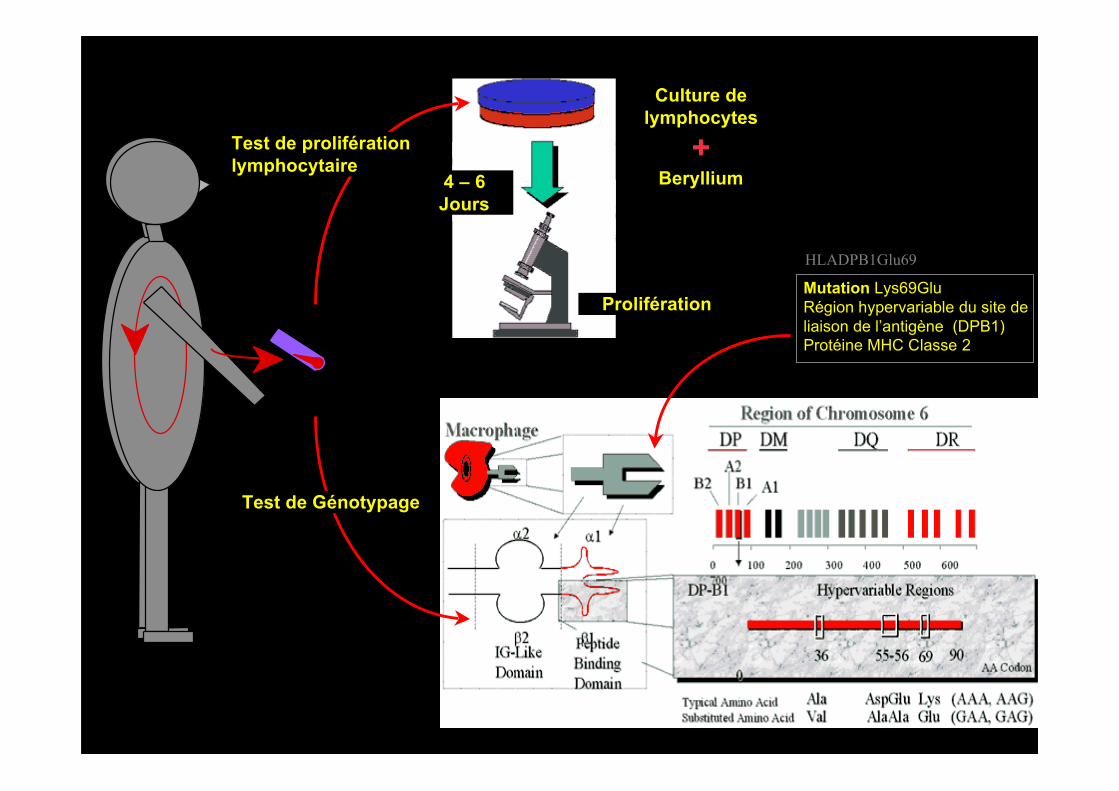
HLADPB1Glu69
Mutation Lys69GluRégion hypervariable du site deliaison de l’antigène (DPB1)Protéine MHC Classe 2
Test de Génotypage
Culture delymphocytes
+Beryllium
Prolifération
4 – 6Jours
Test de proliférationlymphocytaire
ECOGENETIQUEPerspectives

TOXICOGENETIC PHENOMENA
Genetic polymorphisms of xenobiotic metabolizing enzymes and transporters
• CYP1A2• CYP2A6• CYP2C9• CYP2C19• CYP2D6
• CYP2E1• CYP3A5• Alcohol dehydrogenase (ADH1B)• Alcohol dehydrogenase (ADH3)• Aldehyde dehydrogenase (ALDH2)• Arsenic methyltransferase (AS3MT)• Arylamine N-acetyltransferase 1 (NAT1)• Butyrylcholinesterase (Bche)• Catechol-O-methyltransferase (COMT)• Dihydropyrimidine dehydrogenase (DPD)• DT-diaphorase (NQO1)• Glutathione S-transferase-M1 (GSTM1)• Mercaptopyruvate sulfurtransferase (MPST)• Myeloperoxidase (MPO)• N-acetyltransferase (NAT2)
• Paraoxonase (PON1)• Thiocyanate sulfurtransferase (TST)• Thiopurine S-methyltransferase (TPMT)• UDP-glucuronosyl transferase 1A1 (UGT1A1)• •••
Clozapine responseSmoking behaviors and nicotine dependenceAnticoagulant effect of warfarinPeptic ulcer cure rates with omeprazoleTardive diskinesia from antipsychotics, narcotic side effects, efficacy,and dependence, imipramine dose requirement, ß-blockers effectEffect on alcohol consumptionTacrolimus efficacyFetal alcohol spectrum disordersIncreased