





Langages
Pages
Légal

Insuffisance rénale aiguë
Traitement médical Epuration extra-rénale
D. Journois, HEGP
Diurétiques
Expérimental -> l’atteinte rénale résulte de : vasoconstriction ; réduction de perméabilité capillaire ; obstruction tubulaire ; rétrodiffusion de l’ultrafiltrat ; ischémie.
Etudes cliniques Pas d’efficacité (Hager, 1996)
Diurèse seulement (Kleinknecht, 1976 ; Brown, 1981)
Diurétiques
Produisent une diurèse (rassurante) ; Déshydratent ; Réduisent la volémie ; Ne sont efficaces qu’associés à une inflation hydrique ; Doivent être réservés :
hypervolémie ; hyperchlorémie (diurétiques de l’anse) ; indications spécifiques (hyperkaliémie, OAP).
Dopamine Natriurétique/Diurétique (alpha, beta, DA1, DA2…) Notion de dose « dopaminergique » 30 études cliniques :
3 positives (niveaux III-V) ; 27 négatives (700 pts, niveau II-V).
Arguments contre : Ischémie mésentérique (Segal, J Appl Physiol, 1992)
Gangrènes de extrémités (NEJM 1976)
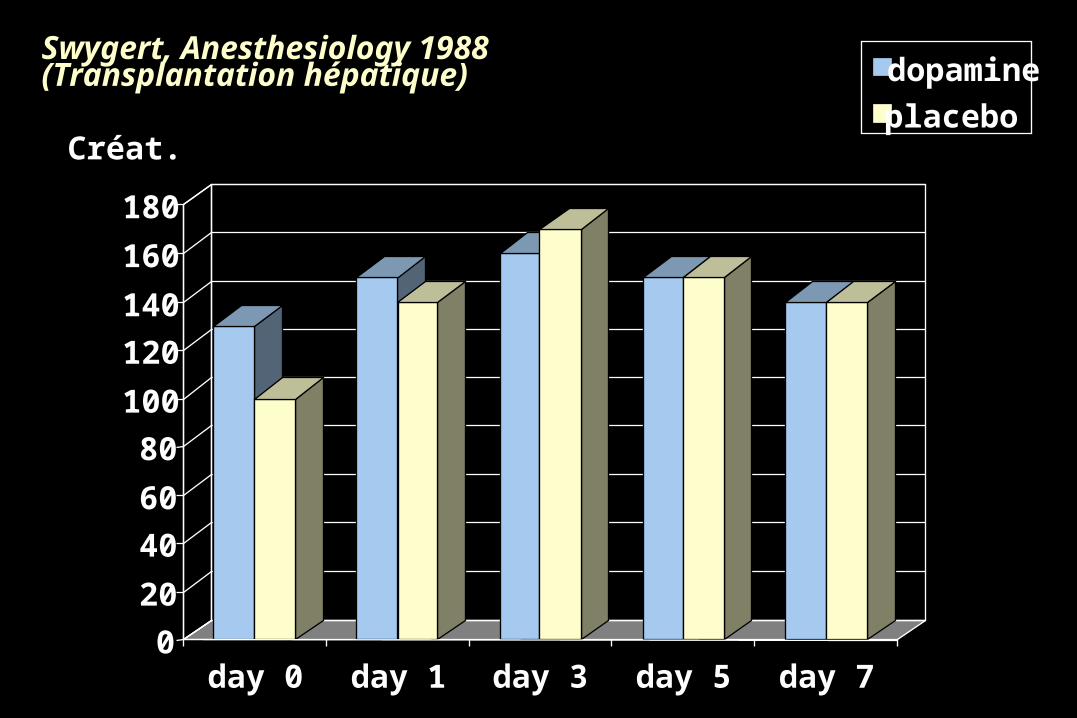
Swygert, Anesthesiology 1988(Transplantation hépatique)
0
20
40
60
80
100
120
140
160
180
day 0 day 1 day 3 day 5 day 7
dopamine
placeboCréat.
Produits de contraste Dopamine : détériore la fonction rénale (Hall) ;
