Les marqueurs prédictifs en immunothérapie : des AMM ... · Les marqueurs prédictifs en...
79
Les marqueurs prédictifs en immunothérapie : des AMM conditionnées aux marqueurs en développement Julien Mazières, Service de Pneumologie, CHU Toulouse Université Paul Sabatier INSERM UMR1037 [email protected]
Transcript of Les marqueurs prédictifs en immunothérapie : des AMM ... · Les marqueurs prédictifs en...

Les marqueurs prédictifs en immunothérapie : des AMM conditionnées aux
marqueurs en développement
Julien Mazières, Service de Pneumologie, CHU Toulouse
Université Paul Sabatier INSERM UMR1037

Quelques idées reçues
L’immunologie est trop compliquée pour trouver un biomarqueur

Quelques idées reçues
L’immunologie est trop compliquée pour trouver un biomarqueur

Immunothérapie en oncologie thoracique Introduction Articles
262 www.thelancet.com/oncology Vol 16 March 2015
1 year was 40·8% (31·6–49·7; fi gure 3B). At the time of analysis, 72 (62%) of 117 participants had died.
We obtained pretreatment archival tumour samples for 86 (74%) of 117 participants, 76 (88%) of which could be assessed for PD-L1 expression. Median time from biopsy to start of nivolumab treatment for all collected tumour samples was 1·3 years (IQR 0·8–2·1). 25 (33%) of 76 patients had PD-L1-positive tumours (≥5% expression). Patients with PD-L1-positive tumours and those with PD-L1-negative tumours achieved an objective response, with more objective responses in patients with PD-L1-positive tumours (table 2). Almost a third of patients with unevaluable PD-L1 expression had an
objective response (table 2). The appendix shows objective response by PD-L1 status using other cutoff s. Reductions in target tumour lesion burden were more common in patients with PD-L1-positive tumours (13 [52%] of 25 patients) than in those with PD-L1-negative tumours (15 [38%] of 40; appendix).
32 (27%) of 117 patients had a dose delay, most often because of an adverse event, with 21 (66%) of 32 having only one delay. Most dose delays lasted less than 15 days. Accordingly, 99 (85%) of 117 patients received at least 90% of their planned dose intensity.
Almost three-quarters of patients reported a treatment-related adverse event of any grade; most commonly, fatigue, decreased appetite, and nausea (table 3). Grade 3–4 treatment-related adverse events occurred in about a sixth of patients, most commonly fatigue, pneumonitis, and diarrhoea (table 3). Most treatment-related immune-mediated adverse events were of low grade, with skin disorders and gastrointestinal events most prevalent (appendix). Three patients had treatment-related grade 3 diarrhoea, which resolved with either corticosteroid treatment (one patient) or supportive care. Six patients had treatment-related pneumonitis (none grade 4 or 5); one additional grade 3 pneumonitis was reported between 30 and 100 days after the last dose of nivolumab. All patients with pneumonitis were treated with corticosteroids, with a median time to resolution of 3·4 weeks (range 1·6–13·4). Four low-grade, treatment-related, renal adverse events were reported, none of which were grade 3–4. Treatment-related adverse events led to discontinuation for 14 (12%) of 117 patients: fi ve (4%) for pneumonitis, two (2%) for fatigue, and one (1%) for each of anaphylactic reaction, hypersensitivity, adrenal insuffi ciency, diarrhoea, polyneuropathy, rash, and sensory neuropathy in both hands. At time of analysis, 15 (13%) of 117 patients were on treatment.
Two deaths were attributed, by the investigator, to nivolumab. One patient died of hypoxic pneumonia 28 days after the last dose of nivolumab. This patient had rapid tumour progression and bronchial obstruction with possible associated opportunistic infection. Although this condition was distinct from pneumonitis, the investigator reported the adverse event as possibly related to nivolumab as an infl ammatory component could not be ruled out, and no bronchoscopy or autopsy was done. A second patient died of ischaemic stroke 41 days after the fi rst and only nivolumab dose. Both patients had multiple comorbidities and progressive disease (appendix).
DiscussionOur fi ndings show that nivolumab monotherapy provides clinically meaningful activity and an acceptable safety profi le for patients with advanced refractory squamous non-small-cell lung cancer. The prognosis for patients who have progressed after treatment with two or more
Figure 3: Kaplan-Meier analysis of progression-free survival (A) and overall survival (B)Progression-free survival was IRC assessed.
10090
80
70
60
0
50
40
30
20
10
15129630
Number at risk
Prog
ress
ion-
free s
urvi
val (
%)
10090
80
70
60
0
50
40
30
20
10
Over
all s
urvi
val (
%)
15129630 18
A
B
09232544117
Number at risk 528516893117
Time since start of treatment (months)
0
Partial response
Stable disease
Progressive disease
<5% (n=51) 7 (14%) 10 (20%) 25 (49%)
≥5% (n=25) 6 (24%) 6 (24%) 11 (44%)
Unevaluable (n=10) 3 (30%) 4 (40%) 2 (20%)
Data are n (%). Patients with indeterminate best overall response (n=7), and best overall response not reported by the IRC (n=5) are not included. PD-L1 expression was evaluable in all these patients, except one with best overall response not reported.
Table 2: Best overall response by PD-L1 expression status
Résistanceprimaire
Résistancesecondaire
Longsurvivants
Comment mieux faire ? Etude CHECKMATE 063 (nivolumab epidermoides
prétraités)

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI, MDSC…)
Suppression immunitaire
(PDL1, CTLA4,...)
TUMEUR
HOTE (microbiote)

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI, MDSC,…)
Suppression immunitaire
(PDL1, CTLA4,…)
TUMEUR
HOTE (microbiote)

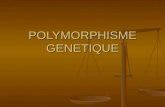
Biomarqueurs : expression de PD-L1
Kerr K, JTO 2015
• Expression de PDL1 dans le CBNPC

Tumor membrane expression Immune cells expression
PDL1 -
Strong + > 5%
PDL1 + (> 1%)
PDL1 - M0 < 1%
IHC0
PDL1 strong > 50%
PDL1 weak+ > 1%
+
-
+
-
+
-
+
-
M1 > 1%
M2 > 25%
M2 > 50%
IHC1 > 1%
IHC2 > 5%
IHC3 > 10%
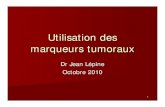
Biomarqueurs : expression de PD-L1
Guibert N, TARD 2015
DAKO 28.8
DAKO 22C3
Ventana SP263
Ventana SP142

Biomarqueurs : expression de PD-L1
Kunger, JCOPO 2018
NSCLC
Study and Cancer Type No. ofEvents
PD-L1 Positive PD-L1 Negative Odds RatioIV, Random (95% CI)
Odds RatioIV, Random (95% CI)Total No.
of PatientsNo. of
EventsTotal No.of Patients
Weight(%)
Melanoma
Bladder cancer
RCC
Gastro esophageal cancer
Head and neck cancer
Total eventsHeterogeneity: W2 = 0.03; F2 = 15.46, df = 13 (P = .28); l2 = 16%Test for overall effect: Z = 7.72 (P < .001)
Subtotal
Subtotal
2.04 (1.19 to 3.49)1,267 720 29.6
Duad et al27
Hamid et al24
Hodi et al25
Larkin et al23
Ribas et al26
Robert et al22
Robert et al28
Weber et al21
4.08 (1.70 to 9.77)118 364 6 57 3.11.45 (0.26 to 8.01)4 15 3 15 1.1
5.33 (1.16 to 24.60)8 18 3 23 1.41.92 (1.14 to 3.24)46 80 86 208 5.12.03 (1.06 to 3.89)51 193 14 93 4.32.25 (1.26 to 4.02)39 74 45 136 4.70.61 (0.39 to 0.94)154 446 47 101 5.83.03 (1.53 to 6.02)34 77 18 87 4.1
359 277
Total eventsHeterogeneity: W2 = 0.42; F2 = 31.39, df = 7 (P < .001); l2 = 78%Test for overall effect: Z = 2.59 (P = .010)
454 222
Total eventsHeterogeneity: W2 = 0.11; F2 = 7.90, df = 6 (P = .25); l2 = 24%Test for overall effect: Z = 3.07 (P = .002)
64 66
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.27, df = 3 (P = .97); l2 = 0%Test for overall effect: Z = 2.27 (P = .02)
21 19
Total eventsHeterogeneity: W2 = 0.28; F2 = 2.44, df = 2 (P = .29); l2 = 18%Test for overall effect: Z = 1.96 (P = .05)
8 6
2.51 (1.99 to 3.17)1,295 1,984 39.5
Antonia et al16
Borghaei et al15
Brahmer et al14
Fehrenbacher et al50
Garon et al12
Gettinger et al11
Gettinger et al20
Herbst et al13
Herbst et al l19
Rittmeyer et al49
Rizvi et al17
Spigel 2015Verschraegen et al18
Wakelee et al48
3.20 (0.37 to 28.01)14 49 1 9 0.74.86 (2.43 to 9.72)34 95 14 136 4.01.59 (0.60 to 4.21)9 42 11 75 2.72.37 (0.93 to 6.05)11 50 10 94 2.8
3.31 (0.96 to11.45)50 176 3 28 1.91.90 (0.42 to 8.70)5 33 3 35 1.4
2.52 (0.57 to11.10)8 26 3 20 1.40.75 (0.08 to 7.44)1 7 6 33 0.73.79 (2.51 to 5.73)86 290 40 400 5.92.73 (1.55 to 4.83)29 129 28 292 4.81.98 (0.59 to 6.70)6 25 7 51 2.01.86 (0.87 to 3.99)14 43 28 136 3.6
4.09 (0.45 to 37.53)6 28 1 16 0.71.75 (1.28 to 2.41)86 302 122 659 6.7
Subtotal 2.20 (1.33 to 3.64)14.6436221
Apolo et al35
Balar et al38
Massard et al36
Plimack et al33
Powles et al34
Rosenberg et al37
Sharma et al39
6.67 (0.97 to 45.79)0.92221041.50 (0.59 to 3.80)2.98718329
3.06 (0.79 to 11.94)1.72761575.00 (0.51 to 48.75)0.7111186
1.24 (0.37 to 4.17)2.03792163.53 (1.84 to 6.76)4.321019100260.89 (0.28 to 2.80)2.24211256
2.34 (1.12 to 4.88)Subtotal 5.413984
3.33 (0.66 to 16.85)Chouieri et al31
McDermott et al32
Motzer et al30
Topalian et al29
1.23831842.22 (0.41 to 12.18)1.1222336
2.06 (0.77 to 5.46)2.778142993.00 (0.08 to 115.34)0.31042
3.85 (1.00 to 14.75)Subtotal 2.59537
12.86 (1.03 to 161.26)Chung et al44
Le et al42
Nishina et al43
0.6461921.63 (0.36 to 7.30)1.4354234
8.67 (0.58 to 130.11)0.514152
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.01, df = 1 (P = .91); l2 = 0%Test for overall effect: Z = 2.14 (P = .03)
16 15
2.26 (0.94 to 5.45)2.52 (0.51 to12.50)2.32 (1.07 to 5.01)
Ferris et al41
Segal et al40
Subtotal 4.4
3.11.3
144
10737
123
76
5422
124
Merkel cell carcinoma
SCLC
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.08, df = 1 (P = .78); l2 = 0%Test for overall effect: Z = 1.29 (P = .20)
28 92.01 (0.70 to 5.83)Subtotal 2.82770
2.28 (0.58 to 8.95)Kaufman et al45
Nghiem et al461.61635820
1.67 (0.31 to 9.01)1.2116128
Total events
Total eventsHeterogeneity: W2 = 0.13; F2 = 65.80, df = 40 (P = .006); I2 = 39%Test for overall effect: Z = 8.12 (P < .001)
Test for subgroup differences: F2 = 1.20, df = 7 (P = .99), I2 = 0%
Heterogeneity: Not applicableTest for overall effect: Z = 1.11 (P = .27)
3 9
953 623
0.01 0.1 1
Favors PD-L1 Negative Favors PD-L1 Positive10 100
2.38 (0.52 to 10.97)Subtotal 1.45910
2.26 (1.85 to 2.75)Total 100.03,6043,060
2.38 (0.52 to10.97)Antonia et al47 1.4599103
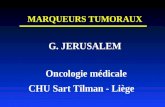
Fig 2. Forest plotsrepresenting odds ratios ofobjective response inprogrammed cell deathligand 1 (PD-L1) –positivepatients compared withPD-L1–negative patientsacross different cancertypes.NSCLC, non–small-cell lung cancer; RCC,renal cell cancer; SCLC,small-cell lung cancer.
8 ascopubs.org/journal/po JCO™ Precision Oncology
Downloaded from ascopubs.org by 193.57.201.2 on May 25, 2017 from 193.057.201.002Copyright © 2017 American Society of Clinical Oncology. All rights reserved.
NSCLC
Study and Cancer Type No. ofEvents
PD-L1 Positive PD-L1 Negative Odds RatioIV, Random (95% CI)
Odds RatioIV, Random (95% CI)Total No.
of PatientsNo. of
EventsTotal No.of Patients
Weight(%)
Melanoma
Bladder cancer
RCC
Gastro esophageal cancer
Head and neck cancer
Total eventsHeterogeneity: W2 = 0.03; F2 = 15.46, df = 13 (P = .28); l2 = 16%Test for overall effect: Z = 7.72 (P < .001)
Subtotal
Subtotal
2.04 (1.19 to 3.49)1,267 720 29.6
Duad et al27
Hamid et al24
Hodi et al25
Larkin et al23
Ribas et al26
Robert et al22
Robert et al28
Weber et al21
4.08 (1.70 to 9.77)118 364 6 57 3.11.45 (0.26 to 8.01)4 15 3 15 1.1
5.33 (1.16 to 24.60)8 18 3 23 1.41.92 (1.14 to 3.24)46 80 86 208 5.12.03 (1.06 to 3.89)51 193 14 93 4.32.25 (1.26 to 4.02)39 74 45 136 4.70.61 (0.39 to 0.94)154 446 47 101 5.83.03 (1.53 to 6.02)34 77 18 87 4.1
359 277
Total eventsHeterogeneity: W2 = 0.42; F2 = 31.39, df = 7 (P < .001); l2 = 78%Test for overall effect: Z = 2.59 (P = .010)
454 222
Total eventsHeterogeneity: W2 = 0.11; F2 = 7.90, df = 6 (P = .25); l2 = 24%Test for overall effect: Z = 3.07 (P = .002)
64 66
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.27, df = 3 (P = .97); l2 = 0%Test for overall effect: Z = 2.27 (P = .02)
21 19
Total eventsHeterogeneity: W2 = 0.28; F2 = 2.44, df = 2 (P = .29); l2 = 18%Test for overall effect: Z = 1.96 (P = .05)
8 6
2.51 (1.99 to 3.17)1,295 1,984 39.5
Antonia et al16
Borghaei et al15
Brahmer et al14
Fehrenbacher et al50
Garon et al12
Gettinger et al11
Gettinger et al20
Herbst et al13
Herbst et al l19
Rittmeyer et al49
Rizvi et al17
Spigel 2015Verschraegen et al18
Wakelee et al48
3.20 (0.37 to 28.01)14 49 1 9 0.74.86 (2.43 to 9.72)34 95 14 136 4.01.59 (0.60 to 4.21)9 42 11 75 2.72.37 (0.93 to 6.05)11 50 10 94 2.83.31 (0.96 to11.45)50 176 3 28 1.91.90 (0.42 to 8.70)5 33 3 35 1.4
2.52 (0.57 to11.10)8 26 3 20 1.40.75 (0.08 to 7.44)1 7 6 33 0.73.79 (2.51 to 5.73)86 290 40 400 5.92.73 (1.55 to 4.83)29 129 28 292 4.81.98 (0.59 to 6.70)6 25 7 51 2.01.86 (0.87 to 3.99)14 43 28 136 3.6
4.09 (0.45 to 37.53)6 28 1 16 0.71.75 (1.28 to 2.41)86 302 122 659 6.7
Subtotal 2.20 (1.33 to 3.64)14.6436221
Apolo et al35
Balar et al38
Massard et al36
Plimack et al33
Powles et al34
Rosenberg et al37
Sharma et al39
6.67 (0.97 to 45.79)0.92221041.50 (0.59 to 3.80)2.98718329
3.06 (0.79 to 11.94)1.72761575.00 (0.51 to 48.75)0.71111861.24 (0.37 to 4.17)2.03792163.53 (1.84 to 6.76)4.321019100260.89 (0.28 to 2.80)2.24211256
2.34 (1.12 to 4.88)Subtotal 5.413984
3.33 (0.66 to 16.85)Chouieri et al31
McDermott et al32
Motzer et al30
Topalian et al29
1.23831842.22 (0.41 to 12.18)1.12223362.06 (0.77 to 5.46)2.77814299
3.00 (0.08 to 115.34)0.31042
3.85 (1.00 to 14.75)Subtotal 2.59537
12.86 (1.03 to 161.26)Chung et al44
Le et al42
Nishina et al43
0.6461921.63 (0.36 to 7.30)1.4354234
8.67 (0.58 to 130.11)0.514152
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.01, df = 1 (P = .91); l2 = 0%Test for overall effect: Z = 2.14 (P = .03)
16 15
2.26 (0.94 to 5.45)2.52 (0.51 to12.50)2.32 (1.07 to 5.01)
Ferris et al41
Segal et al40
Subtotal 4.4
3.11.3
144
10737
123
76
5422
124
Merkel cell carcinoma
SCLC
Total eventsHeterogeneity: W2 = 0.00; F2 = 0.08, df = 1 (P = .78); l2 = 0%Test for overall effect: Z = 1.29 (P = .20)
28 92.01 (0.70 to 5.83)Subtotal 2.82770
2.28 (0.58 to 8.95)Kaufman et al45
Nghiem et al461.61635820
1.67 (0.31 to 9.01)1.2116128
Total events
Total eventsHeterogeneity: W2 = 0.13; F2 = 65.80, df = 40 (P = .006); I2 = 39%Test for overall effect: Z = 8.12 (P < .001)
Test for subgroup differences: F2 = 1.20, df = 7 (P = .99), I2 = 0%
Heterogeneity: Not applicableTest for overall effect: Z = 1.11 (P = .27)
3 9
953 623
0.01 0.1 1
Favors PD-L1 Negative Favors PD-L1 Positive10 100
2.38 (0.52 to 10.97)Subtotal 1.45910
2.26 (1.85 to 2.75)Total 100.03,6043,060
2.38 (0.52 to10.97)Antonia et al47 1.4599103
Fig 2. Forest plotsrepresenting odds ratios ofobjective response inprogrammed cell deathligand 1 (PD-L1) –positivepatients compared withPD-L1–negative patientsacross different cancertypes.NSCLC, non–small-cell lung cancer; RCC,renal cell cancer; SCLC,small-cell lung cancer.
8 ascopubs.org/journal/po JCO™ Precision Oncology
Downloaded from ascopubs.org by 193.57.201.2 on May 25, 2017 from 193.057.201.002Copyright © 2017 American Society of Clinical Oncology. All rights reserved.
• ExpressiondePDL1danslestumeurssolidesetréponsesauxICI:méta-analyse

Biomarqueurs : expression de PD-L1
Peters S, ASCO 2018

Biomarqueurs : expression de PD-L1
type of IHC platform (Dako or Ventana for PD-L1) may not beavailable in some pathology laboratories. Thus, in an effort toevaluate the potential use of LDT, our study simultaneously eval-uated the largest number of PD-L1 LDT to date using the mostcommonly used PD-L1 antibodies and IHC platforms available.Given that the Dako 28-8, Dako 22C3 and Ventana SP263 assays
are considered to have sufficient analytical concordance, wedefined that LDT should be able to achieve a similar concordance(e.g. based on the same statistical criteria) with one of these threeassays for tumor cell staining. Since PD-L1 is expressed as a con-tinuum of percentage and intensities, we have chosen to study theconcordance based on the most clinically relevant thresholds to
28-8 Ref. 0.94 0.79
0.820.91Ref.
0.83 0.83 0.86
0.8 0.73 0.6
0.5
0.83
0.78
0.75 0.78
0.81
0.86
0.62
0.58 28-8 (center 1)
Reference
22C3 (center 1)
SP263 (center 5)
SP263 (center 5)
SP263 (center 5)
0.77
0.45
0.81
0.81
0.81 Ref.
0.61 0.43
0.60.77
0.38
0.65
0.68
0.63
Dako
Cen
ter
1
Cen
ter
2
Cen
ter
3
Cen
ter
4
Cen
ter
5
Cen
ter
6
Cen
ter
7
Ventana Leica
22C3
SP263
SP142
E1L3N
Figure 2. Summary of comparison of laboratory-developed tests (LDTs) and reference PD-L1 assays (Ref.) selected among standardized kits(orange boxes) for tumor cells staining (weighted kappa values for the <1%, 1–49% and !50% categories). LDTs with a weighted kappa con-cordance coefficient !0.75 are considered as concordant with reference PD-L1 assays (green boxes), whereas other tests had insufficientconcordance (red boxes).
Table 1. Comparison of laboratory developped tests to selected assays according to !1% and !50% thresholds
Dako Ventana Leica Reference
Center 1 Center 2 Center 3 Center 4 Center 5 Center 6 Center 7
(A) TC 1%28-8 Reference 97.6% 95.1% 92.7% 92.7% 78.0% 78.1% 28-8 (center 1)
[87.1; 99.9] [83.4; 99.4] [80.1; 98.5] [80.1; 98.5] [62.4; 89.4] [60.0; 90.7]22C3 Reference 97.6% 92.7% 97.6% 90.2% 78.0% 82.9% 22C3 (center 1)
[87.1; 99.9] [80.1; 98.5] [87.1; 99.9] [76.9; 97.3] [62.4; 89.4] [67.9; 92.8]SP263 90.2% 92.7% 90.2% 87.8% Reference 95.1% 92.7% SP263 (center 5)
[76.9; 97.3] [80.1; 98.5] [76.9; 97.3] [73.8; 95.9] [83.4; 99.4] [80.1; 98.5]SP142 90.2% 72.5% 82.9% 78.0% 73.2% 90.2% 90.2% SP263 (center 5)
[76.9; 97.3] [56.1; 85.4] [67.9; 92.8] [62.4; 89.4] [57.1; 85.8] [76.9; 97.3] [76.9; 97.3]E1L3N 85.4% 82.5% 90.0% 82.9% 87.8% 87.8% 87.8% SP263 (center 5)
[70.8; 94.4] [67.2; 92.7] [76.3; 97.2] [67.9; 92.8] [73.8; 95.9] [73.8; 95.9] [73.8; 95.9]
(B) TC 50%28-8 Reference 97.6% 87.8% 90.2% 85.4% 85.4% 84.4% 28-8 (center 1)
[87.1; 99.9] [73.8; 95.9] [76.9; 97.3] [70.8; 94.4] [70.8; 94.4] [67.2; 94.7]22C3 Reference 95.1% 92.7% 87.8% 92.7% 80.5% 85.4% 22C3 (center 1)
[83.4; 99.4] [80.1; 98.5] [73.8; 95.9] [80.1; 98.5] [65.1; 91.2] [70.8; 94.4]SP263 95.1% 92.7% 97.6% 95.1% Reference 87.8% 90.2% SP263 (center 5)
[83.4; 99.4] [80.1; 98.5] [87.1; 99.9] [83.4; 99.4] [73.8; 95.9] [76.9; 97.3]SP142 82.9% 72.5% 82.9% 73.2% 78.0% 90.2% 92.7% SP263 (center 5)
[67.9; 92.8] [56.1; 85.4] [67.9; 92.8] [57.1; 85.8] [62.4; 89.4] [76.9; 97.3] [80.1; 98.5]E1L3N 82.9% 87.5% 90.0% 82.9% 95.1% 90.2% 92.7% SP263 (center 5)
[67.9; 92.8] [73.2; 95.8] [76.3; 97.2] [67.9; 92.8] [83.4; 99.4] [76.9; 97.3] [80.1; 98.5]
Selected reference assays across PD-L1 assays are provided in italics. Overall percentage of agreement and 95% confidence intervals are reported. PD-L1tests with an overall percentage of agreement !90% are considered as concordant with reference PD-L1 assays (bold), whereas other tests had insufficientconcordance.
Original article Annals of Oncology
4 | Adam et al.Downloaded from https://academic.oup.com/annonc/advance-article-abstract/doi/10.1093/annonc/mdy014/4812668by INSERM useron 28 March 2018
• Harmonisation du test PDL1 dans différents centres avec différents tests.
• Les tests 28-8, 22C3 et SP263 ont des performances proches. • Possibilité de développer des tests locaux.
Adam J, Annals Oncol 2018

