




Langages
Pages
Légal


Bruxism: Theory and Practice
Editor: Daniel A. Paesani
Contributors:Monica Andersen, Taro Arima,Lene Baad-Hansen, Marta M. Barreiro,Gunnar E. Carlsson, Fernando Cifuentes,Sergio Fuster, Jorge Mario Galante,Carlos Gianoni, Fernando Goldberg,Hans L. Hamburger, Faramarz Jadidi,Anders Johansson, Ann-Katrin Johansson,Takafumi Kato, Marcelo Kreiner,Stephanos Kyrkanides, Frank Lobbezoo,Ricardo L. Macchi, Daniele Manfredini,Arturo E. Manns Freese, Machiel Naeije,Luca Guarda Nardini, Ridwaan Omar,Claudia Restrepo, Xiomara Restrepo-J.,Andres R. Sanchez, Guillermo Schinini,Teresa Cristina Barros Schütz, José T. T. de Siqueira, Peter Svensson,Ross H. Tallents, Sergio Tufik
London, Berlin, Chicago, Tokyo, Barcelona,Beijing, Istanbul, Milan, Moscow, New Delhi,Paris, Prague, São Paulo, Seoul, and Warsaw


For years the dental profession has been intrigued,fascinated, and sometimes even obsessed with thephenomenon we call bruxism. It has been under-diagnosed, overdiagnosed, and even misdiag-nosed. Some have described it as the most destruc-tive process affecting the masticatory structures,while others refer to it as a benign routine activity.Some suggest it is rare, while others say it is verycommon. Some say it is a major contributor totemporomandibular disorders, while others say itis not even related.
The etiology of bruxism has been hotly debatedfor years. Some believe it is a peripherally gener-ated activity associated with tooth contacts, whileothers believe it is a central brainstem-drivenprocess. There is a long list of suggested causes ofbruxism such as eccentric tooth contacts, dentalmalocclusion, emotional stress, anxiety, sleep dis-turbances, genetic factors, medications, alcoholconsumption, breathing disorders, allergies, men-tal disorders, and even pin worms. Bruxism is evenmentioned in the Holy Bible as the “gnashing ofteeth” associated with anger and frustration.
The dental profession has learned that studyingbruxism is difficult and controversial. Most patientsare unaware of their bruxing activity and thereforedeny it. Bed partners are sometimes more reliablereporters. We dentists seem to inform all ourpatients that they brux; they just don’t know it. Wemost probably do this because we see the evidenceof tooth wear, yet timing may be a serious issue. Forinstance, significant tooth wear in a 40-year-oldpatient may present as a dental problem; yet this
wear might have occurred 20 years earlier and brux-ism is no longer a contributing factor.
Clinicians have also developed a wide varietyof treatments for bruxism, many with no scien-tif ic evidence. Dental treatments have rangedfrom selectively adjusting the occlusion to pros-thetic or orthodontic therapies. We have de-veloped a wide variety of occlusal appliances,most with limited to no supportive data. We havesuggested non-dental therapies such as medica-tions, biofeedback, stress reduction, and acu-puncture. We have even used negative-feedbackdevices including electric shocks, loud noises,and taste aversion. It is obvious that we need tounderstand and document the most effectivemethod to manage bruxism.
It is quite evident that the profession needs acomprehensive review of this complex phenom-enon known as bruxism. Dr. Daniel Paesani rec-ognized this need and has put together the mostthorough body of information ever created by theprofession. He has assembled some of our finestexperts from around the world to contribute theirknowledge and insights to this text. His compre-hensive list of chapters has left no stone unturned.This text is the most complete overview of bruxismthe profession has ever had opportunity to review.
There are several reasons why I am very pleasedto have been asked to write the foreword to thistextbook. First, this text represents the first com-prehensive attempt to review bruxism, and theprofession needs to be enlightened and informedabout this important subject. I am also very pleased
V
Foreword

Foreword
VI
because I have known Daniel Paesani for almost30 years and I know and appreciate his dedicationto the field. Dr. Paesani was one of my very firstinternational residents in our Orofacial PainCenter and he came from Rosario, Argentina toLexington, Kentucky with much passion for thefield and personal sacrifice. I have always admiredhis dedication and work ethic, and this text is a
product of just that. I believe it will serve ourprofession well.
Jeffrey P. Okeson, DMDChair, Department of Oral Health Science
Director, Orofacial Pain ProgramUniversity of Kentucky College of Dentistry
Lexington, Kentucky, USA

