Hearing Loss and Retinitis Pigmentosa: Usher Syndrome?€¦ · hearing loss, progressive visual...
5
Central Annals of Otolaryngology and Rhinology Cite this article: de Carvalho Tasso D, da Silva BLALA, Takara TFM, Sartorato EL, de Carvalho GM, et al. (2015) Hearing Loss and Retinitis Pigmentosa: Usher Syndrome? Ann Otolaryngol Rhinol 2(2): 1025. *Corresponding author Daniela de Carvalho Tasso, Division of External Eye Disease and Cornea Rua Augusto Tortorelli de Araujo, 94 -apto.111, Sao Paulo, Brazil; Tel 55-11 -974-896-165; Fax: 020-40-010; Email: Submitted: 01 December 2014 Accepted: 17 March 2015 Published: 19 March 2015 Copyright © 2015 Tasso et al. OPEN ACCESS Keywords • Usher syndrome • Genetic hearing loss • Retinitis pigmentosa Case Report Hearing Loss and Retinitis Pigmentosa: Usher Syndrome? Daniela de Carvalho Tasso 1 *, Bárbara Lucia Azevedo L. A. da Silva 2 , TammyFumiko M. Takara 2 , Edi Lúcia Sartorato 3 , Guilherme Machado de Carvalho 4 , Brazílio de Carvalho Tasso 2 and Carlos Eduardo Leite Arieta 5 1 Division of External Eye Disease and Cornea, University of São Paulo, Brazil 2 Department of Academic Medicine, University of São Paulo (USP), Brazil 3 Department of Medical Genetics, University of Campinas, Brazil 4 Department of Otolaryngology, Head and Neck State University of Campinas, Brazil 5 Department of Ophthalmology, Hospital of UNICAMP, Brazil Abstract Introduction: Usher Syndrome is a rare syndrome caused by an autosomal recessive genetic disorder and is the most common cause of blindness and deafness combined, representing more than 50% of cases. Objective: This article aims to review the literature on Usher syndrome along with the presentation of a clinical picture. Methods: Review of the medical literature in PubMed and SciELO / Lilacs, using the MeSH terms:”Usher syndrome”, “genetic hearing loss” and “retinitis pigmentosa”. Case report: A case presents a 37-year-old woman patient detected with Usher syndrome. She reported hearing and visual loss since childhood. The onset was with nyctalopia evolving to peripheral field deprivation in both eyes a few years ago. She underwent ophthalmologic examination with dynamic refraction, ocular applanation tonometry,retinography, fluoresce in angiography and computerized visual field, the electroretinography was requested but was not available in the service. Eye fundus biomicroscopy revealed mild temporal pallor of the optic disk, diffuse retinalblood vessel narrowing, retinal sparse hyperpigmentation. The patient uses hearing aids (HA) since adolescence and a audiometric test was performed good adaptation. No alterations were found in the search for mutations in the GJB2 gene and mitochondrial mutations A155G. Discussion: The diagnosis of Usher syndrome is difficult and genetic testing can support this evaluation. We believe that its early diagnosis can bring several benefits, as genetic counseling and better rehabilitation, reducing the damage caused by this syndrome, which has no direct treatment. Unfortunately there is no cure for the disease. Conclusion: This syndrome should be considered as a differential diagnosis in patients who have combined loss of visual acuity and hearing. INTRODUCTION Usher syndrome (USH) was first described in 1958 by von Graefe and established as a hereditary disease in 1914 by Charles Usher [1,2]. It is a syndrome caused by an autosomal recessive genetic disorder that presents with sensor neural hearing loss, progressive visual impairment resulted from retinitis pigmentosa, and in some cases vestibular disorders [3,4]. This syndrome is the most common cause of blindness and deafness combined, representing more than 50% of cases [1,5]. Affects 23,000 people worldwide [3], corresponding to 6% of congenitally deaf population [4]. Clinical classification is divided into 3 types according to the change in hearing. USH2 is the most common type accounting for 50% of cases [4]. Together the USH2 and USH1 undertake 90% of the cases [5]. The type 1 (USH1) manifests with severe congenital deafness and vestibular dysfunction and retinitis pigmentosa manifests in the first childhood or in the beginning of second decade of life [2-4]. Type 2 (USH2) initiate with hearing loss, moderate to severe, normal vestibular function and milder retinitis pigmentosa usually beginning in the second decade of life [2-4].
Transcript of Hearing Loss and Retinitis Pigmentosa: Usher Syndrome?€¦ · hearing loss, progressive visual...

