Tumeurs cérébrales chez lenfant Nadine GIRARD Hôpital Timone Marseille 2008 UMR 6612 P Cozzone.
50
Tumeurs cérébrales chez l’enfant Nadine GIRARD Hôpital Timone Marseille 2008 UMR 6612 P Cozzone
-
Upload
margot-lebas -
Category
Documents
-
view
112 -
download
1
Transcript of Tumeurs cérébrales chez lenfant Nadine GIRARD Hôpital Timone Marseille 2008 UMR 6612 P Cozzone.

Tumeurs cérébrales chez l’enfant
Nadine GIRARD
Hôpital Timone
Marseille
2008
UMR 6612P Cozzone

Introduction
• Population pédiatrique: 2ème cause de cancer de l’enfant (après leucémie)• TFP-sustentorielle=50-50
• Nourrisson: prédominance sustentorielle (gliome VO, PNET, tumeurs des plexus choroïdes)
• Tumeur infratentorielle: 3-11 ans• Incidence égale après 11 ans
• Répartition • le long de la ligne médiane (85%)
• dans la fosse postérieure (50%)• suprasellaire (30°%)• pinéale
• hémisphérique (15%): épilepsie 9-15%
0
4
8
12
16
20
24
No
mb
re
0 2 4 6 8 10 12 14 16 18 20
Histogramme

Introduction
Les tumeurs primitives sont prépondérantes
L.E Becker 1999 Neuroimaging Clin North Am
0,001,002,003,004,00 0,001,002,003,004,00

Présentations cliniques• Dépendent de l’âge et de la localisation• Nourrisson
• augmentation du PC, irritabilité, léthargie, vomissement, perte des acquisitions
• Enfant: idem+• Céphalées, convulsions, diminution acuité visuelle,
paralysie des nerfs crâniens (POM), ataxie, hémiparésie, torticolis
• HTIC sans déficit focal
• Epilepsie: rare, tumeurs du cortex• Crises gélastiques: hamartome plancher V3

Signes endocriniens - Orientation Dg
• Diabète insipide• germinome ++ = 27% , histiocytose X: 15%
• Puberté précoce• gliome voies optiques, hypothalamique• hamartome plancher du V3• germinome (sécrétant ou non)• tumeurs pinéales• kyste suprasellaire, craniopharyngiome
• Retard de croissance par déficit en GH• craniopharyngiome • gliome optique (NF1), histiocytose, hamartome
• Syndrome de Russel (syndrome diencéphalique): boulimie et extrême émaciation: gliome hypothalamique

Variétés histologiques• Tumours of the Neuroepithelial Tissue
• Astrocytic Tumours• Oligodendroglial Tumours• Oligoastrocytic Tumours• Ependymal Tumours• Choroid Plexus Tumours: papilloma, carcinoma, atypical papilloma• Other Neuroepithelial Tumours• Neuronal and Mixed neuronal-glial tumours: ganglioglioma,
gangliocytoma, DNT, cerebellar dysplastic gangliocytoma• Tumours of the Pineal Region: pineocytoma, pineoblastoma • Embryonal Tumours
• Tumours of Cranial and Paraspinal Nerves• Tumours of the Meninges• Lymphomas and Haematopoeitic neoplasms• Germ Cell Tumours• Tumours of the Sellar Region

• Atypical choroid plexus papilloma• ICD-O 9390/1, WHO grade II
• Extraventricular neurocytoma• ICD-O 9506/1, WHO grade II
• Pilomyxoid astrocytoma• ICD-O 9425/3, WHO grade II
• Anaplastic medulloblastoma• ICD-O 9474/3, WHO grade IV
• Medulloblastoma with extensive nodularity• ICD-O 9471/3, WHO grade IV
• Angiocentric glioma• ICD 9431/1, WHO grade I
• Other CNS PNET: new concept
2007 WHO classification of tumours of the CNS Additions: entities, variants and patternreclassifications

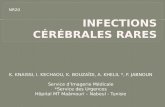
This variant of pilocytic astrocytoma is characterized by a mucoid matrix and angiocentric pattern, and lack of rosenthal fibers or granulomatous bodiesIt is typically located in the hypothalamic/chiasmatic region and occur in very young childrenLocal recurrence and CSF spreading are frequentOrigin: peculiar radial glia?WHO grade 2
Astrocytome pilocytaireAstro à cellules géantes (NF1)AnaplasiqueGB
Kyste intratumoral

