Traitement curatif de -...
38
Traitement curatif de la carcinomatose péritonéale: utopie ou réalité? Isabelle Deshaies, MD, FRCSC
Transcript of Traitement curatif de -...

Traitement curatif de la carcinomatose
péritonéale: utopie ou réalité?
Isabelle Deshaies, MD, FRCSC
Objectifs
• Pouvoir discuter de la différence entre les métastases péritonéales et les métastases d’organes • Connaître les principes de base de la CHIP et les résultats attendus • Identifier les pathologies pour lesquelles une CHIP pourrait être indiquée et discuter de la sélection des patients • Diriger les candidats potentiels vers les ressources appropriées d’évaluation
Conflits d’intérêts
• Comité aviseur Nexavar (Bayer)
Concepts de bases
• Surface péritoine = Surface corporelle totale • 90% péritoine viscéral vs 10% pariétal
• « Barrière péritonéale » • Clairance 1/√Poids moléculaire • Lipophile ou non
• « Efficacité métastatique » élevée • Se défend moins bien contre les cellules tumorales
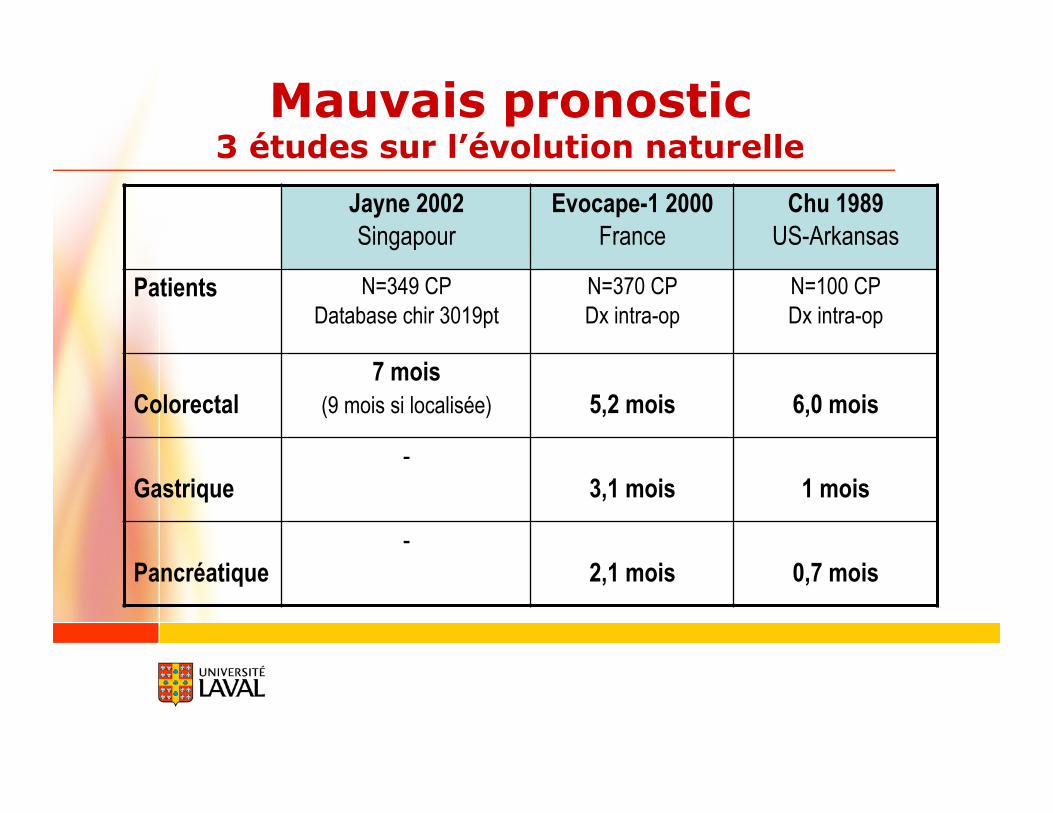
Mauvais pronostic 3 études sur l’évolution naturelle
Jayne 2002 Singapour
Evocape-1 2000 France
Chu 1989 US-Arkansas