Biomarqueurs : expression de PD-L1 • Harmonisation du test PDL1 dans différents centres avec différents
tests.
Adam J, Annals Oncol 2018
Results
Tumor cell staining
Staining of tumor cells with the standardized 22C3 DakopharmDx, 28-8 Dako pharmDx and SP263 Ventana assays wascompared. For each assay individually, we found a very high con-cordance (weighted kappa coefficient: 0.79–0.94) between centers(Figure 1). To compare results across these three assays and tocompare with LDT, we selected for each assay the results from asingle center, based on the highest mean percentage of stainedtumor cells. When comparing these three assays, we found ahigh correlation (weighted kappa coefficient: 0.71–0.89, Figures 1and 2).
The results from the 27 LDT performed in the study were eachcompared with one of the standardized PD-L1 assays. LDTs withclones 22C3, 28-8 and SP263 were compared with the selectedstandardized assay with the corresponding antibody on dedicatedplatform. The other LDTs performed with clone E1L3N andSP142 were compared with the SP263 assay, which had the high-est mean value for the percentage of staining in tumor cells. Toevaluate the analytical performance of LDTs, we considered thatthey should achieve at least a similar concordance with one ofthese three assays when compared with these three assaystogether. Based on this rule, we defined a weighted kappa con-cordance coefficient of at least 0.75 as a sufficient concordancefor selection and further validation of the test. We found that 14/27 (51.8%) of PD-L1 LDT were concordant with one of the refer-ence assays (Figure 2 and supplementary Figures S1 and S2, avail-able at Annals of Oncology online). The overall percentage ofagreement for the !1% and the !50% positivity thresholds wasvery similar to these results (Table 1). The results for the !5%,!10% and !80% thresholds are mentioned in supplementaryTable S2, available at Annals of Oncology online. In our experi-ence, low concordance was mainly related to insufficient sensitiv-ity in PD-L1 expression detection by some LDT.
Immune cell staining
Staining of immune cells was scored by pathologists trained onthe 22C3 and/or 28-8 assays but not SP142 assay, which includesthe evaluation of immune cells. The overall percentage of agree-ment for the !1%, !5% and !10% positivity thresholds waspoor when comparing 28-8, 22C3 and SP263 assays as well aswhen comparing LDT to these assays (supplementary Table S3,available at Annals of Oncology online).
Discussion
PD-L1 expression by IHC has been assessed in all clinical trialsevaluating efficacy of anti-PD-1 and anti-PD-L1 agents. Ourstudy and others [11–14] have shown that the Dako 28-8pharmDx, Dako 22C3 pharmDx and Ventana SP263 assays havea very close analytical performance for the staining of tumor cellsin NSCLC samples. This finding is very important since it indi-cates that these three tests may be interchangeable for PD-L1 test-ing on tumor cells and that a single PD-L1 test could beperformed for the three drugs associated with these assays in clin-ical trials (nivolumab, pembrolizumab and durvalumab, respec-tively). In particular, given the high proportion of pathologylaboratories using Ventana platform across many countries, theSP263 assay may be used as a complementary diagnostic test fornivolumab and companion diagnostic test for pembrolizumab asapproved by the FDA. We did not study the Ventana SP142 assay,but several of these studies [11, 14] have shown that it stained asignificantly lower proportion of tumor cells.
The introduction of ready-to-use, highly standardized, assayshas been in past years an improvement in the quality of predictiveIHC, for instance for HER2 testing. Even if these assays were usedin clinical trials, several issues may prevent pathologists fromusing them and lead to development of LDT instead. In particu-lar, these assays are much more expensive, reimbursement forPD-L1 testing is insufficient in many countries and the adequate
100
80
60
% T
umor
sta
inin
g
40
20
00 5 10 15 20 25
Cases30 35 40 45
28.8
R2 = 0,9344R2 = 0,9478R2 = 0,8864
22C3SP263
Figure 1. Comparison of tumor cells staining with the selected 22C3, 28-8 and SP263 assays.
Annals of Oncology Original article
doi:10.1093/annonc/mdy014 | 3Downloaded from https://academic.oup.com/annonc/advance-article-abstract/doi/10.1093/annonc/mdy014/4812668by INSERM useron 28 March 2018

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI, MDSC,…)
Suppression immunitaire
(PDL1, CTLA4,…)
TUMEUR
HOTE (microbiote)

Microenvironnement
Les trois phénotypes histologiques observés dans les cancers
INFLAMMATOIRECellules-T CD8+
infiltrées mais non-fonctionnelles
EXCLUSION IMMUNECellules-T CD8+
accumulées mais n’ont pas infiltré la tumeur
DESERT IMMUNCellules-T CD8+
absentes de la tumeur et de sa périphérie
Hegde et al. CCR 2016

Statut immunologique
(Fehrenbacher L, Lancet 2016)
• Etude IMPower Chimio + Beva +/- atezo • Intérêt du Teff: The T-effector (Teff) gene signature is
defined by expression of PD-L1, CXCL9 and IFNγ.
Reck M, et al. IMpower150 PFS analysis. 8 The T-effector (Teff) gene signature is defined by expression of PD-L1, CXCL9 and IFNγ and is a surrogate of both PD-L1 IHC expression and pre-existing immunity (Kowanetz M, et al. WCLC, 2017).
IMpower150 study populations and objectives
ITT All randomised
patients
Teff-high WTa High T-effector gene signature expression
Teff-low WTa Low T-effector gene signature expression
Co-primary objectives • Investigator-assessed PFS in ITT-WT • Investigator-assessed PFS in Teff-high WT • OS in ITT-WT
1 EGFR/ALK +
(13% of patients)
ITT-WTa
(87% of patients) a WT refers to patients without EGFR
or ALK genetic alterations.

Statut immunologique
(Fehrenbacher L, Lancet 2016)
• Intérêt du Teff: The T-effector (Teff) gene signature is defined by expression of PD-L1, CXCL9 and IFNγ.
Reck M, et al. IMpower150 PFS analysis. 16 INV, investigator. Data cutoff: September 15, 2017
INV-assessed PFS in Teff-high WT (Arm B vs Arm C)
6.8 mo (95% CI: 5.9, 7.4)
11.3 mo (95% CI: 9.1, 13.0)
HR, 0.505 (95% CI: 0.377, 0.675) P < 0.0001
Minimum follow-up: 9.5 mo
Landmark PFS, % Arm B: atezo + bev + CP
Arm C: bev + CP
6-month 72% 57%
12-month 46% 18%

Statut immunologique
Reck M, ESMO-IO 2017
• Intérêt du Teff: The T-effector (Teff) gene signature is defined by expression of PD-L1, CXCL9 and IFNγ.
Reck M, et al. IMpower150 PFS analysis. 18
a ITT, EGFR/ALK mutants, and ITT-WT % prevalence out of ITT (n = 800); Teff % prevalence out those tested in ITT-WT (n = 658); PD-L1 IHC % prevalence out of ITT-WT (n = 692). b Patients with a sensitising EGFR mutation or ALK translocation must have disease progression or intolerance of treatment with one or more approved targeted therapies. c Stratified HRs for ITT, ITT-WT and Teff-high WT populations; unstratified HRs for all other subgroups. Data cutoff: September 15, 2017
PFS in key biomarker populations
0.25
Population n (%)a
ITT (including EGFR/ALK mutant +) 800 (100%) EGFR/ALK mutant + onlyb 108 (14%) ITT-WT 692 (87%)
Teff-high (WT) 284 (43%)
Teff-low (WT) 374 (57%)
PD-L1 IHC TC2/3 or IC2/3 (WT) 244 (35%) PD-L1 IHC TC1/2/3 or IC1/2/3 (WT) 354 (51%) PD-L1 IHC TC0 and IC0 (WT) 338 (49%)
PD-L1 IHC TC3 or IC3 (WT) 135 (20%) PD-L1 IHC TC0/1/2 or IC0/1/2 (WT) 557 (80%)
Median PFS, mo
1.0
In favour of Arm C: bev + CP
Hazard Ratioc In favour of Arm B:
atezo + bev + CP
0.61 0.59
0.76
0.48 0.50
0.77
0.51
0.62
1.25
0.39 0.68
Arm B Arm C 8.3 6.8 9.7 6.1 8.3 6.8
11.3 6.8 7.3 7.0
11.1 6.8 11.0 6.8 7.1 6.9
12.6 6.8 8.0 6.8

Statut immunologique
Mezquita L, JAMA Oncol 2018
• LIPI score (Lung Immune Prognostic Index) : dLNR (Leucocytes/Leuco-Neutro et LDH)
data were missing for 7% and 3% of the population, respec-tively. Overall, PD-L1 status was positive in 96 patients (21%),negative in 33 (7%) and not available in 337 patients (72%). Thehigh rate of missing PD-L1 status was due to the fact that it wasnot mandatory for ICI prescription. The median number of priorlines of therapy administered before ICI therapy was 1 (range,0-11). The overall response rate with ICI was 27% (n = 126 pa-tients), and 32 patients (7%) had additional atypical or disso-ciated response patterns.
The LIPI was evaluable for 431 patients, giving 63 pa-tients (15%) in the poor group, 206 (48%) in the intermediategroup, and 162 (38%) in the good LIPI group. Median OS was10.1 months (95% CI, 9.0-11.7 months) and median PFS was 4.0months (95% CI, 3.4-5.0 months).
Median OS was 4.8 (95% CI, 3.6-7.7) vs 10.0 (95% CI,7.3-12.6) vs 16.5 (95% CI, 11.4-34.0) months for the poor,intermediate, and good LIPI groups, respectively (Figure,A), and median PFS was 2.0 (95% CI, 1.7-4.0) vs 3.7 (95% CI,3.0-4.8) vs 6.3 (95% CI, 5.0-8.0) months (both P < .001)(Figure, B).
The role of dNLR greater than 3 and LDH greater than ULNwere further validated with a resampling bootstrap proce-dure (1000 replications) in which all statistical analyses werereplicated on each bootstrapped sample (Table 1), with this in-ternal validation procedure reflecting the robustness of the fi-nal model. A dNLR greater than 3 and LDH greater than ULNwere associated with significantly shorter OS (HR, 1.70; 95%CI, 1.27-2.28; P < .001 and HR, 1.36; 95% CI, 1.02-1.83; P = .04,respectively). No differences were observed in our cohort ac-cording to PD-L1 expression (positive/negative/unknown)in terms of PFS and OS.
The LIPI was also correlated with response rate (P < .001).In a multivariate analysis, the intermediate and poor groupswere associated with progressive disease, with an OR of 2.20(95% CI, 1.26-3.84; P = .005) and 3.04 (95% CI, 1.46-6.36;P = .003), respectively (Table 2).
Analysis of OS according to population subgroups re-vealed significant correlations with the LIPI group, regard-less of histologic subtype (eFigure 4 in the Supplement) andage (eFigure 5 in the Supplement). In the smoker population,
Figure. Overall Survival (OS) and Progression-Free Survival (PFS) According to Lung Immune Prognostic Index (LIPI) Groups,in the Immunotherapy Pooled Cohort and in the Chemotherapy Cohort
OS in the immunotherapy pooled cohortA PFS in the immunotherapy pooled cohortB
1.0
0.8
0.6
0.4
0.2
0Pr
opor
tion
Surv
ivin
g0 05 10 15 20 25 30 35 40 45
Time, moNo. at risk
Good LIPIIntermediate LIPIPoor LIPI
118125
29
162206
63
697213
1215
2
3428
5
791
551
320
310
000
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n Su
rviv
ing
5 10 15 20 25 30 35 40 45Time, mo
No. at riskGood LIPIIntermediate LIPIPoor LIPI
847518
3638
5
162206
63
2018
1
260
681
120
020
010
000
P < .001
OS in the chemotherapy cohortC
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n Su
rviv
ing
0 10 20 30 40 50Time, mo
No. at riskGood LIPIIntermediate LIPIPoor LIPI
2430
9
537034
1391
341
220
000
PFS in the chemotherapy cohortD
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n Su
rviv
ing
0 10 20 30 40 50Time, mo
No. at riskGood LIPIIntermediate LIPIPoor LIPI
712
2
506425
420
110
100
000
P = .10 P = .37
P < .001
Good LIPIIntermediate LIPIPoor LIPI
Research Original Investigation Lung Immune Prognostic Index for Advanced Non–Small Cell Lung Cancer
E4 JAMA Oncology Published online January 11, 2018 (Reprinted) jamaoncology.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by Univ of Toulouse 3, julien mazieres on 01/15/2018
Immunothérapie
Chimiothérapie

Statut immunologique
Krieg C, Nature Medicine 2018
• Analyse single-cell et prédiction de la réponse aux anti PD1
• Caractérisation de l’infiltrat immunitaire dans le sang périphérique • Réponse au niveau du compartiment lymphocytaire
A R T I C L E S
150 VOLUME 24 | NUMBER 2 | FEBRUARY 2018 NATURE MEDICINE
0
25
50
75
100
Norm. median expression ResponseNR
–2+2 0
Norm. median expression
–2+2 0
R
T cells
B cells
CD14– myeloid cells
CD14+ myeloid cells
NK cells
cDC
pDC
CD64CD141CD38
Response
CD11bICAM-1CD33CD14PD-L1CD16CD303CD66bHLA-DRCD86CD45CD11cCD123CD1cCD34CD61CD62LCD209
Response
Before After
Global differential myeloid marker expression
CD86 (7.09 × 10–5)
HLA-DR (7.09 × 10–5)
CD141 (7.09 × 10–5)
ICAM-1 (1.01× 10–4)
CD11c (1.01 × 10–4)
PD-L1 (1.03 × 10–4)
CD38 (7.53 × 10–4)
CD16 (7.53 × 10–4)
CD33 (2.49 × 10–3)
CD11b (5.36 × 10–3)
CD303 (1.74 × 10–2)
CD62L (2.19 × 10–2)
CD1c (2.52 × 10–2)
CD64 (2.65 × 10–2)
CD14 (3.72 × 10–2)
CD34 (4.13 × 10–2)
Fre
quen
cy in
PB
MC
(%
)
Beforea
b
c
HD NR R HD NR R
After
ResponseNRR
Figure 5 Patient stratification based on myeloid cell markers and expansion of classical monocytes in responders. (a) Cell population composition in the PBMCs of healthy donors (HD, n = 20), nonresponders (NR, n = 18) and responders (R, n = 22) before and after the initiation of anti-PD-1 therapy. (b) Heat map for patient stratification on the basis of normalized median marker expression, with dendrograms for expression markers (rows) and samples (columns). Bars at the top of the heat map represent individual samples from responders (green) and nonresponders (pink) from the two time points i.e., before or after therapy (n = 39; one baseline sample with a cell count <50 was excluded from further differential expression analysis). (c) Heat map of normalized median expression of markers that were significantly (adjusted p-value < 0.05) differentially expressed between responders and nonresponders before and 12 weeks after therapy initiation, as in Figure 1c, in the myeloid compartment (CD3−CD19−) (n = 39). Bars at the top of the heat maps represent individual samples from responders (green) and nonresponders (pink). Numbers in brackets show adjusted p-values.

Statut immunologique
Delaunay M, ASCO-SITC 2018
• Cellules myéloïdes circulantes: m-MDSC
High M-MDSC
Low m-MDSC
Overallsurvival
M-MDSC
e-MDSC
Low e-MDSC
High e-MDSC
PMN-MDSC
Low PMN-MDSC
High PMN-MDSC
%e-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI]0.97[0.80;1.17] P=0.74
Progressionfree-survival HR[95%CI]0.94[0.80;1.10] P=0.45
%PMN-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI]1.01[0.85;1.21] P=0.89
Progressionfree-survival HR[95%CI]1.03[0.90;1.19 P=0.64
%M-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI][1.01;1.14] P=0.02
Progressionfree-survival HR[95%CI]08 [1.03; 1.15] P=0.004
Marvel and Gabrilovich, J clin invest 2015

Statut immunologique
Delaunay M, ASCO-SITC 2018
• Cellules myéloïdes circulantes: m-MDSC • Faible taux de m-MDSC associé à une meilleure survie
des patients traités par immunothérapie
High M-MDSC
Low m-MDSC
Overallsurvival
M-MDSC
e-MDSC
Low e-MDSC
High e-MDSC
PMN-MDSC
Low PMN-MDSC
High PMN-MDSC
%e-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI]0.97[0.80;1.17] P=0.74
Progressionfree-survival HR[95%CI]0.94[0.80;1.10] P=0.45
%PMN-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI]1.01[0.85;1.21] P=0.89
Progressionfree-survival HR[95%CI]1.03[0.90;1.19 P=0.64
%M-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI][1.01;1.14] P=0.02
Progressionfree-survival HR[95%CI]08 [1.03; 1.15] P=0.004
High M-MDSC
Low m-MDSC
Overallsurvival
%M-MDSCatbaseline(Coxproportionalhazardsmodelforcontinuousvariables)
Overallsurvival HR[95%CI]1.08[1.01;1.14] P=0.02
Progressionfree-survival HR[95%CI]0.8 [1.03; 1.15] P=0.004
M-MDSC

