Revue 2007 · n°4 Acouphènes/TinnitusA single cure for tinnitus, like a cure for cancer may never...
22
R e v u e 2007 · n°4 www.entorl.com Ayant l’honneur de présenter ce 4 ème numéro d’ENT World, nous tenons à rappeler que cette revue franco-américain a été réalisée grâce à la collaboration du Professeur Samuel SELESNICK de New York Presbyterian Hospital et de nous-même. Ce 4 ème numéro concerne les tinnitus (pathologie fréquemment rencontrée dans notre spécialité) il a été réalisé en totalité par le Docteur Catherine de WAELE, nouveau Responsable d’Unité du département d’ORL de l’hôpital Américain. Il est quelquefois facile de réaliser cette revue mais souvent difficile de faire perdurer les choses dans le temps. Grâce à un travail d’équipe et une collaboration entre le service ORL de l’hôpital Américain et le service ORL du New York Presbyterian Hospital, nous avons été en mesure de finaliser ce document. Nous tenons à remercier vivement pour leur soutien la société Positive Audition et les laboratoires IPSEN, sans l'aide desquels ce numéro n'aurait pu voir le jour. Le numéro 5 sera consacré aux abstracts des différents orateurs de la prochaine journée que nous organisons le Samedi 13 Octobre sur le thème : “ORL 2007: the Best of… American Hospital of Paris”. THE JOAN AND STANFORD I. WEILL MEDICAL COLLEGE OF CORNELL UNIVERSITY W D www.nycornell.org New York, USA Professeur Samuel H. SELESNICK Anthony LaBruna MD, Co-Editor for the Facial Plastics Issue Paris, France www.american-hospital.org T here are few problems that otorhinolaryngologists treat that are as vexing yet as common as tinnitus. Over 40 million of America’s 300 million citizens suffer with tinnitus, yet a profound understanding of this entity eludes clinicians and researchers. Many patients with tinnitus are not tinnitus sufferers, but rather these individuals coexist with mild tinnitus that is only noticeable in quiet. Others are devastated by tinnitus, unable to work and saddened to the point of depression. Tinnitus may best be defined as noise in the head, and with this definition includes noise localized to one ear, both ears or anywhere in the head. The sound may be intermittent, constant, buzzing, humming, roaring, pulsatile or a myriad of other descriptive terms: most have no correlation with a specific diagnosis. Not only are manifestations of tinnitus L es acouphènes sont un véritable problème de santé publique en France. A partir de différentes études épidémiologiques, leur prévalence est évaluée à 1% à 8% de la population adulte. Une enquête portant sur plus de six cents patients acouphéniques a montré de plus que 26 % avaient une altération importante de leur qualité de vie avec des modifications notables du comportement : irritabilité, inquiétude, tension, dégradation du sommeil (Bonfils). De nombreuses études expérimentales ont été effectuées chez l’animal et chez l’homme au cours de la dernière décénie, d’où il ressort les principaux points suivants : • Les acouphènes surviennent souvent en cas de perte auditive asymétrique. La perte tonale peut n’affecter que les hautes fréquences (fréquences 3000 et 8000 Hz) et être de faible intensité (Campo). Directeur de la publication : Catherine de WAELE MD, pHD, Paris, (France) Rédacteurs en chef : Samuel H. SELESNICK, MD, FACS, New York, (USA) Stéphane de CORBIÈRE, MD, FACS, Paris, (France) Comité de rédaction : P. BONFILS (France) C. CODREANU (Roumanie) C. FRECHE (France) A. LABRUNA (USA) M. REMACLE (Belgique) J-L SARRAZIN (France) M. STEWART (USA) L. SULICA (USA) A. SZTERN (France) P. TRAN BA HUY (France) R. WARD (USA) Secrétaire de rédaction : Christine LE GALL [email protected] Editeur : Association Franco-Américaine d’ORL (Neuilly, France) Maquette : Cap Numa W D Contacts THE JOAN AND STANFORD I. WEILL MEDICAL COLLEGE OF CORNELL UNIVERSITY New York, USA www.nycornell.org Paris, France www.american-hospital.org Paris, France www.american-hospital.org Dr Catherine de WAELE (directeur de Recherche au CNRS) Unité d’ORL, Hôpital Americain de Paris, Service ORL, Hôpital Lariboisiere. LNRS, CNRS, Faculté Paris V, Paris Dr Stéphane de CORBIÈRE Rédacteur en chef Revue ENT World Hôpital Américain de Paris Editorial Editorial Acouphènes/Tinnitus Acouphènes/Tinnitus Catherine de WAELE, MD pHD Chairman of department of otorhinolaryngology Co-Editor ENT WORLD Hôpital Américain de Paris / American Hospital of Paris 63, boulevard Victor Hugo · 92200 Neuilly-sur-Seine · France Phone: 01 46 41 27 22 Fax: 01 46 41 25 47 [email protected] / [email protected] Samuel H. SELESNICK, MD FACS Co-Editor ENT WORLD Professor and Vice Chairman of the Department of Otorhinolaryngology Weill Medical College of Cornell University Attending Otorhinolaryngologist New York Weill Cornell Center of the New York Presbyterian Hospital Starr Building, Suite 541 · 520 E. 70th St New York, NY 10021 Phone: 212 746 2282 Fax: 212 746 2253 [email protected] Stéphane de CORBIERE, MD FACS, Associated member of French Academy of Surgery Editor in chief ENT WORLD Hôpital Américain de Paris / American Hospital of Paris 63, boulevard Victor Hugo · 92200 Neuilly-sur-Seine · France Phone: 01 46 41 27 22 Fax: 01 46 41 25 47 [email protected]
Transcript of Revue 2007 · n°4 Acouphènes/TinnitusA single cure for tinnitus, like a cure for cancer may never...

R e v u e 2007 · n°4www.entorl.com
Ayant l’honneur de présenter ce 4ème numéro d’ENT World, nous tenons à rappeler que cette revue franco-américain a été réaliséegrâce à la collaboration du Professeur Samuel SELESNICK de New York Presbyterian Hospital et de nous-même.
Ce 4ème numéro concerne les tinnitus (pathologie fréquemment rencontrée dans notre spécialité) il a été réalisé en totalité par leDocteur Catherine de WAELE, nouveau Responsable d’Unité du département d’ORL de l’hôpital Américain. Il est quelquefois facile deréaliser cette revue mais souvent difficile de faire perdurer les choses dans le temps. Grâce à un travail d’équipe et une collaborationentre le service ORL de l’hôpital Américain et le service ORL du New York Presbyterian Hospital, nous avons été en mesure de finaliserce document. Nous tenons à remercier vivement pour leur soutien la société Positive Audition et les laboratoires IPSEN, sans l'aidedesquels ce numéro n'aurait pu voir le jour. Le numéro 5 sera consacré aux abstracts des différents orateurs de la prochaine journéeque nous organisons le Samedi 13 Octobre sur le thème : “ORL 2007: the Best of… American Hospital of Paris”.
THE JOAN ANDSTANFORD I.
WEILL MEDICALCOLLEGE OF
CORNELLUNIVERSITY
W Dwww.nycornell.org
New York, USA
Professeur Samuel H.SELESNICK
Anthony LaBruna MD, Co-Editor for the Facial
Plastics Issue
Paris, France
www.american-hospital.org
There are few problems thatotorhinolaryngologists treat that are asvexing yet as common as tinnitus. Over
40 million of America’s 300 million citizenssuffer with tinnitus, yet a profoundunderstanding of this entity eludes cliniciansand researchers. Many patients with tinnitusare not tinnitus sufferers, but rather theseindividuals coexist with mild tinnitus that isonly noticeable in quiet. Others are devastatedby tinnitus, unable to work and saddened tothe point of depression.
Tinnitus may best be defined as noise in thehead, and with this definition includes noiselocalized to one ear, both ears or anywhere inthe head. The sound may be intermittent,constant, buzzing, humming, roaring, pulsatileor a myriad of other descriptive terms: mosthave no correlation with a specific diagnosis.Not only are manifestations of tinnitus
Les acouphènes sont un véritableproblème de santé publique en France.A partir de différentes études
épidémiologiques, leur prévalence est évaluée à1% à 8% de la population adulte. Une enquêteportant sur plus de six cents patientsacouphéniques a montré de plus que 26 %avaient une altération importante de leurqualité de vie avec des modifications notablesdu comportement : irritabilité, inquiétude,tension, dégradation du sommeil (Bonfils).
De nombreuses études expérimentales ont étéeffectuées chez l’animal et chez l’homme aucours de la dernière décénie, d’où il ressort lesprincipaux points suivants :
• Les acouphènes surviennent souvent en casde perte auditive asymétrique. La pertetonale peut n’affecter que les hautesfréquences (fréquences 3000 et 8000 Hz) etêtre de faible intensité (Campo).
Directeur de la publication :
Catherine de WAELEMD, pHD, Paris, (France)
Rédacteurs en chef :
Samuel H. SELESNICK, MD, FACS, New York, (USA)
Stéphane de CORBIÈRE,MD, FACS, Paris, (France)
Comité de rédaction :
P. BONFILS (France)
C. CODREANU (Roumanie)
C. FRECHE (France)
A. LABRUNA (USA)
M. REMACLE (Belgique)
J-L SARRAZIN (France)
M. STEWART (USA)
L. SULICA (USA)
A. SZTERN (France)
P. TRAN BA HUY (France)
R. WARD (USA)
Secrétaire de rédaction :
Christine LE [email protected]
Editeur : Association Franco-Américaine d’ORL (Neuilly, France)
Maquette : Cap Numa
W DContacts
THE JOAN ANDSTANFORD I. WEILL
MEDICAL COLLEGE OFCORNELL UNIVERSITY
New York, USAwww.nycornell.org
Paris, Francewww.american-hospital.org
Paris, Francewww.american-hospital.org
Dr Catherine de WAELE (directeur de Recherche au CNRS)
Unité d’ORL, Hôpital Americainde Paris, Service ORL, Hôpital
Lariboisiere. LNRS, CNRS,Faculté Paris V, Paris
Dr Stéphane de CORBIÈRERédacteur en chef Revue ENT World
Hôpital Américain de Paris
EditorialEditorial
Acouphènes/TinnitusAcouphènes/Tinnitus
Catherine de WAELE, MD pHD
Chairman of department of otorhinolaryngologyCo-Editor ENT WORLD
Hôpital Américain de Paris / American Hospital of Paris63, boulevard Victor Hugo · 92200 Neuilly-sur-Seine · FrancePhone: 01 46 41 27 22Fax: 01 46 41 25 [email protected] / [email protected]
Samuel H. SELESNICK, MD FACS
Co-Editor ENT WORLD
Professor and Vice Chairman of the Department of Otorhinolaryngology Weill Medical College of Cornell University Attending Otorhinolaryngologist New York Weill Cornell Center of the New York Presbyterian Hospital
Starr Building, Suite 541 · 520 E. 70th St New York, NY 10021 Phone: 212 746 2282 Fax: 212 746 2253 [email protected]
Stéphane de CORBIERE, MD FACS,
Associated member of French Academy of SurgeryEditor in chief ENT WORLD
Hôpital Américain de Paris / American Hospital of Paris 63, boulevard Victor Hugo · 92200 Neuilly-sur-Seine · France Phone: 01 46 41 27 22 Fax: 01 46 41 25 47 [email protected]

Aformerly normal sense of hearingmay, without notice, change andfalter by various causes. Loss of
hair cell function in the inner ear, theprimary cause in most such cases, may bedue to acoustic trauma, infection,intoxication, or deregulation of metabolismor genes. The impairment can be gradualor sudden, partial or total, affectinghearing level or hearing range, and mayoccur in one ear or both. The centralauditory system that receives the sensorysignals from the ear for processing anddistribution will not remain passive to anyof these changes, neither in young nor inadult patients. Instead, molecular andcellular modifications will be initiated thatmodify signal processing in the affectednetwork of nerve cells. Basic researchaims to find out along which rules thisneuroplastic remodelling proceeds andhow it may contribute to counteract themalfunctions.
In order to see how hearing impairmentmodifies the brain, scientists like to workin an experimental context that invokesstrong, clearly recognizable effects [1-2-3]. Atotal unilateral cochlear ablation inducedin an animal model such as the rat causesthe largest possible imbalance betweenthe sensory input from the left and right
ear. Under such conditions, a proteincalled GAP-43 that is associated withgrowth and plasticity of axons and theinterneuronal communication sites knownas synapses rises in the rhombencephaliccochlear nucleus of the affected side. Thisincrease is mainly localized presynaptically.Tracing the origin from which these presynaptic endings are supported led usdeeper into the brainstem to the superiorolivary complex. These cells areresponsible for building new synapses atthe ends of their axonal arborization, orstrengthening old ones, in the cochlearnucleus and were found to cholinergicneurons. In cases of partial cochlearlesions, they modify the neuronal networkonly in those parts of the cochlear nucleusthat correspond tonotopically to thelesion in the cochlea. Within the neuronalnetwork that changes as a consequence ofhearing loss, new and altered synapsesemerge on specific postsynaptic cell typesonly. We conclude that unilateraldeafening, be it partial or total, inducescomplex patterns of reconnectingneurons even in the adult auditorybrainstem. The observed changes supportthe hypothesis that the deafness-inducedchain of events is optimized to alleviateirritations of the bilateral balance ofhearing.
The plasticity responses observed in theadult auditory brainstem upon deafeningas presented here are noteworthy in severalrespects. They appear to be extensive enoughto rival lesion- and experience-dependentstructural readjustments reported to takeplace in the cortex of the mammalianforebrain, the region of the brainnormally cited as the privileged site ofneuroplasticity. Moreover, comparativelyextensive and intricate lesion-inducedsprouting responses have not yet beenreported for adult visual or somatosensorysubcortical systems.
Instead of experimentally removing sensory activation by deafening, a complementary approach may be chosenby inducing specific sensory activation.This can be accomplished by acoustic orelectrical stimulation. Either mode will,when sufficiently deviant from theprevious average activity and applied toone ear only, imprint changes to theneuronal network that necessarily resultin changes of signal processing. Thisplastic remodelling of neurons and the communication network they forminvolves the activation of genes. Amongthe indicators for the initiation ofneuronal remodelling is the expression ofso-called immediate early genes. Followingspectrally and temporally preciselydefined unilateral electrical intracochlearstimulation that corresponded in strengthto physiological acoustic stimuli andlasted for two hours, some, but not alltypes of central auditory neurons initiate
32
protean, but so are its etiologies. Whilespecific diagnostic entities leading totinnitus abound, including the presenceof a vestibular schwanomma, ototoxicinner ear damage or noise trauma toname a few, the vast majority ofpatients with tinnitus do not have thesatisfaction of identifying a specificdiagnosis that causes their symptoms. Itis becoming increasingly clear that whilean insult to the peripheral hearingapparatus may be associated with theonset of tinnitus, the reasons thattinnitus becomes chronic maybe foundcentrally. Chronic tinnitus may be moreclosely related to chronic painsyndromes that it is to chronic vertigo.Researchers in France, the United States,and in fact, around the world arestimulated by the questions of tinnituspathophysiology. There may, in fact, benumerous pathways and mechanismsthat can result in the frustrated tinnituspatient we all see in our offices. Tinnitusis not one diagnostic entity, but many.
Cures for tinnitus are rare. There is theoccasional stapedotomy surgery for anotosclerotic patient leading to tinnitusrelief, or medical therapy for a patientwith Meniere’s disease leading to tinnitusrelief. More often, therapies are intendedto lessen the appreciation of persistenttinnitus or to help the patient withtinnitus tolerate the tinnitus by bluntingnegative reactions that tinnitus canengender. Some of these interventionsare quite effective including tinnitusretraining therapy. Almost none are fastand easy.
This issue of ENT WORLD exploresthe nature of tinnitus: how it arises andhow it can be minimized if noteliminated. We are fortunate to havecontributions by researchers andclinicians who have devoted significantportions of their careers to explorationof tinnitus. Their collective work isparticularly laudable because studyingand treating tinnitus is, by its nature,
nebulous. It is the study and treatmentof a subjective symptom that is difficultto characterize and measure.
A single cure for tinnitus, like a cure for cancer may never be found sincetinnitus, like cancer, is not one problem,but an amalgamation of many.Regardless, knowledge gained in thefield of tinnitus study is gained step bystep, and is being used for the benefit ofour patients left with this annoying andcommon problem.
EditorialEditorial
• Ils sont le plus souvent de typesifflements mais peuvent êtreconstitués de bruits complexes.
• Pour cette raison, tout patientacouphénique doit avoir un bilanaudiométrique soigneux allant del’étude de l’audiométrie tonale, vocaleaux potentiels évoqués auditifs. En casde doute sur une lésion du nerf auditif,une IRM cérébrale centrée sur lesconduits auditifs internes devra êtrepratiquée (Bouccara). On tentera ausside préciser leur fréquence et leurintensité. Des questionnairesd’évaluation (Montano, Hanscombe)chez l’Homme (questionnaireanglophone : THI : francophoneTHQ) ont été validés. Ils permettentd’apprécier l’efficacité des nouveauxtraitements proposés.
• Il est maintenant admis qu’unehyperexcitabilité centrale (colliculusinférieur, cortex auditif) liée à deschangements plastiques de latransmission inhibitrice centrale(diminution de la transmissiongabaergique, glycinergique au niveaudes principaux relais auditifscentraux), se développent (Illing,Moller, Eggermont, de Waele), et sont
à l’origine des acouphènes. Ceci n’estpas sans rappeler les douleurs dumembre fantôme relatées chez lespatients après amputation.
• De nombreux modèlescomportementaux basés sur lestravaux initiaux de Jastrebof se sontdéveloppés soit chez des animauxayant ingéré du salycilate, soit soumisà des traumatismes sonores oucochléectomisés (Avan, Lobarinas,Darlington, Puel). Ces modèlespermettent d’évaluer l’effet denouvelles médications.
• De nouveaux traitements ont trouvéleur place et montré dans un certainnombre de cas leurs effets positifs :préventifs (éviter les traumatismessonores), médicamenteux parfoissuffisants (Ahmar, Azevado, Norena),la thérapie cognitive comportementale(Bonfils, Loreno) ou la prise en chargemultidisciplinaire (Ohresser) incluantpsychologues, otologistes, etaudioprothésistes). Ce type detraitement symtomatique aide lepatient à mieux supporter sonacouphène. Le rétablissement d’uneaudition symétrique à l’aide d’unappareillage prothétique performant
(Waterlot, Bizaguet, Zagolski) est aussi efficace. Finalement, des implantscochléaires de l’oreille moyenne ouinterne (Frachet,Yonehara), desstimulations magnétiques (Fregni,Londero) et électriques (de Ridder) des aires auditives primaires etsecondaires sont en cours d’évaluationaprès caractérisation sous IRM deszones corticales anormalementactivées.
En conclusion, nous ne sommes donc plus dépourvus devant un patient acouphénique : ce dernier doitêtre rassuré et différentes solutionsthérapeuthiques peuvent lui êtreproposées. Une prise en chargemultidisciplinaire est souvent utile. Les progrès en recherche fondamentaleont aidé à mieux comprendre leurorigine. Ce domaine est actuellement en pleine expansion.
“Neuroplastic remodelling of the central auditory system invoked by unilateral hearing”ROBERT-BENJAMIN ILLING
Neurobiological Research Laboratory, Department of Otorhinolaryngology, University of Freiburg, Killianstr. 5, D-79106 Freiburg, Germany. E-mail: [email protected]
Recherche fondamentale sur les acouphènesFondamental research on tinnitus
Dr Catherine de WAELE (directeur de Recherche au CNRS)
Unité d’ORL, Hôpital Americain de Paris,Service ORL, Hôpital Lariboisiere. LNRS,
CNRS, Faculté Paris V, Paris
Professeur Samuel H. SELESNICK
Anthony LaBruna MD, Co-Editor for the Facial
Plastics Issue
References:
1. Gil-Loyzaga P. 2005. Neuroplasticity in theauditory system. Rev. Laryngol. Otol. Rhinol.(Bord.). 126: 203-207.
2. Illing RB. 2001. Activity-dependent plasticity inthe adult auditory brainstem. Audiol. Neurootol.6: 319-345.
3. Illing RB, Reisch A. 2006. Specific plasticityresponses to unilaterally decreased or increasedhearing intensity in the adult cochlear nucleusand beyond. Hear. Res. 216-217: 189-197.
4. Meidinger MA, Hildebrandt-Schoenfeld H, IllingRB. 2006. Cochlear damage induces GAP-43expression in cholinergic synapses of the ratcochlear nucleus: a light and electron microscopicalstudy. Eur. J. Neurosci. 23: 3187-3199.
Figure 1