Patients N=349 CP Database chir 3019pt
N=370 CP Dx intra-op
N=100 CP Dx intra-op
Colorectal 7 mois
(9 mois si localisée) 5,2 mois 6,0 mois
Gastrique -
3,1 mois 1 mois
Pancréatique -
2,1 mois 0,7 mois
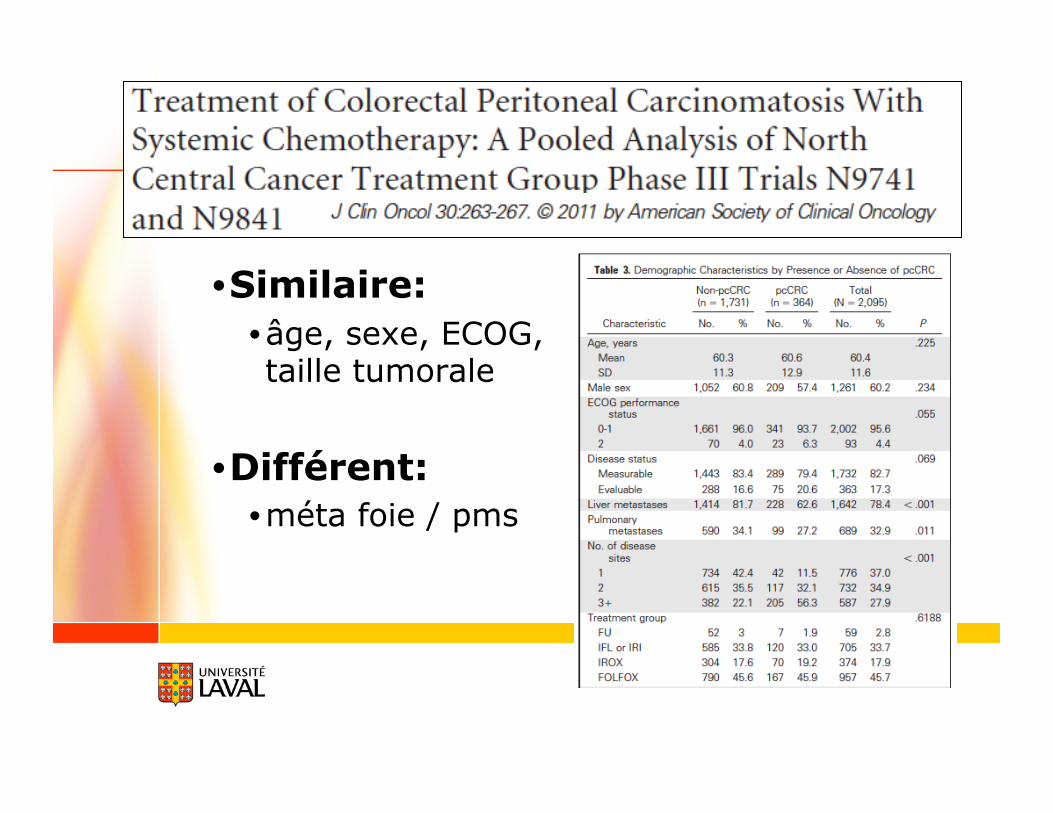
• Similaire: • âge, sexe, ECOG, taille tumorale
• Différent: • méta foie / pms
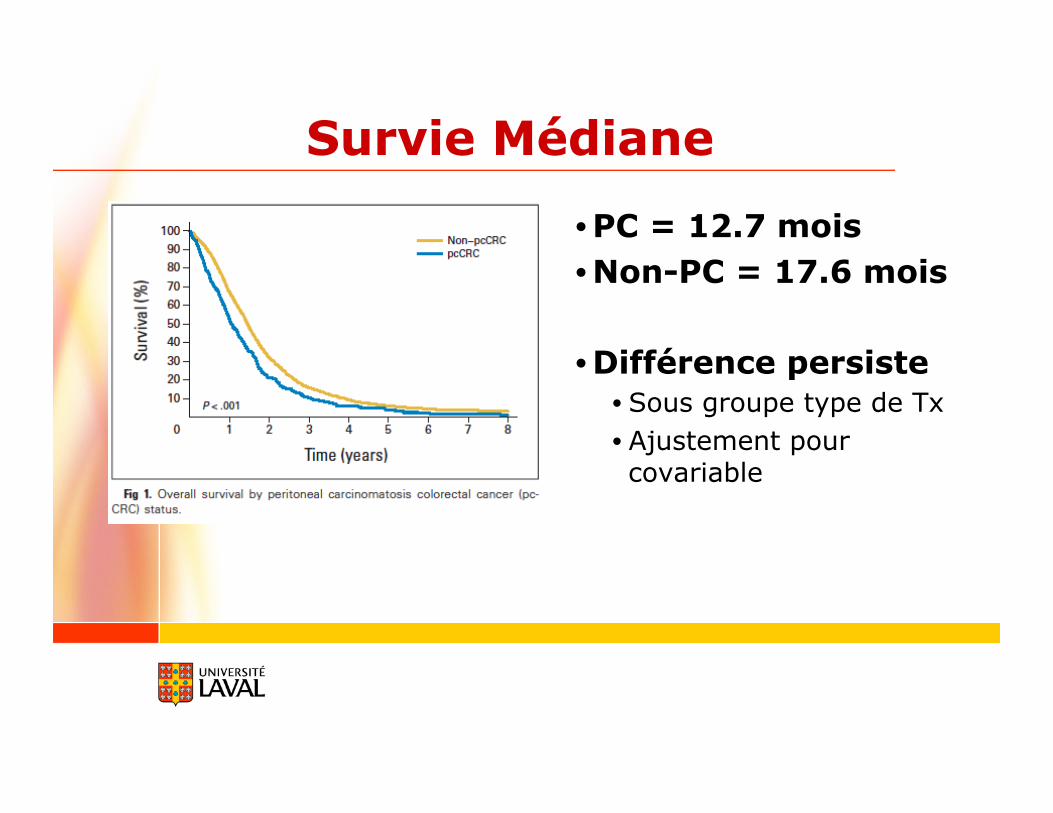
Survie Médiane
• PC = 12.7 mois • Non-PC = 17.6 mois
• Différence persiste • Sous groupe type de Tx • Ajustement pour covariable
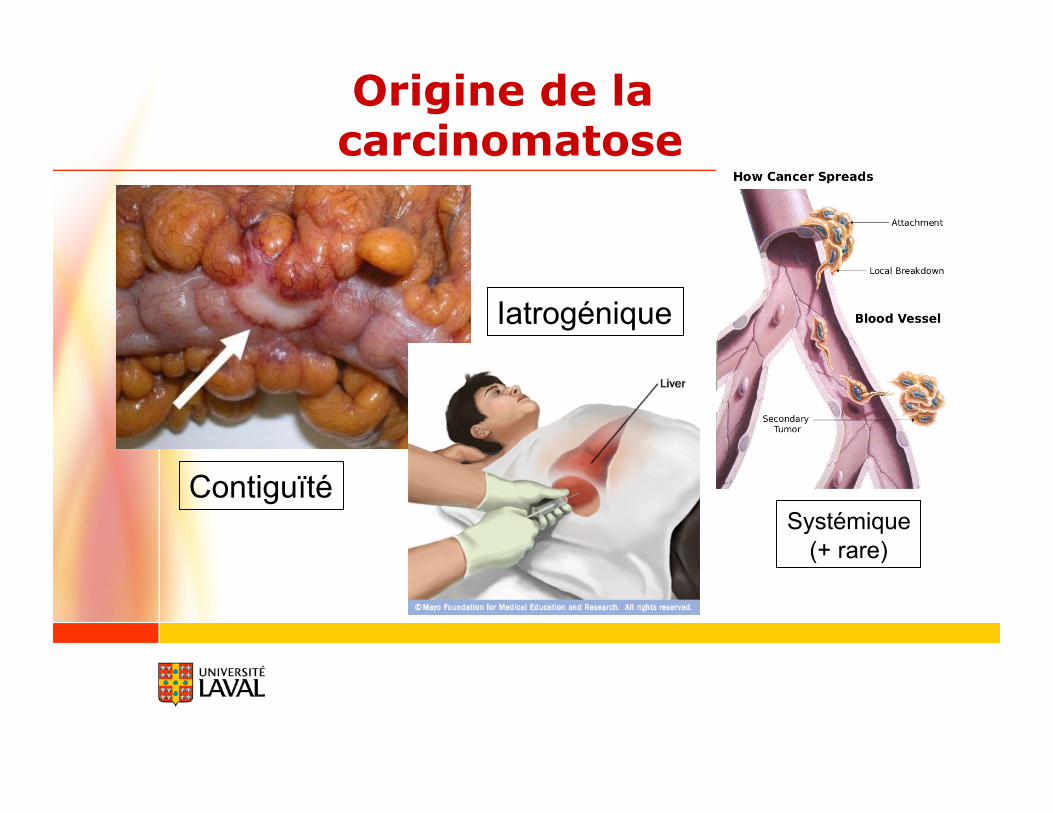
Origine de la carcinomatose
Contiguïté
Iatrogénique
Systémique (+ rare)
Étiologie
2/3 Digestive 50% colo-rectal 20% gastrique
20% Pancréatique
1/3 Non Digestive > 50% ovaire
Pms, sein,mélanome mésothéliome
Essaimage surtout par contiguité
Concepts de base • Peut être le seul site métastatique • Autres voies de dissémination que sang et lymphe • Même des cellules très bien différenciées peuvent s’implanter (pseudomyxome) • Maladie « loco-régionale »
• Péritoine relativement isolée de la chimiothérapie systémique
Besoin d’un Tx local agressif
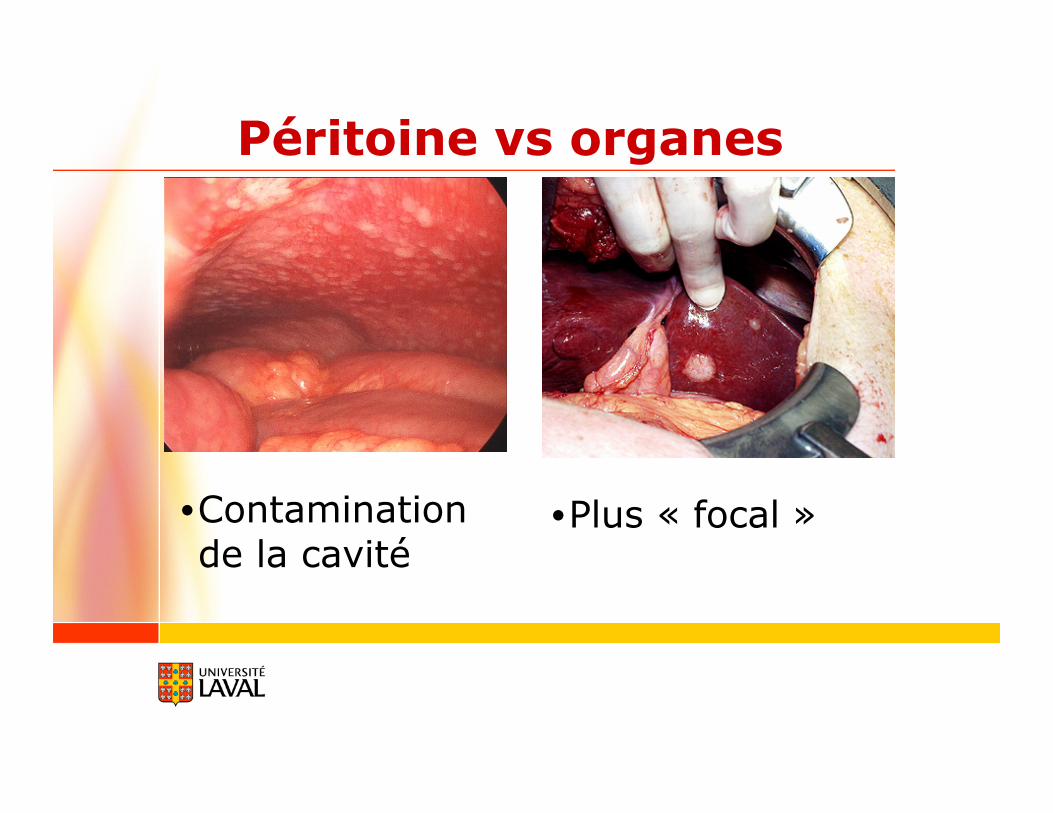
Péritoine vs organes
• Contamination de la cavité