Diurétiques : délétères (Weinstein, Solomon) ;
Mannitol : moins efficace que l’hydratation ; Inhibiteurs calciques : efficaces hors situations cliniques ; Hyperhydratation
N-acétylcystéine ; Théophylline.
Indications de l’EER Situations « classiques » :
hyperkaliémie ; inflation hydrique ou volémique ; acidose (à TA élevé sans lactate) ; urémie
Indications réelles : Objectifs
Survie ? Physiologie ? Supra-physiologiques ?
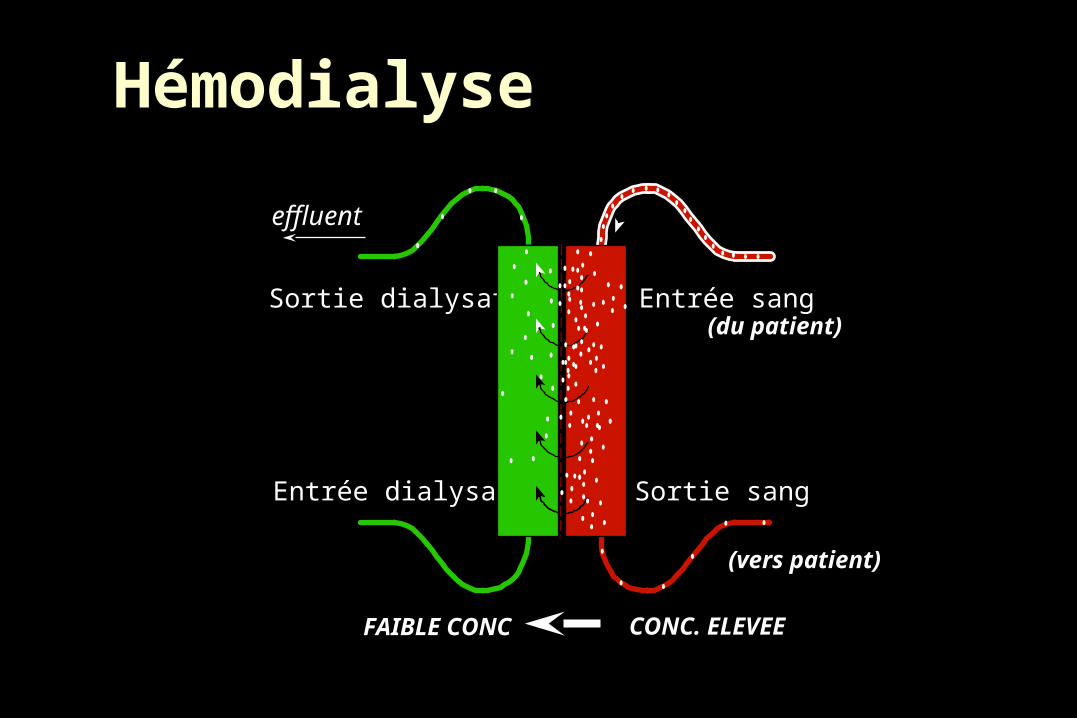
Hémodialyse
Sortie dialysat
Entrée dialysat
Entrée sang
Sortie sang
effluent
(du patient)
(vers patient)
CONC. ELEVEEFAIBLE CONC
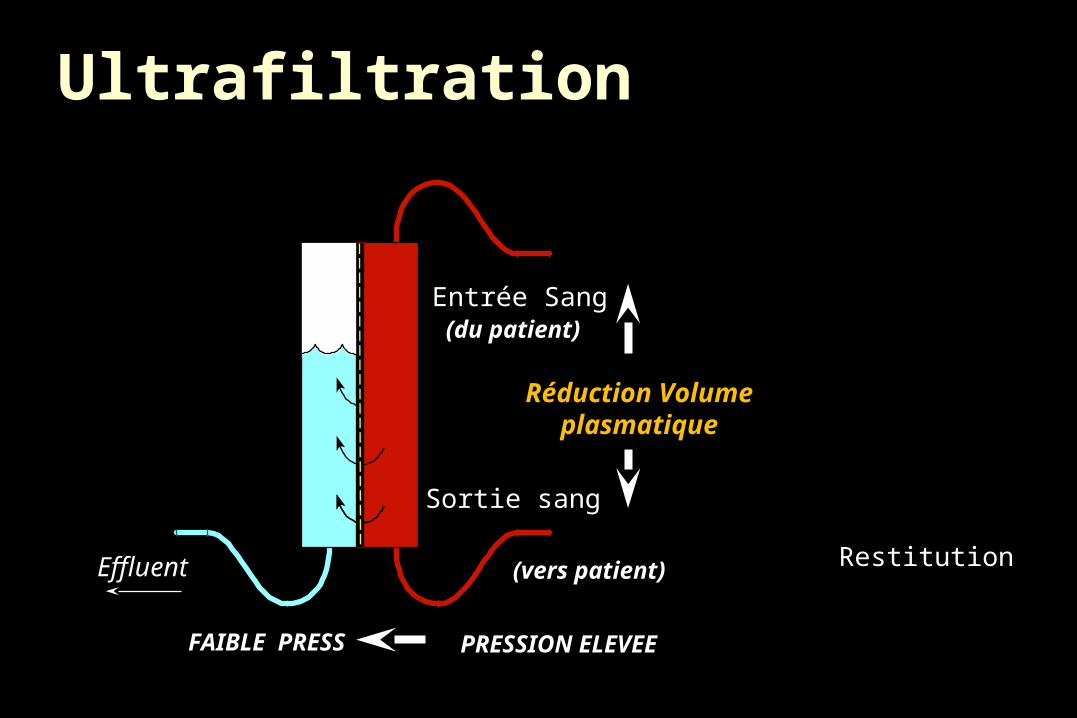
Entrée Sang
Sortie sang
Effluent
(du patient)
(vers patient)
PRESSION ELEVEEFAIBLE PRESS
Réduction Volumeplasmatique
Ultrafiltration
Restitution
Différences HF / HD:
Modalités d’équilibration Poids moléculaire des substances éliminées
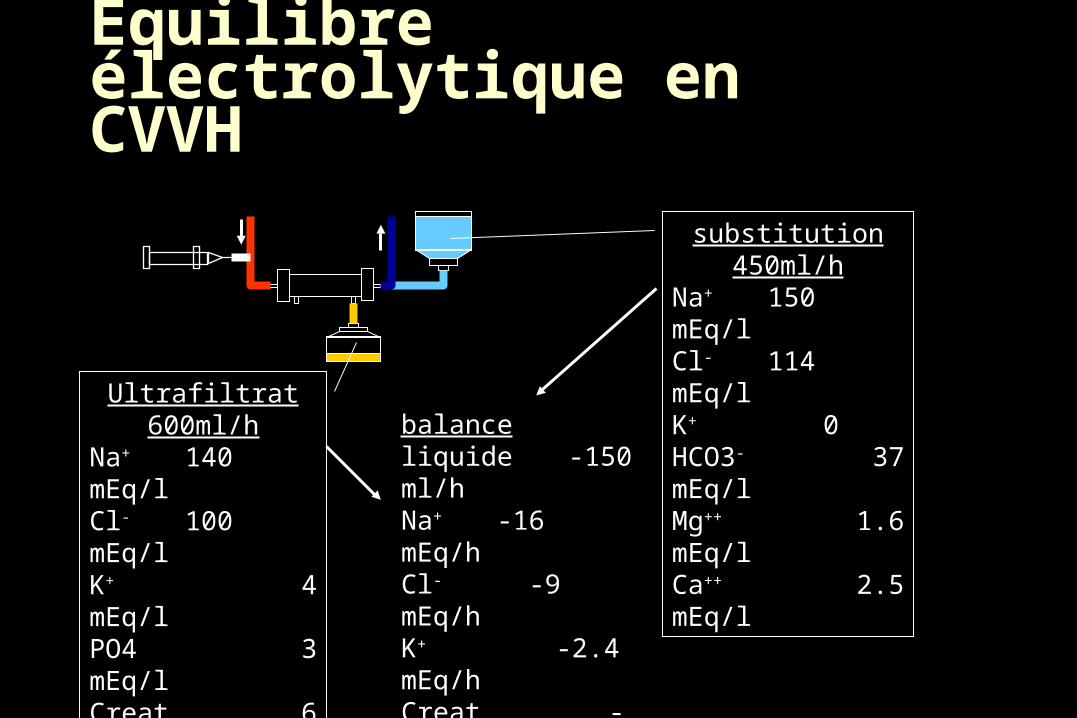
Equilibre électrolytique en CVVH
substitution450ml/h
Na+ 150 mEq/lCl- 114 mEq/lK+ 0HCO3- 37 mEq/lMg++ 1.6 mEq/lCa++ 2.5 mEq/l
Ultrafiltrat600ml/h
Na+ 140 mEq/lCl- 100 mEq/lK+ 4 mEq/lPO4 3 mEq/lCreat 6 mg/dlurée 80 mg/dl
balanceliquide -150 ml/hNa+ -16 mEq/hCl- -9 mEq/hK+ -2.4 mEq/hCreat -36 mg/hurée -480 mg/h
