The importance of clinician, patient and researcher ......REVIEW The importance of clinician,...
10
REVIEW The importance of clinician, patient and researcher collaborations in Alport syndrome Michelle N. Rheault 1 & Judith Savige 2 & Michael J. Randles 3 & André Weinstock 4 & Melissa Stepney 5 & A Neil Turner 6 & Gina Parziale 4 & Oliver Gross 7 & Frances A Flinter 8 & Jeffrey H Miner 9 & Sharon Lagas 4 & Susie Gear 10 & Rachel Lennon 3,11 Received: 24 February 2019 /Accepted: 15 March 2019 /Published online: 1 May 2019 Abstract Alport syndrome is caused by mutations in the genes COL4A3, COL4A4 or COL4A5 and is characterised by progressive glomerular disease, sensorineural hearing loss and ocular defects. Occurring in less than 1:5000, Alport syndrome is a rare genetic disorder but still accounts for >1% of the prevalent population receiving renal replacement therapy. There is also increasing awareness about the risk of chronic kidney disease in individuals with heterozygous mutations in Alport syndrome genes. The mainstay of current therapy is the use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, yet potential new therapies are now entering clinical trials. The 2017 International Workshop on Alport Syndrome in Glasgow was a pre-conference workshop ahead of the 50th anniversary meeting of the European Society for Pediatric Nephrology. It focussed on updates in clinical practice, genetics and basic science and also incorporated patient perspectives. More than 80 international experts including clinicians, geneticists, researchers from academia and industry, and patient representatives took part in panel discussions and breakout groups. This report summarises the workshop proceedings and the relevant contemporary literature. It highlights the unique clinician, patient and researcher collaborations achieved by regular engagement between the groups. Keywords Alport syndrome . COL4A3 . COL4A4 . COL4A5 . Type IV collagen . Basement membrane Introduction The 2017 International Workshop on Alport syndrome took place in Glasgow and was formally designated as a pre- conference meeting prior to the 50th anniversary meeting of the European Society for Paediatric Nephrology (ESPN). Following on from the previous highly successful workshops in Oxford (2014) [1] and Göttingen (2015) [2], the meeting brought together patients, researchers, clinicians and industry participants from across the world. This review of the work- shop proceedings and the contemporary literature highlights the key updates in the following dominant themes that were * Rachel Lennon [email protected] 1 Department of Pediatrics, University of Minnesota Masonic Children’ s Hospital, Minneapolis, MN, USA 2 Department of Medicine, Royal Melbourne Hospital, Victoria, Australia 3 Wellcome Centre for Cell-Matrix Research, Division of Cell Matrix Biology and Regenerative Medicine, School of Biological Sciences, Faculty of Biology Medicine and Health, University of Manchester, Manchester, UK 4 Alport Syndrome Foundation, Phoenix, AZ, USA 5 Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK 6 Renal Medicine, Royal Infirmary, University of Edinburgh, Edinburgh, UK 7 Clinic of Nephrology and Rheumatology, University Medicine Goettingen, Goettingen, Germany 8 Department of Clinical Genetics, Guy’ s & St Thomas’ NHS Foundation Trust, London, UK 9 Division of Nephrology, Washington University School of Medicine, St Louis, MO, USA 10 Alport UK, Tetbury, UK 11 Department of Paediatric Nephrology, Royal Manchester Children’ s Hospital, Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, UK Pediatric Nephrology (2020) 35:733–742 https://doi.org/10.1007/s00467-019-04241-7 # The Author(s) 2019
Transcript of The importance of clinician, patient and researcher ......REVIEW The importance of clinician,...

REVIEW
The importance of clinician, patient and researcher collaborationsin Alport syndrome
Michelle N. Rheault1 & Judith Savige2& Michael J. Randles3 & André Weinstock4 & Melissa Stepney5 & A Neil Turner6 &
Gina Parziale4& Oliver Gross7 & Frances A Flinter8 & Jeffrey H Miner9 & Sharon Lagas4 & Susie Gear10 &
Rachel Lennon3,11
Received: 24 February 2019 /Accepted: 15 March 2019 /Published online: 1 May 2019
AbstractAlport syndrome is caused by mutations in the genes COL4A3, COL4A4 or COL4A5 and is characterised by progressiveglomerular disease, sensorineural hearing loss and ocular defects. Occurring in less than 1:5000, Alport syndrome is a raregenetic disorder but still accounts for > 1% of the prevalent population receiving renal replacement therapy. There is alsoincreasing awareness about the risk of chronic kidney disease in individuals with heterozygous mutations in Alport syndromegenes. The mainstay of current therapy is the use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers,yet potential new therapies are now entering clinical trials. The 2017 International Workshop on Alport Syndrome in Glasgowwas a pre-conference workshop ahead of the 50th anniversary meeting of the European Society for Pediatric Nephrology. Itfocussed on updates in clinical practice, genetics and basic science and also incorporated patient perspectives. More than 80international experts including clinicians, geneticists, researchers from academia and industry, and patient representatives tookpart in panel discussions and breakout groups. This report summarises the workshop proceedings and the relevant contemporaryliterature. It highlights the unique clinician, patient and researcher collaborations achieved by regular engagement between thegroups.
Keywords Alport syndrome . COL4A3 . COL4A4 . COL4A5 . Type IV collagen . Basement membrane
Introduction
The 2017 International Workshop on Alport syndrome tookplace in Glasgow and was formally designated as a pre-conference meeting prior to the 50th anniversary meeting ofthe European Society for Paediatric Nephrology (ESPN).
