Unscheduled visits to the oncology outpatient department: a guide for improving the efficiency of...
8
ORIGINAL ARTICLE / ARTICLE ORIGINAL Unscheduled visits to the oncology outpatient department: a guide for improving the efficiency of the health care framework Visites imprévues au service de consultation externe du département d’oncologie : un guide pour l’amélioration de l’efficacité du système de santé K.R. Alleyne-Mike · K.E.A. Mohamed · R.P. Abratt Received: 22 April 2013; Accepted: 9 October 2013 © Springer-Verlag France 2013 Abstract Objective: To identify the reasons for unplanned visits to the oncology outpatient department with a view to optimising the level of health care delivery. Materials and methods: This prospective observational study of unscheduled patient visits to the oncology outpa- tient department occured during the period 15th November 2012 to 12th December 2012. The different types of malig- nancies, along with referral mechanism, disease status and presenting complaints, were documented. Results: There were unscheduled visits in 169 patients – for clinical assessment in 101 patients (59.8%) or to have a prescription refilled in 68 patients (40.2%). For patients who attended for clinical assessment, the extent of disease was metastatic in 35.6%, locally advanced in 31.7%, loca- lised malignancy in 14.9% and clear of disease in 17.8%. Oncology-related problems were seen in 68 patients. The rate presenting with true oncological emergencies was 7.4%. Pain was the most frequently documented primary symptom experienced by 44 patients, accounting for 43.6% of this grouping. When referred by a physician, patients were likely to have true oncology-related problems in 31.9 % of cases and when self-referred, in 14.7% of cases. Conclusion: This is the first published study assessing the nature of unscheduled visits by cancer patients in South Africa. Pain was the most common presenting complaint. Programmes targeted at pain control and integration of care with primary health care professionals will enhance the ser- vice delivered. Keywords Cancer · Unscheduled visits · Outpatient department Résumé Objectif : Identifier les raisons de visites impré- vues au service de consultation ambulatoire du département d’oncologie, en vue d’une optimisation du niveau des pre- stations du système de santé. Sujets et méthodes : Une étude prospective observationnelle des visites non programmées des patients au département d’oncologie ambulatoire au cours de la période du 15 novem- bre au 12 décembre 2012. Les différents types de tumeurs malignes, le mécanisme de recommendation des patients, le statut de la maladie aussi bien que les plaintes présentées par les patients ont été documentés. Résultats : Des visites imprévues ont eu lieu dans le cas de 169 patients — pour 101 de ces patients (59,8 %), il s’agissait d’une évaluation clinique, dans 68 cas (40,2 %) c’était pour avoir une prescription renouvelée. Pour les patients qui ont participé à l’évaluation clinique, l’étendue de la maladie était métastatique dans 35,6 % des cas, dans 31,7 % des cas elle était localement avancée, dans 14,9 % une tumeur maligne était localisée, et 17,8 % des patients ne présentaient pas de signe de la maladie. Les problèmes liés à l’oncologie ont été observés chez 68 patients. Le taux de présentation avec de véritables urgences oncologiques était de 7,4 %. La douleur était le plus fréquemment documentée comme premier symp- tôme par 44 patients, ce qui représente 43,6 % de ce groupe. Les patients envoyés par un médecin avaient dans 31,9 % des cas de véritables problèmes liés à l’oncologie. Dans les cas d’autoréférence, 14,7 % des problèmes y étaient liés. Conclusion : Cette étude est la première publication sur l’éva- luation de la nature des visites imprévues des patients malades de cancer en Afrique du Sud. La plainte la plus fréquemment présenter était la douleur. Des programmes destinés au con- trôle de la douleur et à l’intégration des soins avec les profes- sionnels des soins de santé primaires permettront d’améliorer les services offerts. Mots clés Cancer · Visites imprévues · Service de consultations externes K.R. Alleyne-Mike (*) · K.E.A. Mohamed · R.P. Abratt Division of radiation oncology, Groote Schuur Hospital and University of Cape Town, South Africa e-mail : [email protected] J. Afr. Cancer (2014) 6:32-39 DOI 10.1007/s12558-013-0300-y
Transcript of Unscheduled visits to the oncology outpatient department: a guide for improving the efficiency of...