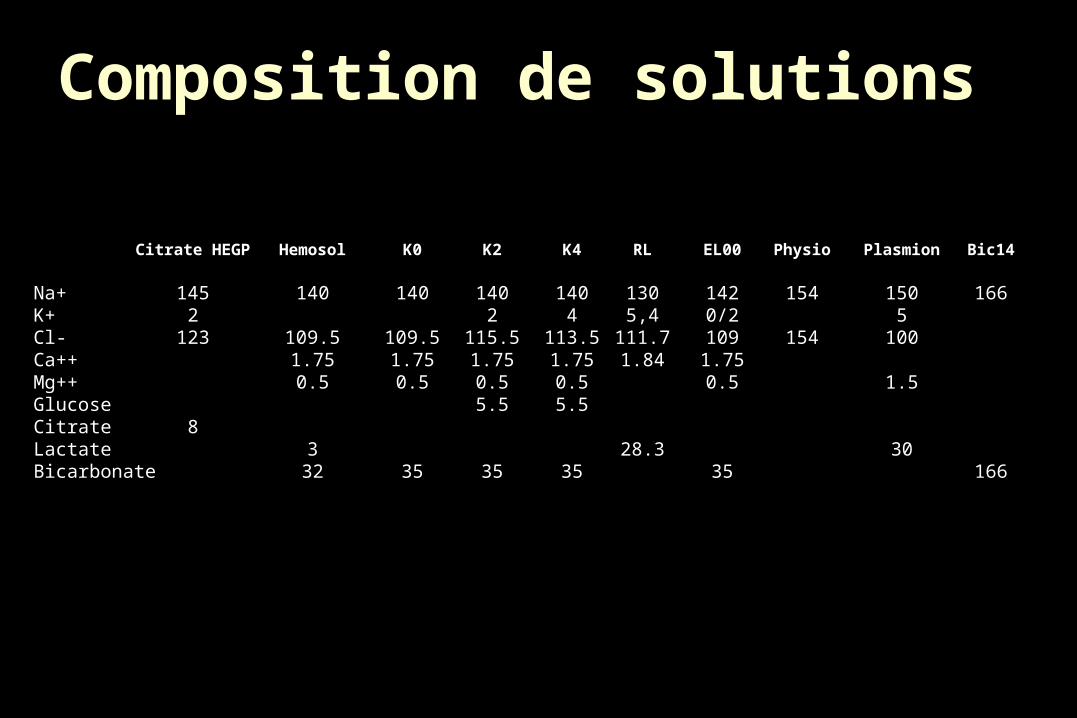
Composition de solutions
Citrate HEGP Hemosol K0 K2 K4 RL EL00 Physio Plasmion Bic14
Na+ 145 140 140 140 140 130 142 154 150 166K+ 2 2 4 5,4 0/2 5Cl- 123 109.5 109.5 115.5 113.5 111.7 109 154 100Ca++ 1.75 1.75 1.75 1.75 1.84 1.75Mg++ 0.5 0.5 0.5 0.5 0.5 1.5Glucose 5.5 5.5Citrate 8Lactate 3 28.3 30Bicarbonate 32 35 35 35 35 166
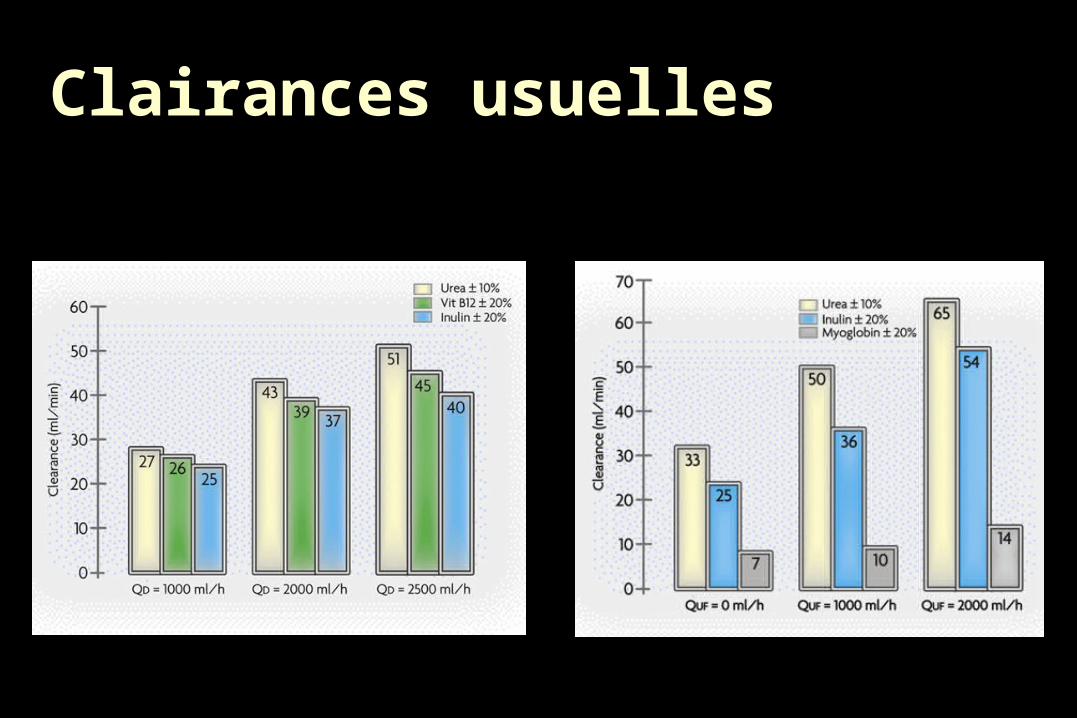
Clairances usuelles
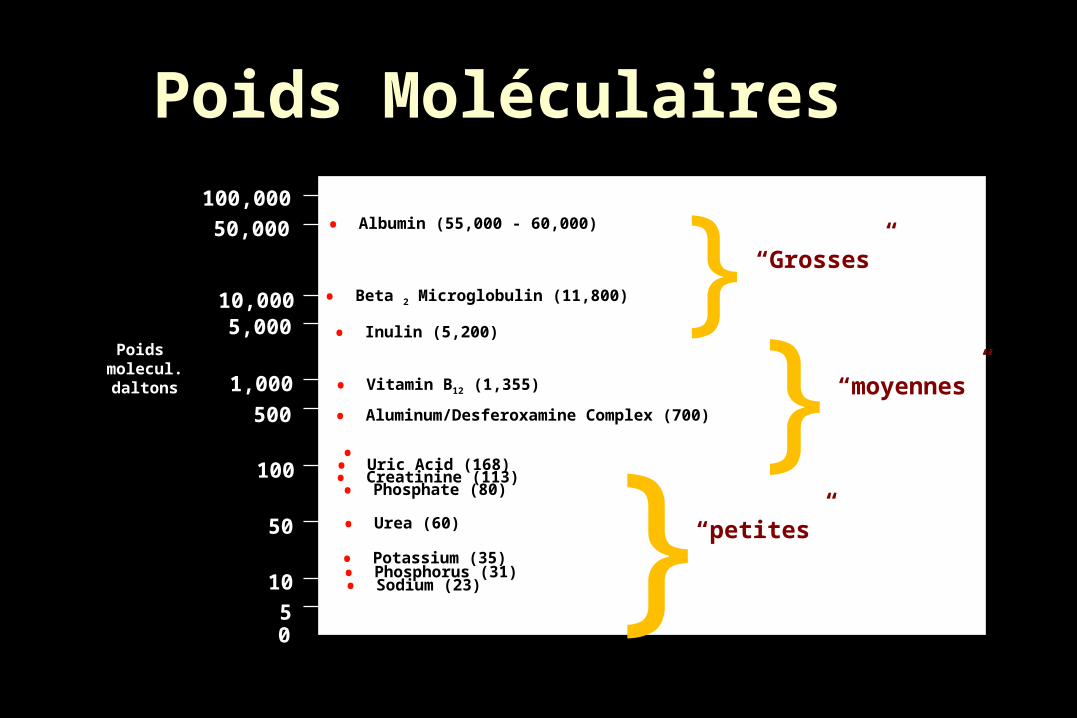
• Albumin (55,000 - 60,000)
• Beta 2 Microglobulin (11,800)
• Inulin (5,200)
• Vitamin B12 (1,355)
• Aluminum/Desferoxamine Complex (700)
• Glucose (180)• Uric Acid (168)• Creatinine (113)• Phosphate (80)
• Urea (60)
• Phosphorus (31)• Sodium (23)
• Potassium (35)
100,000
50,000
10,0005,000
1,000
500
100
50
10
50
Poids molecul. daltons
}
}}
“petites”
“moyennes”
“Grosses”
Poids Moléculaires
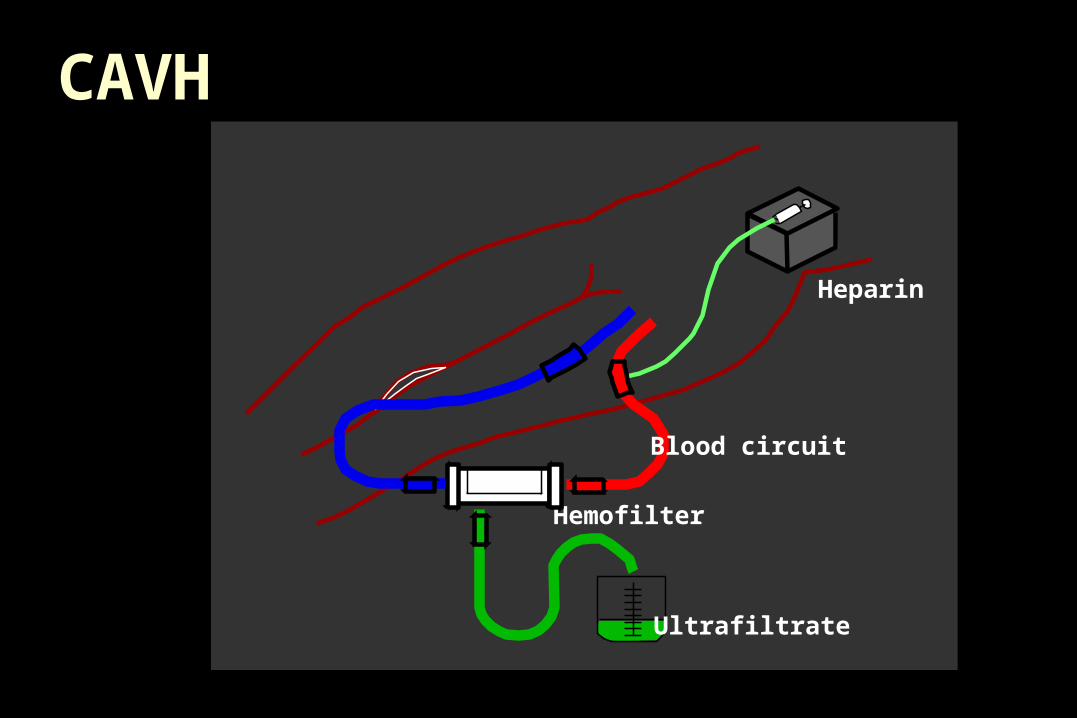
CAVH
Blood circuit
Ultrafiltrate
Hemofilter
Heparin
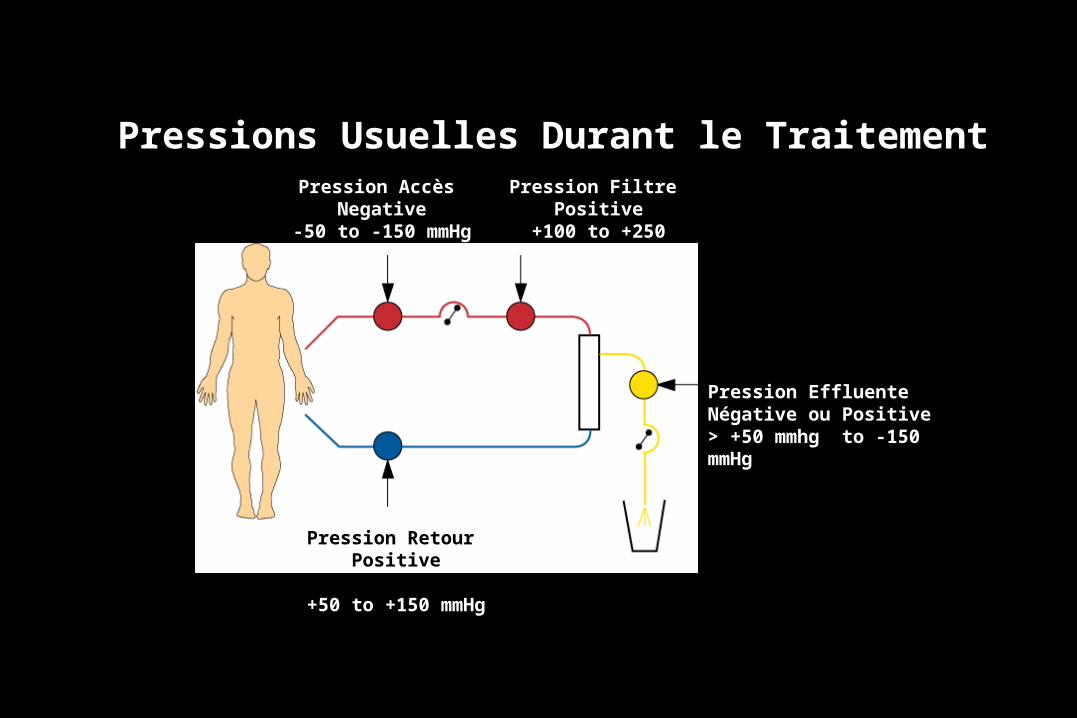
Pressions Usuelles Durant le TraitementPression Accès
Negative-50 to -150 mmHg
Pression Filtre Positive
+100 to +250 mmHg
Pression Retour Positive
+50 to +150 mmHg
