AMDA INTERVIEVV: ProfessorAree Valyaseyjamda.sakura.ne.jp/test/uploads/fckeditor/pdf/journal/...to...
8
| NEXVSLETTER THE ASSOCIATION OF MEDICAL DOCTORS FOR ASIA 漂い ♂♂ %〃♂ %%%%%〃♂ ♂ 惣2j;??:21j雲ツ] j ] 参 | AMDA INTERVIEVV: ProfessorAree Valyaseyj Prof.ルee Va6/asevi graduated medjcjne from Sjrjraj Ho5μta/ Meical Co//ege jn 7957. 771en,/le contjnued llj5 5tuφ/al哨eLノ雨ver5jty of Pennsy八/anja wllere lle eamed 昂5Dφ/omat Amerjcan 8oa�o臼)eiatrjcs jn 7957 and D.5c.rMe哨 jn 7959.為fier /le relumed lo T11aj/and,11e jnjtjated many sludies in tわe fje/山 of nufrjljon, c畑/dわea附l and /aler a&)ruraj commu函ty deve/opmenl. Hewa5 1/le Foundjng l:)ean o白11e Facully of Medjdrle, 尺amat昂boぷHo5μla/.For削s excdent wQrks and 5ervjces, /le /las recejved many awar(瓦jnc拓治ng哨e 01jl- 式andinR Sdentist Award from the しノ・ve�ぼQessen nMヨ51 Gemarが,1/le Natjona/ 8est尺eseardlerAwa�from t/le Natjonal尺esear(iCoun(j/ of 771a而nd and t/le Magsay5ay/xwa�lor Commu�ly£eader511φ.771oug11 /le reljred jn 7986, 11e j5 si/very actjve and worj(jng aj;con51j/tanl lo many naljona/ and jntemaljona/ orga削zaljon5. IN THIS ISSUE EDITORIAL THE CHILD SURVIVAL INDEX 1985 THAILAN[yS GROWTH MONITORING PROGRAM P2 P3 P7 MEMBERy CORNER NEWS&NOTES 四阿
Transcript of AMDA INTERVIEVV: ProfessorAree Valyaseyjamda.sakura.ne.jp/test/uploads/fckeditor/pdf/journal/...to...

|
NEXVSLETTERTHE ASSOCIATION OF MEDICAL DOCTORS FOR ASIA
漂い
♂♂ %〃♂ %%%%%〃♂ ♂惣2j;??:21j雲ツ]
j
] 参 |
AMDA INTERVIEVV:
ProfessorAree Valyaseyj
Prof.ルee Va6/asevi graduated medjcjne from Sjrjraj Ho5μta/ Meical Co//ege
jn 7957. 771en,/le contjnued llj5 5tuφ/al哨eLノ雨ver5jty of Pennsy八/anja wllere
lle eamed 昂5Dφ/omat Amerjcan 8oa�o臼)eiatrjcs jn 7957 and D.5c.rMe哨
jn 7959.為fier /le relumed lo T11aj/and,11e jnjtjated many sludies in tわe fje/山
of nufrjljon, c畑/dわea附l and /aler a&)ruraj commu函ty deve/opmenl. Hewa5
1/le Foundjng l:)ean o白11e Facully of Medjdrle, 尺amat昂boぷHo5μla/.For削s
excdent wQrks and 5ervjces, /le /las recejved many awar(瓦jnc拓治ng哨e 01jl-
式andinR Sdentist Award from the しノ・ve�ぼQessen nMヨ51 Gemarが,1/le Natjona/
8est尺eseardlerAwa�from t/le Natjonal尺esear(iCoun(j/ of 771a而nd and
t/le Magsay5ay/xwa�lor Commu�ly£eader511φ.771oug11 /le reljred jn 7986,
11e j5 si/very actjve and worj(jng aj;con51j/tanl lo many naljona/ and jntemaljona/
orga削zaljon5.
IN THIS ISSUE
EDITORIAL
THE CHILD SURVIVAL INDEX 1985
THAILAN[yS GROWTH
MONITORING PROGRAM
P2
P3
P7
MEMBERy CORNER
NEWS&NOTES
四阿

AMDA NEWSLETTER
A MONTHLY PUBLICATION OF THE ASSOCIATION OF MEDICAL DOCTORS FOR ASIA
PURPOSES
I.To publish informatlon about AMDA activities.
