Work-Related Musculoskeletal Disorders (WMSDs) - Irsst
58
WMSD D WMSD SD WMSD WMSD WMS WMSD WMSD WMSD WMSD W WMSD WMSD WMSD WMSD SERGE SIMONEAU MARIE ST-VINCENT DENISE CHICOINE Work-Related Musculoskeletal Disorders (WMSDs) A BETTER UNDERSTANDING FOR MORE EFFECTIVE PREVENTION Association paritaire pour la santé et la sécurité du travail Secteur fabrication de produits en métal et de produits électriques
Transcript of Work-Related Musculoskeletal Disorders (WMSDs) - Irsst

WMSD
D WMSD
SDWMSD
WMSDWMSWMSD
WMSD
WM
SD
WMSD
W WMSD
WMSDWMSD
WM
SD
SERGE SIMONEAU
MARIE ST-VINCENT
DENISE CHICOINE
Work-Related Musculoskeletal Disorders(WMSDs)
A BETTER UNDERSTANDINGFOR MORE EFFECTIVE PREVENTION
Association paritaire pour la santéet la sécurité du travailSecteur fabrication de produits en métal et de produits électriques
SERGE SIMONEAU
MARIE ST-VINCENT
DENISE CHICOINE
A BETTER UNDERSTANDINGFOR MORE EFFECTIVE PREVENTION
Work-Related Musculoskeletal Disorders(WMSDs)

TranslationLe Dernier Mot Inc
Graphic Design and LayoutHélène Camirand
IllustrationsFrancine Mondor
AcknowledgementsWe would like to thank the following people fortheir comments and suggestions:
Lina Forcier and Sylvie Beaugrand of the IRSST,Nicole Vézina of the UQAM, Denis Dubreuil ofLightolier Canada, Jean-François Beaudry and SophieAlbert of CAE Électronique, Sylvain Blackburn ofNortel,Anne O’Donnell and Diane Mimeault ofMarconi Canada, Clément Trépanier of IBM Canada,Michel Roy of Fertek, and Marie-Josée Ross andChantal Pagé and Michel Charland of the A.S.P.Métal-Électrique.
We would also like to thank Martine Gamache forallowing us to use some of her illustrations.
Certain illustrations are drawn from:Putz-Anderson,V (Ed). (1988). NIOSH, CumulativeTrauma Disorder: A Manual for Musculoskeletal Diseasesof the Upper Limbs, Philadelphia,Taylor & Francis,p. 12, 13, 66, 67Grandjean, E. (1982). (1982). Fitting the Task to theMan:An Ergonomic Approach, London,Taylor &Francis, p.7Lindqvist, B. (1986). Ergonomic Tools in our Time.Stockholm,Atlas Copco, p.14.
All translation rights reserved© 1996 Association paritaire pour la santé et la sécurité du travail –
Secteur fabrication de produits en métal et de produits électriquesInstitut de recherche Robert-Sauvé en santé et en sécurité du travail du Québec
Work-Related MusculoskeletalDisorders (WMSDs)A BETTER UNDERSTANDINGFOR MORE EFFECTIVE PREVENTION
SERGE SIMONEAU
MARIE ST-VINCENT
DENISE CHICOINE
The production of this document was funded by the IRSST and the A.S.P. Métal-Électrique.The conclusions andrecommendations are those of the authors.The reproduction of texts is authorized, provided the source is mentioned and a copy is sent to us at:Association paritaire pour la santé et la sécurité du travail – Secteur fabrication de produits en métal et de produits électriques6075, rue Jean-Talon Est, bureau 201Saint-Léonard, Québec H1S 1N2

Table of ContentsPreface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . V
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VII
Chapter 1 — What is a WMSD?
A matter of definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
A major problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Serious consequences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Characteristics of WMSDs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
WMSDs result from overuse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
WMSDs develop gradually . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
WMSD prevention can be very effective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
WMSDs have multiple causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
How do WMSDs appear? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
First symptoms of WMSDs: early indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Knowing how WMSDs develop for timely intervention . . . . . . . . . . . . . . . . . . . . 6
The most common WMSDs and structures affected . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Tendonitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Tenosynovitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Bursitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Carpal tunnel syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Chapter 2 — Causes of WMSDs
Many risk factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Three major modulators: intensity, frequency, duration . . . . . . . . . . . . . . . . . . . . . . . . 15
Intensity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Frequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Duration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Risk factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Awkward postures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
What determines posture? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Force, effort and musculoskeletal load . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Characteristics of work requiring force . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Factors affecting intensity of effort . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Static muscular work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Repetition and invariability of work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28

VI
Exposure to certain physical aggressors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Mechanical pressures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Shocks and impacts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Vibrations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Cold . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Organizational factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Work load and work pace . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Work schedules . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Technological changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Social environment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Chapter 3 — How to detect a WMSD problem
Monitoring: two possible targets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Health Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Monitoring of risk factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Monitoring to evaluate the efficacy of an action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Chapter 4 — How to handle WMSDs
A comprehensive approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Several possible options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Ergonomic improvement of working conditions . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Rotation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Follow-up of affected workers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Other avenues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Ergonomic improvement of work: concrete cases . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Hanging components on a paint conveyor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Assembly of surge arrestors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53

V
Practical guides are a crystallization of our knowledge, a topographical map whichcontextualizes a given problem and provides vital indicators to guide us in ourchoices to eliminate the problem. This is the mission accomplished by this guide onmusculoskeletal injuries written by Serge Simoneau, Marie St-Vincent and DeniseChicoine.
The concept of work-related musculoskeletal disorders (WMSDs) is still rathervague and knowledge gaps on the subject still abound. The authors therefore had towork extremely hard to extract, weigh and evaluate this knowledge, in order to iden-tify a series of elements that could be put into practice. The weighting was all themore critical as there is no shortage of purveyors of miracle solutions and dubiousscientific ideas.
The development of this guide called for another important and indispensable aspectthat requires special skills: a clear understanding of client needs and, more impor-tantly, of the user’s assimilation capacity. A guide can be as good as it wants, containing all the elements required to initiate a prevention process, but if theclient/user does not find it useful, it will go unheeded.
It is also possible – indeed quite common – to overestimate the receptiveness ofusers, who may reject a document that they find too theoretical, overly complicatedand, above all, not adapted to their current needs.
In this guide, the authors have effectively balanced the choice of knowledge and itssuitability for the target clientele. Achieving this feat took the work and experienceof the Institut de recherche Robert-Sauvé en santé et en sécurité du travail duQuébec, along with the in-depth knowledge of the community by the Associationparitaire pour la santé et la sécurité du travail – Secteur fabrication de produits enmétal et de produits électriques. This collaboration led to the production of a solidguide, which has already won acclaim in several projects.
Ilkka Kuorinka, DirectorSafety-Ergonomics Program, IRSST
January 1996
Preface

VII
This document is the result of a long and productive collaboration betweenthe Institut de recherche Robert-Sauvé en santé et en sécurité du travaildu Québec (IRSST) and the Association paritaire pour la santé et la sécu-rité du travail — Secteur fabrication de produits en métal et de produits électriques (A.S.P. Métal-Électrique). It is based on the expertise acquiredduring several interventions in electrical products manufacturing plants.The content was largely drawn from the reference book produced by theIRSST and coordinated by Ilkka Kuorinka and Lina Forcier.* Producedby a group of international experts, this report presents a summary ofall scientific studies related to the prevention of WMSDs. In this guide,we have reproduced some of its elements, but in a much simpler form.
From the outset, our intention was to develop a practical tool for peoplein the industry concerned about work-related musculoskeletal disorders (WMSDs). To better meet this goal, we decided to publish twoseparate documents.
The first publication is designed for all those who want to improve theirunderstanding of WMSDs in order to prevent them more effectively. Itcontains four chapters. The first defines and explains the characteristicsof WMSDs. The second presents the main risk factors behind WMSDs.The third explains how to detect a WMSD problem, while the fourth outlines the main prevention avenues available.
The guide includes inserts (identified by a “+” in the top left corner),where we explain in more detail the concepts that would help readersunderstand the document. Each chapter ends with a summary, where wereview the main points covered. A reader who is in a hurry may get aquick overview of the contents by consulting the summary pages.
The second document will be aimed at industries that are already facingWMSD problems and that want to implement a participatory ergonomicprogram to improve working conditions. The goal of this second publi-cation is to give people in the industry the tools they need to apply suchan intervention program, in light of the experience of “ergo groups” thathave been established in many companies in the electrical sector for someyears now.
We hope that this guide will help you improve your understanding ofWMSDs and find solutions to this problem.
* Kuorinka, I., Forcier, L. (Eds.), Hagberg, M., Silverstein, B., Wells, R., Smith, M.J., Hendrick, H.W., Cayron, P., Pérusse, M. (1995). LATR, Les lésions attribuables au travailrépétitif; ouvrage de référence sur les lésions musculo-squelettiques liées au travail, ÉditionsMultimondes, 486 p.
Foreword

Our focus here is on work-relatedmusculoskeletal injuries. Thesetypes of disorders may affect the
different parts of the body associated withmovement: upper limbs, lower limbs andthe back. In this document, we will limitour examination to disorders affecting theupper limbs. There have been far fewerstudies done on work-related injuries to thelower limbs, while back pain is a highlycomplex issue that has enough singularcharacteristics to be treated separately.
It should be noted that all the differentgeneric names that are used describe virtu-ally the same problem. It is as if each author had decided to give a different nameto the phenomenon. These names often underscore the association with repetitivework, which can suggest, wrongfully, that
this is the only cause. Yet, the acronym“WMSD” (work-related musculoskeletaldisorders) seems to stand out above the rest, which is why we have decided touse it.
Fig. 1.1
The same reality behind
a multitude of names
A matter of defenition 1
What is a WMSD ?
Chapter 1
This document deals with work-related musculoskeletal injuries and their prevention.It is a complex issue that is not always easy to fully comprehend. There are many difficulties surrounding this issue, beginning with the confusion around nomenclature.This is why it is important for us to start with a clear definition
A matter of definition
R E P E T I T I V E S T R A I N I N J U RY ( R S I )
C U M U L AT I V E T R A U M A D I S O R D E R ( C T D )
U P P E R L I M B S Y N D R O M E
C E R V I C O B R A C H I A L D I S O R D E R

Fig. 1.2
A group of
musculoskeletal
disorders caused
by work
2 Chapter 1
Even though these problems have attracted much attention in recentyears, the phenomenon is not new.
For instance, Ramazinni established the linkbetween musculoskeletal injuries and workover two hundred years ago. The phenom-enon is becoming more and more wide-spread and a source of concern in mostindustrialized countries. Certain economicsectors are more associated with WMSDs,such as the food sector (slaughterhouses,meat packers), the sewing and clothing sector, the electrical and electronic productsmanufacturing sector, assembly plants inthe manufacturing sector, and working witha video display terminal (VDT). These are all sectors characterized by repetitivemanual work, but the problem tends to appear in several other sectors.
Hence, it is a major occupational safety andhealth issue, and specialists on the subjectare not very optimistic about the future.They expect compensation claims for work-related musculoskeletal injuries to keep rising in the coming years, due to a certainn u m b e r o f t r e n d s , i n c l u d i n g t h e unfavourable economic context, which encourages a faster pace, and hence repeti-tive work. With the modernization of production methods and the mechanizationof the most intensive efforts, the expectationwas for repetitive tasks to have disap-peared. Yet, there are no signs of this happening – on the contrary. Moreover, anageing workforce could be more vulnerableto musculoskeletal injuries, particularly at a time of high unemployment, which discourages mobility. People who start feeling pain can no longer change jobs easily, which could help explain the increase in WMSDs
A major problem
Regardless of the generic expression used,WMSDs are relatively diverse disordersthat may affect different structures: tendons, muscles, joints, nerves, and thevascular system. Depending on the struc-ture affected and the type of affliction, theailment would be referred to as tendonitis,
tenosynovitis, bursitis, carpal tunnel syndrome, etc. It should also be noted thatmost of these disorders may appear in circumstances unrelated to work, as in thecase of certain illnesses or following activi-ties outside of work. Since our focus is prevention at the workplace, we will onlydeal here with their appearance in situa-tions caused primarily by work.
E P I C O N DY L I T I S
T E N D I N I T I S
C A R PA L T U N N E L S Y N D R O M E
B U R S I T I S T H O R A C I C O U T L E T S Y N D R O M E