• Plus « focal »
CHIP : 2 Principes clefs
1) Cytoréduction complète (macroscopique) Pas d’autres sites métastatiques Résection complète du cancer Étendue acceptable Bonne QOL post-op: pas de grêle court…
2) Traiter la cavité (microscopique) Traite les cellules isolées < 1-2 mm Traitement à base de chimiotx et hyperthermie
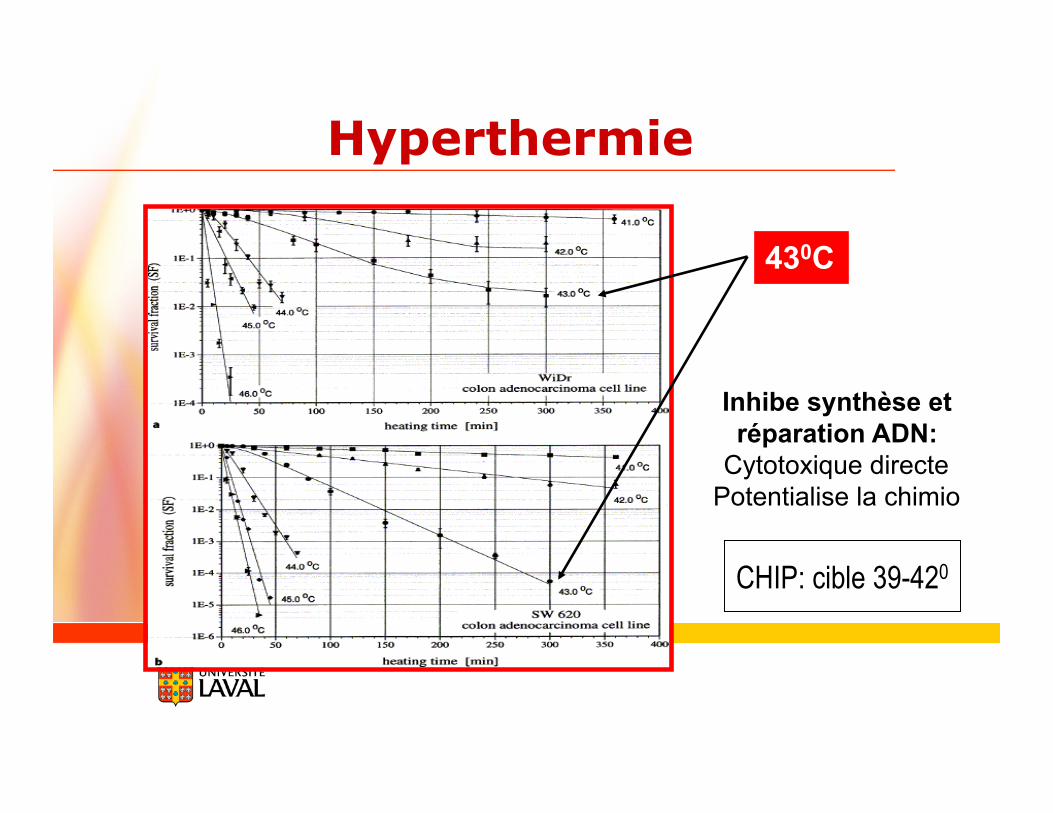
Hyperthermie
430C
Inhibe synthèse et réparation ADN:
Cytotoxique directe Potentialise la chimio
CHIP: cible 39-420
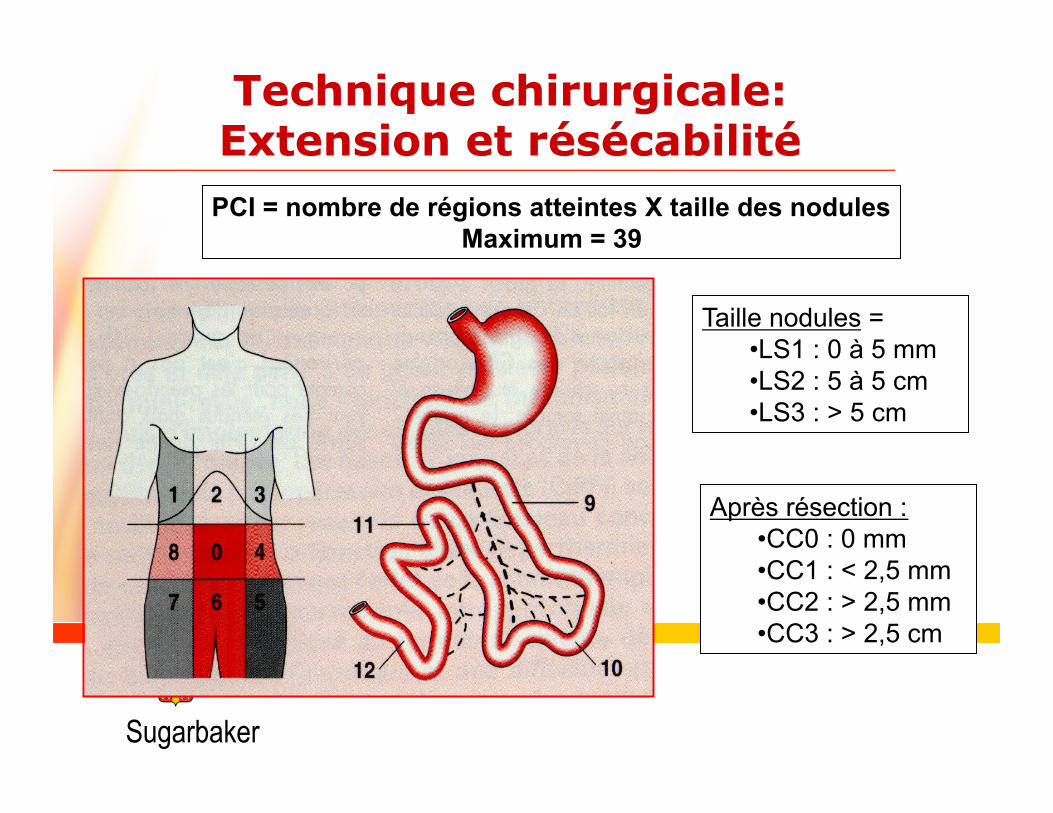
Technique chirurgicale: Extension et résécabilité PCI = nombre de régions atteintes X taille des nodules
Maximum = 39
Taille nodules = • LS1 : 0 à 5 mm • LS2 : 5 à 5 cm • LS3 : > 5 cm
Après résection : • CC0 : 0 mm • CC1 : < 2,5 mm • CC2 : > 2,5 mm • CC3 : > 2,5 cm
Sugarbaker
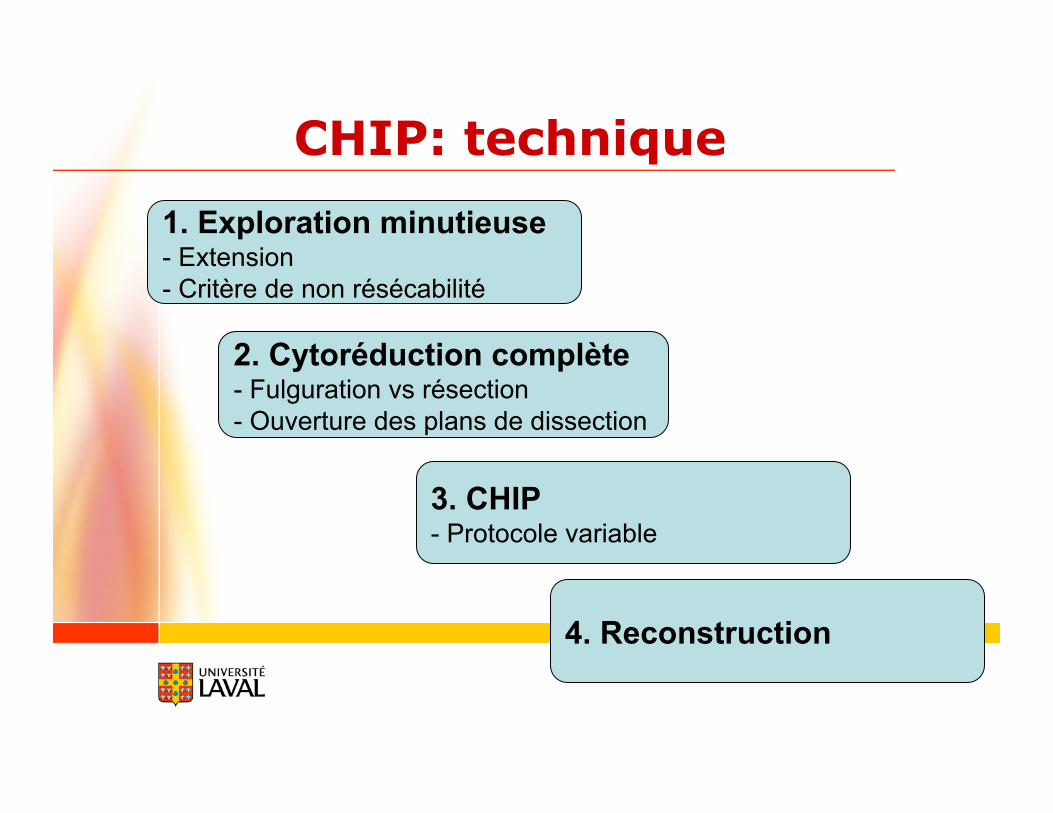
CHIP: technique
1. Exploration minutieuse - Extension - Critère de non résécabilité
2. Cytoréduction complète - Fulguration vs résection - Ouverture des plans de dissection
3. CHIP - Protocole variable
4. Reconstruction
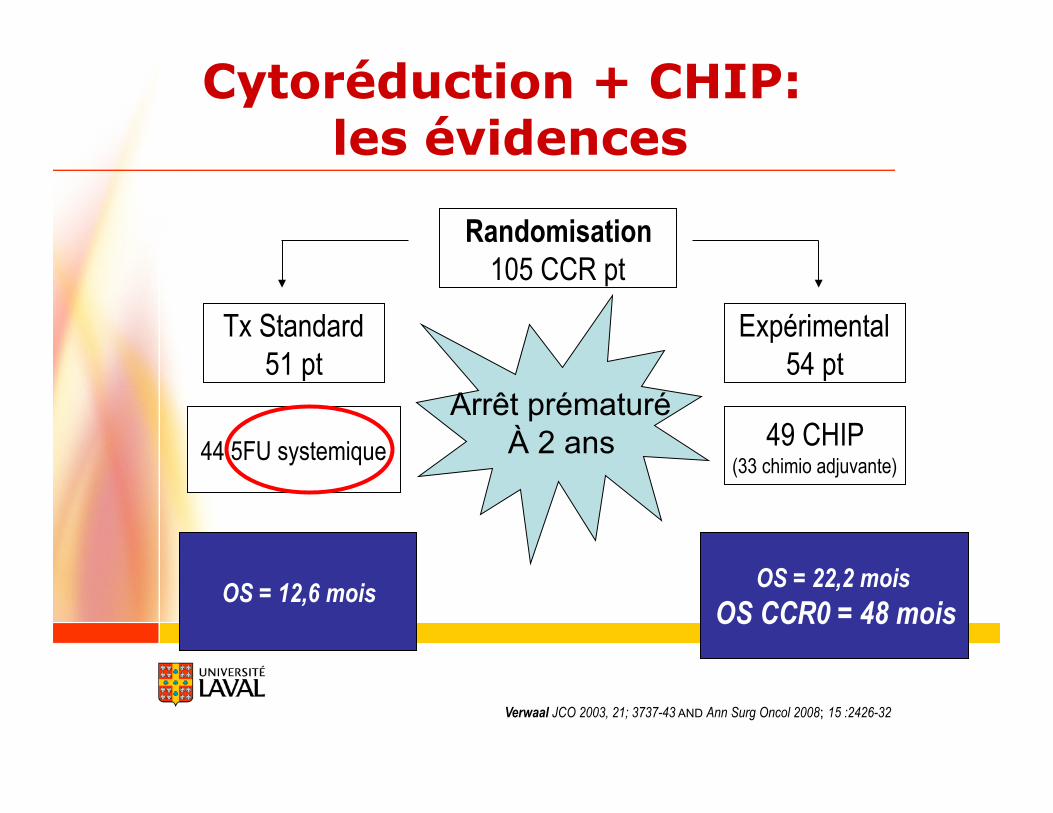
Cytoréduction + CHIP: les évidences
