FB - Deauville canc ropole mai 2011 [Mode de … · Pharmacogénétique Principes, applications aux...
49
Pharmacogénétique Principes, applications aux anticancéreux et perspectives Pr Franck Broly, MD, PhD Unité de Génopathies, Pharmacogénétique et Toxicogénétique, Centre de Biologie et Pathologie, CHRU Lille. EA4483: « Impact de l’environnement chimique sur la santé » Pôle Recherche, Faculté de Médecine, Lille.
Transcript of FB - Deauville canc ropole mai 2011 [Mode de … · Pharmacogénétique Principes, applications aux...
PharmacogénétiquePrincipes, applications aux anticancéreux et perspectives
Pr Franck Broly, MD, PhDUnité de Génopathies, Pharmacogénétique et Toxicogénétique, Centre de Biologie et Pathologie, CHRU Lille.
EA4483: « Impact de l’environnement chimique sur la santé »Pôle Recherche, Faculté de Médecine, Lille.
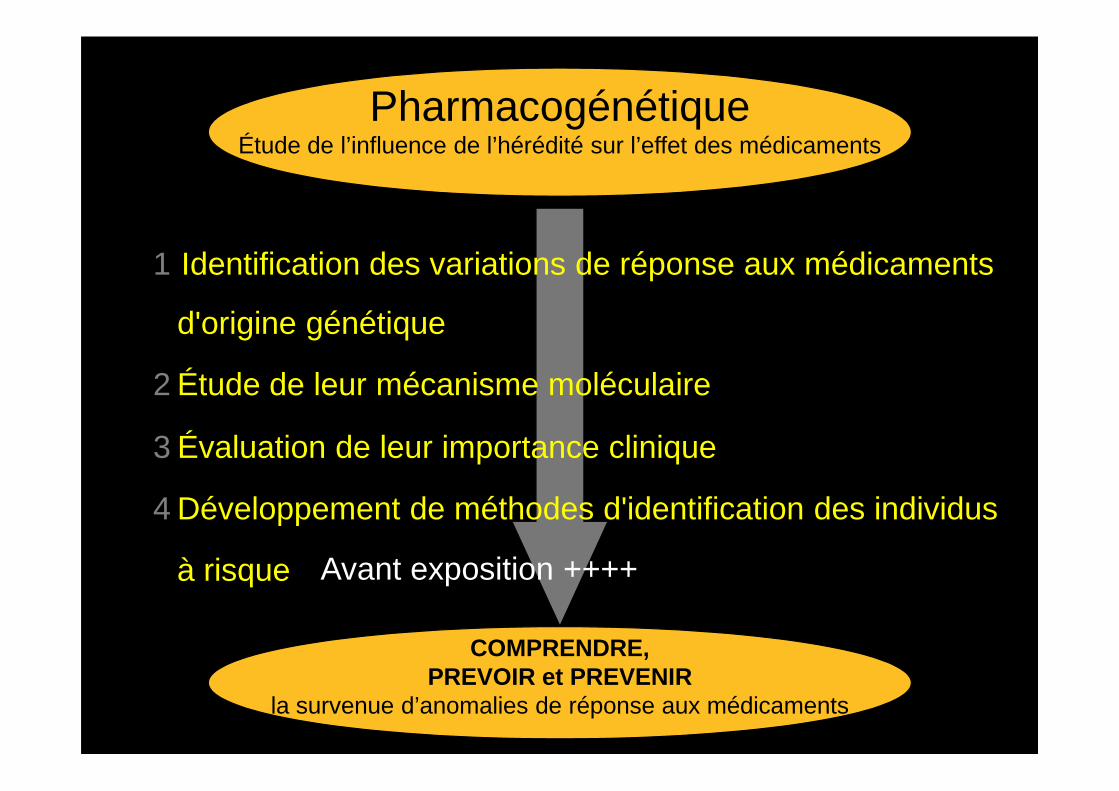
PharmacogénétiqueÉtude de l’influence de l’hérédité sur l’effet des médicaments
1 Identification des variations de réponse aux médicaments
d'origine génétique
2 Étude de leur mécanisme moléculaire
COMPRENDRE,PREVOIR et PREVENIR
la survenue d’anomalies de réponse aux médicaments
2 Étude de leur mécanisme moléculaire
3 Évaluation de leur importance clinique
4 Développement de méthodes d'identification des individus
à risque Avant exposition ++++
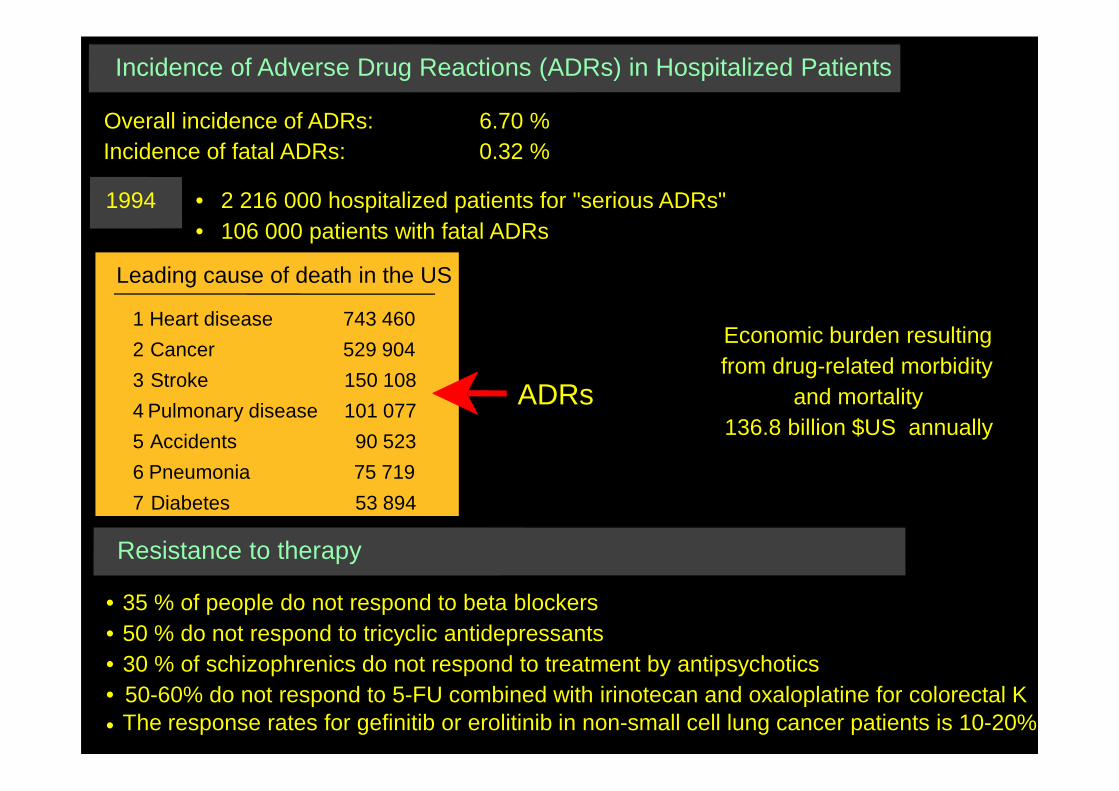
Overall incidence of ADRs: 6.70 %Incidence of fatal ADRs: 0.32 %
Incidence of Adverse Drug Reactions (ADRs) in Hospitalized Patients
1994 • 2 216 000 hospitalized patients for "serious ADRs"• 106 000 patients with fatal ADRs
Leading cause of death in the US
ADRs
Economic burden resultingfrom drug-related morbidity
and mortality
1 Heart disease 743 460
2 Cancer 529 904
3 Stroke 150 108
ADRs
ADRs and mortality136.8 billion $US annually
Resistance to therapy
• 35 % of people do not respond to beta blockers• 50 % do not respond to tricyclic antidepressants• 30 % of schizophrenics do not respond to treatment by antipsychotics••
50-60% do not respond to 5-FU combined with irinotecan and oxaloplatine for colorectal K
...
4 Pulmonary disease 101 077
5 Accidents 90 523
6 Pneumonia 75 719
7 Diabetes 53 894
The response rates for gefinitib or erolitinib in non-small cell lung cancer patients is 10-20%
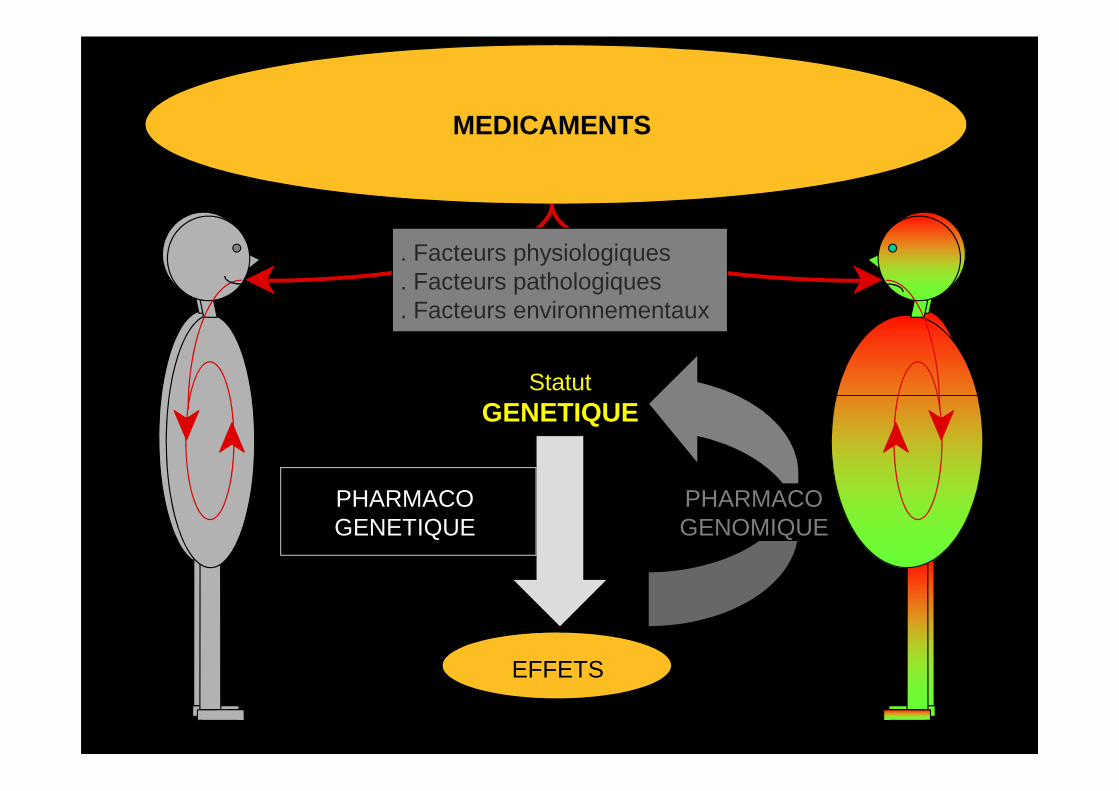
MEDICAMENTS
Statut
. Facteurs physiologiques
. Facteurs pathologiques
. Facteurs environnementaux
EFFETS
GENETIQUE
PHARMACOGENETIQUE
PHARMACOGENOMIQUE
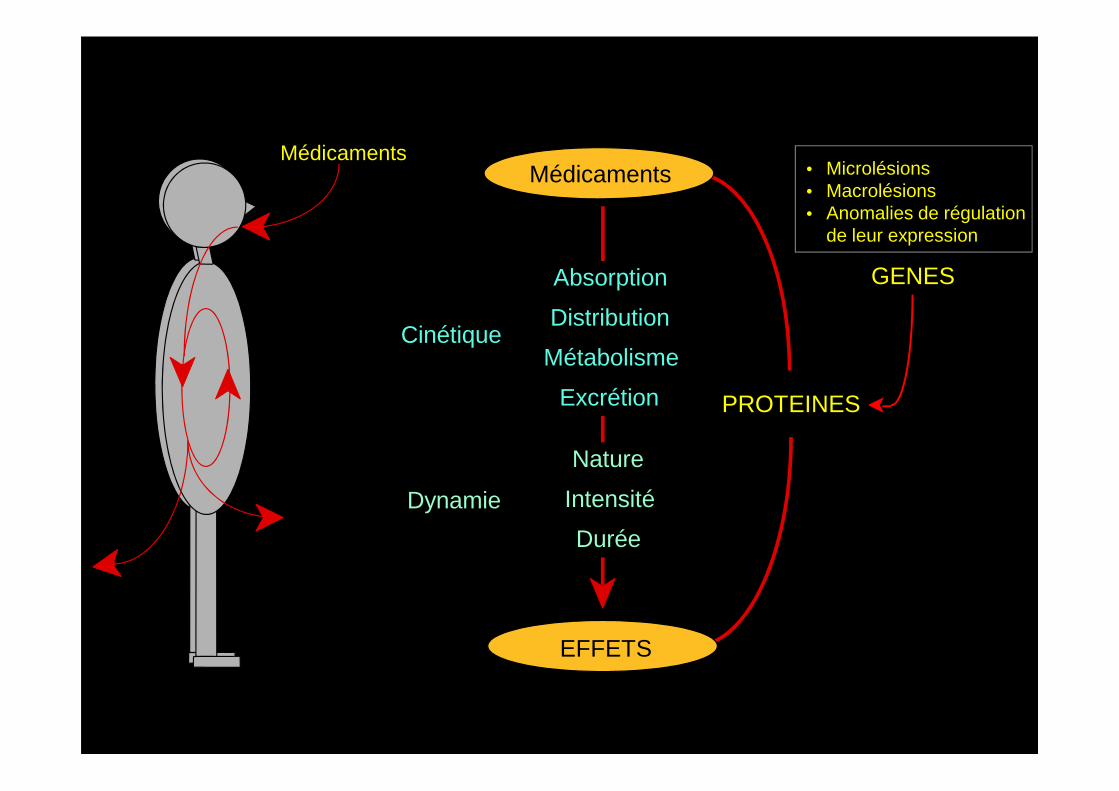
Médicaments
Absorption
Distribution
Métabolisme
Excrétion
Médicaments
Cinétique
PROTEINES
GENES
• Microlésions• Macrolésions• Anomalies de régulation
de leur expression
Excrétion
EFFETS
Dynamie
Nature
Intensité
Durée
PROTEINES
G insFrame shift
Stop codongeneration
Splice sitedisappearance
Frame shift
9 bp rep
3 AA repeat
Frame shift
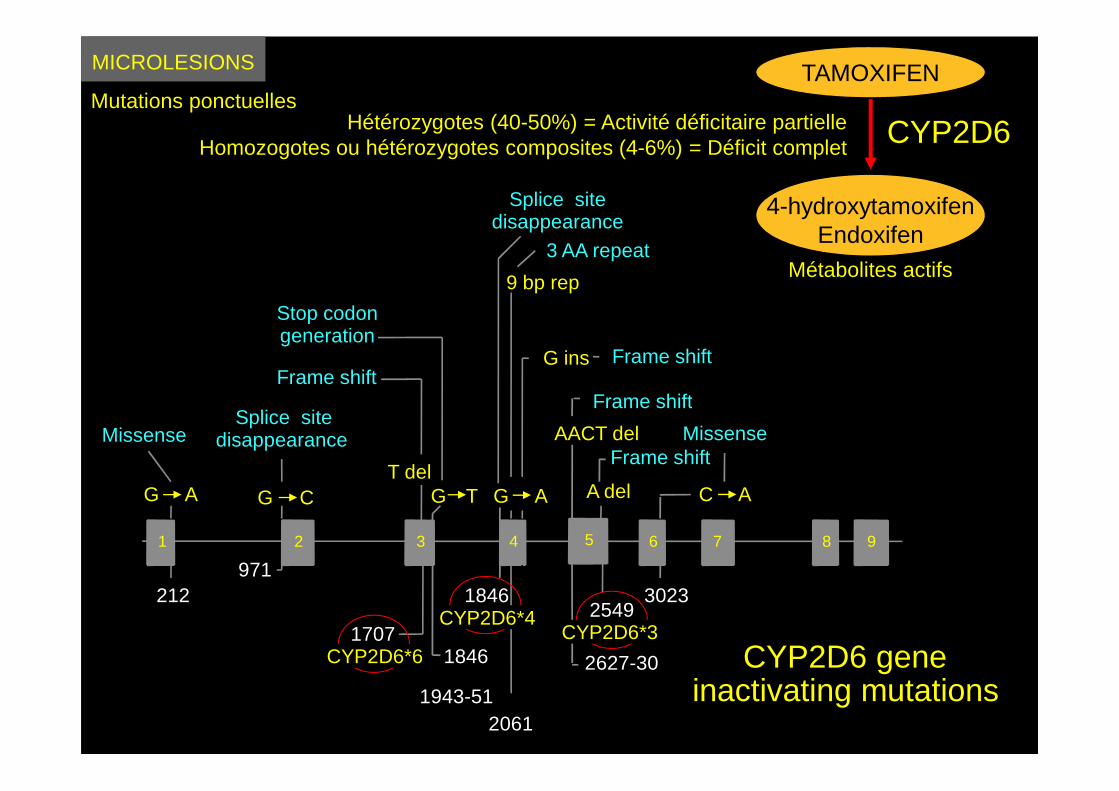
MICROLESIONS
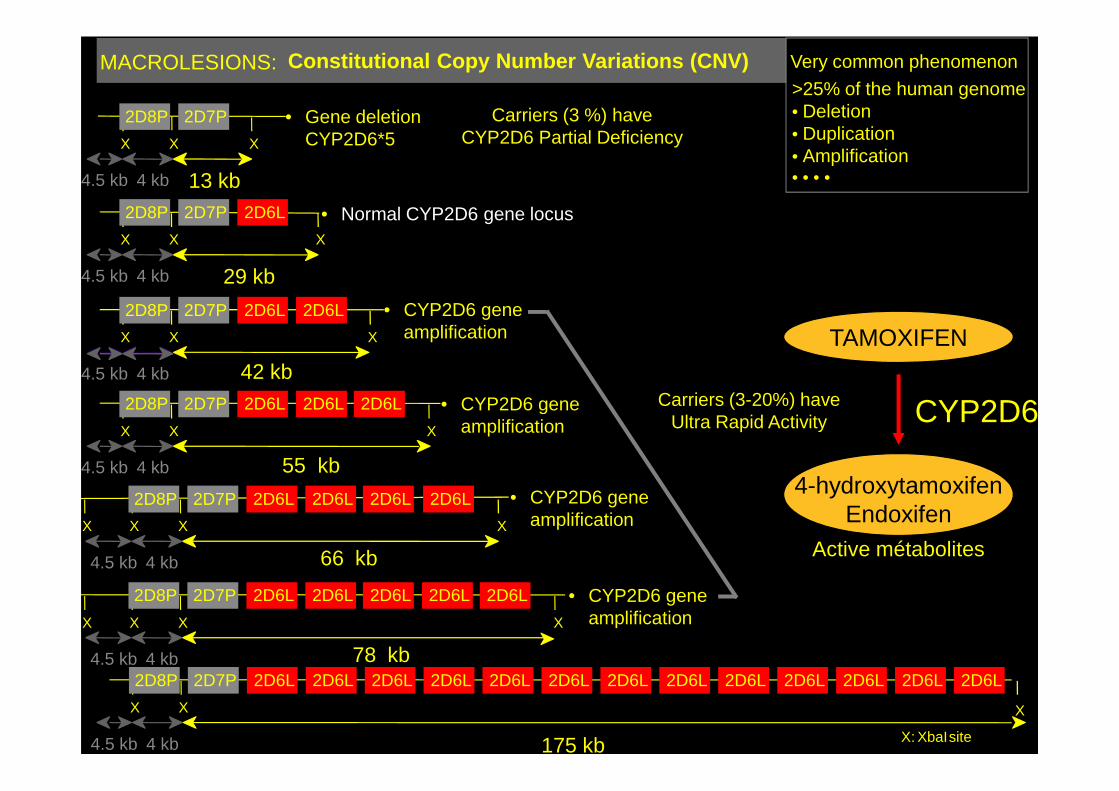
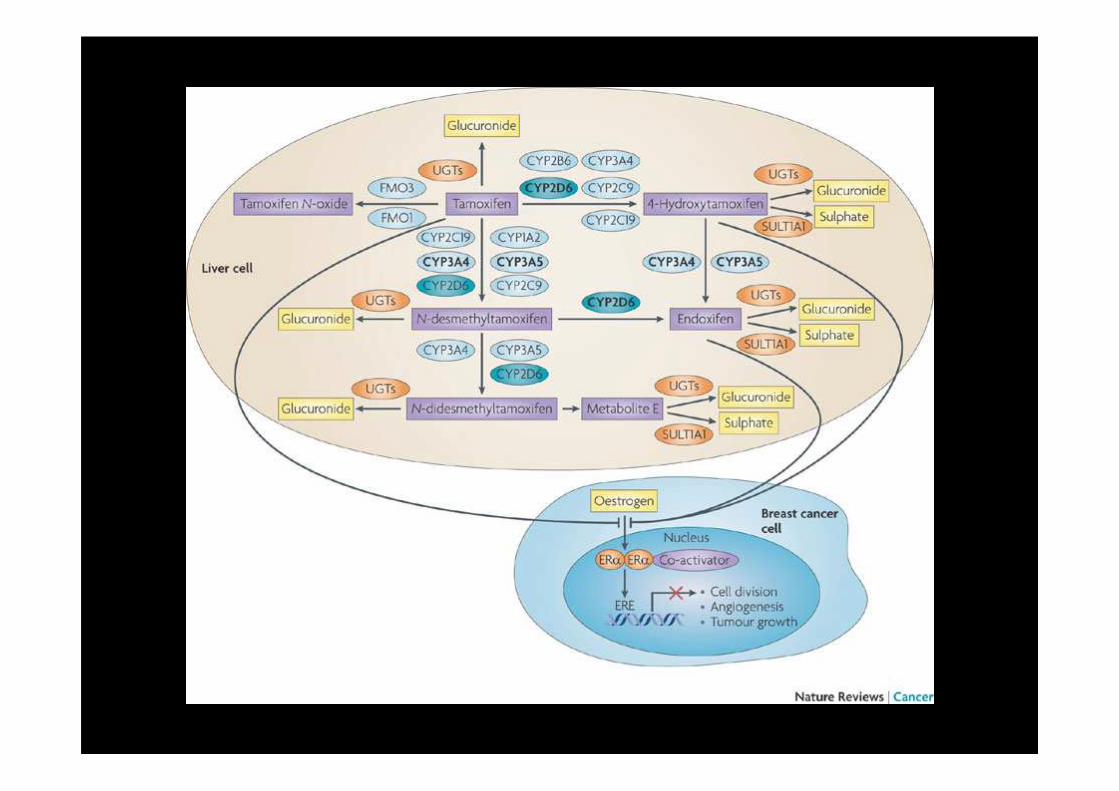
Mutations ponctuellesTAMOXIFEN
4-hydroxytamoxifenEndoxifen
CYP2D6
Métabolites actifs
Hétérozygotes (40-50%) = Activité déficitaire partielleHomozogotes ou hétérozygotes composites (4-6%) = Déficit complet
G C G T
3023971
1846
CYP2D6 geneinactivating mutations
1 4 6 7 8 92
2549
A del
5
Frame shiftT del
3
17071846
Splice sitedisappearance
C A
Missense
212
G A
Missense
2627-30
Frame shift
1943-51
G A
AACT del
2061
CYP2D6*3CYP2D6*4
CYP2D6*6
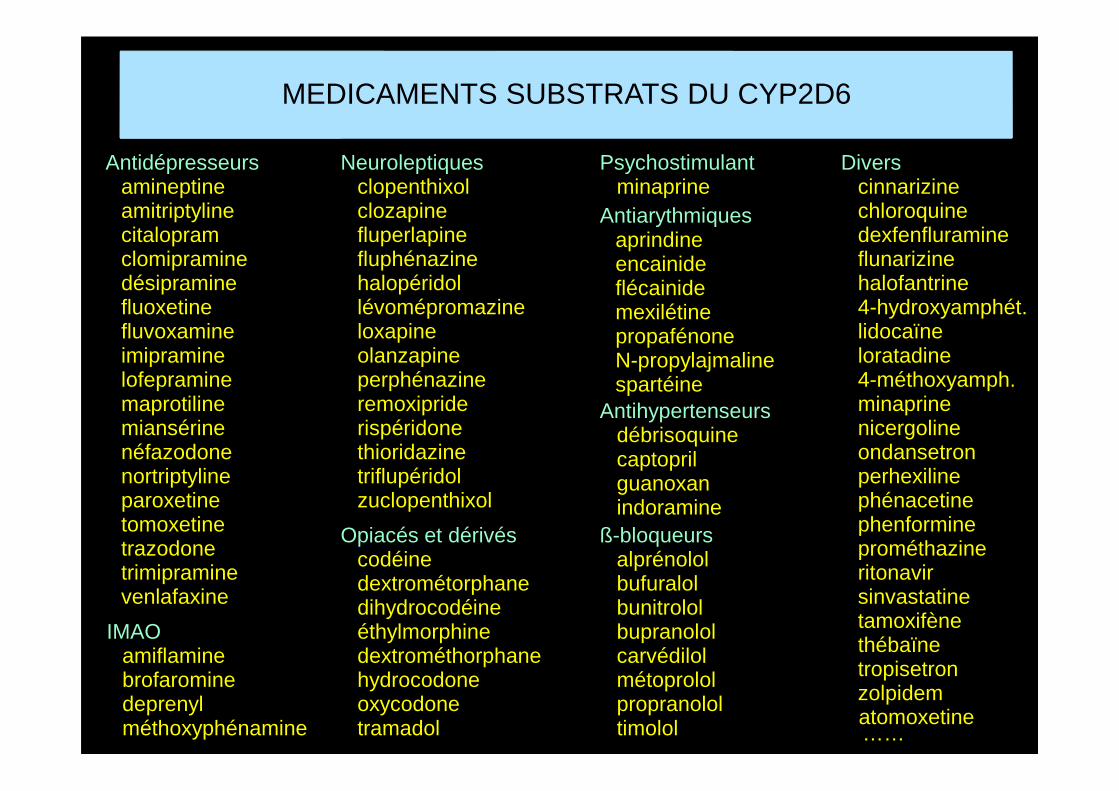
MEDICAMENTS SUBSTRATS DU CYP2D6
Antidépresseursamineptineamitriptylinecitalopramclomipraminedésipraminefluoxetinefluvoxamineimipraminelofepraminemaprotiline
Diverscinnarizinechloroquinedexfenfluramineflunarizinehalofantrine4-hydroxyamphét.lidocaïneloratadine4-méthoxyamph.minaprine
AntiarythmiquesaprindineencainideflécainidemexilétinepropafénoneN-propylajmalinespartéine
Neuroleptiquesclopenthixolclozapinefluperlapinefluphénazinehalopéridollévomépromazineloxapineolanzapineperphénazineremoxipride
Psychostimulantminaprine
ß-bloqueursalprénololbufuralolbunitrololbupranololcarvédilolmétoprololpropranololtimolol
maprotilinemiansérinenéfazodonenortriptylineparoxetinetomoxetinetrazodonetrimipraminevenlafaxine
minaprinenicergolineondansetronperhexilinephénacetinephenformineprométhazineritonavirsinvastatinetamoxifènethébaïnetropisetronzolpidem
spartéineremoxipriderispéridonethioridazinetriflupéridolzuclopenthixol
Opiacés et dérivéscodéinedextrométorphanedihydrocodéineéthylmorphinedextrométhorphanehydrocodoneoxycodonetramadol
