






Langages
Pages
Légal


Traitement des patients atteints d’hépatite chronique virale C
non répondeurs
Vendredi 12 décembre 2008
FORUM HEPATOLOGIE DU CREGG
Denis OUZAN Denis OUZAN Institut Arnauld Tzanck Institut Arnauld Tzanck
Saint Laurent du VarSaint Laurent du Var

Patients Naïfs Incidence de l’échec virologique
PEG-IFN-a 2a+ ribavirine (Fried et al., 2002)
PEG-IFN-a 2b+ ribavirine(Manns et al., 2001)
(Manns et al., Lancet 2001 ; 358 : 958-65 ; Fried et al., N Engl J Med 2002 ; 347 : 975-82 ; Hadziyannis et al., Ann Intern Med 2004 ; 140 : 346-55)
54%
24%
Génotype 1 Génotypes 2/3
48%
18%16%
PEG-IFN-a 2a+ ribavirine (Hadziyannis et al., 2004)
58%

Etude IDEAL (3070 malades de génotype 1 traités
48 semaines) Réponse Virologique Soutenue
ViraféronPegViraféronPeg 1.5µg ViraféronPeg 1µg Pegasys 180µg 1.5µg ViraféronPeg 1µg Pegasys 180µg
RBV 800-1200 mg RBV 800-1200 mg RBV 1000-1200 mgRBV 800-1200 mg RBV 800-1200 mg RBV 1000-1200 mg
n=1019 n=1016 n=1035n=1019 n=1016 n=1035
40% 38% 41%40% 38% 41%
Sulkovski et al EASL 2008

Proportions de patients ayant une Proportions de patients ayant une PCR négativePCR négative
Bithérapie pégylée% PCR neg
EASL 2008 EASL 2008 – Sulkowski M et al. J Hepatol 48: Abstract 991– Sulkowski M et al. J Hepatol 48: Abstract 991

TMA : 10 UI/mL
Seuil thérapeutique: 400 000 UI/mL
1
10
100
1.000
10.000
100.000
1.000.000
copies / mL
Versant RNA 3.0 615 à 8 M UI/mL
8 M UI/mL
Amplicor Roche : 50 UI/mL
Monitor Roche600 à 500 000UI/mL
4
40
400
4.000
40.000
400.000
UI / mL
LCx AbbottCobas Taqman ROCHE10-15 à 200M UI/mL
200 M UI /mL
Echelles de quantification des tests de charge virale

Null response
Treatment of Chronic Hepatitis C:Response and Relapse
2 log decline
Limit of detectionSVR
Relapse
PegIFN/RBV
Weeks
HC
V R
NA
(lo
g1
0 IU
/mL
)
Partial response
0
1
2
3
4
5
6
7
8
0 4 12 18 24 30 36 42 48 54 60 66 728 78
SCHIFFMAN AASLD 2008

2 log decline
Limit of detection
Weeks
HC
V R
NA
(lo
g1
0 IU
/mL
)
RVR
90% SVR
0
1
2
3
4
5
6
7
8
RVR : HCV RNA undetectable at Week 4
SVR
PegIFN/RBV
0 4 12 18 24 30 36 42 48 54 60 66 728 78
Marcellin et al EASL 2007

HC
V R
NA
(lo
g1
0 IU
/mL
)
0
1
2
3
4
5
6
7
8
2 log decline
Limit of detectionRVR
EVR: HCV RNA undetectable at Week 12
EVR
67% SVR
SVR
Weeks
PegIFN/RBV
0 4 12 18 24 30 36 42 48 54 60 66 728 78
Marcellin et al EASL 2007

Individualised Treatment Duration for Hepatitis C Gen. 1 Patients : A Randomized Controlled Trial
GROUPE STANDARD GROUPE VARIABLE n=237 n=459n=237 n=459
S4 ARN VHC negatif : 62 n : 123ARN VHC negatif : 62 n : 123
48 sem RVP : 87% 24 sem RVP : 77 %
S8 ARN 1ere négativité : 64 ARN 1ere négativité : 64 n : 128 n : 128
48 sem RVP : 70% 48 sem RVP : 72%
S12 ARN 1 ère négativité : 21 ARN 1 ère négativité : 21 n : 52 n : 52
48 sem RVP : 38% 72 sem RVP : 63%
Mangia A et al HEPATOLOGY 2008,47,43-50