Tumours of Neuroepithelial Tissue- Astrocytic Tumours- Oligodendroglial Tumours- Oligoastrocytic Tumours- Ependymal Tumours- Choroid Plexus Tumours- Other Neuroepithelial Tumours- Neuronal and Mixed neuronal- glial tumours- Tumours of the Pineal Region- Embryonal TumoursChildren and young adults
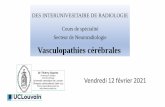
Refractory epilepsyWell-delinated, hyperintense, non-enhancing cortical lesion (T2/FLAIR) with a stalk-like extension to the subjacent ventricle. Fronto-parietal and temporal lobesStable or slowly growing lesionHistogenesis unknown , belongs to the group of « other neuroepithelial tumor »Also reported as angiocentric neuroepithelial tumorWHO grade 1

Children and adults
Relatively large, well-circumscribed, contrast-enhancing
tumor of the pineal region
Recurrence and meningeal spreading may occur after
total surgical excision
Biological behaviour is unpredictable at present and
histological grading criteria remain to be defined
Presumptive origin: specialized ependymal cell of the
subcommissural organ
WHO grade 2/3

Defined as choroid plexus Defined as choroid plexus
papilloma with increased mitotic papilloma with increased mitotic
activityactivityWHO grade 2WHO grade 2

Other CNS PNET: Embryonal tumour with abundant neuropil and true rosettes: ETANTR

Imagerie
• Morphologique• Scanner: pratiqué très rapidement dès que l’arrière
pensée tumeur existe, avant et après injection, CT perfusion diagnostic positif
• IRM: T1, T2, FLAIR, Diffusion, T1 Gd, incluant le canal spinal (tumeurs ligne médiane, drop métastases)
bilan préthérapeutique
• Fonctionnelle: diagnostic et préthérapeutique• Perfusion: Gd, ASL• Spectrométrie de protons (SRM) • DTI• IRM d’activation
lymphome

Localisation Orientation Dg
Tumeurs Fosse Postérieure
• pont: astrocytome fibrillaire (g infiltrant) (mauvais pronostic)
• bulbe, protubérance post.: astro. pilocytaire juvénile
• V4, à partir du vermis: médulloblastome
• V4, vers les citernes: épendymome
• cervelet: astro. pilocytaire juvénile, médullo. desmoplasique

Localisation Orientation Dg
Tumeurs du V3• Antérieures
• Craniopharyngiome: sellaire, ou infundibulaire
• Gliome VO (astro.pilo.)• Astro.pilo.
hypothalamique• Germinome, tératome
• Postérieures • Pinéocytome-blastome• Germinome, tératome,
autres T.germinales

Localisation - Orientation Dg
Ventricules latéraux
• Papillome plexus choroïde• Carcinome rare• Astrocytome à cellules
géantes (Bourneville)• Méningiome: exceptionnel

Localisation - Orientation Dg
Tumeurs hémisphériques• Noyaux gris et thalamus:
• astro.oligo. (haut grade), germinome
• Hémisphérique profonde:• épendymome, astro.
anaplasique, oligodendrogliome malin, tumeurs rares (rhabdoïde-teratoïde, PNET)
• Corticale: • gangliogliome, DNT
(dysplastic neuroepithelial tumor), oligodendrogliome (bénin), gangliocytome infantile
oligo anaplasique
germinome
gangliogliome

Imagerie• Localisation• Retentissement
• hydrocéphalie, engagement, dissémination (IRM tout l’axe nerveux si T ligne médiane)
• Morphologie:focal, infiltrant • Caractérisation tissulaire• TDM
• Densité cellulaire• Calcifications, Sang
• ennemis de la SRM
• Perfusion: simple• Pb abord veineux gros calibre
jeune enfant et nourrisson
• IRM• Diffusion: T compacte/lâche• Perfusion• SRM• DTI
Germinomes
Gangliocytome

15 ans, HIC, xanthoastrocytome malin

Calcifications• Craniopharyngiome (85%)
Épendymome (50%)• Médulloblastome (20%)• Oligodendrogliome (25-50%)• Gangliocytome• Gangliogliome gangliogliome
craniopharyngiome
médulloblastome

Forte densité cellulaire (tumeur compacte)
• Germinome• Médulloblastome, PNET• Tumeurs des plexus
choroïdes• Méningiome
médulloblastome
papillome
diffusion

Faible densité cellulaire (tissu tumoral lache)
• Astrocytome• Gliome tronc• DNT
DNT
Gliome tronc
astrocytome

• Corrélation négative ADC et densité cellulaire entre T du tronc et T embryonnaires (Gauvain et al AJR 2001)
• ADC élevé: DNET (Bulakbasi et al 2007), astrocytome, gliome tronc
• ADC bas: médulloblastome, PNET
Rumboldt et al 2006T cérébelleuses enfant
Schneider J, Girard N JMRI 2007