gene expression. Whereas sub-populationsof glutamatergic and glycinergic cellsrespond in all regions of the auditorybrainstem, GABAergic neurons do soonly exceptionally. Specific types ofneurons participating in majorascending pathways, the commissuralconnection of the cochlear nucleus, andof neurons that are part of thedescending auditory system respond tothe stimulation with altered geneexpression, but others do not.Altogether about half of the neuronsrespond to the stimulation with specificgene expression that eventually causesthem to change their functional role inneuronal networks evaluating thesensory information [4] The patterns ofthese changes led us to suggest thatdominant sensory activity initiates afacilitation of central pathways serving
the active ear at the expense of thoseserving the unstimulated ear.
Neuronal filters of auditory perceptionare known to exist in humans. Theyadjust to differences in the auditoryenvironment, most readily early inontogeny, but also at maturity. It hasbeen shown that hearing filters help todistinguish differences as subtle as thephonemes of the mother tongue and aforeign language by the age of sixmonths, or even before. As humanauditory cortex matures late inpostnatal development, it cannotaccount for the early formation of theselanguage-specific filters. If we acceptthat molecular and cellular changes asindicated above take place not only afterinterventions as drastic as a cochleotomy
or a sustained monotone stimulation,but also under the more delicate settingof our acoustic surrounding, we havebegun to understand how such hearingfilters are custom-made according to ourspecific auditory environment.
54
Tinnitus has two main forms,objective and subjective. Objectivetinnitus is caused by sound
generated in the body and conducted to theear, while subjective tinnitus is a phantomsensation that is caused by abnormalneural activity generated in the ear withoutany sound being involved, or more oftengenerated in the central nervous system.Subjective tinnitus is a common symptom[1]
that has many forms and it occurs withdifferent severity and its degree ofannoyance varies from minimal to havingmajor impact on the life of the individual.Tinnitus occurs often after exposure toloud sounds and it occurs almost always inindividuals with vestibular schwannoma.Ototoxic antibiotics, salicylate and othersubstances can cause tinnitus when ingested[2].
Subjective tinnitus has many similaritieswith hyperactive disorders such as neuropathic pain [3]. There are no knownobjective tests that can evaluate theexistence of tinnitus or its severity. Tinnitusis often accompanied with abnormalperception of sound such as loweredtolerance for sounds (hyperacusis) anddistortion of sound. Affective symptomssuch as depression and phonophobia oftenoccur together with severe tinnitus.
Tinnitus is perceived as a sound and thefocus of research on its causes, ondiagnosis and treatment have earlier beendirected to the ear. It was a major progressin both the understanding of thepathophysiology of tinnitus and treatmentof tinnitus when it became evident that
most forms of subjective tinnitus arecaused by changes in the function of thecentral nervous system. That tinnitus canoccur after the auditory nerve has beensevered is evidence that the anatomicallocation of the physiological abnormalitythat produce tinnitus is the central nervoussystem at least for some forms of tinnitus.There is now considerable evidence thatmany forms of severe tinnitus is caused byplastic changes in the central nervoussystem. While the expression of neuralplasticity that causes tinnitus may beinitiated by injuries or other changes in thefunction of the ear or the auditory nerve,the anatomical location of thephysiological abnormalities that causes thetinnitus is the central nervous system.Deprivation of input is a strong promoter
“Neural Plasticity in Tinnitus”AAGE R. MØLLER
University of Texas at Dallas, School of Behavioral and Brain Science, 2601 N. Floyd Rd., P.O.Box 830688, Richardson, TX 75083-0688,TEXAS, USA. E-mail: [email protected]
Figures Legend:
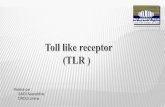
Figure 1: Electron microscopical view of theemergence of the growth-associated protein GAP-43 (asterisks) in presynaptic profiles of thecochlear nucleus on the side of a cochlear ablationin an adult rat. Red arrows point to active zones ofinterneuronal communication. a: axonal profile, n:nucleus of a neuron, m: mitochondria, v: vesicles.
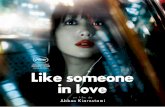
Figure 2: Expression of the gene c-fos (red) inneurons of the auditory brainstem followingelectrical intracochlear stimulation. This expressionoccurs, for instance, in neurons of the cochlearnucleus that do not support an axonal connectionsto the inferior colliculus on the other side of thebrainstem (A, blue, scale bar 20 µm), or in neuronsof the inferior colliculus that do not
contain the neurotransmitter GABA (B, green, scalebar 10 µm). If other connections such as the onefrom the superior olive to the ipsilateral cochlea (C,blue, scale bar 10 µm), or the same molecularmarker in other regions of the brainstem such asGABA (D, green, scale bar 10 µm) in the cochlearnucleus, are investigated, stimulation-dependentgene expression is found inside the characterized cells.
Tinnitus is defined as a sensation ofsound experienced in the absenceof any causal physical stimulation,
such as environmental sounds or pulsatingblood vessels. Tinnitus is typically localizedto one or both ears and for that reasonalone the structures responsible for tinnitushave been suggested to be the ears.Whereas it is clearly so that in case of one-sided hearing loss the tinnitus, if present, isgenerally localized to that ear it does notmean that it is generated in the ear. Takefor instance a lateralized neck injury, thiswill cause a unilateral tinnitus referenced tothe ear ipsilateral to the lesion. It is unlikely
that there is something wrong with the eardue to that injury. Another argumentagainst a cochlear localization of thetinnitus generator is that in al least half ofthe cases tinnitus persists after surgicalsectioning of the 8th nerve, in both humansand animals. A more precise argumentabout why tinnitus is generally notgenerated in the ear is that after noisetrauma (accounting for up to 20% oftinnitus cases) the spontaneous firing rateof auditory nerve fibers is decreased in theregion with the hearing loss compared tothat in the unaffected region. It isincommensurate with auditory physiology
that reduction in the firing rate would beequated with a sound sensation. Localizingthe tinnitus to the ears can be considered aphantom sensation not unlike that ofphantom pain after amputation. There isonly one condition under which one canargue for a cochlear generation site fortinnitus and that is following chronic low-dose application of salicylates, Here nohearing loss results, tinnitus can bedemonstrated in animal models and thespontaneous firing rate of the auditorynerve appears increased.
of expression of neural plasticity, and thatmay explain why hearing loss is oftenassociated with tinnitus and why severanceof the auditory nerve is not a good form oftreatment of tinnitus. Restoration of inputto the nervous system by wearing a hearingaid or cochlear implant is often beneficial.
The changes in the function of the nervoussystem may be in the form of altered balancebetween inhibition and excitation,remapping of structures such as the auditorycerebral cortex, or re-routing of informationsuch as in the form of activating the non-classical (extralemniscal) ascendingpathways. These pathways use the dorsalpart of the thalamus, which projects directlyto secondary and association cortices, thusbypassing the primary auditory cortex. Thedorsal thalamus has subcortical connectionsto limbic structures such as the lateralnucleus of the amygdala and that mayexplain why tinnitus can be accompanied byaffective symptoms. Unlike the classical
auditory pathways, non-classical auditorypathways receive input from other sensorysystems such as the somatosensory systemand that may explain why for exampletemporomandibular joint (TMJ) problemsoften is accompanied by tinnitus and whyelectrical stimulation of peripheral nerves orthe skin can alter tinnitus.
Many forms of treatments have been triedfor tinnitus but because of its diversepathophysiology, no one single treatmentcan be expected to be effective. Since there isno tests that can distinguish between thedifferent forms of tinnitus, the only optionfor the clinician is to try different kinds oftreatment on patients with tinnitus.
References:
1. Hoffmann, H. J. and Reed, G. W. (2004).Epidemiology of Tinnitus. In: Tinnitus: Theoryand Management. pp. 16-41. Ed. J. B. Snow. BCDecker: Hamilton.
2. Møller, A. R. (2006a). Hearing: Anatomy,Physiology, and Disorders of the AuditorySystem, 2nd Ed. Academic Press: Amsterdam.
3. Møller, A. R. (2006b). Neural plasticity anddisorders of the nervous system. CambridgeUniversity Press Cambridge.
Figure Legend:
Schematic drawing of the general outline of theascending pathways of a sensory systememphasizing the difference and the similarities
between the classical (A) and the non-classicalpathways (B). (Note that the two receptors in Bare from two different sensory systems, forinstance auditory and somatosensory). From: A.R.Møller, Sensory Systems: Anatomy and Physiology.(Academic Press, Amsterdam, 2003).
“What’s wrong with the brain in tinnitus?”JOS J. EGGERMONT
Departments of Physiology and Biophysics, and Psychology · University of Calgary, Calgary, Alberta, CanadaE-mail: [email protected]
AA
GE
R. M
ØL
LE
R
RO
BE
RT
-BE
NJA
MIN
IL
LIN
GRecherche fondamentale sur les acouphènes
Fondamental research on tinnitus
Figure 2

76
If not in the ear, where in the brain istinnitus? Tinnitus is a sensation and apercept and it is thus likely that changes inthe spontaneous firing activity of auditorycortical neurons will be involved. Suchchanges could originate in the cortex itselfor could be the result of transmittedincreased spontaneous activity originatingfrom subcortical structures. Thesestructures do not have to be auditory; thehead and neck injury cases surface again.The incidence of tinnitus is high followingthis injury as it counts for about 10% of allreported cases of tinnitus. The trigeminalnerve is the likely carrier of an abnormalmessage from the spinal cord to the dorsalcochlear nucleus in the auditory brainstem.This nucleus receives excitatory input fromthe auditory nerve fibers, inhibitory inputfrom neurons in the ventral cochlearnucleus and excitatory input via thegranule cells and parallel fibers from thevestibular periphery, dorsal column nucleiand spinal trigeminal nuclei, and centralauditory structures such as the inferiorcolliculus and the auditory cortex. The
excitatory inputs from the granule cells andparallel fibers also include feed-forwardinhibition via the cartwheel and stellatecells, and the balance between theexcitatory and inhibitory effect is likelydependent on the input level. Note that theauditory cortex does directly affect thedorsal cochlear nucleus. This is part of thegeneral corticofugal system that allowscortex to modulate the activity of nearly allsubcortical structures in a frequency-specific way.
Tonotopic map changes in primaryauditory cortex (AI) of animals are alwaysaccompanied by increases in spontaneousfiring rates and by increased spontaneousneural synchrony. Neural synchrony isdefined here as the probability that two
neurons will spontaneously fire actionpotentials occurring within a fewmilliseconds from each other. Increasedfiring rate and increased neural synchronyare two aspects of neural activity that innormal animals would occur when a soundis increased in level from just belowthreshold to just above threshold. Thus theincreases in spontaneous firing activityfollowing noise trauma may be neuralsubstrates of tinnitus. The interesting thingis that immediately after noise exposure,the spontaneous firing rates of neuronsthat were recorded from continuouslybefore, during and after the exposure tonoise, were not changed, whereas theneural synchrony was significantlyincreased immediately after the exposure.About 2 hours after the exposure, thespontaneous firing rates were also stronglyincreased, by about a factor two, and theneural synchrony was further enhanced by40-60%. It is in this respect important alsoto note that in the dorsal cochlear nucleusfollowing traumatic noise exposure thespontaneous firing rates were only
increased after 2 days. Becauseof this delay, this effect could well have beenmediated byc o r t i c o f u g a lactivity.
Is there anyevidence frommeasurementsin humans thatpoint to eitheri n c r e a s e d
spontaneous firing rate or increased neuralsynchrony as potential biological correlatesof tinnitus? The measurements that areavailable are from the positron-emissiontomography (PET) and functionalmagnetic resonance imaging (fMRI)techniques as well as from electro-encephalography (EEG) and magneto-encephalography (MEG) based recordingsof evoked cortical neural activity. PET andfMRI indirectly measure the metabolicdemands of the neurons; the greater thedemand the more active the region is inprocessing sound or generating tinnitus.Increased metabolic demand can meaneither more active neurons or that theneurons have a larger firing rate (moreprecisely had more synaptic activity).Activity of the same number of neurons,
the same firing rate but with increasedneural synchrony would not cause greatermetabolic demands. So these techniquesare insensitive to changes in neuralsynchrony. Recordings of auditory evokedpotential or magnetic fields all showincreased amplitudes in midbrain andcortex, but not in the auditory nerve andcochlear nucleus. As evoked potentials andevoked magnetic fields largely reflectneural synchrony and number of activeneurons, this points to evoked neuralsynchrony changes in the midbrain andcortex in addition to the spontaneous firingrate changes suggested by the PET andfMRI measurements.
Animal studies show quite some variationin findings that potentially reflect speciesdifferences, but also might indicate theuncertainty of the proposed neuralcorrelates for tinnitus of different etiology.I will briefly summarize findings withrespect to spontaneous neural firing andneural synchrony after noise exposure(chronic cases only) and after acuteapplication of high doses of salicylate.After noise exposure the spontaneousfiring rate of auditory nerve fibers isinvariable reduced for those in the hearingloss region. Spontaneous firing rates in thedorsal cochlear nucleus, the inferiorcolliculus (IC) and primary auditory cortex(AI) are increased. The spontaneous neuralsynchrony is increased in AI, whereas theevoked neural synchrony (measured byauditory evoked potentials, AEPs) isincreased in IC and AI. After salicylate, thespontaneous firing rate is unchanged inauditory nerve fibers (except in very highdose), is increased in ICx but decreased inICc, decreased or unchanged in AI, butincreased in AII. This suggests that incontrast to noise-induced tinnitus,salicylate-induced tinnitus only has aneural correlate in the extra-lemniscalpathway. Evoked neural synchrony (AEP)was increased in AI but the spontaneousneural synchrony as measured by cross-correlation was not. Table I compares thefindings for these two tinnitus-inducingagents.
Références:
Eggermont, JJ. (2003) Central Tinnitus. Auris NasusLarynx 30, Suppl 1: 7-12.
Eggermont JJ (2005) Tinnitus: neurobiologicalsubstrates. Drug Discovery Today 10: 1283-1290.
Eggermont JJ. and Roberts LE. (2004) TheNeuroscience of tinnitus. Trends in Neuroscience27, 676-682.
Les acouphènes chroniques sont desaffections qui peuvent survenir avecl’âge ou suite à une lésion de
partielle ou complète l’oreille interne. Cessensations peuvent devenir handicapanteset créer une véritable détresse chez lepatient, d’où l’intérêt de mettre en place desmodèles expérimentaux chez l’animal pourmieux en comprendre les mécanismes ettester les effets de traitements potentiels.Ainsi, des modèles de conditionnement ont permis de démontrer l’apparitiond’acouphènes chez le rat suite à une sectiondu nerf auditif [1], à un trauma acoustique[2-3],ou encore à l’injection d’acide salicylique [4-7].
L’une des hypothèses pour expliquerl’apparition de ces sensations fantômes estla modification au niveau central de labalance entre le système excitateur etinhibiteur. De tels changements ont pu êtremis en évidence chez l’homme par desétudes en imagerie, au niveau du colliculusinférieur (CI) [8]. Chez le rongeur, uneaugmentation importante de l’activiténeuronale, spontanée ou évoquée par un son,est mesurée au niveau du CI et du cortexauditif après lésion [9-13]. L’augmentation del’excitabilité colliculaire et corticale sembletenir en partie à la diminution del’inhibition glycinergique et GABAergiquedans les voies auditives centrales. En effet,des changements de la distribution dumarquage immunohistochimique de laglycine ont été mis en évidence dans lesnoyaux cochléaires [14] et dans le complexede l’olive supérieure [15], ainsi que desmodifications complexes de la libération etla recapture de la glycine et du GABA [16-17].De plus, une diminution de l’expression dela GAD, enzyme de synthèse du GABA, estobservée dans le CI après lésion bilatérale [18].
Nos travaux ont recherché dans unpremier temps les potentiels acteursneurochimiques responsables del’hyperexcitabilité colliculaire [19]. Des ratsadultes cochléectomisés unilatéralementont été sacrifiés à différents temps post-lésionnels (J1, J3, J8, J30, J60, J150)pour suivre les modifications induitesimmédiatement et leur éventuellerécupération à long terme. Nous avonscherché, par une méthode d’hybridation insitu en sonde chaude, d’éventuellesmodulations de l’expression des ARNmcodant les sous-unités du récepteur à laglycine (Gly�1-3, �), au GABA (GABAA�1, ‚�2, �2) et au glutamate (GluR2-3,
NR1, NR2A), de lagéphyrine, protéine d’ancragedes récepteurs à la glycine etau GABA, et de la GAD67.Nous avons mis en évidenceune diminution importante del’expression des l’ARNmcodant Gly�1 (-50%) et de laGAD67 (-30%) dans le noyaucentral du CI, du coté opposéà la lésion. Cette baisse estdétectée dès J3 et perdurejusqu’à J150 après la lésion.
Des expériencesd’immunoflurorescence ontpermis de corréler cesvariations transcriptionnellesà des variations de la quantitéde protéines à J8 et J60.Aucun changement n’a étémesuré pour les autres ARNmétudiés. La diminution deGlyalpha1 et de GAD,provoquant une desinhibitiondu CI, pourrait participer àl’augmentation du taux dedécharge spontanée des neurones du CI,enregistré après lésion de la cochlée.
A présent, nous étudions la réversionpotentielle de ces changements par desstimulations électriques du nerf auditif.Pour cela, nous avons mis au point unecochléectomie chimique à l’aide de sulfatede néomycine injecté au niveau de lafenêtre ronde, qui détruit les cellules ciliéesde la cochlée, sans dégénérescence rapidedes fibres du nerf auditif [20]. La surditéinduite en 15 jours par la néomycine a étévérifiée au niveau anatomique par des
études histologiques des cochlées et auniveau fonctionnel par des enregistrementsde potentiels évoqués auditifs. Elle conduità ce stade à la diminution de l’expressionde Gly alpha1 et de la GAD 67 au niveaudu CI. Après injection de néomycine, desélectrodes intracochléaires (fournies par lasociété Cochlear) ont été implantées. Unconnecteur, fixé sur la tête du rat, permetde la relier au système de stimulation. 15jours après, l’étude des potentiels évoquésélectriques induits nous a permis demesurer le seuil d’excitabilité du nerfauditif de chaque animal opéré. Lesstimulations sont réalisées à une intensitéde 2 fois ce seuil (demi phase 60 µs,fréquence 50 Hz), pendant 5 jours, à raisonde 22h, 8h ou 4h de stimulationquotidienne. L’animal est éveillé pendanttoute la durée de la stimulation. Nosrésultats préliminaires sont extrêmementprometteurs. Un retour à la normale del’expression de Gly alpha1 et de GAD67 aété détecté pour les stimulations de longuedurée (22h) en HIS et en immunohistochimie.Les stimulations plus courtes (8h et 4h) ontégalement pour effet d’atténuer leschangements induits par la surdité.
Les stimulations du nerf auditif aprèssurdité, partielle ou totale, permettent depromouvoir la survie des cellules duganglion spiral [21], de favoriser en partie larecapture de 2 desoxyglucose dans le CI [22]
et restaurer la tonotopie corticale [23-24].D’après nos récents résultats, unestimulation chronique de faible intensité dunerf permet de récupérer un taux normald’expression de deux protéines jouant desrôles majeurs dans l’inhibition centrale etpourrait donc constituer une voix detraitement de l’hyperexcitabilité post-lésionnelle du CI.
JOS
J. E
GG
ER
MO
NT
Recherche fondamentale sur les acouphènesFondamental research on tinnitus
“Changements neurochimiques dans le colliculus inférieur : effet d’une lésion périphérique et d’une stimulation du nerf auditif chez le rat adulte.”
CATHERINE DE WAELE, MERITXELL ARGENCE Laboratoire de Neurobiologie des Réseaux Sensorimoteurs, Faculté de Médecine Paris V - CNRS, 45 rue des Saints Pères, 75270 Paris
cedex 06, France. E-mail : [email protected]
Figure 1
Figure 2