HC
V R
NA
(lo
g1
0 IU
/mL
)
0
1
2
3
4
5
6
7
8
Limit of detectionEVR
Slow Virologic Response: HCV RNA Undetectable at Week 24
Slow response
45% SVR
SVR
Weeks
RVR
PegIFN/RBV
0 4 12 18 24 30 36 42 48 54 60 66 728 78
DI MARTINO et al AASLD2008

Modulation de la durée du traitement PEGIFN + RBV : méta-analyse
0,1 1 10 100
Risque relatif
En faveur de 72 sem.En faveur de 48 sem.
Q Cochrane ; p = 0,71
Berg, Gastroenterology 2006
Sanchez-Tapias, Gastroenterology 2006
Moyenne
Ribavirine 800 mg/j
1,39 (0,83-2,31)
2,57 (1,07-6,17)
1,70 (0,96-3,00)
Résultats poolés 1,62 (1,21-2,37)
Ferenci, AASLD 2008
Pearlman, Hepatology 2007
Mangia, Hepatology 2008
Moyenne
Ribavirine en fonction du poids
1,40 (0,86-2,28)
2,03 (1,05-3,96)
3,67 (0,21-65,28)
1,62 (1,10-2,39)
Génotypes 1 répondeurs lents : 72 em. versus 48 sem.Diagramme des risques relatifs
AASLD 2008 – Di Martino V, Abstract 213

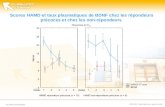
Extension d’un traitement par Peg IFN-2b+RBV à 72 sem chez des malades de génotype 1
répondeurs lents
Pearlman et al Hepatology 2007.46,1688-94Pearlman et al Hepatology 2007.46,1688-94
RV
S %

SVR rate according to cumulative ribavirin exposure
Reddy KR et al Clin Gastroenterol and Hépatol 2007; 5:124-29
67
0
62 62
0
10
20
30
40
50
60
70
SV
R r
ate
(%
)
n= 163 50 39 263
p=0.01
≥97% 80–<97% 60–<80% <60% Total
11
57
33

Neutrophiles et Peg-Interféron
Doser les neutrophiles avant l’injection car Doser les neutrophiles avant l’injection car
21 % neutro dans les 24 premières heures.21 % neutro dans les 24 premières heures. Diminution médiane neutro de 40 % sous PegIFN Diminution médiane neutro de 40 % sous PegIFN
dans les 14 premiers joursdans les 14 premiers jours
(Peck-Radoavjelic M et al Gastroenterology 2002)(Peck-Radoavjelic M et al Gastroenterology 2002)
Pas de relation démontrée entre taux desPas de relation démontrée entre taux des
neutrophiles et infections neutrophiles et infections (Soza A et al Hepatology 2002)(Soza A et al Hepatology 2002)
(Juarez-Navarro A, Methods Find Exp Clin Pharmacol 2005)(Juarez-Navarro A, Methods Find Exp Clin Pharmacol 2005)

Treatment of Chronic Hepatitis C: Impact of Stopping RBV
Those who stopped RBV at Wk 24 had higher breakthrough and relapse ratesThose who stopped RBV at Wk 24 had higher breakthrough and relapse rates
0 2 2 3
14
2629
0
612
32
42 42
5
0
10
20
30
40
50
24 30 36 48 52 60 72Weeks
Continue RBV (n = 173)
Stop RBV (n = 176)
HC
V R
NA
Po
siti
ve (
%)
Reprinted from Gastroenterology, 131, Bronowicki JP, Ouzan D, Asselah T, Desmorat H, Zarski JP, Foucher J, Bourliere M, Renou C, Tran A, Melin P, Hezode C, Chevalier M, Bouvier-Alias M, Chevaliez S, Montestruc F, Lonjon-Domanec I, and Pawlotsky JM, Effect of Ribavirin in Genotype 1 Patients With Hepatitis C Responding to Pegylated Interferon Alfa-2a Plus Ribavirin, pages 1040-1048, Copyright 2006, with permission from Elsevier.

