Décisions thérapeutiques en présence de premières molaires permanentes délabrées chez les...
19
Summary The aim of this exhaustive descriptive epidemiological study was to determine the clinical approach to be adopted by practi- tioners specializing exclusively in pediatric odontology and by orthodontists when confronted with decayed molars in children and adolescents. Material and method: A questionnaire was sent out to all cor- responding practitioners (n = 2076). Six questions related to treatment decisions taken when faced with decayed permanent first molars (unfavorable short or middle-term prognosis) in patients needing, or not, orthodontic care. The Chi 2 test was used to compare responses. Results: Thirty-eight per cent of pedodontists (n = 38) and 12.5% (n = 246) of orthodontists nswered the questionnaire. Faced with a permanent first molar with an unfavorable middle-term prog- nosis, 75.7% needed criteria to help them reach their treatment decision. In decreasing order of importance, these criteria were: presence of the third molar, patient motivation, inter-arch rela- tionship, patient’s oral hygiene, facial type, anterior jaw-teeth R esum e Cette etude epid emiologique descriptive exhaustive avait pour objectif de d eterminer l’attitude clinique des praticiens ayant un exercice exclusif en odontologie p ediatrique et des orthodontistes dans le cas de molaires d elabr ees chez des enfants et des adolescents. Population et m ethode : Un questionnaire a et e envoy e a`l’en- semble des praticiens correspondants (n = 2076) : six ques- tions ferm ees correspondaient aux prises de d ecisions th era- peutiques adopt ees face a` une premi ere molaire permanente d elabr ee (pronostic r eserv e a` court ou moyen terme) chez des patients ayant ou non des besoins orthodontiques. Le test de Chi 2 a permis de comparer les r eponses. R esultats : Trente-huit pour cent des p edodontistes (n = 38) et 12,5 % (n = 246) des orthodontistes avaient r epondu a` notre questionnaire. Face a` une premi ere molaire permanente de pronostic r eserv e a` moyen terme, 75,7 % des praticiens avaient besoin, pour finaliser leur r eflexion th erapeutique, de crit eres qui etaient, par ordre d ecroissant d’importance, la pr esence de la troisi eme molaire, la motivation du patient, la relation inter- Original article Article original Ó 2012 CEO Published by / E ´ dite ´ par Elsevier Masson SAS All rights reserved / Tous droits re ´serve ´s Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiry D ecisions th erapeutiques en pr esence de premi eres molaires permanentes d elabr ees chez les sujets jeunes : enqu ^ ete descriptive Millewa SAYAGH a , Armelle MANIERE-EZVAN ac , Cindy VERNET b , Mich ele MULLER-BOLLA b,* a D epartement orthop edie dentofaciale, UFR odontologie, universit e de Nice Sophia-Antipolis, 24, avenue Diables-Bleus, 06357 Nice, France b D epartement sant e publique, UFR odontologie, universit e de Nice Sophia-Antipolis, 24, avenue Diables-Bleus, 06357 Nice, France c Laboratoire LOM, UFR odontologie, universit e de Nice Sophia-Antipolis, 24, avenue Diables- Bleus, 06357 Nice, France Available online: 21 August 2012 / Disponible en ligne : 21 aou ˆ t 2012 * Correspondence and reprints / Correspondance et tir es a ` part : Mich ele MULLER-BOLLA, D epartement sant e publique, UFR odontologie, universit e de Nice Sophia-Antipolis, 24, avenue Diables-Bleus, 06357 Nice, France. e-mail address / Adresse e-mail : [email protected] 318 International Orthodontics 2012 ; 10 : 318-336 doi:10.1016/j.ortho.2012.06.001
Transcript of Décisions thérapeutiques en présence de premières molaires permanentes délabrées chez les...

Original articleArticle original
� 2012 CEOPublished by / Edite par Elsevier Masson SAS
All rights reserved / Tous droits reserves
Therapeutic decisions in the presence ofdecayed permanent first molars in youngsubjects: A descriptive inquiry
D�ecisions th�erapeutiques en pr�esence depremi�eres molaires permanentes d�elabr�ees chezles sujets jeunes : enquete descriptive
Millewa SAYAGHa, Armelle MANIERE-EZVANac, Cindy VERNETb,Mich�ele MULLER-BOLLAb,*
aD�epartement orthop�edie dentofaciale, UFR odontologie, universit�e de Nice Sophia-Antipolis,24, avenue Diables-Bleus, 06357 Nice, FrancebD�epartement sant�e publique, UFR odontologie, universit�e deNice Sophia-Antipolis, 24, avenueDiables-Bleus, 06357 Nice, FrancecLaboratoire LOM, UFR odontologie, universit�e de Nice Sophia-Antipolis, 24, avenue Diables-Bleus, 06357 Nice, France
Available online: 21 August 2012 / Disponible en ligne : 21 aout 2012
SummaryThe aim of this exhaustive descriptive epidemiological studywas to determine the clinical approach to be adopted by practi-tioners specializing exclusively in pediatric odontology and byorthodontists when confronted with decayed molars in childrenand adolescents.Material and method: A questionnaire was sent out to all cor-responding practitioners (n = 2076). Six questions related totreatment decisions taken when faced with decayed permanentfirst molars (unfavorable short or middle-term prognosis) inpatients needing, or not, orthodontic care. The Chi2 test wasused to compare responses.
Results: Thirty-eight per cent of pedodontists (n = 38) and 12.5%(n = 246) of orthodontists nswered the questionnaire. Faced witha permanent first molar with an unfavorable middle-term prog-nosis, 75.7% needed criteria to help them reach their treatmentdecision. In decreasing order of importance, these criteria were:presence of the third molar, patient motivation, inter-arch rela-tionship, patient’s oral hygiene, facial type, anterior jaw-teeth
318
R�esum�e
Cette �etude �epid�emiologique descriptive exhaustive avaitpour objectif de d�eterminer l’attitude clinique des praticiensayant un exercice exclusif en odontologie p�ediatrique et desorthodontistes dans le cas de molaires d�elabr�ees chez desenfants et des adolescents.Population et m�ethode : Un questionnaire a �et�e envoy�e a l’en-semble des praticiens correspondants (n = 2076) : six ques-tions ferm�ees correspondaient aux prises de d�ecisions th�era-peutiques adopt�ees face a une premi�ere molaire permanented�elabr�ee (pronostic r�eserv�e a court ou moyen terme) chezdes patients ayant ou non des besoins orthodontiques. Le testde Chi2 a permis de comparer les r�eponses.R�esultats : Trente-huit pour cent des p�edodontistes (n = 38) et12,5 % (n = 246) des orthodontistes avaient r�epondu a notrequestionnaire. Face a une premi�ere molaire permanente depronostic r�eserv�e amoyen terme, 75,7 %despraticiens avaientbesoin, pour finaliser leur r�eflexion th�erapeutique, de crit�eresqui �etaient, par ordre d�ecroissant d’importance, la pr�esence dela troisi�eme molaire, la motivation du patient, la relation inter-
*Correspondence and reprints / Correspondance et tir�es a part :
Mich�ele MULLER-BOLLA, D�epartement sant�e publique, UFR odontologie, universit�ede Nice Sophia-Antipolis, 24, avenue Diables-Bleus, 06357 Nice, France.e-mail address / Adresse e-mail : [email protected]
International Orthodontics 2012 ; 10 : 318-336doi:10.1016/j.ortho.2012.06.001

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
discrepancy and the number of molars to be extracted. Faced witha permanent first molar requiring extraction and when orthodon-tic treatment was not required, 31.7% of practitioners decided toclose the maxillary space immediately as opposed to 13.4% whoclosed the space at the mandible. In the presence of a singledecayed first molar, 68.7% of practitioners did not extract theantagonist or contralateral first molars.
Conclusion: These treatment decisions were not always unani-mous and call for a combined approach between dental surgeonand orthodontist.� 2012 CEO. Published by Elsevier Masson SAS. All rightsreserved
Key-words
·First permanent molar.
·Extraction. ·Orthodontic treatment.The permanent first molar, judged by Edward H. Angle to bethe keystone to occlusion, is the permanent tooth most affectedby caries in children and adolescents [1]. Furthermore, theincreased prevalence of molar-incisor hypomineralization(MIH), involving a systemic defect in enamel structure, makesaffected teeth more prone to caries. Of these, at least onepermanent first molar, and sometimes all four, is always car-ious, with varying degrees of severity, as well as one or severalpermanent incisors [2,3]. In permanent molars, in the leastsevere cases, the enamel is soft, porous, chalky and veryfragile, giving rise to rapid and severe decay of the affectedpermanent first molars, often in contrast with an absence ofcaries in the temporary teeth. Frequently, the prognosis ofthese teeth is compromised in the more or less short term.Sometimes, extraction can be envisaged on account of theproblems involved in restoration or periodontal complications,and even more so in the presence of malocclusion [3–5]. In themost severe cases, extraction should be mandatory. Given theage of these patients, the opinion of a specialist shouldbe sought in order to make the most suitable therapeuticchoice taking into consideration the different factors we haveattempted to identify and prioritize. The aim of this descriptiveepidemiological study was thus to determine which clinicalapproach should be adopted by practitioners specializingexclusively in pediatric odontology and by orthodontists inchildren and adolescents exhibiting decayed molars.Material and method
This descriptive epidemiological study was an exhaustivetransverse inquiry.
International Orthodontics 2012 ; 10 : 318-336
arcade, l’hygi�ene du patient, la typologie, la DDM ant�erieure etle nombre de molaires a extraire. Face a une premi�ere molairepermanente condamn�ee et en l’absence de besoin orthodon-tique, 31,7 % des praticiens d�ecidaient d’embl�ee de fermerl’espace au maxillaire alors qu’a la mandibule, ils �etaient13,4 %. En pr�esence d’une seule premi�ere molaire d�elabr�ee,68,7 % des praticiens n’extrayaient pas de premi�ere(s) molaire(s) permanente(s) antagoniste(s) ou controlat�erale(s).Conclusion : Ces d�ecisions th�erapeutiques qui ne faisaientpas toujours l’unanimit�e doivent etre le fruit d’une r�eflexioncommune entre le chirurgien dentiste et les orthodontistes.� 2012 CEO. Edite par Elsevier Masson SAS. Tous droitsreserves
Mots-cl�es
·Premi�ere molaire permanente.
·Extraction.
·Traitement orthodontique.La premi�ere molaire permanente, consid�er�ee comme la cl�e del’occlusion par Edward H. Angle est la dent permanente la plusaffect�ee par lamaladie carieuse chez l’enfant et l’adolescent [1].Par ailleurs, l’augmentation de la pr�evalence des hypo-min�eralisations incisives-molaires (MIH), �equivalentes a und�efaut de structure de l’�email d’origine syst�emique, rend plussensibles a la carie les dents affect�ees. Celles-ci int�eressenttoujours au moins une premi�ere molaire permanente et parfoisles quatre avec un degr�e de s�ev�erit�e souvent variable, ainsiqu’une ou plusieurs incisives permanentes [2,3]. Au niveaudes molaires permanentes, l’�email mou, poreux, crayeux dansles cas les moins s�ev�eres, est tr�es fragile. Il est a l’origine d’unrapide et s�ev�ere d�elabrement des premi�eres molaires perma-nentes affect�ees, qui contraste souvent avec l’absence de carieau niveau des dents temporaires. Ce d�elabrement peut etre telque le pronostic des dents concern�ees s’en trouve compromisa plus ou moins court terme. Ainsi leur extraction peut parfoisetre envisag�ee du fait des difficult�es de restauration ou decomplications parodontales, et ce d’autant plus qu’il existeune malocclusion [3–5]. Dans les cas les plus s�ev�eres, elledoit etre de r�egle. En raison de l’age des patients, l’avis d’unsp�ecialiste doit alors etre recherch�e afin de retenir la meilleuresolution th�erapeutique tenant compte des diff�erents facteursque nous avons voulu identifier et hi�erarchiser. Cette �etude�epid�emiologique descriptive avait donc pour objectif ded�eterminer l’attitude clinique des praticiens ayant un exerciceexclusif en odontologie p�ediatrique et des orthodontistes dans lecas demolaires d�elabr�ees chez des enfants et des adolescents.
Population et m�ethode
Cette �etude �epid�emiologique descriptive �etait une enquetetransversale exhaustive.
319