VII
Over my 12 years as Professor of MasticatorySystem Physiology in the School of Odontology ofthe Universidad del Salvador/AOA (Buenos Aires,Argentina), the biggest problem we have had to facehas been the lack of scientif ic compilations onbruxism, which are needed for students to takebruxism as an object of study.
At first, we used to request students to visit theMedline web page – the most important biomed-ical-literature database worldwide – and performsearches, but before long we realized that was notthe right track. The students faced the difficultyof having to select which pieces of information touse from the thousands of publications retrievedby search engines. Of course, since these weref irst-degree students, they were not yet suff i-ciently qualif ied to differentiate concepts that hadbeen validated by scientific method from con-cepts based simply on mysticism and dogma. We,the professors, would spend long hours assistingthem with these issues, and we would use thescarce, precious time available to us to select andcompile the study material rather than to teach.
This experience made me wonder why –researchers and published books being so many andbruxism being such an important entity in theodontological field – not a single volume existeddevoted exclusively to bruxism. When I found noanswer to this question, I started to think about tak-ing on the responsibility to compile informationwith the aim of publishing a volume exclusivelydevoted to bruxism and its treatment.
After preparing an extensive list of chapters, andwith the purpose of addressing all the topics relat-ed to bruxism, I invited a group of colleagues whosebrilliant professional careers, experience, and ded-ication to the subject would a priori guarantee theiraddressing the specific topics with scientific andscholarly rigor. The premise was that each para-graph, each idea, each suggestion should be basedon scientific evidence, so that the work, apart frombeing useful to college professors and students, isan interesting book for general practitioners, onethat provides answers to the many questions aris-ing in everyday dental practice. Also, specialists incraniomandibular disorders will benefit from thein-depth analysis of the subjects and the extensive,up-to-date bibliographies contained herein, whichprovide a quick, well-organized way to access theevidence they need in their professional practiceand as a tool for planning future research. So, thevolume is divided into three sections.• The first section comprises eight chapters
dealing with bruxism knowledge and guide-lines for diagnosis, sleep physiology, mainetiological theories, inf luence of peripheraland emotional factors, movement disorders,and bruxism in children.
• The second section comprises nine chaptersand is devoted to the effects of bruxism on themasticatory system components. Some of thetopics are: the noxious action of bruxism ondental pulp, periodontal ligament, temporo-mandibular joints, muscles, and its relation-
Preface and Acknowledgments

ship with pain. Some bruxism effects that arecurrently controversial are discussed, forwhich purpose a wide review of the literatureon the subject is provided. Special emphasishas been placed on tooth wear and on the dif-ferential diagnosis of bruxism’s several caus-es. One chapter has been specifically devotedto dental erosion, and another chapter toendogenous erosion mechanisms, since gen-eral practitioners often mistake tooth wearcaused by endogenous erosion for tooth wearcaused by bruxism.
• The third section comprises eight chaptersand deals with various aspects related to thetreatment of bruxism. The pharmacologicaleffects of certain central-action drugs andsome peripheral-action drugs, such as botu-linum toxin, are described. The text also dealswith the treatment of bruxism involving den-tal implants and appliances constructed withdental materials particularly recommendedfor bruxers. Topics related to dental occlu-sion are discussed with the aim of facilitatingunderstanding of the concepts needed toenter the fascinating world of complex oralrehabilitation. One chapter deals with tech-niques used for the reconstruction of teethaffected by significant wear.
The volume also includes a review of the scientif-ic evidence on the treatment of bruxism, especial-ly bruxism splints. The different procedures usedfor protecting the masticatory system against theeffects of bruxism are described and illustrated bymeans of case reports.
AcknowledgmentsI would like to express my gratitude to:• the contributing authors, whose valuable
expertise and thorough dedication ensuredthe excellent coverage of a wide range oftopics related to bruxism
• Professors Jeffrey Okeson, Ross Tallents,Per-Lennart Westesson, and Annika Isbergfor introducing me to the marvelous worldof science
• Quintessence Publishing for believing in thisbook and accepting it for publication
• professional translators Ángela Giottonini(Chapters 1, 15, and 21) and María MirelaPerusia (Chapters 2, 9–14, 20, 23, and 25) fortheir brilliant translations of the originalSpanish text into English
• Valeria Castillo for proofreading the originalSpanish text
• the staff of the library of the AsociaciónOdontológica Argentina (Dental Associationof Argentina) for their valuable help inobtaining the innumerable bibliographicalreferences I have used
• my assistants Liliana Rivalta, Gabriela Allo,and Patricia Peloso for their endless patienceand dedication and their invaluable help inthe management of the numerous patientsand in the process of obtaining the clinicalphotographs
• my family, Triana, Guido, Julia, Pedro,Susana, and Candela, who, in all their love,gave up sharing many irretrievable days withme.
Daniel Angel PaesaniEditor
Preface and Acknowledgments
VIII

