HYSTERO RESECTION. - cice.fr - HYSTEROSCOPIE... · Sélection –“management“- des...
36
HYSTERO RESECTION. Dušan Tóth, MD, PhD. R. Arnaud, A.R.P Cayol,A.Gravier Clinique St.Germain, Brive la Gaillarde www.gynecobrive.fr Clermont Ferrand 2015
Transcript of HYSTERO RESECTION. - cice.fr - HYSTEROSCOPIE... · Sélection –“management“- des...

HYSTERO RESECTION.
Dušan Tóth, MD, PhD.
R. Arnaud, A.R.P Cayol,A.Gravier
Clinique St.Germain, Brive la Gaillarde
www.gynecobrive.fr
Clermont Ferrand 2015
Les développements des nouvelles techniques permettent le traitement des pathologies intra-utérines par hystéroscopie en première ligne.
La majorité des hystéroscopies peut être faite en régime ambulatoire, avec une anesthésie minimale ou sans anesthésie, respectant le confort des patientes.
HS – hospitalisation
HS - ambulatoire / hospit.de jour
HS – „cabinet“ / externe
Un travail d’équipe médicale commun – une prise en charge et approche spécifique - une prise en charge globale de la patiente !!!
I. phase préopératoire
II. phase opératoire
III. phase postopératoire
95 %
I. phase préopératoire.
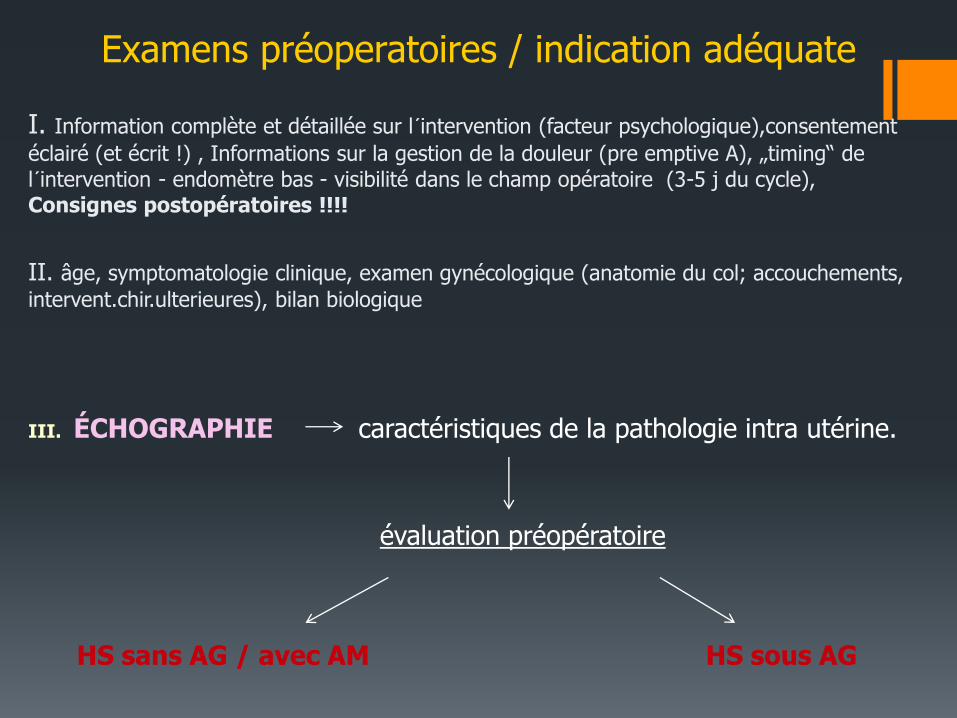
Examens préoperatoires / indication adéquate
I. Information complète et détaillée sur l´intervention (facteur psychologique),consentement
éclairé (et écrit !) , Informations sur la gestion de la douleur (pre emptive A), „timing“ de
l´intervention - endomètre bas - visibilité dans le champ opératoire (3-5 j du cycle), Consignes postopératoires !!!!
II. âge, symptomatologie clinique, examen gynécologique (anatomie du col; accouchements,
intervent.chir.ulterieures), bilan biologique
III. ÉCHOGRAPHIE caractéristiques de la pathologie intra utérine.
évaluation préopératoire
HS sans AG / avec AM HS sous AG
Sélection –“management“- des interventions sans / avec anésthesie genérale.
Interventions sans AG / avec AM:
« see and treat procedures » -
pathologies IU mineures
polypes (<1-2 cm)
myome (type 0 ESH, <1-2 cm)
synéchies (Igr.ESH)
Cloison IU
DIU
stérilisation tubaire Essure
[résections IU, Thermoablation]
Interventions sous AG :
Patientes anxieuses
Contraintes anatomiques
Type d´intervention
(myome I / II, polype >2cm, synéchie II a III)
• [résections IU, Thermoablation]
expérience du chirurgien
II. phase opératoire.
Gestion du bloc opératoire.
