Evaluation du risque cardiaque - ICARWEB
189
Evaluation du risque cardiaque per-opératoire Marc Licker, MD Departement de Médecine Aigue 1
Transcript of Evaluation du risque cardiaque - ICARWEB

Evaluation du risque cardiaque per-opératoire
Marc Licker, MD
Departement de Médecine Aigue1

Evaluation cardio-vasculaire pré-opératoire
1. Importance clinique?
2. Mécanismes des complications CV ?
3. Eléments-clé de la consultation d’anesthésie
2

JAMA Cardiol. 2017;2(2):181-7
10’581’621 hospitalisations, 66 [12] ans, 2004 -13 USA
3% Major CV Complic. (death, myoc infarct, stroke)
Vascular 7.7%
Thoracic 6.5%
Transplantation 6.3%
Neurosurgery 4.5%
General S. 3.9%
ORL
Urol. Orthopedic < 2%
Gyn/Obstetrics
< 0.5%
1. Importance : incidence des complications cardiovasculaires postopératoires

JAMA Cardiol 2017;2(2):181-187
Death
Myoc Infarct
Stroke 0.5% to 0.8%
N = 10’581’621 2004-13
1. Importance : Evolution 2004-13 des complications cardiovasculaires postop

0
2
4
6
8
10
12
14
16
Control
Coronary Artery Disease
Heart Failure
5
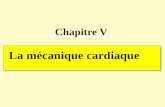
159’327 chir. majeure non-card.> 65ans, 8% mortalité opératoire18% pts + Insuffisance Cardiaque, 34% pts + Coronaropathie
Anesthesiology 2008;108:559-67
Impact de la coronaropathie et de l’insuffisance
cardiaque sur la mortalité postopératoire
% o
pe
rati
veM
ort
alit
y

6
30-daydeath
Prolonged
MechanicalVentilation
UnplannedIntubation
Pneumonia
RenalDysfunction
CardiacArrest
UrinaryInfection
Sepsis
Anesth Analg 2014;119:522–32
2005-10, multicenter cohort 673’422 ACS NSQIP Dataset→ 5’967 matched pairs for 0. 9% New or Worsening HF

7
van Diepen S, et al. Circulation 2011;124:289-96
9,3 9,2
2,9
6,4
13,7
11,812,6
15,2
0
2
4
6
8
10
12
14
16
18
20
IC Ischémique IC Non-Ischémique Coronaropathie Fibrillation A
Mortalité 30-J
Ré-Hospitalisation
MortalityRe-hospitalisation
Ischemic HF Non-Ischemic CAD A FibrillationHeart Failure Heart Failure
181614121086420

Fon
ctio
n
Pu
lmo
nai
reHeures Jours Semaine - Mois
Chirurgie
Fon
ctio
n
Mu
scu
lair
e
Force & Masse Musculaire
AtélectasiePneumonieARDS
ArythmieInfarctus Myoc.Insuf. Cardiaque, AVC
Fatigue
Mét
abio
lism
eSN
Sym
pat
hiq
ue
Inflammation
Anesthésie
1. Importance evaluation CV 2. Mécanismes des complications postopératoires

9
Insuffisance Cardiaque
IschémieInfarctus
Arythmie
1. Importance evaluation CV 2. Mécanismes des complications postopératoires
Inflammation, Stimulation SNSDysfonction musculaire
Atélectasies
PneumonieALI
ARDS
PO
SOP
ERA
TOIR
E
PATIENT + Facteurs de RISQUE
CHIRURGIEHémorragie
Inflammation, stimul. SNSHypercoagulation, Stase
ANESTHESIEHypothermie, ↓ VO2
Inhibition SNS & VagaleAtélectase, VILI, Tr. V/PIN
TRA
OP

Insuffisance cardiaque postopératoire
10
▪ Surcharge liquide
▪ Catecholamines (HTA, FC)
1. Importance evaluation CV 2. Mécanismes des complications
Ischémie myocardique
œdème pulmonaire aigu

Type d’Infarctus Myocardique
11
Coronary Stenosis
Pro
babili
ty o
f M
yocard
ial In
farc
t
Landesberg G et al. Circulation 2009; 119:2936-44
70% DO2/VO2
= IM type 2 (stress)
MINS
30% Plaque ruptureStent + thrombose= IM type 1 STEMI
1. Importance evaluation CV 2. Mécanismes des complications

Impact d’un infarctus péri-opératoire sur la survie
12
MI type 1
MI type 2

N=21’842, 23 hôpitaux (13 pays), 2008-13
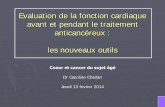
13
Mortalité 30-J : 1.2%
MINS (cT-Tus > 5 ng/ml): 18% (93% asymptomatique)
MINS + ischémie ECG: 4% (infarctus myoc. type 1)
0
5
10
15
20
< 5 ng/ml 5 -40 ng/ml > 40 ng/ml diff. pré-postop
Mortalité 30-JHR ajusté
1.5%
9.7%
HR
2.8
HR
15.7
JAMA 2017;317(16):1642-1651

2.2 Millions 65%; IC 95% 60-70
Silencieux
1.1 Million
35%; IC 95% 30-40
+ Symptôme d’Ischém.
Monde : > 200 Millions adultes + Chir non-cardiaque majeure
100 Millions > 45 ans + Facteurs de risque CV
1 Million 1.1%; IC 95% 0.9-1.2
0.16 Million 26.3%; IC 95% 18-36
0.27 Million 12.5%; IC 95% 8.8-17.1
0.12 Million 9.7%; IC 95% 5.4-15.8
0.36 Million 7.8%; IC 95% 5.7-10
Décès à 30 Jours postopératoires
91.5 Millions
91%; IC 95% 91-92
Trop postop
0.6 Million (sepsis, TE,...) 0.6%; IC 95% 0.5-0.8
Trop + cause non-card.
3 Millions 3.3%; IC 95% 3.1-3.6
Trop - ECG+
4.6 Millions 4.6%; IC 95% 4.4-4.8
Trop isolée (MINS)

Evaluation cardio-vasculaire pré-opératoire
1. Importance clinique?
2. Mécanismes des complications CV ?
3. Eléments-clé de la consultation d’anesthésie
1. Dépister une maladie CV ?
2. Quel(s) examen(s) complémentaire(s) ?
3. Faut-il traiter une maladie CV ?
4. Faut-il reconditionner/préhabiliter ?
15

Recommandations des sociétés d’anesthésie et cardiologie
16
A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014 Jul 29
The Joint Task Force on non-cardiac surgery: CV assessment and management of the European Society of Cardiology and the European Society of Anaesthesiology. Eur Heart J 2014 Sep 14
Pre-operative evaluation of adults undergoing elective noncardiac surgery. Updated guidelines Eur J Anaesth 2018;35:407-65
Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery
Can J Cardiol 2017;33:17-32
1. Importance risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
SFAR Evaluation périopératoire du risque cardiaque en chirurgie non-cardiaqueAnn Fr Anesth Réan 2011:30: e5–e29

17
Les risques CV opératoires dépendent de ….
• Procédure = stress
• Comorbidités
• Capacité fonctionnelle, fragilité
1. Importance risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie

Classes de risque chirurgicale
18
1. Importance risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
Low Risk High Risk

