ESSAIS CLINIQUES EN AFRIQUE: BONNES … CLINIQUES EN AFRIQUE: BONNES PRATIQUES Ogobara K. Doumbo,...
46
ESSAIS CLINIQUES EN ESSAIS CLINIQUES EN AFRIQUE: BONNES PRATIQUES AFRIQUE: BONNES PRATIQUES Ogobara K. Doumbo, MD, PhD Malaria Research and Training Center Département d’Epidémiologie des Affections Parasitaires Faculté de Médecine, de Pharmacie et d’Odontostomatologie du Mali Université de Bamako, Mali
Transcript of ESSAIS CLINIQUES EN AFRIQUE: BONNES … CLINIQUES EN AFRIQUE: BONNES PRATIQUES Ogobara K. Doumbo,...
ESSAIS CLINIQUES ENESSAIS CLINIQUES ENAFRIQUE: BONNES PRATIQUESAFRIQUE: BONNES PRATIQUES
Ogobara K. Doumbo, MD, PhDMalaria Research and Training Center
Département d’Epidémiologie des Affections ParasitairesFaculté de Médecine, de Pharmacie et
d’Odontostomatologie du MaliUniversité de Bamako, Mali

Les essais cliniques en Afriquedoivent répondre aux
“ICH and FDA requirements”• ICH are from consensus: US, Europe, Japan,
WHO, Canada, Scandinavia• Studies realized under ICH/GCP should be
accepted in all ICH region for expediteexamination of new drug dossiers
• ICH GCP have been accepted as FDA guidelines.
• En Afrique l’essai clinique impliquenon seulement le volontaire, maistout un village+++
Malaria = 3 sunamiMalaria = 3 sunamiEn Afrique par anEn Afrique par an> 1,000,000 Décès> 1,000,000 Décès

Durant cette présentation, au moins 80enfants vont mourrir de Plasmodiumfalciparum malaria en Afrique.

Enfant africain est en contactavec les antigènes plasmodiaux in
utero === Impact sur sonDevéloppement immunologique?
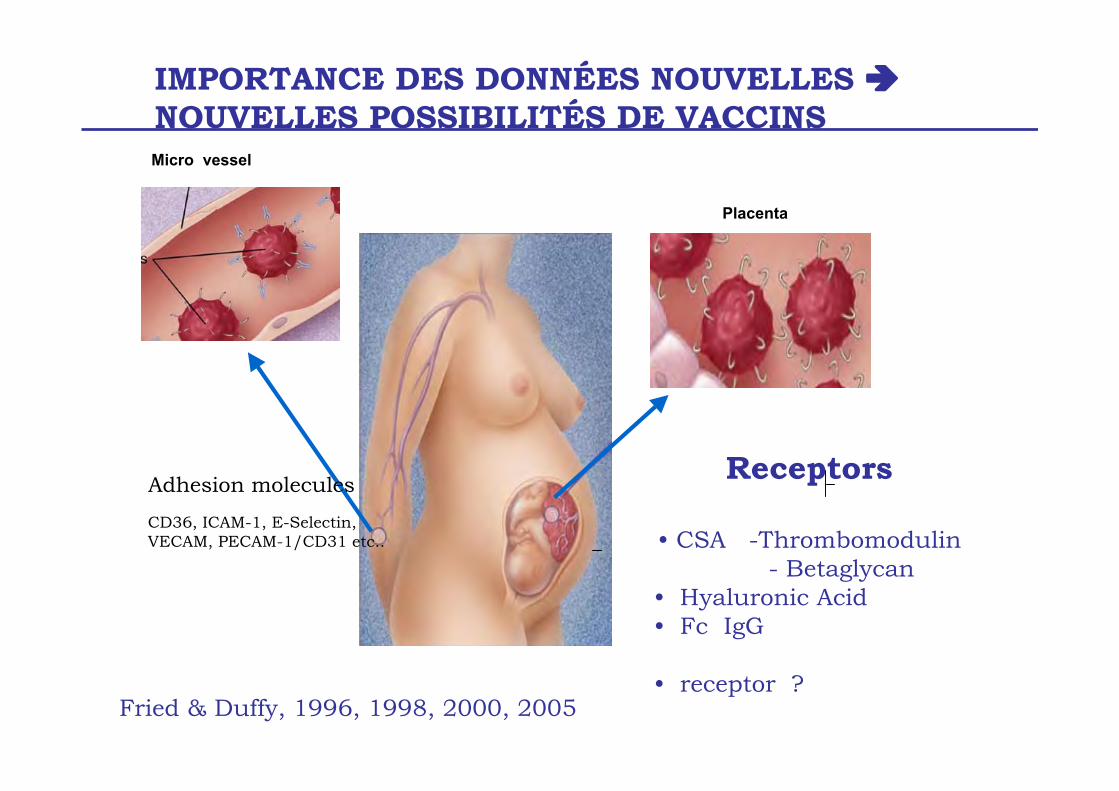
IMPORTANCE DES DONNÉES NOUVELLES NOUVELLES POSSIBILITÉS DE VACCINS
Receptors
• CSA -Thrombomodulin - Betaglycan• Hyaluronic Acid• Fc IgG
• receptor ?
Placenta
Micro vessel
Adhesion molecules
CD36, ICAM-1, E-Selectin, VECAM, PECAM-1/CD31 etc..
Fried & Duffy, 1996, 1998, 2000, 2005
IMPACT SCOLAIRE DU PALUDISMEET CRÉATIVITÉ DE LA NATION
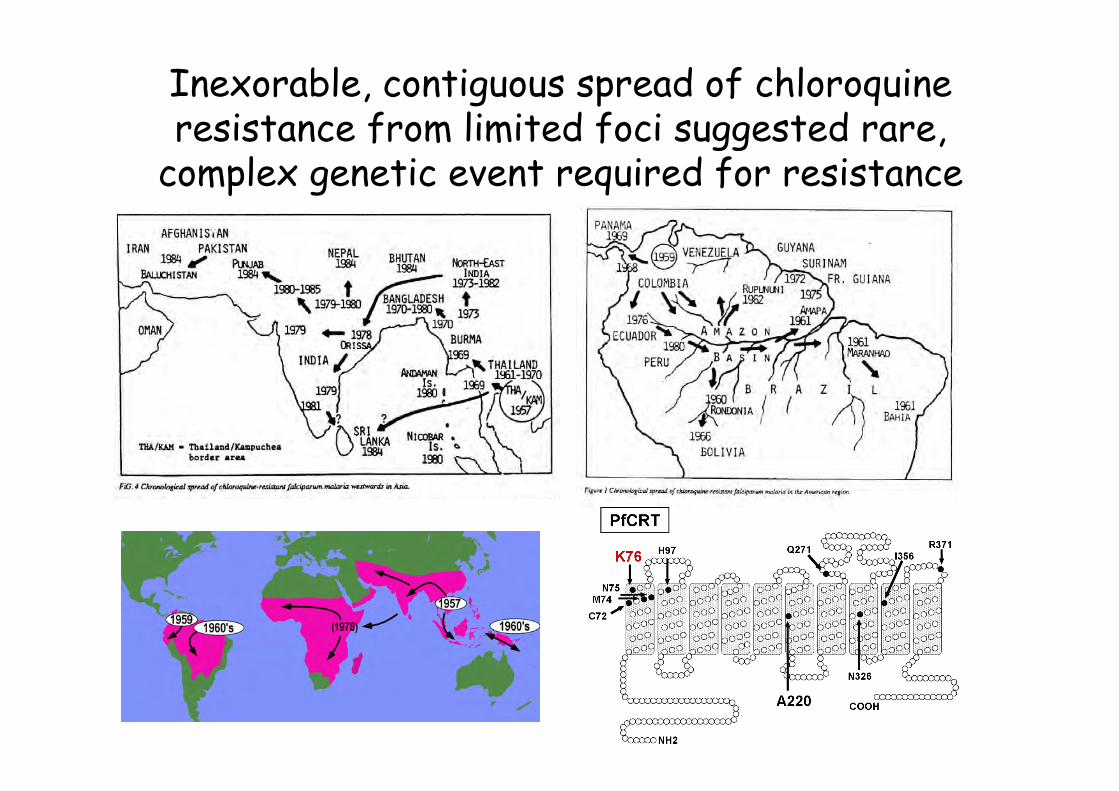
Inexorable, contiguous spread of chloroquineresistance from limited foci suggested rare,
complex genetic event required for resistance
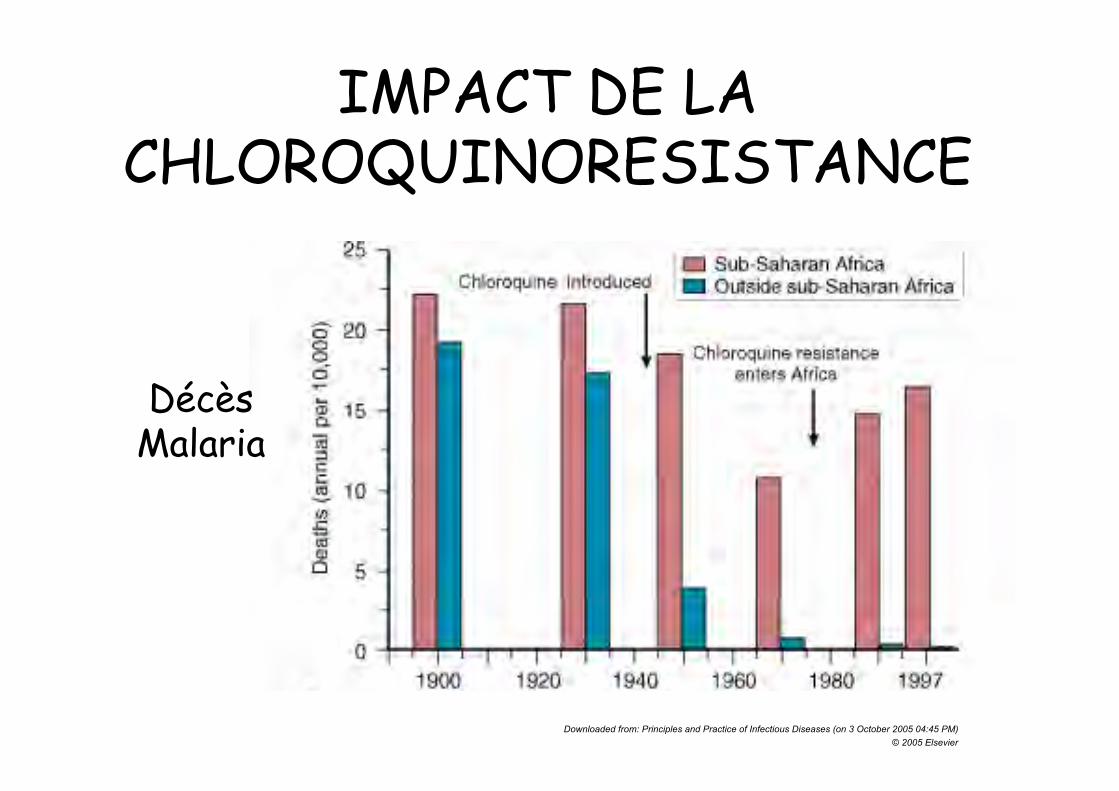
Downloaded from: Principles and Practice of Infectious Diseases (on 3 October 2005 04:45 PM)© 2005 Elsevier
IMPACT DE LACHLOROQUINORESISTANCE
DécèsMalaria