Microenvironnement
• Importance de la présence de lymphocytes CD8 à proximité de la tumeur (Exemple dans le mélanome traité par pembrolizumab)
the response group, pSTAT1 expression was also found to be significantlyhigher during treatment when compared to baseline (P 5 0.007) (Ex-tended Data Fig. 3e). These findings prompted us to investigate the as-sociation between CD81-, CD41-, PD-11- and PD-L11-cell densitiesin baseline biopsies in regards to response to treatment (Fig. 3a). The re-sponse group was associated with significantly higher numbers of CD81,PD-11 and PD-L11 cells at both the invasive margin and the tumourcentre when compared to the progression group (CD8, P , 0.0001; PD-1,P 5 0.0002; PD-L1, P 5 0.006). However, CD4 expression at baseline wasnot found to correlate with treatment outcome. No relationship was foundbetween previous treatment history with ipilimumab (anti-CTLA4) andCD8 expression or treatment outcome (Extended Data Table 3).
We next determined the relative proximity of PD-1 and PD-L1 asevidence of a physical interaction between PD-11 and PD-L11 cells, apresumptive requisite for adaptive immune resistance. Figure 3b showsrepresentative examples of chromogenic PD-1 and PD-L1 expressionin serially cut tissue sections as well as multiplexed PD-1 3 PD-L1 immu-nofluorescence in pre-treatment samples according to treatment outcome.Using quantitative multiplexed PD-1 3 PD-L1 immunofluorescence,we found a significant correlation between proximity of PD-1 and PD-L1 and response to therapy (Fig. 3c; P 5 0.005).
We next investigated the relationship between CD8 and PD-L1 usinga Spearman’s correlation analysis and found the two markers to corre-late in both the tumour (Spearman r 5 0.598, P , 0.001) and the invasive
Tumour Invasive margin
Before Tx Days +20–60
CD
8
Progression (N = 24)
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
Tumoura Invasive margin
Before Tx Days +20–60
CD
8+ de
nsity
(cel
ls m
m–2
)
CD
8
Response (N = 22)
b
c
d
CD
8+ de
nsity
(cel
ls m
m–2
)464
060
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Figure 1 | Immunohistochemical analysis of CD8 1 T cells in samplesobtained before and during pembrolizumab treatment. a, b, Examples ofCD8 expression in melanoma tumours serially biopsied before PD-1 blockingtreatment (Tx) and 20–60 days after treatment began (Days 120–60) from apatient in the response (a) and progression (b) groups. Red line separatestumour parenchyma (below line) and invasive margin (above line).
Magnification, 320. c, d, CD81-cell density at the tumour parenchyma andinvasive margin in samples from all responders (c; n 5 13) and progressors(d; n 5 12) who received a biopsy before and during treatment. Filled circleindicates complete response; open circle indicates partial response; triangleindicates delayed response.
Tumour
Invasive margin
Ki6
7 ×
CD
8
Prophase Metaphase Anaphase Telophase
a b
0.01 mm
0.01 mm 0.01 mm 0.01 mm 0.01 mm
Figure 2 | Regressing tumours during treatment are associated withproliferating CD8 1 T cells that localize to the tumour. a, Representativeexample of CD8/Ki67 chromogenic double staining from a sample obtainedduring tumour regression shows double-positive T cells localized to the tumourparenchyma. The red line separates the invasive margin (above line) and
tumour (below line). b, Top, representative single-positive quiescentCD81 brown cells (no Ki67 labelling) from the invasive margin. Bottom,representative double-positive cells (red, labelled Ki67 nucleus; brown, labelledCD8 membrane) with characteristic chromatin patterns associated withsub-phases of mitosis. Magnification, 340.
LETTER RESEARCH
2 7 N O V E M B E R 2 0 1 4 | V O L 5 1 5 | N A T U R E | 5 6 9
Macmillan Publishers Limited. All rights reserved©2014
the response group, pSTAT1 expression was also found to be significantlyhigher during treatment when compared to baseline (P 5 0.007) (Ex-tended Data Fig. 3e). These findings prompted us to investigate the as-sociation between CD81-, CD41-, PD-11- and PD-L11-cell densitiesin baseline biopsies in regards to response to treatment (Fig. 3a). The re-sponse group was associated with significantly higher numbers of CD81,PD-11 and PD-L11 cells at both the invasive margin and the tumourcentre when compared to the progression group (CD8, P , 0.0001; PD-1,P 5 0.0002; PD-L1, P 5 0.006). However, CD4 expression at baseline wasnot found to correlate with treatment outcome. No relationship was foundbetween previous treatment history with ipilimumab (anti-CTLA4) andCD8 expression or treatment outcome (Extended Data Table 3).
We next determined the relative proximity of PD-1 and PD-L1 asevidence of a physical interaction between PD-11 and PD-L11 cells, apresumptive requisite for adaptive immune resistance. Figure 3b showsrepresentative examples of chromogenic PD-1 and PD-L1 expressionin serially cut tissue sections as well as multiplexed PD-1 3 PD-L1 immu-nofluorescence in pre-treatment samples according to treatment outcome.Using quantitative multiplexed PD-1 3 PD-L1 immunofluorescence,we found a significant correlation between proximity of PD-1 and PD-L1 and response to therapy (Fig. 3c; P 5 0.005).
We next investigated the relationship between CD8 and PD-L1 usinga Spearman’s correlation analysis and found the two markers to corre-late in both the tumour (Spearman r 5 0.598, P , 0.001) and the invasive
Tumour Invasive margin
Before Tx Days +20–60
CD
8
Progression (N = 24)
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
500
2,000
3,500
5,000
6,500
8,000
9,500
11,000
Tumoura Invasive margin
Before Tx Days +20–60
CD
8+ de
nsity
(cel
ls m
m–2
)
CD
8
Response (N = 22)
b
c
d
CD
8+ de
nsity
(cel
ls m
m–2
)
464
060
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Before
Tx Days
+20–6
0Day
s
+80–1
20Day
s
>120
Figure 1 | Immunohistochemical analysis of CD8 1 T cells in samplesobtained before and during pembrolizumab treatment. a, b, Examples ofCD8 expression in melanoma tumours serially biopsied before PD-1 blockingtreatment (Tx) and 20–60 days after treatment began (Days 120–60) from apatient in the response (a) and progression (b) groups. Red line separatestumour parenchyma (below line) and invasive margin (above line).
Magnification, 320. c, d, CD81-cell density at the tumour parenchyma andinvasive margin in samples from all responders (c; n 5 13) and progressors(d; n 5 12) who received a biopsy before and during treatment. Filled circleindicates complete response; open circle indicates partial response; triangleindicates delayed response.
Tumour
Invasive margin
Ki6
7 ×
CD
8
Prophase Metaphase Anaphase Telophase
a b
0.01 mm
0.01 mm 0.01 mm 0.01 mm 0.01 mm
Figure 2 | Regressing tumours during treatment are associated withproliferating CD8 1 T cells that localize to the tumour. a, Representativeexample of CD8/Ki67 chromogenic double staining from a sample obtainedduring tumour regression shows double-positive T cells localized to the tumourparenchyma. The red line separates the invasive margin (above line) and
tumour (below line). b, Top, representative single-positive quiescentCD81 brown cells (no Ki67 labelling) from the invasive margin. Bottom,representative double-positive cells (red, labelled Ki67 nucleus; brown, labelledCD8 membrane) with characteristic chromatin patterns associated withsub-phases of mitosis. Magnification, 340.
LETTER RESEARCH
2 7 N O V E M B E R 2 0 1 4 | V O L 5 1 5 | N A T U R E | 5 6 9
Macmillan Publishers Limited. All rights reserved©2014
Tumeh, PC, Nature 2014

Études qualitatives et multiparamétriques
Faible infiltrat lymphocytairePD-L1 élevé (rouge)
Carcinome malpighien ORL
Fort infiltrat lymphocytaire PD-L1 bas (rouge), violet
CD8 jaune, FOXP3 vert, CD79a (B) violet, Macrophages CD163 orange
Z Feng - 2016Digitalcommons.ohsu.edu/cgi/
Microenvironnement
• Co-infiltration de cellules immunitaires dans les tumeurs PDL1 +. (Exemple dans le CBNPC traité par atezolizumab)
• Exemple K ORL
Herbst R, Nature 2014
Four more patients had unconfirmed responses (Table 2, Fig. 2 and Ex-tended Data Fig. 3a). Responses could also be rapid and durable (Fig. 2band Extended Data Fig. 3a), with shrinking or resolving palpable lesionsdetected within days in some responders and nearly all responders (es-pecially patients with NSCLC) continuing to respond and staying onstudy. In addition, RECIST may not accurately describe the full spectrum
of responses observed because some patients who had a best responseof progressive disease per RECIST went on to develop durable tumourshrinkage or prolonged stable disease (pseudoprogression)17. The med-ian progression-free survival of all patients was 18 weeks. We also per-formed an exploratory analysis of patients with NSCLC and detected apotential trend of former/current smokers responding better to MPDL-3280A versus never smokers (11 of 26 (42%) versus 1 of 10 (10%), re-spectively; P 5 0.4229 using a Fisher exact test; see the accompanyingpaper (ref. 18) for further discussion).
There appears to be an association between response and the expres-sion of PD-L1 in pre-treatment samples (Fig. 3 and Extended Data Figs 3and 4). The association of response to MPDL3280A treatment andtumour-infiltrating immune cell PD-L1 expression reached statisticalsignificance (NSCLC, P 5 0.015 (Fig. 3a and Extended Data Fig. 4a); alltumours, P 5 0.007 (Fig. 3b, c and Extended Data Fig. 4b)), while the as-sociation with tumour cell PD-L1 expression did not (NSCLC, P 5 0.920(Extended Data Fig. 4c); all tumours, P 5 0.079 (Extended Data Fig. 4d)).
Indication n Percentage of PD-L1 positive (IC) Percentage of PD-L1 positive (TC)
NSCLC 184 26 24 RCC 88 25 10 Melanoma 58 36 5 HNSCC 101 28 19 Gastric cancer 141 18 5 CRC 77 35 1 Pancreatic cancer 83 12 4
a PD-L1 prevalence determined with a Genentech/Roche anti-PD-L1 IHC assay
b
PD-L1 negative
c PD-L1/CD163 PD-L1/CD11c
PD-L1/CD3 PD-L1/CK
PD-L1 positive (IC) PD-L1 positive (TC) PD-L1 positive (TC and IC)
Figure 1 | Programmed death-ligand 1 (PD-L1) prevalence and expression.a, PD-L1 prevalence by immunohistochemistry (IHC) in samples collected forPCD4989g. PD-L1 positivity was defined as $5% of tumour-infiltratingimmune cells (ICs) or tumour cells (TCs) staining for PD-L1 by IHC.b, Representative images of PD-L1 by IHC (brown) in tumours from patientswith non-small cell lung cancer (NSCLC). The PD-L1-negative image is at203 magnification, other images at 403 magnification. c, Co-localizationof PD-L1 with selected tumour-infiltrating immune cell and tumour cellmarkers by immunofluorescence in NSCLC and melanoma tumours. PD-L1staining in red; markers of tumour-infiltrating immune cells and tumourcells in green; and DAPI staining in blue. Areas of overlap are indicated withwhite arrowheads. All four images are at 403 resolution. Markers of tumour-infiltrating immune cells: CD163 (macrophages), CD11c (dendritic cells)and CD3 (T cells). Marker of tumour cells: cytokeratin (CK). CRC, colorectalcancer; HNSCC, head and neck squamous cell carcinoma; NSCLC, non-smallcell lung cancer; RCC, renal cell carcinoma.
Table 1 | Adverse eventsTreatment-related AEs (n 5 277) AEs regardless of attribution (n 5 277)
Events ($4% of patients) Any grade (n (%)) Grade 3–4 (n (%)) Events ($5% of patients) Any grade (n (%)) Grade 3–4 (n (%))
Any AE 194 (70.0) 35 (12.6) Any AE 263 (94.9) 108 (39.0)Fatigue 67 (24.2) 5 (1.8) Fatigue 100 (36.1) 9 (3.2)Decreased appetite 33 (11.9) – Nausea 69 (24.9) 2 (0.7)Nausea 32 (11.6) 1 (0.4) Dyspnoea 66 (23.8) 11 (4.0)Pyrexia 32 (11.6) 2 Decreased appetite 64 (23.1) –Diarrhoea 29 (10.5) 2 Cough 60 (21.7) –Rash 29 (10.5) 2 Diarrhoea 60 (21.7) –Pruritus 23 (8.3) 2 Pyrexia 57 (20.6) –Arthralgia 22 (7.9) 2 Constipation 55 (19.9) –Headache 21 (7.6) 1 (0.4) Headache 49 (17.7) –Chills 19 (6.9) 2 Vomiting 46 (16.6) –Influenza-like illness 16 (5.8) 1 (0.4) Anaemia 44 (15.9) 10 (3.6)Asthenia 15 (5.4) 2 (0.7) Insomnia 43 (15.5) –Dyspnea 15 (5.4) 2 (0.7) Back pain 42 (15.2) 4 (1.4)Pain 15 (5.4) 1 (0.4) Arthralgia 41 (14.8) –Myalgia 13 (4.7) 2 Rash 40 (14.4) –Anaemia 12 (4.3) 2 (0.7) Asthenia 34 (12.3) 4 (1.4)Dry skin 12 (4.3) 2 Pruritus 33 (11.9) –Night sweats 12 (4.3) 2 Chills 31 (11.2) –Vomiting 11 (4.0) 1 (0.4) Upper respiratory tract infection 30 (10.8) –Other grade 3–4 AEs, $2 patients Anxiety 20 (7.2) –ALT increased 6 (2.2) 3 (1.1) Influenza-like illness 20 (7.2) –AST increased 4 (1.4) 3 (1.1) Nasal congestion 20 (7.2) –Hypoxia 4 (1.4) 3 (1.1) Urinary tract infection 20 (7.2) 3 (1.1)Hyperglycaemia 4 (1.4) 2 (0.7) Dehydration 19 (6.9) 4 (1.4)Hyponatraemia 4 (1.4) 2 (0.7) Hyperglycaemia 19 (6.9) 7 (2.5)Cardiac tamponade 2 (0.7) 2 (0.7) Myalgia 19 (6.9) –Hypophosphataemia 2 (0.7) 2 (0.7) Night sweats 19 (6.9) –Tumour lysis syndrome 2 (0.7) 2 (0.7) Productive cough 19 (6.9) –
Dry skin 16 (5.8) –Dry mouth 14 (5.1) –Hypoxia 14 (5.1) 6 (2.2)Weight decreased 14 (5.1) –
AE, adverse event; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
RESEARCH LETTER
5 6 4 | N A T U R E | V O L 5 1 5 | 2 7 N O V E M B E R 2 0 1 4
Macmillan Publishers Limited. All rights reserved©2014

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI,…)
Suppression immunitaire
(PDL1, CTLA4, Tregs, MDSC,...)
TUMEUR
HOTE (microbiote)

Charge mutationnelle et néo-antigènes
• Les peptides mutés issus de mutations de l’ADN sont reconnus par les lymphocytes T CD8+ et CD4+
• La réponse des lymphocytes T à ces néo-antigènes contribue à la réponse clinique à l’immunothérapie
Robbins PF, Nat Med 2013 Linneman C, Nat Med 2014
Schumacher TN, Cancer Cell 2015

Charge mutationnelle et néo-antigènes
• Analyse de la réponse au pembrolizumab dans le CBNPC selon la charge mutationnelle.
Rizvi N, Science 2015
NDB (Mann-Whitney P = 0.01 for both) (fig. S5).A previously validated binary classifier to identi-fy the molecular signature of smoking (17) wasapplied to differentiate transversion-high (TH,smoking signature) from transversion-low (TL,never-smoking signature) tumors. Efficacy wasgreatest in patients with tumors harboring thesmoking signature. The ORR in TH tumors was56% versus 17% in TL tumors (Fisher’s exact P =0.03); the rate of DCBwas 77% versus 22% (Fisher’sexact P = 0.004); the PFS was also significantlylonger in TH tumors (median not reached versus3.5 months, log-rank P = 0.0001) (Fig. 2A). Self-reported smoking history did not significantlydiscriminate those most likely to benefit frompembrolizumab. The rates of neither DCB norPFS were significantly different in ever-smokersversus never-smokers (Fisher’s exact P = 0.66 andlog-rank P = 0.29, respectively) or heavy smokers(median pack-years >25) versus light/never smokers(pack-years ≤25) (Fisher’s exact P = 0.08 and log-rank P = 0.15, respectively). Themolecular smokingsignature correlated more significantly with non-
synonymous mutation burden than smoking his-tory (fig. S6, A and B).Although carcinogens in tobacco smoke are
largely responsible for the mutagenesis in lungcancers (19), the wide range of mutation burdenwithin both smokers and never-smokers impli-cates additional pathways contributing to theaccumulation of somatic mutations. We founddeleterious mutations in a number of genes thatare important in DNA repair and replication. Forexample, in three responders with the highestmutation burden, we identified deleterious mu-tations in POLD1, POLE, and MSH2 (Fig. 3). Ofparticular interest, a POLD1 E374K mutation wasidentified in a never-smoker with DCB whose tu-mor harbored the greatest nonsynonymous muta-tion burden (n = 507) of all never-smokers in ourseries. POLD1 Glu374 lies in the exonuclease proof-reading domain of Pol d (20), and mutation ofthis residue may contribute to low-fidelity repli-cation of the lagging DNA strand. Consistent withthis hypothesis, this tumor exome had a relativelylow proportion of C-to-A transversions (20%) and
predominance of C-to-T transitions (51%), similarto other POLD1 mutant, hypermutated tumors(21) and distinct from smoking-related lung can-cers. Another responder, with the greatest muta-tion burden in our series, had a C284Y mutationin POLD1, which is also located in the exonu-clease proofreading domain. We observed non-sense mutations in PRKDC, the catalytic subunitof DNA-dependent protein kinase (DNA-PK),and RAD17. Both genes are required for properDNA repair and maintenance of genomic integ-rity (22, 23).Genes harboring deleterious mutations com-
mon to four or more DCB patients and not presentin NDB patients included POLR2A,KEAP1, PAPPA2,PXDNL, RYR1, SCN8A, and SLIT3. Mutations inKRAS were found in 7 of 14 tumors from patientswith DCB compared to 1 of 17 in the NDB group,a finding that may be explained by the asso-ciation between smoking and the presence ofKRAS mutations in NSCLC (24). There were nomutations or copy-number alterations in antigen-presentation pathway–associated genes or CD274
SCIENCE sciencemag.org 3 APRIL 2015 • VOL 348 ISSUE 6230 125
0 4 8 1 2 1 6 2 0 2 40
5 0
1 0 0
0
2 0 0
4 0 0
6 0 0
8 0 0
0
2 0 0
4 0 0
8 0 0
1 2 0 0
0 5 0 1 0 00
5 0
1 0 0
0
2 0 0
4 0 0
8 0 0
1 2 0 0
# N
onsy
nony
mou
s m
utat
ions
/tum
or
Discovery Cohort Validation Cohort
# N
onsy
nony
mou
s m
utat
ions
/tum
or
All Tumors
0 4 8 1 2 1 6 2 0 2 40
5 0
1 0 0
0 4 8 1 2 1 6 2 0 2 40
5 0
1 0 0
Discovery Cohort Validation Cohort
Months
All Tumors
DCB NDB DCB NDB DCB NDB
High nonsynonymous burdenLow nonsynonymous burden
High nonsynonymous burdenLow nonsynonymous burden
High nonsynonymous burdenLow nonsynonymous burden
800
600
400
200
0
1200
800
400
200
0
100
50
0
% S
ensi
tivity
1 - % Specificity 50 100
1200
800
400
200
0 # N
onsy
nony
mou
s m
utat
ions
/tum
or
100
50
0 4 8 12 16 20 24
Months
100
50
0 4 8 12 16 20 24
Per
cent
pro
gres
sion
-fre
e
Months
100
50
0 4 8 12 16 20 24
Per
cent
pro
gres
sion
-fre
e
Per
cent
pro
gres
sion
-fre
e
Fig. 1. Nonsynonymous mutation burden associated with clinical bene-fit of anti–PD-1 therapy. (A) Nonsynonymous mutation burden in tumorsfrom patients with DCB (n = 7) or with NDB (n = 9) (median 302 versus148, Mann-Whitney P = 0.02). (B) PFS in tumors with higher nonsynony-mous mutation burden (n = 8) compared to tumors with lower nonsynony-mous mutation burden (n = 8) in patients in the discovery cohort (HR 0.19,95% CI 0.05 to 0.70, log-rank P = 0.01). (C) Nonsynonymous mutationburden in tumors with DCB (n = 7) compared to those with NDB (n = 8) inpatients in the validation cohort (median 244 versus 125, Mann-WhitneyP = 0.04). (D) PFS in tumors with higher nonsynonymous mutation burden(n = 9) compared to those with lower nonsynonymous mutation burden(n = 9) in patients in the validation cohort (HR 0.15, 95% CI 0.04 to 0.59,
log-rank P = 0.006). (E) ROC curve for the correlation of nonsynonymousmutation burden with DCB in discovery cohort. AUC is 0.86 (95% CI 0.66to 1.05, null hypothesis test P = 0.02). Cut-off of ≥178 nonsynonymous mu-tations is designated by triangle. (F) Nonsynonymous mutation burden inpatients with DCB (n = 14) compared to those with NDB (n = 17) for theentire set of sequenced tumors (median 299 versus 127, Mann-Whitney P =0.0008). (G) PFS in those with higher nonsynonymous mutation burden(n = 17) compared to those with lower nonsynonymous mutation burden(n = 17) in the entire set of sequenced tumors (HR 0.19, 95% CI 0.08-0.47,log-rank P = 0.0004). In (A), (C), and (F), median and interquartile ranges oftotal nonsynonymous mutations are shown, with individual values for eachtumor shown with dots.
RESEARCH | REPORTS
[encoding programmed cell death ligand-1 (PD-L1)]that were associated with response or resistance.
How does increased mutation burden affect tu-mor immunogenicity? The observation that non-synonymous mutation burden is associated withpembrolizumab efficacy is consistent with thehypothesis that recognition of neoantigens, formedas a consequence of somatic mutations, is impor-tant for the activity of anti–PD-1 therapy. We ex-amined the landscape of neoantigens using ourpreviously described methods (25) (fig. S7). Briefly,this approach identifies mutant nonamers with≤500 nM binding affinity for patient-specific classI human lymphocyte antigen (HLA) alleles (26, 27),which are considered candidate neoantigens (tableS6). We identified a median of 112 candidate neo-antigens per tumor (range 8 to 610), and the quan-tity of neoantigens per tumor correlated withmutation burden (Spearman r 0.91, P < 0.0001),similar to the correlation recently reported acrosscancers (28). Tumors from patients with DCB hadsignificantly higher candidate neoantigen bur-den compared to those with NDB (Fig. 4A), andhigh candidate neoantigen burden was associatedwith improved PFS (median 14.5 versus 3.5 months,log-rank P = 0.002) (Fig. 4B). The presence of sp-
ecific HLA alleles did not correlate with efficacy(fig. S8). The absolute burden of candidate neo-antigens, but not the frequency per nonsynony-mous mutation, correlated with response (fig. S9).We next sought to assess whether anti–PD-1
therapy can alter neoantigen-specific T cell re-activity. To directly test this, identified candidateneoantigens were examined in a patient (StudyID no. 9 in Fig. 3 and table S3) with exceptionalresponse to pembrolizumab and available pe-ripheral blood lymphocytes (PBLs). PredictedHLA-A–restricted peptides were synthesized toscreen for ex vivo autologous T cell reactivity inserially collected PBLs (days 0, 21, 44, 63, 256, and297, where day 0 is the first date of treatment)using a validated high-throughput major histo-compatibility complex (MHC) multimer screeningstrategy (29, 30). This analysis revealed a CD8+T cell response against a neoantigen resultingfrom a HERC1 P3278S mutation (ASNASSAAK)(Fig. 4C). Notably, this T cell response could onlybe detected upon the start of therapy (level ofdetection 0.005%). Three weeks after therapyinitiation, the magnitude of response was 0.040%
126 3 APRIL 2015 • VOL 348 ISSUE 6230 sciencemag.org SCIENCE
0 4 8 12 16 20 240
5 0
1 0 0
Transversion high Transversion low
Per
cent
pro
gres
sion
-fre
e 100
50
0
Months 4 8 12 16 20 24
Fig. 2. Molecular smoking signature is significantlyassociated with improved PFS in NSCLC patientstreated with pembrolizumab. PFS in tumors char-acterized as TH by molecular smoking signatureclassifier (n = 16) compared to TL tumors (n = 18)(HR 0.15, 95% 0.06 to 0.39, log-rank P = 0.0001).
Fig. 3. Mutation burden, clinical response, and factors contributing tomutation burden.Total exonic mutation burden for each sequenced tumor withnonsynonymous (dark shading), synonymous (medium shading), and indels/frameshift mutations (light shading) displayed in the histogram. Columns areshaded to indicate clinical benefit status: DCB, green; NDB, red; not reached6 months follow-up (NR), blue. The cohort identification (D, discovery; V, valida-
tion), best objective response (PR, partial response; SD, stable disease; PD,progression of disease), and PFS (censored at the time of data lock) are reportedin the table.Those with ongoing progression-free survival are labeled with ++.Thepresence of the molecular smoking signature is displayed in the table with THcases (purple) and TL cases (orange). The presence of deleterious mutations inspecific DNA repair/replication genes is indicated by the arrows.
RESEARCH | REPORTS
PFS selon la charge mutationnelle
« non synonyme »
PFS selon le taux de transversion
(lié au tabagisme)
• Mise en évidence d’une signature de néo-épitopes prédictive de la survie
of CD8+ T cells, and this response was main-tained at Day 44. This rapid induction of T cellreactivity correlated with tumor regression, andthis T cell response returned to levels just abovebackground in the subsequent months as tumorregression plateaued (Fig. 4D). HERC1 P3278S-multimer–reactive T cells from PBLs collected onday 44 were characterized by a CD45RA-CCR7-HLA-DR+LAG-3 phenotype, consistent with anactivated effector population (fig. S10). These datareveal autologous T cell responses against cancerneoantigens in the context of a clinical responseto anti–PD-1 therapy.To validate the specificity of the neoantigen-
reactive T cells, PBLs from days 63 and 297 wereexpanded in vitro in the presence of mutant pep-tide and subsequently restimulated with eithermutant or wild-type peptide (ASNASSAAK versus
ASNAPSAAK), and intracellular cytokines wereanalyzed. At both time points, a substantial pop-ulation of polyfunctional CD8+ T cells [charac-terized by production of the cytokines interferon(IFN) g and tumor necrosis factor (TNF) a, themarker of cytotoxic activity CD107a, and the chemo-kine CCL4] was detected in response to mutantbut not wild-type peptide (Fig. 4E and fig. S11).In the current study, we show that in NSCLCs
treated with pembrolizumab, elevated nonsynon-ymous mutation burden strongly associates withclinical efficacy. Additionally, clinical efficacy cor-relates with a molecular signature characteristicof tobacco carcinogen–related mutagenesis, cer-tain DNA repair mutations, and the burden ofneoantigens. The molecular smoking signaturecorrelated with efficacy, whereas self-reportedsmoking status did not, highlighting the power
of this classifier to identify molecularly relatedtumors within a heterogeneous group.Previous studies have reported that pretreat-
ment PD-L1 expression enriches for response toanti–PD-1 therapies (3, 8, 31), but many tumorsdeemed PD-L1 positive do not respond, and someresponses occur in PD-L1–negative tumors (8, 31).Semiquantitative PD-L1 staining results were avail-able for 30 of 34 patients, where strong stainingrepresented ≥50% PD-L1 expression, weak rep-resented 1 to 49%, and negative represented<1% [clone 22C3, Merck (8)]. As this trial largelyenrolled patients with PD-L1 tumor expression,most samples had some degree of PD-L1 ex-pression (24 of 30, 80%) (table S3), limiting thecapacity to determine relationships betweenmutation burden and PD-L1 expression. Amongthose with high nonsynonymous mutation burden
SCIENCE sciencemag.org 3 APRIL 2015 • VOL 348 ISSUE 6230 127
0
2 0 0
4 0 0
6 0 0
DCB NDB
# C
andi
date
neo
antig
ens/
tum
or
Per
cent
pro
gres
sion
-fre
e
Months
High neoantigen burden Low neoantigen burden
Qdot 625 pMHC multimer
BV
421
pMH
C m
ultim
er
0 60 120 180 240 300
Baseline Day 56 Day 315
Live
r m
etas
tasi
s C
linic
al
resp
onse
(irR
C)
% P
BLs
rea
ctiv
e to
HLA
-A*1
1:01
H
ER
C1
P32
78S
mul
timer
s
Day 63
Day 297
IFN
CD8 TNF CD107a CCL4
-88%
0
-91%
-50
-100
Day 63, 0.022%
Day 256, 0.003%
Day 44, 0.044%
Day 21, 0.04%
0.05
0.04
0.03
0.02
0.01
0.00
-78% -88% -89%
Day 297, 0.005%
Pretreatment Day 1, 0.001%
4 0 8 12 16 20 24
600
400
200
0
100
50
0
No StimulationWT-ASNAPSAAKMUT-ASNASSAAK
Days
Fig. 4. Candidate neoantigens, neoantigen-specific T cellresponse, and response to pembrolizumab. (A) Neoantigenburden in patients with DCB (n = 14) compared to NDB (n = 17)across the overall set of sequenced tumors (median 203 versus83, Mann-Whitney P = 0.001). (B) PFS in tumors with higher can-didate neoantigen burden (n = 17) compared to tumors with lowercandidate neoantigen burden (n = 17) (HR 0.23, 95% CI 0.09 to0.58, log-rank P = 0.002). (C) (Top) Representative computedtomography (CT) images of a liver metastasis before and afterinitiation of treatment. (Middle) Change in radiographic response.(Bottom) Magnitude of the HERC1 P3278S reactive CD8+ Tcellresponse measured in peripheral blood. (D) The proportion ofCD8+ Tcell population in serially collected autologous PBLs rec-ognizing the HERC1 P3278S neoantigen (ASNASSAAK) before andduring pembrolizumab treatment. Each neoantigen is encodedby a unique combination of two fluorescently labeled peptide-
MHC complexes (represented individually on each axis); neoantigen-specific T cells are represented by the events in the double positive position indicatedwith black dots. Percentages indicate the number of CD8+ MHC multimer+ cells out of total CD8 cells. (E) Autologous T cell response to wild-type HERC1peptide (black), mutant HERC1 P3278S neoantigen (red), or no stimulation (blue), as detected by intracellular cytokine staining. Tcell costains for IFNg andCD8, TNFa, CD107a, and CCL4, respectively, are displayed for the Day 63 and Day 297 time points.
RESEARCH | REPORTS
PFS selon les néo-antigénes