Verwaal JCO 2003, 21; 3737-43 AND Ann Surg Oncol 2008; 15 :2426-32
44 5FU systemique
Expérimental 54 pt
Tx Standard 51 pt
Randomisation 105 CCR pt
49 CHIP (33 chimio adjuvante)
OS = 12,6 mois OS = 22,2 mois OS CCR0 = 48 mois
Arrêt prématuré À 2 ans
Pas d’autres études de phase III…
• ACOSOG Z 6091 sur traitement standard avec ou sans HIPEC fermée prématurément (1 pt inclus en 2 ans…)
• Similaire aux données sur les hépatectomies pour métastases (aucune étude de phase III)
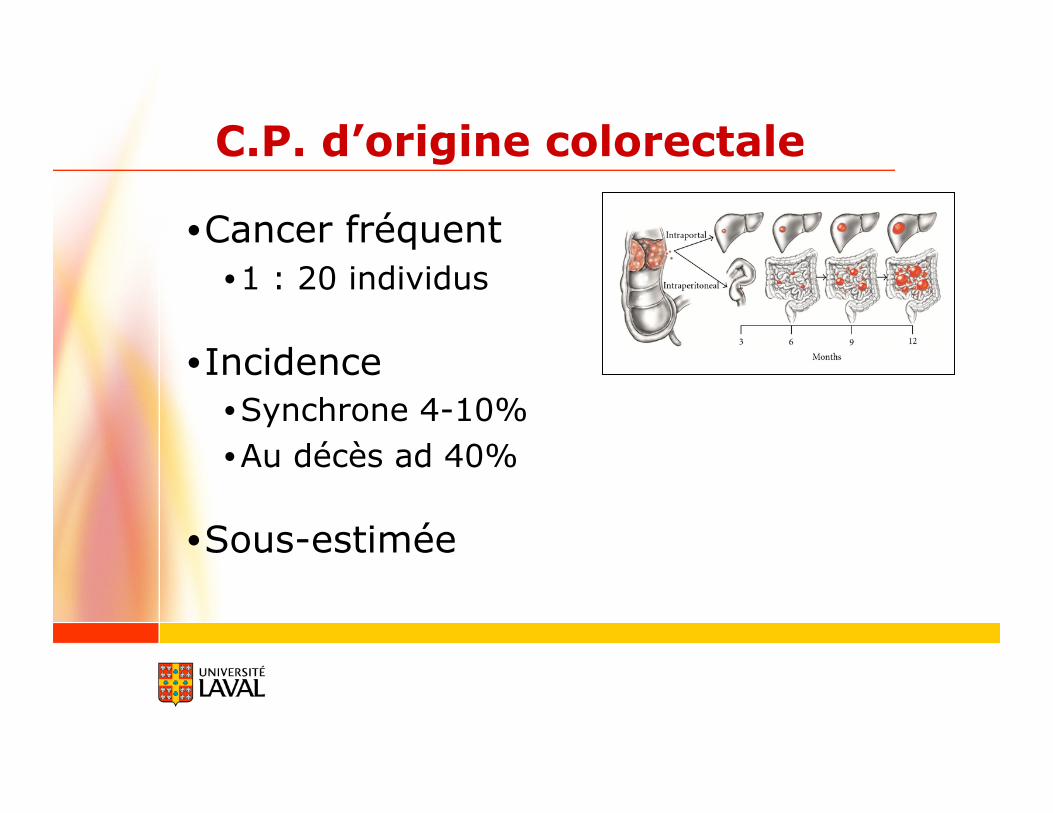
C.P. d’origine colorectale
• Cancer fréquent • 1 : 20 individus
• Incidence • Synchrone 4-10% • Au décès ad 40%
• Sous-estimée
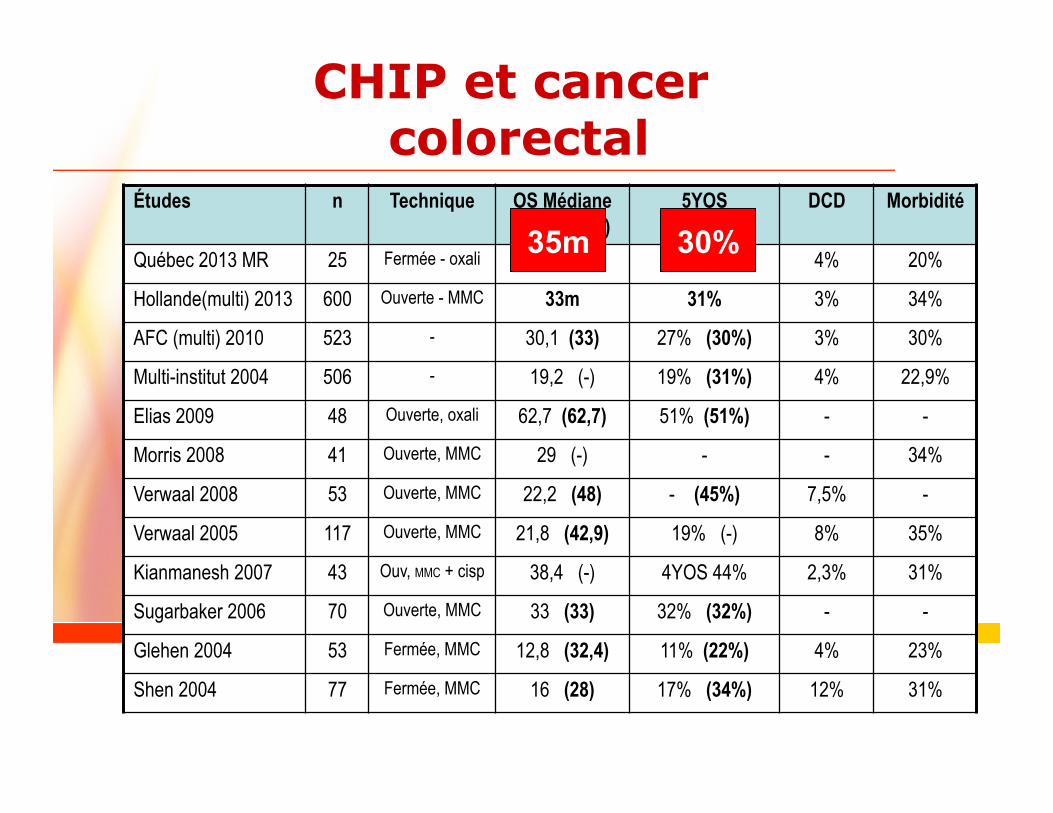
CHIP et cancer colorectal
Études n Technique OS Médiane Mois (CC-0)
5YOS % (CC-0)
DCD Morbidité
Québec 2013 MR 25 Fermée - oxali 36% 4% 20%
Hollande(multi) 2013 600 Ouverte - MMC 33m 31% 3% 34%
AFC (multi) 2010 523 - 30,1 (33) 27% (30%) 3% 30%
Multi-institut 2004 506 - 19,2 (-) 19% (31%) 4% 22,9%
Elias 2009 48 Ouverte, oxali 62,7 (62,7) 51% (51%) - -
Morris 2008 41 Ouverte, MMC 29 (-) - - 34%
Verwaal 2008 53 Ouverte, MMC 22,2 (48) - (45%) 7,5% -
Verwaal 2005 117 Ouverte, MMC 21,8 (42,9) 19% (-) 8% 35%
