Hypertension pulmonaire associée aux pathologies ... filePlan 1. Classification et définition 2....
50
Hypertension pulmonaire associée aux pathologies cardiaques gauches: Une nouvelle cible thérapeutique? Jocelyn Dupuis MD, PhD Pas de conflits d’intérêts à déclarer Association des cardioloques du Québec, Florence, 1er Mai 2017
Transcript of Hypertension pulmonaire associée aux pathologies ... filePlan 1. Classification et définition 2....
Hypertension pulmonaire
associée aux pathologies
cardiaques gauches: Une
nouvelle cible thérapeutique?
Jocelyn Dupuis MD, PhD
Pas de conflits d’intérêts à déclarer
Association des cardioloques du Québec,
Florence, 1er Mai 2017

L’Insuffisance
cardiaque entraine
avec elle d’autres
organes…

Thérapies de l’HTP
post-capillaire
Aucune !
Pourquoi les
insuffisants cardiaque
sont-ils dyspnéiques?

Parce que l’IC est aussi
une maladie
pulmonaire...
Plan 1. Classification et définition
2. Importance du problème
3. Pathophysiologie
4. Impact pronostique
5. Comment mesurer et évaluer Rx
6. Le futur…
Hypertension pulmonaire (PH)
VS
Hypertension artérielle pulmonaire (PAH)
VS
Hypertension pulmonaire post-capillaire (pc-
PH)

Updated PH
Classification 5th World PH Symposium, 2013 1. Pulmonary arterial hypertension
(PAH)
2. PH due to left heart disease
3. PH due to lung disease and/or
hypoxia
4. Chronic thromboebolic PH (CTEPH)
5. PH with unclear multifactorial
mechanisms JACC 2013 62(25):D34-D41.

Group 2 PH:
Due to left heart disease
2.1 Left ventricular systolic dysfunction
2.2 Left ventricular diastolic dysfunction
2.3 Valvular disease
2.4 Congenital/acquired left heart inflow/
outflow obstruction and congenital
cardiomyopathies

Definition of PH
• Mean pulmonary arterial pressure ≥25
mmHg
Cardiac cath.
Echocardiographic screening
• Systolic pulmonary arterial pressure of 36-50 mmHg
Group II PH: confusion with
definitions
Proportionate vs Out-of-
proportion
Passive vs Reactive
Venous vs Arterial
Pre-capillary vs Post-capillary
Reversible vs Irreversible

Définition de l’HTP du groupe II:
HTP post-capillaire
Terminology Abbreviation Mean
PAP PAWP
TPG
or PVR* DPG**
Isolated
post-capillary Ipc-PH ≥25 mmHg >15 mmHg
≤15 mmHg
or
≤3 WU
< 7 mmHg
or
≤3 WU
Combined
pre and post-capillary
Cpc-PH ≥25 mmHg >15 mmHg
>15 mmHg
or
>3 WU
≥7 mmHg
or
>3 WU
*J Heart Lung Transplant 2012;31:913–33
**JACC 2013 62(25);D100-D108
TPG: Mean PAP - PAWP
DPG: diast PAP - PAWP
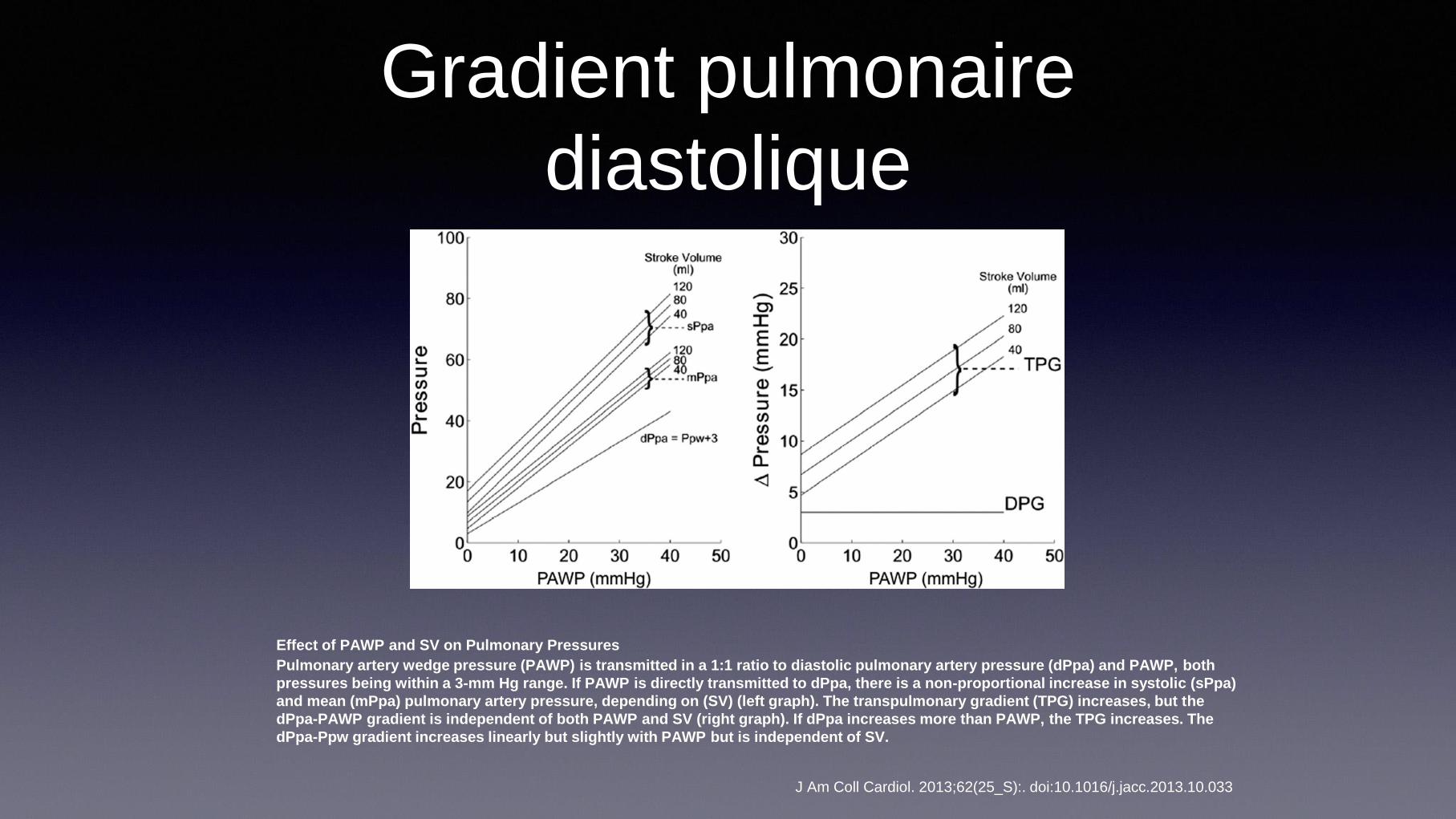
Gradient pulmonaire
diastolique
J Am Coll Cardiol. 2013;62(25_S):. doi:10.1016/j.jacc.2013.10.033
Effect of PAWP and SV on Pulmonary Pressures
Pulmonary artery wedge pressure (PAWP) is transmitted in a 1:1 ratio to diastolic pulmonary artery pressure (dPpa) and PAWP, both
pressures being within a 3-mm Hg range. If PAWP is directly transmitted to dPpa, there is a non-proportional increase in systolic (sPpa)
and mean (mPpa) pulmonary artery pressure, depending on (SV) (left graph). The transpulmonary gradient (TPG) increases, but the
dPpa-PAWP gradient is independent of both PAWP and SV (right graph). If dPpa increases more than PAWP, the TPG increases. The
dPpa-Ppw gradient increases linearly but slightly with PAWP but is independent of SV.