Score clinique de stratification du Risque CV
1. Importance risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
Facteurs de risque RCRI 2005 American College
Surgeons NSQIP 2013
Chirurgie majeure + + (code CPT, emergency/elective
Maladie coronarienne + -
Insuffisance Cardiaque + +
Dysfonction Renale + Créat > 2mg/dl + Créat > 1.5mg/dl
Mal. Cérébro-vasculaire + -
Diabète + type 1 + type 1 ou 2
Classe ASA-PS +
Age avancé +
Classe fonctionnelle +
• Plaie
• Indice de masse corp.
• Steroides
• Ascites (<30 d)
• Sepsis (< 48h)
• Ventilation mécan.
• Cancer étendu
• Hypertension
• Ant. Chir cardiaque
• Dyspnée
• Tabac (< 1yr)
• BPCO sévère
• Dialyse, ARF

20
1. risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
Evaluation fonctionnelleMET Metabolic Equivalent Task1 MET = consommation d’O2 au repos (3.5 ml/kg/min)
« Combien d’étages d’escaliers pouvez-vous monter sans vous arrêter ? »
• > 6 (> 6 MET)• 3-6• < 3

1. risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
Evaluation fonctionnelleQuestionnaire Duke Activity Status Index
VO2peak ml/kg/h =
0.43 x DASI + 9.6
Risque (MET)
> 24 Faible (7)
15-23 Interm (4-6)
10-14 Elevé (3-4)
< 10 Très élevé (3)

Les questionnaires sont-ils fiables pour évaluer picVO2 ?
22
METpeakVO2 peakVO2
Duke Activity StatusN=1’401 dans 25 hôpitaux
Wijeysundera DN et al. Lancet. 2018;391:2631-2640
Très
él
evé
Elev
é
Ris
qu
e F
aib
leInterm
MET7
5
3
7
5
3

Questionnaire d’activités physiques → prédiction des complications cardiaques & de la survie à 1 an
23Wijeysundera DN et al. Lancet. 2018 Jun 30;391:2631-2640

24
Time Up and GO
(TUG)
Evaluation de la fragilité (seniors)
Gait Speed Test
SLOW : > 6secFAST : < 5 sec

25
Ann Surg 2013;258:582-8
Colo-rectal surgery
Time Up and GO (TUG)Gait Speed test
Evaluation de la fragilité→ prédire les Complications & la Survie
J Am Heart Assoc. 2018;7:e010139Cardiac surgery
SLOW < 5sec
FAST > 6sec

26
1. risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
Evaluation fonctionnelle• MET ou Duke Activity Status Index
• Fragilité :
• Mouvements, équilibre: TUG, Gait Speed Test
• Dépendance: Ø, partielle, totale
• Neuro-cognitif: Minimal-Mental State
• Nutrition

27

28
Guidelines 2014 - 18
Urgence ? Chirurgie ▪ Evaluation &
Traitement postopI/C
Condition Critique ?✓ SCA, angor instable
✓ Décompensation Cardiaque
✓ Valvulopathie critique
✓ Arythmies, tr. conduction
▪ Différer la chirurgie
▪ Evaluer & Traiter avant la chirurgieI/B
Chirurgie Mineure OK ChirurgieI/B
Capacité fonctionnelle > 4 MET
& Ø RCRI (Lee score) ? OK ChirurgieIIa/B28

Capacité Fonctionnelle?
Risque Intermédiaire ?
> 1 FRCV > 2 FRCV
Chirurgie VASC ou
MAJEURE
ChirurgieINTERMEDIAIRE
• Coronaropathie
• Insuffisance cardiaque
• Dysfonction rénale (eGFR < 60 ml)
• Diabète type 1
• AVC
Revised Cardiac
Risk Index
Guidelines 2014
> 2 FRCV
ChirurgieMINEURE
ChirurgieINTERM. MAJEURE
MET > 4
TESTCARDIAQUEX
I A
Tolérance Exercice< 3 MET
négatifTEST
CARDIAQUE
I C II B
CHIRURGIEPCI PAC ?
positif

Consensus de la Société française d’anesthésie et de réanimation (SFAR) et la Société française de cardiologie (SFC)D’après Anne-Claire Nonotte, Jean-Luc Fellahi , Rémi Schweizer

31
Rodseth RN et al. Anesthesiology 2013;119:270-83

Test cardiologique : Information modifier le traitement
Tests cardio Rythme Fonction Structure Perfusion
ECG repos + - - (-)
Echocardio - repos - + + (-)
BNP (NT-pro-BNP) - + - -
Stress test• Scintigraphie Tha
• ECG effort
• Echocardiographie
-
+
-
+
-
++
-
-
++
++
+
++
VO2max - + - +
Coronarographie - - (+) +++
Cathétérisme Droit - + (HTAP) - -
Imagerie RMN
CT-scan
SPECT
-
-
-
+
(-)
+
++
+
+
+
+
++ 32

Coronary CT of Master Athlets : the gray zoneBr J Sports 2018; Nov 9, 99840
volume rendering technique imagesnonobstructive mixed plaque in proximal RCA
nonobstructive calcified plaque in proximal LAD

34
CT-coronary angiography in risk stratification prior to non-cardiac surgery: systematic review & meta-analysis
Koshy AN et al. Heart 2019 Sep;105:1335-42
11 trials: N=3’480, MACE in 252 pts (7.2%)

35
Koshy AN et al. Heart 2019 Sep;105:1335-42

36
From 2010 to 2012, 443 LT recipients, age 52 (8)A coronary artery calcium (CAS) score > 400
8.6% had > 1 CV complications within 30 days after LT CAC > 400 in 11 patients (2.5%)
In the multivariate analysis, predictors of CV complic.- CAC > 400 OR 4.6 (95% CI: 1.1– 18.7)- female sex OR 2.8 (1.4–5.6)

Différences entre les Recommandations des sociétés US, UE et Canadiennes
37
• Utilisent l’évaluation fonctionnelle (tolerance à l’effort) pour orienter les patients ayant des facteurs de risque CV vers un stress test cardiologique
• Utilisent la mesure préopératoire de BNP ou NT-pro-BNP pour le suivipostopératoire avec des ECG et la mesure de Troponine
1. Importance risque CV 2. Mécanismes des complications 3. Consultation d’anesthésie
• Utilisent l’évaluation fonctionnelle (tolerance à l’effort) pour orienter les patients ayant des facteurs de risque CV vers un stress test cardiologique
• Intègrent des tests de fragilité

Tachycardie préop = indicateur d’une issue défavorable
38
2016; 117: 172–81

EvaluationRISQUE Préop
Décisionspartagées
Informations anesth -chirRisque / Bénéfice
Suivi du traitement prescritComportement adapté
Engagement
Risques MODIFIABLES
ACQUISCoronaropathie, Insuf. C. Diabète, Athéromatose Malnutrition, Obésité
Infections, Anémie → FRAGILITE
Habitudes
Tabagisme
Alcoolisme
Sedentarité
→ FRAGILITE
Risques FIXES
INNE
Age
SexeGénétique
ACQUISBPCO
DiabèteDémence
Insuf. Card.→ FRAGILITE
1. Risque CV 2. Mécanismes complications 3. Consultation d’anesthésie: Facteurs de risque

Merci!
40

41
ESA –ESC 2014 / 18 ACC/AHA 2014 CCS 2017
Score clinique risque CV
RCRI 1B(NSQIP) 1B
NSQIP 1B(RCRI) 1B
RCRI
Capacité fonctionnelle
MET Score de Fragilité
ASA-PS, TUGTest d’effort VO2max
MET (or DASI)Risque Faible < 4 Interm 4-6,
élevé 7-10, très élevé >10
Test d’effort VO2max
(MET)
Test cardiologique non-invasif
Ø en routine+ maladie cardiaque
+ facteur de risque CV+ capacité fonctionnelle↓
Ø en routine Ø en routine
Scintigraphie myocardique
(echo de stress)
Scintigraphie M (echo stress)
Angio-CT coronarien
Ø
BNP ou NT-pro-BNP Si FRCV >2 Si FRCV >2 Si FRCV >1