Central Annals of Otolaryngology and Rhinology
Cite this article: de Carvalho Tasso D, da Silva BLALA, Takara TFM, Sartorato EL, de Carvalho GM, et al. (2015) Hearing Loss and Retinitis Pigmentosa: Usher Syndrome? Ann Otolaryngol Rhinol 2(2): 1025.
*Corresponding authorDaniela de Carvalho Tasso, Division of External Eye Disease and Cornea Rua Augusto Tortorelli de Araujo, 94 -apto.111, Sao Paulo, Brazil; Tel 55-11 -974-896-165; Fax: 020-40-010; Email:
Submitted: 01 December 2014
Accepted: 17 March 2015
Published: 19 March 2015
Copyright© 2015 Tasso et al.
OPEN ACCESS
Keywords•Usher syndrome•Genetic hearing loss•Retinitis pigmentosa
Case Report
Hearing Loss and Retinitis Pigmentosa: Usher Syndrome?Daniela de Carvalho Tasso1*, Bárbara Lucia Azevedo L. A. da Silva2, TammyFumiko M. Takara2, Edi Lúcia Sartorato3, Guilherme Machado de Carvalho4, Brazílio de Carvalho Tasso2 and Carlos Eduardo Leite Arieta5
1Division of External Eye Disease and Cornea, University of São Paulo, Brazil2Department of Academic Medicine, University of São Paulo (USP), Brazil3Department of Medical Genetics, University of Campinas, Brazil4Department of Otolaryngology, Head and Neck State University of Campinas, Brazil5Department of Ophthalmology, Hospital of UNICAMP, Brazil
Abstract
Introduction: Usher Syndrome is a rare syndrome caused by an autosomal recessive genetic disorder and is the most common cause of blindness and deafness combined, representing more than 50% of cases.
Objective: This article aims to review the literature on Usher syndrome along with the presentation of a clinical picture.
Methods: Review of the medical literature in PubMed and SciELO / Lilacs, using the MeSH terms:”Usher syndrome”, “genetic hearing loss” and “retinitis pigmentosa”.
Case report: A case presents a 37-year-old woman patient detected with Usher syndrome. She reported hearing and visual loss since childhood. The onset was with nyctalopia evolving to peripheral field deprivation in both eyes a few years ago. She underwent ophthalmologic examination with dynamic refraction, ocular applanation tonometry,retinography, fluoresce in angiography and computerized visual field, the electroretinography was requested but was not available in the service. Eye fundus biomicroscopy revealed mild temporal pallor of the optic disk, diffuse retinalblood vessel narrowing, retinal sparse hyperpigmentation. The patient uses hearing aids (HA) since adolescence and a audiometric test was performed good adaptation. No alterations were found in the search for mutations in the GJB2 gene and mitochondrial mutations A155G.
Discussion: The diagnosis of Usher syndrome is difficult and genetic testing can support this evaluation. We believe that its early diagnosis can bring several benefits, as genetic counseling and better rehabilitation, reducing the damage caused by this syndrome, which has no direct treatment. Unfortunately there is no cure for the disease.
Conclusion: This syndrome should be considered as a differential diagnosis in patients who have combined loss of visual acuity and hearing.
INTRODUCTIONUsher syndrome (USH) was first described in 1958 by
von Graefe and established as a hereditary disease in 1914 by Charles Usher [1,2]. It is a syndrome caused by an autosomal recessive genetic disorder that presents with sensor neural hearing loss, progressive visual impairment resulted from retinitis pigmentosa, and in some cases vestibular disorders [3,4]. This syndrome is the most common cause of blindness and deafness combined, representing more than 50% of cases [1,5]. Affects 23,000 people worldwide [3], corresponding to 6% of
congenitally deaf population [4]. Clinical classification is divided into 3 types according to the change in hearing. USH2 is the most common type accounting for 50% of cases [4]. Together the USH2 and USH1 undertake 90% of the cases [5].
The type 1 (USH1) manifests with severe congenital deafness and vestibular dysfunction and retinitis pigmentosa manifests in the first childhood or in the beginning of second decade of life [2-4]. Type 2 (USH2) initiate with hearing loss, moderate to severe, normal vestibular function and milder retinitis pigmentosa usually beginning in the second decade of life [2-4].

Central
Tasso et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1025 (2015) 2/5
Type 3 (USH3) is characterized by progressive damage to the hearing, variable vestibular dysfunction and the onset of Retinitis pigmentosa is variable [2-4]. At least nine genes have been identified and according to some authors, such as WILLEMS et al, 11 genes are related to this syndrome [3,5,6]. Classification of US can also be based on molecular genetic studies and it is divided according to the chromosome and the gene affected. The genetic subtypes are IB, IC, ID, IE, IF, IG, IIA, IIB, IIC and III [2]. This article aims to review the literature on Usher syndrome along with the presentation of a clinical picture.
