Le cuivre échangeable sérique : un nouveau marqueur … · Introduction WD maladie génétique...
49
Le cuivre échangeable : un nouveau marqueur pour le diagnostic de la maladie de Wilson I Mallet (1); O Guillaud (2); J Dumortier (2), AS Brunet (3); A Lachaux (4); M Pelosse (3); E Broussole (3); L Lion-François (3); M Vallin (2); F Juget Pietu (2); M Petronio (2); S El Bakhi (5); J Poupon (5); M Bost (1) (1) Service de Biochimie, Hôpital Edouard Herriot, Lyon (2) Hépatogastroentérologie, Hôpital Edouard Herriot, Lyon (3) Centre national de référence de la maladie de Wilson, HFME, Bron (4) Hépatologie, Gastroentérologie et nutrition pédiatriques, HFME, Bron (5) Laboratoire de toxicologie biologique, GH Lariboisière - Fernand Vidal, Paris
Transcript of Le cuivre échangeable sérique : un nouveau marqueur … · Introduction WD maladie génétique...
Le cuivre échangeable : un nouveau marqueur
pour le diagnostic de la maladie de Wilson
I Mallet (1); O Guillaud (2); J Dumortier (2), AS Brunet (3); A Lachaux (4); M Pelosse (3); E Broussole (3); L Lion-François (3); M Vallin (2); F Juget Pietu (2); M Petronio (2); S El Bakhi (5); J Poupon (5); M Bost (1)
(1) Service de Biochimie, Hôpital Edouard Herriot, Lyon (2) Hépatogastroentérologie, Hôpital Edouard Herriot, Lyon (3) Centre national de référence de la maladie de Wilson, HFME, Bron (4) Hépatologie, Gastroentérologie et nutrition pédiatriques, HFME, Bron (5) Laboratoire de toxicologie biologique, GH Lariboisière - Fernand Vidal, Paris
Conflits d’intérêt
aucun
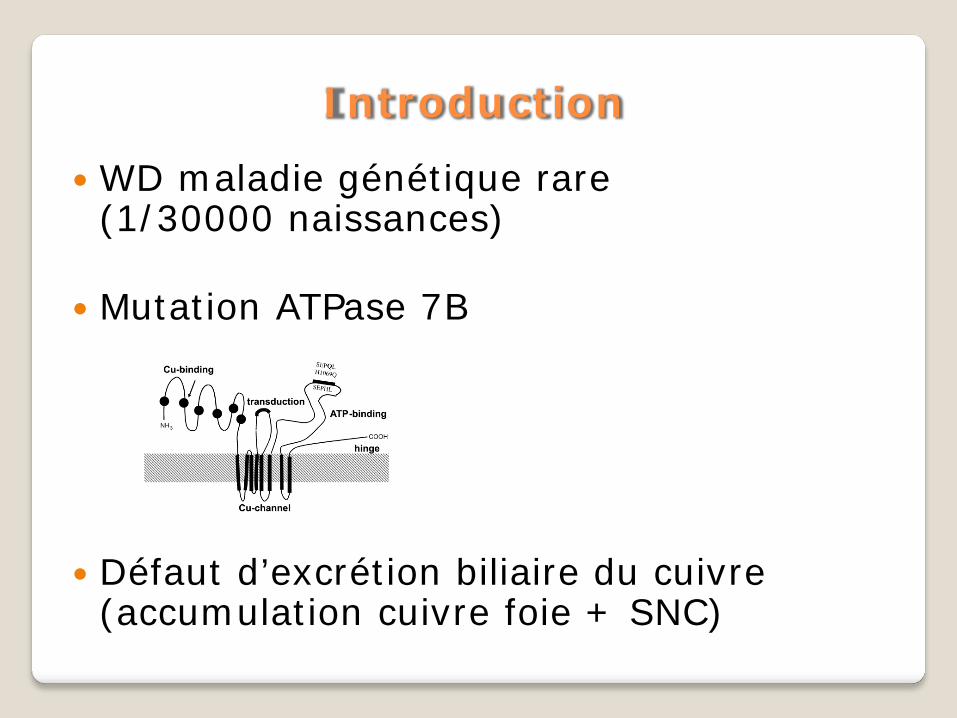
