Transcatheter Mitral Valve Replacement with the Tendyne …Transcatheter Mitral Valve Replacement...
26
Transcatheter Mitral Valve Replacement with the Tendyne Valve. with the Tendyne Valve. A Pichard, L Satler , Ron Waksman, I Ben-Dor , P Corso, L Satler , Ron Waksman, I Ben-Dor , P Corso, C Shults, N Bernardo, E Woo, G Weigold, G Weissman,A Ertel, T. Weddington, S Boyce, A Bafi,P G Weissman,A Ertel, T. Weddington, S Boyce, A Bafi,P Okubagzi. Medstar Washington Hospital Center Medstar Washington Hospital Center Washington, DC Professor of Medicine (Cardiology) Professor of Medicine (Cardiology) Georgetown University
Transcript of Transcatheter Mitral Valve Replacement with the Tendyne …Transcatheter Mitral Valve Replacement...

Transcatheter Mitral Valve Replacementwith the Tendyne Valve.with the Tendyne Valve.
A Pichard,
L Satler, Ron Waksman, I Ben-Dor, P Corso,L Satler, Ron Waksman, I Ben-Dor, P Corso,
C Shults, N Bernardo, E Woo, G Weigold,
G Weissman, A Ertel, T. Weddington, S Boyce, A Bafi, PG Weissman, A Ertel, T. Weddington, S Boyce, A Bafi, POkubagzi.
Medstar Washington Hospital CenterMedstar Washington Hospital Center
Washington, DC
Professor of Medicine (Cardiology)Professor of Medicine (Cardiology)
Georgetown University

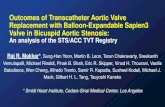
Tendyne Transcatheter Mitral ValveTendyne DeviceTendyne Device
• D-Shaped Self-Expanding Nitinol Outer Frame
• Conforms to Native MV Anatomy
• Circular Self-Expanding Nitinol Inner Frame• Circular Self-Expanding Nitinol Inner Frame
• Large Effective Orifice Area (>3.0cm2), larger thanany Surgical Valve
• Porcine Pericardial Tri-Leaflet Valve• Porcine Pericardial Tri-Leaflet Valve
• Large Valve Size Matrix to Treat Varying Anatomies
• Outer Frame Sizes: 30-43mm AP x 34-50mm CC
• Valve Tether to Apex• Valve Tether to Apex
• Provides Valve Stability - Designed to Reduce PVL
• Apical Pad Assists in Access Closure
Tendyne product is currently in development at Abbott. Neither approved or available for sale.

Tendyne Transcatheter Mitral Valve
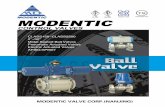
Tendyne Procedure
Fully RepositionableFully Repositionable
Fully Retrievable
No Rapid Pacing or CPB
Procedural Steps
TA Approach TA Approach
Insert Catheter into LA
Intra-Annular Deployment
Ensure Valve Seating Ensure Valve Seating
Adjust Tether Tension
Secure Apical PadTendyne product is currently in development at Abbott. Neither approved or available for sale.

Tendyne Implant Experience
EFS/CE Mark StudySite Name (n=12 sites)
St. Vincent’s
Prince Charles Hospital
Abbott
Cleveland Clinic
• Compassionate cases
– Royal Brompton Hospital
Cleveland Clinic
Baylor
Northshore
MedStar – Royal Brompton Hospital
– University Hospital Zurich
– University of Bonn
– Abbott NW (MHI)
– Bad Nauheim
MedStar
Henry Ford Hospital
Pinnacle Health
West Virginia University – Bad NauheimWest Virginia University
Oslo University Hospital
Emory30Oct2016
Total experience to date: >70 casesLongest follow-up 2yrs

J Am Coll Cardiol. 2017 Jan 31; 69(4): 381-391

P rotocolP rotocolInclusion Criteria:Symptomatic severe MR (3-4+)
Exclusion Criteria:EF <30%EF <30%LV diastolic ID >70mmSevere MV annular calcificationSevere MV annular calcificationSevere RV dysfunction or severe TRPAP > 70 mm Hg

BaselineEchoP aram etersBaselineEchoP aram eters

30 day MV gradient: 3.4 mm Hg• 30 day MV gradient: 3.4 mm Hg• 30 day LVOT gradient: 1.9 mm Hg• KCCQ improved from 50 to 64 p=0.002

Complications

Trial CommentsTrial Comments
• Small initial series of very high risk patients.
• Experience for each Site: 50% of Sites did only 1-2 cases.
• Proved that MVR with dedicated valve and without
CP Bypass is possible.CP Bypass is possible.
• Procedure is safe with low risk of procedural death orcomplications.complications.
• Effectively treated severe MR, with significant clinicalimprovement and LV improvement.

STS score: 5.5%
83 y/o male
Severe MR – restricted posterior mitralleaflet. Mitral jet is eccentric
STS score: 5.5%
leaflet. Mitral jet is eccentric
Ht=175cm, Wt=72g, BMI=22, BSA=1.8, Cr=1.1
PMHx:
Scalp sarcoma
HTN, GERD, AF, seizures, Kidney mass
FEV1= 46% with Sev. Restriction
PMHx:
FrailtyFEV1= 46% with Sev. Restriction
FEV1 41%Frailty
Criteria Score Cutoff
ADL 4 ≤ 4/6
Grip Strength 20 < 30 kgGrip Strength 20 < 30 kg
15-Foot Walk 10.3 > 6 sec
Albumin 3.3 < 3.5g/dl
TOTAL 4/4

TEE (2/23/2016)
Echo Variable (TTE) Measure
Severity of AR Moderate
Severity of MR Severe
Ejection Fraction 30-35 %Ejection Fraction 30-35 %
Severe MR – restricted posteriormitral leaflet. Mitral jet is eccentric

M itralorificedim ensions.CT
13
End DiastoleEnd Systole

Evaluatingneo-LVO T (diastole)Evaluatingneo-LVO T (diastole)
14

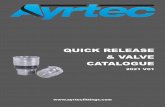
TA AccessSwan from Apex to LA

S w anfrom ApextoL A

Confidaw ireinL A L argeS heathintoApex(34F)Confidaw ireinL A L argeS heathintoApex(34F)

ValveintroducedandDeploym entS tartValveintroducedandDeploym entS tart




FinalR esultFinalR esult


ApicalP lateforT etherApicalP lateforT ether


ConclusionsConclusions
• This is the first percutaneous MVR with a successful clinical start.
• The Trial is actively enrolling patients.
• Much to be learned yet about clinical and procedural aspects.
• It has initiated and exciting new era in Interventional Cardiology.• It has initiated and exciting new era in Interventional Cardiology.