2 log decline
Limit of detection
SVR
Intensify PegIFN dose
Partial Responder : Impact of Intensifying Therapy
Weeks
HC
V R
NA
(lo
g1
0 IU
/mL
)
0
1
2
3
4
5
6
7
8
0 4 12 18 24 30 36 42 48 54 60 66 728 78
PegIFN/RBV
SCHIFFMAN AASLD 2008

Augmenter la dose d’ IFN-PEG alfa 2a permet d’augmenter la RVS
IFN-Peg alfa-2a180 g/S + RBV
(n=28)
IFN-Peg alfa-2a270 g/S + RBV
(n=20)
IFN-Peg alfa-2a360 g/S + RBV
(n=24)
RVS: ARN VHC < 50 UI/mL 24 semaines après le traitement
Diago M, AASLD 2004
RVS

Jensen D, et al. AASLD 2007. Abstract LB4.
Retreatment of PegIFN Nonresponders: High-Dose PegIFN alfa-2a—REPEAT
360/180 μg/wk 180 μg/wk
SVR in pooled 72-wk vs 48 wk arms: 16% vs 8% (P = .0006; OR: 2.22; 95% CI: 1.40-3.52)
ITT Analysis
31 33 31 28
49
78
5967
0
20
40
60
80
100
72 wk (n=317) 48 wk (n=156) 72 wk (n=156) 48 wk (n=313)
SV
R, %
ETR Relapse SVR

J.P.Jacques FORUM HEPATO CREGG J.P.Jacques FORUM HEPATO CREGG 12 décembre 200812 décembre 2008

Maintenance IFN for HCV-HALT-C Final Results
Low dose peginterferon alfa-2a arm (90 µg/week) n=517Low dose peginterferon alfa-2a arm (90 µg/week) n=517 vs control group n=533 vs control group n=533 Ishak Score > 3Ishak Score > 3
No reduction in fibrosis or difference between arms No reduction in fibrosis or difference between arms
No significant difference between arms in any primary No significant difference between arms in any primary outcome outcome 34.1% vs 33.8% : HR 1.01 (95% CI, 0.81-1.26)34.1% vs 33.8% : HR 1.01 (95% CI, 0.81-1.26)
Di Bisceglie A, et al. AASLD 2007. Abstract LB1.
*Ishak Score

ANTI-VIRAL AGENTSONGOING CLINICAL TRIALS
CompanyCompany DrugDrug TypeType PopulationPopulation
VertexVertex VX-950VX-950 ProteaseProteaseNaïveNaïve
NR,PR,RELNR,PR,REL
Schering-Schering-PloughPlough SCH503034SCH503034 ProteaseProtease
NRNR
NaïveNaïve
IdenixIdenix NM283NM283 PolymerasePolymeraseNRNR
NaïveNaïve
RocheRoche R1626R1626 PoymerasePoymerase NaïveNaïve
WyethWyeth HCV-796HCV-796 PolymerasePolymerase NaiveNaive

Télaprevir : étude européenne PROVE2 • Étude de phase IIb, randomisée, contrôlée, multicentrique chez 323 patients
européens naïfs, génotype 1, sans cirrhose
• Télaprévir (TVR) 750 mg/8 heures, PEG-IFN 180 µg/sem, RBV 1 000-1 200 mg/j
• Étude de phase IIb, randomisée, contrôlée, multicentrique chez 323 patients européens naïfs, génotype 1, sans cirrhose
• Télaprévir (TVR) 750 mg/8 heures, PEG-IFN 180 µg/sem, RBV 1 000-1 200 mg/j
AASLD 2008 – Zeuzem S, Allemagne, Abstract 243
PR48(n = 82)
T12/PR24(n = 81)
T12/PR12(n = 82)
T12/P12(n = 78)
PEG-IFNα-2a + RBVTVR + PEG-IFNα-2a
+ RBV
TVR + PEG-IFNα-2a
Placebo + PEG-IFNα-2a + ribavirine (RBV)
724824120
TVR + PEG-IFNα-2a + RBV

Telaprevir : étude européenne PROVE2 Résultats finaux
Réponse virologique soutenue
0
20
40
60
80
PR48 T12/PR24 T12/PR12 T12/P12(pas de RBV)
46
%
6960
36
38/82 56/81 49/82 28/78
NS*
p = 0,004* p = 0,12*
* versus PR48
Rechute (%)
0
10
20
30
50
PR48 T12/PR24 T12/PR12 T12/P12(pas de RBV)
22
%
14
30
48
10/45 8/57 19/63 22/46
40
2 rechutes tardives S36 et S48
AASLD 2008 – Zeuzem S, Abstract 243

PROVE 2: Adverse Events
AASLD 2008 Zeuzem S, et al. Abstract 243.
Adverse Events,* %
PegIFN/RBV 48 (Control)
(n = 82)
TVR Arms
TVR/PegIFN/RBV 12 → PegIFN/RBV 12
(n = 81)
TVR/PegIFN/RBV
12(n = 82)
TVR/PegIFN 12 (No RBV)
(n = 78)
Pruritus 35 51 63 59
Rash 35 49 44 47
Nausea 40 48 48 31
Asthenia 32 46 52 38
Headache 45 44 39 47
Anemia 17 27 18 9 Rate of discontinuation due to adverse events similar between arms
– Control arm: 7% – TVR/pegIFN/RBV 12 → pegIFN/RBV 12 arm: 14%
– TVR/pegIFN 12 (no RBV) arm: 9%– TVR/pegIFN/RBV 12 arm: 11%
– Rash most common cause of discontinuation in TVR/pegIFN/RBV arms: 7%

