Fetal Heart Rate Extraction Using Real PCG-Signals and ...
6
Fetal Heart Rate Extraction Using Real PCG-Signals and Wavelet Transformation Maria Farahi, 1, 2 Al´ ıcia Casals Gelp´ ı, 2 Daniel Lechuga Morente, 1, 3 Naeimeh Behbood, 1 and Hessam Habibian 1 1 Sana Meditech S.L., Barcelona, Spain 2 Center of Research in Biomedical Engineering. Universitat Polit` ecnica de Catalunya, BarcelonaTech, Barcelona, Spain 3 Universitat Pompeu Fabra, Barcelona, Spain (Dated: March 4, 2021) Fetal phonocardiography (fPCG) is a non-invasive measurement of the acoustic cardiac signals. Unfortu- nately, fPCG signals have a low signal to noise ratio which makes detection of relevant information a challeng- ing task. In this study, analysis of fPCG signals is measured by a portable fetal doppler device Baby Heart Beat. In order to extract the fetal heart rate (fHR), the suggested approach is a wavelet transform (WT) based method that combines thresholding analysis in the WT domain for the extraction of fHRs from the underlying noise. The efficiency of the applied method in fHRs extraction has been evaluated with 15 real fPCG signals, along with the simulated fPCGs public database available at PhysioBank. Results have shown promising performance in the identification of the correct location and morphology of the fHRs. PACS numbers: I. INTRODUCTION Fetal heart rate (fHR) observation is important for proper fetal well-being assessment during the period of pregnancy. A passive alternative for long-term monitoring of fetus is the fetal heart auscultation. It has been one of the important meth- ods for the early diagnosis of fetal heart diseases by capturing abnormal heart sounds[1]. The acoustic signal produced by the fetal heart sound (fHS) can be visually depicted in the fetal phonocardiograph (fPCG). Figure 1 clarifies the differ- ence between ECG signals and PCG signals. In PCG signals, a heart sound consists of multiple components including S1, S2, S3, S4 and murmurs [2]. Among these components, two of them are more predominant: S1 and S2. These components are briefly described below. FIG. 1: An example of ECG vs PCG [1]. First row: Normalized ECG signal displaying R-peaks. Second row illustrates a plot of nor- malized heart sound showing S1 and S2 components. • S1: S1 occurs at the onset of the ventricular contraction during the closure of the atrioventricular(AV) valves. It is usually the longest and loudest heart sound, and con- tains a series of low-frequency vibrations. The audible sub-components of S1 are those associated with the clo- sure of each of the two AV-valves. S1 is assumed to have four major components which may be detected by time-frequency decomposition. • S2: S2 is heard at the end of the ventricular systole, during the closure of the semilunar valves. Typically, its frequency is higher than S1, and its duration is shorter. It has aortic and pulmonary sub-components. • S3: A third low-frequency sound (S3, ventricular gal- lop) may be heard at the beginning of the diastole, dur- ing the rapid filling of the ventricles. • S4: A fourth heart sound (S4, atrial gallop) may be heard in late diastole during atrial contraction. • Murmurs: Murmurs are high-frequency, noise-like sounds that are heard between the two major heart sounds during systole or diastole. They indicate certain cardiovascular defects. A PCG is a plot of recorded heart sounds and murmurs which provides significant information about the temporal relation- ship between the heart sound and the mechanical/electrical events of the cardiac cycle [3]. An fPCG is a low-cost and non-invasive technique to extract the acoustic signal of the fe- tal heart sounds. Moreover, the fPCG device is easy to use allowing non experts to record the signals. The mother can take long-term recordings during the day or night and after- ward, they can be examined to get a more complete overview of the fetus functionality. The rest of the paper is organized as follows. Past studies is reviewed in section II. In section III we present data used for the present study. The proposed method is detailed in section IV. The results of suggested methodology are studied in sec- tion V, and then the paper is concluded with few remarks and future works. arXiv:2103.01014v2 [q-bio.QM] 3 Mar 2021
Transcript of Fetal Heart Rate Extraction Using Real PCG-Signals and ...

