Evaluation médicale et dépistage des complications chez...
36
Evaluation médicale et dépistage des complications chez les enfants en surpoids dans le modèle Suisse de thérapie multidisciplinaire D. l' Allemand Endocrinologie/Diabétologie Pédiatrique, Hôpital des Enfants de l’Est de la Suisse, Saint-Gall Groupe de Travail Obésité, SSP & akj, Vice-Présidente & Commission d'évaluation KIDSSTEP, OFSP 2009-2014 Journée de formation, Sion, 30-10-2014 Ostschweizer Kinderspital
Transcript of Evaluation médicale et dépistage des complications chez...

Evaluation médicale et dépistage des complications chez
les enfants en surpoids dans le modèle Suisse de thérapie multidisciplinaire
D. l' Allemand
Endocrinologie/Diabétologie Pédiatrique, Hôpital des Enfants de l’Est de la Suisse, Saint-Gall
Groupe de Travail Obésité, SSP & akj, Vice-Présidente &
Commission d'évaluation KIDSSTEP, OFSP 2009-2014
Journée de formation, Sion, 30-10-2014
Ostschweizer Kinderspital

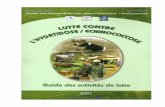
I) 6 mois thérapie individuelle MSIT par méd. de
famille / pédiatre (<6*diététique, 2*physioth.)
(+) 1(-2) ans PMG:
âge 8-18 ans
(mini-PMG:
âge 4-8 ans, Tarmed)
(+) II) = 3-6 mois MSIT certifié avec
env. 6*psychothérapie,
env. 9*physiothérapie,
env. 6*conseils diététiques
(+) III) = Répétition de II) IV) (1-) 5 ans de suivi ≈ bitrimestriel
(+)IMC >p. 99.5, IMC, rapport tour de taille / taille , comorbidité ou problématique psychosociale
Obésité: percentile de l‘IMC >97 , e.a.
Normal: percentile de l‘IMC <90
Surpoids: percentile de l‘IMC >90 <97
Thérapie Thérapie, si
complications
Prévention ciblée
Augmentation de
l‘IMC <6 ans /
fortement en peu
de temps
Sans
complications
(+) Thérapie hospitalière
(planifiée)
(+) Chirurgie bariatrique à
croissance terminée
www.akj-ch.ch ; www.swiss-paediatrics.org; Bull.méd suisse 2014;95(44):1640-1
Examen médical préalable, selon les recommendations (Paediatrica 2006),
y inclus la thérapie de complications somatiques / psychiques

The general practitioner /pediatrician and the
obese society
1. Childhood obesity is a chronic disease
2. > 75% persist into adulthood
3. The whole family is concerned
4. Obesogenic environment 50% & genetic risks 50%
5. Couch Potatoes
6. Unrealistic expectations hamper readiness for lifestyle changes
7. Very long-term treatment required
l‘Allemand
Stern 1997

BMI
Fat
Lean (Muscle)
Mass
Prevalence of Overweight as Defined by BMI in
6 – 12- Year Old Swiss Children & in Adults
Aeberli, 2008, Murer2012 ETH Zürich
BMI
Fat
Lean (Muscle)
Mass
BMI decrease by 3.8%
Fat mass stable
Children <age 18: 2002 2007 2012 men women
Overweight & OB: 18% 15.2% 18.9% 39.2 22.7%
Obese: 4% 3.1% 7.1% 8.3 7.8%
30.10.2014
Fat mass abnormal if
>20-25% in men
>30% in women

3 Definitions de l’obésité pédiatrique en Suisse*
1. IMC (kg / m2 > P.97) (www.swiss-paediatrics.org, Jenni et al, Paediatrica 2011, 22:9-11)
WHO growth standards 0 – 5 y, 2007;
NCHS /US growth references 5-18 y, 1977
2. pourcentage de graisse corporelle totale élevé (> 25 %
pour les garçons et >30% pour les mesuré par BIA
(Bioimpedance), plis cutanés ou DEXA. (Boot et al., Am. J clin Nutr. 66:232, 1997)
3. Tour de taille >2 SD ou Tour de taille taille > 0.5 (Fredriks et al. Eur J Pediatr 164: 216–222, 2005)
*l‘Allemand & Farpour-Lambert, Paediatrica 17:14-18,2006

Therapy inclusion criteria: obesity or overweight +co-morbidity
Obesity>P.97
Overweight >P.90
Extreme Obesity >P.99.5
------------------------
--
Boys Girls
-----------------------
----
SDSLMS≈+1.9 SDSLMS≈+1.9
www.swiss-paediatrics.org; WHO 2007/ NCHS 1977