IX
List of all contributors
Editor
Daniel A. Paesani, DDSProfessor of Stomatognathic PhysiologySchool of DentistryUniversity of Salvador/AOABuenos Aires, Argentina
Contributors
Monica Andersen, PhDAssociate ProfessorDepartment of PsychobiologySchool of MedicineUniversidade Federal de São Paulo (UNIFESP)São Paulo, Brazil
Taro Arima, DDS, PhDAssistant ProfessorDepartment of Oral RehabilitationGraduate School of Dental Medicine University of HokkaidoSapporo, Japan
Lene Baad-Hansen, DDS, PhDAssociate ProfessorDepartment of Clinical Oral PhysiologySchool of DentistryAarhus UniversityAarhus, Denmark
Marta M. Barreiro, DDS, Dr DentProfessor of Dental MaterialsSchool of DentistryUniversity of Buenos AiresBuenos Aires, Argentina
Gunnar E. Carlsson, LDS, Odont Dr/ PhD, Dr Odont hc, Dr Dent hc, FDSRCSProfessor EmeritusDepartment of Prosthetic Dentistry/Dental Materials ScienceSpecialist in Prosthodontics and TMD/Orofacial PainInstitute of OdontologyThe Sahlgrenska AcademyUniversity of GothenburgGöteborg, Sweden
Fernando Cifuentes, DDSAssistance ProfessorDepartment of Stomatognatic PhysiologySchool of DentistryUniversity of Salvador/AOABuenos Aires, Argentina
Sergio Fuster, MDGastroenterology SpecialistPrivate Practice, Rosario, Argentina
Jorge Mario Galante, DDSAssociate ProfessorSchool of DentistryUniversity of Buenos AiresBuenos Aires, Argentina

List of all contributors
Carlos Gianoni, MDGastroenterology SpecialistPrivate PracticeRosario, Argentina
Fernando Goldberg, DDS, PhDProfessorDepartment of EndodonticsSchool of DentistryUniversity of Salvador/AOABuenos Aires, Argentina
Hans L. Hamburger, MD, PhDNeurologistDepartment of Clinical NeurophysiologyAmsterdam Center for Sleep-Wake StudiesSlotervaart HospitalAmsterdam, The Netherlands
Faramarz JadidiPhD studentDepartment of Clinical Oral PhysiologySchool of Dentistry, Aarhus UniversityAarhus, Denmark
Anders Johansson, DDS, Odont Dr/PhDProfessorDepartment of Clinical Dentistry - ProsthodonticsSpecialist in Prosthodontics and TMD/Orofacial PainFaculty of Medicine and Dentistry University of BergenBergen, Norway
Ann-Katrin Johansson, DDS, Odont Lic/MSc,Odont Dr/PhDAssociate Professor and Head of CariologyDepartment of Clinical Dentistry - CariologySpecialist in Pediatric DentistryFaculty of Dentistry, University of BergenBergen, Norway
Takafumi Kato, DDS, PhDAssociate ProfessorInstitute for Oral ScienceGraduate School of Oral MedicineMatsumoto Dental UniversityChiefDental Sleep Medicine ClinicMatsumoto Dental University HospitalMatsumoto, Japan
Marcelo Kreiner, DDSProfessor and ChairmanDepartment of General and Oral PhysiologySchool of DentistryUniversidad de la RepúblicaMontevideo, Uruguay
Stephanos Kyrkanides, DDS, MS, PhDProfessor and ChairmanDepartment of Orthodonticsand Pediatric DentistrySchool of Dental MedicineStony Brook UniversityStony BrookNew York, NY, USA
Frank Lobbezoo, DDS, PhDProfessorDepartment of Oral FunctionAcademic Centre for Dentistry Amsterdam(ACTA), Amsterdam, The Netherlands
Ricardo L. Macchi, DDS, MS, Dr DentProfessor Emeritus of Dental MaterialsSchool of DentistryUniversity of Buenos AiresBuenos Aires, Argentina
Daniele Manfredini, DDSVisiting ProfessorTMD ClinicDepartment of Maxillofacial SurgeryUniversity of Padova, Padova, Italy
X