Dangers de la Résistance àl’Artemisinine
http://www.who.int/malaria/docs/drugresistance/ReportThaiCam.pdf

COMPETENCES REQUISES POURLES EQUIPES AFRICAINES
• 1] ECRITURE DES PROTOLES D’ESSAISCLINIQUES DE PHASE I, II, III
• 2] ECRITURE DES SOPs• 3] PLANIFICATION ET GESTION DU
PROTOCOLE,• 4] GESTION DES DONNÉES = RAPPORTS
SMC, DSMB,• 5] GESTION DES AEs, SAEs.
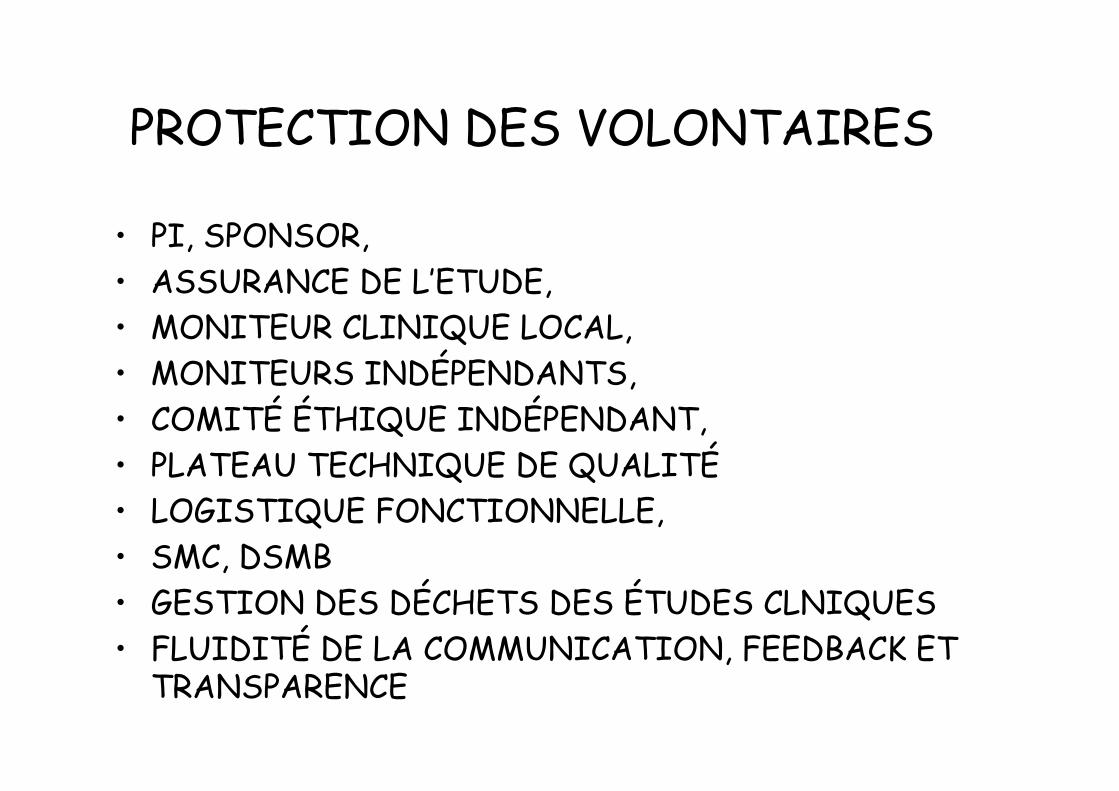
PROTECTION DES VOLONTAIRES
• PI, SPONSOR,• ASSURANCE DE L’ETUDE,• MONITEUR CLINIQUE LOCAL,• MONITEURS INDÉPENDANTS,• COMITÉ ÉTHIQUE INDÉPENDANT,• PLATEAU TECHNIQUE DE QUALITÉ• LOGISTIQUE FONCTIONNELLE,• SMC, DSMB• GESTION DES DÉCHETS DES ÉTUDES CLNIQUES• FLUIDITÉ DE LA COMMUNICATION, FEEDBACK ET
TRANSPARENCE
Malaria vaccines: History• 1920s-1940s Whole parasite vaccines protect
canaries, ducks, chickens, turkeys• 1960s Irradiated sporozoites protect mice• 1970s Irradiated sporozoites protect man
(Clyde, et.al. University of Maryland)
• 1980s Recombinant DNA– Heterologous expression systems
• Viruses, bacteria, yeast transformed with Plasmodia DNA– Sub-unit peptide vaccines
• 1990s DNA, viral vector vaccines• 2000s Whole parasite vaccines

