
ANALYSE BACTERIOLOGIQUE QUANTITATIVE ET QUALITATIVE ...
13
ANALYSE BACTERIOLOGIQUE QUANTITATIVE ET QUALITATIVE DE BIOPSIES OSSEUSES DE PIEDS DIABETIQUES ET RECHERCHE DES FACTEURS DE PATHOGENICITE Florence BAUDOUX Diabétologue CHRU de Lille 04 octobre 2011
Transcript of ANALYSE BACTERIOLOGIQUE QUANTITATIVE ET QUALITATIVE ...
ANALYSE BACTERIOLOGIQUE QUANTITATIVE ET QUALITATIVE DE BIOPSIES OSSEUSES DE PIEDS DIABETIQUESET RECHERCHE DES FACTEURS DE PATHOGENICITE
Florence BAUDOUXDiabétologue CHRU de Lille04 octobre 2011
Pourquoi s’intéresser à l’ostéite dans l’infection du pied diabétique?L’infection osseuse complique 1 /3 à 2/3 des
plaies chroniques du pied
36% des patients qui ont une ostéite subissent une amputation durant le suivi.
68% des patients qui ont subi une amputation seront amputés une seconde fois dans les 5 ans;
Mortalité dans les 5 ans suivant l’amputation initiale est de 50%.
Ramsey, S.D. et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care 22, 382 -387 (1999).Goldner MG. The fate of the second leg in the diabetic amputee. Diabetes 1960;9:100-3Whitehouse, F.W., Jurgensen, C. & Block, M.A. The later life of the diabetic amputee. Another look at fate of the second leg. Diabetes 17, 520-521 (1968).
Objectifs de l’étude Caractériser la microbiologie de
l’ostéite du pied diabétiqueQuantitéQualité
Caractériser l’organisation des bactéries dans l’os
Caractériser les staphylocoquesCapacité d’adhérenceCapacité à créer un biofilm
Matériel et méthodeEtude prospective réalisée entre
février 2010 à mai 2011.
Tout patient diabétique présentant une ostéite du pied nécessitant une biopsie osseuse et/ou une amputation.Ostéite prouvée par clinique + radio ou