List of all contributors
XI
Arturo E. Manns Freese, DDS, PhDProfessor of Oral Physiology and OcclusionSchool of Dentistry, University of the AndesSantiago, Chile
Machiel Naeije, PhDProfessor and ChairDepartment of Oral FunctionAcademic Centre for Dentistry Amsterdam(ACTA), Amsterdam, The Netherlands
Luca Guarda Nardini, MD, DDSDirectorTMD Clinic, Department of Maxillofacial SurgeryUniversity of Padova, Padova, Italy
Ridwaan Omar, BSc, BDS, LDSRCS, MSc,FRACDS, FDSRCSEdProfessor and Head of ProsthodonticsVice Dean for Academic & Clinical AffairsDepartment of Restorative SciencesFaculty of Dentistry, Kuwait UniversityKuwait
Claudia Restrepo, DDSPediatric DentistTeacher, Postgraduate Program of PediatricDentistry and Preventive Orthodontics Director of the CES-LPH Research GroupCES University, Medellin, Colombia
Xiomara Restrepo-J., DDSGeneral Practice ResidentDepartment of General DentistryEastman Institute for Oral HealthRochester, NY, USA
Andres R. Sanchez, DDS, MSPrivate Practice, Eden Prairie, MN, USAFormer Assistant Professor in PeriodonticsMarquette University School of DentistryMilwaukee, WI, USA
Guillermo Schinini, DDSClinical Assistant ProfessorDepartment of PeriodontologyMaimonides UniversityPrivate PracticeRosario, Argentina
Teresa Cristina Barros Schütz, DDS, PhDResearcherDepartment of PsychobiologySchool of MedicineUniversidade Federal de São Paulo (UNIFESP)São Paulo, Brazil
José T. T. de Siqueira, DDS, PhDHead of Orofacial Pain TeamDentistry DivisionHospital das Clínicas, School of MedicineUniversidade de São Paulo (USP)ResearcherDepartment of PsychobiologySchool of MedicineUniversidade Federal de São Paulo (UNIFESP)São Paulo, Brazil
Peter Svensson, DDS, PhD, Dr OdontProfessorDepartment of Clinical Oral PhysiologySchool of Dentistry, Aarhus UniversityAarhus, Denmark
Ross H. Tallents, DDSProfessor of DentistryDepartment of Orthodontics and ProsthodonticsEastman Institute for Oral HealthRochester, NY, USA
Sergio Tufik, MD, PhDProfessorDepartment of PsychobiologySchool of MedicineUniversidade Federal de São Paulo (UNIFESP)São Paulo, Brazil


PART 1: OVERVIEW OF THE PROBLEM
Chapter 1 - Introduction to Bruxism 3Daniel A. Paesani
Introduction 3The Importance of Bruxism in Daily Care 3Oral Habits 4Classification of Bruxism according to the Type and Timing of Activity 4Etiology 5Genetics 5Epidemiology 10Bruxism Variability 15References 15
Chapter 2 – Diagnosis of Bruxism 21Daniel A. Paesani
Introduction 21Clinical Diagnosis 22Complementary Methods for Diagnosis 31References 38
Chapter 3 – Sleep Physiology and Bruxism 41José T. T. de Siqueira, Teresa Cristina Barros Schütz, Monica Andersen, and Sergio Tufik
Introduction 41Basic Facts of Sleep Physiology and Pathophysiology 42Sleep Architecture 44The Sleep Laboratory 47Understanding Bruxism in a PSG 47Conclusion 50References 51
XIII
Contents

Contents
Chapter 4 – Etiology of Bruxism 53Frank Lobbezoo, Hans L. Hamburger, and Machiel Naeije
Introduction 53Categories 55Morphologic Factors 55Psychosocial Factors 57Pathophysiologic Factors 58Conclusion 61References 62
Chapter 5 – Role of Peripheral Sensory Factors in Bruxism: A Physiologic Interpretation for Clinical Dentistry 67Takafumi Kato
Introduction 67Basic Knowledge of Orofacial Sensorimotor Systems 68Which Event Comes First: Tooth Contact or Jaw Muscle Activity? 72Sensory Stimuli and Sleep Bruxism 76Can the Peripheral Sensory System Explain the Role of an Oral Splint in SB Management? 79Conclusion 81References 81
Chapter 6 – Emotional Factors in the Etiology of Bruxism 87Daniele Manfredini
Introduction 87Literature Search 88Bruxism and Stress 89Psychosocial Aspects of Bruxism 91The Relationship between Bruxism and Pain 91Sleep versus Awake Bruxism, and Grinding versus Clenching 93Conclusion 95References 95
Chapter 7 – Movement Disorders in the Dental Office 99Frank Lobbezoo, Hans L. Hamburger, and Machiel Naeije
Introduction 99Literature Search 100Dyskinesias 100Conclusion 105References 106
XIV