Following on from the previous highly successful workshopsin Oxford (2014) [1] and Göttingen (2015) [2], the meetingbrought together patients, researchers, clinicians and industryparticipants from across the world. This review of the work-shop proceedings and the contemporary literature highlightsthe key updates in the following dominant themes that were
* Rachel [email protected]
1 Department of Pediatrics, University of Minnesota MasonicChildren’s Hospital, Minneapolis, MN, USA
2 Department of Medicine, Royal Melbourne Hospital,Victoria, Australia
3 Wellcome Centre for Cell-Matrix Research, Division of Cell MatrixBiology and Regenerative Medicine, School of Biological Sciences,Faculty of Biology Medicine and Health, University of Manchester,Manchester, UK
4 Alport Syndrome Foundation, Phoenix, AZ, USA5 Nuffield Department of Primary Care Health Sciences, University of
Oxford, Oxford, UK
6 Renal Medicine, Royal Infirmary, University of Edinburgh,Edinburgh, UK
7 Clinic of Nephrology and Rheumatology, University MedicineGoettingen, Goettingen, Germany
8 Department of Clinical Genetics, Guy’s & St Thomas’ NHSFoundation Trust, London, UK
9 Division of Nephrology, Washington University School ofMedicine,St Louis, MO, USA
10 Alport UK, Tetbury, UK
11 Department of Paediatric Nephrology, Royal Manchester Children’sHospital, Manchester University Hospitals NHS Foundation Trust,Manchester Academic Health Science Centre, Manchester, UK
Pediatric Nephrology (2020) 35:733–742https://doi.org/10.1007/s00467-019-04241-7
# The Author(s) 2019

covered in depth during the 3-day workshop: clinical scienceand registries, genetics, basic science and the patientperspective.
Clinical science and registries
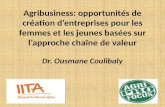
A large portion of the workshopwas focussed on the clinical careof patients with Alport syndrome including care at specific crit-ical junctions such as diagnosis, transition to adult care and preg-nancy (Fig. 1). Dr. Rachel Lennon reviewed the diagnostic eval-uation of children with persistent haematuria including the im-portance of obtaining a thorough family history. She alsodiscussed the importance of recognising the diversity of Alportsyndrome phenotypes and the role of genetic testing in diagnosisto avoid the need for an invasive kidney biopsy. Individualspresenting with early severe disease may have mutations in ad-ditional genes affecting the glomerulus such asMYO1E [3]. Dr.Lennon also reviewed the increasingly recognised phenotype ofnephrotic syndrome with focal segmental glomerulosclerosis onkidney biopsy caused bymutations in type IV collagen genes [4].
Once a diagnosis of Alport syndrome is made, the next step isdetermining a plan for follow-up and treatment. These topicswere reviewed by Drs. Clifford Kashtan and Oliver Gross.Screening for non-renal manifestations of Alport syndrome isimportant. Audiology evaluations are recommended once males
with X-linked Alport syndrome (XLAS) or males and femaleswith autosomal recessive Alport syndrome (ARAS) are 5–6 years of age. Anyone with type IV collagen mutations andovert proteinuria or clinical concern for hearing loss should haveformal audiology evaluations. Ophthalmologic manifestations ofAlport syndrome generally develop after adolescence, andscreening for males with XLAS or males and females withARAS should begin at age 15–16 years or sooner if symptom-atic. Recommendations for the treatment of Alport syndromewere published in 2013, and these remain the standard of care[5]. Based on retrospective registry data, renin-angiotensin aldo-sterone system (RAAS) blockade is recommended at the onset ofproteinuria regardless of genotype. For individuals with severemutations or family history of early (age < 30 years) end-stagekidney disease (ESKD), then treatment may be considered whenpatients are persistently microalbuminuric. Dr. Gross’s phase IIIrandomised placebo controlled study of ramipril treatment inchildren at very early stages of Alport syndrome (isolatedhaematuria or microalbuminuria) remains ongoing and is expect-ed to report after 2019 [6]. The results of this trial will help todetermine if RAAS inhibition should be recommended at evenearlier ages to slow the progression of chronic kidney disease.
Alport syndrome is often diagnosed in childhood, necessi-tating the transition of care from a paediatric to adult nephrol-ogist. Drs. Arvind Nagra and Neil Turner reviewed the suc-cessful ‘Ready Steady Go’ transition program in the UK [7].
734 Pediatr Nephrol (2020) 35:733–742
Fig. 1 Clinical care in Alport syndrome. The presentations covered patient registries, precision medicine, genetic screening and clinical trials

This program of educational materials and readiness assess-ments provides a formal way to ensure smooth transition ofchildren with kidney disease, including children with Alportsyndrome. Pregnancy is also an important time of life forwomen with Alport syndrome; however, little is known aboutoutcomes for women with this disorder [8]. Dr. Matt Hallreviewed outcomes for women with chronic kidney diseaseat the time of pregnancy and discussed improvements in bothmaternal and foetal outcomes over the past several decades[9]. Importantly, he reviewed the risks of RAAS inhibition inpregnancy as these are commonly utilised drugs in this popu-lation and known to be teratogenic.
Despite widespread use of RAAS inhibition, patients withAlport syndrome are still at risk for progression to ESKD,highlighting the need for clinical trials of novel agents in thispopulation. Prior to initiation of clinical trials, a detailed un-derstanding of the natural history and clinical and biomarkerrisk factors for progression is necessary. A number of Alportsyndrome registries are established around the world and pro-vide valuable natural history information. In addition, an in-ternational natural history study of patients with Alport syn-drome recently completed follow-up (ATHENA studyNCT02136862). At the clinical science breakout session, thegroup reviewed the current status of each of the registries andagreed to further discussion of a recommended commondataset of information to guide new registry formation andfacilitate data sharing between registries. In addition, someof the preliminary data from the ATHENA study wasreviewed and publication of results is expected in 2019. Thefirst clinical trial specifically in patients with Alport syndromestarted enrolling in 2017. This randomised, placebo-controlled trial of the NF-κB inhibitor bardoxolone(NCT03019185) is a landmark for the Alport research andpatient communities, and additional clinical trials are in vari-ous stages of planning.