IRM
Laboratoire de bacteriologie clinique, Faculté de Pharmacie U995
Centre hospitalier de TourcoingHôpital Claude Huriez, CHRU Lille
Université Lille 1
2 à 3 biopsies osseuses
1 à 2 biopsies Quantitatif , qualitatif 1 biopsie
MEB
n= 38 prélèvements ; 35 patients65,8% d’hommes 89.4% diabétiques de type II âge moyen 65 ans.55% chirurgie orthopédique du CH de
Tourcoing 33% étaient conclus stériles (n=7) par le
laboratoire de routine.45% chirurgie vasculaire du CHRU de
Lille. 23% étaient conclus stériles (n=4).
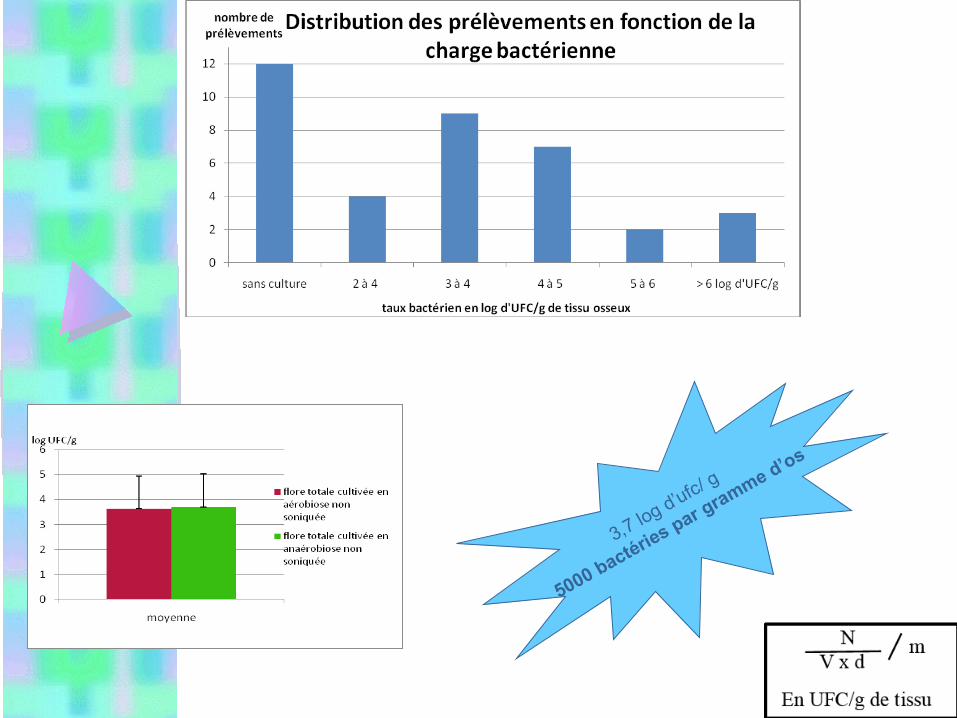
3,7 log d’ufc/ g
5000 bactéries par gramme d’os
Bactérie identifiée dans l’ostéite nb
Cocci Gram+ Staphylococcus aureus 12
Staphylococcus capitis 2
Staphylococcus caprae 2
Staphylococcus epidermidis 9
Staphylococcus lugdunensis 2
Staphylococcus pettenkoferi 2
Staphylococcus sciuri 1
Staphylococcus simulans 1
Staphylococcus warneri 2
Staphylococcus sp 1
Micrococcus luteus 1
Micrococcus sp 1
Streptococcus agalactiae 1
Enterococcus faecalis 5
Enterococcus faecium 1
Bacille Gram+ Corynebacterium 10
Dermabacter hominis 2
Bacille Gram -Entérobactérie
Citrobacter diversus 1
Enterobacter cloacae 3
Escherichia coli 2
Serratia liquefaciens 1
Serratia marcescens 2
Proteus mirabilis 3
Providencia rettgeri 1
Morganella morganii 1
Autres BGN Pseudomonas aeruginosa 1
Anaérobie Anaerococcus prevotii 1
Finegoldia magna 2
Propionibacterium acnes 2
Veillonella 2
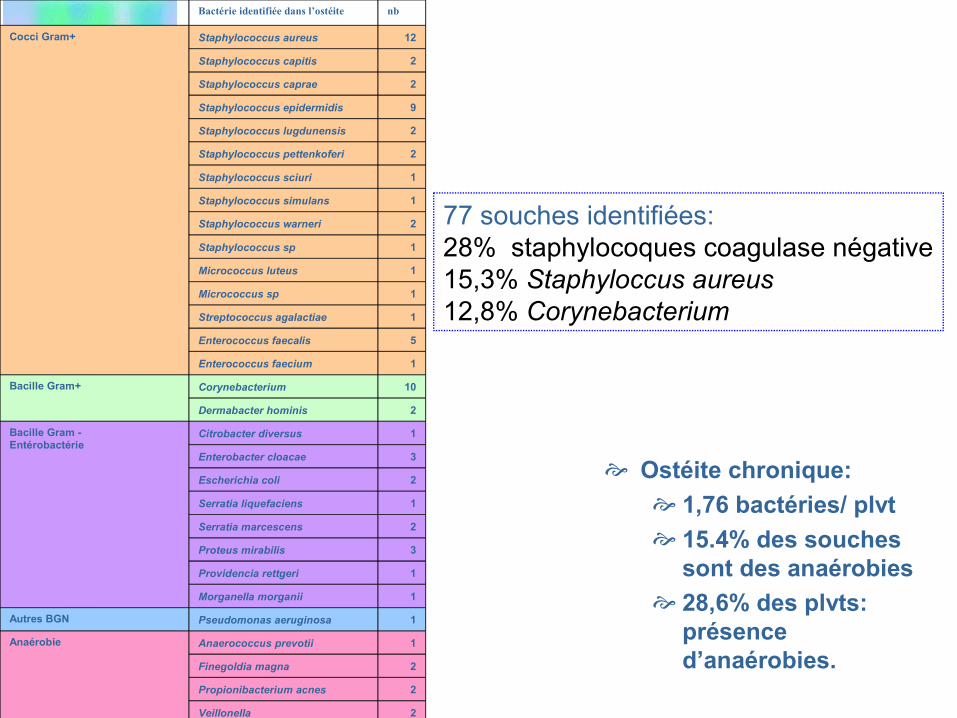
77 souches identifiées:28% staphylocoques coagulase négative15,3% Staphyloccus aureus 12,8% Corynebacterium
Ostéite chronique: 1,76 bactéries/ plvt 15.4% des souches
sont des anaérobies 28,6% des plvts:
présence d’anaérobies.
