Défaillane de la prise en harge d’un patient - orthorisq.fr · SFC SFAR 2010 : chirurgie non...
37
Défaillance de la prise en charge d’un patient sous anticoagulants ou sous antiagrégant plaquettaire : le TT antiplaquettaire ORTHORISQ, Paris – 15 novembre 2013 Professeur Jean Marc DAVY Département de Cardiologie et Maladies Vasculaires CHU de Montpellier U1046
Transcript of Défaillane de la prise en harge d’un patient - orthorisq.fr · SFC SFAR 2010 : chirurgie non...

Défaillance de la prise en charge d’un patient sous anticoagulants ou sous antiagrégant
plaquettaire : le TT antiplaquettaire ORTHORISQ, Paris – 15 novembre 2013
Professeur Jean Marc DAVY Département de Cardiologie et Maladies Vasculaires
CHU de Montpellier
U1046

Presenter disclosure informations
• Biotronik, Boston, Medtronic, Sorin, St Jude, Biosense, Spectranetics
• Astra Zeneca, Bayer, Boehringer, Daiichi-Sankyo, MSD-SP, Novartis, Pfizer, Roche, Sanofi Aventis, Servier

Une balance … individuelle
Gestion du traitement par AAP
La décision de poursuivre ces traitements ou de les arrêter en préopératoire doit prendre en compte les éléments suivants :
• risque hémorragique de la chirurgie (élevé, faible ou intermédiaire).
• risque thrombotique en cas d’arrêt des anti-plaquettaires, dépendant de – de la gravité et de la stabilité de la coronaropathie (syndrome coronaire aigu dans
les 12 derniers mois)
– des antécédents de revascularisation par chirurgie ou angioplastie,
– dans le cas d’une angioplastie, • du type d’endoprothèse utilisée (nue ou couverte),
• du nombre d’endoprothèses,
• de leur site d’implantation,
• et du délai entre la pose de l’endoprothèse et la chirurgie
SFC SFAR 2010 : chirurgie non cardiaque

Les RECOMMANDATIONS
• SFC SFAR 2010 : chirurgie non cardiaque
• ESC 2009 : non cardiac surgery (2014 update)
• ESC 2010 : myocardial revascularisation
• ESC 2011 : NST MI
• ESC 2012 : ST MI
• ESC 2013 : stable CAD

quelques règles simples sur les AAP
1. Quand peut on arrêter ?
2. Quand n’est il pas possible d’arrêter ?
3. Quand doit-on reprendre ?
4. Quels moyens de savoir si le traitement est pris ou non ?
5. Doit-on substituer (cébutid)?
6. Peut-on arrêter (définitivement ou temporairement) ? Doit-on reprendre ?
Coronarien et chirurgie non cardiaque : 3 situations
1.Le post-infarctus
2.Le post-endoprothèse
3.Le coronarien stable

Les risques : événement coronaire
• Phénomène de rebond à l’arrêt des AAP
• Tout syndrome coronaire
1. SCA NST
2. SCA ST+
3. Thrombose de stent : 15 à 45% de mortalité à 1 mois
4. Mort subite

Les agents anti-plaquettaires : AAP
• Aspirine
• Plavix : clopidogrel
• Effient : prasugrel
• Brilique : ticagrelor



Aspirine au long cours chez le coronarien stable
• Aspirin remains the cornerstone of pharmacological prevention of arterial thrombosis. It acts via irreversible inhibition of platelet cyclooxygenase-1 (COX-1) and thus thromboxane production, which is normally complete with chronic dosing ≥75 mg/day.
• Contrary to the antiplatelet effects, the gastrointestinal side-effects of aspirin increase at higher doses.
• The optimal risk–benefit ratio appears to be achieved with an aspirin dosage of 75–150 mg/day
ESC 2013 : stable CAD
La Bi TT
• Dual antiplatelet therapy combining aspirin and a thienopyridine is the standard of care
– for patients with ACS, including after the acute phase, when the patients are stabilized,
– or in SCAD patients who have undergone elective PCI
• in SCAD patients, combined antiplatelet therapy may be beneficial only in selected patients at high risk of ischaemic events,
– but cannot be recommended systematically.
ESC 2013 : stable CAD