Kianmanesh 2007 43 Ouv, MMC + cisp 38,4 (-) 4YOS 44% 2,3% 31%
Sugarbaker 2006 70 Ouverte, MMC 33 (33) 32% (32%) - -
Glehen 2004 53 Fermée, MMC 12,8 (32,4) 11% (22%) 4% 23%
Shen 2004 77 Fermée, MMC 16 (28) 17% (34%) 12% 31%
35m 30%
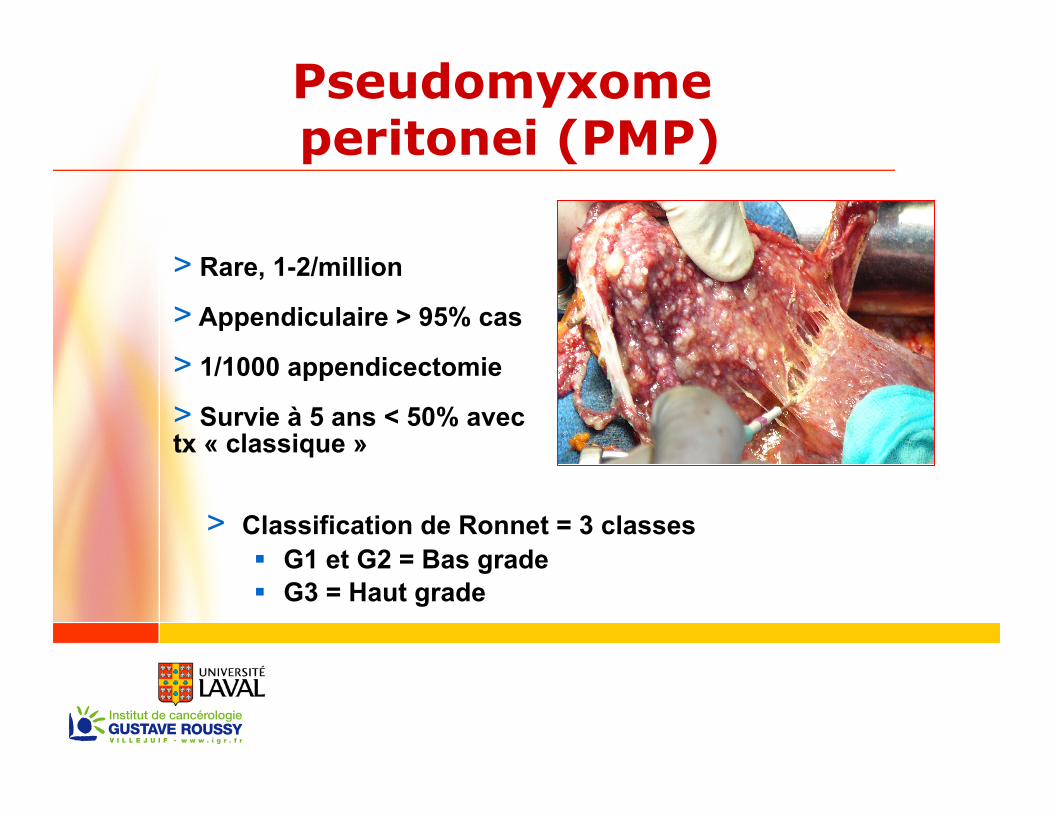
Pseudomyxome peritonei (PMP)
> Classification de Ronnet = 3 classes G1 et G2 = Bas grade G3 = Haut grade
> Rare, 1-2/million
> Appendiculaire > 95% cas
> 1/1000 appendicectomie
> Survie à 5 ans < 50% avec tx « classique »
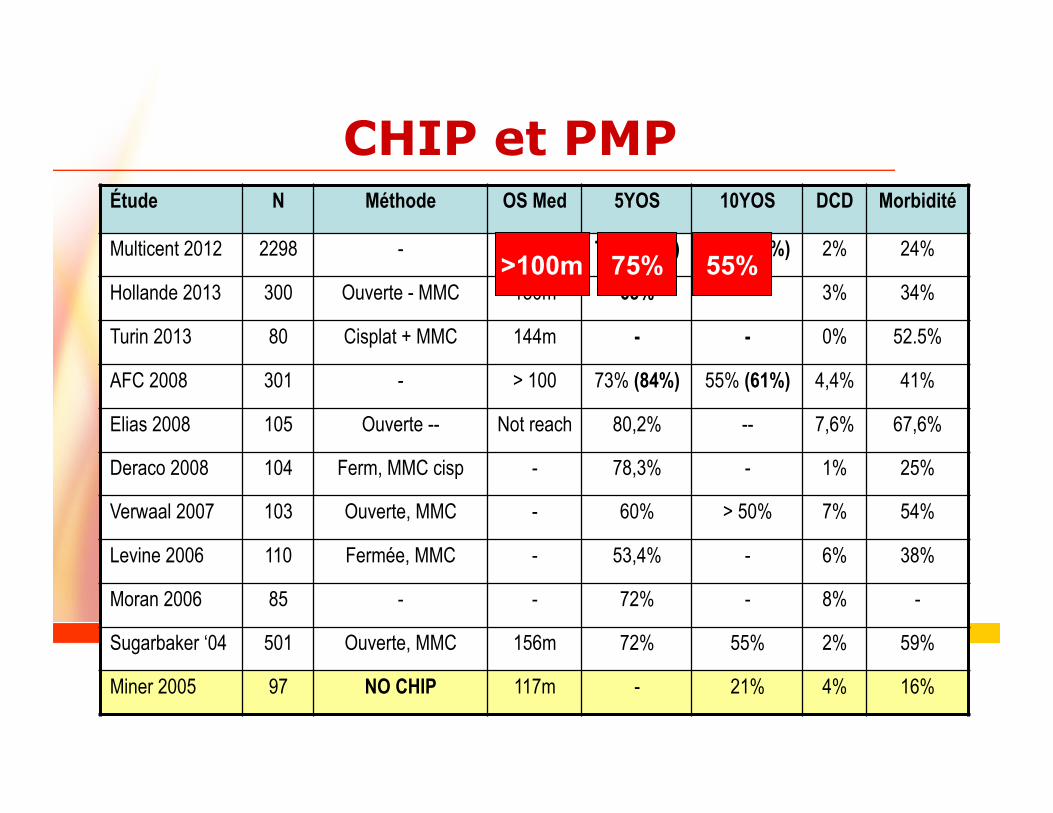
CHIP et PMP Étude N Méthode OS Med 5YOS 10YOS DCD Morbidité
Multicent 2012 2298 - 196m 74% (85%) 63% (75%) 2% 24%
Hollande 2013 300 Ouverte - MMC 130m 65% - 3% 34%
Turin 2013 80 Cisplat + MMC 144m - - 0% 52.5%
AFC 2008 301 - > 100 73% (84%) 55% (61%) 4,4% 41%
Elias 2008 105 Ouverte -- Not reach 80,2% -- 7,6% 67,6%
Deraco 2008 104 Ferm, MMC cisp - 78,3% - 1% 25%
Verwaal 2007 103 Ouverte, MMC - 60% > 50% 7% 54%
Levine 2006 110 Fermée, MMC - 53,4% - 6% 38%
Moran 2006 85 - - 72% - 8% -
Sugarbaker ‘04 501 Ouverte, MMC 156m 72% 55% 2% 59%
Miner 2005 97 NO CHIP 117m - 21% 4% 16%
>100m 75% 55%
