Acquisitions récentes sur la physiologie et la génétique ... 2015 Vignes S..pdf · Acquisitions...
16
Acquisitions récentes sur la physiologie et la génétique des lymphœdèmes S. Vignes, Unité de Lymphologie, Hôpital Cognacq-Jay, Paris
Transcript of Acquisitions récentes sur la physiologie et la génétique ... 2015 Vignes S..pdf · Acquisitions...
Acquisitions récentes sur la physiologie et la génétique des
lymphœdèmes
S. Vignes, Unité de Lymphologie, Hôpital Cognacq-Jay, Paris
Qu’est ce que lymphœdème ?
C’est de la lymphe…
Physiopathologie
1. Stase lymphatique initiale 2. Mais très « rapidement » (jours,
semaines), transformation tissulaire…
Conséquences cliniques
• "Irréversibilité" des modifications tissulaires (fibrose)
• ↓ modeste du volume sous traitement
• ↓ relative de la composante liquidienne au profit de la composante tissulaire
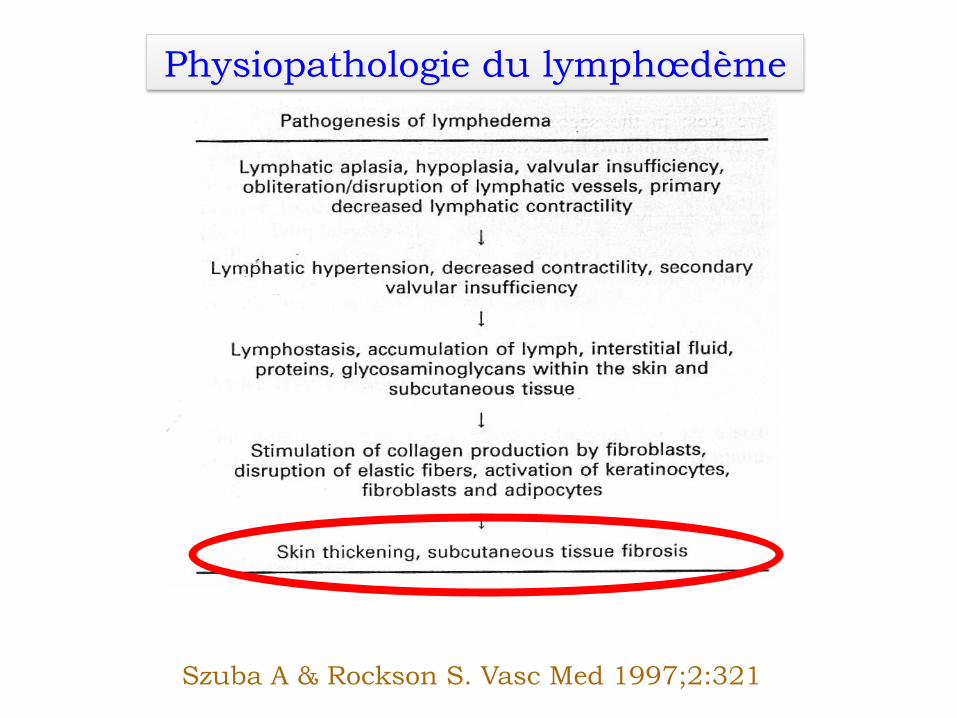
Szuba A & Rockson S. Vasc Med 1997;2:321
Physiopathologie du lymphœdème
Qu’est ce que lymphœdème ?
C’est d’abord de la peau et du tissu adipeux et… un peu de
lymphe (donc en grande partie irréversible et
chronique)
Pourquoi une femme a un lymphœdème après cancer du sein ? • Curage axillaire : 15% vs 6-8%
pour le ganglion sentinelle • Radiothérapie même ne
comprenant pas le creux axillaire • Obésité lors du cancer du sein
(IMC > 30 kg/m2), risque ≈ 4 • Mais les conseils classiques de
prévention (TA, piqûres…) ? DiSipio T et al. Lancet 2013;14:500 Ridner SH et al. Support Care Cancer 2011;19:853
Lifestyle Risk Factors Associated with Arm Swelling amongWomen with Breast Cancer
Shayna L. Showalter, MD1, Justin C. Brown, MA2, Andrea L. Cheville, MD3, Carla S. Fisher,MD1, Dahlia Sataloff, MD4, and Kathryn H. Schmitz, PhD, MPH2
1Department of Surgery, University of Pennsylvania, Philadelphia, PA 191042Center for Clinical Epidemiology and Biostatistics University of Pennsylvania, Philadelphia, PA191043Department of Physical Medicine and Rehabilitation, Mayo Clinic, Rochester, MN 559054Department of Surgery, Pennsylvania Hospital, Philadelphia, PA 19107
AbstractBackground—Breast cancer-related lymphedema (BCRL) is a feared complication for breastcancer patients who have undergone axillary surgery. Although clinical risk factors for BCRL aredefined; data are sparse regarding common exposures that might induce incident arm swelling.The goal of this study was to quantify the association between common exposures thought to bepotential risk factors, and the occurrence of incident arm swelling, among breast cancer survivorswith or at-risk for BCRL.
Methods—This is a prospective sub-analysis of the PAL trial, a randomized controlled trial of295 breast cancer survivors. Participants reported their exposure to 30 different potential risk-factors at three month intervals for one year. Incident arm swelling was defined as a ≥5% increasein inter-limb water volume difference between two consecutive time points.
Results—Twenty-seven participants (9%) experienced incident arm swelling and 268 patients(91%) did not. Sauna use was the only exposure that was significantly predictive of incident armswelling (p=0.05). Non-White and non-Black participants had a significantly increased risk forexperiencing incident arm swelling (p=0.005) for both comparisons.
Conclusions—In our patient cohort, many common exposures that have been reported to be riskfactors did not prove to have a significant predictive relationship for incident arm swelling. Thisstudy supports the recommendation that breast cancer patients who have had axillary surgeryshould avoid sauna use. The results do not confirm the need for other restrictions that mayinterfere with the quality of life in women with breast cancer.