Millewa SAYAGH et al.
Study population
All orthodontic specialists in France (n = 1976, figures for2008) and all practitioners specializing exclusively in pediat-ric odontology in France were asked to complete a writtenquestionnaire. As practitioners traditionally known as pedo-dontists are not officially recognized in France, these werecontacted via the College of teachers of pediatric odontology(n = 100, in 2010).
Questionnaire
The questionnaire was pretested on 20 practising specialistsbefore being sent out by e-mail to the members of the collegesof teachers of pediatric odontology and dentofacial orthope-dics. It was also addressed by mail to independent practi-tioners and to salary-earning practitioners in non-teachinghospital medical centers via the SOF-GAC society. Answerswere to be returned by traditional mail or to a speciallydeigned web site at the Nice, France, Faculty of Odontology.In addition to a few administrative data, the questionnaireasked practitioners six questions in the results section regard-ing their treatment choices in relation to one or severaldecayed upper or lower permanent first molars in a settingwhere orthodontic treatment might be required. Answers wereclosed responses. The administrative data (gender, year ofqualification, type of practice, department in which they prac-tised) helped avoid duplicate questionnaires. Incompletequestionnaires were eliminated.
Statistical analyses
Qualifying variables were described in percentages. Meansand standard deviations were indicated in cases involvingqualifying variables. The Chi2 test, or the Fisher exact testwhen the conditions of application of the previous test were notobserved, was used to compare different qualitative variableswith one another. The significance threshold was set at 0.05.
Results
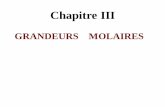
Following elimination of 39 incomplete questionnaires, 38pedodontists (38% of the members enrolled at the COLEP)and 246 orthodontists (12.45%) responded to the question-naire (P < 0.001). The latter were representative of thenational population in terms of their geographical distributioncorresponding to five national telephone (Telecom) regions(fig. 1). They represented, respectively, 12.3, 10.7, 12.2,14.6 and 10.5% of orthodontists in Telecom zones 1, 2, 3, 4and 5 (P = 0.506). Mean age of exclusive orthodontists
320
Population �etudi�ee
Tous les sp�ecialistes orthodontistes exercant en France(n = 1976, chiffres 2008) et tous les praticiens ayant un exer-cice exclusif en odontologie p�ediatrique sur notre territoire ont�et�e interrog�es par l’interm�ediaire d’un questionnaire �ecrit. Lespraticiens classiquement d�esign�es sous le nom dep�edodontistes n’ayant pas une reconnaissance officielle, ilsont �et�e contact�es par l’interm�ediaire du Coll�ege des enseig-nants en odontologie p�ediatrique (COLEP) (n = 100, en 2010).
Questionnaire
Il a �et�e pr�ealablement test�e sur 20 praticiens sp�ecialis�es avantd’etre adress�e par mail aux membres des coll�eges desenseignants en odontologie p�ediatrique ou en orthop�edie den-tofaciale. Il a �et�e �egalement exp�edi�e par courrier aux prati-ciens lib�eraux ou salari�es d’un �etablissement de soins nonhospitalo-universitaire, par l’interm�ediaire de la Soci�et�eSOF-GAC. Les r�eponses devaient se faire par envoi postalou sur un site de l’UFR d’odontologie de Nice pr�evu a ceteffet. En compl�ement de quelques renseignements d’ordreadministratif, ce questionnaire interrogeait le praticien, parl’interm�ediaire de six questions d�etaill�ees dans le para-graphe des r�esultats, sur ses choix th�erapeutiques li�esa une ou plusieurs premi�eres molaires permanentesd�elabr�ees, maxillaires ou mandibulaires, dans un contextede besoin �eventuel en traitement orthodontique. Lesr�eponses �etaient ferm�ees. Les renseignements d’ordreadministratif (sexe, ann�ee d’obtention du diplome, moded’exercice, d�epartement d’exercice) permettaient d’�eliminerles questionnaires adress�es deux fois. Les questionnairesincomplets ont �et�e �elimin�es.
Analyses statistiques
Les variables qualificatives �etaient d�ecrites sous forme depourcentages. Les moyennes et �ecart-types �etaient indiqu�esdans le cas des variables quantitatives. Le test de Chi2, ou letest exact de Fisher lorsque les conditions d’application dupr�ec�edent n’�etaient pas respect�ees, ont �et�e utilis�es pourcomparer diff�erentes variables qualitatives. Le seuil de signi-ficativit�e a �et�e fix�e a 0,05.
R�esultats
Apr�es �elimination de 39 questionnaires incomplets, 38p�edodontistes (38 % des sujets inscrits au COLEP) et 246orthodontistes (12,45 %) ont r�epondu au questionnaire(p < 0.001). Ces derniers �etaient repr�esentatifs de lad�emographie nationale en r�ef�erence a leur r�epartition dansles diff�erentes zones g�eographiques correspondant aux cinqzones T�el�ecom (fig. 1). Ils repr�esentaient respectivement12,3, 10,7, 12,2, 14,6 et 10,5 % des orthodontistes des zonesT�el�ecom 1, 2, 3, 4 et 5 (p = 0,506). L’age moyen des
International Orthodontics 2012 ; 10 : 318-336

[(Fig._1)TD$FIG]
Fig. 1: Map of the five France-Telecom regions: 01: Paris-Ile deFrance; 02: north-west; 03: north-east; 04: south-east; 05: south-west.Fig. 1 : Carte des cinq r�egions France T�el�ecom : 01 : Paris Ile-de-
France ; 02 : nord-ouest ; 03 : nord-est ; 04 : sud-est ; 05 : sud-
ouest.
Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
(47.26 W 11.01 years) was similar to that of the pedodontists(45.03 W 11.10 years) (P = 0.246), as were their other admin-istrative characteristics (Table I).
Frequency of clinical situations involving decayedmolars in everyday practice
Although the prevalence of decayed teeth could not be esti-mated on account of the study design, their approximate fre-quency was investigated using a first question with threepossible answers (at least once per week, once per month,once every 6 months). In 58.5% of cases (n = 166), decayedteeth were encountered in the daily practice of the respondingpractitioners less than once every 6 months. More rarely, in14.8% of cases (n = 42), they were observed once per week.These observations were unrelated to the Telecom zonewhile cases of decayed molars were observed most frequentlyamong pediatric odontologists and in medical institutions(P < 0.001) (Table II).
International Orthodontics 2012 ; 10 : 318-336
orthodontistes exclusifs (47,26 W 11,01 ans) ne diff�erait pasde celui des p�edodontistes (45,03 W 11,10 ans) (p = 0,246),au meme titre que leurs autres caract�eristiques administra-tives (Tableau I).
Fr�equence des situations cliniques avec molairesd�elabr�ees dans la pratique quotidienne
Si la pr�evalence des molaires d�elabr�ees ne pouvait pas etrepr�ecis�ement �evalu�ee du fait du plan de l’�etude, leur fr�equenceapproximative a �et�e recherch�ee par l’interm�ediaire d’une pre-mi�ere question avec trois possibilit�es de r�eponses (au moinsune fois par semaine, une fois par mois, une fois par semes-tre). Dans 58,5 % des cas (n = 166), elles �etaient mises en�evidence dans l’exercice des praticiens interrog�es moinsd’une fois par semestre. Plus rarement, dans 14,8 % descas (n = 42), elles �etaient mises en �evidence une fois parsemaine. Ces observations �etaient ind�ependantes de la zoneT�el�ecom alors que les cas de molaires d�elabr�ees �etaient leplus souvent observ�es chez les odontologistes p�ediatriques etdans les �etablissements de soins (p < 0.001) (Tableau II).
321