The future of Alport syndrome treatment is bright. Dr.Daniel Gale reviewed the complex pathway of bringing anew drug to market including phase 1, 2 and 3 clinical trials;approval and marketing; and cost considerations. Specificchallenges for clinical trials in Alport syndrome include therare nature of the disease for successful recruiting into clin-ical trials as well as potential high costs of therapy for pa-tients if a drug is approved. Dr. Michelle Rheault reviewedthe importance of understanding the molecular pathways ofglomerular filtration barrier dysfunction in Alport syn-drome including molecular and cellular changes inpodocytes and endothelial cells in response to mechanicalstrain, as well as changes in composition of the glomerularbasement membrane (GBM) [10]. A number of agents are inclinical development for non-Alport syndrome indicationsthat may be appropriate for use in this population based onmolecular targets of drug action. For example, endothelin-1appears to be upregulated in Alport glomeruli in response to
mechanical strain and may be targeted by endothelin-1 re-ceptor antagonists currently in development [11].
Genetics
The presentations on genetics and diagnosis of Alport syn-drome demonstrated that our understanding of the value ofgenetic testing in Alport syndrome has increased greatly overthe past 18 months (Fig. 2). In many centres, gene testing hasreplaced renal biopsy for the diagnosis of Alport syndrome[12]. Identifying the underlying mutation(s) indicates themode of inheritance, enabling the targeted genetic testing ofother family members who may be at risk, as well as some-times predicting the age at onset of ESKD [13]. Furthermore,some therapies may be specifically targeted at people withmissense or nonsense variants in the future.
In addition, COL4A3, COL4A4 or COL4A5 mutations arefound in 10–30% of patients with focal and segmentalglomerulosclerosis (FSGS) [4, 14], and Dr. Moin Saleem re-ported that some patients with features consistent with steroid-resistant nephrotic syndrome had COL4A variants on screen-ing with a 70-gene renal panel.
Genetic and non-genetic factors influence the prognosis toa far greater extent than thought previously. Drs. Roser Torraand Alessandra Renieri presented data suggesting that COL44mutations result in a more severe phenotype than COL4A3mutations. In their experience, up to one third of patients withheterozygousCOL4A4mutations developed renal impairmentat an average age of 56 years. In addition, there is now evi-dence for testing for coincidental mutations in NPHS2,MYH9and ACTN4, which all influence proteinuria [3, 15, 16]. In Dr.Constantinos Deltas’ experience, up to 16% of individualswith a heterozygous COL4A3 or COL4A4 mutation developrenal impairment and 41% have FSGS. The p.R229Q variantin NPHS2 predisposes to increased proteinuria and renal fail-ure, and the Rictor gene component of the mTORC2 pathwaymay be a further modifier of renal function.
For men with XLAS, and men or women with ARAS, thegenetic results strongly predict outcome [17, 18], although theclinical coursemay bemodified significantly by screening andearly ACE inhibitor treatment [19, 20]. The debate about anappropriate nomenclature for individuals with a heterozygousCOL4A3 or COL4A4 mutation or a woman with a COL4A5mutation continues [21]. For women with a heterozygousCOL4A5 mutation, or anyone with a heterozygous COL4A3orCOL4A4 pathogenic variant, our ability to predict the futureis more constrained, but these individuals should all undergolife-long renal surveillance [22]. Published data on the risk ofESKD are skewed by ascertainment bias, with an over-representation of people with ESKD in hospital-based series.The risk of ESKD is probably lower in women with aCOL4A5mutation than historical data suggest, but still higher
Pediatr Nephrol (2020) 35:733–742 735

than in individuals with a pathogenic heterozygous COL4A3or COL4A4 variant.
Some congress participants subscribed to the view thatanyone with a heterozygous COL4A3 or COL4A4 mutationshould be diagnosed with Alport syndrome, to ensure that thesignificance of their diagnosis is appreciated and to ensureaggressive management and long-term monitoring [21].Others, while agreeing on the need for life-long follow-up,do not classify people with a single mutation as havingAlport syndrome, because of their lesser risk of ESKD andabsence of extra-renal manifestations. If every person with aheterozygous COL4A3 or COL4A4 mutation were labelledwith the diagnosis of Alport syndrome, its incidence wouldincrease from the current level of 1 in 5–10,000 to as high as 1in 100 [23, 24], with ESKD being uncommon. At the meeting,there was, however, unanimous agreement about the need forlong-term monitoring, screening of other family members anda low threshold for prescribing ACE inhibitors to treat pro-teinuria or hypertension. Clearly, more comprehensivegenotype/phenotype data are needed to enable an objectivecalculation of the risk of renal impairment in heterozygouscarriers. Single mutations are significant susceptibility factorsfor renal impairment in later life, but other factors, includinglifestyle attributes such as obesity, diabetes, exercise, untreat-ed hypertension and proteinuria, are important too.Pregnancy-associated hypertension represents a risk factor in
women with heterozygous COL4A5 mutations, and closemonitoring is required throughout each pregnancy.
Whole-exome and whole-genome studies are identifyingmany more genetic variants in Alport genes, but this abun-dance adds to the work of confirming pathogenicity. TheAmerican College of Medical Genetics Guidelines for theclassification of variants are very clear [25], and their univer-sal adoption, together with submission of variants to theLeiden Open Variation Database (LOVD) or other databases,will help us understand the significance of individual variantsbetter, especially heterozygous variants in the COL4A genes.