Pression EffluenteNégative ou Positive> +50 mmhg to -150 mmHg
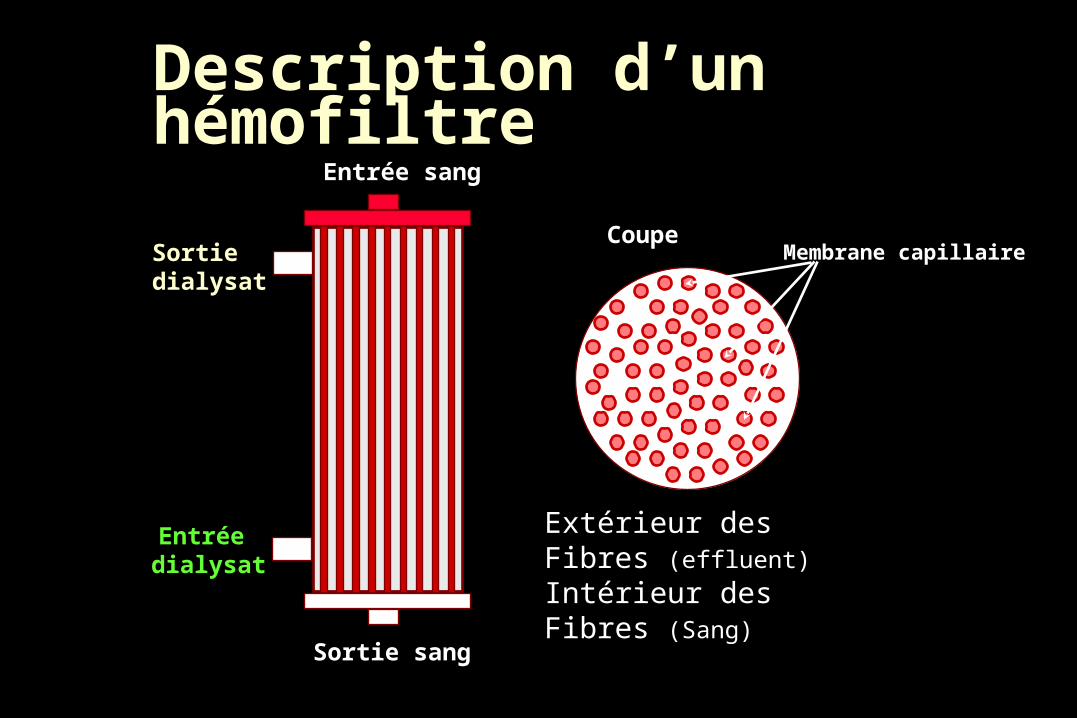
Description d’un hémofiltreEntrée sang
Sortie sang
Entrée dialysat
Sortie dialysat
Extérieur des Fibres (effluent)
Intérieur des Fibres (Sang)
CoupeMembrane capillaire
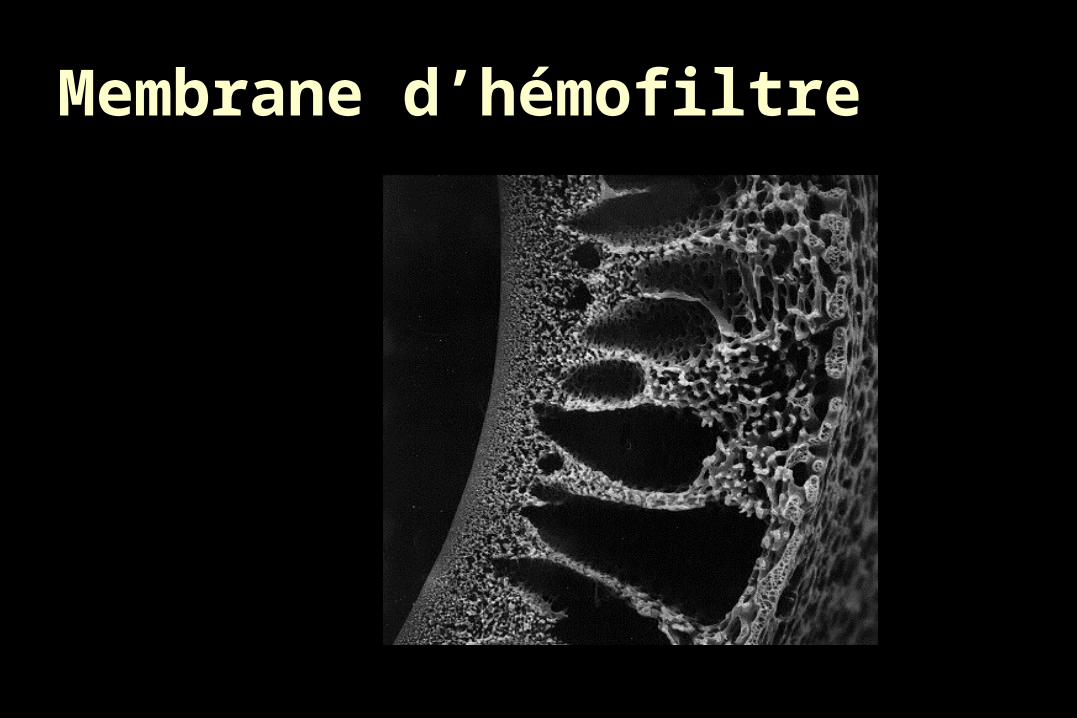
Membrane d’hémofiltre
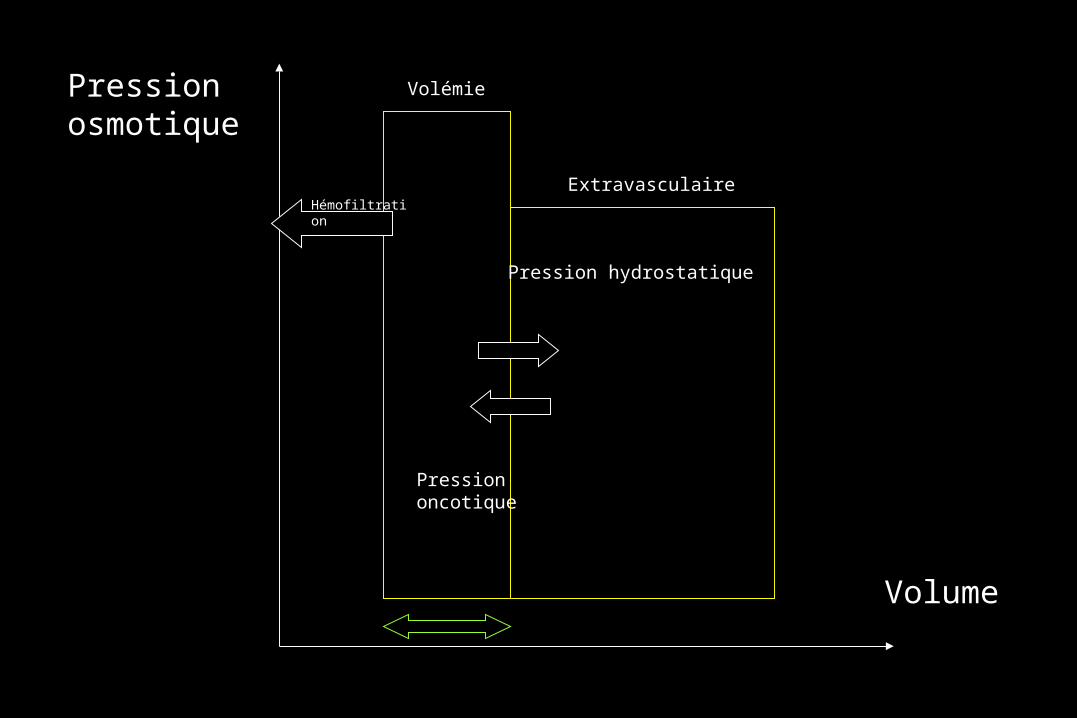
Pressionosmotique
Volume
Pression hydrostatique
Pressiononcotique
Volémie
ExtravasculaireHémofiltration
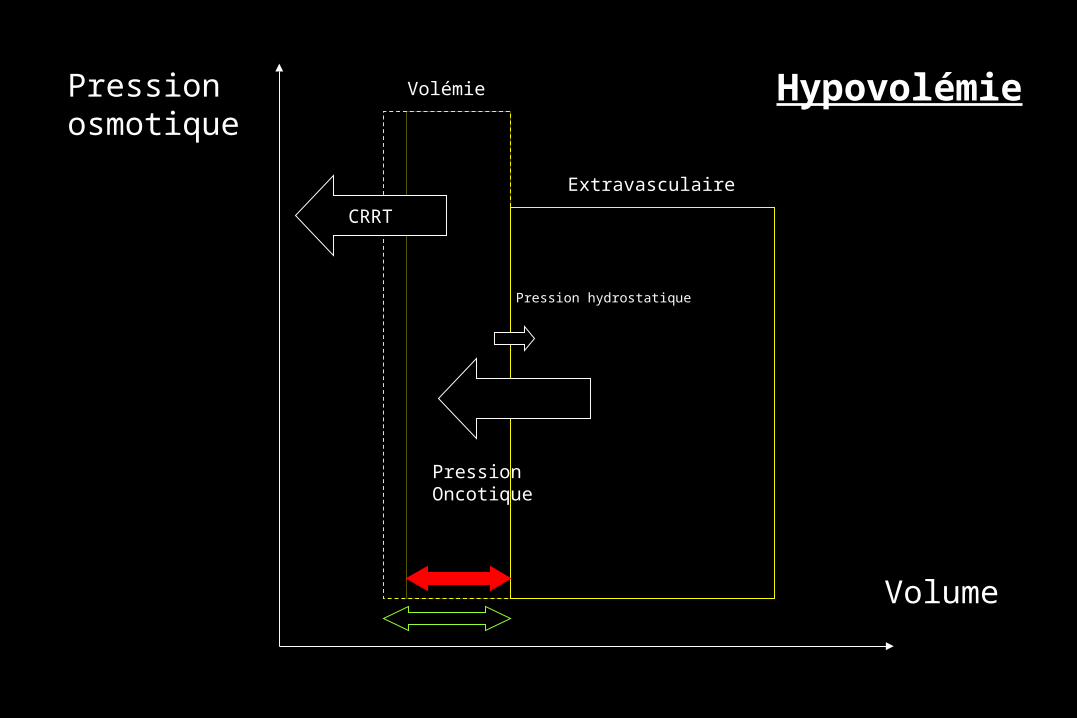
Pressionosmotique
Volume
Pression hydrostatique
PressionOncotique
Volémie
Extravasculaire
Hypovolémie
CRRT
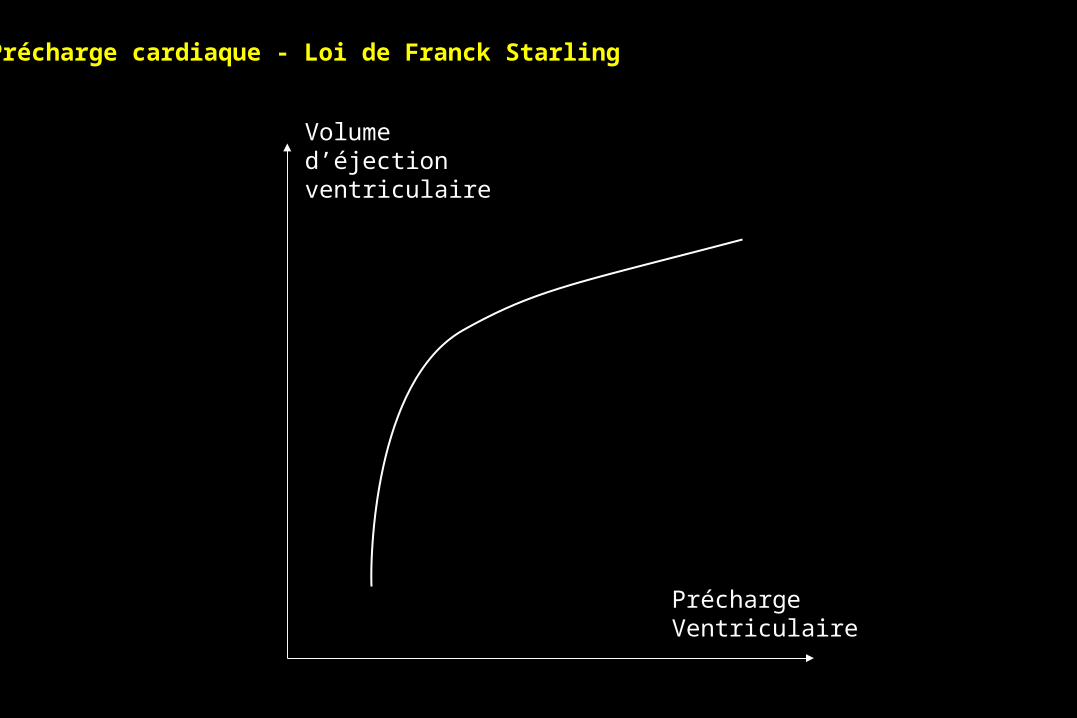
Précharge cardiaque - Loi de Franck Starling
Volume d’éjectionventriculaire
PréchargeVentriculaire
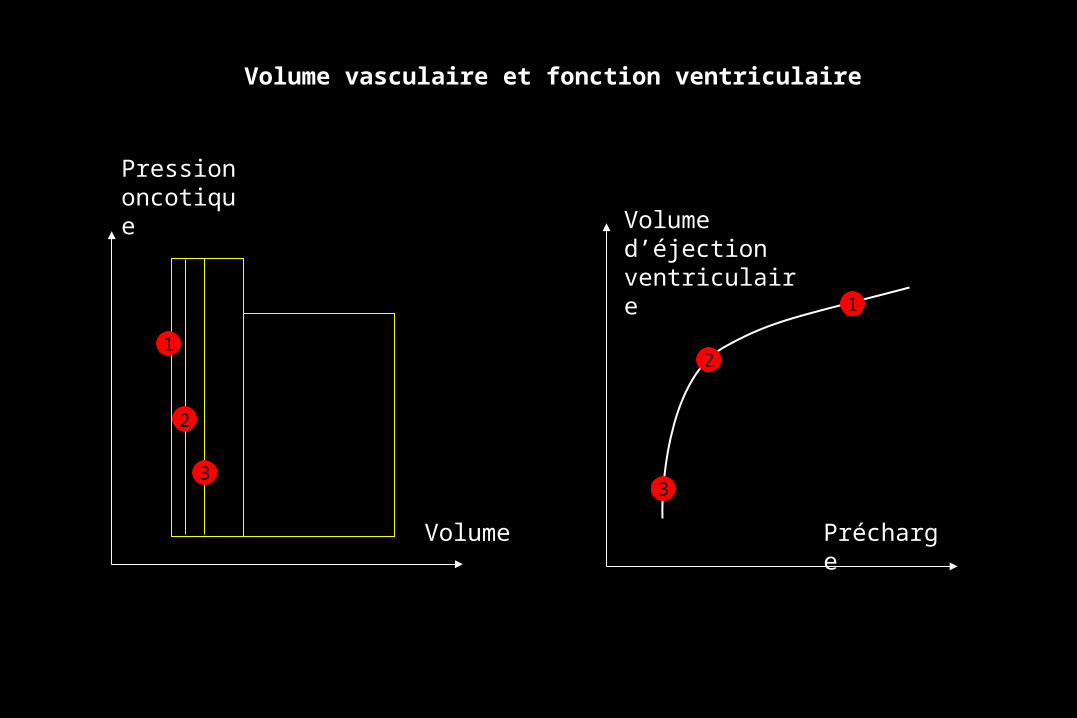
Volume vasculaire et fonction ventriculaire
Volume d’éjectionventriculaire
Précharge
Pression oncotique
Volume
1
1
2
2
33
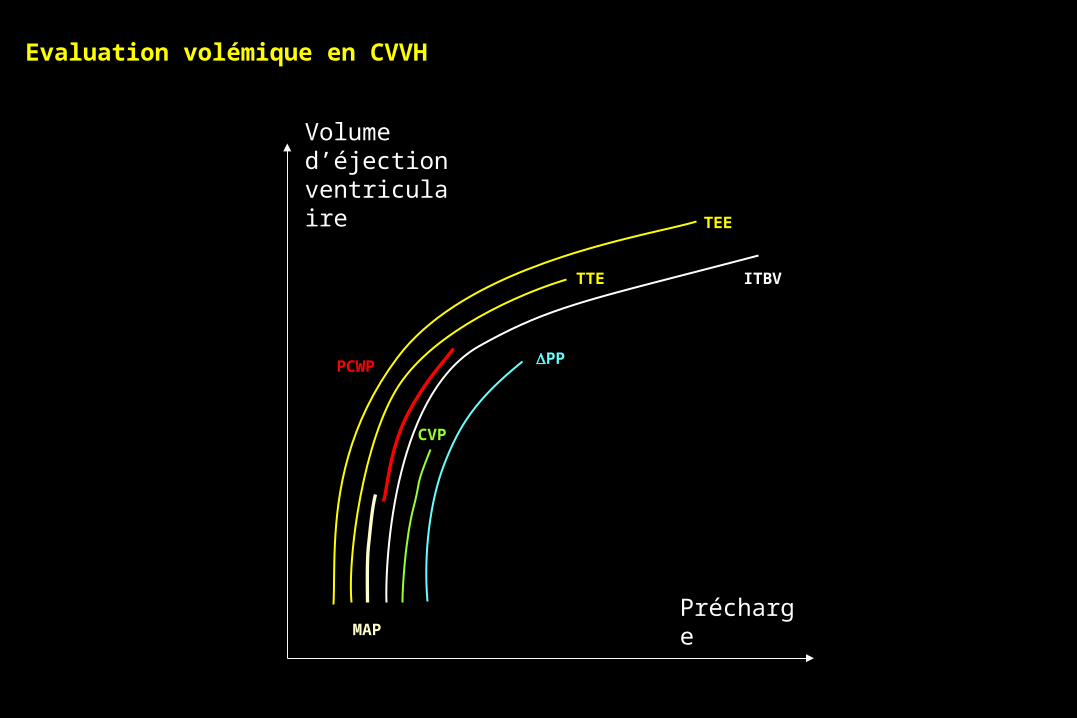
Evaluation volémique en CVVH
Volume d’éjectionventriculaire
Précharge
3
CVP
MAP
TTE
TEE
ITBV
PCWP PP
Points «délicats»
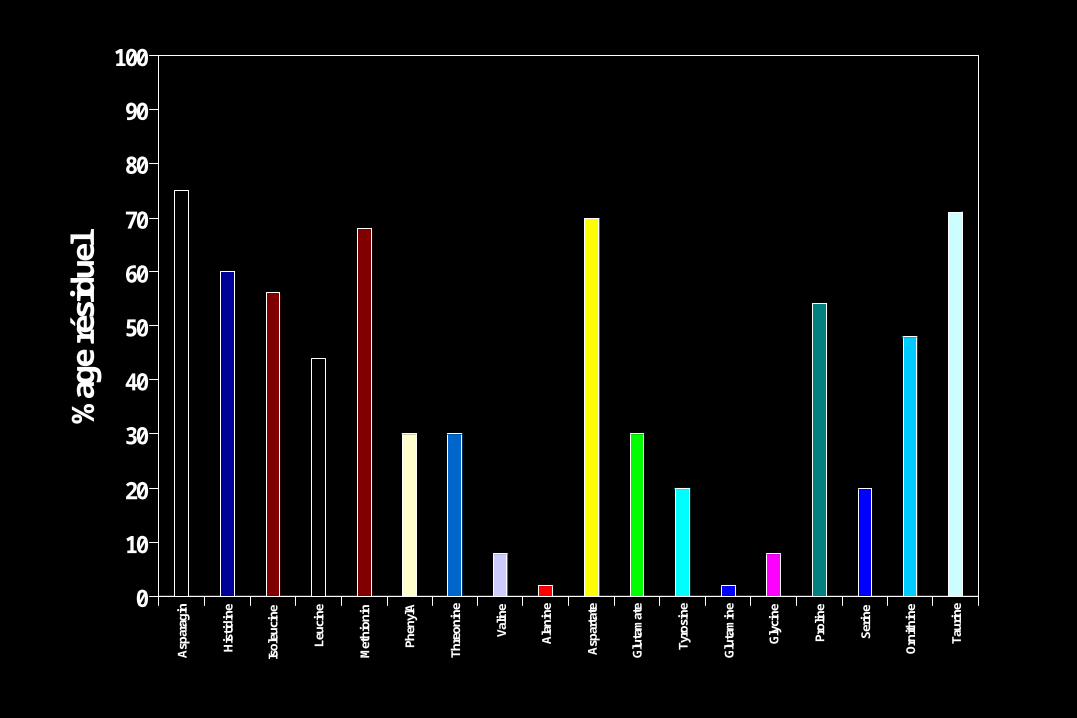
Température ; Elimination de nutriements ; Cathéters ; Solutions de substitution.