Définition de la reversibilité
TPG PVR DPD
Reversible, reactive or
vasoreactive PH <12 mmHg <3 WU ?

JACC: HEART FAILURE VOL. 3, NO. 1, 2015

Les pathologies cardiaques
gauches: la cause la plus
fréquente d’HTP
• Incidence de 20% à 60%
• Dépend de la population étudiée
• Dépend de la définition utilisée…
1. Ghio S, J Am Coll Cardiol. 2001; 37:183-188.
2. Butler J, J Am Coll Cardiol. 1999; 34:1802-1806.
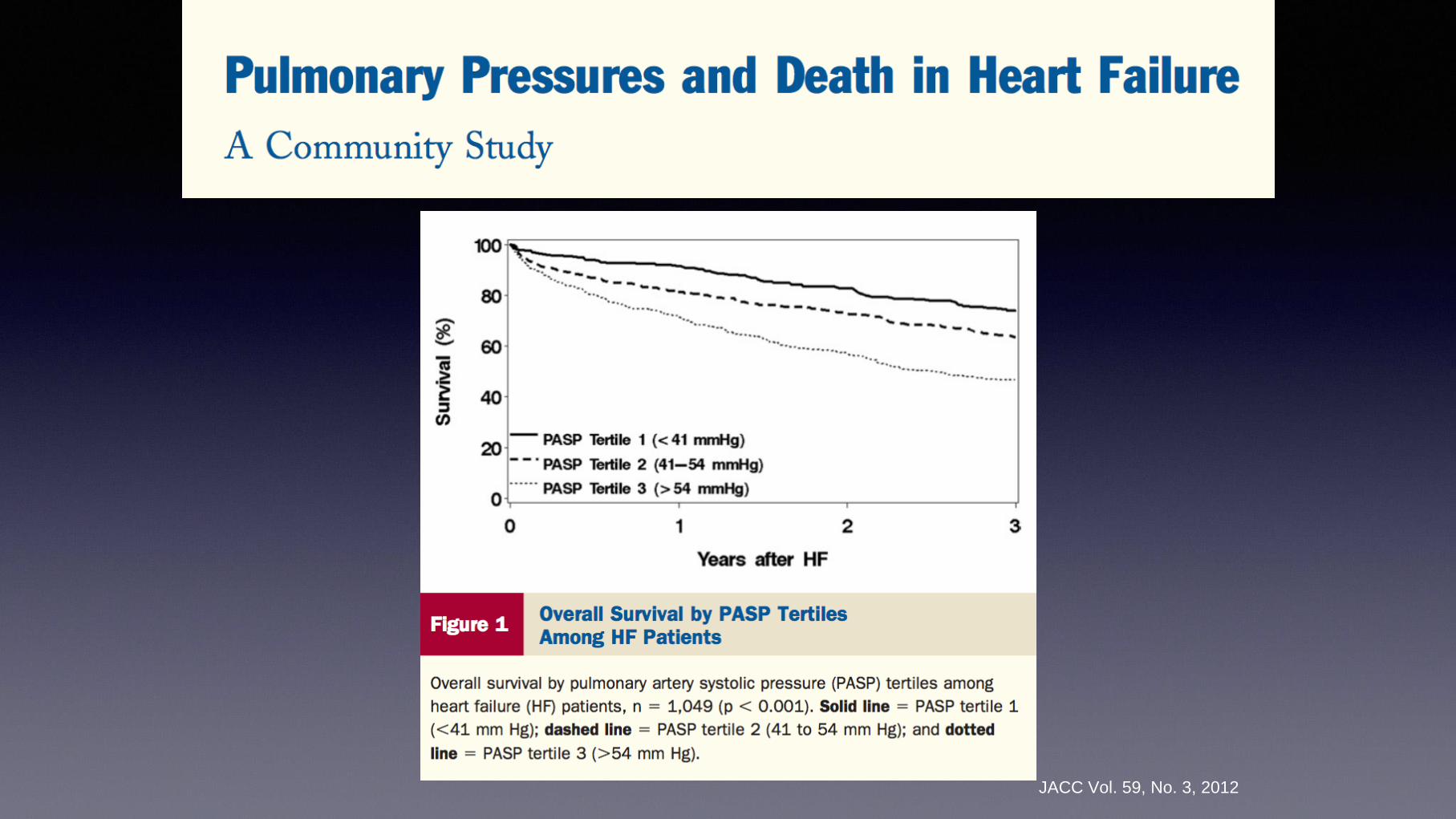
JACC Vol. 59, No. 3, 2012
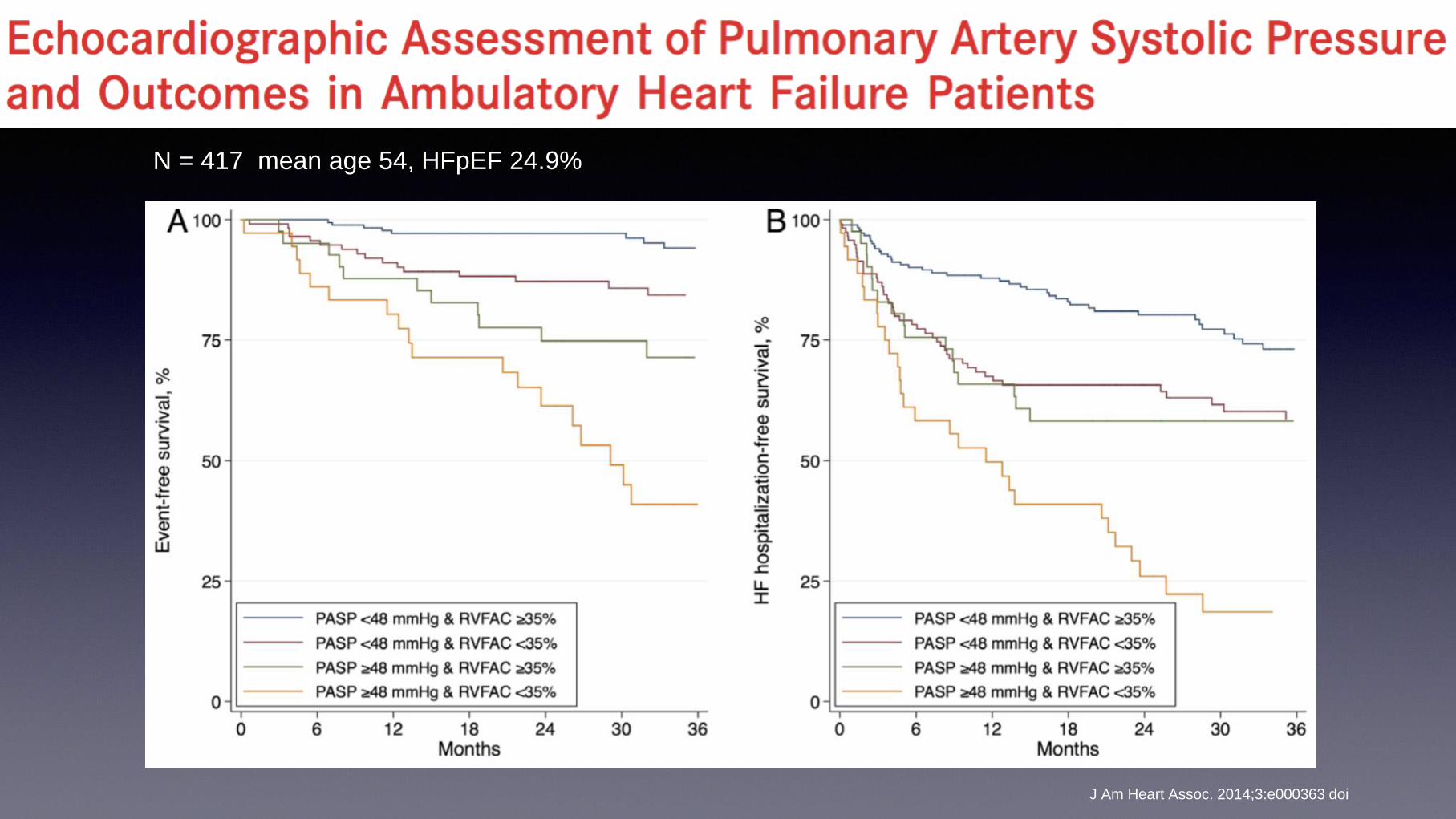
J Am Heart Assoc. 2014;3:e000363 doi
N = 417 mean age 54, HFpEF 24.9%
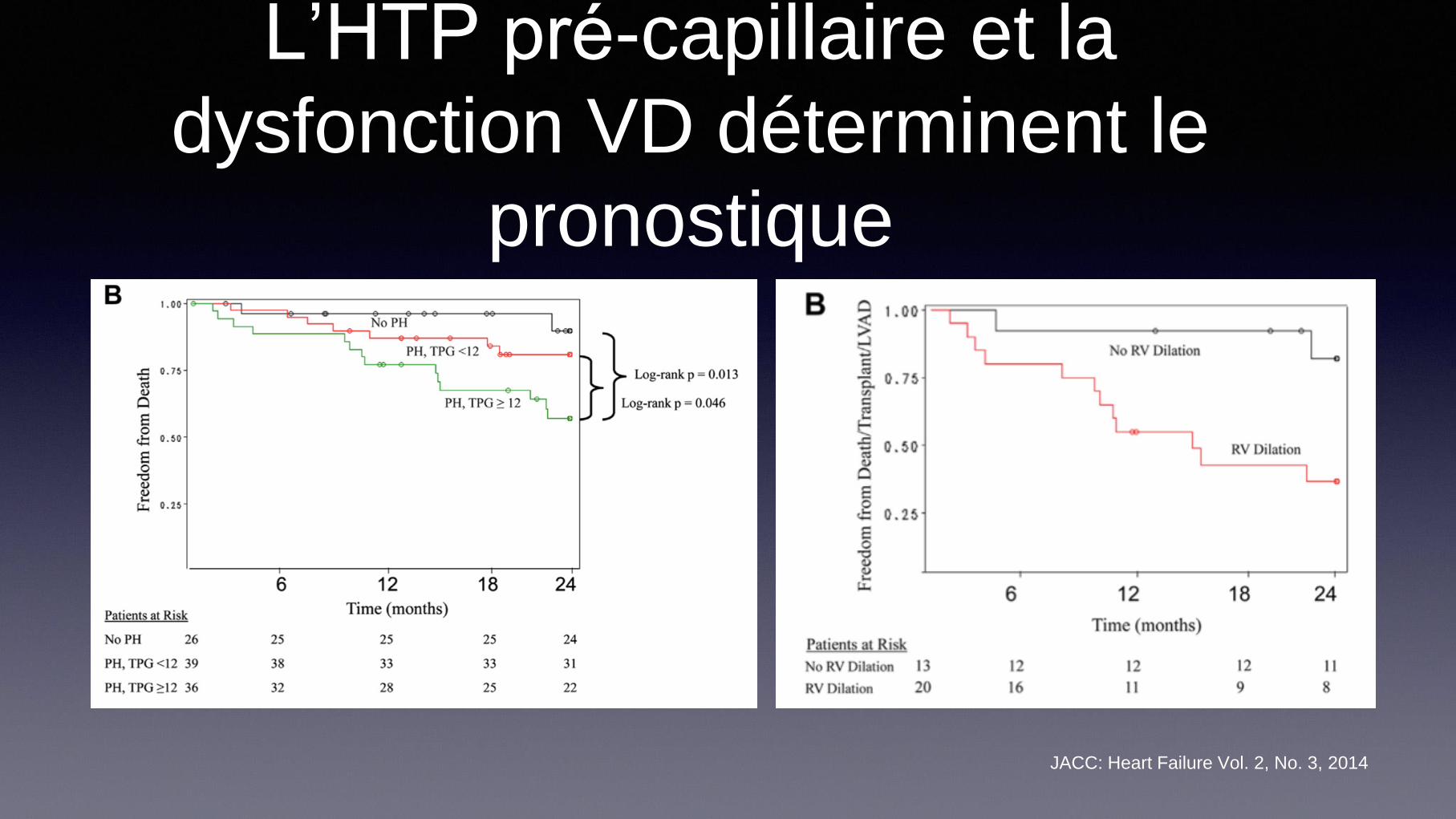
L’HTP pré-capillaire et la
dysfonction VD déterminent le
pronostique
JACC: Heart Failure Vol. 2, No. 3, 2014