Table IIFrequency with which decayed molars were observedaccording to specialty, type of activity and Telecom zone.
Tableau IIFr�equence d’observation des molaires d�elabr�ees en fonctiondes sp�ecialit�es, modes d’exercice et zones T�el�ecom.
Characteristics/Caract�eristiques Once/week/1 fois/semainen
Once/month/1 fois/moisn
< once/quarter/< 1 fois/semestren
P
Specialties/Sp�ecialit�es 0.001/0,001
Exclusive orthodontists/Orthodontistes exclusifs
14 67 165
Pediatric odontologists/Odontologistes p�ediatriques
28 9 1
Type of practice/Exercice 0.001/0,001
Private/Lib�eral 12 46 142
Public health, teaching hospital/�Etablissement de soins, CHU
30 30 24
Telecom Zones/Zones T�el�ecom 0.466/0,466
1 12 13 37
2 6 7 26
3 5 19 28
4 15 25 58
5 4 12 17
Table IDistribution of responding exclusive orthodontists andpediatric odontologists according to gender and Telecom zone.
Tableau IR�epartition des orthodontistes exclusifs et odontologistesp�ediatriques ayant r�epondu au questionnaire, en fonction deszones T�el�ecom et du sexe.
Characteristics/Caract�eristiques Exclusive orthodontists/Orthodontistes exclusifsn
Pediatric odontologists/Odontologistes p�ediatriquesn
Practice Telecom zone/Zone T�el�ecom
1 53 9
2 34 5
3 47 5
4 84 14
5 28 5
Gender/Sexe
Male/Masculin 115 14
Female/F�eminin 128 24
322 International Orthodontics 2012 ; 10 : 318-336
Millewa SAYAGH et al.

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
Changes to the orthodontic treatment plan due tothe presence of a molar with a guarded middle-term prognosis (endodontic treatment andprosthetic crown possibly required)
Conventional malocclusion management was unchanged in3.9% (n = 11) of cases whereas 20.4% (n = 58) envisagedextraction and, consequently, modified or requested modifi-cation of the orthodontic treatment. Finally, 75.7% of practi-tioners (n = 215) needed further criteria before taking theirfinal treatment decision. These three approaches were unre-lated to the practitioner’s characteristics (Table III).
Criteria adopted for choosing extractiontreatment for first molar(s)
Among the 273 responding practitioners, 4.8 (SD W 1.7) cri-teria were considered out of the seven proposed and 23.1%(n = 63) of responders considered fewer than 4. The number ofcriteria considered did not differ significantly according to the
Table IIIDecision to modify the orthodontic treatment plan in thepresence of decayed molars with a guarded middle-termprognosis according to practitioners’ specialty, mode ofactivity and Telecom zone.
Characteristics/Caract�eristiques No change inorthodontic treatment/Pas de changement dutraitement orthodontiqun
Specialty/Sp�ecialit�es
Exclusive orthodontists/Orthodontistes exclusifs
10
Pediatric odontologists/Odontologistes p�ediatriques
1
Type of practice/Exercice
Private/Lib�eral 8
Public health, Teaching Hospital/�Etablissement de soins, CHU
3
Telecom Zones/Zones T�el�ecom
1 0
2 3
3 2
4 4
5 2
International Orthodontics 2012 ; 10 : 318-336
Modification du plan de traitement orthodontique dufait de la pr�esence d’une molaire au pronostic r�eserv�esur le moyen terme (traitement endodontique et coiffeproth�etique a envisager)
La prise en charge conventionnelle de la malocclusion n’a pas�et�e modifi�ee dans 3,9 % (n = 11) des cas alors que 20,4 %(n = 58) des praticiens envisageaient l’extraction et modifiai-ent ou demandaient la modification du traitement orthodon-tique en cons�equence. Enfin 75,7 % des praticiens (n = 215)avaient besoin d’autres crit�eres avant de finaliser leur r�eflexionth�erapeutique. Ces trois conduites �etaient ind�ependantes descaract�eristiques du praticien (Tableau III).
Crit�eres de choix retenus pour mettre en place untraitement par extraction de(s) premi�ere(s) molaire(s)
Chez les 273 praticiens concern�es, 4,8 (ET W 1,7) crit�eres surles sept propos�es �etaient consid�er�es et 23,1 % (n = 63) enconsid�eraient moins de quatre. Le nombre de crit�eresenvisag�es ne diff�erait pas significativement en fonction de la
Tableau IIID�ecision de modification du plan de traitement orthodontiqueen pr�esence de molaire(s) d�elabr�ee(s) avec un pronosticr�eserv�e a moyen terme en fonction des sp�ecialit�es, modesd’exercice et zones T�el�ecom.
e
Extraction andsubsequent change/Extraction etchangementen cons�equencen
Requiring extradecision criteriarequired/Besoin d’autrescrit�eres de d�ecisionsn
P
48 188 0.612/0,612
10 27
36 156 0.295/0,295
22 59
15 47 0.558/0,558
6 30
9 41
20 74
8 23
323

Table IVIncidence of practitioners’ characteristics on the criteriaadopted to modify the treatment plan following possibleextraction of (a) permanent first molar(s).
Tableau IVIncidence des caract�eristiques des praticiens sur le crit�eres retenus pour modifier le plan detraitement orthodontique suite a une �eventuelle ex action de premi�ere(s) molaire(s)permanente(s).
Presence of3rd molars/Pr�esencedes3esmolaires
Patientmotivation/Motivation dupatient
Interarchrelationship/Relationinter-arcade
Oral hygiene/Hygi�enebucco-dentaire
TypologyTypologie
Anterior jaw-toothdiscrepancy/DDMant�erieure
Number of 1stmolars to beextracted/Nombre de1resmolaires aextraire
Yes/Oui
No/Non
Yes/Oui
No/Non
Yes/Oui
No/Non
Yes/Oui
No/Non
Yes/Oui
o/on
Yes/Oui
No/Non
Yes/Oui
No/Non
Specialty/Sp�ecialit�e
Orthodontist/Orthodontiste
227 9 176 60 164 72 166 70 141 5 121 115 113 123
Pedodontist/P�edodontiste
35 2 25 12 24 13 24 13 24 1 24 13 22 15
Type of practice/Mode d’exercice
Private/Lib�eral 185 7 141 51 139 53 132 60 120 2 96 96 87* 105*
Public institution/�Etablissement de soins
77 4 60 21 49 32 58 23 45 6 49 32 48* 33*
Telecom Zone/Zone T�el�ecom
1 58* 4* 39* 23* 41 21 41 21 33 9 33 29 26 36
2 33* 3* 31* 5* 26 10 25 11 19 7 19 17 17 19
3 48* 2* 39* 11* 35 15 36 14 29 1 22 28 25 25
4 94* 0* 74* 20* 67 27 66 28 66 8 56 38 54 40
5 29* 2* 18* 13* 21 10 22 9 18 3 15 16 13 18*P < 0.05.*p < 0,05.
324
Intern
ational
Orth
odontics
2012;10:318-336
Millew
aSA
YAGH
etal.
str
/
NN
9
7
3
2
1
2
2
1