IMAOamiflaminebrofarominedeprenylméthoxyphénamine
Antihypertenseursdébrisoquinecaptoprilguanoxanindoramine
atomoxetine……
X
4.5 kb 4 kb
X
29 kb
2D8P 2D7P 2D6L
X
2D8P 2D7P 2D6L 2D6L 2D6L
X
4.5 kb 4 kb
X
42 kb
2D8P 2D7P 2D6L 2D6L
X
MACROLESIONS: Constitutional Copy Number Variations (CNV)>25% of the human genome• Deletion• Duplication• Amplification• • • •
Very common phenomenon
X
4.5 kb 4 kb
X
13 kb
2D8P 2D7P
X
TAMOXIFEN
CYP2D6
• Gene deletion CYP2D6*5
• Normal CYP2D6 gene locus
• CYP2D6 gene amplification
• CYP2D6 gene Carriers (3-20%) have
Carriers (3 %) haveCYP2D6 Partial Deficiency
X
4.5 kb 4 kb
X
55 kb
2D8P 2D7P 2D6L 2D6L
X
2D6L
X X
4.5 kb 4 kb
X
78 kb
2D8P 2D7P 2D6L 2D6L
X
2D6L 2D6L 2D6L
X X
4.5 kb 4 kb
X
66 kb
2D8P 2D7P 2D6L 2D6L
X
2D6L 2D6L
X: XbaIsite
X
4.5 kb 4 kb 175 kb
2D8P 2D7P 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L 2D6L
X X
4-hydroxytamoxifenEndoxifen
CYP2D6
Active métabolites
• CYP2D6 geneamplification
• CYP2D6 geneamplification
• CYP2D6 geneamplification
Carriers (3-20%) have Ultra Rapid Activity
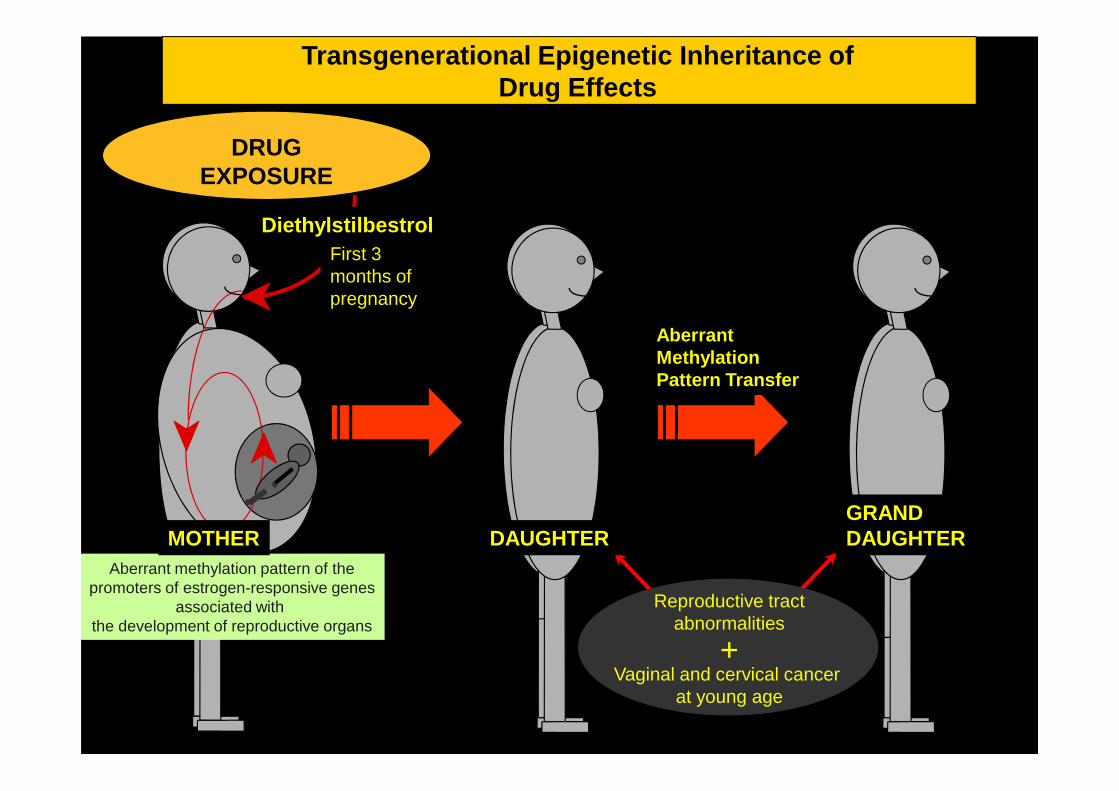
Transgenerational Epigenetic Inheritance ofDrug Effects
DRUGEXPOSURE
Diethylstilbestrol
AberrantMethylationPattern Transfer
First 3 months of pregnancy
Aberrant methylation pattern of thepromoters of estrogen-responsive genes
associated with the development of reproductive organs
Reproductive tractabnormalities
Vaginal and cervical cancer at young age
MOTHER DAUGHTERGRANDDAUGHTER
+
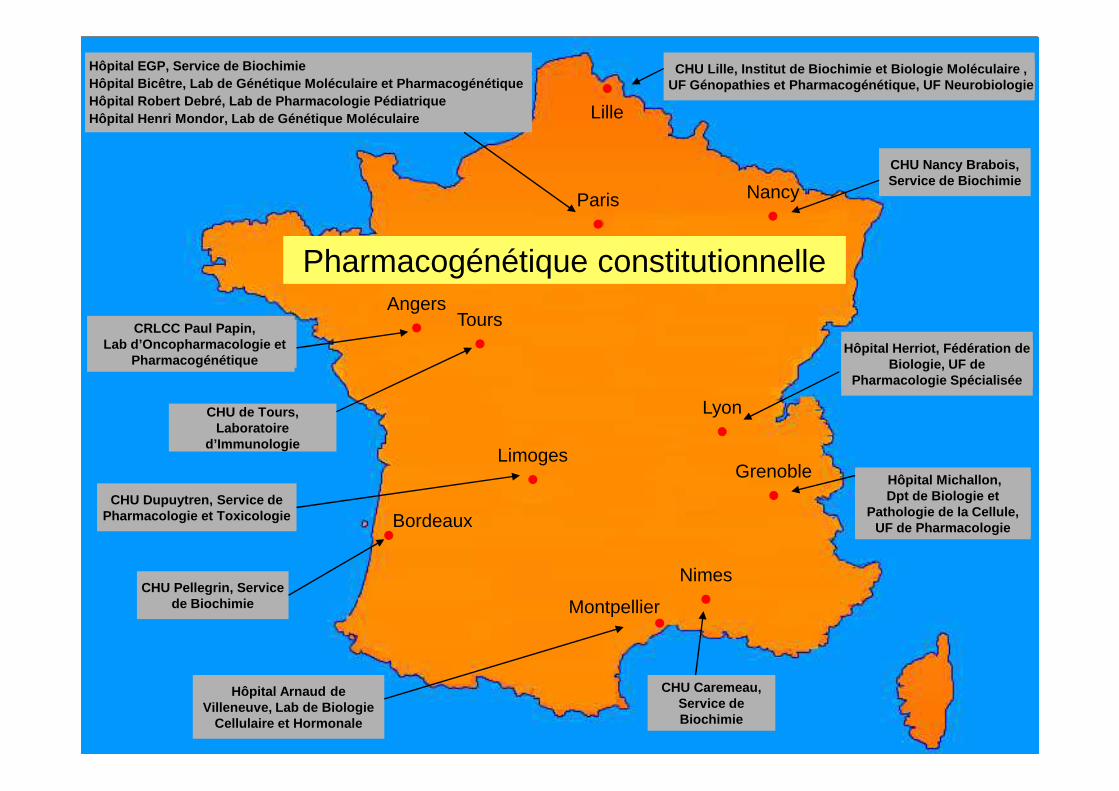
Lille
Paris Nancy
Tours
CHU Lille, Institut de Biochimie et Biologie Molécu laire , UF Génopathies et Pharmacogénétique, UF Neurobiolog ie
Hôpital Herriot, Fédération de Biologie, UF de
Pharmacologie Spécialisée
CHU Nancy Brabois, Service de Biochimie
Hôpital EGP, Service de BiochimieHôpital Bicêtre, Lab de Génétique Moléculaire et Ph armacogénétiqueHôpital Robert Debré, Lab de Pharmacologie Pédiatri que Hôpital Henri Mondor, Lab de Génétique Moléculaire
AngersCRLCC Paul Papin,
Lab d’Oncopharmacologie et Pharmacogénétique
Pharmacogénétique constitutionnelle
Grenoble
Nimes
Montpellier
Bordeaux
Limoges
CHU de Tours, Laboratoire
d’Immunologie
Hôpital Michallon, Dpt de Biologie et
Pathologie de la Cellule,UF de Pharmacologie
CHU Caremeau, Service de Biochimie
Hôpital Arnaud de Villeneuve, Lab de Biologie
Cellulaire et Hormonale
CHU Pellegrin, Service de Biochimie
Lyon
CHU Dupuytren, Service de Pharmacologie et Toxicologie
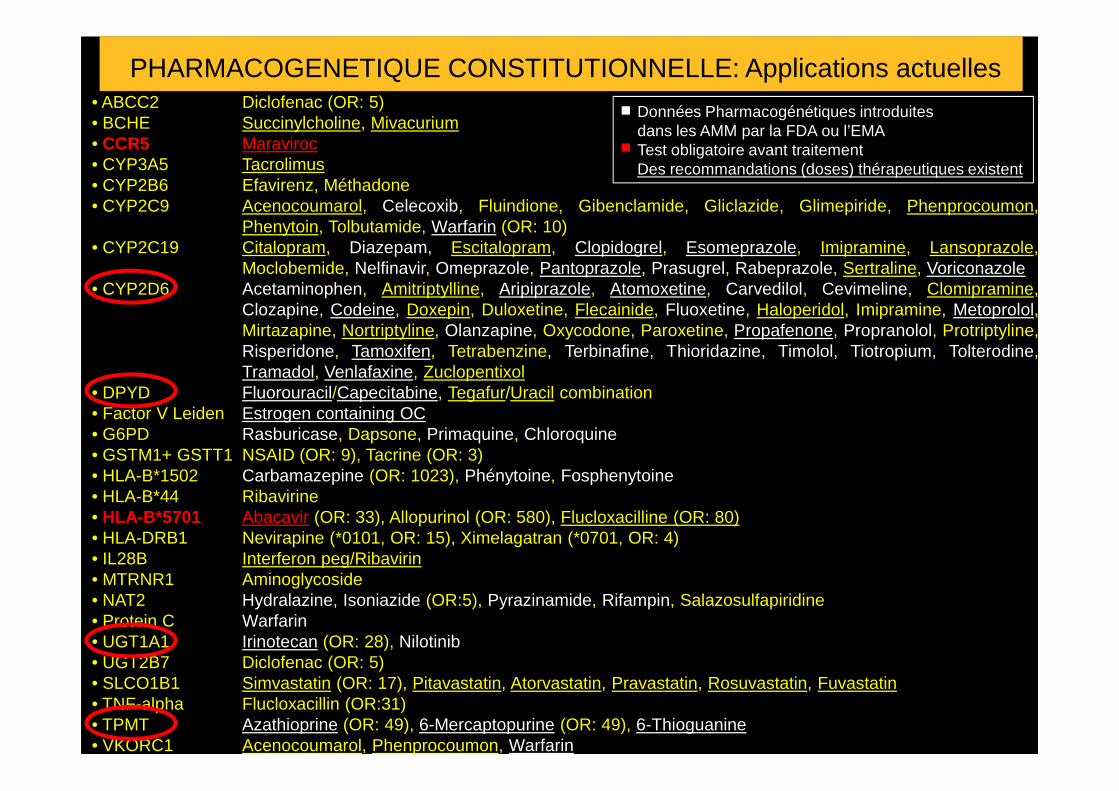
• ABCC2 Diclofenac (OR: 5)• BCHE Succinylcholine, Mivacurium• CCR5 Maraviroc• CYP3A5 Tacrolimus• CYP2B6 Efavirenz, Méthadone• CYP2C9 Acenocoumarol, Celecoxib, Fluindione, Gibenclamide, Gliclazide, Glimepiride, Phenprocoumon,
Phenytoin, Tolbutamide, Warfarin (OR: 10)• CYP2C19 Citalopram, Diazepam, Escitalopram, Clopidogrel, Esomeprazole, Imipramine, Lansoprazole,
Moclobemide, Nelfinavir, Omeprazole, Pantoprazole, Prasugrel, Rabeprazole, Sertraline, Voriconazole• CYP2D6 Acetaminophen, Amitriptylline, Aripiprazole, Atomoxetine, Carvedilol, Cevimeline, Clomipramine,
Clozapine, Codeine, Doxepin, Duloxetine, Flecainide, Fluoxetine, Haloperidol, Imipramine, Metoprolol,Mirtazapine, Nortriptyline, Olanzapine, Oxycodone, Paroxetine, Propafenone, Propranolol, Protriptyline,Risperidone, Tamoxifen, Tetrabenzine, Terbinafine, Thioridazine, Timolol, Tiotropium, Tolterodine,Tramadol, Venlafaxine, Zuclopentixol
• DPYD Fluorouracil/Capecitabine, Tegafur/Uracil combination
PHARMACOGENETIQUE CONSTITUTIONNELLE: Applications actuelles
Données Pharmacogénétiques introduites dans les AMM par la FDA ou l’EMATest obligatoire avant traitementDes recommandations (doses) thérapeutiques existent
• DPYD Fluorouracil/Capecitabine, Tegafur/Uracil combination• Factor V Leiden Estrogen containing OC• G6PD Rasburicase, Dapsone, Primaquine, Chloroquine• GSTM1+ GSTT1 NSAID (OR: 9), Tacrine (OR: 3)• HLA-B*1502 Carbamazepine (OR: 1023), Phénytoine, Fosphenytoine• HLA-B*44 Ribavirine• HLA-B*5701 Abacavir (OR: 33), Allopurinol (OR: 580), Flucloxacilline (OR: 80)• HLA-DRB1 Nevirapine (*0101, OR: 15), Ximelagatran (*0701, OR: 4)• IL28B Interferon peg/Ribavirin• MTRNR1 Aminoglycoside• NAT2 Hydralazine, Isoniazide (OR:5), Pyrazinamide, Rifampin, Salazosulfapiridine• Protein C Warfarin• UGT1A1 Irinotecan (OR: 28), Nilotinib• UGT2B7 Diclofenac (OR: 5)• SLCO1B1 Simvastatin (OR: 17), Pitavastatin, Atorvastatin, Pravastatin, Rosuvastatin, Fuvastatin• TNF-alpha Flucloxacillin (OR:31)• TPMT Azathioprine (OR: 49), 6-Mercaptopurine (OR: 49), 6-Thioguanine• VKORC1 Acenocoumarol, Phenprocoumon, Warfarin