Fetal Heart Rate Extraction Using Real PCG-Signals and Wavelet Transformation
Maria Farahi,1, 2 Alıcia Casals Gelpı,2 Daniel Lechuga Morente,1, 3 Naeimeh Behbood,1 and Hessam Habibian1
1Sana Meditech S.L., Barcelona, Spain2Center of Research in Biomedical Engineering. Universitat Politecnica de Catalunya, BarcelonaTech, Barcelona, Spain
3Universitat Pompeu Fabra, Barcelona, Spain(Dated: March 4, 2021)
Fetal phonocardiography (fPCG) is a non-invasive measurement of the acoustic cardiac signals. Unfortu-nately, fPCG signals have a low signal to noise ratio which makes detection of relevant information a challeng-ing task. In this study, analysis of fPCG signals is measured by a portable fetal doppler device Baby Heart Beat.In order to extract the fetal heart rate (fHR), the suggested approach is a wavelet transform (WT) based methodthat combines thresholding analysis in the WT domain for the extraction of fHRs from the underlying noise.The efficiency of the applied method in fHRs extraction has been evaluated with 15 real fPCG signals, alongwith the simulated fPCGs public database available at PhysioBank. Results have shown promising performancein the identification of the correct location and morphology of the fHRs.
PACS numbers:
I. INTRODUCTION
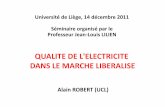
Fetal heart rate (fHR) observation is important for properfetal well-being assessment during the period of pregnancy.A passive alternative for long-term monitoring of fetus is thefetal heart auscultation. It has been one of the important meth-ods for the early diagnosis of fetal heart diseases by capturingabnormal heart sounds[1]. The acoustic signal produced bythe fetal heart sound (fHS) can be visually depicted in thefetal phonocardiograph (fPCG). Figure 1 clarifies the differ-ence between ECG signals and PCG signals. In PCG signals,a heart sound consists of multiple components including S1,S2, S3, S4 and murmurs [2]. Among these components, twoof them are more predominant: S1 and S2. These componentsare briefly described below.
FIG. 1: An example of ECG vs PCG [1]. First row: NormalizedECG signal displaying R-peaks. Second row illustrates a plot of nor-malized heart sound showing S1 and S2 components.
• S1: S1 occurs at the onset of the ventricular contractionduring the closure of the atrioventricular(AV) valves. Itis usually the longest and loudest heart sound, and con-tains a series of low-frequency vibrations. The audiblesub-components of S1 are those associated with the clo-sure of each of the two AV-valves. S1 is assumed tohave four major components which may be detected bytime-frequency decomposition.
• S2: S2 is heard at the end of the ventricular systole,during the closure of the semilunar valves. Typically, itsfrequency is higher than S1, and its duration is shorter.It has aortic and pulmonary sub-components.
• S3: A third low-frequency sound (S3, ventricular gal-lop) may be heard at the beginning of the diastole, dur-ing the rapid filling of the ventricles.
• S4: A fourth heart sound (S4, atrial gallop) may beheard in late diastole during atrial contraction.
• Murmurs: Murmurs are high-frequency, noise-likesounds that are heard between the two major heartsounds during systole or diastole. They indicate certaincardiovascular defects.
A PCG is a plot of recorded heart sounds and murmurs whichprovides significant information about the temporal relation-ship between the heart sound and the mechanical/electricalevents of the cardiac cycle [3]. An fPCG is a low-cost andnon-invasive technique to extract the acoustic signal of the fe-tal heart sounds. Moreover, the fPCG device is easy to useallowing non experts to record the signals. The mother cantake long-term recordings during the day or night and after-ward, they can be examined to get a more complete overviewof the fetus functionality.
The rest of the paper is organized as follows. Past studies isreviewed in section II. In section III we present data used forthe present study. The proposed method is detailed in sectionIV. The results of suggested methodology are studied in sec-tion V, and then the paper is concluded with few remarks andfuture works.
arX
iv:2
103.
0101
4v2
[q-
bio.