INTRODUCTIONLymphedema is a chronic condition that results when inadequate lymphatic drainage leadsto the accumulation of protein-rich fluid in the interstitial space. Lymphedema is
Corresponding Author: Kathryn H. Schmitz, PhD, MPH 423 Guardian Drive 8th Floor Blockley Hall Philadelphia, Pennsylvania19104 Phone: (215) 898-6604, Fax: (215) 898-7392, [email protected].
NIH Public AccessAuthor ManuscriptAnn Surg Oncol. Author manuscript; available in PMC 2014 August 05.
Published in final edited form as:Ann Surg Oncol. 2013 March ; 20(3): 842–849. doi:10.1245/s10434-012-2631-9.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
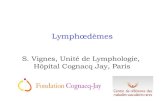
1. Etude prospective (cohorte PAL : Physical Activity Lymphedema)
2. Questionnaire sur 30 items (FDR potentiels) à 3, 6 et 12 mois
3. LO défini > 5% (volumétrie à eau) à 3, 6 et 12 mois
Et si le lymphœdème après cancer du sein avait une composante génétique ?
Lymphatic and Angiogenic Candidate Genes Predict theDevelopment of Secondary Lymphedema followingBreast Cancer SurgeryChristine Miaskowski1*, Marylin Dodd1, Steven M. Paul1, Claudia West1, Deborah Hamolsky2,
Gary Abrams3, Bruce A. Cooper4, Charles Elboim5, John Neuhaus6, Brian L. Schmidt7, Betty Smoot8,
Bradley E. Aouizerat9
1 Department of Physiological Nursing, University of California San Francisco, San Francisco, California, United States of America, 2 Department of Physiological Nursing,
Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America, 3 Department of Neurology,
University of California San Francisco, San Francisco, California, United States of America, 4 Department of Community Health Systems, University of California San
Francisco, San Francisco, California, United States of America, 5 Redwood Regional Medical Group, Santa Rosa, California, United States of America, 6 Department of
Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California, United States of America, 7 Department of Oral and Maxillofacial Surgery,
New York University, New York, New York, United States of America, 8 Department of Physical Therapy and Rehabilitation Science, University of California San Francisco,
San Francisco, California, United States of America, 9 Department of Physiological Nursing, Institute for Human Genetics, University of California San Francisco, San
Francisco, California, United States of America
Abstract
The purposes of this study were to evaluate for differences in phenotypic and genotypic characteristics in women who didand did not develop lymphedema (LE) following breast cancer treatment. Breast cancer patients completed a number ofself-report questionnaires. LE was evaluated using bioimpedance spectroscopy. Genotyping was done using a customgenotyping array. No differences were found between patients with (n = 155) and without LE (n = 387) for the majority ofthe demographic and clinical characteristics. Patients with LE had a significantly higher body mass index, more advanceddisease and a higher number of lymph nodes removed. Genetic associations were identified for four genes (i.e., lymphocytecytosolic protein 2 (rs315721), neuropilin-2 (rs849530), protein tyrosine kinase (rs158689), vascular cell adhesion molecule 1(rs3176861)) and three haplotypes (i.e., Forkhead box protein C2 (haplotype A03), neuropilin-2 (haplotype F03), vascularendothelial growth factor-C (haplotype B03)) involved in lymphangiogensis and angiogenesis. These genetic associationssuggest a role for a number of lymphatic and angiogenic genes in the development of LE following breast cancer treatment.
Citation: Miaskowski C, Dodd M, Paul SM, West C, Hamolsky D, et al. (2013) Lymphatic and Angiogenic Candidate Genes Predict the Development of SecondaryLymphedema following Breast Cancer Surgery. PLoS ONE 8(4): e60164. doi:10.1371/journal.pone.0060164
Editor: Robert Lafrenie, Sudbury Regional Hospital, Canada
Received February 1, 2013; Accepted February 21, 2013; Published April 16, 2013
Copyright: ! 2013 Miaskowski et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was funded by grants from the National Cancer Institute (CA107091 and CA118658) and the National Institute of Nursing Research(NR0101282). Dr. Miaskowski is an American Cancer Society Clinical Research Professor. Dr. Bradley Aouizerat was funded through the National Institutes of Health(NIH) Roadmap for Medical Research Grant (KL2 RR624130). This project was supported by NIH/NCRR UCSF-CTSI Grant Number UL1 RR024131. Its contents aresolely the responsibility of the authors and do not necessarily represent the official views of the NIH. The funders had no role in the study design, data collectionand analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Lymphedema (LE) following treatment for breast cancer is themost common form of LE in the industrialized world [1]. LE iscaused by a reduction in lymph transport capacity associated withthe cancer and its treatment (e.g., surgery, radiation therapy (RT),chemotherapy (CTX)) and results in the accumulation of protein-rich fluid in the interstitial space. LE results in disfigurement,discomfort, and functional impairments. In addition, LE mayprecipitate cellulitis and lymphangitis [2].
The exact prevalence of LE in breast cancer survivors isunknown with estimates ranging from 3% to 87% [3]. This widevariation is due to differences in measurement methods, inconsis-tencies in diagnostic criteria, as well as variations in samplecharacteristics, timing of measurements, and duration of follow-up. However, as noted by Armer [3], if the incidence of LE is
conservatively set at 20%, more than 500,000 breast cancersurvivors in the United States are affected by this condition.
