Radiothérapie et Tumeurs du sein Irradiation partielle: un ... · COSMETIC EVALUATION (SBG): 265...
76
Radiothérapie et Tumeurs du sein Irradiation partielle: un nouveau standard ? Dr V. De Vos CHU-Tivoli Radiothérapie Centre René Goffin
Transcript of Radiothérapie et Tumeurs du sein Irradiation partielle: un ... · COSMETIC EVALUATION (SBG): 265...

Radiothérapie et Tumeurs du sein Irradiation partielle: un nouveau standard ?
Dr V. De Vos
CHU-Tivoli
Radiothérapie
Centre René Goffin

RADIOTHERAPIE Relations Fondamentales
• Relation dose-effet
• Relation dose-volume
Tumeur contrôle local Tissus normaux effets précoces et tardifs
Tumeur moindre efficacité Tissus normaux plus de toxicité

Tumeurs du sein et Radiothérapie Indications
• Traitement conservateur
Irradiation de la glande mammaire
Irradiation des chaînes ganglionnaires
Irradiation du lit tumoral
Irradiation partielle du sein
• Traitement après ablation du sein
• Traitement de lésions douloureuses

CANCER DU SEIN : Traitement Conservateur
• Comprend :
une chirurgie à minima
une radiothérapie de l’ensemble de la glande
But : garder un sein
avec un bon résultat esthétique
• Popularisé après l’étude
de Veronesi

Traitement conservateur du sein Impact de la Radiothérapie
ECBTG 2005
L’irradiation de la glande mammaire permet de diminuer
les récidives loco régionales.
Une récidive locale est un facteur péjoratif qui se traduit par un
risque plus élevé de progression.
La RT réduit aussi la mortalité
liée au cancer du sein.
Le bénéfice est de 5 à 8 %.
5 RL évitées à 5 ans >>> 1 décès évité à 15 ans
N-
N+ 5 ans 15 ans

Irradiation partielle du sein Les différentes approches
La curiethérapie interstitielle:
• A bas débit
• A haut débite
58
Les techniques intracavitaires:
• Orthovoltage photons (Intrabeam, UK)
• Brachytherapy (Mammosite)
• Intraoperative electrons (Mobétron)
L’irradiation externe par IMRT

Irradiation partielle du sein: 2 définitions
• Irradiation partielle accélérée du sein (APBI)
Irradiation du lit opératoire et des tissus
avoisinants délivrant un dose élevée en
1 à 10 séances en 5 jours
• Irradiation peropératoire (IORT)
Délivre une dose élevée au niveau du lit
opératoire durant l’intervention
La patiente endormie, avec le site opératoire ouvert, est
transportée de façon stérile du quartier opératoire en
radiothérapie dans le bunker

IntraOp’s IOERT Solution The Mobetron
The Mobetron makes IOERT practical to deliver.
“Small and lightweight”
No additional shielding (electrons)
Fits in existing operating rooms, hallways and standard elevators
Can be shared between multiple ORs
The Mobetron eliminates the need
for heroic transport and is dedicated to operating rooms
Can move the machine TO the patient !

Mobetron Applicators
2-piece design
Each Al applicator has three stainless tips: 0o , 15o, and 30o bevels.
Field sizes are 3-10 cm in 5 mm steps.
2mm stainless wall has very low leakage

Quick Check: every treatment day

Facteurs de risque de récidive locale
• La taille de la tumeur
• L’âge
• Le sous-type histologique
• Le degré de différentiation
• L’étendue de la chirurgie
• La dose et volume de RT
Essai EORTC:
un complément de dose au lit tumoral (Boost)
diminue de moitié les récidives

EORTC Boost/no Boost Trial

EORTC Boost/No Boost trial
BCS + AD
251 pts
5318 pts
R
A
N
D
O
M
50 Gy WBRT + 16 Gy Boost
50 Gy WBRT
50 Gy WBRT + 10 Gy Boost
50 Gy WBRT + 26 Gy Boost
Microscopic
complete excision
Microscopic
INcomplete excision

Bartelink et al, JCO 2007
Age < 40
23.9%
13.5%
Age 41-50
12.5%
8.7%
Age 51-60 Age >60
7.8% 4.9%
7.3% 3.8%