• Répartition de créneaux opératoires - matin, premières interventions
(occupation des lits ambulatoires / d’hospitalisation)
• Plateau technique – instruments appropriés, dg. /th., blocs opératoires, possibilité de stérilisation ! (choix entre restérilisable et usage unique )
• Coordination et compliance avec anesthésiste
• Engagement du personnel du bloc opératoire et du service d’hospitalisation
Gestion de la douleur – protocole anesthésie multimodale
1. analgésiques avant intervention
AINS – ibuprofene 400 mg + paracetamol 1gr. H-1 ou diclofenac 75 LP la veille 1 cp + 1 cp le matin avec paracetamol 1 gr.
2. Anesthésie locale – para cervicale . Naropeine 2 mg en 2-3 portions – sur 12H , 4 H et 8 H
3. Anesthésie intraveineuse
Propofol 0,8-1mg/kg

Anesthésie locale – para cervicale / intra-utérine.
10 - 20 ml divises en 2 ou 4 portions – le but est l´infiltration du ganglion de Frankensauser.
Xylocaïne 1%, Naropeine 2mg, Chirocaïne 2,5 mg
Anesthésie intra-utérine – infiltration du fond utérin.
Valle 1999, Cohen 1994…..
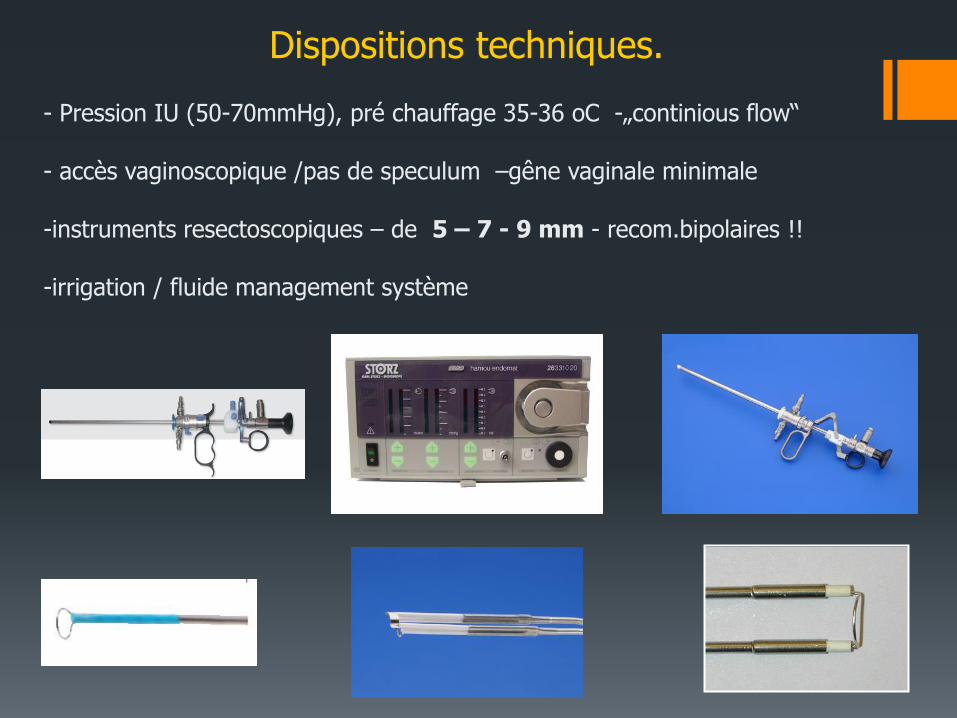
Dispositions techniques.
- Pression IU (50-70mmHg), pré chauffage 35-36 oC -„continious flow“ - accès vaginoscopique /pas de speculum –gêne vaginale minimale
-instruments resectoscopiques – de 5 – 7 - 9 mm - recom.bipolaires !! -irrigation / fluide management système
Electrochirurgie.