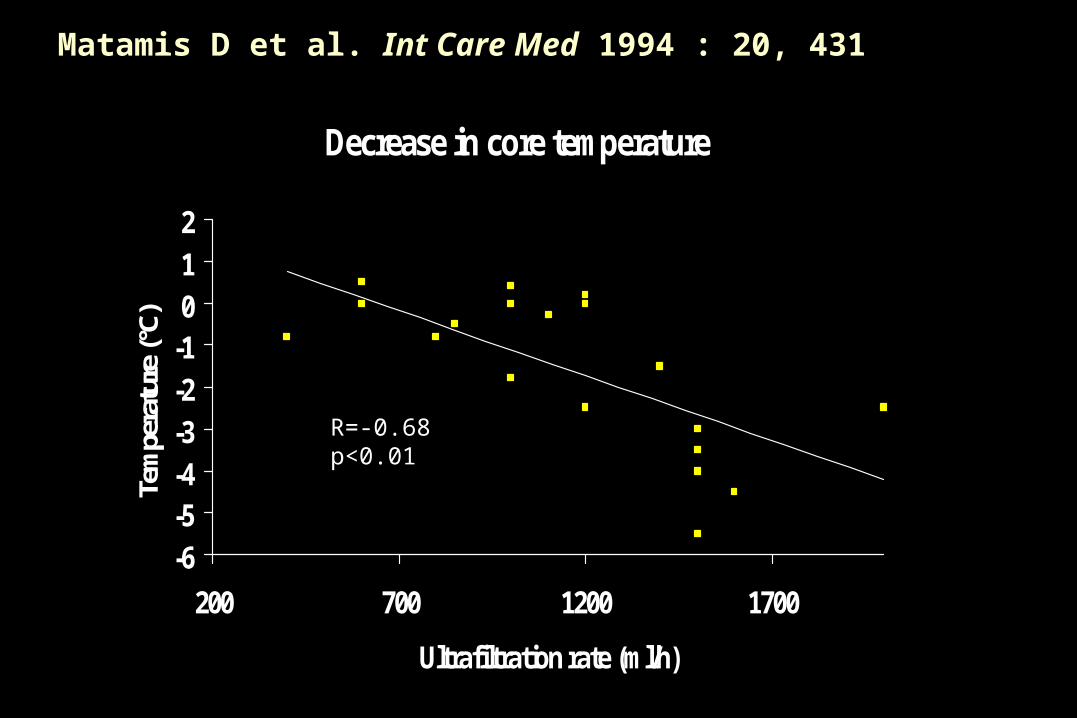
Matamis D et al. Int Care Med 1994 : 20, 431
Decrease in core temperature
-6-5-4-3-2-1012
200 700 1200 1700
Ultrafiltration rate (ml/h)
Tem
pera
ture
(°C)
R=-0.68p<0.01
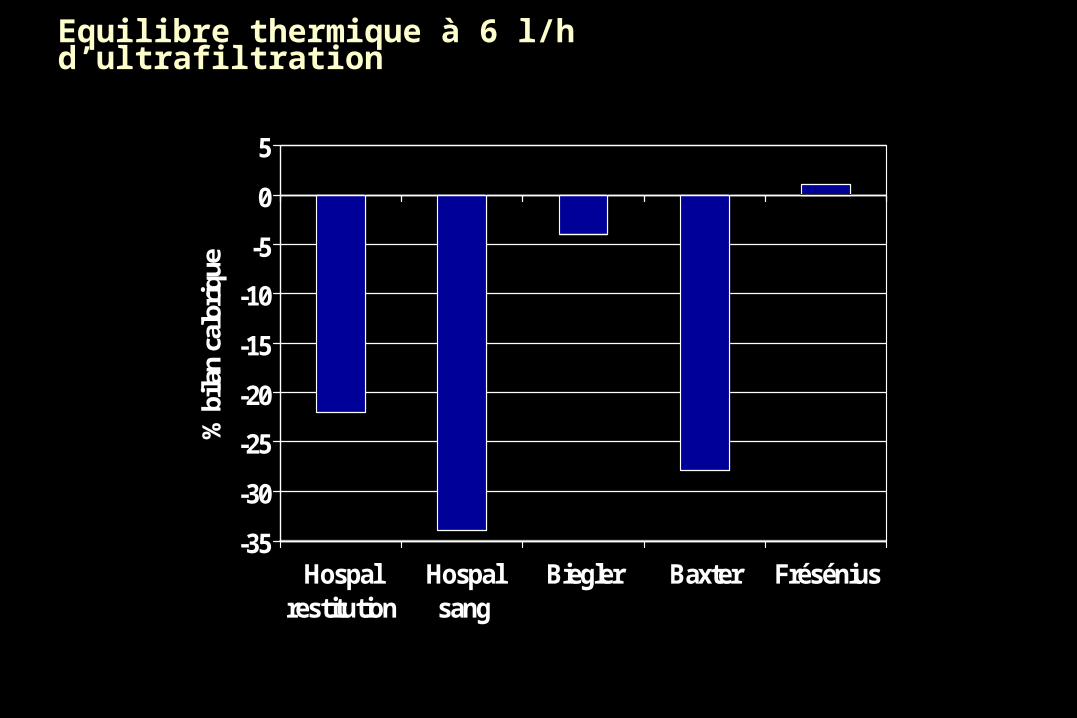
Equilibre thermique à 6 l/h d’ultrafiltration
-35
-30
-25
-20
-15
-10
-5
0
5
% b
ilan
calo
riqu
e
Hospalrestitution
Hospalsang
Biegler Baxter Frésénius
0
10
20
30
40
50
60
70
80
90
100%
age
rési
duel
Asp
arag
in
His
tidin
e
Isol
euci
ne
Leuc
ine
Met
hion
in
Phen
ylA
Thre
onin
e
Valin
e
Ala
nine
Asp
arta
te
Glu
tam
ate
Tyro
sine
Glu
tam
ine
Gly
cine
Prol
ine
Serin
e
Orn
ithin
e
Taur
ine
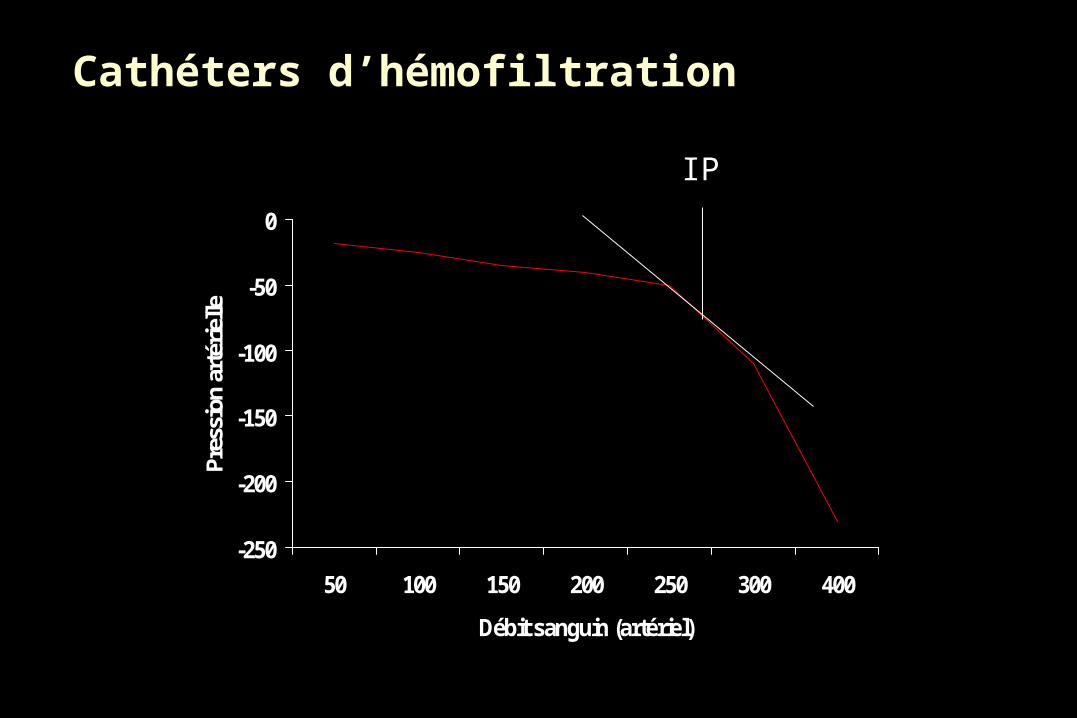
Cathéters d’hémofiltration
-250
-200
-150
-100
-50
0
50 100 150 200 250 300 400
Débit sanguin (artériel)
Pres
sion
art
érie
lle
IP
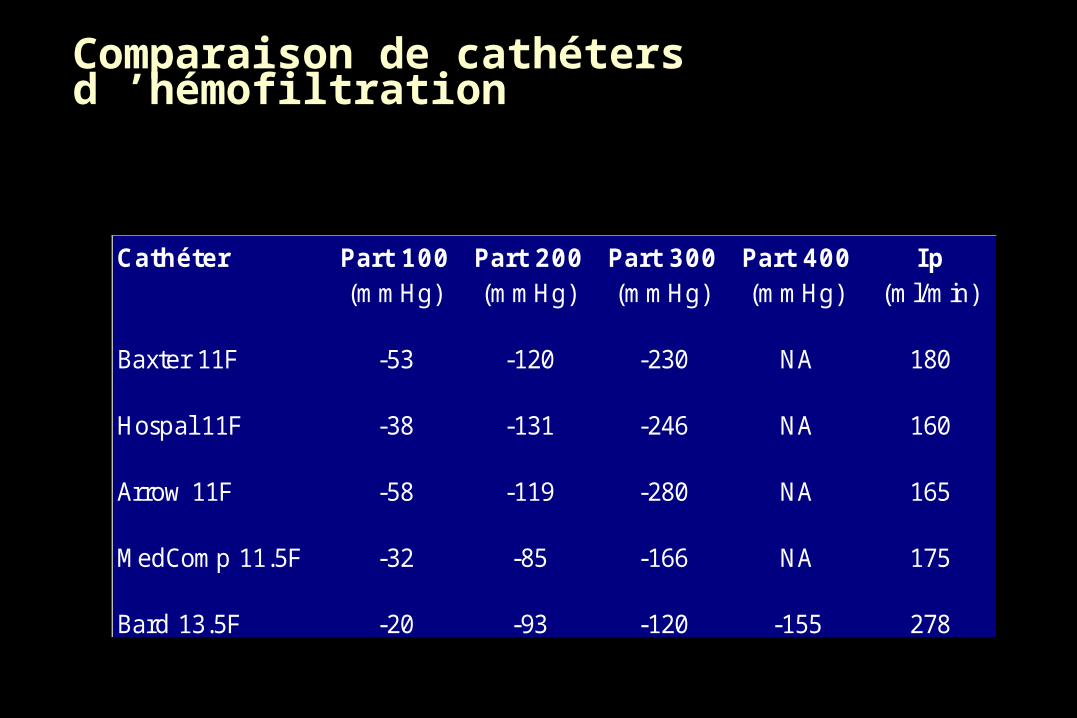
Comparaison de cathéters d ’hémofiltration
Cathéter Part 100 Part 200 Part 300 Part 400 Ip(mmHg) (mmHg) (mmHg) (mmHg) (ml/min)
Baxter 11F -53 -120 -230 NA 180