Contents
Chapter 8 – Bruxism in Children 111Claudia Restrepo
Introduction 111Etiology of Bruxism in Children 111Epidemiology of Bruxism in Children 113Factors Associated with Bruxism 113Diagnosis of Bruxism in Children 115Effect of Bruxism on the Dentition of Children 115Effect of Bruxism on Craniofacial Morphology 117Bruxism in Children with Special Characteristics 117Management of Bruxism in Children 118References 118
PART 2: EFFECTS ON THE MASTICATORY SYSTEM
Chapter 9 – Tooth Wear 123Daniel A. Paesani
Introduction 123Etiology of Tooth Wear 124Types of Attrition 125Physiologic Attrition 125Tooth Wear Quantification 126Factors Involved in Tooth Wear 129Tooth Wear Patterns 132Interpretation of Tooth Wear 138Conclusion 145References 147
Chapter 10 – Dental Erosion 149Daniel A. Paesani
Introduction 149Prevalence 149Clinical Features and Diagnosis of Erosion 150Classification of Erosion according to Its Magnitude 155Classification of Erosion according to Etiology 155Etiopathogenic Mechanism and Conditioning Factors 169Salivary Secretion and Buffering Capacity Quantification 176References 183
XV

Contents
Chapter 11 – Gastroesophageal Reflux as a Cause of Dental Erosion 187Sergio Fuster and Carlos Gianoni
Introduction 187Anatomophysiology of the Upper Digestive Tract 187Definition of Ref lux 190Pathophysiology of Ref lux 191Clinical Manifestations of Ref lux 192Diagnosis of Ref lux 196Role of Dental Practitioners in Diagnosing Ref lux 200Treatment of Ref lux 200Conclusion 202References 202
Chapter 12 – Controversies on the Effects of Bruxism 207Daniel A. Paesani
Introduction 207Effects on Dentition 207Effects on Soft Tissues 220Effects on Bone 222References 229
Chapter 13 – Effects of Bruxism on Teeth and Its Relationship with Endodontics 233Fernando Goldberg
Introduction 233Pulp and Peri-radicular Alterations 233Alterations in Crown and Root Structural Integrity 243References 254
Chapter 14 – Influence of Trauma from Occlusion on the Periodontium 257Guillermo Schinini and Andres R. Sanchez
Introduction 257Periodontal Lesions 258Occlusal Trauma Lesions 258Effect of Occlusal Trauma on the Healthy Periodontium 259Effect of Occlusal Trauma on the Diseased Periodontium 262Human Clinical Evidence 264Conclusion 267References 268
XVI

Contents
Chapter 15 – Effects of Bruxism on Muscles 271Arturo E. Manns Freese
Introduction 271Principles of Skeletal Muscle Physiology 272Ultrastructure of Skeletal Muscle 275Comparing Normal Function and Parafunction 280Pathophysiology of Muscular Disorders and Related Pain 282Types of Muscular Pain 283Conclusion 293References 294
Chapter 16 – Temporomandibular Joint Dysfunction and Bruxism 297Xiomara Restrepo-Jaramillo, Ross H. Tallents, and Stephanos Kyrkanides
Introduction 297Definitions 297Prevalence Studies 298Etiology 299Pathways to Joint Degeneration 300The Role of Bruxism 301Conclusion 304References 304
Chapter 17 – Pain and Bruxism 309Peter Svensson, Faramarz Jadidi, Taro Arima, and Lene Baad-Hansen
Introduction 309Overview of Pain Mechanisms 309Sex-related Differences in Pain Experience 313Pain Genetics 314Experimental Bruxism and Craniofacial Pain 314Clinical Studies of Bruxism and Craniofacial Pain 317Intervention Studies of Bruxism 320Conclusion 321References 322
PART 3: CLINICAL APPROACHES
Chapter 18 – Pharmacologic Considerations in Bruxism 327Marcelo Kreiner
Introduction 327
XVII

Contents
Anxiolytic Drugs 328Antidepressant Drugs 329Neuroleptics 331Addictive Social Drugs 332Adrenergic Antagonists and Agonists 334Agonists of Dopaminergic Receptors 334Antiepileptics 335References 336
Chapter 19 – Dental Materials for the Bruxing Patient 339Marta M. Barreiro and Ricardo L. Macchi
Introduction 339Criteria for Material Selection 340General Wear Processes 343Evaluation of Wear Behavior 348Degradation of Restorative Materials 350Conclusion 355References 355
Chapter 20 – Evidence Related to the Treatment of Bruxism 359Daniel A. Paesani
Introduction 359Treatments for Sleep Bruxism 359Awake Bruxism 374References 378
Chapter 21 – Introduction to Complex Oral Restoration 383Daniel A. Paesani and Fernando Cifuentes
Introduction 383Centric Relation 383Axis of Rotation of the Mandible 394The Anterior bite Plane Method 398References 412
Chapter 22 – Restoration of the Worn Dentition 415Anders Johansson, Ann-Katrin Johansson, Ridwaan Omar, and Gunnar E. Carlsson
Introduction 415Historical Aspects 415Epidemiology 416
XVIII