alcohol consumption and dependenceSCE frequency in lymphocytes (cyclophosphamide)Arsenic dependent carcinogenesisBladder cancer susceptibilitySuccinylcholine or mivacurium sensitivity, cocaine toxicityLevodopa response5-fluorouracil neurotoxicityMenadione-associated urolithiasisLung, laryngeal and urinary bladder cancerCyanide toxicityClozapine-induced agranulocytosisHypersensitivity to sulfonamides, amonafide toxicity, hydralazineinduce lupus, isoniazide neurotoxicity, bladder cancerPesticide sensitivityCyanide toxicityThiopurine toxicity and efficacy, risk of second cancersIrinotecan toxicity• •••
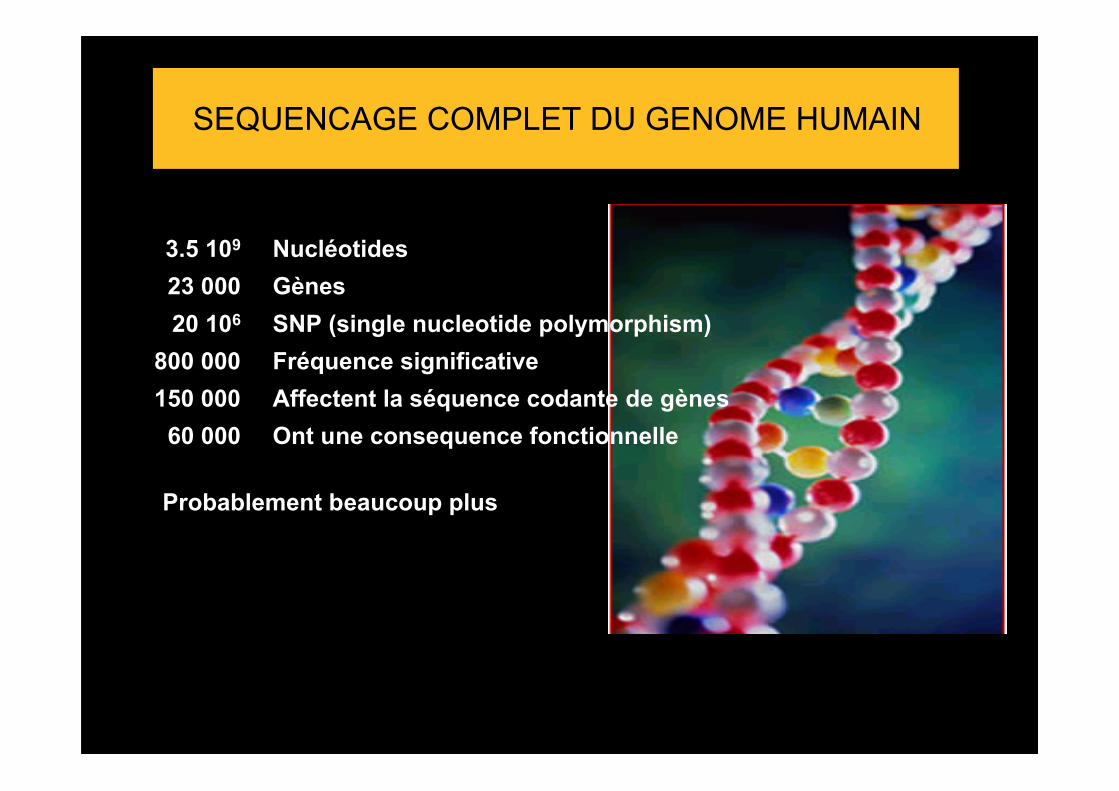
SEQUENCAGE COMPLET DU GENOME HUMAIN
3.5 109
23 00020 106
800 000150 000
60 000
NucléotidesGènesSNP (single nucleotide polymorphism)Fréquence significativeAffectent la séquence codante de gènesOnt une consequence fonctionnelle
Probablement beaucoup plus

(Constitutional) COPY NUMBER VARIATIONS (CNV)
• Very common phenomenon: 1447 CNV, 360 Mb, 12% of the human genome
• Enzyme involved in xenobiotic metabolism
Deletion: CYP2A6CYP2B6 (partial)CYP2D6GSTM1GSTT1SULT1A1SULT1A3UGT2B7UGT2B10UGT2B11UGT2B17
Amplification: CYP2A6CYP2D6SULT1A1SULT1A3

Kinases Phosphatases
Protein arginineMethyltransferases
PRMT1
Histoneacetyltransferases
HAT HDAC Histone Deacetylases
HistoneDemethylases
HDM
HistoneMethylTransferases