4.9.2009
Waist circumference is a simple screening tool to assess overweight-related co-
morbidities° Waist circumference is associated with:
•Hypertension and number of risk factors (present study)
•Insulin resistence in children (Lee SJ, J Pediatr148:188, 2006)
•Coronary events in adults of different ethnic origins (Yusuf S, Lancet 366:1640, 2005)
Waist/Height-Ratio Waist Screening cut-offs female male
< 0.5 children (about 11y.)* 80 cm 90 cm
Adults 88 cm 102 cm °Maffeis J Pediatr,152:207, 2008; *Fredriks Eur J Pediatr 164:216,2005) °Blüher, l'Allemand et al. JCEM 98:3384, 2013;

30.10.2014 8
Weight for Height in tall >p.97 or
short children <P.3
Girls Boys
WHO / US-NCIHS

Anamnèse personnelle et familiale
• comprenant activité physique et sport, modes de déplacement, loisirs, utilisation de la télévision et de l’ordinateurs, alimentation, sommeil, scolarité, facteurs psychosociaux, etc.)
• Mesure du poids – aussi des parents -!, de la taille, du tour de taille et des hanches (Tableaux.)
• Signes dysmorphiques
• Problèmes orthopédiques aigüs ou chroniques: hanches, genoux, pes planus, genu valgum, hyperlordose, etc).
• Force musculaire, coordination.
• Status psychologique (anxiété, dépression, etc.)
• Signes cutanés (acanthosis nicgricans, hirsutisme, vergetures)
• Status cardio-respiratoire, pouls et pression artérielle
• Stade pubertaire

n
TO T1 T2
591 87 160
Father Normal % 23.2 18.9 19.5
Father Overweight % 44.0 47.2 44.1
Father OB 1° % 23.4 24.5 25.4
Father OB 2° % 6.9 5.7 6.8
Father morbid OB 3° % 2.5 3.8 4.2
TO T1 T2
n 638 123 202
Mother Normal % 31.0 37.4 36.1
Mother Overweight % 32.3 26.0 28.7
Mother OB 1° % 23.4 20.3 21.8
Mother OB 2° % 7.1 11.4 8.9
Mother morbid OB 3° % 6.1 4.9 4.5
Most parents are obese and don’t change weight in pediatric programs
10
-Only 31% of mothers and 23% of fathers had a normal BMI, but 55 % think, they are normal weight.
-BMI of mothers (r=0.3, p< 0.0001), but not of fathers, was correlated with BMISDS of the child before & after therapy.
KIDSSTEP

Obésité – une maladie contagieuse!
• Sterile mice = lean
• Microbiote in «Western diet» => overweight mice
• Transplantation of western diet gut microbes=> fat tissue increases.
• =>beneficial effect of dietary fibres, remain lean
• => less OB in breastfed children,
• => more OB after early antibiotics

Genetic defects in weight regulation: Save energy!
Obesity
signals
Satiety
signals
Eating
Energie
NPY Anaboic
pathway
catabolic pathway
MSH
Sym-
pathi-
cus
Ghrelin,
PYY, GLP-1
Adapted from
Schwartz 2000
Amylin Pancreas

13
Motivation& incentive to eat
Taste and hedonism
Information on food as reward
The reward system: a target for appetite-regulating gut hormones
Suzanne Dickson, Sweden
GHrelin-Receptor

Continouous availability of sweet and fat food increases threshold of reward by eating
Reward trigger by implanted electrode regulated by switch:
1. Normal, chow=>rare
2. sweet and fat food => always demanded at increasingly higer doses, similar to cocaine, heroin
14 Kinny JP, Neuron 69, February 24, 2011

14 Jahre, P 75 15 J., P10 11 J., P25 Adipositas simplex Prader-Labhart-Willi- Laurence-Moon-Bardet-Biedl-
Syndrom Syndrom
Petite taille*,
Dysmorphies,
retard mental,
Hypotonie
musculaire
*taille cible
garcon
= (Taille père+
taille mere+13)
/2
…(fille ….-13)/2
Fanconi&Wallgreen 1972
P.50
Obésité & Syndromes