J Thorac Cardiovasc Surg 2016;152:394-400
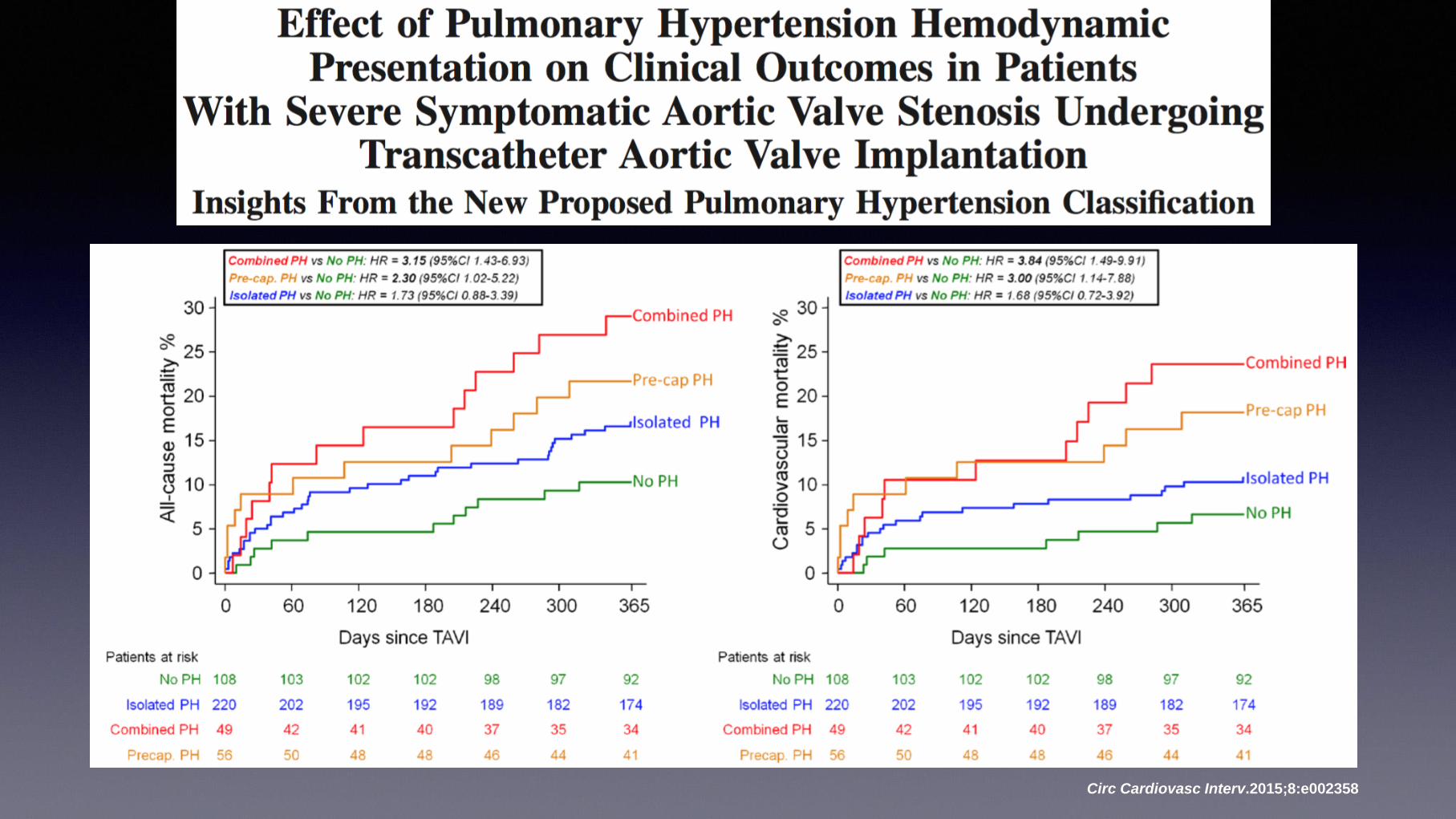
Circ Cardiovasc Interv.2015;8:e002358