The phenomenon of WMSDs musttherefore be treated very seriously.These musculoskeletal disorders
have a considerable socio-economic impact.First, they drive up costs for workers, com-panies, and society in general. This appliesto both direct costs (compensation of victims, medicare, etc.) and indirect costs(loss of production, replacement costs, absenteeism, etc.) associated with occupa-tional diseases and industrial accidents.
Yet, despite the scale of the economic reper-cussions, the serious and sometimes dramatic consequences of WMSDs on victims must not be overlooked. Physicaland mental suffering, compensation diffi-culties, temporary or permanent limitationsin their professional activities are just a fewof the aspects of the tragedy that can strikepeople afflicted with WMSDs.
Characteristics of WMSDs 3
Serious consequences
Work-related musculoskeletal injuries can take differentforms. The onset and develop-
ment of these injuries is still not wellknown. Many theories – some complemen-tary and others contradictory – have attempted to explain the phenomenon, andit is clear that the issue is still not fully understood. Despite the diversity of afflic-tions and mechanisms involved, WMSDsshow a certain number of similar charac-teristics.
WMSDs result from overuse
Although the onset mechanisms are notclearly established, it is generally agreedthat the injuries result from overuse, beyond the body’s recovery capacity.WMSDs occur because a structure is abusedrepetitively and is made to endure a workload that it cannot tolerate without negativeconsequences.
WMSDs develop gradually
It is easy to imagine such overuse that leadsto the sudden appearance of an injury: atorn ligament or a sprain. Such a case isclearly a work-related accident and not amusculoskeletal injury associated withrepetitive work. WMSDs develop overtime; the process evolves gradually with repeated overuse and insufficient recovery.
The process may very well set in surrepti-tiously, with no apparent symptoms, onlyto one day appear suddenly and developrapidly. More often, slight discomforts arefelt, which worsen gradually until they leadto work stoppage. The disorder can onlytake a few days to develop, but more often,it stretches out for weeks, months and evenyears.
Characteristics of WMSDs
WMSDs
WMSDs

The fact that WMSDs appear in so many dif-ferent ways creates confusion. For example,some work-related tendonitis cases arereported as industrial accidents, while others are declared occupational diseases.In fact, it is not at all obvious that these aredistinct health problems. Moreover, it canreasonably be assumed that a good numberof WMSDs do not result in any claims forwork-related injuries, perhaps because thelink with work is not always clear for victims. The official statistics could thereforeseriously underestimate the scope of theproblem
WMSD prevention can be very effective
WMSDs do not constitute a disease that canbe contracted, but a process that developsover time. The fact that WMSDs developgradually is both an advantage and a disadvantage. It is an advantage because,unlike an accident, which is, by definition,unpredictable and sudden, tendonitis andbursitis can be anticipated, since they develop gradually. Action can therefore betaken before the process gets too far. If theoveruse is stopped in time, the body can recover and the ailment can recede withoutleaving any trace. Complete recovery ispossible, and prevention can be termed effective if it occurs early.
The gradual appearance of WMSDs canalso be a disadvantage because, not beingforewarned means not being forearmedagainst symptoms that appear very gradu-ally. The body gets used to the pain, whichcan be blamed on age or other causes. It becomes a normal presence and the feelingis that the discomfort will go away. This increases the risk of the situation gettingworse, to the point where complete recovery becomes impossible.
WMSDs have multiple causes
The starting point of WMSDs is overuse.But this overload generally stems from acombination of factors and not from onesingle cause. Be it repetition, posture or effort, no single risk factor is essential inand of itself. A very demanding effort madein a particularly bad posture can suffice to create musculoskeletal problems, even if the rate of repetition is very low. Converse ly, a l ess demanding task performed in a more or less adequate posture can cause damage if it is repeatedthousands of times per day. Because of these multiple causes, prevention mustoften rely on a combination of solutionsbased on a good knowledge of the situa-tion. And because the situations can be so diverse, a universal solution is also impossible.
4 Chapter 1
WMSDsWMSDs
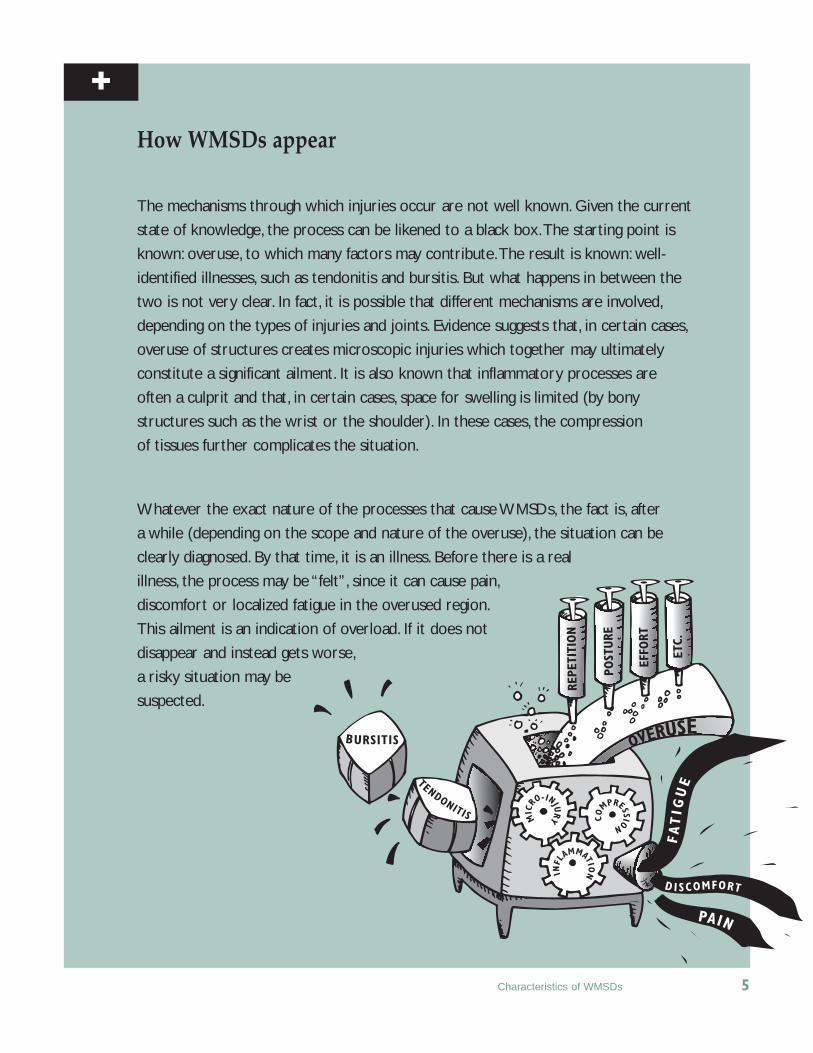
How WMSDs appear
The mechanisms through which injuries occur are not well known. Given the current
state of knowledge, the process can be likened to a black box.The starting point is
known: overuse, to which many factors may contribute.The result is known: well-
identified illnesses, such as tendonitis and bursitis. But what happens in between the
two is not very clear. In fact, it is possible that different mechanisms are involved,
depending on the types of injuries and joints. Evidence suggests that, in certain cases,
overuse of structures creates microscopic injuries which together may ultimately
constitute a significant ailment. It is also known that inflammatory processes are
often a culprit and that, in certain cases, space for swelling is limited (by bony
structures such as the wrist or the shoulder). In these cases, the compression
of tissues further complicates the situation.
Whatever the exact nature of the processes that cause WMSDs, the fact is, after
a while (depending on the scope and nature of the overuse), the situation can be
clearly diagnosed. By that time, it is an illness. Before there is a real
illness, the process may be “felt”, since it can cause pain,
discomfort or localized fatigue in the overused region.
This ailment is an indication of overload. If it does not
disappear and instead gets worse,
a risky situation may be
suspected.
Characteristics of WMSDs 5
FATIG
UE
D I SCOMFORT
PAIN
REPE
TITI
ON
POST
URE
EFFO
RT
ETC.
TENDONITIS
BURSITIS OVERUSE
MIC
RO-INJU
RY CO
MPRESSION
INFL
AMMATION
+

The different WMSDs have similarsymptoms. The overloaded region isoften painful and sensitive when
touched. Certain movements or efforts maycause pain which, in the most serious cases,is felt even when the region is at rest. Thereis very often a swelling* and sometimesnumbness. Mobility may be limited by theswelling or the pain.
The first symptoms of WMSDs :early indicators
By the time the illness is fully declared, it isalready late to intervene. By that stage, thevictim’s health has already been compro-mised and there may be permanent after-effects. Action must be taken early before thesituation reaches a critical point.
But how can workers tell when they are in arisky situation? How do they know if theyare not developing tendonitis?
Most often, when a region of the body isoverused, it will let the worker know, wellbefore the overuse generates negative conse-quences, through a feeling of localizedfatigue or discomfort. Although these mani-festations are often innocuous, they are considered early indicators of a more serious affliction.
This does not mean being alarmed at theslightest discomfort, which may occur especially when carrying out demandingand unaccustomed tasks. However, moreattention must be paid to ailments that donot disappear over time and that tend to
worsen. This may be an early signal of a situation that may degenerate into a WMSDif timely action is not taken.
Knowing how WMSDs develop fortimely intervention
It is not always easy to clearly distinguishbetween an acceptable situation and one that demands preventive action. All ailments do not lead to tendonitis. Every-body suffers, at one point or another, fromwork-related ailments, without necessarilybeing in danger. As well, people often tolerate pain by telling themselves that itwill go away, only to end up with an “itis”ailment that forces them to quit work.
Unfortunately, there is no clear and un-equivocal demarcation between an innocu-ous situation and one that will develop intoa WMSD. Judgment must be exercised,based on what is known about the onset of a typical WMSD and the risk factors present.
At the outset of the process, the discomfortis confined to an articular region. It is oftenassociated with certain movements or efforts that contribute to overuse. Such discomfort which, in the early stages, ismerely symptomatic of fatigue, disappearsrapidly and fully after work.
6 Chapter 1
How WMSDs appear
** Swelling is part of the inflammatory response. It is a protective mechanism of the body as it tries to “repair” aninjury. Inflammation allows more blood to be sent to the injured region (which consequently grows larger andswells), in order to support the healing process.
WMSDs
WMSDs

with continued exposure
with continued exposure
with continued exposure
with continued exposure
At the other extreme, by the time a WMSDis declared, pain is truly present. It hasoften, but not always, radiated to the surrounding structures, such that it is theentire elbow, shoulder or wrist that ispainful, not just a specific region. Some-times, the pain may radiate to another region (from the shoulder to the arm, forexample). Hence, by the time a WMSD isdeclared, pain is often present even in theabsence of movement or effort; it persistsoutside work and can take several weekswithout exposure before disappearing. Infact, if the ailment is serious, full recoverycannot be guaranteed. Partial healing mayvery well have after-effects. Just like with ascar, the tissues may tighten or thicken, andremain particularly vulnerable in case of future overuse.
Similarly, the development of the first innocuous stage toward a clearly definedWMSD can be established. Action must betaken when the situation starts gettingmore serious; for example:
• when the ailment gets more intense orwhen there is pain;
• when the ailment radiates from one verylimited region to a bigger and more diffuse region;
• when the discomfort is associated withincreased movement or effort (for exam-ple, at the outset, the discomfort is feltonly when pressure is applied to insert apiece. Then, the feeling sets in graduallywhen screwing or unscrewing the coverof a container. If action is delayed, anymovement of the forearm will causepain);
• when the discomfort persists longer andlonger after work and the recovery isvery slow.
Fig. 1.3
Development
of a WMSD.
How WMSDs appear 7
Fully Can have recoverable after-effects
Disappears rapidly Persists outside work,after work can disrupt sleep
Associated with certain Present even times at work at rest
Discomfort Discomfort,pain
AT THE OUTSET WMSD

There are dozens of musculoskeletalinjuries that affect the upper limbsand that may be caused by work. It
would be impossible to list them all here.They are sometimes referred to as “itis” diseases, since several of their names havethat ending. In medical parlance, “itis” is asuffix indicating an inflammation. We willtake a look at four of the best known andmost widespread, and we will identify thestructures affected more clearly.
Tendonitis
As its name indicates, tendonitis is an inflammation of a tendon. Tendons arestructures that connect muscles to the skele-ton. Figure 1.4 shows that the biceps are attached to the shoulder and the forearm bythe tendon. When this muscle contracts andshortens, it pulls on the tendon and causesthe forearm to bend.
The tendon “works” each time the muscleworks. Hence, it is when the muscle is over-burdened, for example, by considerable andrepeated effort, that the tendon may beoverused. If the tendon is injured – and theories abound that WMSDs are caused byan accumulation of microscopic injuries –the body may try to repair it. This is wheninf lammation occurs , wi th s igns ofswelling. If the overuse persists, an injuredtendon, swollen by inflammation, may beeven more vulnerable to overload. This produces tendonitis.
Fig. 1.4
Tendons are what
connect muscles
to bones
Fig. 1.5
The fine movements of
the hand are controlled
by many muscles.
Most of them are
attached to the finger
bones by long tendons.
8 Chapter 1
The most common WMSDs and structures affected
Extensor muscles of the finger
Tendon
Tendon
Tendon
Triceps
Tendon
Biceps

Tenosynovitis
Tendons could face terrible ordeals in certain circumstances if they were not pro-tected by the synovial sheath. An example iswhat happens when the hand is completelyflexed and the extensor muscles of the fingerare put to work. The tendons are pressedagainst the bones of the wrist, and the resulting friction can injure the tendon.Fortunately, the tendons that require protec-tion are shielded from excessive friction bythe synovial sheath. These sheaths serve aslubricating covers that enclose the tendon ina space where it can glide freely in a lubri-cating fluid called the synovia.
Although the tendons that are surroundedby a synovial sheath are so protected, theyare nevertheless not completely shieldedfrom overuse. If tendonitis sets in and thetendon swells, the sheath is compressed bythe swollen tendon. The sheath itself then becomes irritated and inflamed.Tenosynovitis is the simultaneousinflammation of a tendon andits surrounding synovialsheath.
Fig. 1.6
Certain tendons are
surrounded by a
synovial sheath.
Fig. 1.7
Synovial sheaths are
located around the
tendons, where they are
needed. They are found
on the wrist on the back
of the hand and virtually
everywhere inside the
hand.
The most common WMSDs and structures affected 9
Back Palm
Synovial sheath
Tendon
Muscle
Bone