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
speciality, whether dentofacial (mean 4.8; SD W 1.6) or pedi-atric odontology (mean 5; SD W 2.1) (P = 0.252). In increas-ing order as classified by the responders, the following criteriawere adopted: presence of third molars for 96.0% of respon-ders (n = 262); patient’s motivation for treatment for 73.6%(n = 201); the inter-arch relationship for 69.6% (n = 165) ororal hygiene for 69.2% (n = 189); facial pattern for 60.4%(n = 165); anterior jaw-tooth discrepancy for 53.1%(n = 145) and the number of permanent first molars to beextracted for 49.5% (n = 135). This last criteria was adoptedsignificantly less often by private practitioners (P = 0.035).Presence of third molars was taken into account significantlymore often in the south-east of France (Telecom zone 4)whereas this criteria was considered the least frequently inzone 2 (P = 0.029). The Centre and South-West regions(Telecom zones 1 and 5) were less concerned about patientmotivation (P = 0.016) (Table IV).
Incidence of the presence of a single permanentfirst molar requiring extraction on the treatmentdecision in patients not needing orthodontictreatment
The majority of practitioners made no first intention decisionregardless of the permanent first molar requiring extraction.Their final decision depended on the socioeconomic context oracceptance of the treatment. For other practitioners, 31.7%(n = 90) and 16.9% (48), respectively, preferred, on the max-illa, to close the space or upright the second molar (whentipped) in order to place a space retainer. At the mandible,13.4% (n = 38) preferred to close the space and 36.4%(n = 103) opted to upright the second molar. In the firstinstance, the practitioner’s choice was related to their speci-ality (P = 0.002) and type of practice (P = 0.025) (Table V).
In the event of extraction of a permanent firstmolar, what are the alternatives to orthodontictreatment for patients not needing orthodontics?
Of the three alternatives suggested in the questionnaire, num-bers one (n = 43; 15.1%), two (n = 26; 9.2%) and three(n = 213; 75%) were adopted. The following solutions wereimplemented, in decreasing order: implant rehabilitation andprosthetic crown (n = 267; 94%), a bridge (n = 237; 83.5%)and autotransplantation of a third molar (n = 219; 77.1%). Theimplant-borne solution was chosen significantly more oftenamong exclusive orthodontists (P = 0.046) and in the privatesector (P = 0.029) (Table VI). The differences betweenTelecom zones were close to significance with a trend to morefrequent usage of implant-borne solutions at the expense ofbridges in south-west France and with a trend towards more
International Orthodontics 2012 ; 10 : 318-336
sp�ecialit�e en orthop�edie dentofaciale (moyenne 4,8 ;ET W 1,6) ou en odontologie p�ediatrique (moyenne 5 ;ET W 2,1) (p = 0,252). Par ordre croissant de classementdans les r�eponses des praticiens, �etaient retenus la pr�esencedes troisi�eme molaires pour 96,0 % d’entre eux (n = 262); lamotivation du patient au traitement pour 73,6 % (n = 201); larelation inter-arcade pour 69,6 % (n = 190) ou l’hygi�ene buc-codentaire pour 69,2 % (n = 189) ; la typologie pour 60,4 %(n = 165) ; la DDM ant�erieure pour 53,1 % (n = 145) ou lenombre de premi�eres molaires permanentes a extraire pour49,5 % (n = 135). La prise en compte de ce dernier crit�ere �etaitsignificativementmoins fr�equente enmilieu lib�eral (p = 0,035).La pr�esence des troisi�eme molaires �etaient significativementplus souvent consid�er�ee dans le sud-est de la France (zoneT�el�ecom 4) alors qu’elles l’�etaient le moins souvent dans lazone 2 (p = 0,029). Ce sont les r�egions du centre et du sud-ouest (zones T�el�ecom 1 et 5) qui �etaient les moins attentivesa la motivation du patient (p = 0,016) (Tableau IV).
Incidence de la pr�esence d’une seule premi�eremolairepermanente condamn�e sur la d�ecision th�erapeutiqueconcernant un patient qui n’a pas besoin de traitementorthodontique
Lamajorit�e des praticiens ne se prononcaient pas en premi�ereintention quelle que soit la premi�ere molaire permanentecondamn�ee a extraire. Leur d�ecision finale d�ependait ducontexte socio�economique ou de l’acceptation du traitement.Concernant les autres praticiens, respectivement 31,7 %(n = 90) et 16,9 % (n = 48) pr�ef�eraient, au maxillaire, fermerl’espace ou redresser la deuxi�eme molaire �eventuellementvers�ee pour mettre en place un mainteneur d’espace. A lamandibule, ils �etaient 13,4 % (n = 38) a fermer l’espace et36,4 % (n = 103), a redresser la deuxi�eme molaire. Dans cedernier cas, leur attitude d�ependait de la sp�ecialit�e du praticien(p = 0,002) et de l’exercice (p = 0,025) (Tableau V).
En cas d’extraction d’une premi�ere molairepermanente, les alternatives au traitementorthodontique propos�ees au patient sans besoinorthodontique
Sur les trois alternatives sugg�er�ees dans le questionnaire, une(n = 43 ; 15,1 %), deux (n = 26 ; 9,2 %) ou trois (n = 213 ;75 %) �etaient retenues. Par ordre d�ecroissant de classement,la r�ehabilitation par implant et coiffe proth�etique (n = 267 ;94 %), un bridge (n = 237 ; 83,5 %) et l’autotransplantationd’une troisi�eme molaire (n = 219 ; 77,1 %) �etaient propos�es.Le choix d’une solution implanto-port�ee �etait significativementplus souvent observ�e chez les orthodontistes exclusifs(p = 0,046) et en milieu lib�eral (p = 0,029) (Tableau VI). Lesdiff�erences entre les zones T�el�ecom �etaient proches de lasignificativit�e avec une tendance a un choix plus fr�equent desolutions implanto-port�ees aux d�epens du bridge dans lesud-ouest et une tendance a un choix plus fr�equent de
325

Millewa SAYAGH et al.
frequent adoption of third molar autotransplantation in thenorth-east (P = 0.058).
Extraction of other molars not requiringextraction in a global treatment setting
The majority, i.e., 68.7% (n = 195) of practitioners, did notcall for extraction of the other molar while only 55 (19.4%) andnine (3.2%), respectively, called for extraction of the contra-lateral molar or the three other molars. Twenty-five (8.8%) didnot answer this question. The practice of responding practi-tioners in Telecom zone 3 differed significantly from that ofpractitioners in other zones (Table VII).
Table VTreatment decision faced with a permanent first molarrequiring extraction in a patient not needing orthodontictreatment according to the specialty, mode of activity andTelecom zone.
Maxillary molar/Molaire maxi
Spaceclosure/Fermerespace
Upright 2nd Mand maintain spaceRedresser 2e
M et maintenirespace
Specialty/Sp�ecialit�es
Exclusive orthodontists/Orthodontistes exclusifs
79 45
Pedodontists/P�edodontistes 11 3
Type of practice/Mode d’exercice
Private/Lib�eral 65 39
Public health/�Etablissements de soins
25 9
Telecom Zones/Zones T�el�ecom
1 23 12
2 9 6
3 13 8
4 35 18
5 10 4*P < 0.05.a Socioeconomic status, treatment acceptance.*p < 0,05.a Situation socio�economique, acceptation du traitement.
326
l’autotransplantation de la troisi�eme molaire dans le nord-est(p = 0.058).
Extraction des autres molaires non condamn�ees dansun contexte de traitement global
La majorit�e, soit 68,7 % (n = 195) des praticiens, ne faisaientpas extraire les autres molaires alors qu’ils �etaient respective-ment 55 (19,4 %) et neuf (3,2 %) a faire extraire la molairecontrolat�erale ou les trois autres molaires. Vingt-cinq prati-ciens (8,8 %) n’avaient pas r�epondu a la question. La pratiquedes patriciens r�epondants de la zone T�el�ecom 3 diff�erait sig-nificativement de celle des autres zones (Tableau VII).
Tableau VD�ecision th�erapeutique en pr�esence d’une premi�ere molairepermanente condamn�ee chez un patient qui n’a pas besoin detraitement orthodontique, en fonction des sp�ecialit�es, modesd’exercice et zones T�el�ecom.
llaire Mandibular molar/Molaire mandibulaire
/Consider overallsituationa/Tenir comptedu contexteglobal,a
Spaceclosure/Fermerespace
Upright 2nd Mand maintainspace/Redresser2eM etmaintenirespace
Consideroverallsituationa/Tenir comptedu contexteglobal,a
122 32* 99* 115*
24 6* 4* 28*
96 27* 82* 91*
50 11* 21* 52*
27 10 22 30
24 2 13 24
31 8 18 26
45 12 40 46
19 6 10 17
International Orthodontics 2012 ; 10 : 318-336

Table VIIncidence of practitioners’ characteristics on the therapeuticalternatives to orthodontic treatment in the presence of a molarrequiring extraction.
Tableau VIIncidence des caract�eristiques des praticiens sur lesalternatives th�erapeutiques au traitement orthodontique enpr�esence d’une molaire condamn�ee.
Implant-bornesolution/Solutionimplanto-port�ee
Bridge/Bridge Autotransplantationof a 3rd molar/Autotransplantationd’une 3emolaires
Yes/Oui No/Non Yes/Oui No/Non Yes/Oui No/Non
Specialty/Sp�ecialit�es
Orthodontists/Orthodontistes 234* 12* 204 42 190 56
Pedodontists/P�edodontistes 33* 5* 33 5 30 8
Type of practice/Mode d’exercice
Private/Lib�eral 192* 8* 166 34 155 45
Care institution/ �Etablissements de soins 75* 9* 71 13 64 20
Telecom Zones/Zones T�el�ecom
1 58** 4** 56** 6** 49** 13**
2 37** 2** 31** 8** 30** 9**
3 48** 4** 47** 5** 43** 9**
4 92** 6** 80** 18** 78** 20**
5 32 1** 23** 10** 19** 14**
*P < 0.05; **P = 0.058*p < 0,05 ; **p = 0.058.
Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
Discussion
This epidemiological study allowed us to analyse the treat-ment decisions made by practitioners working exclusively inpediatric odontology and by orthodontic practitioners in thepresence of (a) decayed permanent first molar(s) with aguarded prognosis in two distinct clinical situations. Eitherthe prognosis was poor in the middle term (with the possibilityof preserving the tooth provided endodontic treatment andprosthetic restoration were performed) in children or adoles-cents requiring orthodontic treatment. In which case theimplied question was: should extraction be performed withthe resulting changes to the orthodontic treatment plan? Orthe prognosis was guarded in the short term (in which case,extraction was indicated) in young patients not requiringorthodontic treatment. In this instance, was orthodontic treat-ment needed in order to close the space created by theextraction?Proportionally more pediatric odontologists (38%) than ortho-dontists (12.45%) took part in the study. The former all prac-tised in a university hospital setting as this specialty is notofficially recognized in France. Contacted through the
International Orthodontics 2012 ; 10 : 318-336
Discussion
Cette �etude �epid�emiologique nous a permis d’analyser lad�ecision th�erapeutique des praticiens exclusifs en odontologiep�ediatrique ou sp�ecialistes en orthodontie en pr�esence depremi�ere(s) molaire(s) permanente(s) d�elabr�ee(s) de pronos-tic r�eserv�e, dans deux situations cliniques distinctes. Soit lepronostic �etait r�eserv�e a moyen terme (conservation possiblesous r�eserve d’un traitement endodontique et d’une reconsti-tution proth�etique) chez un enfant ou un adolescent qui devaitetre trait�e orthodontiquement ; et la question impliqu�ee �etait :fallait-il ou non extraire et modifier le plan de traitement ortho-dontique en cons�equence ? Soit le pronostic �etait r�eserv�ea court terme (extraction indiqu�ee) chez un jeune patient quin’avait pas besoin de traitement orthodontique ; et dans cecas, fallait-il mettre en place ou non un traitement orthodon-tique pour fermer l’espace cr�e�e par l’extraction ?
Les odontologistes p�ediatriques (38 %) ont �et�e proportionnel-lement plus nombreux que les orthodontistes (12,45 %) a par-ticiper a cette �etude. Les premiers �etaient tous hospitalo-universitaires, cette sp�ecialit�e n’�etant pas officiellement
327