Sites d’Action des vaccinsantipaludiques
Bloquant latransmission
Pre-érythrocytaire
Stadessanguins

Cibles Parasitaires desCandidats Vaccins

Malaria vaccines: Targets and goals
•Reduce transmission
•Prevent disease inAfrican children,pregnant women•Improve efficacy of“leaky” pre-erythrocytic vaccines
•Prevent infection intravelers (sterileimmunity)•Eradicate malaria?
Goal ExamplesStage•Circumsporozoite protein (CSP)•Liver stage antigen-1 (LSA-1)•TRAP/SPSS•LSA-3•Whole, live, attenuatedsporozoites
Pre-erythrocytic
•Pfs25, othersSexual stage
•Merozoite surface proteins(MSP-1, 2, 4, 5)•Apical membrane antigen-1(AMA-1)•Erythrocyte binding antigens(EBA-175 and others)•PfEMP1
Blood stage
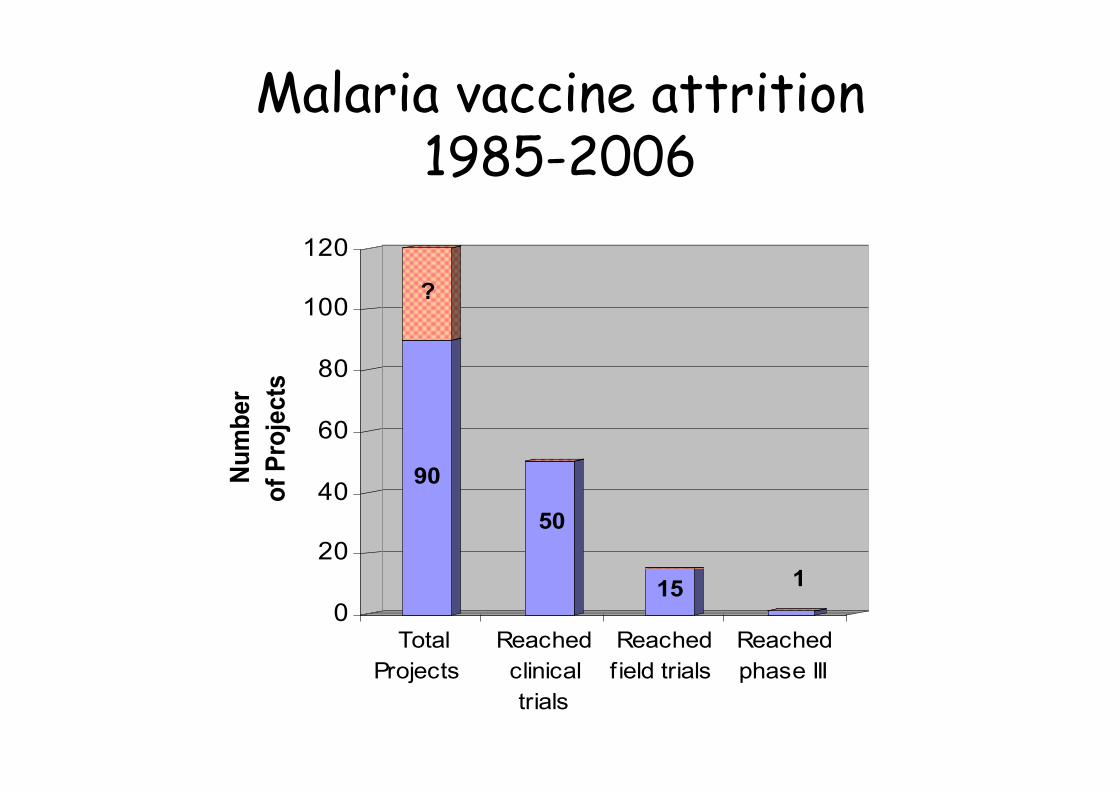
Malaria vaccine attrition1985-2006
90
?
50
15 1
0
20
40
60
80
100
120N
um
ber
of
Pro
jec
ts
Total
Projects
Reached
clinical
trials
Reached
field trials
Reached
phase III
The role of vaccines inmalaria control/eradication
• Administer with standard pediatric vaccines• Use in combination with other tools:
– Insecticide-Treated Nets (ITN)– Intermittent Preventive Treatment (IPT)– Indoor Residual Spraying (IRS)– Artemisinin-based Combination Therapy (ACT)
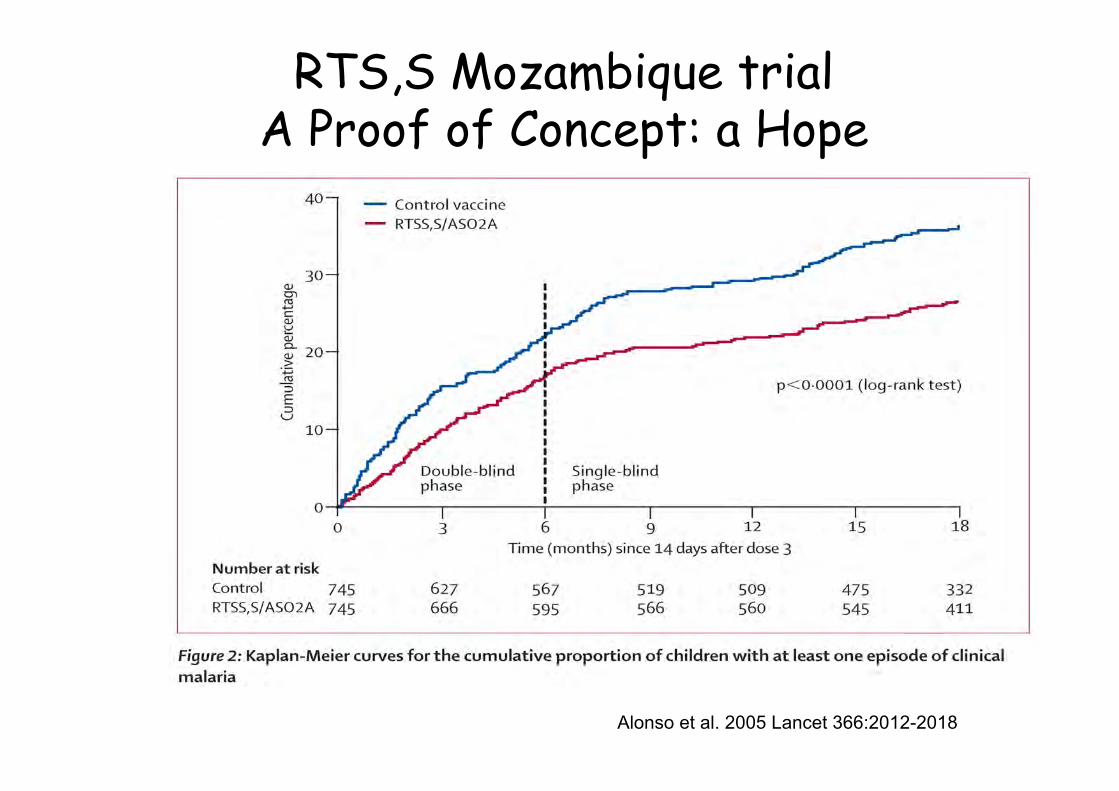
RTS,S Mozambique trialA Proof of Concept: a Hope
Alonso et al. 2005 Lancet 366:2012-2018
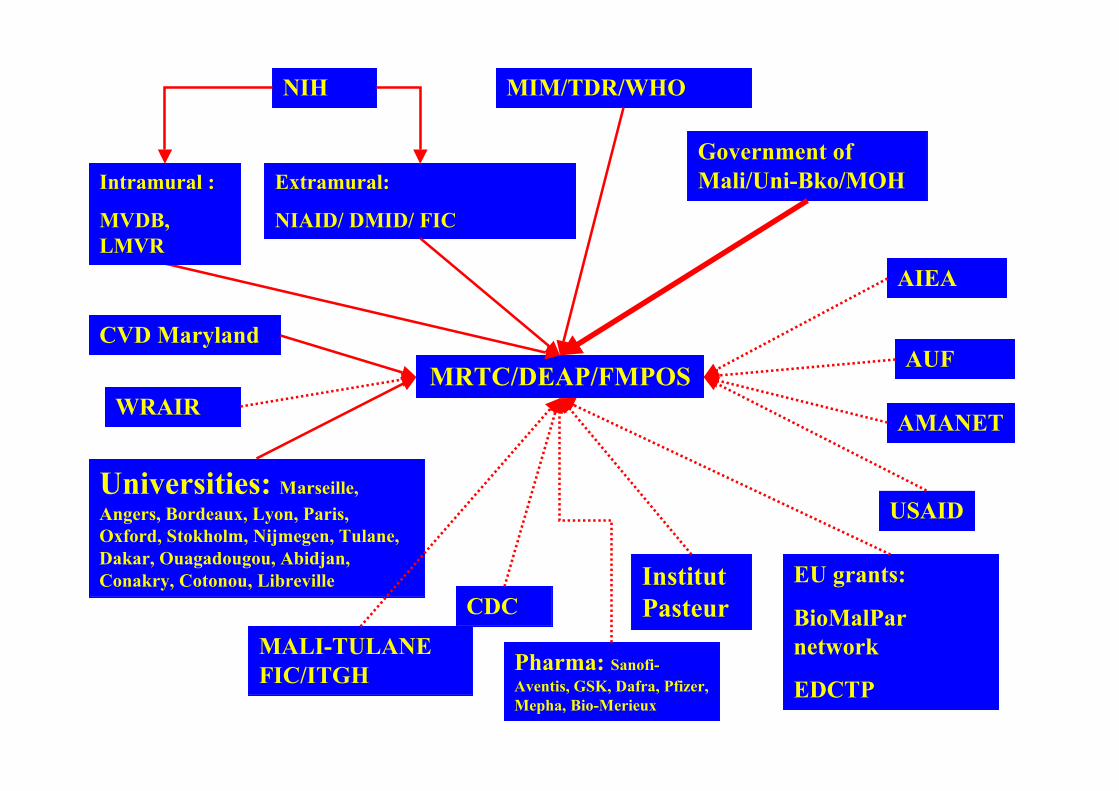
NIH
Extramural:
NIAID/ DMID/ FIC
MRTC/DEAP/FMPOSWRAIR
CDC
USAID
Government ofMali/Uni-Bko/MOH
EU grants:
BioMalParnetwork
EDCTP
CVD MarylandAUF
AMANET
Universities: Marseille,Angers, Bordeaux, Lyon, Paris,Oxford, Stokholm, Nijmegen, Tulane,Dakar, Ouagadougou, Abidjan,Conakry, Cotonou, Libreville
AIEA
InstitutPasteur
MALI-TULANEFIC/ITGH Pharma: Sanofi-
Aventis, GSK, Dafra, Pfizer,Mepha, Bio-Merieux
MIM/TDR/WHO
Intramural :
MVDB,LMVR
IMPORTANCE DE LA SELECTIONDES SITES DE TERRAIN
• 1] VISION A LONG TERME,• 2] STABILITÉ POLITIQUE ET COHÉSION SOCIO-
CULTURELLE DE LA POPULATION,• 3] VALEUR SOCIAL DU SITE POUE LA
COMMUNAUTÉ,• 4] FACILITÉ PERMISSION COMMUNAUTAIRE,• 5] PROCÉDURES ÉTABLIES DE CONCENTEMENT
ÉCLAIRÉ• 6] ETABLIR UN DIALOGUE ET UNE CONFIANCE
MUTUELLE

