






Langages
Pages
Légal



Université de Sherbrooke
Dépistage précoce du diabète gestationnel
par
Masoud Mahdavian
Programmes de sciences cliniques
Mémoire présenté à la Faculté de médecine et des sciences de la santé
en vue de l’obtention du grade de maître ès sciences (M.Sc.)
en sciences cliniques
Sherbrooke, Québec, Canada
Juin 2015
Membres du jury d’évaluation
Jean-Luc Ardilouze, M.D., Ph.D., Département de médecine, Université de Sherbrooke
Jean-Patrice Baillargeon, M.D., M. Sc., Département de médecine, Université de Sherbrooke
S. John Weisnagel, M.D., Département sciences des aliments, Faculté des sciences de
l’agriculture et de l’alimentation, Université Laval
© Masoud Mahdavian, 2015

University of Sherbrooke
Early Screening of Gestational Diabetes Mellitus
by
Masoud Mahdavian
Clinical Sciences Program
Thesis presented at the Faculty of Medicine and Health Sciences
for the obtention of Master degree diploma (M.Sc.) in Clinical Sciences
Sherbrooke, Québec, Canada
June 2015
Members of the evaluation committee:
Jean-Luc Ardilouze, M.D., Ph.D., Department of Medicine, University of Sherbrooke
Jean-Patrice BaillargeonM.D., M. Sc., Department of Medicine, University of Sherbrooke
S. John Weisnagel, M.D., Department of Food Science and Nutrition, Laval University
© Masoud Mahdavian, 2015

RÉSUMÉ
Dépistage précoce du diabète gestationnel
par
Masoud Mahdavian
Programmes de sciences cliniques
Mémoire présenté à la Faculté de médecine et des sciences de la santé en vue de l’obtention du
diplôme de maitre ès sciences (M.Sc.) en sciences cliniques, Faculté de médecine et des sciences
de la santé, Université de Sherbrooke, Sherbrooke, Québec, Canada, J1H 5N4
L’aggravation de certaines caractéristiques cliniques des femmes enceintes (âge, poids) et
l’augmentation de la prévalence du diabète gestationnel (DG) poussent à dépister le DG le plus tôt
possible pour éviter chez la mère et le fœtus les complications à court et à long terme. Le dépistage
du DG est recommandé à 24-28 semaines de grossesse, et le plus souvent un test de tolérance à
50g de glucose (TTG) est réalisé. Pour les femmes qui ont des facteurs de risque, ce test doit être
effectué plus précocement, habituellement pendant le premier trimestre de la grossesse. Cette
dernière recommandation est peu suivie, d’autant qu’il n’y a pas de consensus international sur le
dépistage du DG pendant le premier trimestre de la grossesse.
Objectifs. 1) Définir au premier trimestre de la grossesse la valeur de la glycémie du TTG qui
prédit le diagnostic de DG à 24-28 semaines avec une sensibilité et une spécificité optimales à
l’aide d’une courbe ROC. 2) Déterminer si la glycémie du TTG au premier trimestre est un facteur
prédictif indépendant du DG.
Méthodes. Étude prospective de cohorte. Les facteurs d'inclusion étaient : âge ≥ 18 ans et âge
gestationnel entre 6 et 13 semaines après la dernière menstruation. Les TTG ont été effectués à la
première visite prénatale. Une deuxième visite était programmée à 24-28 semaines pour faire une
hyperglycémie provoquée par voie orale (HGPO) et donc un éventuel diagnostic de DG. Les
critères utilisés pour ce diagnostic étaient ceux de l’Association américaine du diabète.
Résultats. Les TTG ont été faits à 9,1±2,0 semaines et les HGPO à 26.5±1.1semaines chez 1180
femmes (28,2±4,4 ans, IMC : 25,2±5,5 kg/m2). Un DG a été diagnostiqué chez 100 (8,4%)
participantes. La valeur de glycémie du TTG à 5,6 mmol/L a prédit le DG avec une sensibilité de
84,1% et une spécificité de 62,3%, tandis que la valeur prédictive positive était de 0,121 et la
valeur prédictive négative de 0,985. Cette valeur de 5,6 était indépendamment associée au DG
(OR=2,806, IC 95%: 1,98 à 3,97, p <0,001). Comparé à d'autres facteurs de risque, le TTG était le
plus puissant prédicteur indépendant du DG (OR=1,767, IC 95%: 1,52 à 2,05, p <0,001).
Conclusions. Au premier trimestre, la valeur glycémie de 5.6 mmol/L du TTG prédit avec une
bonne sensibilité et spécificité l’apparition d’un DG à 24-28 semaines. La glycémie du TTG au
premier trimestre est le plus puissant prédicteur indépendant de DG.
Mots clés : diabète gestationnel, DG, dépistage, 1er trimestre, grossesse, TTG, OGTT.

SUMMARY Early Screening of Gestational Diabetes Mellitus
by
Masoud Mahdavian
Clinical Sciences Program
Thesis presented at the Faculty of Medicine and Health Sciences for the obtention of Master
degree diploma [maitre ès sciences] (M.Sc.) in Clinical Sciences, Faculty of medicine and health
sciences, Université de Sherbrooke, Sherbrooke, Québec, Canada, J1H 5N4
The changes in clinical characteristics of pregnant women and an increase in the prevalence of
gestational diabetes mellitus (GDM) warrant the importance of screening as early as possible in
order to possibly prevent short and long-term complications in both the mother and fetus. GDM
screening is recommended at 24-28 weeks of pregnancy, using a 50g glucose challenge test (GCT)
although women with multiple risk factors are expected to be assessed “early” in pregnancy, a
recommendation poorly followed. Most importantly, there is no universal agreement currently in
place for GDM screening, particularly during the first trimester of pregnancy.
Objectives. 1) To define the cut-off value of GCT during the first trimester in order to predict
GDM diagnosed at 24-28 weeks of gestation with optimal sensitivity and specificity using ROC
curve. 2) To determine if GCT during the first trimester of pregnancy is an independent predictor
of GDM diagnosed at 24-28 weeks gestation.
Methods. This is a prospective cohort study. Women were recruited at their first prenatal visit.
Inclusion factors were: age ≥ 18 years and gestational age between 6 and 13 weeks from their last
menstrual period. GCT were performed at the first prenatal visit. The second visit was scheduled
at 24-28 weeks for the diagnostic 75g oral glucose tolerance test (OGTT). GDM diagnosis was
made in accordance with the American Diabetes Association guidelines. A variety of statistical
analysis including multivariate logistic regression models and ROC curve were used to address
the aims of the study.
Results. Participants (n=1180, age: 28.2±4.4 years, BMI: 25.2±5.5 kg/m2) underwent GCT at
9.1±2.0 weeks and OGTT at 26.5±1.1 weeks of gestation. GDM was diagnosed in 100 (8.4%)
women. The cut-off value of 5.6 mmol/L predicted GDM with 84.1% (75.4-92.7) sensitivity,
62.3% (59.5-65.1) specificity, while the positive predictive value was 0.121 (0.091-0.150) and the
negative predictive value was 0.985 (0.975-0.994). This 5.6 value was independently associated
with GDM (OR=2.806, 95% CI: 1.98-3.97, p<0.001). Compared to other risk factors, GCT was
the strongest independent predictor of GDM (OR=1.767, 95% CI: 1.52-2.05, p<0.001).
Conclusions. The cut-off value of 5.6 mmol/L has the optimal sensitivity and specificity for the
GCT during the first trimester to predict GDM at 24-28 weeks of gestation according to ADA
guidelines. GCT during the first trimester is the strongest independent predictor of GDM at 24-28
weeks of gestation.
Keywords: Gestational diabetes mellitus, GDM, screening, 1st trimester, pregnancy.

v
TABLE OF CONTENT RÉSUMÉ III
SUMMARY IV
TABLE OF CONTENT V
LIST OF FIGURES VI
LIST OF TABLES VII
LIST OF ABBREVIATIONS VIII
INTRODUCTION 1
1.1 Definition and Epidemiology 1
1.2 GDM Risk Factors 2
1.3 GDM Complications 3
1.4 Screening test 5
1.5 Diagnostic test 5
1.6 Sensitivity and Specificity 5
1.7 Positive and Negative Predictive values, likelihood ratio 6
1.8 ROC Courve 7
1.9 Current ADA and CDA Screening and Diagnosis Recommendations 7
1.10 Why Early Screening? 8
1.11 Review of Previous Published Articles Related to Early Screening 10
HYPOTHESIS 13
OBJECTIVES 14
3.1 Objective No. 1 14
3.2 Objective No. 2 14
ARTICLE 1 15
DISCUSSION 38
Strengths and limits 42
Future and Perspectives 44
THANKS 46
REFERENCES 47
ANNEXES 57

vi
LIST OF FIGURES
Figure 1 Course of the study………………………………………………………. …….....…23
Figure 2 ROC curve of the GCT plasma glucose………………….……………………….….26

vii
LIST OF TABLES
Table 1 Threshold values for the screening and diagnosis of GDM by ADA and CDA…….…..8
Table 2 Demographic and clinical variables of pregnant women….....…………………………24
Table 3 Predictive values of the GCT PG of 5.6 mmol/L for GDM diagnosis according
to ADA criteria……....…….……….…………………………………………………..27
Table 4 Independent predictors significantly associated with GDM diagnosis according
to ADA criteria…...…...…………………..……………………………………………28

viii
LIST OF ABBREVIATIONS
A1c Glycated hemoglobin
ACHOIS Australasian Carbohydrate Intolerance in Pregnancy Study
ADA American Diabetes Association
AUROC Area Under ROC Curve
BMI Body mass index
BSP Blood Sampling in Pregnancy Clinic
CDA Canadian Diabetes Association
CHUS Centre Hospitalier Universitaire de Sherbrooke
GCT 50 grams Glucose Challenge Test
GDM Gestational Diabetes Mellitus
HAPO Hyperglycemia and Adverse Pregnancy Outcome Study
IADPSG International Association of Diabetes and Pregnancy Study Groups
LGA Large for gestational age
LR Likelihood Ratio
MIF Macrophage Migratory Inhibitory Factor
NPV Negative Predictive Value
OGTT Oral Glucose Tolerance Test
PG Plasma glucose
PPV Positive Predictive value
RFs Risk factors
ROC Receiver Operating Characteristic
SGA Small for gestational age
SHBG Sex Hormone Binding Globulin
T2D Type 2 diabetes
TGF-β Transforming Growth Factor- beta
V1 First Visit at 6-13-week gestation
V2 Second Visit at 24-28-week gestation
WHO World Health Organization

INTRODUCTION
1.1 Definition and Epidemiology
Pregnancy is characterized by a progressive increase in nutrient-stimulated insulin responses
despite an only minor deterioration in glucose tolerance, consistent with progressive insulin
resistance (Butte, 2000). Gestational diabetes mellitus (GDM) is a condition in women who
have glucose intolerance with onset or first recognition during pregnancy (Canadian Diabetes
Association Clinical Practice Guidelines Expert Committee, 2013, Metzger and Coustan,
1998).
The prevalence of GDM is estimated between 2% and 18% depending upon the population
studied and the diagnostic tests employed (Kim et al., 2002). We participated in this debate.
In a cohort of 459 pregnant women recruited prospectively, we showed that the prevalence
of GDM (diagnosed with 75g oral glucose tolerance test – OGTT - in a one-step universal
procedure) is multiplied 3.6 fold (Mahdavian et al., 2010) when the International Association
of Diabetes in Pregnancy Study Group (IADPSG) cut-off values vs. those recommended in
2010 by the American Diabetes Association (ADA) were used (American Diabetes
Association, 2010, IADPSG consensus panel, 2010). In addition to the cut-off values
questioning, several parameters influence the detection of GDM by affecting sensitivity and
specificity of GCT and OGTT such as sample handling and processing times, and diurnal
variations in the tests results (Ardilouze, Mahdavian et al., 2012). All these factors should be
considered in the interpretation of tests. Nonetheless, regardless of different diagnostic
methods or cut-off values, GDM prevalence has doubled over the past 10 years in all ethnic
populations and this seems to be related mainly to increasing weight gain (Dabelea et al.,
2005, Ferrara et al., 2004). Although Caucasian women have the lowest GDM risk, one study
reported a 12.3% prevalence of GDM in 3,950 Italian women and an absolute 5.6%
prevalence in women with low risk for GDM (Di Cianni et al., 2003). Another study
performed in the UK (Cosson et al., 2006) found a 13% prevalence using universal screening
versus 8% using a risk-factor approach.
Recognition of diabetes for the first time during pregnancy corresponds to both unrecognized
pre-gestational diabetes and any overt glucose intolerance occurring during this pregnancy.
Pathogenesis of GDM is multifactorial; however, it is not completely clear. Both relative

2
diminished insulin sensitivity causing insulin resistance and β cell dysfunction causing
reduced insulin release have been proposed (Singh et al., 2015, Al-Noaemi and Shalayel,
2013). These changes are affected by multiple factors including but not limited to Human
Placental Lactogen secretion, expression of sex hormone binding globulin (SHBG), cytokine
release such as MIF, TGF- β (Singh et al., 2015, Li et al., 2015, Marcantoni et al., 2015).
GDM may also occur in women with a background of chronic insulin resistance to which the
insulin resistance of pregnancy is partially additive. Sequential measurements of insulin
sensitivity performed in the same women before pregnancy, early in the second trimester and
in the third trimester have documented insulin resistance in both lean and obese women who
eventually develop GDM (Catalano et al., 1999 and Catalano et al., 1993). Changes in
carbohydrate homeostasis have been described as early as at six weeks’ gestation and,
consequently, some women with early onset of GDM could have pregnancy-induced glucose
intolerance (Freinkel, 1980). These findings partially explain why GDM develops not only
in overweight or obese women but also in lean women, which suggests that normal weight
women should be screened for GDM, hypothetical procedure which went against many
recommendations at the time we initiated the present study, in particular those of the ADA
(see below).
1.2 GDM Risk Factors
Several risk factors (RFs) have been described for GDM. Until recently the ADA would state
that women with all of the following characteristics were at low risk for GDM development:
age < 25 years, normal body weight before pregnancy, Caucasian, no known diabetes in a
first degree relative, no history of abnormal glucose intolerance and no history of abnormal
obstetrical outcome (American Diabetes Association, 2009). However, the more recent 2014
ADA guidelines recommend that the RFs for type 2 diabetes (T2D) should be considered for
GDM screening (American Diabetes Association, 2014).
Age ≥ 35 years, body mass index (BMI) ≥ 30 kg/m2, ethnicity, polycystic ovary syndrome,
previous GDM, history of macrosomic infant or current fetal macrosomia or
polyhydramnios, acanthosis nigricans and corticosteroid use have been considered as GDM

3
RFs by the Canadian Diabetes Association (CDA) (Canadian Diabetes Association Clinical
Practice Guidelines Expert Committee, 2013).
1.3 GDM Complications
GDM carries short and long-term health risks for both the fetus and the mother. Short-term
fetal complications include death in utero, prematurity, large (LGA) or small (SGA) for
gestational age neonates, macrosomia, dystocia, admission to neonatal nursery and intensive
care units, hypoglycemia, hypocalcaemia, convulsions and hyperbilirubinemia (Metzger and
Coustan, 1998, Coustan, 2010). The short-term complications for the mother include
preeclampsia, antenatal admission, hydramnios, induced labor and caesarean section
(Metzger and Coustan, 1998). In addition, GDM is a forerunner of T2D (Kim et al., 2002).
It was shown in the Diabetes Prevention Program Study in 3,234 pre-diabetic subjects, that
a history of GDM increases by 74% the risk of developing T2D (Knowler et al., 2002).
The focus of the impact of GDM on offspring has now shifted from the prevention and care
of perinatal morbidity to the long-term prevention of metabolic diseases. GDM, as maternal
BMI, is a risk factor contributing to the worldwide epidemics of obesity and T2D in
childhood ‒ and adulthood (Dabelea et al., 2000, Dabelea and Pettitt, 2001) ‒ although these
epidemics are still not completely understood. Thus, prevention is the key. However, it
requires thorough comprehensive screening strategies.
Furthermore, the level of hyperglycemia and the time of screening/diagnosis matter. Women
with GDM diagnosed early in pregnancy are more hyperglycemic and at higher risk for
obstetrical and neonatal complications during the current pregnancy and for recurrent GDM
in future pregnancies (Ben-Haroush et al., 2004, Berkowitz et al., 1992). The Hyperglycemia
and Adverse Pregnancy Outcome (HAPO) Study showed in 23,325 women (age: 29.2±5.8,
BMI 27.7±5.1 kg/m2) that the relationship between maternal glycaemia and fetal
hyperinsulinemia, LGA, cesarean-section rate and neonatal hypoglycemia, adverse maternal
and fetal outcomes is a continuum (The HAPO Study Cooperative Research Group, 2008).