42

La consultation d’anesthésieLes buts
1. Quel risque opératoire ?
2. Des examens complémentaires sont-ils nécessaires ?
3. Peut-on optimiser la condition du patient en PRE-, PER- et postop?
Indicateurs cliniques, scores (FR)Type & Gravité de la chirurgieTolérance à l’effort (MET)
Standard• ECG ?• RX thorax ?• Labo ?
• CardiovasculairesUS-Coeur ? US-Carotide ?
• Stress: Echocardio, Scinti ?• Angio-CT Cœur ?• Angio Coronarienne ?
Pulmonaires• Spirométrie, pléthysmographie• Gazométrie, DLCO
• Médicament(s)Arrêt / poursuite, introduction• Antiplaquettaire, anticoagulant• B-B, anti-Ca, IECA/Anti-AngII• …
• Intervention(s) préalable • Revascularisation myocardique• Pacing / débfibrillateur• Correction d’une sténose (ex.: TAVI)• CPAP, bi-PAP 43

Risque CV clinique Chirurgie Capacité Fonctionnelle
ECG -ECG +ECG +
Ø> 1 FRCVAge > 65
MineureIntermédiaire
Majeure
BonneDiminuéeDiminuée
Echocardio TT -ETT +
Ø> 1 ou Souffle Card, signes d’Insuf Card
- BonneDiminuée
BNP NT-pro-BNP –+
Ø Min.- Interm. Bonne
44

45

Décès à 30 Jours postopératoires

47

48

49

Preoperative Cardiovascular Risk Stratification
Risk factors RCRI
Lee 2005
MICA 2011
Guptka
Sabate2011
American College
Surgeons NSQIP 2013
Major Surgery + + + (code CPT, emergency/elective
Coronary Artery Disease + + -
Heart Failure + + +
Renal Dysfunction + + +
Stroke + + -
Diabetes mellitus + (insuline) + (oral, insuline)
Peripheral Arteriopathy + -
ASA Class + +
Advanced age + +
Functional class + +
Abnormal ECG + -
*RCRI, Revised Cardiac Risk Index MICA, Myocardial Infaction or Cardiac Arrest
ACS NSQIP, National College of Surgeons’National Surgical Quality Improvement Project

Predicteurs des Complications Cardio-Pulmonaires
• ASA classes 3-4
• Performance status
• Physical fitness
• Alcohol, smoking
• Chemo-therapy
• Coronary artery disease
• Congestive Heart Failure
• Peripheral Arteriopathy
• Cerebro-vasc. disease
• Renal Dysfunction
• Diabetus mellitus
• Age
• Low SpO2 (<95%)
• Respiratory infection
• Emergency surgery
• Upper abdominal or Thoracic S.
• Duration of Surgery (> 120 min)
RevisedCardiac Risk
Index51
LungARISCAT
Score

52
Sheth TE et al. British Medical Journal 2015;350:h1907
Cardiovascular Death: 1% (n=8)
Myocardial Infarct : 7% (n= 71)
4% Normal coronary artery
24% Non-obstructive CAD
41% (29) : Obstructive CAD
31% (22) : Extensive CAD
N=955 pts + CV Risk factors
Major or Intermed. Surgery

Prédiction des complications cardiovasculaires postopératoires
53CCTA → overestimates risk of postop MACE (5x)
C Index = 0.62

Surgery in ElderlyMortality after Hip Fracture Repair
54
Olmsted County, Minnesota, 1988-2004 (N=1’212)
With preop HF
No preop HFMortality
Cullen MVV et al. J Hosp Med 2011;6:507-12
Preop HF N = 327 (27%)
No preop HF N = 885 (73%)
Periop
death

55
Perioperative Cardiovascular Protection
Learning objectives
1. Why is it important ?
2. Mechanisms of CV complications
2. Periop protective interventions
Myocardial
infarct Heart
Failure
Arrhythmia

Mechanisms of postop Cardio-Vascular complications
Prexisting CV disease
• Coronary AD
• Heart Failure
• Valvular disease
• Arrythmias
• Pulm. HT
56
Surgical stress
❑ Inflammation
❑ NeuroendocrineTachycardia, HT
❑ VO2Fever
Periop Adverse Events
Anemia, Hypovolemia
Hypo- Hypertension
Hypoxemia
Sepsis
Myoc infarct
Heart Failure
Arrhythmias

Fronczek J et al. External validation of the Revised Cardiac Risk Index and National Surgical QualityImprovement Program Myocardial Infarction and Cardiac Arrest calculator in noncardiac vascular surgery. Br J Anaesth. 2019 Oct;123(4):421-429
Dhir S1, Dhir A2 The Global Perspective of Cardiovascular Assessment for Noncardiac Surgery: Comparisons from Around the World. J Cardiothorac Vasc Anesth. 2019 Aug;33(8):2287-2295
Kaw R et al. Predictive Value of Stress Testing, Revised Cardiac Risk Index, and Functional Status in Patients Undergoing Noncardiac Surgery. J Cardiothorac Vasc Anesth. 2019 Apr;33(4):927-932
Tateosian VS1, Richman DC2. Preoperative Cardiac Evaluation for Noncardiac Surgery. AnesthesiolClin. 2018 Dec;36(4):509-521
Fleisher LA. The Value of Preoperative Assessment Before Noncardiac Surgery in the Era of Value-Based Care. Circulation. 2017 Nov 7;136(19):1769-1771
Wijeysundera DN1 Assessment of functional capacity before major non-cardiac surgery: an international, prospective cohort study. Lancet. 2018 Jun 30;391(10140):2631-2640.
Go G et al. Negative predictive value of dobutamine stress echocardiography for perioperative riskstratification in patients with cardiac risk factors and reduced exercise capacity undergoing non-cardiacsurgery. Intern Med J. 2017 Dec;47(12):1376-1384
57
https://www.ncbi.nlm.nih.gov/pubmed/?term=Fronczek%20J%5bAuthor%5d&cauthor=true&cauthor_uid=31256916

Currently, 3 major Society Guidelines:
1. the 2014 ACC/AHA Guidelines
2. the 2014 European Society of Cardiology/European Society of Anesthesiology,2
3. the 2017 Canadian Cardiovascular Society (CCS), that address preoperative assessment
Clear differences (interpretation) between 1 and 2; 3 has new updated evidence
Until recently, we include the assumption that surgery was indicated and would occur.
AS health moves from volume to value, shared decision around the risks and benefits of surgery has taken on increasing importance
58
Risk indices have improved over the years.The American College of Surgeons National Surgical Quality Improvement Program risk calculator has greater perioperative discriminatory ability than previous indices.The future challenge will be to incorporate the calculation of short- and longterm risk into the preoperative discussion, especially given the efficiency pressures on many practices