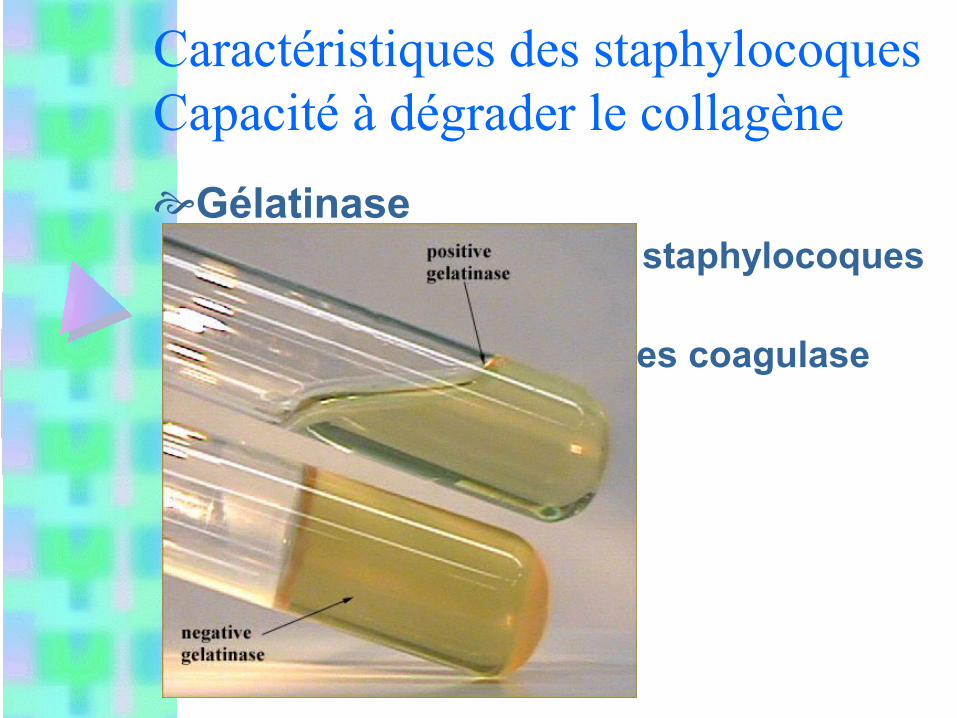
Caractéristiques des staphylocoquesCapacité à dégrader le collagèneGélatinase
Exprimée par 58% des staphylocoques11/12 des S.aureus8/22 des staphylocoques coagulase
négative
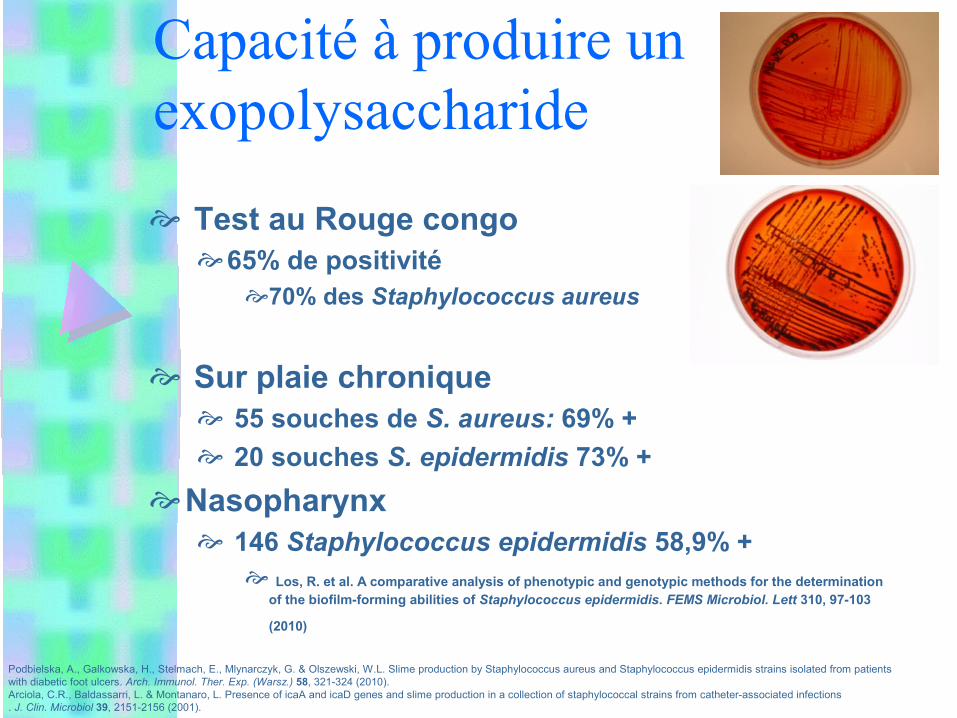
Capacité à produire un exopolysaccharide
Test au Rouge congo65% de positivité
70% des Staphylococcus aureus
Sur plaie chronique 55 souches de S. aureus: 69% + 20 souches S. epidermidis 73% +
Nasopharynx 146 Staphylococcus epidermidis 58,9% +
Los, R. et al. A comparative analysis of phenotypic and genotypic methods for the determination of the biofilm-forming abilities of Staphylococcus epidermidis. FEMS Microbiol. Lett 310, 97-103