Bursitis
Tendons are also found in the shoulder.Because they are located just above a bone(head of humerus), they could be injured byfriction if there was no protective mecha-nism. Indeed, there is a sac containing synovial fluid between the tendon and thebone, called the bursa. It acts as a lubricatingcushion that allows the tendon to glide onthe bone prominence without damage. Asthe name clearly suggests, bursitis is theinflammation of the bursa.
This inflammation of the bursa generallyfollows an inflammation of the tendon. Withthe swelling that accompanies tendonitis,the bursa ends up being compressedbetween two bones. The friction and compression can injure the bursa and causebursitis. The swelling of the tendon can alsosubside, while the bursa remains swollen.The swelling of the bursa can in turn compress the tendon and rekindle the tendonitis. Hence, bursitis is sometimes acomplication of shoulder tendonitis (swim-mer’s shoulder).
Fig. 1.8
Bursitis
10 Chapter 1
Rotator cuff
Tendon
Bursa
Deltoïd
The tendon is swollen,it compresses and irritates the bursa.
The swelling of the tendon has subsided,but the inflammation of the bursa persists.
Os
Tendon

Carpal tunnel syndrome
The wrist joint is made up of several carpusbones. These bones form a cavity – calledcarpal tunnel – in which many tendons,nerves and blood vessels pass. Carpal tunnel syndrome is an affliction of thenerves that get compressed, generally by theswelling of tendons passing nearby, in a limited space that constitutes the carpaltunnel. The affliction of the nerve leads tonumbness and muscle weakness. Carpaltunnel syndrome is also unique in that it ismore painful at night, when the swelling isat its peak. Victims are often awakened bythe pain.
Fig. 1.9
Carpal tunnel
The most common WMSDs and structures affected 11
Carpus bonesTendons
Mediannerve
Ligament
Ulnar nerve

What is a WMSD?WMSDs may affect the different parts of the body associatedwith movement, we will limit our examination to disordersaffecting the upper limbs.
WMSDs are a major problem with serious consequences forworkers, companies, and society in general. Experts believethat the situation could worsen with time.
WMSDs result from overuse of the musculoskeletal system.They generally develop gradually. Prevention is an effectivemeans of combating WMSDs, if action is taken early enough in the process.
Certain symptoms of WMSDs may be considered early indicators, such as fatigue or pain associated with work.Aggravation of the symptoms over time is an alarm signal that must not be overlooked.
WMSDs are sometimes called “itis” diseases.The most common WMSDs are tendonitis, tenosynovitis, bursitis andcarpal tunnel syndrome.
12 Chapter 1
SummaryChapter 1

The causes of WMSDs constitute acomplex web of inter-related factorsthat exert their influence simultane-
ously. Hence, singling them out for indi-vidual description is not an easy task.
In this chapter, we will introduce severalrisk factors that will be described later. Wewill present them one by one, so that theyare easier to grasp, but it should be under-stood that they are often intertwined.A case in point is the relationship betweenexerting force and posture. Both factors cancontribute to the onset of WMSDs and alsoinfluence each other. For instance, a givenposture determines musculoskeletal
geometry and, depending on this geometry,the structures will be more or less well-positioned to generate a given force. Hence,a more or less strong effort will have to bemade to exert the same force, according tothe posture adopted. Conversely, having tomake a more or less significant effort maylead a worker to change his or her posture.
Another example is the fact that monotonyof work is considered in certain studies asa risk factor associated with WMSDs. Yet,the monotony and boredom generated by atask are often tied to its repetitive nature,which is certainly another risk factor.
Many risk factors 13
Causes of WMSDs
Chapter 2
As we have indicated already, WMSDs have multiple causes. Repetition, which is referred to most often, is not the only factor. For the purposes of this document, wewill not look at factors related to non-professional life or individual characteristics thatmay play a role in the onset of WMSDs. We will focus our analysis on the risk factorspresent in the workplace, since they affect the vast majority of individuals, and thepurpose of this guide is prevention at the workplace.
Many risk factors

What is a risk factor?
A risk factor is a condition present in the workplace, such as therequirement of a strong force, and whose presence has been associated with the onset of a health problem.The risk factor maybe directly responsible for the appearance of a health problem,may act as a trigger or may create conditions conducive to theappearance of a problem.The presence of a risk factor does notmean that an exposed worker will automatically develop a healthproblem; it means that he will run a greater risk of developing itthan someone who is not exposed. It is therefore a matter ofprobability. Likewise, when several workers are exposed to different risk factors, all will not react the same way.The effectcaused by the risk factor depends on several conditions, includingthe workers’ individual traits and occupational history.However, it is important to understandthat, overall, the scope of the healthproblem depends on the severity of the risk factors present.
14 Chapter 2
+

The mere presence of a risk factor isnot enough to evaluate the risk. It isnot a matter of being present or not,
but a matter of degree. Generally speaking,the seriousness of a risk factor depends on three main characteristics: intensity (oramplitude), frequency and duration.
Intensity
Most of the time, the contribution of the intensity of a risk factor goes without saying: the more intense the risk factor (thegreater the effort or extreme the posture),the higher the risk. However, there aretimes when the relationship is not that obvious. For example, saying that the com-plete and forced immobility of a body segment can contribute to the risk does notmean that its opposite – uninterrupted mobility – is desirable. The relationshiphere is a more complex one, where too little can be just as harmful as too much.
Frequency
Frequency refers to the number of timesthat a risk factor is present within a giventime interval. Being exposed to vibrations
twice a day is a lower risk factor than being exposed two hundred times per day.The risk therefore increases most of thetime with the frequency*.
Duration
The third characteristic that affects the seriousness of risk factors is duration, aconcept that has several meanings. It can bethe amount of time spent in a given pos-ture within a work cycle or the duration ofthe effort made within the cycle, such as theshoulder being flexed for 45 seconds in atwo-minute cycle. The longer the time spentin the cycle, the higher the risk factor. Duration can also mean the number ofhours in a work shift when a worker is exposed to a given risk. For example, doing repetitive work for 30 minutes doesnot have the same impact as when suchwork is done for the entire shift. Durationcan also refer to a much broader scale. Itthis case, it may mean the number of years during which the worker has been exposedin his or her professional life. In all threecases, one simple principle generally standsout: risk is proportional to duration of exposure.
Fig. 2.1
These three elements are
used to characterize
most risk factors.
Three major modulators 15
Three major modulators:intensity, frequency, duration
* This statement is, however, not etched in stone. Certain risk factors do not always have a linear relationship with the danger. For example, while considerable and frequent effort can constitute a risk, this does not mean thatimmobility and absence of effort are advisable. Nevertheless, when an effort is deemed to contribute to the riskthrough its intensity and frequency, reducing the frequency will always be a step in the right direction..
Risk factor
duration,intensity,frequency
scope ofWMSD riskx =

It is not always easy to recognize a riskfactor. In scientific documents, the listcan vary according to the author. We
have selected six categories of risk factorswhich we will discuss in the followingpages.
• Awkward postures• Effort and force• Static muscular work• Exposure to certain physical aggressors• Repetition and invariability of work• Organizational factors
Awkward postures
Often, because of the characteristics of theworkplace or the methods adopted, wor-kers have to use awkward or demandingpostures. Inadequate work posture can constitute a risk factor.
How can inadequate posture be recog-nized? For each joint, there is a basic posture that creates the least amount ofconstraints. This posture is usually far fromthe limits of the joint’s range of motion; itrequires little effort to maintain and doesnot put the anatomical structures in an unfavourable position. Conversely, posturecan be inadequate for three types of reasons. It is extreme if it is near the limitsof the joint’s range of motion. Anyone canexperience some discomfort if their wrist is
fully flexed or extended. Posture can alsobe demanding if it can only be maintainedby fighting against gravity. For example,the position where the arm is kept fullystretched in front of the body (shoulderflexion) is not extreme in that it is far fromthe limits of the joint’s range of motion.However, having to fight against gravitymakes this posture particularly demanding(see static muscular work on page 25). Finally, certain postures are risky becausethe anatomical structures are placed in aposition where they cannot function effectively. For example, maintaining thearm above the shoulder makes blood flowdifficult, thereby reducing muscle capacity.Moreover, in this posture, the tendon of amuscle is jammed between two bonemasses, thus putting the muscle in a difficult position. The same applies to wristtendons that can be compressed in a limited space when the wrist is flexed.
The pa in caused by a pos ture wi l l obviously depend on how far it is from arelaxed posture (this refers to amplitude ofposture, which is about the equivalent ofintensity of posture), the frequency withwhich this posture is adopted, and its duration.
The main postures for each of the joints areshown on the following pages.
16 Chapter 2
Risk factors

Risk factors 17
Fig. 2.2
Main postures
Neck
Pronation Supination
ExtensionBending forward
Rotation Tilting sideways
Radial deviation
Flexion
Ulnar deviation
Extension
Forearm Wrists

Fig 2.2 (cont’d)
Main postures
18 Chapter 2
Shoulders Back
Extension
Adduction
Abduction
Bending sideways
Bending forward
Extension
Rotation
Flexion

What determines posture?
Given that most awkward postures are uncomfortable, why are they so frequent?The answer is that the work postureadopted depends on the entire workcontext. Workers may sometimesadopt extreme postures becausethe material is poorly located, orbecause the work surface is notadequate (Fig. 2.3 and 2.4).
Often, posture is determined by the shapeof a tool and its conditions of use. Figure2.5 shows a worker with a marked devia-tion of the wrist caused by the shape of thetool she is using. This tool is not adaptedto work on a horizontal surface at thisheight. An awkward posture can also resultfrom access to the product. The workerhas no other choice but to adopt anawkward posture, given the shapeand location of the product.
Fig. 2.3
Placing the reflectors
behind the worker
creates a demanding
posture
Fig. 2.4
The worker has to lean
forward considerably to
reach the boxes because
the conveyor is too low.
Fig. 2.5
The shape of the tool is
not adapted for the work.
Its use leads to ulnar
deviation of the wrist
Risk factors 19
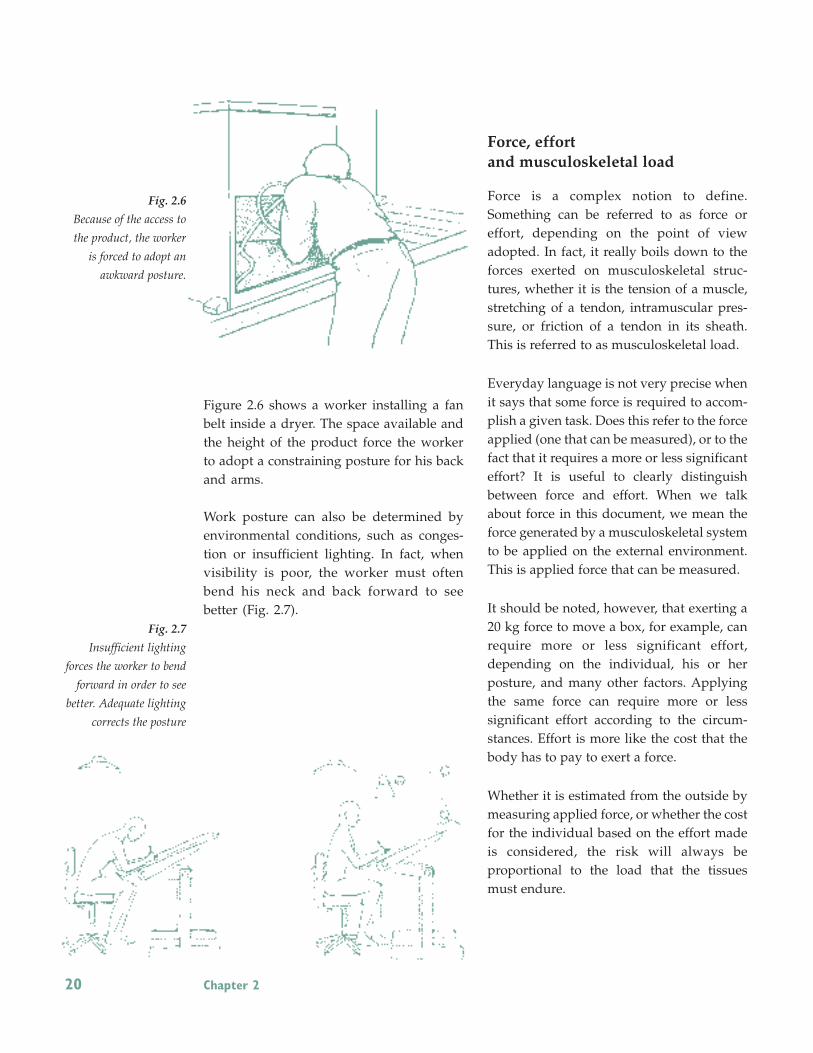
Figure 2.6 shows a worker installing a fanbelt inside a dryer. The space available andthe height of the product force the workerto adopt a constraining posture for his backand arms.
Work posture can also be determined byenvironmental conditions, such as conges-tion or insufficient lighting. In fact, whenvisibility is poor, the worker must oftenbend his neck and back forward to see better (Fig. 2.7).
Force, effort and musculoskeletal load
Force is a complex notion to define.Something can be referred to as force oreffort, depending on the point of viewadopted. In fact, it really boils down to theforces exerted on musculoskeletal struc-tures, whether it is the tension of a muscle,stretching of a tendon, intramuscular pres-sure, or friction of a tendon in its sheath.This is referred to as musculoskeletal load.
Everyday language is not very precise whenit says that some force is required to accom-plish a given task. Does this refer to the forceapplied (one that can be measured), or to thefact that it requires a more or less significanteffort? It is useful to clearly distinguishbetween force and effort. When we talkabout force in this document, we mean theforce generated by a musculoskeletal systemto be applied on the external environment.This is applied force that can be measured.
It should be noted, however, that exerting a20 kg force to move a box, for example, canrequire more or less significant effort,depending on the individual, his or her posture, and many other factors. Applyingthe same force can require more or less significant effort according to the circum-stances. Effort is more like the cost that thebody has to pay to exert a force.
Whether it is estimated from the outside bymeasuring applied force, or whether the costfor the individual based on the effort madeis considered, the risk will always be proportional to the load that the tissuesmust endure.
Fig. 2.6
Because of the access to
the product, the worker
is forced to adopt an
awkward posture.
Fig. 2.7
Insufficient lighting
forces the worker to bend
forward in order to see
better. Adequate lighting
corrects the posture
20 Chapter 2