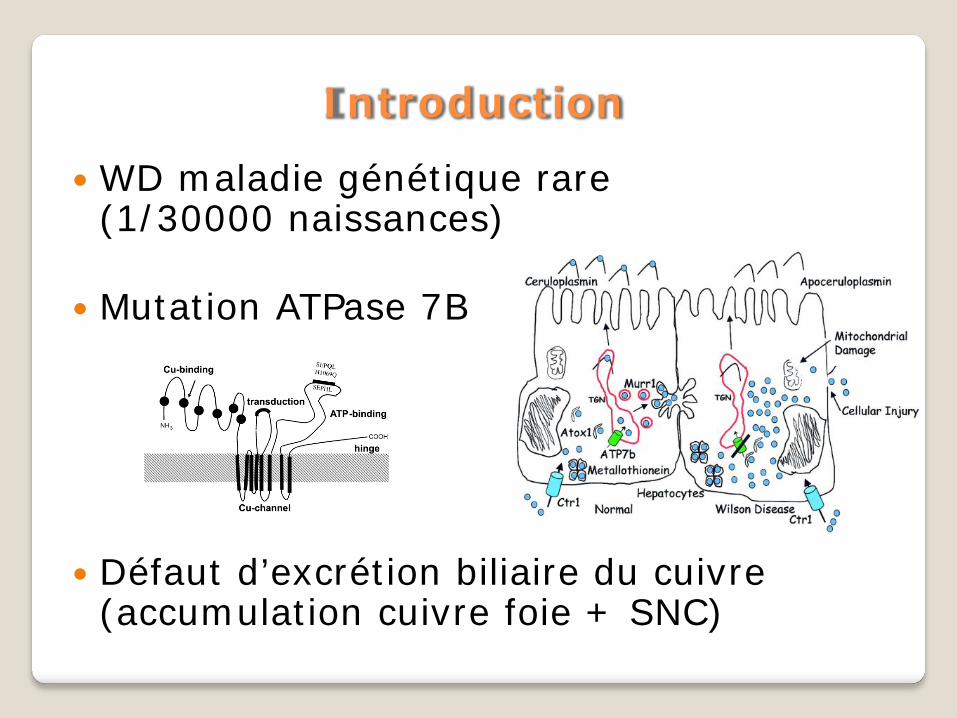
Introduction
WD maladie génétique rare (1/30000 naissances)
Mutation ATPase 7B
Défaut d’excrétion biliaire du cuivre (accumulation cuivre foie + SNC)
Introduction
WD maladie génétique rare (1/30000 naissances)
Mutation ATPase 7B
Défaut d’excrétion biliaire du cuivre (accumulation cuivre foie + SNC)
Introduction (2)
Les éléments du diagnostic de WD : Clinique (atteinte neurologique, FO) Biologique Bilan cuprique (Cp, Cuprémie, cuprurie, test Trolovol) Radiologique : IRM cérébrale Biologie moléculaire (chr 13)
Aucun test fiable 100%, le diagnostic (ou
l’exclusion du diagnostic) repose sur un faisceau d’argument
Ferenci P Liver Int 2003
Introduction : les limites du diagnostic (3)
L’anneau de Kayser-Fleischer non retrouvé 50% formes hépatiques
Cp : 5-10% FN, nbx FP (0,10-0,20) (hz, cirrhose, …)
Cuprurie : peut-être normale en cas de forme hépatique, FP cholestase prolongée
Cuprurie sous Trolovol : pas toujours simple à mettre en œuvre, modalités du test et cut-off mal définis
Cuivre intrahépatique : invasif (PBF)
Biologie moléculaire : coût 1500 euros, long (23 exons, >300 mutations), FN 5%
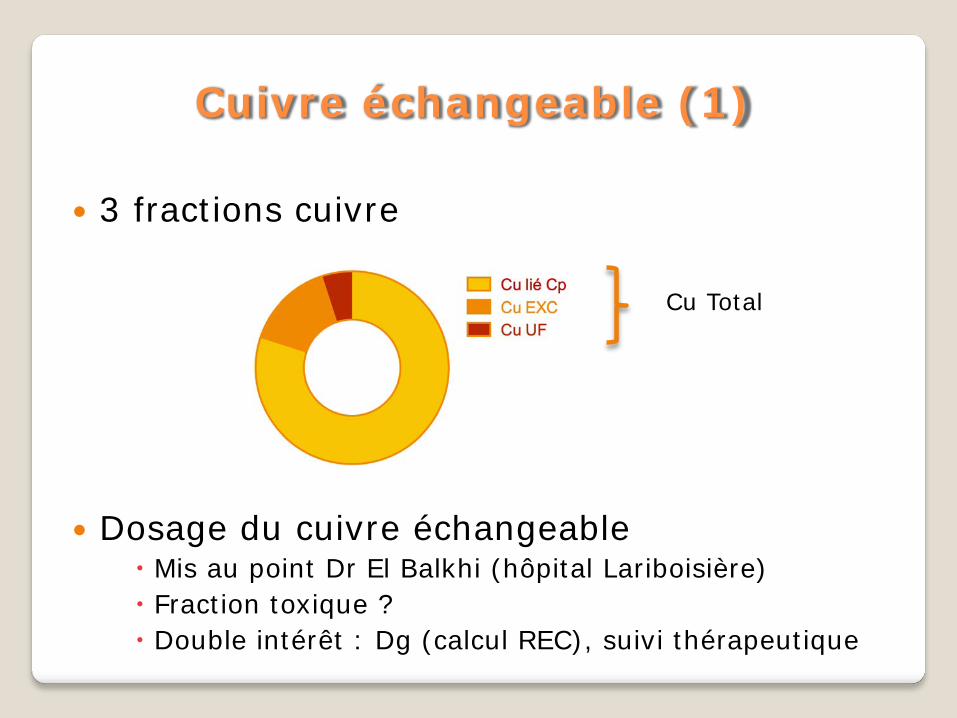
Cuivre échangeable (1)
3 fractions cuivre
Dosage du cuivre échangeable Mis au point Dr El Balkhi (hôpital Lariboisière) Fraction toxique ? Double intérêt : Dg (calcul REC), suivi thérapeutique
Cu Total
Cuivre échangeable (2)
Cuivre échangeable (3) 86 sujets
16 malades (dg bio moléculaire) 70 Dépistage intrafamilial : 45 hétérozygotes , 25 homozygotes sain