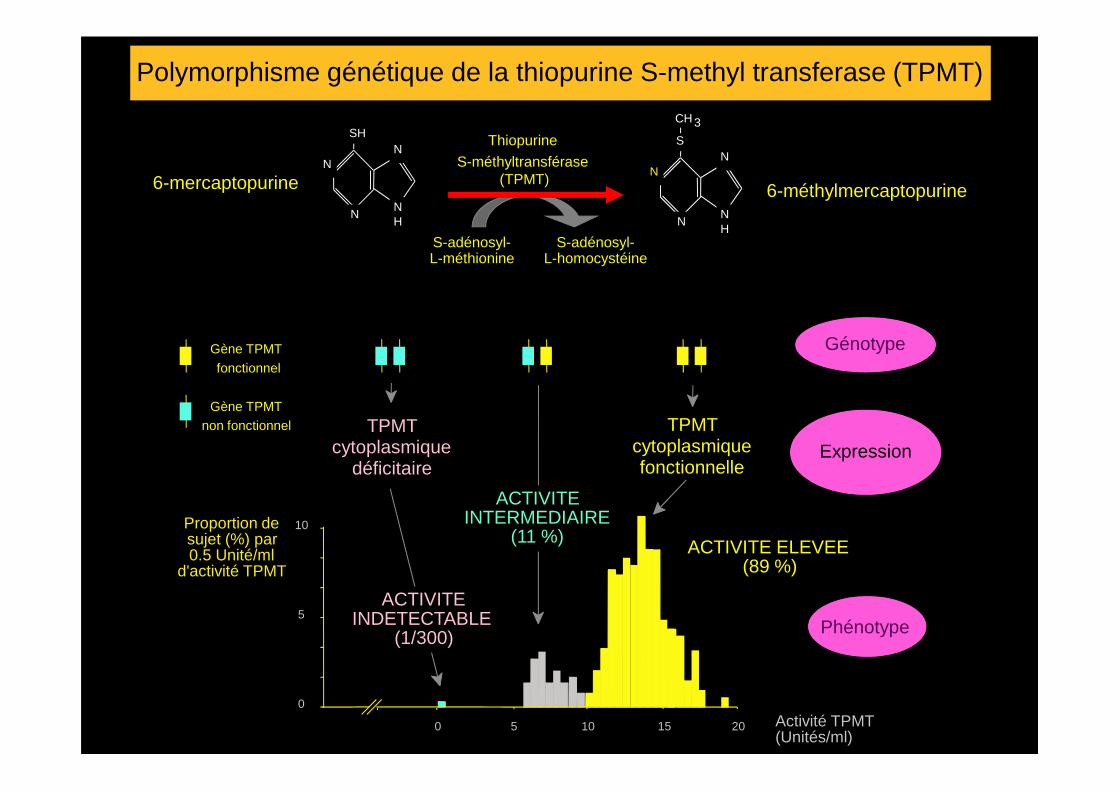
GénotypeGène TPMT
fonctionnel
Thiopurine
S-méthyltransférase (TPMT)
N
NNH
NSH
N
NNH
NS
CH 3
S-adénosyl-L-méthionine
S-adénosyl-L-homocystéine
6-mercaptopurine 6-méthylmercaptopurine
Polymorphisme génétique de la thiopurine S-methyl transferase (TPMT)
Expression
Phénotype
Proportion desujet (%) par0.5 Unité/ml
d'activité TPMT
ACTIVITEINDETECTABLE
(1/300)
ACTIVITE ELEVEE(89 %)
TPMTcytoplasmique
déficitaire
TPMTcytoplasmiquefonctionnelle
Gène TPMT non fonctionnel
0
10
5
0 Activité TPMT(Unités/ml)
5 10 15 20
ACTIVITEINTERMEDIAIRE
(11 %)
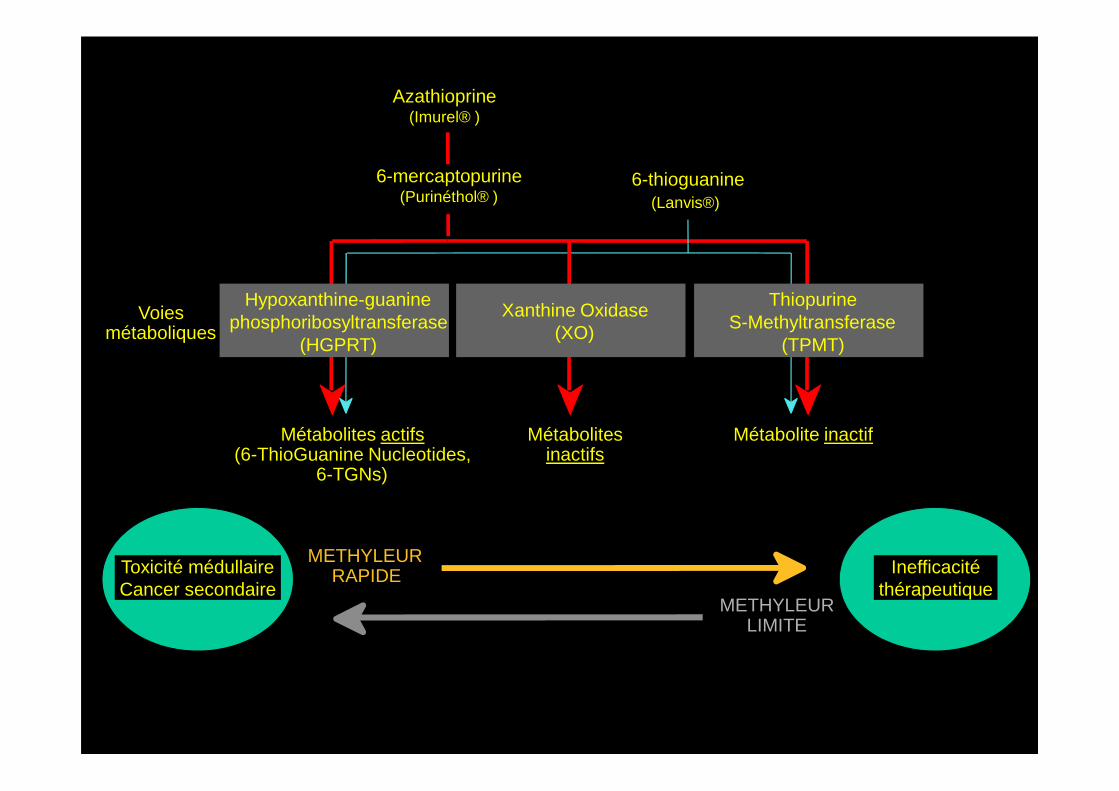
Azathioprine(Imurel® )
6-thioguanine(Lanvis®)
Voiesmétaboliques
Hypoxanthine-guaninephosphoribosyltransferase
(HGPRT)
Xanthine Oxidase(XO)
ThiopurineS-Methyltransferase
(TPMT)
6-mercaptopurine(Purinéthol® )
Métabolites actifs(6-ThioGuanine Nucleotides,
6-TGNs)
Métabolitesinactifs
Métabolite inactif
METHYLEURRAPIDE
METHYLEURLIMITE
Toxicité médullaire Cancer secondaire
Inefficacitéthérapeutique
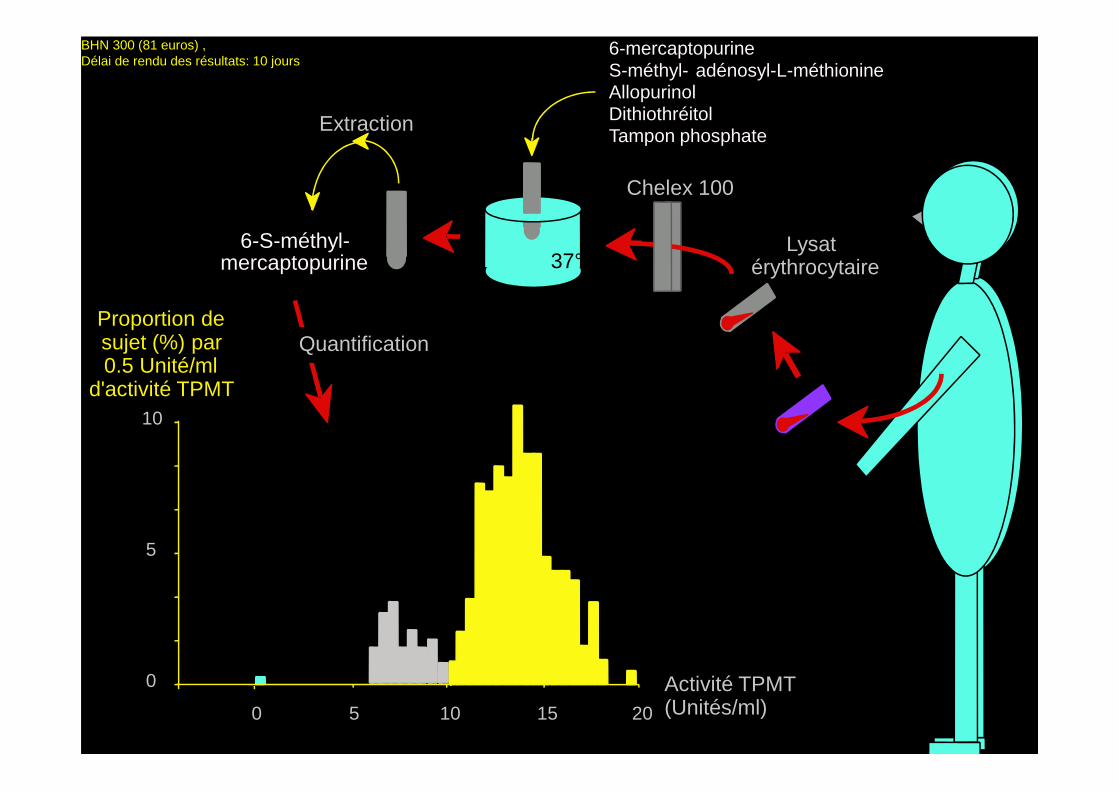
Lysatérythrocytaire
Chelex 100
37°
6-mercaptopurineS-méthyl- adénosyl-L-méthionineAllopurinolDithiothréitolTampon phosphate
Extraction
6-S-méthyl-mercaptopurine
QuantificationProportion desujet (%) par0.5 Unité/ml
d'activité TPMT
BHN 300 (81 euros) , Délai de rendu des résultats: 10 jours
0
10
5
0 5 10 15 20
d'activité TPMT
Activité TPMT(Unités/ml)
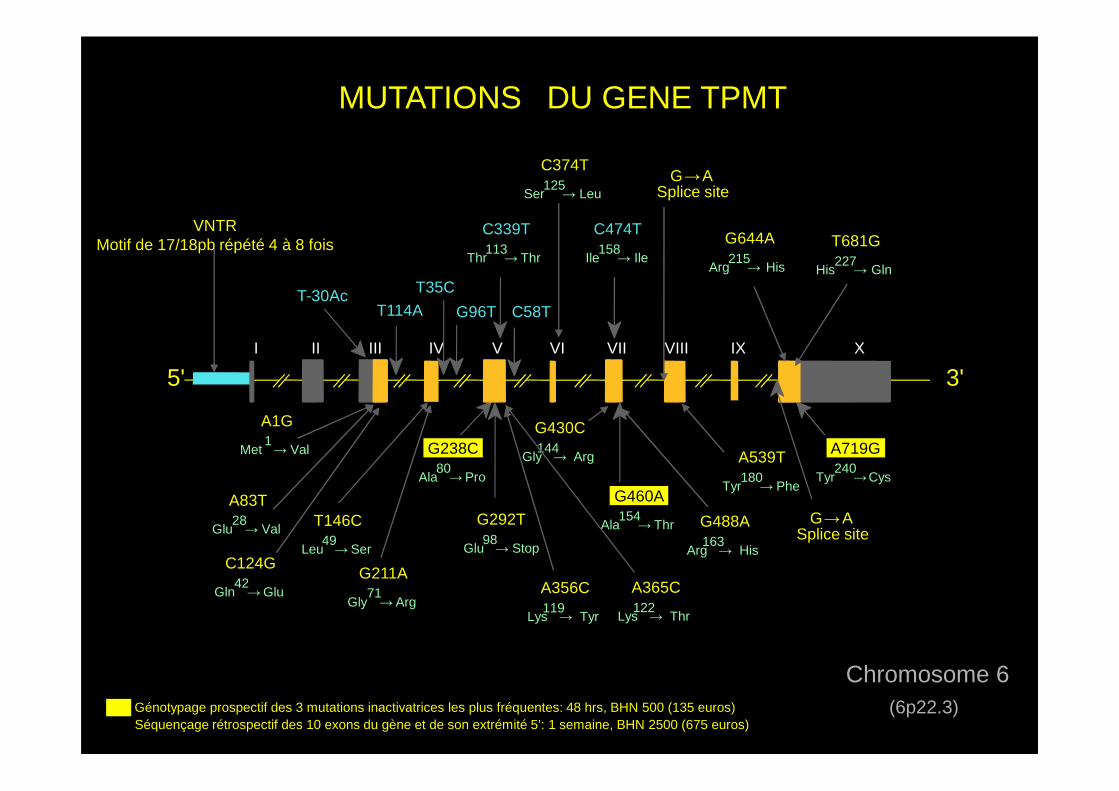
MUTATIONS DU GENE TPMT
I II III IV V VI VII VIII IX X
5' 3'
C474T
Ile158→ Ile
C339T
Thr113→ Thr
T-30AcT114A
T35C
C58TG96T
T681G
His227→ Gln
G644A
Arg215→ His
C374T
Ser125→ Leu
G →ASplice site
VNTRMotif de 17/18pb répété 4 à 8 fois
G238C
Ala80→ Pro
A719G
Tyr240→Cys
G460A
Ala154→ Thr
Chromosome 6(6p22.3)
G292T
Glu98→ Stop
G →AT146C
Leu49→ Ser
A539T
Tyr180→ Phe
Génotypage prospectif des 3 mutations inactivatrices les plus fréquentes: 48 hrs, BHN 500 (135 euros)
Splice site
A356C
Lys119→ Tyr
G430C
Gly144→ Arg
A83T
Glu28→ Val
A1G
Met1→ Val
G488A
Arg163→ His
C124G
Gln42→Glu
G211A
Gly71→ Arg
A365C
Lys122→ Thr
Séquençage rétrospectif des 10 exons du gène et de son extrémité 5’: 1 semaine, BHN 2500 (675 euros)
PRETREATMENT COUNSELLING AND TPMT SCREENING
In the context of the information presented, it is recommended that safety and efficacy issuesare discussed fully with patients before treatment with azathioprine or 6-mercaptopurine isstarted. The obvious concern is the one in 300 chance of an absolute deficiency in TPMT whichwould predispose a patient to a serious risk of early and severe pancytopenia and secondarycancer. Both patients and their physicians will have different responses to such a risk which willbe influenced by cultural, educational and emotional factors in addition to the medical indicationfor its usage. What is certain is that it is no longer adequate for the physician to recommendazathioprine or 6-mercaptopurine on the basis of their personal experience of the efficacy andsafety of the drugs without more detailed discussion concerning possible risks of therapy thanhas hitherto been the case. Patients in the UK will need to be informed that susceptibility to therisk of severe toxicity with these drugs whilst rare, is not yet detectable by pretreatmentrisk of severe toxicity with these drugs whilst rare, is not yet detectable by pretreatmentscreening. Neither TPMT assay nor the measurement of 6-TGNs is currently routinely availablein the UK and until they are, safety monitoring for azathioprine and 6-mercaptopurine willcontinue to follow the manufacturer’s guidelines. These are being amended to highlight concernsabout the genetically determined susceptibility of some individuals to drug toxicity. The goldstandard for TPMT assay is the radiochemical assay of Weinshilboum et al., although work fromseveral groups to assess an HPLC technique has recently been completed. The cDNA for TPMThas recently been cloned, sequenced and expressed and this opens up the possibility of agenotyping test which, if successful, promises to have the potential for usage in routine TPMTmonitoring. Until such a test becomes widely available in the UK an element of Russian roulettewill continue to characterise azathioprine and 6-mercaptopurine usage.
Anstey A. Journal of the Royal Society of Medicine, 1995, 88: 155-160.