98
Légendes des figures :
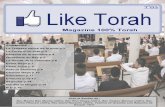
Figure 1 : Anatomie du colliculus inférieur, adapté duPaxinos.
Figure 2 : Effet d’une lésion de la cochlée et d’unestimulation du nerf auditif au niveau du colliculusinférieur (CI). A-F: autoradiographie montrant ladistribution des ARNm codant pour les sous unitésGlyalpha1 (A-D) et GAD67 (C-D), 8 jours après unecochléectomie unilatérale (A-C) et du nerf pendant22 h par jour durant 5 jours (B-D). Le coté lésé estmarqué d’une étoile. La lésion induit une diminutiondu marquage dans le contraléral (CI) du coté opposéà la lésion (flèche). Après stimulation électrique dunerf auditif, aucune asymétrie n’est plus mesurable.
Références :
1. Brozoski TJ, Bauer CA, 2005.The effect of dorsalcochlear nucleus ablation on tinnitus in rats.Hear Res; 206:227-236.
2. Bauer CA, Brozoski TJ, 2001. Assessing tinnitusand prospective tinnitus therapeutics using apsychophysical animal model. J Assoc ResOtolaryngol; 2:54-64.
3. Jastreboff PJ, Sasaki CT, 1994. An animal modelof tinnitus: a decade of development. Am J Otol;15:19-27.
4. Melcher JR, Sigalovsky IS, Guinan JJ, Jr., LevineRA, 2000. Lateralized tinnitus studied withfunctional magnetic resonance imaging:abnormal inferior colliculus activation.J Neurophysiol; 83:1058-1072.
5. Qiu C, Salvi R, Ding D, Burkard R, 2000. Innerhair cell loss leads to enhanced responseamplitudes in auditory cortex of unanesthetizedchinchillas: evidence for increased system gain.Hear Res;139:153-171.
6. Willott JF, Lu SM, 1982. Noise-induced hearingloss can alter neural coding and increaseexcitability in the central nervous system.Science; 216:1331-1334.
7. Asako M, Holt AG, Griffith RD, Buras ED,Altschuler RA, 2005. Deafness-relateddecreases in glycine-immunoreactive labeling inthe rat cochlear nucleus. J Neurosci Res;81:102-109.
8. Buras ED, Holt AG, Griffith RD, Asako M,Altschuler RA, 2006. Changes in glycineimmunoreactivity in the rat superior olivarycomplex following deafness. J Comp Neurol;494:179-189.
9. Potashner SJ, Suneja SK, Benson CG, 2000.
Altered glycinergic synaptic activities in guineapig brain stem auditory nuclei after unilateralcochlear ablation. Hear Res; 147:125-136.
10. Milbrandt JC, Holder TM, Wilson MC, Salvi RJ,Caspary DM, 2000. GAD levels and muscimolbinding in rat inferior colliculus followingacoustic trauma. Hear Res; 147:251-260.
11. Argence M, Saez I, Sassu R, Vassias I, Vidal PP,de Waele C, 2006. Modulation of inhibitory andexcitatory synaptic transmission in rat inferiorcolliculus after unilateral cochleectomy:an in situ and immunofluorescence study.Neuroscience; 141:1193-1207.
12. Zappia JJ, Altschuler RA, 1989. Evaluation of theeffect of ototopical neomycin on spiral ganglioncell density in the guinea pig. Hear Res; 40:29-37.
13. Miller AL, 2001. Effects of chronic stimulation onauditory nerve survival in ototoxically deafenedanimals. Hear Res; 151:1-14.
14. Rajan R, Irvine DR, Wise LZ, Heil P, 1993. Effectof unilateral partial cochlear lesions in adult catson the representation of lesioned andunlesioned cochleas in primary auditory cortex.J Comp Neurol; 338:17-49.
Les schémas actuels expliquant laphysiopathologie de l’acouphèneinvoquent le plus souvent des
changements d’activité dans les circuitscentraux, déclenchés par desdésafférentations d’origine périphérique.Mais expérimentalement, l’accès auxactivités centrales reste difficile, même sichez l’animal la pose d’électrodes àdemeure dans des centres tels que lecolliculus inférieur, ou encore de batteriesd’électrodes au niveau cortical estenvisageable et peut aider à effectuerquelques déductions quant aux corrélatsphysiologiques des acouphènes. Pourpouvoir utiliser avec profit des méthodesd’investigation moins invasives, parexemple, l’imagerie fonctionnelle, ou pourétudier l’efficacité de stratégiespharmacologiques, il est nécessaire dedisposer d’une situation contrôle où onpuisse dire qu’il n’y a pas d’acouphène, etd’une situation à lui comparer quicorresponde à coup sûr à la présence d’unacouphène. Les enregistrements obtenusdans les deux situations peuvent alors êtrecomparés de manière valide (par exemple,en imagerie fonctionnelle cérébrale, lesmesures de débit sanguin régional n’ont desens que différentielles).
C’est pour cela que deux approches sontparticulièrement utiles : chez l’homme, larecherche d’acouphéniques présentant desacouphènes modulables dans descirconstances précises (voir le travail deSalvi), et chez l’animal, celle qui permet a/de déclencher un acouphène aigu à volonté(administration de salicylate, exposition àun bruit traumatisant, etc) puis b/ dedétecter la présence de cet acouphèneinduit, ce qui est possible si l’animal a étépréalablement conditionné à répondre à unson présentant des caractéristiquesacoustiques qu’on imagine similaires àcelles de l’acouphène.
La base de ce dernier modèlecomportemental a été introduite parJastreboff et Coll (1) ; elle consiste à utiliserdes animaux assez évolués du point de vuecomportemental pour être conditionnables
(le cochon d’inde, par ailleurs très utile enphysiologie de l’audition, n’est hélas pasaisément conditionnable ; le rat l’estbeaucoup plus, avec en contrepartie sur leplan de l’électrophysiologie d’autrescontraintes moins favorables). Le 1er
scénario testé a été le suivant : les animauxreçoivent un conditionnement de typepavlovien. Un haut-parleur émet un soncontinu dont on peut ajuster lescaractéristiques pour le rendre similaire àun acouphène, et à certains moments le sonest interrompu brusquement. L’animal faitalors ce pour quoi il a été conditionné. Unefois traité par une injection de salicylate àune dose connue pour déclencher unacouphène temporaire chez l’homme,l’animal ne réagit plus lors de l’interruptiondu son ce qui suggère qu’il ne parvient plusà la détecter parce qu’il perçoit unesensation auditive endogène : unacouphène. Ce protocole a permis àJastreboff et Coll. (1-2), non seulement dedémontrer qu’un animal exposé à uneagression génératrice d’acouphènes chezl’homme développe bien une sensationfantôme, mais aussi de mesurer la hauteurdes acouphènes médicamenteux et leurforce subjective.
“Acouphènes : modèles comportementaux chez l’animal”PAUL AVAN
Laboratoire de Biophysique Sensorielle (EA 2667), Faculté de médecine, 28 Place Henri Dunant, 63000 Clermont-Ferrand, France. E-mail : [email protected]
Des variantes existent dans lesquellesl’animal est conditionné à sauter sur unperchoir en entendant un son. Après prisede salicylate, on détermine le nombre deréponses correctes (l’animal grimpe lorsquele son est émis) et le nombre de fauxpositifs (l’animal grimpe en l’absence de
son extérieur). Le premier index permetd’évaluer la sensibilité auditive (si l’animalest sourd il ne grimpe que s’il entend un sondont l’intensité compense sa surdité), ledeuxième, la présence d’un acouphène.Guitton et Coll (3) ont pu ainsi étudier demanière comportementale l’influence
d’antagonistes NMDA perfusés dans lecompartiment périlymphatique cochléaireet démontrer que le salicylate induit unacouphène via l’activation de récepteursNMDA.
Références :
1. Jastreboff PJ, Brennan JF, Coleman JK, SasakiCT. Phantom auditory sensation in rats: ananimal model for tinnitus. Behav Neurosci.1988;102:811-22
2. Jastreboff PJ, Sasaki CT. An animal model oftinnitus: a decade of development. Am J Otol.1994;15:19-27
3. Guitton MJ, Caston J, Ruel J, Johnson RM, PujolR, Puel JL. Salicylate induces tinnitus throughactivation of cochlear NMDA receptors. JNeurosci. 2003;23:3944-52
Légende figure :
Figure 1 : Evolution dans le temps des réponsescomportementales d’un rat traité par le salicylateet d’autres drogues administrées localement dansla périlymphe, d’après Guitton et coll., 2003.
Subjective tinnitus, a ringing,rushing or roaring sensation thataffects 12-15% of the population,
is frequently associated with hearing loss.In approximately 0.7% of thepopulation, tinnitus can be debilitatingand lead to social isolation anddepression. Although sound therapy andcounseling can provide some relief, mostpatients would prefer a treatmentapproach that totally suppresses theseintrusive and ever present phantomauditory sensations. The search for acure has been hampered by the fact thatthe biological mechanisms underlyingtinnitus are poorly understood. Since thebiological mechanisms that give rise totinnitus are difficult to study in humans,researchers have worked on developing
animal models that can reliably report onwhether they experience tinnitus or not.In the late 1980s, Jastreboff andcolleagues developed the first animalmodel of tinnitus using a lick-suppressionbehavioral paradigm that required both acontrol group and tinnitus-treatmentgroup (1). Although this paradigm proveduseful, it had two limitations. First,tinnitus could only be measured for a fewdays because the behavior extinguishedduring the tinnitus testing phase. Second,the presence of tinnitus could only beinferred by comparing the data from thetinnitus group versus the control group.Tinnitus could not be assessed inindividual animals or over a prolongedperiod of time, these two limitations areproblematic for noise-induced tinnitus
that can be permanent in some subjects,but temporary or absent in others.
To address these issues, we developed anew behavioral model, Schedule InducedPolydipsia Avoidance Conditioning (SIP-AC) that allowed us to measure tinnitusfrom individual subjects over time (2). Toimplement the technique, rats are mildlyfood deprived, but have free access towater. During the first stage of training,the food restricted animals are given afood pellet, but have to wait 60 secondsbefore the next food pellet is delivered(Figure 1). Waiting for the next food pelletcreates a displacement behavior wherebyrats begin to lick for water even thoughthey are not thirsty; this is referred to as schedule induced polydipsia (SIP).
“Do Animals Experience Tinnitus? Can They Tell Us?”EDWARD LOBARINAS, PH. D RICHARD, J. SALVI, PH.D
Center for Hearing and Deafness Department of Communicative Disorders and Sciences, University at Buffalo, NY14214, USA.
PAU
L A
VA
N
ME
RIT
XE
LL
AR
GE
NC
E, C
AT
HE
RIN
E D
E W
AE
LE
Recherche fondamentale sur les acouphènesFondamental research on tinnitus
Figure 1 Figure 2
Figure 1

1110
Afterwards, the SIP induced licking isplaced under stimuli control by applyingmild foot shock (i.e., avoidanceconditioning to sound stimuli) if the ratsattempts to drink whenever a sound ispresent. However, if the sound is off(quiet), the animal is allowed to drink forwater. After some training, animals lickat a high rate during quiet and stoplicking in the presence of any sound.
We reasoned that if the rats developedtinnitus, they should stop drinking duringquiet intervals since they would hear thephantom sounds of tinnitus. To test thishypothesis, we administered sodiumsalicylate (aspirin), a well known inducerof tinnitus. During the baseline testing,licks were high during quiet intervals(2000-4000 licks) and low during soundintervals. The same results were obtainedwhen rats were treated with a salinevehicle drug control. However, when ratswere treated with 350 mg/kg of salicylatefor two days, licks in quiet dropped tonear zero indicating that the rats wereexperiencing the phantom sound oftinnitus. When the drug administrationceased, licks in quiet returned to normallevels after 2 days. When the rat (Figure 2)was treated with 150 mg/kg of salicylatefor 2 days, licks in quiet again dropped to near zero levels suggesting that the rat was experiencing tinnitus. Whensalicylate treatment ended, licks in quietrecovered to normal baseline levels. The ability of salicylate to induce tinnituswas dose dependent. The lowest dose, 50 mg/kg, failed to induce a tinnitus-likereduction of licks in quiet while the 100 mg/kg dose caused a modestreduction. The SIP-AC method is anespecially powerful because (1) the behaviordoes not extinguish over time allowingmeasurements to be made over days orweeks and (2) measurements of tinnituscan be obtained in individual animalsbefore and after tinnitus. SIP-AC hasalso been used to evaluate noise-inducedtinnitus, which can be transient or
permanent, and quinine induced tinnitus(Lobarinas et al., 2006). In addition, wehave used SIP-AC to evaluate the efficacyof pharmaceutical compounds that havebeen proposed as treatments for tinnitus (3).
More recently, we have begun workingwith a new technique to assess tinnitus,Gap Prepulse Inhibition of the AcousticStartle (GPIAS, 4). On baseline trials, wemeasure the amplitude of the rat startlereflex to a brief (20 ms), high level (120dB SPL) noise burst that is superimposedon a low-intensity background noise (60dB SPL) (Figure 3 top). On experimentaltrials a 50 ms silent gap is embedded inthe low-level background noise prior tothe onset of the startle stimulus. If the ratperceives the silent gap in the backgroundnoise, then the amplitude of the startlereflex is reduced (Figure 3 bottom)compared to a continuous backgroundnoise (Figure 3 top). However, when ananimal experiences tinnitus, the tinnitusfills in the silent gap and the startle
response amplitude is similar to thatobserved when there is no silent gap. We have found good correspondencebetween SIP-AC and GPIAS measures of salicylate-induced tinnitus (4). A majoradvantage of GPIAS is that it requireslittle or no training and therefore it is amore efficient method of assessingtinnitus than SIP-AC.
The development of animal models hasbeen a tremendous boon to tinnitusresearch because it provides the basictools for documenting the presence orabsence of tinnitus in animal models.The presence, absence and or recovery oftinnitus in animal models providescientists with tools for identifying drugsthat could conceivably suppress tinnitus.In addition, scientists can now assess theneurophysiological and biochemicalmechanisms of tinnitus and determine ifthese biological markers are correlatedwith the onset, persistence or recovery oftinnitus (4).
References:
1. Jastreboff, P.J., Brennen, J.F., Sasaki, C.T. 1989.An animal model of tinnitus. Laryngoscope 98,280-286.
2. Lobarinas, E., Sun, W., Cushing, R., Salvi, R.2004. A novel behavioral paradigm forassessing tinnitus using schedule-inducedpolydipsia avoidance conditioning (SIP-AC).Hearing Res. 190, 109-14.
3. Lobarinas, E., Yang, G., Sun, W., Ding, D., Mirza,N., Dalby-Brown, W., Hilczmayer, E., Fitzgerald,S., Zhang, L., Salvi, R. 2006. Salicylate- andquinine-induced tinnitus and effects ofmemantine. Acta oto-laryngologica, 13-9.
4. Yang, G., Lobarinas, E., Zhang, L., Turner, J.,Stolzberg, D., Salvi, R., Sun, W. 2006 on line.Salicylate induced tinnitus: Behavioral measuresand neural activity in auditory cortex of awakerats. Hear Res.
Figures legend:
Figure 1: Rat waiting for the sound to go off(quiet) after the scheduled deliver of a food pellet.During quiet intervals, the rat licks for water.
Figure 2: High doses of sodium salicylatesuppress licks-in-quiet but have no effect on licks-in-noise.
Figure 3: Startle reflex amplitude to the startlenoise burst (upper panel) is reduced when the noseburst is preceded by a silent gap (bottom).
“An animal model for testing anti-tinnitus drugs.”CYNTHIA DARLINGTON
Department of Pharmacology and Toxicology, School of Medical Sciences, University of Otago, Dunedin, New Zealand.E-mail: [email protected]
The development and testing ofdrugs to be used for the treatmentof tinnitus requires a method of
validation of the success or failure of thepotential treatment at the experimentallevel. In many areas of pharmacology this is not a problem. The effects ofcardiovascular drugs, for example, can be determined by measuring suchindependent variables as blood pressureand stroke volume in experimentalanimals. Antidiabetic drugs are routinelytested in genetically glucose intolerantrats. However, problems in drugevaluation arise when the dependentvariables to be measured are not availableto direct observation by the researchers.This is particularly important inaudiological research. How do you ask arat if it is experiencing tinnitus?
Using paradigms developed by experimentalpsychologists, several experimentalmethods for tinnitus testing have beenused. These methods, based largely on thePavlovian model of association betweenunconditioned and conditioned stimuli asthe basis for learning, have been used withsome success. In tinnitus research, themain requirement is for the experimentalanimal, usually a rat, to be trained tomake a behavioural distinction betweenperiods of silence and periods with soundpresent. The rational for the behaviouralmeasurement is that a rat experiencingtinnitus will not make the distinctionbetween sound and silence and, in silentperiods, will continue behaving as if thesound is still present. In order to induce
the rats to perform the task, food or waterdeprivation and an aversive stimulus, e.g.electric shock, are usually employed. Insome cases, the learning paradigms usedto produce the conditioned behaviour arequite complex, albeit effective, andrequire complex patterns of training priorto the commencement of training (1). Theuse of such models, while effective, is alsolabour intensive, and in practical termsprecludes the screening of large numbersof animals, e.g. in the case of drugscreening.
In our laboratory we are using asimplified model that we developed basedupon the original work of Jastreboff(1989:2). We developed this model inorder to reduce potential stress to theanimals that may be associated with longperiods of food or water deprivation orwith high levels of electric shock. Stressreduction is important not only on ethicalgrounds; it is the case that stress mayinterfere with drug actions. Our modelrelies on the natural neophobic responseof rats, to “freeze” when confronted witha novel stimulus, in this case mild electricfoot shock.
Using a standard Skinner box with anelectric grid floor, light and speaker, ratsthat have been water deprived for 8 hoursare allowed to drink freely in the presenceof an 11kHz tone. At random intervalsthroughout the half hour training period,1 minute of silence is associated withdelivery of foot shock. The response ofthe rats is immediate and with 3 to 4
“silent” periods the rats make theassociation between silence and shock,cease drinking during the silent periodand begin drinking again as soon as thetone is turned back on. Two half-hourtraining sessions separated by 24 hoursare sufficient to establish the behaviouraldistinction between silence and tone.Following induction of tinnitus, either bysalicylate injection, noise trauma orcochlear lesionsthe testing phase of themodel commences. In this phase, an“extinction” paradigm is used to test theanimals’ response to silent periods, whenshock is not delivered. (see Fig. 1) It takesseveral testing sessions for untreated ratsto cease responding to the silence, buttreated rats fail to respond immediately,indicating the presence of tinnitus. Withdrug treatments that reduce tinnitus, the rats also continue to respond to thesilent periods. Figure 2 represents theresponse of salicylate treated rats to 15 mg/kg i.p. carbamazepine. This dose isapproximately equivalent to the doseadministered to humans for the treatmentof tinnitus, and it clearly attenuatestinnitus in the rats (3).
The equipment we use is supplied by MedAssociates, U.S.A. This equipment allowsthe simultaneous operation of severalSkinner boxes, with the potential for highvolume data acquisition. It includes thehardware and software subroutinesalthough in house programming isnecessary for individualized experimentaldesign.
ED
WA
RD
LO
BA
RIN
AS,
PH
. D R
ICH
AR
D, J
. SA
LVI,
PH
.DRecherche fondamentale sur les acouphènes
Fondamental research on tinnitus
Figure 1 Figure 2
Figure 3

1312
Les acouphènes ou perceptionsauditives fantômes sont dessensations auditives - sifflements
et/ou bourdonnements, perçues enl’absence de stimulation sonoreconcomitante dans l’environnement. Lesacouphènes touchent près de 5% de lapopulation générale et sont associés dansune grande majorité de cas à une perteauditive [1]. La prévalence des acouphènesne cesse d’augmenter en raison del’accroissement des troubles auditifs liésau vieillissement de la population et àl’exposition répétée à des environnementsbruyants et nocifs pour le système auditif(discothèques, concerts, lecteur mp3…).Une enquête récente réalisée chez desjeunes lycéens français révèle une perteauditive moyenne à 6kHz de 13 dB et laprésence d’une perte auditive supérieure à20 dB dans 25% des cas.
Les acouphènes peuvent dégraderconsidérablement la qualité de vie despatients qui en sont affectés. En outre, lesacouphènes sont très souvent associés(dans plus de 40 % des cas [1-2] à unehypersensibilité auditive ou hyperacousie- les sons d’intensité modérée sont perçuscomme étant trop forts ou douloureux.Cette “surestimation” de l’intensité des sonspeut également être très handicapantepour les sujets, les contraignant à éviter lessituations bruyantes (restaurant, concert,…).La présence simultanée de ces deuxperceptions “aberrantes” (acouphènes ethyperacousie) suggère qu’elles pourraientpartager des mécanismes en commun.
A l’heure actuelle, un consensus sembleexister au niveau des mécanismesneurophysiologiques qui sont à l’origine
des acouphènes. Il est bien connu qu’uneperte auditive induit des remaniementstrès importants des centres auditifs. Lesneurones centraux dont la fréquencecaractéristique correspond à la perte auditive
deviennent sensibles aux fréquencesadjacentes au niveau desquelles les seuilsauditifs sont normaux [3]. Les pattern dedécharges évoquées et spontanées desneurones corticaux sont également modifiés.
“Mécanismes neurophysiologiques des acouphènes et approches thérapeutiques potentielles”ARNAUD NORENA
CNRS UMR5020, Université Claude Bernard, Lyon, France.E-mail : [email protected]
References:
1. Lobarinas, E., Sun, W., Cushing, R., Salvi R.(2004) A novel behavioural paradigm forassessing tinnitus using schedule-inducedpolydipsia avoidance conditioning. HearingResearch, 190: 109-114.
2. Jastreboff, P.J. Brennen, J.F., Sasaki, C.T. (1989)An animal model of tinnitus. Laryngoscope 98:280-286.
3. Zheng, Y., Hooton, K., Smith, P., Darlington, C.Carbamazepine reduces the behaviouralmanifestations of tinnitus following salicylatetreatment in rats. “In press” in ActaOtolaryngologica (Stockholm)
Figures Legend:
Figure 1: Administration of 350 mg/kg/d salicylateresults in an increased suppression ratio indicatingthat rats receiving the drug do not respond to the
silent periods. A – acclimatization, T – training, E –extinction days.
Figure 2: Administration of 15 mg/kg/dcarbamazepine alleviates tinnitus produced by350mg/kg/d salicylate. Note: carbamazepine data hasbeen superimposed on data represented in Figure1. A – acclimatization, T – training, E – extinctiondays.
Après traumatisme auditif, le taux dedécharges augmente plus rapidement quela normale en fonction de l’intensité. Cettemodification de la fonction entrée-sortiedes neurones corticaux pourrait être uncorrélat neuronal de l’hyperacousie [4].Enfin, le pattern de l’activité spontanée estégalement modifié après un traumatismeauditif : le taux de décharges et lasynchronie des neurones corticaux sontaugmentés. Il est intéressant de souligner queles neurones présentant une augmentationde synchronie après le traumatisme auditifsont ceux dont la fréquence caractéristiqueétait située au-dessus de la fréquence duson traumatisant. En d’autres mots,l’augmentation de synchronie est manifestedans la région corticale “réorganisée” (au niveau de laquelle la fréquencecaractéristique des neurones a étémodifiée après le traumatisme auditif).Or, cette région fréquentielle correspondau “spectre” perçu des acouphènes estiméchez l’humain [5]. L’augmentation desynchronie dans la région corticaleréorganisée pourrait donc représenter uncorrélat neuronal des acouphènes.
Les modifications centrales décrites ci-dessusseraient initiées par la diminution desentrées sensorielles liée à la perte auditive,laquelle pourrait induire une diminutionde l’inhibition centrale [6]. La réduction de l’inhibition centrale serait ensuiteresponsable d’un “démasquage” deconnexions existantes (mais auparavantnon fonctionnelles) rendant compte desmodifications des champs récepteurs [3-4].
La réduction de l’inhibition centrale seraiten outre à l’origine de la modification dupattern de décharges potentiellement àl’origine des perceptions aberrantes tellesque les acouphènes et l’hyperacousie [7].Dans ce contexte, la compensation de la réduction des entrées sensorielles liée àla perte auditive devrait empêcher la miseen place des modifications centralesénumérées ci-dessus potentiellement àl’origine des acouphènes et de l’hyperacousie.Nous avons testé cette hypothèse chez deschats exposés à un traumatisme auditif (2 à4h d’exposition à un bruit de bande étroitecentré sur 5 kHz, (7). Immédiatement aprèsle traumatisme auditif les animaux étaientplacés dans un environnement enrichi enhautes fréquences de sorte que la perteauditive induite par le traumatisme auditifétait en partie “compensée” par lastimulation acoustique. Les animauxplacés dans l’environnement enrichiprésentaient une perte auditive au niveaudes fréquences proches de la fréquence duson traumatisant et une réduction de laperte auditive dans les hautes fréquences(Figure 1). L’exposition plus longue desanimaux du groupe A3 au sontraumatisant comparée à celle du groupeA2, et la variabilité interindividuellerelative aux effets d’un traumatismeauditif, rendent compte de la perteauditive légèrement plus importante auniveau de la bande de fréquences 6-8 kHzdans le groupe A3 comparée à la pertedans le groupe A2. La récupérationauditive dans les hautes fréquencespourraient être liées à une réparation”
neuronale après excitotoxicité tandis quela perte auditive au niveau des fréquencesdu son traumatisant pourrait être liée auxdommages mécaniques irréversiblesaffectant les cellules sensoriellescochléaires. Ce résultat est d’uneimportance clinique capitale car il suggèrequ’une stimulation acoustique appliquéerapidement après un traumatisme auditifpeut aider à “réparer” le système auditif.De plus, l’organisation tonotopique desanimaux placés dans l’environnementenrichi était normale (Figure 1) et lepattern des décharges inchangé. Lastimulation acoustique a donc suppriméles signes neuronaux putatifs desacouphènes [8].
En résumé, les acouphènes pourraient êtreune conséquence des remaniementscentraux qui se mettent en place après une perte auditive (laquelle induit unediminution des entrées sensorielles). Nostravaux suggèrent qu’une stimulationacoustique appliquée rapidement après untraumatisme auditif réduit la perte auditive.En outre, la compensation de la réductiondes entrées sensorielles liée à une perteauditive “installée” (présente depuis plusd’un mois et donc non réversible) pourraitréduire les acouphènes (et l’hyperacousie).La stimulation acoustique des régionsfréquentielles affectées par une perteauditive ouvre des perspectivesthérapeutiques prometteuses.
Références :
1. Fabijanska A, Rogowski M, Bartnik G, SkarzynskiH. 1999 Epidemiology of tinnitus and hyperacusisin Poland. In: Hazell, J. (Ed), Proceedings of theVIth tinnitus seminar. Cambridge, UK, p. 569-71.
2. Dauman R, Bouscau-Faure F. 2005 Assessmentand amelioration of hyperacusis in tinnituspatients. Acta Otolaryngol 125(5): 503-9.
3. Rajan R, Irvine DR, Wise LZ, Heil P. 1993 Effect ofunilateral partial cochlear lesions in adult cats onthe representation of lesioned and unlesionedcochleas in primary auditory cortex. J CompNeurol 338(1):17-49.
4a.Norena AJ, Eggermont JJ. 2003 Changes inspontaneous neural activity immediately after anacoustic trauma: implications for neuralcorrelates of tinnitus. Hear Res 183(1-2):137-53.
4b.Norena AJ, Tomita M, Eggermont JJ. 2003 Neuralchanges in cat auditory cortex after a transientpure-tone trauma. J Neurophysiol 90(4):2387-401.
5. Norena A, Micheyl C, Chery-Croze S, Collet L.
2002 Psychoacoustic characterization of thetinnitus spectrum: implications for the underlyingmechanisms of tinnitus. Audiol Neurootol7(6):358-69.
6. Milbrandt JC, Holder TM, Wilson MC, Salvi RJ,Caspary DM. 2000 GAD levels and muscimolbinding in rat inferior colliculus following acoustictrauma. Hear Res 147(1-2):251-60.
7. Norena AJ, Eggermont JJ. 2005 Enrichedacoustic environment after noise trauma reduceshearing loss and prevents cortical mapreorganization. J Neurosci 25(3): 699-705.
8. Norena AJ, Eggermont JJ. 2006 Enrichedacoustic environment after noise traumaabolishes neural signs of tinnitus. Neuroreport17(6):559-63.
Légende figure :
Figure 1 : La perte auditive (estimée à partir despotentiels auditifs précoces, une valeur négativeindique une perte auditive) est représentée dans legroupe contrôle (A1), le groupe exposé à un
traumatisme auditif puis placé dans unenvironnement acoustique non enrichi (A2) et legroupe exposé à un traumatisme auditif puis placédans un environnement acoustique enrichi (A3). Onnote que la perte auditive est réduite dans les hautesfréquences lorsque les animaux sont placés dans unenvironnement acoustique enrichi immédiatementaprès le traumatisme auditif (A3). Les cartestonotopiques “composites” (obtenues à partir deplusieurs animaux) dans le cortex auditif primairesont également représentées pour le groupe contrôle(B1), le groupe exposé à un traumatisme auditif puisplacé dans un environnement acoustique non enrichi(B2) et le groupe exposé à un traumatisme auditifpuis placé dans un environnement acoustiqueenrichi (B3). On note que le groupe placé dans unenvironnement acoustique non enrichi après letraumatisme auditif présente une réorganisation dela carte tonotopique, i.e. les hautes fréquences nesont plus représentées (B2). En revanche, le groupeplacé dans un environnement acoustique enrichiprésente une organisation tonotopique normale (B3).
AR
NA
UD
NO
RE
NA
CY
NT
HIA
DA
RL
ING
TO
NRecherche fondamentale sur les acouphènes
Fondamental research on tinnitus
Figure 1