The Value of Preop Assessment Before Noncardiac Surgery in the Era of Value-Based Care Lee A. Fleisher
• Pts with very poor exercise capacity who cannot improve with an exercise regimen will likely not receive benefit from surgery given the probability of complications and prolonged recovery
• The potential benefit of more formal assessment of exercise capacity and prehabilitation within the value framework should lead to more patient-centered care
• strength of the recommendations may differ in incorporating biomarker testing into perioperative care:
• ACC and AHA have advocated the use of functional capacity as a key discriminator of the need for testing, although the evidence is scant (await the MET trial)
• the CCS advocates the use of preoperative brina natriuretic peptide biomarkers (more than determining functional capacity)
• Patients with stents• Currently preop assessment is focused on periop antiplatelet treatment (ACC/AHA 2016)• One remaining questions: in surgery at risk of bleeding, should AAS be continued in pt with “mature” stent (POISE 2 showed
an increased risk of bleeding with AAS; an Italian registry analysis showed increased risk of stent thrombosis if AAS was discontinued; management of GpIIbIIIa inhibitors?) → discussion between cardiologist, surgeons ans anesthesiologists
• Postop surveillance• Troponin monitoring (different between CCS and AHA/ACC); predictive value of isolated Tp elevations (MINS) after
noncardiac surgery (are they really related to myocardial ischemia
• Trend to move from extensive preop testing to more targeted surveillance and treatment
• Key question will be ensuring that patients make the most informed decision regarding the indication for surgery given the patient’s trajectory for recovery, including returning to baseline or improved functional status and health
59

60
Canadian CV Society
Pro-BNP preop ++> 65 yr or 45-65 with CV
disease or RCRI > 1
Transthor. echo (at rest)Coronary CT, angiographyCPETMyocardial scintigraphy
No
Aspirin initiation Aspirin continuation
NoNo
Except Carotid end., pts with recent stents
Alpha-2 Agonists No
ACEI or Angio II R blocker Withhold 24h preop
Smoking cessation Yes
Troponin postop 48h If elevated preop pro-BNPIf RVRI > 1 or > 65 yr
If 45-65 with CV disease
Postop statin & aspirin If periop myocardialinjury/infarct

61

62

Computed tomographic coronary angiography in risk stratification prior to non-cardiac surgery: a systematic review and meta-analysis
Koshy AN et al. Heart 2019 Sep;105:1335-42
11 trials: N=3’480, MACE in 252 pts (7.2%)
Perioperative MACE • severity & extent of CAD (no CAD 2.0%; non-obstructive 4.1%;
obstructive single-vessel 7.1%; obstructive multivessel 23.1%) Multivessel disease (MVD) OR 8.9, 95% CI 5.1 to 15.3)
• CAC score: ≥100 OR 5.1, ≥1000 OR 10.4)
• In a cohort deemed high risk by established clinical indices:
→ absence of MVD on CTA = negative predictive value of 96% (95% CI 92.8 to 98.4) for predicting freedom from MACE
63

64Koshy AN et al. Heart 2019 Sep;105:1335-42

65
Preop CV Risk factorsNT-proBNP – hsCRP
Curr Opin Crit Care 2011;17:409-15 65

66
Reniten (ACE Inhibitor), Sintrom, Statine
2. Influence of CV medications ?
Cardiac Risk ?
Cardiac Protection ?

67
Anesth Analg 2014;
119:1053–63

68

Quel bilan CV pré-op ?
69
1. Score clinique
2. Troponin

Preoperative Risk Assessment & Optimization in Patients with Lung Cancer
1. Outcome : survival & complications?
2. Predictive factors ?
3. Impact of postoperative complications ?
4. How to prevent complications & improve outcome ?
70

Differences & Similarities between Thoracic and non-thoracic surgery
71
Thoracic surgery Non-Thoracic surgery
Patient preop status
• Indication Lung Cancer Cancer, Vascular d.,
• COPD ++ (20-30%) < 20%
• CV disease < 20% Up to 80%
• Smokers 50-80% < 60%
Intraop : need for OLV Yes No
Postoperative complications
• Pulmonary complic. +++ ++
• Cardiovascular + (arhythmias) + (MI)
• Renal dysfct + +
• Wound infection ++ +
• Admission in ICU 5-10% 5-10%

72
1. Outcome : epidemiology of cancer in Europe

Stage 1 : LocalizedStage 2: Larger (>5 cm) or
spread to local lymph node (18%)
SURGERY
Stage 4: Advanced or metastatic (51%)
Chemotherapy & Palliative RXtherapy
Stage 3: locally advanced (24%)
Chemotherapy & Rxther+/- SURGERY
Brain
Bone
Liver Adrenals73
1. Outcome : current treatments of lung cancer

Lung Cancer 2000-2007
5-y survivalFrom 10% to 18%
74
1. Outcome : survival of patients with lung cancer

75
1. Outcome : survival of patients with lung cancer

N=405’580 patients with NSCLC (SEER program), from 1988 to 2008,
Onco Targets Ther 2017; 10: 4295–4303
Surgery Non-surgicalmanagement
76

in EU : only 20% to 30% of patients with NSCLC undergo surgery
in USA : up to 40% of patients with NSCLC undergo surgery
77

• N = 3’363 from January 1st 2007 to 31 December 2011
Green A et al. EJCTS 2016; 49:589–94
Respiratory Failure Cancer Recurrence
CardioVasc problems (IM, HF, Stroke)
78
6-Month7%
90-Day5%30-Day
2%
1-Year14%

Mu
scu
lar
Fun
ctio
n
Muscular Strength & Mass
Pu
lmo
nar
yFu
nct
ion
Hours - Days Weeks - MonthsIn
flam
mat
ion
Surgery
1. Outcome : Mechanisms of Complications & Fatigue
Met
abio
lism
Sym
pat
het
icN
S
Thrombosis
Plaque rupture
AtelectasisPneumoniaBP FistulaARDS
ArrhythmiaMyoc – InfarctHeart Failure, Stroke
WeaknessFatigue
Anesthesia

80Fernandez FG et al. J Thorac Cardiovasc Surg 2018;155:1254-64
STS Database, 2002 - 2013, N= 29’899
30-d Mortality 2.4% 90-d Mortality 4.5%
Morbidity 20% → prolonged hospital stay
Blood transfusion 8.5%
Atrial Fibril. 14% Myocardial infarct 0.5%
Pneumonia 4.3% Kidney injury 1.4%
Re-intubation 3.8% Delirium 2%
Wound infect. 0.6% Sepsis 0.8%
DV Thrombosis 0.6% Pulm. Embolism 0.5%
1. Outcome : early mortality & Morbidity complications after lung resection

81J Thorac Cardiovasc Surg 2018;155:1254-64
STS Database, 2002 - 2013, N= 29’899
2. Predictive factors : Causes of early mortality after lung resection

82J Thorac Cardiovasc Surg 2018;155:1254-64
STS Database, 2002 - 2013, N= 29’899
2. Predictive factors : Causes of mortality after lung resection

83Nojiri T et al. Ann Surg Oncol 2017;24:1135-42
Prospective database N=675, 2007-12
Cancer recurrence48% with PPCs17% without PPCs
2. Predictive factors : Long-term impact of PPCs & Cancer recurrence

84
3. Preoperative assessment : the «classic» approach→ Organ specific
1. ASA (American Society of Anesthesiology Physical Status):
• Score I to IV• (poorly) predict postop outcome
2. RCRI (Revised Cardiac Risk Index):
• 6 items (Major surgery, HF, CAD, Diabetes, Stroke, Renal dysfunction, vascular disease)• Predict early cardiovascular complications
3. ARISCAT (Assess Respiratory Risk in Surgical Patients in Catalonia)
• 7 items (age, preop SpO2, anemia, resp. infection, major surgery, duration surg., emergency)
• Predict postop pulmonary complications (PPCs)
4. STOP-BANG (risk of postop apnea):
• 8 items (Snoring, Tiredness, Observed apnea, bP, BMI, Age, Neck circumf., Gender)
• Predict postop hypoxemia