Bandiagara
DonéguébougouSotuba
Bancoumana
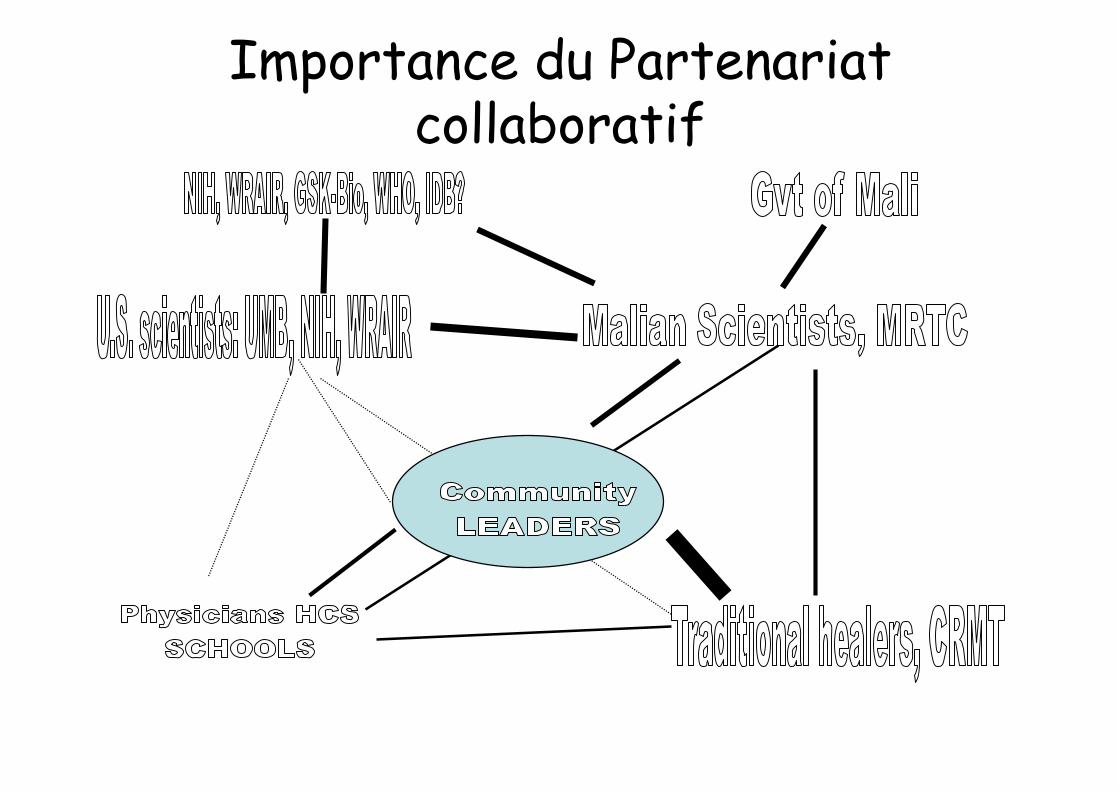
Importance du Partenariatcollaboratif
IMPORTANCE DE LA FORMATIONINITIALE DES EQUIPES CLINIQUES
• CERTIFICATION EN BONNES PRATIQUESCLINIQUES,
• CERTIFICATION EN BONNES PRATIQUESDE LABORATOIRE,
• CERTIFICATION EN ETHIC
• === STANDARDS ICH