ORIGINAL ARTICLE / ARTICLE ORIGINAL
Unscheduled visits to the oncology outpatient department: a guidefor improving the efficiency of the health care framework
Visites imprévues au service de consultation externe du département d’oncologie : un guidepour l’amélioration de l’efficacité du système de santé
K.R. Alleyne-Mike · K.E.A. Mohamed · R.P. Abratt
Received: 22 April 2013; Accepted: 9 October 2013© Springer-Verlag France 2013
Abstract Objective: To identify the reasons for unplannedvisits to the oncology outpatient department with a view tooptimising the level of health care delivery.Materials and methods: This prospective observationalstudy of unscheduled patient visits to the oncology outpa-tient department occured during the period 15th November2012 to 12th December 2012. The different types of malig-nancies, along with referral mechanism, disease status andpresenting complaints, were documented.Results: There were unscheduled visits in 169 patients – forclinical assessment in 101 patients (59.8%) or to have aprescription refilled in 68 patients (40.2%). For patientswho attended for clinical assessment, the extent of diseasewas metastatic in 35.6%, locally advanced in 31.7%, loca-lised malignancy in 14.9% and clear of disease in 17.8%.Oncology-related problems were seen in 68 patients. Therate presenting with true oncological emergencies was7.4%. Pain was the most frequently documented primarysymptom experienced by 44 patients, accounting for43.6% of this grouping. When referred by a physician,patients were likely to have true oncology-related problemsin 31.9 % of cases and when self-referred, in 14.7% ofcases.Conclusion: This is the first published study assessing thenature of unscheduled visits by cancer patients in SouthAfrica. Pain was the most common presenting complaint.Programmes targeted at pain control and integration of carewith primary health care professionals will enhance the ser-vice delivered.
Keywords Cancer · Unscheduled visits · Outpatientdepartment
Résumé Objectif : Identifier les raisons de visites impré-vues au service de consultation ambulatoire du départementd’oncologie, en vue d’une optimisation du niveau des pre-stations du système de santé.Sujets et méthodes : Une étude prospective observationnelledes visites non programmées des patients au départementd’oncologie ambulatoire au cours de la période du 15 novem-bre au 12 décembre 2012. Les différents types de tumeursmalignes, le mécanisme de recommendation des patients, lestatut de la maladie aussi bien que les plaintes présentées parles patients ont été documentés.Résultats : Des visites imprévues ont eu lieu dans le cas de169 patients— pour 101 de ces patients (59,8 %), il s’agissaitd’une évaluation clinique, dans 68 cas (40,2 %) c’était pouravoir une prescription renouvelée. Pour les patients qui ontparticipé à l’évaluation clinique, l’étendue de la maladie étaitmétastatique dans 35,6 % des cas, dans 31,7 % des cas elleétait localement avancée, dans 14,9 % une tumeur maligneétait localisée, et 17,8 % des patients ne présentaient pas designe de la maladie. Les problèmes liés à l’oncologie ont étéobservés chez 68 patients. Le taux de présentation avec devéritables urgences oncologiques était de 7,4 %. La douleurétait le plus fréquemment documentée comme premier symp-tôme par 44 patients, ce qui représente 43,6 % de ce groupe.Les patients envoyés par un médecin avaient dans 31,9 % descas de véritables problèmes liés à l’oncologie. Dans les casd’autoréférence, 14,7 % des problèmes y étaient liés.Conclusion : Cette étude est la première publication sur l’éva-luation de la nature des visites imprévues des patients maladesde cancer en Afrique du Sud. La plainte la plus fréquemmentprésenter était la douleur. Des programmes destinés au con-trôle de la douleur et à l’intégration des soins avec les profes-sionnels des soins de santé primaires permettront d’améliorerles services offerts.
Mots clés Cancer · Visites imprévues · Service deconsultations externes
K.R. Alleyne-Mike (*) · K.E.A. Mohamed · R.P. AbrattDivision of radiation oncology,Groote Schuur Hospital and University of Cape Town,South Africae-mail : [email protected]
J. Afr. Cancer (2014) 6:32-39DOI 10.1007/s12558-013-0300-y

Introduction
The incidence and prevalence of cancer has been rising glob-ally [1–3]. Unscheduled patient visits to oncology depart-ments add to the strain on human resources. This studywas undertaken to assess the main reasons for these visitsand the specific areas of concern for patients. The informa-tion may be helpful in using resources more efficiently.