One of the major goals of LE research is the identification ofwomen at greatest risk for the development of this conditionfollowing breast cancer treatment. Risk factors evaluated in themajority of studies done to date focused on patient, disease, andtreatment characteristics. However, in four large scale prospectivecohort studies [4–7], the factors associated with increased risk forLE were not concordant. In a study of 1,287 women (104 werediagnosed with LE) [5], risk factors for LE included: higher stageof disease, increased number of lymph nodes removed, removal oftumor positive nodes, receipt of adjuvant CTX, higher body massindex (BMI), and poorer health status. In a second study of 997women (133 had LE) [4], risk factors for LE included: beingAfrican American, being better educated, higher stage of disease,and removal of at least one lymph node. In a population-basedsample of 631 women (237 had LE) [6], hazard ratios for the
PLOS ONE | www.plosone.org 1 April 2013 | Volume 8 | Issue 4 | e60164
Lymphatic and Angiogenic Candidate Genes Predict theDevelopment of Secondary Lymphedema followingBreast Cancer SurgeryChristine Miaskowski1*, Marylin Dodd1, Steven M. Paul1, Claudia West1, Deborah Hamolsky2,
Gary Abrams3, Bruce A. Cooper4, Charles Elboim5, John Neuhaus6, Brian L. Schmidt7, Betty Smoot8,
Bradley E. Aouizerat9
1 Department of Physiological Nursing, University of California San Francisco, San Francisco, California, United States of America, 2 Department of Physiological Nursing,
Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America, 3 Department of Neurology,
University of California San Francisco, San Francisco, California, United States of America, 4 Department of Community Health Systems, University of California San
Francisco, San Francisco, California, United States of America, 5 Redwood Regional Medical Group, Santa Rosa, California, United States of America, 6 Department of
Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California, United States of America, 7 Department of Oral and Maxillofacial Surgery,
New York University, New York, New York, United States of America, 8 Department of Physical Therapy and Rehabilitation Science, University of California San Francisco,
San Francisco, California, United States of America, 9 Department of Physiological Nursing, Institute for Human Genetics, University of California San Francisco, San
Francisco, California, United States of America
Abstract
The purposes of this study were to evaluate for differences in phenotypic and genotypic characteristics in women who didand did not develop lymphedema (LE) following breast cancer treatment. Breast cancer patients completed a number ofself-report questionnaires. LE was evaluated using bioimpedance spectroscopy. Genotyping was done using a customgenotyping array. No differences were found between patients with (n = 155) and without LE (n = 387) for the majority ofthe demographic and clinical characteristics. Patients with LE had a significantly higher body mass index, more advanceddisease and a higher number of lymph nodes removed. Genetic associations were identified for four genes (i.e., lymphocytecytosolic protein 2 (rs315721), neuropilin-2 (rs849530), protein tyrosine kinase (rs158689), vascular cell adhesion molecule 1(rs3176861)) and three haplotypes (i.e., Forkhead box protein C2 (haplotype A03), neuropilin-2 (haplotype F03), vascularendothelial growth factor-C (haplotype B03)) involved in lymphangiogensis and angiogenesis. These genetic associationssuggest a role for a number of lymphatic and angiogenic genes in the development of LE following breast cancer treatment.
Citation: Miaskowski C, Dodd M, Paul SM, West C, Hamolsky D, et al. (2013) Lymphatic and Angiogenic Candidate Genes Predict the Development of SecondaryLymphedema following Breast Cancer Surgery. PLoS ONE 8(4): e60164. doi:10.1371/journal.pone.0060164
Editor: Robert Lafrenie, Sudbury Regional Hospital, Canada
Received February 1, 2013; Accepted February 21, 2013; Published April 16, 2013
Copyright: ! 2013 Miaskowski et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was funded by grants from the National Cancer Institute (CA107091 and CA118658) and the National Institute of Nursing Research(NR0101282). Dr. Miaskowski is an American Cancer Society Clinical Research Professor. Dr. Bradley Aouizerat was funded through the National Institutes of Health(NIH) Roadmap for Medical Research Grant (KL2 RR624130). This project was supported by NIH/NCRR UCSF-CTSI Grant Number UL1 RR024131. Its contents aresolely the responsibility of the authors and do not necessarily represent the official views of the NIH. The funders had no role in the study design, data collectionand analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Lymphedema (LE) following treatment for breast cancer is themost common form of LE in the industrialized world [1]. LE iscaused by a reduction in lymph transport capacity associated withthe cancer and its treatment (e.g., surgery, radiation therapy (RT),chemotherapy (CTX)) and results in the accumulation of protein-rich fluid in the interstitial space. LE results in disfigurement,discomfort, and functional impairments. In addition, LE mayprecipitate cellulitis and lymphangitis [2].
The exact prevalence of LE in breast cancer survivors isunknown with estimates ranging from 3% to 87% [3]. This widevariation is due to differences in measurement methods, inconsis-tencies in diagnostic criteria, as well as variations in samplecharacteristics, timing of measurements, and duration of follow-up. However, as noted by Armer [3], if the incidence of LE is
conservatively set at 20%, more than 500,000 breast cancersurvivors in the United States are affected by this condition.
One of the major goals of LE research is the identification ofwomen at greatest risk for the development of this conditionfollowing breast cancer treatment. Risk factors evaluated in themajority of studies done to date focused on patient, disease, andtreatment characteristics. However, in four large scale prospectivecohort studies [4–7], the factors associated with increased risk forLE were not concordant. In a study of 1,287 women (104 werediagnosed with LE) [5], risk factors for LE included: higher stageof disease, increased number of lymph nodes removed, removal oftumor positive nodes, receipt of adjuvant CTX, higher body massindex (BMI), and poorer health status. In a second study of 997women (133 had LE) [4], risk factors for LE included: beingAfrican American, being better educated, higher stage of disease,and removal of at least one lymph node. In a population-basedsample of 631 women (237 had LE) [6], hazard ratios for the
PLOS ONE | www.plosone.org 1 April 2013 | Volume 8 | Issue 4 | e60164
Lymphatic and Angiogenic Candidate Genes Predict theDevelopment of Secondary Lymphedema followingBreast Cancer SurgeryChristine Miaskowski1*, Marylin Dodd1, Steven M. Paul1, Claudia West1, Deborah Hamolsky2,
Gary Abrams3, Bruce A. Cooper4, Charles Elboim5, John Neuhaus6, Brian L. Schmidt7, Betty Smoot8,
Bradley E. Aouizerat9
1 Department of Physiological Nursing, University of California San Francisco, San Francisco, California, United States of America, 2 Department of Physiological Nursing,
Helen Diller Family Comprehensive Cancer Center, University of California San Francisco, San Francisco, California, United States of America, 3 Department of Neurology,
University of California San Francisco, San Francisco, California, United States of America, 4 Department of Community Health Systems, University of California San
Francisco, San Francisco, California, United States of America, 5 Redwood Regional Medical Group, Santa Rosa, California, United States of America, 6 Department of
Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California, United States of America, 7 Department of Oral and Maxillofacial Surgery,
New York University, New York, New York, United States of America, 8 Department of Physical Therapy and Rehabilitation Science, University of California San Francisco,
San Francisco, California, United States of America, 9 Department of Physiological Nursing, Institute for Human Genetics, University of California San Francisco, San
Francisco, California, United States of America
Abstract
The purposes of this study were to evaluate for differences in phenotypic and genotypic characteristics in women who didand did not develop lymphedema (LE) following breast cancer treatment. Breast cancer patients completed a number ofself-report questionnaires. LE was evaluated using bioimpedance spectroscopy. Genotyping was done using a customgenotyping array. No differences were found between patients with (n = 155) and without LE (n = 387) for the majority ofthe demographic and clinical characteristics. Patients with LE had a significantly higher body mass index, more advanceddisease and a higher number of lymph nodes removed. Genetic associations were identified for four genes (i.e., lymphocytecytosolic protein 2 (rs315721), neuropilin-2 (rs849530), protein tyrosine kinase (rs158689), vascular cell adhesion molecule 1(rs3176861)) and three haplotypes (i.e., Forkhead box protein C2 (haplotype A03), neuropilin-2 (haplotype F03), vascularendothelial growth factor-C (haplotype B03)) involved in lymphangiogensis and angiogenesis. These genetic associationssuggest a role for a number of lymphatic and angiogenic genes in the development of LE following breast cancer treatment.