62 volontaires sains
REC = ratio CuEXC / Cu Total
Cut-off REC=18,5% (Se=100%, Sp=100%)
El Balkhi S Clin Chim Acta 2011
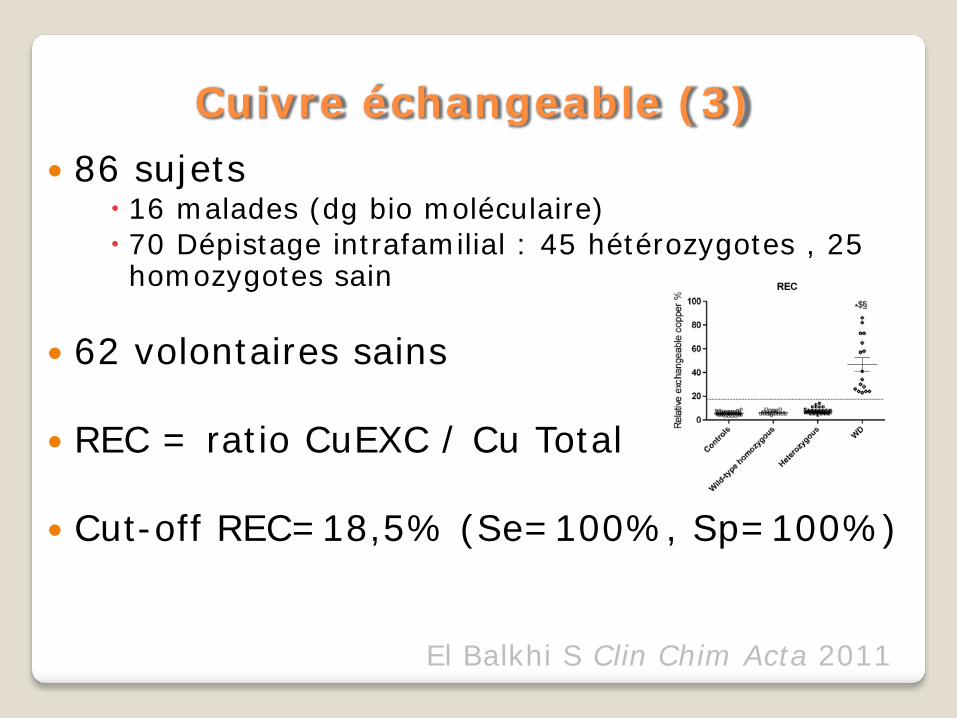
Cuivre échangeable (3) 86 sujets
16 malades (dg bio moléculaire) 70 Dépistage intrafamilial : 45 hétérozygotes , 25 homozygotes sain
62 volontaires sains
REC = ratio CuEXC / Cu Total
Cut-off REC=18,5% (Se=100%, Sp=100%)
El Balkhi S Clin Chim Acta 2011
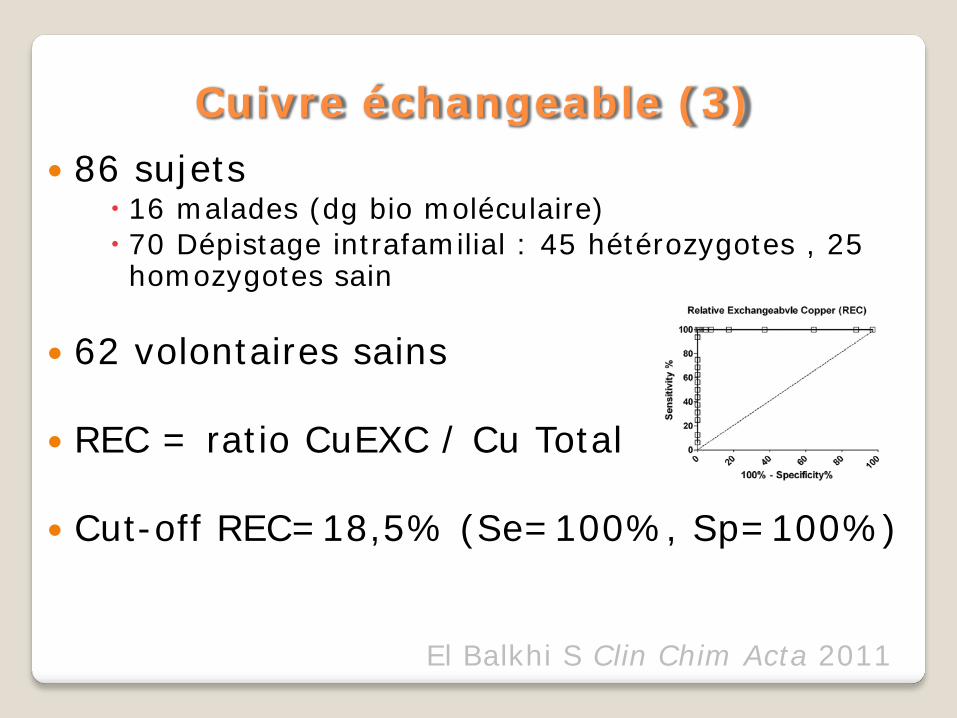
Cuivre échangeable (3) 86 sujets
16 malades (dg bio moléculaire) 70 Dépistage intrafamilial : 45 hétérozygotes , 25 homozygotes sain
62 volontaires sains
REC = ratio CuEXC / Cu Total
Cut-off REC=18,5% (Se=100%, Sp=100%)
El Balkhi S Clin Chim Acta 2011
Cuivre échangeable (3) 86 sujets
16 malades (dg bio moléculaire) 70 Dépistage intrafamilial : 45 hétérozygotes , 25 homozygotes sain
62 volontaires sains
REC = ratio CuEXC / Cu Total
Cut-off REC=18,5% (Se=100%, Sp=100%)
El Balkhi S Clin Chim Acta 2011
But étude (préliminaire)
Déterminer la valeur informationnelle du CuEXC et du REC dans une cohorte de malade suivis pour une maladie de Wilson et dans un service d’hépatologie adulte/enfant
Méthodologie
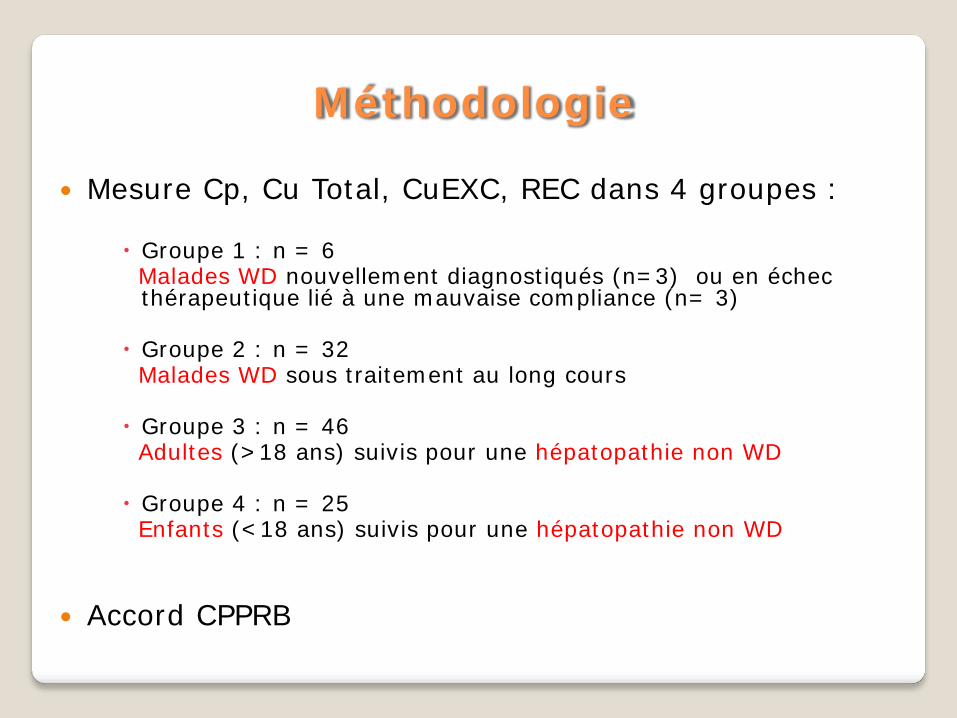
Mesure Cp, Cu Total, CuEXC, REC dans 4 groupes :
Groupe 1 : n = 6 Malades WD nouvellement diagnostiqués (n=3) ou en échec
thérapeutique lié à une mauvaise compliance (n= 3) Groupe 2 : n = 32 Malades WD sous traitement au long cours Groupe 3 : n = 46 Adultes (>18 ans) suivis pour une hépatopathie non WD Groupe 4 : n = 25 Enfants (<18 ans) suivis pour une hépatopathie non WD