1514
Introduction : Les acouphènes,
appelés tinnitus par les Anglo-saxons, sont des sensations de
bourdonnements ou de sifflements del’oreille qu’une personne peut ressentir endépit de l’absence de stimulationsacoustiques venant de son environnement.En fait, les acouphènes proviennent de lapersonne elle-même. Ils peuvent provenird’une seule ou des deux oreilles,bilatéralement ; enfin les acouphènespeuvent avoir une origine rétro-cochléaire. Les acouphènes doivent êtreconsidérés comme un symptôme, et noncomme une maladie.
Dans la grande majorité des cas, lesacouphènes sont rarement “objectifs”,c’est-à-dire perçus par un tiers, mêmelorsque ce dernier est muni d’unstéthoscope. La plupart du temps, lesacouphènes ne sont perçus que par lapersonne qui en souffre : ils sont donc“subjectifs”.
Les sons entendus par les personnessouffrant d’acouphènes peuvent êtrevariés : cigales, grillons, bruit de ligneélectrique à haute tension ou encorevrombissements, claquements ou bruit decocotte-minute… Plus prosaïquement, ils
peuvent se traduire par des sons gravesou aigus dont l’intensité peut êtrevariable. Si pour certaines personnes, lesacouphènes ne sont qu’un désagrément,pour beaucoup d’entre elles, ilsreprésentent un véritable handicap,parfois invalidant, surtout lorsqu’ils sontpermanents. Les personnes atteintessouffrent alors de troubles de sommeil etde la concentration.
1.Origine cochléaire ou centrale ?
L‘origine des acouphènes peut êtrecochléaire, ou rétro-cochléaire, voiremême centrale.
Origine cochléaire :
On a souvent constaté que la perteauditive et les acouphènes évoluentparallèlement. La zone de fréquences quicaractérise la perte auditive et lafréquence de l’acouphène sont souventproches. Ces constats ont amené lescliniciens à penser que l’origine desacouphènes se trouve dans le récepteurauditif périphérique : la cochlée.
La cochlée renferme l’organe de Corti(Fig.1) qui est le récepteur neuro-sensorielde l’audition. Il est constitué de deuxtypes de cellules ciliées : les cellules ciliéesinternes (CCIs) et externes (CCEs). Deuxpathologies cochléaires pourraient bienêtre à l’origine des acouphènes : ledysfonctionnement de la synapseglutamatergique entre la CCI et le nerfauditif et le dérèglement des mécanismesactifs au niveau des CCEs.
Des oscillations spontanées des CCEs,produisant des mécanismes actifs sansstimulation sonore préalable, pourraientêtre suivies de l’activation des CCIs et desfibres auditives. Le message qui partiraitvers le système nerveux serait aussi“vrai” que nature, et le sujet entendraitun sifflement calé en fréquences auniveau de la lésion des CCEs.
Origine centrale :
Une activité anormale au niveau des voiesnerveuses auditives peut également être àl’origine de l’émission d’influx nerveux enboucle au niveau des aires auditives ducerveau. Ces influx seraient alorsinterprétés comme un son par la personnesouffrant d’acouphènes. Certains auteursimpliquent le système efférent médiandans le déclenchement des oscillationsspontanées et donc des acouphènes.Toute atteinte des voies auditives(neurinomes, les tumeurs de l’angleponto-cérébelleux, et les arachnoïdites dela fosse postérieure par exemple)jusqu’aux centres sous-corticaux peutdonner des acouphènes. Pour certains,l’hallucination auditive est une formecorticale de l’acouphène.
2. Ethiologie :
Plus de 5 millions de personnes souffrentd’acouphènes. Ce sont en majorité lespersonnes de plus de 50 ans. 50 000 à 80 000 personnes consultent chaqueannée pour des problèmes d’acouphènes (1,2).
Toutefois, l’étiologie des acouphènes peutêtre multiple :
Les acouphènes peuvent survenir chez lespatients souffrant d’arthrose cervicale lesyndrome de Barré Liéou a été décrit en1926 sous le vocable de syndromecervical postérieur ou chez des patientsayant un problème circulatoire. Certainstraitements médicamenteux peuventégalement provoquer des acouphènes,comme les diurétiques, les antibiotiques(aminoglycosides), l’intoxication à laquinine ou aux salicylates par exemple.Les bourdonnements d’oreille sont unsymtôme très fréquent dans le syndromesubjectif post-commotionnel. Ils sontprésents chez 60 et 80% des patientssouffrant d’une maladie de Ménière :triade surdité, vertige, acouphènes.Finalement, les traumatismes sonoresgénèrent presque toujours des acouphènes.
Les destructions de stéréocils ou les pertesde cellules ciliées qui sont à l’origine dessurdités acquises, peuvent aussi être lefacteur déclenchant d’acouphènes. Avecle temps, les acouphènes issus de ces
traumatismes périphériques peuvent se“centraliser” et persister même aprèsdestruction des cellules de l’organe deCorti. Cela n’est pas sans rappeler lessensations douloureuses reliées aux“membres fantômes”. Dans le cadre de lasurdité professionnelle, les acouphènessurviennent dans la phase d’adaptationau bruit sous une forme fugace, et sous
une forme plus importante et définitivedans la période de surdité avancée. Ilsmanquent souvent dans la périodeintermédiaire, et ce fait a une grandeimportance car il aide le malade à ignorer son affection. Mais l’expositionchronique au bruit n’est pas la seule causede traumatisme sonore, un seul bruitimpulsionnel (explosion), suffit à entraîner
des dégâts de l’oreille interne. Des étudesen milieu industriel ont montré que laprévalence de l’acouphène était deenviron 70 % chez les ouvriers de forgesayant été exposés plus de 10 ans au bruit (3).En milieu extraprofessionnel, la prévalencedes acouphènes (essentiellement liés aubruit) chez les jeunes de 18-24 ans est de8 % (4).
“Qu’appelle-t-on acouphènes ou tinnitus ?”PIERRE CAMPO
INRS (Institut National de Recherche et de Sécurité pour la Prévention des Accidents et des Maladies Professionnelles) Département PS,Avenue de Bourgogne, BP27 54500 Vandoeuvre, France. E-mail : [email protected]
Références :
1. Dauman R. 1999. Communication. 106ème
congrès Français d’ORL 3/5 oct.. Thérapieacoustique d’habituation : pour apprendre àvivre avec des acouphènes”, Quotidien dumédecin, 21 octobre 1999.
2. Dauman R., 2000. Tinnitus and Deafness ; Rev.Prat : 15, 50(2) : 165-168.
3. Sulkowski W., Kowalska S., Lipowczan A.,Prasher D. et Raglan E., 1999. Tinnitus andimpulse noise induced hearing loss in drop-forge operators, Int J Occup Med EnvironHealth, n°12 pp.177-82.
4. Job A., Raynal M., Tricoire A., Signoret J.,Rondet P., 2000. Hearing status of French youthaged from 18 to 24 years in 1997: a cross-sectional epidemiological study in the selectioncentres of the army in Vincennes and Lyon. Rev.Epidemiol. Santé Publique. 48 (3) : 227-237.
Légendes des figures :
Figure 1 : Organe de Corti dans laquelle ondistingue les cellules ciliées externes (CCE) et lescellules ciliées internes (CCI). Dessin artistiqueprécisant l’emplacement des différentesstructures de l’organe de Corti.
Figure 2 : Organe de Corti exposé à un bruitd’intensité élevée. La première rangée de cellulesciliées externes est plus vulnérable que la secondeet la troisième. Les correspondent à des cicatricesaprès digestions des cellules ciliées endommagées.
PIE
RR
E C
AM
PO
Les données épidémiologiquesconcernant les acouphènes sontpeu nombreuses, en particulier en
France. A partir de différentes études leurprévalence est évaluée de 1% à 8% de lapopulation adulte [1]. Une étude récenteportant sur une population de 555 patientsprésentant des acouphènes chroniques,motivant une consultation spécialisée, apermis de préciser les caractéristiques desacouphènes liés à une exposition sonore detype traumatique [2]. Les principales causessont la musique amplifiée (concerts,discothèques et baladeurs) et l’utilisationd’armes à feu. La description habituellequi est faite correspond dans la grandemajorité des cas à des sifflements. Leurintensité est proportionnelle à l’importancede la perte auditive sur les fréquencesaigues. Certains travaux récents montrentqu’il existe une corrélation étroite entre lafréquence ressentie des acouphènes et laperte auditive, sous tendue par desmécanismes de réorganisation corticale [3].En pratique l’identification d’un déficit
auditif repose sur l’audiométrie tonaleconventionnelle, mais aussi l’explorationdes hautes fréquences jusqu’à 18 000 Hz(audiomètre hautes fréquences, Audioscan)dans les cas où les fréquences“conventionnelles” ne sont pas altérées.Chez les musiciens il a été proposé derechercher une atteinte cochléaire précocepar enregistrement des otoémissionsacoustiques. Les acouphènes liés au bruitsurviennent habituellement à un âge plusjeune que les autres causes. Leur prise encharge thérapeutique répond aux mêmesprincipes que celles utilisées pour les autresétiologies d’acouphènes. A un stade précoce,immédiatement après le traumatismesonore certains ont proposés un traitementde même type que celui utilisé pour lessurdités brusques. Il repose sur desassociations de différentes modalitésthérapeutiques dont l’efficacité est discutée : corticothérapie, vasodilatateurs,oxygénothérapie hyperbare, hémodilution…Les travaux de recherche portent sur desthérapeutiques délivrées “in situ” au niveau
de l’oreille interne, afin de limiter leslésions des cellules ciliées et des neuronesliées au bruit. En effet les modèlesexpérimentaux qui ont été développés ontpermis de mieux connaître les rôles dedifférents récepteurs et médiateurs de l’oreilleinterne impliqués dans les acouphènes [4].Enfin, lors des expositions au bruit, lesmodèles expérimentaux retrouvent uneréorganisation thalamo-corticale qui peutfavoriser la pérennisation de l’acouphène.La correction précoce de la perte auditiveidentifiée par une aide auditive aurait doncun effet positif à long terme [5].
Le traitement préventif de la survenue deslésions auditives liées au bruit passe pard’une part, des mesures de protectionindividuelle : limiter les expositionssonores à des intensités trop élevées,utilisation de protections (bouchons anti-bruit, casques), et d’autre part, laprotection collective dans les cadresprofessionnels et de l’environnement engénéral.
Références :
1. Acouphènes et Hyperacousie : Rapport de laSFORL, 2001.
2. Nicolas-Puel C, Charachon G, Rebillard G, BerrC, Uziel A, Puel JL. Description des acouphènesdans une population de 555 patients :
spécificités liées au traumatisme sonore. LesCahiers de l’Audition. 2006 ; 19(6) : 27-34.
3. Eggermont JJ, Roberts LE. The Neuroscience oftinnitus. Trends Neuroscience. 2004 ; 27 :676-82.
4. Guitton MJ, Wang J, Puel JL. Newpharmacological strategies to restore hearing
“Traumatisme sonore et acouphènes”DIDIER BOUCCARA
Service d’ORL, Hôpital Beaujon, AP-HP. E-mail : [email protected]
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
Figure 1Figure 2

1716
The management of patients withtinnitus involves not only precisediagnostic measures and therapeutic
interventions, but must include anunderstanding of the impact on thepatient by the clinician. How does theperson’s health condition affect his/herfunction? The self-assessment of hearingloss has become a common practice inmany ENT/Audiology practices. Patientquestionnaires such as the HearingHandicap Inventory for the Elderly (HHIE)(1)
or the Communication Profile for theHearing Impaired (2) have been designedto provide the clinician with insight intothe patient’s communication function.These tools can help identify areas inneed of rehabilitation and have beenshown to be at measuring the success oftreatment. Many self-assessment scaleshave been developed that can be used asoutcome measures of hearing aid use,quality-of-life indicator and tool forrehabilitative counseling.
As with hearing loss, patients who sufferfrom chronic tinnitus are best servedwhen the clinician has a completeunderstanding of the impact of thiscondition. Since tinnitus has been knownto significantly interfere with anindividual’s daily functioning, the moreknowledge the clinician has about thepatient’s self-perception, the better he/shewill be able to address specific patientconcerns. Individuals who suffer fromtinnitus report a variety of complaintsthat can range from mild interferencewith daily life to complete incapacitation.The use of self-assessment may be a wayto directly measure the impact of tinnituson patient function.
The importance of function is the basis forWorld Health Organization’s recentpublication, the International Classificationof Function, Disability and Health (ICF) (3).The ICF is a categorization of health andhealth-related conditions unifying theclinician’s ability to describe bodyfunctions and structures, activities andparticipations. The ICF provides aframework from which to evaluate theimpact of impairments on activities and
participation within the context of theenvironmental and personal factors thatmake up the individual. Activities refer toan execution of a task while participationrefers to performance within lifesituations. When considering tinnitus, weneed to determine if an individual isexperiencing activity limitations and/orparticipation restrictions as a result ofthis health condition.
If we view tinnitus as the health-relatedcondition, are we able to determine aspecific impairment? Can we isolate achange in either structure or function? Iftinnitus is accompanied by hearing loss,we may be able to determine site of lesionfor the hearing impairment as perhapssensory or neural, but it is more difficultto isolate the cause of the tinnitus. Whilespecific etiology may be elusive, we areable determine the impact of this health-condition on function, in particular, themanner in which tinnitus impacts anindividual’s activities and participations.
Though many believe an in-depthmedical history will provide sufficientinformation to determine the impact oftinnitus on function, most history formsin fact, are not sensitive enough toidentify both the psycho-social andperformance factors necessary to assessbehavior change. While there are a numberof tinnitus questionnaires available, fewhave been given the necessary scientificscrutiny and most lack good reliabilityand validity studies (4). Some assessmentmeasures available that have indeedwithstood the psychometric analysispreferred for clinical inclusion are toospecific in their measurement domain toaccurately determine handicap andfunction.
Alpiner and Schow (5) included the use ofthe Tinnitus Questionnaire as part of acomprehensive evaluation/remediationplan for adults with hearing loss. TheTinnitus Questionnaire was merely aseries of brief questions that described theperception of tinnitus and provided asubjective impression of the degree of theproblem. The authors provided neither
information regarding standardization ofthe instrument nor clinical experiences ofits usage.
The University of Iowa TinnitusQuestionnaire (6) was an in-depth tooldeveloped to study patient reactions totinnitus. The questionnaire consists oftwo parts: Part A, completed by thepatient, includes self-perception of thetinnitus and its associated problems: PartB, completed by the audiologist, describesmedical and audiological characteristics.This survey, while measuring the impactof tinnitus on daily life, has notundergone the psychometric statisticalanalysis to assess reliability and validityof the measurement.
A popular self-assessment measure, theTinnitus Reaction Questionnaire (7) has infact been thoroughly evaluated and foundto have strong test/retest reliability andinternal consistency. The aim of theinstrument is to assess the psychologicalimpact of tinnitus. While certainly a criticalcomponent of any self-assessment,psychological measurement is only onecomponent of handicap. The use of thisscale might not provide sufficientinformation to address the areas suggestedby the World Health Organization 3, inparticular activity limitations andparticipation restrictions.
The Tinnitus Handicap Inventory (THI), was developed specifically todetermine the handicapping effects oftinnitus. The scale is brief and easy toadminister, consisting of 25 questionswith a simple response foil of Yes/No orSometimes. Items are designed to measurethe effects of tinnitus on physical health,emotional status, and social consequenceswith items categorized into three areas:functional, emotional and catastrophicsubscales. The domains addressed in thescale provide a framework for assessmentof function. The inventory was found to haveexcellent internal consistency, test/retestreliability and convergent validity (8).
There are a number of researchers thathave chosen to us the THI in their studies
to help identify the impact of tinnitus andassess the efficacy of treatment. Berry,Gold, Frederick, Gray and Staecker (9)
chose to use the Tinnitus HandicapInventory as a measurement tool in theirstudy of patient-based outcomesfollowing tinnitus retraining therapy(TRT), a counseling-infused method oftreatment reported by Jastreboff &Jastreboff (10). The authors demonstratedsignificant improvement on the subscalesof the THI following their treatmentregime and confirmed the validity of theuse of the inventory as an outcomemeasure. Handscomb (11) used the THI toinvestigate the impact of tinnitus onpeople who may not be severely affectedby the condition. Her research suggestedthat even those with reported minimaltinnitus identified the lack of control overand the inability to escape tinnitus asbeing significant issues. The instrumentwas chosen because of its ability toquantify the handicapping effects oftinnitus and its validation in theliterature.
When looking once again at the WorldHealth Organization’s InternationalClassification of Function Disability andHealth 3, the THI can be a useful tool toevaluate the presence of activitylimitations and participation restrictions.Review of the specific items in the scale, in particular the items containedwithin the function sub-scale, confirmstheir relationship to patient function. A question such as F7) “Because of yourtinnitus do you have trouble fallingasleep at night?” illustrates the possiblepresence of an activity limitation.Question F13) “Does your tinnitusinterfere with your job or householdresponsibilities?” highlights participationrestrictions.
The ICF framework helps the clinicianassess the impact of tinnitus on individualfunction. The use of self-assessmentmeasures can enable a pre- and post-measurement of the selected treatment onthe reduction of impairment, activitylimitation and participation restriction.
The inclusion of any assessment tool requirescareful selection and implementation. A review of the literature regardingavailable questionnaires and scales isimportant before adding self-assessmentmeasuring to your tinnitus evaluationprotocol. While there are a number ofmeasurement tools available, few havehad the psychometric validation as seenin the Tinnitus Handicap Inventory. Thescale has a good research history and theitems can be easily placed within theframework of the ICF.
Regardless of the specific tool chosen or the treatment protocol selected,counseling patients with tinnitus must bean important component in the process.Items on many of the scales offer theclinician a great deal of insight into theissues that impact performance and canprovide a basis for the measure
“Self-assessment of Tinnitus: An Important Component of Evaluation and Treatment”JOSEPH J. MONTANO, ED. D. ASHA FELLOW
Assistant. Professor/ Director of Hearing and Speech - Weill Cornell Medical College - 1305 York Ave 5th Floor - New York, N.Y. 10021
JOSE
PH J
. MO
NT
AN
O, E
D. D
. ASH
A F
EL
LO
W
References:
1. Ventry, I, & Weinstein, B. (1980). The hearinghandicap inventory for the elderly: A new Tool.Ear and Hearing. 14, 128-134.
2. Demorest, M.E & Erdman, S.A (1987).Development of the communication profile forthe hearing impaired. Journal of Speech andHearing Disorders. 52, 129-142.
3. World Health Organization (2001) Internationalclassification of function, disability andhealth. Geneva: World Health Organization.www.who.org
4. Newman, C., Jacobson, G. & Spitzer, B. (1996).Development of the tinnitus handicapinventory. Archives of Otolaryngology, Headand Neck Surgery, 122, 143-147.
5. Alpiner, J, & Schow, R. (2000). Rehabilitativeevaluation of hearing impaired adults. In J.Alpiner, & P. McCarthy Eds. RehabilitativeAudiology: Children and Adults. Baltimore:Lippincott Williams and Wilkens.
6. Stouffer, J.L., Tyler, R. (1990). Characterizationof tinnitus by tinnitus patients. Journal ofSpeech and Hearing Disorders. 55, 439-453.
7. Wilson, P, Henry, J, Bowen, M, Haralambous, G.(1991). Tinnitus reaction questionnaire:Psychometric properties of a measure ofdistress associated with tinnitus. Journal ofSpeech and Hearing Research, 34, 197-201.
8. Newman, C. Sandridge, S. & Jacobson, G.(1998). Psychometric adequacy of the Tinnitushandicap inventory. Journal of the AmericanAcademy of Audiology. 9, 153-160.
9. Berry, J., Gold, S., Frederick, E., Gray, W,. andStaecker, H. (2002). Patient-based Outcomesin patients with primary tinnitus undergoingtinnitus retraining therapy. Archives ofOtolaryngologyHead and Neck Surgery. 128,1153-1157.
10. Jastreboff, P & Jastreboff, M. (2000). Tinnitusretraining therapy (TRT) as a method fortreatment of tinnitus and hyperacusis patients.Journal of the American Academy OfAudiology. 11, 162-177.
11. Handscomb, L. (2006). Analysis of responses to individual items on the tinnitushandicap inventory according to severity oftinnitus handicap. American Journal ofAudiology.
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients