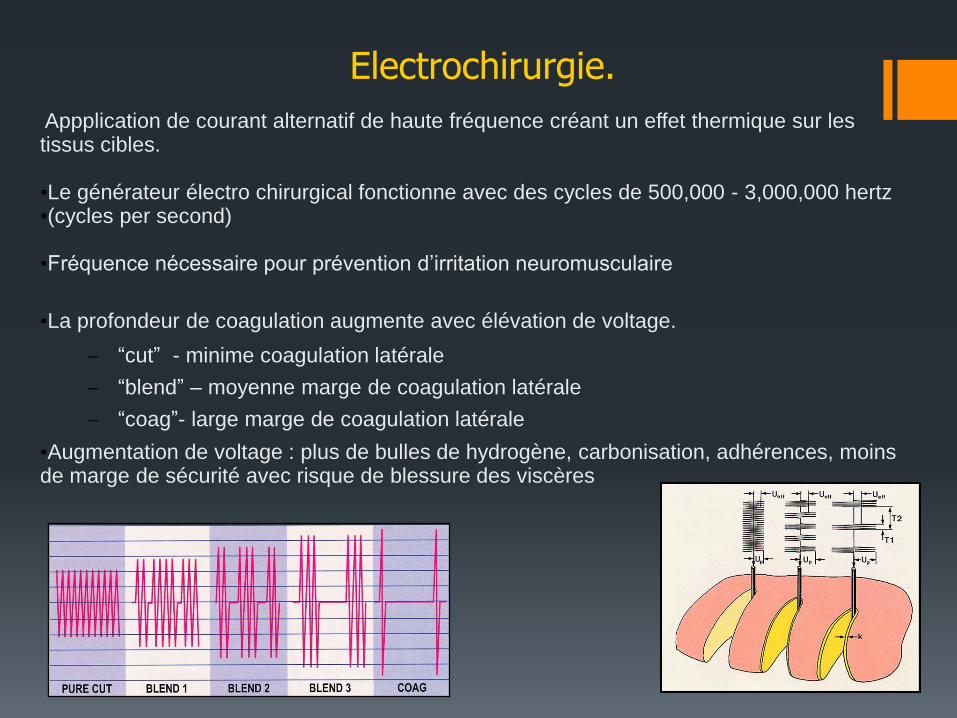
Appplication de courant alternatif de haute fréquence créant un effet thermique sur les tissus cibles. •Le générateur électro chirurgical fonctionne avec des cycles de 500,000 - 3,000,000 hertz •(cycles per second) •Fréquence nécessaire pour prévention d’irritation neuromusculaire
•La profondeur de coagulation augmente avec élévation de voltage.
“cut” - minime coagulation latérale
“blend” – moyenne marge de coagulation latérale
“coag”- large marge de coagulation latérale
•Augmentation de voltage : plus de bulles de hydrogène, carbonisation, adhérences, moins de marge de sécurité avec risque de blessure des viscères

Le courant de haute densité entre dans le tissus par une petite électrode active créant des effets thermiques secondaires.
Le courant traverse le patient par tissus electroconductibles.
Le courent est dispersé sur l’électrode de retour et revient vers le générateur.
Besoins de voltage suffisant pour ioniser le milieu et créer un arc électrique. Le courant est concentré dans points spécifiques. Densité haute de courant créant surchauffe de l’eau cellulaire > vaporisation cellulaire explosive créant une coupe / vaporisation. Le nuage de vapeur enveloppante facilite la création d’un arc électrique – minimalisé par contact avec tissus.
Principes d’électrochirurgie monopolaire
Le liquides de distension non conducteurs sont isolants.
-Glycine, sorbitol, mannitol
-La densité de courant est maintenue, effet chirurgical non réduit.
Chirurgie monopolaire et l’environement liquide.
Minimalisation des risques avec électrode de retour.
Maintenir une minimale résistance avec la peau
Sélectionner les régions de peau avec une bonne perfusion sanguine
Eviter les régions pileux, hyperkératose, cicatrice ou au dessus des régions osseuses
Sélectionnez des sites au dessus des muscles et le plus prés du site opératoire
Monitoring de l’électrode sur générateur
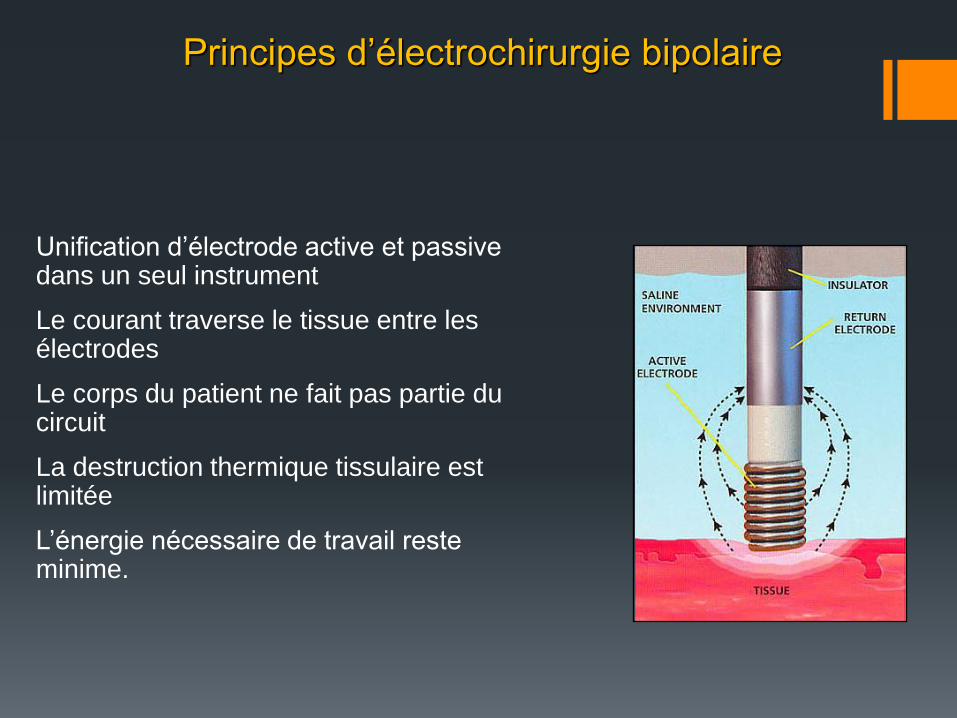
Unification d’électrode active et passive dans un seul instrument
Le courant traverse le tissue entre les électrodes
Le corps du patient ne fait pas partie du circuit
La destruction thermique tissulaire est limitée
L’énergie nécessaire de travail reste minime.