QUALITÉ ICH DES SITESESSAIS CLINIQUES AU MALI

Qualité des Capacités deGestion des SAEs
• Equipements pour les Urgence,• Disponibilité de Kits de prise en charge• Disponibilité d’Urgentistes Compétents• Disponibilité d’une possibilité
d’Evacuation en cas de.
Dr Issaka Soulama, Molecular Biologist from Burkina Faso in training at the MRTC

IMPORTANCE DE LA CAPACITÉ DE FORMATION CONTINUE DES ÉQUIPES Workshop on analysis of Molecular Biology Data And Data ManagementFrom 11 African countries
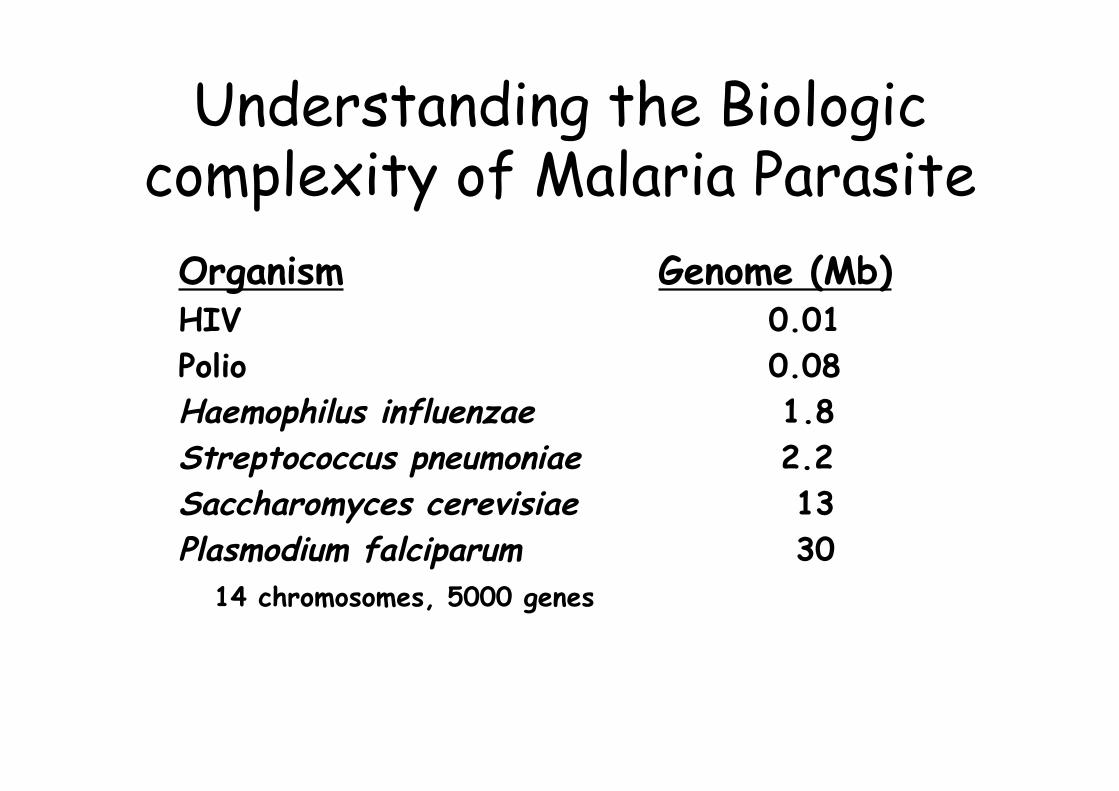
Understanding the Biologiccomplexity of Malaria Parasite
Organism Genome (Mb)HIV 0.01Polio 0.08Haemophilus influenzae 1.8Streptococcus pneumoniae 2.2Saccharomyces cerevisiae 13Plasmodium falciparum 30
14 chromosomes, 5000 genes