HMT
DNA methylases DNM
HistoneN-terminal tail
(25-40 AA)
Methylation Phosphorylation Methylation Acetylation Lys Ser/Thr Arg Cit Lys
PADI demethyliminates
DNA
nucleosome
DNA methylation
Histone modification
EPIGENETIC MECHANISMS • DNA Methylation• Histone modification• Micro RNA
CpG islands
MTHFR
Folates
Homocysteine SAM
S-adenosyl methionine
SAH
Methionine THF 5, 10 methylene THF
Methyl-THF
Diet
MAT
GHMT
BHMT
SAHH
methyl
Genes • Oncogenes• Tumor suppressor genes• Genes involved in cellular disposition of xenobiotics
Arsenic Cadmium
Nickel Chrome
Tabac, alcool Thè vert
Ac valproique
DNA
DNMT DNA methyltransferases Diethylstilbestrol
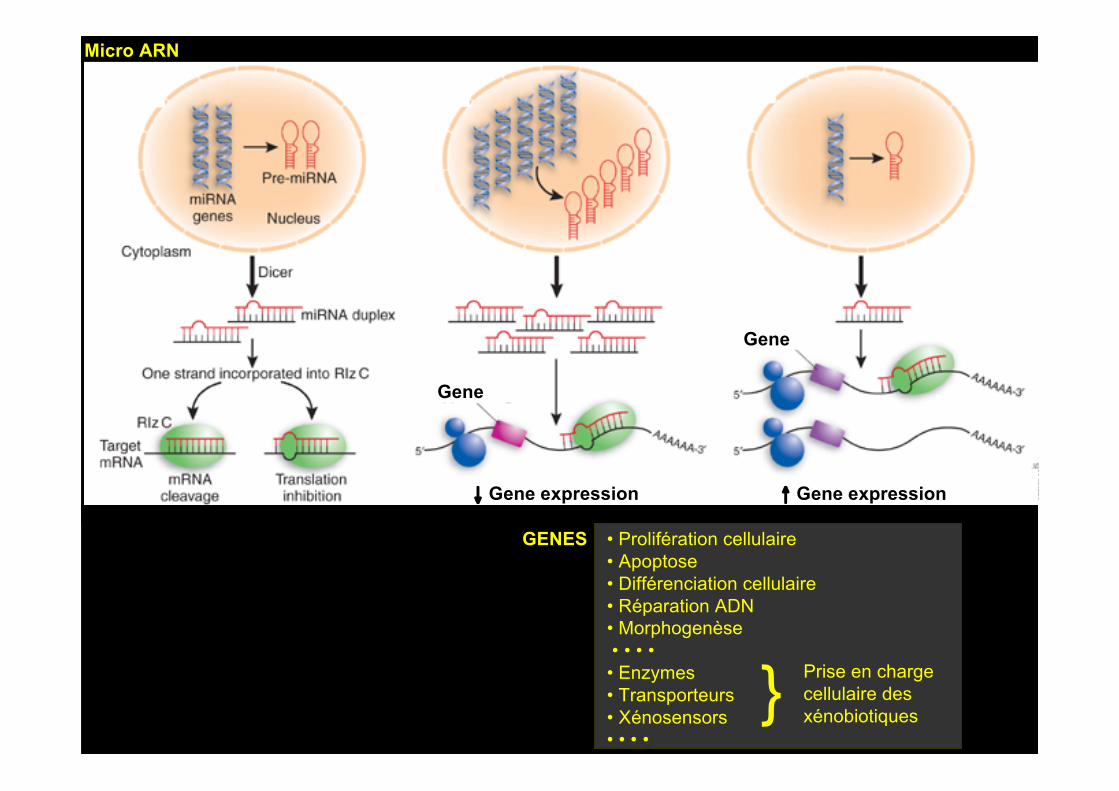
↓ Gene expression ↑ Gene expression
Gene
Gene
• Prolifération cellulaire• Apoptose• Différenciation cellulaire• Réparation ADN• Morphogenèse • • • •• Enzymes• Transporteurs• Xénosensors• • • •
Prise en chargecellulaire desxénobiotiques}
GENES
Micro ARN

Transgenerational Epigenetic Inheritance ofXenobiotic Effects
Aberrant methylation pattern of thepromoters of estrogen-responsive genes
associated with the development of reproductive organs
Reproductive tractabnormalities
XENOBIOTICEXPOSURE
Vaginal and cervical cancer at young age
Diethylstilbestrol
MOTHER DAUGHTERGRANDDAUGHTER
+
AberrantMethylationPattern Transfer
First 3 months of pregnancy

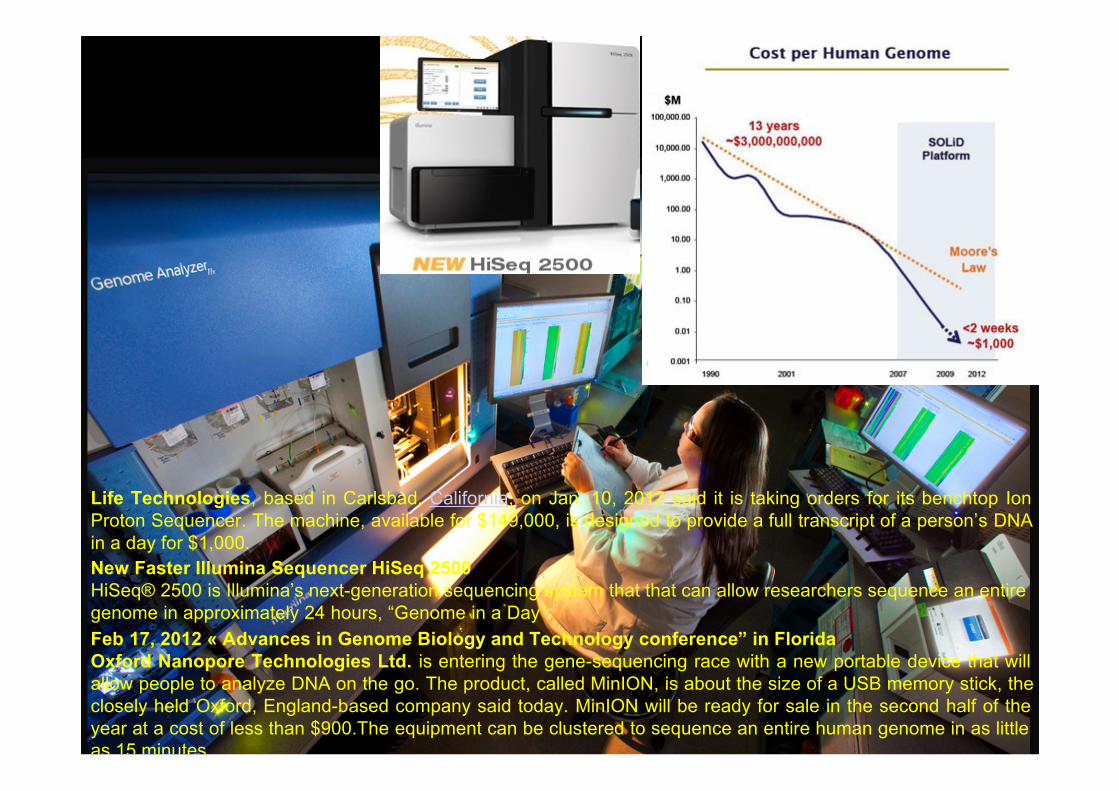