Les nouveaux AAP : pas de place chez le coronarien stable
• Clopidogrel should thus be proposed as a second-line treatment, especially for aspirin-intolerant CVD patients.
• Prasugrel and ticagrelor are new P2Y12 antagonists that achieve greater platelet inhibition, compared with clopidogrel.
• Prasugrel and ticagrelor are both associated with a significant reduction of CV outcomes as compared with clopidogrel in ACS patients, but no clinical studies have evaluated the benefit of these drugs in SCAD patients.
• After unstable angina or myocardial infarction without ST-segment elevation when patients are stabilized and medically managed, there are no data supporting a beneficial effect of intensified platelet inhibition
ESC 2013 : stable CAD
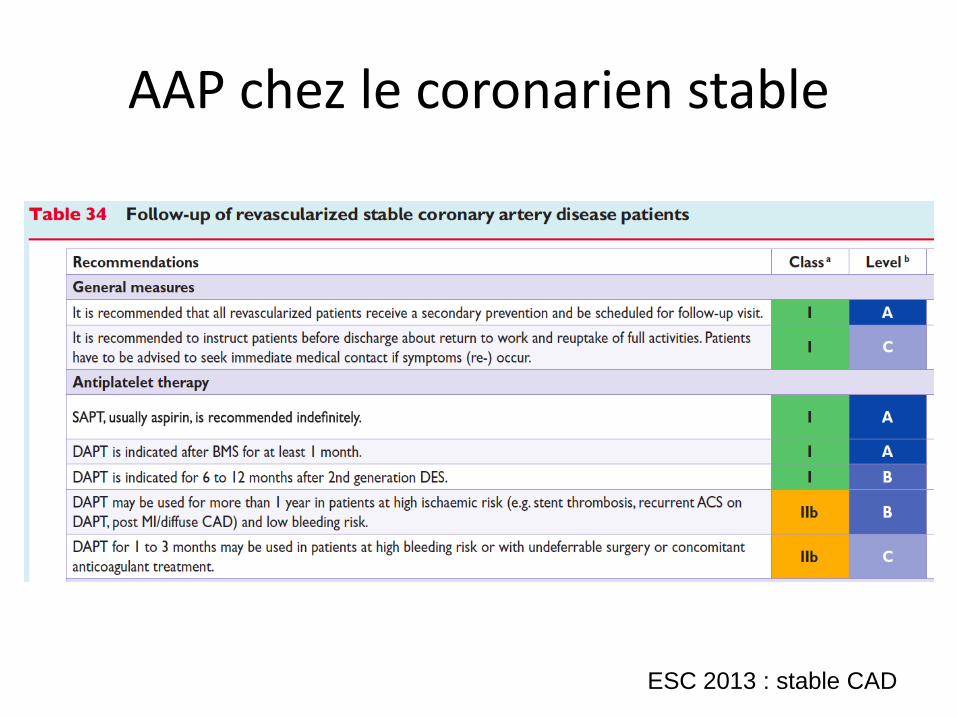
AAP chez le coronarien stable
ESC 2013 : stable CAD





Les bases de la bi TT
• La mise en place d’une endoprothèse recouverte dans les 12 mois précédents implique la poursuite de la double thérapie par AAP (GRADE 1+ Accord fort).
• La mise en place d’une endoprothèse nue implique une double anti-agrégation pendant 4 à 6 semaines (GRADE 1+ Accord fort ).
• La survenue d’un syndrome coronaire aigu implique si possible une double antiagrégation pendant un an.
SFC SFAR 2010 : chirurgie non cardiaque

Au total : 5 règles pour la durée des AAP
1. Aspirine « à vie » !
2. Bi TT AAP si possible 1 an
3. > 1 an : discutable
4. Bi TT AAP au moins 1 mois
1. après SCA
2. après stent nu,
5. Bi TT AAP plus prolongée après stent actif (3, 6 , voire 12 mois)