Characteristics of work requiring force
The word “force” immediately conjures images of the handling of heavy objects. It is, of course, a situation that requires considerable effort, but there are manyother situations that require the use offorce. For example, when using manualtools, it is often necessary to make an effort,if only to support the tool. Often, pneu-matic tools are not suspended, and the retaining system is poorly adjusted. In thesecases, the worker must support some of theload of the tool when handling the object.
Force may also be exerted when workingwith a tool on a product, such as whenbending an object with pliers. Using apneumatic or electric screwdriver requireseffort by the forearm to immobilize the tooland to apply pressure on the head of thescrew. A poorly adjusted tool with inade-quate torque, for example, can also requireadditional effort.
Assembling pieces, even without a tool, canmean exerting force. If the basic materialsare of uneven quality, if the product doesnot fully comply with specifications, thepieces may not fit together properly, forcing the worker to apply considerableforce. In the example in figure 2.8, theworker has to attach a reflector to a deflec-tor. This operation is painful and demandsconsiderable effort. The situation is madeworse by the fac t tha t the work i s performed in a less-than-optimal posture.
Finally, force may be exerted when activa-ting the command to lower a lever or to activate a pedal, for example.
Factors affecting intensity of effort
The effort required to generate externalforce or, as we have defined it, the cost for the body to exert force, depends on sixfactors: intensity of force required, joint involved, direction of effort, grip, postureused, and individual traits. Let us examinethe effects of these different factors.
Intensity of force requiredThis relationship is fairly obvious: thegreater the force requirements, the greaterthe effort to be made. The efforts made are directly proportional to the force that should be applied. A greater effort isrequired to move a 50 kg container than a10 kg container. The physiological cost willtherefore vary accordingly.
Fig. 2.8
To attach the reflector to
the deflector, the worker
must make a significant
effort.
Risk factors 21
Joint involvedForce is easier or harder to generate, depending on the group of muscles used. Ifmajor muscles such as those of the lower
limbs are used, or if the weight of the bodycan be used, it would be easier to apply a given force because these muscles arepowerful. However, if the force is to be generated by smaller muscles such as thoseof the hand, the effort required would begreater. For this reason, even if the forcesapplied are not particularly significant,there may still be a considerable risk if theeffort is made by small muscles. An exam-ple would be assembling small parts or con-necting terminals using the finger tips.
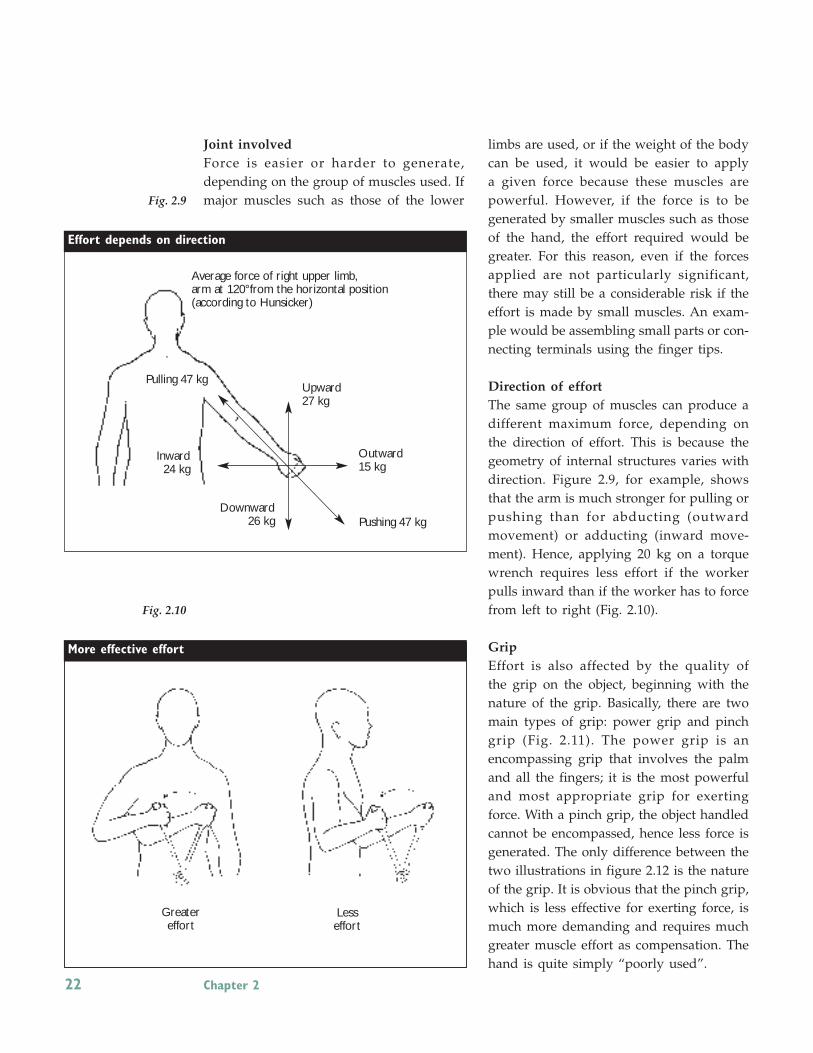
Direction of effortThe same group of muscles can produce adifferent maximum force, depending on the direction of effort. This is because thegeometry of internal structures varies withdirection. Figure 2.9, for example, showsthat the arm is much stronger for pulling orpushing than for abducting (outwardmovement) or adducting (inward move-ment). Hence, applying 20 kg on a torquewrench requires less effort if the workerpulls inward than if the worker has to forcefrom left to right (Fig. 2.10).
GripEffort is also affected by the quality of the grip on the object, beginning with thenature of the grip. Basically, there are twomain types of grip: power grip and pinchgrip (Fig. 2.11). The power grip is an encompassing grip that involves the palmand all the fingers; it is the most powerfuland most appropriate grip for exertingforce. With a pinch grip, the object handledcannot be encompassed, hence less force isgenerated. The only difference between thetwo illustrations in figure 2.12 is the natureof the grip. It is obvious that the pinch grip,which is less effective for exerting force, ismuch more demanding and requires muchgreater muscle effort as compensation. Thehand is quite simply “poorly used”.
Fig. 2.9
Fig. 2.10
22 Chapter 2
Pulling 47 kgUpward27 kg
Outward15 kg
Inward 24 kg
Downward26 kg Pushing 47 kg
Effort depends on direction
Average force of right upper limb,arm at 120°from the horizontal position (according to Hunsicker)
More effective effort
Greater effort
Less effort

The existence of handles reduces the effortconsiderably by allowing the worker to usea power grip.
A similar situation occurs each time aworker uses a pinch grip to exert force. Thishappens, for example, when wires have tobe connected by inserting a terminal onto ametal connector (Fig. 2.13). Depending on the compatibility of the two pieces, theinsertion effort can be considerable, albeitonly in relative terms, since it is a pinchingeffort using the finger tips.
More generally, the quality of the gripshould also be considered. The grip of theobject to be held or on which a force is applied can be too small or too big. Theseare circumstances that would add to the effort. Wearing gloves can also increase the grip effort to compensate for a loss inadherence. The effort generated is also affected by other factors related to the object handled. For instance, a greater effortis required to handle an object with a slippery surface or an awkward shape thatmakes it difficult to grip properly.
Fig. 2.11
Fig. 2.12
Fig. 2.13
This worker uses a pinch
grip to connect wires.
Risk factors 23
Effort depends on grip
Pinch Power
Grips
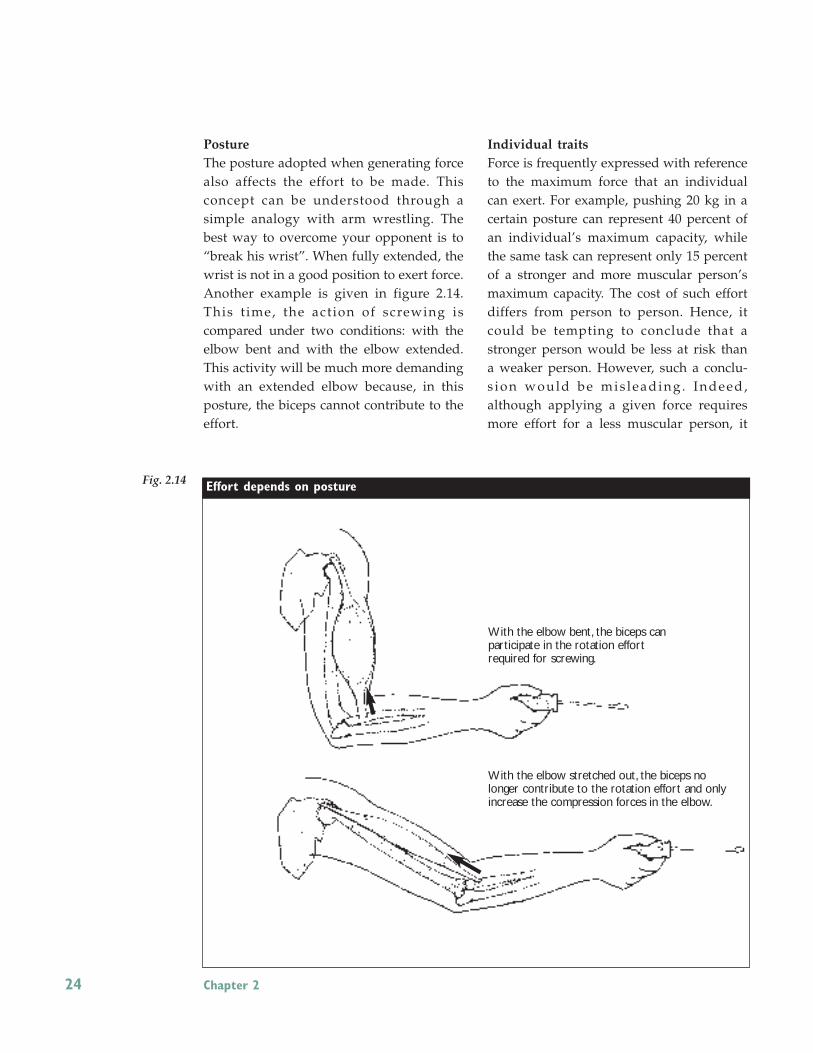
PostureThe posture adopted when generating forcealso affects the effort to be made. This concept can be understood through a simple analogy with arm wrestling. Thebest way to overcome your opponent is to“break his wrist”. When fully extended, thewrist is not in a good position to exert force.Another example is given in figure 2.14.This t ime, the action of screwing is compared under two conditions: with theelbow bent and with the elbow extended.This activity will be much more demandingwith an extended elbow because, in thisposture, the biceps cannot contribute to theeffort.
Individual traitsForce is frequently expressed with referenceto the maximum force that an individualcan exert. For example, pushing 20 kg in acertain posture can represent 40 percent ofan individual’s maximum capacity, whilethe same task can represent only 15 percentof a stronger and more muscular person’smaximum capacity. The cost of such effortdiffers from person to person. Hence, itcould be tempting to conclude that astronger person would be less at risk thana weaker person. However, such a conclu-s ion would be mis leading . Indeed, although applying a given force requiresmore effort for a less muscular person, it
Fig. 2.14
24 Chapter 2
Effort depends on posture
With the elbow bent, the biceps can participate in the rotation effort required for screwing.
With the elbow stretched out, the biceps nolonger contribute to the rotation effort and onlyincrease the compression forces in the elbow.