New Faster Illumina Sequencer HiSeq 2500HiSeq® 2500 is Illumina’s next-generation sequencing system that that can allow researchers sequence an entiregenome in approximately 24 hours, “Genome in a Day”.Feb 17, 2012 « Advances in Genome Biology and Technology conference” in FloridaOxford Nanopore Technologies Ltd. is entering the gene-sequencing race with a new portable device that willallow people to analyze DNA on the go. The product, called MinION, is about the size of a USB memory stick, theclosely held Oxford, England-based company said today. MinION will be ready for sale in the second half of theyear at a cost of less than $900.The equipment can be clustered to sequence an entire human genome in as littleas 15 minutes.
Life Technologies, based in Carlsbad, California, on Jan. 10, 2012 said it is taking orders for its benchtop IonProton Sequencer. The machine, available for $149,000, is designed to provide a full transcript of a person’s DNAin a day for $1,000.
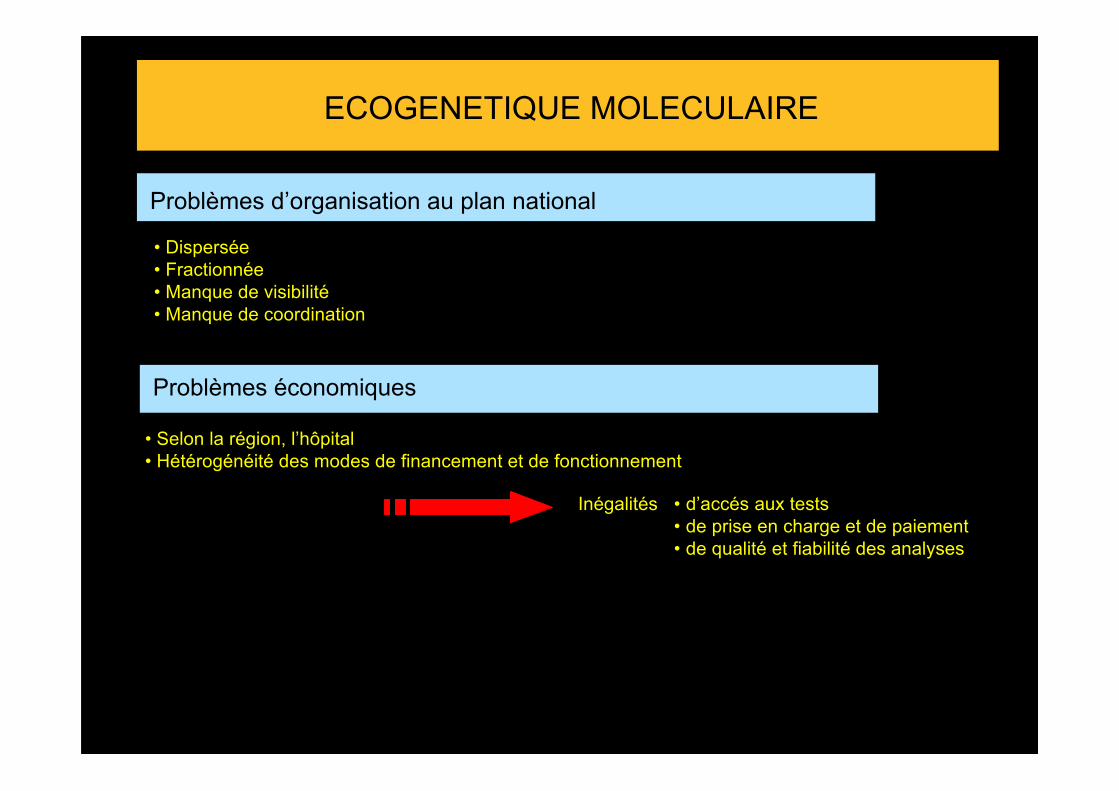
ECOGENETIQUE MOLECULAIRE
Problèmes d’organisation au plan national
• Dispersée• Fractionnée• Manque de visibilité• Manque de coordination
Problèmes économiques
• Selon la région, l’hôpital • Hétérogénéité des modes de financement et de fonctionnement
Inégalités • d’accés aux tests• de prise en charge et de paiement• de qualité et fiabilité des analyses