Materials and methods
A prospective observational study was conducted at the Radi-ation Oncology Department at Groote Schuur Hospital (GSH)in Cape Town, South Africa, between 15th November 2012and 12th December 2012. The primary aim was to determinewhether the unscheduled visits, that is non-booked clinic vis-its by patients, were related to the disease itself, treatment-related or could be ascribed to other causes. A secondaryaim was to identify the more common clinical concerns ofthis cohort of patients.
A data collection sheet was drawn up and included infor-mation regarding patient demographics, type of cancer, dis-ease status, whether the patient was on active treatment or
not and reasons for the visits. Patient admissions were alsodocumented. Patients must have had a confirmed neoplasmand present with a history of an acute problem for review.Physician notes needed to be available for inclusion in thestudy. Patient folders were selected from ward admissionsand clinic and casualty reviews. The department’s databasewas also reviewed to ascertain the total number of patientsseen for that year and during the time period of the study.Permission to perform the data collection was obtained fromHospital Management and the Human Research EthicsCommittee of the Faculty of Health Sciences, University ofCape Town (Ref 609/2012).
Results
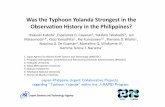
During the study period, the number of booked visits andunscheduled visits were 3404 and 169 respectively (Fig. 1).The total number of clinic visits in 2012 was 33,375.
Patients attended the oncology department either for clin-ical review or to collect medication. Prescriptions may alsobe filled at peripheral health facilities. Table 1 shows demo-graphic information which includes the sources of referrals,common malignancies and disease status of the patient
Fig. 1 Flow chart illustrating the number of scheduled and unscheduled visits seen during the study period and the types of visit
J. Afr. Cancer (2014) 6:32-39 33

cohort. The median age of patients for clinical review was59 years, while patients receiving medication had a medianage of 54.5 years. Patients in both the clinical review groupand the medication group were predominantly female. Themost common malignancy groupings in patients who wereclinically assessed were breast, gastrointestinal (GIT) andgynaecological. The majority of these patients had eithermetastatic (35.6%) or locally advanced (31.7%) disease,with the remaining patients being clear of disease or havingan early stage/localised neoplasm. The majority of patientswere on regular follow up (94%) although there were a few(6%) who had previously defaulted and now presented withadvanced disease (data not shown). The majority of patients
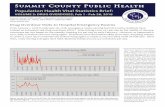
were self-referred, but patients were more likely to have con-firmed oncological problems when referred by a medicalcolleague (31.9% versus 13.7%) (Fig. 2).
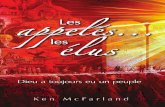
The patients who attended the clinic for a refill of theirprescription medication are shown in Fig. 3. Patients whowere not on active treatment and were being seen on routinefollow up visits only accounted for 59% of this grouping. Ofthe patients who were on active treatment, the majority(29%) were on follow up with hormonal treatment. Therewere an equal proportion of patients on radiation and che-motherapy (6%). Patients attending the clinic for a refill ofprescription medication were also more likely to be clear ofdisease (60.3%).
Table 1 Demographic information, referring bodies, types of malignancies and disease status for all unscheduled visits to the oncology
outpatient department.
Characteristics Assessment % Medication %
n = 101 59.8 n = 68 40.2
Age
Range 4–83 – 20–87 –
Mean 56.5 – 54.3 –
Median 59 – 54.5 –
Sex
Male 43 42.6 17 25.0
Female 58 57.4 51 75.0
Referring body
Self 72 71.2 – –
Private facility 2 2.0 – –
Casualty 14 13.8 – –
Other ward 3 3.0 – –
Community health centre 2 2.0 – –
Treatment area 1 1.0 – –
Hospice 2 2.0 – –
Other public hospital 5 5.0 – –
Malignancy
Breast 21 20.8 21 30.9
Gynaecology 16 15.8 9 13.2
Head and neck/Ear-nose-throat 15 14.8 8 11.8
Neurological 4 4.0 22 32.4
Sarcoma 1 1.0 1 1.5
GIT 19 18.8 3 4.4
Urology 3 3.0 0 0
Chest/Mediastinum 10 10.0 0 0
Lymphoma 8 7.8 2 2.9
Skin 4 4.0 2 2.9
Disease status
Local 15 14.9 15 22.1
Locally advanced 32 31.7 3 4.4
Metastatic 36 35.6 9 13.2
Clear of disease 18 17.8 41 60.3
34 J. Afr. Cancer (2014) 6:32-39

The proportion of assessed patients presenting with non-oncological problems was 26.8%. The precise nature of theissue could not be ascertained in 5.9% of the cases. Theremaining patients are sub-classified in Table 2, whichshows all patients with confirmed oncological problems(67.3%). Information on the types of issues, types of treat-ment, treatment intent and admissions are illustrated.