does not follow automatically that such aperson faces a higher risk. Risk depends ona multitude of factors, including variouspersonal traits, such that the same personwith less muscular capacity would perhapsbe more resistant than a more muscularperson. In conclusion, it can be stated thatrisk varies from person to person, due tointerpersonal differences. In addition, theeffort associated with a given force will depend on individual characteristics.
Static muscular work
As was stated earlier, a risk exists when alimb has to be kept in position by fightingagainst gravity, when the musculoskeletalstructures must support the weight of alimb. This is the case, for example, whenworking with the arms above the shoul-ders. Such a situation is described as staticmuscular work. The intensity of the risk depends on the amplitude and duration of the posture. The longer the posture ismaintained, the higher the risk.
Static muscular work involves keeping themuscles contracted without interruption. Itis the opposite of dynamic muscular work,which refers to an alternation between contraction and relaxation. There are numerous examples of static work in industries as well as in offices. A case inpoint is a person who works with a videodisplay terminal (VDT) and who remainsstationary, the neck bent forward and thehands maintained in radial deviation abovethe keyboard. Also, due to poor design, anoperator may be forced to work with thearms above the shoulders (Fig. 2.15). Sucha posture cannot be maintained for long
without causing significant muscle fatigue.Figure 2.16 shows a worker carefullyputting pieces in a basket. To do this, hisback has to be extremely flexed for a fairlylong time; this static load requires great effort by the back muscles.
If the posture is maintained for a long time,the risk can be considerable, even if the amplitude of the posture is not extreme.
Fig. 2.15
Static effort with the
arms above the shoulder
is particularly painful.
Fig. 2.16
This task causes the back
to lean forward
Risk factors 25

Static work is identified as a risk factor forWMSDs because it can reduce the supply ofblood to the muscles, which rapidly leadsto muscle fatigue.
As figure 2.17 shows, to function normally,the muscles need adequate blood supply. It is the blood that provides the muscleswith oxygen and glucose, its main source ofenergy. It is also the blood that evacuatescombustion waste (carbon dioxide).
The muscle requires more blood when it isworking than when it is resting. In the caseof dynamic effort, when there is alternationbetween contraction and relaxation of themuscle, the active muscle needs more fuel.It is relatively easy to increase the bloodflow, since the contraction and relaxation alternation facilitates circulation. The muscle then receives sufficient blood supply.
The situation is different during static effort. In this case, the muscle contraction is sustained and there is no alternation between contraction and relaxation. Sincethe muscle is working harder, it needs moreenergy. But, during contraction, the pressure inside the muscle increases,thereby compressing the blood vessels,which impedes the entrance of new blood.Indeed, it is more difficult to push bloodinto a contracted muscle. If the contractionis strong enough, the entrance of bloodcould be blocked completely. Whether theentrance of blood is blocked partially orcompletely, the muscle must still work inunfavourable conditions where fatigue setsin much more rapidly.
Compression inside the muscle is related tothe intensity of effort required to maintaina posture. The more extreme the posture,the stronger the contraction and the lowerthe blood supply to the muscle.
Likewise, if force has to be exerted or a loadhas to be carried with static work, the scopeof the load will increase the pain related tothe work proportionately.
Fig. 2.17
Static Muscular Work
26 Chapter 2
Dynamic effort
Static effort
At rest
Amount of bloodneeded
Real blood flow
Alternation betweencontraction andrelaxation
Static effort is oftenpresent when fighting
against gravity
Amount of bloodneeded
Real blood flow
Amount of bloodneeded
Real blood flow

Risk factors 27
+
Is my work repetitive?
This is a question that you have probably been asking yourself for some time now, without
getting a definitive answer. If only someone could define exactly what is meant by repetitive
work! If someone could give a clear definition to help distinguish between repetitive and
non-repetitive work! Despite our desire to please the reader, such an answer does not
exist.There is no clear boundary between the two concepts. It is generally agreed that the
problem revolves around the cyclical use of the same tissues.
In fact, talking about repetitive work can be misleading, because repetition is only one of
the risk factors for “itis” diseases. Repetitiveness is a matter of degree; it is not something
that is present or absent. Even though it has already been suggested, for the purposes of a
specific study, that work be considered repetitive if its cycle is less than 30 seconds or if it
represents a repetition of the same actions during half of the work time, this in no way
constitutes an absolute reference or a safety criterion. It is easy to imagine work that does
not meet this definition but constitutes a major WMSD risk, due to the posture or effort
required. Conversely, the fact that the cycle is less than 30 seconds does not necessarily
mean that a danger is imminent.
The label repetitive work can also mask the real problem by shifting the focus to just the
issue of repetitiveness. It is thought that the problems are caused by the repetitive nature
of the task and that the only possible solution is to reduce the
repetition, something that can be very difficult to accomplish.
In the mean time, no thought is given to improving
postures or reducing effort.
Instead of trying to prove whether a work
process is “repetitive” or not, it is
preferable to identify all the risk
factors present.This means deter-
mining the extent to which the work
is repetitive, along with other factors,
in order to obtain a much clearer
picture of the risk.

28 Chapter 2
Repetition and invariability of work
While repetition is itself a risk factor, it isalso a modulator for the other risk factors.In this regard, repetition creates a multipliereffect. Invariability of work refers to an activity that remains relatively unchangedover time; hence this concept is closely associated with repetition. In both cases, therisk increases when the same muscu-loskeletal structures are solicited all thetime. However, considering the task fromthe standpoint of invariability shows theimportance of the moments, during
the work process, when the structurescan recover. Monotonous tasks,
where the worker remains stationary because of the
requirements, seem topresent a higher riskof WMSD.
Exposure to certain physical aggressors
Certain environmental features can alsocontribute to the risk of WMSDs. For example, exposure to cold, vibrations, impacts and mechanical pressures has beenassociated with WMSDs.
Mechanical pressures
Mechanical pressures occur when the softtissues of the body are “crushed” by directcontact with a hard object present in the work environment. The skin and underlying structures such as nerves, tendons and blood vessels can be injuredby this direct pressure. The hands are mostoften exposed to mechanical pressureswhen handling tools or products. If the objects have sharp edges, or if a handle hasright angles, the palm, the base of thethumb or the fingers can be subjected tostrong local pressures. Figure 2.18 showshow using pliers can compress a tendon atthe base of the thumb. Another scenario iswhere scissors can compress the nervesrunning along the sides of the fingers.
Other regions of the body can be subjectedto local pressures when using hard surfacesor unpadded surfaces for support duringwork. This happens with the wrists, forearms, elbows and knees.
The effects of mechanical pressures obviously depend, like most other risk factors, on the frequency, duration and intensity of the pressure. The latter factor isin turn often associated with intensity of effort. Indeed, everyone has a good idea ofthe difference that may exist between cutting a thin fabric with scissors and cutting a thick fabric. The pressures exertedon the fingers become uncomfortable veryquickly as the force required for cutting increases.
Fig. 2.18
A poorly designed
grip can compress
the tendons at the base
of the thumb

Risk factors 29
Shocks and impactsIt has been shown that using the hand as astriking tool can increase the risk of certainvascular disorders in the hand. Figure 2.19shows a worker trying to hammer a partinto place with his hand. The danger obviously increases with repetition.
Tissues are generally subjected to a tremen-dous ordeal when holding a tool that generates a sudden and intense jolt. This isprobably what happens when using a percussion tool or when turning a screwwith a pneumatic or electric tool. Unless thedevice has a clutch, the screw driver tendsto continue turning after the screw hasstopped. It is the forearm muscles and tendons that feel the effect. The risk also increases because a greater effort is gene-rally required to properly hold a tool thatgenerates jolts.
VibrationsIt is generally when handling electric orpneumatic tools that workers are exposedto the type of vibrations that constitute aWMSD risk for the upper limbs. Thestronger the grip, the better the transmis-sion of vibration to the hand and forearm.Exposure to vibrations can contribute to theonset of vascular disorders such as whitefingers syndrome, neurological problemssuch as carpal tunnel syndrome, andjoint disorders of the wrist , elbow and shoulder, such as osteoarthritis. It also adds tothe musculoskeletal load, because the tendons sufferthe effects of v ibrat ions directly, not to mention thefact that a vibrating tool oftenneeds to be held with greaterforce.
Certain efforts to counter the effect of vibrations can sometimes add to the problem. An example is wearing certaintypes of gloves covered with absorbent materials. The goal is to absorb the vibrations before they reach the hand, butthe tool often has to be held tighter to keepit in position, thereby increasing the muscular effort and facilitating the trans-mission of vibrations. Coverings can also beused on tool handles to limit the trans-mission of vibrations. However, the advan-tage is less clear if the handle is so big thatit is difficult to grip.
Fig. 2.19
Using the hand
as a hammer
Fig. 2.20
Shocks and vibrations
are very hard on
the tendons

Fig. 2.21
Work organization
is also a source
of risk factors
S TAT E O F L A B O U R R E L AT I O N S
PA C E
M E T H O D O F R E M U N E R AT I O N
T Y P E O F S U P E R V I S I O N
WO R K I N G A L O N E
W O R K I N G I N A T E A M
WO R K C L I M AT E
Q U A L I T Y O F I N T E R P E R S O N A L
R E L AT I O N S
WO R K S C H E D U L E
30 Chapter 2
ColdCold is also a risk factor that can contributeto the development of WMSDs. It can actdirectly by increasing the musculoskeletalload on the upper limbs. It is well knownthat cold reduces the dexterity and strengthof the hands for manual work; doing thesame work is therefore more demandingunder cold conditions. It is difficult to distinguish this direct effect of cold fromthe effect of wearing gloves because of thecold. Indeed, gloves can reduce the gripforce and impede the transmission of tactileinformation, which forces the worker totighten his grip even more – often morethan necessary – in order to hold a tool oran object. It has also been observed thatmuscular tension rises around the shoul-ders among workers exposed to a currentof fresh air on the shoulders, no doubt dueto the stooped posture they adopt instinc-tively to protect themselves in such circumstances.
Organizational factorsWork organization encompasses another setof factors that determine the risk of work-related injuries. It refers to all the determi-nants of the terms and conditions of a work
process. Organizational factors can them-selves be risk factors for WMSDs, but theyare also very important because theylargely determine the other risk factors wehave already mentioned.
Risk factors related to work organizationhave a complex effect on the risk of WMSDand one that is not always easy to identifyclearly. It is reasonable to assume that organizing work around autonomous unitsrather than on an assembly line would haveall sorts of consequences on working conditions, and hence on the postures andmethods adopted at each work station. Indeed, work organization largely deter-mines the intensity of the other risk factorssuch as posture, effort and repetition. As aresult, the type of work schedule, workingalone or in a team, method of remunera-tion, type of supervision, and the state oflabour relations are all parameters that canaffect the risk of WMSDs at one point oranother. Simply changing supplier for agiven component can lead to an increase inthe effort required for its installation.
The effect of work organization on the riskof WMSD is not only due to the fact thatorganization ultimately determines the conditions for executing a particular task.Work pace, especially if it is imposed,method of remuneration, work climate andquality of interpersonal relations can alsoaffect the risk of WMSD by generating moreor less stress. Stress is both a physiologicaland a psychological state. When working ina tense or stressful environment, there is anincrease in muscular tension that can contribute directly to musculoskeletal load.In addition, behaviour can be changed, forexample, by adopting a different workmethod to meet increased production requirements, perhaps at the expense ofsafety or comfort.

Risk factors 31
It is impossible here to present all the characteristics of work organization thatcan have an impact on the risk of WMSD,either by generating stress or by influen-cing the scope of other risk factors. We willnevertheless present a few that merit discussion.
Work load and work paceWork load is a risk factor when the amountof work requested is too heavy. Speed of execution, intensity of effort and lack of recovery time are generally associated withan extremely heavy work load. In addition,when the pace is imposed by a machine,workers usually cannot adjust their pace ofwork throughout the work day or week according to their state or level of fatigue.It is recognized that a work pace controlledby external factors is more constrainingthan one that is not imposed. Apart fromthe risk factors that are often present whena pace is imposed, such as a heavy workload, a high rate of repetitiveness andstrong psychological pressure, workerscharacteristically have little decision-making leeway. Yet, the lack of control thatworkers have over their work has a significant impact on the tension that theycan feel and is considered a major factor forthe onset of WMSDs.
Work pace is obviously affected by otherfactors associated with work organization,such as method of remuneration. For example, piecework pay and other forms of
performance-based salaries lead workers to push themselves to the limits of theirphysical capacity. It has been observed insewing shops that sewing machine opera-tors paid for performance suffer fromWMSDs nine times more than those paidby the hour*.
Work schedulesWork schedules can affect the level of riskof WMSDs because they can extend the duration of the work day, which constitutesan increase in work load. Schedules alsorepresent a stress factor (night shifts, for example), which can shorten the periods ofrest needed for recovery.
When the amount of work accomplished issignificant, the musculoskeletal load stemsnot just from the sustained work process,but also from the absence or reduction ofrecovery time. Breaks during the shift arevery important to allow the muscles to restbetween work periods. For example, three10-minute breaks may be more effective, in terms of recovery, than a work day shortened by 30 minutes.
Overtime and 12-hour shifts affect the mus-culoskeletal load by extending the workprocess and exposure to risk factors alreadypresent in the workplace. In these cases, therest period is also reduced. Finally, shiftwork also increases the general level offatigue and stress.
* Vézina, M., Vinet, A., Brisson, C. « Le vieillissement prématuré associé à la rémunération au rendementdans l’industrie du vêtement », Travail humain, vol. 52, n0 3, 1989, p.202-212.