2.To provide a venue of communication among
AMDA members.
3.To be a forum for AMDA members to express
ideas and comments.
4.To publish articles about health care and
community development
EDITOR
NipitPiravej,刀la池nd
ASSISTANT EDITOI勿
Praphai Piravej,7?la1∃ndAntonio C. Sison,Philippines
EDITORIAL BOARDM.S.Kamath.lndia
Tsuyoshi Kawakami,Japan
Ewan Murugasu,Singapore
Christmas Tanchatchawan.Thailand
♂%%%%%%%♂♂ ♂♂♂ %%%♂ %%%%♂ %%♂♂%% %%%%%♂♂♂ ♂%%%♂♂- ♂♂♂ ♂♂♂ ♂%♂♂♂%%%%%♂♂♂ %%% ;`l .゛`、゛...ゝ゛u、ら;. ゛゛゛a゛、uu゛`゛゛%゛、、、、`.゛.....v、..、、ぷ.. ・゛g゛ .`ミ`ミミミ゛.;・zl、、l、、uごぷ..;..、、、`.、、、u、、、、胞図箔箔.iuミミミミミぶ.箔g鏝゛、忌ミ`、.`弧.`M;ぷ、、、に.゛゛゛` ^゛″;・゛、ミミ、`ぷg ゛、'、 ゛、 ″゛゛ぶF゛、n`ミM`;ぷ・l ヾ に ヾヾゝヾ ゛;.゛、IU`l`゛..;%、l、、、、....゛%゛゛、、l、、`l ゛;%%%.、l、UUご;.゛゛、、、、、、UZ;;%.w%%%%%%%%♂〃% ♂♂♂♂-%%%%%%%%♂♂♂♂♂♂♂♂%%%%%%%♂♂♂♂♂♂%%%%%%%%%% %%%%% ♂%♂♂♂♂♂♂♂♂♂4、IUU゛;.;...゛♂♂♂゛゛;゛.♂♂%%♂♂♂♂ %%%%%%%w♂♂♂♂♂♂♂♂% ♂%%♂♂♂♂♂♂♂♂♂ ♂♂ %%% ♂ ♂%%♂♂♂♂♂♂♂%%%%%%v♂♂|呂]巾几回呂
、
l゛ ゛゛JI沁/1ミミ゛泌幽幽齢辰|涵如他面函1禰面ぼ.J紬IJ面りtlj(ytd、汐嫉消叫娠JI……醵lp。|(1瞬時い4/四A陶函㈱働回二万゛゛|11
v.;♂♂ %♂ la`l♂♂♂♂゛;゛、`l゛..%..゛゛ヾ2゛`l ゛.%.IUU`%. ..;゛、U~゛%;汐、U ゛.%.IUU、IU`昌r゛; ;゛.穴`UU`、.゛%%%゛、、、IU、l`...;゛、、l、U`、、.、 ; % 、U`゛.%゛゛l、゛%%.゛%%%%%%♂ 、`.;..`、nl ;..゛゛゛l、、、 、.%゛.l`、U、....゛゛゛ゝ`;..;゛
に□☆
回
締拙以緬|面前
EDITORIAL
D「.Nipit Piravei
Happy New Year 1989 to alI AMDA members.
May the new year bring new hopes and successes
to all of you !
As the firstissue of this year, we would like
to present something special for the members. For-
tunately,we were able to get a rare opportunity to
interview Professor Aree valyasevi,one of the Mag-
saysay Award vvinners of Thailand. Though he has
PAGE 2 AMDA NEWSLETrER
retired,he is stillvely active and busy. This exdusive
interview forAMDA Newsletter was given just prior
he lefi for New Zealand for an intemational meeting。
ln the interview, ProfessorAree hastouched
many aspects of health and community development,
but above all on the topic of child health develop-
ment which is his specialty. l believe that all of us
would agree that the general well being of children
will reflect the future of the community. Howevr
we shall learn from Professor Aree that there al・ぎ・
stijltoo many risks for the children in the ruralarea
to overcome in order to grow up. Although the
discussion concerns mainly with Thailand,l am
certain that his philosophical viewpoints may be
applied to the situationsin many other Asian countries
as well。
Child health development is a hot issue.|
believe that a lot of mem・bers may feel eager to
express their ideas.So please send in, weare con-
sidering devoting one issue of the newsletter for
this topic.