Hospital admission was required in 45.6% of patients.Disease-related issues accounted for 60.3% of this sub-group and treatment-related issues were present in 19.1%of the patients. The problems related to treatment were
mainly attributed to chemotherapy-induced side effects,of which nausea, vomiting and diarrhoea were the mostfrequently documented. Patients with GIT malignancieswere the most likely to be admitted, followed by patientswith breast malignancies. The proportion of the patientson active treatment was 55.9%.
Table 3 documents the main presenting symptoms andthe frequency with which these occurred. In patients withoncology-related problems, this was most commonly pain(47.1%) followed by respiratory symptoms (16.1%) and neu-rologic manifestations (10.2%).
Fig. 2 Relationship between referral types and proportions of oncological problems in unscheduled patients requiring clinical review
Fig. 3 Chart illustrating the distribution of unscheduled patients who attended the outpatient department for medication with regards
to treatment type
J. Afr. Cancer (2014) 6:32-39 35

Discussion
The incidence of cancer is increasing and consequentlyoncology clinics are seeing increasing numbers of unsched-uled visits. This can put increased pressure on facilities anddivert human resources which are needed to manage patientsbooked in the normal way. The problem of unscheduled vis-its has been described elsewhere [4,5]. Cancer patients, bythe nature of their disease and expected side effects of treat-ment, are inclined to experience unwanted symptoms. Onco-logical emergencies such as spinal cord compression, super-ior vena cava syndrome and febrile neutropenia requireprompt referral to an oncologist. However, in many othercases, appropriate management can be delivered by a physi-cian in a primary/peripheral facility.
The proportion of patients attending the clinic during thestudy period in order to have a prescription filled was 40.2%(Fig. 1). The majority of patients were not on any type ofactive treatment (59%), and a smaller grouping were eitherbreast cancer patients on hormone manipulation therapy orpatients with neurological neoplasms on hormone replace-ment therapy (29% in total) (Fig. 3). Thus, a significant per-centage of these patients were not on cytotoxic treatment(88%) and could have collected medication at their periph-eral centres.
A possible reason for unscheduled visits is that patientswho are on active treatment are advised to come into theclinics should they have acute problems. Patients who arenot on active treatment are expected to seek assessment firstat a peripheral facility and only be referred on to the tertiarycentre as required. However, many maintain the policy ofattendance at the tertiary centre, even when treatment is notactive. Figure 2 shows that, of the patients who attended for
Table 2 Characteristics of non-booked patients presenting with
proven oncological problems.
Characteristics Oncological patients
All Admitted
n = 68 % n = 31 %
Malignancy
Breast 14 20.6 5 16.0
Gynaecology 10 14.7 4 12.9
Head and neck/Ear-
nose-throat
9 13.2 3 9.7
Neuro 3 4.4 0 0
Sarcoma 0 0 0 0
GIT 15 22.1 10 32.3
Urology 3 4.4 1 3.2
Chest/Mediastinum 8 11.8 2 6.5
Lymphoma 4 5.9 4 12.9
Skin 2 2.9 2 6.5
Type of problems
Disease related 41 60.3 19 61.3
Treatment related 13 19.1 7 22.6
Both 9 13.2 4 12.9
Unclear 5 7.4 1 3.2
On active treatment 38 55.9 19 61.3
Radiotherapy 11 16.2 4 12.9
Chemotherapy 19 27.9 13 41.9
Hormone 8 11.8 2 6.5
Treatment intent
Radical 10 14.7 5 16.1
Palliative 28 41.2 14 45.2
Not on active treatment 30 44.1 12 38.7
Table 3 Frequency of distributions of primary symptom complaints in patients without scheduled appointments.