Citation: Miaskowski C, Dodd M, Paul SM, West C, Hamolsky D, et al. (2013) Lymphatic and Angiogenic Candidate Genes Predict the Development of SecondaryLymphedema following Breast Cancer Surgery. PLoS ONE 8(4): e60164. doi:10.1371/journal.pone.0060164
Editor: Robert Lafrenie, Sudbury Regional Hospital, Canada
Received February 1, 2013; Accepted February 21, 2013; Published April 16, 2013
Copyright: ! 2013 Miaskowski et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This study was funded by grants from the National Cancer Institute (CA107091 and CA118658) and the National Institute of Nursing Research(NR0101282). Dr. Miaskowski is an American Cancer Society Clinical Research Professor. Dr. Bradley Aouizerat was funded through the National Institutes of Health(NIH) Roadmap for Medical Research Grant (KL2 RR624130). This project was supported by NIH/NCRR UCSF-CTSI Grant Number UL1 RR024131. Its contents aresolely the responsibility of the authors and do not necessarily represent the official views of the NIH. The funders had no role in the study design, data collectionand analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Lymphedema (LE) following treatment for breast cancer is themost common form of LE in the industrialized world [1]. LE iscaused by a reduction in lymph transport capacity associated withthe cancer and its treatment (e.g., surgery, radiation therapy (RT),chemotherapy (CTX)) and results in the accumulation of protein-rich fluid in the interstitial space. LE results in disfigurement,discomfort, and functional impairments. In addition, LE mayprecipitate cellulitis and lymphangitis [2].
The exact prevalence of LE in breast cancer survivors isunknown with estimates ranging from 3% to 87% [3]. This widevariation is due to differences in measurement methods, inconsis-tencies in diagnostic criteria, as well as variations in samplecharacteristics, timing of measurements, and duration of follow-up. However, as noted by Armer [3], if the incidence of LE is
conservatively set at 20%, more than 500,000 breast cancersurvivors in the United States are affected by this condition.
One of the major goals of LE research is the identification ofwomen at greatest risk for the development of this conditionfollowing breast cancer treatment. Risk factors evaluated in themajority of studies done to date focused on patient, disease, andtreatment characteristics. However, in four large scale prospectivecohort studies [4–7], the factors associated with increased risk forLE were not concordant. In a study of 1,287 women (104 werediagnosed with LE) [5], risk factors for LE included: higher stageof disease, increased number of lymph nodes removed, removal oftumor positive nodes, receipt of adjuvant CTX, higher body massindex (BMI), and poorer health status. In a second study of 997women (133 had LE) [4], risk factors for LE included: beingAfrican American, being better educated, higher stage of disease,and removal of at least one lymph node. In a population-basedsample of 631 women (237 had LE) [6], hazard ratios for the
PLOS ONE | www.plosone.org 1 April 2013 | Volume 8 | Issue 4 | e60164
• Diagnostic de lymphœdème par impédancemétrie
• 110 femmes avec LO, 297 sans LO • Analyse en aveugle du polymorphisme
de différents gènes
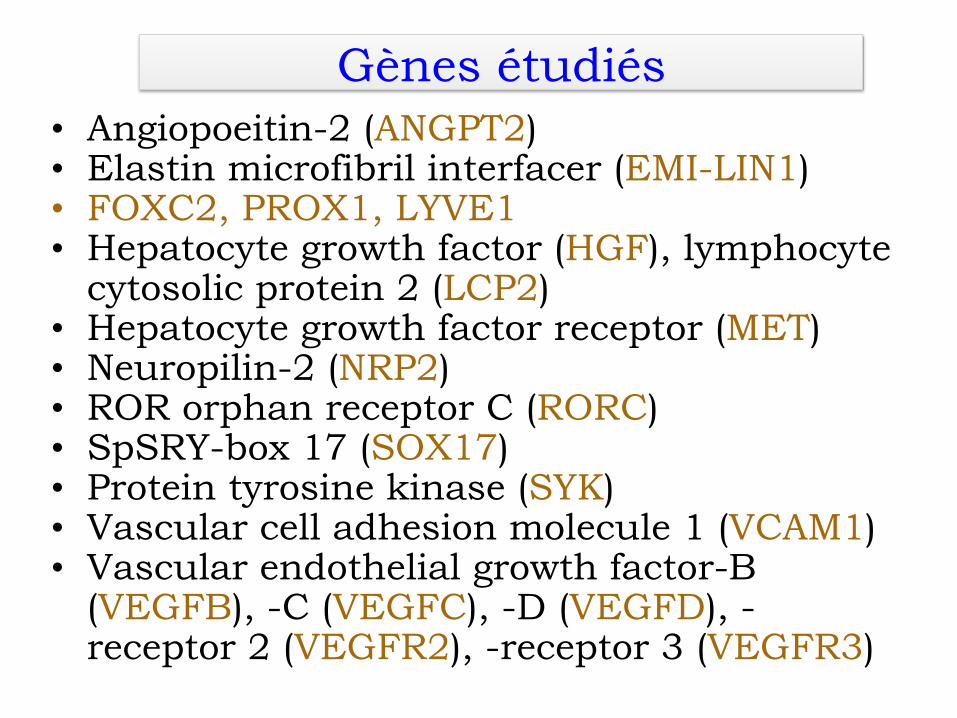
Gènes étudiés • Angiopoeitin-2 (ANGPT2) • Elastin microfibril interfacer (EMI-LIN1) • FOXC2, PROX1, LYVE1 • Hepatocyte growth factor (HGF), lymphocyte
cytosolic protein 2 (LCP2) • Hepatocyte growth factor receptor (MET) • Neuropilin-2 (NRP2) • ROR orphan receptor C (RORC) • SpSRY-box 17 (SOX17) • Protein tyrosine kinase (SYK) • Vascular cell adhesion molecule 1 (VCAM1) • Vascular endothelial growth factor-B
(VEGFB), -C (VEGFC), -D (VEGFD), -receptor 2 (VEGFR2), -receptor 3 (VEGFR3)
BMI, stage of disease, having a SLNB, and number of lymphnodes removed. Receipt of CTX and RT, while not significantafter the inclusion of genomic estimates of and self-reported race/ethnicity, were retained in all of the regression models for facevalidity.