The Editor
3 N0.3 JANUARY,

198555588991445578999112
666666677777777778只)
999999999999999999G)
98.3
98,4
98.6
98.7
98.7
98.7
98.7
98.7
98.8
98.8
98.8
98,8
98,8
98,9
98,9
98.9
99,0
99.0
99.0
99.0
99.1
99.1
99.2
99,2
AMDA NEWSLETTER PAGE 3
present, the life expectancy of Thai female is 65
and of Thai male is 61 years. The next to be con-
sidered may be the crude death rate; it has decreased
from 10.4 per thousand in 1970 to about 7 per
thousand recently. More interestingly, the major
causes of death have shifted from infective causes
towards non-infective causes.Among these are
cardiovascular diseases, malignancies and trauma。
contjnued on page 4
|
心
`、ノ
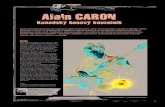
The child
survival index The basic measure of infant and child survival is the under-five mortality rate or U5MFUnumberof
deaths under the age of flve,per l,000 1ive births).A child sun/ん/a/rate perl,000 ♭,rths can be simply
calculated by subtracting the U5MR from l,000.Dividing this flgure by ten shows the percenl∂gθof
those bom who survlve to lhe age of five.The following table shows that percentage child survival rate for
allcountrles in both 1960 and 1985.
Percentage of those bom who survive to reach the age of five
AfQhanlslanMali
SierraLeone
Malawl
Guinea
EthioplaSomalia
Mozambique
BL」rkinaFaso
AngolaNiger
Centra卜AfncanRep・Chad
Guinea-Bissau
Senegal
Mauritan旧Kampuchea
Liberia
RwandaYemen
Yemen,Dem.
Bhutan
Nepal
BurundlBangladesh
日白nin
SLJdan
BOIlvia
Tanzania,U.Rep,of
Nlgeria
Halliuganda
Pakistanoman
Lao People‘sDem, Rep・Zaire
Cameroon
Togoindia
Cote dllvolre
Gha・na
LesothoFgypt
1960
62.0
63.0
60.3
63.6
65,4
70.6
70.6
69.8
61.2
65.4
68.0
69.2
67.4
68.5
68,7
69.0
78.2
69.7
75.2
62.2
62.2
70.3
70.3
74.2
73.8
69.0
70.7
71.8
75.2
68.2
70,6
77.6
72.3
62.2
76.8
74.9
72.5
69,5
71.8
68,0
77.6
79.2
70.0
1985
67.1
69,8
69.8
72.5
74.1
74.3
74.3
74.8
75,5
75.8
76.3
76.8
76.8
76.8
76.9
77.7
78.4
78.5
78.6
79.0
79.0
79.4
79.4
80.0
80.4
736780268008
01111222233〔j
888888888888
84.0
84,2
84.3
84.7
85.6
86.4
Zambla
Peru
LIbyan ArabJamahlrlya
MOrOCcolndonesla
Congo
KenyaZimbabwe
Algeria
HOnduras
Tunisla
Guatemala
Saudl ArablaNicaragua
South Africa
Turkev
lraq
日olswana
vlet NamMadagascar
Papua New Guinea
EcuadorBrazil
Burm8EI Salvador
Domlnlcan Rep・Philippines
MexlcoColombla
Svrlan Arab Rep・
」Ordan
Mongol旧ParaQuay
Lebanon
Thalland
AIbaniaCh,na
Sri Lanka
venezuela
unlted Arab F�rates
Guyana
ArgentlnaMalaysia
conljnuedfrom page 7
AMDA : 哨lhat is the present health status of
Thai people ?