Genetics of Obesity
• ≈15% of early onset
extreme obesity can be explained by genetics
• KSR2 gene in obesity and severe insulin resistance, can be treated with Metformin
• Leptin deficiency can be treated with leptin
leptin deficiency
leptin receptor deficiency
prohormone convertase-1 def.
proopiomelanocortin def. (red hair)
melanocortin-4 rec.polymorphism
FTO[8]
GNPDA2[8]
NEGR1[8]
BDNF (hyperactivity)[8]
KSR2
SIM-1 (Autonomous dysfuntion)
SH2B1
BMIQ1
BMIQ2
BMIQ3
BMIQ4
BMIQ5
BMIQ6
INSIG2…

• Maladie chronique ou traumatisme avec immobilisation
(Rhumatisme, Spina bifida, …)
• Petite taille ou retard de croissance (syndrome de Cushing, hypothyroïdie),
• sans/avec retard mental, hypotonie musculaire (syndrome génétique p. ex. Prader-Labhart-Willi, Bardet-Biedl, pseudohypoparathyroïdie, Alström, M. Down, …).
• Et microcephalie (Cohen-Syndrom)
• Pathologie ou traumatisme SNC, altération visuelle (p. ex. Craniophanyngiome, autisme, TDAH (25%))
• Effets secondaires de médicaments (entre autres glucorticoïdes, Valproate, Phenothiazine, etc.)
Obesity in children with chronic diseases

Adulthood diseases in the obese child –
treatment necessary!
1.Arthrosis • Motor Coordination Deficit • Malarticulation (50-75%!)
2.Mental Health Diseases (30 -50%)
• Depression / emotional dis. • Hyperactivity / ADHS
3.Cardiovascular Diseases • Hypertension • Dyslipidemia
4.Liver Disease /Cirrhosis • Steatohepatitis
5.Diabetes • Glucose Intolerance • Insulin Resistance
6.Sleep Apnea • Neurocognitive Deficit
l‘Allemand
Ebbeling et al. Lancet 2002

Musculoskeletal system
• Consultation orthopédique, imagerie: hanches, genoux, pieds, dos, en cas de symptômes. P. ex. épiphysiolyse de la tête fémorale.
Children investigated for
orthopaedic problems
T0 T1 T2 T3 T0-T2-T3
longitudinal
η2 T2-T0
Total n 817 436 523 177 (n=157)
Any orthopaedic
pathology (%/total)
68.1 33.7 53.7 57.1 -
Total n 816 436 517 169
Genua valga (%/total) 46.5 25.0 41.1 39.0 F=3.5, p<.03 0.21 p=.028
Hip motility (%/total) 3.4 0.7 1.6 3.6 n.s.
Pes planus (%/total) 27.6 17.4 28.5 25.0 F=3.7, p<.05 0.26 p=.04
LWS
hyperlordosis(%/total)
35.4 15.4 28.6 22.5 n.s.

20
7.7%
6.6%
9.8%
7.0%
10.0%
30.0%
40.3%
17.3%
68.7%
46.0%
0% 50% 100%
EmotionaleProbl.
Verhaltensprobl.
Hyperaktivität
Probl. mitGleichaltrigen
Gesamtscore
Studien-Tn(N=605-686)
Normativessample(N=930)
Mental health status at T0 significantly predicted BMI-SDS change from T0 to T2
(Strenght and Difficulties SDQ-Fragebogen, Elternversion; Wörner, 2004
Mental Health in OB Children
Psychosocial Difficulties in 46% of Youth (SDQ) (General Adolescent Population 10.7%)

AD-EVA: Eating and health behaviour in children
before OB group therapy
Ardelt-Gattinger & Meindl, 2010
Girls >12 >>Boys (η2 =.10) n.s.
***
Dropout-Analyses: n.s.
*** ***
** p < .01
Predictor of
BMI-reduction

Recherche des co-morbidités et facteurs de risque
Diagnostic Valeurs limites (P97)
Pression artérielle
Somu, Arch Dis Child 2003; 88:302; 4th Int Task Force,Pediatrics 2004;114:555)
Courbes (âge, sexe et taille) ou
Syst. 1 - 17 ans = 100 + (âge en années x 2),
Dias. 1 - 10 ans = 60 + (âge en années x 2)
11 - 17 ans = 70 + (âge en années)
Pré-hypertension P. 90-97 ou > 120/ 80 mmHg
Glucose
OGTT
6.1 mmol/L (WHO)
2h post Glucose max. 7.75 mmol/l
HDL-Cholesterol 0.9 mmol/L (Am. Acad. Pediatrics 1998; 101; 141)
LDL-Cholesterol 3.4 mmol/L
Triglycérides 1.7 mmol/L
ALAT 39 U/L 7-12 ans, 25 U/L > 12 ans
TSH 4.6 (-10) mU/L
Urines Stix, protéinurie, glomérulopathie associée?
Acide urique, ferritine si anamnèse positive.