The only genetic associations that remained significant in themultivariate logistic regression analyses were for FOXC2 haplo-type A03, LCP2 rs315721, NRP2 rs849530, NRP2 haplotype F01,SYK rs158689, VCAM1 rs3176861, and VEGFC haplotype B03(see Table 4 and Figures 1, 2, 3, and 4). In the regression analysisfor the FOXC2 haplotype A3, which was composed of two SNPs(i.e., rs34221221, rs1035550), the overall model explained 18.6%of the variance in the odds of developing LE. Each additional doseof the FOXC2 haplotype A03 was associated with 37.0% decreasein the odds of developing LE. Figure 1 displays the FOXC2 LD-based heatmap and haplotype analysis.
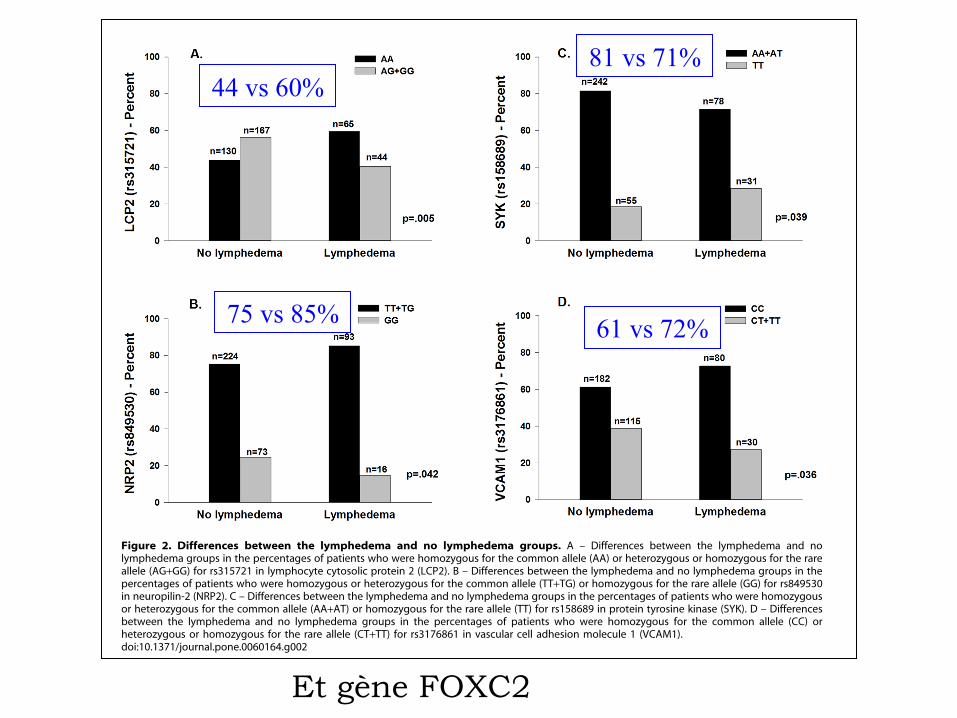
In the regression analysis for LCP2 rs315721, the overall modelexplained 18.9% of the variance in the odds of developing LE.Carrying one or two doses of the rare allele (i.e., AA versus AG +GG) was associated with a 50.0% decrease in the odds ofdeveloping LE (Figure 2A).
In the regression analysis for NRP2 rs849530, the overall modelexplained 19.0% of the variance in the odds of developing LE.Carrying two doses of the rare allele (i.e., TT+TG versus GG) wasassociated with 62.0% decrease in the odds of developing LE(Figure 2B). In the regression analysis for the NRP2 haplotypeF01, which was composed of three SNPs (i.e., rs849530, rs950219,rs3771052), the overall model explained 19.4% of the variance inthe odds of developing LE. Each additional dose of the NRP2haplotype F01 was associated with 46.0% decrease in the odds ofdeveloping LE. Figure 3 displays the NRP2 LD-based heatmapand haplotype analysis.
In the regression analysis for SYK rs158689, the overall modelexplained 20.1% of the variance in the odds of developing LE.Carrying two doses of the rare allele (i.e., AA + AT versus TT) wasassociated with 3.43-fold increase in the odds of developing LE(Figure 2C).
In the regression analysis for VCAM1 rs3176861, the overallmodel explained 18.4% of the variance in the odds of developingLE. Carrying one or two doses of the rare allele (i.e., CC versusCT + TT) was associated with a 45.0% decrease in the odds ofdeveloping LE (Figure 2D).