Basic science
As with previous Alport workshops, there were exceptionalspeakers who delivered talks regarding fundamental researchrelevant to Alport syndrome (Fig. 3). Dr. Billy Hudson, fromVanderbilt Medical Centre, gave an impassioned talk wherehe emphasised the critical importance of understanding thebasic molecular mechanisms governing the ‘molecular rope’formed by the three type IV collagen alpha chains that, whendefective, cause Alport syndrome. His research group recentlyinvestigated type IV collagen at the evolutionary dawn ofmetazoan tissues by utilising Ctenophora. This is due toCtenophora being one of the earliest branching extant animal
736 Pediatr Nephrol (2020) 35:733–742
Fig. 2 Diagnosis and genetics. The importance of education and raising awareness was discussed together with the classification of Alport syndrome.Genomic sequencing projects such as 100,000 (100 k) genomes in the UK will help inform about the frequency of Alport gene mutations

phyla. Their studies revealed that type IV collagen is presentin Ctenophora but absent in unicellular sister-groups, thussuggesting that type IV collagen is one of the fundamentalarchitectural units for multicellular tissue genesis [26]. Dr.Hudson stressed the key role of protein–protein interactions,not only intra-type IV collagen interactions but also of theinteractions of type IV collagen with other basement mem-brane (BM) components, including laminins and nidogens,in addition to cell surface receptors such as integrins.
Dr. Wilhelm Kriz followed up Billy Hudson’s talk by firstpresenting data on the mesangium as a ‘dumping ground’ fordefective and degraded glomerular BM (GBM) material.Evidence from the 1970s suggests that the GBM is turnedover approximately every 65–100 days [27], and undoubtedly,this turnover is essential for a normal functioning GBM. Dr.Kriz demonstrated, using transmission electron microscopy(TEM), in addition to staining for specific GBMmarkers, thatthe mesangial matrix contains turned over GBM material.Furthermore, he showed evidence that increased productionand defective degradation of GBM during diabetic nephropa-thy (DN) contributes towards mesangial matrix expansion[28]. He then drew parallels between DN and Alport syn-drome by analysing Alport patient TEM samples. Dr. Krizhypothesised that the defective GBM component in Alportsyndrome is likely to be shunted to the mesangial
compartment in a mechanism similar to that seen in DN.This process may have an important role in Alport syndrome,leading to expansion of the mesangial matrix compartmentand eventual loss of glomerular function. Interestingly, Dr.Kriz went on to explore the role of mechanical force withinglomeruli and the consequent impact on Alport pathology.The glomerular capillary wall is exposed to high flow ratescausing sheer stress [29]. The GBM is known to create themain wall tension during glomerular filtration; however, thiscauses the GBM to expand, and at a critical point, the GBMcan no longer cope with the forces involved. Therefore, con-traction of podocytes [30, 31] and mesangial cells [32] isrequired to contribute to withstand the forces across the glo-merular capillary wall. Dr. Kriz described how the location ofpodocytes, attached to the outside of the GBM, leaves themsusceptible to detachment and loss from the glomerulus in theurine. Moreover, podocytes located close to the hilum aremore susceptible to this process because of the high flow rates;it is likely that podocytes that detach here cause a local in-crease in force that prevents reattachment [29].
Dr. Oliver Gross presented work from his laboratory ex-ploring the role of environmental modifiers of glomerular dis-ease such as obesity, high calorie intake and high sodium, inaddition to treatment with angiotensin-converting enzyme in-hibitors, the most common treatment for Alport patients
Pediatr Nephrol (2020) 35:733–742 737
Fig. 3 Basic science. The presentation covered the different experimental systems in use to investigate the biology of type IV collagen and basementmembranes. There was a focus on the mechanisms of hearing loss in Alport syndrome

(Fig. 4). Mouse models of both steroid-resistant nephroticsyndrome and Alport syndrome are being used, and this ap-proach has the potential to discover the efficacy of the stan-dard treatment for Alport syndrome taking into account manyenvironmental factors.
Mouse models and human patient data are the mostfrequently used in the Alport research community, whichhas led to major discoveries in the past 30 years.However, both higher throughput systems includingzebrafish, which have utility for high throughput screensand high-resolution in vivo imaging, and larger mamma-lian models of Alport syndrome are required to bridge thegap in Alport research. Dr. Mary Nabity is studying acanine model of XLAS. These animals have a lifespanof around 1 year, and Dr. Nabity has analysed RNA-seqsamples collected at clinical milestones of glomerular dis-ease development in these animals [33]. From this study,Dr. Nabity has discovered new genes that are differential-ly expressed between the slow and rapid progressing an-imals with Alport syndrome, including lysyl oxidase(LOX) transcripts. Further studies into the role of thesetranscript changes may provide powerful insight into themechanisms leading to slow or rapidly progressing Alportsyndrome. Another key area of research pertinent toAlport syndrome is regenerative medicine. In recentyears, there has been tremendous progress in the genera-tion of protocols for the differentiation of stem cells intorenal progenitors and kidney organoids [34, 35]. Dr.Laura Perin is seeking to apply regenerative medicine toderive a treatment for Alport syndrome. She has developedsystems involving stem cells taken from amniotic fluid [36]and has discovered a potential role for extracellular vesicles,
produced by stem cells, in modulating vascular endothelialgrowth factor (VEGF) signalling in glomerular pathobiology.Deeper understanding of this process may indeed lead to po-tential drug targets in Alport syndrome.
Protocols for isolating and culturing podocytes from urinehave been employed in a number of studies [37], and althoughknown to be challenging, these approaches enable researchersto gain insights into podocyte biology. Dr. Sergio Daga, fromThe University of Siena, has been using this approach to iso-late podocytes and subsequently use CRISPR gene editingtechnology to study Alport syndrome. This area of researchhas the potential to unlock further mechanistic insights inAlport syndrome.
