Nausées et vomissements post- opératoires (NVPO PONV)...Risque élevé : 4 points / échelle...
28
I I I I Nausées et vomissements post- opératoires (NVPO – PONV) 1 Jacques Berthod Centre de Formation des Soins HFR - Fribourg Jacques Berthod, enseignant EPD ES SA, CFS
Transcript of Nausées et vomissements post- opératoires (NVPO PONV)...Risque élevé : 4 points / échelle...

II II
Nausées et vomissements post-
opératoires (NVPO – PONV)
1
Jacques Berthod
Centre de Formation des Soins
HFR - Fribourg
Jacques Berthod, enseignant EPD ES SA, CFS

II II 2
PAS DE CONFLITS D’INTERETS

II II
➢ Définition des NVPO
➢ Mécanisme physiopathologique
➢ Risques et complications (patient et hôpital)
➢ Facteurs de risque et scores d’évaluation
➢ Agents pharmacologiques
➢ Algorithmes de prise en charge (prévention et ttt)
➢ Pédiatrie
➢ Antalgie par PCA
➢ Moyens non-pharmacologiques
➢ Take hospital message
PLAN
3Jacques Berthod, enseignant EPD ES SA, CFS

II II 4Jacques Berthod, enseignant EPD ES SA, CFS
DEFINITIONS
➢ mouvements objectifs
➢ contraction
➢ expulsion
➢ sensations subjectives désagréables
➢ imminence du vomissement
➢ précoces
➢ tardives

II II 5Jacques Berthod, enseignant EPD ES SA, CFS
RISQUES ET COMPLICATIONS
➢30 % => 80 % groupes à
risques
➢0.2 complications
potentiellement graves

II II 6Jacques Berthod, enseignant EPD ES SA, CFS
MECANISME PHYSIO-PATHOLOGIQUE

II II 7Jacques Berthod, enseignant EPD ES SA, CFS
FACTEURS DE RISQUEConsensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002
(Mal des transports)
Forte et prouvéeMaux des transports
Contradictoire
Jeûne pré-opératoire
Réfuté ou pertinence
clinique limitée

II IIJacques Berthod, enseignant EPD ES SA, CFS
SCORES DE RISQUE VALIDES
+
Apfel Koivuranta Palazzo Synclair BSP (A + S)
Femme + + + + + (x 2)
ATCD NVPO + + + +
Mal des
transports
+ + + +
Non-fumeur + + + + ( x 2)
Morphine
post-op
+ + +
Durée op >
60 min
+ + +
Age < 50 ans + +
Type de
chirurgie *
+ +
+
* Chirurgie laparoscopique, gynécologique, cholécystectomie

II II
SCORES D’EVALUATION DU RISQUE NVPO
9Jacques Berthod, enseignant EPD ES SA, CFS
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002
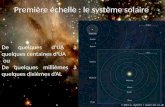
Figure 2. Simplified risk score for PDNV
in adults. Simplified risk score from
Apfel et al.19 to predict the risk for
PDNV in adults. When 0, 1, 2, 3, 4, and
5 risk factors are present, the
corresponding risk for PDNV is
approximately 10%, 20%, 30%, 50%,
60%, and 80%, respectively. PDNV =
postdischarge nausea and vomiting;
PONV = postoperative nausea and
vomiting; PACU = postanesthesia care
unit.
SCORES D’EVALUATION DU RISQUE NVPO

II II
STRATEGIE ANESTHESIQUE
10Jacques Berthod, enseignant EPD ES SA, CFS
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002

II II 11Jacques Berthod, enseignant EPD ES SA, CFS
STRATEGIE ANESTHESIQUE PREVENTIVE
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002
30 ml/kg
1ère action : Diminuer les facteurs de risque causés par l’anesthésie
1. ALR > AG
2. Si AG : PROPOFOL
3. Eviter morphine en post-op si possible
4. Eviter déshydratation

II II 12Jacques Berthod, enseignant EPD ES SA, CFS
AGENTS PHARMACOLOGIQUES
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002
Prix public
fr. 103.40
Fr. ???
Fr. 6.-
Fr , 22.-/ 1mg
Fr. 58.90 / fr. 95.60

II II 13Jacques Berthod, enseignant EPD ES SA, CFS
AGENTS PHARMACOLOGIQUES

II II 14Jacques Berthod, enseignant EPD ES SA, CFS
AGENTS PHARMACOLOGIQUES
A. Pospiech*, B. Yemnga*, F. Veyckemans*, M. De Kock*, PRISE EN CHARGE DES NAUSÉES ET DES
VOMISSEMENTS POSTOPÉRATOIRES : UNE PRIORITÉ, Louvain Med. 2014; 133 (2): 077-085

