Diagnostiquer une Aspergillose -...
50
Diagnostiquer une Aspergillose N. Milpied CHU Bordeaux
Transcript of Diagnostiquer une Aspergillose -...
Diagnostiquer une Aspergillose
N. Milpied CHU Bordeaux

Fréquence, terrain, mortalité

Bitar D et al. Bull Epidemiol Hebdo 2013

Bitar D et al. Bull Epidemiol Hebdo 2013

0-1 jours 2-3 jours
> 4 jours
Délai de diagnostic (160 pts) (Caillot et al. Clin Microb Infect Dis. 2001, 7: 54-61.)
Semaines
0
,25
,5
,75
1
0 4 8 12 16 20 24
P = 0.0022
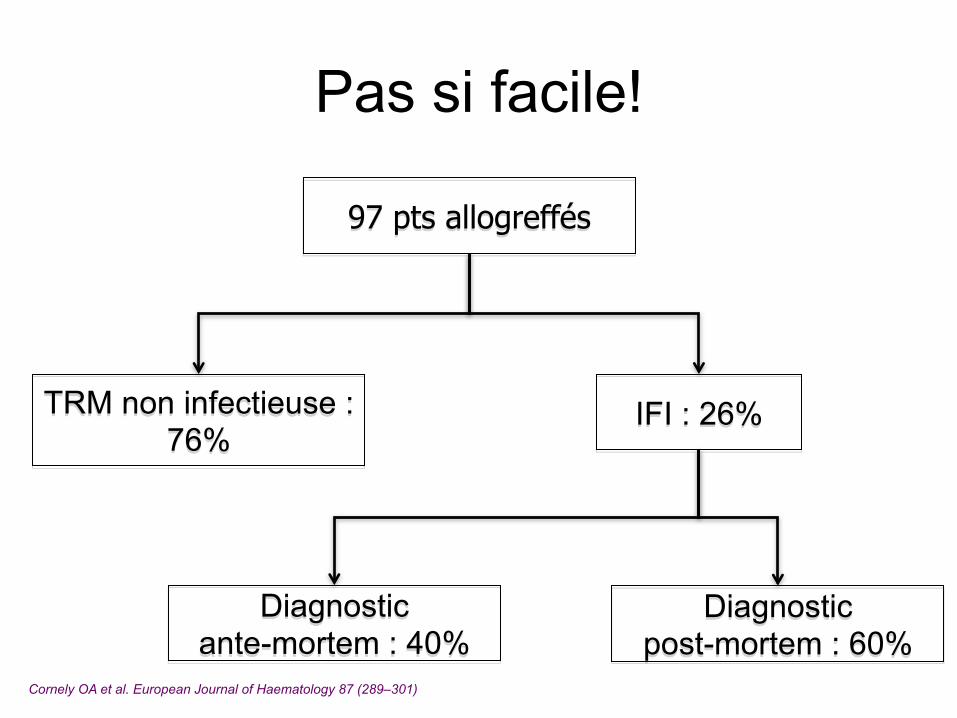
Cornely OA et al. European Journal of Haematology 87 (289–301)
IFI : 26%
97 pts allogreffés
TRM non infectieuse : 76%
Diagnostic ante-mortem : 40%
Diagnostic post-mortem : 60%
Pas si facile!
Les critères diagnostiques

Niveau diagnostique des aspergilloses
Aspergillose prouvée Biopsie positive ou examen direct positifs sur tissus Ou culture positive d’un site normalement stérile
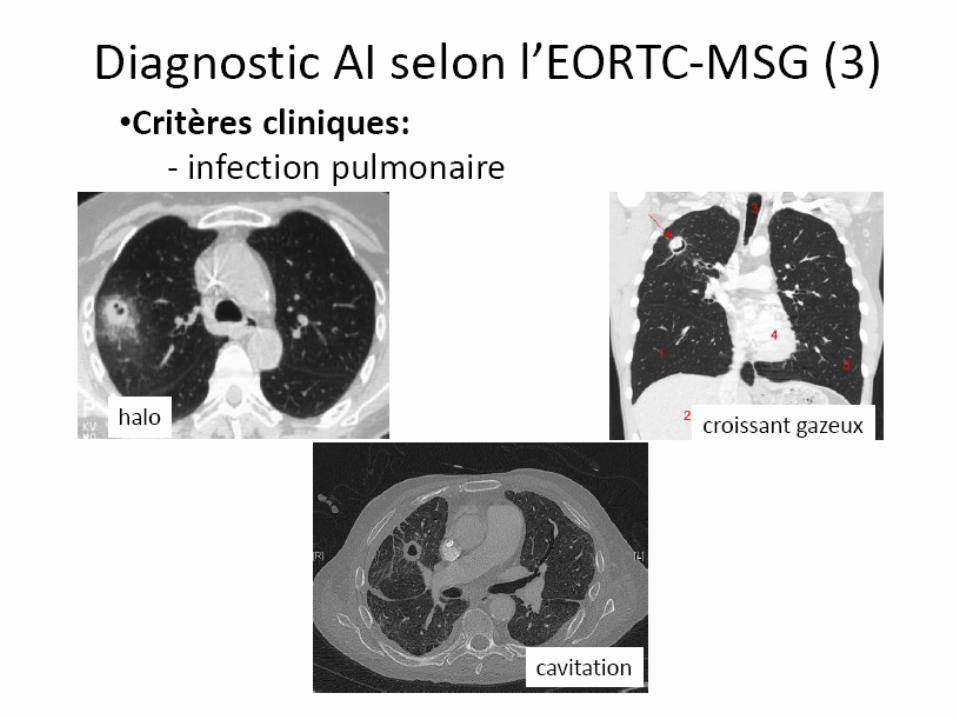
1) Critères d’hôte = Neutropénie > 10 jours (ou allogreffé moelle ou corticoides > 3 sem ou Campath ou analogue Purine) 2) Critères Cliniques = Poumons : CT scan : opacité +/- halo ou croissant Sinus - Bronches/trachée - SNC - Disséminé 3) Critères Microbio = Culture + Aspergillus ou Ex direct + (site non stérile) Antigen aspergillaire + : serum, plasma, LBA, LCR B-Glucan sérique +
Aspergillose Probable
De Pauw et al. Clin Infect Dis. 2008. 46 : 1813-20
Aspergillose Possible