Hypertension arterielle: 15 (-47)% des enfants obèses à 8 ans**
• 40 % enfants Hypertension art. ont une hypertrophie ventriculaire gauche**
• «Tracking / progression» enfant => adulte
• age 12 ans: Correlation Hypertonie avec intima-media carotides et atherosclerose des adultes
• Risk factors for arterial Hypertension (BP Screening >age 3 years !) – Body Mass Index (BMI) – Low birthweigth (50% salt-sensitive!) or high birthweight (both
metabolic syndrome) – Parent’s Hypertension or smoking – Recherche de l’étiologie et de lésions d‘organes cibles (EKG,
Echographie, Sonogr. Rénale, evt. 24h-TA)
• 1ere therapie: Perte pondérale obèses, alimentation pauvre en sel (<2.5g/d) activité physique régulière > 3*30’ hors école.
Cachat, Paediatrica 15(5):35-42, 2004; Simonetti, Forum medical Suisse 10(17):299-303, 2010;**Maggio A, Farpour-Lambert et al. J Pediatrics 2008

Prevalence of risk factors in Central European Children according to weight
classes
0
10
20
30
40
50
60
Hyp
erte
nsio
n
Chol
.>5.1
LDL>
3.4
HDL<0
.91
Trigl
>1.7
Fast
.Glu
.>6.1
IGT>
7.8
Diab.
mell.2
1 Risk
Fact
.
Clu
ster
>3Risk F.
Pre
vale
nce
%
BMI<P90 BMI>P90 BMI>P97 BMI>P99.5***
***
***
***
*** ***
% • >1 Risk Factor
in 58% of obese children
• >2 Risk Factors in 11.3% of obese children
L‘allemand 2008

Decreased HDL-Cholesterol
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
6
Bo
ys >
Gir
ls
.
OW
>N
orm
.
OB
>N
orm
.
XX
L >N
orm
.
12-1
6y v
s <1
2y
.16
-20y
vs
<12
y .
pub.
>pre
pub
. .
Effects
Od
ds
Rat
io
.
******
***
***
Biological determinants and their relative risk for abnormal HDL- & LDL-Cholesterol
Elevated LDL-Cholesterol
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
6
Bo
ys >
Gir
ls .
OW
>N
orm
.
OB
>N
orm
.
XX
L >
No
rm .
12-1
6y v
s <
12y .
16-2
0y v
s <
12 y
.
pu
b.>
pre
pu
b. .
Effects
Od
ds
Ra
tio
.
****** ***
If cholesterol elevated: homocystéine, apolipoprotéines, lipoprotéine(a). HDL-cholesterol, but not LDL-chol., depends on BMI mainly, and less on gender or puberty. L‘allemand 2008

Insulin Resistance &
Diabetes
Cutoff « Glucose a jeun » >6.1 mmol/L in children due to stress-related increase
OGTT (avec l’insuline basale et résistance à l’insuline (HOMA-IR-)), IMC > P90; à partir de 10 ans; si 1–2 critères positifs:
-acanthosis nigricans, -origine africaine, hispanique ou asiatique - anamnèse familiale positive chez un parent pour un diabète de type 2 (ADA 2000)
Critères pour le diagnostic du diabète 1
1(Selon l’American diabetes association – ADA)

4.9.2009
Metabolic Syndrome: Clustering of cardiovascular risk factors
Criteria Children Adults
(Di Caprio et al 2004) (ADA 2004 Panel III)
1. Obesity kg/m2 or BMI-SDS > 2 -
Waist circumference cm: (>P97, Waist-/ >102 men,
Height-R. >0.5) > 88 women
2. Triglycerides mmol/l: >1.71*high risk >1.71*
3. HDL-Chol mmol/l: <0.9 <0.9
4. Blood Pressure mmHg: > P95 f. Height&Age >135/85 mmHg
5. Glucose mmol/l: IGT >7.8 2h-OGTT IFG >5.6 fasting
IFG >6.1 fasting
(3 of 5 Criteria positive to define the metabolic syndrome in adults)
*Moderate risk >1.15 – 1.71 mmol TG/l, PROCAM 2002