Primary symptom Total number of patients Oncology problems Non-oncology/unclear
problems
n = 101 % n = 68 % n = 33 %
Pain 44 43.6 32 47.1 12 36.4
Bleeding 3 3.0 1 1.5 2 6.1
Upper gastrointenstinal 3 3.0 3 4.4 0 0
Lower gastrointenstinal 6 5.9 6 8.8 0 0
Fever 2 2.0 1 1.5 1 3.0
Respiratory 16 15.8 11 16.1 5 15.2
Genito-urinary 1 1.0 0 0 1 3.0
Neurologic 9 8.8 7 10.2 2 6.0
Fatigue 4 4.0 3 4.4 1 3.0
Other 13 12.9 4 5.9 9 27.3
36 J. Afr. Cancer (2014) 6:32-39

clinical review, presentation with non-oncological problemswas more than twice as likely in those who were self-referred (31.9%) than in those referred by other health profes-sionals (13.7%). Encouraging patients to visit their local facil-ities may thus help reduce unnecessary visits. McKenzie et alsimilarly identified this problem and suggested that the prob-lem can best be addressed by ensuring that the different tiersin our health care framework work in sequence with eachother allowing for a seamless process [6].
A small percentage of all the clinically assessed patientswere clear of disease (17.8% in this study). The problem wasconsidered to be oncology-related in 3 of the 18 patients andin each case it was related to side effects of previous treat-ment. It was difficult to ascertain the nature of the problemin 2 patients, and the remaining 13 patients were not consid-ered to have a problem related to either their disease or treat-ment. It has been suggested that fear of recurrence is one ofthe main reasons why patients who are clear of their diseasetend to present at clinics unexpectedly. Lebel and co-workersfound that health care use was higher in this group ofpatients but was also influenced by other demographic fac-tors [7]. They found that female patients and older patientswere the sub-group of patients more likely to attend clinicianvisits. In this study, the patients who were clear of diseasewere female in 67% of the cases.
True oncological malignancies are haematological, meta-bolic or structural/compressive in nature [8]. Díaz-Couselo, ina short review article, identified 30 patients with true oncolog-ical emergencies out of a total of 365 non-scheduled visits [9].This accounted for 8.2% of all patients seen in that study.In this current study, only 5% of all patients had a true onco-logical emergency. This corresponded to 7.4% of the patientswith confirmed oncological problems. These consisted of2 patients with neutropenic sepsis, 1 with superior mediastinalsyndrome, another with spinal cord compression and 1 patientwith hypercalcaemia.
Most patients whose health has been in rapid decline dueto their disease are referred to a hospice facility where possi-ble. However, not all residential areas currently have hospicecover and thus a percentage of the referrals involve patientsrequiring end of life care (8.8% of patients with oncologicalproblems).
The most common symptom reported by patients in thestudy was pain (47.1% of patients with oncological pro-blems), which other studies have similarly identified as themost frequent complaint [10–12]. Reasons for inadequatepain control include lack of reporting, poor use of analgesicsdue to concerns about the risk of addiction, misinformationregarding associated side effects and sometimes cultural andsocial beliefs [13,14]. Other frequently reported presentingcomplaints included respiratory symptoms, neurologic pro-blems and lower GIT complaints (Table 3). A pain interven-tion strategy was described in a randomised clinical study by
Miaskowski et al. [15]. Patients were advised not only ondifferent ways to assess the response to treatment for painand make dosage intensity and frequency adjustments butalso on how to cope with and treat the side effects experi-enced from their analgesics. The patients benefitted from thispsycho-educational intervention but regular patient homevisits and contact via telephone were necessary to ensuresuccess. This may prove difficult especially for patientswho live in rural areas.
Another more generalised intervention measure wasdescribed by Ferrer-Roca and colleagues, which involved a24-hour call centre being established and patients able tocall in to discuss concerns [16]. The intervention spanned aperiod of four years. Interestingly, most calls lasted less than5 min (87%). Only 10% of the calls resulted in a patient hos-pital visit, while the remaining 90% of call issues were man-aged telephonically. The study resulted in a reduction in thenumber of unplanned visits by oncology patients. Reports ofother intervention strategies in the literature have also provensuccessful [17].
Further studies have suggested that the projected demandfor oncologists will exceed the supply in the future [18,19].Thus increases in cancer incidence, coupled with theconcomitant increase in survivors, will further complicatethe issue of unscheduled visits, particularly when seen inthe light of a diminishing human resource base of trainedprofessionals.