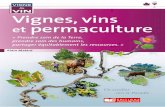
Figure 2. Differences between the lymphedema and no lymphedema groups. A – Differences between the lymphedema and nolymphedema groups in the percentages of patients who were homozygous for the common allele (AA) or heterozygous or homozygous for the rareallele (AG+GG) for rs315721 in lymphocyte cytosolic protein 2 (LCP2). B – Differences between the lymphedema and no lymphedema groups in thepercentages of patients who were homozygous or heterozygous for the common allele (TT+TG) or homozygous for the rare allele (GG) for rs849530in neuropilin-2 (NRP2). C – Differences between the lymphedema and no lymphedema groups in the percentages of patients who were homozygousor heterozygous for the common allele (AA+AT) or homozygous for the rare allele (TT) for rs158689 in protein tyrosine kinase (SYK). D – Differencesbetween the lymphedema and no lymphedema groups in the percentages of patients who were homozygous for the common allele (CC) orheterozygous or homozygous for the rare allele (CT+TT) for rs3176861 in vascular cell adhesion molecule 1 (VCAM1).doi:10.1371/journal.pone.0060164.g002
Candidate Genes and Lymphedema
PLOS ONE | www.plosone.org 15 April 2013 | Volume 8 | Issue 4 | e60164
Et gène FOXC2
44 vs 60% 81 vs 71%
75 vs 85% 61 vs 72%
Original Articles
Possible Genetic Predisposition to Lymphedemaafter Breast Cancer
Beth Newman, Ph.D.,1 Felicity Lose, Ph.D.,2 Mary-Anne Kedda, Ph.D.,1
Mathias Francois, Ph.D.,3 Kaltin Ferguson,2 Monika Janda, Ph.D.,1 Patsy Yates, Ph.D.,4
Amanda B. Spurdle, Ph.D.,2,* and Sandra C. Hayes, PhD1,*
Abstract
Background: Known risk factors for secondary lymphedema only partially explain who develops lymphedemafollowing cancer, suggesting that inherited genetic susceptibility may influence risk. Moreover, identification ofmolecular signatures could facilitate lymphedema risk prediction prior to surgery or lead to effective drugtherapies for prevention or treatment. Recent advances in the molecular biology underlying development of thelymphatic system and related congenital disorders implicate a number of potential candidate genes to explore inrelation to secondary lymphedema.Methods and Results: We undertook a nested case-control study, with participants who had developed lym-phedema after surgical intervention within the first 18 months of their breast cancer diagnosis serving as cases(n = 22) and those without lymphedema serving as controls (n = 98), identified from a prospective, population-based, cohort study in Queensland, Australia. TagSNPs that covered all known genetic variation in the genesSOX18, VEGFC, VEGFD, VEGFR2, VEGFR3, RORC, FOXC2, LYVE1, ADM, and PROX1 were selected forgenotyping. Multiple SNPs within three receptor genes, VEGFR2, VEGFR3, and RORC, were associated withlymphedema defined by statistical significance ( p < 0.05) or extreme risk estimates (OR < 0.5 or > 2.0).Conclusions: These provocative, albeit preliminary, findings regarding possible genetic predisposition to sec-ondary lymphedema following breast cancer treatment warrant further attention for potential replication usinglarger datasets.
Introduction
Lymphedema is one of the most problematic complica-tions following breast cancer treatment, experienced by
approximately 30% of breast cancer survivors.1–3 It representsfailure of the lymphatic system to adequately drain fluid andproteins from the interstitial tissue and to circulate lympho-cytes. Removal or damage to the lymph nodes or lymphaticvasculature during cancer treatment may impede properphysiological function of this network. Although lymphede-ma can occur in any part of the body, it generally refers to anaccumulation of fluid and subsequent distortion of a limb.4
Little is known about its prevention, and it is regarded as an
incurable, progressive, disfiguring, and disabling disorderthat is difficult to manage, compromising function5 andquality of life.6
Lymphedema may present immediately or years afterbreast cancer treatment,7 although the majority of cases seemto appear within the first 12-18 months post-surgery.3,8–9 Thepublished literature on risk factors is characterized by in-consistent relationships, but evidence is mounting for a few,including extent of surgery, extent of lymph node resection,radiation therapy, obesity, and surgical wound infection.10
Nevertheless, it is clear that these characteristics only partiallyexplain who develops lymphedema, and lymphedema canand does occur in women lacking these risk factors. It is
1Institute of Health and Biomedical Innovation and School of Public Health, and 4Institute of Health and Biomedical Innovation and Schoolof Nursing, Queensland University of Technology, Brisbane, Australia.
2Molecular Cancer Epidemiology Laboratory, Genetics and Population Health Division, Queensland Institute of Medical Research, Bris-bane, Australia.
3Institute of Molecular Bioscience, University of Queensland, Brisbane, Australia.*ABS led laboratory-related activities, while SCH led field-related activities.
LYMPHATIC RESEARCH AND BIOLOGYVolume 10, Number 1, 2012ª Mary Ann Liebert, Inc.DOI: 10.1089/lrb.2011.0024
2
Original Articles
Possible Genetic Predisposition to Lymphedemaafter Breast Cancer
Beth Newman, Ph.D.,1 Felicity Lose, Ph.D.,2 Mary-Anne Kedda, Ph.D.,1
Mathias Francois, Ph.D.,3 Kaltin Ferguson,2 Monika Janda, Ph.D.,1 Patsy Yates, Ph.D.,4
Amanda B. Spurdle, Ph.D.,2,* and Sandra C. Hayes, PhD1,*
Abstract
Background: Known risk factors for secondary lymphedema only partially explain who develops lymphedemafollowing cancer, suggesting that inherited genetic susceptibility may influence risk. Moreover, identification ofmolecular signatures could facilitate lymphedema risk prediction prior to surgery or lead to effective drugtherapies for prevention or treatment. Recent advances in the molecular biology underlying development of thelymphatic system and related congenital disorders implicate a number of potential candidate genes to explore inrelation to secondary lymphedema.Methods and Results: We undertook a nested case-control study, with participants who had developed lym-phedema after surgical intervention within the first 18 months of their breast cancer diagnosis serving as cases(n = 22) and those without lymphedema serving as controls (n = 98), identified from a prospective, population-based, cohort study in Queensland, Australia. TagSNPs that covered all known genetic variation in the genesSOX18, VEGFC, VEGFD, VEGFR2, VEGFR3, RORC, FOXC2, LYVE1, ADM, and PROX1 were selected forgenotyping. Multiple SNPs within three receptor genes, VEGFR2, VEGFR3, and RORC, were associated withlymphedema defined by statistical significance ( p < 0.05) or extreme risk estimates (OR < 0.5 or > 2.0).Conclusions: These provocative, albeit preliminary, findings regarding possible genetic predisposition to sec-ondary lymphedema following breast cancer treatment warrant further attention for potential replication usinglarger datasets.