Accord CPPRB
Groupe 1
WD diagnostic ou inobservance
Groupe 2
WD traités
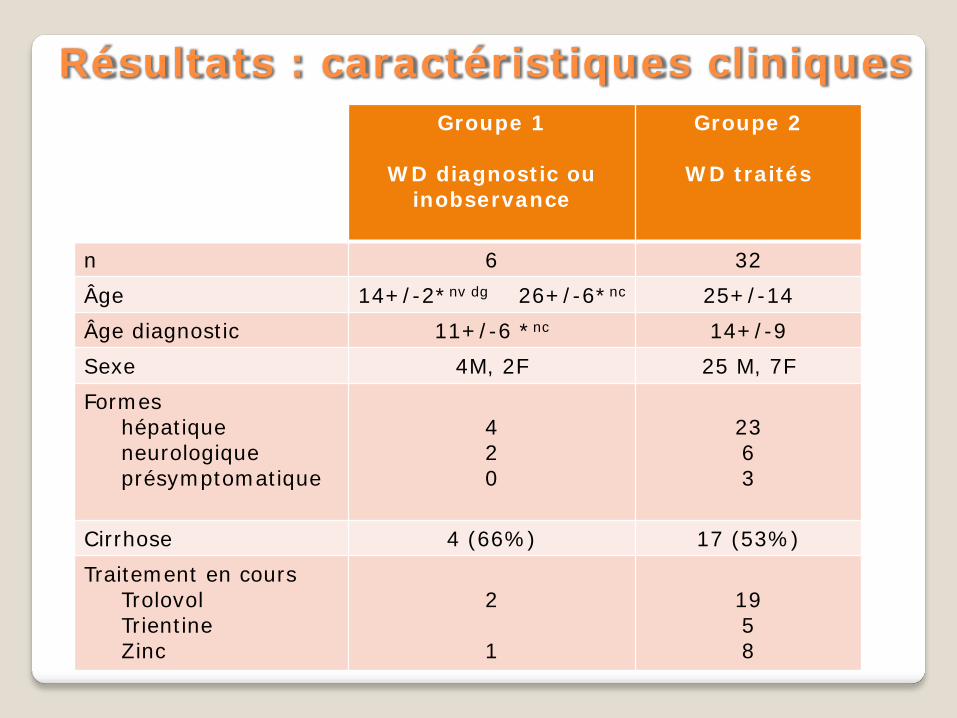
n 6 32 Âge 14+/-2*nv dg 26+/-6*nc 25+/-14 Âge diagnostic 11+/-6 *nc 14+/-9 Sexe 4M, 2F 25 M, 7F Formes hépatique neurologique présymptomatique
4 2 0
23 6 3
Cirrhose 4 (66%) 17 (53%) Traitement en cours Trolovol Trientine Zinc
2 1
19 5 8
Résultats : caractéristiques cliniques
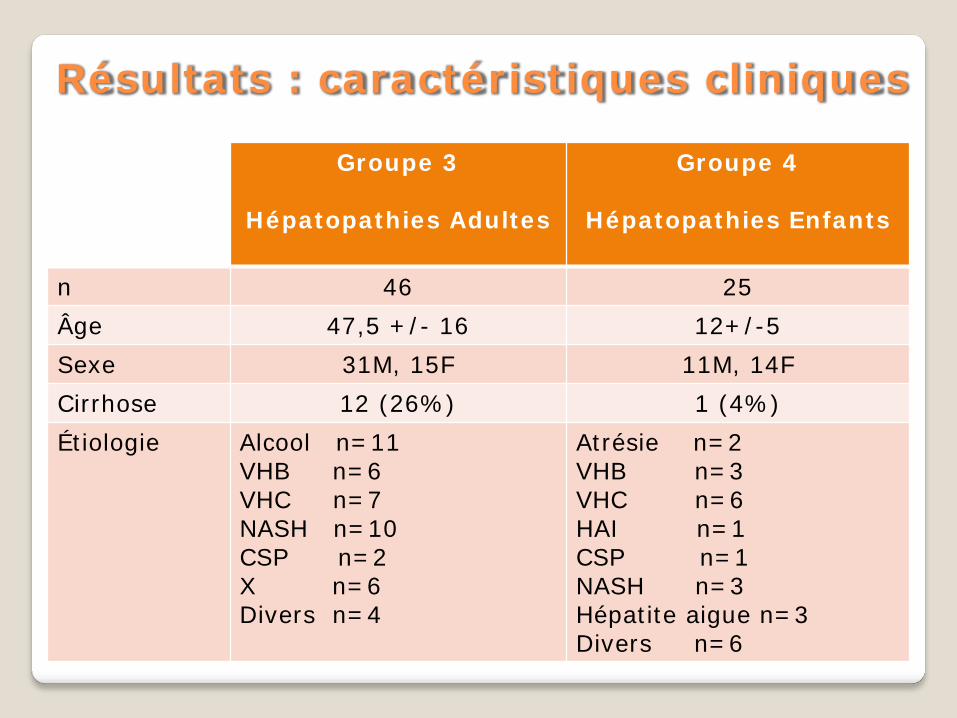
Résultats : caractéristiques cliniques
Groupe 3
Hépatopathies Adultes
Groupe 4
Hépatopathies Enfants
n 46 25 Âge 47,5 +/- 16 12+/-5 Sexe 31M, 15F 11M, 14F Cirrhose 12 (26%) 1 (4%) Étiologie
Alcool n=11 VHB n=6 VHC n=7 NASH n=10 CSP n=2 X n=6 Divers n=4
Atrésie n=2 VHB n=3 VHC n=6 HAI n=1 CSP n=1 NASH n=3 Hépatite aigue n=3 Divers n=6
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
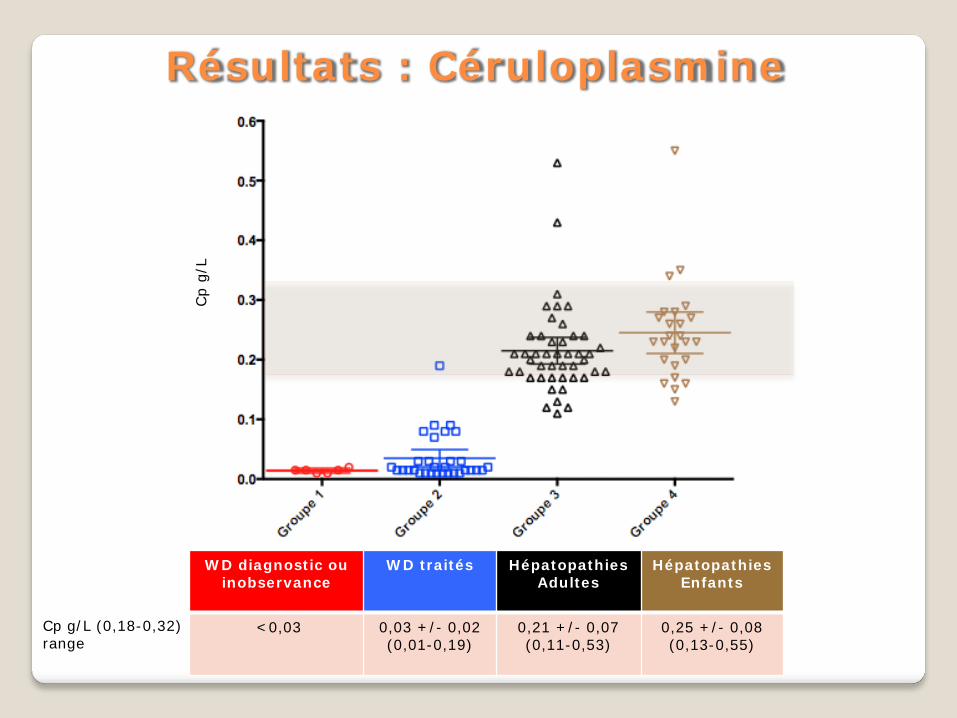
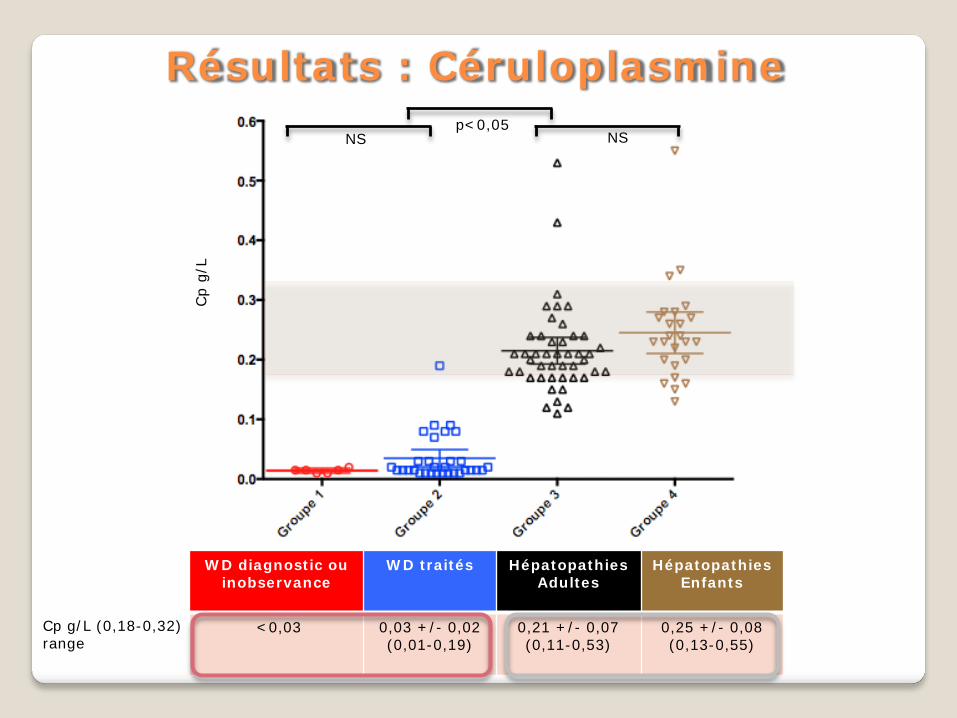
<0,03 0,03 +/- 0,02 (0,01-0,19)
0,21 +/- 0,07 (0,11-0,53)
0,25 +/- 0,08 (0,13-0,55)
Résultats : Céruloplasmine
Cp g/L (0,18-0,32) range
Cp
g/L
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
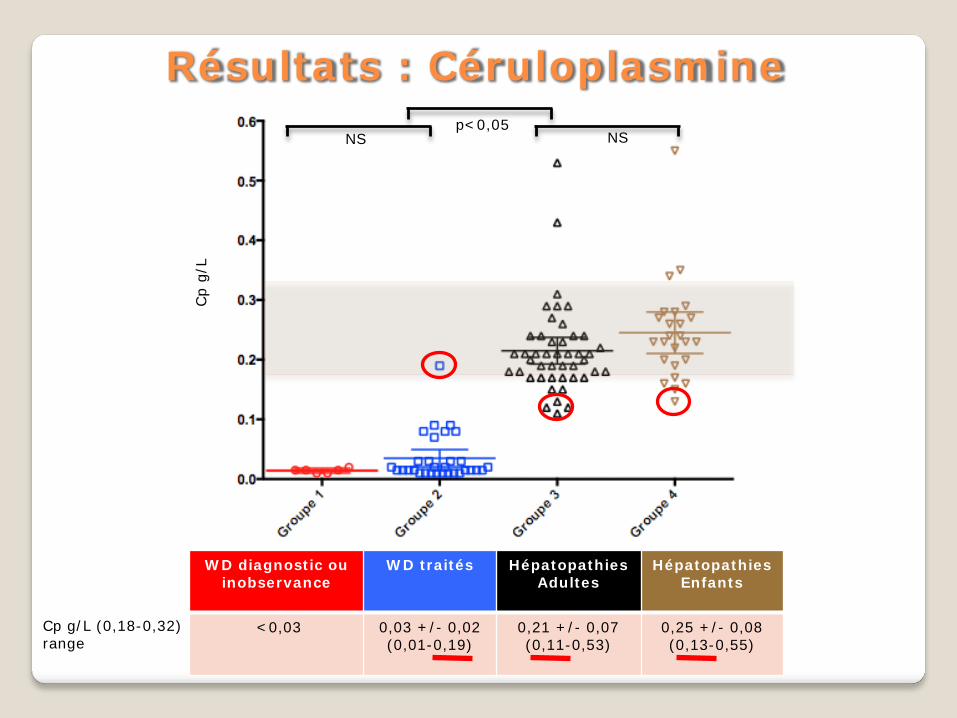
<0,03 0,03 +/- 0,02 (0,01-0,19)
0,21 +/- 0,07 (0,11-0,53)
0,25 +/- 0,08 (0,13-0,55)
Cp g/L (0,18-0,32) range
Résultats : Céruloplasmine
Cp
g/L
NS NS p<0,05
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
<0,03 0,03 +/- 0,02 (0,01-0,19)
0,21 +/- 0,07 (0,11-0,53)
0,25 +/- 0,08 (0,13-0,55)
Cp g/L (0,18-0,32) range
Résultats : Céruloplasmine
Cp
g/L
NS NS p<0,05