The therapeutic potential of anti-miR-21 for the treat-ment of Alport syndrome was first investigated by Dr.Jeremy Duffield and colleagues in 2015 with promisingresults [38]. Dr. Tsubasa Yokota from Dr. Hirofumi Kai’slaboratory has been building on some of these findings fromthis study. STAT3 and IL6 were found to be increased inmice with Alport syndrome before anti-miR-21 treatment;the group, therefore, investigated the impact of STAT3 andIL6 inhibitors in Alport mice. They found that STAT3 inhi-bition reduced proteinuria, whereas IL6 inhibition had noeffect on this metric of glomerular function [39]. This is notthe only treatment that the group have tested in Alport mice;bromide supplementation was also tried, as Billy Hudsonhad shown bromide to be important for type IV collagennetwork formation [40]. However, bromide supplementa-tion exacerbated Alport pathology [41]. Dr. Kai’s researchgroup investigations into both the repurposing of licenseddrugs, including metformin, and novel therapies are of vitalimportance for the Alport community.
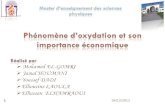
Fig. 4 Factors that influence theprogression of Alport syndrome.Treatments that have confirmedor proposed effects on protectingkidney function, cardiovascularrisk and hearing (top half ingreen) and factors that are knownor thought to be deleterious(bottom half in blue). ACEangiotensin-converting enzyme,ARB angiotensin receptorblocker, HMG-CoA β-hydroxyβ-methylglutaryl-CoA, NSAIDsnon-steroidal anti-inflammatorydrugs
738 Pediatr Nephrol (2020) 35:733–742

Despite renal pathologies being the focus of the Alportworkshop, there is a desperate need for more research intothe hearing impairment caused by Alport syndrome. Dr.Dan Jagger, from University College London, delivered atalk to provide some insights into the sensorineural hear-ing loss found in individuals with Alport syndrome. It isknown that hearing loss occurs in Alport syndrome, butthere is no evidence for a disorder in balance, which maybe anticipated if there is progressive damage to the innerear. The structure thought to be most likely progressivelydamaged in Alport patients is the basilar membrane of thecochlea. The basilar membrane sits on a basement mem-brane which is composed of type IV collagen a3a4a5.Both inner and outer hair cells of the cochlea are exposedto forces, which in turn are converted to electrical signalsinterpreted by the brain as sound. Evidence suggests thatit is the outer hair cells that are damaged in Alport syn-drome. The outer hair cells are the ‘amplifiers’ of thesignal generated by the inner hair cells, which is why a‘base level’ of hearing that can be amplified with hearingaids remains in individuals with Alport syndrome.Although it is uncertain whether the hearing loss pheno-type is present in all mouse models with Alport syndrome,Dr. Jagger warned about the future of hearing research inAlport mice, as it is well known that there is age-relatedhearing loss in mice, which may confound studies. Themost obvious current advice to patients with Alport syn-drome is to avoid exposure to mechanical damage, forinstance use of head phones.
Patient perspectives
Representatives from National Patient Organizations were inattendance from Australia, China, France, Germany, Italy,The Netherlands, Spain, the UK and the USA. In addition toattending the main session, a pre-event meeting took placewith these groups to discuss how they could better collaboratewith each other to provide improved resources and support topatients and encourage research. The creation of anInternational Alport Organization was discussed to achievethis and elements of this organization were captured by themeeting illustrators. It was agreed that there are significantchallenges to the creation of such an organization. Amongstthese were:
& Dependence on volunteers for organization and resources.& Significant differences in treatment resources and needs
between different countries.& Differences in effective communication modes.& Differences in cultural attitudes towards disease, privacy
and the physician–patient relationship
These challenges closely mirror those posed to creationof an International Alport Patient Registry discussed inpast workshops. Susie Gear of Alport UK proposed aseries of potential logos for an International AlportOrganization (Fig. 3).
Recognising the importance of the patient perspective inresearch and the development of potential therapies, patientswere asked to share their stories with the larger group (Fig. 5).Andre Weinstock from the USA shared his experience as apatient who had a transplant and continues to experience hear-ing loss. This led to a discussion about the role of hearing lossin Alport syndrome as an important quality of life concern.Jessie Zhang, a mother of an Alport patient from China, spokeabout the need for patients to connect with each other as partof a community to alleviate feelings of isolation, gain knowl-edge and resources, and work together for advocacy. TheAlport Collective, a group of teenage patients from the UK,shared videos they created to improve communication amongteens about Alport syndrome, and these are accessible onYouTube : h t t p s : / /www.you tube . com/wa t ch?v=Ps3rMpx7YZg, https://www.youtube.com/watch?v=5gJEtmhcClU. Maria Jose, from Spain, spoke of the patientadvocacy organization’s efforts to unite their community.While each journey was different, all conveyed theimportance of having a community to provide support andresources.
In addition, patient groups play a critical role in re-search and the development of potential therapies. Thesegroups are instrumental not only in recruiting patients forresearch but also conveying the patient perspective to re-searchers and industry. Gina Parziale, Executive Directorof the Alport Syndrome Foundation in the USA sharedtheir plans for an Externally Led Patient DevelopmentMeeting. It took place in San Diego in October 2018and brought together patients and their care-partners, rep-resentatives from the US Food and Drug Administration(FDA), pharmaceutical companies interested in develop-ing drugs for the disease, and physicians—all to hear frompatients about Alport syndrome. In these meetings, thepatient’s experience is brought to the forefront for govern-mental regulatory bodies, pharmaceutical companies andacademic researchers to understand.
The Healthtalk project on Alport syndrome
As a further expansion of the patient voice, the meet-ing also heard about the Healthtalk project on Alportsyndrome. The importance of listening to patient expe-riences is central to formulating health policy in theUK (and many other countries) [42]. Research suggeststhat hearing other people’s experiences, alongside
Pediatr Nephrol (2020) 35:733–742 739

factual information, engages people’s attention and in-fluences and supports treatment decision making [43,44].