Contents
Etiology of Tooth Wear 418Principles and Management Strategies for Tooth Wear 419Rehabilitative Strategies 423Maintenance Phase 436Conclusion 436References 437
Chapter 23 – Effects of Bruxism on Restorative Implant-assisted Prosthesis Treatments 439Jorge Mario Galante
Introduction 439Peri-implant Pathology Classification 441Classification of Complications of IAP Restorative Treatments 449Prosthetic Rehabilitation with Implants in Bruxers 454Conclusion 464References 464
Chapter 24 – Botulinum Toxin in the Treatment of Bruxism 467Daniele Manfredini and Luca Guarda Nardini
Introduction 467History of Botulinum Toxin as a Therapeutic Drug 467Mechanism of Action 468Fields of Application 469Safety of Botulinum Toxin Treatments 469Orofacial Pain Relief 470Temporomandibular Disorders 470Botox and Bruxism 471Conclusion 473References 473
Chapter 25 – Clinical Treatment of Bruxism 477Daniel A. Paesani and Fernando Cifuentes
Canine Guidance in the Control of Bruxism Effects 477Bruxism Splints 484Fabrication of the Bruxism Splint 490Bruxism Splint Maintenance 515Treatments with Botulinum Toxin 516References 522
Index 525
XIX


Overview of the problem
Part 1


Introduction
In the glossary of terms of the American Academyof Orofacial Pain, bruxism is defined as a “totalparafunctional daily or nightly activity thatincludes grinding, gnashing, or clenching of theteeth. It takes place in the absence of subjectiveconsciousness and it can be diagnosed by the pres-ence of tooth wear facets which have not resultedfrom the chewing function”.1
In order to understand the remoteness of the actof “gnashing the teeth”, we can cite the followingpassages from the Bible:
Psalm 35:16 “Like profane mockers at a feast,they gnash at me with their teeth”
Psalm 112:10 “The sinner shall see and beangry, he shall gnash his teeth and consume away”
Job 16:9 “he grinds his teeth at me”Matthew 8:12 “But the children of the king-
dom shall be cast out into outer darkness: thereshall be weeping and gnashing of teeth”
At the beginning of the twentieth century,Karolyi used the term “traumatic neuralgia” to
refer to the grinding of the teeth and described itas the cause of a periodontal condition by thencalled pyorrhea.2 The term “bruxism” comes fromthe Greek expression brychein odontas that meansgrinding the teeth. In French, bruxomanie was usedfor the first time by Marie and Pietkiewicz in1907.3 Then, Frohman was responsible for the firstpublication in the odontological literature whenhe referred to “bruxomania” as a pure psycho-logical state.4
The Importance of Bruxism in Daily Care
Bruxism may be considered a normal habit; butunder certain circumstances, such as an increase inthe frequency of episodes and the strength of mas-seter contractions, it may turn into a phenomenonwith pathological consequences.5 Bruxism maydramatically change the result and the duration ofthe delicate and careful treatments performed byclinicians. Whereas a soft form of bruxism hardlyever affects oral structures, a hard manifestation
Chapter 1
3
Daniel A. Paesani
Introduction to Bruxism

• complementary methods: use of intraoral devicesfor tooth wear quantification (splints; Brux-core®, Boston, MA, USA) and bite force detec-tors; masseter electromyography (EMG, ambu-latory EMG, disposable EMG devices such asBiteStrip®); and sleep polysomnography.
Clinical Diagnosis
SymptomsA rapid way of collecting information is to requestthe patient to answer a questionnaire. It is the mostwidely available method to be used in everydaypractice. Chapter 1 has already discussed the advan-tages and disadvantages of this method in the diag-nosis of bruxism symptoms.
Questionnaires are very useful for obtaining agreat amount of information in a short time. A goodquestionnaire should include a wide range of ques-tions concerning the patient’s general health status,diseases, medication, etc. Of course, as the mainsubject of this book is bruxism, we will just be deal-ing with the questions that specifically refer to it.
Table 2-1 shows sample questions that can beadded to the general questionnaire usually usedduring the patient’s first appointment; such a gen-eral questionnaire is simply about a collection ofsymptoms that can be attributed to bruxism. It isadvisable to include “Don’t know” among the
Daniel A. Paesani
22
Questionnaire for detection of bruxism.Yes No Don’t know
Do you grind your teeth when you sleep?
Has anybody heard you grind your teeth while you sleep?
On waking up, do you usually find that you are clenching your teeth?
When you wake up, do you usually have jaw pain or jaw fatigue?
When you wake up, do you usually have the feeling that your teeth are loose?
When you wake up, do you usually have sore teeth and/or sore gums?
When you wake up, do you usually have a headache in the temples?
When you wake up, do you usually have a jaw lock?
Have you ever found that you were clenching your teeth in the daytime?
Have you ever found that you were grinding your teeth in the daytime?
Table 2-1
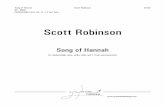
Fig 2-1 Enamel fracture in both central incisors, as a result ofbruxism in the protrusive direction. Note also the abrasivewear of vestibular enamel, caused by hard tooth brushing.