Hospal 11F -38 -131 -246 NA 160
Arrow 11F -58 -119 -280 NA 165
MedComp 11.5F -32 -85 -166 NA 175
Bard 13.5F -20 -93 -120 -155 278
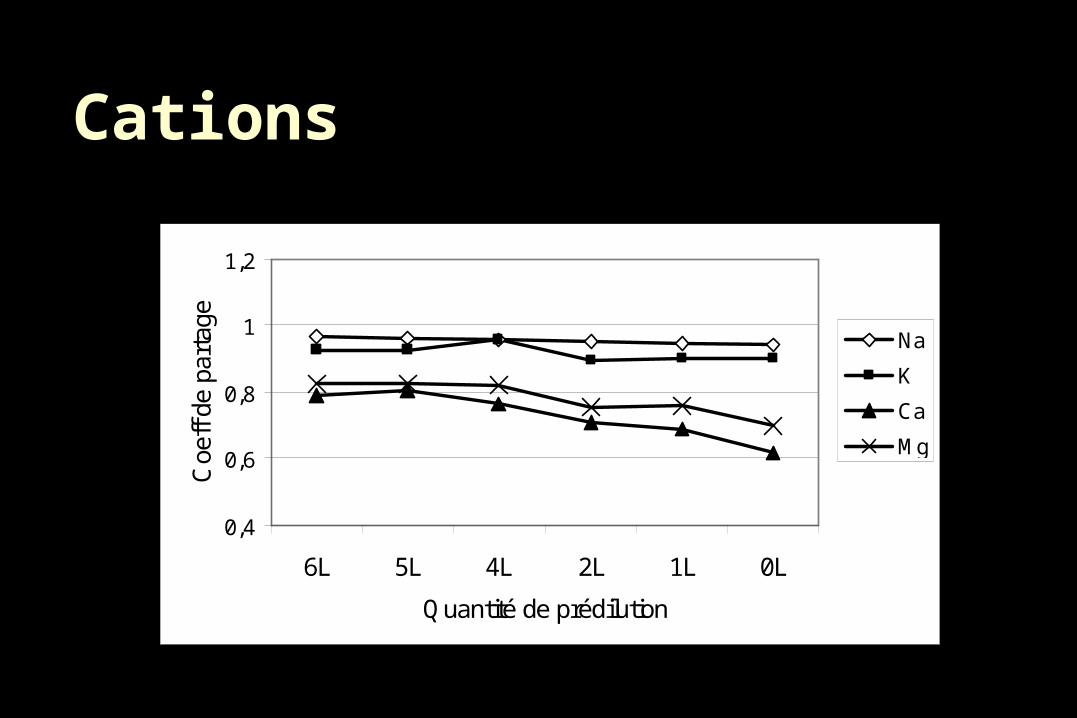
Cations
0,4
0,6
0,8
1
1,2
6L 5L 4L 2L 1L 0L
Quantité de prédilution
Coe
ff de
par
tage
Na
K
Ca
Mg
Indications spécifiques de l’HF
Etats septiques sévères Etats inflammatoires sévères
0
5
10
15
20
25
30
35
Témoin 1hr post-sepsis
4hrs post-HFC
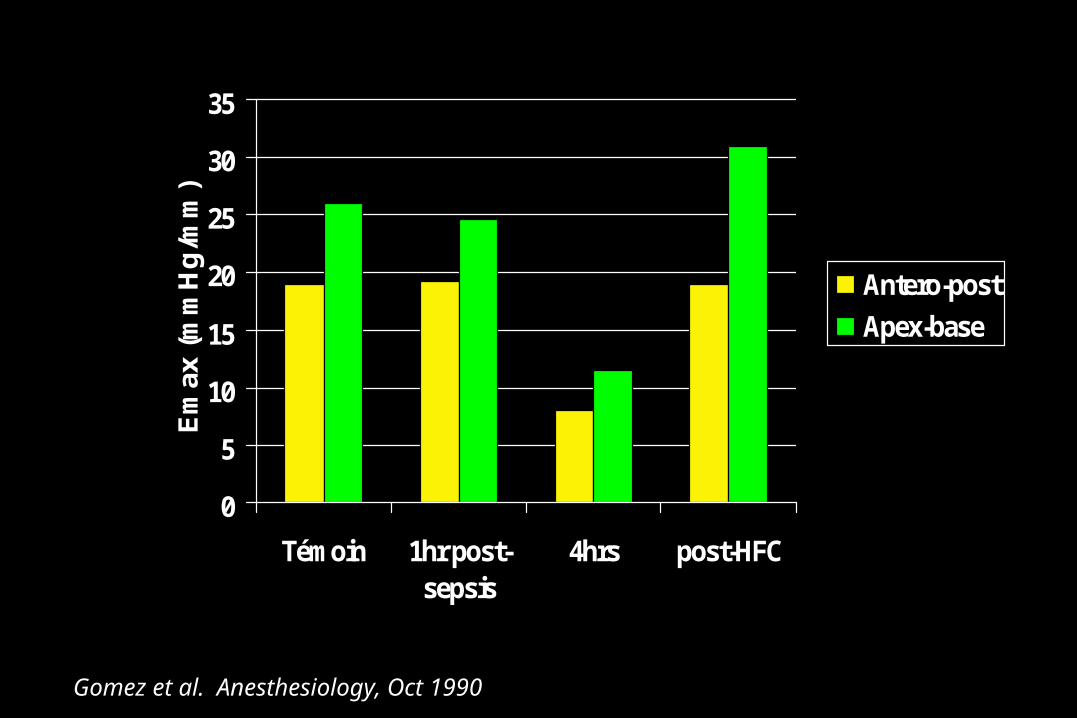
Em
ax (
mm
Hg
/mm
)
Antero-post
Apex-base
Gomez et al. Anesthesiology, Oct 1990
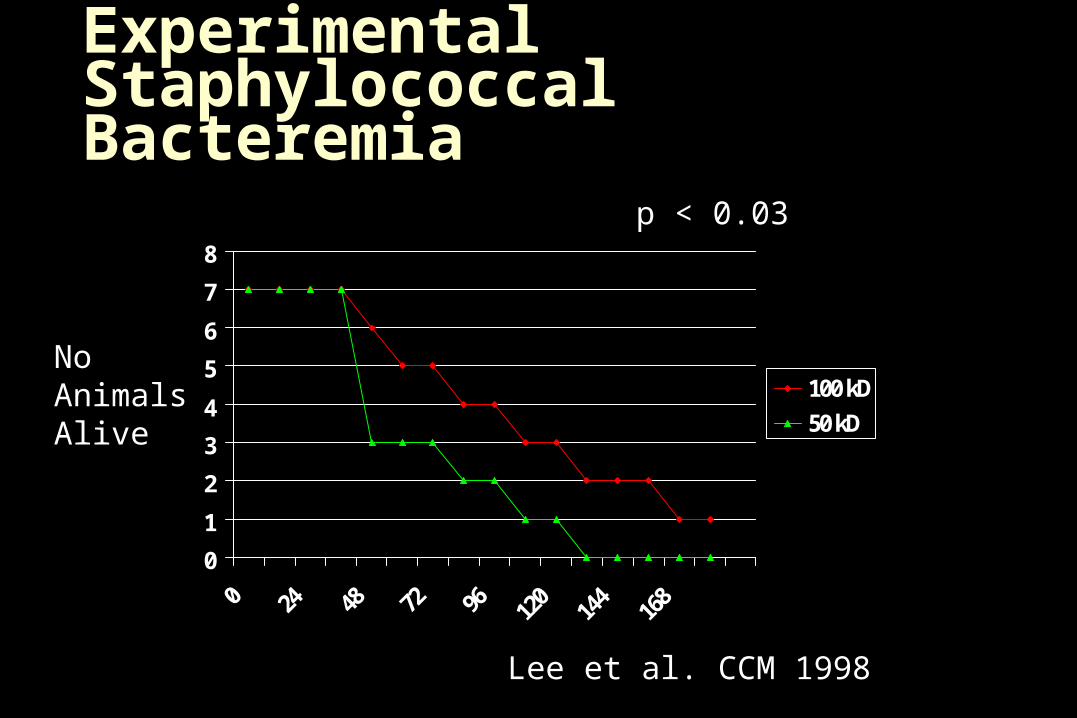
Filter Pore Size in Experimental Staphylococcal Bacteremia
0
1
2
3
4
5
6
7
8
0 24 48 72 96 120
144
168
100 kD
50 kD
NoAnimalsAlive
p < 0.03
Lee et al. CCM 1998
• TNF
• IL-1
• IL-8
• IL-10
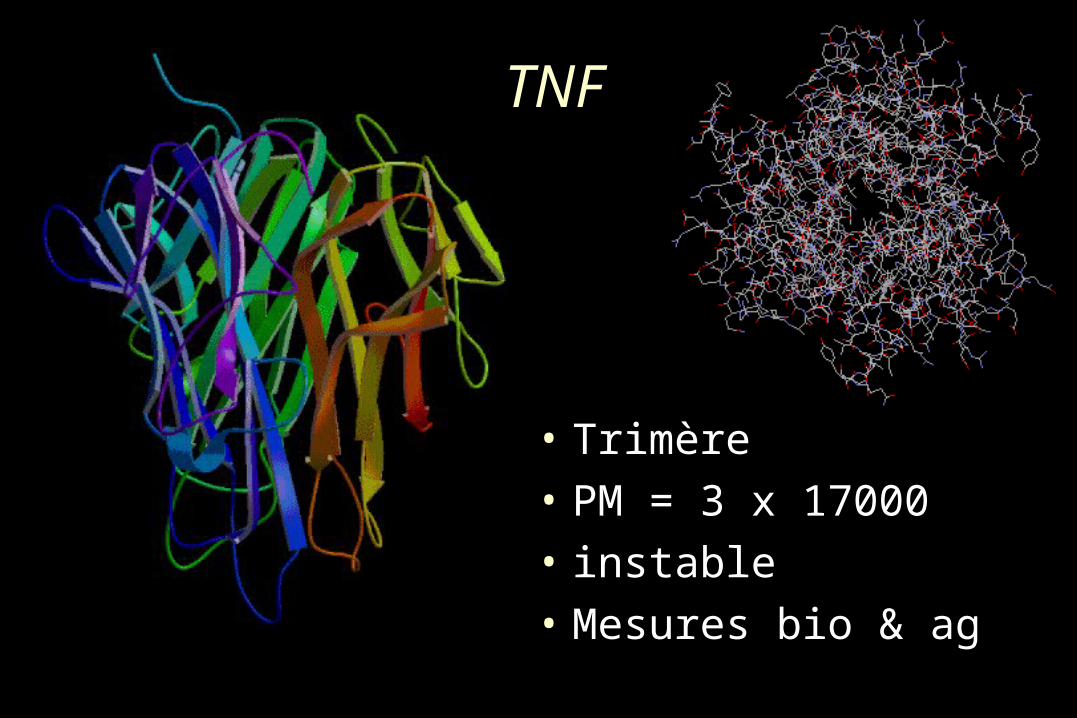
TNF
• Trimère
• PM = 3 x 17000
• instable
• Mesures bio & ag
IL-10
• Cytokine « protectrice »
• PM = 14000
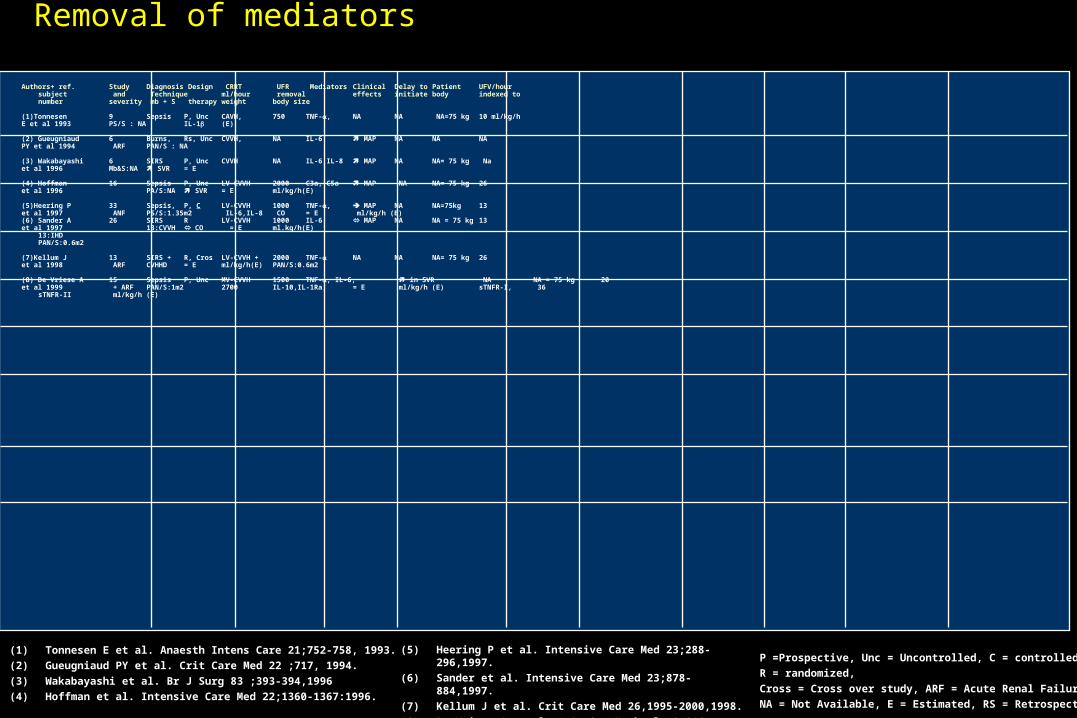
Removal of mediators
(1) Tonnesen E et al. Anaesth Intens Care 21;752-758, 1993.