Prof.valyasevi : Undoubtedly, the health status
of Thai people in general have improved remarkably
over the past 2 decades. To make it more obvious,
we may consider some of the statistics.Let's start
with the life expectancy. About 20 years ago, an
average Thai would live for about 50 years. But at
1960
77,2
76.7
73,2
73.5
76.5
75.9
79.2
81.8
73.0
76.8
74.5
77.0
70.8
79,0
80.8
74,2
77,8
82.6
76.7
81.9
75.3
81.7
84.0
77.1
79.4
80,0
86.5
86.0
85.2
78.2
78.2
84.2
86.6
90.8
85パ
83.6
79,8
88.7
88.6
76.1
90.6
92.5
89.4
1985
86.5
86.7
87.0
87,0
87.4
87.8
87.9
87.9
88.3
88,4
89,0osQ(n
(Z)CXD(7D
CXD
R)6
89.6
89.9
90,1
90,2
90.3
90.6
90.8
90,9
90,9
90.9
91,2
92.2
92.7
92.8
92.9
93.5
93.6
93.6
94.4
94.5
94。日
95.0
95.2
95,5
95,7
95,9
96.0
96.2
Kcrea,Dem.Rep. ofKorea,Rep.0fPanama
MaUrltlusUrLJguayRoman旧YugoslavlaUSSRChileTrlnldadand TobagoJamalcaKuwaltCosla RicaPor↑LJoalBulgarla
HLJngarVPolandCubaGreeceCzechoslovaklalsraelNewZealandALJstrla日elQiumGerman Dem. Rep・11alyUSAGermany,Fed.Rep. oflrelandSinQaporeSpalnunitedKingdomAustrallaFranceHong KongCanadaDenmarkNetherlandsNorwayJapanSwilzerlandFinlandSweden
1960
88.0
88.0
89.5
89.6
94.4
91.8
88.7
94.7
85,8
93,3
91,2
87.2
87.9
88.8
93.8
94.3
93.0
91.3
93.6
96.8
96.0
3756002404356575870320
75655フ/6654776367776778
9999999999999999999999

co�nuecHrom page 3
Apparently,the reasons for such a change are related
to the increase in the proportion of elderly people,
the more industrialized of the country and perhaps
also the improper adoption of sonle..Westem life styles。
Next,we may look at the infant mortality rate,
anotheraccepted important indicator of social de-
velopment.According to Ⅵ/HO recommendation,
developing countries should try to improve their
infant mortality rates to under 50 per thousand live
births.Thailand has actually achieved this target
with a figure of around 40 per thousand in 1985.
However,we should not satisfy with this figure
because it is stillabout 3 folds higher than that of
most developed countries, and we know we can
do better.And if we look closer, we would find
that perinatal death has now constituted a major
portion of infant mortality. This means that we have
to encourage antenatal monitoring and improve
our obstetrical care especially in the rural area of
the country。
Among children, the statistics also demonstrate
the marked decrease in the mortality caused by
infections diseases, especially the preventable groups
such as measles, whooping cough and diptheria.
The rapid decrease of moderate and severe protein
energy malnutrition is also encouraging. However,
the rising rate of dengue hemorrhagic fever, the
persistent high prevalence of hepatitis B virus carriers
and the emergence of HIV (Human lmmunodekiency
virus)infected patient5 are alarming and constitute
the major problems to be tackle next。
ln brief,the overall health status of Thai people
is much improved. Nevertheless, we have to under-
stand that Thailand is not a homogeneous society・
At least,the country can be divided into urban and
rural area5. 1n my point of view, the enormous
improvement in health status of Thai people is mainly
concemed with the urban people. The people in
the rural area are subjected to a lesser degree of
change.
lnfant mortalityrate of Thailand by regions
Regions lnfant mortality
(per l,000 1ive births)
North
North-east
Central(excludeBangkok)
South
Bangkok
57.8
52.8
39.0
39.4
26.5
(Source : Thai National StatisticsCouncil, 1985)
Q : ln 1988, what do you perceive as the major
advance in the health care development in Thailand !
A : l am afraid that l could not point out a single
major advance that happened so acutely in one
year. Actually, the process of health care develop-
ment in this country is rather an evolutionary process
than a revolutionary one. ln that sense, lwould point
our that the most important achievement over the
past decade was the change of the national he-lj・11
plan from a りnarrow base broad top” to a �tヲr6
desirable “broad base narrow top” system through
primary health care. ln short,the narrow base broad
top is the system that emphasize too much on the
sophisticated medical technology but pay very little
attention to basic health problems in the community・
So most of the govemmental resourcesⅥ/ere used
at the tertiary medical care level which usually serve
only few people. This was the system in the past.
Now,we have succeeded in establishing the broad
b.ase system through primary health care and the
emphasis on the local community hospitals so that
the rural people are novv rnore accessible to go-
vemmental medical services. This has brought about
the improvement in the community sanitation, the
more awareness of basic health problems and so forth.
Howeyer,with the population transition and
the changes in social structures, we are now faci,~,
more and more diseases of the elderly and malignancies.