Table VIIDecision to extract other molars in the presence of a singlemaxillary first molar requiring extraction according topractitioners’ specialty, mode of activity and Telecom zone.
Tableau VIID�ecision d’extraire d’autres molaires face a une seulepremi�ere molaire maxillaire condamn�ee en fonction dessp�ecialit�es, modes d’exercice et zones T�el�ecom.
Characterisics/Caract�eristiques Extraction ofcontralateral molar/Extraction de lamolaire contro-lat�erale
Extraction of3 other molars/Extraction des3 autres molaires
No extraction ofother molars/Pas d’extractiondes autres molaires
Specialty/Sp�ecialit�es
Exclusive orthodontists/Orthodontistes exclusifs
48 6 172
Pedodontists/P�edodontistes 7 3 23
Type of practice/Mode d’exercice
Private/Lib�eral 37 5 141
Public institution/�Etablissements de soins
18 4 54
Telecom Zones/Zones T�el�ecom
1 9* 2* 47*
2 4* 2* 26*
3 19* 2* 27*
4 19* 2* 68*
5 4* 1* 27*
*P <0.05.*p < 0,05.
Millewa SAYAGH et al.
COLEP, all 16 French faculties, with the exception ofClermont-Ferrand, were represented. The orthodontists,although proportionately under-represented in the study sam-ple, were nonetheless representative of the demography oftheir profession in view of their distribution in the differentTelecom zones (Table I). In contrast, university hospital ortho-dontists were over-represented relative to their private-sectorcolleagues since they constituted 18.7% of the orthodontists inour sample, i.e., three times the normal ratio. Consequently,the external validity of these results was not very satisfactoryand the results need to be interpreted with caution, in partic-ular regarding the orthodontists. On the other hand, the inter-nal validity was satisfactory and the differences observedbetween the two groups could be thought of as resulting fromthe practitioners’ specialty as the other administrative char-acteristics displayed no significant difference.
The difference in response rates between the two groups ofpractitioners can be explained by the necessarily teaching-hospital-based activity of the pediatric odontologists who aremore concerned by this problem which is found most fre-quently in the hospital setting (Table II). Prevalence studies
328
reconnue en France. Sollicit�es par l’interm�ediaire du COLEP,les 16 facult�es francaises, a l’exception de celle de Clermont-Ferrand, �etaient repr�esent�ees. Si les seconds, les orthodon-tistes, �etaient proportionnellement sous-repr�esent�es dansl’�echantillon �etudi�e, ils �etaient n�eanmoins repr�esentatifs dela d�emographie professionnelle en r�ef�erence a leur r�epartitiondans les diff�erentes zones T�el�ecom (Tableau I). En revanche,les orthodontistes hospitalo-universitaires �etaient sur-repr�esent�es par rapport a leurs coll�egues lib�eraux car ilsconstituaient 18,7 % des orthodontistes de notre �echantillon ;soit deux a trois fois le ratio normal. De ce fait, la validit�eexterne de ces r�esultats n’�etait pas tr�es satisfaisante et lesr�esultats doivent etre interpr�et�es avec prudence, en particulierchez les orthodontistes. En revanche, la validit�e interne �etaitsatisfaisante et les diff�erences observ�ees entre ces deuxgroupes pouvaient etre consid�er�ees comme le fruit de lasp�ecialit�e car les autres caract�eristiques administratives nediff�eraient pas significativement.La diff�erence de taux de r�eponses dans les deux groupes depraticiens peut s’expliquer par l’exercice obligatoirementhospitalo-universitaire des odontologistes p�ediatriques plusconcern�es par ce probl�eme plus fr�equent en milieu hospitalier(Tableau II). En effet, les �etudes de pr�evalence ont toujours
International Orthodontics 2012 ; 10 : 318-336

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
have always demonstrated more frequent and more severecarious decay in the least favored socioeconomic categories,which prefer to consult in hospitals as opposed to privateoffices [1]. Moreover, while cases of MIH are not associatedwith an underprivileged socioeconomic context [4,5], they areoften referred to hospital pediatric odontology departments asgeneral practitioners are often circumspect when faced withthese major cases of tooth decay in children who are not alwayseasy to treat on account of their young age or the problemsinherent in this type of hypomineralization [4,6]. This hypoth-esis can also explain the overrepresentation of university hos-pital practitioners in the orthodontists group since they aremore aware of this problem of permanent first molar decay.
Changes in the orthodontic treatment plan due tothe presence of a molar with a guarded middleterm prognosis
In other words, this first molar could remain on the arch forseveral years provided it was treated endodontically and pros-thetically, even if the survival period remained unknown.Nonetheless, 20.4% of practitioners extracted immediatelyand adopted a treatment plan with no further criteria whereasa minority did not extract and did not change the treatmentplan. Although inclusion of permanent first molar extraction,notably in the presence of crowding or malocclusion [7], can-not be contested, extraction of a molar which could be treatedendodontically and/or with a crown deserves some thought.Indeed, patient age, the position of the first molar and maloc-clusion were not specified in the question. Despite a signifi-cant difference between answers depending on the type ofactivity of the responders (Table III), the percentage of20.4% of practitioners who immediately extracted the molarcould be explained by the high proportion of hospital practi-tioners. The latter are frequently required to treat patients withsocioeconomic difficulties who cannot afford the additionalprosthetic expense. The majority of practitioners (75.5%)needed other criteria in order to make their final treatmentdecision.
Criteria adopted for choices related to treatmentrequiring extraction of one or several permanentfirst molar(s)
Of the seven proposed criteria, most responders requiredbetween three and seven criteria. In compliance with recom-mendations, few practitioners (1.8%) considered fewer thantwo [7]. The number and choice of criteria were independent ofthe type of speciality (Table IV).
International Orthodontics 2012 ; 10 : 318-336
mis en �evidence une atteinte carieuse plus fr�equente et pluss�ev�ere dans les cat�egories socioprofessionnelles les plusd�efavoris�ees qui consultent les services hospitaliers depr�ef�erence aux cabinets lib�eraux [1]. Par ailleurs, si les casdeMIH n’ont pas �et�e associ�es a un contexte socio�economiqued�efavorable [4,5], ils sont souvent adress�es aux d�epartementshospitaliers d’odontologie p�ediatrique, les omnipraticiens�etant souvent circonspects face a ces importantsd�elabrements dentaires chez des enfants pas toujours facilesa prendre en charge a cause de leur jeune age ou desdifficult�es d’anesth�esie inh�erentes a cette hypomin�eralisation[4,6]. Cette hypoth�ese peut �egalement expliquer la sur-repr�esentation des patriciens hospitalo-universitaires dans legroupe des orthodontistes, plus sensibilis�es par ce probl�emede d�elabrement des premi�eres molaires permanentes.
Modification du plan de traitement orthodontique dufait de la pr�esence d’une molaire au pronostic r�eserv�esur le moyen terme
Autrement dit cette premi�ere molaire pouvait rester plusieursann�ees sur l’arcade a partir du moment ou elle �etait trait�ee(traitement endodontique et reconstitution proth�etique),meme si le nombre d’ann�ees �etait une inconnue. Pourtant,20,4 % des praticiens l’extrayaient imm�ediatement et adoptai-ent un plan de traitement en cons�equence, sans plus decrit�eres, alors qu’une minorit�e n’extrayait pas et ne changeaitpas le plan de traitement. Si l’int�egration de l’extraction d’unepremi�ere molaire permanente au plan de traitement global,notamment en pr�esence d’un encombrement ou d’une mal-occlusion [7], ne prete pas a discussion, l’extraction d’unemolaire qui pouvait etre trait�ee endodontiquement et/oucouronn�eem�eritait r�eflexion. En effet, l’age du patient, la loca-lisation de la premi�ere molaire et la malocclusion n’�etaient paspr�ecis�es dans la question. Malgr�e une absence de diff�erencesignificative entre les r�eponses en fonction du type d’exercice(Tableau III), ce pourcentage de 20,4 % de praticiens extra-yant d’embl�ee la molaire pourrait s’expliquer par la proportion�elev�ee d’hospitalo-universitaires. Ils sont souvent amen�esa traiter des patients confront�es a des difficult�es socio�econo-miques ne permettant pas toujours la prise en charge de fraisproth�etiques compl�ementaires. A juste titre, la majorit�e despraticiens (75,7 %) avaient besoin d’autres crit�eres avant definaliser leur r�eflexion th�erapeutique.
Crit�eres de choix retenus pour mettre en place untraitement par extraction de(s) premi�ere(s) molaire(s)
Sur sept crit�eres propos�es, la majorit�e des praticiens ayantr�epondu au questionnaire avaient besoin de trois a septcrit�eres et, conform�ement aux recommandations, peu d’entreeux (1,8 %) en avaient consid�er�e moins de deux [7]. Le nom-bre et le choix des crit�eres ne d�ependaient pas de la sp�ecialit�e(Tableau IV).
329