1918
Tinnitus is known to affectindividuals to varying degreesand in a great number of different
ways 1. Much attention has rightly beenpaid to factors that make the experienceof tinnitus particularly distressing forcertain individuals2,3. However, in theauthor’s experience, a large number ofpeople who are not highly distressed (notshowing signs of desperation, anxiety ordespair) also seek professional help fortheir tinnitus. The aim of this study wasto investigate whether certain aspects oftinnitus tend to trouble people even whenthey are not severely affected by it inmany ways.
The Tinnitus Handicap Inventory4 was usedin this study. This is a 25- item questionnairewith “yes”/ “no”/ “sometimes” responsesdesigned to assess the effects of tinnituson individuals. Some of the items dealwith emotional and behaviouralresponses to tinnitus while others dealwith beliefs about it. The THI is mostoften used as an outcome measure, butNewman et al 5 have also used it to dividepatients into four separate categories (nohandicap, mild, moderate and severe),based on total scores, prior to treatment:
Previous studies carried out on mixedgroups of patients (not using anycategorisation) have shown that certainitems on the THI tend to attract a largernumber of positive responses than others,in particular those concerning lack ofcontrol and inability to escape 4, 6 Thequestion under investigation in this studywas whether the same pattern of response
was present in all groups when patientswere divided into categories.
There were 274 participants, all of whom had requested a tinnitus clinicappointment following a visit to the Ear,Nose and Throat department at St Mary’sHospital. They were divided into four
categories depending on their THI scores:no handicap (0-16), mild handicap (18- 36),moderate handicap (38-56), and severehandicap (58-100.) Mean scores for eachof the 25 items on the questionnaire werecalculated and compared within eachgroup and between the four groups.
It was found that the 2 items: “Do you feelthat you have no control over your tinnitus?”(item 19) and “Do you feel as though youcannot escape your tinnitus?” (item 8)had the highest mean score overall and ineach category, and elicited a ‘yes’ or
“sometimes” responses from the majority ofpatients (>85%) in all but the “no handicap”group. Item 11: “Because of your tinnitusdo you feel that you have a terrible disease?”had the lowest mean score overall and ineach category and elicited a ‘no’ responsefrom the majority of patients (>78%) inall but the “severe handicap” group.
These findings indicate that only thosewho are severely handicapped by tinnitustend to see themselves as having a terribledisease, and that lack of control andinability to escape are common feelingsamongst many people with tinnitus, fromthe most to the least severelyhandicapped. Helping patients to gain asense of control may thus be a keycomponent of successful therapy.
References:
1. Sanchez L, Stephens D (1997) A tinnitusproblem questionnaire in a clinic population. Ear& Hearing 18 (3) 210- 217
2. Meikle M, Vernon J, Johnson M (1984) Theperceived severity of tinnitus. Otolaryngology,head & neck surgery 92:689- 696.
3. Holgers K-M, Erlandsson S, Barrenas M-L(2000) Predictive factors for the severity oftinnitus. Audiology; 39:284- 291.
4. Newman C, Jacobson G, Spitzer B (1996).Development of the tinnitus handicap inventory.Archives of otolaryngology, head & necksurgery; 122: 143-147.
5. Newman C, Sandridge S, Jacobson G (1998)Psychometric adequacy of the tinnitus handicapinventory for evaluating treatment outcome.Journal of the American Academy of Audiology9: 153- 160
6. Baguley D, Andersson G (2003) Factor analysisof the tinnitus handicap inventory. American.Journal of Audiology. 12; 1, 31-34
Tinnitus affects millions of peopleall over the world and itstreatment is still a challenge. The
mechanisms of tinnitus generation arenot completely understood, but mostresearchers assume that it is generated bycochlear damage, followed by abnormalneural activity in peripheric and centralauditory pathways (1).
Amongst many types of therapies thatmay be applied to tinnitus, drug therapyis one of the most accepted by patients (1).If we search only for methodologicallywell conducted clinical trials, we mayclassify tinnitus`drugs in 5 classes:
a) Supplements – many studies show thatZinc is essential for cochlear functionand it may be also found in cochlearnucleii at the brainstem. So, it can beused in tinnitus treatment, specially inthe elderly (2).
b) Drugs that act in cochlear methabolismand perfusion – these drugs arespecially helpful in early tinnitus (upto 2 years of symptoms). They mayincrease cochlear bloodflow andglycose income and also reduces thefree radical production. Trimetazidine(Vastarel)3 and Ginkgo biloba Egb761: Tanakan4 are in this class of drugs.
c) Drugs that act in Auditory EfferentPathways – these drugs inhibits neuralactivity at the auditory pathways,acting as GABA agonists (clonazepan:Rivotril 5, gabapentin: Neurontin 6 andBaclofen7 or dopamin agonists(Piribedil)1. Abnormal neural activity,like tinnitus, can be reduced withincrease in Efferent activity, at leasttheoretically.
d) Drugs that act in Auditory AfferentPathways – these drugs reduces neuralactivity acting directly at the afferent
pathways by decreasing celldepollarization (Carbamazepine:Tegretol)8 or decreasing serotoninreuptake (Paroxetine: Prozac)9.
e) Drugs that act in both the Afferent andEfferent Auditory Systems – the onlydrug that shows this double actionmechanism is Acamprosate (Aotal). Itacts as a NMDA blocker and also as aGABA agonist. A double-blindrandomized clinical trial showedpromising results ( 86,9 % of generalimprovement, 47,8 % of improvementsuperior to 50 % in the tinnitus`score).Further larger studies shoul be done toconfirm its effectiveness 10.
Beyond drug therapy, other types oftreatment have been studied for tinnitus,such as habituation, biofeedback,transcranial magnetic stimulation,general counselling and musical therapy.
“Analysis of responses to individual items on the tinnitus handicap inventory according to severity of tinnitus handicap”
LUCY HANDSCOMBAudiology Department - St Mary’s Hospital - Praed Street - London - W2 1NY - UK - E-mail: [email protected]
“Tinnitus treatment with drugs”ANDRÉIA AZEVEDO,MD, RICARDO FIGUEIREDO,MD,MSC
OTOSUL,Otorrinolaringologia Sul-Fluminense,Volta Redonda, Brasil Assistant Professor of Otolaryngology,Faculdade de Medicina deValença,RJ,Brasil - Tinnitus Research Initiative Member - E-mail: [email protected]
References:
1. Azevedo AA ,Figueiredo Rr. Tinnitus Update.Rev Bras Otorrinolaringol 2004; 70 (1 (Cadernode Debates)):27-40.
2. Botti AS, Feres MCLC. Zinc: Presence inAuditory System. Rev Bras Otorrinolaringol2003; 69 (1):111-16.
3. Azevedo AA FR. Tinnitus treatment withtrimetazidine. Revista da Sociedade de ORL doRio de Janeiro 2005; 5 (1):14-7.
4. Sanchez TG KM, Lima AS,Bento RF,LourençoKG,Miniti,A. Clinical experience in tinnitustreatment with EGb 761. Arq Otorrinolar 2002;6 (3):198-204.
5. Ganança MM CH, Ganança FF,GanançaCF,Munhoz MSL,da Silva ML et al. Clonazepamin the pharmacological treatment of vertigoand tinnitus. Int Tinnitus J 2002; 8 (1):50-3.
6. Bauer CA BT. Effect of Gabapentin on theSensation and Impact of Tinnitus.Laryngoscope 2006; 116 (5):675-81.
7. Szczepaniak WS MA. Effects of baclofen,clonazepam, and diazepam on tone exposure-induced hyperexcitability of the inferiorcolliculus in the rat:possible therapeuticimplications for pharmacological managementof tinnitus and hyperacusis. Hear Res 1996; 97(1-2):46-53.
8. Sanchez TG BA, Bittar RSM,Bento,RF. Teste daLidocaína em Pacientes com Zumbido: QuandoRealizar e Como Interpretar. Arq Otorrinolar1998; 2 (2):48-55.
9. Robinson SK VE, Bailey KA,Gerke MA,Harris JP,Stein,MB. Randomized Placebo-Controlled Trialof a Selective Serotonin Reuptake Inhibitor inthe Treatment of Nondepressed TinnitusSubjects. Psychosom Med 2005; 67(6):981-8.
10. Azevedo AA FR. Tinnitus treatment withacamprosate: a doublé-blind study. Rev BrasOtorrinolaringol 2005; 71 (5):618-23.
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients

2120
Tinnitus is derived from the Latinword “tinnere”, meaning to ring,and represents a complex
neurotologic symptom, whose treatmentoptions include a bewildering array ofbehavioral, technological, medical andsurgical therapies. The lack of auniversally accepted and effectivetreatment for tinnitus reflects its complexpathophysiology and its diverse andsubjective individual expression.
Among the potential therapies availableand worthy of consideration are variouseffective alternative therapies for tinnitus.Herbal remedies, vitamin and mineralsupplementation, and complementarymedicinal therapies are included under therubric of alternative therapies orcomplementary/integrative therapies. Therepresentative list of therapies belowprovides the clinician with a broadspectrum of complementary/integrativemedicine options to consider in themanagement of tinnitus as compared toconventional treatments such as maskingdevices, hearing aids, antidepressant andanxiolytic agents, and tinnitus retrainingtherapy.
Herbal remedies, in the form of herbs,exotic fruits, plant roots, and seed oils,have been used effectively for thousand ofyears to treat various diseases. Thoughevidence based studies regarding theirefficacy are generally lacking, there havebeen a plethora of anecdotal accounts ofsuccessful treatment, thereby justifyingtheir consideration and use, especially inpatients who have not responded toconventional therapies. Arguably themost studied and well known of these
herbal remedies is Gingko biloba, ormaidenhair. Gingko biloba is widelythought to increase circulationthroughout the body. Several studies havedemonstrated its efficacy in tinnitus.Typical dosages range from 120-480mgper day, divided equally at mealtime. Inwestern countries a standardized 50:1concentrate of 24% gingko flavonoids isused, either in liquid or capsule form. Oneof the appealing aspects of Ginkgo bilobawith regard to the treatment of tinnitus,has been the fact that it is relativelyinexpensive, and has negligible sideeffects, such as increase risk for epistaxis.As with any medication, the physicianshould take a careful history beforerecommending Gingko as it maypotentiate hemorrhage in people takingprescription blood thinners, such ascoumadin, loveonx, heparin, and possiblyeven plavix. The German Commission E,which is considered an excellent referencefor the medicinal use of therapeutic herbs,rates Ginkgo as a positive herb andrecommends 240 mg twice per day fortinnitus and vertigo. The response toGinkgo can occur within weeks, but ismost noticeable within 3 to 4 months.
Ginkgo is not effective in every patientwith tinnitus, but the risk to benefit ratiowould suggest that a trial with Ginkgo isreasonable.
Another herb, Black cohosh (derived fromthe forest plant Cimicifuga racemosa), hasbeen reported to improve chronic tinnitus.Similar to Gingko, it is postulated toimprove cerebral blood flow and therebyproviding relief from tinnitus. Dosagesrange from 20 to 40 mg per day in liquid
form for this ailment, but driedpreparations may also be of some benefit.Ligustrum (ligustrum lucidum) is anotherherb that has been advocated in themanagement of tinnitus. Therecommended dosage is 400mg threetimes per day. Mullein (verbascumdensiflorum), Pulsatilla (anemonepulsatilla), Lycium Fruit (Lyciumbarbarum or Lycium chinense), Cornus(Cornus officinalis) in combination withChinese foxglove root and Chinese yam,Cuscuta (Cuscuta chinensis), ChineseFoxglove Root (Rehmannia glutinosa),Alisma (Alisma plantago-aquatica), andSesame Oil (Sesamum indicum) have allbeen reported to be effective in themanagement of tinnitus.
Vitamin and mineral supplementationhave also been used with varying degreesof success in the treatment of tinnitus.Their efficacy in treating tinnitus isattributed to their role in maintainingneural and vascular homeostasis. Thetable above lists some of thesesupplements and their recommendeddoses for tinnitus treatment.
Often times, tinnitus can be severe enoughto interfere with activities of daily living,and have adverse effects on sleep andquality of life. In addition to the herbalremedies and supplements discussedabove, there are complementary medicaltherapies that can have profound positiveeffect on a person’s general well-being andtheir ability to cope with the tinnitus. Inmany cases, the treatments can leaddirectly to tinnitus abolition, for example,by relaxing the strained neck musculaturethat is causing the tinnitus.Complementary therapies include thoselisted in the Table and should be regardedas viable alternatives especially inpatient’s who have been refractory toconventional medical therapy.
Complementary/intergrative therapies inthe treatment of tinnitus generally have alow risk profile and their anecdotalsuccess justifies their consideration andinclusion in the standard armentarium fortinnitus treatment.
References:
1. Rudolph, Fritz, Weiss, 1998: editors: HerbalMedicine. Beaconfield Publishers, LTD,Beaconsfield, England.
2. Newall CA, Anderson LA, Phillipson JD, 1996:editors: Herbal Medicine, A Guide for Health-Care Professionals. The PharmaceuticalPress, London, Enland.
3. Seidman M, Jacobson G, 1996: Update onTinnitus. Otolaryngologic Clinics of NorthAmerica; 29:455-465.
4. Meyer B, 1980: Tinnitus-multicenter study. Amutlicentric study of the ear. Annals ofOtolaryngology; 103: 185-188.
6. Thomas M, Laurell G, Lundeberg T, 1988.Acupuncture for the alleviation of tinnitus.Laryngoscope; 98:664-667.
7. Shulman, Abraham, 1992: SubjectiveIdiopathic Tinnitus: A Unified Plan ofManagement. American Journal ofOtolaryngology; 13: 63-74.
8. Balch J, Balch P, 1997: Prescription forNutritional Healing. 2nd Edition, BalchPublishing,
9. Paaske P, Kjems G, Pedersen C, 1991: Zinc inthe Management of Tinnitus. Annals of OtolRhinol Laryngol; 100: 647-49.
10. Holgers KM, Axelsson A, Pringle, 1994: GinkgoBiloba Extract for the Treatment of Tinnitus.Audiology; 33 (2): 85-92.
11. Drew S, Davies E, 2001. Effectiveness ofGinkgo biloba in treating tinnitus: double blind,placebo controlled trial. BMJ. 322(7278):73.
12. Blumenthal, Busse, Goldberg, 1998 editors:The Complete German Commission EMonographs. Integrative MedicineCommunications, Boston, Massachusetts.
13. Morgenstern C. Biermann E. 2002. Theefficacy of Ginkgo special extract EGb 761 inpatients with tinnitus. International Journal ofClinical Pharmacology & Therapeutics.40(5):188-97.
14. Seidman MD, Babu S. 2003. Alternativemedications and other treatments for tinnitus:facts from fiction. Otolaryngol Clin NorthAm.;36(2):359-81.
“Alternative Therapies for Tinnitus”NADIR AHMAD MD, MICHAEL D. SEIDMAN MD.
Division of Otologic/Neurotologic Surgery -F.A.C.S., Henry Ford Health System, W. Bloomfield, (Detroit) MI, USA.E-mail: [email protected]
NA
DIR
AH
MA
D M
D, M
ICH
AE
L D
. SE
IDM
AN
MD
.
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
Alternative Therapies for Tinnitus
HerbsGinkgo biloba - Black Cohosh - Ligustrum - Mullein - Pulsatilla -
St. John Wort
Vitamins and
Minerals
Magnesium (400mg/day) - Calcium (1000mg/day) - Potassium
(2500mg/day) - Zinc - Manganese - Copper - Vitamin B12 - Beta
Carotene - Selenium - Vitamin C - Vitamin E - Niacin
Complementary
Therapies
Relaxation training - Biofeedback training - Acupuncture - St.
John’s neuromuscular therapy
Table:
Les acouphènes sont un véritableproblème de santé publique. EnFrance, une enquête portant sur
plus de six cents patients acouphéniques amontré que 26 % avaient une altérationimportante de leur qualité de vie avec desmodifications notables du comportement :irritabilité, inquiétude, tension, dégradationdu sommeil. L’échec de nombreuxtraitements, notamment médicamenteux,a conduit quelques équipes à proposerdes thérapeutiques fondées sur desconcepts radicalement différents. Si laplupart des auteurs estimaient quel’origine des acouphènes était cochléaire(lésions des cellules ciliées de l’oreilleinterne après un traumatisme sonore, unepresbyacousie…), il semble acquis que lagêne ressentie est largement exacerbéepar des processus centraux, en particulierl’anxiété. Sur le plan cognitif, il s’agitd’attributions péjoratives au symptôme etd’un état d’hypervigilance globale et
élective pour les stimulations auditives ;les patients développent un réflexeconditionné d’attention dirigé versl’acouphène mais également pour certainsbruits d’ordinaire totalement anodins, encas d’hyperacousie associée. Plusieursétudes épidémiologiques montrent quel’anxiété et la dépression aggravent lagêne engendrée par la présence desacouphènes. Le rôle attribué au système ausystème limbique ou au système nerveuxautonome dans le vécu de l’acouphène està l’origine du développement destechniques d’habituation largementutilisées dans les thérapies cognitives etcomportementales ou dans la “TinnitusRetraining Therapy”. L’utilisation desthérapies cognitives et comportementales(TCC) appliquées au traitement desacouphènes a été initialement proposéepar Sweetow et Mac Leod Morgan dès ledébut des années 1980. Un grand nombrede patients ont des acouphènes qu’ils
Références :
1. Londero A, Peignard P, Malinvaud D, Nicolas-Puel C, Avan P, Bonfils P. Traitement desacouphènes par thérapie cognitive etcomportementale. Implication de l’anxiété et dela dépression. Ann Otolaryngol Chir Cervicofac2004 ; 121 :334-45.
2. Londero A, Peignard P, Malinvaud D, Avan P,Bonfils P, Acouphènes et thérapie cognitive etcomportementale : analyse à un an. La PresseMédicale 2006 ; 35:1213-21
3. Kuk FK, Tyler RS, Russell D, Jordan H. Thepsychometric properties of a tinnitus handicapquestionnaire. Ear Hear. 1990; 11(6):434-45.
Résultats comparatifs des principaux items desquestionnaires utilisés avant et après TCC :mesure de la détresse psychologique (détressegénérale DG), items du questionnaire hospitalierd’évaluation de l’anxiété (HADa) et de ladépression (HADd), questionnaire de mesure duhandicap (THQ). Pour chaque graphe le scoremédian avec l’intervalle de confiance de 95% de lamoyenne est noté. Il existe une diminutionsignificative de tous les items après TCC(p<0,0001).
“Acouphènes et thérapie cognitive et comportementale”PIERRE BONFILS
Département d’ORL et de Chirurgie Cervico-Faciale, Faculté de Médecine, Université Paris-Descartes. Correspondance et tirés à part : Hôpital Européen Georges Pompidou, Service ORL, 25 rue Leblanc, 75015 Paris, France. E-mail : [email protected]

