Soins de Support en cours de Radiothérapie - TAO-CTM meeting · Optimisation de la Prise en Charge...
77
Paris, HEGP - 20 Novembre 2014 - TAO 2014 Soins de Support en cours de Radiothérapie Gestion de la Toxicité aiguë de la Radiothérapie Exemple des K des Voies Aéro-Digestives Supérieures -------------------------- - René-Jean Bensadoun -
Transcript of Soins de Support en cours de Radiothérapie - TAO-CTM meeting · Optimisation de la Prise en Charge...
Paris, HEGP
- 20 Novembre 2014 -
TAO 2014
Soins de Support en cours de Radiothérapie
Gestion de la Toxicité aiguë de la Radiothérapie
Exemple des K des Voies Aéro-Digestives Supérieures
--------------------------
- René-Jean Bensadoun -
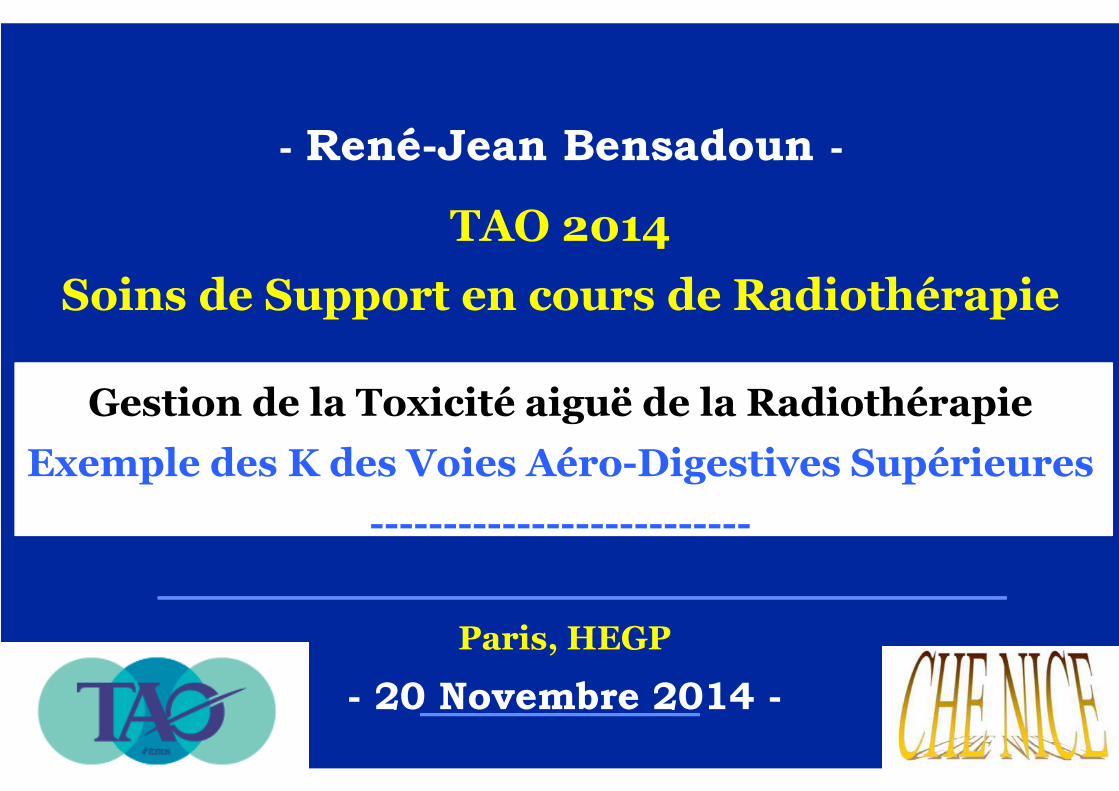
OPTIMISATION DE LA RADIOTHERAPIEDES CANCERS des VADS
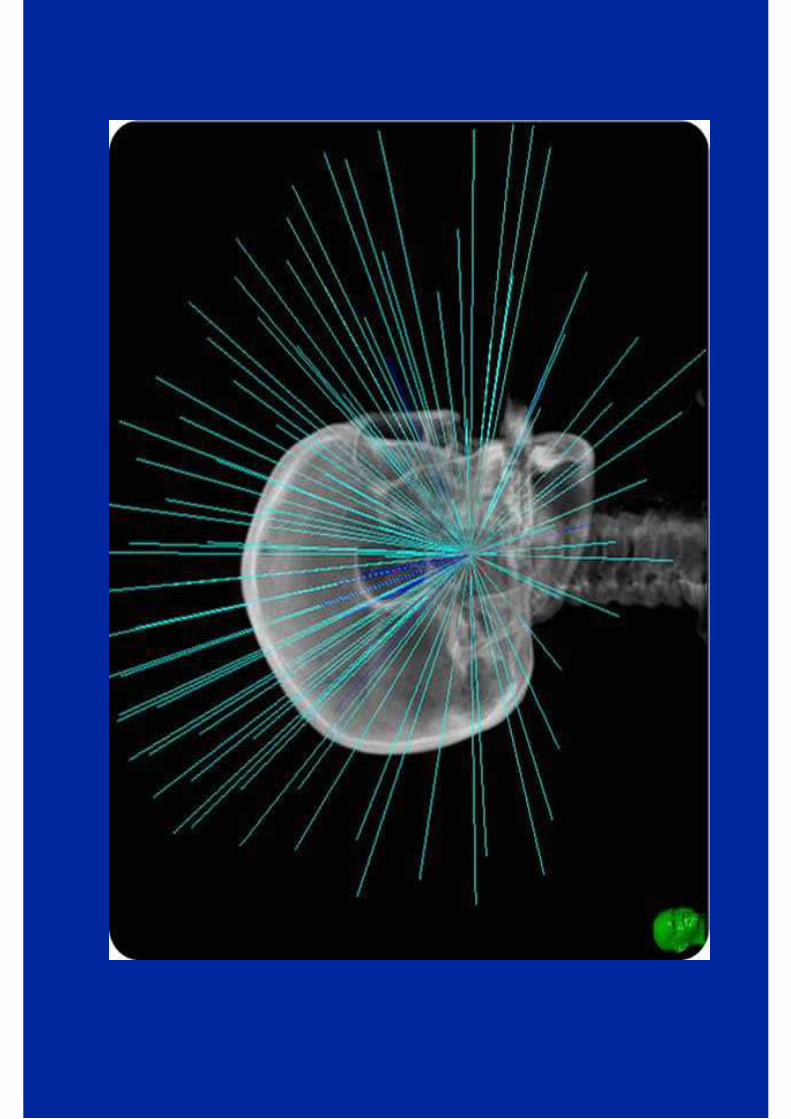
BALISTIQUE : RCMI (IMRT) ++++
CHIMIOTHERAPIE CONCOMITANTE
ASSOCIATION AUX THERAPIES CIBLEES
SOINS DE SUPPORT : Place du Laser de Basse Energie; Nutrition Entérale; «S.O.T» (soins d’optimisation thérapeutique)