II II 15Jacques Berthod, enseignant EPD ES SA, CFS
EFFETS SECONDAIRES
Classe de
médicaments
Médicaments Effets secondaires
Anticholinergiques Atropine,
Scopolamine
Sécheresse des muqueuses, troubles
visuels, hallucinations, confusion,
désorientation, rétention urinaire
Antagonistes
dopaminergiques
Métoclopramide
(Primpéran)
Syndrome extrapyramidal, somnolence,
lassitude, vertiges, troubles digestifs,
hypotension orthostatique
Antagonistes
dopaminergiques
DHPB
(Dropéridol)
Syndrome extrapyramidal, somnolence
Allongement du QT (> torsade de pointe)
Hypotension orthostatique
Antagonistes
sérotoninergiques
Odansetron
(Zofran)
Granisétron
(Kytril)
Céphalées, bouffées de chaleur, hoquet
constipation, hypotension, troubles du
rythme cardiaque, douleurs thoraciques
Syndrome extrapyramidal,
Réactions allergiques immédiates

II II 16Jacques Berthod, enseignant EPD ES SA, CFS
Classe de
médicaments
Médicaments Effets secondaires
Corticoïdes Dexamethasone
(Fortecortin)
Augmentation de la glycémie
Antagoniste de la
neurokinine 1
Aprépitant
(Emembed)
Fatigue, constipation, dyspepsie, anorexie,
céphalées, hoquet
EFFETS SECONDAIRES

II II 17Jacques Berthod, enseignant EPD ES SA, CFS
STRATEGIE ANESTHESIQUE PREVENTIVE
2. Administrer un traitement antiémétique au bon moment
en fonction du risque NVPO du patient
Risque faible : 0 – 1 point / échelle d’Apfel (ou 0 - 2 pts sur échelle
BSP)=> Pas de prophylaxie (TIVA dès 1er risque)
Risque moyen : 2 – 3 points / échelle d’Apfel (ou 3-6 pts sur échelle BSP)
TIVA + ttt préventif (Dexaméthasone 4 mg à l’induction
+ DHBP 1mg en fin d’intervention)
Risque élevé : 4 points / échelle d’Apfel (ou 7-10 pts sur échelle BSP)
prévention per-os Aprétitant 40 mg (si disponible) , TIVA + ttt
préventif (Dexaméthasone 4 mg à l’induction et DHBP 1 mg 20 min
avant la fin de l’intervention et Odansetron/Granisetron à la fin de
la chirurgie (si risque très élevé)
1. Diminuer les facteurs de risque causés par l’anesthésie

II II 18Jacques Berthod, enseignant EPD ES SA, CFS
STRATEGIE ANESTHESIQUE EN CAS DE NVPO
Prophylaxie Médicament reçu Médicament à donner
NON Aucun médicament Odansetron / Granisetron
(25 % dose préventive)
OUI DHPB, Dexamethasone, Odansetron / Granisetron
(25 % dose préventive)
OUI Odansetron / Granisetron DHPB (pour effet rapide) +
Dexamethasone (effet
prolongé)
OUI DHBP + Dexamethasone +Setron Propofol 20 mg (en SSPI)

II II 19Jacques Berthod, enseignant EPD ES SA, CFS
ALGORITHME POUR PREVENTION ET TTT DES NVPO
A. Pospiech, Prise en charge des nausées et vomissements post-opératoires : une priorité, Louvain Med.
2014; 133 (2): 077-085

II II
SCORES D’EVALUATION DU RISQUE NVPO EN
PEDIATRIE
20Jacques Berthod, enseignant EPD ES SA, CFS
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.; Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002
Figure 3. Simplified risk score for POV in Children. Simplified risk score from Eberhart et al.48 to predict the risk for POV in children. When 0, 1, 2, 3, or 4 of the depicted independent predictors are present, the corresponding risk for PONV is approximately 10%, 10%, 30%, 50%, or 70%, respectively. POV = postoperative vomiting; PONV = postoperative nausea and vomiting.
Autres facteurs de risque : amygdalectomie, hernie inguinale, neurochirurgie, chirurgie de l’oreille moyenne, l’orchidopexie, la chirurgie
herniaire et la chirurgie pénienne, fille après la puberté)