Les conséquences
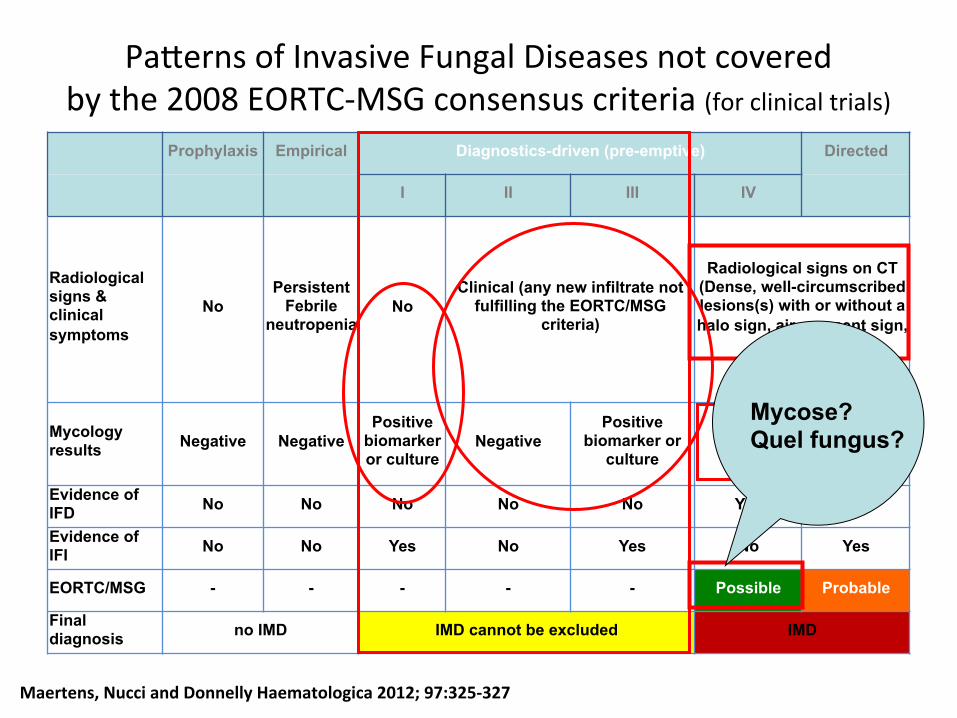
Pa#erns of Invasive Fungal Diseases not covered by the 2008 EORTC-‐MSG consensus criteria (for clinical trials)
Prophylaxis Empirical Diagnostics-driven (pre-emptive) Directed
I II III IV
Radiological signs & clinical symptoms
No Persistent
Febrile neutropenia
No Clinical (any new infiltrate not
fulfilling the EORTC/MSG criteria)
Radiological signs on CT (Dense, well-circumscribed lesions(s) with or without a halo sign, air-crescent sign,
or cavity)
Mycology results Negative Negative
Positive biomarker or culture
Negative Positive
biomarker or culture
Negative
Positive Biomarker or microscopy or culture
Evidence of IFD No No No No No Yes Yes
Evidence of IFI No No Yes No Yes No Yes
EORTC/MSG - - - - - Possible Probable
Final diagnosis no IMD IMD cannot be excluded IMD
Maertens, Nucci and Donnelly Haematologica 2012; 97:325-‐327
Mycose? Quel fungus?

Cumulative mortality rate 12 weeks after initiation of a non-prophylactic antifungal therapy according to classification at day 7 (n=419 patients, 4708 patient-weeks) p=0.016
Indications and Outcomes of Antifungal Therapy in French Patients with Haematological Conditions or Recipients of HSCT
Herbrecht R et al, JAC ,2012
Questions
• Interprétation du scanner • Biomarqueurs: types et valeur

halo J0 J3
J10
femme (34 ans) LAL
(neutropénie depuis J-18)