Principes d’électrochirurgie bipolaire

Resection de pathologie IU pediculée.
Si vaisseaux visibles – coagulation Si diamètre de la lésion + grande que diamètre du resectoscope – ne jamais couper le pied Lésion partiellement intra murale – utiliser ¨hydro massage¨ (variation de pression IU) >expulsion de la partie intra murale vers la cavité utérine Extraction des copaux si possible à la fin de l’intervention En cas de fibromes partiellement dans paroi – respecter la zone de sécurité / sous contrôle écho.
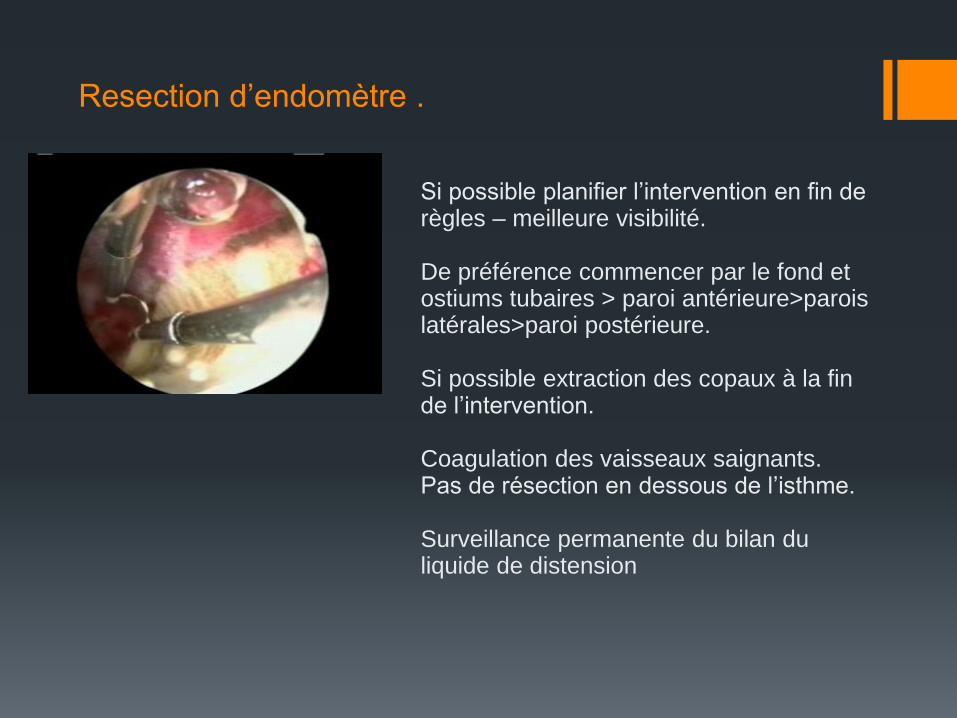
Resection d’endomètre .