30.10.2014 28 Belenchia, Am J Clin Nutr 2013;97:774–81
• age: 14.1 ± 2.8 y; BMI: 39.8 ± 6.1kg/m2;
25(OH)D: 48 nmol/L
• 4000 IU vitamin D3/d
• 6 months & standard care (2*phys., diet.)
• Adiponectin /Leptin relative improvement ~ to Vit. D increase
=> Reduction of insulin secretion with unchanged BMI & Waist circumference!
Vit. D improves insulin sensitivity in obese youth

Apnée du sommeil et Asthme
Status respiratoire et dépistage de l’apnée du sommeil: polysomnographie, si pauses respiratoires, ronflements, énurésie nocturne secondaire, fatigue, troubles de la concentration
• Asthme: 21% des enfants en surpoids avec anamnese positive!

Problèmes endocrinologiques
• Croissance accelerée prépubérale (adiposogigantisme), mais taille adulte normale.
• Pilosité pubienne et adrenarche précoce (avant 8 ans), mais
• puberté retardée/hypogonadisme chez les garçons;
• troubles menstruels ou hirsutisme chez les filles après une puberté légèrement accélérée.
• Pseudoproblèmes thyroidiens

TSH-elevation reflects insulin resistance° and
correlates with weight* reduction
*Stichel & l’Allemand 2003; °Aeberli 2012

Significant reduction of obesity
32
• At start T0: 78.8% of 1013 children with extreme obesity
• 70.5% of 874 children decreased their BMISDS or waist circumf. after the end of therapy
• at T3, 1 year after the end of therapy, 71.2 % of 354 children had decreased their BMISDS.
• Reduction is significantly more in children <12 years of age until T3
1
2
3
4
T0 T2 T3
BM
I-S
DS
aaa,
bbb aaa bbb
-1.00
-0.80
-0.60
-0.40
-0.20
0.00
0.20
0.40dBMISDS Age<12y
dBMISDS Age>12y
dBMISDS Obclass1&2 dBMISDSOBclass3
T1-T0 (n=663) T2-T0 (n=680) T3-T0 (n=351)
aaa aaa
bbb bbb
c c
DBM
ISD
S

• Vulnerable Groups, low
ressources
• Genetically determined
energy metabolism
• Addiction
• Parents are not treated
themselves
• Psychological problems
Why is treatment of children difficult?

La thérapie de l‘obésité est difficile…
Toujours aborder la question du surpoids !
Avec empathie, entretien motivationel,
Dépistage structuré
Suivi à long-terme & thérapie des comorbidités (d‘apres Reinehr 2013 seulement dans 10 % des enfants)
Les professionnels ont besoin d‘aide !
Formation des infirmières (MPA)
Association Suisse Obésité Enfant et Adolescent (www.akj-ch.ch)
SSP (www.swiss-paediatrics.ch)
Groupes sportifs/associations (www.sportsmile.ch)

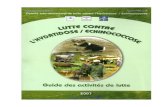
I) 6 mois thérapie individuelle MSIT par méd. de
famille / pédiatre (<6*diététique, 2*physioth.)
(+) 1(-2) ans PMG:
âge 8-18 ans
(mini-PMG:
âge 4-8 ans, Tarmed)
(+) II) = 3-6 mois MSIT certifié avec
≈ 6*psychothérapie,
≈ 9*physiothérapie,
≈ 6*conseils diététiques
(+) III) = Répétition de II) IV) (1-) 5 ans de suivi ≈ bitrimestriel
(+)IMC >p. 99.5, IMC, rapport tour de taille / taille , comorbidité ou problématique psychosociale
Obésité: percentile de l‘IMC >97 , e.a.
Normal: percentile de l‘IMC <90
Surpoids: percentile de l‘IMC >90 <97
Thérapie Thérapie, si
complications
Prévention ciblée
Augmentation de
l‘IMC <6 ans /
fortement en peu
de temps
Sans
complications
(+) Thérapie hospitalière
(planifiée)
(+) Chirurgie bariatrique à
croissance terminée
www.akj-ch.ch ; www.swiss-paediatrics.org; Bull.méd suisse 2014;95(44):1641-2)
Examen médical préalable, selon les recommendations (Paediatrica 2006),
y inclus la thérapie de complications somatiques / psychiques

le 17.1.2009
Suivi à long-terme, même si thérapie peu effective -
mieux vaut prévenir que guérir !
Ostschweizer Kinderspital
www.kig-adipositas.com
www.akj-ch.ch
www.sportsmile.ch
www.promotionsante.ch