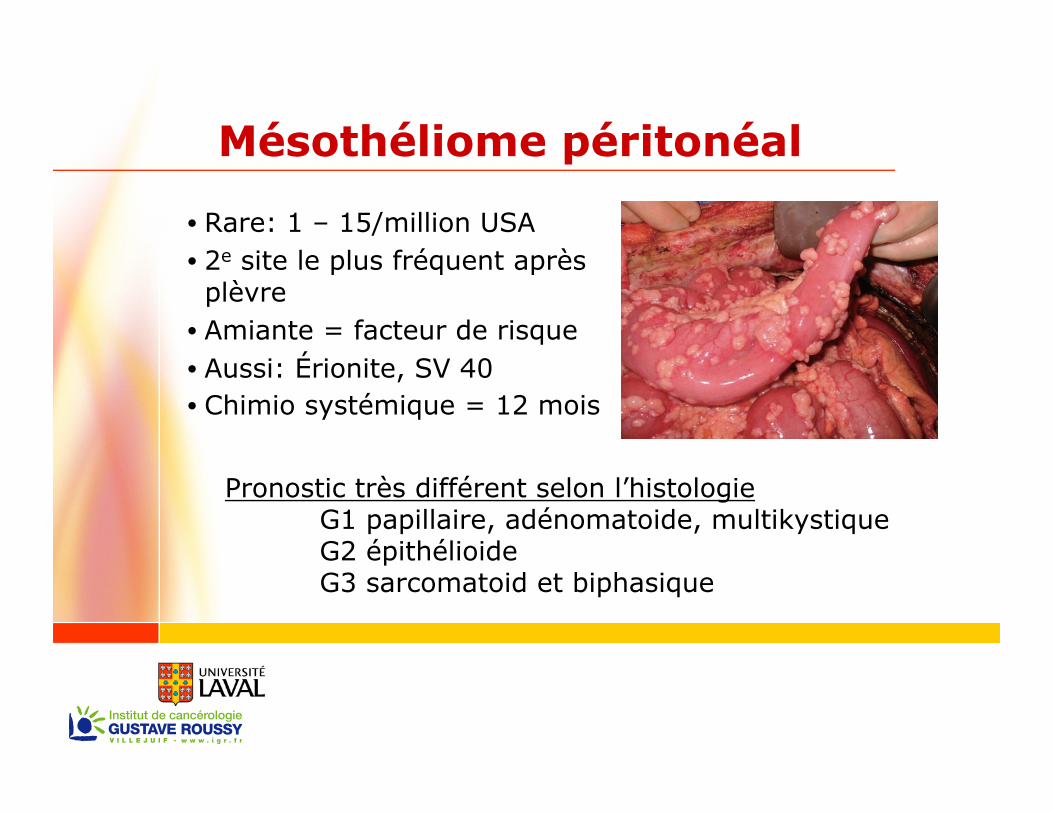
Mésothéliome péritonéal
• Rare: 1 – 15/million USA • 2e site le plus fréquent après plèvre • Amiante = facteur de risque • Aussi: Érionite, SV 40 • Chimio systémique = 12 mois
Pronostic très différent selon l’histologie G1 papillaire, adénomatoide, multikystique G2 épithélioide G3 sarcomatoid et biphasique
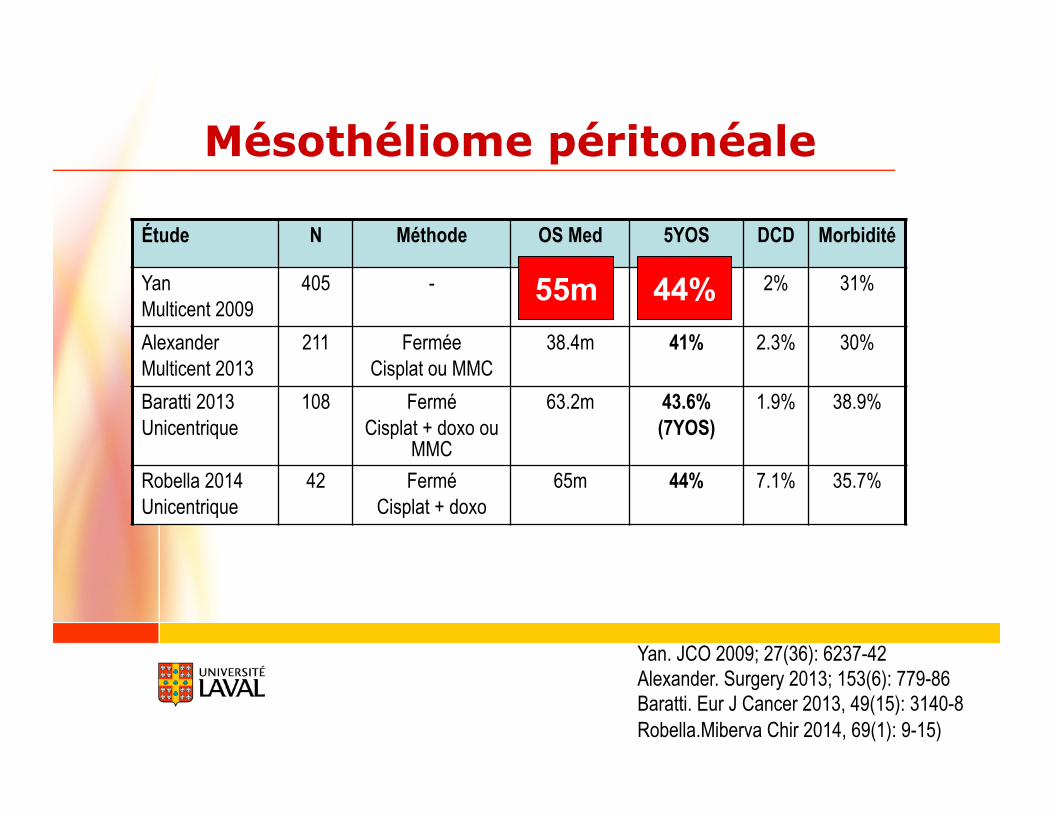
Mésothéliome péritonéale
Étude N Méthode OS Med 5YOS DCD Morbidité
Yan Multicent 2009
405 - 53m (94m) 47% 2% 31%
Alexander Multicent 2013
211 Fermée Cisplat ou MMC
38.4m 41% 2.3% 30%
Baratti 2013 Unicentrique
108 Fermé Cisplat + doxo ou
MMC
63.2m 43.6% (7YOS)
1.9% 38.9%
Robella 2014 Unicentrique
42 Fermé Cisplat + doxo
65m 44% 7.1% 35.7%
Yan. JCO 2009; 27(36): 6237-42 Alexander. Surgery 2013; 153(6): 779-86 Baratti. Eur J Cancer 2013, 49(15): 3140-8 Robella.Miberva Chir 2014, 69(1): 9-15)
55m 44%
CHIP et autres cancers
• Estomac • Études surtout japonaises • Phase III n=68 pt (34 CHIP) • OS 6.5m vs 11m (CHIP) • 3YOS 0% vs 5.9%
• AFC peu encourageant (OS: 7 mois)
• Ovaire • Bonne survie avec cytoréduction + chimio systémique • CHIP pour cancer récidivant?