One of many intervention strategies discussed by authorssuch as Erikson et al is to facilitate patient follow up visitsthrough primary care facilities [20]. However, this is not with-out its own challenges. A systematic review conducted byLewis et al documented that patients often felt that a primarycare physician (PCP) did not have the expertise to conduct athorough follow up assessment, or often felt that these physi-cians were unwilling to undertake this responsibility [21].This was corroborated in an article by Nissen et al in which175 PCPs were questioned regarding follow up care for breastand colorectal cancer patients [22]. Only 52% were comfort-able with the task and even less (43%) felt that they wereappropriately adhering to established guidelines. In anotherstudy by Del Giudice, PCPs were willing to shoulder theresponsibility of follow up care but with the proviso thatoncologists were willing to provide supplemental informationwhich included clear guidelines on relevant investigations,detailed patient summary outlines with information on poten-tial treatment side effects, and, of particular importance,greater availability to services for investigations and rapidreferral systems for patients deemed to require oncologicalassessment [23].
To this end, many institutions have implemented survi-vorship programmes aimed at facilitating this structuredapproach. The plan is to develop a more cohesive structure
J. Afr. Cancer (2014) 6:32-39 37

for treatment consultations with the aim of producing acomprehensive follow-through plan of care.
Thus physicians in peripheral centres or other oncologycentres will be provided with written information regardingthe patient’s diagnosis, prognosis, details of disease manage-ment, implications of the treatment modalities used andguidelines for follow up assessment [24]. It is believed thatthis will serve to help guide other clinicians in not only mak-ing timely appropriate referrals to specialised centres butalso in guiding them to manage some of the side effectsthat may not require care at a tertiary level facility. The ben-efits of this are many: PCPs will feel empowered to under-take follow up management, oncology clinics and emer-gency departments will not be besieged by excessive visitsand patients who live in rural areas may be spared the finan-cial burden and logistical difficulties of transporting them-selves or their family members to a distant tertiary facility foran issue that can be easily managed by the doctor in theirarea. Moreover there is growing evidence that these pro-grammes do make a difference and can positively influencepatient care [25]. A framework like this can be of great ben-efit in developing countries like South Africa and the depart-ment is taking steps to develop care pathways which willsupport this system. Implementation of survivorship pro-grammes can thus serve to bridge the gap of continuum ofcare for all patients who have been diagnosed with cancer.
Conclusion
This prospective study is limited in that it serves as a snap-shot of a brief period. It also does not take into account thenumber of oncology patients who are managed in the emer-gency department of Groote Schuur Hospital without refer-ral to the oncology department.
There are many reasons why oncology patients may visitthe outpatient department without a clinical appointment.Pain is by far the most common reason for referral. In thesecases the establishment of pain clinics or telephone hotlineservices may be valuable in advising patients on medicationoptimisation and advising on other related issues.
Decentralisation of follow up care services is a viableway forward which can serve to improve the situation ofunscheduled visits by providing patients with first consultcare at the level of the primary care facilities. Patients aremore likely to be referred for specific oncological problemswhen referred by a clinician and thus informed colleague-based referral may be an effective way of encouragingappropriate referrals.
Another way forward is a survivorship program whichaims to adopt care pathways which streamline patient man-agement. This management course is communicated to phy-sicians in peripheral centres, better equipping them with the
relevant information to aid patient assessment. An importantcomponent of this is the end-of-treatment consultation withpatients and the provision of written information to thepatient.
There have not been many studies of this nature publishedin the setting of the African continent. However, the provi-sion of optimal quality of post treatment care for patientswith cancer will be facilitated by engendering greater collab-oration between peripheral clinics and the core cancer treat-ment facilities.
Conflict of Interest: K.R. Alleyne-Mike, K.E.A. Mohamedand R.P. Abratt have no conflict of interest to declare.
Funding support: No funding received.