Diagnosis of Bruxism
possible choices; this will prevent false-positiveand false-negative answers from patients who arenot sure of how to respond. At the first appoint-ment, during history taking, it is recommendedthat the clinician quickly asks the patient the samequestions from the questionnaire again in order toconfirm the accuracy of the patient’s answers.
SignsIn the clinical examination, some signs may bepresent to suggest bruxism. The character of thesesigns (and symptoms) is “relative”, since they aloneare not sufficient evidence of bruxism; althoughfrequently mentioned in the literature, the fact isthat they have not yet been validated by scientificmethod. Future controlled investigations will haveto determine the corresponding sensitivity andspecificity values for each of them. So far, only theclinical validity of tooth-grinding sounds during
sleep (witness statements based on two episodesper week) has been studied. When checked againstpolysomnography, they showed a sensitivity of78% and a specificity of 98%.1
Tooth wearAlthough this has a strong association with bruxism,it is not a specific sign since there are many causes oftooth wear. Grinding causes the teeth to deterioratein a specific way (attrition). Tooth wear can be stud-ied by direct visual inspection of the mouth, byexamining plaster models of the patient’s teeth, andby taking a look at intraoral pictures. This subject isdiscussed in detail in Chapter 9.
FracturesThere may be fractures in natural teeth, prosthe-ses, dental implants, and dental restorations (Figs2-1 to 2-11).
23
a b
c
Fig 2-2 (a) Fracture line in a mandibular molar (arrow)caused by bruxism of the clenching type. (b) No frac-ture is evident in the periapical radiograph, although areactive area in the interradicular space can be seen(arrow). (c) Opening of the molar reveals that the frac-ture has reached the pulp chamber (arrow).

Marta M. Barreiro and Ricardo L. Macchi
lubricant that acts in each case can be seen in Table19-3. The contacts can be tooth against tooth,tooth against restoration, restoration againstrestoration, as well as a tooth brush or other foreignbody – which includes foods.
Corrosive wear or erosion can take place whena chemical process is added, as happens by theeffect of acid in bulimic patients. Wear by superfi-cial fatigue can be the consequence of a habit suchas biting on a solid object (e.g., a pen), whichinvolves the application of high compressive loads.
In the case of bruxism, two-body wear or attritionis found. Tooth surfaces come into direct contact,the frequency of sliding is incremented as well asthe loads that are applied, and all these factors leadto significantly greater wear and increased possi-bility of fatigue failure.15
Evaluation of Wear Behavior
Laboratory simulator and clinical studies can beused to evaluate intraoral wear.
In-vitro Laboratory StudiesThe use of in-vitro studies provides an approxi-mation of the evaluation of wear of new materialsbefore their clinical application.31,32
Is the prediction of wear behavior of dentalmaterials possible? One important point to keep inmind when evaluating lab studies is the difficultiesthat appear when attempting to simulate conditionspresent in the oral cavity. The very many variablesthat participate in wear make its measurement witha single parameter difficult, even when variationsseen from patient to patient are not considered.31
The weak correlation that is seen betweenmechanical properties and wear is remarkable.Some physical properties such as water sorptioncan give just a hint of potential wear, particularlywhen corrosive wear is considered.
348
Fig 19-10 Proximal contact between restorations with different hardnesses: (a) porcelain–metal, and (b) porcelain–composite.Several mechanisms are present – two-body, three-body, and corrosive wear.
Fig 19-11 (a and b) Proximal wear in teeth with proximalcomposite resin restorations. This type of wear is also seen onenamel and is increased in the presence of periodontal mobil-ity. (Modified from Söderholm.28)
a b
a
b