SPRINT-1: Boceprevir + PegIFN/RBV in Treatment-Naive GT1 Patients
Kwo P, et al. AASLD 2008. Abstract LB16.
Phase II TrialTreatment-naive
patients with GT 1HCV; all liver
histology grades
(N = 520)*
PegIFN/RBV + Boceprevir 800 mg TID
(n = 103)
PegIFN alfa-2b/RBV* + Boceprevir 800 mg TID(n = 107)
PegIFN alfa-2b/RBV* + Boceprevir 800 mg TID(n = 103)
PegIFN alfa-2b/RBV* (n = 104)
PegIFN alfa-2b/RBV + Boceprevir 800 mg TID
(n = 103)
PegIFN alfa-2b/ RBV
PegIFN alfa-2b/RBV
24-week follow-up
24-weekfollow-up
24-weekfollow-up
44-weekfollow-up
44-weekfollow-up
Week 4 Week 28 Week 48

SPRINT-1: Boceprevir + PegIFN/RBV in Treatment-Naive GT1 Patients
Kwo P, et al. AASLD 2008. Abstract LB16.
Sustained Virologic Response*
P/R Control48 Wk
P/R/B 28 Wk
P/R 4 Wk → P/R/B 24 Wk
P/R/B 48 Wk
P/R 4 Wk → P/R/B 44 Wk
Virologic Breakthrough‡
Pro
po
rtio
n o
f P
atie
nts
(%
)
Pat
ien
ts H
CV
Neg
ativ
e (%
)
P/R Control48 Wk
P/R/B 28 Wk
P/R 4 Wk →P/R/B24 Wk
P/R/B48 Wk
P/R 4 Wk →P/R/B44 Wk
80
60
40
20
0
7466
5655
38
100
07 4
115
0
20
40
60
80
100

PEG-IFN alfa-2a 180 µg qw Ribavirine 800 mg qd
PEG-IFN α-2a 180 µg qwRibavirine 800-1200 mg qd
PEG-IFN α-2b 1.0 µg/kg qwRibavirine 1000-1200 mg qd
PEG-IFN α-2b 1.5 µg/kg qwRibavirine 800-1400 mg qd
Non Oui Oui Oui
1221531 469(993 US)
273
Monde Italie Allemagne Norvège
~0,6 x 106 1 ~1,5 x 106~1 x 1065,6 x 106
46 46,6-49,7 38-42 37
81,5 69,5 74-80 76
50 % 78 % 25 % 19 %
Schéma
% G-2
Nombre
Régions
Charge viraleinitiale UI/ml
Age (années)
Durée Txbasée sur RVR?
Poids (kg)
ACCELERATE
VON WAGNER
MANGIA DALGARD
Traitement des malades de Génotypes 2,3

Schiffman et al N Eng J Med 2007.357:124 -34
378/461
p = 0,0007
82 %90 %
55/205 105/215
p < 0,00127 %
49 %
16 semaines
24 semaines
16 semaines
24 semaines
RV S4 : oui67 %
Tous patients
(n = 1291)
ARN VHC < 50 IU/ml
Réponse virologique précoce à S4
Génotype 2/316 semaines versus 24 semaines
370/410
Réponse virologique prolongée
RV S4 : non33 %

ITT population
67 %64 %
89 % 89 %
HC
V R
NA
un
dete
ctab
le (
%)
S4
16 sem 24 sem
0
20
40
60
80
100
n=243725n= 730 730 725 730 725 730 725
89 %82 %
62 %70 %
S 12 FDT RVS
La majorité des malades de génotype 2,3ont une réponse virologique sous traitement
Shiffman M, et al. N Engl J Med 2007; 357: 124

RVS en fonction de l’existence d’une cirrhose chez les maladies qui n’ont pas de RVR
32,2 %
51,7 %
14,9 %
27,8 %
n = 174n = 146 n = 72n =74
16 semaines 24 semaines
Non-RVR ; ITT population
Non Oui
RV
S (
%)
0
20
40
60
80
100
Shiffman M, et al. AASLD 2007