4
Interestingly, the most frequent short-term complications are preventable in neonates, even
with moderately hyperglycemic mothers, as shown by the Australasian Carbohydrate
Intolerance in Pregnancy Study (ACHOIS) (Crowther et al., 2005). In this study, performed
in women with glucose intolerance diagnosed during pregnancy (subjects with pre-
gestational diabetes were excluded), the number to treat was 34 to avoid 1 serious perinatal
complication, 11 and only 9 to avoid LGA and macrosomia, respectively in the neonate
(Crowther et al., 2005). This study demonstrated the clinical validity of screening for GDM.
However, the impact of universal “early” screening remains to be demonstrated.
Data from several studies suggest that exposure of the fetus to the mother’s GDM
environment confers a risk for T2D and obesity during childhood and adolescence that
overrides any genetically transmitted susceptibility. Maternal antenatal glycaemia is related
to the long-term risk of obesity, metabolic syndrome, abnormal levels of inflammatory and
coagulation markers, and diabetes in the offspring (Boney et al., 2005, Dabelea et al., 2000a,
Dabelea et al., 2000b Dabelea and Pettitt, 2001).
The concept of ‘metabolic programming’ (Ismail-Beigi et al., 2006) was first illustrated in
Pima Indians (Dabelea et al., 2000b) and thereafter in offspring of GDM women in the USA
(Boney et al., 2005, Metzger, 2007), Canada (Keely et al., 2007),
and Denmark (Clausen et
al., 2007). However, these cross-sectional studies failed to control for maternal disease
history and genetic background since heredity is a major epidemiologic risk factor for type 2
diabetes. Exclusion of confounding genetic factors is a key element to establish the role of
GDM as an independent marker of cardio-metabolic risk in GDM offspring. Our team is
carrying out a study that aims to demonstrate in children that metabolic syndrome and cardio-
metabolic markers are more frequent in offspring of GDM mothers than in their siblings born
from non-GDM pregnancies.
In addition, the exact effects of GDM and maternal obesity remain to be established (Gillman
et al., 2003, Schaefer-Graf et al., 2005). Compounding this worrisome future is a suggestion
that treatment of GDM decreases the prevalence of obesity in 5-7 year-old offspring (Hillier

5
et al., 2007). This data, taken together with the “Programming hypothesis,” points to early
screening and treatment of GDM.
1.4 Screening test
Many women with GDM are asymptomatic; however, GDM has a significant impact on them
and their offspring (The HAPO Study Cooperative Research Group, 2008). Most of these
short and long-term complications are preventable (Crowther et al., 2005, Hillier et al.,
2007). Screening test is used to determine individual who may have a disease in apprently
healthy and asymptomatic people. In addition, a screening test requires to be done when it
can fulfil Wilson’s criteria (Wilson and Jungner, 1968), and these criteria must be attained:
1) early screening, 2) in asymptomatic people, 3) validity and reliability, 4) affordable costs,
5) acceptance, and 6) follow-up services. A screening test does not establish a diagnosis. The
major benefit of a screening test is to identify an asymptomatic person at risk for the disease
to reduce the mortality and morbidity of the disease of interest.
1.5 Diagnostic test
A positive screening test is usually followed by a diagnostic (confirmatory) test to verify a
definitive diagnosis (Kanchanaraksa & Diener-West, 2008). A diagnstic test is used to verify
the presence or absence of a disease when a person has signs or symptoms of the disease of
interest (Kanchanaraksa & Diener-West, 2008). The best available test to determine a person
has the disease of interest is considered as the “Gold Standard test”. Validity and reliabity of
other tests are compared to the gold standard test to diagnose the disease of interest
(Kanchanaraksa & Diener-West, 2008).
1.6 Sensitivity and Specificity
Sensitivity and specificity are two indices of validity of a test when the outcome and the
exposure are categorical variable (Szklo and Nieto, 2014). An ideal screening test should
have both high sensitivity and high specificity (Bonita et al., 2006). Sensitivity of a test is
the ability of a test to determine accurately people who have the disease of interest.
Specificity of a test is the ability of a test to determine accurately people who do not have the

6
disease of interest (Szklo and Nieto, 2014). A more sensitive test usualy is initially the first
step to detect more possible cases; however, it will increase the number of false positive
cases. Therefore, it is followed by a more specific (diagnostic or confirmatory) test. A
sequential screening (two step) will increase net gain in specificity of the screening
(Kanchanaraksa & Diener-West, 2008). Sensitivity and specificity of the test are not
dependent on the disease prevalence.
1.7 Positive and Negative Predictive values, likelihood ratio
To interpret a test result, healthcare providers need to know about the positive and negative
predictive values. A positive predictive value (PPV) is the proportion of true positive among
people who have a positive test result. A negative predictive value (NPV) is the proportion
of true negative results among people who have a negative test result. PPV and NPV are
affected by the prevalence of the disease in the population that is being tested. If the
prevalence of a disease is high, it is more possible that the person with a positive test has a
true positive result. Healthcare providers also need to know the positive and negative
likelihood ratios (LRs) which are also used to assess the value of a positive or negative
diagnostic test (Szklo and Nieto, 2014). A positive LR gives us the probability of a positive
finding in a patient with the disease of interest compare to the probability of the same finding
in a subject without the disease of interest (McGee, 2002).
Disease + Disease - Total
Positive test result a (True Positive) b a + b
Negative test result C d (True Negative) c + d
Total a + c b + d a + b + c + d
Sensitivity= a / (a + c) Specificity= d / (b + d) PPV= a / (a + b) NPV= d / (c + d)
𝑃𝑜𝑠𝑖𝑡𝑖𝑣𝑒 𝐿𝑖𝑘𝑒𝑙𝑖ℎ𝑜𝑜𝑑 𝑟𝑎𝑡𝑖𝑜𝑛 =𝑃𝑟𝑜𝑏𝑎𝑏𝑖𝑙𝑖𝑡𝑦 𝑜𝑓 𝑡ℎ𝑒 𝑓𝑖𝑛𝑑𝑖𝑛𝑔 𝑖𝑛 𝑎 𝑝𝑎𝑡𝑖𝑒𝑛𝑡 𝑤𝑖𝑡ℎ 𝑑𝑖𝑠𝑒𝑎𝑠𝑒 𝑜𝑓 𝑖𝑛𝑡𝑒𝑟𝑒𝑠𝑡
Probability of the finding in a subject without the disease of interest

7
1.8 ROC Curve
If the test results are reported as ordinary or continuous scale, the different cutoff (threshold)
values affect the sensitivity and specificity of the test, and specificity is inversly related with
sensitivity (Hajian-Tilaki, 2013). Receiver operating characteristic (ROC) curve is the plot
of sensitivity versus 1-specificity. The area under the ROC curve (AUROC) is the measure
of the accuracy of the test (Hanley and McNeil, 1982, Hajian-Tilaki, 2013). This curve has a
pivotal role in the assessment of a diagnostic test to determine the optimal cutoff value
(Hajian-Tilaki, 2013). This type of analysis has been used in many clinical studies to assess
the diagnostic ability of the tests (biomarkers and imaging studies) to differentiate population
with the disease from healthy ones (Hajian-Tilaki, 2013). Furthermore, it is commonly used
to predict the risk of an adverse event (Hajian-Tilaki, 2013).
1.9 Current ADA and CDA Screening and Diagnosis Recommendations
The ADA recommends that pregnant women with RFs for T2D should be screened for
previously unrecognized T2D during the first prenatal visit. Otherwise, GDM screening
should be undertaken on pregnant women who do not have a history of diabetes at 24-28
weeks of gestation (American Diabetes Association, 2014). The CDA recommends a
universal screening for GDM at 24-28 weeks of gestation. However, women with multiple
RFs should be screened during the first trimester (Canadian Diabetes Association Clinical
Practice Guidelines Expert Committee, 2013).
Both the ADA and CDA guidelines currently recommend the one-step or two-step
approaches. In the one-step approach, there is no requirement for a 50g glucose challenge
test (GCT) and pregnant women directly undergo a 75g oral glucose tolerance test (OGTT).
The 75g-OGTT results are interpreted according to the IADPSG guidelines with GDM
diagnosed if any plasma glucose (PG) value exceeds the thresholds presented in Table 1
(IADPSG Consensus Panel, 2010).
In the two-step approach, pregnant women are initially tested with a GCT. If the GCT plasma
glucose (PG) value is above the threshold (≥ 7.8 mmol/L), women will proceed to a 75g-
OGTT (CDA preferred approach and NIH consensus of the ADA [NDDG]) or a 100g-OGTT

8
(NIH consensus of the ADA [Carpenter/Coustan]). The PG results of the second step are
interpreted according to thresholds presented in Table 1. According to ADA, GDM diagnosis
is made when at least two of the four 100g-OGTT PG values exceed thresholds shown in
Table 1 (American Diabetes Association, 2014). However, according to CDA, GDM is
diagnosed if one 75g-OGTT PG value meets or exceeds the recommended threshold
(Canadian Diabetes Association Clinical Practice Guidelines Expert Committee, 2013).
Table 1. Threshold values for the screening and diagnosis of GDM by ADA and CDA.
Method ADA (mmol/L) CDA (mmol/L)
One-step
(IADPSG
Consensus)
75g-OGGT
Two-step
(NIH Consensus)
One-step
(IADPSG
Approach)
75g-OGGT
Two-step
(Preferred
Approach)
75g-OGTT
Carpenter/
Coustan
100g-OGTT
NDDG
75g-OGGT
GCT NA ≥7.8 ≥7.8 NA ≥ 7.8
Fasting PG ≥ 5.1 >5.3 >5.8 ≥ 5.1 ≥ 5.3
1hr 75g-OGTT ≥ 10.0 ≥ 10.0 ≥ 10.6
2hr 75g-OGTT ≥ 8.5 ≥ 8.5 ≥ 9.0
1hr 100g-OGTT >10.0 >10.6
2hr 100g-OGTT >8.6 >9.2
3hr 100g-OGTT >7.8 >8.0
ADA: American Diabetes Association 2014, CDA: Canadian Diabetes Association 2013,
NDDG: National Diabetes Data Group, IADPSG: International Association of Diabetes and
Pregnancy Study Groups, NA: Not applicable and GCT is not necessary in this approach.
1.10 Why Early Screening?
Although there are still controversies surrounding the screening and consequences of GDM
(Sermer, 2003, Wen et al., 2000, Ouzilleau et al., 2003, Brody et al., 2003), there is a general
agreement that screening should be performed as soon as possible in at-risk women
(American Diabetes Association, 2014, Canadian Diabetes Association Clinical Practice
Guidelines Expert Committee, 2013).

9
Nowadays, universal early GDM screening sounds crucial; the reason could be simply
because it is recommended by most diabetes professional associations in a large part of the
population since aging and overweight are RFs. The common assumption that “the earlier
the treatment, the better the outcomes” is another reason, although weaker. However, several
strong lines of evidence reinforce the universal early screening policy hypothesis.
First, clinical characteristics of pregnant women have changed (Ferrara et al., 2004). Over
the last decades, RFs for insulin resistance have increased rapidly in the population of
childbearing women. The percentage of overweight and obese women of childbearing age
has increased tremendously, reaching a whopping 43% in Canada (Tjepkema, 2006, Shields
et al., 2011). This weight gain causes a parallel increase in insulin resistance, a condition
contributing to GDM (Kauffman et al., 2006). Moreover, pregnancy is occurring at an older
age (Ferrara et al., 2004) and age is another well-known risk factor for GDM (Ben-Haroush
et al., 2004). Both of these trends (weight gain and aging) increase the risk and precocity of
the GDM onset and underline the importance of early screening.
Second, the proportion of women with undiagnosed T2D is also on the rise in the North
American population (Casson et al., 2006). It was also reported that T2D represents 27.3%
of pre-gestational diabetes in a United Kingdom population including, indeed, a large ethnic
(Pakistanis and South India) proportion (Casson, 2006).
Third, early-onset GDM is a serious condition. Women with early-onset GDM are more
likely to be hypertensive, to have higher glycemic values, and to need insulin therapy than
those in whom diabetes develops later (Bartha et al., 2000, Svare et al., 2001). In one Spanish
study, all cases of neonatal hypoglycemia and perinatal death occurred within the early-onset
group (Bartha et al., 2000).
Fourth, testing in early pregnancy potentially allows for earlier and more efficient
intervention (diet, exercise and pharmacotherapies). One explanation to the current
controversy surrounding the benefits of GDM screening and treatment might be that

10
screening at 24-28 weeks of gestation is too late. Nonetheless, it has been demonstrated that
treatment of GDM is effective in reducing short-term (Crowther et al., 2005) and long-term
complications (Hillier et al., 2007). Taken together, the above-mentioned evidence provides
strong justification for early screening.
1.11 Review of Previous Published Articles Related to Early Screening
We found six papers focusing on early GDM screening.
1) In 1986, Benjamin et al. performed GCTs during the first trimester (weeks 6 to 13) and a
100g-OGTT (American Diabetes Association standards) during the second (weeks 14 to 26)
and third trimesters (weeks 27 to term) in a small cohort of 101 high-risk women aged 26.4±6
years, classified obese although BMI and weight were not specified. The third trimester 100g-
OGTT was the diagnostic test. With a 7.7 mmol/L threshold, the sensitivity and specificity
of the GCT were 88% and 73%, respectively, using the third trimester 100g-OGTT results
for the GDM diagnosis. However, the GCT sensitivity was only 25% when GDM women
were discovered by a positive 100-OGTT during the second trimester. Similar issues were
found when the GCT threshold was > 8.25 mmol/L. Therefore, authors concluded that
guidelines for GDM screening should include follow-up with a third trimester OGTT on all
patients who test positive at screening, even in the presence of normal second trimester
OGTT, and that OGTT should be deferred until the early third trimester (Benjamin et al.,
1986). However, because the number of events (8) was very low, one ponders the validity
and conclusions of this pioneering study.
2) Nahum and Huffaker (1990) performed GCT in first and in early third trimesters in a small
cohort of 124 American women described as white (61%) and non-white, normal weight
(47%) and obese. They found a correlation (r=0.54, P= 0.000001) between the first trimester
and the third trimester (28-32 weeks) GCTs. The correlation was stronger among white
people (r= 0.67, P= 0.000001). A 100g-OGTT was performed in subjects with 1h post GCT
≥ 7.4 mmol/L. Nine (7%) were found to have GDM during the third trimester. No one was
diagnosed with GDM among white women with first trimester GCT value < 6.1mmol/L.
They recommended there is no yield from a third trimester GCT when the first trimester GCT
is less than 6.1 mmol/L (NPV= 91%). In addition, when the first trimester GCT is > 7.8