Considérations éthiques, légales, sociales et économiques
Proposition du test• Connaissances • Médecin
• Patient• Informations scientifiques
• Recommandations • Autorités• Industriels
• Xénobiotique / pathologie / poste• Facilités à réaliser le test• Coût de l'analyse• Responsabilités • Médicales
• Autorités
Prospectif ou Rétrospectif
Consentement éclairé écrit du patient
• Dépend de l'information que transporte le test • Pharmacogénétique• Révélatrice d'une pathologie• Facteur de risque pathologique ou autre
• Contenu va dépendre • Capacité du patient à comprendre l'information et ses conséquences• Effet psychologique du résultat du test• Informations complémentaires devront être données
Au cas par cas
Fréquence des phénotypes, pénétrance•
Considérations éthiques, légales, sociales et économiques
Réalisation de l'analyse
Qui doit faire les tests et dans quels conditions ?
• Vide juridique• Professionnel de la santé agréés dans des structures autorisées
• Possibilité d'information touchant à la santé• Difficultés d'interprétation et de fiabilité des tests
Résultats et interprétation de l'analyse
Fournis au prescripteur
Interprétés par le labo et le prescripteur • Pharmacologue ?• Généticien ?• Conseil génétique ?Utilisation du résultat
• Dépend de nb facteurs • Maladie / emploi• Traitement / emploi alternatif ou non• Thérapeutique / exposition "off-label"• Balance bénéfice / risque