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
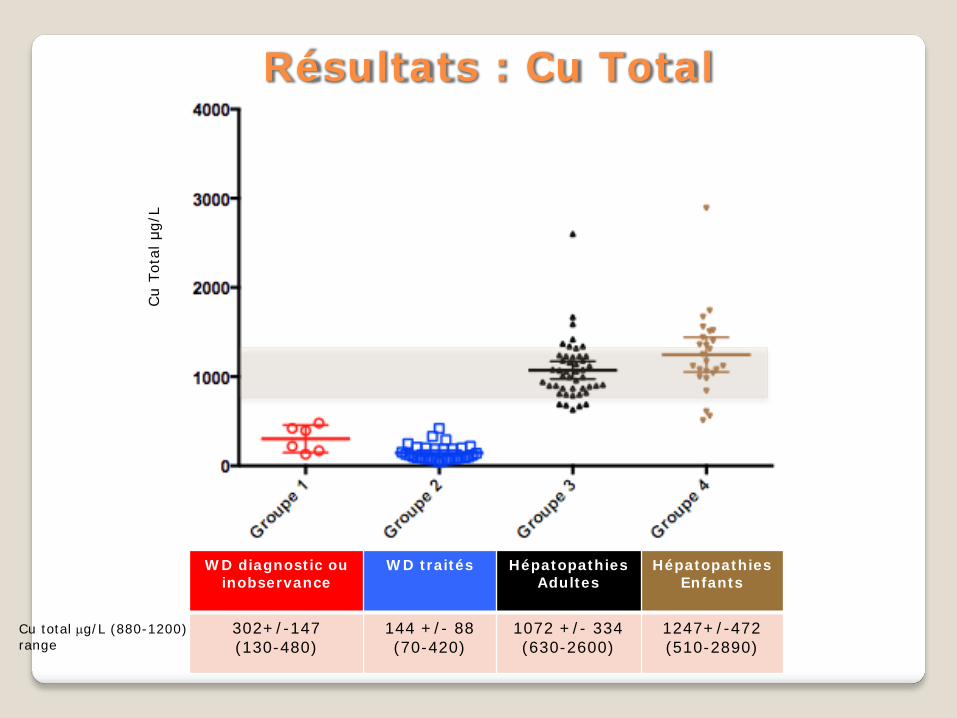
302+/-147 (130-480)
144 +/- 88 (70-420)
1072 +/- 334 (630-2600)
1247+/-472 (510-2890)
Résultats : Cu Total
Cu total µg/L (880-1200) range
Cu
Tota
l μg/
L

WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
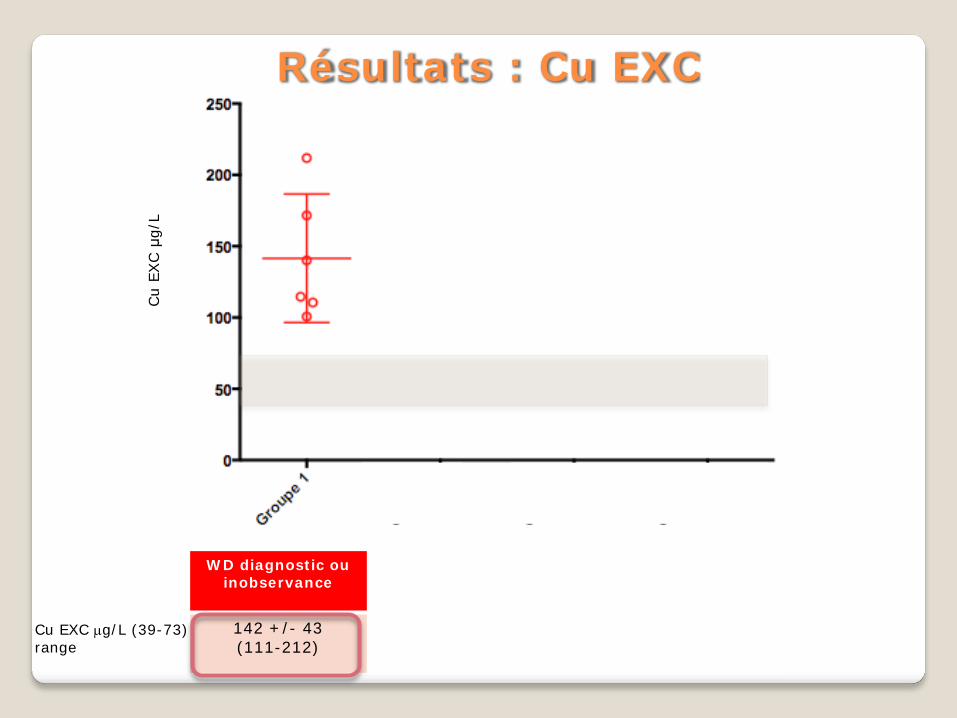
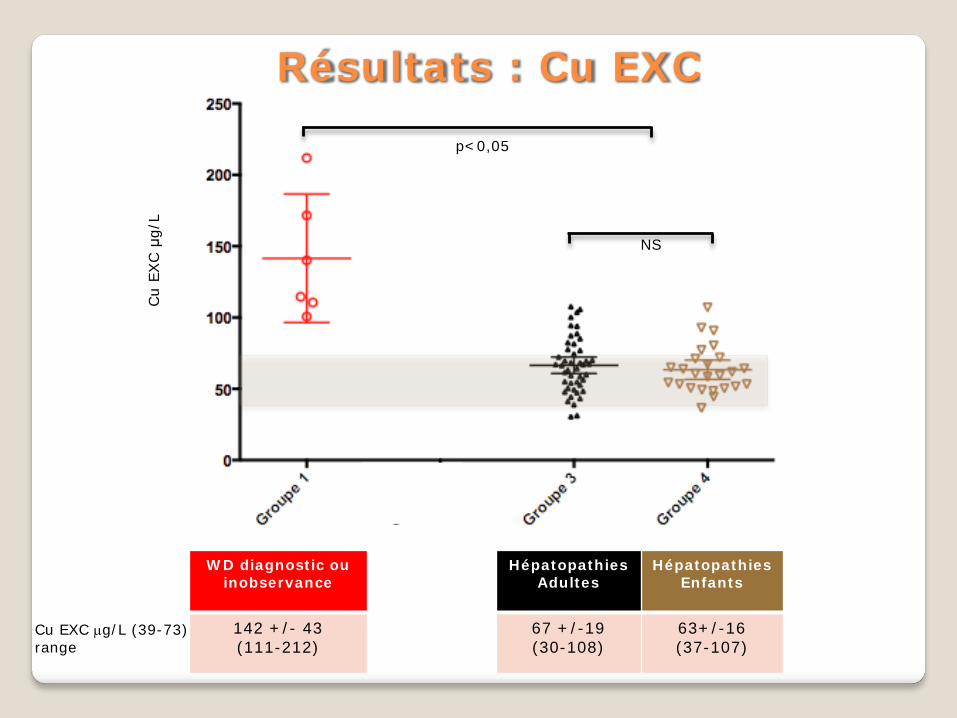
142 +/- 43 (111-212)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
142 +/- 43 (111-212)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
142 +/- 43 (111-212)
67 +/-19 (30-108)
63+/-16 (37-107)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L
NS
p<0,05
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
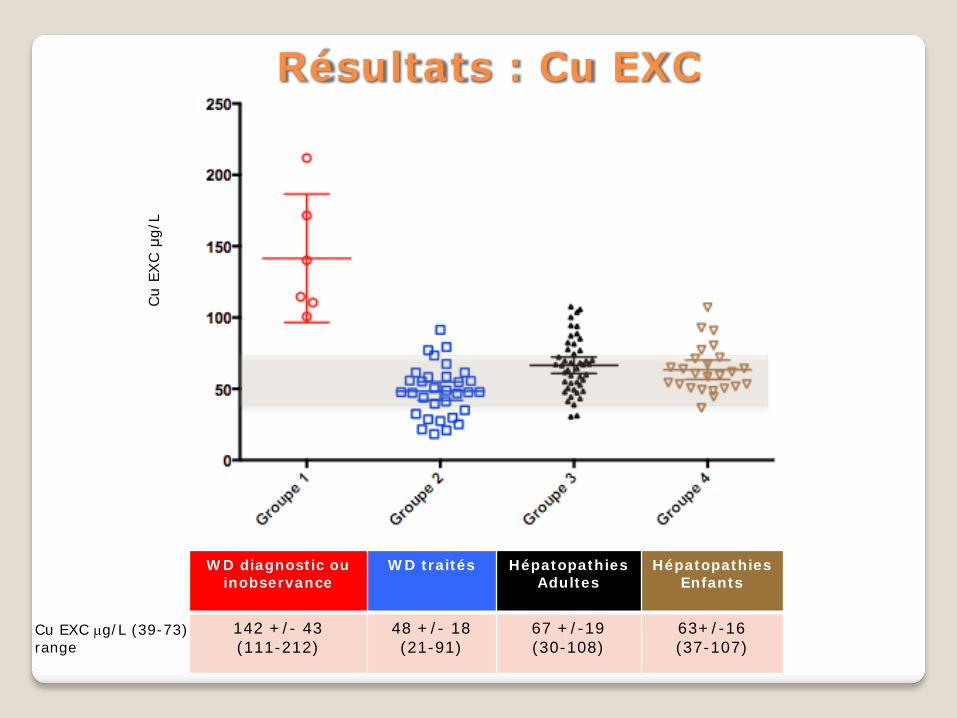
142 +/- 43 (111-212)
48 +/- 18 (21-91)
67 +/-19 (30-108)
63+/-16 (37-107)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
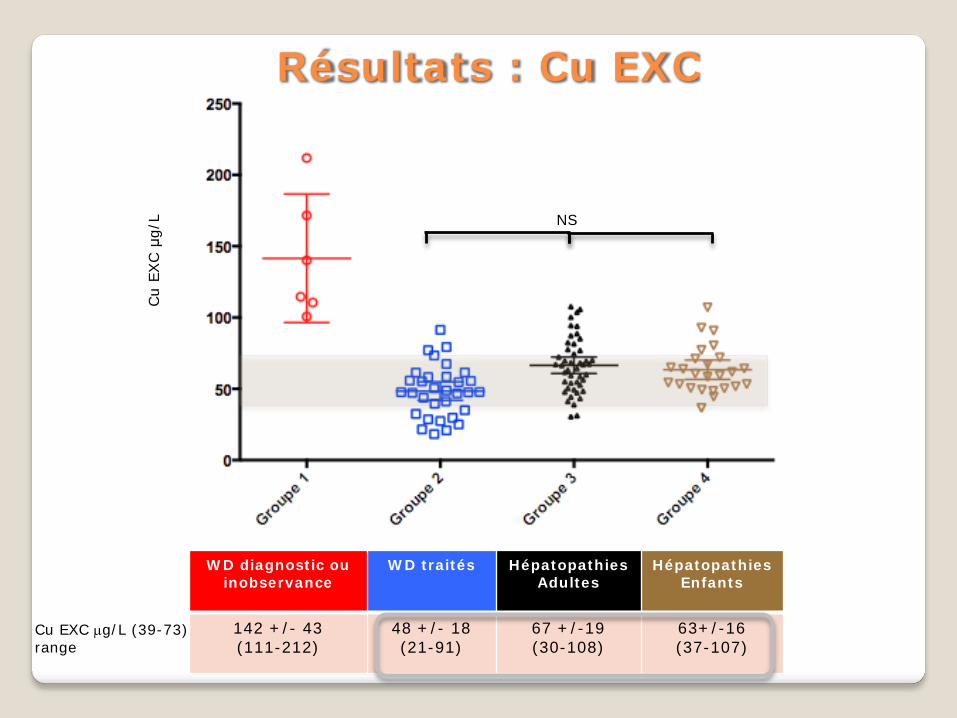
142 +/- 43 (111-212)
48 +/- 18 (21-91)
67 +/-19 (30-108)
63+/-16 (37-107)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L NS
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
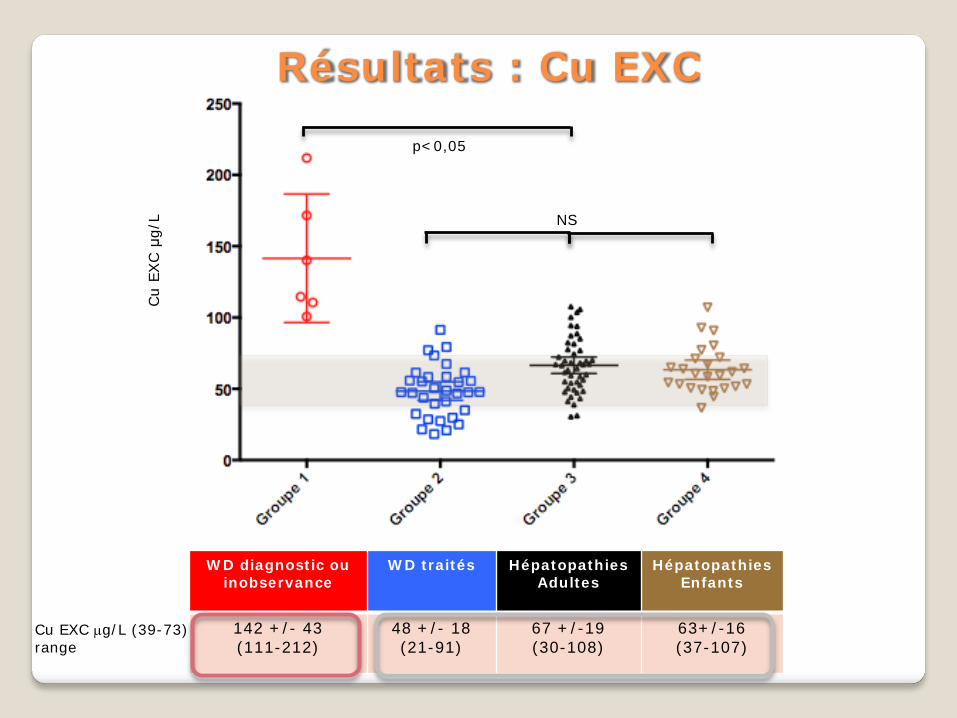
142 +/- 43 (111-212)
48 +/- 18 (21-91)
67 +/-19 (30-108)
63+/-16 (37-107)
Résultats : Cu EXC
Cu EXC µg/L (39-73) range
Cu
EXC μ
g/L NS
p<0,05
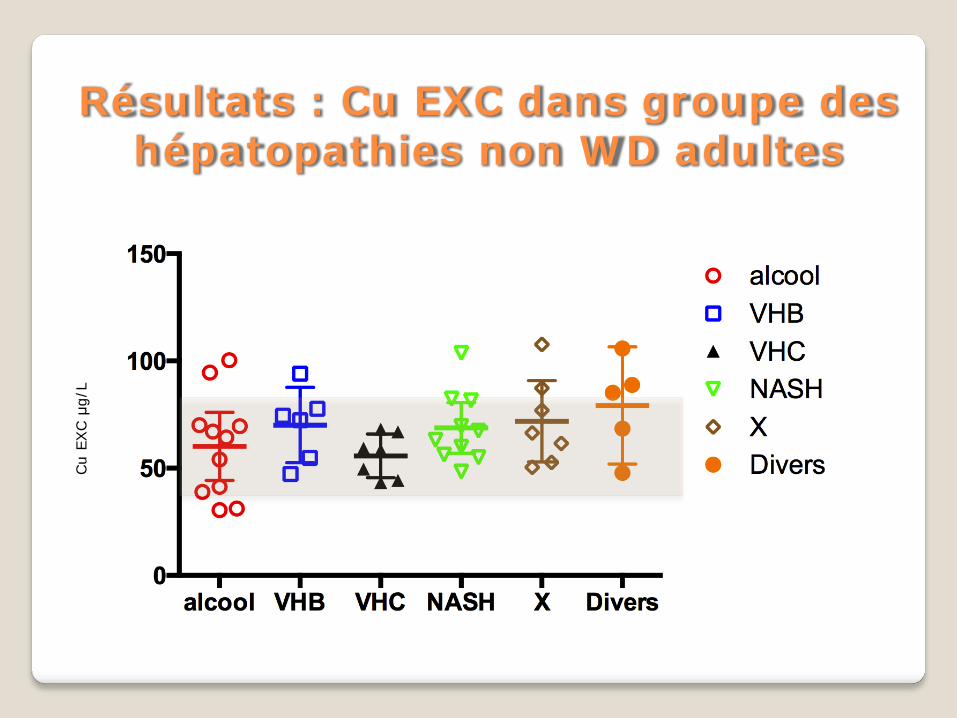
Résultats : Cu EXC dans groupe des hépatopathies non WD adultes
Cu
EXC μ
g/L
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
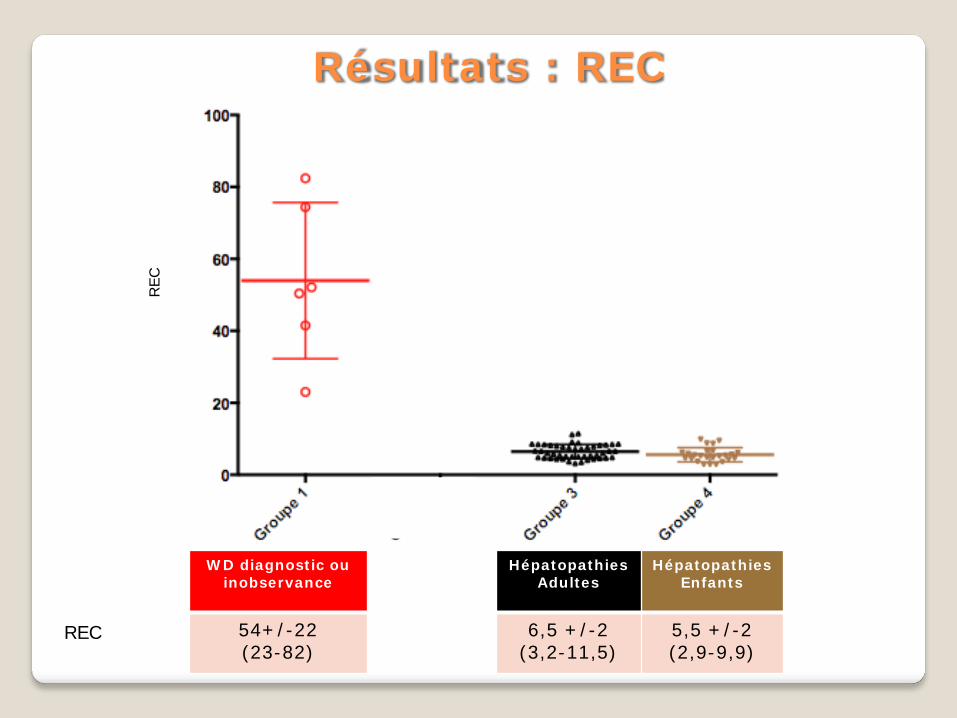
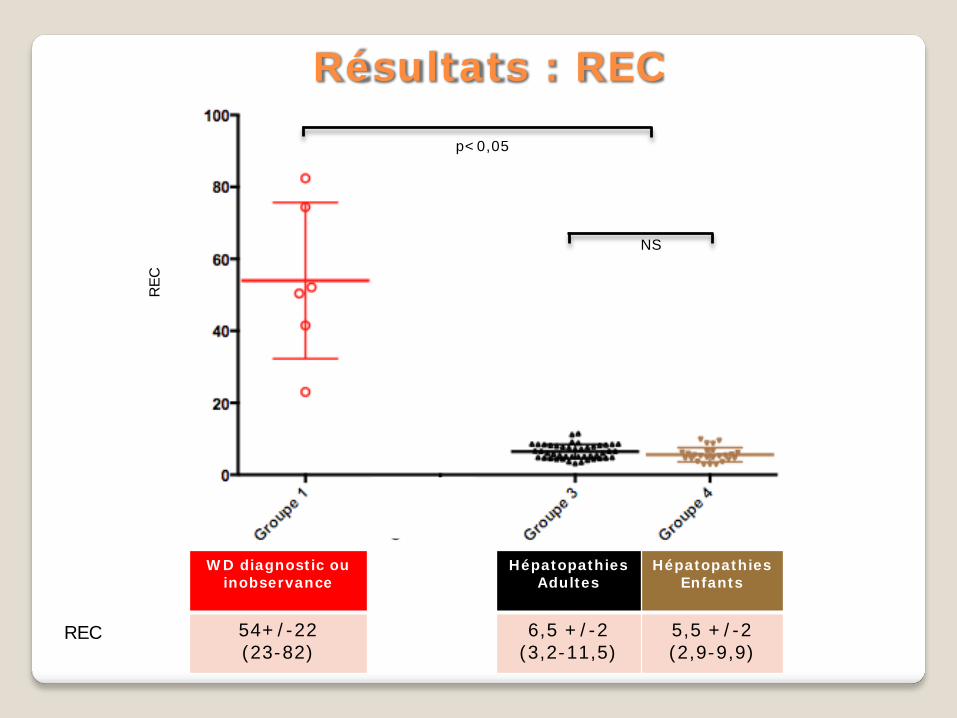
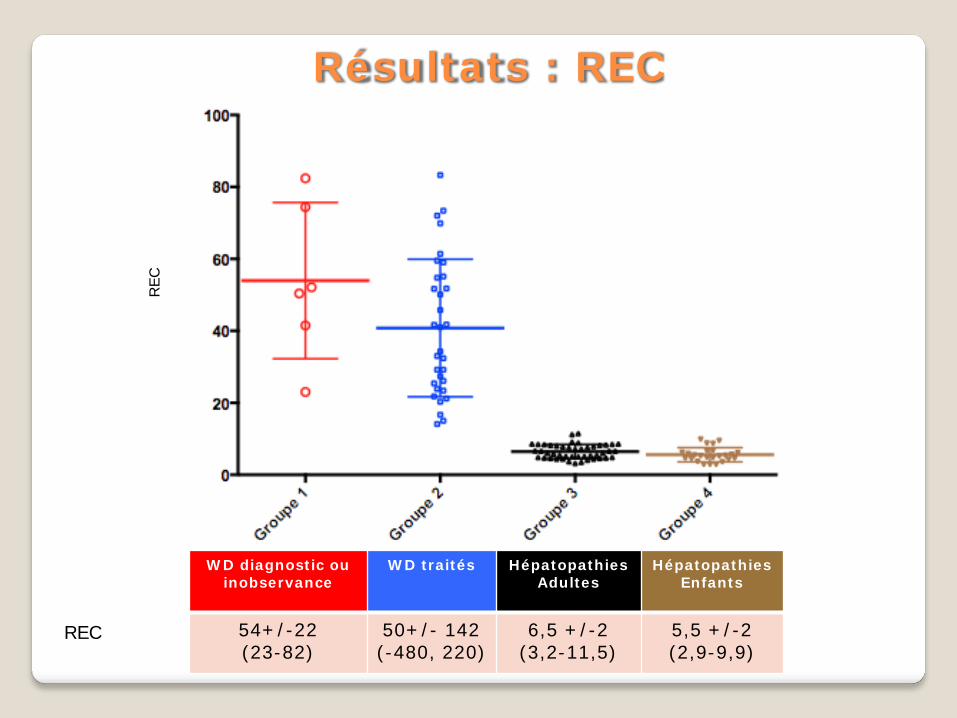