RTS,S sustained efficacy(Alonso et al., Lancet 2005, Aponte et al., Lancet 2007)
• Highest antibody titers in younger children• Anti-CSP antibodies associated with protection in infants
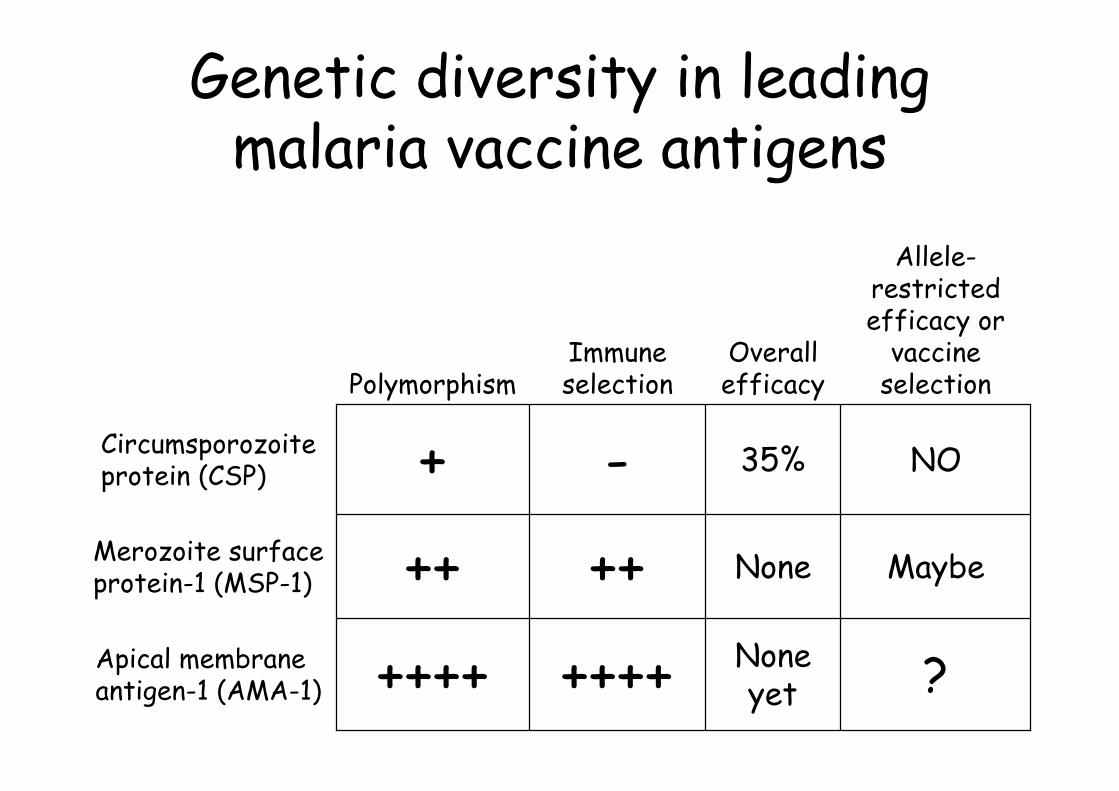
Genetic diversity in leadingmalaria vaccine antigens
?Noneyet++++++++Apical membrane
antigen-1 (AMA-1)
MaybeNone++++Merozoite surfaceprotein-1 (MSP-1)
NO35%-+Circumsporozoiteprotein (CSP)
Allele-restrictedefficacy or
vaccineselection
Overallefficacy
ImmuneselectionPolymorphism
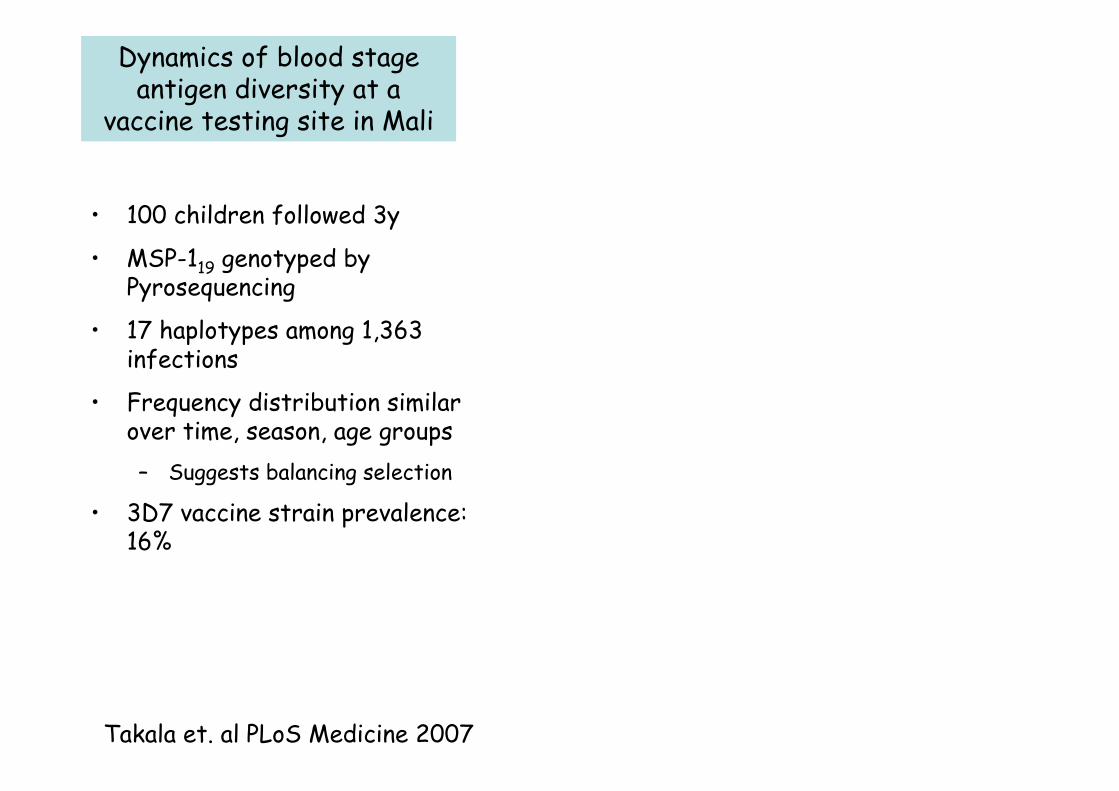
Takala et. al PLoS Medicine 2007
• 100 children followed 3y
• MSP-119 genotyped byPyrosequencing
• 17 haplotypes among 1,363infections
• Frequency distribution similarover time, season, age groups– Suggests balancing selection
• 3D7 vaccine strain prevalence:16%
Dynamics of blood stageantigen diversity at a
vaccine testing site in Mali
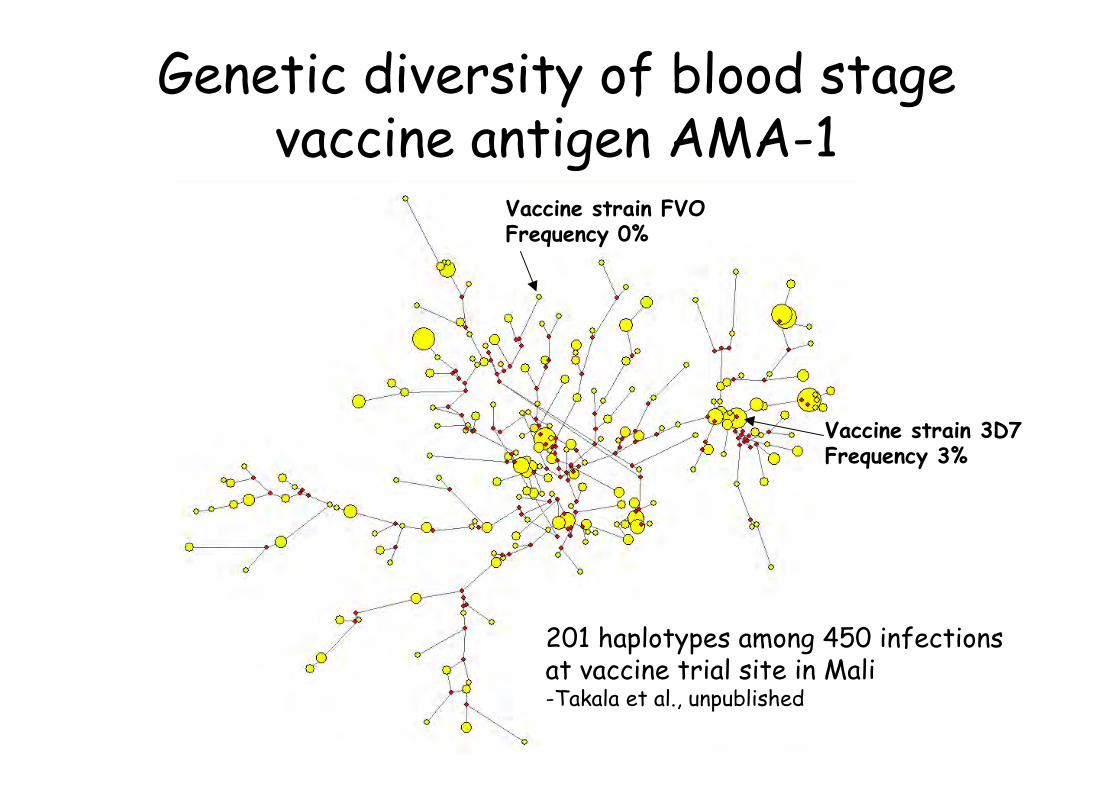
Genetic diversity of blood stagevaccine antigen AMA-1
Vaccine strain 3D7Frequency 3%
Vaccine strain FVOFrequency 0%
201 haplotypes among 450 infectionsat vaccine trial site in Mali-Takala et al., unpublished
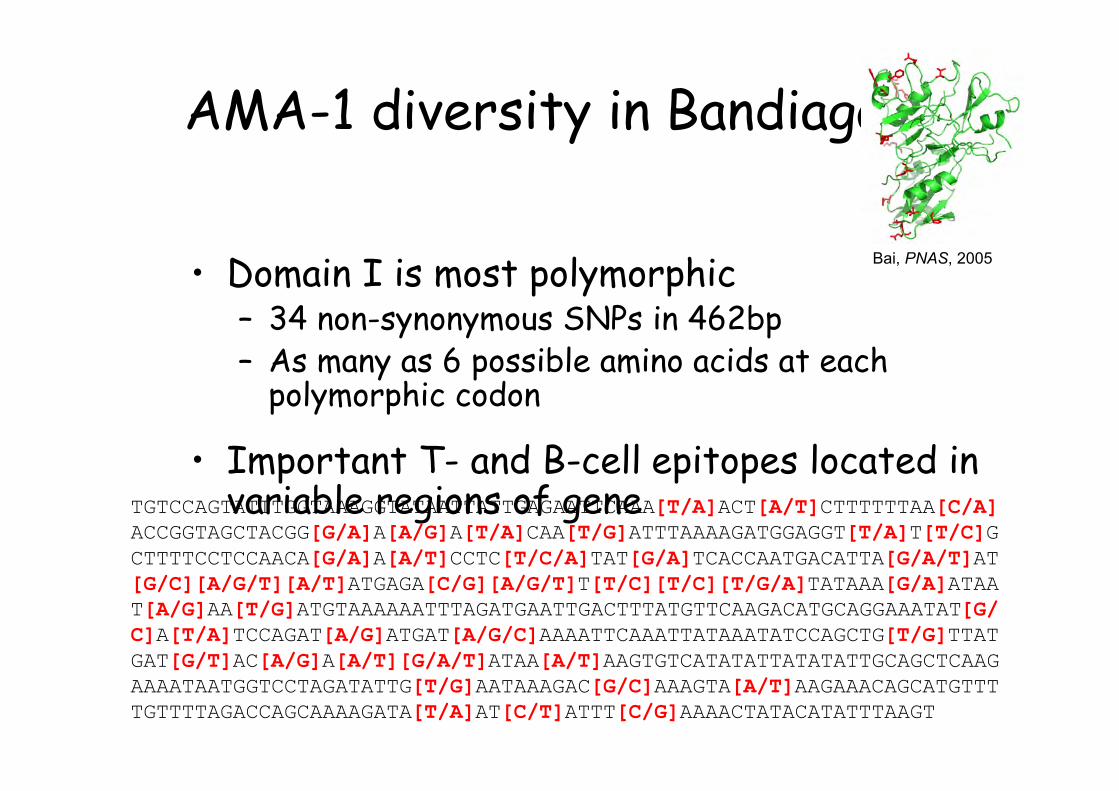
AMA-1 diversity in Bandiagara
• Domain I is most polymorphic– 34 non-synonymous SNPs in 462bp– As many as 6 possible amino acids at each
polymorphic codon
• Important T- and B-cell epitopes located invariable regions of geneTGTCCAGTATTTGGTAAAGGTATAATTATTGAGAATTCAAA[T/A]ACT[A/T]CTTTTTTAA[C/A]