(2010)
Podbielska, A., Galkowska, H., Stelmach, E., Mlynarczyk, G. & Olszewski, W.L. Slime production by Staphylococcus aureus and Staphylococcus epidermidis strains isolated from patients with diabetic foot ulcers. Arch. Immunol. Ther. Exp. (Warsz.) 58, 321-324 (2010).Arciola, C.R., Baldassarri, L. & Montanaro, L. Presence of icaA and icaD genes and slime production in a collection of staphylococcal strains from catheter-associated infections. J. Clin. Microbiol 39, 2151-2156 (2001).
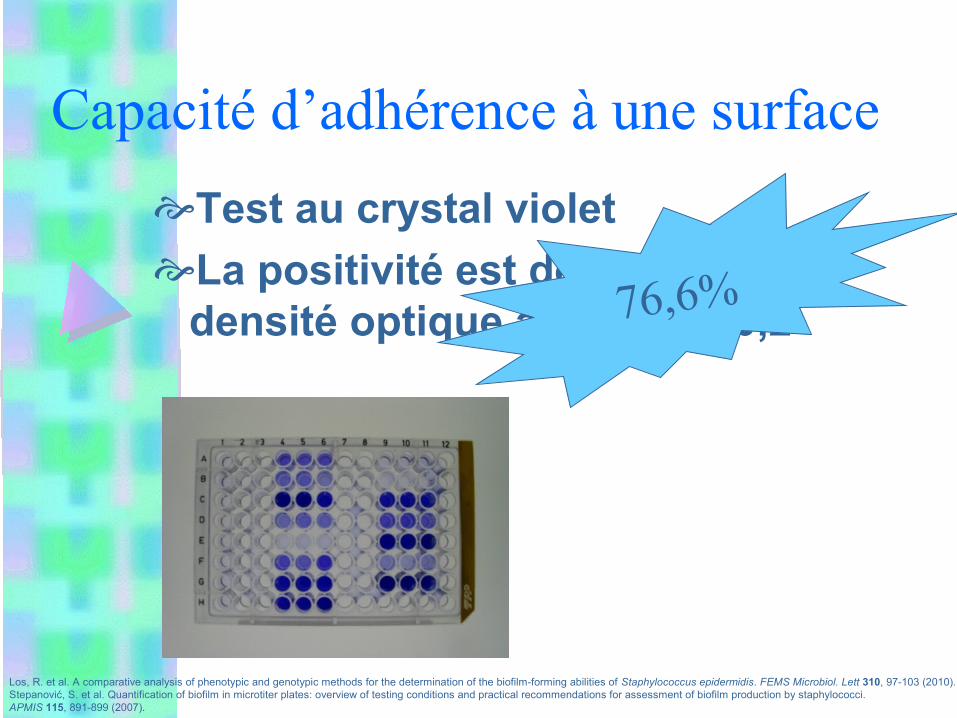
Capacité d’adhérence à une surfaceTest au crystal violetLa positivité est définie par une
densité optique à 570 nm >0,2