54+/-22 (23-82)
6,5 +/-2 (3,2-11,5)
5,5 +/-2 (2,9-9,9)
Résultats : REC
REC
REC
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
54+/-22 (23-82)
6,5 +/-2 (3,2-11,5)
5,5 +/-2 (2,9-9,9)
Résultats : REC
REC
REC
NS
p<0,05
WD diagnostic ou inobservance
WD traités
Hépatopathies Adultes
Hépatopathies Enfants
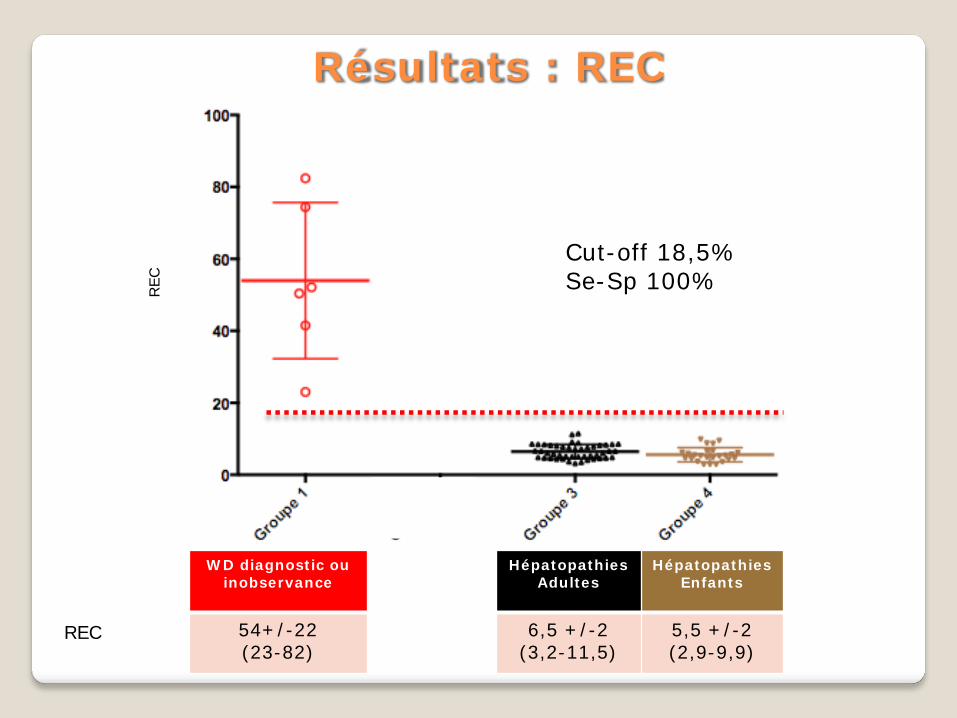
54+/-22 (23-82)
6,5 +/-2 (3,2-11,5)
5,5 +/-2 (2,9-9,9)
Cut-off 18,5% Se-Sp 100%
Résultats : REC
REC
REC
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
54+/-22 (23-82)
50+/- 142 (-480, 220)
6,5 +/-2 (3,2-11,5)
5,5 +/-2 (2,9-9,9)
Résultats : REC
REC
REC
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
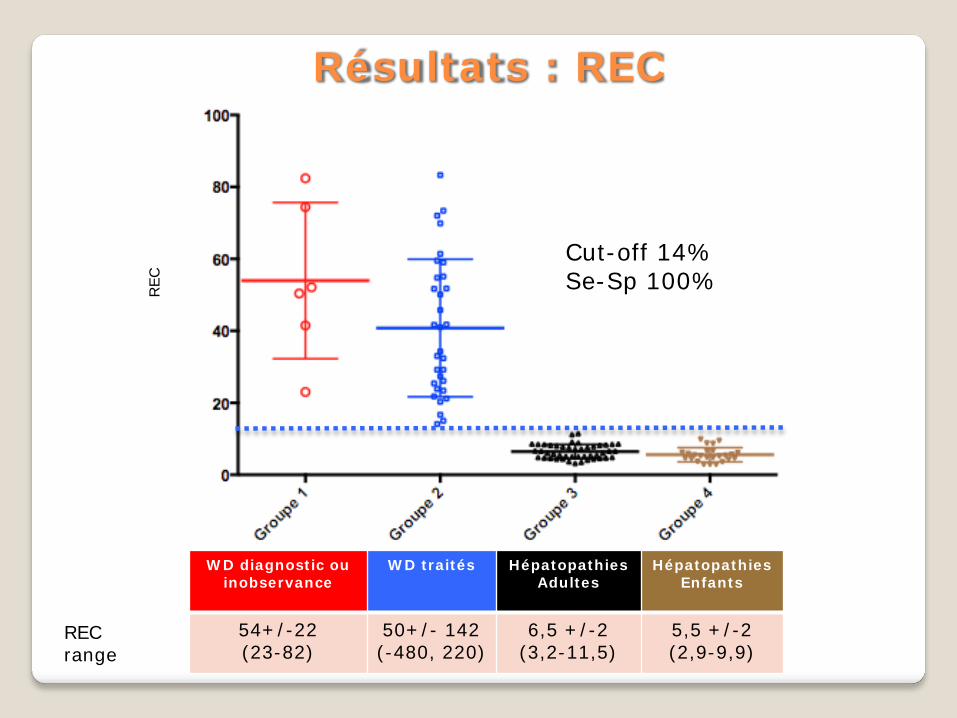
54+/-22 (23-82)
50+/- 142 (-480, 220)
6,5 +/-2 (3,2-11,5)
5,5 +/-2 (2,9-9,9)
Cut-off 14% Se-Sp 100%
Résultats : REC
REC range
REC
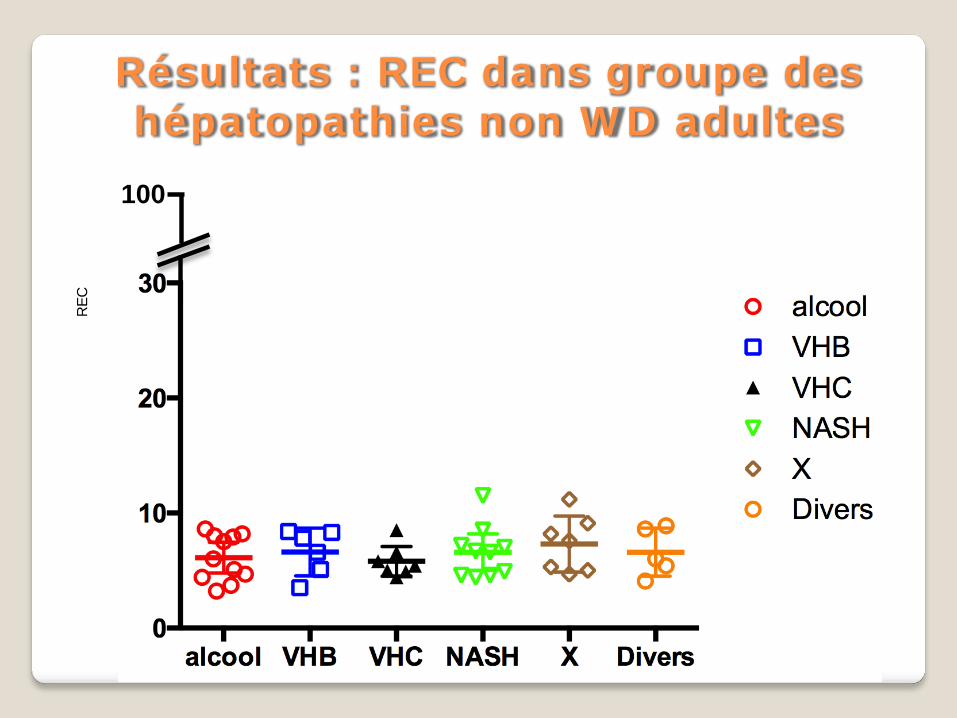
Résultats : REC dans groupe des hépatopathies non WD adultes
100
REC
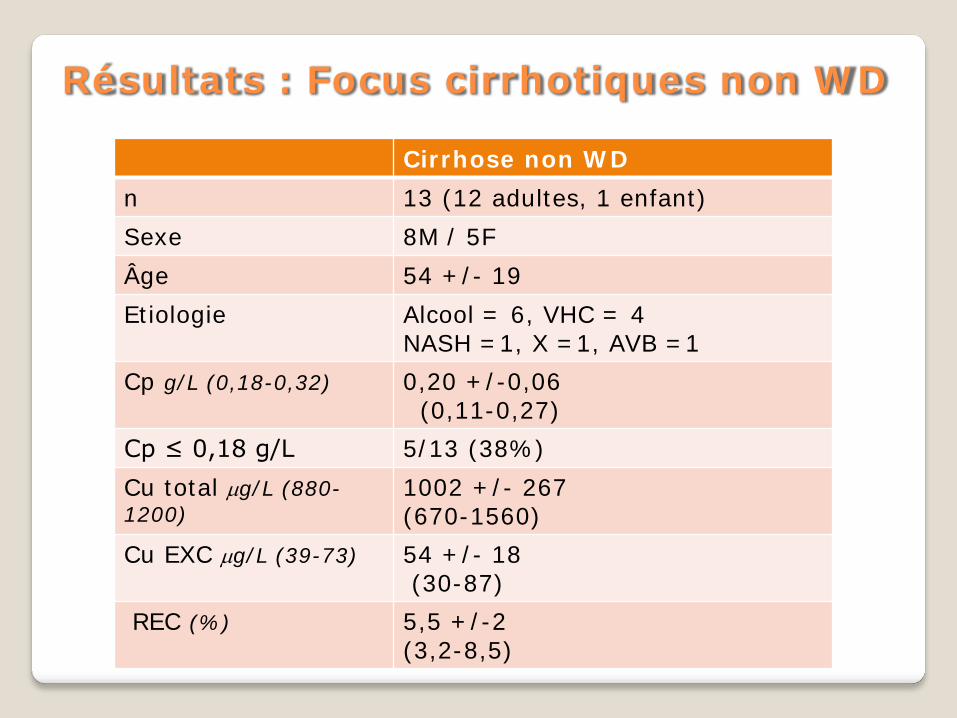
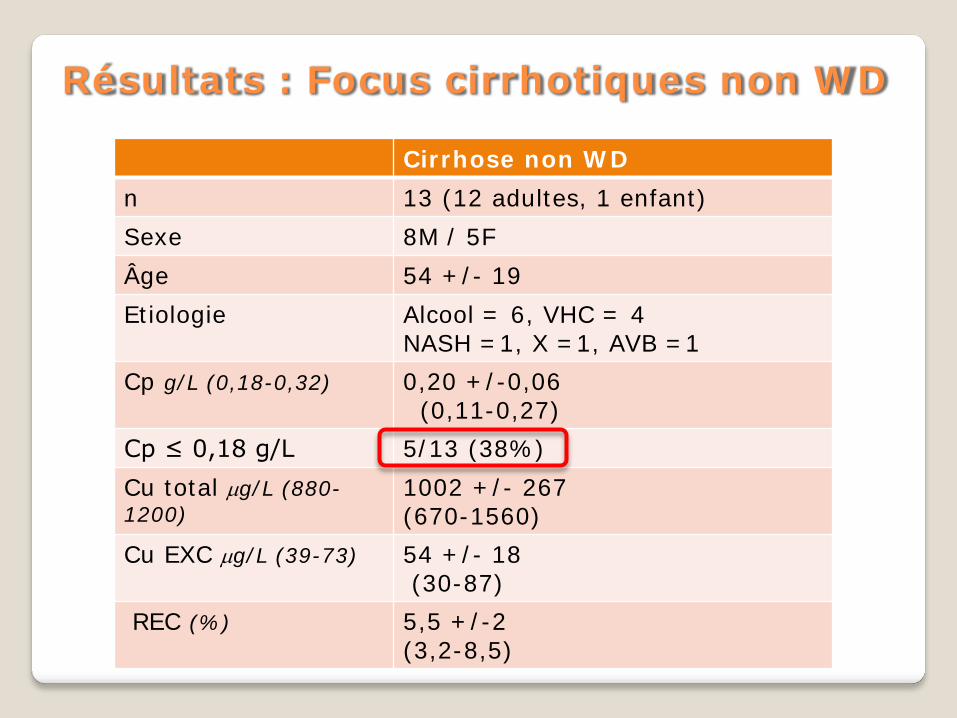
Résultats : Focus cirrhotiques non WD
Cirrhose non WD n 13 (12 adultes, 1 enfant) Sexe 8M / 5F Âge 54 +/- 19 Etiologie Alcool = 6, VHC = 4
NASH =1, X =1, AVB =1 Cp g/L (0,18-0,32) 0,20 +/-0,06
(0,11-0,27) Cp ≤ 0,18 g/L 5/13 (38%) Cu total µg/L (880-1200)
1002 +/- 267 (670-1560)
Cu EXC µg/L (39-73) 54 +/- 18 (30-87)
REC (%) 5,5 +/-2 (3,2-8,5)
Résultats : Focus cirrhotiques non WD
Cirrhose non WD n 13 (12 adultes, 1 enfant) Sexe 8M / 5F Âge 54 +/- 19 Etiologie Alcool = 6, VHC = 4
NASH =1, X =1, AVB =1 Cp g/L (0,18-0,32) 0,20 +/-0,06