Millewa SAYAGH et al.
Presence of the third molars
Presence of the third molars was the most frequently citedcriterion (96% of cases) and, in agreement with scientific data,was held to be the most important [8]. Indeed, extraction of apermanent first molar can be envisaged only in the presence ofthe wisdom tooth buds (and those of the second premolars) andprovided the anatomy and eruption path are favorable [9,10].In this case, prosthetic solutions can be avoided and rehabil-itation performed by mesializing the second and third molars[9].In these cases, the stage of development of the third molarshould be assessed in order to determine the optimum time forextraction of the first molar. Spontaneous mesialization of thethird molar during orthodontic mesialization of the secondmolar can only occur if it has entered the active eruption stage[10]. In other cases where the extraction space is preserved ingrowing children, autotransplantation of the tooth is prefera-ble to the implant option [11–14]. The choice of criteria wasunrelated to the practitioners’ characteristics, with the excep-tion of the geographical area in which they practised (TableIV). The presence of the third molar was taken into accountmost often in zone 4 and least often in zone 2. This differencecould be explained by the teaching delivered in the dentalschools or, alternatively, by a difference in the treatmentoffering due to professional demography or the make-up ofthe corresponding populations.
Patient motivation
Patient motivation was cited in 75% of cases and manifestlyconstitutes an important criterion in the drawing up of an oftenlong and complex treatment plan [10]. Indeed, although one ofthe better solutions involves closing the extraction space bymesialization of the second and third molars, this process doesnot always occur spontaneously. If the timing of the extractionand the existing malocclusion are not always conducive tospontaneous mesialization, orthodontic treatment should alsoensure satisfactory positioning of these teeth [10,15] and,therefore, should not be interrupted.Lack of motivation and non-acceptance of long orthodontictreatment can be indications for conservation of the tooth or ofthe space followed by later rehabilitation. The choice of thiscriterion was also closely related to the Telecom zone. Itwas respectively most and least adopted in zones 4 and 1(Table IV). The same arguments regarding regional variationsin teaching and treatment offering are also valid here.
The inter-arch relationship and patient oral hygiene
The inter-arch relationship and patient oral hygiene were alsofrequently quoted and were joint third criterion of choice.According to the recommendations of the ScottishIntercollegiate Guidelines Network (SIGN) [7], the inter-arch
330
La pr�esence de la troisi�eme molaire
La pr�esence de la troisi�eme molaire �etait le crit�ere a la fois leplus souvent cit�e (96 % des cas), et consid�er�e comme le plusimportant conform�ement aux donn�ees acquises de la science[8]. En effet, l’extraction d’une premi�ere molaire permanentene peut etre envisag�ee qu’en pr�esence des germes des dentsde sagesse (et des deuxi�eme pr�emolaires), sous r�eserved’une anatomie et d’un axe d’�eruption favorables [9,10] carelle autorise une r�ehabilitation sans artifice proth�etique du faitde la m�esialisation des deuxi�eme et troisi�eme molaires [9].D�es lors, le stade de d�eveloppement de la troisi�eme molairedoit etre �evalu�e pour �etablir la date optimale d’extraction de lapremi�ere molaire. En effet, la m�esialisation spontan�ee de latroisi�eme molaire lors de la m�esialisation orthodontique de ladeuxi�eme molaire ne se fait que si elle est au stade d’�eruptionactive [10]. D’autres fois, dans les cas ou l’espace d’extractionest conserv�e chez un enfant en cours de croissance, l’auto-transplantation de la dent de sagesse sera pr�ef�er�ee a l’optionimplantaire [11–14]. Le choix de ce crit�ere �etait ind�ependantdes caract�eristiques des praticiens a l’exception de la zoneg�eographique dans laquelle ils exercaient (Tableau IV). Lapr�esence de la troisi�eme molaire a �et�e consid�er�ee le plussouvent dans la zone 4 et le moins souvent, dans la 2. Cettediff�erence pourrait s’expliquer par les enseignements d�elivr�esselon les facult�es, a moins qu’il ne s’agisse d’une offre desoins diff�erente du fait des d�emographies professionnellesou des populations correspondantes.
La motivation du patient
La motivation du patient, cit�ee dans environ 75 % des cas, est�evidemment un crit�ere important lors de l’�elaboration d’un plande traitement souvent long et complexe [10]. En effet, si l’unedes bonnes solutions est la fermeture de l’espace d’extractionpar m�esialisation des deuxi�eme et troisi�eme molaires, elle nese fait pas toujours spontan�ement. Si le moment d’extractionou la malocclusion existante n’autorise pas une m�esialisationspontan�ee, le traitement orthodontique doit �egalementassurer la mise en place satisfaisante de ces dents [10,15]et ne doit donc pas etre interrompu.Lemanque demotivation et la non acceptation d’un traitementorthodontique long peuvent indiquer la conservation de la dentou de l’espace avec r�ehabilitation ult�erieure. Le choix de cecrit�ere d�ependait �egalement uniquement de la zone T�el�ecom.Il �etait respectivement le plus et le moins pris en compte dansles zones 4 et 1 (Tableau IV) ; le meme argument d’enseigne-ments et d’offres de soins variables d’une r�egion a l’autre peutdonc �egalement etre retenu.
La relation inter-arcade et l’hygi�ene du patient
La relation inter-arcade et l’hygi�ene du patient ont �et�e cit�eesaussi souvent et intervenaient toutes deux comme troisi�emecrit�ere de choix. D’apr�es les recommandations de ScottishIntercollegiate Guidelines Network (SIGN) [7], la relation
International Orthodontics 2012 ; 10 : 318-336

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
relationship is a crucial treatment decision criterion andneeds to stand alongside age and the presence of the thirdmolar as one of the three main decision-making criteria. Theserecommendations use the Angle class and crowding to deter-mine the indication for extraction. The space must definitelybe preserved to correct Class II malocclusions, with or withoutmaxillary crowding and in cases of severe crowding in themandible. In contrast, the extraction space is not necessaryto correct Class IIs with minimal mandibular crowding. InClass IIIs, extraction of the decayed first molars is contra-indicated [7,8,16].
Patient oral hygiene obviously needs to be considered duringpreparation of the treatment plan, particularly regardingorthodontics. Although the wording of the question referringto orthodontic treatment had already led this criterion to bedealt with, it was decided to retain the criterion since treat-ment involving space closure, particular at the mandible, islengthy and cannot be interrupted; Good hygiene is therefore amust during treatment while, conversely, poor hygiene canconstitute a contraindication to its adoption [10].
Typology
Typology, the fifth choice criterion, was taken into account in60% of cases although it could have been cited more often. Forinstance, Ong and Bleakley contraindicated extraction of firstmolars in hypodivergent Class II, division 2 patients, sincereduction of the overbite and closure of the space would thenbe difficult to achieve [8].
Anterior tooth-jaw discrepancy
Anterior tooth-jaw discrepancy, the sixth criterion, was quotedin only half the responses although it is cited more frequentlyin the literature. In Class Is associated with crowding, thechoice of extraction timing takes the crowding into account.If it is severe, extraction is postponed until the second molarsare present on the arch in order to enhance extraction spacemanagement, particularly at the maxilla [7,8].
The number of molars requiring extraction
The number of molars requiring extraction, the seventh crite-rion determining decisions, was quoted in 49.5% of cases.Private practitioners gave it less importance than colleaguesin the hospital setting, probably because of the nature of theclinical cases encountered in the daily practice of each cate-gory (Tables II and IV). Nevertheless, “balancing” and“compensation” were often mentioned in cases of mixed den-tition without implying a prognosis of the corresponding toothrequiring extraction, which can be healthy [4,5,7,16–19].“Balancing” referred to extraction of the first contralateral
International Orthodontics 2012 ; 10 : 318-336
inter-arcade est un crit�ere de d�ecision th�erapeutique essen-tiel. Elle doit faire partie, avec l’age et la pr�esence de la troi-si�eme molaire, des trois principaux crit�eres de d�ecision. Cesrecommandations d�eduisent l’indication d’extraction selon lesClasses d’angle et l’encombrement. L’espace doit etreimp�erativement conserv�e pour la correction de la malocclu-sion de Classe II avec ou sans encombrement au maxillaire etavec un encombrement important a la mandibule. Enrevanche, l’espace d’extraction n’est pas n�ecessaire pour cor-riger une Classe II avec un encombrement minime a la man-dibule. Dans les cas de Classe III, l’extraction de premi�eresmolaires d�elabr�ees est contre-indiqu�ee [7,8,16].L’hygi�ene du patient est �evidemment a consid�erer lors del’�elaboration du plan de traitement, en particulier orthodon-tique. Si ce crit�ere a d�eja du etre consid�er�e du fait de laformulation de la question pos�ee �evoquant un traitementorthodontique, il a �et�e l�egitimement retenu car un traitementpar fermeture d’espace, notamment mandibulaire, est longet ne peut etre interrompu. Il faut donc avoir la garantie d’unebonne hygi�ene pendant le traitement et, a l’inverse, unemauvaise hygi�ene peut contre-indiquer sa mise en place[10].
La typologie
La typologie, cinqui�eme crit�ere de choix, a �et�e consid�er�eedans 60 % des cas alors qu’elle aurait pu etre �evoqu�ee plussouvent. Par exemple, Ong et Bleakley contre-indiquaientl’extraction des premi�eres molaires chez les patients hypodi-vergents en Classe II division 2, car la diminution du recouvre-ment et la fermeture de l’espace seraient alors difficiles a obte-nir [8].
La DDM ant�erieure
La DDM ant�erieure, sixi�eme crit�ere de choix, n’a �et�e retenueque dans la moiti�e des cas, alors qu’elle a plus d’importanceau regard de la litt�erature. En effet, dans les cas de Classe Iavec encombrement, le choix du moment de l’extraction tientcompte de l’encombrement. S’il est important, les extractionssont diff�er�ees jusqu’a la mise en place sur l’arcade des deu-xi�eme molaires pour une meilleure gestion de l’espaced’extraction, notamment au maxillaire [7,8].
Le nombre de molaires a extraire
Le nombre de molaires a extraire, septi�eme crit�ere de choix, a�et�e consid�er�e, dans 49,5 % des cas. Les praticiens lib�eraux ypretaient moins attention que leurs coll�egues exercant enmilieu hospitalier, probablement du fait des cas cliniquesrencontr�es dans l’exercice quotidien de chacun (Tableaux IIet IV). Pourtant, les notions de « balancing » et« compensating » ont souvent �et�e �evoqu�ees en denturemixte, sans notion de pronostic de la dent correspondantea extraire qui peut etre saine [4,5,7,16–19]. Le « balancing »concerne l’extraction de la premi�ere molaire controlat�erale
331