Dose? 10Gy vs 16Gy vs 26Gy?
• 5318 pts microscopic complete resection
• 251 pts microscopic incomplete resection
LR S Fibrosis
Boost 6.2 % 82 % 4.4 %*
No Boost 10.2% 82 % 1.6 %
LR S Fibrosis
10 Gy 17.5 % 76.7 % 3 %
26 Gy 10.8% 77.8 % 14.4 %*
LR S
Boost 6.2 %* 82 %
No Boost 10.2% 82 %
LR S
10 Gy 17.5 % 76.7 %
26 Gy 10.8% 77.8 %
* p<0.0001
Bartelink et al. JCO 2007, Poortmans et al. Rad Onc 2009
RL Fibrose OS
RL OS Fibrose

IOERT & BOOST

Surgery
Surgery
Wait
Wait
Treatment 50 Gy
Treatment 50 Gy
Boost (e- or γ) 16 Gy
Boost IORT 9 Gy
Classic scheme for breast
IOERT Boost scheme
Why IOERT Boost for breast tumors ?

RATIONALE FOR IOERT BREAST BOOST
• Shortens overall adjuvant radiation treatment by about 2 weeks
• Decreases possibility of boost missing surgical margins
• Reduced skin dose as boost is given subcutaneously
• Starts adjuvant therapy at the time of lumpectomy when tumor cells most active
• Randomized studies show EBRT electron boost improves local control for every age group (1)
• Lancet meta-analysis and Danish Breast Study Group show that improvement in LC at 5 years impacts long term survival at 15 years (4/1)(2)
• Studies show delay in RT results in higher local recurrences (3)
• Studies show IORT impairs the stimulation of breast cancer cell proliferation caused by surgical wounding (4)
• (1) J. Clin Oncol. 25(22):3259-65, 2007, H. Bartelink, et. al; (2) Lancet 366:2087-2106,2005, M. Clarke, et. al.;
• (3) J. Clin Oncol. 21:555-563, 2003, J. Huang, et. al.; (4) Clin Cancer Res .14(5), 1325-32, 2008, B. Belletti, et. al.

IORT Boost: Outcome (LR)
• TARGIT boost trial
IJROBP Vol.81, N°4, pp. 1091-1097, 2011
(Intrabeam source)
• Series of pilot cases to test the feasability and sefaty of TARGIT-A

TARGIT Boost trial: design
• 299 patients
• Tumor size < 4 cm
• Unifocal
• Treatment schedule
BCS + IORT (20 Gy, kV) WBRT (45-50 Gy/1.8-2 Gy)CT

TARGIT Boost trial: results
• Results (5y LR) compared with:
• EORTC boost trial
• START-B trial
• !!! Small number of pts
• « It was clearly not a selected good-prognosis cohort »
• Results = chance?
• !!! Dose distribution:
• 18 - 20 Gy at the surface of the applicator
• 5 – 7 Gy at 1 cm into the surrouding tissues

IORT Boost: Outcome (LR)
• ISIORT pooled analysis
Radiotherapy & Oncology 108 (2013) 279-286
(Mobetron)

ISIORT Pooled analysis: design
• 7 european institutions
performing IOERT Boost
• 1109 patients (1998-2005)
• Treatment schedule
BCS + IOERT (10 Gy) WBRT (50-54 Gy/1.7-2 Gy)CT
RQ: 10 Gy = 23 Gy (α/β = 4)

ISIORT Pooled analysis: design

ISIORT Pooled analysis: results
• Median F-up: 72,4 months (6 y)
• In-Breast recurrences 16: • 8 (in-quadrant) trus local reccurences
• 8 out-quadrant relapses
• Local control: 99,2 %
• Negative hormonal receptors (IBR)
• In-Quadrant relapses: • ~ grade 3 (multivariate analyses: p = 0,03)
• Role of HER status? (missing 1/3 patient information)
• NO Role of delay between IOERT-Boost & WBRT • < 70 ; 70 ≥ - ≤140; > 140 days

IBTR after 5 yrs. FU: 4.3 vs. 0 % P < 0.1

Breast’s Surgery
• Incision
• Sentinel node detection
• Resection of tumour

Surgical technique
tumor resection till the muscle detachment of the gland shield positioning on the muscle
suture of the tumor bed applicator positionning