METHODSThe realization of this article was completed after a review
of the medical literature in PubMed and SciELO / Lilacs, using the following terms (MeSH terms):”Usher syndrome”, “genetic hearing loss” and “retinitis pigmentosa”.
Furthermore, we describe a case of a patient with Retinitis pigmentosa and sensori neural hearing loss, with profound clinical research laboratorial for discussion and illustration.This case report complies with the rules of the ethics committee of the institution.
CASE REPORTPatient, female, 37 years old, white, complaints of hearing and
visual acuity loss since childhood, both slowly and progressive. Clinical history of hypothyroidism, nonsmoker and non-alcoholic, no family history of eye or ear, nose and throat (ENT) diseases and parents are not consanguineous.
The patient reported onset with nyctalopia, evolving with decreased visual acuity and loss of peripheral field in both eyes (BE) a few years ago. Despite the optical prescription was hindering their daily activities. At baseline ocular examination showed visual acuity (VA) corrected 0,40 (BE) according to Snelling chart, with examination of dynamic refraction: right eye(RE) flat, -1, 00CD x 10° and left eye (LE) +1.25 SD -2.25 CDx 160°, and best corrected VA of 20/40 0,50 (+1) and 20/40 0,50 (+1), respectively. Ocular applanation tonometry: 16 mmHg
(RE) and 13 mmHg (LE). Slit- Lamp Biomicroscopy showed no abnormalities Binocular indirect ophthalmoscopy, similar in BE: attached retina, mild temporal pallor of the optic disc, sparse spicules hyper pigmentation (resembling osteoclasts), and vascular attenuation.
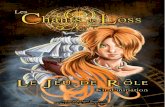
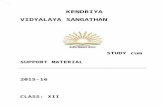
The hearing loss is present since childhood with slow progression. She uses Personal Sound Amplification Product (HA) since adolescence with good adaptation. The audiogram shows a lowering of tone thresholds at all frequencies, with percentages ranging between 40 and 75 dB. It an be noted a good functional hearing outcomes when in use the bilateral hearing aids, as evidenced by free field audiometry (Figure 1).The clinical laboratory tests (metabolic, rheumatologic and serology) are normal. No alterations were found in the search for mutations in the GJB2 gene and mitochondrial mutations like A155G.Ushersyndrome genes havenotbeenscreened, andthisis a bias to confirm the genteic diagnosis. New optical correction was prescribed and the patient was referred for multidisciplinary treatment. The computerized eye campimetry (visual field) showed (annular scotoma paracentral, with central scotoma worst in the RE (Figure 2). After two years without fundoscopy alterations, a mild opacity in lens in the LE was diagnosed. Was performed a retinography and angiography of retina and a new perimetry (Figure 3,4).
The patient completed training in the Visual Rehabilitation Center, receiving orientation and being adapted to the use of a cane. There was no indication for physiotherapy. The patient showed no interest in learning Braille. Psychologically she was managing to cope well with their psycho-emotional complaints and had no demand for social service at the time. The occupational therapist observed improvement in the use of residual vision remains in Ophthalmology and Otorhinolaryngology clinical follow evaluation.
DISCUSSIONThe diagnosis of Usher syndrome is difficult because
patients can show a wide range of characteristics, both clinic
Figure 1 Illustration shows the patient audiometry in both ears using hearing aids.

Central
Tasso et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1025 (2015) 3/5
Figure 2 Visual field – campimetry (right and left eye): Reduced sensitivity of the fovea compared to the normal pattern. Total deviation shows adjacent points with diffuse reduction of sensitivity. Pattern deviation: such a intense reduction of sensitivity that shows no alterations. MD and PSD indices outside the normal limit tests with good reliability. Conclusion: the island of central vision in both eyes.
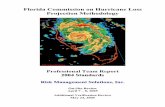
Figure 3 Monochromatic fundus (red free), followed by angiofluoresceina: hyper fluorescence background, default transmission RPE (window defect) and the corresponding areas hypo fluorescence pigmentary spicules.

Central
Tasso et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1025 (2015) 4/5
Figure 4 Retina angiography of the right and left eye: arteriolar narrowing, slightly pallor optic disc and bone spurs. Fundus features of Retinitis pigmentosa.
and genetic. Initially, should be discarded differential diagnoses such as Ahlstrom syndrome, Bardet-Biedl syndrome and Mohr-Tranebjaerg syndrome beside others [1].