REFERENTIELS (contourage, dose
intensité…)
1
2
34
5
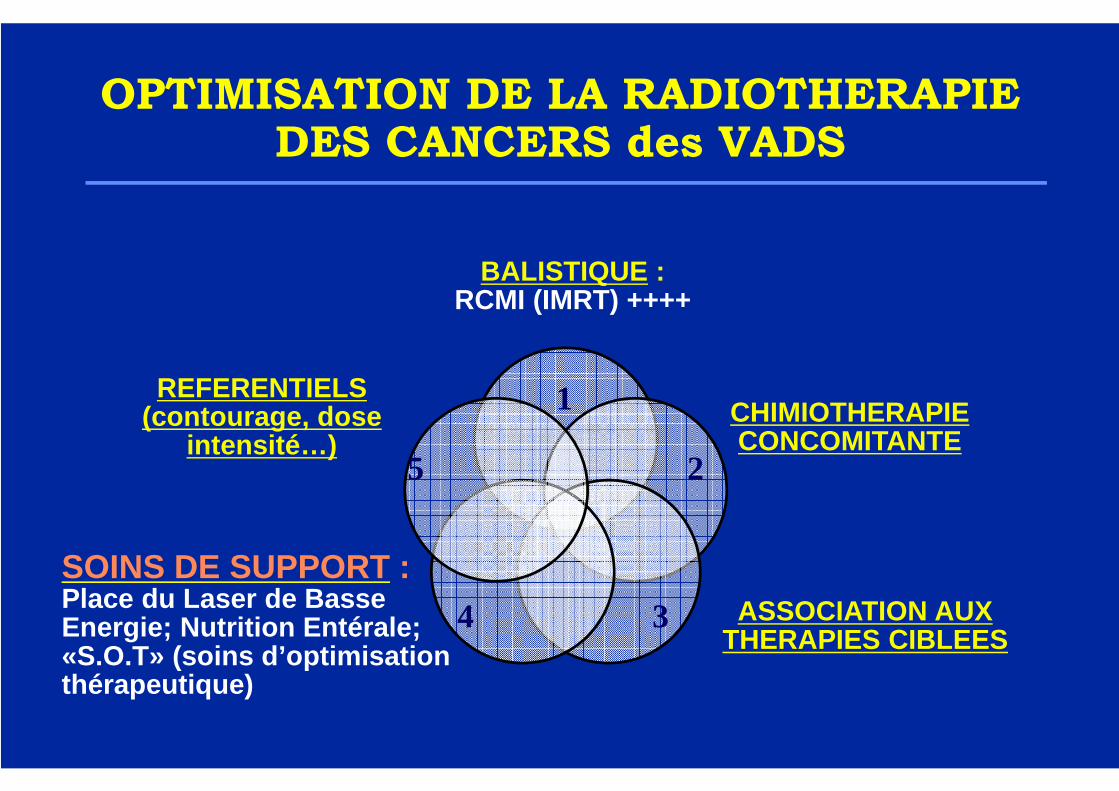
IMRT 3D CONFORMAL TRADITIONAL 2D
45 54 70 84 Gy PTV BRAINSTEM/SPINAL CORD
D’’’’après Clifton Ling , Memorial SK, New York
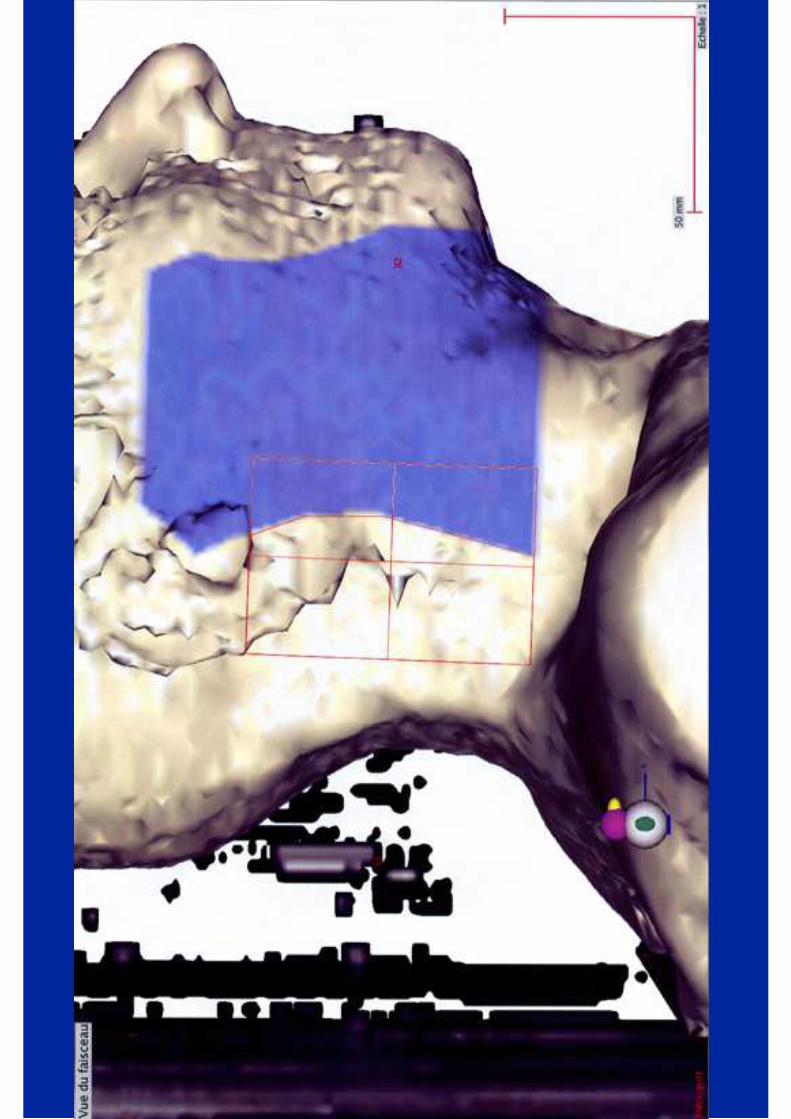