Treatment : positioning
• Positioning conus and clamp • Orientation check • Feasibility check

Technique
• Direct visualisation of the tumor bed

Docking
Move Couch and dock with laser system

Traitement

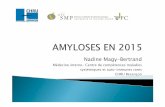
COSMETIC EVALUATION (SBG): 265 PATIENTS
MIN. 3 YEARS POST IOERT (36-96, MED.59)
0%
20%
40%
60%
80%
100%
Patients Score Doctors Score
unacceptable / complications
bad
acceptable
good
excellent
Patients: 93% excellent/good
Doctors: 96 % acceptable, 64% satisfactory

IOERT - THE BEST BREAST BOOST
Direct localization of the surgical bed with uniform exposure of the tissue at risk, reducing the risk of geographic miss
Best dose uniformity compared to other boost alternatives
Reduced skin dose as boost is subcutaneous
Relatively insensitive to depth of tumor or location
Insensitive to tumor asymmetry
Can treat virtually all of BCT eligible patients
Improved radiobiological effect of a high dose in single fraction
EBRT duration shortened by 7-10 days
Small treatment volumes (no seroma)
BUT: prolongation of the anesthesia and enlargement of the incision in case of small tumor

Expérience TIVOLI

Expérience CHU TIVOLI
• 03/2013 – 08/2015: 45 patientes
• CCI 44 / CLI 1
• Boost 36 / Exclusif 9 (1 pte reprise en mastectomie pour DCIS)
• GI 33 / GII 12
• D 22 / G 23

Expérience CHU TIVOLI
• Boost
• > ou = 50 ans
• taille tumorale max 20 mm
• Récepteurs Hormonaux
positifs
• Neu négatif
• Ki de 1 à 20%
• ganglions négatifs
• Exclusif
• 4 ré-irradiations
• 4 > âge et/ou état général
• 1 Antécédents
psychiatriques
RTE: 32 ptes 25x2Gy: 3 ptes hypofractionnement 40Gy 15#, en moyenne 4
semaines plus tard

Expérience CHU TIVOLI
6 semaines post-mobétron
+ RTE en cours (11#)
20 mois post-mobétron
+ RTE (50Gy; 2Gy/#)

Critères d’inclusion BOOST
• Age > ou = 50ans
• BRCA1/2 négatif
• Taille tumorale < ou = 20mm
• Ganglions négatifs (N0)
• Grade I (II à discuter)
• Emboles lymphovasculaires négatifs
• RO positifs
• RP positifs/négatifs
• Neu o à (+)
• Ki à discuter fct autres critères
• Multicentriques NON
• Multifocales NON
• Chimio (néo)adjuvante NON
• CCI OUI
• CLI NON
• DCIS pure NON
• DCIS associé à invasif voir avec AP
• EDCIS/ELCIS associés à invasif NON

MERCI




Irradiation partielle du sein par IOERT exclusif

Irradiation partielle du sein: Une nouvelle approche
Le concept :
La plupart des récidives s’observent
dans le quadrant initialement touché
Donner une dose élevée à un petit volume
Epargner les tissus normaux : poumons/ coeur
Obtenir un bon résultat esthétique
Essai de Milan

Irradiation partielle du sein
• Avantages • Réduction de la durée du traitement
(de 5 à 6 semaines à moins d’une semaine voire pendant la chirurgie)
• Réduction du volume du sein irradié
• Réduction du volume des organes adjacents irradiés
• Inconvénients • Risque de rechute dans une autre partie du sein en cas de foyer occulte
• Problème d’obtenir une analyse anatomo-pathologique en cas de traitement peropératoire

Irradiation partielle du sein: 2 définitions
• Irradiation partielle accélérée du sein: APBI
Irradiation du lit opératoire et des tissus
avoisinants délivrant un dose élévée en 1 à 10 séances en 5 jours
• Irradiation peropératoire: IORT
Délivre une dose élévée au-niveau
du lit opératoire durant l’intervention

Irradiation partielle peropératoire du sein Expérience de Veronesi : Breast Cancer Res.Treat.2010
- 1822 patientes traitées de
1/2000-12/2008
- Lésion unicentrique < 2.5 cm
- Quandrantectomie + IORT 21 Gy
- Suivi médian : 3 ans
Récidive locale : 2.3%
2ème T. mammaire : 1.3%
Survie à 5 ans : 97,4%
RQ: pas d’irradiation
des chaînes
ganglionnaires!!!