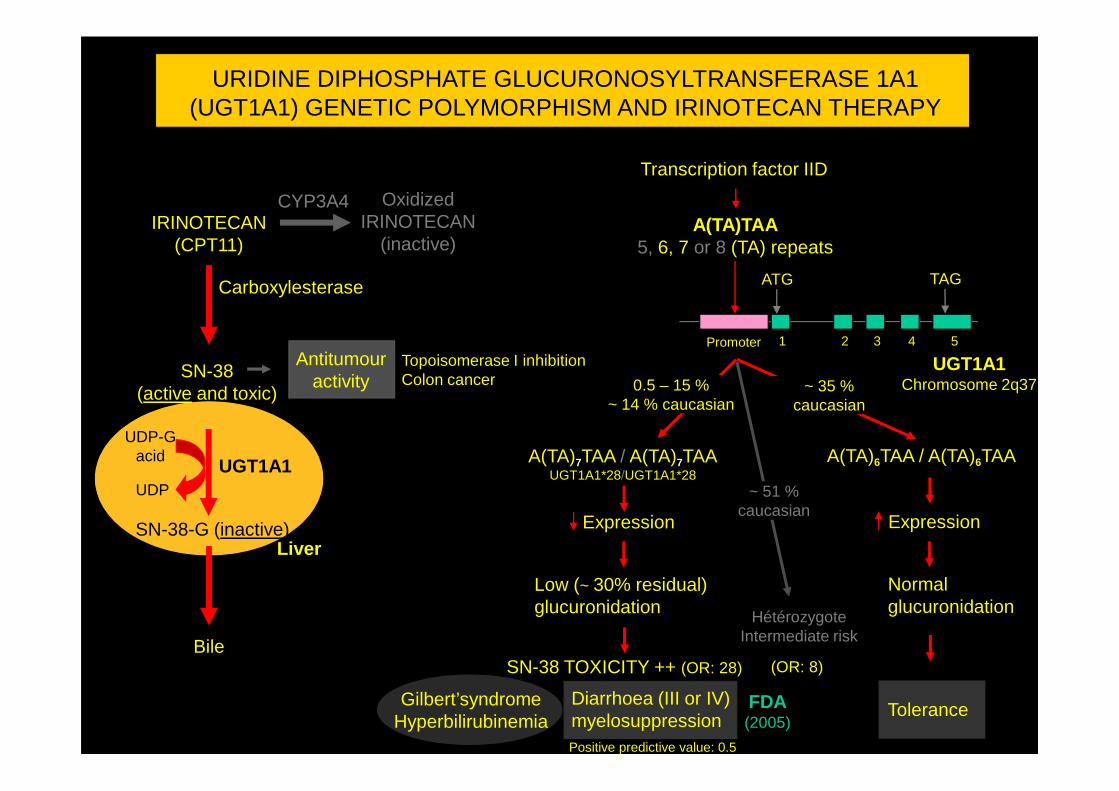
IRINOTECAN(CPT11)
Transcription factor IID
ATG TAG
A(TA)TAA5, 6, 7 or 8 (TA) repeats
Promoter 1 2 3 4 5
OxidizedIRINOTECAN
(inactive)
SN-38(active and toxic)
Antitumour activity
Carboxylesterase
UGT1A1Chromosome 2q37
CYP3A4
URIDINE DIPHOSPHATE GLUCURONOSYLTRANSFERASE 1A1 (UGT1A1) GENETIC POLYMORPHISM AND IRINOTECAN THERAPY
0.5 – 15 %~ 14 % caucasian
Topoisomerase I inhibitionColon cancer ~ 35 %(active and toxic)
SN-38-G (inactive)
Bile
Liver
UGT1A1 A(TA)7TAA / A(TA)7TAAUGT1A1*28/UGT1A1*28
Expression
Low (~ 30% residual)glucuronidation
Diarrhoea (III or IV)myelosuppression
Expression
Normal glucuronidation
Tolerance
~ 14 % caucasian
UDP-Gacid
UDP
Gilbert’syndrome Hyperbilirubinemia
SN-38 TOXICITY ++ (OR: 28)
A(TA)6TAA / A(TA)6TAA
HétérozygoteIntermediate risk
caucasian
~ 51 %caucasian
(OR: 8)
FDA(2005)
Positive predictive value: 0.5
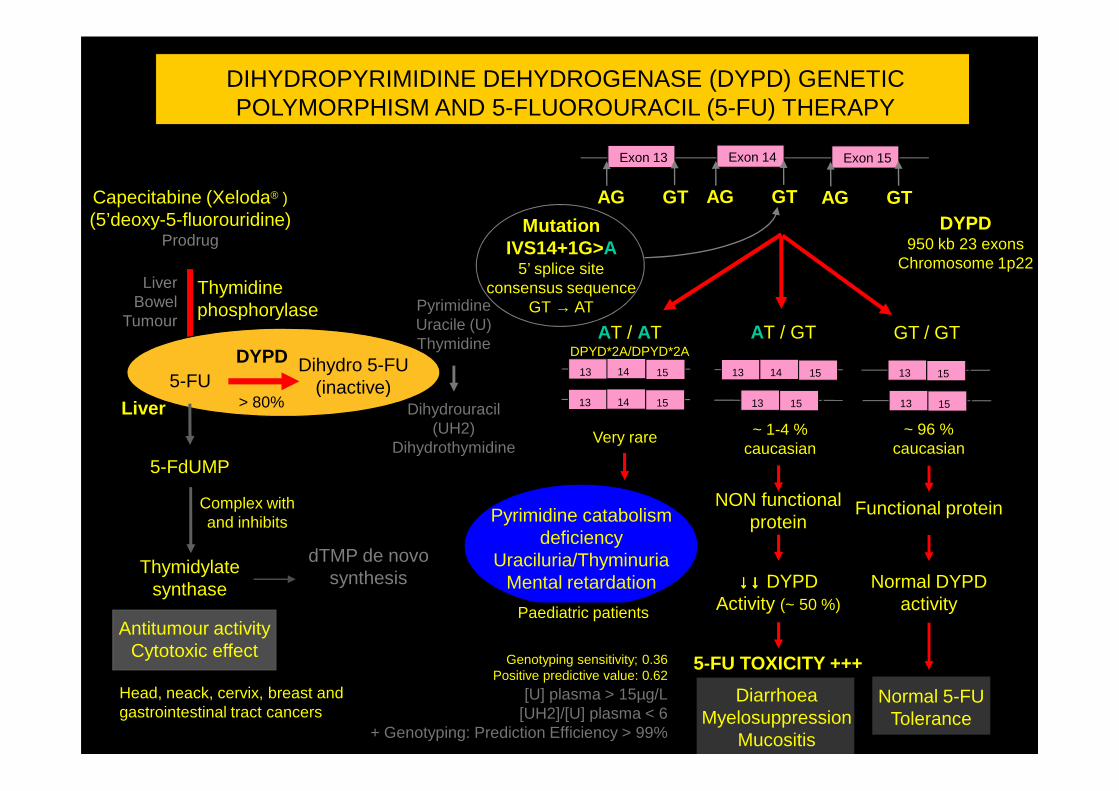
Capecitabine (Xeloda® )(5’deoxy-5-fluorouridine)
ProdrugMutation
IVS14+1G>A5’ splice site
consensus sequenceGT → AT
Exon 13
Thymidinephosphorylase
DYPD950 kb 23 exons
Chromosome 1p22
AT / ATDPYD*2A/DPYD*2A
DIHYDROPYRIMIDINE DEHYDROGENASE (DYPD) GENETIC POLYMORPHISM AND 5-FLUOROURACIL (5-FU) THERAPY
GTAG
Exon 14
GTAG
Exon 15
GTAG
GT / GTAT / GT
13 14 15 13 14 15 13 Exon1415
LiverBowel
TumourPyrimidineUracile (U)Thymidine
5-FUDihydro 5-FU
(inactive)
DYPD
> 80%
DiarrhoeaMyelosuppression
Mucositis
Antitumour activityCytotoxic effect
Functional protein
Normal 5-FU Tolerance
~ 1-4 %caucasian
Head, neack, cervix, breast and gastrointestinal tract cancers
Pyrimidine catabolism deficiency
Uraciluria/ThyminuriaMental retardation
5-FU TOXICITY +++
~ 96 %caucasian
13 14 15 13 Exon1415 13 Exon1415
Very rare
Normal DYPD activity
NON functional protein
↓↓↓↓↓↓↓↓ DYPDActivity (~ 50 %)Paediatric patients
Thymidylate synthase
dTMP de novosynthesis
5-FdUMP
Complex withand inhibits
Dihydrouracil (UH2)
Dihydrothymidine
(inactive)> 80%Liver
[U] plasma > 15µg/L[UH2]/[U] plasma < 6
+ Genotyping: Prediction Efficiency > 99%
Genotyping sensitivity; 0.36Positive predictive value: 0.62
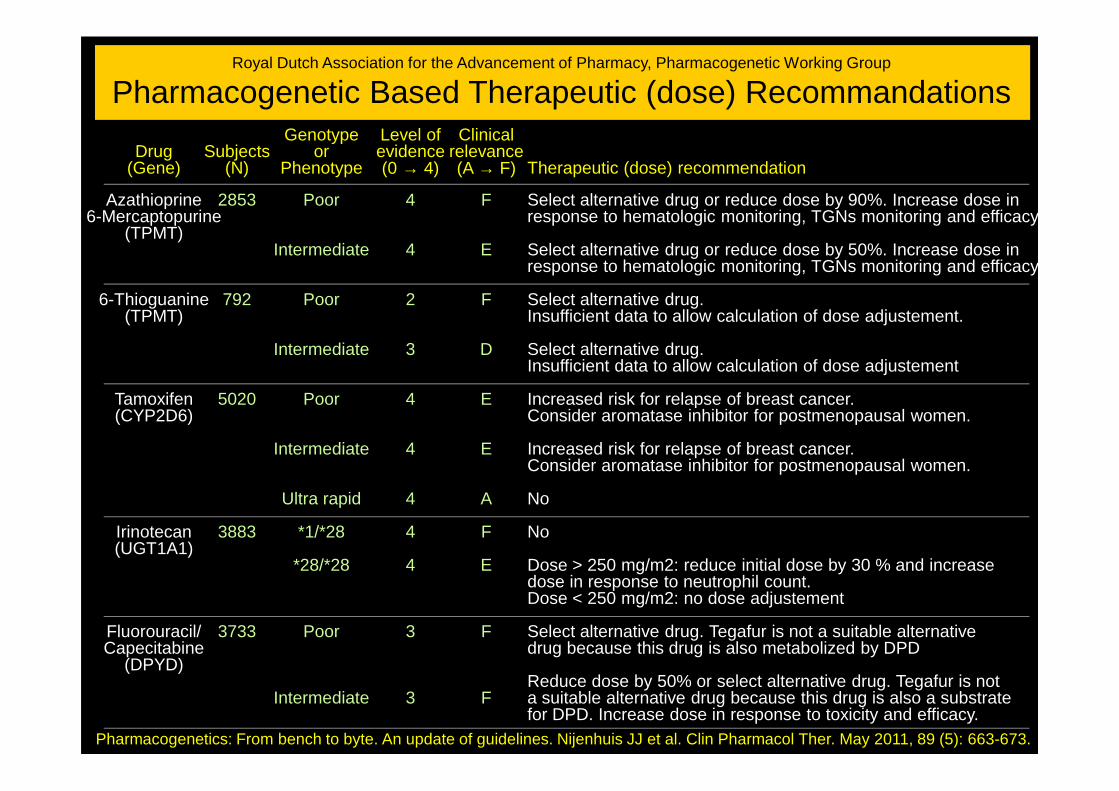
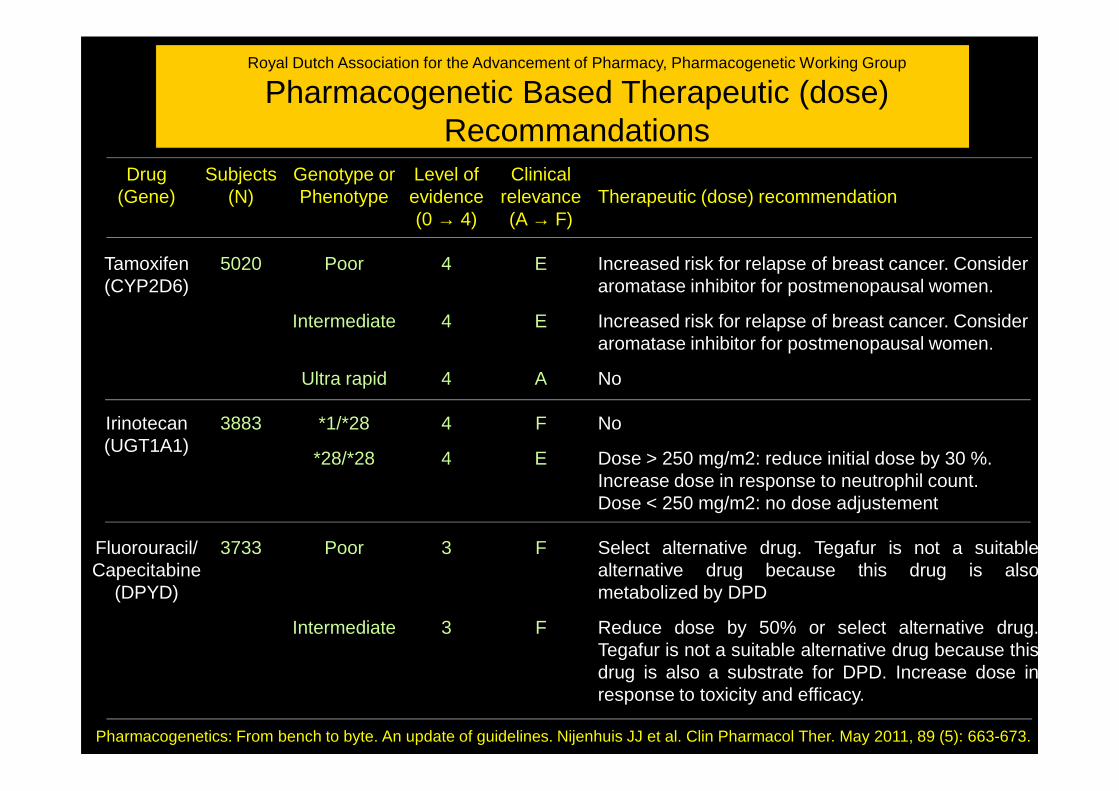
Royal Dutch Association for the Advancement of Pharmacy, Pharmacogenetic Working Group
Pharmacogenetic Based Therapeutic (dose) Recommandations
Drug(Gene)
Azathioprine6-Mercaptopurine
(TPMT)
6-Thioguanine(TPMT)
Tamoxifen
Subjects(N)
2853
792
5020
Genotypeor
Phenotype
Poor
Intermediate
Poor
Intermediate
Poor
Level of evidence(0 → 4)
4
4
2
3
4
Clinical relevance(A → F)
F
E
F
D
E
Therapeutic (dose) recommendation
Select alternative drug or reduce dose by 90%. Increase dose in response to hematologic monitoring, TGNs monitoring and efficacy
Select alternative drug or reduce dose by 50%. Increase dose in response to hematologic monitoring, TGNs monitoring and efficacy
Select alternative drug. Insufficient data to allow calculation of dose adjustement.
Select alternative drug. Insufficient data to allow calculation of dose adjustement
Increased risk for relapse of breast cancer. Tamoxifen(CYP2D6)
Irinotecan(UGT1A1)
Fluorouracil/Capecitabine
(DPYD)
Pharmacogenetics: From bench to byte. An update of guidelines. Nijenhuis JJ et al. Clin Pharmacol Ther. May 2011, 89 (5): 663-673.
5020
3883
3733
Poor
Intermediate
Ultra rapid
*1/*28
*28/*28
Poor
Intermediate
4
4
4
4
4
3
3
E
E
A
F
E
F
F
Increased risk for relapse of breast cancer. Consider aromatase inhibitor for postmenopausal women.
Increased risk for relapse of breast cancer. Consider aromatase inhibitor for postmenopausal women.
No
No
Dose > 250 mg/m2: reduce initial dose by 30 % and increase dose in response to neutrophil count.Dose < 250 mg/m2: no dose adjustement
Select alternative drug. Tegafur is not a suitable alternativedrug because this drug is also metabolized by DPD
Reduce dose by 50% or select alternative drug. Tegafur is nota suitable alternative drug because this drug is also a substratefor DPD. Increase dose in response to toxicity and efficacy.