Possum : Physiological & Operative Severity Score for the enUmeration of Morbidity & Mortality
Operative (6 items)
• Type of operation
• Number of procedures
• Blood loss
• Peritoneal contamination
• Extent of malignancy
• Elective / emergency
Physiological (12 items)
• Age
• Cardiac status
• ECG
• Respiratory status
• Blood Pressure
• Heart Rate
• Glasgow Coma Score
• Hemoglobin
• White Blood Cells
• Urea
• Sodium
• Potassium
→Scoring system for auditing general, digestive,
vascular, bariatric, orthopedic surgery
→Complex (research)
Copeland G et al. Br J Surg 1991;78:355-60
3. Preoperative assessment : the «academic» approach→ POSSUM

Signes de déconditionnement
1. MET (Metabolic Task Equivalent)• « How many stairs can you climb, … distance walk … ? »• 1 MET = VO2 at rest, 2 MET = 2x VO2 rest,…• Very High Risk< 2-3 MET, High Risk < 4-5,… Fit > 10 MET
2. Duke Activity Status Index• Questionnaire based on DLA (12 items)• Better than MET to estimate VO2 max
3. Six Minute Walk Test or Shuttle test • Simple, reproductible• Intermediate predictor for PPCs
4. Cardiopulmonary Exercise Test• Need material, logistics, reproductible• Better predictor for early and late outcome (< 16 ml/kg/min = interm. risk)86
3. Preoperative assessment : the «functional» approach

87

Org
an
fu
ncti
on
Age
Functional impairment
Myoc.
InfarctF
un
cti
on
al
Re
se
rve
0 20 30 40 50 60 70 80 90
Cancer
SurgeryUnfit
3. Preop assessment : Modern approach→ assess FRAILTY in elderly

89
Am J Surg. 2013 October ; 206(4): 544–550
7 frailty traits measured preop
- Katz Score ≤5
- Timed Up and-Go ≥15 seconds,
- Charlson Index ≥3
- Anemia < 35% Hct
- Mini-Cog score ≤3
- Albumin < 3.5 g/L
- > 1 fall within last 6 months
• Nonfrail: 0–1 trait• Pre-frail: 2–3 traits • Frail: ≥4 traits
Patients ≥65 years undergoing elective colorectal or cardiac surgery
Am J Surg. 2013 October ; 206(4): 544–550
3. Preop assessment : Modern approach→ assess FRAILTY

Preop RISK Evaluation
ComorbidityManagement
Collaborative Decision-making
Collaborative Behavioural change
MODIFIABLE
ACQUIREDCoronary AD
Diabetes Arterial DAnemia, malnutrition
Infections (mouth)
→ FRAILTY
LIFESTYLEObesitySmokingAlcohol
Sedentarity→ FRAILTY
FIXED
INNATE
Age
SexGenetics
ACQUIREDCOPD
DiabetesDementia
Heart Failure
1. Outcome, 2. Predictive factors 3. Preop assessment : Fixed vs Modifiable Risk Factors

MODERN CONCEPT OF PERIOPERATIVE INTEGRATIVE MEDICINE
91
• …Mrs Smith, 77yr has a lung cancer.
• Clinical, biological and pathological data are electronically communicated to a multidisciplinary care team to balance the relative benefits and harms of chemotherapy and surgery
• Mrs Smith is empowered to be fully involved in shared decision-making with an individualized pathway for her pre-operative journey.
• Optimisation of physical and psychological function starts in parallel with the evaluation of treatment options.
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition

92
Patient Empowerment
Case-manager
Enhanced Recovery After SurgeryPreop – Intraop & Postoperative Processes
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition

❑ Oral & Dental Care • Mechanical removal of dental biofilm
or plaques
• Use of oral disinfectants
93
1. PATIENT EDUCATION & EMPOWERMENT
❑ Tobacco cessation
❑ Alcohol withdrawal
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition

94
2. NUTRITIONAL ASSESSMENT & CORRECTION
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition

95
Minimal level of functioning
PREHABILITATION
FitSurgery
Unfit
Fun
ctio
nal
Sta
tus
Death
Complications
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition
3. EXERCISE TRAINING PRESCRIPTION

Endurance
Inspiratory Muscle Tr.
96
SurgeryPreoperative (1 – 4 weeks) Postoperative
3. EXERCISE TRAINING MODALITIES Hospital, Fitness center, Home-basedW & W/o Supervision

Improve Preoperative Function
• peakVO2 + 12% (95%CI 5-65)
• Max Inspir P + 13 mmHg (95%CI 7-19)
• 6Min Walk T + 47 m (95%CI 36-54)
97
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition
3. EXERCISE TRAINING EFFICACY META-ANALYSIS 28 RCTs (N=2’040)
• Thoracic S. 0.33 (0.21 – 0.51)
• Cardiac S. 0.44 (0.29 - 0.67)
• Abdominal S. 0. 40 (0.21 – 0.77)
Improve Postop Outcome→ lower incidence PPCs OR (95%CI)
• Endurance T 0.39 (0.21 – 0.61)
• Respiratory MT 0.60 (0.36 - 0.91)
• Combined T 0. 28 (0.15 – 0.51)
BUT, no benefit on :• 30-day-Mortality • Cardiovascular complic.

98
PREOP EXERCISE TRAINING & PPCS
DURATION OF TRAINING
<2 Weeks OR 0.32 (0.2 – 0.5)
2-4 Weeks OR 0.50 (0.3 – 0.8)

99
BMJ 2018
Multi-center RCT in NZ, Australia;
Upper Abdominal Surgery, N= 441
30 min education, teachingHow to breath
PPC

100
Mortality
Preop education : respiratory breathing by experienced physiotherapists
Boden I et al. BMJ. 2018 Jan 24;360:5916

IN 2025, MR SMITH PERIOP MANAGEMENT…
• …Mrs Smith has been optimized with diet, physical exercise and, with meditation or self-hypnosis, she feels a level of control to minimize her anxiety.
• an individualised ‘e-health navigator’ guides her nutrition, exercise and psychology programme.
• … investigations and chemoradiotherapy are carried out.
• Following surgery, Mrs Smith is prepared for the expectation that she will drink, eat and mobilize the same day, and be discharged from hospital 2 days after her operation.
• Her ‘e-health navigator’ guides her recovery phase, and 6 weeks later she returns to her baseline level of function, physically and mentally.
101
1. Outcome, 2. Predictive factors 3. Preop assessment 4. How to optimize patient condition

Preoperative exercise training
• Short period of time• 1 to 4 weeks
• Medical prescription• Type of exercise• Goals : duration, intensity, repetition
• Settings• home, fitness center or hospital, or combination
• Supervision• Coaching, Monitoring
102

Aerobic Training (Endurance)
103
Inspiratory Muscle Training
Stretching, Relaxation
Power, Resistance

How does it work ?
Fast-twitchSlow-twitch
Classification based on: Myosin subtype, ATPase, metabolism, twitch, fatigability
Intermediate
GlycolyticOxidative Mixed Oxydative-glycolytic
Type 1 Type 2A Type 2X Type 2B
TRAINING
Hyperplasia
Endurance
Hypertrophy
Resistance

Endurance Training
105AMPK, adénosine mono-P kinase; CaMK, calmoduline kinase; PGC-1a, coactivateur 1α du récepteur γ activé par le proliférateur du
peroxisome; GLUT4, transporteur de glucose membranaire; ROS, radical oxygen species
ROS ++ ROS +
Angio-
genese
1. Postop complications 2. Modern periop context 3. Solutions to improve outcome
VO2max

Max Inspir P
106
peakVO2
IMPACT OF PREHABILITATION ON FUNCTIONAL PARAMETERS
6 Min Walk T
+ 12% (5 –
65)
+ 13 mmHg (7 –19)
+ 47 m (36 –
54)