(2) Gueugniaud PY et al. Crit Care Med 22 ;717, 1994.
(3) Wakabayashi et al. Br J Surg 83 ;393-394,1996
(4) Hoffman et al. Intensive Care Med 22;1360-1367:1996.
Authors+ ref. Study Diagnosis Design CRRT UFR Mediators Clinical Delay to Patient UFV/hoursubject and Technique ml/hour removal effects initiate body indexed tonumber severity mb + S therapy weight body size
(1)Tonnesen 9 Sepsis P, Unc CAVH, 750 TNF-, NA NA NA=75 kg 10 ml/kg/hE et al 1993 PS/S : NA IL-1 (E)
(2) Gueugniaud 6 Burns, Rs, Unc CVVH, NA IL-6 MAP NA NA NAPY et al 1994 ARF PAN/S : NA
(3) Wakabayashi 6 SIRS P, Unc CVVH NA IL-6,IL-8 MAP NA NA= 75 kg Na et al 1996 Mb&S:NA SVR = E
(4) Hoffman 16 Sepsis P, Unc LV-CVVH 2000 C3a, C5a MAP NA NA= 75 kg 26et al 1996 PA/S:NA SVR = E ml/kg/h(E)
(5)Heering P 33 Sepsis, P, C LV-CVVH 1000 TNF-, MAP NA NA=75kg 13et al 1997 ANF PS/S:1.35m2 IL-6,IL-8 CO = E ml/kg/h (E) (6) Sander A 26 SIRS R LV-CVVH 1000 IL-6 MAP NA NA = 75 kg 13et al 1997 13:CVVH CO = E ml.kg/h(E)
13:IHDPAN/S:0.6m2
(7)Kellum J 13 SIRS + R, Cros LV-CVVH + 2000 TNF- NA NA NA= 75 kg 26 et al 1998 ARF CVHHD = E ml/kg/h(E) PAN/S:0.6m2
(8) De Vriese A 15 Sepsis P, Unc MV-CVVH 1500 TNF-, IL-6, in SVR NA NA = 75 kg 20et al 1999 + ARF PAN/S:1m2 2700 IL-10,IL-1Ra, = E ml/kg/h (E) sTNFR-I, 36
sTNFR-II ml/kg/h (E)
(5) Heering P et al. Intensive Care Med 23;288-296,1997.
(6) Sander et al. Intensive Care Med 23;878-884,1997.
(7) Kellum J et al. Crit Care Med 26,1995-2000,1998.
(8) De Vriese A et al. J Am Soc Nephrol 10;846-53:1999
P =Prospective, Unc = Uncontrolled, C = controlled,
R = randomized,
Cross = Cross over study, ARF = Acute Renal Failure,
NA = Not Available, E = Estimated, RS = Retrospective
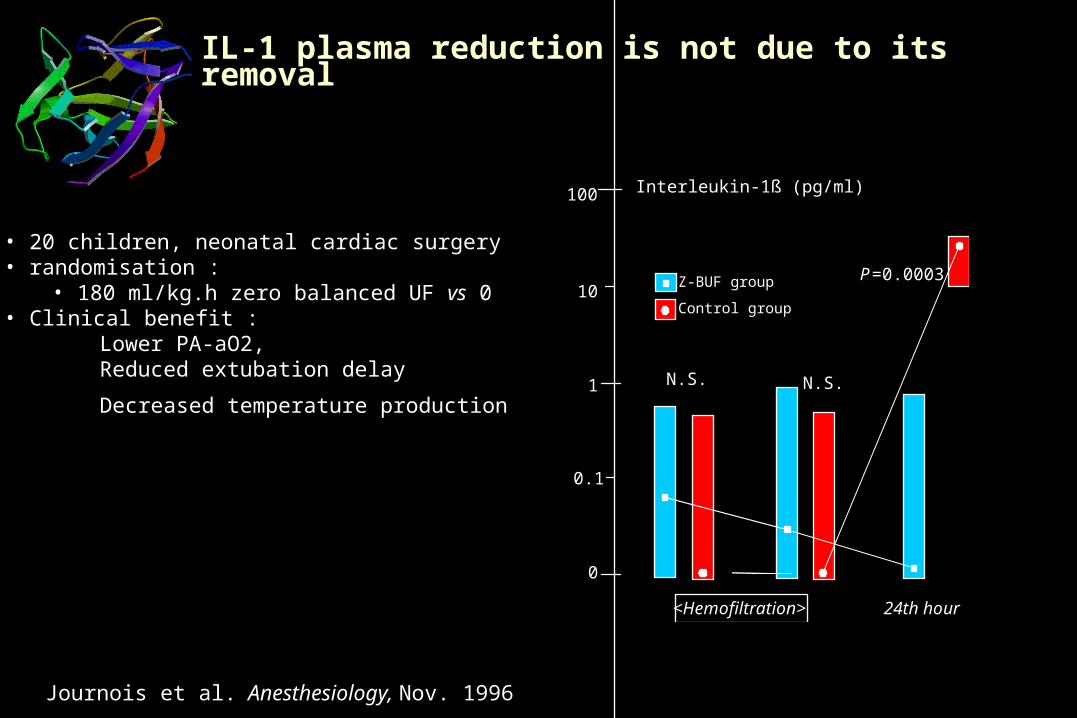
IL-1 plasma reduction is not due to its removalIL-1 plasma reduction is not due to its removal
Z-BUF group
Control group
<Hemofiltration> 24th hour
Interleukin-1ß (pg/ml)100
10
1
0.1
0
N.S. N.S.
P=0.0003
Journois et al. Anesthesiology, Nov. 1996
• 20 children, neonatal cardiac surgery20 children, neonatal cardiac surgery• randomisation : randomisation :
• 180 ml/kg.h zero balanced UF 180 ml/kg.h zero balanced UF vsvs 0 0• Clinical benefit :Clinical benefit :
Lower PA-aO2,Lower PA-aO2,Reduced extubation delayReduced extubation delay
Decreased temperature productionDecreased temperature production
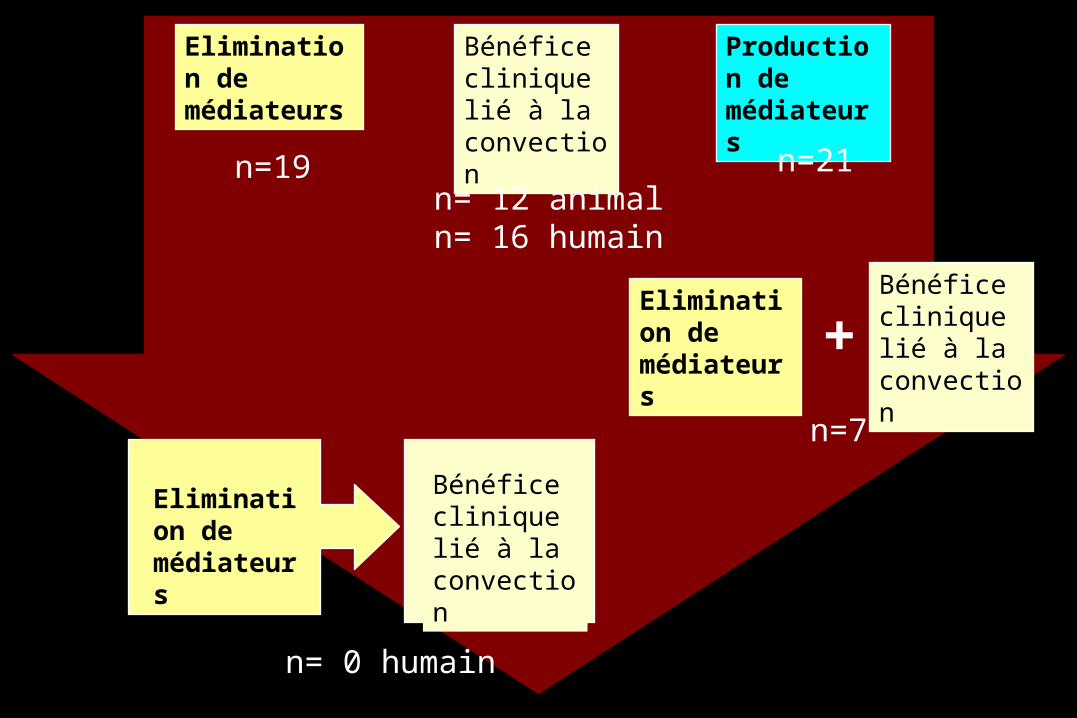
Elimination de médiateurs
Production de médiateurs
Bénéfice clinique lié à la convection
Elimination de médiateurs
Elimination de médiateurs