Introduction
Lymphedema is one of the most problematic complica-tions following breast cancer treatment, experienced by
approximately 30% of breast cancer survivors.1–3 It representsfailure of the lymphatic system to adequately drain fluid andproteins from the interstitial tissue and to circulate lympho-cytes. Removal or damage to the lymph nodes or lymphaticvasculature during cancer treatment may impede properphysiological function of this network. Although lymphede-ma can occur in any part of the body, it generally refers to anaccumulation of fluid and subsequent distortion of a limb.4
Little is known about its prevention, and it is regarded as an
incurable, progressive, disfiguring, and disabling disorderthat is difficult to manage, compromising function5 andquality of life.6
Lymphedema may present immediately or years afterbreast cancer treatment,7 although the majority of cases seemto appear within the first 12-18 months post-surgery.3,8–9 Thepublished literature on risk factors is characterized by in-consistent relationships, but evidence is mounting for a few,including extent of surgery, extent of lymph node resection,radiation therapy, obesity, and surgical wound infection.10
Nevertheless, it is clear that these characteristics only partiallyexplain who develops lymphedema, and lymphedema canand does occur in women lacking these risk factors. It is
1Institute of Health and Biomedical Innovation and School of Public Health, and 4Institute of Health and Biomedical Innovation and Schoolof Nursing, Queensland University of Technology, Brisbane, Australia.
2Molecular Cancer Epidemiology Laboratory, Genetics and Population Health Division, Queensland Institute of Medical Research, Bris-bane, Australia.
3Institute of Molecular Bioscience, University of Queensland, Brisbane, Australia.*ABS led laboratory-related activities, while SCH led field-related activities.
LYMPHATIC RESEARCH AND BIOLOGYVolume 10, Number 1, 2012ª Mary Ann Liebert, Inc.DOI: 10.1089/lrb.2011.0024
2
• 120 femmes : 98 sans et 22 avec lymphœdème (apparu 6-18 mois après la chirurgie)
• Etude polymorphisme de plusieurs gènes candidats • Résultats : VEGFR3, VEGFR2 et RORC (Retinoic
acid receptor-related Orphan Receptor gamma) => organogénèse lymphoïde, lymphangiogénèse
Original Articles
Possible Genetic Predisposition to Lymphedemaafter Breast Cancer
Beth Newman, Ph.D.,1 Felicity Lose, Ph.D.,2 Mary-Anne Kedda, Ph.D.,1
Mathias Francois, Ph.D.,3 Kaltin Ferguson,2 Monika Janda, Ph.D.,1 Patsy Yates, Ph.D.,4
Amanda B. Spurdle, Ph.D.,2,* and Sandra C. Hayes, PhD1,*
Abstract
Background: Known risk factors for secondary lymphedema only partially explain who develops lymphedemafollowing cancer, suggesting that inherited genetic susceptibility may influence risk. Moreover, identification ofmolecular signatures could facilitate lymphedema risk prediction prior to surgery or lead to effective drugtherapies for prevention or treatment. Recent advances in the molecular biology underlying development of thelymphatic system and related congenital disorders implicate a number of potential candidate genes to explore inrelation to secondary lymphedema.Methods and Results: We undertook a nested case-control study, with participants who had developed lym-phedema after surgical intervention within the first 18 months of their breast cancer diagnosis serving as cases(n = 22) and those without lymphedema serving as controls (n = 98), identified from a prospective, population-based, cohort study in Queensland, Australia. TagSNPs that covered all known genetic variation in the genesSOX18, VEGFC, VEGFD, VEGFR2, VEGFR3, RORC, FOXC2, LYVE1, ADM, and PROX1 were selected forgenotyping. Multiple SNPs within three receptor genes, VEGFR2, VEGFR3, and RORC, were associated withlymphedema defined by statistical significance ( p < 0.05) or extreme risk estimates (OR < 0.5 or > 2.0).Conclusions: These provocative, albeit preliminary, findings regarding possible genetic predisposition to sec-ondary lymphedema following breast cancer treatment warrant further attention for potential replication usinglarger datasets.
Introduction
Lymphedema is one of the most problematic complica-tions following breast cancer treatment, experienced by
approximately 30% of breast cancer survivors.1–3 It representsfailure of the lymphatic system to adequately drain fluid andproteins from the interstitial tissue and to circulate lympho-cytes. Removal or damage to the lymph nodes or lymphaticvasculature during cancer treatment may impede properphysiological function of this network. Although lymphede-ma can occur in any part of the body, it generally refers to anaccumulation of fluid and subsequent distortion of a limb.4
Little is known about its prevention, and it is regarded as an
incurable, progressive, disfiguring, and disabling disorderthat is difficult to manage, compromising function5 andquality of life.6
Lymphedema may present immediately or years afterbreast cancer treatment,7 although the majority of cases seemto appear within the first 12-18 months post-surgery.3,8–9 Thepublished literature on risk factors is characterized by in-consistent relationships, but evidence is mounting for a few,including extent of surgery, extent of lymph node resection,radiation therapy, obesity, and surgical wound infection.10
Nevertheless, it is clear that these characteristics only partiallyexplain who develops lymphedema, and lymphedema canand does occur in women lacking these risk factors. It is
1Institute of Health and Biomedical Innovation and School of Public Health, and 4Institute of Health and Biomedical Innovation and Schoolof Nursing, Queensland University of Technology, Brisbane, Australia.
2Molecular Cancer Epidemiology Laboratory, Genetics and Population Health Division, Queensland Institute of Medical Research, Bris-bane, Australia.
3Institute of Molecular Bioscience, University of Queensland, Brisbane, Australia.*ABS led laboratory-related activities, while SCH led field-related activities.
