Antibio - lcr
14
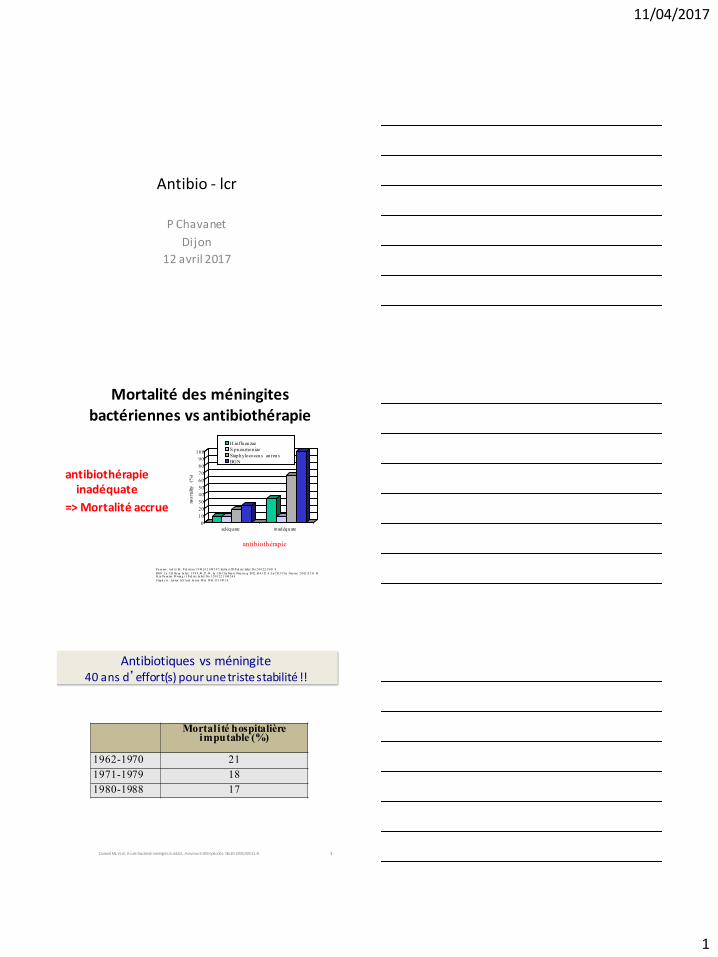
11/04/2017 1 Antibio - lcr P Chavanet Dijon 12 avril 2017 Mortalité des méningites bactériennes vs antibiothérapie antibiothérapie inadéquate => Mortalité accrue P n eu mo : Ard iti M , P ed iatrics 1 9 98 , 1 0 2:1 08 7-9 7; Kelln er JD Ped iatr Infect Dis 2 0 0 2;2 1:9 03 -9 BGN: Lu CH Ho sp In fect. 1 9 9 8 , 40 :27 -34 ; Lu CH Clin Neu ro lNeu rsu rg 20 02 ;10 4:3 52 -8 ;Lu CH J Clin Neu rosc. 2 0 02 ;9:5 33 -38 H. in flu en zae: M wan g i I P ed iatr In fect Dis J 2 0 0 2;2 1:1 04 2-4 8 S tap h y lo : Jen sen AG Arch In tern M ed 19 93 ;15 3:1 90 2-8 0 10 20 30 40 50 60 70 80 90 100 mortality (%) ad éq u ate in ad éq u ate antibiothérapie H .in flu en zae S.pneumoniae Stap h y lo co ccu s au reu s BG N 3 Antibiotiques vs méningite 40 ans d’effort(s) pour une triste stabilité !! Mortalité hospitalière imputable (%) 1962-1970 21 1971-1979 18 1980-1988 17 Durand ML et al. Acute bacterial meningitis i n adults. A reviewof 493 epi sodes. NEJM 1993;328:21-8.
Transcript of Antibio - lcr
11/04/2017
1
Antibio - lcr
P Chavanet
Dijon
12 avril 2017
Mortalité des méningites bactériennes vs antibiothérapie
antibiothérapie inadéquate
=> Mortalité accrue
Pn eu mo : Ard iti M, Ped iatrics 1 9 98 ,1 0 2:1 08 7-9 7; Kelln er JD Ped iatr Infect Dis 2 0 0 2;2 1:9 03 -9
BGN: Lu CH Ho sp In fect. 1 9 9 8 ,40 :27 -34 ; Lu CH Clin Neu ro l Neu rsu rg 20 02 ;10 4:3 52 -8 ; Lu CH J Clin Neu rosc. 2 0 02 ;9:5 33 -38 H.in flu en zae: Mwan g i I Ped iatr In fect Dis J 2 0 0 2;2 1:1 04 2-4 8
Stap h y lo : Jen sen AG Arch In tern Med 19 93 ;15 3:1 90 2-8
0
10
20
30
40
50
60
70
80
90
100
mo
rtal
ity
(%)
adéquate inadéquate
antibiothérapie
H.influenzae
S.pneumoniae
Staphylococcus aureus
BGN
3
Antibiotiques vs méningite 40 ans d’effort(s) pour une triste stabilité !!
Mortalité hospitalière imputable (%)
1962-1970 21
1971-1979 18
1980-1988 17
Durand ML et al. Acute bacterial meningitis in adults. A review of 493 episodes. NEJM 1993;328:21-8.