11
mmol/L, it has a high predictive value (PPV= 91%) for an abnormal third trimester GCT
which requires a subsequent OGTT (Nahum and Huffaker, 1990). Again, the limited number
of events and the heterogeneity of the sample bring into question the validity of these
findings.
3) Nahum et al. (2002) again found a correlation between the GCT results at the end of the
first trimester and at week 28 in 255 (out of 439 enrolled) normal-weight pregnant women
aged 27.6±6.2 years (BMI: 23.9±5.2 kg/m2) except in 37 Pacific Islanders with a BMI
28.9±6.8 kg/m2 who had the lowest mean PG post GCT at 5.6±1.5 mmol/L. In subjects with
1-h post GCT ≥ 7.4 mmol/L, a 100g-OGTT diagnostic test was performed. GDM was
diagnosed in 10% of subjects (only 25 women). Patients with first GCT PG ≥ 7.5 mmol/L
had a positive predictive value showing a 55% risk of developing diabetes during pregnancy,
while the risk was 0.6% in patients with values ≤ 6.1 mmol/L (Nahum et al., 2002). However,
a plasma hexokinase glucose determination was used during the second trimester GCT,
whereas capillary whole-blood reflectance glucometer was used at 28 weeks.
4) Bhattacharya et al. (2002) studied an Indian population (n=458) of non-diabetic women
[100g-OGTT early in the first trimester, Coustan’s criteria (Coustan et al., 1989)] with BMI
< 25 kg/m2. The 100g-OGTT diagnostic test was performed in only 133 women with GCT
≥ 7.8 mmol/L at third trimester. GDM was found in 38 women (8.3% of the cohort). When
the first trimester GCT PG was under 5.5 mmol/L, no subject tested positive for GDM during
the third trimester OGTT. When the first trimester GCT glucose was ≥ 7.8 mmol/L (n=18),
72% (n=13) cases tested positive for GDM. The GCT during the first trimester was predictive
(correlation coefficients= 0.38) of the early third trimester OGTT result (substantial
correlation for 0.20< CC<0.70). However, it is well established that the Indian population is
predisposed to cardiovascular disease, T2D and visceral obesity (Retnakaran et al., 2006).
Moreover, it was reassessed that international standards are not appropriate for Indian women
(Kulkarni et al., 2007). Accordingly, the external validity of this study is very low.
5) Maegawa et al. (2003) measured GCT and OGTT during the first
trimester in a Japanese
population (n=749, age 28.9±4.1 years, BMI 21±2.9 kg/m2). Subjects with normal results

12
were tested again at 24–28 weeks of gestation with GCT and 75g-OGTT. Only 22 women
(2.9%) tested positive for GDM (Japan Diabetes Society and the Japan Society of Obstetrics
and Gynecology criteria) with OGTT. Among those 22 women who diagnosed with GDM,
14 were predicted with the first trimester (threshold: 7.2 mmol/L) and 8 with the second
trimester GCT (threshold: 7.2 mmol/L). This study concluded that the majority of cases of
GDM were detected during the first trimester with a positive GCT. However, the absence of
the clear definition of first trimester (gestational weeks) and the low prevalence of GDM were
both weaknesses of the study. In addition, the OGTT cutoff values for the GDM definition
were different with ADA and CDA guidelines.
6) Bito et al. (2005) studied a cohort of 163 women having one or two risk factors for GDM
(mostly familial history of diabetes, obesity and age). A 75g-OGTT was performed at ≤ 16
weeks, 24-28 weeks and 32-34
weeks and the World Health Organization (WHO) criteria
were used for the GDM diagnosis. Using logistic regression analysis and ROC curves, it was
determined that at 14 weeks, fasting (5.0 mmol/L) and 2-hr 75g-OGTT (6.2 mmol/L) glucose
are cut-off values under which GDM at 24-28 weeks is unlikely. The best combined cut-off
values to exclude subsequent GDM were ≤ 5.3 mmol/L (fasting) and ≤ 6.8 mmol/L (2-hr post
load) (Bito et al., 2005). However, using these cut-off values, the lowest false-positive rate
was very high, 73.5% at 24-28 weeks. Results from this study must be considered with
caution since this Hungarian cohort (age: 29±5 years, pre-gestational BMI: 29.5±5.6 kg/m2)
had a noteworthy and surprising risk for GDM: 54% of the 163 women developed GDM at
some point during pregnancy although no risk factor was significant for the prediction of
GDM. This suggests that risk factors are useful to identify at-risk women yet they have low
predictive value (Griffin et al., 2000).
There are several important drawbacks in these above-mentioned studies. First of all, there
is an extended definition of first trimester in the first, second and fourth papers. Two other
papers (Bartha et al., 2000 and Meyer et al., 1996)
were not included in this review because
screening was performed at 18 weeks and 22 weeks, respectively. In addition, the CDA
recommended threshold (7.8 mmol/L) was seldom used (in the first and fourth papers).
Furthermore, all papers were underpowered as previously explained.

13
Although some reported sensitivities or specificities seem high, 95% confidence intervals
were not reported and are expected to be very large (for sensitivity and likelihood ratios, for
example). The fourth and fifth studies are encouraging but were performed on Japanese and
Indian women, respectively. In these studies, women with a negative GCT were not assessed
and excluded although it was shown that 6.3% of women with a GCT < 7.8 mmol/L develop
GDM (Di Cianni et al., 2003, Naylor et al., 1997). True GDM and pre-existing T2D were
not differentiated in these studies. Another important weakness of these studies is the absence
of blinding in their research design. None of these papers specify whether or not first
screening results were blinded for the participants and/or the research team.
The above-mentioned weaknesses have been considered in our study design.
HYPOTHESIS Rational: As described in the above section, the escalating prevalence of obesity and the
increasing age of pregnancy, both risk-factors to increase insulin resistance, strengthen the
need to find an appropriate method to screen universally for GDM in the early stage of
pregnancy. Moreover, it would be very appropriate to identify early on women who will later
develop GDM, in order to prevent the mother and her fetus from the appearance of GDM as
well as the short and long-term complications of GDM, assuming that “the earlier the
treatment, the better the outcomes”. However, in early pregnancy there is no approved and
generalizable screening method to predict GDM with high sensitivity and acceptable
specificity. Such determination of prediction criteria would enable healthcare providers to
distinguish pregnancies at high risk of GDM from those at low risk. This criteria would allow
for early intervention and prevention of GDM providing that the clinical validity of such
approach is demonstrated in future study.
Hypothesis: GCT plasma glucose value obtained during the first trimester is an independent
predictor of GDM determined by 75g-OGTT at 24-28 weeks of gestation despite presence or
absence of other risk factors for GDM.

14
OBJECTIVES
3.1 Objective No. 1
To determine if GCT obtained during the first trimester of pregnancy is an independent
predictor of GDM diagnosed by 75g-OGTT at 24-28 weeks of gestation.
3.2 Objective No. 2
To define the cut-off value of the one hour GCT plasma glucose value obtained during the
first trimester in order to predict GDM with optimal sensitivity and specificity as diagnosed
by 75g-OGTT at 24-28 weeks of gestation.

15
ARTICLE 1 First-trimester 50g-glucose challenge test: A robust predictor of gestational diabetes
mellitus at 24-28 weeks of pregnancy.
Auteurs de l’article : Masoud Mahdavian, Marie-France Hivert, Julie Menard, Jean-Marie
Moutquin, Annie Ouellet, Patrice Perron, Ghislaine Houde, Jean-Patrice Baillargeon, Jean-
Luc Ardilouze
Statut de l’article : submitted to JAMA.
Avant-propos : my contribution in this article was in acquisition, analysis and interpretation
of data, statistical analysis, drafting of the manuscript and critical revision of the manuscript
for important intellectual content.
Résumé en français
Objectif : Déterminer au premier trimestre de la grossesse quelle est la valeur de la glycémie
d’un test de tolérance à 50g de glucose (TTG) qui permet de prédire l’apparition d’un diabète
gestationnel (DG) à 24-28 semaines.
Méthodes. Étude prospective d’une cohorte de femmes enceintes (âge ≥ 18 ans, sans diabète
connu). Les TTG étaient effectués avant la 14e semaine de grossesse et les hyperglycémies
provoquées par voie orale (HGPO) à 24-28 semaines. Les résultats des TTG étaient gardés
en aveugle. Le diagnostic de DG était posé sur l’HGPO, en utilisant les critères 2014 de
l’Association américaine du diabète.
Résultats. Les dossiers de 1180 femmes (âge : 28,2±4,4 ans, IMC : 25,2±5,5 kg/m2) ont été
analysés. Les TTG ont été faits à 9,1±2,0 semaines et les HGPO à 26.5±1.1semaines. Un DG
a été diagnostiqué chez 100 (8,4%) participantes. La glycémie post-TTG (5,6 mmol/L)
prédisait le DG avec une sensibilité de 84,1% et une spécificité de 62,3%. Outre la glycémie
post-TTG à 5.6 mmol/L, les autres prédicteurs indépendants du DG étaient les antécédents
d’intolérance au glucose, l'âge ≥ 35 ans et l’IMC ≥ 25 kg/m2. Le TTG était le meilleur

16
marqueur de DG : après ajustement pour les autres facteurs prédictifs, la glycémie post-TTG
≥ 5.6 mmol/L multipliait les risques de DG par 7.8 (IC 95% de 4,15 à 16,1, p <0,001).
Conclusions. Le TTG au premier trimestre est un puissant facteur prédicteur de DG à 24-28
semaines de gestation. Nous proposons qu’il soit utilisé pour identifier les femmes à risque
élevé de DG à qui des soins préventifs pourraient être offerts.

17
Title: First-trimester 50g-glucose challenge test: a robust predictor of gestational diabetes
mellitus at 24-28 weeks of pregnancy.
Short running title: First trimester GCT predicts 24-28 weeks GDM.
Authors: Masoud Mahdavian, MD1,2, Marie-France Hivert, MD, MMSc1,2,3, Julie Menard,
PhD1, Jean-Marie Moutquin, MD, MSc1,4, Annie Ouellet, MD1,4, Patrice Perron, MD, MSc1,2,
Ghislaine Houde, MD1,2, Jean-Patrice Baillargeon, MD, MSc1,2*, Jean-Luc Ardilouze, MD,
PhD1,2*
*co-senior authors
Affiliation: 1Centre de recherche du Centre hospitalier universitaire de Sherbrooke,
Sherbrooke, QC, Canada, 2Endocrine Division, Department of Medicine, Université de
Sherbrooke, Sherbrooke, QC, Canada, 3Harvard Pilgrim Health Care Institute, Department
of Population Medicine, Harvard Medical School, Boston, MA, 4Department of Obstetrics
and Gynecology, Université de Sherbrooke, Sherbrooke, QC, Canada.
Corresponding author:
Jean-Luc Ardilouze
Tel.:
Fax:
Email:

18
ABSTRACT
Objectives. To determine first-trimester 50g-glucose-challenge test (GCT) glucose cut-off
value that is most predictive of development of gestational diabetes mellitus (GDM)
diagnosed at 24-28 weeks using 75g oral glucose tolerance test (OGTT), according to 2014
ADA thresholds.
Research Design and Methods. Population-based, prospective cohort study of pregnant
women (age ≥18 years, no diabetes prior to pregnancy). GCT was performed before 14th
week of pregnancy and diagnostic OGTT at 24-28 weeks. GCT results were blinded until
OGTT for GDM diagnosis.
Results. Complete data from 1180 women were analyzed. Women were 28.2±4.4 years old,
and had a BMI of 25.2±5.5 kg/m2. They completed GCT at 9.1±2.0 weeks of gestation and
OGTT at 26.5±1.1 weeks. A total of 100 (8.4%) women were diagnosed with GDM. The 1h-
glucose post-GCT cut-off value of 5.6 mmol/L predicted GDM with 82.0% (74.5-89.5)
sensitivity and 60.8% (57.9-63.7) specificity. The significant independent clinical predictors
of GDM measured in our study were GCT result ≥5.6 mmol/L, history of abnormal glucose
tolerance, age ≥35 years and BMI ≥ 25 kg/m2, among which GCT was the strongest predictor.
After adjustment for these predictors, a GCT ≥5.6 mmol/L increased the odds of GDM 7.8
folds (95% CI of OR: 4.15-16.1, p<0.001).
Conclusions. First-trimester GCT is a strong predictor of GDM at 24-28 weeks of gestation.
We propose that first-trimester GCT could be used to identify women at high-risk for GDM
and to offer them appropriate preventive care.
Keywords: Gestational diabetes mellitus, GDM, screening, predicting, 1st trimester,
pregnancy
Trial Registration: NCT01026675, ClinicalTrials.gov

19
Introduction
Clinical characteristics of pregnant women have changed. More and more women delay
starting a family (Kjos and Buchanan, 1999) and the proportion of childbearing-age women
who are overweight and obese has significantly increased (Gingras et al., 2012, Coustan,
1996). The prevalence of gestational diabetes mellitus (GDM) and pre-existing glucose
intolerance or diabetes has also sharply risen (Ferrara, 2007, Lawrence et al., 2008). Some
studies report GDM prevalence as high as 10%, 12% and 28% in Caucasian, Japanese and
Southeast Asia region populations, respectively (Jiwani et al., 2012). GDM is therefore a
serious public health concern, the prevalence of which will in all likelihood only increase in
coming years. Screening and prevention are thus cornerstone to reducing the short and
perhaps long-term complications of GDM for mothers and their babies.
However, screening recommendations remain the subject of ongoing debate (American
Diabetes Association, 2014, Canadian Diabetes Association Clinical Practice Guidelines
Expert Committee, 2013, Nankervis et al., 2014, Vandorsten et al., 2013). Meanwhile,
prevention recommendations have yet to be firmly established. This is partly due to a lack of
robust means to adequately identify those women at high risk of GDM early during
pregnancy. For screening, the American Diabetes Association (ADA) and many others
recommend the two-step strategy consisting of a universal 50g-glucose challenge test (GCT)
at 24-28 weeks of gestation, although women with multiple risk factors should in fact be
tested earlier (Canadian Diabetes Association Clinical Practice Guidelines Expert
Committee, 2013, Nankervis et al., 2014, Vandorsten et al., 2013). When 1h-glucose post-
GCT results exceed a certain threshold, the value of which varies according to national and
international professional associations or organizations, women then undergo a diagnostic
75g or 100g oral glucose tolerance test (OGTT). Others however perform the one-step 75g-
OGTT approach according to the 2010 recommendations of the International Association of
Diabetes and Pregnancy Study Groups, which have since been adopted by the ADA. This
latter approach calls for the OGTT in all clinical settings of pregnancy i.e. early on in high-
risk pregnancies to detect diabetes, and at 24-28 weeks as part of a universal screening
strategy (IADPSG Consensus Panel, 2010).