Pharmacogénétique constitutionnelleApplications aux anticancéreux: Perspectives
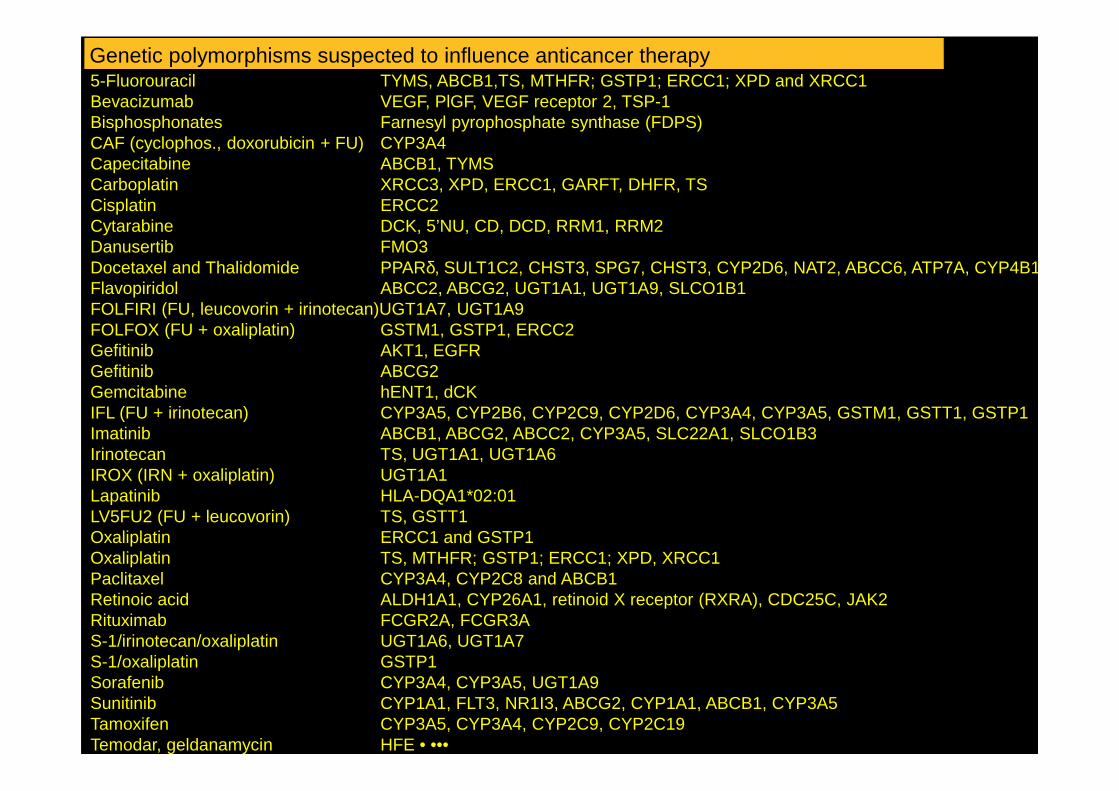
Genetic polymorphisms suspected to influence anticancer therapy5-Fluorouracil TYMS, ABCB1,TS, MTHFR; GSTP1; ERCC1; XPD and XRCC1Bevacizumab VEGF, PlGF, VEGF receptor 2, TSP-1Bisphosphonates Farnesyl pyrophosphate synthase (FDPS)CAF (cyclophos., doxorubicin + FU) CYP3A4Capecitabine ABCB1, TYMSCarboplatin XRCC3, XPD, ERCC1, GARFT, DHFR, TSCisplatin ERCC2Cytarabine DCK, 5’NU, CD, DCD, RRM1, RRM2Danusertib FMO3Docetaxel and Thalidomide PPARδ, SULT1C2, CHST3, SPG7, CHST3, CYP2D6, NAT2, ABCC6, ATP7A, CYP4B1, SLC10A2 Flavopiridol ABCC2, ABCG2, UGT1A1, UGT1A9, SLCO1B1FOLFIRI (FU, leucovorin + irinotecan)UGT1A7, UGT1A9FOLFOX (FU + oxaliplatin) GSTM1, GSTP1, ERCC2Gefitinib AKT1, EGFRGefitinib ABCG2Gemcitabine hENT1, dCKGemcitabine hENT1, dCKIFL (FU + irinotecan) CYP3A5, CYP2B6, CYP2C9, CYP2D6, CYP3A4, CYP3A5, GSTM1, GSTT1, GSTP1Imatinib ABCB1, ABCG2, ABCC2, CYP3A5, SLC22A1, SLCO1B3Irinotecan TS, UGT1A1, UGT1A6IROX (IRN + oxaliplatin) UGT1A1Lapatinib HLA-DQA1*02:01LV5FU2 (FU + leucovorin) TS, GSTT1Oxaliplatin ERCC1 and GSTP1Oxaliplatin TS, MTHFR; GSTP1; ERCC1; XPD, XRCC1Paclitaxel CYP3A4, CYP2C8 and ABCB1Retinoic acid ALDH1A1, CYP26A1, retinoid X receptor (RXRA), CDC25C, JAK2Rituximab FCGR2A, FCGR3AS-1/irinotecan/oxaliplatin UGT1A6, UGT1A7S-1/oxaliplatin GSTP1Sorafenib CYP3A4, CYP3A5, UGT1A9Sunitinib CYP1A1, FLT3, NR1I3, ABCG2, CYP1A1, ABCB1, CYP3A5Tamoxifen CYP3A5, CYP3A4, CYP2C9, CYP2C19Temodar, geldanamycin HFE • •••
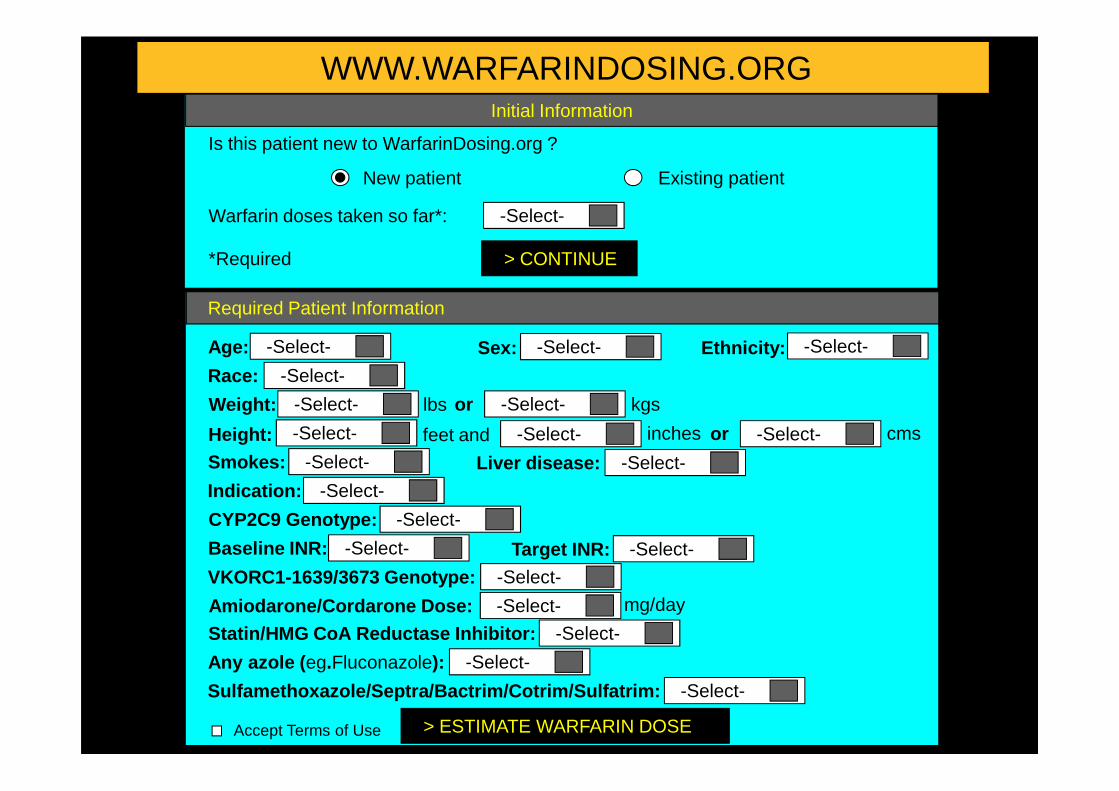
WWW.WARFARINDOSING.ORGInitial Information
Is this patient new to WarfarinDosing.org ?
New patient Existing patient
Warfarin doses taken so far*: -Select-
*Required > CONTINUE
Required Patient Information
Age: -Select-
Race: -Select-
Weight: -Select-
-Select- -Select-Ethnicity:Sex:
lbs or kgs-Select-
> ESTIMATE WARFARIN DOSE
Weight: -Select-
Height: -Select-
Smokes: -Select-
Indication: -Select-
CYP2C9 Genotype: -Select-
Baseline INR: -Select-
VKORC1-1639/3673 Genotype: -Select-
Amiodarone/Cordarone Dose: -Select-
Statin/HMG CoA Reductase Inhibitor: -Select-
Any azole ( eg.Fluconazole): -Select-
Sulfamethoxazole/Septra/Bactrim/Cotrim/Sulfatrim: -Select-
Accept Terms of Use
lbs or kgs-Select-
feet and inches-Select- or cms-Select-
Liver disease: -Select-
Target INR: -Select-
mg/day
PHARMACOGENETIQUE MOLECULAIRE
Problèmes d’organisation au plan national
• Dispersée• Fractionnée• Manque de visibilité• Manque de coordination
Problèmes économiquesProblèmes économiques
• Selon la région, l’hôpital • Hétérogénéité des modes de financement et de fonctionnement
Inégalités • d’accés aux tests• de prise en charge et de paiement• de qualité et fiabilité des analyses
Considérations éthiques, légales, sociales et économiques
Proposition du test
• Connaissances • Médecin• Patient
• Informations scientifiques
• Recommandations • Autorités• Industriels
• Médicament / pathologie• Facilités à réaliser le test
Prospectif ou Rétrospectif
Fréquence des phénotypes, pénétrance•
• Facilités à réaliser le test• Coût de l'analyse• Responsabilités • Médicales
• Autorités
Consentement éclairé écrit du patient
• Dépend de l'information que transporte le test • Pharmacogénétique• Révélatrice d'une pathologie• Facteur de risque pathologique ou autre
• Contenu va dépendre • Capacité du patient à comprendre l'information et ses conséquences• Effet psychologique du résultat du test• Informations complémentaires devront être données
Au cas par cas
Considérations éthiques, légales, sociales et économiques
Réalisation de l'analyse
Qui doit faire les tests et dans quels conditions ?
• Vide juridique• Professionnel de la santé agréés • Possibilité d'information touchant à la santé
• Difficultés d'interprétation et de fiabilité des tests
Résultats et interprétation de l'analyse
Fournis au prescripteur
Interprétés par le labo et le prescripteur • Pharmacologue ?• Généticien ?• Conseil génétique ?Utilisation du résultat
• Dépend de nb facteurs • Maladie / médicament• Traitement alternatif ou non• Thérapeutique / exposition "off-label"• Balance bénéfice / risque
• Biologiste ?
Considérations éthiques, légales, sociales et économiques
Propriété et confidentialité de l'information
Pour le sujet • Résultats inclus dans le dossier médical• Information disponible à l'ensemble du personnel médical directement
responsable de sa santé mais appréhende la possibilité d'un accès à cesinformations par d'autres groupes sociaux
Pour la famille
• Conséquences possibles Information PG+++ ex: situation d'urgence
Informations donnés par le médecin aux patients avec ses conséquences
• Conséquences possibles Information PG+++ ex: situation d'urgenceSusceptibilité à une pathologie ou autres
Il est évident que dans certaines circonstances le médecin doit
encourager le patient à donner ces informations au reste de la famille.
Autres groupes sociaux
• Inconvénients • Patient "difficile à traiter " "cher à traiter" ou "maladie sérieuse intraitable "
• Informations associées (maladie, addictions)
• Avantages • Patient pourra être traité efficacement, mieux que la population générale
• Problème de l’information révélée indirectement
• Réponse ?
• Individu "inemployable"
• Seul capable d’occuper un emploi
PharmacogénétiqueÉtude de l’influence de l’hérédité sur l’effet des médicaments
1 Identification des variations de réponse aux médicaments
d'origine génétique
2 Étude de leur mécanisme moléculaire
COMPRENDRE,PREVOIR et PREVENIR
la survenue d’anomalies de réponse aux médicaments
2 Étude de leur mécanisme moléculaire
3 Évaluation de leur importance clinique
4 Développement de méthodes d'identification des individus
à risque Avant exposition ++++
Susceptibilité de l’organisme humain à l’environnement chimique
Mise en évidence de facteurs (génétiques et épigénétiques) de variation interindividuelleMise en évidence de facteurs (génétiques et épigénétiques) de variation interindividuelle
Pr Franck Broly, MD, PhDUnité de Génopathies, Pharmacogénétique et Toxicogénétique, Centre de Biologie et Pathologie, CHRU Lille;
EA4483: « Impact de l’environnement chimique sur la santé »Pôle Recherche, Faculté de Médecine, Université Lille Nord de France, Lille.
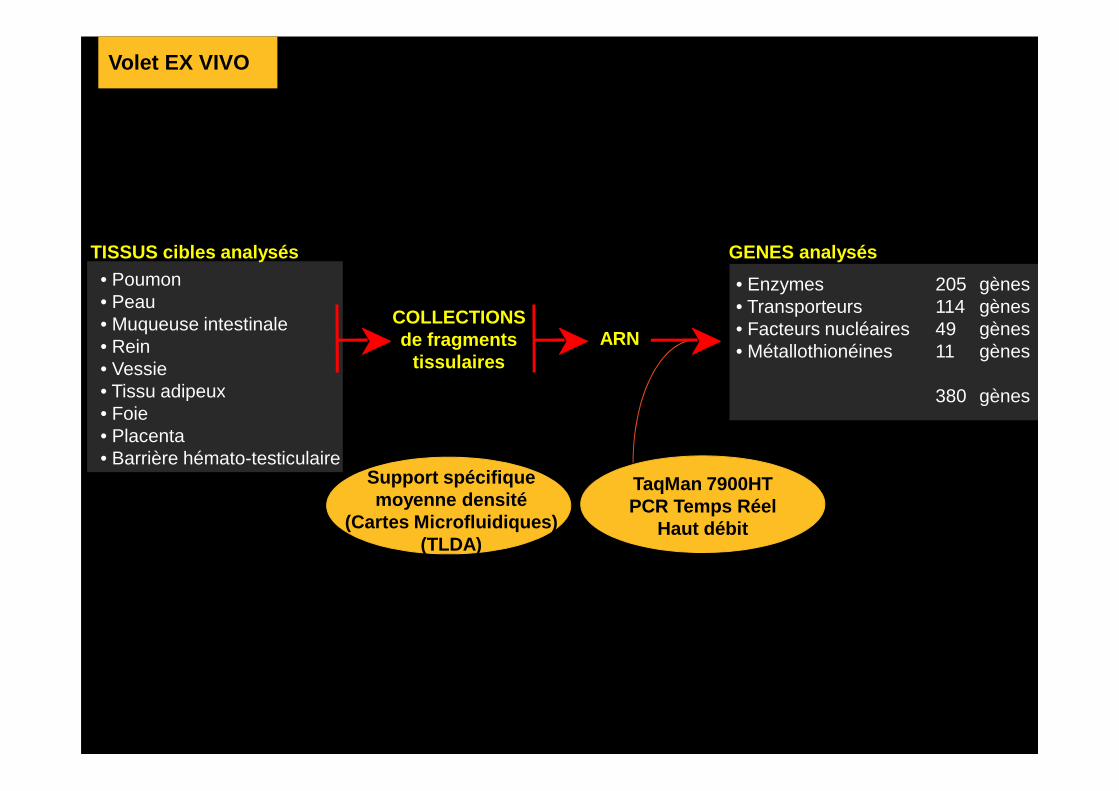
TISSUS cibles analysés• Poumon• Peau• Muqueuse intestinale• Rein• Vessie• Tissu adipeux
COLLECTIONSde fragments
tissulairesARN
GENES analysés
• Enzymes 205 gènes• Transporteurs 114 gènes• Facteurs nucléaires 49 gènes• Métallothionéines 11 gènes
380 gènes
Volet EX VIVO
• Tissu adipeux• Foie• Placenta• Barrière hémato-testiculaire
380 gènes
TaqMan 7900HTPCR Temps Réel
Haut débit
Support spécifique moyenne densité
(Cartes Microfluidiques)(TLDA)
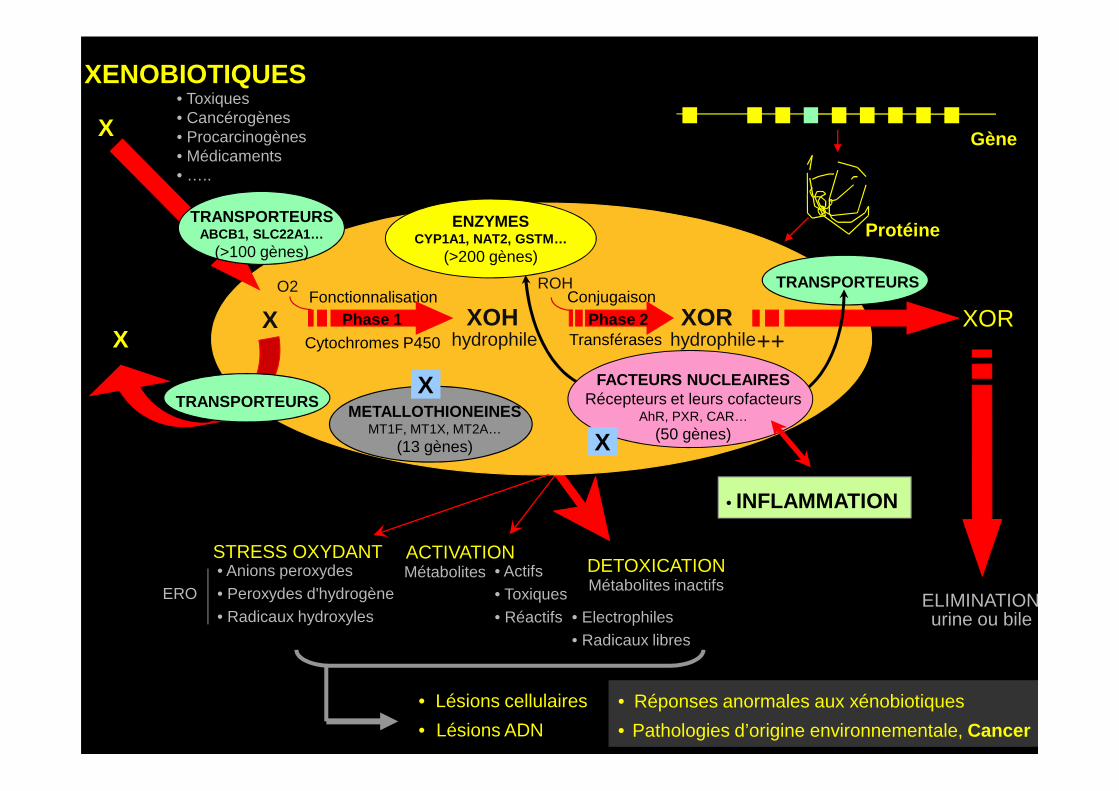
FACTEURS NUCLEAIRESRécepteurs et leurs cofacteurs
XORhydrophile ++
XENOBIOTIQUES
XORX
ENZYMESCYP1A1, NAT2, GSTM…
(>200 gènes)
TRANSPORTEURS
TRANSPORTEURS
Gène
Protéine
• Toxiques• Cancérogènes• Procarcinogènes• Médicaments• …..