Some proteins responsible for the visual and hearing impairment were identified as Usherin, Cadherin 23, Harmonin, Protocadherin 15 and Clarin 1 [5]. The usherin protein is required for maintenance of photoreceptor cells of the retina and the development of cochlear hair cells [4].
The Usher syndrome accounts rage for 10% to 30%of the entire population with retinitis pigmentosa (RP) [4,6]. The retinitis pigmentosa is a degenerative retinal disease that starts in the periphery and progresses to the macula and fovea, firstly affecting the rods and after the cones [6,7].
The intra retinal pigment deposition leads to apoptosis, as a likely consequence, of retinal cells, reducing the thickness of the retina’s external nuclear layer [7]. Symptoms include night blindness and progressive visual field loss, leading to tunnel vision and then to a clinic blindness [3,7].
The RP may predispose to myopia and sub capsular cataract [1]. The clinical findings are fundoscopy with “bones spicules” and attenuation of retinal vessels; reduction or absence of “a” and “b” waves of the electro retinogram (ERG); reduction of the visual field [7]. Sensorineural deafness and vestibular alteration of USH are caused by changes in the morphogenesis and stability of stereocilia, a mechano sensitive organelle. Knowledge of the causes of this disease is utmost importance to define the commonalities between the sensorineural process and the deprivation of hearing and vision [5].
Genetic testing can aid in the diagnosis however may not be conclusive. Although nine genes were isolated, they were not all of the genes responsible for the syndrome encountered, and so in some cases there is a genetic alteration [1]. Currently, 3 loci (USH2A, USH2C, USH2D) and three genes USH2A (USH2A), GPR98 (USH2C) and DFNB31 (USH2D)
were identified related to Usher syndrome type 2 [1,3]. Ushersyndrome genes havenotbeenscreened, andthisis a bias to confirmthegenteicdiagnosis.
We believe that its early diagnosis can bring several benefits, as genetic counseling and early rehabilitation, reducing the damage caused by this syndrome.There is no cureyet for thedisease, but different treatment modalities may be present in the near future as the use ofantioxidants, hormone growth factors, stemcells, retinal prostheses and genetic treatments. In Europe a new treatment to Retinosis pigmentosa was recently approved with a retinal prosthesis, The Retinal Prosthesis ArgusII, System, to blind patients, there is also the controversial use of oral vitamin A in high doses (in cases where there is only genetic diagnosis, as it may adversely der some mutations in) [2,8].
CONCLUSIONThe Usher syndrome should always be considered as a
differential diagnosis in patients who have combined loss of visual acuity and hearing, Due to the significant prevalence in this population and the large negative impact on quality of life for those patients.
REFERENCES1. Millán JM, Aller E, Jaijo T, Blanco-Kelly F, Gimenez-Pardo A, Ayuso C.
An update on the genetics of usher syndrome. J Ophthalmol. 2011; 2011: 417217.
2. Alessandro Martini. Genes, Hearing, and Deafness from Molecular Biology to Clinical Practice. London: Informa Healthcare.2007; 56-59.
3. Yang J, Wang L, Song H, Sokolov M. Current understanding of usher syndrome type II. Front Biosci (Landmark Ed). 2012; 17: 1165-1183.
4. López G, Gelvez NY, Tamayo M. [Mutational frequencies in usherin (USH2A gene) in 26 Colombian individuals with Usher syndrome type II]. Biomedica. 2011; 31: 82-90.

Central
Tasso et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1025 (2015) 5/5
de Carvalho Tasso D, da Silva BLALA, Takara TFM, Sartorato EL, de Carvalho GM, et al. (2015) Hearing Loss and Retinitis Pigmentosa: Usher Syndrome? Ann Otolaryngol Rhinol 2(2): 1025.
Cite this article
5. Willems PJ. Genetic hearing loss. New York, Basel: Marcel Dekker, Inc. 2004; 65-71.
6. Audo I, Bujakowska K, Mohand-Said S, Tronche S, Lancelot ME, Antonio A, et al. A novel DFNB31 mutation associated with Usher type 2 syndrome showing variable degrees of auditory loss in a consanguineous Portuguese family. Mol Vis. 2011; 17: 1598–1606.
7. Ferrari S, Di Iorio E, Barbaro V, Ponzin D, Sorrentino FS, Parmeggiani F.
Retinitis pigmentosa: genes and disease mechanisms. Curr Genomics. 2011; 12: 238-249.
8. Ahuja AK, Dorn JD, Caspi A, McMahon MJ, Dagnelie G, Dacruz L, et al. Blind subjects implanted with the Argus II retinal prosthesis are able to improve performance in a spatial-motor task. Br J Ophthalmol. 2011; 95: 539-543.