32 Chapter 2
Technological changesIt is difficult to predict all the consequencesof the technological choices made today.New technologies sometimes create newproblems concerning the musculoskeletalload. Who could have predicted 10 yearsago that working in front of a computerscreen would cause such an epidemic ofmusculoskeletal problems? It seemed mucheasier to use a computer keyboard than theold typing machines. Few people had anticipated that the nature of the taskwould change and that new problemswould emerge. It is therefore crucial toremain alert with regard to the impact ofnew technologies.
Any time there is a major change in production method, the possible impacts onwork processes should be analyzed. Willworkers have to acquire new skills? Willwork be easier or more demanding? Whatwould be the impact on work postures, onefforts to be made, and on work pace?
Social environmentThe social environment can be a majorsource of motivation, but also a source ofconcern and stress.
The climate can contribute even more directly to the risk of WMSD if it preventsthe expression of musculoskeletal problemsexperienced when executing a task. In anenvironment where workers can feelblamed or accused if they complain aboutdiscomfort or pain, they may tend to waituntil the last minute to report a muscu-loskeletal problem. The consequences thenare more serious. An environment that fosters expression and communication willalso benefit from the workers’ expertise inimplementing a continuous improvementprocess for work situations.
Summary 33
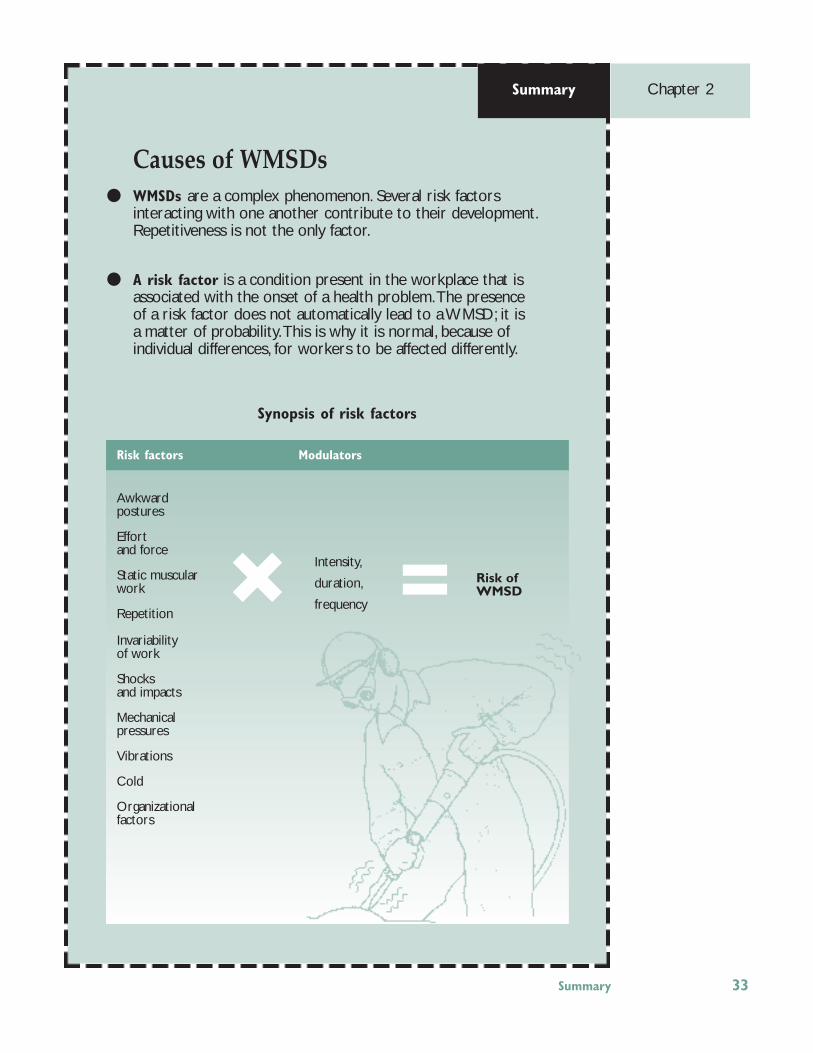
Causes of WMSDsWMSDs are a complex phenomenon. Several risk factors interacting with one another contribute to their development.Repetitiveness is not the only factor.
A risk factor is a condition present in the workplace that isassociated with the onset of a health problem.The presenceof a risk factor does not automatically lead to a WMSD; it is a matter of probability.This is why it is normal, because ofindividual differences, for workers to be affected differently.
Synopsis of risk factors
Summary Chapter 2
Risk factors Modulators
Awkward postures
Effort and force
Static muscular work
Repetition
Invariability of work
Shocks and impacts
Mechanical pressures
Vibrations
Cold
Organizational factors
Intensity,
duration,
frequency
Risk ofWMSD=✖

It is certainly very useful to know what WMSDs are, as well as their possible risk factors. However, this knowledge must be applied concretely when answering the following question: does the problem exist at our facility, in this plant, or in this department? Before taking action, and in order to determine the amount of resourcesto be devoted to the issue, it is essential to understand the scope of the problem inthe workplace.This can be achieved through a set of measures designed to documentthe existence of an occupational health problem. These measures constitute what isknown as monitoring.
Monitoring: two possible targets 35
How to detect a WMSD problem
Chapter 3
Monitoring: two possible targets
The data on the problem are nowknown: certain working conditionshave been identified as risk factors,
namely, effort, posture, repetition, etc. Thepresence of these risk factors can lead to thedevelopment of WMSDs, preceded by signssuch as pain, discomfort and localized fatigue. In short, certain working conditionshave an effect on health. To evaluate thepresence of this problem in a workplace,two options are worth exploring: evalua-tion of the health status of the exposed population, and evaluation of the risk factors.
Health monitoring
Health monitoring is certainly very effec-tive in detecting WMSD problems. There is,indeed, no better proof of the existence ofa problem that to observe its effects. Thedata most frequently used in this regard arethose related to CSST claims, but they arenot the only ones that can be consulted.
Most WMSDs do not really stem from anaccident, yet when reported, they are oftencounted as work-related accidents. It is important, therefore, to analyze accident

data in order to detect musculoskeletal disorders that affect the upper limbs, in addition to any possible “itis” injuries thathave been reported as occupational diseases. Obviously, the number of WMSDsoccurring during a given period can becounted and compared against the totalnumber of accidents and diseases occurringduring the same period. This gives the proportion of WMSDs in relation to total injuries. Yet, it is still more useful to evalu-ate the number of days lost due to WMSDs,which gives a better indication of the contribution of WMSDs to workmen’s compensation. Indeed, WMSDs often account for a low proportion of accidents asopposed to cuts and contusions. However,when the duration of absences and the proportion of the costs incurred are takeninto account, WMSDs figure more promi-nently most of the time.
It should be noted, though, that WMSDsthat are compensated are often only the tipof the iceberg. The impact of WMSDs is notonly felt on claims for work-related injuries,but also on general absenteeism. Hence, anumber of WMSDs are not reported as work-related accidents, resulting in a relatively large number of absences beingrecorded by the company’s health insur-ance plan.
This raises the question as to whethersomeone who has to undergo wrist surgeryis a victim of a WMSD even though the linkwith work has not been established. Theeffect of the “tip of the iceberg” can also beseen in the fact that , for every one person who is the victim of a recognizedWMSD, there are many others who haveless serious symptoms that can neverthelesslead to an absence.
Finally, workers sometimes complain aboutfeeling pain or discomfort that they associ-ate with their work. In certain companies,these complaints and episodes of discom-fort are noted. This is another indicator thatcan shed some light on the problems thatproduce WMSDs.
The data that we have referred to so far(statistics on accidents, absenteeism, complaints) are those usually found in companies and that generally suffice to establish that there is a WMSD problem. Ifthe data are non-existent, it is important toestablish measures through which they canbe collected.
Nevertheless, it is possible to go further, ifnecessary. One method frequently used is apain questionnaire. These are fairly simplequestionnaires with diagrams of the human
Fig. 3.1
36 Chapter 3
STATICWORK
COLD
VIBRATION
POSTURE
EFFORT
REPETITION
ETC.
The presence of risk factors can be evaluated. The health of the exposed population can be evaluated.
CAUSES EFFECTS
MONITORING OF RISK FACTORS HEALTH MONITORING

Fig. 3.2
Body chart
Monitoring: two possible targets 37
body on which workers indicate the regionswhere they feel pain (Fig. 3.2). The ques-tionnaires are used to gather informationbefore people even feel obliged to reporttheir discomfort. It is also possible to obtainindications on the seriousness of the ailments: intensity and frequency, conse-quences on work life and leisure, taking ofmedication, absence from work, etc.
Another possibility is medical screening,notably by clinical examinations to show reduced force of grip or limitations in amplitude of movement. Obviously, thesemeasures usually require help from specialists or health professionals.
Monitoring of risk factors
To establish the existence of a WMSD problem, it is also important to evaluate theworking conditions in order to documentthe presence of risk factors that are knowncauses of WMSDs. There too, the processmay begin by consulting the existing data.But, most often, companies do not have direct data on the presence of risk factors atthe workplace. The situation gets furthercomplicated because certain risk factors areso “normal” that their presence alone is nolonger considered proof of the existence ofa risk. Merely noting that work cycles areless than 15 seconds does not always seemto be sufficient to establish the WMSD risk.The comparison between different workstations is sometimes more “eloquent”. Inthis regard, workers’ complaints about theirwork are often good indicators. If they report that a work station is “too hard onthe shoulder”, they are no doubt reporting,in their own words, that WMSD risk factorsare present.
Likewise, a high rate of employee turnoverat a given station or average seniority below that of the rest of the plant are oftenpain indicators. This may be associatedwith other r isk factors unrelated toWMSDs, but the question clearly deservesto be studied.
Additional information on risk factors canalso be sought more actively, if the availabledata are not sufficient. This could beachieved by carrying out inspections usingevaluation grids or check lists, keepingrecords of the various stations, and conducting analyses. However, these tasksare not always easy and it is often profitableto have them performed by an ergonomist.
Neck,napeShoulders
Upper back
Lower backHands,wrists
Thighs,hips
Elbows
Ankles,feet
Knees

38 Chapter 3
The first t ime that the question of monitoring arises is when tryingto determine whether the situation
requires intervention or when documentingthe need to take action. But monitoring is always useful and should be part of aregular prevention program. It helps keeptrack of the situation and evaluate the impact of measures taken. Once certaindata have been identified as constituting avalid indicator of the
situation, such as statistics on accidents, thenumber of complaints or force require-ments, attention can then shift to how theseindicators evolve over time. Effective preventive actions will help improve theseindicators. It should be noted, of course,that just as WMSDs develop gradually, preventive actions can also take time to produce concrete results.
Monitoring to evaluate the efficacy of an action
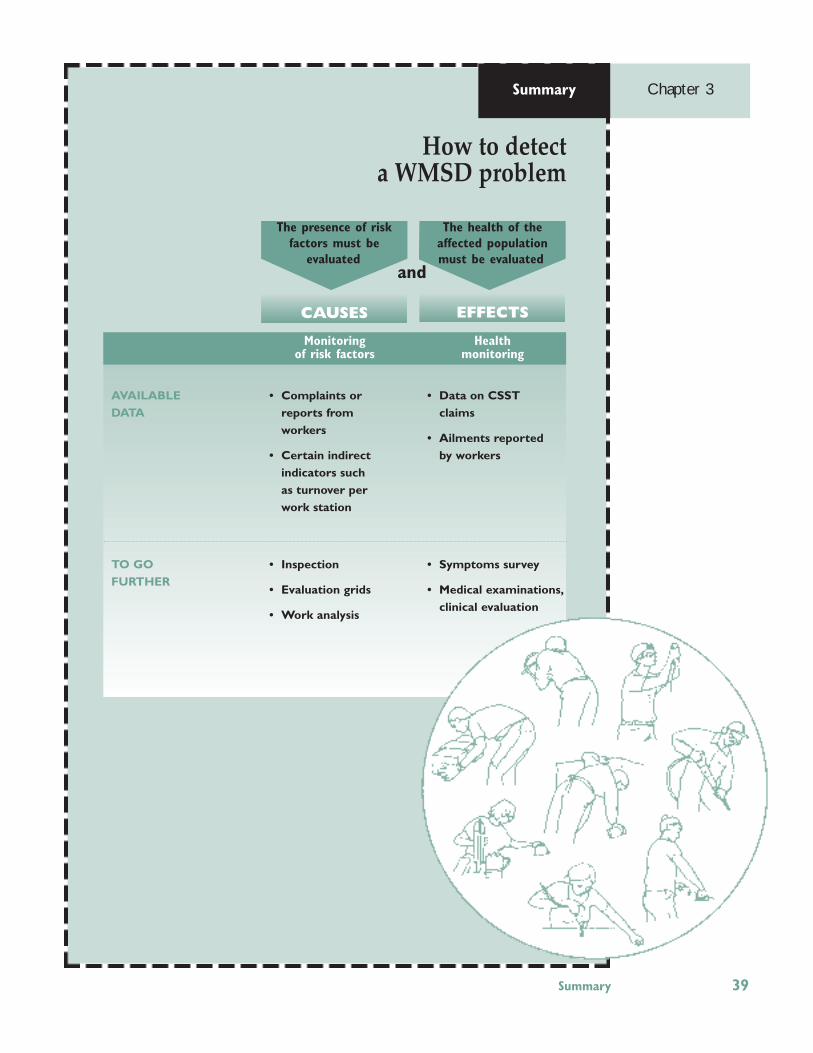
How to detect a WMSD problem
Summary Chapter 3
AVAILABLEDATA
TO GO FURTHER
• Complaints or reports from workers
• Certain indirect indicators such as turnover per work station
• Inspection
• Evaluation grids
• Work analysis
• Data on CSST claims
• Ailments reported by workers
• Symptoms survey
• Medical examinations,clinical evaluation
Monitoring of risk factors
Health monitoring
CAUSES EFFECTS
The health of the affected population must be evaluated
The presence of risk factors must be
evaluated and
Summary 39