J6 - J10 18
22%
50%
28%
900
J0 - J5 37
70-100%
0-30%
< 5% 0
TDM (n) Signe halo typique TDM non spécifique Signe croissant typique PNN/mm3 (median)
Evolution ds 71 scanners séquentiels
Caillot et al. J Clin Oncol. 2001; 19: 253-9.
J11 - J20 16
19%
18%
63%
2900
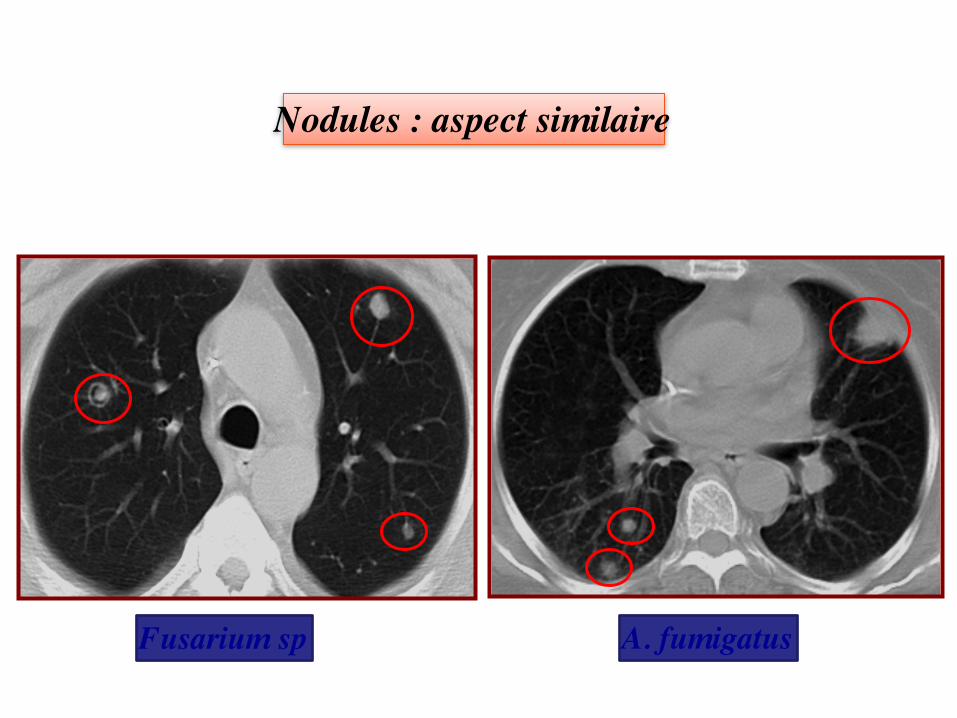
A. fumigatus Fusarium sp
Nodules : aspect similaire
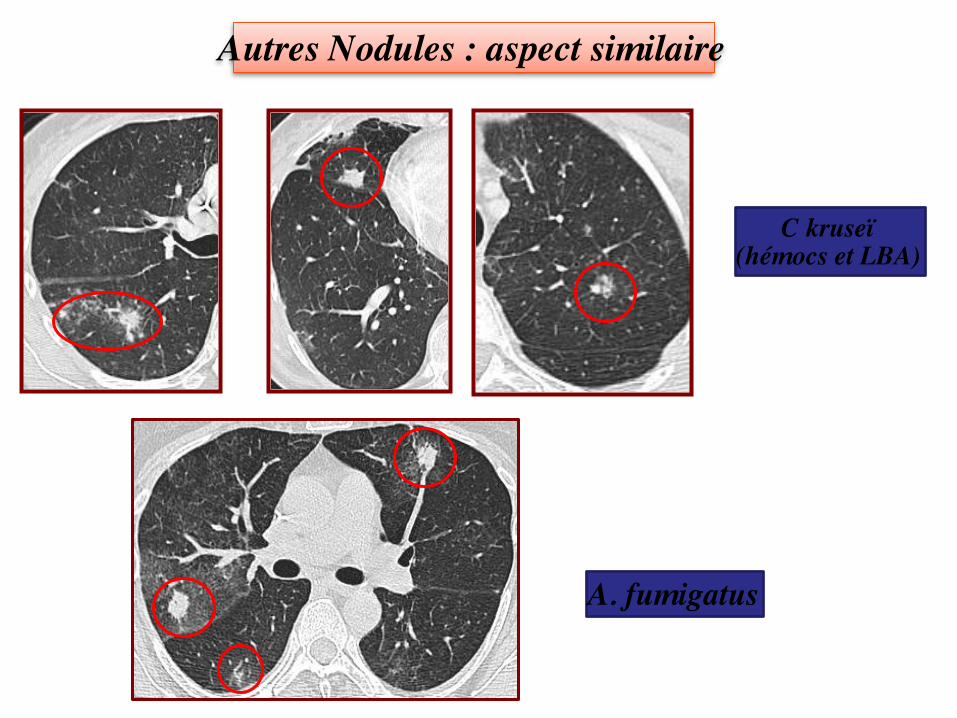
C kruseï (hémocs et LBA)
A. fumigatus
Autres Nodules : aspect similaire

Specificity of pulmonary nodules on CT scan? Examples Selected risk factors
Fungi Aspergillus Cryptococcus Zygomycetes Candida Pneumocystis
Stem cell transplant, neutropenia Disseminated disease Voriconazole prophylaxis Candidemia with septic pulmonary emboli Prolonged steroid use
Bacteria Nocardia Legionella Pseudomonas Staph. aureus
High-dose steroid use Exposure
Mycobacteria Exposure
Viruses Cytomegalovirus Adenovirus
Recipient-negative, donor-positive
Other PTLD Lung cancer Metastatic cancer Chronic GvHD Drugs (fludarabine)
Seronegative SOT recipient, small bowel transplant, pediatric transplant recipients
Kaul et al. Current Fungal InfecFon Reports 2009; 3: 45
Nodules w/wo halo