2322
tolèrent bien, ne se plaignant d’aucunegêne et de demandant aucune aide médicale.Il apparaît actuellement la négligence del’acouphène et, par conséquent, sa tolérance,devrait être la réponse normale à cephénomène. Ainsi, la TCC a pour but demodifier les comportements délétères et lespensées corollaires en utilisant destechniques de déconditionnement et dequestionnement dit “socratique” c’est-à-direimpliquant la coopération active du sujetdans la définition du traitement et sa mise enœuvre (1,2,3).
La coordination d’une consultation ORLavec une consultation psychologique estréalisable et bénéfique aux patientsprésentant un acouphène chroniqueinvalidant. Le relais d’une prise en chargeà visée somatique avec la mise en œuvred’un protocole de TCC se révèle utile queles patients présentent ou non desmanifestations psychopathologiques.Cette approche innovante ayant étévalidée dans cette indication et ouvrantsur une prise en charge globale du patientnous a, en outre, permis de reconsidérer
les modes d’action thérapeutique en causedans la procédure de TCC que nousavons appliquée à l’acouphène, laquellene semble pas se cantonner aux domainesde l’anxiété et de la dépression, maisconcerner d’autres processus commel’attention et l’adaptation. Près de 80%des patients souffrant d’acouphènes ontété améliorés avec un an de recul par uneTCC.
“La prise en charge de l’acouphène chronique invalidant.”DOCTEUR MARTINE OHRESSER
Centre d’Explorations Fonctionnelles Oto-Neurologiques, 10 rue Falguière, 75015 Paris, FranceE-mail : [email protected]
La prise en charge du patientacouphénique, tout particulièrementlorsqu’il s’agit d’un acouphène
chronique invalidant, dépasse trèslargement la seule compétence del’otologiste et nécessite l’intervention deplusieurs autres disciplines car, pour êtreefficace, l’action thérapeutique doitconsidérer l’individu dans sa globalité.
Ceci nous a amenés, il y a quatre ans, àconstituer une équipe pluridisciplinaire,regroupée au sein d’une associationnommée AERA (Association d’Etude etde Recherche en Acouphénologie). Elle estcomposée de deux otologistes, troisaudioprothésistes, une psychologuepratiquant la thérapie cognitive etcomportementale, un médecin pratiquantla relaxation sophrologique et un médecinacupuncteur. Le rôle des audioprothésisteset de plus en plus important car nousappareillons tôt les patients acouphéniquesporteurs d’un déficit auditif et nousutilisons également les générateurs debruit blanc dans le cas où l’audition etnormale ou sub-normale. Les psychologuesde thérapie cognitive et de sophrologienous apportent deux techniques qui pournous ont des résultats semblables et ontl’intérêt d’être des thérapies courtes etcentrées sur le symptôme.
Je n’ai nommé ici que les disciplines dontnous avons besoin en permanence pour laprise en charge de l’acouphène chronique
et/ou de l’hyperacousie. Nous disposonségalement de correspondants auquel nous nefaisons appel que plus exceptionnellement :un médecin psychiatre, un médecinostéopathe et un médecin spécialisé enmaxillo-faciale.
Après la réalisation du bilan auditif debase et de l’acouphénométrie, le premiercontact du patient avec l’équipe a lieu trèstôt dans son cursus par la participation à une matinée d’information qui se faitpar groupe de quinze à dix sept patients.Il s’agit de trois heures au cours desquellesnous faisons le point sur ce que l’on sait actuellement sur l’acouphène. Nous exposons notamment le modèleneurophysiologique de Jastreboff etHazell, le rôle du système limbique, dusystème cognitif et du système nerveuxautonome de façon à ce que les patientscomprennent les thérapeutiques qui vontensuite leur être proposées. Chacun desmembres de l’AERA prend ensuite laparole pour exposer en quoi consiste sadiscipline et en quoi elle est impliquéedans le traitement de l’acouphènechronique. Cette matinée est également unlieu d’échange entre le groupe et lesintervenants par les questions qui leurssont régulièrement posées mais égalementà l’intérieur même du groupe. Elle a unimpact très important sur les patientscomme l’attestent les enquêtes desatisfaction que nous avons faites àplusieurs reprises.
Après cette matinée informative, ilappartient à l’otologiste, qui est lecoordinateur du groupe, d’envisager avecson patient les différentes possibilitésthérapeutiques qui lui conviennent. Lechoix est fait avec lui en fonction duretentissement de l’acouphène mais ausside la personnalité du patient, de sescroyances, de sa psychologie, etc. Il estessentiel pour nous que le patient prenneune part active dans l’établissement de sonprojet thérapeutique. Le fait que nousreprésentions cinq spécialités différentespermet d’offrir autant de points d’ancragepour débuter la prise en charge.
Le but de cette prise en chargepluridisciplinaire est d’amener son patientà l’indifférence à l’acouphène. Il s’agitdonc d’une thérapie d’habituation,dérivée de la Tinnitus Retraining Therapy(TRT) décrite par Jastreboff et Hazell. LaTRT se compose à la fois de la thérapiesonore et de ce que les auteurs nomment“counseling” c’est-à-dire du conseil, del’information et la lutte contre les idéesnégatives. Dans notre cas, cette deuxièmepartie, informative, est faite par chacund’entre nous chaque fois que nous voyonsle patient, il s’agit d’un travail de base quenous devons tous faire. Mais nousassocions à la thérapie sonore, la thérapiecognitive et comportementale ou larelaxation sophrologique. Il arrive aussiparfois que certains de ces modules soientutilisés à l’exclusion des autres qu’il
PIE
RR
E B
ON
FIL
SDiagnostic et traitement des acouphènes chez les patients
Clinical diagnosis and therapy of tinnitus in patients
s’agisse de port de bruiteurs chez un patientqui a très bien compris l’acouphène et sesconséquences et chez lequel une aidepsychologique n’est pas nécessaire. Onpeut tout autant dans certains casenvisager une prise en charge uniquementpsychologique sans thérapie sonore.
Cependant, cette prise en charge n’excluepas le recours à certaines thérapeutiquesmédicamenteuses. C’est notamment le casdu Clonazépam° qui reste pour nous,dans les cas où l’acouphène est trèsinvalidant, une utile amorce de la prise encharge. Il est en effet très difficile demobiliser sur ces thérapies d’habituationun patient complètement envahi par son
acouphène. La souffrance qui est aupremier plan lui rend difficilementpossible la perspective d’un investissementdans une rééducation de longue haleine.Le Clonazépam° permet de passer ce capdifficile. Dans plus de trois quarts des cas,il permet de modifier l’acouphène et dedémontrer ainsi au patient qu’il y apossibilité d’agir sur son symptôme. C’estune étape importante pour l’instaurationde la relation de confiance nécessaire aubon déroulement de la prise en charge.Plus nous avons progressé dans la prise encharge pluridisciplinaire, plus nous avonsrestreint en durée ce traitement deRivotril° et actuellement nous l’utilisonsdans une durée moyenne de trois mois. Ce
temps nous permet difficilement réductiblecompte tenu de la nécessité de monter etde descendre très progressivement lesdoses.
En novembre 2006, nous avons réuni lesdifférentes équipes pluridisciplinaires deprise en charge de l’acouphène duterritoire français. Il y a actuellement unedizaine d’équipes de ce type. Cette journéenous a permis de partager nosexpériences, de commencer à réfléchir àun consensus de prise en charge et aumode d’évaluation de nos pratiques. Laprochaine réunion aura lieu au printemps2007.
DO
CT
EU
R M
AR
TIN
E O
HR
ESS
ER
“Pourquoi proposer une prise en charge de l’acouphène chronique invalidant par les TCC (thérapies cognitivo-comportementales) ?”
ALAIN LONDERO Hôpital Européen Georges Pompidou, Service ORL, 25 rue Leblanc, 75015 Paris, France. E-mail : [email protected]
L’acouphène est une pathologieinitialement périphérique :
• L’acouphène fait suite dans plus de80% des cas à une atteinte auditivepériphérique le plus généralementcochléaire (traumatisme sonore oupressionnel, ototoxicité, séquelles depathologies inflammatoires otologiques…)ou parfois nerveuse (neurinome duVIII, boucles vasculaires du CAI).
Mais il n’y a pas de corrélation entrel’intensité perçue de l’acouphène et lagêne induite :
• L’intensité de l’acouphène n’excèdegénéralement pas de plus de quelquesdB le seuil auditif et de nombreusesétudes ont montré l’absence totale delien entre le niveau de l’acouphènedécrit par les patients et le degré dehandicap ou de détresse qu’il procure.A acouphène égal, 80 % des patientsdéclarent une gêne mineure et négligentleur acouphène qui ne requiert pas deprise en charge particulière. Cettenégligence ou “habituation” peut êtreconsidérée comme la réponse “normale”au phénomène.
La gêne induite par l’acouphène : le reflet d’activations de systèmescentraux extra auditifs :
• La mauvaise tolérance décrite parcertains est par voie de conséquence
supposée être le reflet d’activationsanormales de systèmes extra-auditifscomme le système nerveux autonome(élévation du niveau de stress, troublesdu sommeil), le système limbique(mémorisation, connotation émotionnelle,anxiété-dépression), le système attentionnel(capture attentionnelle, troubles de laconcentration…). Ce serait cetteadaptation centrale “anormale”, et nonpas la perception seule de l’acouphène,qui in fine rendrait compte de la gêneparfois majeure ressentie par uneminorité de patients.
En l’absence de traitement périphériquevalidé il est légitime de tenter d’agir surcette composante centrale :
• En l’état actuel des connaissancesaucun traitement curatif étiologique n’afait la preuve de son efficacité. Lestraitements médicamenteux prescritscomme le Clonazepam (Rivotril°), lesanxiolytiques ou les anti-dépresseurs lesont à titre palliatif. Ils agissent surcette composante centrale et non pas surla cause périphérique de l’acouphène.C’est également le but des TCC.
Les TCC : une autre façon d’agir :
• Les TCC se proposent d’agir de façonpragmatique et brève en favorisant desstratégies optimales d’adaptation et de“coping” à la fois sur le versant cognitif(par modification de schémas de penséeinvalidants) et sur le versant

2524
L’acouphène touche 1,8 % de lapopulation et 50 % de ces patientsprésentent en même temps une
perte auditive et un acouphène.L’acouphénique est donc un patienthabituel de l’activité professionnelle del’audioprothésiste. Dans la majorité descas, cet acouphène est cité par ledéficient auditif sans que celui-ci soit lemotif de la prise en charge, mais il arriveque cet acouphène ait un impactpsychologique suffisamment importantpour qu’il soit la raison de la demande dupatient.
Dans ce cas, le rôle de l’audioprothésistedifférera en fonction des différentsparamètres suivants : l’acouphène est-ilisolé et doit-il s’inscrire dans une thérapieà base de générateur de bruits ?. Est-ilassocié à une surdité et doit-il être traitéde façon conjointe à la perte auditive elle-même ? Est-il invalidant et représente-t-ille problème principal ? Est-il accompagnéd’une hyperacousie ? Crée-t-il un impactpsychologique nécessitant une prise encharge pluridisciplinaire ?
La prise en charge est donc variée et doitêtre adaptée non seulement au cas dupatient, mais aussi à son évolution. Iln’existe donc pas de protocole standard
pour tous les acouphéniques etl’adaptabilité au problème particulierd’un patient et à son profil psychologiquedoit être la règle. Le suivi doit par ailleurs être renforcé par rapport à unappareillage classique. La notiond’équipe pluridisciplinaire est iciparticulièrement importante car l’acouphèneest le signe extériorisé d’un problèmemais peut participer à un tableaubeaucoup plus large, notamment auniveau psychologique.
Le traitement global a évolué au fur et àmesure des années en intégrant l’aspectprothétique grâce aux progrès techniqueset aux avancées de la compréhension del’association de la participation centrale,notamment au niveau du systèmenerveux végétatif et du système limbique.
La technique prothétique est d’ailleurspassée par un certain nombre d’étapes dontla première a été l’utilisation de masqueursdestinés à masquer l’acouphène. Leprincipe était de remplacer l’acouphènepar un son extérieur, réputé mieux toléré.Cette technique est aujourd’huiabandonnée en dehors du traitement desacouphènes pulsatiles et des cas raresd‘inhibition résiduelle post-stimulation.
L’étape suivante a été celle desgénérateurs de bruits blancs, identiquesaux masqueurs, mais utilisés dans un butdifférent. La finalité est d’obtenir la miseen œuvre de l’habituation qui est ladisparition des réactions du systèmenerveux central à la perception d’unstimulus dépourvu d’information. C’estd’ailleurs quand ces phénomènesd’habituation ne se mettent pas en placeque l’acouphène peut devenir invalidant.Pour tenter de les activer, un générateurde sons est adapté par l’audioprothésistede façon à ce que le sujet perçoive à lafois son acouphène et le signal dubruiteur. Cette stimulation régulière àfaible intensité entraînerait desphénomènes centraux de traitement dubruit émis, permettant dans certains casde créer du même coup l’habituation à l’acouphène. D’après les travaux de Jonathan Hazell, ce générateur de sonsréaliserait dans le même temps une stimulation régulière des élémentsmusculaires des cellules ciliées externes, ce qui sous-entend une actionconcomitante en périphérie et au niveaucentral. L’audioprothésiste participe doncau traitement par la TRT (tinnitusretraining therapy) et réserveactuellement ce générateur de sons auxpatients à audition normale.
Il existe par contre certains patients quiprésentent de façon conjointe acouphène etsurdité, ce qui conduit l’audioprothésiste àmodifier spécifiquement l’appareillagepour coupler deux buts : disparition del’acouphène lors du port et correction dela surdité.
Il est essentiel de choisir l’amplificationen tenant compte de plusieurs paramètres: l’acouphène et ses caractéristiques, lasurdité et surtout la nature du bruit danslequel vit l’acouphénique. Ce bruitenvironnant est en effet l’élément clé car c’estson amplification qui crée le masquage.La recherche des caractéristiques del’acouphène peut se faire de différentesmanières et doit être couplée avec unerecherche de courbe de masque oùl’acouphène est l’élément à masquer(Méthode de l’encadrement, Méthode des choix forcés, Mesure de l’intensitééquivalente à la hauteur tonale del’acouphène : Méthode Fowler, etc..).
L’effet de masque recherché est trèsdifférent de celui du masqueur quiapporte un bruit surajouté non traité parle cerveau car considéré comme parasite.En revanche, le masque procuré par laprothèse auditive est le bruit variableenvironnant traité par les voies centrales.C’est l’univers sonore habituel du patient,d’où un apprentissage plus facile etrapide. Par chance, l’acouphène estrarement émergent de plus de 10 dB parrapport au seuil auditif et un bruit dequelques décibels supplémentaires dans la
zone de l’acouphène permet un masquageefficace. L’amplification dépend d’ailleursde l’intensité du milieu sonore du patient.Plus l’intensité rencontrée sera faible etplus l’amplification de la zone del’acouphène devra être importante, sanstoutefois entraîner une gêne subjective.L’amplification doit pouvoir exercer unmasquage de l’acouphène pour un milieusonore calme, ce qui conduit parfois àune amplification plus importante quepour un appareillage classique.
Le choix de l’appareil, en plus de sescapacités de masquage, doit permettreune amplification importante des bruitsfaibles dans la zone de l’acouphène sanstoutefois entraîner une augmentation tropimportante des bruits d’intensité moyenneou forte. L’important est d’évoluer defaçon à exercer un compromis entreacceptation de l’amplification et premiersrésultats de masquage. Il arrive d’ailleursparfois, qu’après une période plus oumoins longue, le patient se plaigne moinsde son acouphène et que le masquagedevienne un élément moins imprtant quela correction de la perte auditive elle-même, conduisant à redéfinir le gain.
Du fait du confort subjectif qu’il procure,l’appareillage va réduire l’impact négatifde l’acouphène, contribuant à la maîtrisedu handicap, parallèlement au travail sur lamaîtrise de la composante émotionnelle.
Tous les travaux convergent pour direque le salut du patient acouphènique
n’est donc pas dans le silence comme onaurait pu le penser mais bien dans laréacclimatation à l’univers sonore. A ce titre,l’appareillage du patient acouphéniqueprend une place très importante. Associéeà la reprogrammation du vécu émotionnelqui se rattache à l’acouphène, elle permetde conduire le patient à l’indifférence.
Conclusion:
La prise en charge de l’acouphéniqueprésente des particularités aussi bien aupoint de vue de l’accompagnement, cetype de patient ayant une souffrancepsychologique importante qu’au point devue prothétique proprement dit. Le rôlede l’audioprothésiste concerne aussi bienla prise en charge de type TRT par leréglage et le suivi des générateurs debruits que l’appareillage dans le choixd’une amplification particulière intégrantaussi bien les caractéristiques de lasurdité que celles de l’acouphène. Devantla complexité de certains cas, la techniqueprothétique utilisée de façon isoléedevient cependant insuffisante et doits’intégrer dans une prise en chargepluridisciplinaire où chaque partenaire varenforcer le potentiel des autresintervenants. Dans les cas les plusinvalidants, l’audioprothésiste se doit detravailler dans le cadre d’une équipepluridisciplinaire, ce qui sous-entend lanotion de réseau et la nécessité à moyenterme d’une véritable politique de santéde la part des pouvoirs publics.
ER
IC B
IZA
GU
ET
et P
AU
L E
DO
UA
RD
WA
TE
RL
OT
“L’acouphène : le point de vue de l’audioprothésiste.”ERIC BIZAGUET et PAUL EDOUARD WATERLOT AUDIOPROTHÉSISTE.
Laboratoire de Correction Auditive, 6 rue du 8 Mai, 75010 Paris. Tel. : 01 40 34 36 22 E-mail : [email protected]
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
comportemental (par modification descomportements inadaptés). Leurobjectif est de faire obtenir à despatients, jusque là invalidés par leuracouphène, l’état de négligence obtenuspontanément par la majorité des sujetsprésentant un acouphène. Les TCCsont également actives sur les étatsanxieux ou dépressifs préalables, ousecondaires à l’apparition de l’acouphène.
Les TCC : méthodologie :
• Il existe différents protocoles de TCCqui associent à des degrés divers :
• - apprentissage de techniques de relaxationet de gestion du stress
• - apprentissage de comportements
alternatifs non inducteurs de stress(restructuration comportementale)
• - analyse critique des schémas de penséedélétères et invalidants
• - adoption de schémas de penséealternatifs (restructuration cognitive)
• Les TCC sont des thérapies courtes(une dizaine de séances d’environ uneheure en individuel ou en petit groupe)nécessitant la collaboration du patientqui devra s’astreindre aux exercicesproposés par le thérapeute. L’évaluationdu résultat d’une TCC est réalisée parl’analyse de l’évolution des scoresmesurés par EVA (Echelle VisuelleAnalogique) ou par questionnairesvalidés (Tinnitus Handicap Questionnaire,
Tinnitus Handicap Inventory, TinnitusSeverity Scale…).
Les TCC une thérapeutiquepsychologique validée :
• Les TCC sont le traitement de référenceet de première intention : des troublesdu sommeil primaires ou secondaires,des addictions (sevrage tabagique), destroubles anxieux, des phobies…Différentes études cliniques, dont uneméta-analyse, ont montré l’intérêt decette prise en charge psychologiquedans l’indication spécifique acouphèneet hyperacousie. La persistance durésultat bénéfique à long terme.
AL
AIN
LO
ND
ER
O