From 2015 to 2017, a research project collaborationbetween Alport UK and the University of Oxford led toa freely accessible resource on Alport syndrome at thewebsite Healthtalk.org. Based on rigorous qualitativeresearch, Healthtalk provides a multi-media internet re-source on the experiences, information and supportneeds of people with different health issues. The sitealready features 110 different conditions, had more than6 million visitors in 2018 and is based on more than4,000 in-depthnarrative interviews of peoples’ experi-ences of health and illness. Health conditions on thesite include several major cancers,cardiovascular disease,mental health, epilepsy, rheumatoid arthritis, pregnancy,screening, sexual health and experiences of carersofpeople with dementia. The interviews are generatedand analysed by experienced social science researchers,most of whom are based in the Health ExperiencesResearch Group within the University of Oxford’sNuffield Department of Primary Care Health Scienceswww.phc.ox.ac.uk/research/health-experiences. Dr.Melissa Stepney (co-author) conducted the interviewsand analysis for the section on Alport Syndrome. TheHealthtalk sections have direct relevance for health and
social care professionals and students, schools, under-graduate and post-graduate learning and teaching.
Further, the website section on Alport syndrome providesan evidence base for patients and the public, learning andteaching, policy makers, all who want to consult a balanced,patient-led collection of experiences. Here, narrative inter-views were conducted with 38 people with Alport syndrome,including families and partners, and 3 interviews withhealthcare professionals with expertise on Alport syndrome.The patient interviews offer in-depth knowledge and first-hand experiences of what it is like to actually live withAlport syndrome. On the site http://healthtalk.org/peoples-experiences/long-term-conditions/alport-syndrome/overview,there are around 27 topic summaries with 250 video clipschosen to reflect issues important to participants, such as thefirst signs and symptoms of Alport syndrome, getting adiagnosis of Alport syndrome, medication, reproductivechoices, living as a female ‘carrier’ and the emotional sideof living with Alport syndrome. Although this study wasUK based, many of the overall experiences are similaracross the world—in practice, this means that when a personwith Alport syndrome looks at any of these summaries, theyshould find that an experience or perspective akin to their ownis included, although this may not necessarily be reported by aperson of the same age, family situation or social class asthemselves. This baseline understanding of UK patients is
740 Pediatr Nephrol (2020) 35:733–742
Fig. 5 Patient perspective. Four presentations from members of Alport syndrome patient organisations highlighted the importance of the patient voice

critical in order to inform further projects and toolkits to bettersupport patients in the future, including improving communi-cation, more effective and efficient clinical care, much neededmental health support and the treatment of female ‘carriers’.
Summary
Overall, this review highlights the current and significant de-velopments in Alport syndrome research from clinical andbasic science to genetics and qualitative research with pa-tients. The collaboration between clinicians, patients and re-searchers is key to accelerating the current research efforts inorder to deliver the unmet needs of patients living with Alportsyndrome.
Acknowledgements The author time was supported by a WellcomeSenior Fellowship award (202860/Z/16/Z) to R.L. and a ResearchProject Award to R.L. from Kidney Research UK (K1199). The authorsalso acknowledge core funding from the Wellcome Trust (203128/Z/16/Z) to the Wellcome Centre for Cell-Matrix Research at the University ofManchester.
Compliance with ethical standards
Conflict of interest MR receives research funding from RegulusTherapeutics and Reata Pharmaceuticals. The other authors declare noconflicts of interests.
Open Access This article is distributed under the terms of the CreativeCommons At t r ibut ion 4 .0 In te rna t ional License (h t tp : / /creativecommons.org/licenses/by/4.0/), which permits unrestricted use,distribution, and reproduction in any medium, provided you give appro-priate credit to the original author(s) and the source, provide a link to theCreative Commons license, and indicate if changes were made.
References
1. Miner JH, Baigent C, Flinter F, Gross O, Judge P, Kashtan CE,Lagas S, Savige J, Blatt D, Ding J, Gale DP, Midgley JP, PoveyS, Prunotto M, Renault D, Skelding J, Turner AN, Gear S (2014)The 2014 International Workshop on Alport Syndrome. Kidney Int86:679–684
2. Gross O, Kashtan CE, Rheault MN, Flinter F, Savige J, Miner JH,Torra R, Ars E, Deltas C, Savva I, Perin L, Renieri A, Ariani F,MariF, Baigent C, Judge P, Knebelman B, Heidet L, Lagas S, Blatt D,Ding J, Zhang Y, Gale DP, Prunotto M, Xue Y, Schachter AD,Morton LCG, Blem J, Huang M, Liu S, Vallee S, Renault D,Schifter J, Skelding J, Gear S, Friede T, Turner AN, Lennon R(2017) Advances and unmet needs in genetic, basic and clinicalscience in Alport syndrome: report from the 2015 InternationalWorkshop on Alport Syndrome. Nephrol Dial Transplant 32:916–924