Si possible planifier l’intervention en fin de règles – meilleure visibilité. De préférence commencer par le fond et ostiums tubaires > paroi antérieure>parois latérales>paroi postérieure. Si possible extraction des copaux à la fin de l’intervention. Coagulation des vaisseaux saignants. Pas de résection en dessous de l’isthme. Surveillance permanente du bilan du liquide de distension
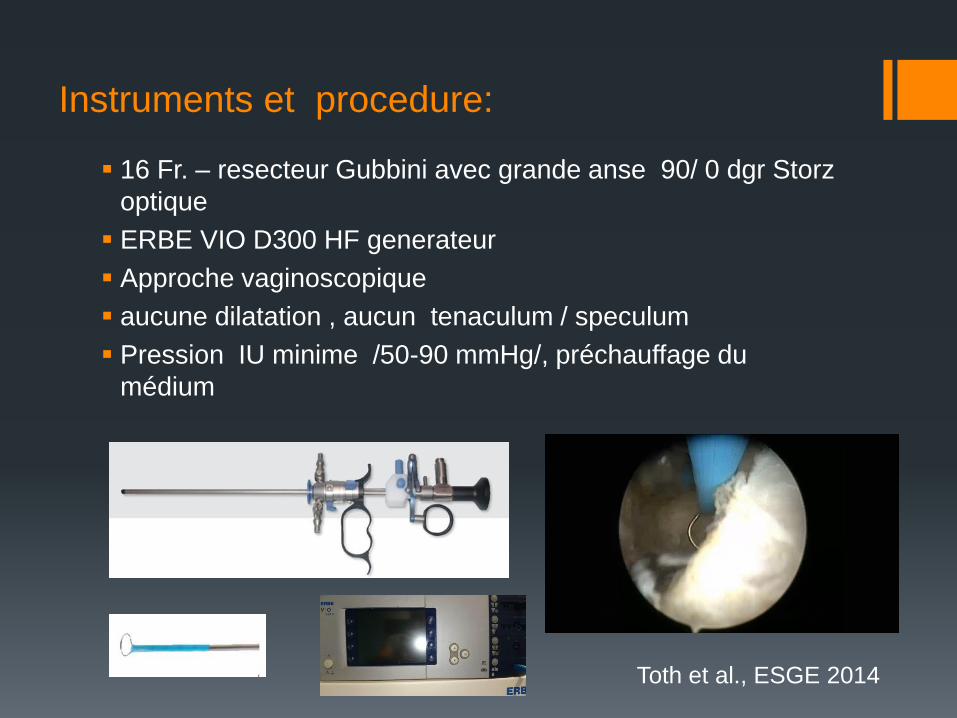
Instruments et procedure:
16 Fr. – resecteur Gubbini avec grande anse 90/ 0 dgr Storz
optique
ERBE VIO D300 HF generateur
Approche vaginoscopique
aucune dilatation , aucun tenaculum / speculum
Pression IU minime /50-90 mmHg/, préchauffage du
médium
Toth et al., ESGE 2014
0
10
20
30
40
50
60
70
80
90
100
1 3 5 7 9 11 13 15 17 19 21 23 25
Time
VAS
Uterus L
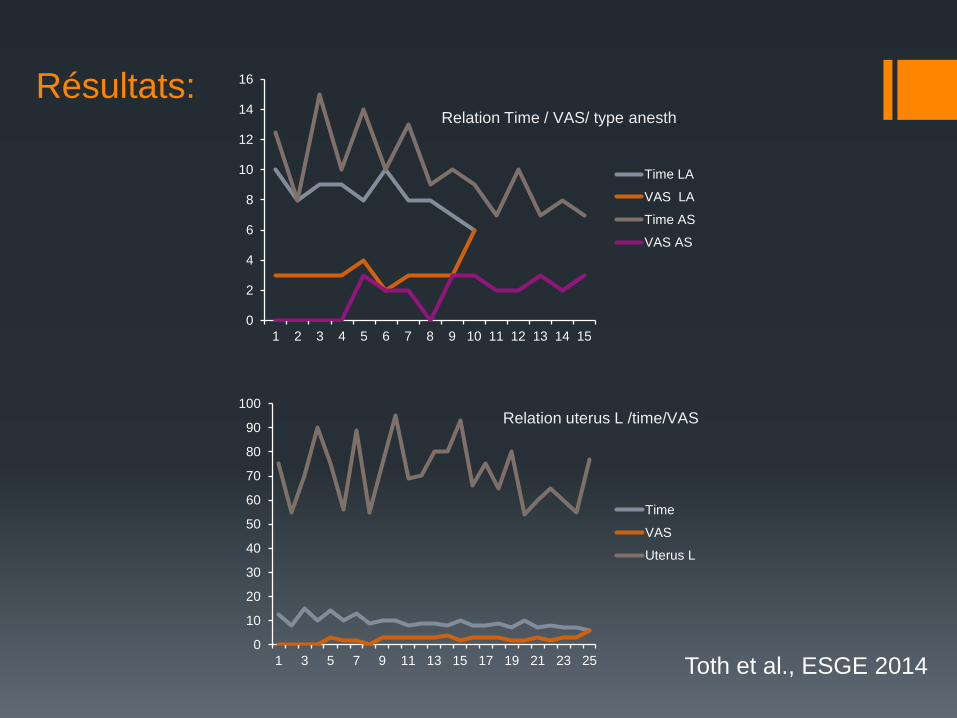
Relation uterus L /time/VAS
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Time LA
VAS LA
Time AS
VAS AS
Relation Time / VAS/ type anesth.
Résultats:
Toth et al., ESGE 2014
Prévention et résolution d’éventuelles complications
afin d´éviter les complications : RESPECTER LA SÉCURITÉ
visibilité du champ opératoire
électrode sous contrôle optique direct (200 oC !!!)
expérience (chir. IU, connaiss. de mécanismes d’intravasation )
puissance minimales
respecter l’anatomie /ostiums tubaires/
toutes manœuvres ¨douces¨, précise et rapides
contrôles du plateau technique
en cas de problème chirurgical / non chirurgical (fluide overload) une prise en charge multidisciplinaire
informations sur procédures dg. et thérapeutiques / personnel
dispo. ou lien vers unité de réanimation
Toute intervention IU ne devrait pas dépasser 20 min sans anesthésie !