2726
l’appareil et cotation sur une échellevisuelle analogique (EVA de 1 à10) del’intensité de l’acouphène
- par le renseignement toutes les 2 semainesd’un questionnaire d’évaluation de ladétresse induite par l’acouphène.
L’étude clinique s’est conclue, asseznormalement, dans la moitié des cas parl’explantation du dispositif, chez lespatients qui ne le considéraient plusnécessaire ou utile.
Au delà de la prise en charge “mentale”…
Dans ces situations de désafférentationavec cophose unilatérale, il est essentielde prendre en compte toutes les doléanceset de les ordonner pour mieux les prendreen charge. En plus d’aider le patient àmettre en route un processus d’habituation,il est primordial d’identifier tant que fairese peut la part de la surdité, celle del’acouphène, celle d’un éventuel étatdépressif dans ses doléances.
La solution idéale sera bien évidemmentla réparation de la surdité par des moyens“cellulaires et chimiques”… d’ici quelquesannées.
Mais d’ores et déjà, on peut rappeler quela surdité unilatérale est responsabled’une diminution de sonie, de défaut delocalisation, de défaut de débruitage de laparole et dans certains cas d’exacerbationde l’acouphène si l’oreille contro-latéraleest exposée à un bruit fort. C’est ainsi quesouvent, l’arbre cache la forêt, autrementdit l’acouphène, symptôme le plusévident, présenté comme doléancepremière, relègue au second plan lamauvaise fonction auditive que le patientanalyse mal…
Avec une surdité inappareillable, lepatient n’a plus aucune chance deretrouver son audition automatique etirrépressible : il doit faire un effort pourcomprendre surtout si les conditions
sonores ambiantes sont dégradées. Il tendl’oreille, il écoute “son” acouphène.Celui-ci s’impose, c’est le symptômeimmédiatement et facilement perçu, c’estla première doléance…
Aussi à côté du développement del’habituation, il faut rechercher toutes lespossibilités de corriger la surdité par tousles moyens : la stimulation électrique telleque présentée ci-dessus éventuellementéquipée avec un système CROS sonorecontrolatéral, voire stimulation sonoresignifiante d’un implant cochléaire oupilotée par la prosodie si le côté nonacouphènique mérite une aide auditive…
Au total : Même en cas de cophoseunilatérale l’acouphène ne résume pas lagêne. Le bilan ORL doit être bilatéral etla solution, globale. Cette proposition desoin intègre avec bénéfice la stimulationélectrique de l’oreille sourde.
Références :
1. Aran J-M (1981) Electrical stimulation of theauditory system and tinnitus control. J.Laryngol. Otol. Suppl 4, 153-161.
2. Watanabe K., Okawara D., Baba S., and Yagi T.(1997) Electrocochleographic analysis of thesuppression of tinnitus by electrical promontorystimulation. Audiology, 36, 147-154.
3. Frachet B., Théoleyre B., Wable J., Vormès E.,Répetto J.C., Gallégo S. Les Cahiers del’Audition - Vol. 17 - N°2 - Mars/Avril 2004
4. Théoleyre B., Péan V., Philippon B., Gallégo S.,Vormès E., Frachet B. Acouphènes aveccophose unilatérale. Thérapie par stimulationélectrique. Suivi de 8 patients. CommunicationCongrès National ORL Paris 2005
Légende Figure :
Un exemple d’implant utilisé dans le cas depatients acouphéniques cophosés.
BR
UN
O F
RA
CH
ET
(su
ite)
“Un espoir thérapeutique pour les acouphènes d’origine périphérique”JEAN-LUC PUEL
INSERM U.583 et Université Montpellier 1, 80 rue Augustin Fliche, 34 295 Montpellier cedex 5. E-mail : [email protected]
On estime qu’en France plus de 5 millions de personnes souffrentd’acouphènes. Une enquête
nationale menée en 1999 à l’aide d’unquestionnaire adressé aux médecins ORL,montre que 50 000 à 80 000 personnesconsultent chaque année pour un problèmed’acouphène. Chaque spécialiste voit 70nouveaux cas par an. Malheureusement,peu de traitements sont réellement efficaces,conduisant les patients à un nomadismemédical, à la recherche de solutionsinexistantes.
Notre laboratoire vient de découvrir quel’oreille interne est bien à l’origine decertains acouphènes. Ces travauxreposent sur deux approchesexpérimentales. La première consiste àenregistrer l’activité électrophysiologiquedes fibres du nerf auditif. Nous avonsmontré que de fortes doses d’aspirine (oude son composé actif, le salicylate),connues pour induire des acouphèneschez l’homme, provoquent uneaugmentation de l’activité basale et desdécharges ‘‘en bouffées’’ dans le nerf
auditif ; on peut parler, en quelque sorte,“d’une épilepsie du nerf auditif”.Cependant, faire la démonstration que lesalicylate provoque des activitésanormales ne suffit pas à démontrer qu’ilinduit des acouphènes. Nous avons doncmis au point un test comportementald’acouphènes, qui n’induit ni stress, nianxiété chez l’animal (1). L’animal est toutd’abord conditionné à exécuter une tâchemotrice en réponse à un son extérieur,généré par un haut-parleur. Lorsque cesanimaux sont traités avec de fortes doses
La partie externe ressemble à la partie externe d’un implant cochléaire conventionnel (Digisonic‚ de la société Neurelec)
La partie implantée comporte le récepteur et 2 électrodes : celle de masse et la
cupule placée à l’extrémité d’un piston-téflon très classique, fixée normalement sur la
branche descendante de l’enclume.
“ACOUPHENES ET COPHOSE : quand les acouphènes sont encore moins faciles à prendre en charge…”
BRUNO FRACHETService ORL - Hôpital Avicenne (APHP) - Université Paris 13 - 93009 Bobigny Cedex - E-mail : [email protected]
Les patients qui présentent uneoreille sourde avec acouphènesposent au médecin O. R. L. un
problème délicat à gérer .
L’acouphène est souvent une séquellesurajoutée d’une surdité brusque oud’une cophose iatrogène. Pour le patientla situation est d’autant plus désagréablequ’elle est difficilement compréhensible :l’oreille non seulement n’apporte plusd’audition mais est quand même sourced’une perception sonore.
Lorsque la cophose avec acouphènesiatrogène est conséquente à une interventionpour otospongiose, la situation estparticulièrement difficile : éprouvantepour l’opéré, atteint dans son corps etsouvent déçu ou revendicatif vis-à-vis dumonde médical, pénible pour le chirurgienqui se trouve démuni quant aux choixthérapeutiques.
Impossible de proposer à ce patient unestimulation sonore (qui associée à unconseil thérapeutique spécifique constituela thérapeutique habituelle des acouphènes)puisque l’oreille est désormais cophotique !
Le chirurgien ne peut donc proposer quedes thérapeutiques adjuvantes :
- Anxiolytiques pour limiter les angoisseshabituelles et légitimes du patient :“Comment vais-je vivre avec ce bruit ?Est-ce qu’il va augmenter ? Est-ce que çava m’abîmer le cerveau ? Est-ce que c’estpour toute ma vie ?”
- Thérapies comportementales et cognitives,
yoga, relaxation… pour améliorer latolérance de l’acouphène
- Prise en charge des co-morbidités commel’insomnie…
L’expérience montre que le développementde l’habituation à l’acouphène est pluslent lorsqu’il y a cophose. L’ hypothèseexplicative est qu’il en est ainsi parcequ’on ne peut pas favoriser par un signalsonore la naissance de ce fameux “filtrehabituationnel”, qui, à terme, limitesinon la perception du moins la gêne del’acouphène.
Des hypothèses physiopathologiquesmettent en avant l’intérêt de corriger cettehyper-activité neuronale aberrante sourcede l’acouphène.
Nous savons que le courant électriquereste toujours capable de faire naître une sensation sonore dans une oreillecophotique (1-2). Cette technique estrégulièrement employée en cliniquequand on stimule électriquementl’environnement de l’oreille interne parvoie transtympanique. Mais les résultatsen sont très variables et la stimulationainsi fournie ne peut pas être permanente.
Cette stimulation peut déclencher unmasquage de l’acouphène, soit uniquementpendant la durée de la stimulation, soitprolongé après l’arrêt de la stimulation :cette “inhibition résiduelle” peut être plusou moins durable , mais par définition,jamais ni permanente ni définitive.L’explication de ce bénéfice n’est à ce jourpas vraiment claire. On peut, dans le
registre psychologique par exemple,évoquer la possibilité que cettestimulation constitue un objettransitionnel entre le médecin et sonpatient... Un effet somatique n'estenvisageable que si la stimulationperdure, au point de modifier lesconditions locales d'excitabilité de lacellule sensorielle, ou le réarrangementdes circuits centraux vis à vis de ladésafférentation, ce qui n'est pas le cas desstimulations temporaires transtympaniques.
Une recherche multicentrique est en coursqui propose une stimulation à la fenêtreovale avec une électrode en forme decupule, à l’extrémité d’un “piston -téflon”. Pour une otospongiose, il s’agitdonc simplement de changer le piston etd’implanter le générateur sous la peau,comme le processeur d’un implantcochléaire, avec son générateur externe.(Voir figure).
Une étude précédente (3) a été complétée (4).8 patients dont une oreille cophotiquegénérait des acouphènes chroniques,invalidants, résistants à tout traitement,ont été implantés. La sensation sonoreainsi créée induit bien l’habituation et cespremiers résultats favorables ont conduità cette extension multicentrique.L’évaluation de cette technique étaitréalisée
- par l’observation des variations de lastimulation électrique choisie par lepatient
- par la tenue quotidienne d’un journald’observance et d’observation tenu parle patient : durée quotidienne de port de
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients

2928
Sensorineural hearing loss in elderlypatients (presbycusis) results fromatrophy of hair cells in the cochlea,
degeneration of nerve fibres in thecochlear ganglion and cochlear nuclei,changes in metabolism of the inner ear,and impaired blood supply of the spiralligament and vascular stripe. Individualcases of presbycusis do not separate intoa specific type but have mixtures of thesepathologic types, and are termed mixedpresbycusis. Presbycusis is classified as:type I (normal ageing), and type II (pre-existent sensorineural hearing loss, e.g.caused by prolonged exposure toexcessive noise). About 11% patientswith presbycusis complain of annoyingtinnitus, called by some authors‘presbytinnitus’ (PT), being usually astable, high-pitched whistling [1-6]. In manycases vestibular disorders can accompanycochlear dysfunction [7]. PT is consideredto begin in the fifth decade of life [7], beinga challenging interdisciplinary therapeuticproblem [8-9]. PT is usually detected in theear with higher hearing threshold [7]. Inmany cases it causes further reduction incommunication skills [7]. The two types ofPT are type I, the minority group (inwhich PT develops as a primary initialcomplaint in association with a pre-existing high tone sensorineural hearingloss), and type II, the majority group (inwhich the PT history is long-standing,with a recent exacerbation, significantpre-existing sensorineural hearing loss,subjective hearing loss, deterioration inspeech discrimination, and significantsystemic complaints) [2-6-7]. Both type I andtype II PT exhibit a mild, gradual,progressive hearing loss, demonstrated inaudiometry as a downward sloping type ofloss [7]. Degenerative changes may involve
not only the cochlea, confirmed inotoacoustic emissions recordings, butretrocochlear parts of the auditorypathway (low scores on speechdiscrimination, which is a very sensitivetest for pathologies of the centralsegments of the auditory pathway) [1].Tinnitus characteristics are assessed usingdetailed questionnaires [9]. The tinnituspatients require a very compassionateattitude, particularly during the initialinterview [10]. Statements that “there isnothing that can be done” are highlyinappropriate and should be avoided [10].The principles of sound therapy withtinnitus generators used in normallyhearing subjects are particularly difficultto obtain in elderly subjects with PTaccompanying sensorineural or mixedhearing loss. Properly fitted hearing aidcan amplify the level of background noiseand thus reduce the perception of PT[8-9-11-12-13].
Patients with PT require thoroughdiagnostic procedures to exclude life-threatening causes of the complaint [14].
The evaluation of subjective tinnitusintensity is accomplished using a scale.The most commonly used is the scaleranging from 0 to l0 [11-13]. Elderly patientssuffering from intense PT are usuallyready to accept the fitting, even whentheir hearing is relatively good [11]. Szymiecet al. [l0] obtained satisfactory results in PTtreatment of 29 persons after fitting themwith hearing aids. Also, Nicolas-Puel etal. [8] reported a successful clinical coursein 18 patients with PT. Shulman observedinterference in speech discrimination,particularly in type II PT [7]. In patientswith subjectively louder tinnitus, areas ofimpaired hair cells are most probably
wider than in individuals with minorcomplaints. Background noise suppliedby the hearing aids influences a greaternumber of the hair cells and thus givessignificantly greater improvement inthose subjects than in patients withsubjectively quieter tinnitus. Rosenhall [3]
proved that a lifetime of exposure tonoise is likely to have negative effects onhearing, but determining the interactionbetween noise-induced hearing loss andage-related hearing loss is difficult. Themost commonly accepted assumption is asimple accumulating effect of noise andageing on hearing, particularly oncochlear pathology [3]. However, both aless than additive effect and a supra-additive effect have been proposed [3-7].Podoshin et al. [2] and Rosenhall andKarlsson [13] proved a correlation betweenthe severity of tinnitus and a history ofexposure to noise. Ueda et al. [6] notedhigh-pitched tinnitus (above 4000 Hz) inboth presbycusis and noise deafness.Therefore, if the main functional defectcausing tinnitus is dysfunction of theorgan of Corti (pathological recordingsof otoacoustic emissions, 100% speechdiscrimination), fitting the patient withhearing aids could be effective for PT.
It is concluded that the results of theclinical studies confirm effectiveness offitting the majority of patients withtinnitus in presbycusis with hearing aids.In patients with unilateral sensorineuralhearing loss and tinnitus fittingexclusively the impaired ear is effective.Individuals with bilateral complaintsrequired bilateral fitting. Effectiveness offitting in elderly patients depends onspeech discrimination scores prior tofitting.
de salicylate, ils exécutent la tâche enl’absence de son. En fait, l’acouphèneperçu par l’animal fait office de “sondéclenchant” et induit pour le comportementmoteur. L’animal perçoit son acouphènecomme un son extérieur et exécute latâche. Nous avons ainsi deux moyens(electrophysiologique et comportemental)pour objectiver et quantifier la présenced’un acouphène chez l’animal.
Nous avons pu ainsi disséquer lesmécanismes moléculaires impliqués dansla genèse des acouphènes et montrerqu’ils sont liés à un dérèglement, dans lacochlée, de la neurotransmission entrecellules sensorielles et fibres du nerfauditif. Ce dérèglement est du à uneactivation anormale des récepteursNMDA du glutamate (neurotransmetteurdes cellules sensorielles), qui créent desactivités parasites en l’absence de toutestimulation sonore. Ces activité parasitesse propagent le long de la voie auditive,
jusqu’au cortex, où elles sont perçuescomme un son (acouphène). Ce modèle“salicylate” nous a aussi permis demontrer chez l’animal que, si l’anxiété necrée pas d’acouphènes, elle potentialisaitgrandement leur perception (2). Cesrecherches sont maintenant étendues auxgrands pourvoyeurs d’acouphènes quesont le bruit ou le vieillissement del’oreille interne (presbyacousie) ; en effet,ces pathologies se caractérisent par desaltérations des fibres du nerf auditif liéesà la toxicité au glutamate (excitotoxicité).La connaissance des mécanismes degénération des acouphènes permet deproposer des stratégies thérapeutiquesciblées sur la neurotransmission dans lacochlée. En appliquant au contact de lacochlée, des molécules qui bloquentsélectivement les récepteurs NMDA, onstoppe les activités anormales du nerfauditif et les acouphènes induits par lesalicylate !
On voit bien l’intérêt clinique de telsrésultats. L’obstacle majeur à la mise enœuvre d’essais cliniques réside dans leseffets secondaires des substances délivréespar voie générale. Par exemple, les anti-NMDA efficaces sur les acouphènes ont deseffets catastrophiques sur l’apprentissageet la mémoire. La mise au point d’unepharmacologie locale (trans-tympanique),issue des recherches sur l’animal, vapermettre de s’affranchir de ces effetssecondaires. Souhaitons que les essaiscliniques suivent de près ces recherchesexpérimentales. D’autant qu’avec les“bruits de loisirs” toute une “jeune”génération de sourds et d’acouphéniquesest en train de se constituer. Autrementdit, les problèmes auditifs liés à l’âge(presbyacousie), au lieu de débuter à 60-70 ans, comme c’est le cas aujourd’hui,vont débuter bien plus tôt, dès 35-40 ans.
Légende de la figure : Thérapie in situ sur une modèle comportemental d’acouphènes chez le rat.
A Les animaux sont conditionnés à sauter à unmât en réponse à une stimulation sonore.Chaque série est constituée de 10 essais. Leconditionnement en lui-même nécessite de 4 à7 séries d’une durée comprise entre 15 et 20minutes. Une fois conditionné, l’animal est testéquotidiennement pendant 9 jours. Deux types demesures sont réalisées : 1) les réponsescorrectes (le nombre de fois où l’animal exécutela tâche en réponse au son) et 2) les faux positifs(le nombre de fois où l’animal exécute la tâchealors qu’aucun son ne lui est présenté). En
absence de son, l’animal n’exécute pas la tâcheet le nombre de faux positif est quasi nul(contrôle). Si ce même animal reçoit uneinjection quotidienne de salicylate (300mg/kg,i.p.), il exécute la tâche alors qu’aucun son ne luiest présenté. En fait, il se comporte comme s’ilentendait un son parce qu’il a un acouphène.
B L’administration i.p. de m-Chlorophenylpiperazine(m-CPP), connue pour induire de l’anxiété chezl’animal et chez l’homme, n’induit pasl’apparition d’acouphènes. Par contre, ce
traitement potentialise la perception desacouphènes induits par le salicylate. Autrementdit, si l’anxiété induit pas d’acouphènes, elleexacerbe, voire démasque, la perceptiond’acouphènes existants ou pré-existants. Danstous les cas, la mise en place d’un gelfoam(Gelita tampon) d’un gelfoam contenant unantagoniste des récepteurs NMDA bloquent lesacouphènes chez tous les animaux, y comprisceux potentialisés par l’anxiété. (d’après Guittonet al., 2003, 2005).
JEA
N-L
UC
PU
EL
References :
1. Guitton MJ, Caston J, Ruel J, Johnson RM, PujolR, Puel JL. 2003 Salicylate induces tinnitusthrough activation of cochlear NMDAreceptors.J Neurosci. May 1;23(9):3944-52.
2. Guitton MJ, Pujol R, Puel JL. 2005 m-Chlorophenylpiperazine exacerbates perceptionof salicylate-induced tinnitus in rats.Eur JNeurosci. Nov;22(10):2675-8.
“Management of the tinnitus patient with presbycusis”OLAF ZAGÓLSKI
Correspondence: Olaf Zagólski MD, PhD, ul. Dept. of Otorhinolaryngology, Diagnostic and Therapeutic Medical Centre ‘Medicina’, Dunin-Wàsowicza 20/II/9, 30-112 Kraków, Poland. E-mail: [email protected]
References:
1. Schuknecht HF, Gacek MR 1993 Cochlearpathology in presbycusis. Ann Otol RhinolLaryngol. 102:1-16.
2. Podoshin L, Ben-David J, Teszler CB 1997Pediatric and Geriatric Tinnitus. Int Tinnitus J.3:101-103.
3. Rosenhall U 2003 The influence of ageing onnoise-induced hearing loss. Noise Health.20:47-53.
4. Preyer S, Bootz F 1995 Tinnitus models for usein tinnitus counselling therapy of chronictinnitus patients. HNO 43:338-51.
5. Nagel D, Drexel MK 1989. Epidemiologicstudies of tinnitus aurium. Auris Nasus Larynx16,Suppl 1:23-31.
6. Nicolas-Puel C, Faulconbridge RL, Guitton M,Puel JL, Mondain M, Uziel A 2002Characteristics of tinnitus and etiology ofassociated hearing loss: a study of 123patients. Int Tinnitus J. 8:37-44.
7. Oliveira CA, Venosa A, Araujo MF 1999 Tinnitusprogram at Brasilia University Medical School.Int Tinnitus J. 5:141-3.
8. Szymiec E, DàBrowski P, Banaszewski J,Szyfter W 2002 The problem of tinnitus inpatients with presbyacusis. Otolaryngol Pol.56:357-60.
9. Henry JA, Jastreboff MM, Jastreboff PJ,Schechter MA, Fausti S.A. 2002 Assessment ofpatients for treatment with tinnitus retrainingtherapy. J Am Acad Audiol. 13:523-44.
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients

3130
References:
1. Brackmann DE. 1981. Reduction of tinnitus incochlear implant patients. J Laryngol OtolSuppl 4:163–165.
2. Ito J, Sakakihara J. 1994. Tinnitus suppressionby electrical stimulation of the cochlear walland by cochlear implantation. Laryngoscope104:752–754.
3. Quaranta N, Wagstaff S, Baguley D. 2004.Tinnitus and cochlear implantation. Int J Audiol43:245–251.
4. Tyler RS, Kelsay D. 1990. Advantages anddisadvantages reported by some of the bettercochlear-implant patients.Am J Otol 11:282–289.
5. Ruckenstein MJ, Hedjepeth C, Rafter KO, et al.2001. Tinnitus suppression in patients withcochlear implants. Otol Neurotol 22:200–204.
6. Demajumdar R, Stoddart R, Donaldson I, PropsW. 1999. Tinnitus, cochlear implants and howthey affect patients. J Laryngol Otol Suppl113:24–26.
7. Souliere CR, Kileny PR, Zwolan TA, Kemink JL.1992. Tinnitus suppression following cochlearimplantation–a multifactorial investigation.Arch Otolaryngol Head Neck Surg118:1291–1297.
8. McKerrow WS. Tinnitus suppression bycochlear implants. 1991. Ann Otol RhinolLaryngol 100:552–558.
9. Giraud AL, Price CJ, Graham JM, FrackowiakRSJ. 2001. Functional plasticity of language-related brain areas after cochlearimplantation. Brain 124:1307–1316.
10. Salvi RJ, Lockwood AJ, Burkard R. 2000.Neural Plasticity and Tinnitus. In RS Tyler (ed),Tinnitus Handbook. San Diego: Singular.123–148.
Figure Legend:
Figure 1: Evolution of tinnitus after cochlearimplant activation
T innitus is a frequent symptom,occurring in approximately 10 to15% of adults and increasing up
to 33% in the elderly population (1, 2). Inmany patients, tinnitus becomes chronic,lasting for several years. Maladaptiveplastic brain changes might account forsuch instances of sustained symptoms,reminiscent of the postulatedpathophysiology of phantom pain orvisual hallucinations after blindness. Iftinnitus is associated with a dysfunction ofbrain activity, then it is conceivable thattreatments aiming at a modulation of thecortical activity might be suitable for thiscondition. Indeed recent studies show thattwo methods of noninvasive brainstimulation – repetitive transcranialmagnetic stimulation (rTMS) andtranscranial direct current stimulation(tDCS) - are powerful tools to modulatebrain excitability. Consistent with thisnotion, it has been shown that rTMS ofthe auditory cortex can induce a tinnitussuppression (3-5).
We performed a study to confirm thenotion that modulation of cortical activityin temporoparietal cortex can suppresstinnitus and explore whether such effectcan also be achieved by transcranial directcurrent stimulation (tDCS). In tDCS, thecerebral cortex is stimulated through aweak dc current in a non-invasive andpainless manner. Several studies haveshown that this technique might modulatecortical excitability in the human motor (6)
and visual cortex (7). In rTMS, a time-
varying magnetic field generates an electriccurrent inside the skull, where it can befocused and restricted to small brain areasby appropriate stimulation coil geometryand size (8). It has been demonstrated thatthis current, if applied repetitively (rTMS),induces a cortical modulation that lastsbeyond the time of stimulation (8).
Patients and methods:
We studied 7 patients with chronic tinnitus(4 men and 3 women; mean age of 51.7 ±8.4 years). All had twice unilateral tinnitus(tinnitus on both ears) and bilateralhearing loss that varied from 10 to 50 dB.Two patients had both high (>2000Hz)and low (<2000Hz) frequencies affectedand the other five patients had only high-frequency hearing loss.
Each patient underwent six different typesof stimulation: 10-Hz rTMS of the lefttemporoparietal area (LTA), 10-Hz rTMSof mesial parietal (Pz) area, sham rTMS,0anodal tDCS of LTA, cathodal tDCS ofLTA and sham tDCS. The order of these
conditions was counterbalanced andrandomized across subjects. We evaluatedtinnitus reduction using a scale in whichpatients were asked to rate tinnitus changefrom 0 to 4 with 0 indicating no reduction,1 to 3 indicating slight, marked and strongreduction, and 4 indicating completesuppression of tinnitus immediately afterstimulation (in the most symptomatic ear).
Transcranial magnetic stimulation wasapplied with the following parameters:frequency of 10Hz and stimulationintensity of 20% above motor threshold(MT). Each patient received nine trains (3 for each condition) of 30 stimuli (3 seconds-duration). There was an intervalof 5 minutes between trains. Transcranialdirect current stimulation was wastransferred by a saline-soaked pair ofsurface sponge electrodes (35cm2) anddelivered by a specially developed, battery-driven, constant current stimulator. Aconstant current of 1mA intensity wasapplied for 3 minutes.
Reduced tinnitus has been reportedafter cochlear implant surgery,including in the contralateral
ear [1-2-3]. Understand the suppressionmechanism of tinnitus by cochlearimplant may help us to understand thepathophysiology of tinnitus and improveits treatment.
The purpose of our research was to studytinnitus before surgery and afteractivation of the cochlear implant, toobserve the suppression of tinnitusperception and to correlate these resultswith data in the literature.
We conducted a retrospective studyinvolving 29 adults who had post-lingualsensorineural hearing impairment andunderwent surgery for Nucleus 24Kmultichannel (Cochlear Ltd.) cochlearimplant at the Cochlear Implant Sector ofthe Otorhinolaryngology, Head andNeck Surgery Department, University ofCampinas (UNICAMP), São Paulo,Brazil, from May 2003 to June 2005. Afterthe internal component was activated, thepatients completed a questionnaire.
Before surgery, 21 individuals (72%)presented with tinnitus, which wasbilateral in 14 patients (67%). After thecochlear implant was activated, tinnituscompletely disappeared in seven patients(33%) and partially decreased in eight(39%). Tinnitus remained unaltered inthree patients (14%) and worsened inthree (14%). One individual reported theonset of tinnitus after the device beganfunctioning.
Twelve (86%) of the 14 individuals whopresented with bilateral tinnitus reportedeither complete disappearance ordecrease in both ears and, in 2 patients
(14%), the tinnitus worsened, even in thecontralateral ear. Seven (47%) of the 15patients who continued with tinnituswere aware of the buzz only when thedevice was disconnected; 5 patients(33%) perceived tinnitus even when theimplant was activated; and 3 patients(20%) continued under both conditions.
After the internal component wasactivated, patients completed aquestionnaire. Before surgery, 21 of the29 patients (72%) who later underwentcochlear implant surgery presented withtinnitus, which was bilateral in 14 cases(67%). After the cochlear implant wasactivated, seven patients (33%) presentedwith total suppression, and eight patients(39%) reported partial relief. In the 14cases with bilateral symptoms, tinnituswas totally suppressed or decreased inboth ears in 12 cases (86%).
Our results in relation to tinnitussuppression and partial suppression(72%) were similar to those found in theliterature [2-4-8].
The literature contains no consensusregarding the cochlear implantmechanism of tinnitus suppression. Themasking effect most probably works likeenvironmental noise that inducesvibration of the basilar membrane at thedamaged site, suppresses abnormalactivity of the cilia cells in the internalear, and produces a buzzing noise. Asimilar effect could be produced by ahearing prosthesis [2].
Electrical stimulation of the implant istransmitted to the cochlear and superiorolivary nuclei, causing direct inhibition ofthe inner-ear cilia cells through theefferent pathways. Activation of this
efferent system would explain thesuppressive effect of the cochlear implanton tinnitus [2].
Asymmetrical stimulation produced bythe cochlear implant has proved to bebeneficial even in the contralateral ear [2-4-7-8].The plastic alterations in the corticalareas may have a physiologicalexplanation [9]. According to Salvi et al. [10],spontaneous action of the damaged areasof the hearing system is responsible forsome cases of tinnitus. Reorganization ofthese areas, which occurs after cochlearimplant, may reduce this activity and, asa result, diminish tinnitus. Owing todecussation in the central hearing system,decrease of tinnitus is also expected in the contralateral ear after cochlearimplantation [3]. In our study, 12 patientsalso presented with tinnitus improvementin the contralateral ear.
Reports have cited the possibility oftinnitus worsening or being exacerbatedafter cochlear implant surgery but,according to Ruckenstein et al. [5], thisprocedure does not present a significantrisk for poorer outcomes. In our study,we observed tinnitus to worsen in onlythree patients.
Conclusion:
Cochlear implants had a positive effecton tinnitus and could also induce itspartial or total suppression in thecontralateral ear.
10. Bartnik G, Fabijaƒska A, Rogowski M.: Effectsof tinnitus retraining therapy (TRT) for patientswith tinnitus and subjective hearing lossversus tinnitus only. 2001.Scand Audiol Suppl.52:206-8.
11. Zagólski O 2005 Tinnitus in elderly patients.Otolaryngol Pol. 59:91-6.
12. Ueda S Treatment of tinnitus with intravenouslidocaine. 1992. Nippon Jibiinkoka GakkaiKaiho. 95:1389-97,
13. Rosenhall U, Karlsson AK 1991.Tinnitus in oldage. Scand Audiol. 20:165-71.
14. Ueda S, Asoh S, Watanabe Y 1992 Factorsinfluencing the pitch and loudness of tinnitus.Nippon Jibiinkoka Gakkai Kaiho. 95:1735-43.
OL
AF
ZA
GÓ
LSK
I
“Can Cochlear Implants Decrease Tinnitus?”EMA YONEHARA, RAQUEL MEZZALIRA, PAULO R.C. PORTO, WALTER A. BIANCHINI, LUCIANE
CALONGA, SILVIA BADUR CURI AND GUITA STOLER. Dept. Otorhinolaryngology, Head and Neck Surgery, School of Medical Sciences, University of Campinas, Rua Visconde de Inhaúma,
480 apto 21A, São Paulo, SP, Brazil 04145-030. E-mail: [email protected]
Noninvasive brain stimulation for the treatment of tinnitusFELIPE FREGNI, MD, PHD, MMSC
Center for Noninvasive Brain Stimulation, Beth Israel Deaconess Medical Center, Harvard Medical School at Boston. Address for correspondence: Center for Noninvasive Brain Stimulation - Harvard Medical School - 330 Brookline Ave -
KS 452, Boston, MA 02215. USA. E-mail: [email protected]
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
Figure 1
Figure 2