Myelome Non neutropénique Fièvre long cours + Toux
LAM rechute Neutropénie = 20 jours Fièvre 39° + Douleurs Thorax
Tuberculose LBA : - Ex direct = BAAR
- Culture = BK
Aspergillose Platelia® serum : +++ Platelia® LBA : +
Infiltrats : aspect similaire
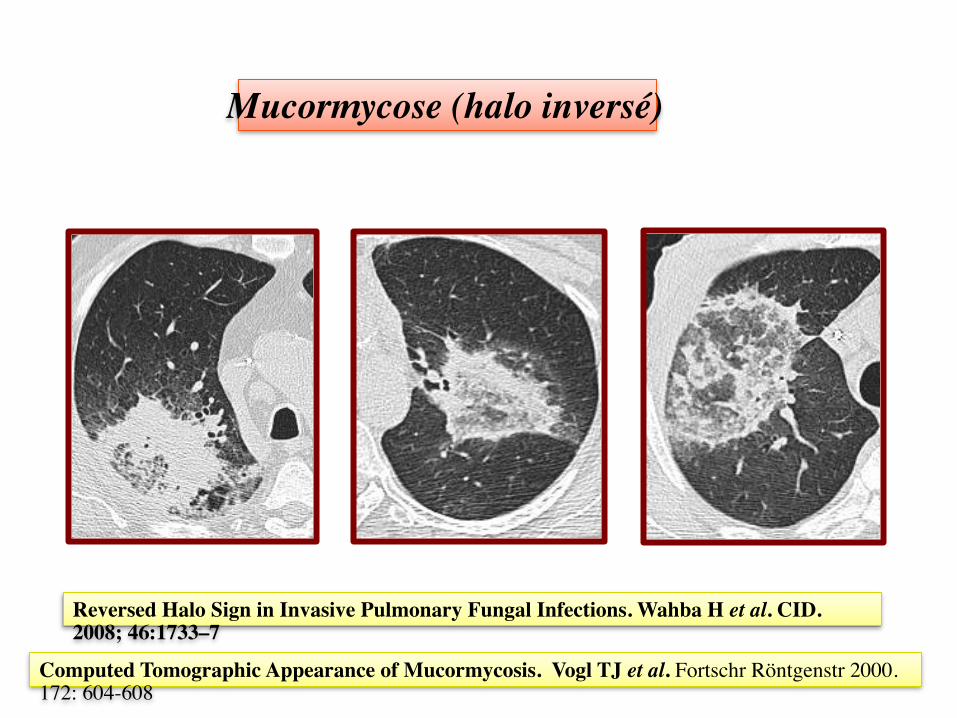
Mucormycose (halo inversé)
Reversed Halo Sign in Invasive Pulmonary Fungal Infections. Wahba H et al. CID. 2008; 46:1733–7
Computed Tomographic Appearance of Mucormycosis. Vogl TJ et al. Fortschr Röntgenstr 2000. 172: 604-608

C’est le CT scan initial qui est discriminant…
J0 J7 J15
Mucor
API
Halo
Halo inversé

The strategy for the diagnosis of invasive pulmonary aspergillosis should depend on both the underlying condition and the leucocyte count of patients with hematological malignancies. Bergeron et al. Blood. Oct 2011
Angio-invasive disease
Neutropénie
Nodule (macro) Halo
Airway-invasive disease
Non Neutropénique
Micronodules Arbre en bourgeons
Infarctus hémorragique (verre dépoli)
Broncho-pneumonie +/- Bronchiolite

Angio-invasive disease
Neutropénie
Airway-invasive disease
Non Neutropénique
Bergeron et al. Blood. Oct 2011

Bergeron et al. Blood. Oct 2011

Bergeron et al. Blood. Oct 2011

Scanner
• Doit être effectué tôt • L’interprétation doit tenir compte du
contexte: Neutropénique ou pas… • N’est pas suffisant pour faire un
diagnostic microbiologique: Fungi ou autre, quel champignon?
Questions
• Interprétation du scanner • Biomarqueurs: types et valeur

371 références

Antigènes aspergillaires et stratégie
diagnostique. Détection GM dans le serum :
Antigénémie aspergillaire
(Test Platelia®) !
M Mennink-Kersten, J Donnelly, P Verweij. Lancet infect dis. 2004, 4 : 349-57.
CD Pfeiffer, J P Fine, N Safdar. Clin Infect Dis. 2006, 42 : 1417-27.

Design Sensibilité Spécificité
Pfeiffer et al.
Clin Infect Dis. 2006,
42 : 1417-27.
1996-2005
27 études retenues
Hémato adulte 70% Greffe de CSH 82%
92%
86%
Ag GM : performance comme critère diagnostique AI
Ag GM : recommandation AII (aide au diagnostic) par ECIL-3 (A) : Good evidence to support a recommandation of use (II) Evidence from > 1 well-designed clinical trial, without randomization
Marchetti et al. BMT, 2011.