Bénéfice clinique lié à la convection
+
Bénéfice clinique lié à la convection n=21
n=7
n= 0 humain
n=19n= 12 animal n= 16 humain
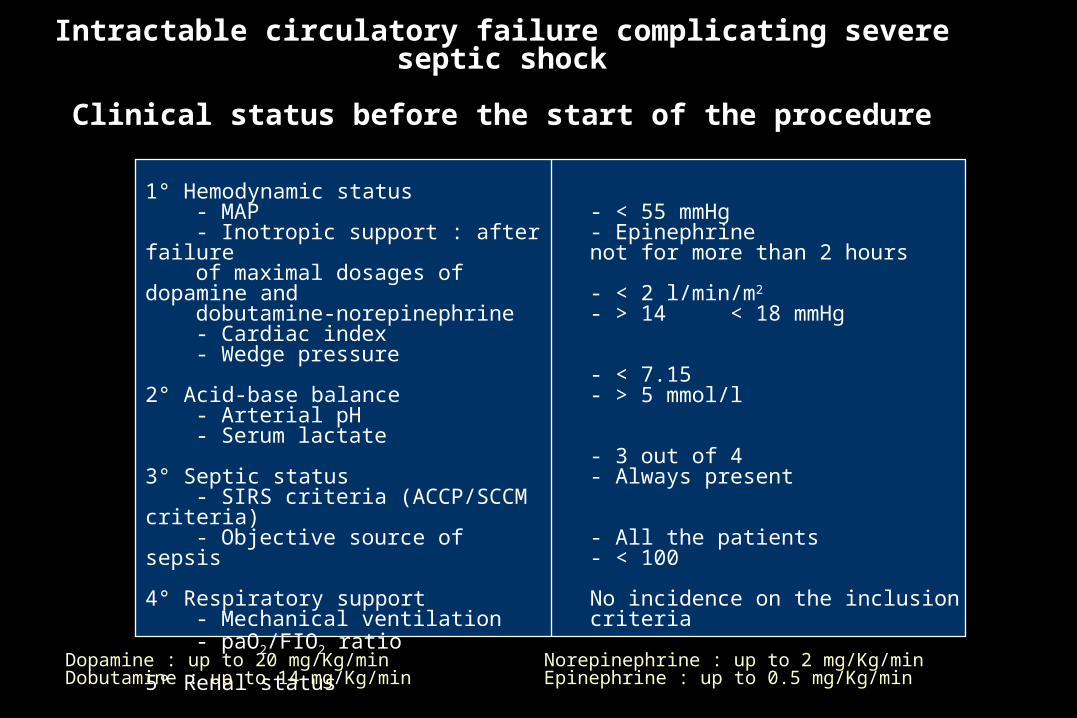
1° Hemodynamic status- MAP- Inotropic support : after failure
of maximal dosages of dopamine and
dobutamine-norepinephrine- Cardiac index- Wedge pressure
2° Acid-base balance- Arterial pH- Serum lactate
3° Septic status- SIRS criteria (ACCP/SCCM
criteria)- Objective source of sepsis
4° Respiratory support- Mechanical ventilation- paO2/FIO2 ratio
5° Renal status
- < 55 mmHg- Epinephrine not for more than 2 hours
- < 2 l/min/m2
- > 14 < 18 mmHg
- < 7.15- > 5 mmol/l
- 3 out of 4- Always present
- All the patients- < 100
No incidence on the inclusion criteria
Intractable circulatory failure complicating severe septic shock
Clinical status before the start of the procedure
Dopamine : up to 20 mg/Kg/min Norepinephrine : up to 2 mg/Kg/minDobutamine : up to 14 mg/Kg/min Epinephrine : up to 0.5 mg/Kg/min
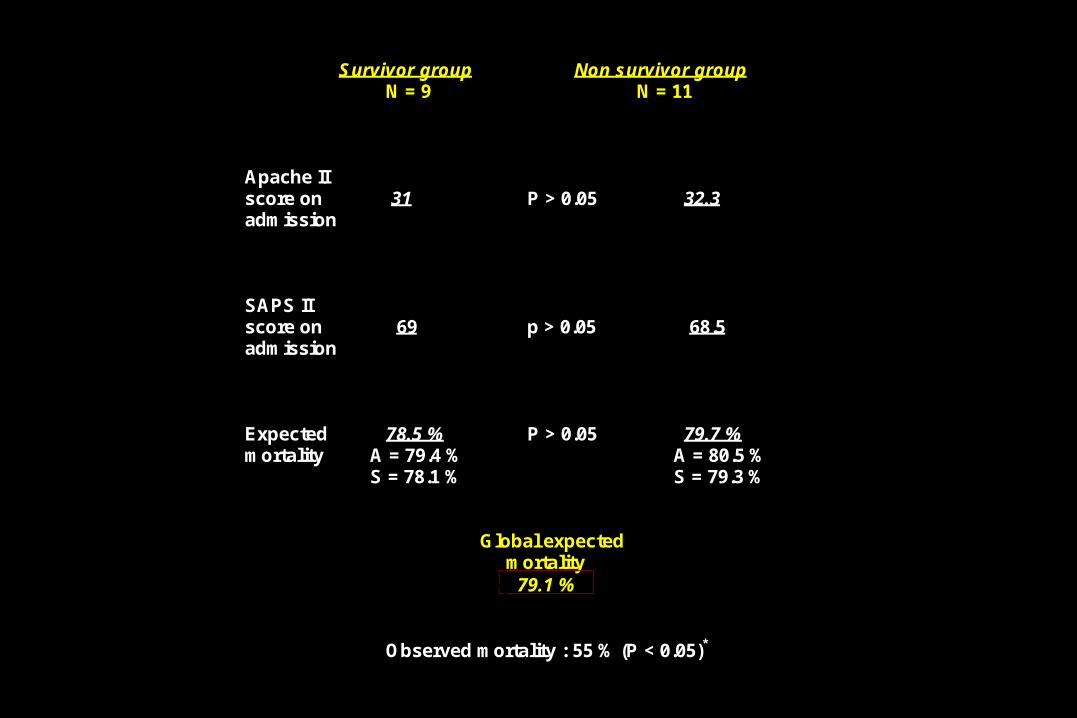
Survivor group Non survivor groupN = 9 N = 11
Apache IIscore on 31 P > 0.05 32.3admission
SAPS IIscore on 69 p > 0.05 68.5admission
Expected 78.5 % P > 0.05 79.7 %mortality A = 79.4 % A = 80.5 %
S = 78.1 % S = 79.3 %
Global expected mortality
79.1 %
Observed mortality : 55 % (P < 0.05)*
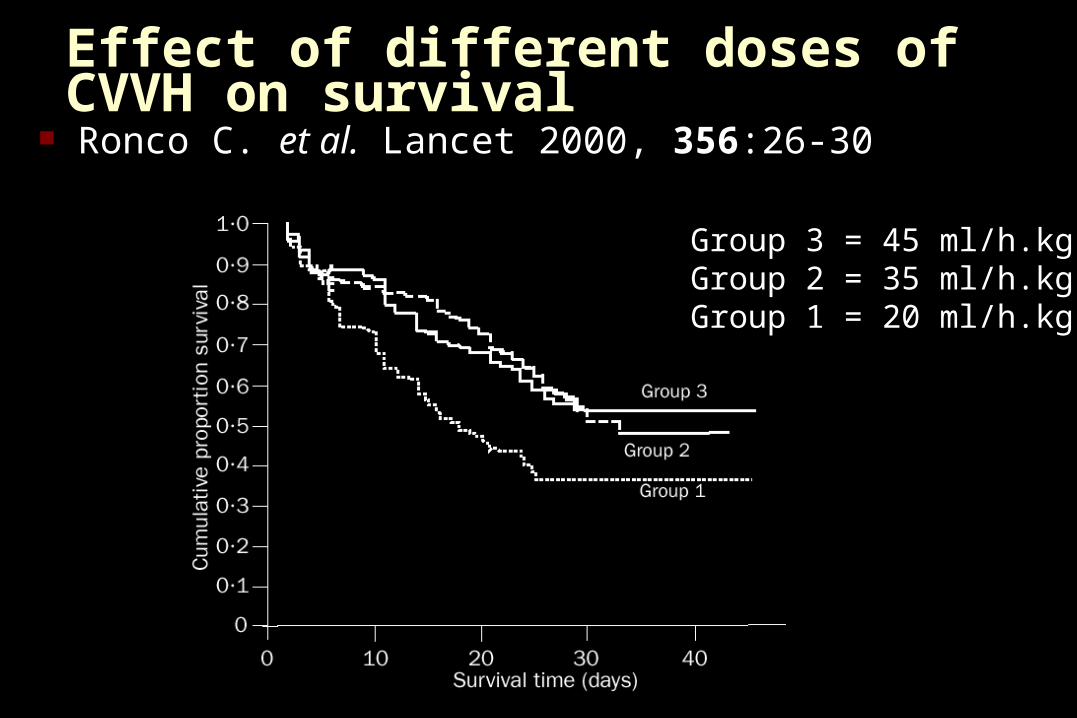
Effect of different doses of CVVH on survival Ronco C. et al. Lancet 2000, 356:26-30
Group 3 = 45 ml/h.kgGroup 2 = 35 ml/h.kgGroup 1 = 20 ml/h.kg
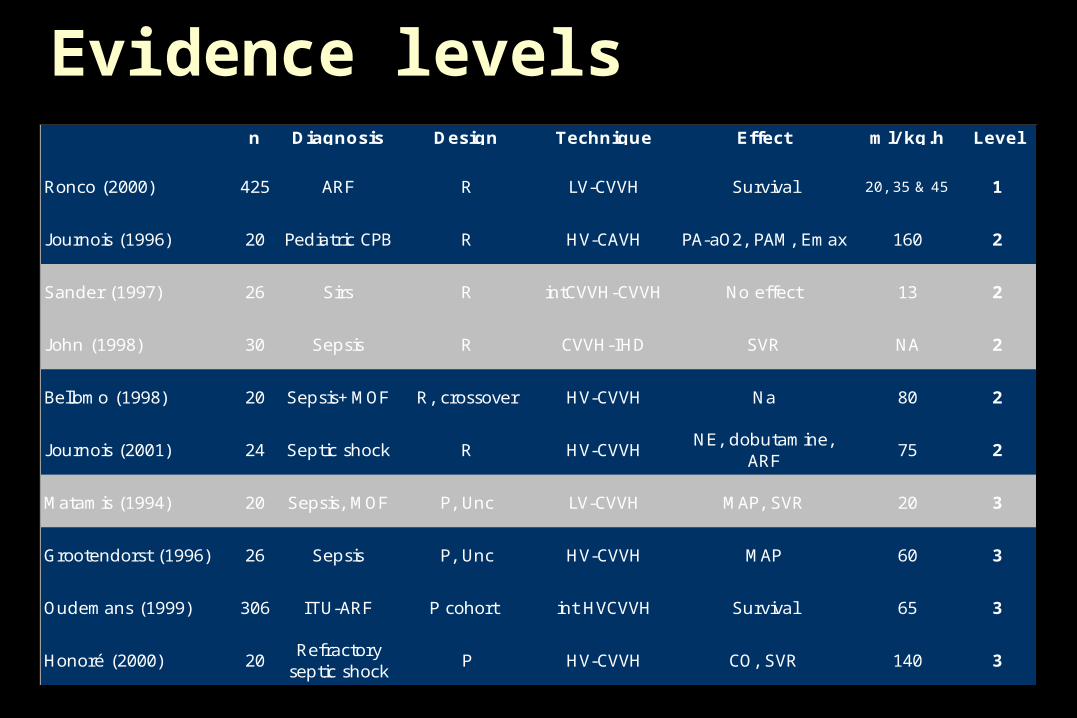
n Diagnosis Design Technique Effect ml/ kg.h Level
Ronco (2000) 425 ARF R LV-CVVH Survival 20, 35 & 45 1
J ournois (1996) 20 Pediatric CPB R HV-CAVH PA-aO2, PAM, Emax 160 2
Sander (1997) 26 Sirs R intCVVH-CVVH No effect 13 2
J ohn (1998) 30 Sepsis R CVVH-IHD SVR NA 2
Bellomo (1998) 20 Sepsis+MOF R, crossover HV-CVVH Na 80 2
J ournois (2001) 24 Septic shock R HV-CVVHNE, dobutamine,
ARF75 2
Matamis (1994) 20 Sepsis, MOF P, Unc LV-CVVH MAP, SVR 20 3
Grootendorst (1996) 26 Sepsis P, Unc HV-CVVH MAP 60 3
Oudemans (1999) 306 ITU-ARF P cohort int HVCVVH Survival 65 3
Honoré (2000) 20Refractory
septic shockP HV-CVVH CO, SVR 140 3
Evidence levels
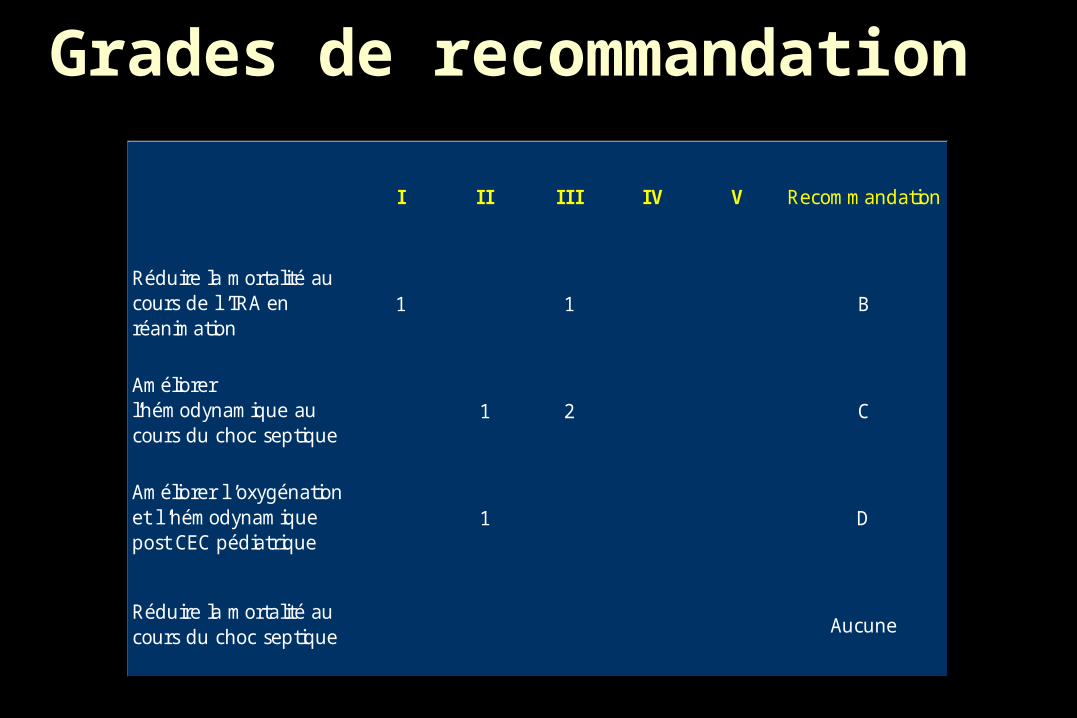
Grades de recommandation
I I I I I I IV V Recommandation
Réduire la mortalité au cours de l ’IRA en réanimation
1 1 B
Améliorer l’hémodynamique au cours du choc septique
1 2 C
Améliorer l ’oxygénation et l ’hémodynamique post CEC pédiatrique
1 D
Réduire la mortalité au cours du choc septique Aucune
Top Related