Once the presence of a WMSD problem has been confirmed and recorded, the nextstep is to take action. But what measures should be implemented? Various preventionoptions can be considered and some are more effective than others. Here is anoverview.
A comprehensive approach 41
How to handle WMSDs
Chapter 4
A comprehensive approach
Whatever the prevention methodsconsidered to fight WMSDs, theissue should be addressed
comprehensively. As we saw previously,W M S D s a re a c o m p l i c a t e d , m u l t i -dimensional problem. Given the complexityof this issue, an effective strategy shouldalso involve concerted actions at variouslevels. While work station adaptation is thebackbone of a prevention-at-source strategy,the value of a training program or the monitoring of injured workers cannot beoverlooked.
The comprehensive approach is also essen-tial in reducing risk factors by improvingwork stations. The workplace can be seenas a system with five main components: the individual, technical work aspects,
work organization, job characteristics andphysical and social environment (Fig. 4.1).At the heart of the system is the individualor worker, with his physical or psycholo-gical features, who is affected by the four other components of the system. Theinteraction between the worker, with hisparticular traits, and these components constitutes the work process, namely a specific set of gestures and actions involvedin performing the work.
First of all, the technology used largely determines the knowledge required by theworker, as well as the work methods to beused. General work organization also has adirect impact on the individual, the workstation and the conditions of work perfor-mance. Organization determines the
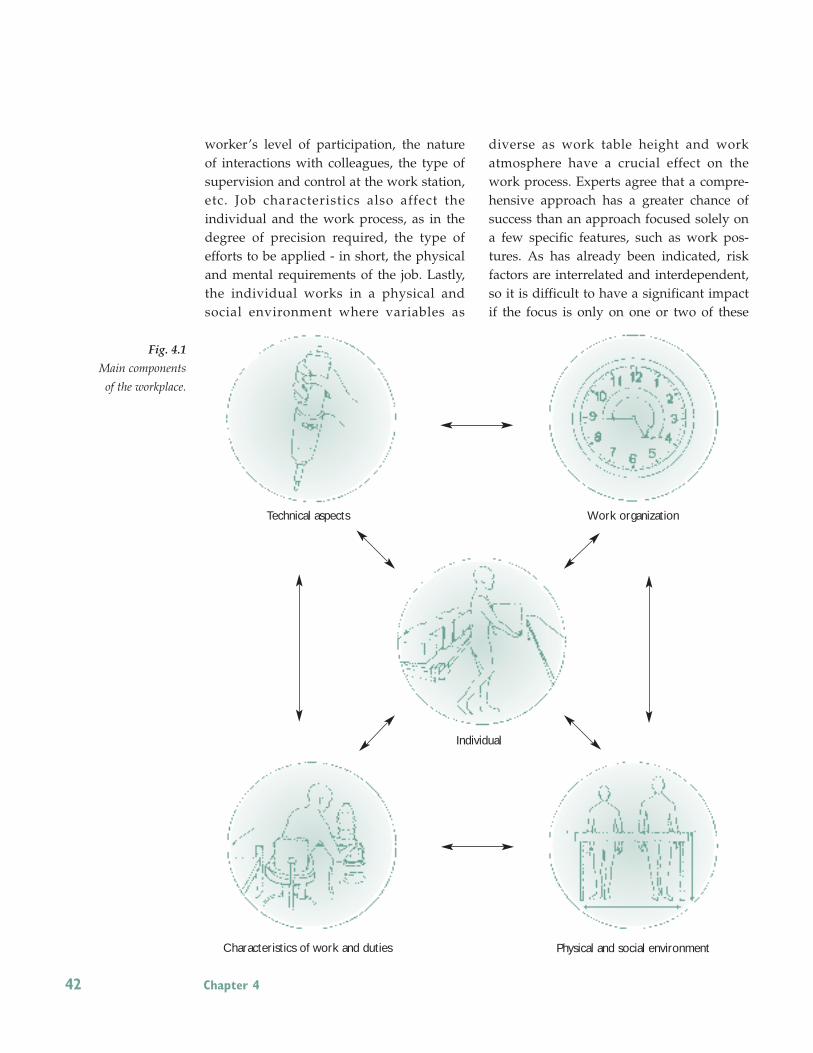
worker’s level of participation, the natureof interactions with colleagues, the type ofsupervision and control at the work station,etc. Job characteristics also affect the individual and the work process, as in thedegree of precision required, the type of efforts to be applied - in short, the physicaland mental requirements of the job. Lastly,the individual works in a physical and social environment where variables as
diverse as work table height and work atmosphere have a crucial effect on thework process. Experts agree that a compre-hensive approach has a greater chance ofsuccess than an approach focused solely ona few specific features, such as work pos-tures. As has already been indicated, riskfactors are interrelated and interdependent,so it is difficult to have a significant impactif the focus is only on one or two of these
Fig. 4.1
Main components
of the workplace.
42 Chapter 4
Technical aspects Work organization
Individual
Characteristics of work and duties Physical and social environment

Several possible options 43
factors in isolation. Risk factors must bedealt with as a whole. Hence, to solve anergonomic problem, the intervention musttake into account the five main componentsof the work system: the individual with his special traits, work organization, job design, the technology used and the physical and social environment. Work improvement is contingent upon a betterbalance of these main components of thework system. The preventive approachmust also be comprehensive because actionneeds to be taken in a complicated systemgoverned by dictates other than health protection alone. For example, ergonomic
improvements are suggested in a contextdominated by production and quality requirements. Workers do not always havethe leeway they would like. Thus, if thesystem is considered as a whole, certainnegative work characteristics can be offsetby reinforcing other more positive aspects.For example, if it is difficult to change the repetitive nature of a particular job, this problem could perhaps be offset by improving work postures, reducing the efforts required, and getting workers moreinvolved in determining the content of theirjobs.
Several possible options
Acomplete intervention program for preventing WMSDs will comprise several complementary segments and be designed to have a multi-level impact. Hence,even though the most effective action is to try to eliminate the risk at its source,
action must also be taken to help workers who have already been or are in the process ofbeing affected.
Ergonomic improvement of working conditions
Prevention requires taking action at thesource. In the case of WMSDs, this meansr e d u c i n g r i s k f a c t o r s t h r o u g h t h e ergonomic improvement of working conditions. This can involve specific modi-fications, in terms of work station layout, as well as changes in work organization.Ergonomics is a strict, systematic processused to collect relevant informationthrough interviews and observations, identify the key elements involved, andpropose possible solutions. Ergonomics offers analysis and intervention tools
that are particularly well-adapted to the problem of WMSDs. Instead of describingthese tools and this process here, we will illustrate the main steps of an ergonomicintervention through a few examples thatwill be presented at the end this chapter.
Typically, there are two approaches to ergonomics. In the first, more traditionaloption, known as expert ergonomics, workimprovement is entrusted to an ergonomicsexpert, who analyzes the work stations andpresents a report to the company. This approach is direct and efficient, but the ergonomics expertise remains outside thecompany. The other option is to implement

44 Chapter 4
a participatory ergonomics process. In thiscase, an ergonomics work group, dubbed an“ergo group”, is formed within the com-pany. This group, whose work is initiallymonitored by an ergonomics expert , develops know-how in this field that remains within the company. The followingexamples will illustrate these two scenarios.
Rotation
While rotation can be used as part of the ergonomic improvement of working condi-tions, it is often proposed in isolation to correct the effects of particularly demandingstations. Consequently, it merits further discussion.
In fact, rotation among several work stationsis recommended in order to reduce exposureto the risk factors presented by one of thesestations. The idea is particularly effective if the task can be diversified and total exposure reduced. It is therefore necessaryto ensure that rotation takes place amongjobs with different requirements, so as to allow the most overburdened joints to recover. This condition is not so easy to meeton an assembly line where major demandsare made on the upper limbs.
Rotation is not a universal solution. It maybe unadvisable for work stations that require a lot of training and a long learningcurve for workers to be able to keep up. Inthese cases, changing jobs too rapidly wouldmean always being in the learning stage andnever being able to optimize operatingmethods. Changes would then have to bemade less frequently, thereby reducing theadvantages of rotation.
Training
Training is often a very important aspect ofan integrated WMSD prevention strategy.However, most of the time, it will play acomplementary role to other preventivemeasures.
In fact, the idea of worker training oftenalludes to training that focuses on “propermethods” or “proper postures”. In otherfields, notably that of handling, several studies have shown that training programsbased solely on the teaching of work meth-ods have produced disappointing results.There are various reasons for the failure ofthese programs. Often, the “theoretical”methods taught cannot be applied as is,given the restrictions of the workplace (limited space, characteristics of load handled, etc.). In addition, it is often forgot-ten that there is no single “proper workmethod” that applies universally to allworkers and all conditions. Workers willadopt different strategies based on the s i tuat ion at hand. For WMSDs, l ike handling, training aimed solely at teaching“proper work methods” would likely produce unsatisfactory results.
This does not mean that training is useless– on the contrary. However, rather thanshooting for “proper work methods”, training can focus on the transfer of infor-mation and knowledge. This approachseems more promising in terms of WMSDs.Training, for example, can be geared towardteaching workers how to detect early symptoms of WMSDs and identify the mainrisk factors at their station. Such trainingcould enable workers to make adjustmentsto their work station themselves and helpthem recognize the development of aWMSD in time. Management staff, particu-larly foremen and team leaders, as well as

Several possible options 45
engineers and mechanics, also constitute anideal training clientele. They are importantcompany players when i t comes toWMSDs, since they are often responsiblefor work transformations, at both an orga-nizational and a technical level. They cantherefore benefit from a sound knowledgeof basic ergonomic concepts, which is whytraining focusing on WMSD causes andprevention methods can be a very valuableasset. Lastly, decision-makers can alsoprofit from training on the relevance of different prevention options to help themimprove their planning.
It should also be noted that, for WMSD prevention and prevention in general, it isalways useful for new workers to have on-the-job training so that they can learntheir work properly before they are forcedto adopt the regular, often quite rapid pace.Training upon hiring can inform and fore-warn workers about WMSDs, while promoting the adoption of appropriatework methods.
In conclusion, training based on knowledgetransfer seems to offer more potential thanhighly specialized training focusing solelyon “proper work methods”. Training cantarget various clienteles: workers, foremen,engineers, mechanics, managers, health andsafety committee members, purchasing andmaintenance supervisors, etc. Themes aregeared toward the specific needs of the targeted clientele: type of WMSDs, recogni-tion of early symptoms, identification ofrisk factors, ergonomic concepts, main prevention approaches, etc.
Follow-up of affected workers
Any good prevention program should include secondary and tertiary preventionelements, in order to take into account
workers who show symptoms of WMSDs,as well as those who are absent due to awork-related accident or disease. Thus, it isrecommended that when workers at agiven station show WMSD symptoms, thisis a sign to take action to reduce the riskfactors.
The return to work of workers affected byWMSDs must also be considered. Even ifmeasures have been taken to reduce the risk of WMSDs at the work station, agradual return to the work station is generally recommended. It may be usefulto develop mechanisms that provide work-ers with working conditions adapted totheir health status. For example, a workersuffering from bursitis or shoulder painwould not be assigned a job involvingawkward shoulder postures. The goal is toprovide workers with work stationsadapted to their capacities, whatever theymay be.
Other avenues
When all is said and done, WMSD preven-tion is a relatively new field and new intervention avenues may still emerge. It isimportant to keep an open mind. Somehave already been explored, with moderatesuccess.
When it comes to preventing a work-relatedillness, many wonder if it is possible toidentify “workers at risk”, that is those whowould be the most vulnerable to this illness, in order to assign them to less demanding work stations. This is based onthe assumption that, using various tests or indicators, it is possible to predict which individuals would most likely develop a WMSD. At the present time, there is noscientific evidence suggesting that this ispossible. In the absence of a valid indicator

46 Chapter 4
of WMSD vulnerab i l i ty, i t must be concluded, given the extent of currentknowledge, that identifying workers at riskis simply not a viable means of preventingWMSDs.
Workplace fitness programs
Some companies have set up workplace fitness programs. For example, twice a day,work is interrupted for ten minutes ofstretching and warm-up exercises for over-taxed joints. Some have expressed doubt asto the true effectiveness of these programs,others say that certain exercises can beharmful, while still others give a glowingreport of the programs in progress. This issue will continue to be the subject of numerous studies in the years to come.