(0,11-0,27) Cp ≤ 0,18 g/L 5/13 (38%) Cu total µg/L (880-1200)
1002 +/- 267 (670-1560)
Cu EXC µg/L (39-73) 54 +/- 18 (30-87)
REC (%) 5,5 +/-2 (3,2-8,5)
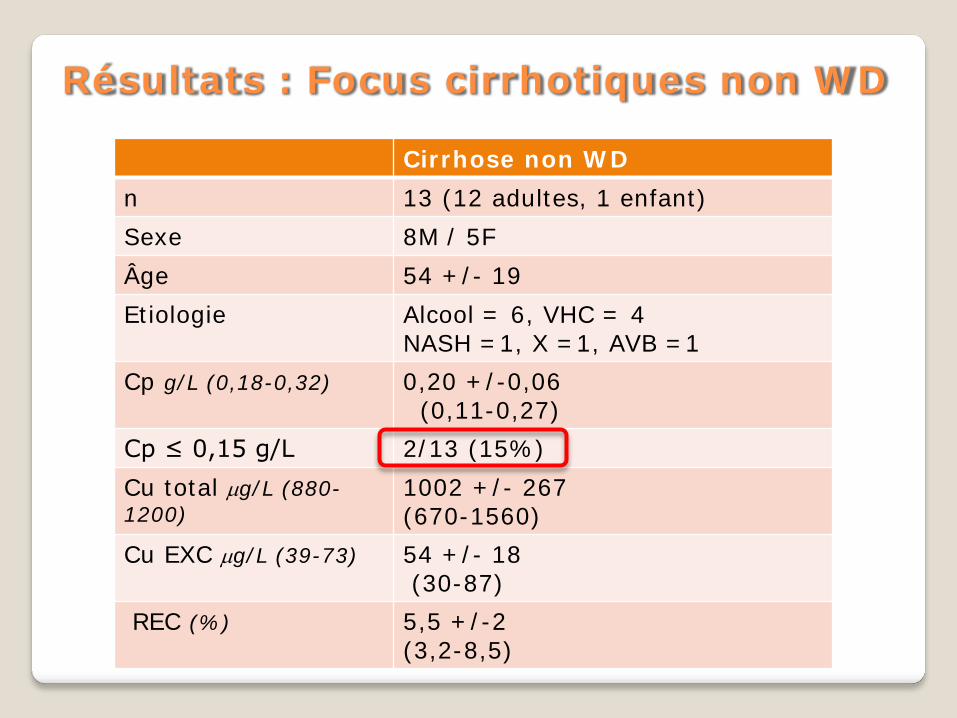
Résultats : Focus cirrhotiques non WD
Cirrhose non WD n 13 (12 adultes, 1 enfant) Sexe 8M / 5F Âge 54 +/- 19 Etiologie Alcool = 6, VHC = 4
NASH =1, X =1, AVB =1 Cp g/L (0,18-0,32) 0,20 +/-0,06
(0,11-0,27) Cp ≤ 0,15 g/L 2/13 (15%) Cu total µg/L (880-1200)
1002 +/- 267 (670-1560)
Cu EXC µg/L (39-73) 54 +/- 18 (30-87)
REC (%) 5,5 +/-2 (3,2-8,5)
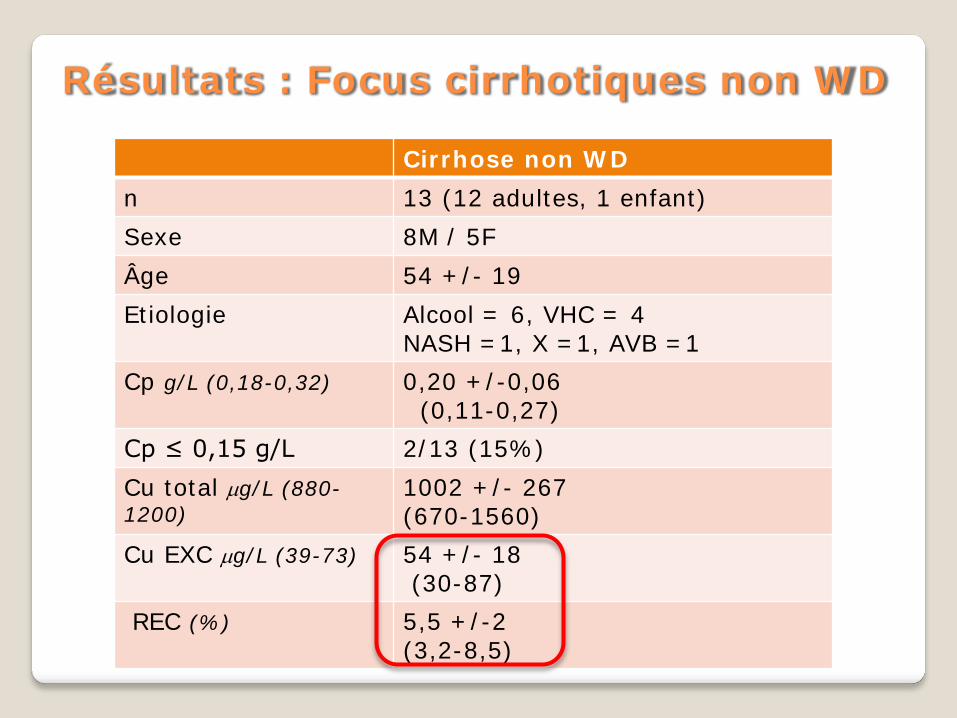
Résultats : Focus cirrhotiques non WD
Cirrhose non WD n 13 (12 adultes, 1 enfant) Sexe 8M / 5F Âge 54 +/- 19 Etiologie Alcool = 6, VHC = 4
NASH =1, X =1, AVB =1 Cp g/L (0,18-0,32) 0,20 +/-0,06
(0,11-0,27) Cp ≤ 0,15 g/L 2/13 (15%) Cu total µg/L (880-1200)
1002 +/- 267 (670-1560)
Cu EXC µg/L (39-73) 54 +/- 18 (30-87)
REC (%) 5,5 +/-2 (3,2-8,5)
Résultats : Focus cirrhotiques non WD
CA 92 – Etude du cuivre échangeable dans les hépatopathies cirrhotiques non Wilsoniennes
S El Balkhi, J Poupon, JM Trocello, F Woimant, N Tinant, V Ozenne
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
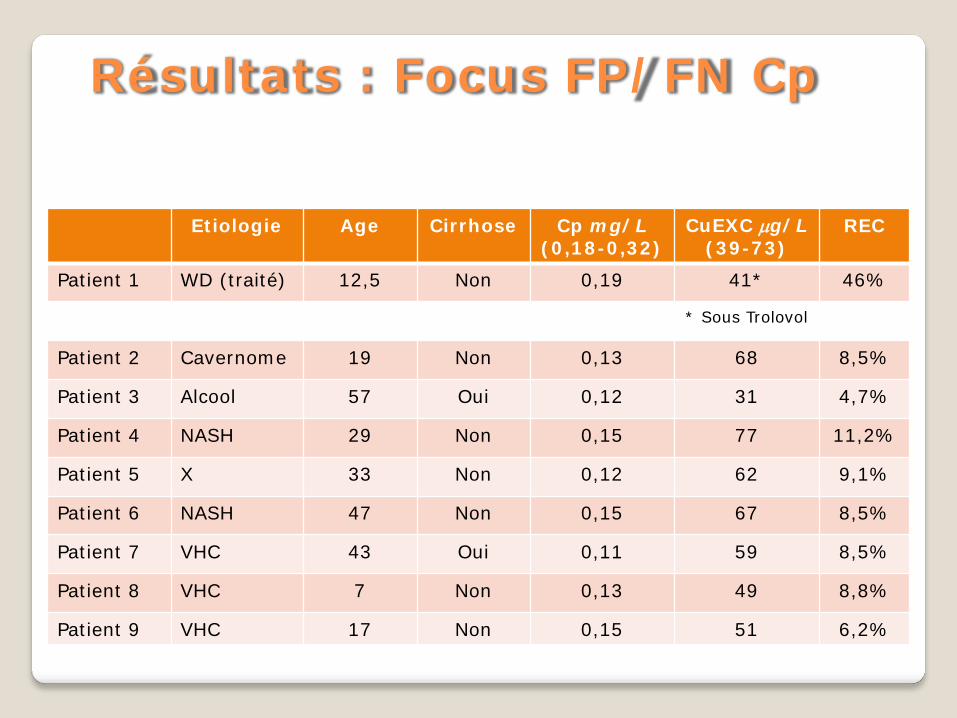
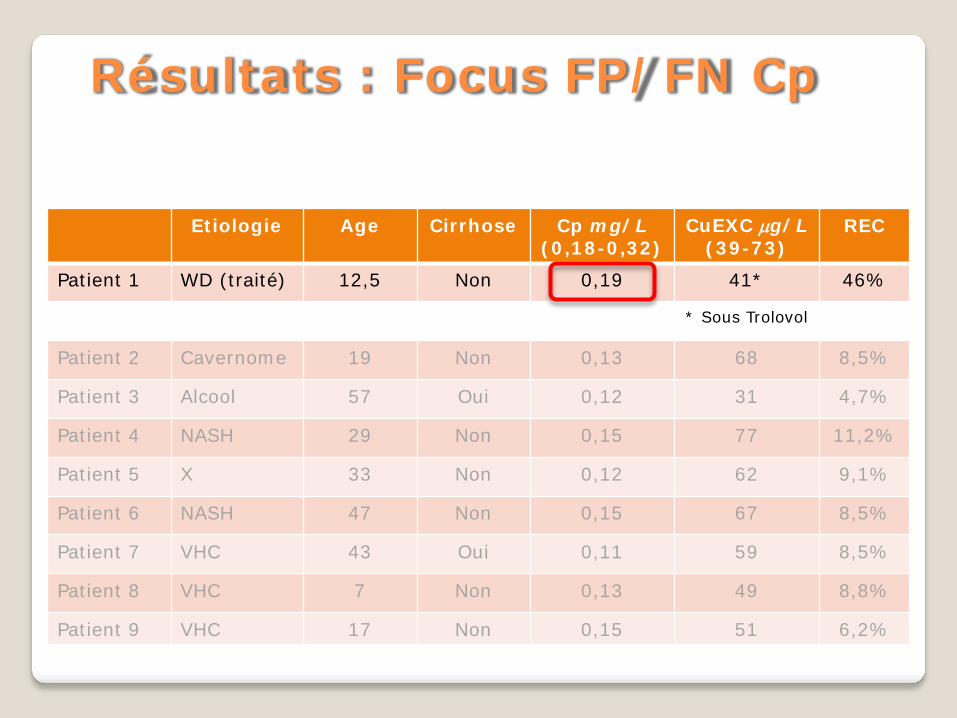
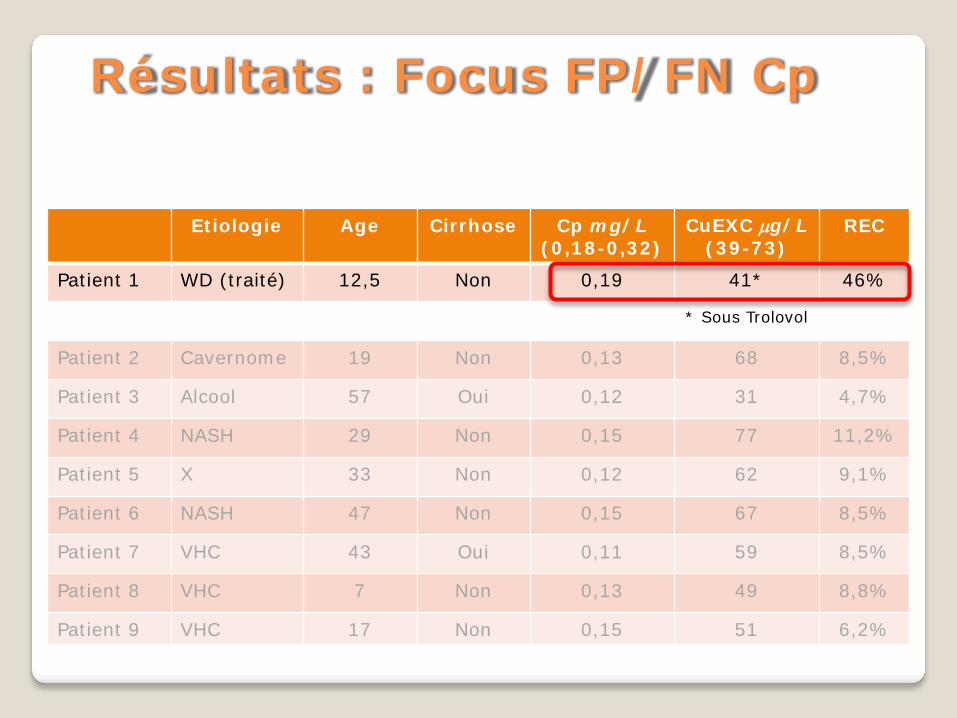
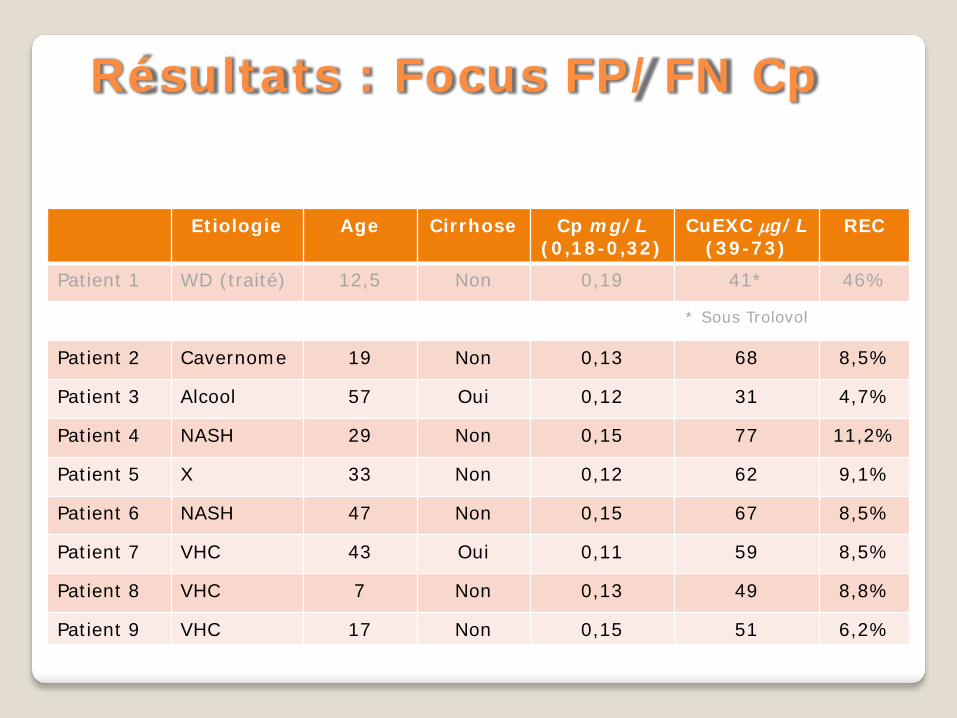
Résultats : Focus FP/FN Cp
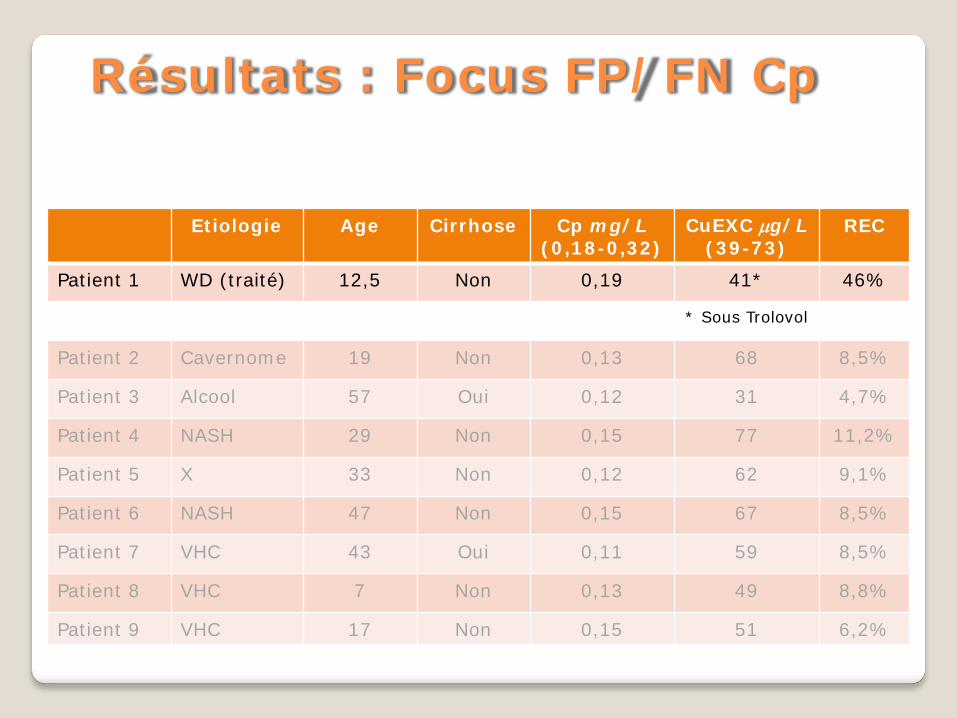
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
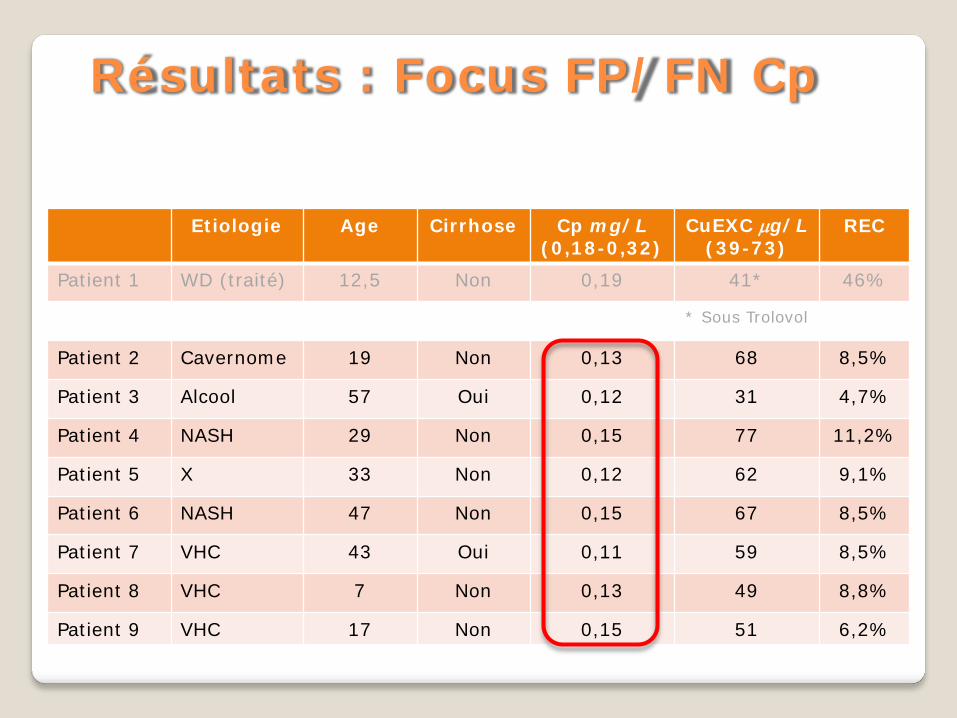
Résultats : Focus FP/FN Cp