Design Sensibilité Spécificité
Leeflang et al.
Cochrane Database Syst Rev
2008
1996-2007 35 études retenues Analyse de l’effet
« seuil »
Seuil à 0,5 : 78% Seuil à 1,0 : 75% Seuil à 1,5 : 64%
81% 91% 95%
Ag : Seuil de positivité
Ag GM : recommandation AII par l’ECIL-3 :
Seuil => ≥ 0.7 (1 échantillon) ou ≥ 0.5 (2 ech. consécutifs)

La sensibilité du Platelia est altérée par administration d’antifongique actifs sur les filamenteux…
Antifungal therapy decreases sensitivity of the Aspergillus galactomannan enzyme immunoassay. K Marr et al. Clin Infect Dis. 2005 ; 40 : 1762-9.
315 pts allogreffe 46 AI (prov + prob)
Sensibilité Ag (la semaine du Dc)
52% si antifongique
89% sans antifongique (P = 0.02)
Mais, comme toujours il y a un bémol…
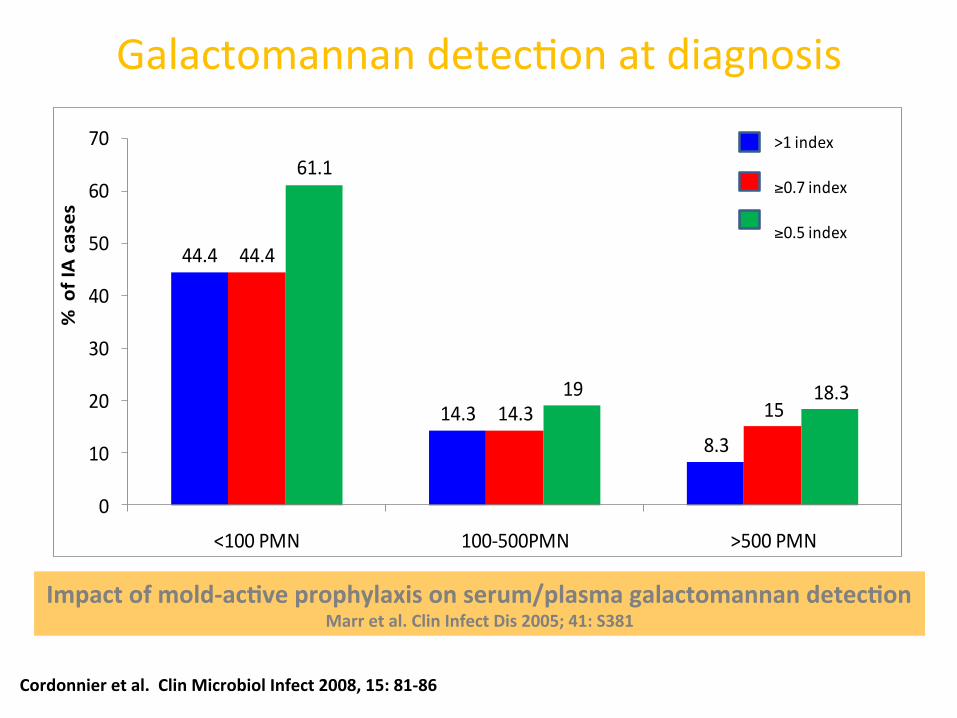
44.4
14.38.3
44.4
14.3 15
61.1
19 18.3
0
10
20
30
40
50
60
70
<100 PMN 100-‐500PMN >500 PMN
% of IA cases
>1 index
≥0.7 index
≥0.5 index
Cordonnier et al. Clin Microbiol Infect 2008, 15: 81-‐86
Galactomannan detecKon at diagnosis
Impact of mold-‐acFve prophylaxis on serum/plasma galactomannan detecFon Marr et al. Clin Infect Dis 2005; 41: S381

Antigénémie aspergillaire sérique Uniquement pour patients à haut risque aspergillaire
LAM - LAL - MDP (neutropénie ++) Allogreffe CSH (GVHd ++)
Mennink-Kersten at al. Lancet infect dis. 2004, 4 : 349-57. !
Spécificité!85% - 90%!
Dépistage!Systématique!(2 à 3 fois/semaine)!
1-2 tests consécutifs!
Recherche arguments!
Clinique!
Scannographique!
Microbiologique!
Seuil : 0.5
(dens. optique)
Sensibilité!60% - 80%!
Confirmation
diagnostique
Présence arguments!
Clinique!Scanner!
Microbiologique!
Au moins!
2 tests consécutifs!
Faire une série de tests!
(3-7 tests consécutifs)!
Faux +!Adulte : 5% - 10%!
Enfant : 15% - 50%!
Alimentation, Fungus!
Pipe-Tazo, Amoxy!
AI probable
Pfeiffer et al. Clin Infect Dis. 2006, 42 : 1417-27

Mycologie
Détection GM !
LBA et aspergilloses pulmonaires
!