X
TRANSPORTEURSABCB1, SLC22A1…
(>100 gènes)
X
Conjugaison
XOHhydrophile
X Phase 2Fonctionnalisation
Phase 1
O2 ROH
TransférasesCytochromes P450
Récepteurs et leurs cofacteursAhR, PXR, CAR…
(50 gènes)
DETOXICATIONMétabolites • Actifs • Toxiques • Réactifs
ACTIVATION
ELIMINATIONurine ou bile
• Réponses anormales aux xénobiotiques
• Pathologies d’origine environnementale, Cancer
TRANSPORTEURSMETALLOTHIONEINES
MT1F, MT1X, MT2A…(13 gènes)
Métabolites inactifs
X
X
• Lésions cellulaires
• Lésions ADN
• Electrophiles • Radicaux libres
STRESS OXYDANT• Anions peroxydes• Peroxydes d'hydrogène• Radicaux hydroxyles
ERO
• INFLAMMATION
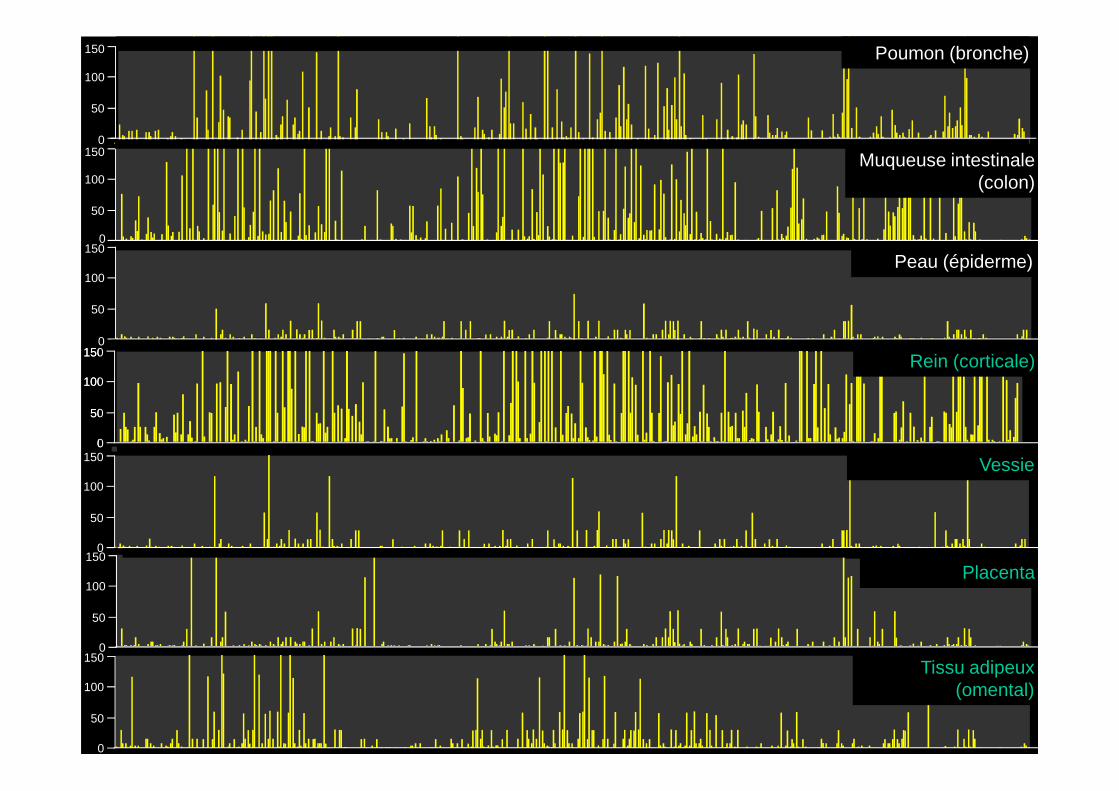
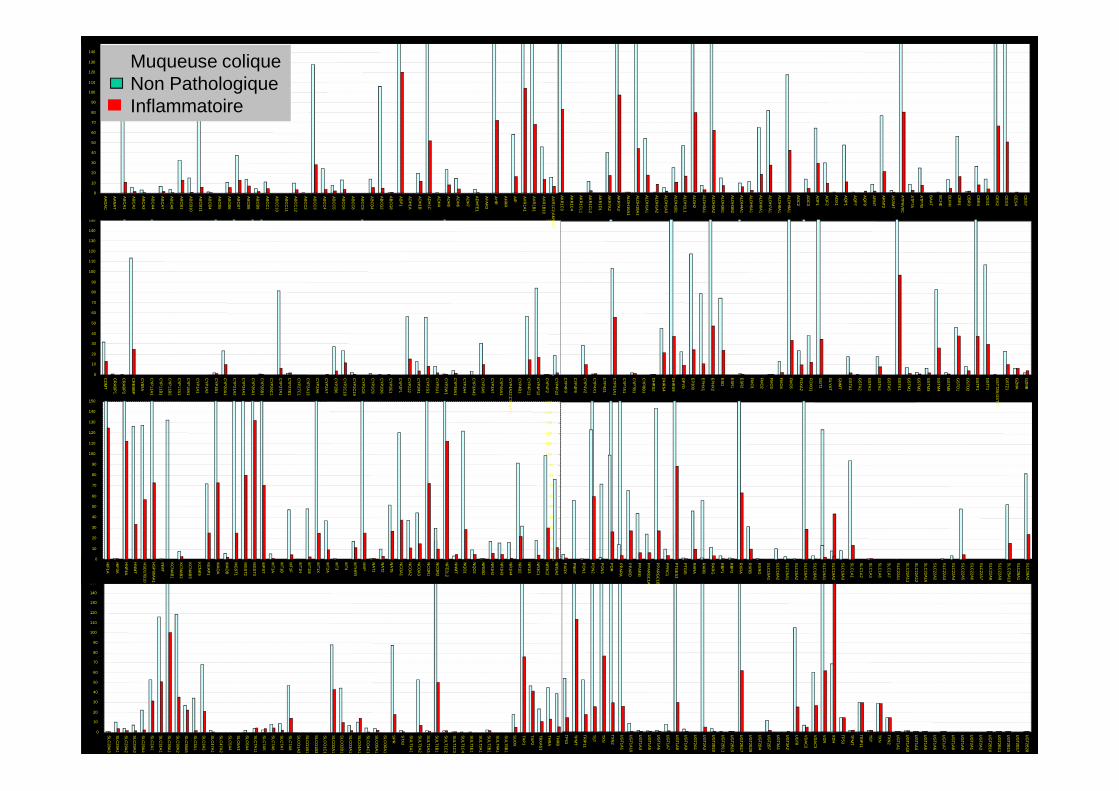
Muqueuse intestinale (colon)100
50
Inflammation +++
150
100
50
0150
100
50
Peau (épiderme)150
0
0
100
150Rein (corticale)
100
150
Poumon (bronche)
Enzymes Phase 1 Enzymes Phase 2 Transporteurs Facteurs n ucléaires
Placenta
Non pathologique
Muqueuse intestinaleVessie
50
0
100
50
150
0
100
50
150
0
100
50
150
0
Tissu adipeux (omental)
50
0
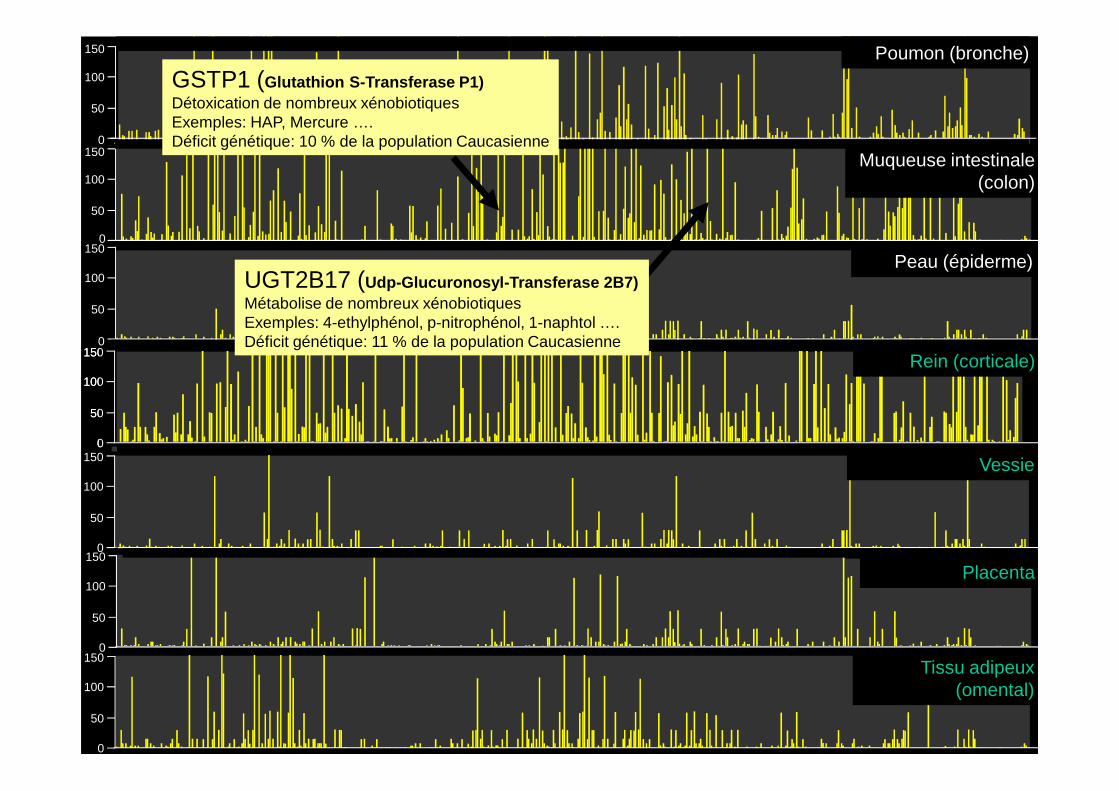
Muqueuse intestinale (colon)100
50
Inflammation +++
150
100
50
0150
100
50
Peau (épiderme)150
0
0
100
150Rein (corticale)
100
150
Poumon (bronche)
GSTP1 (Glutathion S-Transferase P1)Détoxication de nombreux xénobiotiquesExemples: HAP, Mercure ….Déficit génétique: 10 % de la population Caucasienne
UGT2B17 (Udp-Glucuronosyl-Transferase 2B7)Métabolise de nombreux xénobiotiquesExemples: 4-ethylphénol, p-nitrophénol, 1-naphtol ….Déficit génétique: 11 % de la population Caucasienne
Enzymes Phase 1 Enzymes Phase 2 Transporteurs Facteurs n ucléaires
Placenta
Non pathologique
Muqueuse intestinaleVessie
50
0
100
50
150
0
100
50
150
0
100
50
150
0
Tissu adipeux (omental)
50
0
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
CY
P4F
3
CY
P4F
8
CY
P4V
2
CY
P4X
1
CY
P4Z
1
CY
P51A
1
CY
P7A
1
CY
P7B
1
CY
P8B
1
DH
RS
2
DH
RS
4
DH
RS
9
DP
YD
EP
300
EP
HX
1
EP
HX
2
ES
D
ES
R1
ES
R2
FM
O1
FM
O2
FM
O3
FM
O4
FM
O5
FO
XA
2
FO
XO
1
GG
T1
GLY
AT
GN
MT
GS
TA1
GS
TA2
GS
TA3
GS
TA4
GS
TA5
GS
TK1
GS
TM1
GS
TM2
GS
TM3
GS
TM4
GS
TM5
GS
TO1
GS
TO2
GS
TP1
GS
TT1
GS
TT2B;G
ST
T2
GS
TZ1
GZ
MA
GZ
MB
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
CO
MT
CR
AB
P1
CR
AB
P2
CR
EB
BP
CY
B5A
CY
P11A
1
CY
P11B
1
CY
P11B
2
CY
P17A
1
CY
P19A
1
CY
P1A
1
CY
P1A
2
CY
P1B
1
CY
P20A
1
CY
P21A
2
CY
P24A
1
CY
P26A
1
CY
P26B
1
CY
P26C
1
CY
P27A
1
CY
P27B
1
CY
P27C
1
CY
P2A
13
CY
P2A
6
CY
P2A
7
CY
P2B
6
CY
P2C
18
CY
P2C
19
CY
P2C
8
CY
P2C
9
CY
P2D
6
CY
P2E
1
CY
P2F
1
CY
P2J2
CY
P2R
1
CY
P2S
1
CY
P2U
1
CY
P2W
1
CY
P39A
1
CY
P3A
4
CY
P3A
43
CY
P3A
5
CY
P3A
7
CY
P46A
1
CY
P4A
22;CY
P4A
11
CY
P4B
1
CY
P4F
11
CY
P4F
12
CY
P4F
2
CY
P4F
22
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
AK
R1C
3
AK
R1C
4
AK
R1C
L1
AK
R1C
L2
AK
R1D
1
AK
R7A
2
AK
R7A
3
ALD
H16A
1
ALD
H18A
1
ALD
H1A
1
ALD
H1A
2
ALD
H1A
3
ALD
H1B
1
ALD
H1L1
ALD
H2
ALD
H3A
1
ALD
H3A
2
ALD
H3B
1
ALD
H3B
2
ALD
H4A
1
ALD
H5A
1
ALD
H6A
1
ALD
H7A
1
ALD
H8A
1
ALD
H9A
1
AO
C2
AO
C3
AO
F1
AO
F2
AO
X1
AQ
P1
AQ
P7
AQ
P9
AR
NT
AR
NT2
AS
3MT
ATP
6V0C
ATP
7A
ATP
7B
BA
AT
BC
HE
BLM
H
CB
R1
CB
R3
CB
R4
CE
S1
CE
S2
CE
S3
CE
S4
CE
S7
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
AA
DA
C
AA
NA
T
AB
CA
1
AB
CA
2
AB
CA
3
AB
CA
4
AB
CA
7
AB
CA
8
AB
CB
1
AB
CB
10
AB
CB
11
AB
CB
4
AB
CB
5
AB
CB
6
AB
CB
7
AB
CB
8
AB
CB
9
AB
CC
1
AB
CC
10
AB
CC
11
AB
CC
12
AB
CC
2
AB
CC
3
AB
CC
4
AB
CC
5
AB
CC
6
AB
CC
8
AB
CC
9
AB
CD
4
AB
CG
2
AB
CG
8
AB
P1
AD
H1A
AD
H1B
AD
H1C
AD
H4
AD
H5
AD
H6
AD
H7
AD
HF
E1
AF
AR
3
AH
R
AH
RR
AIP
AK
R1A
1
AK
R1B
1
AK
R1B
10
AK
R1C
2;AK
R1C
1
Muqueuse coliqueNon PathologiqueInflammatoire
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
TP53
TPM
T
TRIP
11
TST
TXN
TXN
2
UG
T1A1
UG
T1A10
UG
T1A4
UG
T1A5
UG
T1A6
UG
T1A7
UG
T1A8
UG
T1A9
UG
T2A1
UG
T2A3
UG
T2B10
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
SLC
28A3
SLC
29A1
SLC
29A2
SLC
29A3
SLC
29A4
SLC
2A1
SLC
31A1
SLC
38A1
SLC
38A2
SLC
38A5
SLC
3A1
SLC
3A2
SLC
47A1
SLC
47A2
SLC
5A4
SLC
6A3
SLC
6A4
SLC
7A11
SLC
7A5
SLC
7A6
SLC
7A7
SLC
7A8
SLC
O1A
2
SLC
O1B
1
SLC
O1B
3
SLC
O1C
1
SLC
O2A
1
SLC
O2B
1
SLC
O3A
1
SLC
O4A
1
SLC
O4C
1
SLC
O5A
1
SLC
O6A
1
SP
R
STX
2
SU
LT1A1
SU
LT1A2
SU
LT1A3;S
ULT1A
4
SU
LT1B1
SU
LT1C2
SU
LT1C3
SU
LT1C4
SU
LT1E1
SU
LT2A1
SU
LT2B1
SU
LT4A1
SU
LT6B1
SU
OX
TAP
1
TAP
2
TBX
AS
1
THR
A
THR
B
UG
T2B11
UG
T2B15
UG
T2B17
UG
T2B28
UG
T2B4
UG
T2B7
UG
T3A1
UG
T3A2
UG
T8
VD
AC
2
VD
AC
3
VD
R
XD
H
TP53
TPM
T
TRIP
11
TST
TXN
TXN
2
UG
T1A1
UG
T1A10
UG
T1A4
UG
T1A5
UG
T1A6
UG
T1A7
UG
T1A8
UG
T1A9
UG
T2A1
UG
T2A3
UG
T2B10
UG
T2B11
UG
T2B15
UG
T2B17
UG
T2B28
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
PA
OX
PN
MT
PO
N1
PO
N2
PO
N3
PO
R
PP
AR
A
PP
AR
D
PP
AR
G
PP
AR
GC
1A
PP
AR
GC
1B
PP
RC
1
PTG
ES
3
PTG
IS
RA
RA
RA
RB
RA
RG
RB
P1
RB
P2
RX
RA
RX
RB
RX
RG
SLC
10A1
SLC
10A2
SLC
15A1
SLC
15A2
SLC
16A1
SLC
18A2
SLC
19A1
SLC
19A2
SLC
19A3
SLC
1A1
SLC
1A2
SLC
1A3
SLC
1A6
SLC
1A7
SLC
22A1
SLC
22A11
SLC
22A12
SLC
22A16
SLC
22A2
SLC
22A3
SLC
22A4
SLC
22A5
SLC
22A6
SLC
22A7
SLC
22A8
SLC
22A9
SLC
25A13
SLC
28A1
SLC
28A2
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
HIF
1A
HIF
3A
HN
F4A
HN
MT
HS
D17B
10
HS
P90A
A1
INM
T
KC
NA
B1
KC
NA
B2
KC
NA
B3
KC
NK
9
KE
AP
1
MA
OA
MA
OB
MG
ST1
MG
ST2
MG
ST3
MP
ST
MT1A
MT1B
MT1F
MT1H
MT1M
MT1X
MT2A
MT3
MT4
MTH
FR
MV
P
NA
T1
NA
T2
NA
T5
NC
OA
1
NC
OA
2
NC
OA
3
NC
OR
1
NC
OR
2
NF
E2L2
NN
MT
NQ
O1
NQ
O2
NR
0B2
NR
1H2
NR
1H3
NR
1H4
NR
1I2
NR
1I3
NR
3C1
NR
3C2
NR
5A2
GS
TT2B;G
ST
T2
CY
P11A
1
CY
P11B
1
CY
P11B
2
CY
P17A
1
CY
P19A
1
CY
P20A
1
CY
P21A
2
CY
P24A
1
CY
P26A
1
CY
P26B
1
CY
P26C
1
CY
P27A
1
CY
P27B
1
CY
P27C
1
CY
P2A
13
CY
P2C
18
CY
P2C
19
CY
P39A
1
CY
P3A
43
CY
P46A
1
CY
P4A
22;CY
P4A
11
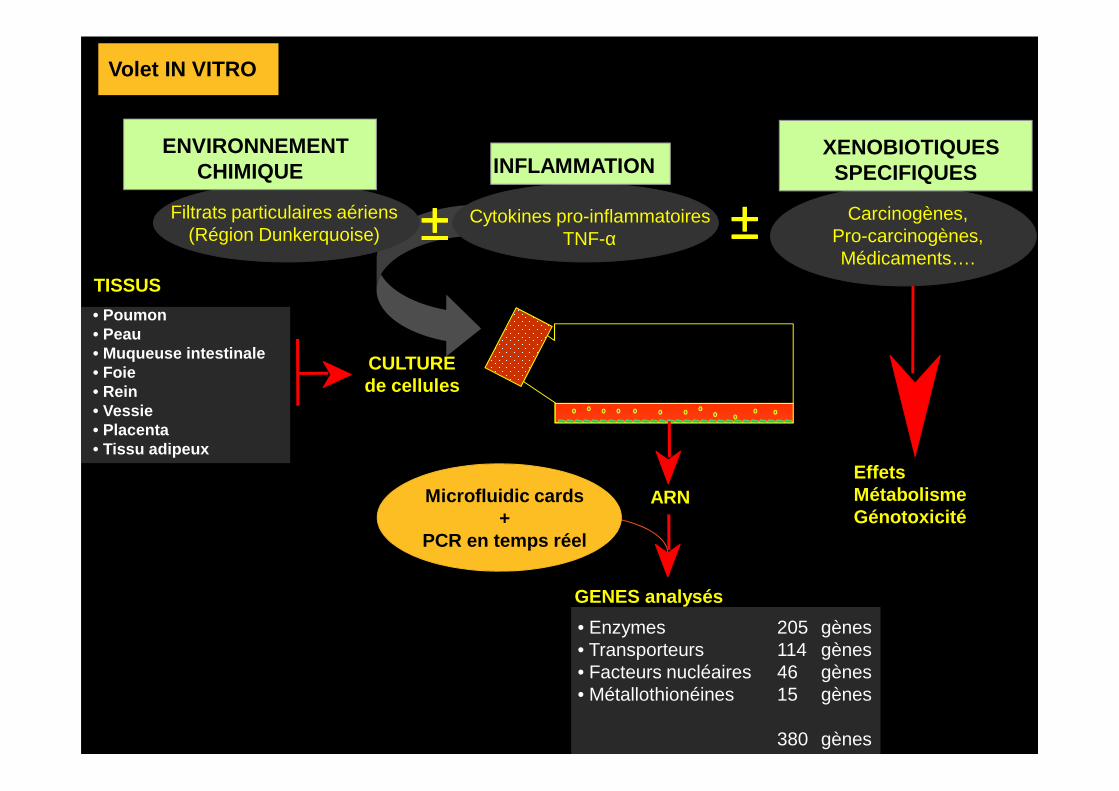
Volet IN VITRO
TISSUS
• Poumon• Peau• Muqueuse intestinale• Foie• Rein
CULTUREde cellules
Filtrats particulaires aériens(Région Dunkerquoise)
Cytokines pro-inflammatoiresTNF-α
INFLAMMATIONENVIRONNEMENT
CHIMIQUE
±±±±
Volet IN VITRO
Carcinogènes, Pro-carcinogènes, Médicaments….