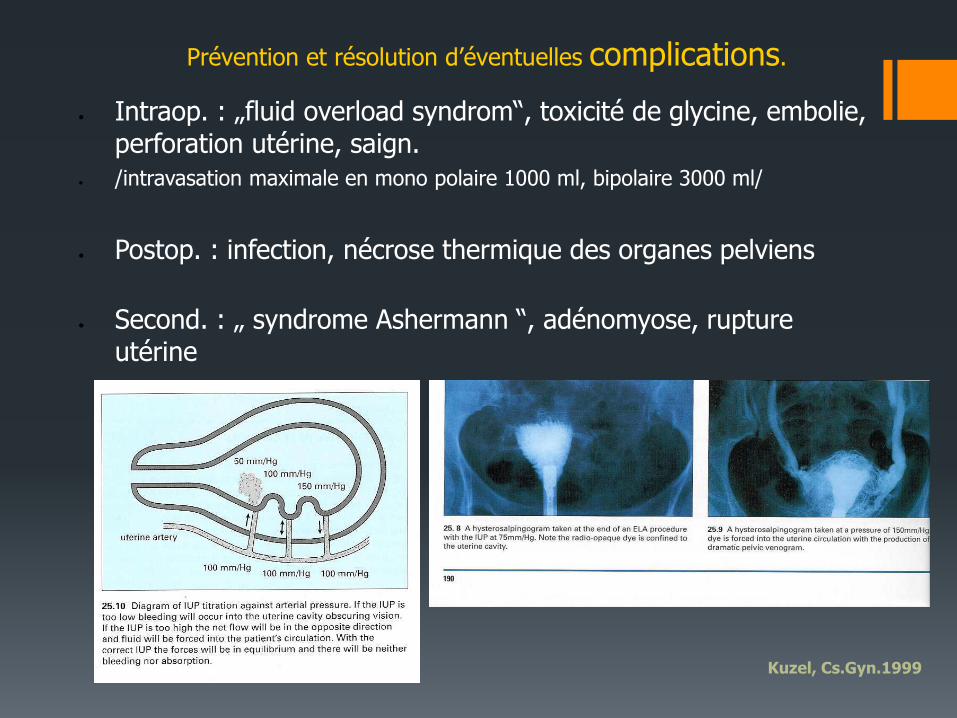
Intraop. : „fluid overload syndrom“, toxicité de glycine, embolie, perforation utérine, saign.
/intravasation maximale en mono polaire 1000 ml, bipolaire 3000 ml/
Postop. : infection, nécrose thermique des organes pelviens
Second. : „ syndrome Ashermann “, adénomyose, rupture utérine
Prévention et résolution d’éventuelles complications.
Kuzel, Cs.Gyn.1999
III. phase postopératoire.

Informations postopératoires.
Consignes à la sortie /heures et jours après intervention, et possibles complications/.
Lien envers le chirurgien ou service compétent
Gestion d’éventuelle douleur postopératoire (AINS, antalgiques)
Coût-bénéfice.
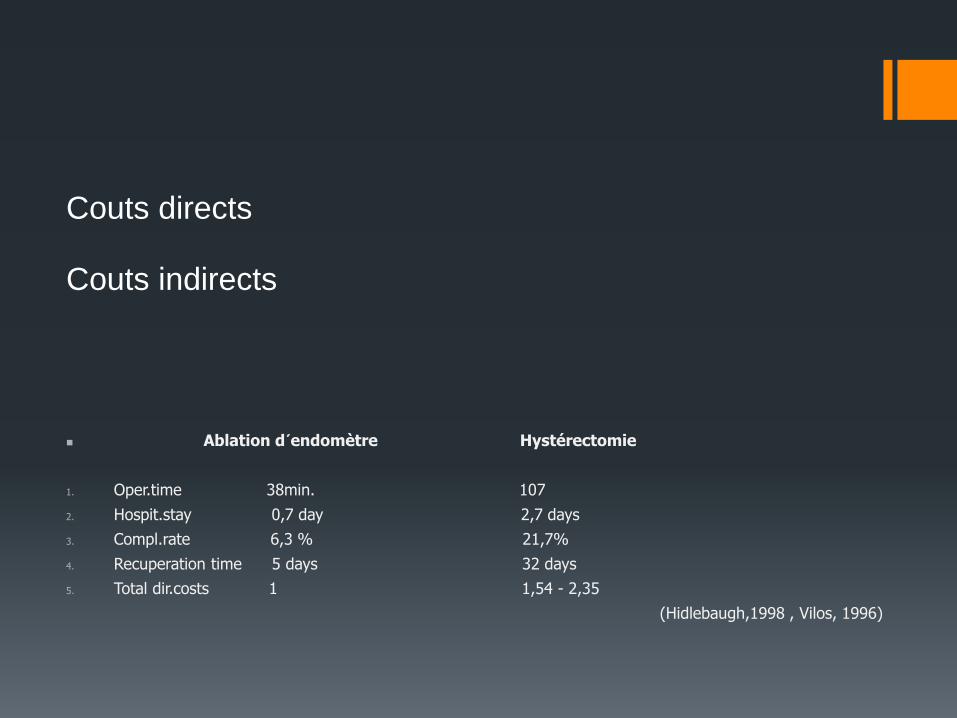
Ablation d´endomètre Hystérectomie
1. Oper.time 38min. 107
2. Hospit.stay 0,7 day 2,7 days
3. Compl.rate 6,3 % 21,7%
4. Recuperation time 5 days 32 days
5. Total dir.costs 1 1,54 - 2,35
(Hidlebaugh,1998 , Vilos, 1996)
Couts directs Couts indirects

GHMF SCP Saint Germain
Brive la Gaillarde Correze
www.gynecobrive.fr

SHORTCUT
Minimal anesthesia in transcervical surgery :
how far can we go?