• Toxicologue ?
Considérations éthiques, légales, sociales et économiques
Propriété et confidentialité de l'information
Pour le sujet • Résultats inclus dans le dossier médical• Information disponible à l'ensemble du personnel médical directement
responsable de sa santé mais appréhende la possibilité d'un accès à cesinformations par d'autres groupes sociaux
Pour la famille• Conséquences possibles Information PG+++ ex: situation d'urgence
Susceptibilité à une pathologie ou autres
Informations donnés par le médecin aux patients avec ses conséquences
Il est évident que dans certaines circonstances le médecin doitencourager le patient à donner ces informations au reste de la famille.
Autres groupes sociaux
• Inconvénients • Patient "difficile à traiter " "cher à traiter" ou "maladie sérieuse intraitable "
• Informations associées (maladie, addictions)
• Avantages • Patient pourra être traité efficacement, mieux que la population générale
• Problème de l’information révélée indirectement
• Réponse ?
• Individu "inemployable"
• Seul capable d’occuper un emploi
Inégalité face àl’environnement chimique
Conséquencesmédicales, sociales et économiques
considérables
Problème de santé publique
XENOBIOTIQUESBiosphère: 3 106 substances chimiquesIndustrie: 3 104 nouvelles/anAbsorption quotidienne: 1 104