3. Lennon R, Stuart HM, Bierzynska A, Randles MJ, Kerr B, HillmanKA, Batra G, Campbell J, Storey H, Flinter FA, Koziell A, WelshGI, Saleem MA, Webb NJ, Woolf AS (2015) Coinheritance ofCOL4A5 and MYO1E mutations accentuate the severity of kidneydisease. Pediatr Nephrol 30:1459–1465
4. Malone AF, Phelan PJ, Hall G, Cetincelik U, Homstad A, AlonsoAS, Jiang R, Lindsey TB, Wu G, Sparks MA, Smith SR, Webb NJ,Kalra PA,AdeyemoAA, ShawAS, Conlon PJ, Jennette JC, HowellDN, Winn MP, Gbadegesin RA (2014) Rare hereditary COL4A3/COL4A4 variants may be mistaken for familial focal segmentalglomerulosclerosis. Kidney Int 86:1253–1259
5. Kashtan CE, Ding J, Gregory M, Gross O, Heidet L, KnebelmannB, Rheault M, Licht C, Alport Syndrome Research Collaborative(2013) Clinical practice recommendations for the treatment ofAlport syndrome: a statement of the Alport Syndrome ResearchCollaborative. Pediatr Nephrol 28:5–11
6. Gross O, Friede T, Hilgers R, Gorlitz A, Gavenis K, AhmedR, DurrU (2012) Safety and efficacy of the ACE-inhibitor ramipril inAlport syndrome: the double-blind, randomized, placebo-con-trolled, multicenter phase III EARLY PRO-TECT Alport trial inpediatric patients. ISRN Pediatr 2012:436046
7. Nagra A, McGinnity PM, Davis N, Salmon AP (2015)Implementing transition: ready steady go. Arch Dis Child EducPract Ed 100:313–320
8. Yefet E, Tovbin D, Nachum Z (2016) Pregnancy outcomes in pa-tients with Alport syndrome. Arch Gynecol Obstet 293:739–747
9. HallM (2016) Pregnancy in womenwith CKD: a success story. AmJ Kidney Dis 68:633–639
10. Noone D, Licht C (2013) An update on the pathomechanisms andfuture therapies of Alport syndrome. Pediatr Nephrol 28:1025–1036
11. Dufek B, Meehan DT, Delimont D, Cheung L, Gratton MA,Phillips G, SongW, Liu S, Cosgrove D (2016) Endothelin A recep-tor activation onmesangial cells initiates Alport glomerular disease.Kidney Int 90:300–310
12. Savige J, Gregory M, Gross O, Kashtan C, Ding J, Flinter F (2013)Expert guidelines for the management of Alport syndrome and thinbasement membrane nephropathy. J Am Soc Nephrol 24:364–375
13. Savige J, Storey H, Il Cheong H, Gyung Kang H, Park E, Hilbert P,Persikov A, Torres-Fernandez C, Ars E, Torra R, Hertz JM,Thomassen M, Shagam L, Wang D, Wang Y, Flinter F, Nagel M(2016) X-linked and autosomal recessive Alport syndrome: patho-genic variant features and further genotype-phenotype correlations.PLoS One 11:e0161802
14. Gast C, Pengelly RJ, Lyon M, Bunyan DJ, Seaby EG, Graham N,Venkat-RamanG, Ennis S (2016) Collagen (COL4A) mutations arethe most frequent mutations underlying adult focal segmentalglomerulosclerosis. Nephrol Dial Transplant 31:961–970
15. Tonna S, Wang YY, Wilson D, Rigby L, Tabone T, Cotton R,Savige J (2008) The R229Q mutation in NPHS2 may predisposeto proteinuria in thin-basement-membrane nephropathy. PediatrNephrol 23:2201–2207
16. Bullich G, Trujillano D, Santin S, Ossowski S,Mendizabal S, FragaG, Madrid A, Ariceta G, Ballarin J, Torra R, Estivill X, Ars E(2015) Targeted next-generation sequencing in steroid-resistant ne-phrotic syndrome: mutations in multiple glomerular genes may in-fluence disease severity. Eur J Hum Genet 23:1192–1199
17. Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, RenieriA, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Dahan K,Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM,Schroder C, Sanak M, Carvalho MF, Saus J, Antignac C, SmeetsH, Gubler MC (2003) X-linked Alport syndrome: natural historyand genotype-phenotype correlations in girls and women belongingto 195 families: a BEuropean Community Alport SyndromeConcerted Action^ study. J Am Soc Nephrol 14:2603–2610
18. Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, RenieriA, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Verellen C,Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM,Schroder C, Sanak M, Krejcova S, Carvalho MF, Saus J,Antignac C, Smeets H, Gubler MC (2000) X-linked Alport
Pediatr Nephrol (2020) 35:733–742 741

syndrome: natural history in 195 families and genotype- phenotypecorrelations in males. J Am Soc Nephrol 11:649–657
19. Temme J, Peters F, Lange K, Pirson Y, Heidet L, Torra R, GrunfeldJP, Weber M, Licht C, Muller GA, Gross O (2012) Incidence ofrenal failure and nephroprotection by RAAS inhibition in heterozy-gous carriers of X-chromosomal and autosomal recessive Alportmutations. Kidney Int 81:779–783
20. Gross O, Licht C, Anders HJ, Hoppe B, Beck B, Tonshoff B,Hocker B, Wygoda S, Ehrich JH, Pape L, Konrad M, Rascher W,Dotsch J,Muller-Wiefel DE, Hoyer P, Study GroupMembers of theGesellschaft für Pädiatrische Nephrologie, Knebelmann B, PirsonY, Grunfeld JP, Niaudet P, Cochat P, Heidet L, Lebbah S, Torra R,Friede T, Lange K, Muller GA,Weber M (2012) Early angiotensin-converting enzyme inhibition in Alport syndrome delays renal fail-ure and improves life expectancy. Kidney Int 81:494–501
21. Kashtan CE, Ding J, Garosi G, Heidet L, Massella L, Nakanishi K,Nozu K, Renieri A, Rheault M, Wang F, Gross O (2018) Alportsyndrome: a unified classification of genetic disorders of collagenIValpha345: a position paper of the Alport SyndromeClassificationWorking Group. Kidney Int 93:1045–1051