3332
Même si de nombreusesthérapeutiques palliatives(Thérapies cognitives et
comportementales, Tinnitus RetrainingTherapy et autres thérapies sonores...),visant à en améliorer la tolérance, ont étédeveloppées en matière d’acouphènesubjectif invalidant aucun traitementscientifiquement validé ne permetaujourd’hui d’en atténuer l’intensitépropre. Si la survenue de l’acouphène fait leplus souvent suite à une lésion périphériquecochléaire, justifiant les tentativesexpérimentales de traitement local précoce,la mise en jeu secondaire de foyerspersistants d’hyperactivité et deréorganisation structurelle au sein des voiesauditives centrales, en particulier au seindes cortex auditifs (fig 1), peut êtreaujourd’hui considérée comme le corrélatneural de la perception consciente del’acouphène chronique [1]. Agir sur cettehyperactivité est l’objectif de la stimulationmagnétique transcrânienne répétée (SMTr).
La SMTr est en effet une technique non invasive permettant de moduler
transitoirement l’activitécérébrale des aires corticalessituées immédiatement sousle scalp (fig 2), ce qui est lecas des cortex auditifs. Endélivrant localement unchamp magnétique intense(>2Tesla) sur une zone ciblede quelques centimètrescarrés préalablement définiesur des critères anatomiques(IRM structurelle) oufonctionnels (IRMfonctionnelle, PETscan oumagnétoencéphalographie)la SMTr est à même deproduire, en fonction desparamètres de stimulation,une activation ou uneinhibition prolongée del’activité neurale de la zonecible et/ou des structurescérébrales qui lui sont fonctionnellementconnectées. Ces champs magnétiques sontappliqués, sur les cortex auditifs primairesou secondaires détectés comme hyperactifs,à une intensité d’environ 100% du seuil
déclenchant une réaction motrice, à lafréquence de 1Hz (stimulation de typeinhibiteur avec effet retardé et prolongé),pour une période de 20 minutes (1200stimulations par séance), 4 à 5 jours parsemaine pendant une à deux semaines.Cependant d’autres paramètres destimulation sont possibles comme lesstimulations à haute fréquence (>10Hz)dont l’effet serait plus bref par sidérationde l’activité neurale.
La SMTr est employée depuis denombreuses années, et a fait la preuve deson efficacité clinique, dans le domainepsychiatrique (syndromes dépressifs,hallucinations auditives…) et dans celui dela prise en charge de la douleur chroniqueneuropathique de déafférentation dont onconnaît les parentés physiopathologiquesétroites avec l’acouphène chronique.
Results:
There was an overall significant maineffect of type of stimulation (Chi-square=18.48, D.F.=5, p=0.0024). Post-hoc analysis showed that there was asignificant effect on tinnitus reductionafter rTMS of LTA (p=0.015) and anodaltDCS of LTA (p=0.014). Three patients(42%) had a significant reduction intinnitus (tinnitus reduction of at least 1 inmore than one trial) after rTMS of LTAand anodal tDCS of LTA. There were noresponders after sham rTMS, active rTMSof Pz, sham tDCS and cathodal tDCS(figure 1).
The same patients responded to rTMS andtDCS, therefore, in an exploratorymanner, we analyzed whether these threepatients differed from the four non-responder patients regarding clinicalfeatures. This analysis disclosed thatresponders had less hearing loss comparedto non-responders – the mean hearingthreshold for responders was 14.2 ± 2.0dB (range 10 to 15) and for non-responders was 21.9 ± 11.9 dB (range 15to 50).
Conclusion:
This study shows that 10-Hz rTMS andanodal tDCS of the left temporoparietalarea (LTA) result in a transient reductionof tinnitus. There were no adverse effectsassociated with these two types ofstimulation and the effects were short-lasting. This study encourages furtherexploration of both techniques of non-invasive brain stimulation – rTMS andtDCS – for the study of thepathophysiology and the treatment oftinnitus. Studies investigating the effects ofconsecutive stimulation sessions of longerduration on tinnitus might find greaterand long-lasting effects on tinnitusreduction.
References:
1. Nondahl DM, Cruickshanks KJ, Wiley TL, KleinR, Klein BE, Tweed TS. Prevalence and 5-yearincidence of tinnitus among older adults: theepidemiology of hearing loss study. J Am AcadAudiol 2002;13(6):323-31.
2. Sindhusake D, Golding M, Wigney D, Newall P,Jakobsen K, Mitchell P. Factors predictingseverity of tinnitus: a population-basedassessment. J Am Acad Audiol 2004;15(4):269-80.
3. Plewnia C, Bartels M, Gerloff C. Transientsuppression of tinnitus by transcranial magneticstimulation. Ann Neurol 2003;53(2):263-6.
4. Langguth B, Eichhammer P, Wiegand R, et al.Neuronavigated rTMS in a patient with chronictinnitus. Effects of 4 weeks treatment.Neuroreport 2003;14(7):977-80.
5. Eichhammer P, Langguth B, Marienhagen J,Kleinjung T, Hajak G. Neuronavigated repetitivetranscranial magnetic stimulation in patientswith tinnitus: a short case series. Biol Psychiatry2003;54(8):862-5.
6. Nitsche MA, Paulus W. Sustained excitabilityelevations induced by transcranial DC motorcortex stimulation in humans. Neurology2001;57(10):1899-901.
7. Antal A, Nitsche MA, Paulus W. Externalmodulation of visual perception in humans.Neuroreport 2001;12(16):3553-5.
8. Pascual-Leone A, Bartres-Faz D, Keenan JP.Transcranial magnetic stimulation: studying thebrain-behaviour relationship by induction of‘virtual lesions’. Philos Trans R Soc Lond B BiolSci 1999;354(1387):1229-38.
Figure Legend:
Figure 1: Tinnitus reduction immediately aftereach type of stimulation: rTMS of LTA (lefttemporoparietal area), sham rTMS, rTMS of Pz(mesial parietal area), anodal tDCS of LTA, cathodaltDCS of LTA, sham tDCS. Tinnitus reduction wasevaluated by a scale in which 0 indicates noreduction and 1 slight, 2 marked and 3 strongreduction and 4 complete suppression of tinnitusimmediately after stimulation. Each bar representsmean scores for each treatment and error barsrepresent S.E.M.
Table 1. Demographic and clinical characteristics
rTMS of LTA – repetitive transcranial magnetic stimulation of left temporoparietal area; A-tDCS of LTA – Anodal transcranial dc stimulation of left temporoparietal area;F – female; M – male; R – right; L – left.
R=L indicates similar tinnitus intensity (but not pitch) – twice unilateral tinnitus.
FEL
IPE
FR
EG
NI
Figure 1:Stimulateur magnétique.
“Stimulation magnétique transcrânienne répétée (SMTr) : une nouvelle approche thérapeutique des acouphènes subjectifs invalidants ?”
ALAIN LONDERO Hôpital Européen Georges Pompidou, Service ORL, 25 rue Leblanc, 75015 Paris, France. E-mail : [email protected]
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
Figure 1
Figure 2

3534
The stimulation parameters for tinnitussuppression are such that the patient isnot aware of the stimulation being on oroff. Side effects can be induced atabnormally high frequency, high intensitystimulation. Such side effects can consistof a feeling of being tipsy, altered spatiallocalization of external sounds, hearingperception changes (hearing perceived asbeing clearer, even for their own voice),word finding problems, dizziness, andvertigo. At normal stimulation settingsthese side effects are not noted.
In patients with successful tinnitussuppression, also the associated hyperacusis,if present, improves as well, as does afeeling of aural pressure, but the pressure
and the tinnitus do not always decreasewith identical programming of theirstimulation
Epileptic seizures never occurred duringTMS but occurred in two patients. Inthese two patients the epileptic seizuresmost likely occurred because of prolongedstimulation without stimulation freeintervals when the patient was stillhaving an external stimulator, whichcould not be programmed at that time bythe investigator, but relied on patientcooperation.
With the IPG implanted, no epilepticseizures were seen with currentstimulation parameters: high frequency
stimulation (>10 Hz) in cycle mode, withthe stimulator 5 seconds on, 5 seconds offand low frequency stimulation (<10 Hz)in cycle mode with the same parametersor a cycle mode with 1 to15 minutes on,30 seconds to 5 minutes off.
The preliminary results of the firstimplantations suggest that the followingcriteria can be offered, albeit withprecaution : unilateral tinnitus of puretone type, of recent origin and withsuppression on TMS could be goodsurgical candidates for electrodeimplantation. New stimulation designsmight be capable of extending theinclusion criteria.
References:
Smith JA, Mennemeier M, Bartel T, Chelette KC,Kimbrell T, Triggs W, Dornhoffer JL. Repetitivetranscranial magnetic stimulation for tinnitus: a pilotstudy.Laryngoscope. 2007 Mar;117(3):529-34.
Figure legend:
Figure 1: Lateralized tinnitus is correlated to highlysynchronous gamma band hyperactivity in thecontralateral auditory cortex. In lateralized tinnitusfMRI activation is decreased on the side contralateralto the side of perceived tinnitus. This may beexplained by a higher neural activity during rest or bya lower neural activity during stimulation on theaffected side (saturation effect) (Smits et al, 2007).
Any lesion along the auditory tract,interfering with its ascending ordescending pathways can
generate an auditory phantomperception, better known as tinnitus.Auditory deprivation is a strong activatorof neural plasticity, resulting inreorganization of the auditory cortex.Tinnitus is also associated with increasedsynchronous auditory cortex hyperactivity,with a persistent increase in gamma bandactivity. It is plausible that the increasedsynchrony is responsible for thereorganization following simple Hebbianmechanisms (cells that fire together wiretogether). The auditory cortex hyperactivityand reorganization can be visualizedusing functional neuroimaging techniques.This visualized area of hyperactivity canbe used as a target for modulatingassociated abnormal neuronal activity.Based on this philosophy 20 patientshave been implanted with auditory cortexelectrodes so far.
Patients are selected for implantation ofan extradural auditory cortex electrodebased on a positive response to transcranial
magnetic stimulation, targeting theauditory cortex contralateral to the sideto where the tinnitus is perceived.Selection criteria are intractable unilateraltinnitus with >50% suppression ontranscranial magnetic stimulation afterexclusion of all treatable causes. Inpatients who have >50% suppression onTMS a frequency specific fMRI isperformed, presenting sounds matched tothe tinnitus frequency, in an attempt tofind the neural generator of the patient’stinnitus. The rationale is that the gammaband ERS (event related synchronization),which correlates with the tinnituspercept, also correlates and co-localizeswith BOLD signal effect on fMRI(figure). The fMRI can subsequently beincorporated in a neuronavigationmachine to localize the area exactly wherean electrode has to be implanted.
Using this technique mean pure tonetinnitus and white noise suppression issignificant at 97% and insignificant at24% respectively. In patients whosetinnitus recurs every time afterreprogramming the electrode an electrode
can be implanted on the primary auditorycortex resulting in a stable suppression.This is based on animal studies thatsuggest that plasticity of the secondarycortices is greater than on the primarycortices. However in the near future newstimulation designs should be capable ofsolving the problem as well without theneed for reoperation. In two patientswith bilateral tinnitus no suppressioncould be obtained. However, veryrecently a third patient with bilateraltinnitus was implanted with anextradural electrode overlying thesecondary auditory cortex resulting in abilateral tinnitus suppression.
It is not known whether TMS has apredictive value for electrodeimplantation. We have only implantedone patient with unilateral pure tonetinnitus of recent origin, i.e. the idealprofile who was TMS non-responsive,and have not been able to suppress histinnitus with electrical stimulation either.A randomized study comparing TMSresponders to non-responders should beable to solve this important question.
Références :
1. Eggermont JJ, Roberts LE. 2004.The neuroscienceof tinnitus. Trends Neurosci; 27: 676–82.
2. Londero A et al. 2006. Repetitive transcranialmagnetic stimulation (rTMS): a new therapeuticapproach in subjective tinnitus? Neurophysiologie
Clinique; 36: 145–155.
AL
AIN
LO
ND
ER
O
DIR
K D
E R
IDD
ER
, PA
UL
VA
N D
E H
EY
NIN
G, A
AG
E M
OL
LE
R
Plusieurs études cliniques ont récemmentmontré qu’en matière d’acouphènesubjectif invalidant la SMTr permettaitd’obtenir, de façon statistiquementsignificative par rapport à des stimulationsplacebo, une diminution temporaire (maisparfois prolongée jusqu’à plusieurssemaines chez quelques patients) del’intensité de l’acouphène et de la gêne qu’ilprocure. Ces résultats sont prometteurs [2].Ils permettent d’envisager desdéveloppements futurs à la fois sur planthérapeutique mais également sur le plan
d’une meilleure compréhension desmécanismes physiopathologiques centrauxde genèse et d’entretien de la perception del’acouphène.
Il reste que de nombreux points sontencore à élucider en particulier en ce quiconcerne la meilleure méthode dedétermination de la zone cible, lesparamètres optimaux de stimulation, ladurée et la fréquence des séances, le côtéà stimuler préférentiellement en présenced’un acouphène bilatéral, les éventuels
effets secondaires (possible intensificationtemporaire de l’acouphène, problème detolérance de la stimulation qui est trèsbruyante chez les patients hyperacousiques…),les critères de sélection des patients.
Des études cliniques sont en cours qui devraient permettre de répondreprochainement à ces questions de façon àce que la SMTr puisse être raisonnablementajoutée à l’arsenal thérapeutique disponiblepour la prise en charge des patientsacouphèniques chroniques invalidants.
Diagnostic et traitement des acouphènes chez les patientsClinical diagnosis and therapy of tinnitus in patients
“Surgically implanted electrodes on primary and secondary auditory cortex as a treatment for tinnitus”
DIRK DE RIDDER, PAUL VAN DE HEYNING, AAGE MOLLERDept of Neurosurgery and ?ENT, University Hospital Antwerp, Belgium.
School of Behavioral and Brain Sciences, University of Texas at Dallas, USA.
Figure 1

3736
Auteurs / Authors
Nous remercions les auteurs de cette revue pour leur contribution ainsi que la société “Positive Audition” et lesLaboratoires “Ipsen” pour leur soutien :
Auteurs / Authors
NADIR AHMAD MD, MICHAEL D. SEIDMAN MDMD.“Alternative Therapies for Tinnitus”
PAUL AVAN
“Acouphènes : modèles comportementaux chez l’animal”
ANDRÉIA AZEVEDO, MD, RICARDO FIGUEIREDO, MD, MSC
“Tinnitus treatment with drugs”
ERIC BIZAGUET et PAUL EDOUARD WATERLOT
“L’acouphène : le point de vue de l’audioprothésiste”
PIERRE BONFILS
“Acouphènes et thérapie cognitive et comportementale”
DIDIER BOUCCARA
“Traumatisme sonore et acouphènes”
PIERRE CAMPO
“Qu’appelle-t-on acouphènes ou tinnitus ?”
CYNTHIA DARLINGTON PH
“An animal model for testing anti-tinnitus drugs”
DIRK DE RIDDER, PAUL VAN DE HEYNING, AAGE MOLLER
“Surgically implanted electrodes on primary and secondary auditory cortex as a treatment for tinnitus”
JOS J. EGGERMONT
“What’s wrong with the brain in tinnitus?”
BRUNO FRACHET
“ACOUPHENES ET COPHOSE : quand les acouphènes sont encore moins faciles à prendre en charge...”
FELIPE FREGNI, MD, PHD, MMSC
“Noninvasive brain stimulation for the treatment of tinnitus”
LUCY HANDSCOMB
“Analysis of responses to individual items on the tinnitus handicap inventory according to severity of tinnitus handicap”
ROBERT-BENJAMIN ILLING
“Neuroplastic remodelling of the central auditory system invoked by unilateral hearing”
EDWARD LOBARINAS, PH. D RICHARD, J. SALVI, PH.D
“Do Animals Experience Tinnitus? Can They Tell Us?”
ALAIN LONDERO
“Stimulation magnétique transcrânienne répétée (SMTr) : une nouvelle approche thérapeutique des acouphènes subjectifs
invalidants ?”
ALAIN LONDERO
“Pourquoi proposer une prise en charge de l’acouphène chronique invalidant par les TCC (thérapies cognitivo-
comportementales) ?”
AAGE R. MØLLER
“Neural Plasticity in Tinnitus”
ARNAUD NORENA
“Mécanismes neurophysiologiques des acouphènes et approches thérapeutiques potentielles”

39
PUB“Positive Audition®”
MARTINE OHRESSER
“La prise en charge de l’acouphène chronique invalidant”
JOSEPH J. MONTANO, ED. D. ASHA FELLOW LOW
“Self-assessment of Tinnitus: An Important Component of Evaluation and Treatment”
JEAN-LUC PUEL
“Un espoir thérapeutique pour les acouphènes d’origine périphérique”
CATHERINE DE WAELE, MERITXELL ARGENCE
“Effet d’une lésion périphérique et d’une stimulation du nerf auditif chez le rat adulte”
EMA YONEHARA, RAQUEL MEZZALIRA, PAULO R.C. PORTO, WALTER A. BIANCHINI,LUCIANE CALONGA, SILVIA BADUR CURI AND GUITA STOLER.
“Can Cochlear Implants Decrease Tinnitus?”
OLAF ZAGÓLSKI
“Management of the tinnitus patient with presbycusis”
Auteurs / Authors
C O N T A C T
Anne Jol ly
23 rue Bucour t92210 Saint CloudTél. : 01 47 11 07 14E-mail : [email protected]
AGENCE CONSEIL EN ÉDITION ET IDENTITÉ VISUELLELivrets d'accueil, invitations, revues, journaux
C A P N U M A S A N T É

41

Notes
Rendez-vous le Samedi 13 Octobre sur le thème :
“ORL 2007: the Best o f… Amer ican Hospi ta l o f Par is”