LBA
Leucémies Aigues 162 API
(44 Prouv, 113 Prob, 5 Poss)
Autres Hémopathies
41 API (4 Prouv, 34 Prob, 3
Poss)
P
Ex direct + 22% (n = 35) 38% (n = 14) 0.09
Culture Myco + 26% (n = 42) 50% (n = 19) 0.015
A. fumigatus 86% (36/42) 84% (16/19) NS
Rendement mycologique (culture/direct) du LBA
203 LBA pour API (1988 - 2012)
Hémato CHU Dijon
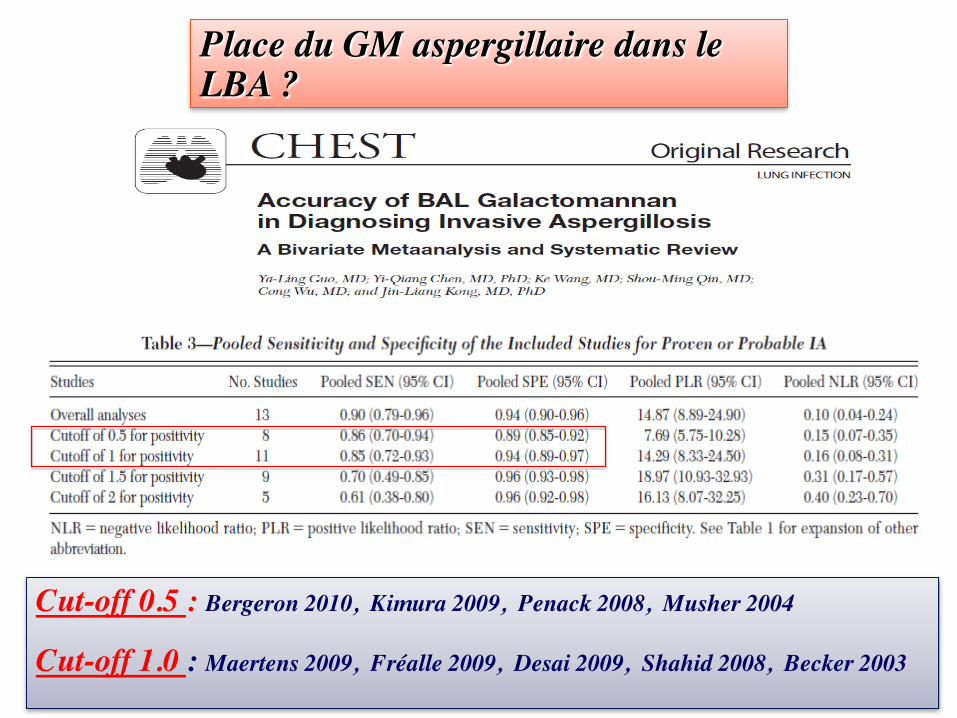
Cut-off 0.5 : Bergeron 2010, Kimura 2009, Penack 2008, Musher 2004 Cut-off 1.0 : Maertens 2009, Fréalle 2009, Desai 2009, Shahid 2008, Becker 2003
Place du GM aspergillaire dans le LBA ?
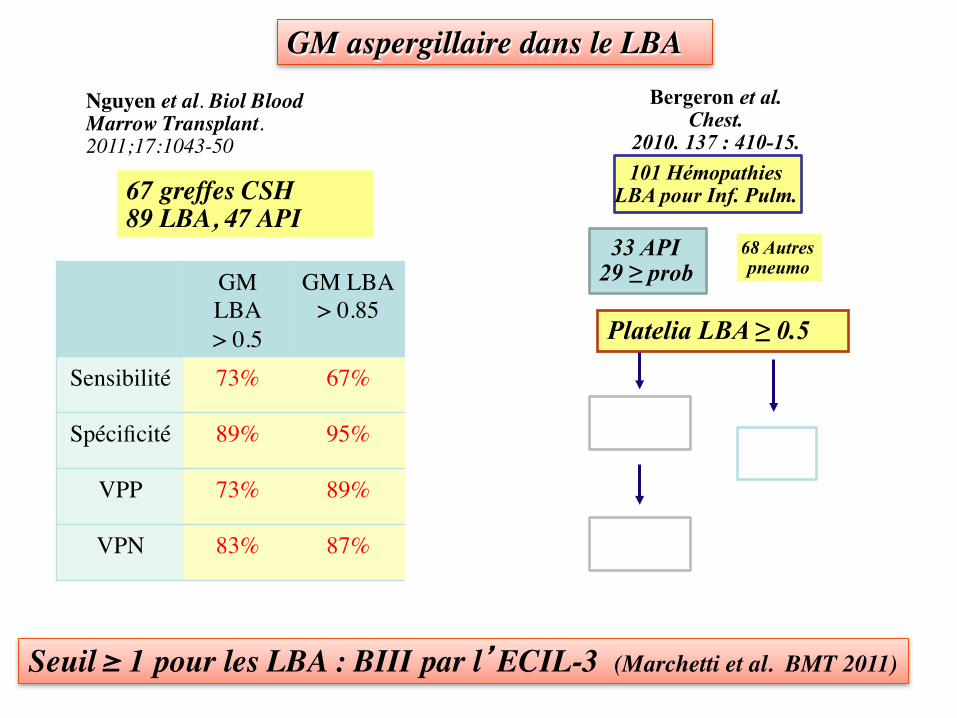
GM LBA > 0.5
GM LBA > 0.85
Sensibilité 73% 67%
Spécificité 89% 95%
VPP 73% 89%
VPN 83% 87%
Seuil ≥ 1 pour les LBA : BIII par l’ECIL-3 (Marchetti et al. BMT 2011)
67 greffes CSH 89 LBA, 47 API
Nguyen et al. Biol Blood Marrow Transplant.2011;17:1043-50
Bergeron et al. Chest.
2010. 137 : 410-15. 101 Hémopathies
LBA pour Inf. Pulm.
33 API 29 ≥ prob
68 Autres pneumo
Sensibilité 58% Faux +
4%
Platelia LBA ≥ 0.5
Spécificité 96%
GM aspergillaire dans le LBA