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
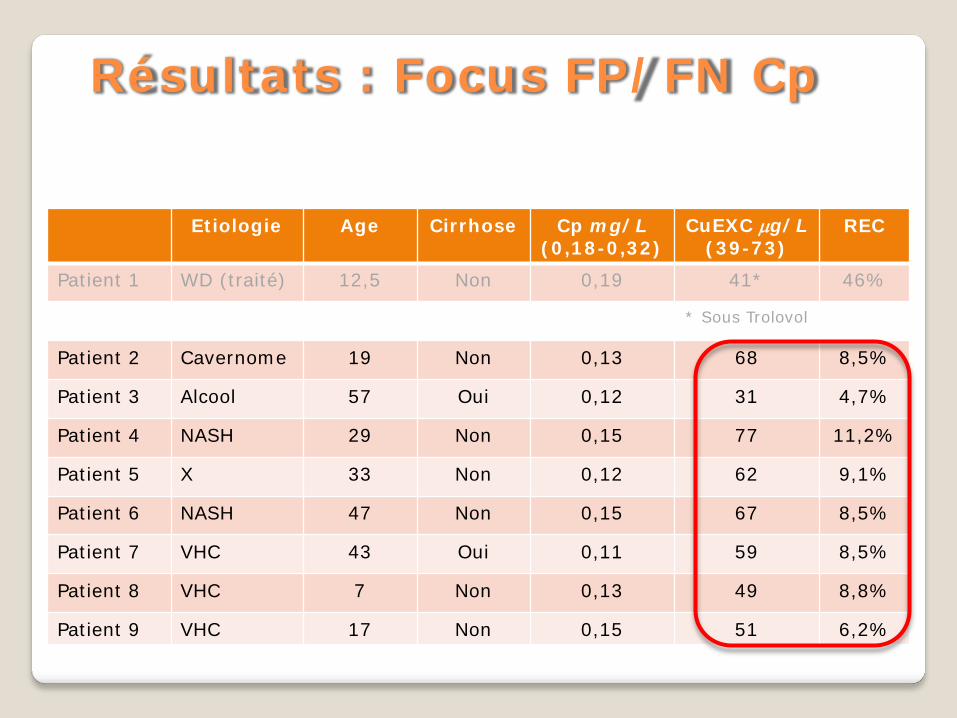
Résultats : Focus FP/FN Cp
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
Résultats : Focus FP/FN Cp
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
Résultats : Focus FP/FN Cp
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
Résultats : Focus FP/FN Cp
Etiologie Age Cirrhose Cp mg/L (0,18-0,32)
CuEXC µg/L (39-73)
REC
Patient 1 WD (traité) 12,5 Non 0,19 41* 46%
* Sous Trolovol
Patient 2 Cavernome 19 Non 0,13 68 8,5%
Patient 3 Alcool 57 Oui 0,12 31 4,7%
Patient 4 NASH 29 Non 0,15 77 11,2%
Patient 5 X 33 Non 0,12 62 9,1%
Patient 6 NASH 47 Non 0,15 67 8,5%
Patient 7 VHC 43 Oui 0,11 59 8,5%
Patient 8 VHC 7 Non 0,13 49 8,8%
Patient 9 VHC 17 Non 0,15 51 6,2%
Résultats : Focus FP/FN Cp
Cuivre échangeable semble un excellent marqueur pour le diagnostic de WD avec calcul REC (outil discriminant) aussi bien chez l’adulte que chez l’enfant
Limites : peu de nouveaux diagnostics, pas assez de patients Cp borderline
Nécessite études confirmatives sur grosses cohortes (PHRC) Intérêt dans hépatite aigue sévère ?
Conclusion
Cuivre échangeable semble un bon marqueur pour suivi patient
Études en cours
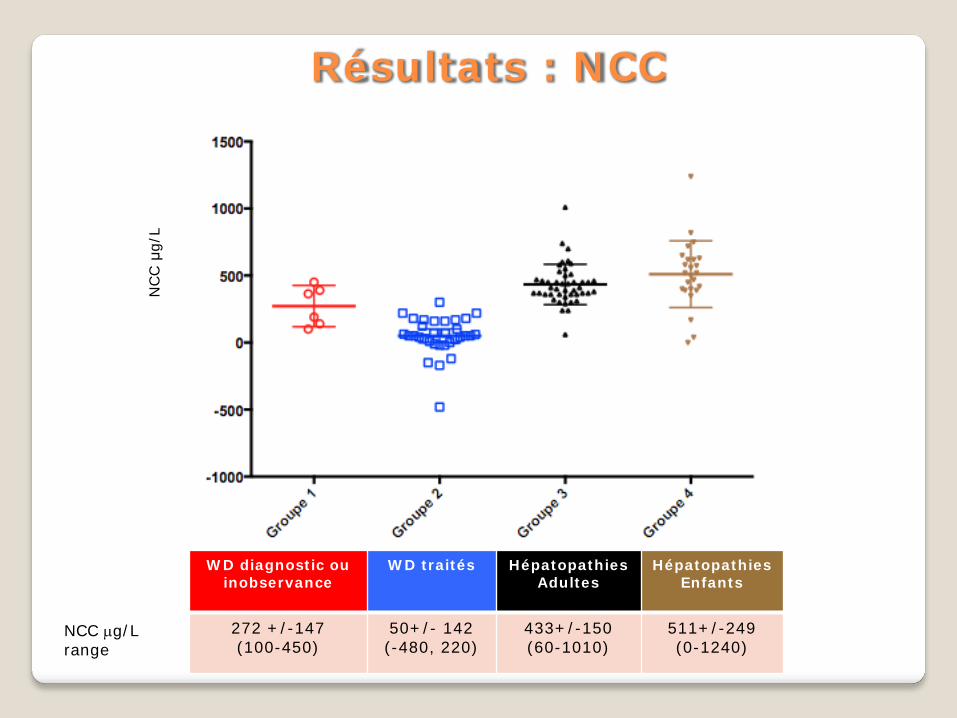
WD diagnostic ou inobservance
WD traités Hépatopathies Adultes
Hépatopathies Enfants
272 +/-147 (100-450)
50+/- 142 (-480, 220)
433+/-150 (60-1010)
511+/-249 (0-1240)
Résultats : NCC
NCC µg/L range
NCC μ
g/L
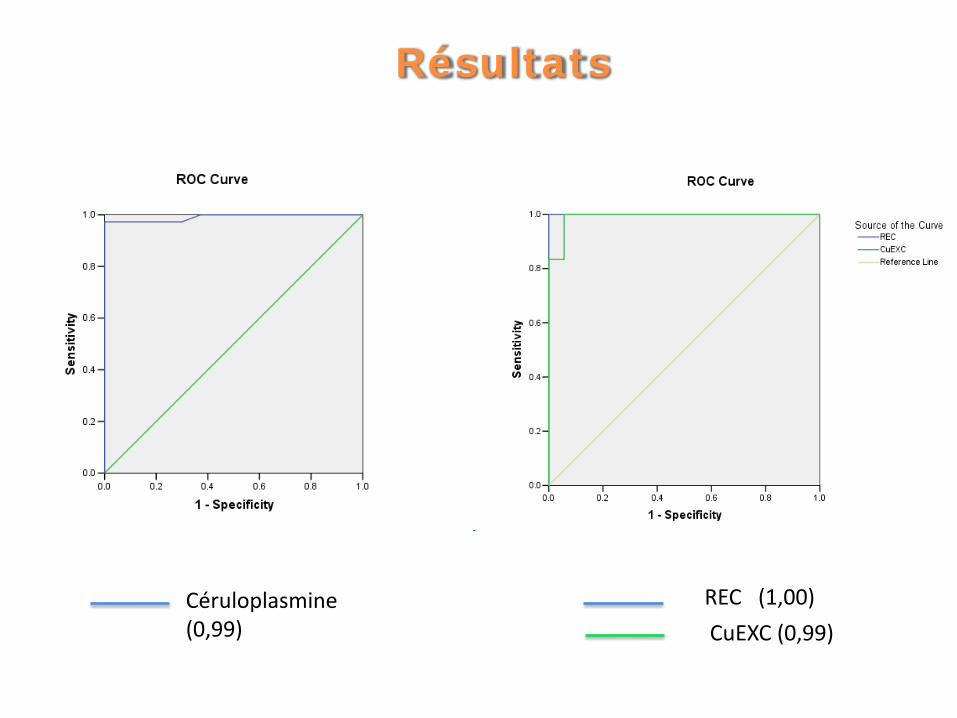
Résultats
Céruloplasmine (0,99)
REC (1,00) CuEXC (0,99)