II II
TRAITEMENT PHARMACOLOGIQUE
21Jacques Berthod, enseignant EPD ES SA, CFS
➢ Recommandations semblables à l’adulte, mais utilisation réservée du DHBP (en cas d’échec aux autres ttt
et si enfant est hospitalisé).
➢ La Dexamethasone est préférable comme en prévention à cause de son délai d’action
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
Gan, Tong J.; Diemunsch, Pierre; Habib, Ashraf S.; Kovac, Anthony; Kranke, Peter; Meyer, Tricia A.; Watcha, Mehernoor; Chung, Frances; Angus, Shane; Apfel, Christian C.; Bergese, Sergio D.;
Candiotti, Keith A.; Chan, Matthew TV; Davis, Peter J.; Hooper, Vallire D.; Lagoo-Deenadayalan, Sandhya; Myles, Paul; Nezat, Greg; Philip, Beverly K.; Tramèr, Martin R.
Anesthesia & Analgesia. 118(1):85-113, January 2014.
doi: 10.1213/ANE.0000000000000002

II II 22Jacques Berthod, enseignant EPD ES SA, CFS
PREVENTION DES NVPO EN PEDIATRIE
Bourdaud N, Xavier L, Bientz J. Prise en charge des NVPO. Particularités en chirurgie pédiatrique. Conférence d’Experts SFAR 2007.
(http://www.sfar.org/t/IMG/pdf/cexp_nvpo.pdf)

II II 23Jacques Berthod, enseignant EPD ES SA, CFS
PREVENTION NVPO AVEC PCA OPOÏDES
DHBP dans perfusion de Morphine => 15 à 150 mcg (10 x !) DHBP par mg morphine
Pour 100 mg de morphine :
petite dose : 15 x 100 = 1500 mcg = 1,5 mg DHPB/100 mg morphine
grande dose : 150 X 100 = 15000 mcg = 15 mg DHBP/100 mg morphine
Dose maximale : 4 mg DHPB par jour, soit 265 mg, versus 26 mg de morphine !
➢ pas de relation dose-réponse (1 mg = 10 mg /jour)
➢ effet dose-réponse pour les effets indésirables (risque de sédation
augmenté si dose > 4 mg/jour> 4 mg /j)

II II 24Jacques Berthod, enseignant EPD ES SA, CFS
A meta-analysis of 40 articles including 4858 subjects226 concluded that P6 stimulation with 10 different acupuncture
modalities reduces nausea, vomiting, and the need for rescue antiemetics compared with sham stimulation (Evidence A1).
The efficacy of P6 stimulation is similar to that of prophylactic antiemetics such as ondansetron, droperidol,
metoclopramide, cyclizine, and prochlorperazine.
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting
TECHNIQUES ALTERNATIVES PREVENTION NVPO

II II 25Jacques Berthod, enseignant EPD ES SA, CFS
Prévention des nausées et vomissements pré-opératoires, Eve Charest, mai 2013,
Université de Laval, Canada

II II 26Jacques Berthod, enseignant EPD ES SA, CFS

II II 27Jacques Berthod, enseignant EPD ES SA, CFS
TAKE HOSPITAL MESSAGE

II II 28Jacques Berthod, enseignant EPD ES SA, CFS
BIBLIOGRAPHIE
1. Ton J et al, Consensus Guidelines for the Management of Postoperative Nausea
and Vomiting, Society for Ambulatory Anesthesiology, Anesth Analg 2014;118:85–
113
2. A. Pospiech, Prise en charge des nausées et vomissements post-opératoires : une
priorité, Louvain Med. 2014; 133 (2): 077-085
3. S. Pierre, Nausées et vomissements postopératoires chez l’adulte et l’enfant:
gestion en 2014, Le Congrès Médecins. Conférence d’essentiel © 2014 SFAR
4. B.Capron, Nausées et vomissements post-opératoires : tolérance zéro ? MAPAR
2013
5. P. Diemunsch, Conférence d’experts – Texte court. Prise en charge des nausées
et vomissements postopératoires, Annales Françaises d’Anesthésie et de
Réanimation 27 (2008) 866–878
6. N. Bourdaud, Nausées-vomissements postopératoires chez l’enfant, MAPAR 2009
7. Dr. L’Hermite, Prévention et traitement des NVPO chez l’adulte au bloc opératoire
et en SSPI, Protocole du CHU de Nîmes, 2008
8. C. Barry, Evaluation de l’efficacité et de la sécurité de l’acupuncture, Institut
national de la santé et de la recherche médicale, 2014