Essais de phase III
Essai Targit Lancet 2010
R/ 20Gy

Essais de phase III
Traitement RL à 4 ans
Targit 996
854 IPS
142 IPS+Rtext
RT ext 1025
1.2%
0.95%
Essai Targit Lancet 2010

ESTRO Forum Genève 2013

APBI GEC-ESTRO Trial Polgar et al
• Inclusion criteria
• DCIS ( 5% of the cases)
• Invasive ductal…. Lobular ( 6% of the cases)
• Less than 3 cm
• LV neg
• Margin > 2 mm
• pN0 or pNmic
• 86 % hormonotherapy
• 11 % chemotherapy

APBI GEC-ESTRO Trial Polgar et al
• Radiotherapy
• Whole breast 50 Gy plus a boost of 10 Gy
• PBI
• HDR 32 Gy 8 fr
• HDR 30.3 Gy 7 fr
• PDR 50 Gy
• PTV margin 20 mm

APBI GEC-ESTRO Trial Polgar et al
Acute skin toxicity
RTOG 1 2 3 4
APBI 18.2 2.1 0.2
Ext Rt 49.5 35.7 7
Late skin toxicity at 1 Y
RTOG 1 2
APBI 21.2 1.1
Ext Rt 24 3.7

Targit trial
• Randomization between IORT and Ext RT but if high risk factors additional whole breast (19% of the cases) or
mastectomy
• Two groups for IORT:
immediate (2298) versus delayed (1153)
• 1122 cases with median follow up of 5 Y
• 2020 cases with median follow-up of 4 years

Targit Résultats
EBRT Targit
Ipsilat rec Breast ca death Non cancer death
11 16 35
23 20 17
P= 0.O42
P=0.009
N patients 1730 1731
EBRT 1.3 %
11
Targit
Loc relapse
3.3 % 23
Timing Immediate 6
Delayed 5
Immediate 10
2.3 %
Delayed 13
5.0 %
Death EBRT Targit
Other cancer Cardiovascular
16 112
8 2

Eliot 2000-2007
• T de moins de 2, 5 cm et âge > 48
• Whole breast 50 + 10 Gy
• APBI : 21 Gy
• Patientes eligibles 601/ 654 vs 585/ 651

Caractéristiques
• N: No 876 1à 3 : 246 et > 3 64
• G: G1: 327 / G2: 580 / G3: 255
• Ki67 > 20% : 473
• HER 2+ 39
• Triple négatif : 71
• Luminal A: 441
• Luminal B: 635

Résultats
EBRT IORT
Loc relapse 5 Y Cumulative 8 Y Cumulative 10 Y True loc relapse New breast ca Contralateral Ipsilateral Regional relapse
0.7 % 1.5 % 1.5 %
4 12 12 0 2
5.3 % 6.4 % 9.2 %
20 21 7 14 9
Pas de différence en survie
Nouvelle étude : small T > 1 cm with G1; Ki 67 < 20 %; Luminal A T > 2 cm; N > 4; Gr 3; Triple negatif to add whole breast 21 Gy boost plus 4 Gy x 8 whole breast
?

Tumeurs du sein et Radiothérapie
• Evolution sera l’individualisation du traitement
• Irradiation partielle du sein est une approche pleine d’espoir pour certaines indications
• Les études sont en cours et un plus long suivi reste nécessaire




Essais de phase III
Traitement Réc.Locale
Curiethérapie (IPS)
Rt du sein
6/128
4/130
Essai de Budapest

Courbes d’isodoses pour des électrons
Isodose 90%

EUROPEAN ISIORT POOLED ANALYSIS ISIORT BIO-BOOST
• 1220 Patients from six European
Centers; IORT 10/98 – 10/05
• 58 Pats.: secondary mastectomy
• 6 Pats.: refused WBRT
• 3 pats.: non-primary treatment
• 35 pats.: treatment after October 2005
• Remaining: 1118 Patients
• Median FU: 66.5 mos (1-126 mos.)
66