Les arrêts de la bi TT AAP
• Dans le cas de risque hémorragique périopératoire élevé, l’interruption du clopidogrel avec poursuite de l’aspirine peut être indiquée. (GRADE 2+ Accord fort ).
• Si le patient est sous bithérapie par AAP, il est recommandé de conserver au moins un AAP, idéalement l’aspirine, sauf contre-indication liée à un risque hémorragique chirurgical (GRADE 1+ Accord fort).
SFC SFAR 2010 : chirurgie non cardiaque

Arrêt 5 jours avant
• En cas d’arrêt d’un AAP, il est recommandé de réaliser la chirurgie après 5 jours d’arrêt, de façon à réduire le risque hémorragique tout en limitant le risque thrombotique (maximal au-delà du 8ème jour d’arrêt) (GRADE 1+ Accord faible).
SFC SFAR 2010 : chirurgie non cardiaque

Une reprise précoce, avant 8 jours
• Après la chirurgie et en concertation avec le chirurgien, il est recommandé de faire une reprise précoce du traitement AAP s’il a été interrompu.
• Une dose de charge peut être indiquée en cas de risque thrombotique élevé (GRADE 2+ Accord fort).
SFC SFAR 2010 : chirurgie non cardiaque
Le mono TT • En cas de traitement par aspirine seule, il est
recommandé de poursuivre le traitement, sauf en cas de contre-indication liée à un très haut risque hémorragique chirurgical (GRADE 1+ Accord fort).
• Si le patient reçoit du clopidogrel en monothérapie et que la chirurgie ne peut pas être réalisée sous ce médicament, il est recommandé de le remplacer par de l’aspirine, en l’absence de contre-indication (GRADE 1+ Accord fort) .
SFC SFAR 2010 : chirurgie non cardiaque

La « paresse » du cardiologue
Re-discuter régulièrement toutes les indications de bi TT AAP

Pas de TT de substitution
•Ni héparine
•Ni HBPM
•Ni Cébutid
SFC SFAR 2010 : chirurgie non cardiaque
Information du patient et traçabilité dans le dossier
• La gestion péri-opératoire des AAP doit faire l’objet d’une traçabilité dans le dossier et d’une information au patient.
SFC SFAR 2010 : chirurgie non cardiaque

Merci !

Withdrawal of chronic dual antiplatelet therapy
• Withdrawal of antiplatelet agents may lead to an increased rate of • recurrent events.112,144 Interruption of DAPT soon after stent • implantation increases the risk of subacute stent thrombosis, • which carries a particularly adverse prognosis, with mortality • varying from 15% to 45% at 1 month. Interruption of DAPT in • the case of a necessary surgical procedure .1 month after ACS • in patients without a drug-eluting stent (DES) may be reasonable

En urgence
• If interruption of DAPT becomes mandatory, such as need for
• urgent surgery (e.g. neurosurgery), or major bleeding that cannot
• be controlled by local treatment, no proven efficacious alternative
• therapy can be proposed as a substitute. Low molecular weight
• heparins (LMWHs) have been advocated, without proof of
• efficacy
Quand arrêter ? 7 jours avant
• The summary of product characteristics of all three P2Y12 inhibitors • stipulates that they have to be discontinued 7 days before • surgery. However, management of patients under DAPT who • are referred for surgical procedures depends on the degree of • emergency as well as the thrombotic and bleeding risks of the
individual • patient. Most surgical procedures can be performed under • DAPT or at least under acetylsalicylic acid alone with acceptable • rates of bleeding. A multidisciplinary approach is required
(cardiologist, • anaesthesiologist, haematologist, and surgeon) to determine • the patient’s risk and choose the best strategy.

Balance risques / bénéfices
• For NSTE-ACS patients, the risk of bleeding related to surgery • must be balanced against the risk of recurrent ischaemic events • related to discontinuation of therapy, bearing in mind the nature • of the surgery, the ischaemic risk and extent of CAD, the time • since the acute episode, and—for patients who have undergone • PCI—the time since PCI, whether or not a DES was used, and • the risk of stent thrombosis.