Charge mutationnelle et néo-antigènes
• Mutations et néo-antigènes selon les cancers.
meaningful frequencies and may therefore beconsidered patient-specific. Because of this, tech-nologies to interrogate T cell reactivity againstputative mutation-derived neoantigens need tobe based on the genome of an individual tumor.With the development of deep-sequencing tech-nologies, it has become feasible to identify themutations present within the protein-encodingpart of the genome (the exome) of an individualtumor with relative ease and thereby predictpotential neoantigens (9). Two studies in mousemodels provided the first direct evidence thatsuch a cancer exome–based approach can be usedto identify neoantigens that can be recognizedby T cells (10, 11). In brief, for all mutations thatresulted in the formation of novel protein se-quence, potential MHC binding peptides werepredicted, and the resulting set of potential neo-antigens was used to query T cell reactivity. Sub-sequent studies have demonstrated that cancerexome–based analyses can also be exploited in aclinical setting, to dissect T cell reactivity in pa-tients who are treated by either tumor-infiltratinglymphocyte (TIL) cell therapy or checkpoint block-ade (12, 13). Furthermore, following this earlywork, the identification of neoantigens on thebasis of cancer exome data has been documentedin a variety of experimental model systems andhuman malignancies (10–22).The technological pipeline used to identify
neoantigens in these different studies has variedsubstantially, and further optimization is likely pos-sible (Fig. 1). Accepting the limitations of probingthemutational profile of a tumor in a single biopsy(23), the genetic analysis of the tumor itself can beconsidered a robust process. Specifically, based onthe analysis of neoantigens previously identifiedby other means, the false-negative rate of cancer
exome sequencing is low—i.e., the vast majority ofneoantigens occur within exonic sequence forwhich coverage is sufficient (24). At the same time,it is apparent from unbiased screening efforts—inwhich the entire collection of identified muta-tions was used to query T cell reactivity—that thevastmajority ofmutationswithin expressed genesdo not lead to the formation of neoantigens thatare recognized by autologous T cells (16, 17). Becauseof this, a robust pipeline that can be used for thefiltering of cancer exome data is essential, in par-ticular for tumors with high mutational loads.How can such filtering be performed? With
the set of mutations within expressed genes as astarting point, two additional requirements canbe formulated. First, a mutated protein needs tobe processed and then presented as a mutantpeptide by MHC molecules. Second, T cells needto be present that can recognize this peptide-MHC complex. In two recent preclinical studies,presentation of a handful of predicted neoanti-gens byMHCmolecules was experimentally dem-onstrated by mass spectrometry (15, 20), and thisapproach may form a valuable strategy to furtheroptimize MHC presentation algorithms. At thesame time, the sensitivity of mass spectrometryis presently still limited, thereby likely resultingin a substantial fraction of false negatives. For thisreason, but also because of logistical issues, imple-mentation of this approach in a clinical setting isunlikely tohappen soon.Lackingdirect evidence forMHC presentation, as can be provided by massspectrometry, presentation of neoantigens byMHCclass Imoleculesmay be predicted using previouslyestablished algorithms that analyze aspects such asthe likelihood of proteasomal processing, transportinto the endoplasmic reticulum, and affinity forthe relevant MHC class I alleles. In addition,
gene expression levels (or perhaps preferablyprotein translation levels) may potentially alsobe used to help predict epitope abundance (25).Althoughmost neoantigen identification studies
have successfully used criteria for epitope predic-tion that are similar to those previously estab-lished for the identification of pathogen-derivedepitopes [e.g., (12, 13)], Srivastava and colleagueshave argued that neoantigens in a transplantablemouse tumor model display very different prop-erties from viral antigens and generally have avery low affinity for MHC class I (14). Althoughlacking a satisfactory explanation to reconcilethese findings, we do note that the vast majorityof human neoantigens that have been identifiedin unbiased screens do display a high predictedMHC binding affinity (24, 26). Likewise, minorhistocompatibility antigens, an antigen class thatis conceptually similar to neoantigens, are cor-rectly identified by classical MHC binding algo-rithms (27). Moreover, the mutations that wereidentified in a recent preclinical study as formingtumor-specific mutant antigens that could in-duce therapeutic tumor rejection when used intumor vaccines (15) were not predicted to be sig-nificant using the Srivastava approach. Anotherpotential filter step that has been suggestedexamines whether the mutation is expected toimprove MHC binding, rather than solely alter theT cell receptor (TCR)–exposed surface of the mu-tant peptide. However, with examples of bothcategories in both mouse models and humandata, the added value of such a filter may berelatively modest (11, 15, 20, 26). For MHC classI restricted neoantigens, conceivably the biggestgain in prediction algorithms can be made withrespect to identification of the subset of MHCbindingpeptides that can successfully be recognized
70 3 APRIL 2015 • VOL 348 ISSUE 6230 sciencemag.org SCIENCE
1,000
Pilo
cytic
ast
rocy
tom
a
AM
L
ALL
Thyr
oid
Kid
ney
chro
mop
hobe
CLL
Med
ullo
blas
tom
a
Neu
robl
asto
ma
Glio
ma
low
gra
de
Glio
blas
tom
a
Pros
tate
Ova
ry
Mye
lom
a
Panc
reas
Bre
ast
Kid
ney
papi
llary
Lym
phom
a B
-cel
l
Kid
ney
clea
r cel
l
Hea
d an
d ne
ck
Live
r
Cer
vix
Ute
rus
Bla
dder
Col
orec
tum
Lung
sm
all c
ell
Esop
hagu
s
Sto
mac
h
Lung
ade
no
Lung
squ
amou
s
Mel
anom
a
Occasionally
Regularly
Frequently
Formation ofneoantigens
100
10
1.0
0.1
0.01
Som
atic
mut
atio
n pr
eval
ence
(num
ber m
utat
ions
per
meg
abas
e)
Fig. 2. Estimate of the neoantigen repertoire in human cancer. Data depict the number of somatic mutations in individual tumors. Categories on the rightindicate current estimates of the likelihood of neoantigen formation in different tumor types. Adapted from (50). It is possible that the immune system inmelanoma patients picks up on only a fraction of the available neoantigen repertoire, in which case the current analysis will be an underestimate. A value of 10somatic mutations per Mb of coding DNA corresponds to ~150 nonsynonymous mutations within expressed genes.
CANCER IMMUNOLOGY AND IMMUNOTHERAPY
CANCER ETIOLOGY
Mutational signatures associated withtobacco smoking in human cancerLudmil B. Alexandrov,1,2,3* Young Seok Ju,4 Kerstin Haase,5 Peter Van Loo,5,6
Iñigo Martincorena,7 Serena Nik-Zainal,7,8 Yasushi Totoki,9 Akihiro Fujimoto,10,11
Hidewaki Nakagawa,10 Tatsuhiro Shibata,9,12 Peter J. Campbell,7,13 Paolo Vineis,14,15
David H. Phillips,16 Michael R. Stratton7*
Tobacco smoking increases the risk of at least 17 classes of human cancer. We analyzedsomatic mutations and DNA methylation in 5243 cancers of types for which tobaccosmoking confers an elevated risk. Smoking is associated with increased mutation burdensof multiple distinct mutational signatures, which contribute to different extents in differentcancers. One of these signatures, mainly found in cancers derived from tissues directlyexposed to tobacco smoke, is attributable to misreplication of DNA damage caused bytobacco carcinogens. Others likely reflect indirect activation of DNA editing by APOBECcytidine deaminases and of an endogenous clocklike mutational process. Smoking isassociated with limited differences in methylation. The results are consistent withthe proposition that smoking increases cancer risk by increasing the somatic mutationload, although direct evidence for this mechanism is lacking in some smoking-relatedcancer types.
Tobacco smoking has been associated withat least 17 types of human cancer (Table 1)and claims the lives of more than 6 millionpeople every year (1–4). Tobacco smoke is acomplex mixture of chemicals, among which
at least 60 are carcinogens (5). Many of these arethought to cause cancer by inducing DNA damagethat, if misreplicated, leads to an increased bur-den of somatic mutations and, hence, an elevatedchance of acquiring driver mutations in cancergenes. Such damage often occurs in the form ofcovalent bonding of metabolically activated re-active species of the carcinogen to DNA bases,termed DNA adducts (6). Tissues directly exposedto tobacco smoke (e.g., lung), as well as sometissues not directly exposed (e.g., bladder), showelevated levels of DNA adducts in smokers and,thus, evidence of exposure to carcinogenic com-ponents of tobacco smoke (7, 8).Each biological process causing mutations in
somatic cells leaves a mutational signature (9).Many cancers have a somatic mutation in theTP53 gene, and catalogs of TP53mutations com-piled two decades ago enabled early explorationof these signatures (10), showing that lung can-cers from smokers have more C>A transversionsthan lung cancers from nonsmokers (11–14). Toinvestigate mutational signatures using the thou-sands of mutation catalogs generated by systematic
cancer genome sequencing, we recently describeda framework in which each base substitutionsignature is characterized using a 96-mutationclassification that includes the six substitutiontypes together with the bases immediately 5′ and3′ to the mutated base (15). The analysis extractsmutational signatures frommutation catalogs andestimates the number of mutations contributedby each signature to each cancer genome (15).Using this approach, more than 30 differentbase substitution signatures have been identi-fied (16–18).In this study, we examined 5243 cancer ge-
nome sequences (4633 exomes and 610 wholegenomes) of cancer classes for which smokingincreases risk, with the goal of identifying mu-tational signatures and methylation changes as-sociated with tobacco smoking (table S1). Of thesamples we studied, 2490 were reported to befrom tobacco smokers and 1063 from never-smokers (Table 1). Thus, we were able to inves-tigate the mutational consequences of smokingby comparing somatic mutations and methyla-tion in smokers versus nonsmokers for lung,larynx, pharynx, oral cavity, esophageal, bladder,liver, cervical, kidney, and pancreatic cancers(Fig. 1 and table S2).We first compared total numbers of base sub-
stitutions, small insertions and deletions (indels),
and genomic rearrangements. The total numberof base substitutions was higher in smokerscompared with nonsmokers for all cancer typestogether (q-value < 0.05) and, for individual can-cer types, in lung adenocarcinoma, larynx, liver,and kidney cancers (table S2). Total numbers ofindels were higher in smokers compared withnonsmokers in lung adenocarcinoma and livercancer (table S2). The whole-genome–sequencedcases allowed comparison of genome rearrange-ments between smokers and nonsmokers in pan-creatic and liver cancer, where no differenceswere found (table S2). However, subchromo-somal copy-number changes entail genomicrearrangement and can serve as surrogates forrearrangements. Lung adenocarcinomas fromsmokers exhibited more copy-number aberra-tions than those from nonsmokers (table S2).We then extracted mutational signatures, es-
timated the contributions of each signature toeach cancer, and compared the numbers of mu-tations attributable to each signature in smokersand nonsmokers. Increases in smokers comparedwith nonsmokers were seen for signatures 2, 4, 5,13, and 16 [the mutational signature nomencla-ture is that used in the Catalogue of SomaticMutations in Cancer (COSMIC) and in (16–18)].There was sufficient statistical power to show thatthese increases were of clonal mutations (muta-tions present in all cells of each cancer) forsignatures 4 and 5 (q < 0.05), as expected ifthese mutations are due to cigarette smoke ex-posure before neoplastic change (supplemen-tary text).Signature 4 is characterized mainly by C>A
mutations with smaller contributions from otherbase substitution classes (Fig. 2B and fig. S1). Thissignature was found only in cancer types inwhich tobacco smoking increases risk and mainlyin those derived from epithelia directly exposedto tobacco smoke (figs. S2 and S3). Signature 4 isvery similar to the mutational signature induced invitro by exposing cells to benzo[a]pyrene (cosinesimilarity = 0.94) (Fig. 2B and fig. S3), a tobaccosmoke carcinogen (19). The similarity extends tothe presence of a transcriptional strand bias in-dicative of transcription-coupled nucleotide ex-cision repair (NER) of bulky DNA adducts onguanine (fig. S1), the proposed mechanism ofDNA damage by benzo[a]pyrene. Thus, signa-ture 4 is likely the direct mutational consequenceof misreplication of DNA damage induced bytobacco carcinogens.Most lung and larynx cancers from smokers
had many signature 4 mutations. Signature 4mutations occurred more often in cancers from
618 4 NOVEMBER 2016 • VOL 354 ISSUE 6312 sciencemag.org SCIENCE
1Theoretical Biology and Biophysics (T-6), Los Alamos National Laboratory, Los Alamos, NM 87545, USA. 2Center for Nonlinear Studies, Los Alamos National Laboratory, Los Alamos, NM 87545,USA. 3University of New Mexico Comprehensive Cancer Center, Albuquerque, NM 87102, USA. 4Graduate School of Medical Science and Engineering, Korea Advanced Institute of Science andTechnology, Daejeon 34141, Republic of Korea. 5The Francis Crick Institute, 1 Midland Road, London NW1 1AT, UK. 6Department of Human Genetics, University of Leuven, 3000 Leuven, Belgium.7Cancer Genome Project, Wellcome Trust Sanger Institute, Hinxton CB10 1SA, Cambridgeshire, UK. 8Department of Medical Genetics, Addenbrooke’s Hospital National Health Service Trust,Cambridge, UK. 9Division of Cancer Genomics, National Cancer Center Research Institute, Chuo-ku, Tokyo, Japan. 10Laboratory for Genome Sequencing Analysis, RIKEN Center for IntegrativeMedical Sciences, Tokyo, Japan. 11Department of Drug Discovery Medicine, Kyoto University Graduate School of Medicine, Kyoto 606-8507, Japan. 12Laboratory of Molecular Medicine, HumanGenome Center, The Institute of Medical Science, The University of Tokyo, Minato-ku, Tokyo, Japan. 13Department of Haematology, University of Cambridge, Cambridge CB2 0XY, UK. 14HumanGenetics Foundation, 10126 Torino, Italy. 15Department of Epidemiology and Biostatistics, Medical Research Council (MRC)–Public Health England (PHE) Centre for Environment and Health,School of Public Health, Imperial College London, Norfolk Place, London W2 1PG, UK. 16King’s College London, MRC-PHE Centre for Environment and Health, Analytical and EnvironmentalSciences Division, Franklin-Wilkins Building, 150 Stamford Street, London SE1 9NH, UK.*Corresponding author. Email: [email protected] (L.B.A.); [email protected] (M.R.S.)
RESEARCH | REPORTS
on
Nov
embe
r 5, 2
016
http
://sc
ienc
e.sc
ienc
emag
.org
/D
ownl
oade
d fr
om
Alexandrov L, Nature 2011 Alexandrov L, Science 2016

Charge mutationnelle et néo-antigènes
• Charge mutationnelle et réponse à l’immunothérapie
Yarchoan M, NEJM 2017

Charge mutationnelle et néo-antigènes
• Impact de la charge mutationnelle sur la réponse au nivolumab (essai CHECKMATE 026)
Carbone DP, NEJM 2017

Charge mutationnelle et néo-antigènes
• Impact de la charge mutationnelle sur la réponse à nivolumab + ipilimumab (essai CHECKMATE 227)
Hellmann M, NEJM 2018
1739 299

Charge mutationnelle et néo-antigènes
• Impact de la charge mutationnelle sur la réponse à nivolumab + ipilimumab (essai CHECKMATE 227)
Hellmann M, NEJM 2018

Charge mutationnelle et néo-antigènes
• Impact de la charge mutationnelle sur la réponse à nivolumab + ipilimumab (essai CHECKMATE 227)
Hellmann M, ASCO 2018