22. Savige J, Colville D, Rheault M, Gear S, Lennon R, Lagas S, FinlayM, Flinter F (2016) Alport syndrome in women and girls. Clin J AmSoc Nephrol 11:1713–1720
23. Savige J, Rana K, Tonna S, Buzza M, Dagher H, Wang YY (2003)Thin basement membrane nephropathy. Kidney Int 64:1169–1178
24. Papazachariou L, Papagregoriou G, Hadjipanagi D, DemosthenousP, Voskarides K, Koutsofti C, Stylianou K, Ioannou P, Xydakis D,Tzanakis I, Papadaki A, Kallivretakis N, Nikolakakis N, PerysinakiG, Gale DP, Diamantopoulos A, Goudas P, Goumenos D,Soloukides A, Boletis I, Melexopoulou C, Georgaki E, Frysira E,Komianou F, Grekas D, Paliouras C, Alivanis P, Vergoulas G,Pierides A, Daphnis E, Deltas C (2017) Frequent COL4 mutationsin familial microhematuria accompanied by later-onset Alport ne-phropathy due to focal segmental glomerulosclerosis. Clin Genet92:517–527
25. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, GrodyWW, Hegde M, Lyon E, Spector E, Voelkerding K, Rehm HL,ACMG Laboratory Quality Assurance Committee (2015)Standards and guidelines for the interpretation of sequence variants:a joint consensus recommendation of the American College ofMedical Genetics and Genomics and the Association forMolecular Pathology. Genet Med 17:405–424
26. Fidler AL, Darris CE, Chetyrkin SV, Pedchenko VK, Boudko SP,Brown KL, Gray Jerome W, Hudson JK, Rokas A, Hudson BG(2017) Collagen IV and basement membrane at the evolutionarydawn of metazoan tissues. Elife. https://doi.org/10.7554/eLife.24176
27. Price RG, Spiro RG (1977) Studies on the metabolism of the renalglomerular basement membrane. Turnover measurements in the ratwith the use of radiolabeled amino acids. J Biol Chem 252:8597–8602
28. Kriz W, Lowen J, Federico G, van den Born J, Grone E, Grone HJ(2017) Accumulation of worn-out GBMmaterial substantially con-tributes to mesangial matrix expansion in diabetic nephropathy. AmJ Physiol Ren Physiol 312:F1101–F1111
29. Kriz W, Lemley KV (2017) Mechanical challenges to the glomer-ular filtration barrier: adaptations and pathway to sclerosis. PediatrNephrol 32:405–417
30. Endlich K, Kliewe F, Endlich N (2017) Stressed podocytes-mechanical forces, sensors, signaling and response. Pflugers Arch469:937–949
31. Kriz W, Mundel P, Elger M (1994) The contractile apparatus ofpodocytes is arranged to counteract GBM expansion. ContribNephrol 107:1–9
32. Kriz W, Elger M, Lemley K, Sakai T (1990) Structure of the glo-merular mesangium: a biomechanical interpretation. Kidney IntSuppl 30:S2–S9
33. Chu CP, Hokamp JA, Cianciolo RE, Dabney AR, Brinkmeyer-Langford C, Lees GE, NabityMB (2017) RNA-seq of serial kidneybiopsies obtained during progression of chronic kidney diseasefrom dogs with X-linked hereditary nephropathy. Sci Rep 7:16776
34. Takasato M, Er PX, Chiu HS, Little MH (2016) Generation ofkidney organoids from human pluripotent stem cells. Nat Protoc11:1681–1692
35. Takasato M, Er PX, Chiu HS, Maier B, Baillie GJ, Ferguson C,Parton RG, Wolvetang EJ, Roost MS, Chuva de Sousa Lopes SM,Little MH (2015) Kidney organoids from human iPS cells containmultiple lineages and model human nephrogenesis. Nature 526:564–568
36. Sedrakyan S, Da Sacco S, Milanesi A, Shiri L, Petrosyan A,Varimezova R, Warburton D, Lemley KV, De Filippo RE, Perin L(2012) Injection of amniotic fluid stem cells delays progression ofrenal fibrosis. J Am Soc Nephrol 23:661–673
37. Krtil J, Platenik J, Kazderova M, Tesar V, Zima T (2007) Culturemethods of glomerular podocytes. Kidney Blood Press Res 30:162–174
38. Gomez IG, MacKenna DA, Johnson BG, Kaimal V, Roach AM,Ren S, Nakagawa N, Xin C, Newitt R, Pandya S, Xia TH, Liu X,Borza DB, Grafals M, Shankland SJ, Himmelfarb J, Portilla D, LiuS, Chau BN, Duffield JS (2015) Anti-microRNA-21 oligonucleo-tides prevent Alport nephropathy progression by stimulating meta-bolic pathways. J Clin Invest 125:141–156
39. Yokota T, Omachi K, Suico MA, Kamura M, Kojima H, Fukuda R,Motomura K, Teramoto K, Kaseda S, Kuwazuru J, Takeo T,Nakagata N, Shuto T, Kai H (2018) STAT3 inhibition attenuatesthe progressive phenotypes of Alport syndrome mouse model.Nephrol Dial Transplant 33:214–223
40. McCall AS, Cummings CF, Bhave G, Vanacore R, Page-McCawA, Hudson BG (2014) Bromine is an essential trace element forassembly of collagen IV scaffolds in tissue development and archi-tecture. Cell 157:1380–1392
41. Yokota T, Omachi K, Suico MA, Kojima H, Kamura M, TeramotoK, Kaseda S, Kuwazuru J, Shuto T, Kai H (2017) Bromide supple-mentation exacerbated the renal dysfunction, injury and fibrosis in amouse model of Alport syndrome. PLoS One 12:e0183959
42. Gann B (2013) Understanding and using experiences of health andillness: the policy landscape. In: Ziebland S C, A., Calabrese, J.,Locock, L, (ed) Understanding and using health experiences OUP,Oxford
43. Prinjha SEJ, Ziebland S, McPherson A (2011) A mastectomy forsomething that wasn't even truly invasive cancer. Women’s under-standings of having amastectomy for screen-detectedDCIS: a qual-itative study. J Med Screen 18:34–40
44. Feinmann J (2011) Listening to patients’ narratives can help im-prove quality of psychosis care. BMJ 342:d2245
Publisher’s note Springer Nature remains neutral with regard tojurisdictional claims in published maps and institutional affiliations.
742 Pediatr Nephrol (2020) 35:733–742