ACCGGTAGCTACGG[G/A]A[A/G]A[T/A]CAA[T/G]ATTTAAAAGATGGAGGT[T/A]T[T/C]GCTTTTCCTCCAACA[G/A]A[A/T]CCTC[T/C/A]TAT[G/A]TCACCAATGACATTA[G/A/T]AT[G/C][A/G/T][A/T]ATGAGA[C/G][A/G/T]T[T/C][T/C][T/G/A]TATAAA[G/A]ATAAT[A/G]AA[T/G]ATGTAAAAAATTTAGATGAATTGACTTTATGTTCAAGACATGCAGGAAATAT[G/C]A[T/A]TCCAGAT[A/G]ATGAT[A/G/C]AAAATTCAAATTATAAATATCCAGCTG[T/G]TTATGAT[G/T]AC[A/G]A[A/T][G/A/T]ATAA[A/T]AAGTGTCATATATTATATATTGCAGCTCAAGAAAATAATGGTCCTAGATATTG[T/G]AATAAAGAC[G/C]AAAGTA[A/T]AAGAAACAGCATGTTTTGTTTTAGACCAGCAAAAGATA[T/A]AT[C/T]ATTT[C/G]AAAACTATACATATTTAAGT
Bai, PNAS, 2005
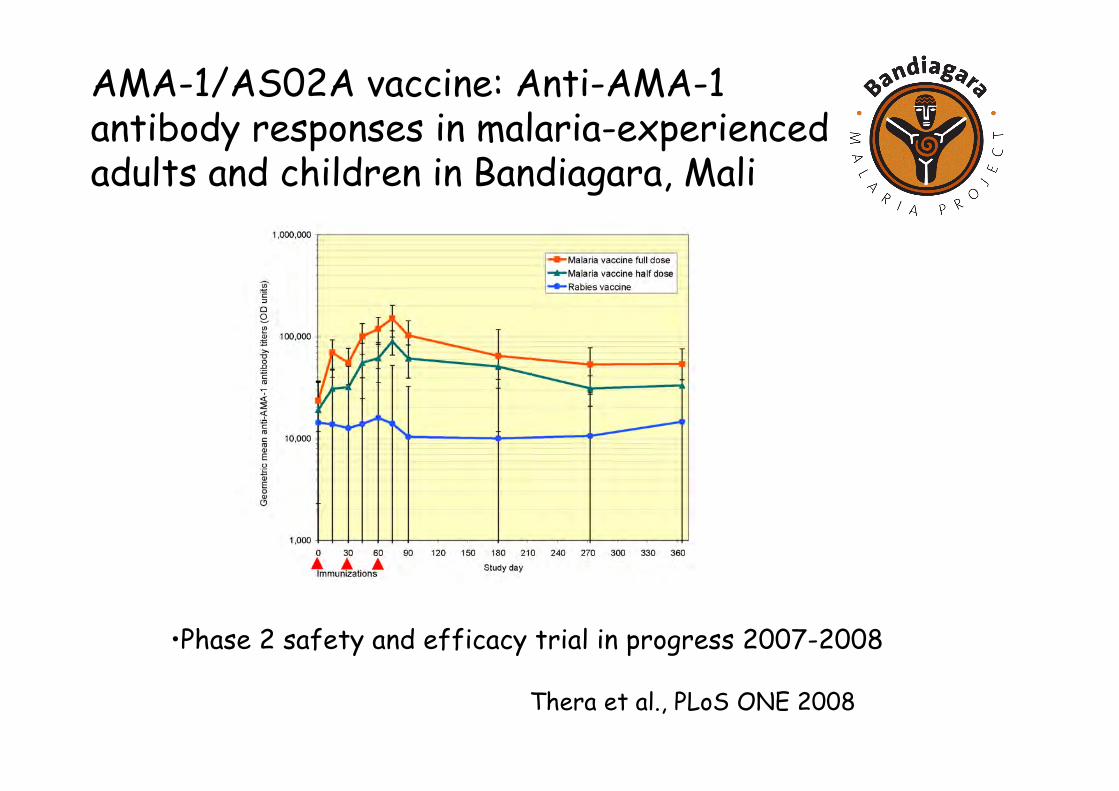
AMA-1/AS02A vaccine: Anti-AMA-1antibody responses in malaria-experiencedadults and children in Bandiagara, Mali
•Phase 2 safety and efficacy trial in progress 2007-2008
Thera et al., PLoS ONE 2008
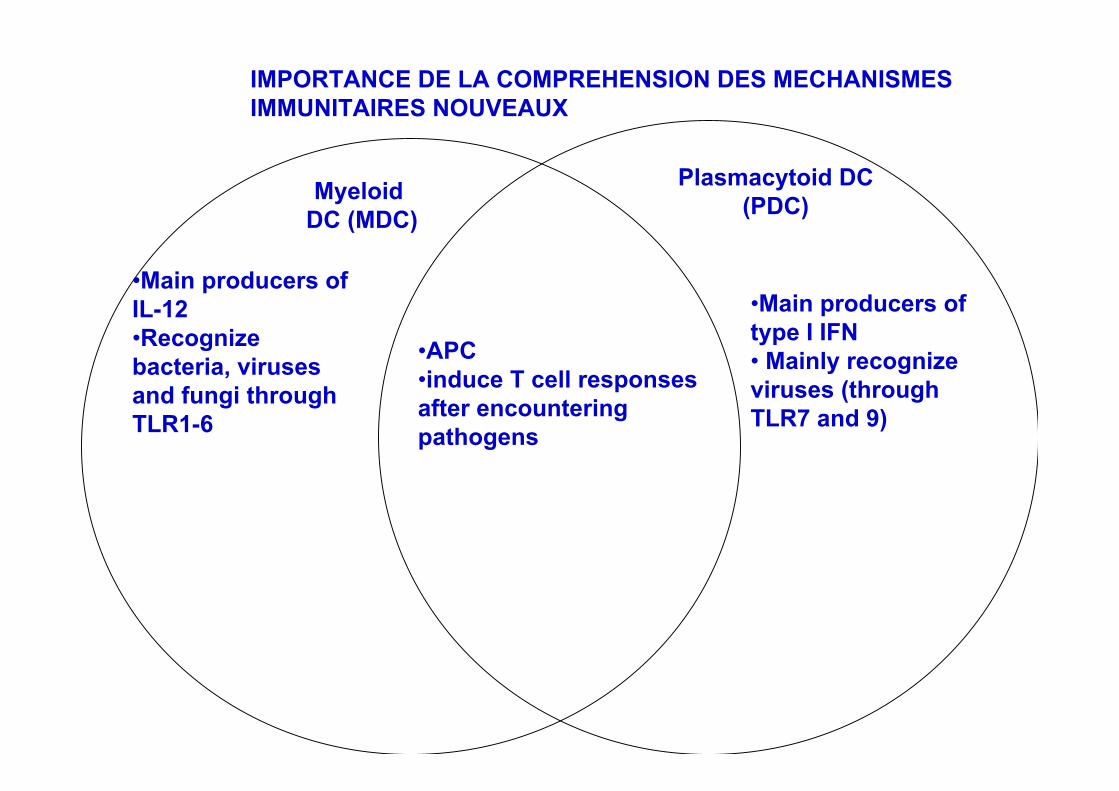
•APC•induce T cell responsesafter encounteringpathogens
•Main producers oftype I IFN• Mainly recognizeviruses (throughTLR7 and 9)
•Main producers ofIL-12•Recognizebacteria, virusesand fungi throughTLR1-6
IMPORTANCE DE LA COMPREHENSION DES MECHANISMES IMMUNITAIRES NOUVEAUX
Plasmacytoid DC(PDC)Myeloid
DC (MDC)
IMPACT SUR LA SANTÉ DELA POPULATION
• 1] AMELIORATION EN GCP, GLP, ETHIQUE DESEQUIPES LOCALES,
• 2] FORMATION CONTINUE “BY DOING”• 3] DEVELOPPEMENT DES FACILITÉS DE SOINS
DANS LES SITES ET ENVIRONNANTS• 4]ACCÈS DE LA POPULATION AUX MEILLEURS
SOINS• 5] VISIBILITÉ DE L’IMPACT SUR L’ETAT DE
SANTÉ DE LA POPULATION.