Charge mutationnelle et néo-antigènes
Hellmann M, Cancer Cell 2018
Cancer Cell
Article
Tumor Mutational Burden and Efficacy of NivolumabMonotherapy and in Combination with Ipilimumabin Small-Cell Lung CancerMatthew D. Hellmann,1,11,12,* Margaret K. Callahan,1,11 Mark M. Awad,2 Emiliano Calvo,3 Paolo A. Ascierto,4
Akin Atmaca,5 Naiyer A. Rizvi,6 Fred R. Hirsch,7 Giovanni Selvaggi,8 Joseph D. Szustakowski,9 Ariella Sasson,9
Ryan Golhar,9 Patrik Vitazka,9 Han Chang,9 William J. Geese,9 and Scott J. Antonia101Thoracic Oncology Service, Division of Solid Tumor Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center,Weill Cornell Medical College, and Parker Center for Cancer Immunotherapy, 885 2nd Avenue, New York, NY 10017, USA2Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA 02215, USA3START Madrid, Centro Integral Oncologico Clara Campal, Medical Oncology Division, Hospital Universitario Madrid Norte Sanchinarro,Madrid 28050, Spain4Unit of Melanoma, Cancer Immunotherapy and Innovative Therapy, Istituto Nazionale Tumori Fondazione G. Pascale, Naples 80131, Italy5Department of Hematology and Oncology, Krankenhaus Nordwest, UCT-University Cancer Center, Frankfurt am Main 60488, Germany6Division of Hematology and Oncology, Columbia University Medical Center, New York, NY 10032, USA7Department of Medicine, Division of Medical Oncology, University of Colorado Anschutz Medical Campus, Aurora, CO 80045, USA8Clinical Development, Bristol-Myers Squibb, Princeton, NJ 08648, USA9Translational Medicine, Bristol-Myers Squibb, Princeton, NJ 08648, USA10Department of Thoracic Oncology, H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL 33612, USA11These authors contributed equally12Lead Contact*Correspondence: [email protected]://doi.org/10.1016/j.ccell.2018.04.001
SUMMARY
Durable responses and encouraging survival have been demonstrated with immune checkpoint inhibitorsin small-cell lung cancer (SCLC), but predictive markers are unknown. We used whole exome sequencing toevaluate the impact of tumor mutational burden on efficacy of nivolumab monotherapy or combined withipilimumab in patients with SCLC from the nonrandomized or randomized cohorts of CheckMate 032.Patients received nivolumab (3 mg/kg every 2 weeks) or nivolumab plus ipilimumab (1 mg/kg plus 3 mg/kgevery 3 weeks for four cycles, followed by nivolumab 3 mg/kg every 2 weeks). Efficacy of nivolumab ±ipilimumabwasenhanced in patientswith high tumormutational burden. Nivolumabplus ipilimumabappearedto provide a greater clinical benefit than nivolumab monotherapy in the high tumor mutational burden tertile.
INTRODUCTION
Small-cell lung cancer (SCLC) accounts for 10%–15% of all pa-tients with lung cancer (Alvarado-Luna and Morales-Espinosa,2016; Herbst et al., 2008), and approximately 75% of patientspresent with extensive-stage disease. Standard first-line treat-ment consists of platinum-based chemotherapy, but patientswho progress have few effective treatment options and a
routinely poor prognosis (Alvarado-Luna and Morales-Espinosa,2016; National Comprehensive Cancer Network, 2017). In pa-tients with previously treated SCLC, nivolumab, a fully humanimmunoglobulin (Ig) G4 programmed death (PD)-1 immunecheckpoint inhibitor antibody, showed durable responses andencouraging survival as monotherapy and in combination withipilimumab, a fully human IgG1 cytotoxic T lymphocyte anti-gen-4 (CTLA-4) immune checkpoint inhibitor antibody (Antonia
Significance
The identification of predictors of response to immune checkpoint blockade in small-cell lung cancer (SCLC) has beenelusive. Expression of tumor programmed death ligand 1, a common biomarker in non-small-cell lung cancer, is uncommonand not predictive in SCLC. We show that efficacy of nivolumab with or without ipilimumab was increased in SCLCs thathave high tumormutational burden. The differential benefit of combination immunotherapy wasmost substantial in patientswith high tumormutational burden. Our results suggest that tumor mutational burden has a role as a biomarker in SCLC andmay help identify patients most likely to benefit from combination immunotherapy. Our findings are a critical contribution inmoving toward greater precision in patient selection for treatments in lung cancer.
Cancer Cell 33, 853–861, May 14, 2018 ª 2018 Elsevier Inc. 853
Figure 4. Progression-Free Survival by Treatment and Tumor Mutational Burden TertileCI denotes confidence interval.
Cancer Cell 33, 853–861, May 14, 2018 857
Figure 5. Overall Survival by Treatment and Tumor Mutational Burden TertileCI denotes confidence interval. See also Figure S6.
858 Cancer Cell 33, 853–861, May 14, 2018
• Impact de la charge mutationnelle sur la réponse à nivolumab + ipilimumab dans le CPC

Charge mutationnelle et néo-antigènes
• Comment analyser la charge mutationnelle ?
– NGS • Whole exome • RNAseq • Panel ciblé de gènes: quantification des mutations
somatiques après exclusion des drivers oncogéniques et des polymorphismes de la lignée germinale. Ex. FoundationOne
– Etude plus qualitative par analyse des épitopes néo-antigéniques

Charge mutationnelle et néo-antigènes
• Combien de gènes doit comporter le test TMB ? • Analyse modélisée en faveur de panel 300+ genes pour
la détermination de la TMB
Garofalo et al. Genome Medicine 2016

Charge mutationnelle et néo-antigènes
• Combien de gènes doit comporter le test TMB ?

Charge mutationnelle et néo-antigènes
• Exigence de l’analyse de la charge mutationnelle

Charge mutationnelle et néo-antigènes
• Le problème du seuil dans le TMB

Charge mutationnelle et néo-antigènes
• Attention au faux positif de l’aneuploidie
Davoli, Science 2017

Charge mutationnelle et néo-antigènes
• TMB dans le sang circulant ? • TMB sérique et bénéfice clinique dans le CBNPC traité par
atezolizumab • Lien tissu vs sang
ARTICLESNATURE MEDICINE
with a high TMB count (> 30 mutations) in both the blood and tissue, on average, one-third of the variants were unique to the blood sample and one-fourth of the total variants were unique to the tissue sample, with the remaining variants identified in both (Fig. 1f,g). Patients with > 30 mutations in tissue had a range of concordance between bTMB and tTMB. Seven out of 22 patients had very few mutations detected in the blood and therefore very little overlap with tissue. By contrast, 68% of samples shared the majority of TMB variants between tissue and the blood. This shows that the presence of different variants might account for a large portion of the difference between tTMB and bTMB.
To determine whether factors associated with the samples them-selves contributed to the variation we observed in the pairwise comparison of tTMB and bTMB in POPLAR and OAK samples, we evaluated a series of sample characteristics, including the sam-ple type (biopsy versus resection), stage at diagnosis, the fraction of cfDNA that is ctDNA as measured by the MSAF detected in a sample (see the Methods for more details on the MSAF), sample collection time (blood versus tissue), the baseline tumor burden as determined by Response Evaluation Criteria In Solid Tumors ver-sion 1.1 (RECIST v1.1) and tumor purity (see the Methods), among
Blood collection,plasma isolation and
cfDNA extraction
>��//�'&6*�68'67.787.216�:.7-� ≥����&//*/*�+5*48*1(<
>�"*029*�,*50/.1*���32/<0253-.606�&1)�35*).(7*)���)5.9*5�087&7.216
'$�B
#*48*1(.1,POPLA"�75&.1.1,�
OAK�9&/.)&7.21�
�*75.( Performance
PPA � ������������ =� ��
NPA ���������������=����
PPA (%�'$�B
≥10
≥11
≥12
≥13
≥14
≥15
≥16
≥17
≥18
≥19
≥20
NPA (%�10094.6
89.1
9490
85.789.1
90.2
92.194.4
97.1
10092.3
92.9
84.289.5
90100
89.3
83.981.8
82.4
Spearman correlation = 0.93
�*75.( %&/8* ctDNA samples Comments
PPA93.4%
(171/183 9&5.&176�
���6&03/*6�:.7- 9&5.&176����727&/�
samples
�&/6*�1*,&7.9*�%��6�5&1,*�+520����72����.1����$��352'&'/<0.66*)�)8*�72�/2:�5*&)�683325t
PPV93.5% (43/46 9&5.&176��
���6&03/*6�:.7- 9&5.&176����727&/�
samples
�&/6*�326.7.9*�%��6����������&1)������.1�'$����352'&'/<�)8*72�&�1*&5'<�-20232/<0*5�6*48*1(*
a
b c
d
0 16
16
60 800
20
40
60
807$��
326.7.9*�28'/*�326.7.9*
�28'/*1*,&7.9* '$���326.7.9*
40
'$��
7$��
1 10 16 100
500
1
1016
500
100
7$���326.7.9* �28'/*�326.7.9*
�28'/*�1*,&7.9* '$���326.7.9*
'$�B
��7$��
#-&5*)�9&5.&17s(N������������
�/22)�21/<(N���� �������
$.668*�21/<(N�����������
f g
R 2 = 0.6783 R 2 = 0.998
00
1
2
3
4
1 2 3 4
'$���&//*
/*�+5*4
8*1(
<���
�
���$�&//*/*�+5*48*1(<����
0
20
40
60
80
100
0 20 40 60 80 100
'$���&//*
/*�+5*4
8*1(
<���
�
���$�&//*/*�+5*48*1(<����
e
�80
'*5�2+�0
87&7.216
��$���(28
17� �27-
$.668*�68'6$.668*�.1)*/s�/22)�68'6
Pat
ient
1P
atie
nt 2
Pat
ient
3P
atie
nt 4
Pat
ient
5P
atie
nt 6
Pat
ient
7P
atie
nt 8
Pat
ient
9P
atie
nt 1
0P
atie
nt 1
1P
atie
nt 1
2P
atie
nt 1
3P
atie
nt 1
4P
atie
nt 1
5P
atie
nt 1
6P
atie
nt 1
7P
atie
nt 1
8P
atie
nt 1
9P
atie
nt 2
0P
atie
nt 2
1P
atie
nt 2
2
140
120
100
80
60
40
20
0 $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣B
20
NATURE MEDICINE | www.nature.com/naturemedicine
ARTICLESNATURE MEDICINE
with a high TMB count (> 30 mutations) in both the blood and tissue, on average, one-third of the variants were unique to the blood sample and one-fourth of the total variants were unique to the tissue sample, with the remaining variants identified in both (Fig. 1f,g). Patients with > 30 mutations in tissue had a range of concordance between bTMB and tTMB. Seven out of 22 patients had very few mutations detected in the blood and therefore very little overlap with tissue. By contrast, 68% of samples shared the majority of TMB variants between tissue and the blood. This shows that the presence of different variants might account for a large portion of the difference between tTMB and bTMB.
To determine whether factors associated with the samples them-selves contributed to the variation we observed in the pairwise comparison of tTMB and bTMB in POPLAR and OAK samples, we evaluated a series of sample characteristics, including the sam-ple type (biopsy versus resection), stage at diagnosis, the fraction of cfDNA that is ctDNA as measured by the MSAF detected in a sample (see the Methods for more details on the MSAF), sample collection time (blood versus tissue), the baseline tumor burden as determined by Response Evaluation Criteria In Solid Tumors ver-sion 1.1 (RECIST v1.1) and tumor purity (see the Methods), among
Blood collection,plasma isolation and
cfDNA extraction
>��//�'&6*�68'67.787.216�:.7-� ≥����&//*/*�+5*48*1(<
>�"*029*�,*50/.1*���32/<0253-.606�&1)�35*).(7*)���)5.9*5�087&7.216
'$�B
#*48*1(.1,POPLA"�75&.1.1,�
OAK�9&/.)&7.21�
�*75.( Performance
PPA � ������������ =� ��
NPA ���������������=����
PPA (%�'$�B
≥10
≥11
≥12
≥13
≥14
≥15
≥16
≥17
≥18
≥19
≥20
NPA (%�10094.6
89.1
9490
85.789.1
90.2
92.194.4
97.1
10092.3
92.9
84.289.5
90100
89.3
83.981.8
82.4
Spearman correlation = 0.93
�*75.( %&/8* ctDNA samples Comments
PPA93.4%
(171/183 9&5.&176�
���6&03/*6�:.7- 9&5.&176����727&/�
samples
�&/6*�1*,&7.9*�%��6�5&1,*�+520����72����.1����$��352'&'/<0.66*)�)8*�72�/2:�5*&)�683325t
PPV93.5% (43/46 9&5.&176��
���6&03/*6�:.7- 9&5.&176����727&/�
samples
�&/6*�326.7.9*�%��6����������&1)������.1�'$����352'&'/<�)8*72�&�1*&5'<�-20232/<0*5�6*48*1(*
a
b c
d
0 16
16
60 800
20
40
60
807$��
326.7.9*�28'/*�326.7.9*
�28'/*1*,&7.9* '$���326.7.9*
40
'$��
7$��
1 10 16 100
500
1
1016
500
100
7$���326.7.9* �28'/*�326.7.9*
�28'/*�1*,&7.9* '$���326.7.9*
'$�B
��7$
��
#-&5*)�9&5.&17s(N������������
�/22)�21/<(N���� �������
$.668*�21/<(N�����������
f g
R 2 = 0.6783 R 2 = 0.998
00
1
2
3
4
1 2 3 4
'$���&//*/*�+5*4
8*1(
<���
����$�&//*/*�+5*48*1(<����
0
20
40
60
80
100
0 20 40 60 80 100
'$���&//*/*�+5*4
8*1(
<���
�
���$�&//*/*�+5*48*1(<����
e
�80
'*5�2
+�087&7.216
��$���(28
17� �27-
$.668*�68'6$.668*�.1)*/s�/22)�68'6
Pat
ient
1P
atie
nt 2
Pat
ient
3P
atie
nt 4
Pat
ient
5P
atie
nt 6
Pat
ient
7P
atie
nt 8
Pat
ient
9P
atie
nt 1
0P
atie
nt 1
1P
atie
nt 1
2P
atie
nt 1
3P
atie
nt 1
4P
atie
nt 1
5P
atie
nt 1
6P
atie
nt 1
7P
atie
nt 1
8P
atie
nt 1
9P
atie
nt 2
0P
atie
nt 2
1P
atie
nt 2
2140
120
100
80
60
40
20
0 $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣� $∣B
20
NATURE MEDICINE | www.nature.com/naturemedicine
Gandara, Nature Medecine 2018

Charge mutationnelle et néo-antigènes
• TMB dans le sang circulant ? • TMB sérique et bénéfice clinique dans le CBNPC traité par
atezolizumab
Gandara, Nature Medecine 2018
ARTICLESNATURE MEDICINE
Additional exploratory analyses were conducted at various cut-points of bTMB in the OAK study. Overall, there was a clear monotonic relationship between an increasing bTMB score and PFS outcomes (Fig. 4a). A similar, although less compelling, mono-tonic trend was observed for OS (Fig. 4b). Unlike PFS, numerical decreases in the OS HR were observed relative to the BEP only at the highest cut-points (bTMB ≥ 24 and bTMB ≥ 26; Fig. 4b). We were unable to assess the reproducibility of outcomes in these subgroups owing to low prevalence. The best overall response rate trended towards benefit with atezolizumab (21%) versus docetaxel (10%) in patients with bTMB ≥ 16 (Supplementary Fig. 5).
Association of bTMB with clinical characteristics and PD-L1 immunohistochemistry. The clinical characteristics of the bTMB subgroups in the OAK study are shown in Supplementary Tables 5 and 6. Within the OAK BEP, a positive bTMB status (≥ 16) was
associated with smoking (P = 1.3 × 10–10), which is consistent with heavy mutagen exposure32, the sum of longest distances of target lesions at baseline (P = 4.8 × 10–8), the number of metastatic sites (P = 0.0055) and PD-L1 expression (TC1/2/3 or IC1/2/3; that is, ≥ 1% of tumor cells or tumor-infiltrating immune cells express-ing PD-L1 (P = 0.0062)) (Supplementary Table 6). Baseline char-acteristics were balanced between treatment arms above the bTMB ≥ 16 cut-point (Supplementary Table 5). The mean bTMB value in patients with non-squamous histologies was 11.22 (95% CI: 10.09–12.36) and 12.4 (95% CI: 11–13.8) in those with squamous histology (Supplementary Fig. 6).
Previously, we showed in the OAK study that atezolizumab sig-nificantly improved OS compared to docetaxel in the overall ITT study population and across all PD-L1 subgroups. By contrast, a significant PFS benefit was observed only in patients with tumors expressing the highest levels of PD-L1 (TC3 or IC3; that is, with
PF
S (
%)
Time (months)
0
0 2 4 6 8 10 12 14 16 18 20 22
102030405060708090
100
Time (months)
0
0 2 4 6 8 10 12 14 16 18 20 22 2624
102030405060708090
100P
FS
(%
)a b
Atezolizumab (N = 77)Docetaxel (N = 81)
+
Atezolizumab (N = 216)Docetaxel (N = 209)
+
Atezolizumab (N = 77)Docetaxel (N = 81)
+
Atezolizumab (N = 216)Docetaxel (N = 209)
+
bTMB ≥ 16 bTMB ≥ 16
bTMB < 16
bTMB < 16
0.25 1.0 1.5
HR
Favors atezolizumab Favors docetaxel
Population N (%)
bTMB ≥ 16 158 (27)
bTMB < 16 425 (73)
BEP 583 (100)
ITT population 850
PFS HR (95% CI)
0.65 (0.47–0.92)
0.98 (0.80–1.20)
0.87 (0.73–1.04)
0.95 (0.82–1.10)
c
0.25 1.0 1.5HR
Favors atezolizumab Favors docetaxel
Population N (%)
bTMB ≥ 16
bTMB < 16
158 (27)
425 (73)
BEP 583 (100)
ITT population 850
d
e
f gOS HR (95% CI)
0.64 (0.44–0.92)
0.65 (0.52–0.81)
0.64 (0.53–0.77)
0.73 (0.62–0.87)
5 10 15 20 25
0.8
0.7
0.6
0.5
Minimum bTMB + value
PF
S H
RO
S (
%)
Time (months)
0
0 2 4 6 8 10 12 14 16 18 20 22 2624
102030405060708090
100O
S (
%)
Time (months)
0
0 2 4 6 8 10 12 14 16 18 20 22 24
102030405060708090
100
Censored Censored Censored
Censored
Fig. 3 | Association of clinical outcome and bTMB in the OAK study. a–f, Kaplan–Meier estimates and forest plots of HRs of PFS (a–c) and OS (d–f) in the bTMB!< !16 and bTMB!≥ !16 subgroups in the atezolizumab (bTMB!≥ !16: N!= !77; bTMB!< !16: N!= !216 patients) and docetaxel (bTMB!≥ !16: N!= !81; bTMB!< !16: N!= !209 patients) treatment arms. The interaction P value for PFS was 0.036 and for OS was 0.75. The interaction P value is from an unstratified proportional Cox model including the terms of treatment, the bTMB subgroup and the treatment by subgroup interaction. HRs are shown for PFS and OS in the ITT population, the BEP and the bTMB!< !16 and bTMB!≥ !16 subgroups. In c and f, N refers to the absolute number of patients with bTMB data above each cut-point and the prevalence (%) relative to the BEP. The error bars indicate 95% CIs. g, Multivariate adaptive regression splines analysis (line) of the relationship between PFS HRs (open circles) and the bTMB cut-point values (≥ 4: N!= !441; ≥ 5: N!= !403; ≥ 6: N!= !371; ≥ 7: N!= !340; ≥ 8: N!= !302; ≥ 9: N!= !272; ≥ 10: N!= !251; ≥ 11: N!= !235; ≥ 12: N!= !211; ≥ 13: N!= !200; ≥ 14: N!= !188; ≥ 15: N!= !166; ≥ 16: N!= !158; ≥ 17: N!= !147; ≥ 18: N!= !136; ≥ 19: N!= !121; ≥ 20: N!= !105; ≥ 21: N!= !97; ≥ 22: N!= !84; ≥ 23: N!= !76; ≥ 24: N!= !69; ≥ 25: N!= !62; ≥ 26: N!= !54 patients).
NATURE MEDICINE | www.nature.com/naturemedicine
ARTICLES NATURE MEDICINE
≥ 50% of tumor cells or ≥ 10% of tumor-infiltrating immune cells expressing PD-L1)1. To determine whether the clinical benefit observed in the bTMB ≥ 16 population might be explained by an over-representation of the PD-L1 TC3/IC3-positive population, we compared the overlap between bTMB and PD-L1 immunohisto-chemistry (IHC). We found similar proportions of overlap between bTMB and PD-L1 IHC subgroups; the median and maximum bTMB values were also similar (Fig. 5a and Supplementary Table 5). A total of 229 patients were positive for either bTMB ≥ 16 or the highest levels of PD-L1 IHC (TC3 or IC3), whereas only 30 patients (19.2% of bTMB ≥ 16 patients; 29.1% of TC3 or IC3 patients) were found to be positive by both assays (not significant, Fisher’s exact test) (Fig. 5b). The extent of the overlap between bTMB and IHC cut-offs was also examined (Supplementary Fig. 7 and Supplementary Table 6). These results indicate that bTMB is independent of the high PD-L1 expression as measured by IHC.
Although no significant correlation was observed between high PD-L1 expression and bTMB, we further evaluated the inde-pendence of their contribution towards the PFS benefit using two different approaches: first, we fitted a Cox model for the PFS ben-efit from treatment adjusted for the PD-L1 status (TC3 or IC3, or
not), the bTMB status (≥ 16 or not), PD-L1 by treatment interac-tion and the bTMB status by treatment interaction. The interaction HRs were 0.73 (95% CI: 0.46–1.13; P = 0.160) for PD-L1 and 0.66 (95% CI: 0.45–0.97; P = 0.035) for bTMB. The significant treatment interaction suggests that the bTMB status would affect the PFS HR while controlling for the PD-L1 status and its interaction with treat-ment. Second, we examined the PFS benefit in overlapping and non-overlapping subsets between the two biomarkers. Patients with bTMB ≥ 16 and TC3 or IC3 seemed to derive the most clinical ben-efit from atezolizumab (PFS HR: 0.38 (95% CI: 0.17–0.85); OS HR: 0.23 (95% CI: 0.09–0.58); Table 1), whereas patients with only TC3 or IC3 or only bTMB ≥ 16 (negative for the other marker) had PFS HRs of 0.71 (95% CI: 0.43–1.16) or 0.70 (95% CI: 0.48–1.03), respec-tively (Supplementary Table 7), compared with a HR of 0.87 (95% CI: 0.73–1.04) in the BEP in the OAK study. Notably, patients with no or low PD-L1 expression (TC0 and IC0) and bTMB ≥ 16 showed a trend towards a PFS benefit (HR: 0.68 (95% CI: 0.37–1.25)).
DiscussionIn this study, we demonstrated that TMB measured from the blood is a predictive biomarker for PFS in patients receiving atezolizumab monotherapy in NSCLC. This is the first demonstration that TMB can be accurately and reproducibly measured in plasma and that bTMB is associated with clinical benefit from immune checkpoint inhibitor therapy. Analyses performed in POPLAR samples and then confirmed in OAK samples demonstrate that bTMB ≥ 16 is a clinically meaning-ful and technically robust cut-point in NSCLC. We further show that bTMB is not associated with high PD-L1 expression and is indepen-dently predictive of the PFS benefit. The use of plasma instead of tis-sue as a DNA source makes the bTMB assay a particularly attractive alternative for patients with metastatic NSCLC who are not amenable to biopsy or whose tumor tissue is otherwise unavailable.
We validated the analytic performance of the bTMB assay based on accuracy, precision and the limit of detection and performed an agreement analysis between the tTMB and the bTMB assays using POPLAR and OAK tissue and plasma samples. This analysis showed that tTMB and bTMB are positively correlated; however, the assays detected overlapping but not identical variants in DNA isolated from asynchronous matching plasma and tissue samples. An in-depth analysis of technical and biological parameters sug-gested that the main source of variance between bTMB and tTMB originated from the samples themselves, rather than from computa-tional or analytic factors. More specifically, we showed that the same ctDNA samples run on both the bTMB and the tTMB assays gave highly concordant results, and that a lower proportion of tumor-derived plasma DNA (MSAF) and a longer time between tissue and plasma collections were associated with higher discordance. It is important to note that the POPLAR and OAK studies were second-line or higher therapy studies. As a result, it is likely that many of the tissue samples collected within ~3 months of study entry were prob-ably obtained from patients after disease progression on first-line therapy, whereas the samples collected after 3 months were prob-ably obtained before first-line platinum-based doublet chemother-apy. Thus, along with tumor heterogeneity and clonal selection, it is reasonable to hypothesize that the intervening therapy with DNA-damaging agents, such as chemotherapy, may have contributed to the relative discordance between bTMB and tTMB.
The identification of a biomarker that enriches for patients who may derive PFS benefit has been an important component of the development and treatment decision strategy for PD-L1–PD-1 agents in the first-line setting4,6. The inability to validate the improved OS benefit that was observed in the POPLAR study with the OAK trial is probably owing to the superior OS benefit observed in the OAK BEP (HR: 0.64) relative to the ITT population (HR: 0.73). However, the OS will be evaluated as a key second-ary end point in an ongoing, prospective, first-line NSCLC study
bPopulation N (%)
441 (76)371 (64)302 (52)251 (43)211 (36)188 (32)158 (27)136 (23)105 (18)84 (14)69 (12)54 (9)
BEP 583 (100)ITT population 850
OS HR (95% CI)
0.70 (0.57–0.87)0.71 (0.56–0.90)0.70 (0.54–0.91)0.69 (0.52–0.93)0.68 (0.50–0.94)0.66 (0.47–0.92)0.64 (0.44–0.92)0.61 (0.41–0.90)0.65 (0.41–1.03)0.67 (0.40–1.13)0.53 (0.30–0.94)0.50 (0.27–0.95)
0.64 (0.53–0.77)0.73 (0.62–0.87)
1.0 1.5
HR
Favors atezolizumab Favors docetaxel
1.0 1.5
HR
Favors atezolizumab Favors docetaxel
Population N (%)
441 (76)371 (64)302 (52)251 (43)211 (36)188 (32)158 (27)136 (23)105 (18)84 (14)69 (12)
bTMB ≥ 4bTMB ≥ 6bTMB ≥ 8bTMB ≥ 10bTMB ≥ 12bTMB ≥ 14bTMB ≥ 16bTMB ≥ 18bTMB ≥ 20bTMB ≥ 22bTMB ≥ 24bTMB ≥ 26
bTMB ≥ 4bTMB ≥ 6bTMB ≥ 8bTMB ≥ 10bTMB ≥ 12bTMB ≥ 14bTMB ≥ 16bTMB ≥ 18bTMB ≥ 20bTMB ≥ 22bTMB ≥ 24bTMB ≥ 26
54 (9)
BEP 583 (100)ITT population 850
PFS HR (95% CI)
0.89 (0.73–1.08)0.83 (0.67–1.03)0.79 (0.62–1.00)0.73 (0.56–0.95)0.73 (0.54–0.97)0.68 (0.50–0.92)0.65 (0.47–0.92)0.66 (0.46–0.95)0.61 (0.40–0.93)0.57 (0.35–0.91)0.54 (0.32–0.91)0.51 (0.28–0.95)
0.87 (0.73–1.04)0.95 (0.82–1.10)
0.2
0.2
a
Fig. 4 | Forest plots showing the association between the clinical benefit of atezolizumab and bTMB in the OAK study. a,b, HRs for PFS (a) and OS (b) in the ITT population, the BEP and cut-points from bTMB!≥ !4 to bTMB!≥ !26. N refers to the absolute number of patients with bTMB data above each cut-point and the prevalence (%) relative to the BEP. The error bars indicate 95% CIs.
NATURE MEDICINE | www.nature.com/naturemedicine