20
The “early-screening” expert recommendation suggests that the same GCT or OGTT plasma
glucose (PG) cut-off values be used both at 24-28 weeks and earlier. For prevention purposes,
it is currently unknown whether the GCT early on in pregnancy helps identify those women
at high risk of developing GDM later on.
Accordingly, the aims of this study were to 1) determine the first-trimester GCT cut-off value
with optimal sensitivity and specificity to predict development of GDM as diagnosed by
standard 75-g OGTT between 24 and 28 weeks of gestation; 2) determine if first-trimester
1h-glucose levels post-GCT predict GDM incidence independently of traditional first-
trimester risk factors.
Research Design and Methods
We conducted a population-based prospective study of pregnant women receiving care at the
Centre Hospitalier Universitaire de Sherbrooke (CHUS). The CHUS Research Ethics Board
approved the study protocol and all participants gave written informed consent prior to their
participation in accordance with the Helsinki declaration and all applicable laws and
regulations.
Inclusion criteria were age ≥ 18 years, gestational age between 6 and 13 weeks from last
menstrual period, no diabetes prior to pregnancy, < 2 alcoholic drinks/day, no regular high-
intensity physical activity, singleton pregnancy, and otherwise good health status.
Women were recruited between April 2009 and June 2012, during their first prenatal visit
(V1) at the CHUS Blood Sampling in Pregnancy (BSP) Clinic. The BSP Clinic offers routine
prenatal blood sampling, including GCT and OGTT. The BSP Clinic is also a clinical
research platform ensuring first-rate healthcare and follow-up for pregnant women with
GDM by highly-trained staff (Hivert et al., 2012).
At V1, non-fasting women arrived between 8h30 AM and 3h30 PM. Weight was measured
barefoot, in light clothing on a body composition analyzer (Tanita, TBF-300A, Tanita
Corporation, Arlington Heights, IL) to the nearest 0.1 kg and height, with a stadiometer to

21
the nearest 0.01 m. BMI was calculated as weight (kg) divided by squared height (m2).
Women self-reported their pre-gestational weight which was used to calculate pre-gestational
BMI. In addition to age and BMI, other traditional GDM risk factors were documented (2010
ADA guidelines) (American Diabetes Association, 2010): history of diabetes in first-degree
relatives, personal medical history of abnormal glucose metabolism including previous
GDM, ethnicity, and poor obstetrical outcomes such as previous delivery of a newborn with
fever, infection, hypoglycemia, jaundice, respiratory problem, fraction or malformation,
being admitted to the intensive care unit, or stillborn.
Women were asked to drink a 300-ml 50g-glucose oral solution (Glucodex, Rougier Pharma,
Mirabel, Qc, Canada) within 5 minutes. Each bottle contained 166.6 mg dextrose, as
recommended. Over the next hour, women remained seated and venous PG was measured
once the hour was up. An appointment was then set for the second visit (V2). No dietary or
exercise counseling was provided. A qualified biochemist verified GCT results. These were
kept blinded to the study team members and participating women until V2, except when PG
reached ≥ 10.3 mmol/L. Pursuant recommendations from the Canadian Diabetes Association
(CDA) at the time (Canadian Diabetes Association Clinical Practice Guidelines Expert
Committee, 2013). 11 women with GCT 1h-glucose ≥ 10.3 mmol/L were considered as
GDM, and thus were excluded and referred for usual care (Hivert et al., 2012).
For V2, scheduled between 24 and 28 weeks of gestation, women were asked to fast during
the 12 hours preceding their appointment. Anthropometric data were collected according the
same standardized protocols described for V1. Blood samples were collected (fasting, at 1h
and 2h post 300-ml 75g-glucose oral solution (Glucodex) drunk within 5 minutes). Each
bottle contained 250 mg dextrose, as recommended. Women remained seated during the 2h
wait. Those with GDM were referred for usual care (Hivert et al., 2012).
Venous plasma glucose was measured using the oxidase method (Modular Analytics, Roche
Diagnostics, USA) at the CHUS Biochemistry Laboratory.

22
The main outcome of this study was GDM diagnosed between the 24th and 28th weeks of
gestation (V2), according to 2014 ADA recommended criteria: one glycaemia ≥ 5.1, 10.0 or
8.5 mmol/L at time 0, 60 and 120 min post-glucose, respectively. This main outcome was
pre-specified, before the initiation of the study.
We reported continuous variables as means ± standard deviations and categorical variables
as percentages with 95% confidence intervals. We tested for differences between women
with or without GDM; unpaired Student’s t-tests were used for continuous variables and chi-
squared tests for dichotomous variables. P-values < 0.05 were considered statistically
significant for all analyses. Under objective 1, we constructed a ROC curve using sensitivities
and specificities calculated from results of first trimester GCT to predict GDM at 24-28
weeks. We used the knee of the ROC curve to select the GCT 1h-glucose cut-off value where
sensitivity and specificity are both optimal. Such a cut-off maximizes case-finding rates
while minimizing false-positive rates and misclassification. Under objective 2, multivariate
logistic regression models were performed in order to determine independent first-trimester
predictors of GDM, using stepwise forward-backward methods: all variables collected at V1
(Table 2) that were associated with a GDM diagnosis in univariate analyses (p≤0.10) were
successively added to the model, based on the lowest p-value, and then removed from the
model if not independently associated with the outcome (p>0.05) in the multivariate model.
We calculated the area-under-the-ROC-curve (AUROC) for the post-GCT selected 1h-PG
value and for each multivariate model. Older age was associated with increased risk of GDM
in a non-linear fashion in our population, such that age ≥ 25 years (ADA GDM risk factor
definition) was not associated with GDM diagnosis, but age ≥ 35 years was (CDA GDM risk
factor definition) (Canadian Diabetes Association Clinical Practice Guidelines Expert
Committee, 2013). This is why age ≥ 35 years, instead of 25 years, was used for multiple
logistic regression analyses. Statistical analyses were performed using JMP version 11.0
(SAS Institute).
Results
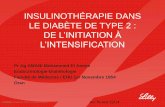
At V1, we recruited 1442 women who underwent a GCT. Of these, 216 women were
excluded from the analyses (miscarriages: 101, withdrew for personal reason: 74, multiple

23
pregnancies: 15, medical abortion: 14, GCT plasma glucose ≥ 10.3 mmol/L: 11, ectopic
pregnancy: 1). The other 1226 women were invited to V2. Of these, 46 were excluded from
analyses (did not tolerate fasting: 12, vomited during the OGTT: 7, lost samples: 7, moved
away from region: 7, GCT performed instead of OGTT: 6, high capillary glucose testing: 5,
metformin therapy: 1, lost to follow-up: 1). Complete data from a total of 1180 women were
thus analyzed.
Figure 1. Course of the study.
Footnotes: GCT: glucose challenge test; OGTT: oral glucose tolerance test.
*GCT was performed instead of the OGTT. †Measured capillary glycaemia before the visit
and were high.
Characteristics of participants are provided in Table 2. Women self-reported a mean pre-
pregnancy weight of 66.0±15.1 kg. Using the measured height at first trimester, we calculated
that the mean pre-pregnancy BMI was 24.5±5.4 kg/m2, including 35.7% of women with BMI
≥ 25 kg/m2 and 14.8% with BMI ≥ 30 kg/m2. At V1, the mean BMI was 25.2±5.5 kg/m2. The
V1: screening test (GCT)
(n=1442)
V2: diagnosis test (75g-OGTT)
(n=1180)
Miscarriages: 101
Withdrew for personal reason: 74
Multiple pregnancies: 15
Abortion (voluntary or for malformation): 14
Ectopic pregnancy: 1
GCT ≥10.3 mmol/L: 11
Do not tolerate fasting: 12
Vomited during the OGTT: 7
Lost samples: 7
Moved: 7
GCT instead of OGTT: 6*
Capillary hyperglycemia: 5†
Metformin therapy: 1
Lost to follow-up: 1
V2 planned for 1226 women
Excluded from the
study before the
second visit: 216
Excluded from the
analysis: 46

24
correlation between the pre-gestational BMI and BMI at V1 was r = 0.986 (P<0.001). The
mean GCT PG was 5.5±1.4 mmol/L ranging from 2.6 to 10.2 mmol/L.
Table 2. Demographic and clinical variables of pregnant women (n=1180)
V1
GCT visit
V2
OGTT visit
Gestational age (weeks) 9.1±2.0 26.5±1.1
Age (years) 28.2±4.4 -
BMI (kg/m2) 25.2±5.5 27.8±5.2
Primiparous (n, %) 568 (48.1%) -
ADA risk factors
Age ≥ 25 years (n, %) 949 (80.4%)
(78.2 – 82.7)
-
Pre-pregnancy BMI ≥ 25 kg/m2 (n, %)a 417 (35.7%)
(33.0 – 38.5)
-
Non-Caucasian (n, %) 53 (4.5%)
(3.3 – 5.7)
-
Familial history of diabetes (n, %)b 135 (18.2%)
(15.4 – 21.0)
-
History of abnormal glucose tolerance (n, %)c 49 (5.7%)
(4.1 – 7.2)
-
Prior history of poor obstetrical outcomes (n,%)d 217 (24.9%)
(22.0 – 27.8)
-
GCT (mmol/L) 5.5±1.4 -
OGTT 0 min (mmol/L) - 4.2±0.4
OGTT 60 min (mmol/L) - 7.2±1.6
OGTT 120 min (mmol/L) - 5.9±1.4
Results are means ± SD or n, percentage and 95% confidence interval.
V1: visit 1; GCT: glucose challenge test; V2: visit 2; OGTT: oral glucose tolerance test;
ADA: American Diabetes Association. adata collected in n=1165; bdata collected in n=741; cdata collected in n=863; ddata collected in n=872.

25
Women gained a mean of 2.6±0.3 kg/m2 of BMI (7.0±0.4kg) between V1 and V2. Mean
OGTT PG values are shown in Table 2. According to ADA criteria, a total of 100 (8.4%)
women were diagnosed with GDM.
The ROC curve (Figure 2) indicates that the GCT 1h-PG value with optimal sensitivity and
specificity to predict GDM is 5.6 mmol/L. This cut-off value has the following predictive
values (95% CI) for GDM diagnosis using ADA criteria: sensitivity 82.0%, specificity
60.8%, positive predictive value 16.2% and negative predictive value 97.3% (Table 3). In
other words, 505 women had first trimester GCT PG ≥ 5.6 mmol/L, among which 82 were
classified with GDM at 24-28 weeks, therefore a GCT PG > 5.6 mmol/L at first trimester
doubles the probability to develop GDM at 24-28 weeks (16.2 vs 8.5%), while this risk is 3
times lower (2.7 vs 8.5%) in those with PG ≤ 5.6 mmol/L. Accordingly, the LR+ of GCT is
close to 2, which is the threshold for a good test to rule-in a condition; and its LR- is close to
0.2, the threshold for a very good test to rule-out a disease (Sackett et al., 2000).

26
Figure 2. ROC curve of the GCT plasma glucose.
Footnotes: GCT: glucose challenge test.
5.6 mmol/L

27
Table 3. Predictive values of the GCT PG of 5.6 mmol/L for GDM diagnosis according
to ADA criteria.
Sensitivity (%) 82.0 (74.5 – 89.5)
Specificity (%) 60.8 (57.9 – 63.7)
False positive rate (%) 39.2 (36.3 – 42.1)
False negative rate (%) 18.0 (10.5 – 25.5)
Positive predictive value (%) 16.2 (13.0 – 19.5)
Negative predictive value (%) 97.3 (96.1 – 98.5)
Positive likelihood ratio 2.094 (1.86 – 2.36)
Negative likelihood ratio 0.296 (0.19 – 0.45)
Precision (%) 62.6 (59.9 – 65.4)
Values are presented with 95% confidence interval.
GCT: glucose challenge test; PG: plasma glucose; GDM: gestational diabetes mellitus; ADA:
American Diabetes Association
The first-trimester 5.6 mmol/L GCT value to discriminate women ‘at high risk of GDM’ vs.
‘not at risk’ was significantly increased the odds of developing GDM by 7 folds (OR=7.1)
(see Table 4). The AUROC based on the GCT 1h-PG value alone was 0.714. The best overall
predictive model included results of the GCT and three other clinical risk factors: history of
abnormal glucose tolerance, age ≥ 35 years and BMI ≥ 25 kg/m2. Each of the latter risk
factors added statistically to the logistic regression model and the AUROC of the full model,
including all 4 variables, was 0.831. However, the 1h-PG result of the first-trimester GCT
was the single best GDM predictor (Table 4). GCT used as a continuous variable was also
independently and significantly associated with GDM and yields results similar to those of
the model using the 5.6 GCT cut-off (OR=1.74 per mmol/L increase, 95% CI: 1.51-2.00,
p<0.001).