11/04/2017
2
4
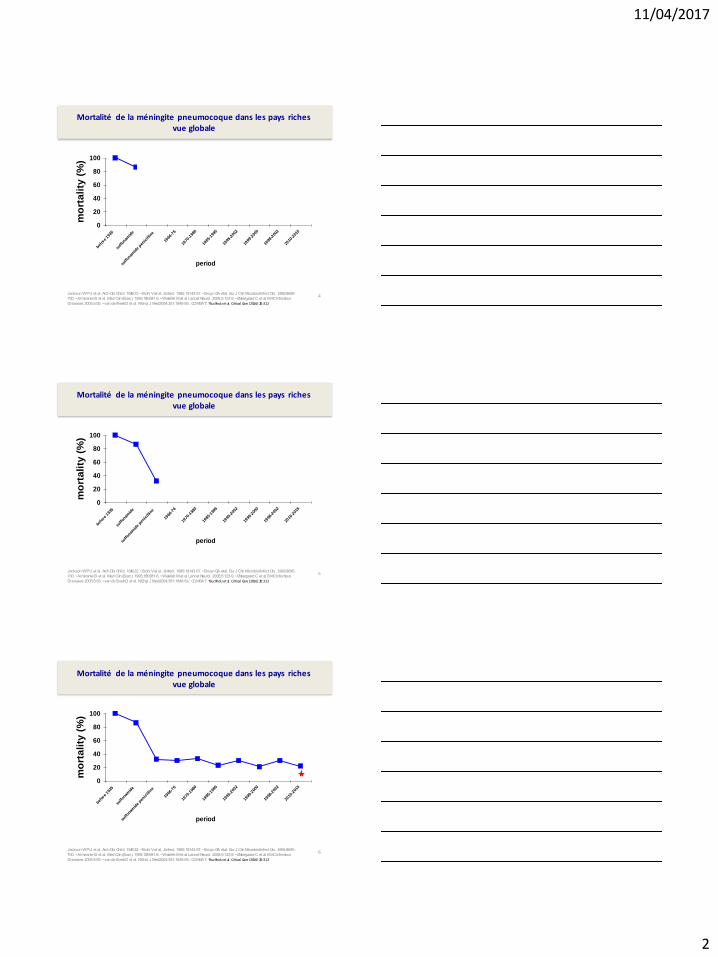
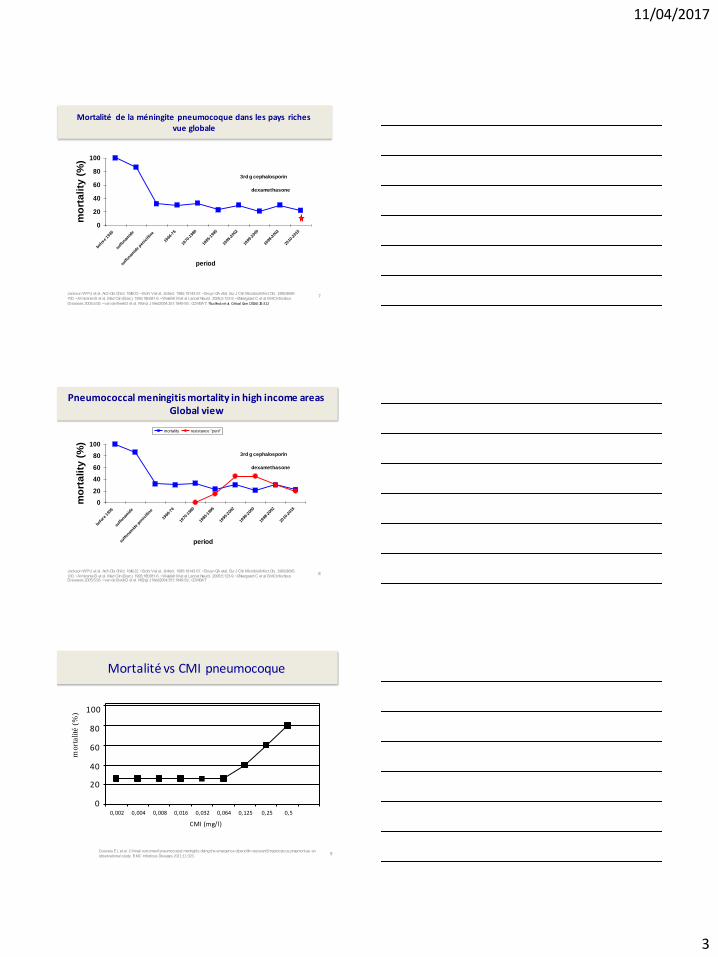
Mortalité de la méningite pneumocoque dans les pays riches vue globale
Jackson WPU et al. Arch Dis Child. 1949:22. • Bohr V et al, J Infect. 1985;10:143-57. • Bruyn GA et al. Eur J Clin Microbiol Infect Dis. 1989;8:695-
700. • Almirante B et al. Med Clin (Barc). 1995;105:681-6. • Weisfelt M et al. Lancet Neurol. 2006;5:123-9. • Østergaard C et al. BMC Infectious
Diseases 2005;5:93. • van de Beek D et al. N Engl J Med 2004;351:1849-59.; COMBAT; *Buchholz et al. Critical Care (2016) 20:312
0
20
40
60
80
100
befor
e 193
5
sulfo
namid
e
sulfo
namid
e pen
icill
ine
1966
-76
1970
-198
0
1985
-199
5
1995
-200
2
1999
-200
0
1998
-200
2
2010
-201
5
period
mo
rta
lity
(%
)
3rd g cephalosporin
dexamethasone
5
Mortalité de la méningite pneumocoque dans les pays riches vue globale
Jackson WPU et al. Arch Dis Child. 1949:22. • Bohr V et al, J Infect. 1985;10:143-57. • Bruyn GA et al. Eur J Clin Microbiol Infect Dis. 1989;8:695-
700. • Almirante B et al. Med Clin (Barc). 1995;105:681-6. • Weisfelt M et al. Lancet Neurol. 2006;5:123-9. • Østergaard C et al. BMC Infectious
Diseases 2005;5:93. • van de Beek D et al. N Engl J Med 2004;351:1849-59.; COMBAT; *Buchholz et al. Critical Care (2016) 20:312
0
20
40
60
80
100
befor
e 193
5
sulfo
namid
e
sulfo
namid
e pen
icill
ine
1966
-76
1970
-198
0
1985
-199
5
1995
-200
2
1999
-200
0
1998
-200
2
2010
-201
5
period
mo
rta
lity
(%
)
3rd g cephalosporin
dexamethasone
6
Mortalité de la méningite pneumocoque dans les pays riches vue globale
Jackson WPU et al. Arch Dis Child. 1949:22. • Bohr V et al, J Infect. 1985;10:143-57. • Bruyn GA et al. Eur J Clin Microbiol Infect Dis. 1989;8:695-
700. • Almirante B et al. Med Clin (Barc). 1995;105:681-6. • Weisfelt M et al. Lancet Neurol. 2006;5:123-9. • Østergaard C et al. BMC Infectious
Diseases 2005;5:93. • van de Beek D et al. N Engl J Med 2004;351:1849-59.; COMBAT; *Buchholz et al. Critical Care (2016) 20:312
0
20
40
60
80
100
befor
e 193
5
sulfo
namid
e
sulfo
namid
e pen
icill
ine
1966
-76
1970
-198
0
1985
-199
5
1995
-200
2
1999
-200
0
1998
-200
2
2010
-201
5
period
mo
rta
lity
(%
)
3rd g cephalosporin
dexamethasone
11/04/2017
3
7
Mortalité de la méningite pneumocoque dans les pays riches vue globale