QM
] 3
Mar
202
1

2
II. PREVIOUS STUDIES OVERVIEW
Nowadays, telemedicine plays an important role in people’slife style. In this way, remote fetal monitoring systems enablethe mothers to record their fetus biological signals at homeand to submit them to a medical specialist for remote diag-nosis. Therefore, in the past decade, many efforts have beendedicated to find a suitable way for remote fHR extraction.Among such efforts, fPCG analysis can be considered as anon-invasive method for remote fHR monitoring. It is sim-ple to use and low-cost which makes it more convenient forordinary people. However, fPCG signals are profoundly cor-rupted by noise since they are recorded at the maternal ab-dominal surface. Fetal movements, contractions of mother’suterus, maternal digestive sounds, sensor movements, ambi-ent sounds, maternal respiratory and heart sound are the majorsources of noise [4].
Dia et al. in [5] estimated HR from PCG signals. Theyapplied non-negative matrix factorization approach on thespectrogram of the adult PCGs. They evaluated their workby considering synchronous ECG and PCG signals. In [6]Samieinasab et al. used a single-channel denoising frameworkto reduce the noise of fPCG. Then, as in [5], they utilized non-negative matrix factorization method to decompose fPCGs intime-frequency domain.
In Aydana S. Kyzdarbekova et al. [7], the noise reduc-tion on PCG is approached using an iterative process basedon wavelet transforms. The noise is automatically eliminatedby thinning twice at each decomposition stage. According tothe results obtained, the best wavelet-carrier for filtering thenoise is the Daubechies 4 (”db4”), since this wavelet functionis identical to the shape of the components and correspondingto the nonlinear local regions of the PCG. The authors claimto have developed a method to filter the PCG to be purifiedwithout loss of cardiographic information.
As in [7], in Elisavet Koutsiana et al. [8], noise reduction isperformed by means of the process described in a tree schemebased on ”db4” wavelet transforms. However, in this study theauthors go further, developing a Fractal Dimension approachcapable of finding the peaks in the signal obtained after ap-plying the wavelet transforms and, based on the amplitudeof these peaks and the distance between them, determiningthe fHR. From their results, the authors concluded that a WT-FD scheme is quite satisfactory in the analysis of fetal heartsounds, becoming a promising technique for the segmentationof fetal heart sounds although they didn’t test it in real PCGs.
Additionally, in terms of PCG analysis, we see studiesbased on machine learning, such as that of Chowdhury et al.[9] and Yadav et al. [10]. In the first one, a deep learningnetwork is trained for classification between normal and ab-normal PCGs. The architecture is fed with features extractedfrom signals previously denoised by discrete wavelet trans-forms and segmented using Shannon energy envelopment andzero-crossing. These features are obtained employing Mel-scaled power spectrogram and Mel-frequency cepstral coeffi-cients. In the second case, a Support Vector Machine (SVM)classifier is trained for the same purpose with features ex-tracted from PCG using Fourier transforms and Cepstrum
analysis. In this case, the preprocessing consists of a down-sampling, to reduce the computational load, and the applica-tion of a band-pass filter for denoising. The main drawbacksof these approaches are the need of large datasets to train thealgorithms [9], better feature extraction [9] or stronger pre-processing. [10]
Finally, in Anita Devi et. al. [11] a different use of wavelettransforms can be seen, which are used for the extraction offeatures such as mean energy, mean standard deviation, meanvariance and maximum entropy. However, the downside ofthis method is the difference between the optimal levels ofdecomposition which highly depends on the amplitude andduration of the signals.
Taking into account the contributions made in these previ-ous works, in the present study, an approach for the estima-tion of fHR from fPCG has been developed. In this case, thedenoising task was performed using wavelet transforms as de-scribed in [7],[8]. Nevertheless, the mother wavelet used wasthe bi-orthogonal with 4 levels of decomposition, instead of”db4”, providing a better denoising performance. Then, theextraction of S1 peaks was achieved using an approach basedon the top enveloping and local maximums finding. Finally,the estimation of fHR, as in [8], has been carried taken intoaccount the amplitude and the distance between S1 peaks.
The procedure which is explained in more detail belowpresents some advantages with respect to the other method-ologies that has been exposed during this section. Firstly, theapplication of this method is as fast as could be used in real-time approaches. Moreover, the extraction of S1 peaks is de-veloped using a simpler approach than the Fractal Dimensionone used in [8], based solely on the top enveloping and localmaximums finding. Additionally, it has to be stated that thismethodology has been evaluated with real fHR signals and theobtained results are trustworthy.