Charge mutationnelle et néo-antigènes
• TMB sérique et bénéfice clinique dans le CBNPC traité par atezolizumab
Gandara, Nature Medecine 2018
ARTICLESNATURE MEDICINE
(BFAST; NCT03178552) of atezolizumab versus standard-of-care doublet chemotherapy in bTMB-positive patients.
The analyses presented here show that a combination of multiple biomarkers may be better at predicting outcomes than any single bio-marker. PFS outcomes were best in patients whose tumors had high PD-L1 expression (TC3 or IC3) and bTMB ≥ 16 (HR: 0.38). We also demonstrated that bTMB and PD-L1 IHC are largely orthogonal to one another, and each could identify a unique subgroup that derived a PFS benefit from atezolizumab and retained an OS benefit in the second-line setting. In addition, the availability of a blood-based assay would be particularly advantageous in the ~30% of patients with NSCLC who lack tumor tissue for molecular testing. However, it is important to note that both the POPLAR and the OAK studies had a mandatory tissue requirement, which may have had an effect on fac-tors that influence the detection of ctDNA (such as tumor burden).
An important limitation of the bTMB assay is that it requires a min-imum amount of ctDNA to be present in the blood for optimal assay performance, meaning that tumors must shed DNA into the blood and that this ctDNA must contain mutations with an allele frequency of ≥ 1% for a bTMB score to be valid. In addition, the likelihood of detecting ctDNA is also dependent on the overall tumor burden. Consistent with this, among OAK patients whose samples passed sequence coverage and contamination quality control, those with a MSAF of < 1% had a lower mean baseline sum of longest diameters than those with a MSAF
of > 1% (62.3 mm versus 80.4 mm, respectively). Another limitation of the bTMB assay is that the TMB calculation is based only on SNVs. Although this did not affect the concordance between bTMB and tTMB in this study, it is conceivable that, in certain rare cases, the assay may miss a patient whose tumor has a large number of indels but rela-tively few SNVs. Future versions of the assay will incorporate indels into the bTMB calling algorithm.
In summary, our data show that measuring bTMB is feasible and that using a cut-point of ≥ 16 reproducibly identifies patients who obtained an increased PFS benefit from atezolizumab. Additional work is needed to better understand the dynamics and biology of bTMB and its relevance to other indications beyond NSCLC. Our data suggest that the integration of this bTMB assay into the molecular diagnostic and therapeutic algorithms for patients who have progressed on first-line therapy for advanced NSCLC may be warranted. Prospective validation of the bTMB assay in first-line NSCLC is ongoing in the randomized phase III BFAST trial.
MethodsMethods, including statements of data availability and any asso-ciated accession codes and references, are available at https://doi.org/10.1038/s41591-018-0134-3.
Received: 13 April 2018; Accepted: 22 June 2018; Published: xx xx xxxx
References 1. Rittmeyer, A. et al. Atezolizumab versus docetaxel in patients with previously
treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 389, 255–265 (2017).
2. Borghaei, H. et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373, 1627–1639 (2015).
3. Brahmer, J. et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373, 123–135 (2015).
4. Reck, M. et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375, 1823–1833 (2016).
5. Fehrenbacher, L. et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016).
bTMB ≥ 16
TC3 or IC3
N = 126 N = 30 N = 73
N = 156N = 103
BEP (N = 229)
a b
20
40
60
0
bTM
B
TC0 and IC0N = 250
TC1/2/3 or IC1/2/3N = 328
TC2/3 or IC2/3N = 200
TC3 or IC3N = 103
Fig. 5 | Comparison of PD-L1 expression and bTMB counts in the OAK study. a, The raw bTMB score is plotted for each patient sample (N represents the number of patients), grouped according to the PD-L1 IHC subgroup. The boxes and the line within the box indicate the 25%, 50% and 75% quartiles for each PD-L1 subgroup. Individual observations are shown as open dots. Within each mutually exclusive IHC subgroup, the lower and upper hinges correspond to the first and third quartiles; the bar in between indicates the median. The upper whiskers extend from the hinge to the largest value no further than the 1.5-times interquartile range from the hinge. The lower whiskers extend from the hinge to the smallest value no further than the 1.5-times interquartile range of the hinge. TC0 and IC0, < 1% of tumor cells and immune cells expressing PD-L1; TC1/2/3 or IC1/2/3, ≥ 1% of tumor cells or immune cells expressing PD-L1; TC2/3 or IC2/3, ≥ 5% of tumor cells or immune cells expressing PD-L1; TC3 or IC3, ≥ 50% of tumor cells or ≥ 10% of tumor-infiltrating immune cells expressing PD-L1. b, A Venn diagram showing the overlap of the 229 patients with bTMB and PD-L1 IHC data; PD-L1 expression was measured by the Ventana PD-L1 (SP142) assay.
Table 1 | OS and PFS HRs in the OAK BEP with valid bTMB and PD-L1 IHC results
N PFS HR (95% CI)
OS HR (95% CI)
bTMB!≥ !16 156 0.64 (0.46–0.91)
0.64 (0.44–0.93)
TC3 or IC3 103 0.62 (0.41–0.93) 0.44 (0.27–0.71)
bTMB!≥ !16 and TC3 or IC3 30 0.38 (0.17–0.85) 0.23 (0.09–0.58)
N represents the number of patients in each subgroup. TC3 or IC3, ≥ 50% of tumor cells or ≥ 10% of tumor-infiltrating immune cells expressing PD-L1.
NATURE MEDICINE | www.nature.com/naturemedicine
ARTICLESNATURE MEDICINE
(BFAST; NCT03178552) of atezolizumab versus standard-of-care doublet chemotherapy in bTMB-positive patients.
The analyses presented here show that a combination of multiple biomarkers may be better at predicting outcomes than any single bio-marker. PFS outcomes were best in patients whose tumors had high PD-L1 expression (TC3 or IC3) and bTMB ≥ 16 (HR: 0.38). We also demonstrated that bTMB and PD-L1 IHC are largely orthogonal to one another, and each could identify a unique subgroup that derived a PFS benefit from atezolizumab and retained an OS benefit in the second-line setting. In addition, the availability of a blood-based assay would be particularly advantageous in the ~30% of patients with NSCLC who lack tumor tissue for molecular testing. However, it is important to note that both the POPLAR and the OAK studies had a mandatory tissue requirement, which may have had an effect on fac-tors that influence the detection of ctDNA (such as tumor burden).
An important limitation of the bTMB assay is that it requires a min-imum amount of ctDNA to be present in the blood for optimal assay performance, meaning that tumors must shed DNA into the blood and that this ctDNA must contain mutations with an allele frequency of ≥ 1% for a bTMB score to be valid. In addition, the likelihood of detecting ctDNA is also dependent on the overall tumor burden. Consistent with this, among OAK patients whose samples passed sequence coverage and contamination quality control, those with a MSAF of < 1% had a lower mean baseline sum of longest diameters than those with a MSAF
of > 1% (62.3 mm versus 80.4 mm, respectively). Another limitation of the bTMB assay is that the TMB calculation is based only on SNVs. Although this did not affect the concordance between bTMB and tTMB in this study, it is conceivable that, in certain rare cases, the assay may miss a patient whose tumor has a large number of indels but rela-tively few SNVs. Future versions of the assay will incorporate indels into the bTMB calling algorithm.
In summary, our data show that measuring bTMB is feasible and that using a cut-point of ≥ 16 reproducibly identifies patients who obtained an increased PFS benefit from atezolizumab. Additional work is needed to better understand the dynamics and biology of bTMB and its relevance to other indications beyond NSCLC. Our data suggest that the integration of this bTMB assay into the molecular diagnostic and therapeutic algorithms for patients who have progressed on first-line therapy for advanced NSCLC may be warranted. Prospective validation of the bTMB assay in first-line NSCLC is ongoing in the randomized phase III BFAST trial.
MethodsMethods, including statements of data availability and any asso-ciated accession codes and references, are available at https://doi.org/10.1038/s41591-018-0134-3.
Received: 13 April 2018; Accepted: 22 June 2018; Published: xx xx xxxx
References 1. Rittmeyer, A. et al. Atezolizumab versus docetaxel in patients with previously
treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 389, 255–265 (2017).
2. Borghaei, H. et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373, 1627–1639 (2015).
3. Brahmer, J. et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373, 123–135 (2015).
4. Reck, M. et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375, 1823–1833 (2016).
5. Fehrenbacher, L. et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016).
bTMB ≥ 16
TC3 or IC3
N = 126 N = 30 N = 73
N = 156N = 103
BEP (N = 229)
a b
20
40
60
0
bTM
B
TC0 and IC0N = 250
TC1/2/3 or IC1/2/3N = 328
TC2/3 or IC2/3N = 200
TC3 or IC3N = 103
Fig. 5 | Comparison of PD-L1 expression and bTMB counts in the OAK study. a, The raw bTMB score is plotted for each patient sample (N represents the number of patients), grouped according to the PD-L1 IHC subgroup. The boxes and the line within the box indicate the 25%, 50% and 75% quartiles for each PD-L1 subgroup. Individual observations are shown as open dots. Within each mutually exclusive IHC subgroup, the lower and upper hinges correspond to the first and third quartiles; the bar in between indicates the median. The upper whiskers extend from the hinge to the largest value no further than the 1.5-times interquartile range from the hinge. The lower whiskers extend from the hinge to the smallest value no further than the 1.5-times interquartile range of the hinge. TC0 and IC0, < 1% of tumor cells and immune cells expressing PD-L1; TC1/2/3 or IC1/2/3, ≥ 1% of tumor cells or immune cells expressing PD-L1; TC2/3 or IC2/3, ≥ 5% of tumor cells or immune cells expressing PD-L1; TC3 or IC3, ≥ 50% of tumor cells or ≥ 10% of tumor-infiltrating immune cells expressing PD-L1. b, A Venn diagram showing the overlap of the 229 patients with bTMB and PD-L1 IHC data; PD-L1 expression was measured by the Ventana PD-L1 (SP142) assay.
Table 1 | OS and PFS HRs in the OAK BEP with valid bTMB and PD-L1 IHC results
N PFS HR (95% CI)
OS HR (95% CI)
bTMB!≥ !16 156 0.64 (0.46–0.91)
0.64 (0.44–0.93)
TC3 or IC3 103 0.62 (0.41–0.93) 0.44 (0.27–0.71)
bTMB!≥ !16 and TC3 or IC3 30 0.38 (0.17–0.85) 0.23 (0.09–0.58)
N represents the number of patients in each subgroup. TC3 or IC3, ≥ 50% of tumor cells or ≥ 10% of tumor-infiltrating immune cells expressing PD-L1.
NATURE MEDICINE | www.nature.com/naturemedicine

Génétique et immunothérapie
ARTICLES NATURE GENETICS
mutations in KRAS occurred predominantly in patients with com-plete or partial response across multiple cancer types (Fig. 2d). Genetic events in PIK3CA and KRAS were too infrequent to fully clarify their relationships to response in this study, but these results demonstrate that single-gene associations with response to immune checkpoint therapy can provide additional information beyond mutational burden, in a manner that may be dependent on or inde-pendent of cancer type.
Despite combining data from multiple studies and cancer types, our analyses were still statistically underpowered to detect important
relationships; thus, we sought to estimate the sample sizes needed for discovery of single-gene correlates of response with appropriate correction for multiple-hypothesis testing (Methods). We modeled statistical significance values for common or rare variants associ-ated with complete or partial response versus progressive disease at various sample sizes (Fig. 2e). In the best-case scenario, where a variant is both relatively common (~10% prevalence) and specific to responders, sample sizes of around 300 would be adequate to detect significant associations. Meanwhile, detection of rare response-associated variants (~1% frequency), even if highly specific, would
–log
10 (P
val
ue) (
Bon
ferr
oni-a
djus
ted)
Number of patients in cohort
Prevalence of mutation1% CR/PR, 0.01% PD 10% CR/PR, 1% PD
5% CR/PR, 0.5% PD 10% CR/PR, 2% PD
10% CR/PR, 4% PD5% CR/PR, 1% PD
5% CR/PR, 2% PD
BRAF
KRAS
NF1
NRAS
PBRM1PIK3CA
TP53
EGFR
–1
0
1
2
3
0 10 20 30 40 50
Res
pond
er s
igni
fican
ce –
log 1
0 (P
val
ue)
Fisher's exact test in CR/PR vs. PDa b
c
d
e
APC
ARID2BRAF
EGFR
KMT2D
KRAS
NF1
NRAS
PIK3CA
PBRM1TP53
–1
0
1
2
3
0 10 20 30 40 50Number of patients with clonal oncogenic mutation in gene
A B B B M H M H L L L L M M B M M M L
B
CR/PR Hotspot mutation Anal cancerABladder cancerBHead and neck cancerHLung cancerLMelanomaM
SD Non-hotspot mutationPD
L L M M L L L L M L L LL LL L L L M M L
PIK3CA hotspots arising fromAPOBEC-associated mutations
Simulated cohort: 40% CR/PR, 60% PDPIK3CA
p.E542Kp.E545Kp.E726Kp.R88Q
p.C420Rp.H1047R
p.E600Kp.V344Gp.S323Fp.R916Cp.E418Kp.D454Hp.V71Ll
p.Q16Hp.L19F
p.G13Dp.G12Vp.G12Sp.G12Dp.GI2C
p.F156Lp.AT8T
p.A155V
KRAS
Logistic regression for CR/PR vs. PDadjusting for mutational burden
0
1
2
3
0 1,000 2,000 3,000 4,000
Enriched inCR/PR
Enriched inPD
Enriched inCR/PR
Enriched inPD
Fig. 2 | Mutations in specific genes associated with response to immune checkpoint therapy. a, Response-associated mutations in CR/PR versus PD (two-tailed Fisher’s exact test, n!= !70 biologically independent samples with CR/PR, n!= !123 biologically independent samples with PD). The dashed red line indicates P!= !0.05 (Fisher’s exact test), and the dashed dark red line indicates q!= !0.05 (FDR). b, Response-associated mutations corrected for mutational burden. Sample size and dashed lines for P- and q-value cutoffs are the same as in a. c,d, Tile plots showing known hotspot and non-hotspot mutations in PIK3CA (c) and KRAS (d) by response group (bottom), with cancer types indicated by capital letter. The top four rows of c represent mutations arising in APOBEC-associated mutational contexts (Supplementary Fig. 6). e, Simulated statistical power calculation for detection of response-associated genes. The significance of association between response and the presence of a mutation in a gene (two-tailed Fisher’s exact test) is shown on the y axis for varying sample sizes (x axis). Colors represent the frequency of mutations and the specificity of alterations to OR versus NR. The dashed horizontal line represents Bonferroni-corrected P!= !0.05 after correcting for multiple comparisons over the 116 cancer driver genes assessed in this study. The simulated cohort contained 40% patients with CR/PR and 60% patients with PD.
NATURE GENETICS | www.nature.com/naturegenetics
• Corrélation altérations génomiques et réponse aux anti PD1 / PDL1 dans les tumeurs solides
Miao D, Nature Medecine 2018