Jackson WPU et al. Arch Dis Child. 1949:22. • Bohr V et al, J Infect. 1985;10:143-57. • Bruyn GA et al. Eur J Clin Microbiol Infect Dis. 1989;8:695-
700. • Almirante B et al. Med Clin (Barc). 1995;105:681-6. • Weisfelt M et al. Lancet Neurol. 2006;5:123-9. • Østergaard C et al. BMC Infectious
Diseases 2005;5:93. • van de Beek D et al. N Engl J Med 2004;351:1849-59.; COMBAT; *Buchholz et al. Critical Care (2016) 20:312
0
20
40
60
80
100
befor
e 193
5
sulfo
namid
e
sulfo
namid
e pen
icill
ine
1966
-76
1970
-198
0
1985
-199
5
1995
-200
2
1999
-200
0
1998
-200
2
2010
-201
5
period
mo
rta
lity
(%
)
3rd g cephalosporin
dexamethasone
8
Pneumococcal meningitis mortality in high income areas Global view
Jackson WPU et al. Arch Dis Child. 1949:22. • Bohr V et al, J Infect. 1985;10:143-57. • Bruyn GA et al. Eur J Clin Microbiol Infect Dis. 1989;8:695-
700. • Almirante B et al. Med Clin (Barc). 1995;105:681-6. • Weisfelt M et al. Lancet Neurol. 2006;5:123-9. • Østergaard C et al. BMC Infectious Diseases 2005;5:93. • van de Beek D et al. N Engl J Med 2004;351:1849-59.; COMBAT
0
20
40
60
80
100
befor
e 193
5
sulfo
namid
e
sulfo
namid
e pen
icill
ine
1966
-76
1970
-198
0
1985
-199
5
1995
-200
2
1999
-200
0
1998
-200
2
2010
-201
5
period
mo
rta
lity
(%
)
mortality resistance "peni"
3rd g cephalosporin
dexamethasone
9
Mortalité vs CMI pneumocoque
Gouveia EL et al. Clinical outcome of pneumococcal meningitis during the emergence of pencillin-resistant Streptococcus pneumoniae: an
observational study. BMC Infectious Diseases 2011;11:323.
100
80
60
40
20
0
mort
alité
(%
)
0,002 0,004 0,008 0,016 0,032 0,064 0,125 0,25 0,5
CMI (mg/l)
11/04/2017
4
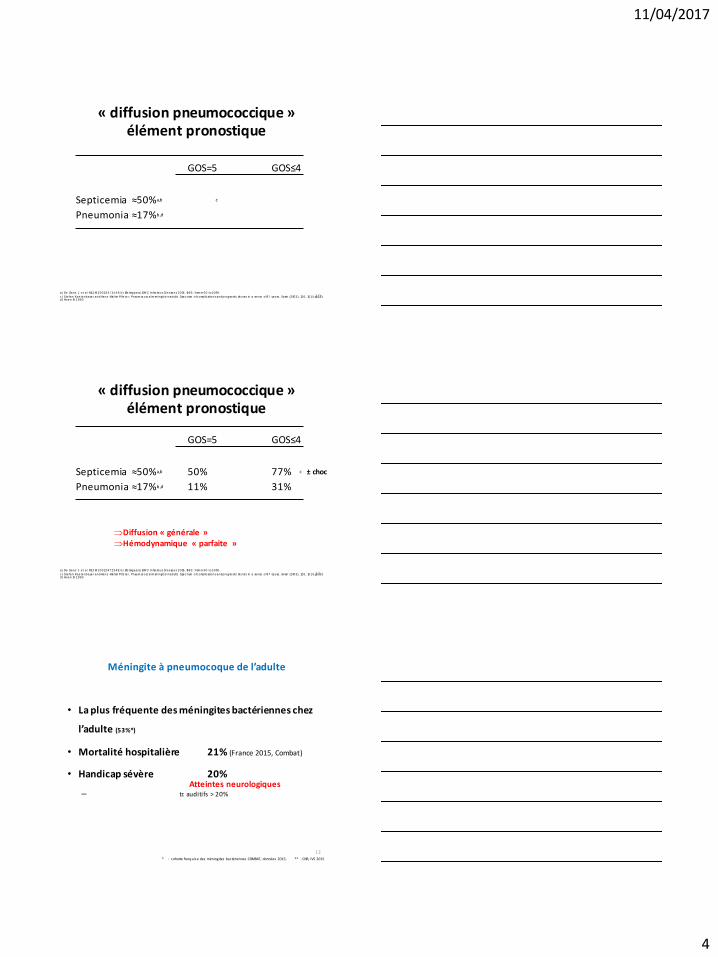
« diffusion pneumococcique » élément pronostique
GOS=5 GOS≤4
Septicemia ≈50%a,b c
Pneumonia ≈17%b,d
10 a) De Gans J et a l NEJ M 2002;347:1549; b) Øs tergaard, BM C Infec tious Dis eas es 2005, 5 :93: from m 60 to 100%
c ) Stefan Kas tenbauer and Hans -Wal ter P®s ter, Pneum oc occ al m eningi tis in adults Spec trum of c ompl ic ations and prognos tic fac tors in a series of 87 cas es , Bra in (2003), 126, 1015 ±1025 d) Hoen B 1993
« diffusion pneumococcique » élément pronostique
GOS=5 GOS≤4
Septicemia ≈50%a,b 50% 77% c
Pneumonia ≈17%b,d 11% 31%
11 a) De Gans J et a l NEJ M 2002;347:1549; b) Øs tergaard, BM C Infec tious Dis eas es 2005, 5 :93: from m 60 to 100%