28
Table 4. Independent predictors significantly associated with GDM diagnosis according
to ADA criteria.
Variables OR 95% CI AUC P-value
Model 1 0.714 <0.001
GCT PG ≥ 5.6 mmol/L 7.08 4.29-12.3 <0.001
Model 2 0.767 <0.001
GCT PG ≥ 5.6 mmol/L 8.40 4.50-17.2 <0.001
Abnormal glucose tolerance 5.16 2.52-10.4 <0.001
Model 3 0.798 <0.001
GCT PG ≥ 5.6 mmol/L 7.97 4.25-16.3 <0.001
Abnormal glucose tolerance 5.14 2.47-10.5 <0.001
Age ≥ 35 years 3.68 1.84-7.13 <0.001
Model 4 0.831 <0.001
GCT PG ≥ 5.6 mmol/L 7.82 4.15-16.1 <0.001
Abnormal glucose tolerance 5.39 2.54-11.2 <0.001
Age ≥ 35 years 3.60 1.78-7.09 <0.001
BMI ≥ 25 kg/m2 2.27 1.34-3.87 0.002
GDM: gestational diabetes mellitus; ADA: American Diabetes Association; OR: odds ratio;
AUC: area under the curve; GCT: glucose challenge test; PG: plasma glucose.
Multivariate logistic regression models were built using stepwise forward-backward
methods. All variables in Table 2 associated with GDM diagnosis in univariate analyses
(p≤0.10) were tested.
Conclusion
Different methods, using maternal clinical data and/or biomarkers, have been proposed for
early screening of GDM during the first trimester of pregnancy. The aim of such screening
is to protect mothers and fetuses from the short and long-term complications of GDM
(Lacroix et al., 2013, Rasanen et al., 2013, Nanda et al., 2011, Kazandi, 2010, Punthumpol
et al., 2008, Georgiou et al., 2008, Plasencia et al., 2011, Teede et al., 2011). Exposure to
abnormally high concentrations of blood glucose during pregnancy can lead to abnormal fetal
metabolic programming (Portha et al., 2011). In clinical practice, early identification of
women at risk of developing GDM would allow the convenient detection of hyperglycemia

29
as soon as it arises during pregnancy, and thus closer follow-up, or offer preventive
interventions.
Previous studies have proposed the early identification of women at risk of GDM through a
combination of clinical risk factors. A retrospective study (Teede et al., 2011) proposed
considering maternal demographics and medical characteristics at first trimester including
the ADA’s classical risk factors (see Table 2). The proposed clinical scoring system had an
AUROC of 0.703. A clinical risk score ≥ 4 points (out of possible total 8 points) identified
women developing GDM with a sensitivity of 61.3% and a specificity of 71.4% (Teede et
al., 2011). This clinical risk score seems promising, should it be validated in other
populations outside Australia, and as long as clinicians are willing to adopt a multi-factor
scoring system. Nevertheless, clinical risk-factor scoring may be improved by additional
biochemical predictive markers.
Biochemical compounds measured early on in pregnancy as risk markers of developing
GDM during the second trimester have been proposed as isolated predictors per se, or as part
of a set to improve clinical risk-factor predictive scoring. One promising circulating protein
is adiponectin. Low adiponectin levels during the first trimester of pregnancy are associated
with increased risk of GDM in the second trimester, and this association was demonstrated
in several cohorts including our own (Lacroix et al., 2013, Rasanen et al., 2013, Nanda et al.,
2011). Unfortunately, adiponectin is not measured in routine clinical practice. Thus, it is
unlikely to be adopted in real life. Another proposed biomarker was sex hormone-binding
globulin (SHBG) levels (Thadhani et al., 2003). However, adding SHBG levels to clinical
factor predictive scores provided relatively limited additional predictive value (Nanda et al.,
2011).
Hemoglobin A1c is now part of the diagnostic criteria for diabetes. It can also be
conveniently measured in a non-fasting state. It could thus be an interesting predictive
biomarker. In one study, no case had GDM when A1c was less than 5.2% whereas all women
with A1c ≥ 6.1% developed GDM (Anaka et al., 2014). Another study in high-risk women
(Garner et al., 2014) showed that, half of women with A1c between 5.7 and 6.4% had GDM,

30
whereas only 13.6% of those with A1c less than 5.7% (P=0.002) developed GDM.
Adjustment for race and history of GDM showed that women with A1c between 5.7 and
6.4% had five times higher estimated risk of developing GDM compared to those with A1c
< 5.7% (OR 5.43, 95% CI 1.69-17.44) (Garner et al., 2014). Yet, because hemoglobin levels
vary greatly during pregnancy (hemodilution, red blood cell turnover, anemia) from woman
to woman, the use of A1c is limited.
Measurement of the glycation of other proteins has also been proposed. For example, a case-
control study on 182 Finnish pregnant women showed that glycosylated fibronectin
concentration might be considered as an early independent predictor of GDM during the first
trimester (Rasanen et al., 2013). A threshold at 107 mg/dl had a sensitivity of 81% (95% CI
73–89), a specificity of 90% (95% CI 84–96) and an AUROC of 0.91 (95% CI 0.87–0.96) to
predict GDM (Rasanen et al., 2013). However, glycated fibronectin is not a biochemical
measurement commonly available in clinical settings and its predictive value of GDM
incidence needs to be confirmed further in a population-based study before it is considered
for clinical application.
Our results are in line with a report that 1h-glucose post-GCT at first trimester was a very
strong predictor of risk for GDM during the second trimester with an AUROC of 0.912
(Plasencia et al., 2011). Interestingly, -1h-PG was a better predictor than baseline glucose
(pre-glucose load) during the GCT. One of the limitations of that study was that GDM cases
at second trimester were diagnosed based on a two-step procedure. Thus many cases may
have been missed since OGTT was not performed in all women. Also nor did it assess or
propose any optimal cut-off.
Our own study established that first trimester GCT is an excellent predictor of GDM in a
large prospective population-based cohort where all women underwent a full 75g-OGTT, as
recommended in the most recent ADA guidelines. The 1h-PG threshold of 5.6 mmol/L
provided a sensitivity of 82.0%, specificity 60.8% and AUROC of 0.714. The AUROC
reached 0.831 by adding three simple maternal clinical factors including history of abnormal
glucose tolerance, age ≥ 35 years and BMI ≥25 kg/m2. This threshold is substantially lower

31
(- 2.2 mmol/L) than the 2014 value proposed by the ADA for GDM screening at the second
trimester i.e. 7.8 mmol/L, or even the 7.2 mmol/L value of previous recommendations. Of
note, the same screening value is recommended at the first trimester in women with risk
factors. Our low threshold value is not surprising given the physiologic variation in glycemic
regulation during pregnancy. Indeed, early pregnancy is usually characterized by enhanced
insulin sensitivity which in turn decreases over the second and third trimesters (Lain and
Catalano, 2007).
Our results are in line with previous research (Plasencia et al., 2011, Nahum and Huffaker,
1990, Bhattacharya, 2002, Yeral et al., 2013) showing a correlation between first-trimester
GCT and early third-trimester OGTT. Furthermore, compared to other above-mentioned
GDM screening methods used during the first trimester, GCT fulfills all WHO guideline
criteria for screening-tests (Wilson’s Criteria) (Wilson and Jungner, 1968). GCT is also more
feasible for health institutions than are biomarkers such as adiponectin or glycosylated
fibronectin. Additionally, using the GCT may prove more practical than fasting PG
measurement or OGTT for pregnant women who often preferred not to remain fasting during
their first trimester while experiencing nausea or morning sickness.
Our study showed that GCT results taken as a continuous variable are a predictor of GDM.
However, use of a ROC curve verified optimal sensitivity and specificity with a cut-off value
of 5.6 mmol/L. In real-life clinical practice, clinicians need cut-off values to take action.
Here, we propose that physicians should monitor women more closely when first trimester
GCT PG ≥ 5.6 mmol/L as well as provide advice on the adoption of healthful lifestyle habits
that reduce the risk of GDM. Other higher-specificity thresholds could be proposed if GCT
is used for identification of ‘very high-risk’ women to offer high intensity preventive
interventions, or higher-sensitivity thresholds to identify women who are most unlikely to
develop GDM in order to avoid futile GDM testing during the second trimester.
To our knowledge, this is the first study of its kind specifically designed to determine GCT
as a predictive test in a large population. We conducted the study prospectively and recruited
a representative sample of the population of pregnant women receiving care at our tertiary

32
and quaternary care institution. GCT results were blinded until OGTT diagnosis, thus
ensuring that study participants did not modify their lifestyle habits; consequently, our data
were collected under real-life condition. Nevertheless, our study also has certain limitations.
It was performed mainly in Caucasian women, due to the homogeneous population of mostly
French/European descent in the province of Quebec and relatively low immigration rates in
our area. Our data however can likely be generalized to other Caucasian women. Our
hypotheses need to be now tested further in other ethnicities to determine whether the 5.6
mmol/L cut-off value is appropriate for other ethnic groups.
This prospective longitudinal cohort study in a Caucasian population showed that first-
trimester GCT predicts GDM incidence at second trimester with both high sensitivity and
specificity. This could allow, from now on, closer follow-up and advice relating to lifestyle
improvement early on in the first trimester of pregnancy in women found to be at risk for
GDM. More research is clearly needed to assess whether lifestyle modification and/or
pharmacotherapy initiated early on in pregnancy decreases complication rates of GDM or
even avoids development of GDM all together. Thus, we propose a GCT 1h-glucose value >
5.6 mmol/L for early identification of at-risk women and for use in future preventive-
intervention studies starting early of pregnancy.

33
Acknowledgments
Author Contributions: JLA (principal investigator) and JPB had full access to all of the
data and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: JLA and JPB.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: MM, MFH, JLA.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: MM, JPB.
Obtained funding: PI: JLA, Collaborators: JMM, JPB.
Administrative, technical, or material support: MM, JM, AMO, PP, GH.
Study supervision: JLA, JPB, MFH.
Conflicts of Interest Disclosures: All authors report no conflicts of interest.
Funding/Support: This project was funded by a grant from the Canadian Diabetes
Association (CDA - OG-3-08-2622 – PI: JLA). JLA and JPB were awarded a Fonds de la
Recherche du Québec - Santé (FRQS) junior 2 research scholar and senior clinician
investigator scholar, respectively. MFH received a Clinical Scientist Award by the CDA and
the Maud Menten Award from the Canadian Institute of Genetics. This work was also
supported by the FRQS-funded Research Center of the Centre hospitalier universitaire de
Sherbrooke and the Sun Life Financial (PI: JLA).
Role of the Sponsors: The funders were not involved in the design and conduct of the study;
in the collection, management, analysis, and interpretation of the data; preparation, review,
or approval of the manuscript; and decision to submit the manuscript for publication.
Additional Contributions: We thank Marie-Josée Gosselin, Maude Gérard, Susan Hayes
and Georgette Proulx, RN, Sonia Lemay, medical technologist, and Pascal Brassard, PhD,
Caroline Rousseau, MSc, Myriam Doyon, MSC, and Marie-Claude Battista, PhD, research
assistants, for their work in this study. We also thank Jean Dubé, MD, PhD, biochemist for
verifying all glucose challenge test plasma glucose values. No one received compensation

34
for their contribution besides their salary. We also thank all the women who participated in
this study.

35
References
American Diabetes Association. Standards of medical care in diabetes-2010. Diabetes Care.
2010;33(Suppl 1):S11-S61.
American Diabetes Association. Standards of medical care in diabetes 2014. Diabetes Care.
2014;37(Suppl 1):S14-S80.
Anaka O, Houlihan C, Beim R, Ranzini AC. Does first-trimester hemoglobin A1C predict
gestational diabetes and fetal outcome? Obstet Gynecol. 2014;123(Suppl 1):38S-9S.
Bhattacharya SM. Glucose screening test results in first and early third trimester of
pregnancy: Is there any correlation? J Obstet Gynaecol Res. 2002;28(6):304-307.
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian
Diabetes Association 2013 clinical practice guidelines for the prevention and management
of diabetes in Canada. Can J Diabetes. 2013;37(Suppl 1):S1-S212.
Coustan DR. Screening and testing for gestational diabetes mellitus. Obstet Gynecol Clin
North Am. 1996;23(1):125-136.
Ferrara A. Increasing prevalence of gestational diabetes mellitus: A public health
perspective. Diabetes Care. 2007;30(Suppl 2):S141-146.
Garner LA, Miller E, Katon J. First-trimester A1c as a tool to predict the development of
gestational diabetes in high-risk women. Obstet Gynecol. 2014;123(Suppl 1):52S.
Georgiou HM, Lappas M, Georgiou GM, et al. Screening for biomarkers predictive of
gestational diabetes mellitus. Acta Diabetol. 2008;45(3):157-165.
Gingras V, Paradis AM, Tchernof A, Weisnagel SJ, Robitaille J. Relationship between the
adoption of preventive practices and the metabolic profile of women with prior gestational
diabetes mellitus. Appl Physiol Nutr Metab. 2012;37(6):1232-1238.
Hivert MF, Allard C, Menard J, Ouellet A, Ardilouze JL. Impact of the creation of a
specialized clinic for prenatal blood sampling and follow-up care in pregnant women. J
Obstet Gynaecol Can. 2012;34(3):236-242.
International Association of Diabetes and Pregnancy Study Groups Consensus Panel,
Metzger BE, Gabbe SG, et al. International association of diabetes and pregnancy study
groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy.
Diabetes Care. 2010;33(3):676-682.
Jiwani A, Marseille E, Lohse N, Damm P, Hod M, Kahn JG. Gestational diabetes mellitus:
Results from a survey of country prevalence and practices. J Matern Fetal Neonatal Med.
2012;25(6):600-610.

36
Kazandi M. Conservative and surgical treatment of abnormal placentation: Report of five
cases and review of the literature. Clin Exp Obstet Gynecol. 2010;37(4):310-312.
Kjos SL, Buchanan TA. Gestational diabetes mellitus. N Engl J Med. 1999;341(23):1749-
1756.
Lacroix M, Battista MC, Doyon M, et al. Lower adiponectin levels at first trimester of
pregnancy are associated with increased insulin resistance and higher risk of developing
gestational diabetes mellitus. Diabetes Care. 2013;36(6):1577-1583.
Lain KY, Catalano PM. Metabolic changes in pregnancy. Clin Obstet Gynecol.
2007;50(4):938-948.
Lawrence JM, Contreras R, Chen W, Sacks DA. Trends in the prevalence of preexisting
diabetes and gestational diabetes mellitus among a racially/ethnically diverse population of
pregnant women, 1999-2005. Diabetes Care. 2008;31(5):899-904.
Nahum GG, Huffaker BJ. Correlation between first- and early third-trimester glucose
screening test results. Obstet Gynecol. 1990;76(4):709-713.
Nanda S, Savvidou M, Syngelaki A, Akolekar R, Nicolaides KH. Prediction of gestational
diabetes mellitus by maternal factors and biomarkers at 11 to 13 weeks. Prenat Diagn.
2011;31(2):135-141.
Nankervis A, McIntyre H, Moses R, et al. ADIPS consensus guidelines for the testing and
diagnosis of hyperglycaemia in pregnancy in Australia and New Zealand.
http://adips.org/downloads/2014ADIPSGDMGuidelinesV18.11.2014_000.pdf Accessed
12/2014.
Plasencia W, Garcia R, Pereira S, Akolekar R, Nicolaides KH. Criteria for screening and
diagnosis of gestational diabetes mellitus in the first trimester of pregnancy. Fetal Diagn
Ther. 2011;30(2):108-115.
Portha B, Chavey A, Movassat J. Early-life origins of type 2 diabetes: Fetal programming of
the beta-cell mass. Exp Diabetes Res. 2011;2011:105076.
Punthumapol C, Tekasakul P. 50 grams glucose challenge test for screening of gestational
diabetes mellitus in each trimester in potential diabetic pregnancy. J Med Assoc Thai.
2008;91(6):787-793.
Rasanen JP, Snyder CK, Rao PV, et al. Glycosylated fibronectin as a first-trimester
biomarker for prediction of gestational diabetes. Obstet Gynecol. 2013;122(3):586-594.
Teede HJ, Harrison CL, Teh WT, Paul E, Allan CA. Gestational diabetes: Development of
an early risk prediction tool to facilitate opportunities for prevention. Aust N Z J Obstet
Gynaecol. 2011;51(6):499-504.

37
Thadhani R, Wolf M, Hsu-Blatman K, Sandler L, Nathan D, Ecker JL. First-trimester sex
hormone binding globulin and subsequent gestational diabetes mellitus. Am J Obstet
Gynecol. 2003;189(1):171-176.
Vandorsten JP, Dodson WC, Espeland MA, et al. NIH consensus development conference:
Diagnosing gestational diabetes mellitus. NIH Consens State Sci Statements. 2013;29(1):1-
31.
Wilson JM, Jungner YG. Principles and practice of mass screening for disease. Bol Oficina
Sanit Panam. 1968;65(4):281-393.
Yeral MI, Ozgu-Erdinc AS, Uygur D, Seckin KD, Karsli MF, Danisman AN. Prediction of
gestational diabetes mellitus in the first trimester, comparison of fasting plasma glucose, two-
step and one-step methods: A prospective randomized controlled trial. Endocrine.
2014;46(3):512-18.