107
Cardiac surgery
Thoracic surgery
Abdominal surgery
OR 0.33 (0.2 – 0.5)
NNT 5Number Needed to
Treat to avoid 1 complications
PREHABILITATION & POSTOPERATIVE PULMONARY COMPLICATIONS

Max Inspir P
108
peakVO2
IMPACT OF PREHABILITATION ON FUNCTIONAL PARAMETERS
6 Min Walk T
+ 12% (5 –
65)
+ 13 mmHg (7 –19)
+ 47 m (36 –
54)

109
Cardiac surgery
Thoracic surgery
Abdominal surgery
OR 0.33 (0.2 – 0.5)
NNT 5Number Needed to
Treat to avoid 1 complications
PREHABILITATION & POSTOPERATIVE PULMONARY COMPLICATIONS

Aerobic Endurance T
Inspiratory Muscle T
110
PREOP EXERCISE TRAINING & PPCS
TYPE OF TRAINING
OR 0.39 (0.2 –
0.6)
OR 0.60 (0.36 –
0.99)
Combined Training
OR 0.28 (0.15 –
0.5)

But, some limittiona…
• 20-30% are unable to attend the program• Too far from hospital• Poor motivation• Exercise program not adapted to patient
• Some patients do not respond (?)
111

112

113
People > 65yr10 % → 30%

114

Cognitive disorders after surgery
115Can Anesth 2011; 58:216–223

116J Thorac Cardiovasc Surg 2018;155:1254-64
J Thorac Cardiovasc Surg 2018;155:1254-64

• From 2007 to 2017, N=697 Mortality 30-d: 0.9%, 90-d 1.4%
Causes of death at 30 days 90 days
30 Day MortalityCardiovasc 33% Pulmonary 67%
90 Day MortalityCardiovasc 30%Pulmonary 60%
117

118
Eur J Cardio-Thor Surg 2017;52: 1041–48N=62’774, 2007-2016 (VATS 21%)
30-D Mortality 2.6%, Morbidity 18.5%
2. Predictive factors

119Adapted from Files et al. Critical Care 2015: 19:266
1. Why is it important : From Physiology to Clinical applications

• 250 millions operations are performed worldwide
• 1-3% early mortality
• Pulmonary C. > Wound infection > Cardiac C. Economic burden : prolonged hospital stay, ICU
admission
Prognostic implications : reduced survival and qualityof life
120
1. Why is it important: EPIDEMIOLOGY of postoperative complications
• > 50% surgeries performed in pts > 65yrs

2015;150:1034-40
National Cancer Data Base (~1’500 Hospitals, ~70% of all cancers)
→ Identification of hospitals with lowest and highest mortality, 01.2005 to 12.2006
NO difference regarding :
o Neoadjuvant tretament
o Use of Epidural catheter
o Use of beta-blockers
o Intraop monitoring
o AB prophylaxis
o VT prophylaxis
o Open vs VATS121
Correct management of Cardio-Pulm Complications
→ better outcome

LowMortality (%)
LowMortality (%)
High Mortality (%)
High Mortality (%)
LowMortality (%)
JAMA 2015;150:1034-40
Hospitals with lower mortality
- Preop risk management- Protective organ strategies- Early detection of postop
complication (PC)- Appropriate treatment of PC

Thoracic SurgeryRisk factors for mortality & morbidity
Preop condition
• ASA classes 3-4
• Cardiovasc. Condition (RCRI)
• Alcohol, tobacco
• Physical fitness (METs, VO2max)
• COPD
• Lung Volume: ppo FEV1 < 40%
• Diffusion capacity: ppoD <40%
• Extent of resection
• VATS < Thoracotomy
• Duration of M. Ventilation
• Ventilatory strategy
Surgery -Anesthesia

124

125

N=202’914, from 2004 to 2013
J Cancer Res Clin Oncol 2018;144:145–55
5-y survival20.4%
10-y survival11.5%
1. Outcome
126

2. Causes of death in pts with NSCLCJ Cancer Res Clin Oncol 2018;144:145–55
--- Lung Cancer (88% deaths)
127

• n = 3363 from January 1st 2007 to 31 December 2011
Green A et al. EJCTS 2016; 49:589–94
128

Mortality after Lung Cancer Surgery
1. Current survival & early/late mortality ?
2. Causes of mortality & Predictive factors ?
3. Impact of postoperative complications &
Failure to Rescue ?
4. Improved outcome in patients with LC ?129

4. How to improve outcome in patients with LC
Preoperative management• Better detection of « operable » patients with CT-scan, gated-MRI
→ Increase the number of patients with early disease stage
• Chemo-RX-photodynamic therapy
• Immune system enhancement
→ Noninvasive curative treatment
• PREHABILITATION : → Improve physiological reserve to sustain surgical stress
Physical exercise training
Nutritional and psychological support130
CONCLUSION

4. How to reduce early post-thoracotomy mortality
Intra-operative management
• Minimally invasive surgical approach (e.g., VATS)
• Lung isolation (experts!) & Lung protective ventilation
• Hemodynamic homeostasis (BP, fluids titration, Hb, …)
• Appropriate analgesia
131
CONCLUSION
Postoperative
• Physiotherapy (respiration, mobilization), resume oral intake,…
• Remove as soon as possible cathters, drains
• Selective admission in ICU/intermediate care

Eur J Epidemiol 2019 Jul 16
5-Yr Survival (%)
9.4 (8.1-10.8) 14 (12.3 – 15.2) 18 (16.4 – 19.5) 20 (19.2 – 21)
132

5 yr survival35%
5 yr survival8%
5 yr survival40%
5 yr survival15%
7%
6%
N=4’780 from the SEER database, from 2004 to 2014
133

• N=10’991, operation between 2004-2010
• 30-Day mortality = 3.0% 90-Day mortality = 5.9%
• Risk factors (90-d death)
• Age > 75
• Poor physical performance
• Bi-lobectomy, Pneumonectomy
Powell HA, et al. Thorax 2013;68:826–34
134

135

Service d’AnesthésiologieDépartement de Médecine Aigue
Marc Licker
PATIENT’S EMPOWERMENT
TO IMPROVE OUTCOME AFTER SURGERY

patient’s optimization to improve postoperative outcome
Learning objectives
1. Postoperative complications : why is it important!o From physiology to clinical applicationso Epidemiologyo Preoperative risk evaluation
2. Modern context of perioperative medicine
o An example …
o Enhanced Recovery After Surgery (ERAS) Program
3. Are there solutions ?o Patient’s education: risk controlo Concept of prehabilitationo Encouraging results with exercise training
137

138
FATIGUE
Organ dysfonction
COMPLICATIONS
Neuro-humoral
Inflammatory
Response
Anesthesia
Surgery
1. Postop complications
WHY IS IT IMPORTANT : From physiology to clinical applications
LowSpO2
Dyspnea
Œdema
Oliguria
HTATachycardia
Anemia
Cognitive disorders
PAIN
FEVER

139Adapted from Files et al. Critical Care 2015: 19:266
1. Why is it important : From Physiology to Clinical applications

140

• 250 millions operations are performed worldwide
• 1-3% early mortality
• Pulmonary C. > Wound infection > Cardiac C. Economic burden : prolonged hospital stay, ICU
admission
Prognostic implications : reduced survival and qualityof life
141
1. Why is it important: EPIDEMIOLOGY of postoperative complications
• > 50% surgeries performed in pts > 65yrs

142
8.5% 9.5%
> 65 ans 18 %
25 %en 2030

Non-Frail versus FrailImpact on postoperative outcome
143
BetterOutcome
Poor Outcome
BetterOutcome
Poor Outcome
1. Postoperative complications Preop Risk Assessment: FRAIL or not
Cardiovascular D.Pulmonary D.