c ) Stefan Kas tenbauer and Hans -Wal ter P®s ter, Pneum oc occ al m eningi tis in adults Spec trum of c ompl ic ations and prognos tic fac tors in a series of 87 cas es , Bra in (2003), 126, 1015 ±1025 d) Hoen B 1993
± choc
Diffusion « générale » Hémodynamique « parfaite »
Méningite à pneumocoque de l’adulte
• La plus fréquente des méningites bactériennes chez
l’adulte (53%*)
• Mortalité hospitalière 21% (France 2015, Combat)
• Handicap sévère 20%
– tr. auditifs > 20%
* : cohorte française des méningites bactériennes COMBAT, données 2015; ** : CNR, IVS 2015
12
Atteintes neurologiques
11/04/2017
5
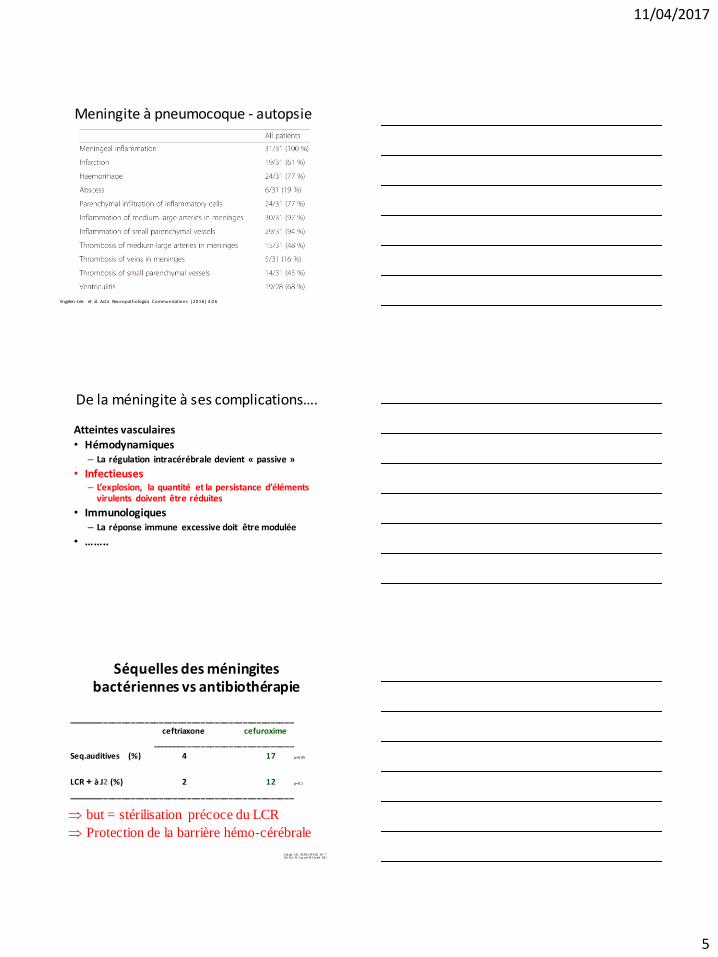
Meningite à pneumocoque - autopsie
Engelen-Lee et al. Acta Neuropathologica Communications (2016) 4:26
De la méningite à ses complications….
Atteintes vasculaires • Hémodynamiques
– La régulation intracérébrale devient « passive »
• Infectieuses – L’explosion, la quantité et la persistance d’éléments
virulents doivent être réduites
• Immunologiques – La réponse immune excessive doit être modulée
• ……..
Séquelles des méningites bactériennes vs antibiothérapie
_________________________________________________
ceftriaxone cefuroxime
_______________________________
Seq.auditives (%) 4 17 p=0.05
LCR + à J2 (%) 2 12 p=0.1
_________________________________________________
Sch aad UB, NEJM 1 99 0;322 :141 -7 Del Rio M Lan cet 1 98 3; Ju ne4 :124 1
but = stérilisation précoce du LCR
Protection de la barrière hémo-cérébrale
11/04/2017
6
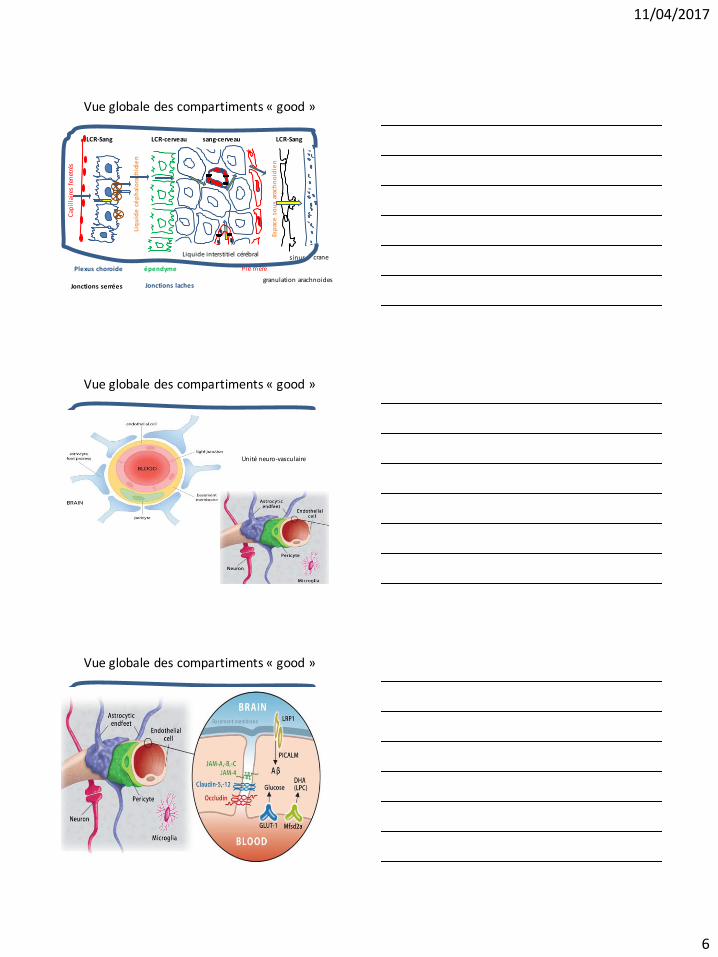
Vue globale des compartiments « good »
Liq
uid
e c
ép
hal
ora
chid
ien
LCR-Sang LCR-cerveau sang-cerveau
Plexus choroide épendyme Pie mère
granulation arachnoides
sinus crane
Cap
illa
ires
fen
etré
s
Jonctions laches Jonctions serrées
Esp
ace
so
us
arac
hn
oid
ien
Liquide interstitiel cérébral
LCR-Sang
Vue globale des compartiments « good »
Liq
uid
e c
ép
hal
ora
chid
ien
LCR-Sang LCR-cerveau sang-cerveau
Plexus choroide épendyme Pie mère
granulation arachnoides
sinus crane
Cap
illa
ires
fen
etré
s
Jonctions laches Jonctions serrées
Esp
ace
so
us
arac
hn
oid
ien
Liquide interstitiel cérébral
LCR-Sang
Unité neuro-vasculaire
Unité neuro-vasculaire
Vue globale des compartiments « good »
Liq
uid
e c
ép
hal
ora
chid
ien