Couplage VD-AP:
Compliance
pulmonaire
TAPSE/PAPs
J Am Coll Cardiol 2017;69:1718–34
Un paradoxe de l’IC…
• Un sujet préalablement sain développe de
l’œdème pulmonaire critique quand sa PCPB
augmente à 25 mmHg de façon aigue
• Plusieurs patients avec IC chronique stable sont
ambulatoire avec des pressions encore plus
élevées…

Manifestations pulmonaires de
l’insuffisance cardiaque
• Physiologie restrictive: dimimution des volume et
de la compliance
• Reduction de la Dlco: surtout par réduction de
perméabilité capillaire
• Pas amélioré par: diurèse, ultra-filtration et même
transplantation
• Corrélé avec capacité d’exercice et facteur
pronostique indépendant The pulmonary manifestations of left heart failure. Chest. 2004;125:669-82.

Alveolar–capillary membrane gas conductance:
a novel prognostic indicator in chronic heart
failure 106 CHF patients, LVEF 33 ± 1%
Eur Heart J. 2002;23:467-76.

Gas diffusion and alveolar–capillary
unit in chronic heart failure
European Heart Journal (2006) 27, 2538–2543

Cardiopulmonary Exercise Testing as a Diagnostic Tool for
the Detection of Left-sided Pulmonary Hypertension in
Heart Failure
Journal of Cardiac Failure Vol. 19 No. 7 2013

Oscillatory Breathing and Exercise Gas Exchange Abnormalities
Prognosticate Early Mortality and Morbidity in Heart Failure
J. Am. Coll. Cardiol.2010;55;1814-1823

Qu’est-ce qui cause le
remodelage alvéolaire
pulmonaire ?

Human lungs Rat lungs
Control
Left heart disease
Clinical Science 2014, 127; 65-76

Prolifération de Myofibroblastes
MI MI + Irbe
Smooth muscle α-actin
Cardiovascular Research 58 (2003) 621-631


Alveolar remodelling in left heart disease
Increased lung capillary
pressure
Alveolar-capillary stress failure
TGF-ß
Cytokines
PDGF
CTGF
TGF-ß
Angiotensin II
Endothelin
Aldosterone
Osteopontin
Systemic neurohumoral activation
Reduced cardiac output
Endothelial mesenchymal transition
Epithelial mesenchymal transition
Resident mesenchymal cells
Circulating fibrocytes
Myofibroblasts Differentiation and proliferation
α-SMA
Desmin
Cadherin
Extracellular matrix deposition: Elastin
Collagen
Reticulin
Basement membrane-like material
Thickening of alveolar
septa
Protective: Reduced pulmonary oedema
Maladaptive: Reduce oxygen diffusing capacity
increased lung weight and stiffness
Restrictive lung syndrome
Contribution to pulmonary hypertension
Reduced exercise tolerance
Genetic
predisposition?
Clinical Science 2014, 127; 65-76
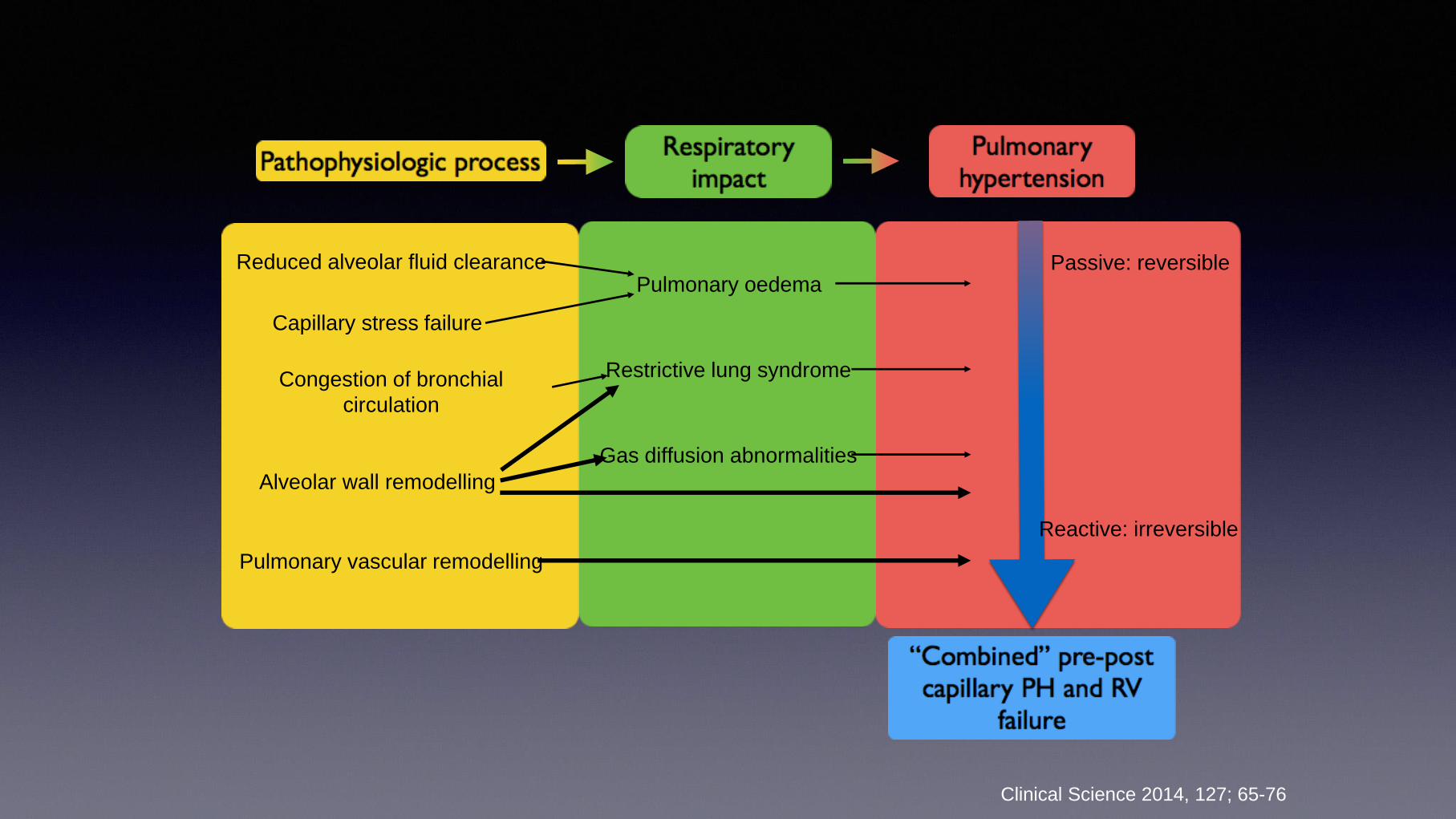
Capillary stress failure
Congestion of bronchial
circulation
Reduced alveolar fluid clearance
Alveolar wall remodelling
Pulmonary vascular remodelling
Pulmonary oedema
Restrictive lung syndrome
Gas diffusion abnormalities
Passive: reversible
Reactive: irreversible
Clinical Science 2014, 127; 65-76