Millewa SAYAGH et al.
premolar in order to avoid midline deviations in crowdedcases. “Compensation” involved only the antagonist perma-nent maxillary first molar in order to prevent it intruding.Henceforth, this approach should be reviewed given the avail-ability of the new treatment tools such as anchorage minis-crews, which, among other things, facilitate molar intrusion. Incontrast, these approaches need to be carefully considered ifthe corresponding teeth are decayed.
Incidence of presence of a single permanent firstmolar requiring extraction on treatment decisionfor patients not in need of orthodontic treatment
In approximately half of cases, practitioners from whicheverspecialty, type of practice and Telecom zone took into consid-eration the patient’s general context (socioeconomic status,treatment consent) before deciding to maintain or close thespace left by extracting a decayed maxillary permanent firstmolar (Table V). A third of practitioners immediately indi-cated space closure, which can be considered a therapeuticsolution of choice up to the age of 12 [10,20,21]. After 12years, spontaneous mesialization of the second molar is hin-dered by occlusion with the first permanent molar [20] andorthodontic treatment is needed to position it correctly[10,15].
In the presence of a decayed mandibular permanent firstmolar, the same proportion (half) of practitioners took accountof the global context. The age of patients not needing ortho-dontic treatment is a criterion, which was not listed in ourquestionnaire although it is an indispensable factor whendrawing up a treatment plan. According to the recommenda-tions of the SIGN (moderate level of proof), particularly for themandible, extraction must be performed before eruption of thesecond molar in order to achieve functional occlusion with no,or minimal, orthodontic treatment [7,17,20,21]. It is a fact thatthe second mandibular molar cannot spontaneously take theplace of the first unless, and only unless, the first molar hasbeen extracted at the ideal age of 8 to 10 years as shown byradiographic observation of the crown and to the onset ofbifurcation of the permanent second molar [4,5,8,16,17,20,22–26].
Before this period, at the onset of mixed dentition, extractionof a decayed mandibular first molar raises a problem since thebud of the third molar cannot yet be detected [7]. Moreover,extraction can trigger lingual tipping of the anterior teeth,increased overbite [4,7] and problems related to prematureand ectopic eruption of the mandibular second molar. Onaccount of the very apical and distal position of its bud relativeto the roots of the temporary second molar, it can impact thebud of the permanent second molar, which has been mesia-lized following the extraction [20,21]. More seldom, the sec-ond premolar erupts early on the arch, distal to the temporary
332
pour pr�evenir la d�eviation des milieux en cas d’encombre-ment. Le « compensating » int�eresse uniquement la premi�eremolaire permanente maxillaire antagoniste pour pr�evenir son�egression. D�esormais, cela doit etre reconsid�er�e avec lesnouveaux outils th�erapeutiques, tels que les minivis d’anc-rage, qui permettent, par exemple, l’ingression des molaires.En revanche, ces notions doivent etre examin�ees avec int�eretsi les dents correspondantes sont d�elabr�ees.
Incidence de la pr�esence d’une seule premi�eremolairepermanente condamn�ee sur la d�ecision th�erapeutiqueconcernant un patient qui n’a pas besoin de traitementorthodontique
Dans environ lamoiti�e des cas, les praticiens, quels que soientleur sp�ecialit�e, leur type d’exercice ou leur zone T�el�ecom,prenaient en consid�eration le contexte global (niveau socio-�economique, consentement au traitement) avant de d�eciderdu maintien ou de la fermeture de l’espace inh�erent a l’extrac-tion de la premi�ere molaire permanente maxillaire d�elabr�ee(Tableau V). Un tiers des praticiens indiquaient d’embl�ee lafermeture de l’espace, qui peut etre consid�er�ee comme unesolution th�erapeutique de choix jusqu’a la l’age de 12 ans[10,20,21]. Apr�es 12 ans, la m�esialisation spontan�ee de ladeuxi�eme molaire est gen�ee du fait de son occlusion avec lapremi�ere molaire permanente [20] : un traitement orthodon-tique s’impose pour la positionner correctement [10,15].En pr�esence d’une premi�ere molaire permanente mandibu-laire d�elabr�ee, la meme proportion de praticiens s’int�eressaitau contexte global, soit la moiti�e d’entre eux. L’age du patientsans besoin orthodontique est un crit�ere qui n’a pas �et�epropos�e par notre questionnaire alors qu’il est un �el�ementindispensable a la mise en place du plan de traitement.Selon les recommandations de SIGN (niveau de preuve mod-�er�e), et en particulier a la mandibule, l’extraction doit etrer�ealis�ee avant l’�eruption de la deuxi�eme molaire pour l’obten-tion d’une occlusion fonctionnelle sans prise en charge ortho-dontique, voire avec une prise en charge orthodontique mini-mum [7,17,20,21]. En effet, la deuxi�ememolaire mandibulairene peut prendre la place de la premi�ere spontan�ement que si,et seulement si, cette derni�ere a �et�e extraite a l’age id�eal dehuit a dix ans qui correspond a l’observation radiographiquede la couronne et du d�ebut de bifurcation de la deuxi�ememolaire permanente [4,5,8,16,17,20,22–26].En amont de cette p�eriode, soit en d�ebut de denture mixte,l’extraction de la premi�ere molaire mandibulaire condamn�eepose probl�eme car il est impossible de constater la pr�esencedu germe de la troisi�eme molaire [7]. Par ailleurs, elle peutprovoquer une linguo-version des dents ant�erieures avec uneaugmentation du recouvrement [4,7] et des difficult�esd’�eruption pr�ecoce et ectopique de la deuxi�eme pr�emolairemandibulaire. Du fait de sa position trop apicale et distale parrapport aux racines de la deuxi�eme molaire temporaire, legerme de la troisi�eme molaire peut impacter le germe de ladeuxi�eme molaire permanente m�esialis�ee du fait de
International Orthodontics 2012 ; 10 : 318-336

Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive
second premolar, thus preventing mesialization of the perma-nent second molar. In this instance, root resorption of thetemporary second premolar does not occur [7,16,20,21]. Inview of this, some authors have recommended simultaneousextraction of the temporary second premolar and of thedecayed permanent mandibular first molar in order to allowthe second premolar to erupt freely and vertically[4,16,20,23]. When extraction is needed after the 8 to 10age slot, at the end of mixed dentition, the second molar hasbegun to erupt and will rotate lingually and tip mesially butwithout completely closing the space [7,8,16,20,21,24,27]. Inthis case, it will require orthodontic uprighting. Consequently,some authors prefer to immediately adopt a prosthetic/auto-transplantation solution [8,10,12,21]. This option was selectedby 36% of practitioners with no indication of patient age beingmade in the question posed.
The trends observed in cases of extraction of decayed perma-nent maxillary first molars were confirmed in the mandibleand showed no statistically significant difference. Hence, sig-nificantly more orthodontists favored space maintenancewhile the pediatric odontologists paid greater attention tothe global context (Table V). The significant differencesobserved between the types of activity of responders resultedfrom different approaches between orthodontists and pediatricodontologists, who were, respectively, most often in private orhospital practice. Moreover, these findings can perhaps beexplained by the experience acquired by the orthodontists,who have the difficult task of closing this space on themandible.
Alternatives to orthodontic treatment proposed topatients requiring extraction of a permanent firstmolar but not in need of orthodontic treatment
One (15.1%), two (9.2%) or three (75%) alternatives wereproposed to orthodontic treatment. While implant-borne reha-bilitations, prosthetic crowns and bridges were cited by allresponders, this was not the case however regarding autotrans-plantation. And yet, this technique has a high success rate,notably in the presence of an immature transplant[11–13,28,29]. The best results were achieved when root edi-fication occurs between the second third and the third quarterof the root [11,28]. Furthermore, autotransplantation does notneed to be postponed although implantology should be contra-indicated in young patients before the end of adolescence.Nevertheless, the implant-borne solution was most frequentlyindicated by orthodontists and by the private sector, perhapson account of a problem of available care since autotransplan-tation remains a seldom-used technique whereas implantologyis now more widespread. The trend towards more frequentadoption of autotransplantation in the north-east of France
International Orthodontics 2012 ; 10 : 318-336
l’extraction [20,21]. Plus rarement, la deuxi�eme pr�emolairepeut faire son �eruption pr�ecocement sur l’arcade en distal dela deuxi�eme molaire temporaire, empechant la m�esialisationde la deuxi�eme molaire permanente. Dans ce cas, il n’y a pasde rhizalyse de la deuxi�eme molaire temporaire [7,16,20,21].A la suite de ce constat, certains auteurs ont recommand�ed’extraire en meme temps la deuxi�eme molaire temporaire etla premi�ere molaire mandibulaire permanente d�elabr�ee afinde permettre l’�eruption libre et verticale de la deuxi�emepr�emolaire [4,16,20,23]. Si la n�ecessit�e d’extraction survientapr�es l’age de huit a dix ans, soit en fin de denture mixte, ladeuxi�eme molaire a d�ebut�e son �eruption et va effectuer unerotation linguale et se verser m�esialement sans assurer lafermeture compl�ete de l’espace [7,8,16,20,21,24,27]. D�eslors, elle doit etre redress�ee par un traitement orthodontique.De ce fait, certains auteurs pr�ef�erent d’embl�ee opter pour unesolution proth�etique/autotransplantation [8,10,12,21]. C’est lasolution qui a �et�e choisie par 36 % des praticiens sans aucunepr�ecision de l’age du patient dans notre question.Les tendances observ�ees dans le cas de l’extraction demolaires permanentes maxillaires d�elabr�ees, sans etre statis-tiquement significatives, se sont confirm�ees a la mandibule :ainsi, les orthodontistes �etaient significativement plus nom-breux a etre en faveur du maintien de l’espace et les odonto-logistes p�ediatriques, plus attentifs au contexte global(Tableau V). Les diff�erences significatives �egalementobserv�ees entre les types d’exercice �etaient le fruit des atti-tudes diff�erentes des orthodontistes et odontologistesp�ediatriques respectivement plus souvent lib�eraux et hospita-liers. Par ailleurs, ces r�esultats peuvent peut-etre s‘expliquerpar l’exp�eriencememe des orthodontistes qui ont la charge decette difficile fermeture de l’espace a la mandibule.
En cas d’extraction d’une premi�ere molairepermanente, les alternatives au traitementorthodontique propos�ees au patient sans besoinorthodontique
Une (15,1 %), deux (9,2 %) ou trois (75 %) alternatives ont�et�e propos�ees au traitement orthodontique. Si lesr�ehabilitations par implant et coiffe proth�etique ou les bridgesont �et�e cit�es par tous, il n’en a pas �et�e de meme pour l’auto-transplantation. Cette technique est pourtant une solutiondont le taux de r�eussite est �elev�e, notamment en pr�esenced’un transplant immature [11–13,28,29] : les meilleursr�esultats ont �et�e obtenus avec une �edification radiculaire entreles deux tiers et les trois quarts de la racine [11,28]. Parailleurs, l’autotransplantation n’a pas besoin d’etre autantdiff�er�ee que l’implantologie contre-indiqu�ee chez des jeunespatients avant la fin de l’adolescence. Pourtant, c’�etait la solu-tion implanto-port�ee qui a �et�e la plus souvent indiqu�ee chezles orthodontistes et en milieu lib�eral ; peut-etre du fait d’unprobl�eme d’offre de soins, car si la pratique de l’implantologiea tendance a se g�en�eraliser, celle de l’autotransplantation estplus rare. La tendance au choix plus fr�equent de
333