Génétique et immunothérapie
• Corrélation altérations génomiques et réponse aux anti PD1 / PDL1 dans les tumeurs solides
Miao D, Nature Medicine 2018
ARTICLES NATURE GENETICS
10
20
30
40
60
a
b c d e
Mutation clonality Tumor purity
EGFR
hotspotO
ther EGFR
mutation
0.75
0.50
0.25
Subclonal nonsynonymous
Nonsynonymous, clonality unknownSynonymous
Clonal nonsynonymous
40
20
Mut
atio
ns p
er M
b
0
p.T790Mp.L858Rp.G719A
p.ELREA701delp.T363Ap.L707Wp.G428Vp.C781Fp.A871G
p.727_728insHAp.725_726insGT
Response to immunecheckpoint therapy
CR/PR
Smoking history
>5 pack-years
0–5 pack-years
Histology Mutational signature
Adenocarcinoma
Squamous cell carcinoma
Smoking (S4)
Unknown (S5)
APOBEC (S2 or S13)
Aging (S1)
Unspecified NSCLC
Small cell
SD
PD
40 0.7540
ns ns ns ns
30
20
10
0
Aging/unknown(S1/S5) dominant
(n = 27)
APOBEC/smoking(S2/S13/S4) dominant
(n = 30)
*** **
0.50
0.25
0.00
CR/PR SD PD
CR/PR SD PD
ns ns
30.2%
71.4%
53.5%
Majority clonalmutations (n = 43)
Majority subclonalmutations (n = 14)
Dominant mutationalsignature (n = 57)
**
30
20
10
0
Aging/unknown
APOBEC
Smoking
No EGFR hotsp
ot mutatio
n
EGFR hotspot m
utation
Non
syno
nym
ous
mut
atio
ns p
er M
b
Prop
ortio
n of
mut
atio
ns s
ubcl
onal
Non
syno
nym
ous
mut
atio
ns p
er M
b
Fig. 3 | Integrated analysis of EGFR mutational status, intratumoral heterogeneity, and mutational signatures in lung cancer. a, Stacked plots show mutational burden (histogram, top), estimated tumor purity (tile plot, top), mutations in EGFR (tile plot, middle), mutational signatures (filled histogram, middle), and clinical response and clinical covariates (bottom). b, Interaction between smoking-related mutational signatures and mutational burden. For aging/unknown versus smoking signatures, P!= !0.0001; for aging/unknown versus APOBEC, P!= !0.43; for APOBEC versus smoking, P!= !0.158. c, Proportion of patients with a given dominant mutational signature by clonal mutation composition. d, Proportion of subclonal mutations in EGFR-mutant versus EGFR-wild-type tumors (n!= !57 biologically independent samples, P!= !0.035, unpaired two-sample t test). e, Relationship between mutational burden and response by dominant mutational signature (aging/unknown-dominant samples: CR/PR versus PD, P!= !0.0044; CR/PR versus SD, P!= !0.07; SD versus PD, P!= 0.060; APOBEC/smoking-dominant samples: CR/PR versus PD, P!= !0.0023; CR/PR versus SD, P!= !0.08; SD versus PD, P!= !0.25). A two-sided Mann–Whitney U test was used in b and e: *P!< !0.05, **P!< !0.005; ns, not significant. The box plots in b, d and e show the median, first and third quartiles, whiskers extend to 1.5 times the interquartile range, and outlying points are plotted individually.
NATURE GENETICS | www.nature.com/naturegenetics

Génétique et immunothérapie
• Et les addictions oncogéniques ?
Mazieres J, ASCO 2018
Driver PD SD CR/PR
BRAF 46% 30% 24%
MET 50% 34% 16%
KRAS 51% 23% 26%
HER2 67% 26% 7%
EGFR 67% 21% 12%
ALK 68% 32% 0
RET 75% 19% 6%
ROS1 83% 0 17%
TOTAL 57% 24% 19%

Génétique et immunothérapie
• Impact de STK11-LKB11 • Démontré en co-mutation de KRas
• Dans les CBNPC PDL1 +
Skoulidis, Cancer Disc 2018
STK11/LKB1 genomic alterations promote primary resistance to PD-1/PD-L1 inhibitor monotherapy in non-squamous NSCLC
0%
34.5%
SU2C cohort
KRAS-mutant LUAC
PD-L1 expressing non-squamous NSCLCMDACC cohort (N=66)
P=0.026, Fisher’s exact test
Skoulidis F et al., Cancer Discovery, 2018
Ferdinandos Skoulidis M.D., Ph.D., The University of Texas MD Anderson Cancer Center, USA

Génétique et immunothérapie
• Score composite avec 5 éléments sur biopsie liquide
Guibert, ASCO 2018, soumis.
PFS Training Inivata Immune High = 14 mos (14 - 14 mos)
Inivata Immune Low = 2 mos (2 - 2 mos) Test Set Inivata Immune High = 10 mos (8 - 24 mos)
Inivata Immune Low = 1.5 mos (1.5 - 2 mos)
Comparison of survival curves (Logrank test) P = 0.0009
Hazard Ratio - Training 3.582 (1.50-8.57) Hazard Ratio - Test 2.866 (1.22-6.73)
TargetableDriver?BRAFV600E,EGFR,
ROS1,ALK
ImmuneLow-TargetedTherapy
ctDNADetected Indeterminant
STK11orPTENmutation?
ImmuneLow
SomaticSignature ImmuneHigh
ImmuneLow
Yes
Yes
Yes
No
No
No
No
Yes

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI, MDSC,…)
Suppression immunitaire
(PDL1, CTLA4,…)
TUMEUR
HOTE (microbiote)

Le microbiote Microbiome and response
to anti-PD1/L1
Routy et al, Science 2017Gopalakrishnan et al, Science 2017
• Intérêt du microbiome en oncologie: marqueur et ciblé thérapeutique
Routy B, Science 2018

Le microbiote
Routy et al., Science 359, 91–97 (2018) 5 January 2018 4 of 7
SPF
FMT
MCA-205inoculation
αPD-1
D-18
D-15
D0
D+5
D+14
ATB
GF
Germ - free
0 5 10 15 200
50
100
150
200
250 Iso CtrlαPD-1
n=5
Iso CtrlαPD-1
NR
R
*
Days after tumor inoculation
MC
A-2
05Tu
mor
siz
e (m
m2 )
SPF + ATB
0 5 10 15 200
50
100
150
200
n=6
***
L1 L2 L5 L6 L3 L4
NR
- +αPD-1 &αCTLA-4
R
- +
FMT
RE
NC
AN
orm
aliz
ed T
otal
Flu
x (D
x/D
0)
TILs
% C
XC
R3
NR
- +αPD-1
R
- +FMT
0
10
20
30
40**
80
85
90
95
100 ***
NR
- +αPD-1
R
- +FMT
Spl
enoc
ytes
L7 L8
10
100
1000
10000 **
Iso Ctrl
0
100
200
300
NR R
ns
Tum
or s
ize
(mm
2 )
FMT FMT
αPD-1 ***
NR R
MC
A-2
05
FMT NR R
** ** **
* ****
**
αPD-1
Iso-CtrlαPD-1 &αCTLA-4
NR
R
2.0
1.5
1.0
0.5
x10 8
/ CD
4
+
+
% P
D-L
1 / C
D4
+
+Fig. 3. Fecal microbiota transplantation(FMT) of stool samples from NSCLC and RCCpatients into mice dictates outcome afterPD-1 blockade. (A) Experimental setting: FMTwas performed in germ-free recipients or after3 days of ATB in SPFmice.Two weeks later,MCA-205 sarcoma cells were inoculated andPD-1 mAb was injected intraperitoneally every3 days starting on D+5. (B) RepresentativeMCA-205 tumor growth curves after FMT fromNSCLC patients into germ-free (left) or ATB-treatedmice (right) during therapy with PD-1mAb.(C) Means ± SEM of tumor sizes after Iso CtrlmAb(left) or after PD1 mAb (center and right) in MCA-205–bearing, SPF-reared mice treated with ATBand then receiving FMT fromeight NSCLCpatients(n = 4 NR, n = 4 R) before PD1 mAb. Pooled datafrom all patients (left and center) or individualpatients (right) are shown; each fecal sample wastransferred into fivemice per group. (D andE) Flowcytometry analysis of CXCR3 (D) or PD-L1 (E)expression on tumor-infiltrating lymphocytes(TILs) (D) or CD3+CD4+ splenocytes (E) in 38 and80 animals, respectively, analyzed at killing timescorresponding to those in (C). (F) Monitoring ofRENCA progression via bioluminescence imagingof luciferase activity in ATB-treated mice (n = 133)after FMTwith feces from threeR and fourNRRCCpatients and treated with a combination of PD-1and CTLA-4 mAbs. All experiments included five toseven mice per group and were performed atleast twice in similar conditions yielding similarresults. Data are means ± SEM. *P < 0.05, **P <0.01, ***P < 0.001 (ANOVA and Student t test).Dx, last IVIS (bioluminescent imaging)measurement; D0, day of randomization.
RESEARCH | REPORT
on April 7, 2018
http://science.sciencemag.org/
Dow
nloaded from
• Intérêt du microbiome en oncologie: marqueur et ciblé thérapeutique
Routy B, Science 2018

Le microbiote
influence the host immune system. The genera-tion of diagnostic tools and novel therapeuticswill provide a challenge that will require molec-ular analysis of the microbiome, metabolism, andimmunity cycle via novel “omics” technologiesand subsequent integration through systems bio-logy methods (Fig. 2).
Microbial interventionsas a cancer therapeutic
If patients lack colonizationwith a community ofcommensal microbes that support endogenousT cell priming against tumor antigens, it is some-what intuitive to consider FMT from a donor pa-tient who has a favorable microbiome. Impressiveresults of FMT (up to 81% response rate) are wellknown to be effective for the treatment of re-fractory Clostridium difficile diarrhea (29). How-ever, there are multiple critical parameters toconsider for this approach, most notably the se-lection of the ideal donor. In principle, it shouldbe an individual with a diverse microbial com-position that includes bacteria associated withfavorable treatment outcomes. One consideration
could be to usematerial from cancer patients thathad a major clinical response to mAbs to PD-1.However, there are reasons to approach this strat-egy with caution. In addition to modulating im-mune responses, the composition of commensalmicrobiota has been linked to chronic diseases,with a theoretical risk of transferring obesity fromdonor to recipient (30). Transfer of pathogens isalso a potential concern—either bacterial, viral,or parasitic—necessitating careful screening. Inaddition, some bacteria appear to contribute toinflammation-induced carcinogenesis. FMT fromcolorectal patients into germ-free mice can elicitdysplasia and polyp formation, which did not occurwith transplantation from normal donors (31).Additional variables are whether to use fresh orfrozen donor fecal material, identification of op-timal storage conditions, andwhether a single FMTis sufficient, or multiple will be required (32).A desirable alternative to transfer of a mixed
population of commensal bacteria from a givendonor is to use defined bacteria, either singly orin combination. This strategy will depend onidentification of the precise bacterial isolates
capable of supporting improved antitumor immu-nity in the human host, combined with cultureconditions that can support their expansionin vitro and encapsulation protocols that preservebiologic activity upon oral administration. Thecurrent 16S rRNA and shotgun sequencing strat-egies are likely preferentially detecting the mostabundant bacteria correlatedwith favorable clin-ical outcome. However, it is conceivable that lessabundant bacterial entities that coexist with themore abundant species are functionally impor-tant. Therefore, careful culture, isolation, andmech-anistic testing of rare species (some ofwhichmayreside in the small intestine and be less abundantin stool samples) will need to be considered.Communities of bacteria also may be involved inthe immune-potentiating effects of gut microbes,rather than a singlemajor species. For protectionagainst vancomycin-resistant Enterococci feacium,a consortium of five bacteria was identified thatfunctioned together in vivo (33). Because only aminority of bacterial entities identified throughsequencing appear to be culturable with standardmethods, improvement of protocols for optimal
Zitvogel et al., Science 359, 1366–1370 (2018) 23 March 2018 4 of 5
ToxicityEfficacy
Microbiome therapy Fecal microbial transplantation
BiomarkersSequencing stool samples
Precision medicineComputational biologist
Therapy optimizationImmunotherapeutic effects
Drug discoveryMicrobiome-derived compounds or microbiome -targeted drugs
Fig. 2. Harnessing the microbiome for the discovery of diagnosis andtherapeutic tools in cancer.The complex interplay between cancer,immunity, and microbiota may be partially elucidated by novel “omics”technologies: metagenomics, metatranscriptomics, culturomics,metabolomics, co-occurrence analyses, and three-dimensional cryptstem cell–derived enteroid in contact with distinct species of the microbiomeand immune subsets, all integrated through computational biology. Suchan apothecary of omics technologies will generate diagnosis tools fordysbiosis, for drug screening and novel therapeutics, such as artificialecosystems or new microbial species, as well as small bioactives that eitheract on the microbiota to induce favorable shifts in its composition or mimic
desirable microbial effects on the host. Microbial intervention as acancer therapeutic includes prebiotics, probiotics or live bacteria (andassociated phages), and natural products (autologous or allogeneic fecalmicrobial transplantation). These interventions will have to be adaptedaccording to the patient’s life style, comorbidities, comedications, andgenetic inheritance for an optimized personalization of his or her therapy.Building on pioneering studies (14, 19, 20), new biomarkers based onmicrobial composition of the stool will likely emerge. Monitoring themicrobiome will also be essential as a pharmacokinetic and dynamicparameter, longitudinally on new interventional studies aimed attargeting the intestinal ecosystem.
CRE
DITS(G
RAPH
IC)K
.SUTL
IFF/SC
IENCE
on April 7, 2018
http://science.sciencemag.org/
Dow
nloaded from
Zitvogel, Nature Med 2018
• Intérêt du microbiome en oncologie: marqueur et ciblé thérapeutique

Le microbiote
Figure 1: Best overall response (A), progression-free survival (B), and overall survival (C) in patients with RCC treated with ICI, stratified by use of ATB within 30 days of initiating ICI. Best overall response (D),
progression-free survival (E), and overall survival (F) in patients with NSCLC treated with ICI, stratified by use of ATB within 30 days of initiating ICI. P-values calculated with chi-squared and log rank tests.
213x151mm (100 x 100 DPI)
Downloaded from https://academic.oup.com/annonc/advance-article-abstract/doi/10.1093/annonc/mdy103/4956695by Inserm/Disc useron 07 April 2018
• Impact de la prescription d’antibiotiques sur la réponse aux ICI
• Effet négatif sur la PFS et la survie globale de patients traités par immunothérapie
Derosa L, Annals Oncol 2018

Les biomarqueurs en immunothérapie
Antigènes tumoraux (TMB, MSI, néo-
antigènes,..)
Inflammation (gene signature, TILS,
LIPI, MDSC,…)
Suppression immunitaire
(PDL1, CTLA4,…)
TUMEUR
HOTE (microbiote)

Synthèse des tests prédictifs
Expression de PD-L1
Charge mutationnelle
Signature inflammatoire
Technique IHC Séquençage Signature d’expression
Matériel 1-2 lames FFPE Tissu congelé. FFPE (6-10 lames ?)
2-3 lames FFPE
Technique IHC sur lames NGS, RNAseq, bioinformatique
Extraction ARN. Nanostring
Complexité Faible Elevée Modérée
Délai 3-5 jours 2 semaines 10 jours
Prédiction modérée Modérée-forte Modérée-forte
Commentaires Méthodes variables
Complexe (difficile en routine)
Quantitatif. Automatisé

Synthèse des tests prédictifs
Peters S, ASCO 2018

Conclusion
D’après Peters S, ASCO 2018
CBNPC

Conclusion
PDL1
TMB
Microbiote
MDSC
Methylation

COURS DU GOLF 7 AU 10 OCTOBRE 2019
Groupe d’Oncologie de la Société de Pneumologie de Langue Française
TOULOUSE Amphithéâtre Pierre Paul Riquet,
Hôpital Purpan.
Comité d’organisation J. Mazieres
L. Bigay-Game L. Brouchet
A. Rabeau I. Rouquette
J. Khalifa C. Massabeau
Inscription [email protected]

Back-up

QUIZZ 1
• Question 1: Quels tests ont montré leur intérêt dans un essai clinique d’immunothérapie en oncologie thoracique.
1. Charge mutationnelle 2. LIPI score 3. Expression de PDL1 4. Lymphocyte T gene signature (Teff) 5. Microbiote digestif

QUIZZ 1
• Question 1: Quels tests ont montré leur intérêt dans un essai clinique d’immunothérapie en oncologie thoracique.
1. Charge mutationnelle 2. LIPI score 3. Expression de PDL1 4. Lymphocyte T gene signature (Teff) 5. Microbiote digestif

QUIZZ 2
• Question 2: Quel(s) test(s) est/sont validés en routine en oncologie thoracique.
1. Charge mutationnelle 2. LIPI score 3. Expression de PDL1 4. Test Teff 5. Microbiote digestif

QUIZZ 2
• Question 2: Quel(s) test(s) est/sont validés en routine en oncologie thoracique.
1. Charge mutationnelle 2. LIPI score 3. Expression de PDL1 4. Test Teff 5. Microbiote digestif

Charge mutationnelle et néo-antigènes
• Analyse de la réponse au pembrolizumab dans le CBNPC selon la « signature » mutationnelle.
Rizvi N, Science 2015
[encoding programmed cell death ligand-1 (PD-L1)]that were associated with response or resistance.
How does increased mutation burden affect tu-mor immunogenicity? The observation that non-synonymous mutation burden is associated withpembrolizumab efficacy is consistent with thehypothesis that recognition of neoantigens, formedas a consequence of somatic mutations, is impor-tant for the activity of anti–PD-1 therapy. We ex-amined the landscape of neoantigens using ourpreviously described methods (25) (fig. S7). Briefly,this approach identifies mutant nonamers with≤500 nM binding affinity for patient-specific classI human lymphocyte antigen (HLA) alleles (26, 27),which are considered candidate neoantigens (tableS6). We identified a median of 112 candidate neo-antigens per tumor (range 8 to 610), and the quan-tity of neoantigens per tumor correlated withmutation burden (Spearman r 0.91, P < 0.0001),similar to the correlation recently reported acrosscancers (28). Tumors from patients with DCB hadsignificantly higher candidate neoantigen bur-den compared to those with NDB (Fig. 4A), andhigh candidate neoantigen burden was associatedwith improved PFS (median 14.5 versus 3.5 months,log-rank P = 0.002) (Fig. 4B). The presence of sp-
ecific HLA alleles did not correlate with efficacy(fig. S8). The absolute burden of candidate neo-antigens, but not the frequency per nonsynony-mous mutation, correlated with response (fig. S9).We next sought to assess whether anti–PD-1
therapy can alter neoantigen-specific T cell re-activity. To directly test this, identified candidateneoantigens were examined in a patient (StudyID no. 9 in Fig. 3 and table S3) with exceptionalresponse to pembrolizumab and available pe-ripheral blood lymphocytes (PBLs). PredictedHLA-A–restricted peptides were synthesized toscreen for ex vivo autologous T cell reactivity inserially collected PBLs (days 0, 21, 44, 63, 256, and297, where day 0 is the first date of treatment)using a validated high-throughput major histo-compatibility complex (MHC) multimer screeningstrategy (29, 30). This analysis revealed a CD8+T cell response against a neoantigen resultingfrom a HERC1 P3278S mutation (ASNASSAAK)(Fig. 4C). Notably, this T cell response could onlybe detected upon the start of therapy (level ofdetection 0.005%). Three weeks after therapyinitiation, the magnitude of response was 0.040%
126 3 APRIL 2015 • VOL 348 ISSUE 6230 sciencemag.org SCIENCE
0 4 8 12 16 20 240
5 0
1 0 0
Transversion high Transversion low
Perc
ent p
rogr
essi
on-fr
ee 100
50
0
Months 4 8 12 16 20 24
Fig. 2. Molecular smoking signature is significantlyassociated with improved PFS in NSCLC patientstreated with pembrolizumab. PFS in tumors char-acterized as TH by molecular smoking signatureclassifier (n = 16) compared to TL tumors (n = 18)(HR 0.15, 95% 0.06 to 0.39, log-rank P = 0.0001).
Fig. 3. Mutation burden, clinical response, and factors contributing tomutation burden.Total exonic mutation burden for each sequenced tumor withnonsynonymous (dark shading), synonymous (medium shading), and indels/frameshift mutations (light shading) displayed in the histogram. Columns areshaded to indicate clinical benefit status: DCB, green; NDB, red; not reached6 months follow-up (NR), blue. The cohort identification (D, discovery; V, valida-
tion), best objective response (PR, partial response; SD, stable disease; PD,progression of disease), and PFS (censored at the time of data lock) are reportedin the table.Those with ongoing progression-free survival are labeled with ++.Thepresence of the molecular smoking signature is displayed in the table with THcases (purple) and TL cases (orange). The presence of deleterious mutations inspecific DNA repair/replication genes is indicated by the arrows.
RESEARCH | REPORTS



Charge mutationnelle et néo-antigènes
• Combien de gènes doit comporter le test TMB ?
Garofalo et al. Genome Medicine. 2016