Failure of trials in
LHD
JACC 2013 62(25);D100-D108
.
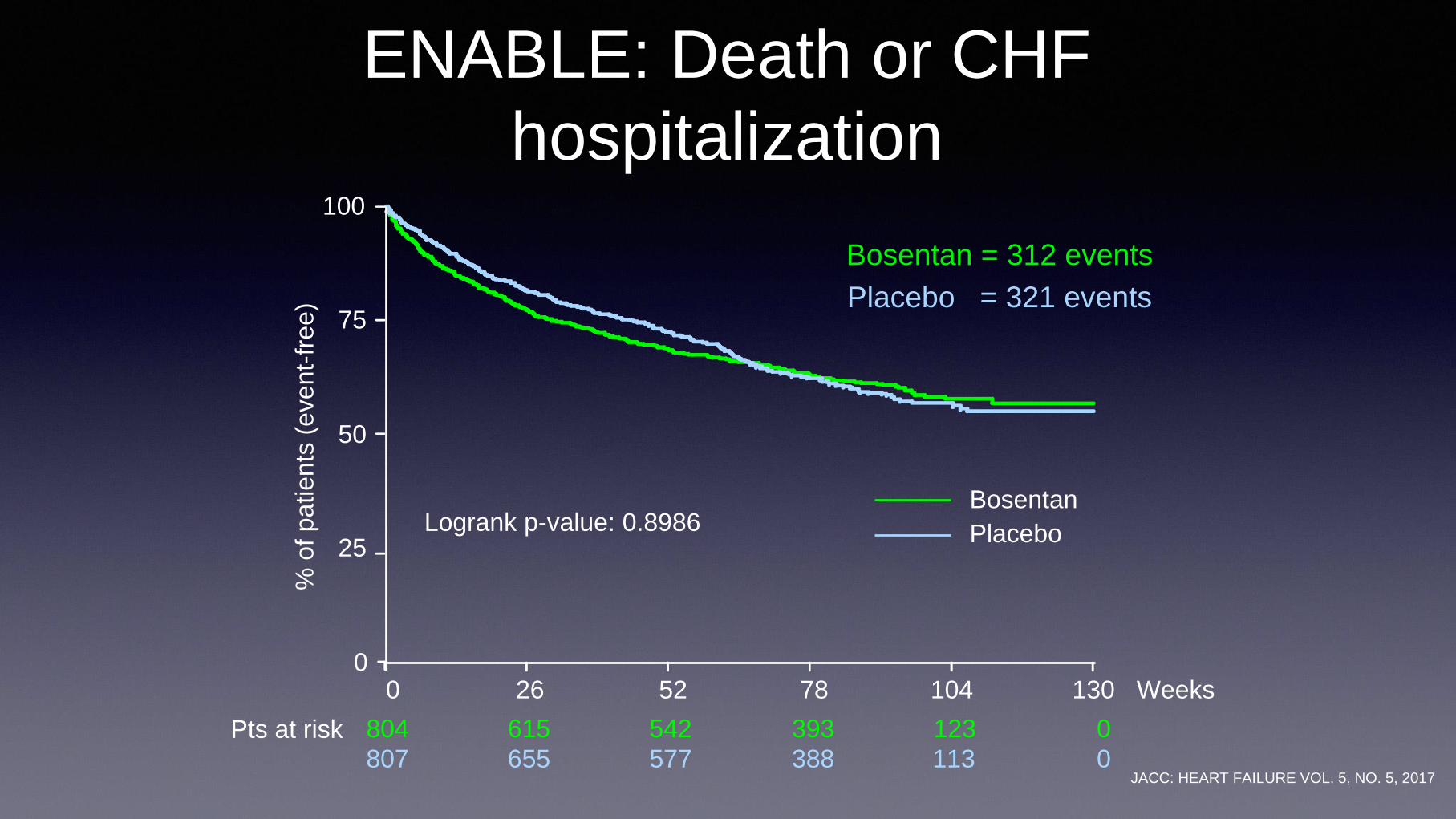
Pts at risk 804 615 542 393 123 0
807 655 577 388 113 0
ENABLE: Death or CHF
hospitalization
Bosentan = 312 events
Placebo = 321 events
Logrank p-value: 0.8986
0 26 52 78 104 130 Weeks
Bosentan
Placebo
% o
f patients
(event-
free)
0
25
50
75
100
JACC: HEART FAILURE VOL. 5, NO. 5, 2017