Org
an
fu
ncti
on
Age
Functional impairment
Fu
nc
tio
na
l
Re
se
rve
0 20 30 40 50 60 70 80 90
1. Postoperative complications Preop Risk Assessment: AGING & functional impairment
High Physical Activity = FIT

145
5h36 !

Org
an
fu
ncti
on
Age
Functional impairment
Myoc.
InfarctF
un
cti
on
al
Re
se
rve
0 20 30 40 50 60 70 80 90
1. Postoperative complications Preop Risk Assessment: AGING & functional impairment
Cancer
SurgeryUnfit

148
Patient
Case-managerMonitoring
Enhanced Recovery After SurgeryPreop – Intraop & Postoperative Processes
1. Postoperative complications 2. Modern context of perioperative medicine

patient’s optimization to improve postoperative outcome
1. Postoperative complications : why is it important!
o From physiology to clinical applications
o Epidemiology
o Preoperative risk evaluation
2. Modern context of perioperative medicine
o An example …
o Enhanced Recovery After Surgery (ERAS) Program
3. Are there solutions ?o Patient’s education: risk controlo Concept of prehabilitationo Results with preop exercise training
149

1. Oral hygiene• Mechanical removal of dental biofilm
or plaques
• Use of oral disinfectants
150
1. Postop complications 2. Context of periop med 3. Solutions to improve outcome
Patient EDUCATION & EMPOWERMENT
2. Tobacco cessation
3. Alcohol withdrawal

151
NUTRITIONAL ASSESSMENT & CORRECTION
1. Postop complications 2. Modern context of periop med 3. Solutions to improve outcome

152
Minimal level of functioning
PREHABILITATION
FitSurgery
Unfit
Fun
ctio
nal
Sta
tus
Death
Complications
Concept of Prehabilitation → Exercise training
1. Postop complications 2. Modern periop context 3. Solutions to improve outcome

Preoperative exercise training
• Short period of time
• 1 to 4 weeks
• Medical prescription
• Type of exercise
• Goals : duration, intensity, repetition
• Settings
• home, fitness center or hospital, or combination
• Supervision
• Coaching, Monitoring
153

Aerobic Training (Endurance)
154
Inspiratory Muscle Training
Stretching, Relaxation
Power, Resistance

How does it work ?
Fast-twitchSlow-twitch
Classification based on: Myosin subtype, ATPase, metabolism, twitch, fatigability
Intermediate
GlycolyticOxidative Mixed Oxydative-glycolytic
Type 1 Type 2A Type 2X Type 2B
TRAINING
Hyperplasia
Endurance
Hypertrophy
Resistance

Endurance Training
156AMPK, adénosine mono-P kinase; CaMK, calmoduline kinase; PGC-1a, coactivateur 1α du récepteur γ activé par le proliférateur du
peroxisome; GLUT4, transporteur de glucose membranaire; ROS, radical oxygen species
ROS ++ ROS +
Angio-
genese
1. Postop complications 2. Modern periop context 3. Solutions to improve outcome
VO2max

High Intensity Interval Training2-3 series 4 x 1 min + Recuperation 4 x 1 min
Echauffement
100% HRmax
Re
cup
era
tio
n
Re
cup
era
tio
n
Re
cup
era
tio
n5 min
1. Postop complications 2. Modern periop context 3. Solutions to improve outcome

PREOP EXERCISE TRAININGDOES IT WORK IN PATIENTS UNDERGOING MAJOR SURGERY ?
158
28 RCTs , N=2’040
2 Oesophageal s. (N=301)
10 Thoracic surgery (N=563)
6 Cardiac surgery (N=628)
10 Abdominal surg (N=536)
1. Postop complications 2. Modern periop context 3. Solutions to improve outcomeAssouline B, Cools E & Licker M

Max Inspir P
159
peakVO2
IMPACT OF PREHABILITATION ON FUNCTIONAL PARAMETERS
6 Min Walk T
+ 12% (5 –
65)
+ 13 mmHg (7 –19)
+ 47 m (36 –
54)

160
Cardiac surgery
Thoracic surgery
Abdominal surgery
OR 0.33 (0.2 – 0.5)
NNT 5Number Needed to
Treat to avoid 1 complications
PREHABILITATION & POSTOPERATIVE PULMONARY COMPLICATIONS

Aerobic Training
Inspiratory Muscle Tr.
161
PREOP EXERCISE TRAINING = EFFECTIVE INTERVENTION
TO PREVENT POSTOPERATIVE PULMONARY COMPLICATIONS
SurgeryPreoperative (1 – 4 weeks) Postoperative

Aerobic Endurance T
Inspiratory Muscle T
162
PREOP EXERCISE TRAINING & PPCS
TYPE OF TRAINING
OR 0.39 (0.2 –
0.6)
OR 0.60 (0.36 –
0.99)
Combined Training
OR 0.28 (0.15 –
0.5)

163
PREOP EXERCISE TRAINING & PPCS
DURATION OF TRAINING
<2 Weeks OR 0.32 (0.2 –0.5)
2-4 Weeks OR 0.50 (0.3 –0.8)

But, some limittiona…
• 20-30% are unable to attend the program• Too far from hospital• Poor motivation• Exercise program not adapted to patient
• Some patients do not respond (?)
164

165
BMJ 2018
Multi-center RCT in NZ, Australia;
Upper Abdominal Surgery, N= 441
30 min education, teachingHow to breath
Pu
lmo
nar
y C
om
plic
atio
ns

166
Mortality
Preop education : respiratory breathing by experienced physiotherapists
Boden I et al. BMJ. 2018 Jan 24;360:5916

New project
167
Preop exercise training to prevent postoperative pulmonary
complications in patients undergoing thoracic or abdominal
surgery:a multicentre Randomized Controlled Trial
Single education & teaching session (1h) : HOME-Based intervention- Endurance training (>10’000 steps/day)- Inspiratory muscle training- stop smoking/alcohol
Interactions Patient - Health Care Professionals : - Patient adhesion to program- Supervision, counselling, ….

Thank you !
168

Postoperative Muscle Weakness
Organ cross-talks→Metaboreflex
Modified from Dempsey J et al. Respir Physiol & Neurobiol 2006; 151:242–50
Phrenic n. discharge
Fatiguing contractions• Diaphragm (intercostal muscles)
• Expiratory & Accessory muscles
Sympathetic NS hyperactivity• Limb flow & O2 availability•Muscle fatigue
• Ambulation
Work of Breathing

Trial sequential analysisPreHabilitation & PPCs: Meta-analysis of RCTs
170

171
500’148 habitantsCroissance annuelle 1.02% (1996-2018)
> 65 ans 16.5%
28 %en 2030

IN 2025, MRS SMITH PERIOP
MANAGEMENT…• …Diet, physical exercise, psychology and co-existing
conditions are all optimised
• Mrs Smith feels a level of control that minimizes her anxiety.
• She uses an individualised ‘electronic health navigator’ to guide her nutrition, exercise and psychology programme.
• …in parallel the investigations and chemoradiotherapy is carried out.
• Following surgery, Mrs Smith is prepared for the expectation that she will drink, eat and mobilise the same day, and is discharged from hospital only 2 days after her operation.
• Her ‘electronic health navigator’ guides her recovery phase, and 6 weeks later she returns to her baseline level of function, both physically and mentally.
172