References
1. Parkin DM, Bray F, Ferlay J, et al (2001) Estimating the worldcancer burden: Globocan 2000. Int J Cancer 94(2):153–6
2. Parkin DM, Bray F, Ferlay J, et al (2005) Global cancer statistics,2002. CA Cancer J Clin 55(2):74–108
3. Jemal A, Bray F, Center MM, et al (2011) Global cancer statis-tics. CA Cancer J Clin 61(2):69–90
4. Livingston PM, Craike M, Considine J (2011) Unplanned presen-tations to emergency departments due to chemotherapy inducedcomplications: opportunities for improving service delivery. Aus-tralas Emerg Nurs J 5;14(2):62–8
5. Vandyk AD, Harrison MB, Macartney G, et al (2012) Emergencydepartment visits for symptoms experienced by oncology patients:a systematic review. Support Care Cancer 20(8):1589–99
6. McKenzie H, Hayes L, White K, et al (2011) Chemotherapy out-patients’ unplanned presentations to hospital: a retrospective study.Support Care Cancer 19(7):963–9
7. Lebel S, Tomei C, Feldstain A, et al (2013) Does fear of cancerrecurrence predict cancer survivors’ health care use? SupportCare Cancer 21(3):901–6
8. Higdon ML, Higdon JA (2006) Treatment of oncologic emergen-cies. Am Fam Physician 74(11):1873–80
9. Diaz-Couselo FA, O’Connor JM, Nervo A, et al (2004) Non-scheduled consultation in oncologic patients. How many of themare true emergencies? An observational prospective study. SupportCare Cancer 12(4):274–7
10. Aprile G, Pisa FE, Follador A, et al (2013) Unplanned presenta-tions of cancer outpatients: a retrospective cohort study. SupportCare Cancer 21(2):397-404
11. Mayer DK, Travers D, Wyss A, et al (2011) Why do patientswith cancer visit emergency departments? Results of a 2008 pop-ulation study in North Carolina. J Clin Oncol 29(19):2683–8
12. Tsai SC, Liu LN, Tang ST, et al (2010) Cancer pain as the pre-senting problem in emergency departments: incidence and relatedfactors. Support Care Cancer 18(1):57–65
13. Beck SL (2000) An ethnographic study of factors influenc-ing cancer pain management in South Africa. Cancer Nurs 23(2):91–9
14. Anderson KO, Richman SP, Hurley J, et al (2002) Cancer painmanagement among underserved minority outpatients: perceivedneeds and barriers to optimal control. Cancer 94(8):2295–304
38 J. Afr. Cancer (2014) 6:32-39

15. Miaskowski C, Dodd M, West C, et al (2004) Randomized clini-cal trial of the effectiveness of a self-care intervention to improvecancer pain management. J Clin Oncol 22(9):1713–20
16. Ferrer-Roca O, Subirana R (2002) A four-year study of telephonesupport for oncology patients using a non-supervised call centre.J Telemed Telecare 8(6):331–6
17. Kurtz ME, Kurtz JC, Given CW, et al (2006) Effects of a symp-tom control intervention on utilization of health care servicesamong cancer patients. Med Sci Monit 12(7):CR319–24
18. Smith BD, Haffty BG, Wilson LD, et al (2010) The future ofradiation oncology in the United States from 2010 to 2020: willsupply keep pace with demand? J Clin Oncol 28(35):5160–5
19. Warren JL, Mariotto AB, Meekins A, et al (2008) Current andfuture utilization of services from medical oncologists. J ClinOncol 26(19):3242–47
20. Erikson C, Salsberg E, Forte G, et al (2007) Future supply anddemand for oncologists: challenges to assuring access to oncol-ogy services. J Oncol Pract Mar 3(2):79–86
21. Lewis R, Neal R, Hendry M, et al (2009) Patients’ and healthcareprofessionals’ views of cancer follow-up: systematic review. Br JGen Pract 59(564):248–59
22. Nissen M, Beran M, Lee M, et al (2007) Views of primary careproviders on follow-up cancer patients. Fam Med 39(7):477–82
23. Del Giudice ME, Grunfeld E, Harvey BJ, et al (2009) Primarycare physicians’ views of routine follow-up care of cancer survi-vors. J Clin Oncol 27(20):3338–45
24. Earle CC, Ganz PA (2012) Cancer survivorship care: don’t let theperfect be the enemy of the good. J Clin Oncol 30(30):3764–8
25. Shalom MM, Hahn EE, Casillas J, et al (2011) Do survivorshipcare plans make a difference? A primary care provider perspec-tive. J Oncol Pract 7(5):314–8
J. Afr. Cancer (2014) 6:32-39 39