PATIENT CHARACTERISTICS ISIORT BIO-BOOST
T N G
NS 20 30 66
Cis 10 N0 680 G1 153
T1 762 N1 347 G2 583
T2 303 N2 34 G3 302
T3 6 N3 7 Gx 3
T4 1 Nx 9
Tx 1
T0 4
High-risk selection: N pos. and/or T3/4 and/or G3 and/or age<40 years = n: 763pts. (68,2%) Low-risk selection: T1-2 and N0 and G1-2 and age > 50 year = n: 361pts. (32,28%)
N: 1118; Age: med. 57.6 y (22.5 – 89.9); FUP: med. 66.5 mths (1 – 126)

POOLED ANALYSIS RESULTS MEDIAN FOLLOW-UP = 66.5 MONTHS
68
66.5 mths: 94.8 %
Local Control (all data)
94,0
95,0
96,0
97,0
98,0
99,0
100,0
0 20 40 60 80 100
Survival time [months]
Perc
en
tag
e l
ocal
co
ntr
ol
rate
66.5 mths: 92.3%
66.5 mths: 88.75%
66.5 mths: 99.2 %
LC: 99.2 %
6 Out Quadrant LR
7 In Quadrant („true“) LR

ANALYSIS OF RECURRENCES AT 66.5 MOS. MEDIAN
FU
LR G
3
HR- Dcis Close
Margins (<
2mm)
Close
Margins w/
re-excision
Close
Margins w/o
re-excision
N+ Time
Gap* IORT-
WBI (wks)
Time to
LR
(mos.)
All = 13 7 8 8 8/13 1 7 1 7.5 med. (3.2-31.6)
57 med (12.5-110)
OQ=6 0 2 3 3 0 3 0 6.5 med. (5-8.6)
51.6 med (17-103)
IQ = 7 7 6 5 5 1 4 1 8.4 med. (3.2-31.6)
60.9 med (12.5-110)
69
*whole cohort: median 7 weeks (1.5-35)
The presence of histological risk factors like DCIS components,neg. HR-status,G3 and resection-status may influence the development of all detected LR.

TYPICAL CLINICAL RESULTS OF IOERT FOR
BREAST BOOST
1118 patients from six European centers
68% of patients with one or more adverse factors: young age, positive nodes, T3 or high tumor grade
Median Follow Up 66.5 months (1-126)
In-Breast Recurrences: 13
True Local recurrence: 7
In-Breast Tumor Control Rate: 99.2 %
Overall Survival: 92.3% (5.5 yrs)
Disease Specific Survival: 94.8% (5.5 yrs)
NO BCT STUDIES HAVE DEMONSTRATED
RESULTS AS GOOD
IBTR after 5 yrs. FU: 4.3 vs. 0 % P < 0.1
70

RESULTS IBTR 5 YEARS
Group 1 Group 2 P-value
n 188 190
IBTR 12 (6.4%) 0
5y actuarial
rates of IBTR
4.3% (95%CI 1.9-8.3%)
0.0% (95%CI 0.0-1.9%)
0.0018
Reitsamer et al., Int J Cancer 2006;118:2882-2887

Ipsilateral breast tumor recurrence-free survival

RESULTS IBTR 10-YEARS
Group 1 Group 2
IORT
P-value
n 180 189
IBTR
cumulative
13 (7.2%) 3 (1.6%) 0.0023
10y actuarial
rates of IBTR
7.1% (95%CI 3.2-11.0%)
2.7% (95%CI 0.0-5.9%)
0.062

Ipsilateral breast tumor recurrence rates: 10 years results
P=0.062

RESULTS TRUE LOCAL RECURRENCES 10-YEARS
Group 1 Group 2
IORT
P-value
n 180 189
TLR
cumulative
8 (4.4%) 1 (0.5%) 0.0029
10y actuarial
rates of TLR
4.8% (95%CI 1.5-8.0%)
0.7% (95%CI 0.0-2.0%)
0.016

TRUE LOCAL RECURRENCE-RATES: 10 YEARS RESULTS
P=0.016 Δ 4.1%