• Autres cancers: anecdotique
Pourquoi la CHIP demeure peu acceptée / utilisée par les médecins?
1) Croyance répandue que la C.P. est une maladie incurable
2) Taux rapporté de mortalité et morbidité de la CHIP initialement élevé
3) Pas de grandes études de phase III disponible, critique du « biais de sélection »
4) Peu de centres offrent ce traitement
Cytoréduction + CHIP =
Survie long terme BEG
CP Isolée
Toujours est-il que…
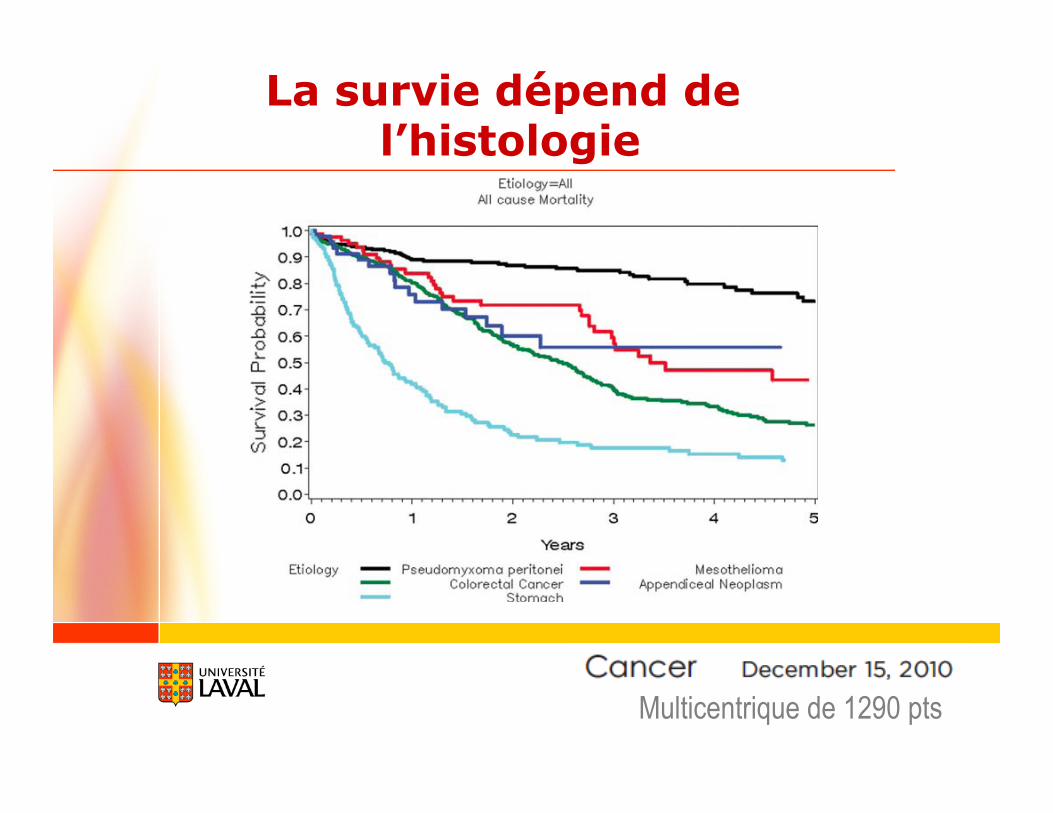
La survie dépend de l’histologie
Multicentrique de 1290 pts
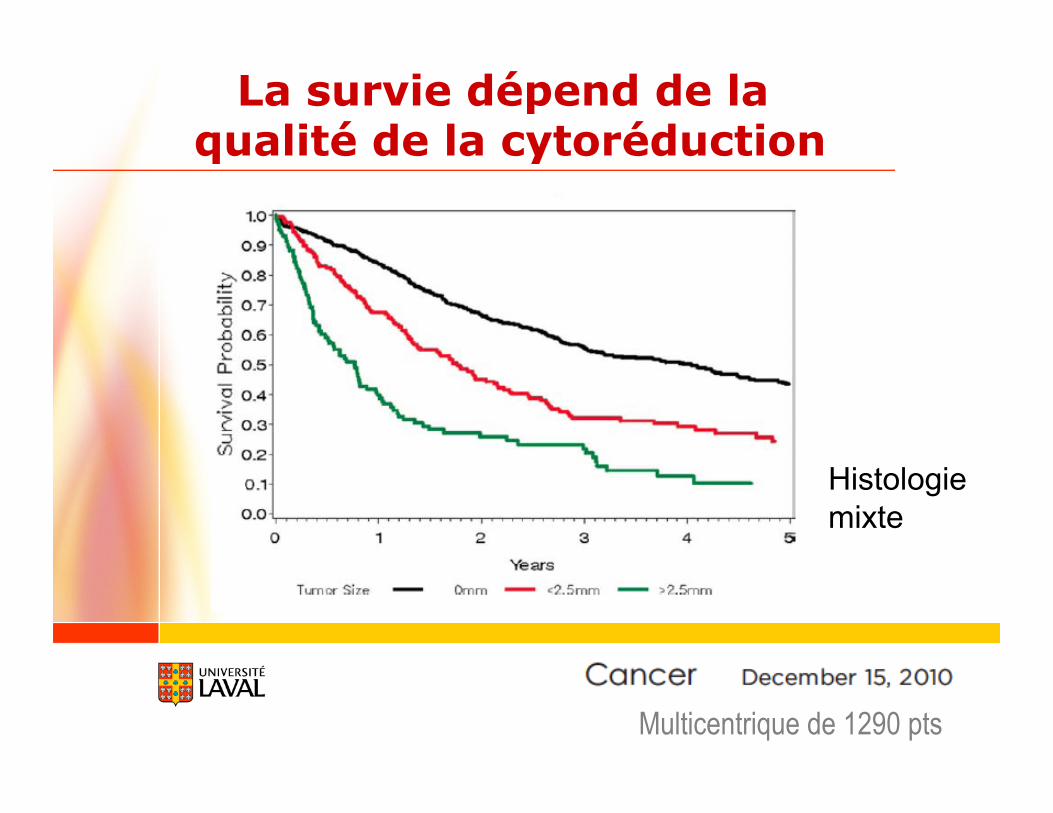
La survie dépend de la qualité de la cytoréduction
Histologie mixte
Multicentrique de 1290 pts
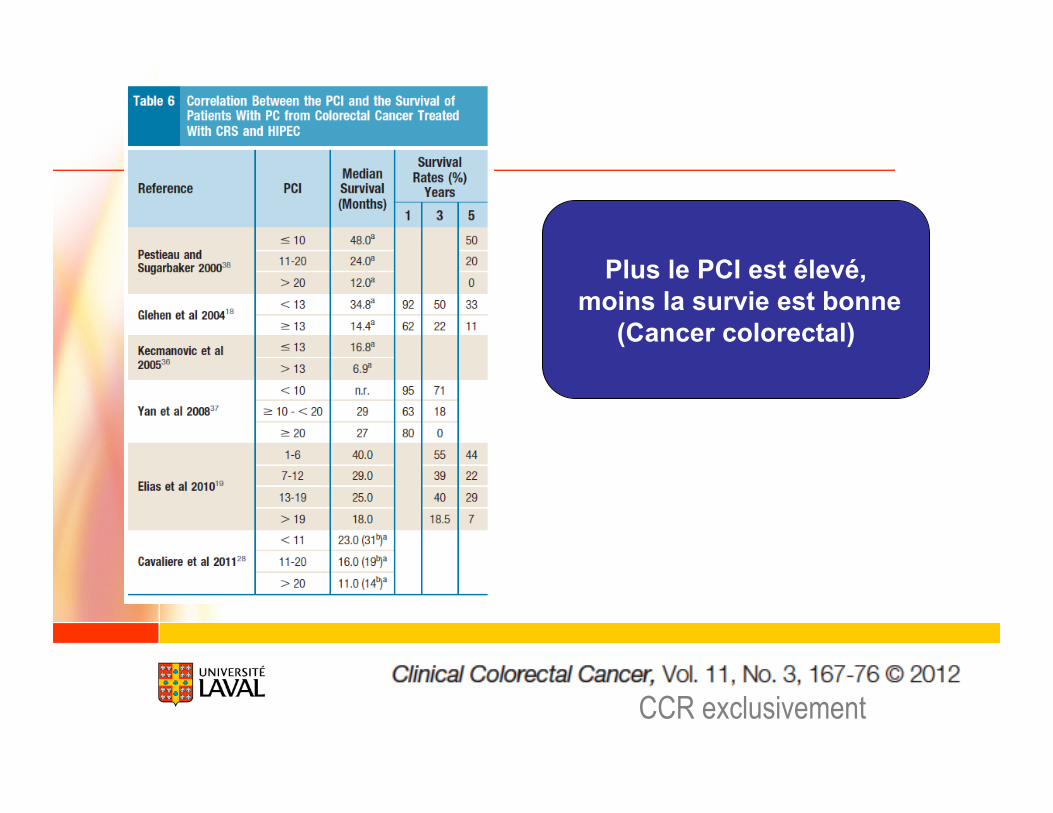
CCR exclusivement
Plus le PCI est élevé, moins la survie est bonne
(Cancer colorectal)
Sélection des patients
1) Histologie tumorale Pseudomyxome péritonei Mésothéliome péritonéale Adénok colorectal et appendiculaire PCI < 16-20
2) Étendue de la maladie Cytoréduction complète possible Pas de métastases (extra-abdominales) Pas de grêle court
3) Bon état de santé global Âge < 65 – 70 ans
Centre de référence
• Hôpital Maisonneuve-Rosemont • Dr Pierre Dubé • Dr Lucas Sidéris
• Hôpital Notre Dame • Dr Rami Younan
• RUIS McGill
Conclusion
• La carcinomatose péritonéale est différente des autres types de métastases, il faut initialement la considérer comme une maladie locorégionale
• Pour des patients très sélectionnés, la chirurgie de cytoréduction complète associée à la CHIP peut être curative
Bibliographie • Elias, Gilly, Glehen & al., Carcinose péritonéales d’origines digestives et
primitives, Arnette 2008 • Esquivel & al., Cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy in the management of peritoneal surface malignancies of colonic origin: a consensus statement, Ann Surg Oncol 2007, 14: 128-33
• Esquivel & al., Consensus statement on the locoregional treatment of colorectal cancer with peritoneal dissemination, J Surg Oncol 2008; 98: 263-7
• Jayne & al., Peritoneal carcinomatosis from colorectal cancer, BJS 2002; 89: 1545-1550
• Sadeghi & al., Peritoneal carcinomatosis from non-gynecologic malignacies: results of the EVOCAPE-1 multicentric prospective study, Cancer 2000; 68: 58-64
• Chu & al., Peritoneal carcinomatosis in nongynecologic malignacy: a prospective study of prognostic factors, Cancer 1989; 63: 364-367
• Butler & al., Small bowel obstruction in patients with a prior history of cancer, Am J Surg 1991; 162: 624-28
• Glehen & al., Cytoreduction surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study, JCO 2004; 22: 3284-92
Bibliographie-suite • DaSilva, Sugarbaker & al, Analysis of prognostic factors in seventy patients
having a complete cytoreduction plus perioperative intraperitoneal chemotherapy for carcinomatosis from colorectal origin, J Am Coll Surg 2006; 203: 878-86
• Kianmanesh & al., Iterative cytoreductive surgery associated with hyperthermic intraperitoneal chemotherapy for the treatement of peritoneal carcinomatosis of colorectal origin with or without liver metastasis, Ann Surg 2007, 245: 597-603
• Shen & al., Cytoreductive surgery and intraperitoneal chemotherapy with Mitomycin C for peritoneal carcinomatosis from nonappendiceal colorectal carcinoma, Ann Surg Oncol 2004, 11: 178-86
• Yan, Morris & al., Cytoreductive surgery and perioperative intraperitoneal chemotherapy for isolated colorectal peritoneal carcinomatosis: experimental therapy or standard of care? Ann Surg 2008; 248: 829-35
• Smeenk & al., Appendiceal neoplasms & pseudomyxoma peritonei: a population based study, Eur J Surg Oncol 2008; 34: 196-201
• Bradley & al., Pseudomyxoma peritonei: review of the controversy. Current Diagnostic Pathology 2007; 13: 410-6