Aerobic fitness = good predictor of outcome
173Imboden MT etal. Cardiorespiratory Fitness and Mortality in Healthy Men and Women. J Am Coll Cardiol 2018;72:2283-2292.
1. Postoperative complications 2. Preop Risk Assessment: Aerobic Fitness

peakVO2 = Good predictor of Cardiac & Respiratory Complications
174
Lung Cancer Surgery
1. Hennis PJ et al. CPET predicts postoperative outcome in patients undergoing gastric bypass surgery. Br J Anaesth 2012;109:566-712. Wijeysundera DN et al. Assessment of functional capacity before major non-cardiac surgery. Lancet. 2018;391:2631-26403. Licker M et al. Impact of aerobic exercise capacity and procedure-related factors in lung cancer surgery. Eur Respir J 2011;37:1189-98
1. Postoperative complications 2. Preop Risk Assessment: Aerobic Fitness

175
Cardio-Pulmonary Exercise Test
Low peakVO2< 15 ml/kg/min
High VE/VCO2
> 35-40
Peak VO2, VE/VCO2 & Anaerobic threshold
Anaerobic threshold< 10 ml/kg/min

176
Respiratory Muscle Weakness in Thoracic Pts
Maximal Inspiratory Pressure (MIP)
Refai M et al. Eur J Cardio-Thor Surg 2014;45:665–70
After max exerciseAt rest

177
2011;254:1044–49
Myofibrillar dysfunctiondiaphragm
• Catabolic pathway• Immobilization, Inflammation
• E3-ligases MuRF-1 degradation of Myosin HC 2A
Muscle biopsies in pts undergoing thoracotomies with OLV (2h)
Dia
ph
ragm
Lati
ssim
us
do
rsis
Myosin Heavy Chain (MHC)

Enhanced Recovery After Surgery(ERAS) Program
• Standardisation and streamlining of immediate peri-operative processes with relevant patient benefit.
• Ideally peri-operative medicine should encompass patient-centred, multidisciplinary and integrated medical care from the moment of contemplation of surgery until full recovery .
• ERAS should embrace collaborative decision-making, prehabilitation, proactive management of comorbidities and individualised postoperative care.
178

Cardio-Pulmonary Exercise Test (CPET) = Gold Standard
Low peakVO2< 15 ml/kg/min
High VE/VCO2
> 35-40
Anaerobic threshold< 10 ml/kg/min
1. Postoperative complications 2. Preop Risk Assessment: Aerobic Fitness

peakVO2 = Good predictor of Cardiac & Respiratory Complications
180
Lung Cancer Surgery
1. Hennis PJ et al. CPET predicts postoperative outcome in patients undergoing gastric bypass surgery. Br J Anaesth 2012;109:566-712. Wijeysundera DN et al. Assessment of functional capacity before major non-cardiac surgery. Lancet. 2018;391:2631-26403. Licker M et al. Impact of aerobic exercise capacity and procedure-related factors in lung cancer surgery. Eur Respir J 2011;37:1189-98
1. Postoperative complications 2. Preop Risk Assessment: Aerobic Fitness

Non-invasive tools to predict postop outcome1. MET (Metabolic Task Equivalent)
• « How many stairs can you climb ? »
• 1 MET = VO2 at rest, 2 MET = 2x VO2 rest,…
• Very High risk < 2-3 MET, High Risk < 4-5,… Fit > 10 MET
2. Duke Activity Status Index (1,2)• Questionnaire based on Daily life activities (12 items) (1)
• More reliable than MET to estimate peakVO2 (2)
3. Six Minute Walk Test (3)• Simple, reproducible
• Moderate predictor of outcome
4. Shuttle Walk test (3) • Simple reproducible, substitute for 6MWT
1. Coute RA et al. Electronically self-assessed functional capacity and exercise testing: A comparison of the Duke Activity Status Index and Patient-Reported Outcomes Measurement Information System tools. Am Heart J 2017;188: 82-862. Wijeysundera DN et al. Assessment of functional capacity before major non-cardiac surgery. Lancet. 2018;391:2631-2640Moran J et al. The preoperative use of field tests of exercise tolerance to predict postoperative outcome in intra-abdominal surgery: a systematic review. J Clin Anesth 2016; 35:446-455
1. Postoperative complications 2. Preop Risk Assessment: Exercise Capacity/Tolerance

Duke Activity Status Index
182

183
1. Postoperative complications 2. Preop Risk Assessment: New tools of functionality
Gait Speed test (5m)Walk 5 m, repeated 3x
▪ > 6 sec = Slow
▪ < 6 sec = Fast
Time Up and GO (TUG)

184
Geriatric Evaluation Functionality Indicators→ Postop Clinical Outcome
JACC 2010 2010;56:1668-78 Ann Surg 2013;258:582-8
Time Up and GO (TUG)Gait Speed test

Multimodal Perioperative Protection
Pre
op
era
tive
•Clean lungs & airways• Stop smoking & OH
EXERCISE !Muscles, Heart & Lung
Intr
aop
erat
ive
• Lung isolation /separation• Protective lung ventilation
✓ P Inspir < 20 cmH20✓ VT 4-8 ml/kg IBW✓ PEEP 5-10 cmH20✓ Recruitment
• Low-opiate anesthesia• Restrictive fluid management
Fast-Track surgeryVATS (> open)
Po
sto
per
ativ
e
• Analgesia• Control Fluid balance
Early extubation
MOBILIZE !ALL muscles
CLEAR the AIRWAYSRECRUIT the LUNG
RESPIRATORY Muscles

Impact of Rehabilitation in chronic diseases
Strong evidence for clinical benefits in patients with
• Chronic Obstructive Pulmonary Disease
• Heart Failure, Coronary Artery Disease
• Cerebrovascular & NeurologicalDdisease
• Diabetus mellitus
• Sedentary persons
186
… But, requires long term training (months)combined with diet, behavioral changes …

Volatil anesthetics > propofol II B
Restrictive vs goal-directed fluid loading ?
IMPACT OF PERIOPERATIVE CARE IN THORACIC PATIENT
Open Lung Ventilation (LowVT + PEEP + Recruit; PI<
20)
II B
FIO2 (<60%)? PEEP? Recruitment ? -
Interventions Evidence
Risk assessment for complications II B
Alcohol – Tobacco arrest II C
Dental & oral care II C
Nutrition assessment & correction II C
PRE-
Op
INTRA-
Op
Post -
Op
Exercise training (endurance, IMT, combined) II A
Optimal analgesia, early mobilization, NIV, HFNO2, control fluids, remove chest tubes, vasc. canula, urinary c.
??
Normothermia (body & fluid warming) IIA

Mechanisms of Postop pulmonary complications
188
Preoperative
• Weak muscles, low peakVO2
• Airway obstruction
• Infection
• Alcohol, tobacco
• COPD, lung fibrosis
Intraoperative
• High inspiratory pressure (MV)
• Surgical

Awake preop
Elastic LUNG Recoil
Elastic CHEST Recoil
Atelectasis
PostoperativeInflammation
Muscle weakness
Anesthesia
Mechanical ventilation
X X
XX
FRC
MECHANISMS OF POSTOP PULMONARY COMPLICATIONS
IC
RV RV
Pneumonia
Resp. Failure

190
Impaired Postop respiratory function
Postop
Estenne M et al. Thorax 1985;40:293-99
1st day after thoracic surgery
• Restrictive lung syndrome
FRC
• Lower Max Inspir. P (-50%)
« shallow breathing »▪ Smaller VT
Lunardi ACet al. Respir Physiol Neurobiol2013;186:40-44