This means that our health strategy need further
modification again to suits the futUre problems.
lthink the strategy now should be to build up the
top while maintaining the firm base. The present
medical curriculum needs modification as well. ln
health development,we can not stand stillbecause
the system is so dynamic.
Q : ln 1988, what do you think is the most im-
portant health carerelated event thal happened
in Thailand !
A : Again,this is difficult to answer exactly. Some
may say the success of cardiac transplantation, others
may raise the success of other sophisticated medical
techniques. But l would like to mention about the
National Health Assembly taken place during September
contllnued orlpage 5
4 AMDA NEWSL日‾「ER

|
|
|
co咄・nued from page 4
12-15,1988.1t was a comprehensive meeting that
brought people not only from public health and
medical sectors but also experts in education, agri-
culture,economics and social development, together
and discuss about the direction and strategy of health
development.The most important impact of this
meeting is to bring about a better awareness of
the present problems and emphasize the multi-
disciplinary approach to tackle the problems.
Q : vve all know that you have a great experience
in child health development, what d6 you think
is(are)still the majorhealth problems among Thai
children ?
A : Although l have mentioned that the mortality
fr⌒m infection is decreasing,infection is still the
k4Jing cause of child lmobidity, especially in the
rural area. This includes respiratory tract infection,
diarrhea and other viral infections. Also of important
is the recent surge in the incidence of dengue he-
morrhagic fever which is the top killer in the school
age children. Parasitic infestation is common though
it is rather chronic and indolent in nature. ln spite
of the fact that severe malnutrition has generally
disappered, we now have to face the milder degree
or subclinical form of the problem. lt i5 interesting
to say that just opposite to the rural area, we begin
to 5ee the problem of obesity in the urban children.
Q : Because you have done a brilliant work to
improve the child nutri量ionalproblem in rural area
of Thailand, whatdo you think about the present
status of this problem l
A : l would say that over the past decade, we have
quite successfully tackled down the problem of
severe malnutrition. But this is only the tip of the
iceberg.Vvhat stillpersistsis the portion under the
surface. Vve know that minor deficiency of some
nutrientscan be a problem too. A study in lndonesia
shows that in mild degree of iron deficiency with
anemia or without anemia, the child may have
impairment of motor function and he may be more
VOL.3 N0.3 1989
easy to get fatigue. lmpaired cognitive function and
short attention span in school children with mild
degree of iron deficiency have been shown in a
study performed here in Chonburi. Another example
is iodine deflciency. lodine deiiciency is not equivalent
to goitre. Vve leamed that a 5uboptimal level of
thyroxine can produce physical sluggishness, lowered
prQductivity in adult which can be reverted by adding
iodine to the diet.ln growing child and in unbom
fetus,the result of iodine deficiency can be irrepar-
able damage to both brain and body growth. For
vitamin A, mild deficiency can cause impairment
in epithelialization and immune system. ln children
with such a deficiency, they are more prone to
have respiratory tract infection and diarrhea。
The reasons l{}r the persistent nutritional problem
are certainly the poverty, but what should not be
overlooked is the problem of improper food habits.
For instance, in some part of the country, people
still(:onsume large amount of food containing phytate
and oxalate which apart from having no nutritional
value these compounds can interfere with the ab-
soption of other nutrients. Therefore,we can see
why education is so important in solving these problems.
continuedon page 6
AMDA NEWSLETTER Pj

rnntinued行om page 5
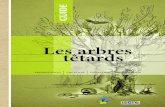
|ron,iodine, and vitamin A deficiency
`WIノ
`-
Areas of high prevalence of vitamin A deficiency and xerophthalmia ’- ・皿皿-(literally “dry eye")゛among children, 1986
0ver500,000childrenUnder 5 lose theirsighteveryyear. show si9nsofmoderatev趙min A defi(jencyand are
Withina few weeks of becoming blind60-70percent of thereforemorevulnerable to㈹ectious diseases.