API Pneumopathies non API
Total
Ag LBA positif (≥ 0.5) 68 7 75
Ag LBA négatif (< 0.5) 10 65 75
Total 78 72 150
Valeur médiane Ag LBA quand il est positif 5 (0.5 - >5) 0.7 (0.5-1.7)
Performance du GM dans le LBA pour le Dc d’API chez des leucémiques en aplasie (Hémato CHU Dijon)
Mai 2000 à juin 2012 : 150 Pneumopathies (LAM et LAL en aplasie) - 78 LBA pour API Prouv/Prob (sans le critère Ag LBA) - 72 LBA pour Pneumopathies non API
Sensibilité = 87%
Spécificité = 89%
VPP = 91%
VPN = 87% Chi2 : P < 0.001 Coefficient Q de Yule = 0.97
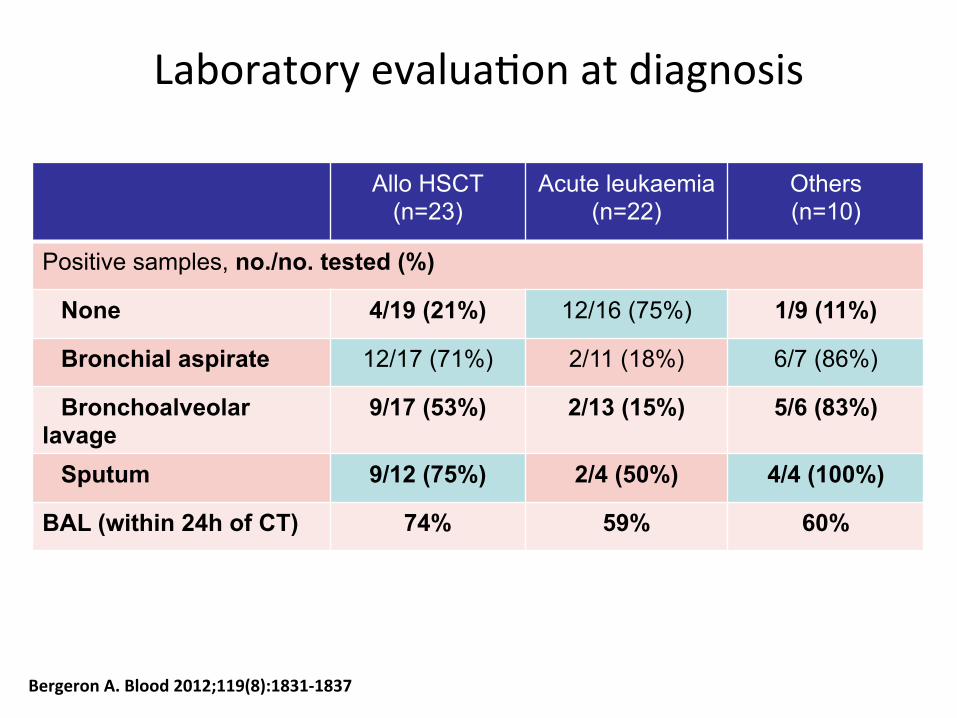
Allo HSCT (n=23)
Acute leukaemia (n=22)
Others (n=10)
Positive samples, no./no. tested (%)
None 4/19 (21%) 12/16 (75%) 1/9 (11%)
Bronchial aspirate 12/17 (71%) 2/11 (18%) 6/7 (86%)
Bronchoalveolar lavage
9/17 (53%) 2/13 (15%) 5/6 (83%)
Sputum 9/12 (75%) 2/4 (50%) 4/4 (100%)
BAL (within 24h of CT) 74% 59% 60%
Bergeron A. Blood 2012;119(8):1831-‐1837
Laboratory evaluaKon at diagnosis

GM
• Sérum: – Oui, mais attention à la sensibilité si antifongique
systémique • LBA:
– Sensibilité variable • Méthode • Contexte
• Crachat: – Alternative sensible moins invasive – Technique
Spécificité!85% - 90%!
Dépistage!Systématique!(2 à 3 fois/semaine)!
1-2 tests consécutifs!
Recherche arguments!
Clinique!
Scannographique!
Microbiologique!
Seuil : 0.5
(dens. optique)
Sensibilité!60% - 80%!
Confirmation
diagnostique
Présence arguments!
Clinique!Scanner!
Microbiologique!
Au moins!
2 tests consécutifs!
Faire une série de tests!
(3-7 tests consécutifs)!
Faux +!Adulte : 5% - 10%!
Enfant : 15% - 50%!
Alimentation, Fungus!
Pipe-Tazo, Amoxy!
AI probable