Donnéespersonnelles

Ewing PNET hémorragique
InfiltrationŒdèmeHémorragie
T MALIGNE
Oligo III
DNT

Kyste intra-péritumoral
• Astrocytome pilocytaire• Variété pilomyxoïde• Nécrose: médulloblastome,
épendymome, PNETpilomyxoïde
Astro. Pilo.
PNET
épendymome

Tumeur infiltrante• Ependymome• Oligodendrogliome profond (malin)• Gliomatose: rare chez l’enfant
épendymome
oligodendrogliomes
gliomatose

Vaisseaux anormaux
• Ependymome• Médulloblastome• PNET
Ependymome
PNET

Contraste• Rupture barrière
• Destruction des capillaires normaux par la tumeur
• Paroi anormale de capillaires anormaux
• Néoangiogénèse• Enfant: rehaussement
n’est pas synonyme de malin • Astrocytome pilocytaire• DNET• Papillome
oligo
PNET
Astro.pilo
papillome

Perfusion avec injection• Technique
• Difficile chez le petit enfant• Voie veineuse de petit calibre• Adapter l’injection au poids et calibre veineux• Limitation de la dose de contraste
• Rehaussement par le PDC• Rupture de la BHE (perméabilité anormale): astrocytome
pilocytaire +++• Néoangiogénèse: rCBV
• pas de corrélation avec le grade histologique au stade initial• Suivi tumoral rTBV élevé dans T progessive/T stable (Tzika AA et al,
Cancer 2004)
• CBF: augmenté dans haut grade (Tzika AA et al AJNR 1997)• Pas de corrélation (Ball W et al 2001)


DNT, tuber, hamartome: rCBV le plus bas
hamartome

DNT, tuber, hamartome: rCBV le plus bas
DNT
tuber

Médulloblastome
Ependymome

Embryonal tumour with abundant neuropil and true rosettes: ETANTR
Médulloblastome desmoplasique


SRM
• Monovoxel: TE court et long (PRESS)• CSI 2D: TE long, + TE court• Peu d’études pour le diagnostic positif
• Panigrahy et al 2006 (60 patients), • Schneider, Girard et al 2007 (17 patients, TFP),• Bulakbasi et al 2007 (22 patients, DNET, population
pédiatrique et adulte)
• Intensité de la Cho non liée au grade de la tumeur

MédulloblastomeTau, Cho élevée
EpendymomemI, NAA très bas
Gliome TCmI, Cho
Astrocytome pilocytaireCho élevée, lactate, Cr et NAA bas
Schneider J, Girard N, JMRI 2007

MRS + ADC
•ependymoma, + astro pilo, *glioma BS, o medulloblastoma
Schneider J, Girard N, JMRI 2007

Tumeurs supratentorielles• Astrocytome anaplasique, oligodendrogliome malin, GB, PNET• GB: Ala, Glx, Gly (Panigrahy 2006)
• Cr: diminué dans haut grade (Tzika et al 2002)
01234
PNET
GB
Oligo III
Oligo-Astro anaplasique
ETANTR

• Papillome plexus choroïde: mI (le plus élevé)• Carcinome plexus choroïde: Cho (le plus
élevé)• Germinome: Glx
Germinomepinéal
TRT atypique
Panigrahy et al
01234

Tumeurs épileptogènes• Oligodendrogliome versus DNT versus
gangliogliome : pas d’étude rapportée• DNT: augmentation mI (Bulakbasi et al), chute NAA
non significative

gangliogliome

NF1 • Lésion focale hyper T2 versus tumeur• Cho/tCr >2 et NAA: gliome• 1,3 < Cho/tCr <2 et NAA normal : lésion focale de
la NF1• Gonen et al, AJNR 1999
0123401234

SRM et suivi• Progression: augmentation Cho (sup 20%) / tumeur
stable (Tzika AA et al, Cancer 2004) associé à augmentation du TBV
• Gliome du TC: augmentation Cho et Cho/NAA malgré amélioration clinique (Thakur SB et al, AJNR 2006)
+ 6 mois

8 ans après fin de trt médulloblastomePas de plainte clinique

IRM DTI - Tenseur• Peu utilisée• Tumeur périphérique corticale peu fréquente• Connectivité non ou peu développée• Problématique adulte: forme localisée ou infiltrante des gliomes pour
prédire les récidives (Price et al 2007)


Tumeurs du troncInfiltration du FCS
Infiltration diffuse Helton et al 2006

Conclusion1. Incidence: 2ème cause de cancer2. Grande variété histologique3. Localisation: orientation Dg4. Morphologie: IRM et scanner
Perfusion: astrocytome pilocytaireSRM + ADC: distinction des TFP
La route est longue5. DG de nature: histologie et marqueurs avec deux
exceptions: gliome infiltrant du tronc cérébral (morphologie spécifique)germinome (morphologie plus ou moins spécifique)