Effect of Phosphodiesterase-5 Inhibition on Exercise Capacity and Clinical
Status in Heart Failure With Preserved Ejection Fraction: RELAX trial
JAMA 2013 309, 1268–1277
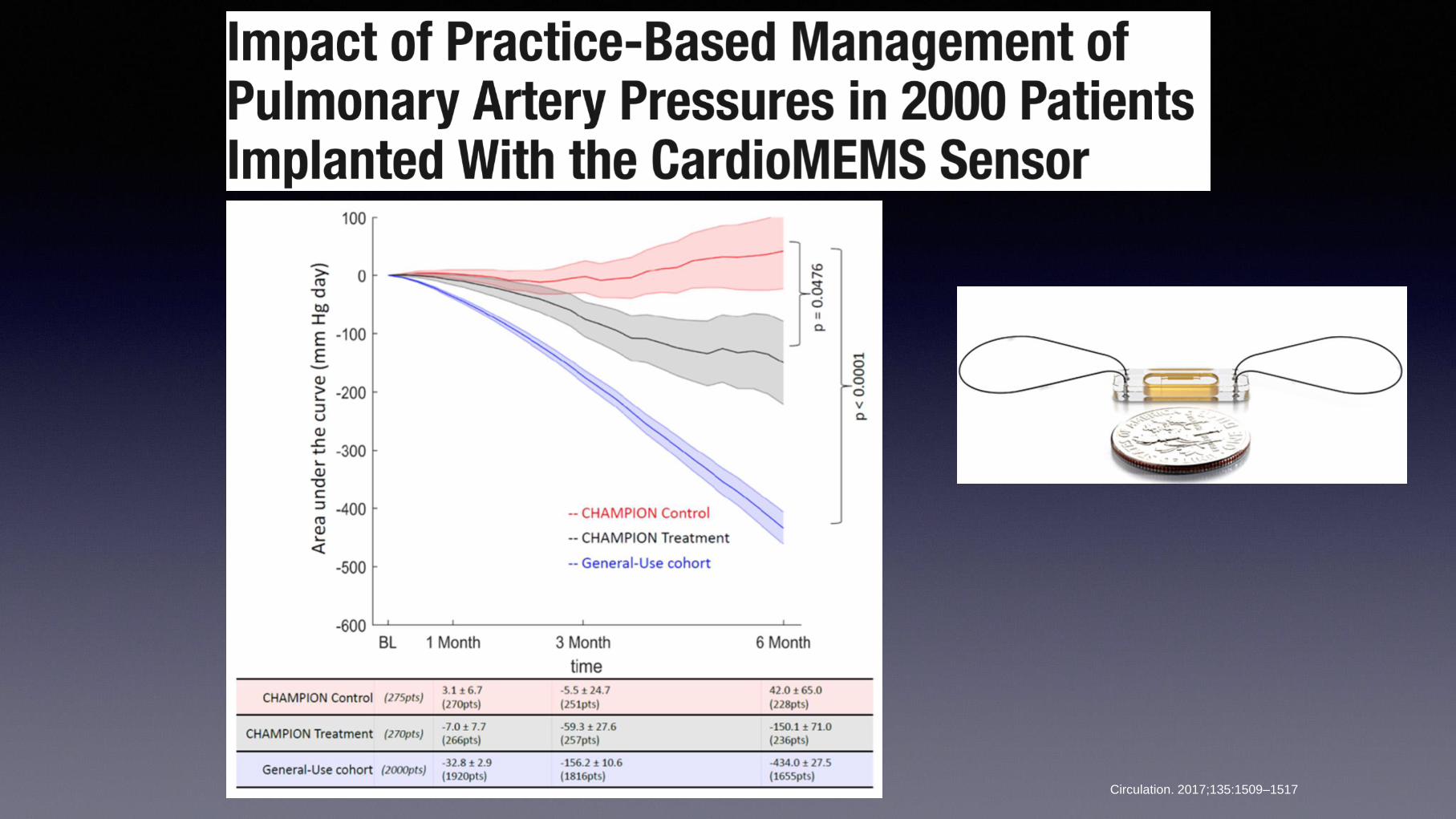
Circulation. 2017;135:1509–1517

Future trials should… • Evaluate the presence of PH and select subjects
accordingly
• combined PH
• reversible vs not reversible
• Incorporate evaluation of RV function and coupling
• Incorporate evaluation of lung remodeling
• Lung function testing
• CPX testing with VE/VCO2
• Novel markers of lung damage

Dynamic lung uptake of PulmoBind
in human
Mol Imaging 2015: 14: 1535-1538.
1) Hagner S. et al. Cell Tissue
Res (2002) 310:41–50

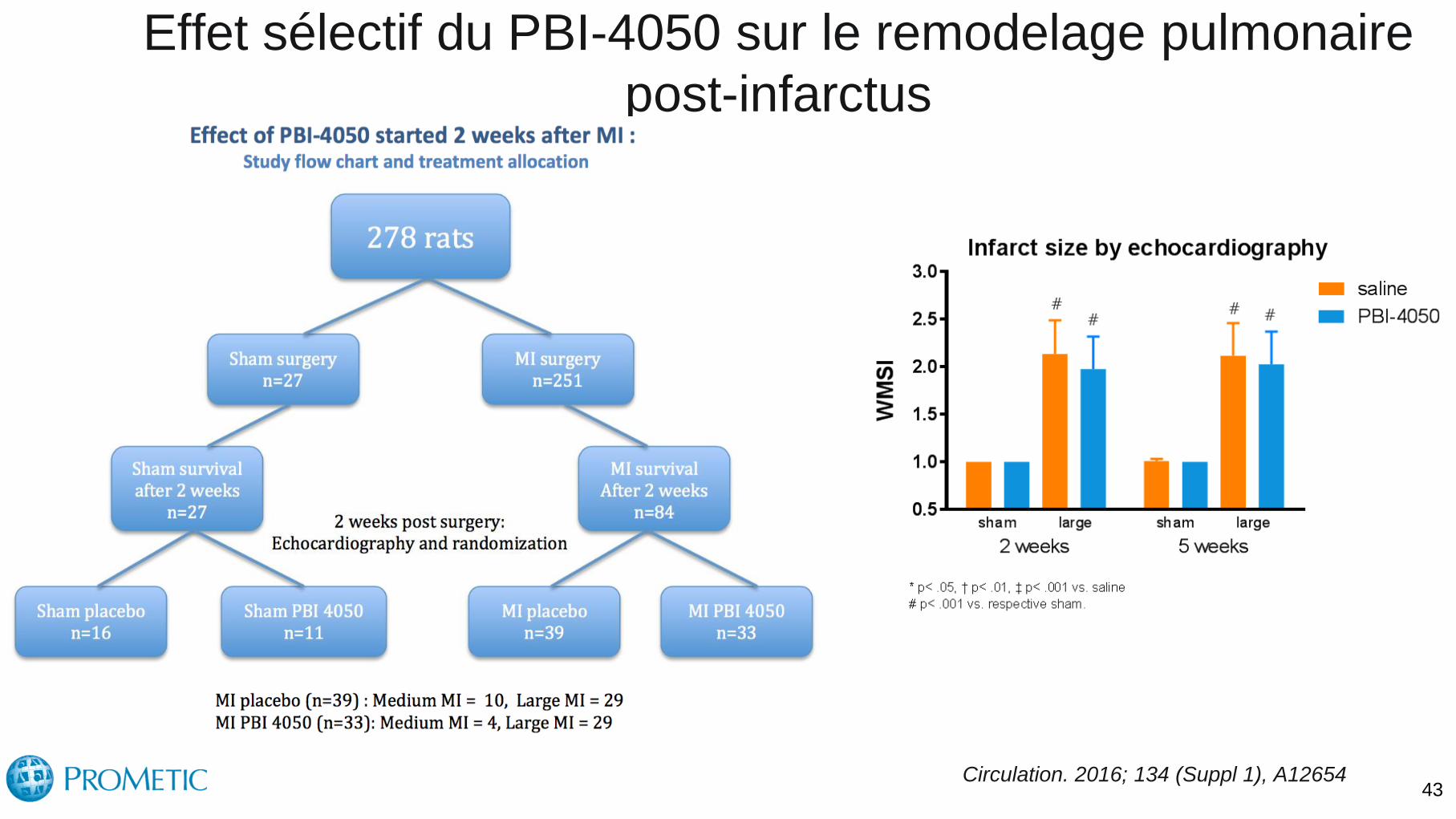
Effet sélectif du PBI-4050 sur le remodelage pulmonaire
post-infarctus
43 Circulation. 2016; 134 (Suppl 1), A12654