III. DATA ACQUISITION
In order to achieve an accurate remote monitoring, therecording device must have some capabilities including easyof use by any mother, comfortable to wear, able to distinguishthe mother heart rate from the fetal, and reliability. The prop-erties of the used device and the protocol defined for data ac-quisition are described below.
In order to collect clinical data a portable Baby Sound Apocket fetal doppler device manufactured by Contec Medi-cal Co. [12] is used which is certified under medical CE andFDA approval. The device is utilized by Sana Meditech com-pany [13] with a brand of Baby Heart Beat [14] (see Figure2). Obtaining data for algorithm development, simultaneousmeasurement of Baby Heart Beat together with a clinical de-vice PHILIPS model Avalon FM30 [15] is performed. Totalnumber of 15 records from pregnant women (average age 32)who were in week 20 and week 35 of their pregnancy life hasbeen acquired. The duration of each record is at least 4 min-utes. These clinical data are gathered and recorded for rig-orous analysis of the algorithm and continuous improvementduring the development process.

3
FIG. 2: The device used by Sana Meditech Company with a brandof Baby Heart Beat.
In addition, proposed algorithm is applied on a public fPCGdata set provided by [16]. This data set contains 110 recordswhich have been recorded from women between the 30th andthe 40th weeks of pregnancy an with an average age of 25years old.
IV. METHODOLOGY
The overall proposed signal processing schema for fHR ex-traction from fPCG signals is shown in fig 3. As depicted,the algorithm starts with pre-processing stage. In two fur-ther steps, all peaks are extracted as well as the first valuefor fHRs. After that, it is proceeded to the estimation offHR/second. Finally, post processing is performed to avoidsudden increase/decrease in output fHR-graph. Followingsections describe the main stages of the flowchart in detail.
A. Pre-Processing
Pre-processing and noise reduction is performed by the useof wavelet transformation (WT) and adaptive thresholdingmethod. WT is a time-frequency processing method whichits definition for an input signal x(t) is as Eq. 1
WTx(a,b) =
∫x(t)Ψ∗a,b(t)dt ; a , 0 (1)
where the basic function, Ψa,b(t), is featured by scale andtime-shift parameters (a and b, respectively) as Eq.2:
Ψa,b(t) =1√
aψ(
t − ba
) (2)
Ψa,b(t) can be also used for signal decomposition. As WTis sensitive to noise level, WT procedure requires appropri-ate selection of wavelet family, level of decomposition andthreshold for achieving better accuracy. In this work, decom-position, denoising and reconstruction were performed by a
FIG. 3: Proposed schema for fHR extraction.
FIG. 4: A sample of an original fPCG signal vs its filtered one. Firstrow: original signal, and second row: after wavelet denoising.
bi-orthogonal mother wavelet (bior2.4) with 4 levels of de-composition and soft threshold, providing the higher signal tonoise ratio for all types of fPCG signals. An example of anoisy fPCG signal vs its denoised one is shown in Fig.4.
where, the first row shows 1-second of the original fPCGsignal and the result of denoising by wavelet is illustrated inthe second row.

4
FIG. 5: An example of the result of enveloping and finding the localmaxima. The red graph shows the obtained envelop and red bulletsrepresent local maxima.
B. All-peaks Estimation
Fig.?? shows a sample of adult ECG wave with the place-ment of R-peaks, as well as adult PCG and related S1 peaks.They show the correlation between S1 and R peaks. In fetalPCG, the distance between S1 and S2 is much shorter than thatin adult’s PCG. Considering the diastolic duration is longerthan systolic duration, S2 falls at least 100ms after precedingS1 and at most 200ms before successive S1 [8]. As a result, areasonable approach for S1-peaks extraction among all peaks,is to first find all local maximums (all peaks) in a PCG sig-nal, then perform amplitude and distance threshold (S1-peaksextraction).
With this aim, a combination of enveloping and finding thelocal maxima technique is applied. Here, the selection of twoparameters is important: Average Heart Rate (AHR) and En-velop Size (ES). Hence, various ESs from 50ms to 1000mswith an step of 10ms have been investigated. The envelopswith a size between [160ms 180ms] are more efficient. As aresult, in this study, an ES of 170ms is chosen. AHR Selection(here, 140bpm) is done based on the normal fetus’s heart ratewhich is between 120bpm and 160bmp [4]. Figure 5 showsan example of the result of enveloping and finding the localmaxima.