LCR-Sang LCR-cerveau sang-cerveau
Plexus choroide épendyme Pie mère
granulation arachnoides
sinus crane
Cap
illa
ires
fen
etré
s
Jonctions laches Jonctions serrées
Esp
ace
so
us
arac
hn
oid
ien
Liquide interstitiel cérébral
LCR-Sang
Unité neuro-vasculaire
Unité neuro-vasculaire
11/04/2017
7
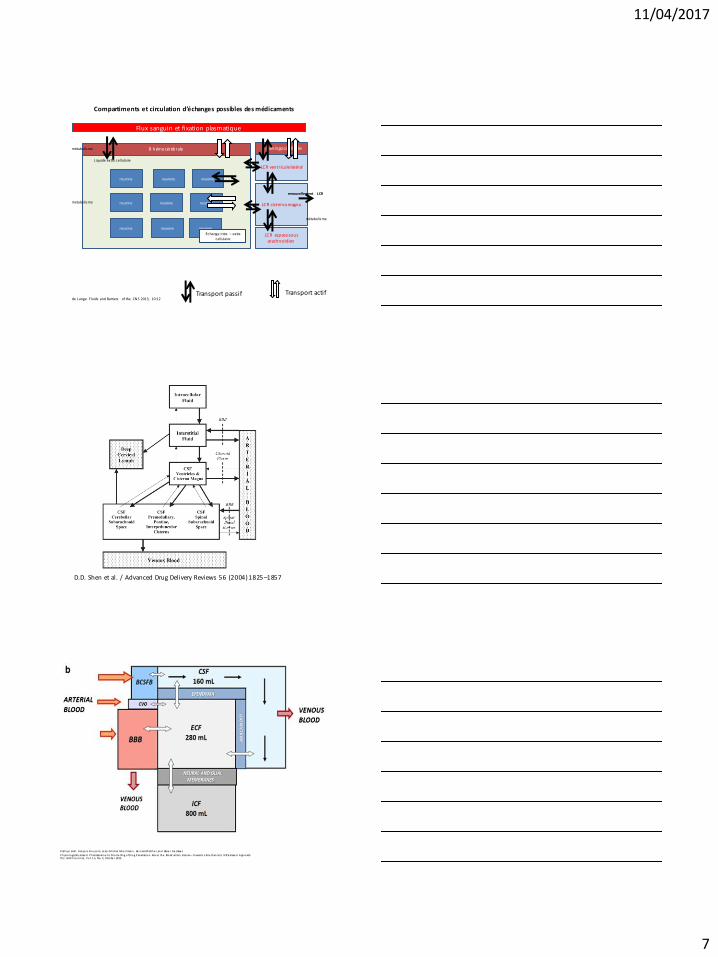
Compartiments et circulation d’échanges possibles des médicaments
de Lange Fluids and Barriers of the CNS 2013, 10:12
B méningocérébrale
LCR ventricule latéral
LCR cisterna magna
LCR espace sous arachnoidien
Flux sanguin et fixation plasmatique
Transport passif Transport actif
renouvellement LCR
métabolisme
neurone neurone neurone
neurone neurone neurone
neurone neurone neurone
B hémocérébrale
Liquide extra cellulaire
métabolisme
métabolisme
Échange intra – extra cellulaire
D.D. Shen et al. / Advanced Drug Delivery Reviews 56 (2004) 1825 –1857
K ath ryn B al l , Fran ço is B o u zo m, Je an -M ich el Sch e rrman n , Be rn ard Walth e r, an d Xavie r De clève s
P h ysio lo gical ly B ase d P h armaco kin e tic M o d e l lin g o f Dru g P en etratio n Acro ss th e Blo od –B rain B arrier—To ward s a M e ch an istic IVIVE-B ase d App ro ach Th e AAP S Jo u rn al , Vo l . 1 5, No. 4, Octo be r 20 13
11/04/2017
8
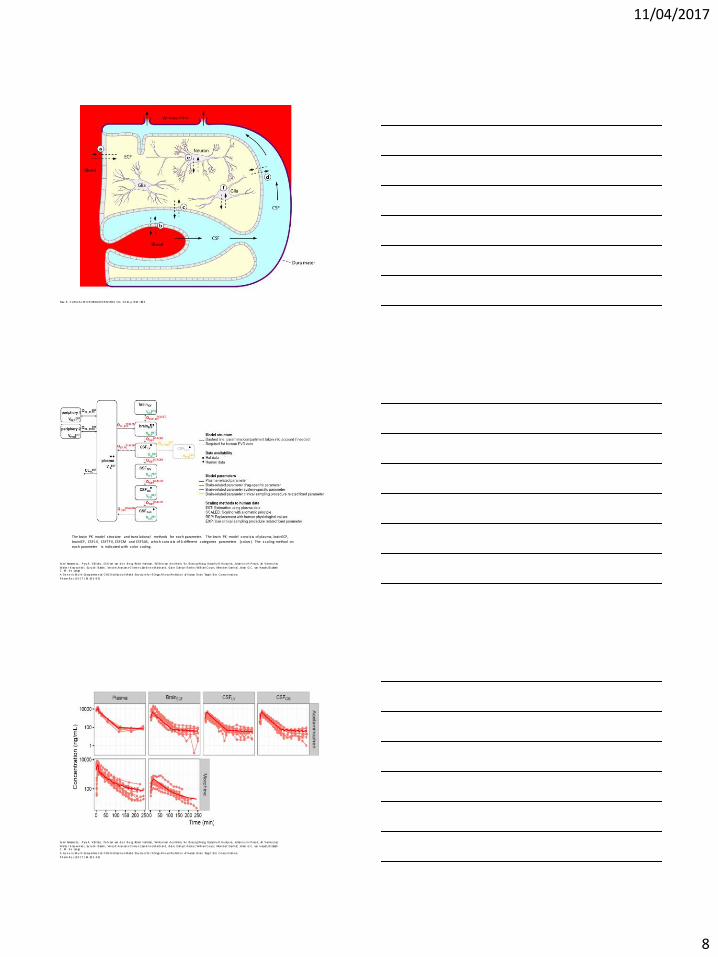
Nau R . C LINIC AL M IC R OB IOLOGY R EVIEWS, Oct. 2 0 10 , p . 8 58 – 88 3
Yu mi Yamamo to , P yry A. Väl i talo , Dirk-Jan van d e n B e rg, Ro b in Hartman , Wi l le m van d e n B rin k, Yin Ch eo n g Won g, Dymp h y R . Hu ntje ns, Jo han n e s H. P roo st, An Verme u len,
Walte r K rau win ke l , Su ru ch i B aksh i , V in ce nt Aran zan a-C l ime n t, San d rin e M arch an d , Clai re Dah yo t-Fize lie r, Wi ll iam C o ue t, Me in d ert Dan h of, Jo han G. C . van Hassel t, El i zabeth C . M . d e Lan ge
A Ge n e ric M u lti -Co mp artme n tal C NS Distribu tio n M od el Stru ctu re fo r 9 Drugs Al lo ws Pre d ictio n of Human B rain Targe t Si te C o nce n tratio ns
P h arm R e s (2 0 1 7 ) 34 :33 3 –3 51
The brain PK model s tructure and trans lational methods for each parameter. The brain PK model cons is ts of plasma, brainECF, brainICF, CSFLV, CSFTFV, CSFCM and CSFSAS, which cons is ts of 4 different categories parameters (colors ). The scaling method on each parameter is indicated with color coding.