Los, R. et al. A comparative analysis of phenotypic and genotypic methods for the determination of the biofilm-forming abilities of Staphylococcus epidermidis. FEMS Microbiol. Lett 310, 97-103 (2010).Stepanović, S. et al. Quantification of biofilm in microtiter plates: overview of testing conditions and practical recommendations for assessment of biofilm production by staphylococci. APMIS 115, 891-899 (2007).
76,6%
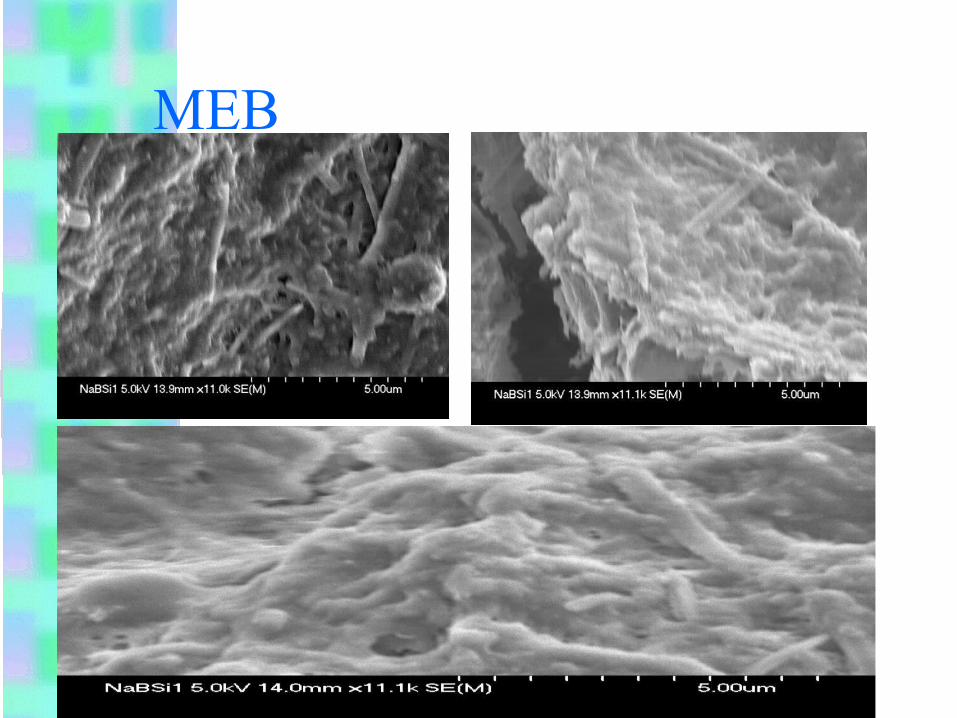
MEB
PerspectivesPoursuite de la collection
bactérienneEvaluation moléculaire Collaboration avec l’équipe du Dr.
Brad Spellberg of UCLA Evaluation en microscopie
électronique des biofilms formés sur disques de biocéramique.


