Radiothérapie de l’’’’oropharynx et du cavum(RT2D, RC3D, IMRT)
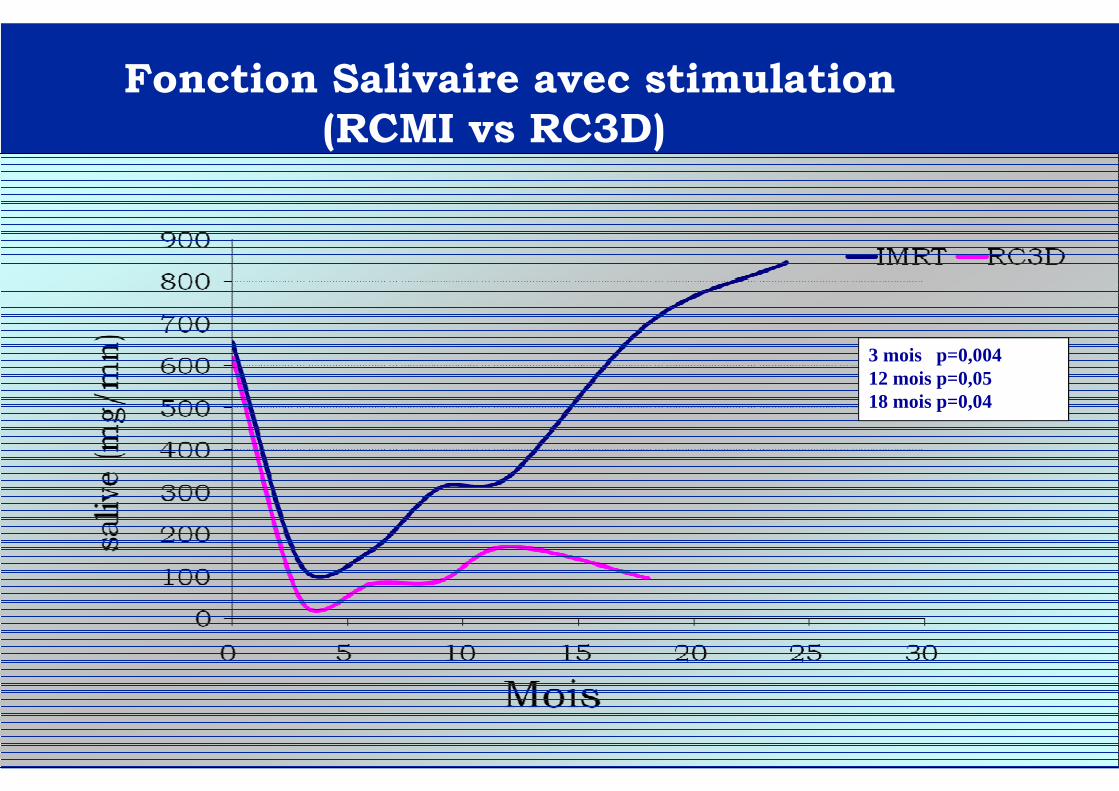
3 mois p=0,00412 mois p=0,0518 mois p=0,04
Fonction Salivaire avec stimulation(RCMI vs RC3D)

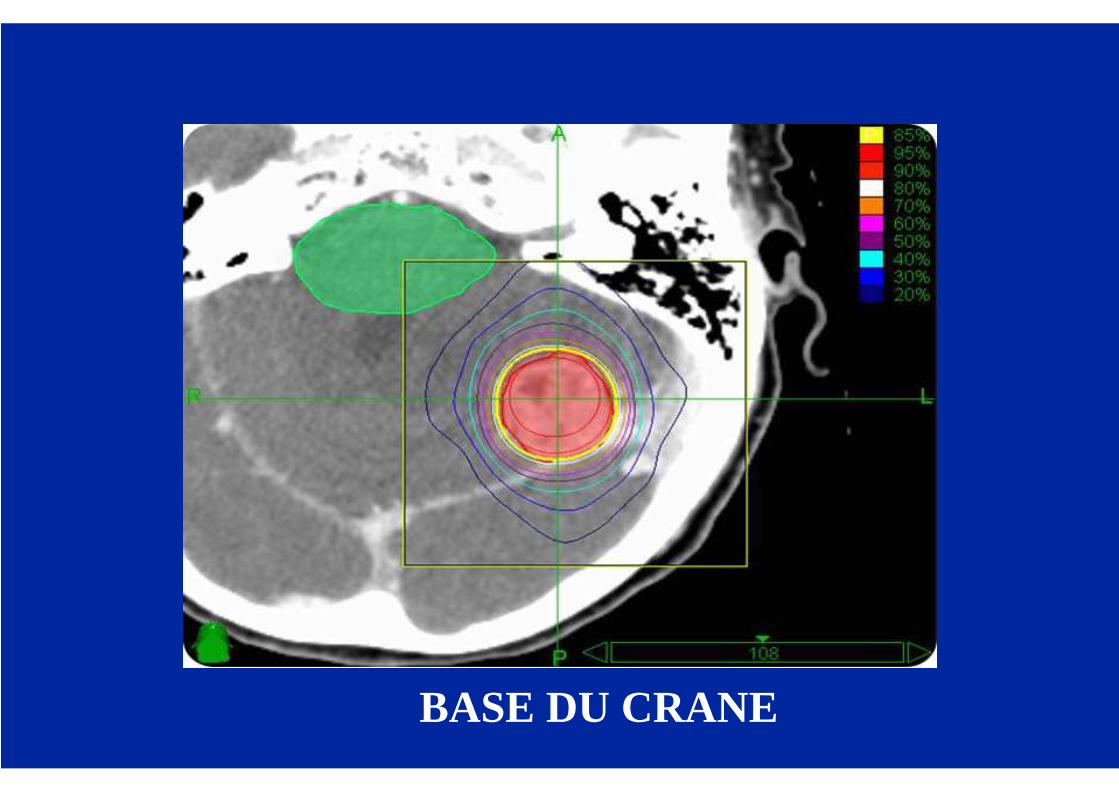
BASE DU CRANE

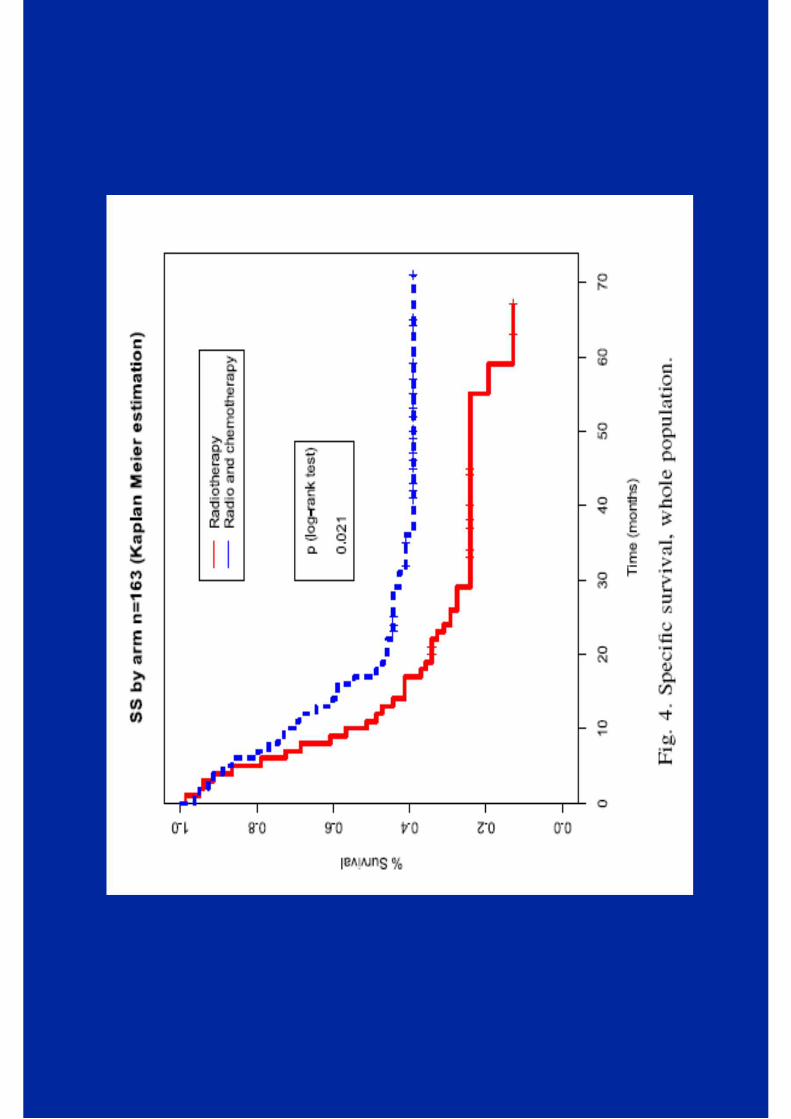
Radiochimiothérapie
Concomitante
Radiochimiothérapie
Concomitante