Dušan Tóth, MD, PhD.
R. Arnaud, A.R.P Cayol,A.Gravier GHMF -Clinique St.Germain, Brive la Gaillarde
D.Kuzel,L.Hrazdirova,M.Mara **
**Gynekologicko porodnickà klinika VFN, Prague, Czech Republic .
ESGE – BERLIN - 2013
Main outcomes.
1/ diagnostic procedures – diagnostic hysteroscopy and biopsy :
Small diameters - reduction of diameter (Bettochi2002,2004, Vilos 2005)
No routine cervical priming /misoprostol/ with scopes less 5mm (Cooper
2011)
Minimal uterine distention – 25-70mmHg(Baker 1997)
Vaginoscopic approach, minimal distention pressure, pre heating od DM.
Paracervical block – decrease pain while cervix manipulation and
passage of internal os, but not effect on pain during biopsy
(Cooper2010).
Topical anesthesia and smaller hysteroscopes - decreased risk of
vasovagal syndrome (Cicinelli2003-10,Vilos2005 – versus Cooper ), do
not impact on pain relief during hysteroscopy/biopsy (Cooper2010).
Main outcomes.
2/ see and treat procedures
(concerning 4-5 mm scopes and 5Fr.instruments)
Low diameters – no need dilatation, no need anesthesia if proper patient
selection (DiSpiezio2010,Bettochi2002,2004….)
No differences in pain with 5 mm scope – LA versus any
anesth.(Garutti2008)
LA alone – paracervical block reduce pain during some portions of the
intervention –cervix, internal os – but not have effetc on pain during
implant placement in Essure (Kaneshiro2012)
Size of IU (<2cm) pathology and time (<than 15min) limiting factors in
S&T without anesthesia (Garutti2008,Cicinelli 2010)
Complet polyp/myoma resection – 60-80%cases (Gulumser2010)
Main outcomes.
3/ second generation ablation techniques
end 90ies – outpatient procedure – local anesth./ conscious sedation
Last years – oral analgesia and mowing from outpatient unit to office
(Clark2011,Chapa2010)
Pre-heating phase more painful
Novasure - 80-95 % suitable for office or outpatient in LA
(Kalkat2011,Pennix2009…..)
Microwave ablation - no difference between LA or GA , allocation to type
of anesthesia, parity , cavity depth, POVN and recovery (Wallage2003) –
but shorter stay if LA comparing to GA(Varma2008)
Shorter than TCRE, local anesthesia more used, equipement failure
more likely; less fluid overload,hematometra,perforations; but PONV and
deleyed pain (Lethaby 2010) – prevention !

Main outcomes.
4/ ¨traditional¨ resections
TCRE suitable with local anaesthesia – intracervical block – 278 w – 3
not completed and 9 i.v sedation due to pain (Ferry1994)
Local anesthesia and pre operative NSAID – enhance succes rate - 90%
acceptance (Readman2004).