these children die. Anadditional 6 to アmillion children
Africa
CentraはSouth America
South Asia
Southeast
Asia
WestAsia
EastAs厄
Prevalence is a significant
health problem
An9ola,Benin,Burkina Faso.Chad(north),
Ethiopia,Ghana(north),Kenya,Malawi,Mali,
Mauritania,Mozambique,Niger,Nigeria(north),
Sudan,Uganda,U.R.0fTanzania,Zambia
Bolivia,Brazil(northeast),曰Salvador,Haiti,
Mexico
Afghanistan,Bangladeshjndia,Nepal,SriLanka
Burma,Kampuchea,lndonesia,Lao People's
Dem.Republic,viet Nam
oman
Reports of sporadic cases callfor
close monitoring of the situation
Algeria,Botswana,BL」rundi,Lesotho,
Madagascar. Morocco,Rwanda,Somal胤
Senegal,Zimbabwe
Equador,Peru
Pakistan
Malaysia,Thailand
Egypt,|「an,|raq,JOrdan, Syria,Turkey, Yemen
China
-
゛xerophthalmia applles to all ocularma�estations of vltaminAdeficiency:
difficutty of seeing in dim light、 dryin9of the conjuctlva、foamy patches
forming on the coniuctiva、a hazyor 9ranuiar surface、 a pebblydryness
apparent on the comea、 comeal ulcer油on、andretina目eslons.Prevalence
ofthedeficlencyisgreaterformalesthanforfemales.
Souにa.・≒rl。。、、。、。4、。。、nHrnn抒ni nf wltgrnlnA dpfhencv. xerOOhthajm旧and
na帥むoり∂/わ励c加ess‘ρのpos∂/だyateりツ∂∂ΓρのgGmme�sリρpoけ
tocountnesl'. Wodd Health
oman、zation(NしノTノ845旧V.リ、February
IQQQ。nパrnnQtrQrpnnΛZHnノ目NICEF aSSeSSmentS、
i函i‾&iiiency disorders (IDD)゛in
the developing world, 1986 estimates
780 million
AT RISK“
180 m曲○∩
GOITRE
3 million
CRETINS
disability resultin9
deie;lts,slrabismus ’【squinl】,nyslagmus.spasticity,neuromuscular
weakness,endemic cretinism,and intrauterine death (spontaneous
皿1・,-4:一一ss;ssa・。iarlalrhildrQnhnm to iodine-daiiCient motherS Can-■--■■■■㎜㎜-I’
abortlarl,mlscarfisg91.Childrgn bom to ia6ina-d●licisl
- ■ ●・・jtjl●IWII●・・・・wミ=●・・-�‾j‾‾”hav白variabled白grees of ment白|retardation,ranging from the mild forms
up to marked cretinism.Prevalence of deficigncy is grealerlor females
than lor males,
゛゛Livinginaraaswherethaenvironmentisdeliciantiniodin8,solhatlhe
soil,watef, and bolh animal・and vegetable foods hav8 greatlyreduc白d
iodine content compared lo other areas.
SQぼCa. ‘jGC-SCS programた]rかleαy11roj�jIod1lrlS d6配II6rlCydlSOderSjln
iSdS哨4)jlngWQrがI,Zかj0,19S6yljQdne de5CjlalCy djI`sofdersiln
South-FggtAsia’I,WHO,?9S5.
Prevalence of anaemia゛ among
children and women, 1986
Percentageof childrenunder 5 anaemicPercentageofpregnantwomen anaemic
Percentage ofwomen 15-49 anaemic
゛Ana8mia is deiined as a haemoglobinconcenlration belowwHO
reference values ior age, sex and pregnarlcy status
SoUrce,1 Ds Ma6yer. E. arldM,4dj・elsl- ie!7man. ¨771Sprevaj6nCs�anasmjla
j‘rlがISWOrjdII, WOrld H6a泄I
SlaljISljICSQUar拍哨/.vd.38,nQ.3,
・㎜㎜■7986pQpLJばjGQ,・UNPopulatl1Qn DI'vsISjQn 6助lma飴s.
Q: Atpresent,which particulargroup of children
that need the most attention,as faras health pro-
blems are concerned !
A : l would s.ay that the more urgent attention
should be paid to the pre-school children. The pre-
school period (afterl year to about 4-5 years)can
be considered as the foundation of life'because it
is the critical time for both somatic and mental
development川f there is any disturbance happened,
it may easilycause sorTlerTloreorless permanent
changes that can severely debilitate the chil(汽future。
con面Ued on page ア
6 AMDA NEWSLETTER

|
49・2%
3rd degree
2・1%
斑
猫
VOL.3 N0.3 JANUARY,1989
64・8%
o・8%
peLj5!eM
g6e‘OZZ‘1
9961
1enu9
‐S96
Deq0ち○
70・5%
O・3%
pgq619M669'Z917‘1
寸96FjequJec)e()
‐t786Ueq0ち○
c(jntinuedfromμa卵6
The second group that we should considered is the
pregnant women because the fetal period is ajso
very crucial and we know that some degree of
nutrient deficiency for example iron deficiency is
stillcommon among the pregnant women in the
rUral area.