Yu mi Yamamo to , P yry A. Väl i talo , Dirk-Jan van d e n B e rg, Ro b in Hartman , Wi l le m van d e n B rin k, Yin Ch eo n g Won g, Dymp h y R . Hu ntje ns, Jo han n e s H. P roo st, An Verme u len,
Walte r K rau win ke l , Su ru ch i B aksh i , V in ce nt Aran zan a-C l ime n t, San d rin e M arch an d , Clai re Dah yo t-Fize lie r, Wi ll iam C o ue t, Me in d ert Dan h of, Jo han G. C . van Hassel t, El i zabeth C . M . d e Lan ge
A Ge n e ric M u lti -Co mp artme n tal C NS Distribu tio n M od el Stru ctu re fo r 9 Drugs Al lo ws Pre d ictio n of Human B rain Targe t Si te C o nce n tratio ns
P h arm R e s (2 0 1 7 ) 34 :33 3 –3 51
11/04/2017
9
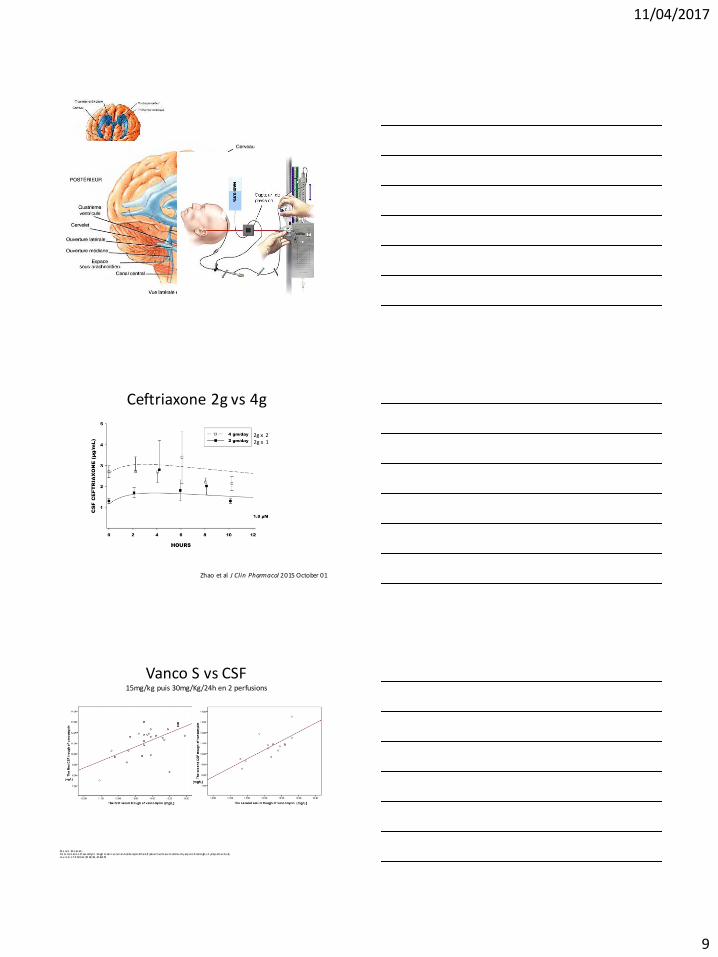
Ceftriaxone 2g vs 4g
Zhao et al J Clin Pharmacol 2015 October 01
2g x 1 2g x 2
Vanco S vs CSF 15mg/kg puis 30mg/Kg/24h en 2 perfusions
Sh e rvin Sh o ko uh i De te rmin atio n of van comycin tro ugh le vel in se rum an d cereb rosp in al fluid of patien ts with acu te commu n ity-acq u ire d men in gitis: A prosp ective stu dy Jo u rn al o f In fection (20 14) 69 , 42 4e4 29
11/04/2017
10
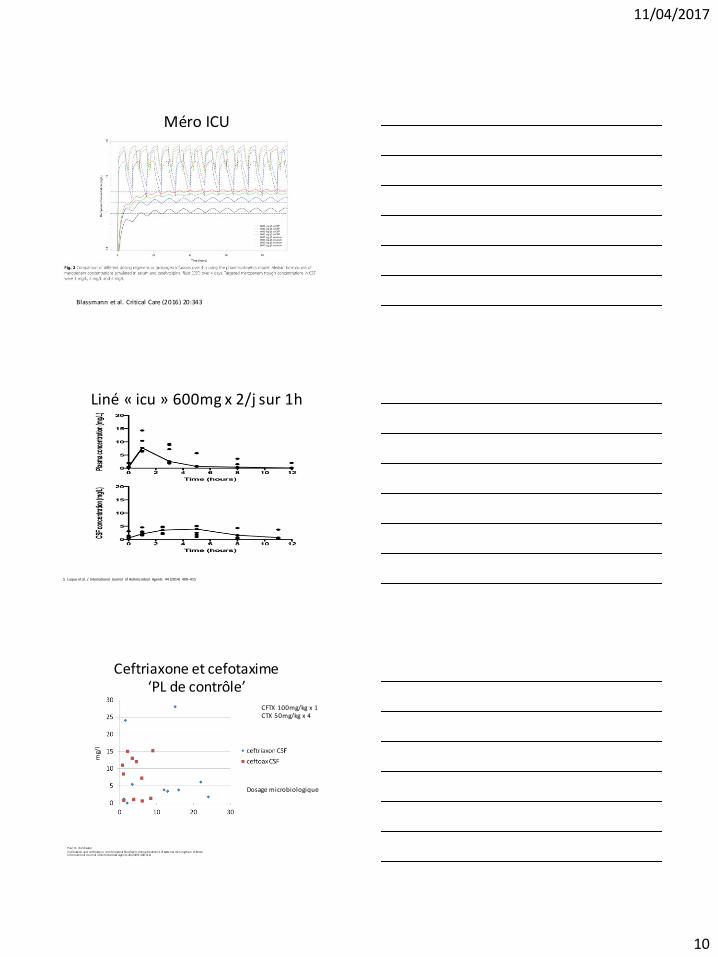
Méro ICU
Blassmann et al. Critical Care (2016) 20:343
Liné « icu » 600mg x 2/j sur 1h
S. Luque et al. / International Journal of Antimicrobial Agents 44 (2014) 409–415
Ceftriaxone et cefotaxime ‘PL de contrôle’
Dosage microbiologique
P au l N. Go ld wate r
C e fo taxime an d ce ftriaxo n e ce re b ro spin al flu id leve ls d urin g tre atme n t of bacte rial me n in gitis in ch ild ren In te rn atio n al Jo u rn al o f An timicro b ial Age n ts 26 (2 00 5) 4 08 –4 11
mg/
l
CFTX 100mg/kg x 1 CTX 50mg/kg x 4
11/04/2017
11
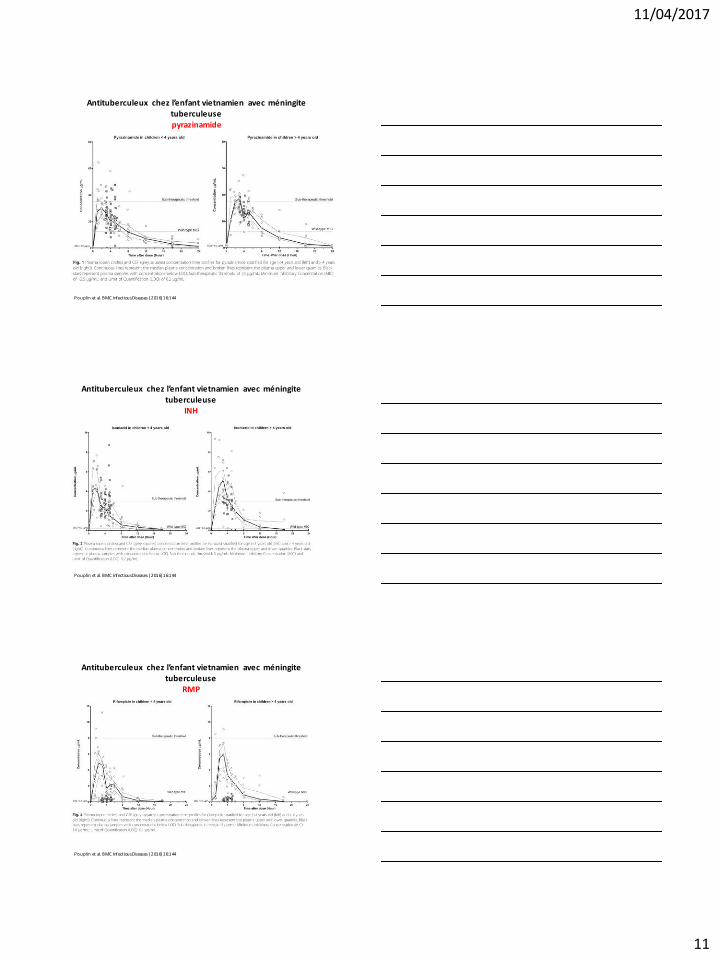