LYMPHATIC RESEARCH AND BIOLOGYVolume 10, Number 1, 2012ª Mary Ann Liebert, Inc.DOI: 10.1089/lrb.2011.0024
2
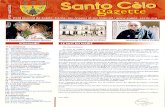
Lymphœdème primaire et génétique
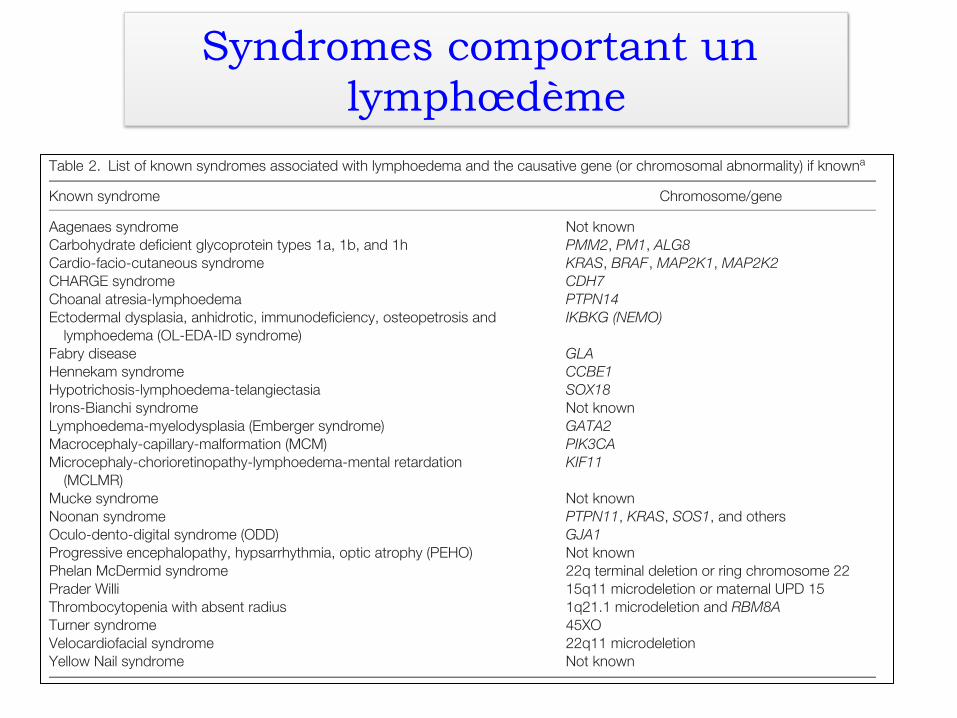
Syndromes comportant un lymphœdème
Connell et al.
Table 1. Definition of terminology used in the classification pathwaya
Congenital onset Onset of lymphoedema before the age of one year.Cutaneous manifestations Naevi/pigmentation variations (e.g. epidermal naevi)/vascular malformations.Distichiasis Presence of aberrant eyelashes arising from the meibomian glands.Disturbed growth Hypertrophy (overgrowth) and hypotrophy of bone or soft tissue resulting in altered length of a limb
or body part.KT/KT-like Klippel – Trenaunay/ Klippel – Trenaunay-like syndrome.Late onset Swelling presenting after one year of age.Prenatal onset Detection of lymphatic abnormality in the prenatal period. Isolated pedal oedema is excluded from
this definition as this may be a presentation of Milroy disease.Segment A region of the body affected by lymphoedema (i.e. face, conjunctiva, genitalia, upper limbs, lower
limbs – each constitute one body part). Multisegmental refers to more than one segmentaffected by lymphoedema. Bilateral lower limb swelling is not considered to be multisegmentallymphoedema.
Syndromic A constellation of abnormalities, one of which is lymphoedema.Systemic involvement Systemic lymphatic problems persisting beyond the newborn period or manifesting at any age
thereafter. This includes hydrops fetalis, chylous ascites, intestinal lymphangiectasia, pleural andpericardial effusions, and pulmonary lymphangiectasia.
Vascular anomalies Include congenital vascular abnormalities.
aThis table should be used in conjunction with Fig. 1.
Table 2. List of known syndromes associated with lymphoedema and the causative gene (or chromosomal abnormality) if knowna
Known syndrome Chromosome/gene
Aagenaes syndrome Not knownCarbohydrate deficient glycoprotein types 1a, 1b, and 1h PMM2, PM1, ALG8Cardio-facio-cutaneous syndrome KRAS, BRAF, MAP2K1, MAP2K2CHARGE syndrome CDH7Choanal atresia-lymphoedema PTPN14Ectodermal dysplasia, anhidrotic, immunodeficiency, osteopetrosis and
lymphoedema (OL-EDA-ID syndrome)IKBKG (NEMO)
Fabry disease GLAHennekam syndrome CCBE1Hypotrichosis-lymphoedema-telangiectasia SOX18Irons-Bianchi syndrome Not knownLymphoedema-myelodysplasia (Emberger syndrome) GATA2Macrocephaly-capillary-malformation (MCM) PIK3CAMicrocephaly-chorioretinopathy-lymphoedema-mental retardation
(MCLMR)KIF11
Mucke syndrome Not knownNoonan syndrome PTPN11, KRAS, SOS1, and othersOculo-dento-digital syndrome (ODD) GJA1Progressive encephalopathy, hypsarrhythmia, optic atrophy (PEHO) Not knownPhelan McDermid syndrome 22q terminal deletion or ring chromosome 22Prader Willi 15q11 microdeletion or maternal UPD 15Thrombocytopenia with absent radius 1q21.1 microdeletion and RBM8ATurner syndrome 45XOVelocardiofacial syndrome 22q11 microdeletionYellow Nail syndrome Not known
aFurther information for each of these genes can be found on the OMIM website.
The most common conditions in this category includeTurner, Noonan (NS; MIM 163950) and Prader Willi(PWS; MIM 176270) syndromes. The genetic causesof many of these syndromes are known and testing isavailable. A molecular result means that the mode ofinheritance can be established and where indicated, pre-natal diagnosis can be offered. Table 2 provides a listof syndromes that include lymphoedema as a feature.
A new addition to this list is Oculo-dento-digital syn-drome (ODD; MIM 164200) which is caused by muta-tions in the GJA1 gene. Lymphoedema has recentlybeen reported as an associated feature of ODD syn-drome in a family, where a novel GJA1 mutation co-segregated with the affected status (29).
The pathway works in such a way that in conditionsin which lymphoedema/lymphatic dysplasia is a mainfeature, the condition may also be classified elsewhere
4
Conclusions
1. Meilleure compréhension de la physiopathologie des lymphœdèmes (inflammation à « bas bruit »)
2. « Implication » génétique dans les formes secondaires (MS)
3. Démembrement des lymphœdèmes primaires avec les découvertes génétiques…
futur : prévention, traitement...