44
PBI-4050 Reduced RV Hypertrophy and Improved RV Function in Heart Failure with Reduced Ejection Fraction
Circulation. 2016; 134 (Suppl 1), A12654

Conclusion • LHD is the most frequent cause of PH
• Pathophysiology different form PAH: Capillary injury with MYF proliferation
• Restrictive lung syndrome with reduced gas exchange
• Effects of PAH treatments cannot be extrapolated to group II PH (ERAs, PDE5 inh etc)
• Properly sized studies need to be performed with better phenotyping:
• Combined pre-post capillary PH
• Reversibility vs no reversibility
• RV function
• Restrictive lung syndrome
• Gaz exchange (VE/VCO2)
• Markers of lung remodeling
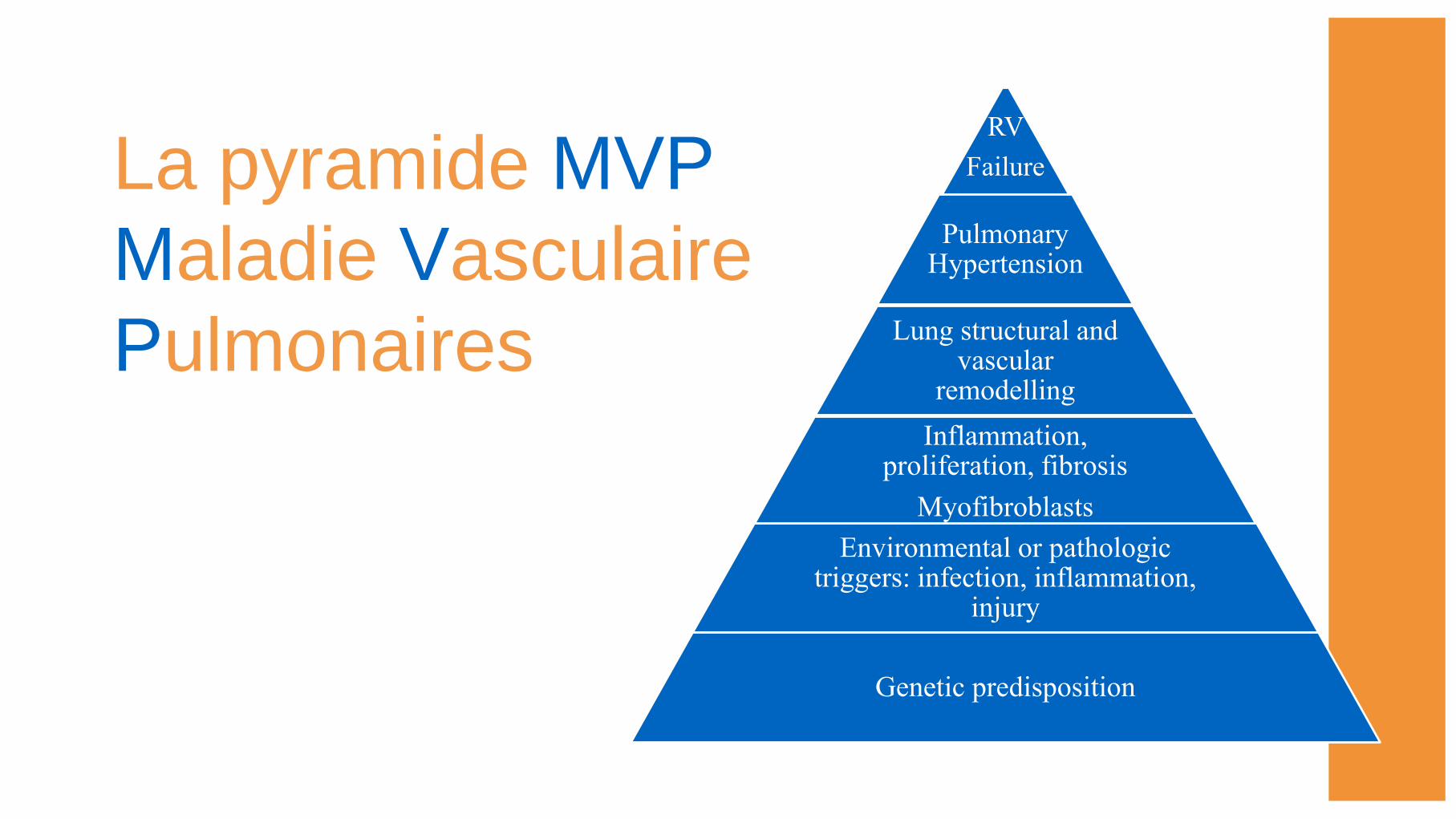
La pyramide MVP
Maladie Vasculaire
Pulmonaires
RV
Failure
Pulmonary Hypertension
Lung structural and vascular
remodelling
Inflammation, proliferation, fibrosis
Myofibroblasts
Environmental or pathologic triggers: infection, inflammation,
injury
Genetic predisposition
References
• J Am Coll Cardiol 2013, 62(25); D100 -
D108
• J Heart Lung Transplant 2012, 31;913–33
• Clinical Science 2014, 127; 65-76
• Can J Cardiol 2015, 31; 416-429