Antituberculeux chez l’enfant vietnamien avec méningite tuberculeuse pyrazinamide
Pouplin et al. BMC Infectious Diseases (2016) 16:144
Antituberculeux chez l’enfant vietnamien avec méningite tuberculeuse
INH
Pouplin et al. BMC Infectious Diseases (2016) 16:144
Antituberculeux chez l’enfant vietnamien avec méningite tuberculeuse
RMP
Pouplin et al. BMC Infectious Diseases (2016) 16:144
11/04/2017
12
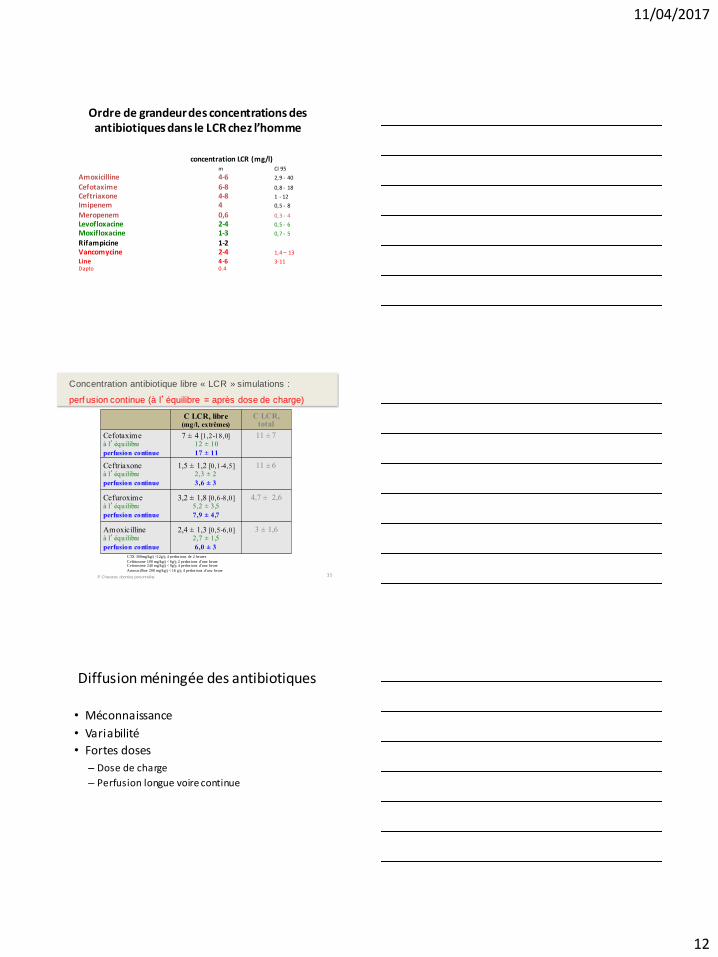
Ordre de grandeur des concentrations des antibiotiques dans le LCR chez l’homme
concentration LCR (mg/l) m CI 95
Amoxicilline 4-6 2,9 - 40 Cefotaxime 6-8 0,8 - 18
Ceftriaxone 4-8 1 - 12
Imipenem 4 0,5 - 8
Meropenem 0,6 0,3 - 4
Levofloxacine 2-4 0,5 - 6
Moxifloxacine 1-3 0,7 - 5
Rifampicine 1-2 Vancomycine 2-4 1,4 – 13
Line 4-6 3-11 Dapto 0.4
35
C LCR, libre (mg/l, extrêmes)
C LCR, total
Cefotaxime à l’équilibre
perfusion continue
7 ± 4 [1,2-18,0]
12 ± 10
17 ± 11
11 ± 7
Ceftriaxone à l’équilibre
perfusion continue
1,5 ± 1,2 [0,1-4,5]
2,3 ± 2
3,6 ± 3
11 ± 6
Cefuroxime à l’équilibre
perfusion continue
3,2 ± 1,8 [0,6-8,0]
5,2 ± 3,5
7,9 ± 4,7
4,7 ± 2,6
Amoxicilline à l’équilibre
perfusion continue
2,4 ± 1,3 [0,5-6,0]
2,7 ± 1,5
6,0 ± 3
3 ± 1,6
P Chavanet, données personnelles
Concentration antibiotique libre « LCR » simulations :
perf usion continue (à l’équilibre = après dose de charge)
CTX 300mg/kg/j <12g/j; 4 perfus ions de 2 heures
Ceftriaxone 100 mg/kg/j < 6g/j; 2 perfus ions d’une heure Cefuroxime 240 mg/kg/j < 9g/j; 4 perfus ions d’une heure
Amoxicilline 200 mg/kg/j < 16 g/j; 4 perfus ions d’une heure
Diffusion méningée des antibiotiques
• Méconnaissance
• Variabilité
• Fortes doses
– Dose de charge
– Perfusion longue voire continue