XENOBIOTIQUESSPECIFIQUES
±±±±
GENES analysés
• Enzymes 205 gènes• Transporteurs 114 gènes• Facteurs nucléaires 46 gènes• Métallothionéines 15 gènes
380 gènes
Microfluidic cards+
PCR en temps réel
• Rein• Vessie• Placenta• Tissu adipeux
de cellules
ARNEffetsMétabolismeGénotoxicité
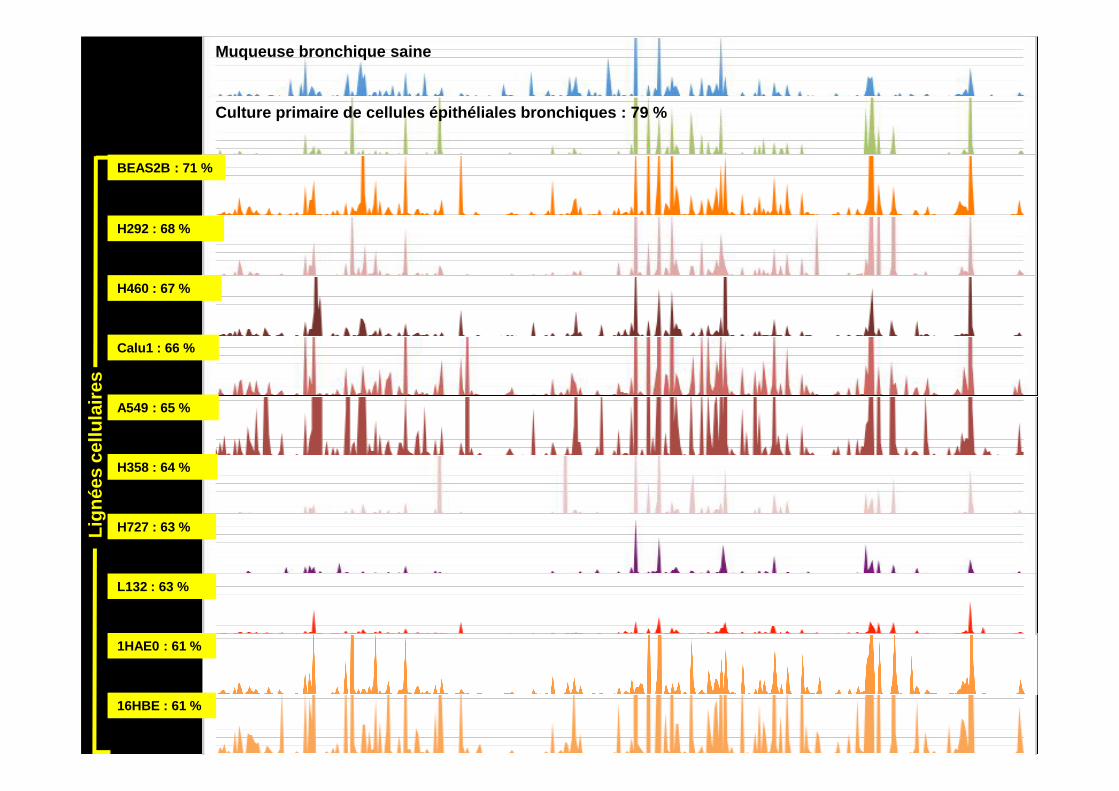
Muqueuse bronchique saine
Culture primaire de cellules épithéliales bronchiqu es : 79 %
BEAS2B : 71 %
Calu1 : 66 %
H292 : 68 %
H460 : 67 %
Lign
ées
cellu
laire
s
16HBE : 61 %
1HAE0 : 61 %
A549 : 65 %
H358 : 64 %
H727 : 63 %
L132 : 63 %
Lign
ées
cellu
laire
s
AK
R6A
9
MA
OB
FM
O2
DH
RS
2
AO
X1
CY
P8B
1
CY
P3A
4
CY
P2B
6
CY
P21
A2
CY
P4F
22
CY
P11
A1
CY
P2C
19
ALD
H3B
2
ALD
H1A
2
ALD
H3A
1
ALD
H8A
1
CY
P2W
1
CY
P1B
1
CY
P1A
10,1
1
10
100
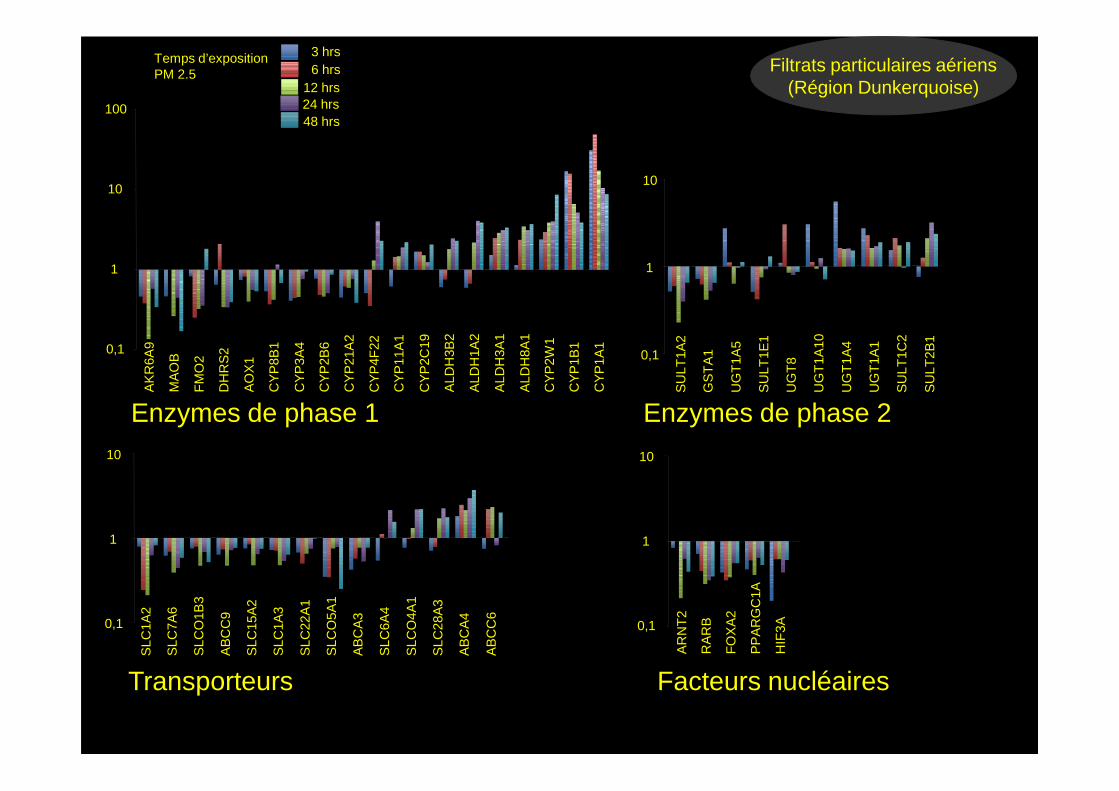
Temps d’expositionPM 2.5
3 hrs6 hrs
12 hrs24 hrs48 hrs
SU
LT1A
2
GS
TA
1
UG
T1A
5
SU
LT1E
1
UG
T8
UG
T1A
10
UG
T1A
4
UG
T1A
1
SU
LT1C
2
SU
LT2B
1
0,1
1
10
Filtrats particulaires aériens(Région Dunkerquoise)
Enzymes de phase 1
Transporteurs Facteurs nucléaires
Enzymes de phase 2
SLC
1A2
SLC
7A6
SLC
O1B
3
AB
CC
9
SLC
15A
2
SLC
1A3
SLC
22A
1
SLC
O5A
1
AB
CA
3
SLC
6A4
SLC
O4A
1
SLC
28A
3
AB
CA
4
AB
CC
6
0,1
1
10
AR
NT
2
RA
RB
FO
XA
2
PP
AR
GC
1A
HIF
3A0,1
1
10
Enzymes de phase 1
KC
NA
B1
CY
P7A
1C
YP
2A7
AD
H4
CE
S7
XD
H
CY
P4Z
1
CY
P21
A2
CY
P27
B1
MA
OA
CY
P3A
5
CY
P7B
1
ALD
H1A
2
CY
P2B
6
KC
NA
B2
PO
N3
AO
X1
ALD
H3B
1
CY
P2R
1
NQ
O1
HS
D17
B10
SU
OX
CY
P1B
1
FM
O5
ALD
H4A
1
MG
ST
1
ALD
H1A
1
CY
P1A
1
CY
P2C
18
CY
P4F
12
FM
O2
CY
P4F
11
CE
S2
EP
HX
2
EP
HX
1
AK
R1B
10
DH
RS
2
DH
RS
9
FM
O3
ALD
H1L
1
ALD
H3A
1
AB
P1
CY
P4B
1C
YP
2W1
AD
H7
MA
OB
CY
P4F
2
AK
R1C
L1
AK
R7L
CY
P4F
22
0,001
0,01
0,1
1
10
100
10
100
10
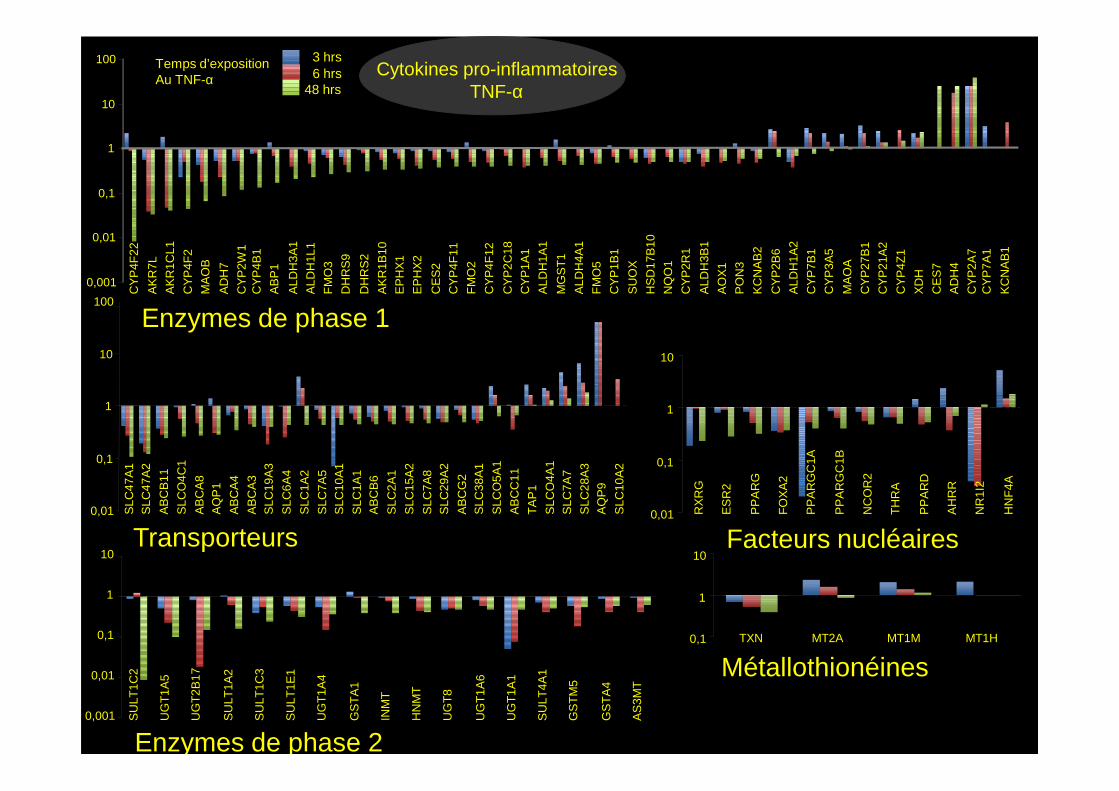
Temps d’expositionAu TNF-α
3 hrs6 hrs
48 hrsCytokines pro-inflammatoires
TNF-α
SLC
10A
2
AQ
P9
SLC
28A
3
SLC
7A7
SLC
O4A
1
TA
P1
AB
CC
11
SLC
O5A
1
SLC
38A
1A
BC
G2
SLC
29A
2S
LC7A
8
SLC
15A
2
SLC
2A1
AB
CB
6S
LC1A
1
SLC
10A
1S
LC7A
5
SLC
1A2
SLC
6A4
SLC
19A
3A
BC
A3
AB
CA
4
AQ
P1
AB
CA
8
SLC
O4C
1
AB
CB
11
SLC
47A
2S
LC47
A1
0,01
0,1
1
HN
F4A
NR
1I2
AH
RR
PP
AR
D
TH
RA
NC
OR
2
PP
AR
GC
1B
PP
AR
GC
1A
FO
XA
2
PP
AR
G
ES
R2
RX
RG
0,01
0,1
1
MT1HMT1MMT2ATXN0,1
1
10
AS
3MT
GS
TA
4
GS
TM
5
SU
LT4A
1
UG
T1A
1
UG
T1A
6
UG
T8
HN
MT
INM
T
GS
TA
1
UG
T1A
4
SU
LT1E
1
SU
LT1C
3
SU
LT1A
2
UG
T2B
17
UG
T1A
5
SU
LT1C
2
0,001
0,01
0,1
1
10Transporteurs Facteurs nucléaires
Enzymes de phase 2
Métallothionéines
CY
P1A
1
CY
P1B
1
KC
NA
B1
ALD
H1A
2
CY
P4F
12
ALD
H1A
3
ALD
H3A
1
DH
RS
9
CY
P4F
22
CY
P2C
9
CE
S3
AK
R7A
2
CB
R1
ALD
H3B
2
CY
P3A
4
DH
RS
2
CY
P2U
1
CY
P21
A2
CY
P26
B1
0,1
1
10
100
1000
UGT1A1
UG
T1A
5
UG
T1A
4
UG
T1A
6
SU
LT1A
2
SU
LT2B
1
GS
TM
5
NA
T1
GG
T1
NN
MT
SU
LT1E
1
GS
TO
2
GS
TA
1
MG
ST
1
SU
LT1C
2
0,1
1
10
100
UG
T1A
1
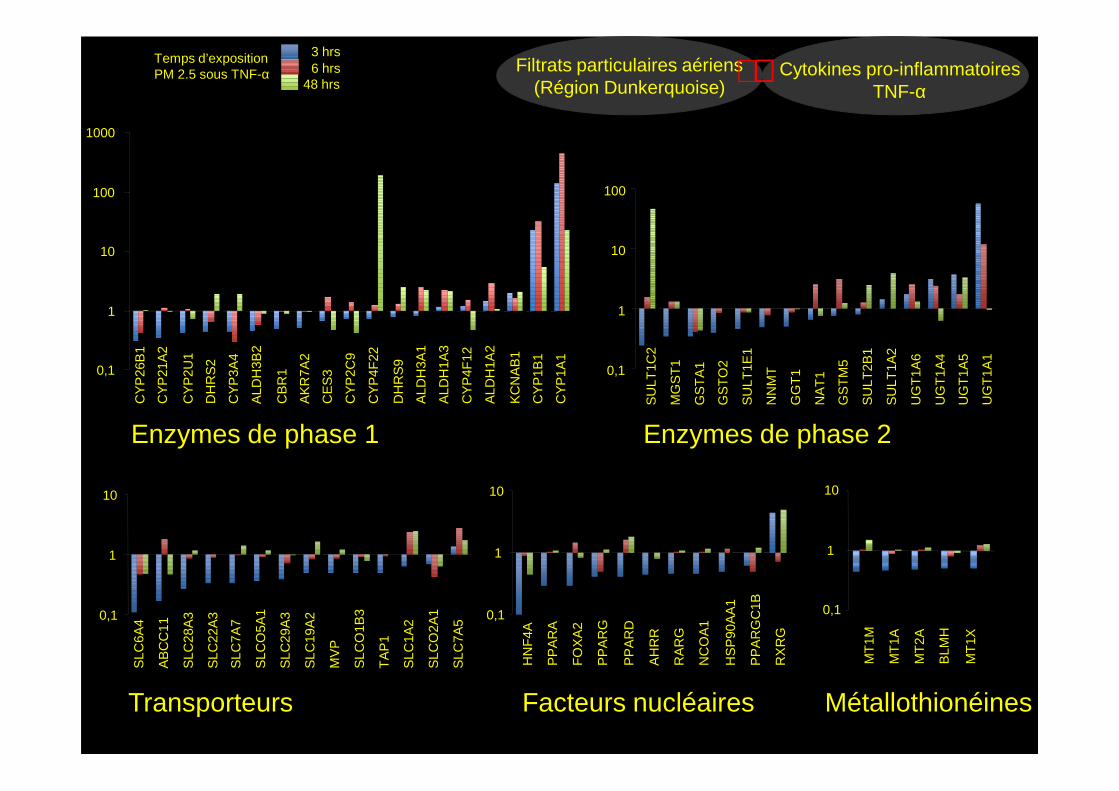
Temps d’expositionPM 2.5 sous TNF-α
3 hrs6 hrs
48 hrsCytokines pro-inflammatoires
TNF-αFiltrats particulaires aériens
(Région Dunkerquoise)++++
Enzymes de phase 1
Transporteurs Facteurs nucléaires
Enzymes de phase 2
Métallothionéines
CY
P1A
1
CY
P1B
1
KC
NA
B1
ALD
H1A
2
CY
P4F
12
ALD
H1A
3
ALD
H3A
1
DH
RS
9
CY
P4F
22
CY
P2C
9
CE
S3
AK
R7A
2
CB
R1
ALD
H3B
2
CY
P3A
4
DH
RS
2
CY
P2U
1
CY
P21
A2
CY
P26
B1
UG
T1A
5
UG
T1A
4
UG
T1A
6
SU
LT1A
2
SU
LT2B
1
GS
TM
5
NA
T1
GG
T1
NN
MT
SU
LT1E
1
GS
TO
2
GS
TA
1
MG
ST
1
SU
LT1C
2
UG
T1A
1
SLC
7A5
SLC
O2A
1
SLC
1A2
TA
P1
SLC
O1B
3
MV
P
SLC
19A
2
SLC
29A
3
SLC
O5A
1
SLC
7A7
SLC
22A
3
SLC
28A
3
AB
CC
11
SLC
6A40,1
1
10
RX
RG
PP
AR
GC
1B
HS
P90
AA
1
NC
OA
1
RA
RG
AH
RR
PP
AR
D
PP
AR
G
FO
XA
2
PP
AR
A
HN
F4A
0,1
1
10
0,1
1
10
MT
1X
BLM
H
MT
2A
MT
1A
MT
1M
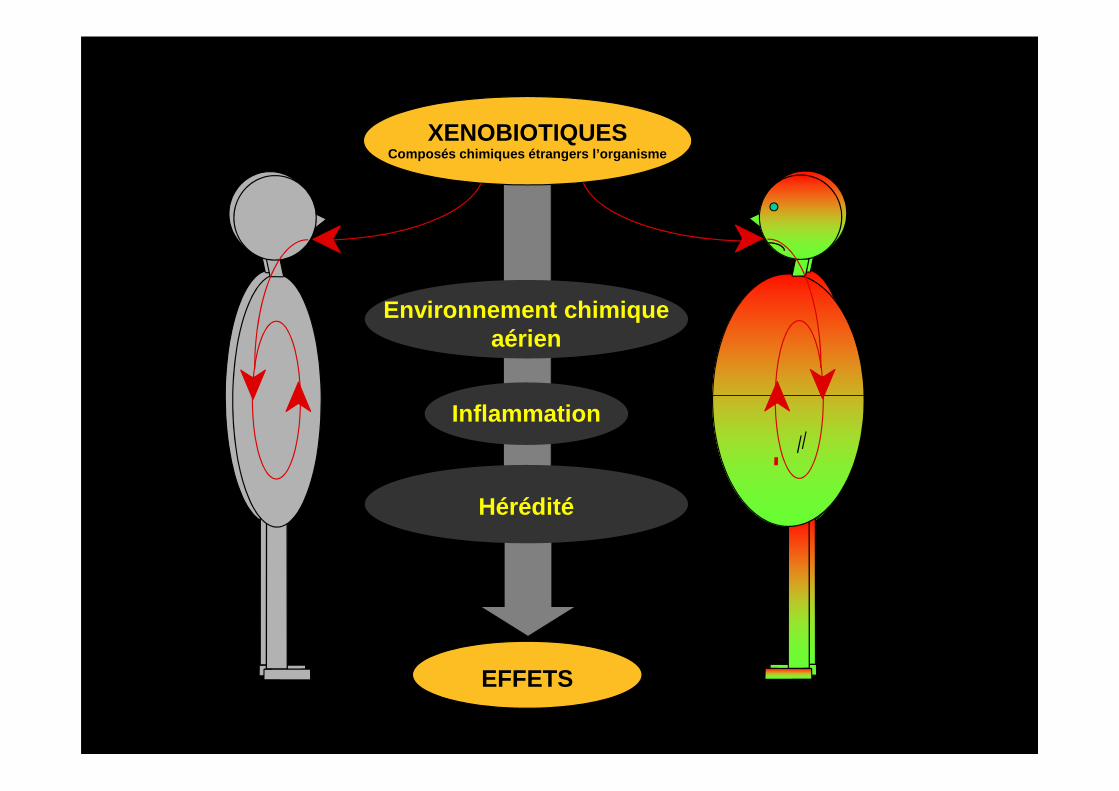
XENOBIOTIQUESComposés chimiques étrangers l’organisme
Environnement chimiqueaérien
EFFETS
Inflammation
Hérédité
Rapport sur les implications éthiques, sociales, lé gales des tests génétiquesSollicité par la commission de l’Union Européenne – Rendu publique en Mai 2004
25 Recommandations
19. PHARMACOGENETIQUELe terme « pharmacogénétique » décrit l'étude des différences de réactions aux médicaments (efficacitéou effets indésirables) qu'ont les individus, directement liées aux variations dans les séquences d'ADN etdans les différences de séquence de protéine, de structure ou d'expression génique, elles-mêmesconséquence directe de telles variations de l'ADN. L'objet principal de la pharmacogénétique est depermettre la délivrance de médicaments aux patients, qui sont le plus à même d'en tirer profit et le moinssusceptibles d'en subir des effets indésirables. Bien que la pharmacogénétique soit encore, à ce jour,dans une phase essentiellement exploratoire, un accroissement de ses applications dans les soins desanté est attendue et des mesures appropriées devraient être prises dans la perspective de cetteévolution.évolution.