HFrEF PH Trials Trial Agent n
Inclusion
criteria Duration Endpoint Results
LEPHT1 Riociguat 201 LVEF ≤ 40%
mPAP ≥ 25 mmHg 16w
Change in
mPAP
No change
improved CI,
PVR, SVR
PITCH-
HF2 Tadalafil 2102
LVEF ≤ 40%
Documented PH
(echo or cath)
54m
Time to CV
death or HF
hops.
Terminated by
funding agency
Sil-HF3 Sildenafil 210
LVEF ≤ 40%
sPAP > 40 mmHg
echo
24w global ass.
and 6mwd recruiting
Corean4 Sildenafil 140
LVEF ≤ 40%
sPAP ≥ 40 mmHg
echo
12w 6 mwd recruiting
Melody-15 Macitentan 60
Combined pre-
post PH due to
LVD
12w safety Recruiting
1) Circulation. 2013;128:502-511 2) NCT01910389 3) Eur J Heart Fail (2013) 15, 119–122 4)NCT01913847 5)NCT02070991
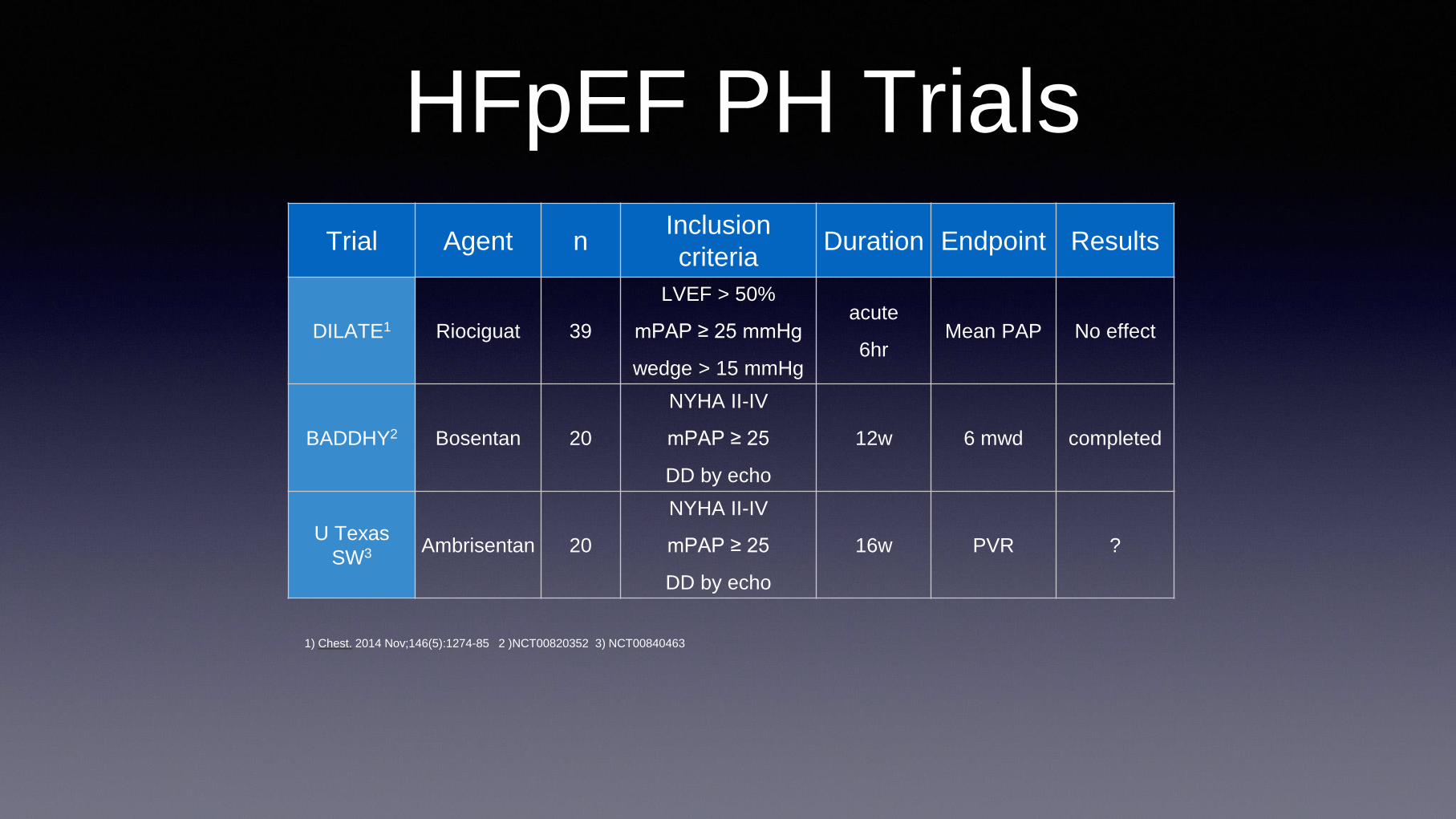
Trial Agent n Inclusion
criteria Duration Endpoint Results
DILATE1 Riociguat 39
LVEF > 50%
mPAP ≥ 25 mmHg
wedge > 15 mmHg
acute
6hr Mean PAP No effect
BADDHY2 Bosentan 20
NYHA II-IV
mPAP ≥ 25
DD by echo
12w 6 mwd completed
U Texas
SW3 Ambrisentan 20
NYHA II-IV
mPAP ≥ 25
DD by echo
16w PVR ?
HFpEF PH Trials
1) Chest. 2014 Nov;146(5):1274-85 2 )NCT00820352 3) NCT00840463
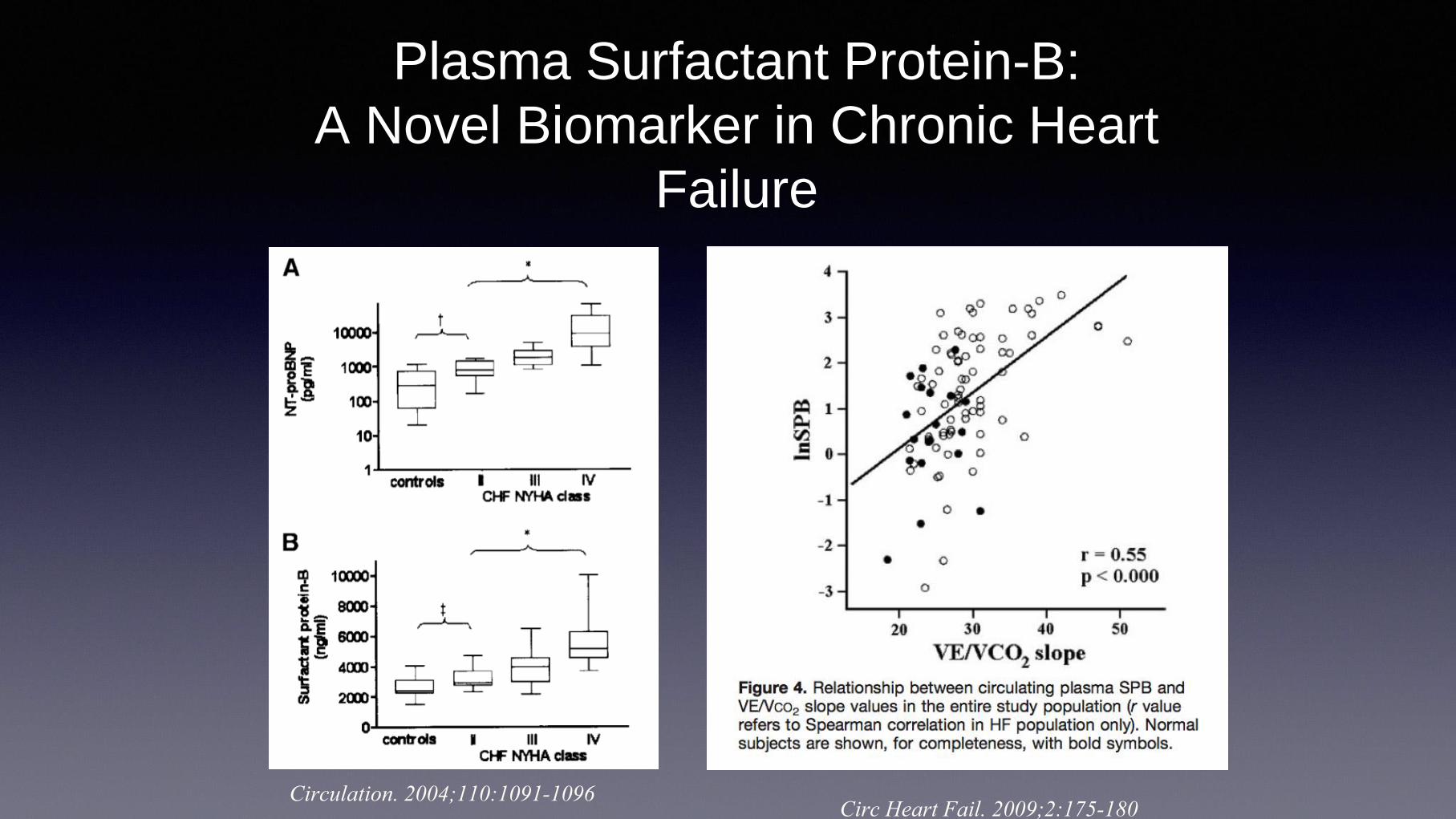
Plasma Surfactant Protein-B:
A Novel Biomarker in Chronic Heart
Failure
Circulation. 2004;110:1091-1096 Circ Heart Fail. 2009;2:175-180

Jpn Heart J 1984