• Smeenk, Verwaal& al., Survival analysis of pseudomyxoma peritonei patients treated by cytoreductuve surgery and hyperthermic intraperitoneal chemotherapy, Ann Surg 2007, 245 : 104-9
Bibliographie-suite • Gozalez-moreno, Sugarbaker & al., Right-hemicolectomy does not confer a
survival advantage in patient with mucinous carcinoma of the appendix and peritoneal seeding, BJS 2004; 91:304-311
• Deraco& al., Peritonectomy & intraperitoneal hyperthermic perfusion : a strategy that have confirmed its efficacy in patients with pseudomyxoma peritonei, Ann Surg Oncol 2004, 11; 393-8
• Moran & al., Operability and early outcomes in 100 consecutive laparotomies for peritoneal malignacies, Br J Surg 2006, 93; 100-4
• Yan & al., Cytoreductive surgery & intraperitoneal chemotherapy for pseudomyxoma peritonei from appendiceal mucinous neoplasm, BJS 2006; 93 : 1270-76
• Miner & al., Long term survival following treatment for pseudomyxoma peritonei, Ann Surg 2005, 241 : 300-8
• Feldman, Alexandre & al, Analysis of factors associated with outcomes in patients with malignant peritoneal mesothelioma undergoing debulking and intra-peritoneal chemotherapy,J Clin Oncol 2003, 21: 4560-7
• Deraco & al., Prognosis analysis of clinicopathologic factors in 49 patients with diffuse malignant peritoneal mesothelioma treated with cytoreductive surgery and intraperitoneal hyperthermic perfusion Ann Surg Oncol 2006, 13; 229-37
Bibliographie suite • Legendre & al., Survival and quality of life after palliative surgery for neoplastic
gastrointestinal obstruction, Eur J Surg Oncol 2001, 27: 364-7 • Mangili & al., Palliative care for intestinal obstruction in recurrent ovarian cancer : a
multivariate analysis, Int J Gynecol Cancer 2005, 15: 830-5 • Woolfson & al., Management of bowel obstruction in patients with abdominal cancer, Arch
Surg 1997, 132: 1093-7 • Gervais et al. Cytoreductive surgery plus HIPEC with oxaliplatin for peritoneal carcinomatosis
arising from colorectal cancer, J Surg Oncol 2013, 108(7): 438-43 • Robella et al., Treatment of peritoneal carcinomatosis from colonic cancer by cytoreductive,
peritonectomie and HIPEC: preliminary results in highly selected patients. Minerva Chir 2013, 68(6): 551-8
• Robella et al. Treatment of pseudomyxoma peritonei by cytoreductive surgery and HIPEC: a single center experience. Minerva chir 2013, 68(6): 569-77
• Glehen et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Cancer2010, 5608-18
Bibliographie suite • Elias & al., Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with
oxaliplatin for peritoneal carcinomatosis of colorectal origin JCO 2009; 27: 681-5 • Glehen & al, Intraperitoneal chemotherapy & attempted cytoreductive surgery in patient with
peritoneal carcinomatosis of colorectal origin, BJS 2004; 91: 747-54 • Verwall & al, Long term survival of peritoneal carcinomatosis of colorectal origin, Ann Surg
Oncol 2005; 12: 65-71 • Elias & al., Peritoneal pseudomyxoma: results of systematic policy of complete cytoreductive
surgery and intraperitoneal hyperthermic chemotherapy, BJS 2008; 95: 1164-71 • Levine, Sugarbaker & al., Appendiceal Neoplasms with peritoneal dissemination: outcomes
after cytoreductive surgery and intraperitoneal hyperthermic chemotherapy, Ann Surg Oncol 2006; 13: 624-34
• Elias & al., Malignant peritoneal mesothelioma: treatement with maximal cytoreductive surgery plus intraperitoneal chemotherapyGastroenterol Clin Biol 2007, 31: 784-8
• Sugarbaker & al., Comprehensive management of diffuse malignant peritoneal mesothelioma, Eur J Surg Oncol 2006, 32; 686-91
• Chua et al., Early and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. JCO 2012, 30(20): 2449-56
• Kuijpers et al., Cytoreductuve and HIPEC in the Netherlands: a nationwide long-term outcome following the dutch protocol, Am Surg Oncol 2013; 20: 4224-30