Détection Glucan dans le sérum
G-test (Fungitell®)!
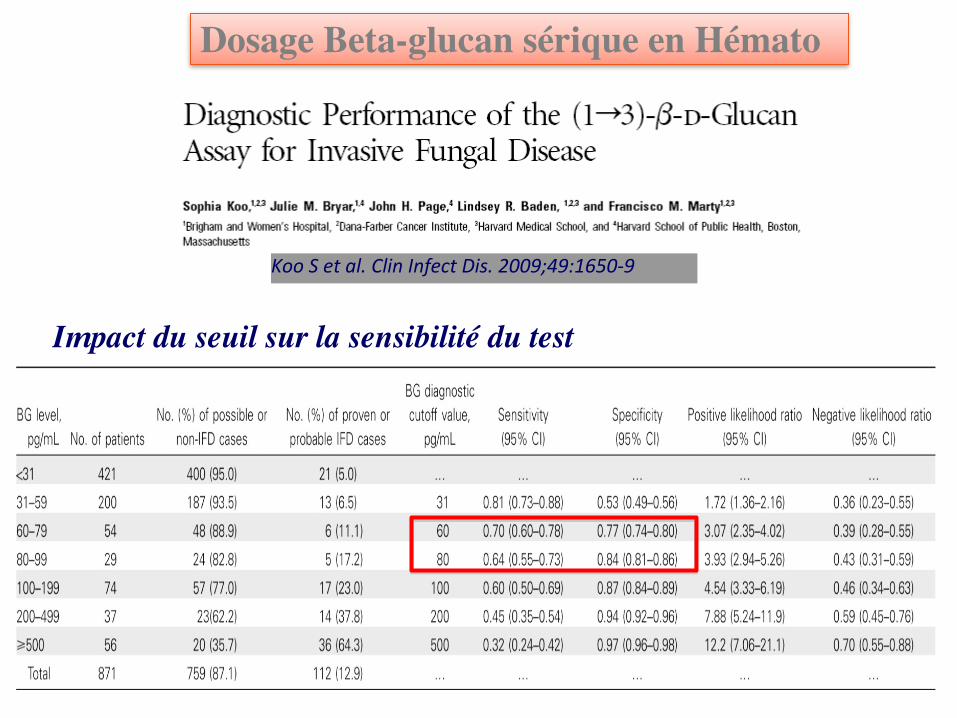
Koo S et al. Clin Infect Dis. 2009;49:1650-‐9
Impact du seuil sur la sensibilité du test
Dosage Beta-glucan sérique en Hémato
• Sensibilité plutôt faible en hématologie
• + Causes multiples de faux-positifs (comme en réanimation) : – Immunoglobulines IV – Hémodialyse – Albumine – Septicémie bactérienne – Multi-colonisation à Candida – …
Recommandation comme aide au diagnostic par l’ECIL-3 : BII (moderate evidence to support a recommendation)
Marchetti O et al. Bone Marrow Transplant 2011;1-9
Dosage Beta-glucan sérique en Hémato

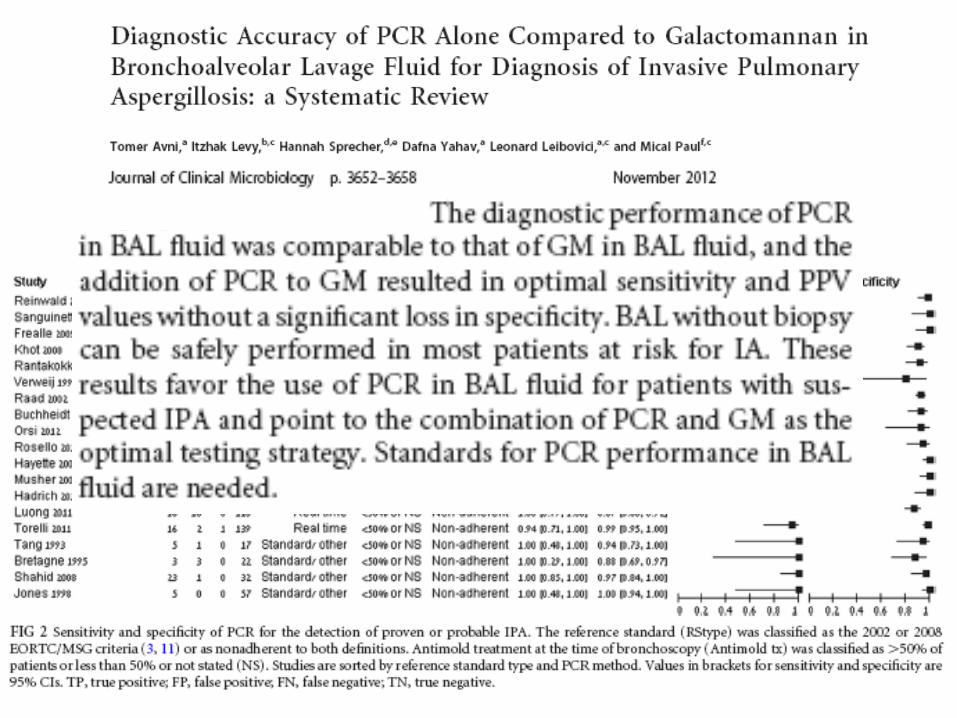
PCR

Conclusion
• Pas de vérité simple, pas d’algorithme infaillible
• Faisceau d’arguments – Cliniques – Scannographiques – Biologiques
• Analyse spécialisée des données • Connaissance de l’épidémiologie locale • Réévaluation périodique

Remerciements
• Denis Caillot • Anne Bergeron