Spinal block versus short GA /propofol-remifentanyl – better acceptance
of GA-accurate titration of of short acting anesthetics (Danelli2002)
Less glycine absorption in LA/SED than GA , less resorbtion with GA
than PDA (Goledenberg2001)
Perspectives of mini resectoscope in outpatient setting and LA
(Fernandez2011,Papalampros2009,Dealberti2013)
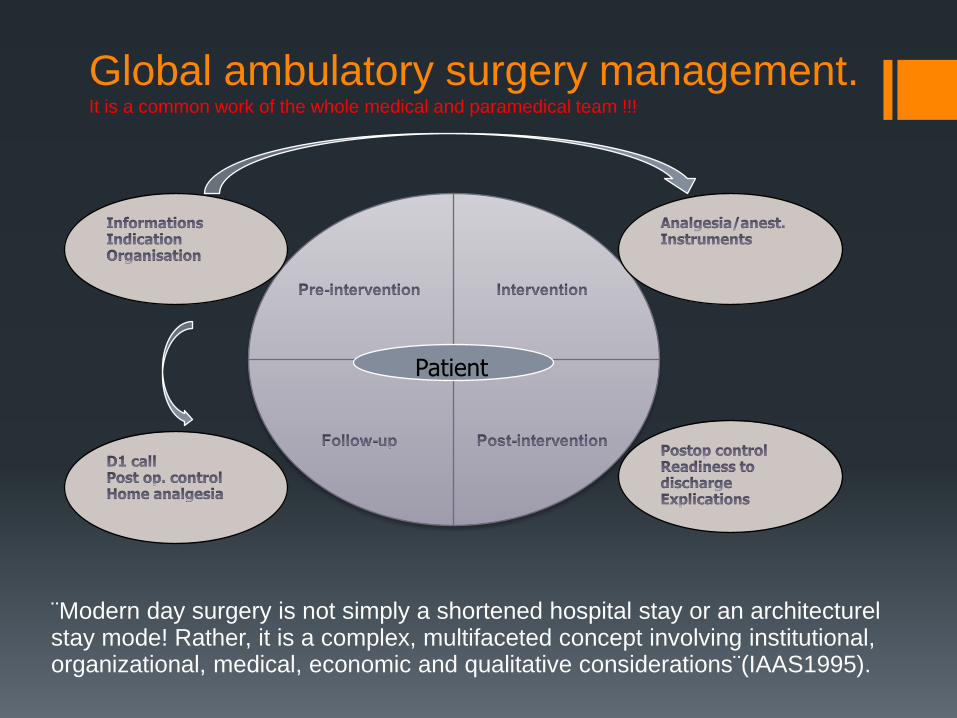
Global ambulatory surgery management. It is a common work of the whole medical and paramedical team !!!
¨Modern day surgery is not simply a shortened hospital stay or an architecturel stay mode! Rather, it is a complex, multifaceted concept involving institutional, organizational, medical, economic and qualitative considerations¨(IAAS1995).
Patient
Management of anesthesia/analgesia for
TCS.
1/ Pre emptive analgesia
NSAID do not relieve pain in surgical incision techniques comparing post op administration(animal models,Moiniche2002)
NSAID decrease the postoperative analgetics consumption (Duellman2009).
NSAID not significant effect for pain during anesthesia but significant after procedure versus placebo(Nagele1997)
NSAID+drotaverine synergic effect significant difference during and after the procedure comparing to LA alone or diazepam sedation (Sharma2009).
Oral premedication alone in HTA (NSAID+BD+COD) – 231/1 procedure converted to GA because of pain (Glasser2009)
Coxibs – reduction of gastrointestinal bleeding and platelet function – preferred option ? To be evaluate (Wickerts2011)
NSAID in association with paracetamol – faster and longer effect (O Flynn2010, Merry2010)
Role of long acting NSAID ?
Anxiolytics – hydroxyzine – better anxiolysis than placebo (Boon1996)
Management of anesthesia/analgesia for TCS.
• 2/ Local anesthesia
• Anesthetics :
• quick/short acting -Lignocaine, Lidocaine, Xylocaine
• slow/long acting : Bupivacaine 0,5% (bupivacaine liposome solution –longer action –Dasta 2012)
• levobupivacaine 2,5 mg
• ropivacaine 2mg
• Topical-spray/gel, intracervical, paracervical, intrauterine
Management of anesthesia/analgesia for TCS.
• 3/ i.v short anesthesia
• Benzodiazepines – Midazolam 1-2 mg
• /delayed elimination – obeses, aged patients/
• Propofol – 0,5 – 2 mg / kg /av. 1mg /kg/ - patient controlled sedation – reduction of total dosage
• Not recommended : Thiopenthal (PONV) ? Ketamine /dissociative anesthesia/ ?
• Alfentanyl > sufentanyl > remifentanil
• Corticoides – Dexamethasone – 8mg H-1, reduces NSAID and analgesic consumption
• Prevention of PONV /multimodal approach/
The analgesia / anesthesia solution.
Combination of described techniques
Multimodal anesthesia – synergic effect of minimal doses
(but no consensus or protocol up to day )
NSAID+paracetamol+paracerv.block +/- sedation +(prevention
of POVN) + ¨home¨rescue analgesia
Significant lower pain scores in postop period, less POVN and decrease length of
stay – Efectivness of multimo.pain management protocol in total knee
arthroplasty patients (Lewis2012) –
Minimal invasive LPSK myomectomy - signif. lower VAS scores for postoperative
pain betwen MMA protocol and without MMA.(Xiromeritis2011)
MMA 636 items!!!
Conclusion : minmal anesthesia end transcervical
surgery – how far can we go?
Not the procedure but patient is ambulatory /IAAS 1999/.
Proper surgical indication – selection
Proper instrumentation / reduction of diameter
Autoevaluation – practice and skill- rapidity and gentle manœuvres/manipulation – share of informations.
Minimal dosage and combination of methods – multimodal anesthesia
Pre operative and postoperative care /complete and true information -analgesia – rescue analgesia, complications, follow up /.
large majority of TCS (up to 95%?)