To attack the problem, lthink the most im-
portant step is tocreate awareness among politicians
and government. Vvithout strong political conviction,
we shall never get sufficient resources for child
development.just saying that children are the nation's
future is not enough. lt's high time policy makers
realized that the budget for child development is
a kind of investment for the country rather than
just routine expenses. 0nly after we recognize this
basic concept, should any strategic and 6perational
planning begun and can be expected to be really
effective.
Q : ln the recent years, the rapid economic growth
in-Thailand has bmught mudl pmud to most people,
do you agree that economic growth alone is ihe
majordeterminantin s)dal and health development:
A : Undoubtedly, economic growth is very important
for the development of a country. However,ljust
want to emphasize a little bit that the figure of
gross economic growth does not mean so much.
To reflect the real economic situation of a country,
we have to stress on the distribution. Actually,|
have the impression that the gap between those
who have and those who do not have is increasing
at present. So our answer is a more proper distribution
of the economic gain. ln addition, economic achieve-
ment or money alone may not be enough for health
develoβment.い/e stillneed other things forexarTlple
education.
continued on page 8
m

|
continued from page 7
Q : whahhould be the majorstrategies to booster
areal community development !
A : lfthe aim of community development is at a
better quality oHife, we would find that the essential
strategies towards that goal must be very comprehen-
sive.The emphasis on only one or two aspects will
never be sufficient. As a matter of fact,the concept
of real happiness is so broad, so variable and .philo-
sophical.To make it simple, you may agree that for
an individual money alone doesn't mean happiness.
So do the reillcommunity development. To achieve
a better quality of life,at least the community needs
better income, better education, better health care
system,appropriate social.values- and above all
better morale.l personally have an experience.
Some years ago, we had carried a community de-
velopment program in a model village in ubol(North-
eastern of Thailand).After we started the program,
substantial materialistic development occurred in
the community which at first brought to us much
satisfaction.However,when we retumed to the
village sometimes later, we found a lot of new problem5
such as gambling,drug addiction,quarrels and
even murder !
Q : At present, what do you think is the most
urgent health problem of Thailand i
A : Actually,there are stillmany important health
problems in our country,but if you talk about some-
thing urgent]would say AIDS problem。
The infection of HIV (Human lmmunodeficiency
viru5)has become a worldwide problem. Though
we have only few AIDS cases, we have at l,こ1
900 cases of asymptomatic HIVblood positive sub-
jects who are mainly intravenous drug users. XA/hat
is alarming is that the rate rises so shar口ly that it
nearly triples just in one year. lt'shigh time the
govemment brought out more effective measures
to contain the spreading of the infection。
MEMBERy CORNER
DR.Kuni lwai
Happy new year;
l have been working in Karumai Provincial
Hospital since April in 1968. Karumai is a 5mall
town,located at the northem part of lwate Pre-
fecture.Vve have 77 beds in the hospital,and l am
working as a doctor of intemal medicine.
lsee ahd talk with many patients,medical staff,o「
stafroHocal govemment everyday, and l am facing
every kind of problem, not only medical problem,
but also economical,social,familial…sometimes
l fee目t is difficultto settlethe problem.
lthink every doctor and medical staffhas the
same problems as me in his/her daily work.
lam eager to meet and to talk with you about
various problems at the Conference Hall this August.
NEWS&NOTES
The First Live-in Nationa目ntersectoral vvorkshop
on the Health of Youth will be held at the university
of Life,Meralco Avenue, Pasig,Metro Manila from
February 21-23, 1989。
The workshop is jointly sponsored by the
Ⅵ/orld Health organization, the Presidential Council
for Youth Affairs (PCYA)and the Association of
Medical Doctors for Asia(AMDA-Philippines).The
purposeof the vvorkshop is to promote direct parti-
cipation of yout'h leaders and representatives from
governmental,non‘govemmental organizations and
the media in di5cussing youth health problems and
the current responses to them in order to plan actions.
●AMDA NEWSLETTER
㎜・■|■・㎜a■・■㎜■’㎜-’-・
VOL.3N0.3 JANUARY