38
DISCUSSION
GDM develops with pregnancy, is asymptomatic, and has significant early and late
complications for the mother and fetus. Pregnancy complications are prevented by treatment
even in mild GDM (Crowther et al., 2005) while the issue of GDM for offspring has now
gone beyond the prevention and care of perinatal morbidity to the long-term prevention of
metabolic diseases (Metzger and Coustan, 1998, Coustan, 2010, Kim et al., 2002, Knowler
et al., 2002, Dabelea et al., 2000, Dabelea and Pettitt, 2001). While the epidemics of obesity
and T2DM in childhood are still not yet completely understood, prevention requires the
careful identification of at-risk individuals through adequate screening strategies. Therefore,
early GDM screening is crucial.
Besides actual recommendations (revised above), finding the best method or test to screen
for GDM as early as possible was the aim of many research projects around the globe. Thus,
adiponectin was assessed by our team and others (Lacroix et al., 2013). Glycosylated
fibronectin (Rasanen et al., 2013), combination of maternal clinical factors and biomarkers
(Nanda et al., 2011, Georgiou et al., 2008, Teede et al., 2011), placental growth factors
(Kazandi, 2010), and even GCT (Punthumpol et al., 2008) or 100g-OGTT (Plasencia et al.,
2011) have been also suggested. However, finding a GDM screening method which fulfills
all WHO criteria is much more difficult.
Indeed, according to WHO, screening tests aim to detect as early as possible asymptomatic
people who probably have a given disease using a valid and reliable test with high yield at
an affordable cost with a high acceptance for the people while follow up services are available
(Wilson’s Criteria) (Wilson and Jungner, 1968). Simply put, 6 factors must be achieved: 1)
early screening, 2) in asymptomatic people, 3) validity and reliability, 4) affordable costs, 5)
acceptance, and 6) follow-up services.
The method we propose, GCT at 6-13 weeks gestation for GDM screening, fulfills all above
mentioned Wilson’s screening criteria:

39
1) Early screening. We recommend performing GCT at the 6th week after the last
menstruation period, i.e. at earliest time for diagnosis of pregnancy. In practice, GCT
cannot be performed earlier.
2) Asymptomatic people. First-trimester-GCT can detect GDM as an important medical
issue for mother and offspring, in early or latent stages of disease, whereby they can be
managed and protected from GDM complications.
3) Validity and reliability. GCT has been validated and used for many years for GDM
screening at 24-28 weeks gestation; however, this current recommendation is not able to
detect GDM as early as possible in order to prevent mother and fetus from GDM
complications and potential fetal programming (Portha et al., 2011). The 24-28 week
period is rather late in the evolution of a pregnancy. In our study, GCT were performed
at 9th week, which is 17 weeks earlier than the recommended period.
4) Affordable costs. GCT is available worldwide, and at an acceptable burden for women
and acceptable cost for health systems, which is not the case for other tests discussed in
our paper, such as OGTT, adiponectin, glycosylated fibronectin and others (Lacroix et
al., 2013, Rasanen et al., 2013, Nanda et al., 2011, Georgiou et al., 2008, Teede et al.,
2011, Kazandi, 2010, Punthumpol et al., 2008, Plasencia et al., 2011). Other proposed
methods require much more expensive equipment and are not feasible around the world
although GCT can be realized everywhere with a reliable result.
5) Acceptance. The absence of gastrointestinal secondary effects following GCT, i.e. 50g
glucose load, in the whole cohort of this study, and the continuing success of the method
implemented in our area since the creation of the Blood Sampling and Research in
Pregnancy clinic in 2007 (Hivert et al., 2012, Allard et al., 2015) are facts implying that
GCT in the first trimester is well accepted. Several points help to increase acceptance
for the pregnant women and health care providers: women do not have to be fasting or
to absorb a high load of glucose, GCT can be done anytime during the day with no
prerequisite such as fasting. Using OGTT require fasting for several hours and
swallowing a big (75g or 100g) load of glucose although women experience morning
nausea and sickness during that period of pregnancy. In this study, the main reason for
loss to follow-up was related directly to the OGTT test (19 cases) including fasting
intolerance (12 cases) and vomiting during OGTT (7 cases). However, none of our initial

40
study population (1442 subjects) experienced nausea related to GCT during first
trimester.
6) Follow-up services. In industrialized countries at least, follow-up services are available.
However, literature shows that care of GDM becomes a concern in India, China,
Thailand, and in some African countries (Jindal et al., 2015, Chang et al., 2014, Nielsen,
2011).
Our study is the first large prospective cohort study evaluating first trimester GCT as a
predictor of GDM diagnosis at 24-28 weeks of gestation. In addition to the screening, we
aimed to predict during the first trimester for a GDM diagnosis during the third trimester of
pregnancy. Different statistical models have been used to find the best predictive model for
GDM. Our data showed that first trimester GCT as a continuous or dichotomous variable is
an independent predictor, stronger than other usual risk factors. In addition to the first
trimester GCT, our data demonstrated that history of abnormal glucose tolerance, age, and
BMI can improve the predictive value of our model, and AUROC can be increased from 0.71
(Model 1: GCT PG ≥ 5.6 mmol/L) to 0.83 (Model 4) (Table 4).
We showed that a cut-off value of 5.6 mmol/L has a sensitivity and specificity of 84% and
62%, respectively, to predict GDM. These findings are in line with several published papers
showing a correlation between first trimester GCT results and early third trimester OGTT
(Yeral et al., 2013, Nahum et al., 1990, Bhattacharya et al., 2002). However, these studies
have several drawbacks: some are retrospective, they were underpowered, performed in
heterogenic populations, or were performed in non-Caucasian (i.e. Turkish, Indian or
Japanese, respectively) women; they were inappropriately designed, with common pitfalls
such as: 1) only women with positive GCT performed OGTT; 2) methods used for glucose
measurements were suboptimal, 3) it is not clear whether GCT results were blinded to
investigators or not. In the Yeral et al. paper, two conditions are surprising: 1) women are
Turkish or from the Middle East, i.e. at higher risk than Caucasian women; therefore, the low
percentage of GDM (between 5.1 and 11.3%, depending on the method) is really surprising;
this may be due to lower BMI or other risk factors. 2) the high rate of withdrawing and lost
to follow-up (34%) is another concern. If a loss ≤ 20% does not alter the validity of

41
longitudinal studies (Fewtrell et al., 2008, Kristman et al., 2004, Touloumi et al., 2001) 34%
is probably detrimental for a study.
Our study addressed these flaws: we assessed prospectively a homogenous population of
1180 Caucasian women, GCT results were blinded until OGTT, and a reliable method was
used for glucose measurement. To our knowledge, this blinding of results is unique in
literature. A distinctive aspect of our study is homogeneity: we determined a - potential -
predictive cut-off value in a large population 95% of which was Caucasian women. This
allows our data to be generalized to other Caucasian populations of women.
Our study also showed that GCT as a continuous variable is a predictor of GDM. However,
a ROC curve verified the optimal sensitivity and specificity, showing a cut-off value of 5.6
mmol/L with a significant NPV (97%). This first trimester cut-off value at least means that
women with a GCT < 5.6 are at low risk for GDM, and should encourage healthcare providers
to monitor more closely women with GCT ≥ 5.6 mmol/L. More research is needed before we
suggest starting preventive management (using lifestyle or pharmacotherapy) in these women
We think that our data may have several clinical implications.
First, we believe that a lower cut-off value for GCT should be used during the first trimester
to predict GDM at third trimester rather than the standard 24-28 week cut-off as it is
suggested by ADA and CDA guidelines and as it was proposed by Plasencia et al. as well
(Plasencia et al., 2011). Of note, they used a 100g-OGTT as diagnosis test, according to one
ADA recommendation. Glucose metabolism in the first trimester is very different from that
of the third trimester, as discussed earlier in this thesis. This should be taken into account. If
insulin resistance is lower during the first trimester, plasma glucose cut-off values should
logically be lower as well. Simon et al. suggested that the fasting plasma glucose cut-off
value for GDM diagnosis during the first trimester should be as low as 4.7 mmol/L (85 mg/dl)
(Simon et al., 2013). Plasencia et al. also showed lower glucose values during OGTT: PG 1,
2 and 3 hours after the 100g-OGTT at 6-14 weeks was, respectively, 18, 29 and 35% lower
than at 20-30 weeks.

42
Second, we think that using GCT for screening during the first trimester might be more
practical than fasting PG or OGTT for pregnant women, as discussed above.
Third, GCT during the first trimester can potentially increase the compliance to screening.
This thought implies to continue to use GCT i.e. to recommend the 2-step procedure for
screening and diagnosing GDM. We are aware that nowadays, the 1-step procedure is
promoted, albeit carefully, by ADA, CDA and other organizations, although in practice,
clinicians often favor the old-fashion (2-step) way. It was demonstrated that using the
IADPSG criteria (1-step) increases the prevalence of GDM (Mahdavian et al., 2010, Langer
et al., 2013). We think that increasing diagnosis and care is certainly a progress, with positive
consequences to the mother and her offspring, thanks to IADPSG. However, we believe that
if the 2-step method is used instead of the 1-step proposed by the IADPSG (IADPSG
consensus panel, 2010), the negative impacts evoked above may vanish.
Strengths and limits
Our study has many strengths, as depicted above. It is the first of this kind: it is a large,
double-blinded, prospective cohort study and it was performed in a very homogenous
population. This study allowed us to calculate accurately the GDM incidence in our
Caucasian population and to evaluate the effect of different RFs on GDM incidence. An
additional strength was the fact that selection bias was low and the study was not biased by
knowledge of outcome status.
Our work has also limitations, including expected limitations of any prospective cohort study
and our own specific limitations. The main expected limitations come from the sample size
and the single-center design. A large population (more than 1000 people) was required to
generate acceptable numbers of cases of disease (GDM) and to evaluate the predictive effect
of RFs and early GCT tests on GDM incidence. The protocol was time consuming for
personnel, recruitment was difficult, and more than three years (between April 2009 and June
2012) were necessary for recruitment. Another expected bias or limitation of a prospective
cohort study is the loss to follow up. In this study, after considering inclusion and exclusion
criteria, 1226 pregnant women were enrolled and only 46 cases (3.7%) were excluded from

43
analysis for different reasons, including secondary effects of OGTT (see Fig 1). However,
this does not seem to be an issue as it was shown repeatedly that loss ≤ 20% does not affect
the validity of longitudinal studies (Fewtrell et al., 2008, Kristman et al., 2004, Touloumi et
al., 2001).
Besides, we want here to insist on three other weaknesses. First, the homogeneity of our study
population (only Caucasian women from Quebec referred to the CHUS) is an advantage but
also a disadvantage as it affects results generalizability: further research in other ethnicities
is needed. Our team aims to be provided for initiating a large multicenter study, including
centers in Toronto and Winnipeg, in order to recruit a multiethnic sample (Caribbean, Asian
and South Asian women in Toronto, Asian and First-nation in Winnipeg). Second,
complications of pregnancy and peripartum have not been included in this study particularly
to compare the incidence of these complications in two groups: women (and offspring born
to them) with GCT < 5.6 versus those with GCT ≥ 5.6 mmol/L at first trimester. Future
investigations should explore this topic to clarify the importance of early screening and its
effect on the incidence of GDM complications. Third, the effect of time of day on GCT cut-
off value should be investigated, given the circadian rhythm of glucose tolerance (Lee et al.,
1992, Massicotte et al., 2012). The effect of BMI of women (or weight, a more practical data
for many clinicians) should also be assessed. We previously showed that GCT value
increases with maternal BMI assessed at the first prenatal visit (Mahdavian et al., 2010).
Finally, although we state that GCT is a validated and reliable method recommended by most
authorities in GDM diagnosis, we must say that reproducibility is a concern for both GCT
and OGTT. It was shown that reproducibility was 90% for normal test results and 83% for
abnormal results when GCT was repeated on two consecutive days and that the probability
of GCT ≤ 6.9 mmol/L to be ≥ 7.8 mmol/L was 5% (Phillipov, 1996), Time since last meal
may induce 5% variation in positive predictive values of GCT (Sermer et al., 1994, Cetin
and Cetin, 1997). Then, we must admit that no ideal screening test for GDM has yet been
developed. Repeating GCT another time or another day in our participants may have changed
the 5.6 cut-off value.

44
OGTT has also limitations: test duration, time of performance (morning only after nocturnal
fast), discomfort as well as supra-physiological glucose load unrelated to body weight and
the degree of glucose intolerance (de Nobel and Van't Laar, 1978). The main issue of OGTT is
again reproducibility. Reproducibility was 78% in a study of 64 subjects i.e. in 50 (Harlass et
al., 1991), and 1.43 mmol/L and 1.1 mmol/L differences at 1-h and 2-h, respectively, were
found in another study (Rushforth et al., 1975). When women are retested at a one-week
interval, the variability in diagnosis varies from 10% to 24% for at first GDM women to 18%
for non-GDM women (Langer, 2006, Catalano et al., 1993). This resulted in reclassification of
many patients. It was speculated that maternal stress contributed. Therefore our data must be
interpreted as carefully as possible. However, our experimental conditions were very close
to usual clinical practice, another strength of our work. Our data are realistic data, most
probably applicable to the regular clinical setting.
Future and Perspectives
Our work was performed in a Caucasian population. For generalization of the concept, a
multiethnic population must be assessed. This will allow us to define a cut-off value usable
in the whole Canadian population and even world widely. This concept of general index for
detecting women at risk of GDM is scientifically prominent; however, it is possible that huge
ethnic differences of cut-off values will be discovered. This plausible finding will have to be
discussed. Using various cut-offs could become a complicated procedure for physicians.
The next step of our research is to determine whether this GCT cut-off during the 1st trimester
is associated with GDM complications or not even if GDM is diagnosed and treated during
the third trimester. If there is an association, another study should test whether treatment of
pregnant women with GCT ≥ 5.6 mmol/L prevents development of GDM and its
complications. This implies large prospective randomized studies in a multiethnic
population.
In conclusion, this study proposes GCT at 6-13 weeks gestation as a method to predict GDM.
GCT fulfills all Wilson’s criteria for a screening tool. Further studies are required to

45
determine if the proposed GCT cut-off value of 5.6 mmol/L is generalizable to other
ethnicities and operational for prevention of GDM.
As glucose metabolism changes during pregnancy, the same screening and diagnostic criteria
verified for the third trimester (24 to 28-week gestation) should be cautiously used to
determine glucose intolerance at first trimester (6-13 week-gestation).
Further investigations require to assess if predicting GDM early can prevent mother and her
fetus from GDM and complications of GDM. These worries include long term detrimental
consequences of fetal programming. Should our hypothesis be confirmed, screening of
mothers and prediction of GDM will allow prevention of GDM which in turn will allow
prevention of cardio-metabolic diseases in offspring. Our work should help to build healthier
generations of Canadians.