POINTS FAIBLES EN AFRIQUE
• 1] INSUFFISANCE DES SYSTEMES DEREGLEMENTATION ET DE CONTROL DE QUALITÉ– L’OMS ET D’AUTRES PARTENAIRES SONT ENTRAIN DE
COMBLER CETTE LACUNE,
• 2] INSUFFISANCE DE LA COORDINATION ENTRELES PAYS– UTILSATION DES ORGANISATIONS SOUS RÉGIONALES
COMME L’OOAS,• L’EPINEUX PROBLEME DE LA CHAINE DE FROID,• ARCHIVAGE DES DOSSIERS CLINIQUES?
INFORMATISATION: CONNECTIVITÉ ENAFRIQUE
• 1-NIVEAU CENTRAL• 2-INTRANET• 3-SITES DE TERRAINS ET
PARTENAIRES• 4-ACCES AU NTIC• 5-GESTION ET PARTAGE DE
L’INFORMATION SUR LES ESSAISCLINIQUES == TRANSPARENCE

CONNECTIVITÉ AU MRTC ET SITES
Bamako
Bamako NionoSatellite link
Bandiagara
Mopti
Satellite
Packet Radio
NIH Hub SITE
Sikasso
Sotuba
Donéguebougou
BancoumanaBanambani
Koro
300 km
350 km
670 km
60 km
600 km
25 km
32 km
75 km
512kbps 128 kbps
512 kbps
EQUIPE CLINIQUE

EQUIPE INTERNATIONALE D’ESSAICLINIQUE A BANDIAGARA
• University of Bamako:– Ogobara K. Doumbo– Mahamadou A. Thera– Dapa A. Diallo– Alassane Dicko– Issaka Sagara– Drissa Coulibaly– Abdoulaye Koné– Ando Guindo– Mohammed B. Niambélé– Moussa Sogoba– Mounirou Baby– Karim Traoré– Modibo Daou– Issa Diarra– Yacouba Cissoko– Amagana Dolo– Hamar Alassane Traoré
• University of Maryland:– Christopher V. Plowe– Kirsten E. Lyke– Aric Gregson– Karen Kotloff– Robert Edelman– Linda L. Rosendorf
• MVDB/NIAID:– David Diemert– Louis H. Miller
• DMID/NIAID:– Abdi Naficy
• WRAIR:– D. Gray Heppner
– Christian F. Ockenhouse– Kurt Schaecher– Kent E. Kester– Jeff Lyon– Evelina Angov
• USAID:– Carter Diggs– Lorraine Soisson
• GSK:– Rip Ballou– Amanda Leach– Alfred Tiono