Millewa SAYAGH et al.
may result from the regional variations in courses available inDental Schools (Table VI). In chronological order, theimplant-borne solution, bridges and autotransplantation werelisted, respectively, in first, second and third position.However, with improved oral hygiene [1], bridges should havefewer and fewer indications since they should be contraindi-cated if the adjacent teeth supporting the bridge are healthy[4,5,7,16–19].
Extraction of the other non-decayed molars in aglobal treatment setting
Most practitioners (68.7%) responded that they did not extractthe other molars whereas 19.4% and 3.2% extracted, respec-tively, the contralateral molar and the three others.
In practice, the issue of extracting or not the contralateral orantagonist molar revolves around many of the factors outlinedabove. [4,5,7,16–19]. Practitioners in the south-west of Francewere, overall, significantly the least conservative (Table VII).
In conclusion, the responses to our questionnaire should beinterpreted with some caution on account of the responserates. Nevertheless, situations involving decayed molars andthe problems surrounding the treatment decisions inherent insuch cases were of most concern to practitioners devotedexclusively to pediatric odontology and, more generally, toall practitioners working in a hospital environment. On theother hand, these types of practice had no influence on treat-ment decisions with the exception of those required in cases ofpatients with a decayed permanent first molar requiringextraction but not in need of orthodontics. In every case,extraction of a permanent first molar should be the result ofcareful reflection and should be decided in collaboration andfollowing exchanges with the dental surgeon, the specialists,the parents and the child.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
AcknowledgementsWe would like to thank the presidents of the colleges ofteachers of pediatric odontology and dentofacial orthopedicsand the SOF-GAC society for their help in organizing thisstudy.
334
l’autotransplantation dans le nord-est de la France peut etre un�el�ement de r�eponse inh�erent aux formations variables enfonction des facult�es (Tableau VI). Par ordre chronologique,la solution implanto-port�ee, le bridge et l’autotransplantationintervenaient respectivement en premi�ere, deuxi�eme et troi-si�eme position. Pourtant, le bridge avec l’am�elioration de lasant�e buccodentaire [1] devrait avoir des indications de plusen plus rares car il doit etre contre-indiqu�e si les dents adja-centes, piliers de bridge, sont saines.
Extraction des autres molaires non condamn�ees dansun contexte de traitement global
La majorit�e des praticiens (68,7 %) r�epondaient qu’ils n’extra-yaient pas les autres molaires, alors que 19,4 % et 3,2 %extrayaient respectivement la molaire controlat�erale et lestrois autres.Or en pratique, le choix d’extraire la molaire controlat�erale ouantagoniste d�epend des nombreux facteurs d�evelopp�esci-dessus [4,5,7,16–19]. Les patriciens du sud-ouest �etaientd’embl�ee significativement moins nombreux a etre les plusconservateurs (Tableau VII).En conclusion, l’interpr�etation des r�eponses a notre question-naire doit nous amener a consid�erer les r�esultats avec unecertaine prudence du fait du taux de r�eponses. N�eanmoins,les situations de molaires d�elabr�ees et les difficult�es de choixth�erapeutiques inh�erentes a celles-ci concernaient davantageles praticiens exclusifs en odontologie p�ediatrique et plusg�en�eralement tous les praticiens exercant dans des structureshospitali�eres. En revanche, ces types d’exercice n’avaient pasd’incidence sur les d�ecisions th�erapeutiques a l’exception decelles a prendre dans le cas d’une premi�ere molaire mandi-bulaire condamn�ee chez un patient sans besoin orthodon-tique. Dans tous les cas, l’extraction d’une premi�ere molairepermanente doit etre envisag�ee avec pr�ecaution et faire l’objetd’une r�eflexion et d’une discussion entre chirurgien-dentiste,sp�ecialistes, parents et enfant.
D�eclaration d’int�erets
Les auteurs d�eclarent ne pas avoir de conflits d’int�erets enrelation avec cet article.
RemerciementsNous remercions les pr�esidents des coll�eges des enseignantsen odontologie p�ediatrique ou en orthop�edie dento-faciale etla Soci�et�eSOF-GACpour leur aide dans la r�ealisation de cette�etude.
International Orthodontics 2012 ; 10 : 318-336

References/R�ef�erences
1. UFSBD: La sant�e bucco-dentaire des enfants de 6 et 12 ans en France, en 2006 .2. Weerheijm KL. Molar incisor hypomineralisation (MIH). Eur J Paediatr Dent 2003;4
(3):115–20.3. Vuillemin A, Chafaie A, Muller-Bolla M. Hypomin�eralisation incisive-molaire du diag-
nostic a la prise en charge. Clinic 2011;32:227–8.4. Fitzpatrick L, O’Connell A. First permanent molars with molar incisor hypomineralisation.
J Ir Dent Assoc 2007;53:32–7.5. Lygidakis NA, Wong F, J€alevik B, Vierrou AM, Alaluusua S, Espelid I. Best clinical
practice for clinicians dealing with children presenting with molar-incisor-hypominerali-sation (MIH). An EAPD policy document. Eur Arch Paediatr Dent 2010;11(2):75-81.
6. Lepp€aniemi A, Lukinmaa PL, Alaluusua S. Non-fluoride hypomineralizations in the per-manent first molars and their impact on the treatment need. Caries Res 2001;35:36-40.
7. Cobourne M, Williams A, McMullan R. A guideline for the extraction of first permanentmolars in children. Royal College of Surgeons Guidelines, England Available at: http://www.rcseng.ac.uk 2009.
8. Ong DCV, Bleakley JE. Compromised first permanent molars: an orthodontic perspective.Aust Dent J 2010;55:2-14.
9. Albadri S, Zaitoun H, McDonnell ST, Davidson LE. Extraction of first permanent molarteeth: results from three dental hospitals. Br Dent J 2007;203(7):E14 [discussion 408–9.Epub 2007 Jul 27].
10. Bassigny F. Que faire en pr�esence d’une premi�ere molaire tr�es d�elabr�ee ou d�eja extraite?Plaidoyer pour l’option orthodontique. Rev Odontostomatol 2008;37:135–48.
11. Catherine JH, Mockers O, Richard O, Roche-Poggi P, Guyot L, Olivi P, et al.Autotransplantation de dent immature. Rev Stomatol Chir Maxillofac 2007;108:46-50.
12. Torres JH, Favre de Thierrens C, Jacquard C, Jacquey N. Transplantations etr�eimplantations dentaires. EMC 22-305-A-10 .
13. Patel A, Brennan JA, Sandler PJ. Autotransplantation of an impacted third molar: anorthodontic case report. Dent Update 2004;31:596-601.
14. Mendes RA, Rocha G. Mandibular third molar autotransplantation – Literature review withclinical cases. J Can Dent Assoc 2004;70(11):761–6.
15. Yavuz I, Baydas B, Ikbal A, Dagsuyu IM, Ceylan I. Effects of early loss of permanent firstmolars on the development of third molars. Am J Orthod Dentofacial Orthop 2006;130(5):634–8.
16. Williams JK, Gowans AJ. Hypomineralised first permanent molars and the orthodontist.Eur J Paediatr Dent 2003;3:115–20.
17. Shargill I, Hutton A. The management of hypomineralized first permanent molar teeth. DentUpdate 2007;34:636–40.
18. J€alevik B, M€oller M. Evaluation of spontaneous space closure and development of perma-nent dentition after extraction of hypomineralized permanent first molars. Int J PaediatrDent 2007;17:328–35.
19. Sandler PJ, Atkinson R, Murray AM. For four sixes. Am J Orthod Dentofacial Orthop2000;117(4):418–34.
20. Gill DS, Lee RT, Tredwin CJ. Treatment planning for the loss of first permanent molars.Dent Update 2001;28:304–8.
21. Penchas J, Peretz B, Becker A. The dilemma of treating severely decayed first permanentmolars in children: to restore or to extract. J Dent Child 1994;61(3):199-205.
22. Weerheijm KL. Molar incisor hypomineralization (MIH): clinical presentation, aetiologyand management. Dent Update 2004;31:9-12.
23. Conway M, Petrucci D. Three cases of first permanent molar extractions where extraction ofthe adjacent second deciduous molar is also indicated. Dent Update 2005;32:338–42.
24. Mahoney EK. The treatment of localised hypoplastic and hypomineralised defects in firstpermanent molars. N Z Dent J 2001;97:101–5.
International Orthodontics 2012 ; 10 : 318-336 335
Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiryD�ecisions th�erapeutiques en pr�esence de premi�eres molaires permanentes d�elabr�ees chez les sujets jeunes : enquete descriptive

25. Mathu-Muju K, Wright JT. Diagnosis and treatment of molar incisor hypomineralization.Compendium 2006;27(11):604–11.
26. Davies SJ, Gray RJM, Mackie IC. Good occlusal practice in children’s dentistry. Br Dent J2001;191(12):655–9.
27. Seddon JL. Extraction of four first molars: a case for a general practitioner? J Orthod2004;31(2):80–5.
28. Cho SY, Lee CK. Autotransplantation of a supplemental premolar: a case report. J Can DentAssoc 2007;73(5):425–9.
29. Kvint S, Lindsten R, Magnusson A, Nilsson P, Bjerklin K. Autotransplantation of teeth in215 patients a follow-up study. Angle Orthod 2010;80(3):446–51.
336 International Orthodontics 2012 ; 10 : 318-336
Millewa SAYAGH et al.