11/04/2017
13
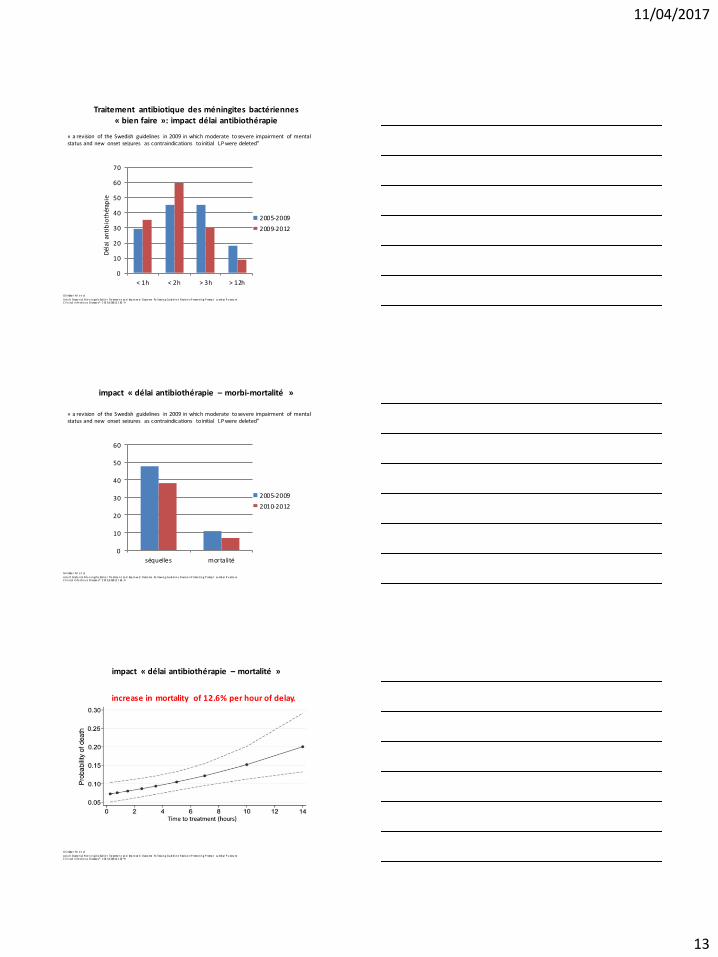
Traitement antibiotique des méningites bactériennes « bien faire »: impact délai antibiothérapie
Gl imåke r M e t al
Ad u lt B acte rial M e n in gitis: Earl ie r Tre atme n t an d Imp ro ve d Outco me Fo l lowin g Gu id el in e R evisio n P romo tin g P romp t Lu mb ar P u nctu re C l in ical In fe ctio u s Disease s® 2 01 5;6 0(8 ):1 1 62 –9
« a revision of the Swedish guidelines in 2009 in which moderate to severe impairment of mental status and new onset seizures as contraindications to initial LP were deleted”
0
10
20
30
40
50
60
70
< 1h < 2h > 3h > 12h
2005-2009
2009-2012
Dél
ai a
nti
bio
thér
apie
impact « délai antibiothérapie – morbi-mortalité »
Gl imåke r M e t al
Ad u lt B acte rial M e n in gitis: Earl ie r Tre atme n t an d Imp ro ve d Outco me Fo l lowin g Gu id el in e R evisio n P romo tin g P romp t Lu mb ar P u nctu re C l in ical In fe ctio u s Disease s® 2 01 5;6 0(8 ):1 1 62 –9
0
10
20
30
40
50
60
séquelles mortalité
2005-2009
2010-2012
« a revision of the Swedish guidelines in 2009 in which moderate to severe impairment of mental status and new onset seizures as contraindications to initial LP were deleted”
impact « délai antibiothérapie – mortalité »
Gl imåke r M e t al
Ad u lt B acte rial M e n in gitis: Earl ie r Tre atme n t an d Imp ro ve d Outco me Fo l lowin g Gu id el in e R evisio n P romo tin g P romp t Lu mb ar P u nctu re C l in ical In fe ctio u s Disease s® 2 01 5;6 0(8 ):1 1 62 –9
increase in mortality of 12.6% per hour of delay.
11/04/2017
14
Antibiotiques et méningites
• Bien prescrire oui !
• Sans délai
• Un médicament a des chances – d’être utile
– s’il est administré !