46
THANKS First and foremost, I would like to thank my supervisor, Dr. Jean-Luc Ardilouze. Without his
encouragement this project would never have been completed. I am truly thankful for his
friendship and continual support. Thanks to him for being there each step of the way and
showing me what Medicine and research are all about.
Thanks to Dr. Julie Ménard for her patience, interest, time, invaluable assistance, numerous
suggestions and edits.
You two made my experience at the University of Sherbrooke a great one.

47
REFERENCES
Al-Noaemi, M., & Shalayel, M. (2013). Pathophysiology of gestational diabetes mellitus:
The past, the present and the future. M. Radenkovic (Ed.), Gestational diabetes (pp. 91-114)
InTech.
American Diabetes Association. (2010). Standards of medical care in diabetes-2010.
Diabetes Care, 33(Suppl 1), S11-S61.
American Diabetes Association. (2014). Standards of medical care in diabetes--2014.
Diabetes Care, 37 Suppl 1, S14-80. doi:10.2337/dc14-S014; 10.2337/dc14-S014
Anaka, O., Houlihan, C., Beim, R., & Ranzini, A. C. (2014). Does first-trimester hemoglobin
A1C predict gestational diabetes and fetal outcome? Obstetrics and Gynecology, 123 Suppl
1,38S-9S.
Ardilouze, J. L., Mahdavian, M., Baillargeon, J. P., & Hivert, M. F. (2012). Glucose
challenge test for detecting gestational diabetes mellitus: A systematic review. BJOG: An
International Journal of Obstetrics and Gynaecology, 119(10), 1283; author reply 1283-4.
Bartha, J. L., Martinez-Del-Fresno, P., & Comino-Delgado, R. (2000). Gestational diabetes
mellitus diagnosed during early pregnancy. American Journal of Obstetrics and Gynecology,
182(2), 346-350. doi:S0002937800676603.
Ben-Haroush, A., Yogev, Y., & Hod, M. (2004). Epidemiology of gestational diabetes
mellitus and its association with type 2 diabetes. Diabetic Medicine: A Journal of the British
Diabetic Association, 21(2), 103-113. doi:985.
Benjamin, F., Wilson, S. J., Deutsch, S., Seltzer, V. L., Droesch, K., & Droesch, J. (1986).
Effect of advancing pregnancy on the glucose tolerance test and on the 50-g oral glucose load
screening test for gestational diabetes. Obstetrics and Gynecology, 68(3), 362-365.
Bhattacharya, S. M. (2002). Glucose screening test results in first and early third trimester of
pregnancy: Is there any correlation? The Journal of Obstetrics and Gynaecology Research,
28(6), 304-307.
Bito, T., Nyari, T., Kovacs, L., & Pal, A. (2005). Oral glucose tolerance testing at gestational
weeks < or =16 could predict or exclude subsequent gestational diabetes mellitus during the
current pregnancy in high risk group. European Journal of Obstetrics, Gynecology, and
Reproductive Biology, 121(1), 51-55. doi:10.1016/j.ejogrb.2004.11.006
Boney, C. M., Verma, A., Tucker, R., & Vohr, B. R. (2005). Metabolic syndrome in
childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus.
Pediatrics, 115(3), e290-6. doi:115/3/e290.

48
Bonito, R., Beaglehole, R., & Kjellstrom, T. (2006). Basic epidemiology (Second Edition
ed.). China: World Health Organization. ISBN 978-92-4-154707-9
Brody, S. C., Harris, R., & Lohr, K. (2003). Screening for gestational diabetes: A summary
of the evidence for the U.S. preventive services task force. Obstetrics and Gynecology,
101(2), 380-392. doi:S0029784402030570.
Butte, N. F. (2000). Carbohydrate and lipid metabolism in pregnancy: Normal compared with
gestational diabetes mellitus. The American Journal of Clinical Nutrition, 71(5 Suppl),
1256S-61S.
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. (2008).
Canadian diabetes association 2008 clinical practice guidelines for the prevention and
management of diabetes in Canada. Canadian Jounal of Diabetes, 32(Suppl 1), S1-S201.
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. (2013).
Canadian diabetes association 2013 clinical practice guidelines for the prevention and
management of diabetes in Canada. Can J Diabetes, 37(Suppl. 1), S1-S212.
Casson, I. F. (2006). Pregnancy in women with diabetes--after the CEMACH report, what
now? Diabetic Medicine: A Journal of the British Diabetic Association, 23(5), 481-484.
doi:DME1896.
Catalano, P. M., Avallone, D. A., Drago, N. M., & Amini, S. B. (1993). Reproducibility of
the oral glucose tolerance test in pregnant women. American Journal of Obstetrics and
Gynecology, 169(4), 874-881.
Catalano, P. M., Huston, L., Amini, S. B., & Kalhan, S. C. (1999). Longitudinal changes in
glucose metabolism during pregnancy in obese women with normal glucose tolerance and
gestational diabetes mellitus. American Journal of Obstetrics and Gynecology, 180(4), 903-
916. doi:S0002937899002446
Catalano, P. M., Tyzbir, E. D., Wolfe, R. R., Calles, J., Roman, N. M., Amini, S. B., et al.
(1993). Carbohydrate metabolism during pregnancy in control subjects and women with
gestational diabetes. The American Journal of Physiology, 264(1 Pt 1), E60-7.
Cetin, M., & Cetin, A. (1997). Time-dependent gestational diabetes screening values.
International Journal of Gynaecology and Obstetrics: The Official Organ of the
International Federation of Gynaecology and Obstetrics, 56(3), 257-261.
Chang, Y., Chen, X., Cui, H., Zhang, Z., & Cheng, L. (2014). Follow-up of postpartum
women with gestational diabetes mellitus (GDM). Diabetes Research and Clinical ractice,
106(2), 236-240.
Clausen, T. D., Mathiesen, E. R., Hansen, T., Pedersen, O., Jensen, D. M., Lauenborg, J., et
al. (2008). High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women

49
with gestational diabetes mellitus or type 1 diabetes: The role of intrauterine hyperglycemia.
Diabetes Care, 31(2), 340-346. doi:dc07-1596
Cosson, E., Benchimol, M., Carbillon, L., Pharisien, I., Paries, J., Valensi, P., et al. (2006).
Universal rather than selective screening for gestational diabetes mellitus may improve fetal
outcomes. Diabetes & Metabolism, 32(2), 140-146. doi:MDOI-DM-04-2006-32-2-1262-
3636-101019-200517727
Coustan, D. R. (1996). Screening and testing for gestational diabetes mellitus. Obstetrics and
Gynecology Clinics of North America, 23(1), 125-136.
Coustan, D. R. (2010). Diabetes: Finding and treating gestational diabetes mellitus-does it
help? Nature Reviews.Endocrinology, 6(10), 540-542. doi:10.1038/nrendo.2010.148 [doi]
Coustan, D. R., Nelson, C., Carpenter, M. W., Carr, S. R., Rotondo, L., & Widness, J. A.
(1989). Maternal age and screening for gestational diabetes: A population-based study.
Obstetrics and Gynecology, 73(4), 557-561.
Crowther, C. A., Hiller, J. E., Moss, J. R., McPhee, A. J., Jeffries, W. S., Robinson, J. S., et
al. (2005). Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. The
New England Journal of Medicine, 352(24), 2477-2486. doi:NEJMoa042973.
Dabelea, D., Hanson, R. L., Lindsay, R. S., Pettitt, D. J., Imperatore, G., Gabir, M. M., et al.
(2000). Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity: A
study of discordant sibships. Diabetes, 49(12), 2208-2211.
Dabelea, D., Knowler, W. C., & Pettitt, D. J. (2000). Effect of diabetes in pregnancy on
offspring: Follow-up research in the Pima Indians. The Journal of Maternal-Fetal Medicine,
9(1), 83-88. doi:10.1002/(SICI)1520-6661(200001/02)9:1<83::AID-MFM17>3.0.CO;2-O
[doi]
Dabelea, D., & Pettitt, D. J. (2001). Intrauterine diabetic environment confers risks for type
2 diabetes mellitus and obesity in the offspring, in addition to genetic susceptibility. Journal
of Pediatric Endocrinology & Metabolism: JPEM, 14(8), 1085-1091.
Dabelea, D., Snell-Bergeon, J. K., Hartsfield, C. L., Bischoff, K. J., Hamman, R. F.,
McDuffie, R. S., et al. (2005). Increasing prevalence of gestational diabetes mellitus (GDM)
over time and by birth cohort: Kaiser Permanente of Colorado GDM screening program.
Diabetes Care, 28(3), 579-584. doi:28/3/579.
de Nobel, E., & Van't Laar, A. (1978). The size of the loading dose as an important
determinant of the results of the oral glucose tolerance test: A study in subjects with slightly
impaired glucose tolerance. Diabetes, 27(1), 42-48.

50
Di Cianni, G., Volpe, L., Lencioni, C., Miccoli, R., Cuccuru, I., Ghio, A., et al. (2003).
Prevalence and risk factors for gestational diabetes assessed by universal screening. Diabetes
Research and Clinical Practice, 62(2), 131-137. doi:S0168822703001748.
Ferrara, A. (2007). Increasing prevalence of gestational diabetes mellitus: A public health
perspective. Diabetes Care, 30 Suppl 2, S141-6. doi:10.2337/dc07-s206
Ferrara, A., Kahn, H. S., Quesenberry, C. P., Riley, C., & Hedderson, M. M. (2004). An
increase in the incidence of gestational diabetes mellitus: Northern California, 1991-2000.
Obstetrics and Gynecology, 103(3), 526-533. doi:10.1097/01.AOG.0000113623.18286.20
[doi]
Fewtrell, M. S., Kennedy, K., Singhal, A., Martin, R. M., Ness, A., Hadders-Algra, M., et al.
(2008). How much loss to follow-up is acceptable in long-term randomised trials and
prospective studies? Archives of Disease in Childhood, 93(6), 458-461.
doi:10.1136/adc.2007.127316 [doi]
Freinkel, N. (1980). Gestational diabetes 1979: Philosophical and practical aspects of a major
public health problem. Diabetes Care, 3(3), 399-401.
Garner, L. A., Miller, E., & Katon, J. (2014). First-trimester A1C as a tool to predict the
development of gestational diabetes in high-risk women. Obstetrics and Gynecology, 123
Suppl 1,52S.
Georgiou, H. M., Lappas, M., Georgiou, G. M., Marita, A., Bryant, V. J., Hiscock, R., et al.
(2008). Screening for biomarkers predictive of gestational diabetes mellitus. Acta
Diabetologica, 45(3), 157-165. doi:10.1007/s00592-008-0037-8; 10.1007/s00592-008-
0037-8
Gillman, M. W., Rifas-Shiman, S., Berkey, C. S., Field, A. E., & Colditz, G. A. (2003).
Maternal gestational diabetes, birth weight, and adolescent obesity. Pediatrics, 111(3), e221-
6.
Gingras, V., Paradis, A. M., Tchernof, A., Weisnagel, S. J., & Robitaille, J. (2012).
Relationship between the adoption of preventive practices and the metabolic profile of
women with prior gestational diabetes mellitus. Applied Physiology, Nutrition, and
Metabolism = Physiologie Appliquée, Nutrition et Metabolisme, 37(6), 1232-1238.
doi:10.1139/h2012-114; 10.1139/h2012-114
Griffin, M. E., Coffey, M., Johnson, H., Scanlon, P., Foley, M., Stronge, J., et al. (2000).
Universal vs. risk factor-based screening for gestational diabetes mellitus: Detection rates,
gestation at diagnosis and outcome. Diabetic Medicine: A Journal of the British Diabetic
Association, 17(1), 26-32.
Hajian-Tilaki, K. (2013). Receiver operating characteristic (ROC) curve analysis for medical
diagnostic test evaluation. Caspian Journal of Internal Medicine, 4(2), 627-635.

51
Hanley, J. A., & McNeil, B. J. (1982). The meaning and use of the area under a receiver
operating characteristic (ROC) curve. Radiology, 143(1), 29-36.
Harlass, F. E., Brady, K., & Read, J. A. (1991). Reproducibility of the oral glucose tolerance
test in pregnancy. American Journal of Obstetrics and Gynecology, 164(2), 564-568.
Hillier, T. A., Pedula, K. L., Schmidt, M. M., Mullen, J. A., Charles, M. A., & Pettitt, D. J.
(2007). Childhood obesity and metabolic imprinting: The ongoing effects of maternal
hyperglycemia. Diabetes Care, 30(9), 2287-2292. doi:dc06-2361.
Hivert, M. F., Allard, C., Menard, J., Ouellet, A., & Ardilouze, J. L. (2012). Impact of the
creation of a specialized clinic for prenatal blood sampling and follow-up care in pregnant
women. Journal of Obstetrics and Gynaecology Canada : JOGC = Journal d'Obstetrique et
Gynecologie du Canada : JOGC, 34(3), 236-242.
International Association of Diabetes and Pregnancy Study Groups Consensus Panel,
Metzger, B. E., Gabbe, S. G., Persson, B., Buchanan, T. A., Catalano, P. A., et al. (2010).
International association of diabetes and pregnancy study groups recommendations on the
diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care, 33(3), 676-682.
doi:10.2337/dc09-1848; 10.2337/dc09-1848
Ismail-Beigi, F., Catalano, P. M., & Hanson, R. W. (2006). Metabolic programming: Fetal
origins of obesity and metabolic syndrome in the adult. American Journal of
Physiology.Endocrinology and Metabolism, 291(3), E439-40. doi:00105.2006.
Jindal, R., Siddiqui, M. A., Gupta, N., & Wangnoo, S. K. (2015). Prevalence of glucose
intolerance at 6 weeks postpartum in Indian women with gestational diabetes mellitus.
Diabetes & Metabolic Syndrome, doi: 10.1016/j.dsx.2015.04.016.
Jiwani, A., Marseille, E., Lohse, N., Damm, P., Hod, M., & Kahn, J. G. (2012). Gestational
diabetes mellitus: Results from a survey of country prevalence and practices. The Journal of
Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of
Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International
Society of Perinatal Obstetricians, 25(6), 600-610. doi:10.3109/14767058.2011.587921;
10.3109/14767058.2011.587921
Kanchanaraksa, S., & Diener-West, M. (2008) Fundamentals of Epidemiology I, Johns
Hopkins University, Online Course
http://ocw.jhsph.edu/index.cfm/go/viewCourse/course/FundEpi/coursePage/index/
Kauffman, R. P., Castracane, V. D., Peghee, D., Baker, T. E., & Van Hook, J. W. (2006).
Detection of gestational diabetes mellitus by homeostatic indices of insulin sensitivity: A
preliminary study. American Journal of Obstetrics and Gynecology, 194(6), 1576-82;
discussion 1582-4. doi:S0002-9378(06)00052-4.