EPIC RVP en fonction du génotype et de
réponse au 1er traitement
Rechuteursà IFN/RBV
Rechuteurs
à PegIFN/RBVNonrépondeursà IFN/RBV
Non-répondeurs
à PegIFN/RBV
G1/4 : 34% (52/154)
G2/3 : 73% (41/56)
G1/4 : 29% (24/83)
G2/3 : 55% (16/29)
G1/4 : 13% (75/592)
G2/3 : 51% (40/78)
G1/4 : 4% (6/160)
G2/3 : 10% (1/10)
Poynard et al EASL 2008
1354 patients traités par ViraferonPeg® (1,5 µg/kg/sem) + Rebetol® 800 - 1400 mg/j pendant 48 semaines

Recherche de l’ARN du VHC à la fin du traitement
et 24 semaines après la fin du traitement
(1441 patients traités par IFN ou PEG-IFN (1441 patients traités par IFN ou PEG-IFN 48 sem) 48 sem)
348 rechutes348 rechutes
342/ 348 (98%) des rechutes sont apparues dans 342/ 348 (98%) des rechutes sont apparues dans les 3 mois qui suivent l’arrêt du traitement les 3 mois qui suivent l’arrêt du traitement
Zeuzem S et al., J of Hepatol 2003, 39,106-11.

Quel que soit le génotype une durée fixe de traitement n’est pas toujours appropriée
Seuil detection <10 IU/ml
log
HC
V R
NA
Temps
Rechute
RVS0
1
2
3
4
5
6
7
Seuil detection <50 IU/ml
durée avec PCR négative
durée avec PCR négative
La probabilité de RVS augmente avec la rapidité avec laquelle est obtenue une virémie indétectable
Durée du traitement

24 Weeks24 Weeks
DurationDuration
48 or 72 Weeks48 or 72 Weeks
DurationDuration
STOPSTOP
TreatmentTreatment
72 or + Weeks72 or + Weeks
DurationDuration
Week 4 HCV Week 4 HCV
RNA POSRNA POS
Start Start PEG-IFN + RBVPEG-IFN + RBV
STOPSTOP
TreatmentTreatment New therapeutic algorithm based on
virological response whatever genotypes
12 Weeks12 Weeks
RNA POSRNA POS
Week 4 HCV Week 4 HCV RNA NEGRNA NEG
= RVR
Week 4 < 1 logWeek 4 < 1 log
or non decreasingor non decreasing
= Null R
12 Weeks12 Weeks
RNA NegRNA Neg
= cEVR
24 Weeks24 Weeks
RNA NegRNA Neg
= Slow R
24 Weeks24 Weeks
RNA POSRNA POS
Halfon PHalfon P
Gemhep 2008Gemhep 2008
Ouzan DOuzan D
•If cirrhosis • RNA>400000UI
48 Weeks48 Weeks
DurationDuration

Nonresponders and Relapsers:Summary
Identifying the reason for nonresponse and relapse is Identifying the reason for nonresponse and relapse is the key to successful retreatment the key to successful retreatment
Patients with a null response are likely resistant to IFN Patients with a null response are likely resistant to IFN and unlikely to respond to retreatment and unlikely to respond to retreatment
Patients with a partial response may achieve undetectable Patients with a partial response may achieve undetectable HCV RNA with higher than standard doses pegIFNHCV RNA with higher than standard doses pegIFN
Extend the duration of retreatment in patients who achieved Extend the duration of retreatment in patients who achieved undetectable HCV RNA late in the course of their initial undetectable HCV RNA late in the course of their initial treatmenttreatment

Hépatites B et C 10 raisons de se faire dépister
1. J’ai été transfusé avant 19922. J’ai essayé des drogues par sniff ou injections3. J’ai été hospitalisé ou opéré il y a plus de 10 ans4. Ma mère est porteuse du virus B ou C5. Mon partenaire est porteur du virus B ou C6. Un membre de ma famille est porteur du virus B7. J’ai eu de l’acupuncture ou de la mésothérapie
sans matériel à usage unique8. Je me suis fait un piercing ou un tatouage9. J’ai été incarcéré à un moment de ma vie10. J’ai vécu dans un pays d’Asie, d’Afrique ou
du Moyen- Orient Si vous répondez OUI au moins une fois, parlez-en à votre médecin traitant et faites vous dépister Le test de dépistage est remboursé par la sécurité sociale, il est gratuit dans les Centres de Dépistage Anonyme et gratuit (CDAG)
www.hepatite06.org
Top Related