C. S1 Extraction
Considering the extracted envelope, local maxima could betaken into account as potential S1 peaks. The procedure forS1 selection among the detected peaks is based on this factthat the values of the normal duration of a fetal heart cycleis 430ms while the minimum is 375ms and the maximum is545ms. In addition, the S1 sound is usually the component ofthe signal with the greatest amplitude. Therefore, in this study,a thresholding method has been chosen to extract S1s. In this
FIG. 6: An example of filtered signals and related S1-peaks.
step, a windowing of 3sec with an overlap of 2sec is applied.The selected peaks are then post processed to check if they fallbetween the S1S1-intervals. Peaks which cross these limita-tions, are considered as noise. The rest of the peaks are passedas S1-peaks to the next step, fHR calculation. An example ofthe results of S1-selection stage are shown in Fig.6. In thefigure, red graph shows the obtained envelope. All peaks areillustrated in red bullets while selected S1-peaks are shown ingreen stars.
D. fHR Estimation
Knowing that the time elapsed between two successive S1waves in a phonocardiogram signal (and its reciprocal, theHR), is a combination of systolic time and diastolic time[2],fHR could be calculated using Eq.3.
f HR(bpm) =60
Tbb(sec)(3)
where, Tbb is the time duration between two S1s.
E. Report fHR(bpm)/(sec)
In next step, estimated fHRs are used to defineHR(bpm)/Sec. To do this, an average value of fHRs is cho-sen as a representative fHR per second. Each section takes 3seconds, hence 3 fHR(bpm) should be reported for each sec-tion. Since sections have a 2-seconds overlap, each sectionhas 1-second new data. Considering these information, sec-tions that report less than 3 fHRs, should be refined. For this,if the fHR related to the last second exists among the reportedfHRs, it will be reported as new fHR. But, when timing isnot matched, the reported fHR for the previous second will beconsidered as new fHR.

5
FIG. 7: Final estimated HR for a 4-minutes real fPCG data. Firstrow: results using a clinical device (PHILIPS model Avalon FM30[15]). Second row: results obtained by proposed algorithm.
V. RESULTS
The analysis of this study was applied on a personal com-puter using Matlab R2020a and tested on real data and alsopublic databases. Every input signal was tested for at least4 minutes (10 seconds) considering Fs =8,000Hz (1,000Hz),i.e., 1,920,000 (10,000) samples for real (public) data. In or-der to validate the accuracy of the current system, final fHRgraph achieved by current study is compared to those reportedby standard ECG devices in hospital environment. In addi-tion, the efficiency of the proposed method in fHS extractionhas been evaluated with a real fPCG public database avail-able at PhysioBank[16]. Reported fHR graph for a sample of4-minutes real fPCG signal is shown in Fig.7.
VI. CONCLUSIONS AND FUTURE WORKS
Fetal phonocardiography signals, generally, are of low am-plitude and hidden by high-amplitude noises that may comefrom the sounds of mother breathes, contact of the stethoscopewith the skin, fetal movements and other ambient sounds.This fact makes challenging the analysis of fPCG waveforms.
In the present work, it has been developed an algorithm forthe estimation of fHR from fPCG. Firstly, a pre-processingfor the denoising task based on wavelet transformation is per-formed. Then, a combination of enveloping and finding localmaximums is applied for subsequent extraction of S1 peaksand, finally, the fHR calculation through the computation ofelapsed times between the peaks is carried out. On the ba-sis of the obtained results and the comparison between thoseand the ones obtained by standard ECG devices, we can con-clude that the method exposed during the previous sections isa promising tool for the identification of the correct locationof S1 peaks and, subsequently, the correct fHR calculation.
In future work we would like to leverage the measurementprecision by sophisticated machine learning algorithms [17].Moreover deep analysis over signals correlation and possibleprediction over risk would be in a scope of our upcoming stud-ies.
[1] W. Phanphaisarn, A. Roeksabutr, P. Wardkein, J. Koseeyaporn,and P. Yupapin, “Heart detection and diagnosis based on ecgand epcg relationships,” Medical devices (Auckland, NZ), vol. 4,p. 133, 2011.