Ergonomic improvement of work: concrete cases 47
Hanging components on a paint conveyor
In a paint workshop, the health and safetycommittee discovered that work stations forhanging components on an overhead conveyor were relatively demanding on theback. The committee called upon the services of the joint sector-based associa-tion, which promptly sent an ergonomist tothe site. The latter first met with a few committee members to find out their inten-tions and their perception of the problem.After a short tour of the premises, he suggested a more in-depth study.
His initial meetings with the workers at thehanging stations helped redefine the problem. In fact, while workers sometimesexperienced back fatigue, they complainedmainly about shoulder pain, which they attributed to having to work with theirarms in front of them, often above theirshoulders. Workers also reported often being in a hurry.
Observing the work made it possible totake stock of demanding postures and otherrisk factors. Arms have to be lifted high, especially when taking large-sized objectsfrom the row at the top of a pallet, or whenhanging small objects at shoulder level orhigher. The back is also taxed as a result ofthe flexion required to pick up components
in the bottom of a basket and to bend overto hang them at the base of the supports.
Observations also revealed certain uniquebehaviour patterns in workers’ attempts toreduce the limitations of the work station.For example, when they have to hang smallcomponents at the base of the conveyor,some workers sit on an overturned bucket.To avoid frequent trips between the conveyor and the basket of small compo-nents, many workers fill a cardboard boxwith a large number of components, hold-ing the box with one hand while hangingwith the other (Fig. 4.2). The sustained effort required to hold the box and the factthat all the hanging is done with one hand
Ergonomic improvement of work:concrete cases
To illustrate the ergonomic approach, we have decided to outline some concrete examples. The first case is presented by an expert in cooperation with the healthand safety committee, while the second describes the application of a participatory
ergonomics approach.
Fig. 4.2
Holding a box reduces
trips back and forth
and bending, but is a
demanding static load
for the shoulder.

48 Chapter 4
Fig. 4.3
The table helps reduce
the number of trips to
the basket and frees up
both arms for work. definitely puts a lot of strain on the shoul-ders. When people fall behind, and thishappens relatively often (when they go tothe basket to fill their box, for example),they play catch-up, resulting in more trips,strained postures and accelerated execution.Thus, the catch-up phenomenon is an aggravating circumstance. After analyzingthe situation, the ergonomist asked to meetwith members of the work group to informthem of his diagnosis and to work withthem to find concrete solutions for chang-ing the job. This work committee comprisedtwo workers, two group leaders, the personnel manager and the worker representative. The ergonomist reviewedparticularly demanding postures and efforts. Workers were already well aware ofsome risk factors, but had not consideredthe difficulty of holding a box in their arms(static muscular work) or the catch-up phenomenon, which aggravates all posturesand efforts.
The committee, together with the ergono-mist, looked at several possible solutionsand came up with three changes that couldbe implemented quickly and economically.Other measures will be considered later on,
notably, to raise certain baskets when theyare nearly empty.
• Install a table on casters to support a large box filled with small hangingcomponents (Fig 4.3). This eliminates thestatic muscular work required to holdthe box, results in fewer trips to the basket because the box contains morecomponents, and gives the worker twohands free for hanging components;
• Provide a small bench on casters to replace the reversed bucket;
• Build wooden steps so that workers canaccess the higher row of pallets withouthaving to lift their arms excessively.
Assembly of surge arrestors
Analyzing this work station serves as an illustration of a participatory ergonomicsapproach involving the establishment of anergonomics work group. The mandate ofthis committee, composed of six people andone ergonomist, is to improve work stationsmost likely to cause WMSDs. The ergono-mist’s role is to guide the group in learningthe work station analysis method devel-oped by the IRSST.
The first work station this committee choseto study was the assembly of surge arrestors. In fact, this station, which thecompany plans to reorganize shortly, ischaracterized by a high staff turnover andvery repetitive work. To practice preven-tion, the committee members found it important to formulate their recommenda-tions before proceeding with reorganiza-tion. Thus, accident frequency was not adeciding factor in this case.
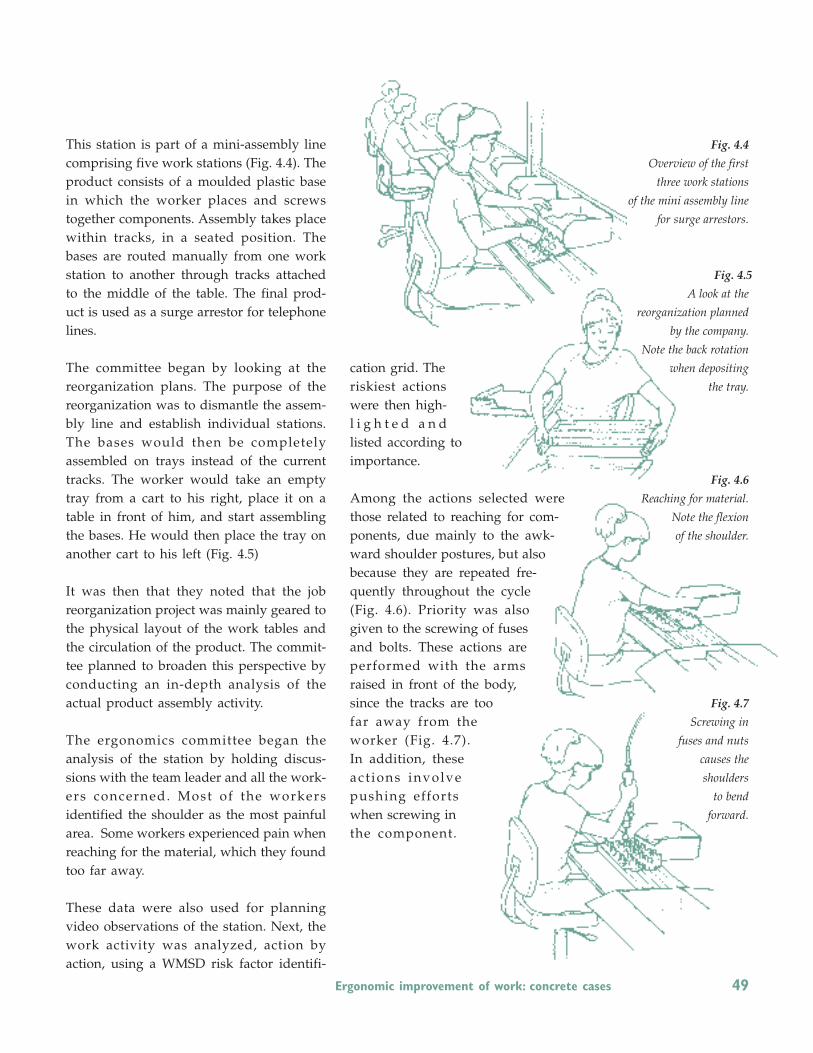
Ergonomic improvement of work: concrete cases 49
This station is part of a mini-assembly linecomprising five work stations (Fig. 4.4). Theproduct consists of a moulded plastic basein which the worker places and screws together components. Assembly takes placewithin tracks, in a seated position. Thebases are routed manually from one workstation to another through tracks attachedto the middle of the table. The final prod-uct is used as a surge arrestor for telephonelines.
The committee began by looking at the reorganization plans. The purpose of the reorganization was to dismantle the assem-bly line and establish individual stations.The bases would then be completely assembled on trays instead of the currenttracks. The worker would take an emptytray from a cart to his right, place it on atable in front of him, and start assemblingthe bases. He would then place the tray onanother cart to his left (Fig. 4.5)
It was then that they noted that the job reorganization project was mainly geared tothe physical layout of the work tables andthe circulation of the product. The commit-tee planned to broaden this perspective byconducting an in-depth analysis of the actual product assembly activity.
The ergonomics committee began theanalysis of the station by holding discus-sions with the team leader and all the work-ers concerned. Most of the workersidentified the shoulder as the most painfularea. Some workers experienced pain whenreaching for the material, which they foundtoo far away.
These data were also used for planningvideo observations of the station. Next, thework activity was analyzed, action by action, using a WMSD risk factor identifi-
cation grid. Theriskiest actionswere then high-l i g h t e d a n dlisted according to importance.
Among the actions selected werethose related to reaching for com-ponents, due mainly to the awk-ward shoulder postures, but alsobecause they are repeated fre-quently throughout the cycle(Fig. 4.6). Priority was alsogiven to the screwing of fusesand bolts. These actions areperformed with the armsraised in front of the body,since the tracks are toofar away from theworker (Fig. 4.7). In addition, theseact ions involvepushing effortswhen screwing inthe component.
Fig. 4.4
Overview of the first
three work stations
of the mini assembly line
for surge arrestors.
Fig. 4.5
A look at the
reorganization planned
by the company.
Note the back rotation
when depositing
the tray.
Fig. 4.6
Reaching for material.
Note the flexion
of the shoulder.
Fig. 4.7
Screwing in
fuses and nuts
causes the
shoulders
to bend
forward.

Fig. 4.8
View of the reorganized
work station. Note how
bringing the tracks
closer to the worker and
installing a pantograph
reduces stress on the
shoulders and the
amount of effort
required for
screwing
50 Chapter 4
The committee was also able to simulatethe assembly of surge arrestors according tothe reorganization. This simulation made itpossible to anticipate certain risk factors associated with the use of trays. In fact,transferring the trays would have causedawkward shoulder postures and back rotation (Fig. 4.5), in addition to the effortsinvolved in handling trays.
The committee therefore decided to formu-late a new reorganization proposal to bet-ter take into account identified risk factors,production requirements and product qual-ity. At this step, the manager, the engineerin charge of thereorganization and the teamleader joined the committee. The discussionfocused initially on the worst actions, beginning with the circulation of the basesand the assembly support. Several scenar-ios were developed, two of which were selected for testing in the department. The
first prototype, in accordance with the re o rg a n i z a t i o n p u t f o r w a rd b y t h e company, kept the assembly and emptyingof the bases on trays. The second prototypeproposed maintaining the assembly ontracks with the addition of a chute at theend of the table, to facilitate the emptyingof the bases. The chute and the tracks of-fered the advantage of eliminating trayhandling. Following the prototype tests, theworkers opted for assembly on tracks witha chute as the system best adapted to theirwork. At the same time, the committeemade sure that the chute system would notaffect product quality.
Regarding the use of the screwdriver, thecommittee suggested moving the trackscloser to the worker, which would reducethe amplitude of shoulder postures and allow the arms to work closer to the body.The committee also proposed adding a pan-tograph (Fig. 4.8) to reduce screwing effortsand keep the tool straight. Bringing thetracks and component containers closer tothe worker would make it easier to reachthe components.
After implementing the recommendations,the committee conducted another work sta-tion analysis to evaluate the impact of theimprovements on work activity. Workerssaid they appreciated the extended workcycle, the individualized stations, the pan-tograph for the tool, the chute system andthe reduced effort required for screwing. Interms of posture risk factors, observationsshow that most risk factors have decreased.

Summary 51
How to handle WMSDsTo prevent WMSDs it is important to take a comprehensiveapproach and to intervene in an integrated manner through a series of complementary measures that will impact technical work aspects, work organization, the physical and social environment and work characteristics and tasks.
An effective prevention strategy must eliminate the danger at the source while at the same time helping workers who are already affected.
Several prevention options can be considered:
• Ergonomic improvement of working conditions remains one of the most effective intervention routes, since it goes to the source by targeting the reduction or elimination of risk factors.
• Training is an important aspect of an integrated intervention, but cannot constitute a complete intervention in itself.
• Monitoring affected workers can be done through work station adaptation measures and gradual return-to-work measures.
• Some explore the option of workplace exercise programs.
Chapter 4 Summary

Conclusion 53
There are many causes of WMSDs, and to prevent them, the whole work situation must be taken into consideration; it is therefore a difficult issue tohandle. First, it is important to understand what is going on, to get rid of anybiases, to find out the facts. Then, it is necessary to address and evaluate theseriousness of the situation prevailing in the workplace. If the situation isacceptable, it may be sufficient to simply remain alert and ready to interveneat the slightest sign of deterioration. If, however, it becomes obvious that thesituation is problematic, either because there are already signs of identifiedWMSDs or because it is just a matter of time before they appear, action mustbe taken, and it is at this point that many may feel overwhelmed.
In fact, there are no quick fixes or ready-made solutions. The reader will nodoubt have noted that, in the chapter describing how to detect a problem,there are no exposure standards to help decide whether or not a problemexists. There are no reliable standards because too many variables areinvolved. Evaluating the problem remains basically a judgement call.
Likewise, it is also not realistic to draw up a list of possible solutions, andeven less so, to develop a guide indicating under what circumstances eachof these solutions can be used effectively. In this regard, reading Chapter 4may leave the reader yearning for more, since the possible options it offersare very general. The concrete examples presented at the end of the chapter,however, explain how the ergonomic approach can be applied.
To better meet this need for concrete intervention tools, a second document,Le groupe ergo : un outil pour prévenir les LATRs has been prepared as a follow-up to this work. The first focuses on identifying the problem, while the second provides methods for correcting it.
Aimed at those who want to take action to prevent WMSDs, this secondpublication also cannot provide recipes, in that it will not offer direct methods of modifying a given work station. It contains an in-depth presen-tation of a particular intervention method; the ergonomics work group,commonly known as the ergo group.
We favour this participatory approach to the point of devoting an entirepublication to it, because it offers numerous advantages, the main one beingto develop ergonomics expertise within the company. Through training andexperience, the members of the ergonomics work group acquire a methodthrough which they can analyze and solve their problems themselves.Another advantage is that, generally speaking, since they are developed by
Conclusion

54
people in the plant, solutions are incorporated quickly into company practices and are therefore more readily accepted by the workers. Anothersignificant advantage is that the participatory approach tends to improvecommunication within the company, because of the consultations and discussions that it involves. Lastly, the entire working atmosphere is affect-ed by the fact that the participatory approach actively involves the workers,making them feel more respected, more listened to and more motivated.