Dental Materials for the Bruxing Patient
Clinical StudiesUnderstanding clinical wear requires studies inwhich the different factors that interact are takeninto account. Clinical studies are the best option inthe actual evaluation of wear, but they are expen-sive and need to be long term.33–35
Clinical wear can be expressed by the amount(in micrometers) of material loss per year, usingnormal tooth wear for comparison. For example,the American Dental Association considers that aloss no greater than 50 μm per year has to be estab-lished by means of systematic clinical studies if amaterial is to be used in posterior restorations.
Both direct and indirect methods are used inthese studies. Most of the direct studies follow cri-teria that have been established by Ryge:36 colormatching, marginal integrity, secondary caries,anatomic form, and surface roughness. Somechanges in categorization are introduced accordingto each study’s specific needs. Inter-examiner vari-ability is the main limitation to obtaining adequatediscrimination in the use of scales.
Indirect methods use impressions and models,which are evaluated, or epoxy resin replicas thatcan reproduce worn surfaces, and scanning elec-tron microscopy observation.
Loss of vertical dimension is commonly meas-ured in clinical studies. Visual examination is fastand no additional cost is required, but it is proneto subjective variation; often just changes inanatomic force are registered without any quan-tification. Special optical or scanning electronmicroscopes and profilometers allow for greaterprecision in the evaluation of material loss. Surfacechanges in exposed cavity walls can be evaluated soas to establish the types of wear that are present.
Many discrepancies are seen between resultsfrom in-vitro lab studies and observation in long-term clinical studies. The evaluation of actualbehavior with reliable measurements is still a prob-lem to be solved. Present efforts are focused on theuse of wear simulators for wear studies, and theseresults have be corroborated later by clinical stud-ies.31
349
Table 19-3
Most frequent wear types within the oral cavity: comparison between dental and materials science terminology (modified from Vale Antunes and Ramalho3).
Causes of wear Dental term Material terminology Lubricant/abrasive
PhysiologicWithout occlusal contactDirect contactContact and sliding
AbrasionAttritionAttrition
Three-bodyTwo-bodyTwo-body
Saliva/foodSalivaSaliva
PathologicBruxismXerostomiaChemical attackNegative habits
AttritionAttritionErosionAttrition/abrasion
Two-bodyTwo-bodyCorrosionTwo- or three-body
Saliva–Saliva–
HygieneTooth brushing Abrasion Three-body Water/dentifrice

Daniel A. Paesani and Fernando Cifuentes
Splint attachment problems are much simpler tosolve, since only retainer tightening is re quired.
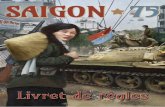
In order to perform splint occlusal adjustment,it is advisable not to polish the surface of the splintfully. Another option is to request the laboratoryto deliver the splint with a coarse surface, or toremove the splint’s gloss by using thin sandpaperin order to better visualize occlusal contacts. Oncethe patient is in the dorsal recumbent position,they are requested to give a series of quick tapswith their teeth on the splint, while articulatingpaper is made to come between splint and teeth(Fig 25-32). An acrylic bur is used to wear out allthe premature contact points. This procedure isrepeated as many times as necessary, until all thevestibular cusps and incisal edges simultaneouslyocclude on the surface of the splint. The simul -taneous contacts obtained during mouth closureare comparable to maximum intercuspation at adental level. Thus, each of these points (closurestops) will be responsible for the stability of itsrespective antagonist tooth. Also, the combinedaction of all of them guarantees a steady positionof the jaw during mouth closure and, especially,during tooth clenching episodes while the bruxeris wearing the splint.
Next, the aim is to make anterior guidance har-monious (Figs 25-33 and 25-34). To do this, it isadvisable to use articulating paper of a differentcolor. Articulating paper is placed between theteeth and the splint while having the patient makelateral and protrusive movements. Any contact inthe posterior segment should be carefullyremoved, with the exception of those contactsmatching the ones obtained in the previous step(closure stops). In short, during closure, one con-tact per cusp or lower incisal edge should occur inthe splint; during eccentric movements (lateralmovement and protrusion), the anterior guidanceshould prevent premolar and molar cusps fromcoming into contact with the surface of the splint.
502
a
b
c
Fig 25-32 Occlusal adjustment of the splint. (a) Ask thepatient to close their mouth repeatedly and give a series of tapswith their teeth on the splint, while articulating paper is placedbetween the splint and the teeth. (b and c) The aim is to obtainone contact point per cusp or antagonist incisal edge.

Clinical Treatment of Bruxism
503
Fig 25-33 (a) With articulating paper of a different color, anterior guidance functioning is tested. (b) The white arrows indicatethe trajectories created during lateral movements; the black arrows indicate protrusive movement trajectories.
a b
a b
c
Fig 25-34 (a–c) Correct functioning of the anterior guid-ance of the splint causes the posterior segments to separate andprotects them against premature wear during tooth grindingepisodes.
Top Related