[2] F. Kovacs, C. Horvath, A. T. Balogh, and G. Hosszu, “Fetalphonocardiography—past and future possibilities,” Computermethods and programs in biomedicine, vol. 104, no. 1, pp. 19–25, 2011.
[3] J. Nedoma, M. Fajkus, R. Martinek, S. Kepak, J. Cubik,S. Zabka, and V. Vasinek, “Comparison of bcg, pcg and ecg sig-nals in application of heart rate monitoring of the human body,”in 2017 40th International Conference on Telecommunicationsand Signal Processing (TSP). IEEE, 2017, pp. 420–424.
[4] A. Strazza, A. Sbrollini, V. Di Battista, R. Ricci, L. Trillini,I. Marcantoni, M. Morettini, S. Fioretti, and L. Burattini, “Pcg-delineator: an efficient algorithm for automatic heart soundsdetection in fetal phonocardiography,” in 2018 Computing in
Cardiology Conference (CinC), vol. 45. IEEE, 2018, pp. 1–4.[5] N. Dia, J. Fontecave-Jallon, P.-Y. Gumery, and B. Rivet,
“Heart rate estimation from phonocardiogram signals usingnon-negative matrix factorization,” in ICASSP 2019-2019 IEEEInternational Conference on Acoustics, Speech and Signal Pro-cessing (ICASSP). IEEE, 2019, pp. 1293–1297.
[6] M. Samieinasab and R. Sameni, “Fetal phonocardiogram ex-traction using single channel blind source separation,” in 201523rd Iranian Conference on Electrical Engineering. IEEE,2015, pp. 78–83.
[7] A. S. Kyzdarbekova, D. M. Dutbaeva, and K. B. Kasymbekova,“Adaptive noise reduction phonocardiograms based on wavelettransformation,” in 2017 International Conference ”QualityManagement,Transport and Information Security, InformationTechnologies” (IT&QM&IS). IEEE, 2017, pp. 391–394.
[8] E. Koutsiana, L. Hadjileontiadis, I. Chouvarda, and A. Khan-doker, “Fetal heart sounds detection using wavelet transform

6
and fractal dimension,” Frontiers Bioengineering and Biotech-nology, vol. 5, pp. 1–8, 2017.
[9] T. H. Chowdhury, K. N. Poudel, and Y. Hu, “Time-frequencyanalysis, denoising, compression, segmentation, and classifica-tion of pcg signals,” IEEE Access, vol. 8, pp. 160 882–160 890,2020.
[10] A. Yadav, M. K. Dutta, C. M. Travieso, and J. B. Alonso, “Auto-matic classification of normal and abnormal pcg recording heartsound recording using fourier transform,” in 2018 IEEE Inter-national Work Conference on Bioinspired Intelligence (IWOBI).IEEE, 2018, pp. 1–9.
[11] A. Devi, A. Misal, and G. R. Sinha, “Performance analysis ofdwt at different levels for feature extraction of pcg signals,” inInternational Conference on Microelectronics, Communicationand Renewable Energy (ICMiCR-2013). IEEE, 2013.
[12] C. M. Company. Baby sound a pocket fetal doppler device.[Online]. Available: https://www.contecmed.com/index.php?page=shop.product details&flypage=flypage.tpl&product id=
66&category id=14&option=com virtuemart&Itemid=606[13] Sana meditech company. [Online]. Available: https://www.
sanameditech.com/
[14] Baby heart beat device. [Online]. Avail-able: http://www.oepm.es/es/signos distintivos/detalle.html?mod=N&exp=0402889&bis=
[15] Avalon fm30 philips fetal monitor. [Online].Available: https://www.usa.philips.com/healthcare/product/HC862199/avalon-fm30-fetal-monitor
[16] S. M. Sameni R. (2021) Shiraz University Fetal Heart SoundsDatabase (version 1.0.1), physionet. [Online]. Available:https://doi.org/10.13026/42eg-8e59
[17] Z. Zhao, Y. Zhang, Z. Comert, and Y. Deng, “Computer-aideddiagnosis system of fetal hypoxia incorporating recurrence plotwith convolutional neural network,” Frontiers in physiology,vol. 10, p. 255, 2019.