Recommandation 19
a. Les autorités sanitaires nationales devraient jouer un rôle plus actif et encourager le développement dela pharmacogénétique: en prévoyant des incitants particuliers pour permettre le développement de testspharmacogénétiques et d'une thérapeutique associée, cliniquement souhaitables mais économiquementnon viables ; en accroissant, dans ce domaine, les possibilités de coopération entre industrie, patients etmonde universitaire;
b. Un cadre juridique, réglementaire et de politique de soins de santé harmonisé, adapté à lapharmacogénétique devrait être développé au niveau de l'UE, qui prenne en compte la recherche, lamise au point de thérapies et la pratique clinique.
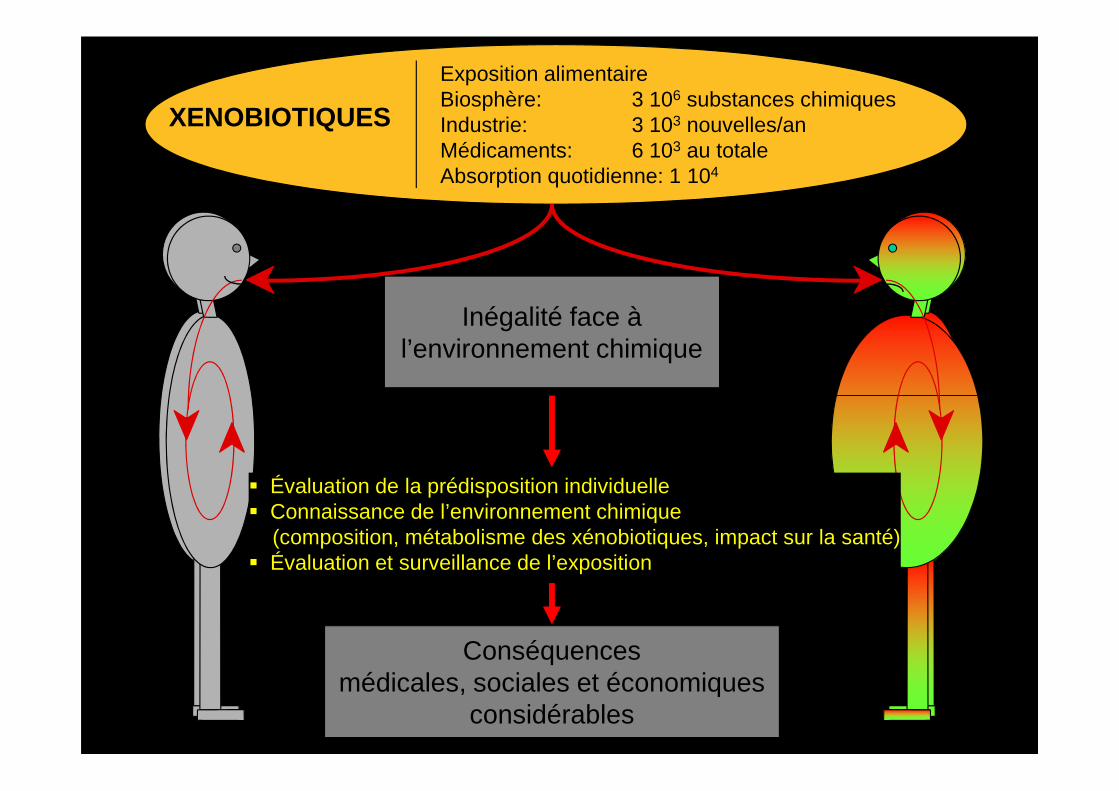
XENOBIOTIQUES
Exposition alimentaireBiosphère: 3 106 substances chimiquesIndustrie: 3 103 nouvelles/anMédicaments: 6 103 au totaleAbsorption quotidienne: 1 104
Inégalité face à l’environnement chimique
Conséquences médicales, sociales et économiques
considérables
� Évaluation de la prédisposition individuelle� Connaissance de l’environnement chimique
(composition, métabolisme des xénobiotiques, impact sur la santé)� Évaluation et surveillance de l’exposition
OBJECTIFS DE LA RECHERCHE EN
PHARMACOGENETIQUE
1 Identification des variations de réponse aux médicaments
d'origine génétique
2 Etude de leur mécanisme moléculaire2 Etude de leur mécanisme moléculaire
3 Evaluation de leur importance clinique
4 Développement de méthodes d'identification des individus
à risque Avant exposition ++++
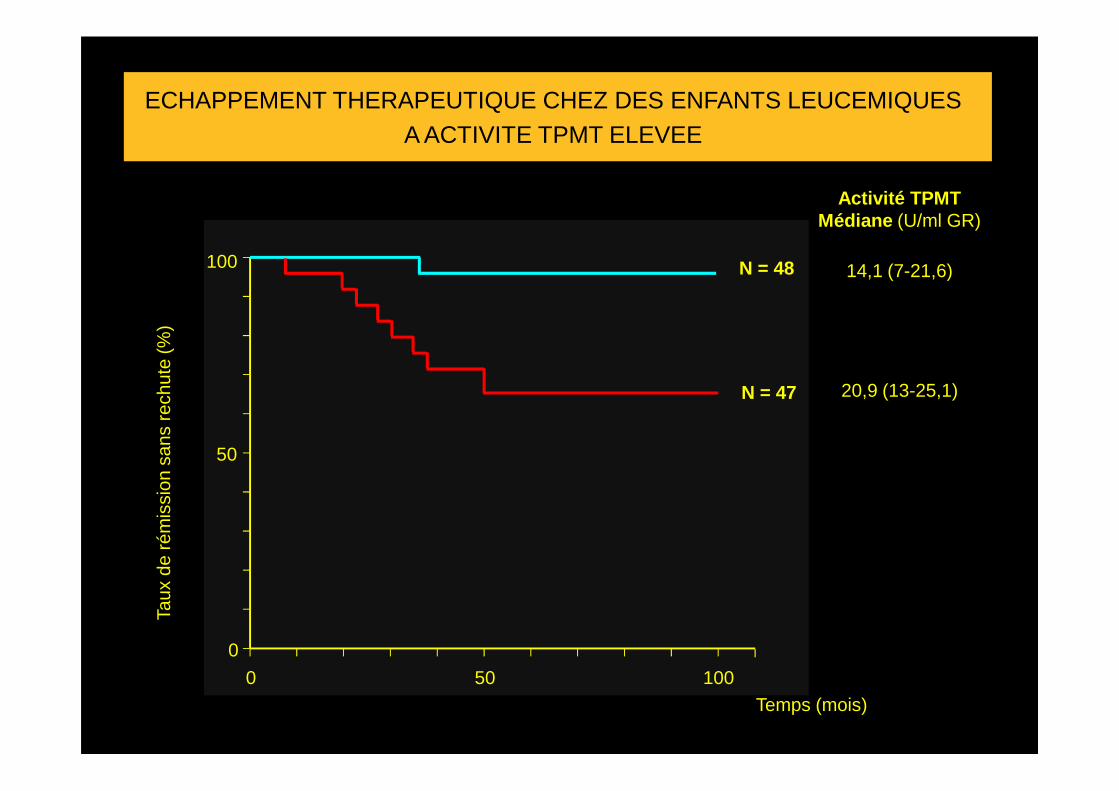
ECHAPPEMENT THERAPEUTIQUE CHEZ DES ENFANTS LEUCEMIQUESA ACTIVITE TPMT ELEVEE
Taux
de
rém
issi
on s
ans
rech
ute
(%)
100
Activité TPMTMédiane (U/ml GR)
14,1 (7-21,6)
20,9 (13-25,1)
N = 48
N = 47
Taux
de
rém
issi
on s
ans
rech
ute
(%)
Temps (mois)
0
50
0 50 100
20,9 (13-25,1)N = 47
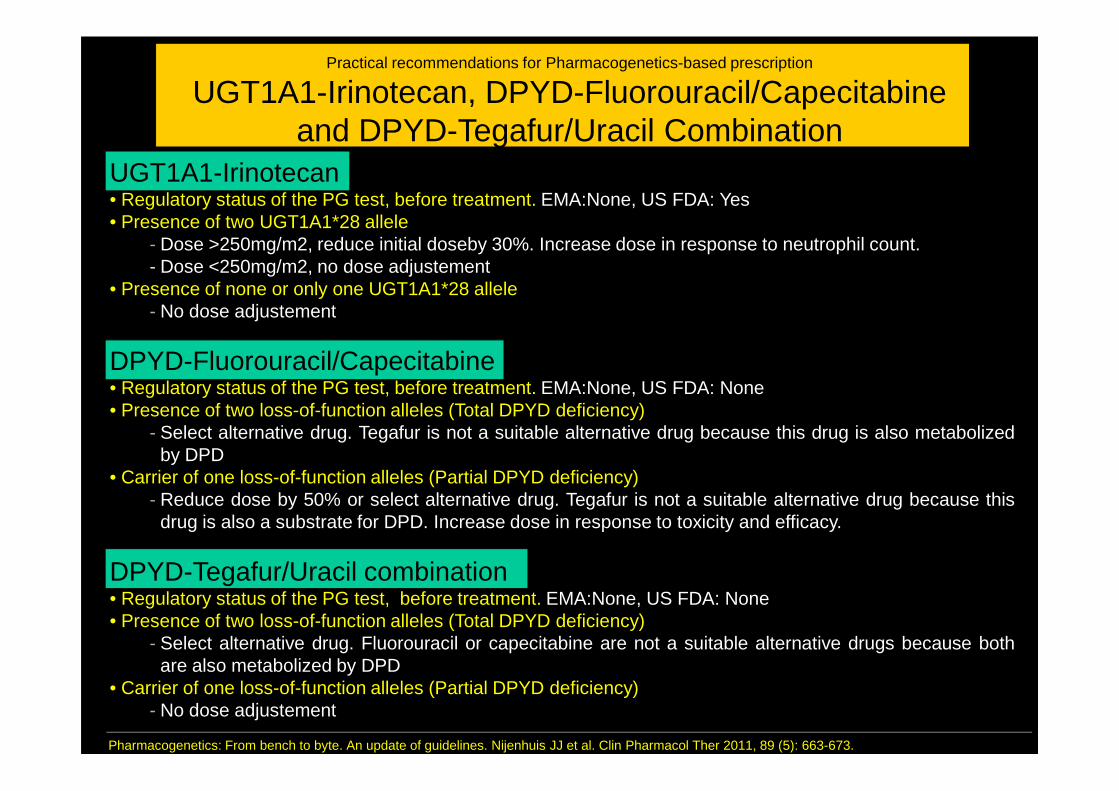
Practical recommendations for Pharmacogenetics-based prescription
UGT1A1-Irinotecan, DPYD-Fluorouracil/Capecitabineand DPYD-Tegafur/Uracil Combination
UGT1A1-Irinotecan• Regulatory status of the PG test, before treatment. EMA:None, US FDA: Yes• Presence of two UGT1A1*28 allele
- Dose >250mg/m2, reduce initial doseby 30%. Increase dose in response to neutrophil count.- Dose <250mg/m2, no dose adjustement
• Presence of none or only one UGT1A1*28 allele- No dose adjustement
DPYD-Fluorouracil/Capecitabine• Regulatory status of the PG test, before treatment. EMA:None, US FDA: None• Regulatory status of the PG test, before treatment. EMA:None, US FDA: None• Presence of two loss-of-function alleles (Total DPYD deficiency)
- Select alternative drug. Tegafur is not a suitable alternative drug because this drug is also metabolizedby DPD
• Carrier of one loss-of-function alleles (Partial DPYD deficiency)- Reduce dose by 50% or select alternative drug. Tegafur is not a suitable alternative drug because this
drug is also a substrate for DPD. Increase dose in response to toxicity and efficacy.
DPYD-Tegafur/Uracil combination• Regulatory status of the PG test, before treatment. EMA:None, US FDA: None• Presence of two loss-of-function alleles (Total DPYD deficiency)
- Select alternative drug. Fluorouracil or capecitabine are not a suitable alternative drugs because bothare also metabolized by DPD
• Carrier of one loss-of-function alleles (Partial DPYD deficiency)- No dose adjustement
Pharmacogenetics: From bench to byte. An update of guidelines. Nijenhuis JJ et al. Clin Pharmacol Ther 2011, 89 (5): 663-673.
Royal Dutch Association for the Advancement of Pharmacy, Pharmacogenetic Working Group
Pharmacogenetic Based Therapeutic (dose) Recommandations
Drug(Gene)
Tamoxifen(CYP2D6)
Subjects(N)
5020
Genotype or Phenotype
Poor
Intermediate
Ultra rapid
Level of evidence(0 → 4)
4
4
4
Clinical relevance(A → F)
E
E
A
Therapeutic (dose) recommendation
Increased risk for relapse of breast cancer. Consider aromatase inhibitor for postmenopausal women.
Increased risk for relapse of breast cancer. Consider aromatase inhibitor for postmenopausal women.
No
Irinotecan(UGT1A1)
Fluorouracil/Capecitabine
(DPYD)
Pharmacogenetics: From bench to byte. An update of guidelines. Nijenhuis JJ et al. Clin Pharmacol Ther. May 2011, 89 (5): 663-673.
3883
3733
*1/*28
*28/*28
Poor
Intermediate
4
4
3
3
F
E
F
F
No
Dose > 250 mg/m2: reduce initial dose by 30 %. Increase dose in response to neutrophil count.Dose < 250 mg/m2: no dose adjustement
Select alternative drug. Tegafur is not a suitablealternative drug because this drug is alsometabolized by DPD
Reduce dose by 50% or select alternative drug.Tegafur is not a suitable alternative drug because thisdrug is also a substrate for DPD. Increase dose inresponse to toxicity and efficacy.
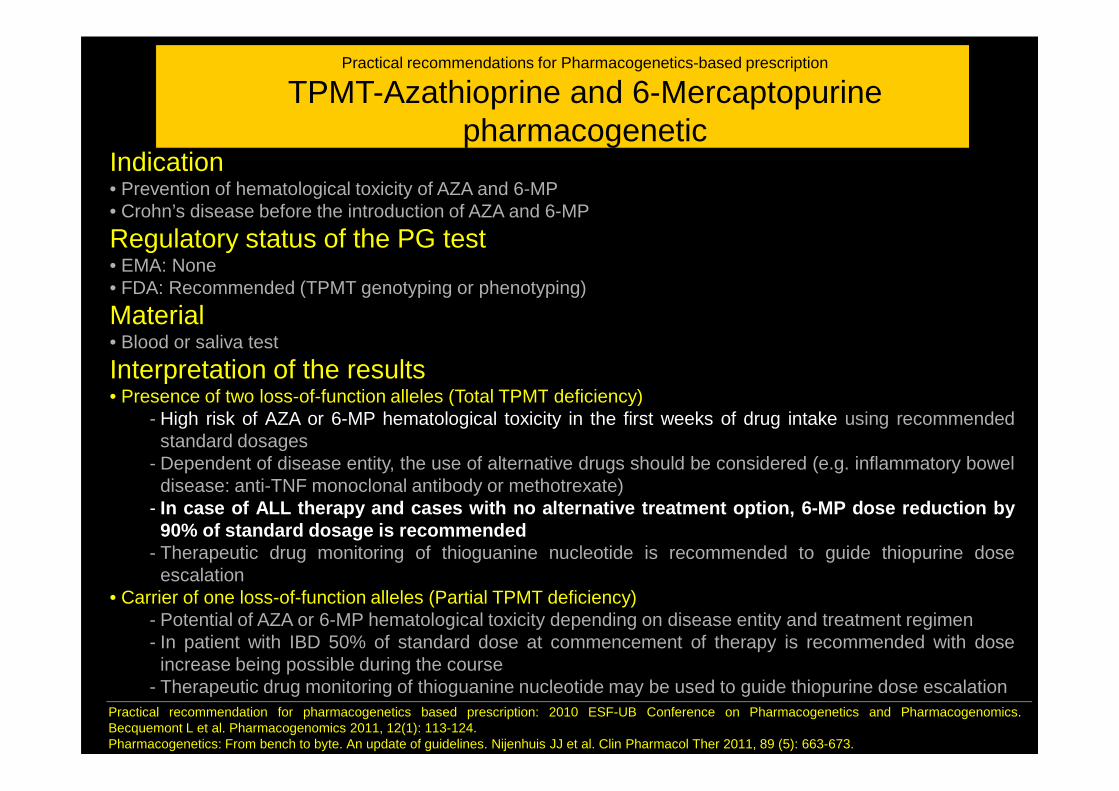
Practical recommendations for Pharmacogenetics-based prescription
TPMT-Azathioprine and 6-Mercaptopurinepharmacogenetic
Indication• Prevention of hematological toxicity of AZA and 6-MP• Crohn’s disease before the introduction of AZA and 6-MP
Regulatory status of the PG test• EMA: None• FDA: Recommended (TPMT genotyping or phenotyping)
Material• Blood or saliva test
Interpretation of the results• Presence of two loss-of-function alleles (Total TPMT deficiency)• Presence of two loss-of-function alleles (Total TPMT deficiency)
- High risk of AZA or 6-MP hematological toxicity in the first weeks of drug intake using recommendedstandard dosages
- Dependent of disease entity, the use of alternative drugs should be considered (e.g. inflammatory boweldisease: anti-TNF monoclonal antibody or methotrexate)
- In case of ALL therapy and cases with no alternative treatmen t option, 6-MP dose reduction by90% of standard dosage is recommended
- Therapeutic drug monitoring of thioguanine nucleotide is recommended to guide thiopurine doseescalation
• Carrier of one loss-of-function alleles (Partial TPMT deficiency)- Potential of AZA or 6-MP hematological toxicity depending on disease entity and treatment regimen- In patient with IBD 50% of standard dose at commencement of therapy is recommended with dose
increase being possible during the course- Therapeutic drug monitoring of thioguanine nucleotide may be used to guide thiopurine dose escalation
Practical recommendation for pharmacogenetics based prescription: 2010 ESF-UB Conference on Pharmacogenetics and Pharmacogenomics.Becquemont L et al. Pharmacogenomics 2011, 12(1): 113-124.Pharmacogenetics: From bench to byte. An update of guidelines. Nijenhuis JJ et al. Clin Pharmacol Ther 2011, 89 (5): 663-673.