ARTICLESNATURE GENETICS
response (Figs. 2a,b and 5f, and Supplementary Fig. 13). Other mutations that have previously been described in association with acquired resistance to immune checkpoint therapies include JAK–STAT pathway mutations and alterations in antigen-presentation machinery (for example, β 2-microglobulin and tapasin)40,41. Loss-of-function mutations and deletions in these pathways were rare in this cohort (Supplementary Fig. 14a–c), perhaps reflecting differ-ences in genetic mechanisms of intrinsic versus acquired resistance, and further work is required to determine the functional signifi-cance of these variants.
Neoantigens associated with response to immune checkpoint therapy. Given the complexities of computationally assessing the impact of oncogenic pathway alterations and tumor mutational burden on response to immune checkpoint therapy, we lastly exam-ined mutations that could more directly influence tumor–immune interactions by generating tumor-specific neoantigens that induce a T cell–mediated antitumor response42. We inferred neoantigens in silico (Methods and Supplementary Table 10) and found that, on average, each nonsynonymous mutation generated 2.24 predicted neoantigens, with extremely high correlation between nonsynony-mous mutational burden and neoantigen burden across patients (R2 = 0.99, P < 0.00001) (Fig. 6a), making it difficult to disentangle the effects of mutational versus neoantigen burden on response using in silico methods alone.
Recent studies have demonstrated that personalized cancer vac-cines targeting neoantigens specific to an individual’s tumor can lead to durable clinical benefit alone or in concert with immune
checkpoint blockade therapies43,44. More than 99% of the predicted neoantigens in this study arose from passenger mutations, which occur throughout the exome, are frequently found in subclonal tumor populations, and are largely unique to each patient’s tumor. However, 871 predicted neoantigens were generated by driver mutations, and 8 of these ‘driver’ neoantigens occurred recurrently in patients with complete or partial response but not in patients with progressive disease, in a human leukocyte antigen (HLA)-dependent manner (Fig. 6b,c). Additionally, as expected given the known oncogenic effects of the mutations yielding these neoanti-gens, these eight neoantigens were clonal in all samples, suggesting that a T cell–mediated response, if present, would target all can-cer cells14. Thus, driver alterations can generate tumor neoantigens and may contribute to provoking an effective immune response to checkpoint blockade therapy in HLA-matched patients, although further experimental study is required to clarify the biological sig-nificance of these putative neoantigens.
DiscussionWES and analysis of 249 tumors from patients treated with anti-PD-1/PD-L1 or anti-CTLA-4 therapies suggest that genomic fea-tures beyond mutational burden, including genetic driver events, intratumoral heterogeneity, and mutational signatures, may affect response to immune checkpoint blockade. In this work, we com-bined data from multiple institutions using a standardized compu-tational pipeline and applied a uniform and well-accepted definition of radiographic response to cancer therapy to more robustly assess genetic predictors of response to immune checkpoint therapy.
10,000
a
c
b
244,240 unique predicted neoantigensin 249 pre-treatment tumor samples
870 neoantigens arisingfrom driver mutations
8 neoantigens arisingfrom driver mutations
seen recurrently inCR/PR but not PD
R 2 = 0.99
10,000
5,000
5,000
Nonsynonymous mutations/exome
Predicted neoantigen burden =2.24 × (nonsynonymous mutation burden) – 12.4P
redi
cted
neo
antig
ens/
exom
e (r
ank
< 2%
)
0
0
Peptide Mutation Cancer type HLA Response
KRAS p.G12D Bladder, lung A03:01, A11:01 3 PR
2 PR
2 PR
2 PR
2 PR, 1 SD
2 PR, 1 SD
2 PR, 2 SD
1 CR, 1 PR, 1 SD
A11:01, A03:01
A11:01, A03:01
A11:01, A03:01
B44:02, B44:03
C07:01, C07:02
C07:01, C07:02
A02:01
Bladder, lung
Bladder, lung
Bladder, lung
Bladder, lung, anal
Melanoma, HNSCC
Melanoma, HNSCC
Lung
BRAF p.G469A
BRAF p.G469A
BRAF p.G469A
PIK3CA p.E545K
PIK3CA p.H1047R
PIK3CA p.H1047R
KRAS p.G12C
Fig. 6 | Response-associated in silico–predicted neoantigens. a, Relationship between predicted neoantigen burden (y axis) and nonsynonymous mutational burden (x axis). Linear regression excludes one outlier (Pat110) (n!= !249 biologically independent samples). b, Prioritization of clinically actionable predicted neoantigens by presence in cancer driver genes and exclusive presence in CR/PR samples. c, Response-associated predicted neoantigens generated by cancer driver mutations.
NATURE GENETICS | www.nature.com/naturegenetics

initially hypothesized that TMB in patients with NSCLCs wouldnot impact response to PD-1 plus CTLA-4 blockade therapy. Inan analogous scenario, the impact of PD-L1 expression isabated in patients with melanoma treated with PD-1 plusCTLA-4 blockade (Wolchok et al., 2017), and in a report of 17 pa-tients with melanoma treated with combination immunotherapy,TMB did not correlate with response (Goodman et al., 2017). Incontrast, we found that TMB is the strongest predictor of efficacyidentified in our dataset of patients with NSCLC. Similar resultswere seen in a recent report of patients with small cell lung can-cer treated with PD-1 plus CTLA-4 blockade (Hellmann et al.,2018), suggesting the importance of TMB as biomarker for com-bination immunotherapy across lung cancers.Given the correlation between TMB and efficacy, it is tanta-
lizing to consider how TMB may be applied prospectively as abiomarker. One criticism of determining TMB by WES, as wehave in this study, is that WES is currently challenging to perform
in an expeditious time frame and at adequate scale needed forgeneral use in patients with advanced NSCLC. Emerging inde-pendent sets of data have demonstrated that targeted next-gen-eration sequencing (NGS) panels, which are already being usedroutinely in clinic, may provide a reasonable estimate of exonicmutation burden (Chalmers et al., 2017; Rizvi et al., 2018; Zehiret al., 2017). We found that estimated TMB using only genescovered in US Food and Drug Administration-approved targetedNGS panels MSK-IMPACT (Zehir et al., 2017) and Foundatio-nOne (Frampton et al., 2013) were similarly predictive to theTMB derived from WES. These currently available assays mayprovide a practical platform for clinical practice now. Further-more, although the technology is still being optimized, use ofcell-free DNA in plasma to estimate TMB has recently beenshown to be feasible and, when detectable, to correlate withTMB estimated from tumor tissue (Fabrizio et al., 2017; Gandaraet al., 2017).
Figure 2. Summary of Clinical and Molecular Features Associated with Response or Non-response in Patients with NSCLC Treated withNivolumab Plus IpilimumabIndividual patients are represented in each column, organized by those with objective response on the left (blue) and those with no objective response on the right
(red). Categories of histology (squamous or non-squamous) and smoking status (never or ever) are characterized. PD-L1 expression is stratified as 0%, 1%–49%,
orR50%. PFS is shown in months, with the color of each bar representing those who are censored (dark blue) or have progressed (light blue). The NSCLC TCGA
percentile rank for each case is described from 0% to 100% in light to dark purple. Nonsynonymous TMB andmutation burden quantified using genes including in
theMSK-IMPACT targeted next-generation sequencing panel are shown in histograms. The percent of transitions (light green) and transversions (dark green) are
shown. Candidate neoantigen burden is quantified in histograms, stratified by predicted patient-specific HLA binding affinity 0–50 nM (orange) or 50–500 nM (light
yellow). The occurrences of selected genes in each case are represented in the oncoprint, with the percent frequency in responders or non-responders shown.
See also Figures S2 and S3; Tables S3 and S4.
Cancer Cell 33, 843–852, May 14, 2018 847

Génétique et immunothérapie
Cancer Therapy: Clinical
EGFR Mutations and ALK Rearrangements AreAssociated with Low Response Rates to PD-1Pathway Blockade in Non–Small Cell Lung Cancer:A Retrospective AnalysisJustin F. Gainor1, Alice T. Shaw1, Lecia V. Sequist1, Xiujun Fu2, Christopher G. Azzoli1,Zofia Piotrowska1, Tiffany G. Huynh2, Ling Zhao2, Linnea Fulton1, Katherine R. Schultz1,Emily Howe1, Anna F. Farago1, Ryan J. Sullivan1, James R. Stone2, Subba Digumarthy3,Teresa Moran4, Aaron N. Hata1, Yukako Yagi2, Beow Y.Yeap1, Jeffrey A. Engelman1, andMari Mino-Kenudson2
Abstract
Purpose: PD-1 inhibitors are established agents in the man-agement of non–small cell lung cancer (NSCLC); however, only asubset of patients derives clinical benefit. Todetermine the activityof PD-1/PD-L1 inhibitors within clinically relevant molecularsubgroups, we retrospectively evaluated response patterns amongEGFR-mutant, anaplastic lymphoma kinase (ALK)-positive, andEGFR wild-type/ALK-negative patients.
Experimental Design: We identified 58 patients treated withPD-1/PD-L1 inhibitors. Objective response rates (ORR) wereassessed using RECIST v1.1. PD-L1 expression and CD8þ
tumor-infiltrating lymphocytes (TIL) were evaluated by IHC.Results:Objective responses were observed in 1 of 28 (3.6%)
EGFR-mutant or ALK-positive patients versus 7 of 30 (23.3%)EGFR wild-type and ALK-negative/unknown patients (P ¼0.053). The ORR among never- or light- (#10 pack years)smokers was 4.2% versus 20.6% among heavy smokers (P ¼0.123). In an independent cohort of advanced EGFR-mutant
(N¼ 68) and ALK-positive (N¼ 27) patients, PD-L1 expressionwas observed in 24%/16%/11% and 63%/47%/26% of pre–tyrosine kinase inhibitor (TKI) biopsies using cutoffs of $1%,$5%, and $50% tumor cell staining, respectively. AmongEGFR-mutant patients with paired, pre- and post-TKI–resistantbiopsies (N ¼ 57), PD-L1 expression levels changed afterresistance in 16 (28%) patients. Concurrent PD-L1 expression($5%) and high levels of CD8þ TILs (grade $2) were observedin only 1 pretreatment (2.1%) and 5 resistant (11.6%) EGFR-mutant specimens and was not observed in any ALK-positive,pre- or post-TKI specimens.
Conclusions:NSCLCs harboring EGFRmutations or ALK rear-rangements are associated with low ORRs to PD-1/PD-L1 inhi-bitors. Low rates of concurrent PD-L1 expression and CD8þ TILswithin the tumor microenvironment may underlie these clinicalobservations. Clin Cancer Res; 22(18); 4585–93. !2016 AACR.
See related commentary by Gettinger and Politi, p. 4539
IntroductionTwo major treatment paradigms have recently emerged in the
management of non–small cell lung cancer (NSCLC): targetedtherapies and immunotherapy. The former relies on stratificationand treatment based upon genetic alterations in oncogenic dri-vers, such as EGFR and anaplastic lymphoma kinase (ALK).Despite the impressive activity of tyrosine kinase inhibitors (TKI)
in these subgroups (1, 2), resistance almost invariably develops(3). Furthermore, a significant proportion of patientswithNSCLCdo not have genetic alterations that are currently targetable withFDA-approved therapies (4).
More recently, mAbs targeting the programmed death 1 (PD-1)receptor and its ligand (PD-L1) have demonstrated impressiveantitumor activity in NSCLC (5–7). Furthermore, in randomizedphase III trials, the PD-1 inhibitors nivolumab and pembrolizu-mab have produced significant improvements in overall survivalcomparedwith single-agent docetaxel delivered in the second-linesetting, effectively establishing a new standardof care (8–10). Thishas culminated in the regulatory approvals of nivolumab andpembrolizumab in the United States for NSCLC patients withdisease progression on or after platinum-based chemotherapy.
Despite the promise of PD-1/PD-L1 inhibitors in NSCLC, it isnoteworthy thatmost patients donot respond to therapy (ORRs¼20%), underscoring the need for better predictive biomarkers(8, 9). In analyses to date, increased PD-L1 expression has gen-erally been associated with higher ORRs to PD-1/PD-L1 blockade(5–7). Studies have also shown a strong association betweenPD-L1 expression and improved clinical outcomes with PD-1/PD-L1 inhibition compared with chemotherapy (9, 11).
1Department of Medicine, Massachusetts General Hospital, Boston,Massachusetts. 2Department of Pathology, Massachusetts GeneralHospital, Boston, Massachusetts. 3Department of Radiology, Massa-chusetts General Hospital, Boston, Massachusetts. 4Catalan Instituteof Oncology, Barcelona, Spain.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Authors: Justin F. Gainor, Department of Medicine, Massachu-setts General Hospital, 10 North Grove Street, POB #238, Boston, MA 02114.Phone: 617-724-4000; Fax: 617-726-0453; E-mail: [email protected]; andMari Mino-Kenudson, [email protected]
doi: 10.1158/1078-0432.CCR-15-3101
!2016 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 4585smokers was 4.2% versus 20.6% among heavy smokers (P ¼0.123; Fig. 1B). As this analysismay have been confounded by theassociation between a lack of smoking and the presence of EGFRmutations andALK rearrangements, we also investigated responserates to PD-1/PD-L1 inhibitors as a function of smoking withineach molecular subgroup. Among EGFR-mutant or ALK-positivepatients, one unconfirmed partial response was observed among22 never-/light-smokers (ORR 4.5%), and no responses were seenamong six heavy smokers. Within the EGFR WT and ALK-nega-tive/unknown group, seven partial responses were seen among 28heavy smokers (25%). Only two never-/light-smokers were in theEGFR WT and ALK-negative cohort, neither of whom respondedto PD-1/PD-L1 inhibitors. Further assessments of smoking statusindependent of EGFR and ALK status were limited by sample size.
Altogether, our data suggest that patients with EGFRmutationsand ALK rearrangements have a significantly shorter PFS (Fig. 1C)and a trend toward lower response rates to PD-1/PD-L1 inhibitorscompared with EGFR WT/ALK-negative patients.
PD-L1 expression in EGFR-mutant and ALK-positive patients:Baseline
In light of the low antitumor activity of PD-1/PD-L1 inhibitorsin our EGFR-mutant and ALK-positive cohorts above, we soughtto investigate patterns of PD-L1 expression and levels of TILs inthese molecular subgroups. Amajority of EGFR-mutant and ALK-positive patients who received PD-1 inhibitors above had beentreated previously with TKIs. Thus, wewished to determine PD-L1expression and levels of CD8þ TILs in both treatment-na€"ve andTKI-resistant cancer. Because of tissue availability, our analyseswere limited to a separate cohort of 95patientswith EGFR-mutant(N ¼ 68) or ALK-rearranged (N ¼ 27) NSCLC. Baseline clinico-pathologic characteristics are summarized in Supplementary
Table S1. Of note, this population consisted largely of patientswho did not receive PD-1/PD-L1 inhibitors during their diseasecourse.
We first evaluated PD-L1 expression in EGFR-mutant patients(N ¼ 62) using tissue samples obtained prior to EGFR TKItreatment. PD-L1 expression was observed in 15 (24%), 10(16%), and 7 (11%) patients using cutoffs of #1%, #5%, and#50% tumor cell staining, respectively (Table 2). To contextualizethese findings, we next identified a cohort of 65 patients withadvanced, KRAS-mutant NSCLC and performed PD-L1 expres-sion analysis. KRAS-mutant lung cancer was used as a comparatorto have a homogeneous control population. Moreover, KRASmutations are the most frequent oncogenic driver in NSCLC (4).Among KRAS-mutant patients, we observed PD-L1 expression in23 (35%), 20 (31%), and 11 (17%) patients using cutoffs forpositivity of #1%, #5%, and #50%, respectively (Table 3).Although these rates were consistently higher than those amongEGFR-mutant specimens, the numerical differences were notstatistically significant due to limited power.
Recently, PD-L1 expression and the presence of TILs have beenshown to be associated with clinical outcomes to PD-1/PD-L1inhibitors (6, 17). Therefore, we next performed CD8 IHC andquantitative, image-based CD8 TIL analysis in our cohorts ofEGFR-mutant and KRAS-mutant patients (Tables 2 and 3). ByIHC, CD8þ TILs were present in 31 of 48 (65%) evaluable, EGFR-mutant cases, but only 2 (4.2%) showed high levels (grade #2).Moreover, only 1 (2.1%) treatment-na€"ve EGFR-mutant patientexhibited both PD-L1 expression (#5%) and high-level CD8þ
TILs in the same specimen. When CD8þ TILs were quantifiedusing a digital imaging platform, similar findings were observed(Table 2). Only 2 of 46 (4.3%) EGFR-mutant specimens hadconcurrent PD-L1 expression and highCD8þ TILs (#330.1/mm2).
C
A
ORR
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
EGFR-mutant or ALK-posi!ve EGFR WT/ALK-nega!ve
3.6%
23.3%
P = 0.053
0.0%
100
80
60
40
20
00 5 10 15 20 25 30 35
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Never/light smokers Heavy smokers
4.2%
20.6%
P = 0.123
ORR
EGFR Mut or ALK+
EGFR WT or ALK−
Median 95% CI
2.07 Months 1.84–2.07 Months
2.58 Months 1.91–6.37 Months
P = 0.018HR = 0.515
B
PFS
(% p
a!en
ts)
Months
Figure 1.A, unconfirmed/confirmed ORRs toPD-1/PD-L1 inhibitors comparingEGFR-mutant (Mut) or ALK-positiveNSCLC patients with EGFR wild-type and ALK-negative/unknownpatients. B, ORRs to PD-1/PD-L1inhibitors of never- or light-smokersversus heavy smokers (>10 packyears). C, PFS on PD-1/PD-L1inhibitors based upon EGFR mutationor ALK rearrangement status.
Gainor et al.
Clin Cancer Res; 22(18) September 15, 2016 Clinical Cancer Research4588
specimens (Table 3), the numerical differences were not statisti-cally significant (P¼ 0.195 and P¼ 0.274, respectively), likely dueto limited power.
Collectively, these results suggest that only a subset ofTKI-na€"ve, EGFR-mutant, and ALK-positive lung cancers expressPD-L1 andhaveCD8þTILs, and it is rare for anyof these tumors tocontain both.
Acquired TKI resistance and PD-L1 expressionTo determine whether targeted therapies affect PD-L1 expres-
sion, we analyzed repeat biopsies obtained from patients at thetime of acquired resistance to EGFR or ALK TKIs. Among EGFR-mutant patients, we observed PD-L1 expression in 19 (31%), 18(29%), and 9 (14%) post-TKI specimens using cutoffs of #1%,#5%, and #50%, respectively (Table 2). Concurrent PD-L1expression (#5%) and CD8þ TILs were present in 9 (21%)post-EGFR TKI specimens using IHC. Only 5 (12%) specimensdemonstrated both PD-L1 expression and high-level (grade #2)CD8þ TILs. Similar findings were observed using quantitativeCD8þ TIL analysis (Table 2). Notably, paired pre- and post-TKIbiopsies were available in 57 EGFR-mutant patients (Fig. 2). Thedegree of PD-L1 expression was consistent in both biopsies in41 (72%) patients but varied upon the development of resistancein 16 (28%),with 12 showing higher levels of PD-L1 expression inthe resistant biopsy.
Among 12 ALK-positive, resistant biopsies, we observed PD-L1expression in 5 (42%), 3 (25%), and 2 (17%) specimens usingcutoffs of#1%,#5%, and#50%, respectively (Table 2), but noneshowed high levels of CD8þ TILs using either IHC or quantitativeCD8þ TIL analysis. Thus, like pre-TKI specimens, resistant biop-sies from EGFR-mutant and ALK-positive patients rarely showedconcomitant PD-L1 expression and CD8þ TILs.
Evaluating heterogeneity of PD-L1 expressionTo evaluate whether changes in PD-L1 staining in serial biop-
sies were due to tumor heterogeneity and/or different biopsy sites
over time, we analyzed a series of autopsy specimens obtainedfrom EGFR-mutant (N ¼ 3) and ALK-positive (N ¼ 1) patients.Multiple distinct sites of metastatic disease were sampled in eachpatient. The median number of autopsy sites examined was 4(range 3–8). All three EGFR-mutant patients demonstratedhomogeneity of PD-L1 expression across sites. Two EGFR-mutantpatients exhibited diffuse PD-L1 expression (#50%) in all sitesexamined (N ¼ 5 and 8; Fig. 3). Both patients had 1 to 2þ CD8þ
TILs in the corresponding sites of disease. A third EGFR-mutantpatient was PD-L1 negative in 3 of 3 examined sites. Finally, onepatient with ALK-positive NSCLC demonstrated PD-L1 expres-sion in all examined sites, but the degree of PD-L1 expression washeterogeneous (Supplementary Fig. S5) with low-level (5%–
49%) expression in some sites and diffuse (#50%) expressionin others. None of these sites showed increased levels of CD8þ
TILs. Collectively, across of all of these autopsies, PD-L1 stainingwas relatively consistent across synchronous sites of disease.
DiscussionIn this retrospective analysis, we evaluated the efficacy of
PD-1/PD-L1 inhibitors according to molecular genotype, focus-ing on patients with EGFR mutations and ALK rearrangements.Importantly, we observed a statistically significant shorterPFS and borderline significant lower ORR for EGFR-mutant/ALK-positive patients treated with PD-1/PD-L1 inhibitors com-pared with a cohort of EGFR WT and ALK-negative/unknownpatients. Such findings are consistent with recent prospectivedata from the CheckMate 057 and KEYNOTE 010 trials (9, 10).In both studies, PD-1 inhibitors produced significant improve-ments in overall survival compared with docetaxel in theoverall intention-to-treat populations. However, in subgroupanalyses, there was no difference between study arms amongEGFR-mutant patients.
PD-L1 expression has been associated with improved responserates to PD-1 pathway blockade in NSCLC (6, 18). To date, two
PD-L1 (<5%) PD-L1+ (5%-49%) PD-L1+ (≥50%)
PD-L1 Expression Pre-EGFR TKI Post-EGFR TKI
37 (64.9%)
7 (12.3%)
4 (7.0%)
1 (1.8%)
0 (0.0%)
1 (1.8%)
3 (5.3%)
0 (0.0%)
4 (7.0%)
N = 57
Pre-TKI biopsy Post-resistance biopsy
Figure 2.PD-L1 expression levels in paired, pre- and post-TKIbiopsies among EGFR-mutant patients alongwith representative PD-L1 immunohistochemicalimages. A majority of EGFR-mutant patients (72%)exhibited consistent PD-L1 staining across bothspecimens, but 16 (28%) patients demonstratedvariable staining across biopsies.
Gainor et al.
Clin Cancer Res; 22(18) September 15, 2016 Clinical Cancer Research4590

Mutations de résistance aux IO
• Analyse de la résistance au pembrolizumab dans le CBNPC selon la « signature » mutationnelle (mélanome).
Zaretsky, NEJM 2016
• Apparition de néo-mutations
• Acquisition de la mutation JAK1/JAK2
• Induction de la résistance à l’interféron gamma et la présentation antigénique

Mutations de résistance aux IO
• Rôle prédictif de la SERPIn B3 et B4 dans la réponse aux anti-CTLA4 (mélanome).
• Serpin: homologues de l’antigène ovalbumine (auto-immunité)
Riaz, Nature Genetics 2016

Statut immunologique
• Analyse de différents marqueurs de la réponse immunologique (présentation des Ag, priming et activation)
– Cytokines proinflammatoires (e.g., TNF-α, IL1, IFN-α) – Cofacteurs cellulaires: CD40L/CD40 – Adjuvants endogènes libérés par les tumeurs: CDN (STING
ligand), ATP, HMGB1 – Produits du microbiomes digestif: TLR ligands – Interleukines : IL-10, IL-4, IL-13 – Prostaglandines – Maturité des cellules dendritiques

Statut immunologique
(Fehrenbacher L, Lancet 2016)
• Analyse de biomarqueurs sériques dans le sang • Etude de phase 2 atezolizumab vs docetaxel • Intérêt de l’interféron gamma

« The cancer immunogram »
Blank C, Science 2016

« The cancer immunogram »
Blank C, Science 2016


Immunothérapie en oncologie thoracique
PDL1 dans le sang: CTC
Guibert N, ASCO-SITC 2018

Immunothérapie en oncologie thoracique
PDL1 dans le sang: CTC
Guibert N, ASCO-SITC 2018