52
Kazandi, M., Hasdemir, P. S., Zeybek, B., & Akcay, A. (2010). Placental growth factor: A
putative screening test for gestational diabetes mellitus in first trimester. Clinical and
Experimental Obstetrics & Gynecology, 37(4), 322-323.
Keely, E. J., Malcolm, J. C., Hadjiyannakis, S., Gaboury, I., Lough, G., & Lawson, M. L.
(2008). Prevalence of metabolic markers of insulin resistance in offspring of gestational
diabetes pregnancies. Pediatric Diabetes, 9(1), 53-59. doi:PDI258.
Kim, C., Newton, K. M., & Knopp, R. H. (2002). Gestational diabetes and the incidence of
type 2 diabetes: A systematic review. Diabetes Care, 25(10), 1862-1868.
Kjos, S. L., & Buchanan, T. A. (1999). Gestational diabetes mellitus. The New England
Journal of Medicine, 341(23), 1749-1756. doi:10.1056/NEJM199912023412307
Kristman, V., Manno, M., & Cote, P. (2004). Loss to follow-up in cohort studies: How much
is too much? European Journal of Epidemiology, 19(8), 751-760.
Kulkarni, S. R., Fall, C. H., Joshi, N. V., Lubree, H. G., Deshpande, V. U., Pasarkar, R. V.,
et al. (2007). Determinants of incident hyperglycemia 6 years after delivery in young rural
Indian mothers: The Pune Maternal Nutrition Study (PMNS). Diabetes Care, 30(10), 2542-
2547. doi:dc07-0329.
Lacroix, M., Battista, M. C., Doyon, M., Menard, J., Ardilouze, J. L., Perron, P., et al. (2013).
Lower adiponectin levels at first trimester of pregnancy are associated with increased insulin
resistance and higher risk of developing gestational diabetes mellitus. Diabetes Care, 36(6),
1577-1583. doi:10.2337/dc12-1731; 10.2337/dc12-1731
Lain, K. Y., & Catalano, P. M. (2007). Metabolic changes in pregnancy. Clinical Obstetrics
and Gynecology, 50(4), 938-948. doi:10.1097/GRF.0b013e31815a5494
Langer, O. (2006). Chapter 26: Gestational diabetes: A diagnostic dilemma.
In O. Langer (Ed.), The diabetes in pregnancy dilemma (First ed., pp. 444-461) University
press of America.
Langer, O., Umans, J. G., & Miodovnik, M. (2013). Perspectives on the proposed gestational
diabetes mellitus diagnostic criteria. Obstetrics and Gynecology, 121(1), 177-182.
doi:http://10.1097/AOG.0b013e31827711e5; http://10.1097/AOG.0b013e31827711e5
Lawrence, J. M., Contreras, R., Chen, W., & Sacks, D. A. (2008). Trends in the prevalence
of preexisting diabetes and gestational diabetes mellitus among a racially/ethnically diverse
population of pregnant women, 1999-2005. Diabetes Care, 31(5), 899-904.
doi:10.2337/dc07-2345; 10.2337/dc07-2345
Lee, A., Ader, M., Bray, G. A., & Bergman, R. N. (1992). Diurnal variation in glucose
tolerance. Cyclic suppression of insulin action and insulin secretion in normal-weight, but
not obese, subjects. Diabetes, 41(6), 750-759.

53
Li, C., Qiao, B., Qi, W., Zhan, Y., Ma, C., Zhao, L., et al. (2015). Association of macrophage
migration inhibitory factor polymorphisms with gestational diabetes mellitus in han chinese
women. Gynecologic and Obstetric Investigation, May 13, PMID: 25998484
Maegawa, Y., Sugiyama, T., Kusaka, H., Mitao, M., & Toyoda, N. (2003). Screening tests
for gestational diabetes in japan in the 1st and 2nd trimester of pregnancy. Diabetes Research
and Clinical Practice, 62(1), 47-53.
Mahdavian, M., Hivert, M. F., Baillargeon, J. P., Menard, J., Ouellet, A., & Ardilouze, J. L.
(2010). Gestational diabetes mellitus: Simplifying the international association of diabetes
and pregnancy diagnostic algorithm using fasting plasma glucose: Comment on agarwal,
dhatt, and shah. Diabetes Care, 33(11), e145; author reply e146-1454.
Mahdavian, M., Baillargeon, J. P., Vanasse, A., Moutquin, J. M., Houde, G., et al. (2010).
O’Sullivan test plasma glucose value during the 1st trimester of pregnancy: preliminary data.
Canadian Journal of Diabetes, December Suppl (abstract #22).
Marcantoni, E., Dovizio, M., O Gaora, P., Di Francesco, L., Bendaya, I., Schiavone, S., et
al. (2015). Dysregulation of gene expression in human fetal endothelial cells from gestational
diabetes in response to TGF-beta1. Prostaglandins & Other Lipid Mediators,
Massicotte, M. H., Constant, F., Baillargeon, J. P., Gosselin, M. J., Ménard, J., et al. (2009).
Gestational Diabetes Mellitus Screening: AM vs. PM Testing? 5th International Symposium
on Diabetes and Pregnancy, Sorrento, Italy, March 26-28, 2009. Published in the proceedings
of the conference (abstract #473).
McGee, S. (2002). Simplifying likelihood ratios. Journal of General Internal Medicine,
17(8), 646-649.
Metzger, B. E. (2007). Long-term outcomes in mothers diagnosed with gestational diabetes
mellitus and their offspring. Clinical Obstetrics and Gynecology, 50(4), 972-979.
doi:10.1097/GRF.0b013e31815a61d6 [doi]
Metzger, B. E., & Coustan, D. R. (1998). Summary and recommendations of the fourth
international workshop-conference on gestational diabetes mellitus. The organizing
committee. Diabetes Care, 21 Suppl 2, B161-7.
Meyer, W. J., Carbone, J., Gauthier, D. W., & Gottmann, D. A. (1996). Early gestational
glucose screening and gestational diabetes. The Journal of Reproductive Medicine, 41(9),
675-679.
Nahum GG, Wilson SB, Stanislaw H. (2002). Early-pregnancy glucose screening for
gestational diabetes mellitus. J Reprod Med, 47, 656-662.
Nahum, G. G., & Huffaker, B. J. (1990). Correlation between first- and early third-trimester
glucose screening test results. Obstetrics and Gynecology, 76(4), 709-713.

54
Nanda, S., Savvidou, M., Syngelaki, A., Akolekar, R., & Nicolaides, K. H. (2011). Prediction
of gestational diabetes mellitus by maternal factors and biomarkers at 11 to 13 weeks.
Prenatal Diagnosis, 31(2), 135-141. doi:10.1002/pd.2636; 10.1002/pd.2636
Nankervis, A., et al. For the Australasian diabetes in pregnancy: ADIPS consensus
guidelines for the testing and diagnosis of gestational diabetes mellitus in Australia., 2013,
from http://adips.org/information-for-health-care-providers-approved.asp
Naylor, C. D., Sermer, M., Chen, E., & Farine, D. (1997). Selective screening for gestational
diabetes mellitus. Toronto trihospital gestational diabetes project investigators. The New
England Journal of Medicine, 337(22), 1591-1596. doi:10.1056/NEJM199711273372204
[doi]
Nielsen, K. (2011). Gestational diabetes mellitus: Review of projects addressing
gestational diabetes mellitus supported by the world diabetes foundation in the period
2002-2010 World Diabetes Foundation. from
http://www.worlddiabetesfoundation.org/sites/default/files/GDM%20Review.pdf
Ouzilleau, C., Roy, M. A., Leblanc, L., Carpentier, A., & Maheux, P. (2003). An
observational study comparing 2-hour 75-g oral glucose tolerance with fasting plasma
glucose in pregnant women: Both poorly predictive of birth weight. CMAJ : Canadian
Medical Association Journal = Journal de l'Association Médicale Canadienne, 168(4), 403-
409.
Pettitt, D. J. (2001). The 75-g oral glucose tolerance test in pregnancy. Diabetes Care, 24(7),
1129.
Phillipov, G. (1996). Short- and long-term reproducibility of the 1-h 50-g glucose challenge
test. Clinical Chemistry, 42(2), 255-257.
Plasencia, W., Garcia, R., Pereira, S., Akolekar, R., & Nicolaides, K. H. (2011). Criteria for
screening and diagnosis of gestational diabetes mellitus in the first trimester of pregnancy.
Fetal Diagnosis and Therapy, 30(2), 108-115. doi:10.1159/000324684; 10.1159/000324684
Portha, B., Chavey, A., & Movassat, J. (2011). Early-life origins of type 2 diabetes: Fetal
programming of the beta-cell mass. Experimental Diabetes Research, 2011, 105076.
doi:10.1155/2011/105076; 10.1155/2011/105076
Punthumapol, C., & Tekasakul, P. (2008). 50 grams glucose challenge test for screening of
gestational diabetes mellitus in each trimester in potential diabetic pregnancy. Journal of the
Medical Association of Thailand = Chotmaihet Thangphaet, 91(6), 787-793.
Rasanen, J. P., Snyder, C. K., Rao, P. V., Mihalache, R., Heinonen, S., Gravett, M. G., et al.
(2013). Glycosylated fibronectin as a first-trimester biomarker for prediction of gestational
diabetes. Obstetrics and Gynecology, 122(3), 586-594.

55
Retnakaran, R., Hanley, A. J., Connelly, P. W., Sermer, M., & Zinman, B. (2006). Ethnicity
modifies the effect of obesity on insulin resistance in pregnancy: A comparison of Asian,
south Asian, and Caucasian women. The Journal of Clinical Endocrinology and Metabolism,
91(1), 93-97. doi:jc.2005-1253.
Ruchat, S. M., Hivert, M. F., & Bouchard, L. (2013). Epigenetic programming of obesity and
diabetes by in utero exposure to gestational diabetes mellitus. Nutrition Reviews, 71 Suppl 1,
S88-94. doi:10.1111/nure.12057; 10.1111/nure.12057
Rushforth, N. B., Bennett, P. H., Steinberg, A. G., & Miller, M. (1975). Comparison of the
value of the two- and one-hour glucose levels of the oral GTT in the diagnosis of diabetes in
Pima Indians. Diabetes, 24(6), 538-546.
Sackett, D. L., Straus, S. E., Richardson, W. S., Rosenberg, W., & Haynes, R. B. (Eds.).
(2000). Evidence-based medicine: How to practice and teach EBM (2 edition ed.) Churchill
Livingstone.
Schaefer-Graf, U. M., Pawliczak, J., Passow, D., Hartmann, R., Rossi, R., Buhrer, C., et al.
(2005). Birth weight and parental BMI predict overweight in children from mothers with
gestational diabetes. Diabetes Care, 28(7), 1745-1750. doi:28/7/1745.
Sermer, M. (2003). Does screening for gestational diabetes mellitus make a difference?
CMAJ: Canadian Medical Association Journal = Journal de l'Association Médicale
Canadienne, 168(4), 429-431.
Sermer, M., Naylor, C. D., Gare, D. J., Kenshole, A. B., Ritchie, J. W., Farine, D., et al.
(1994). Impact of time since last meal on the gestational glucose challenge test. The Toronto
tri-hospital gestational diabetes project. American Journal of Obstetrics and Gynecology,
171(3), 607-616.
Shields, M., Carroll, M. D., & Ogden, C. L. (2011). Adult obesity prevalence in Canada and
the United States. NCHS Data Brief, (56)(56), 1-8.
Simon, C. Y., Marques, M. C., & Farhat, H. L. (2013). First trimester fasting glycemia and
risk factors of pregnant women diagnosed with gestational diabetes mellitus. [Glicemia de
jejum do primeiro trimestre e fatores de risco de gestantes com diagnostico de diabetes melito
gestacional] Revista Brasileira De Ginecologia e Obstetricia : Revista Da Federacao
Brasileira Das Sociedades De Ginecologia e Obstetricia, 35(11), 511-515.
Singh, A., Subramani, E., Datta Ray, C., Rapole, S., & Chaudhury, K. (2015). Proteomic-
driven biomarker discovery in gestational diabetes mellitus: A review. Journal of
Proteomics, July 26, doi: S1874-3919(15)30074-9 [pii]
Svare, J. A., Hansen, B. B., & Molsted-Pedersen, L. (2001). Perinatal complications in
women with gestational diabetes mellitus. Acta Obstetricia Et Gynecologica Scandinavica,
80(10), 899-904. doi:801006.

56
Szklo, M., & Nieto, F. J. (2014). Epidemiology: Beyond the Basics, (Third Edition), Jones &
Bartlett Learning, USA
Teede, H. J., Harrison, C. L., Teh, W. T., Paul, E., & Allan, C. A. (2011). Gestational
diabetes: Development of an early risk prediction tool to facilitate opportunities for
prevention. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 51(6),
499-504. doi:10.1111/j.1479-828X.2011.01356.x; 10.1111/j.1479-828X.2011.01356.x
The HAPO Study Cooperative Research Group. (2008). Hyperglycemia and adverse
pregnancy outcomes. New England Journal of Medicine, 358, 1991-2002.
Tjepkema, M. (2006). Adult obesity. Health Report, Statistics Canada Catalogue, 17(3), 9-
25.
Touloumi, G., Babiker, A. G., Pocock, S. J., & Darbyshire, J. H. (2001). Impact of missing
data due to drop-outs on estimators for rates of change in longitudinal studies: A simulation
study. Statistics in Medicine, 20(24), 3715-3728.
Vandorsten, J. P., Dodson, W. C., Espeland, M. A., Grobman, W. A., Guise, J. M., Mercer,
B. M., et al. (2013). NIH consensus development conference: Diagnosing gestational
diabetes mellitus. NIH Consensus and State-of-the-Science Statements, 29(1), 1-31.
Wen, S. W., Liu, S., Kramer, M. S., Joseph, K. S., Levitt, C., Marcoux, S., et al. (2000).
Impact of prenatal glucose screening on the diagnosis of gestational diabetes and on
pregnancy outcomes. American Journal of Epidemiology, 152(11), 1009-14; discussion
1015-6.
Wilson, J. M. G., & Jungner, G. (1968). Principles and practice of screening for disease.
[Principios y metodos del examen colectivo para identificar enfermedades] Boletin De La
Oficina Sanitaria Panamericana.Pan American Sanitary Bureau, 65(4), 281-393.
Yeral, M. I., Ozgu-Erdinc, A. S., Uygur, D., Seckin, K. D., Karsli, M. F., & Danisman, A.
N. (2013). Prediction of gestational diabetes mellitus in the first trimester, comparison of
fasting plasma glucose, two-step and one-step methods: A prospective randomized controlled
trial. Endocrine, 46(3), 512-518. doi:10.1007/s12020-013-0111-z

57
ANNEXES
Letters relating to my MSc work.
Ardilouze JL, Mahdavian M, Baillargeon JP, Hivert MF. Glucose challenge test for detecting
gestational diabetes mellitus: a systematic review. British Journal of Obstetrics and
Gynecology (BJOG). 2012;119(10):1283; author reply 1283-4. doi: 10.1111/j.1471-
0528.2012.03423.x. [Reproduction authorized by Blackwell Publishing]
Mahdavian M, Hivert MF, Baillargeon JP, Menard J, Ouellet A, Ardilouze JL. Gestational
diabetes mellitus: simplifying the international association of diabetes and pregnancy
diagnostic algorithm using fasting plasma glucose: comment on Agarwal, Dhatt, and Shah.
Diabetes Care. 2010;33(11):e145; author reply e146. doi: 10.2337/dc10-1454.
[Reproduction authorized by the American Diabetes Association]

58

59

Top Related