(et/ou association aux thérapies
ciblées (anti REGF): cetuximab)
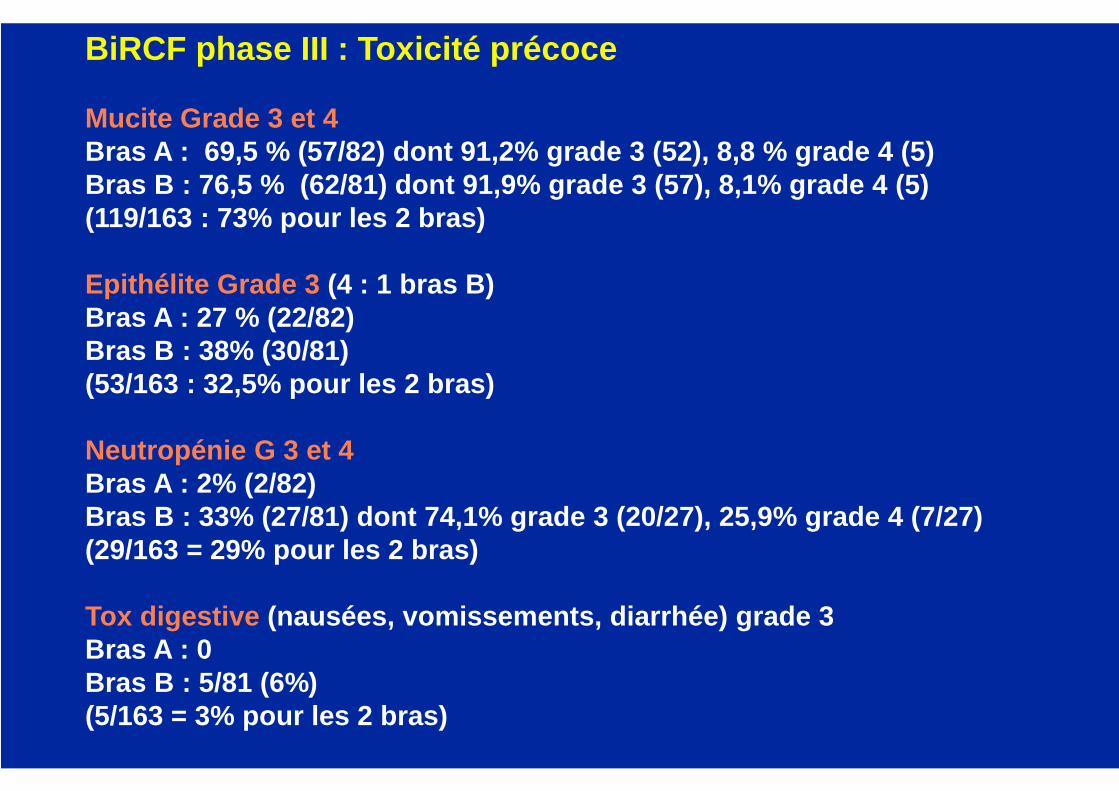
BiRCF phase III : Toxicité précoce
Mucite Grade 3 et 4 Bras A : 69,5 % (57/82) dont 91,2% grade 3 (52), 8, 8 % grade 4 (5)Bras B : 76,5 % (62/81) dont 91,9% grade 3 (57), 8, 1% grade 4 (5)(119/163 : 73% pour les 2 bras)
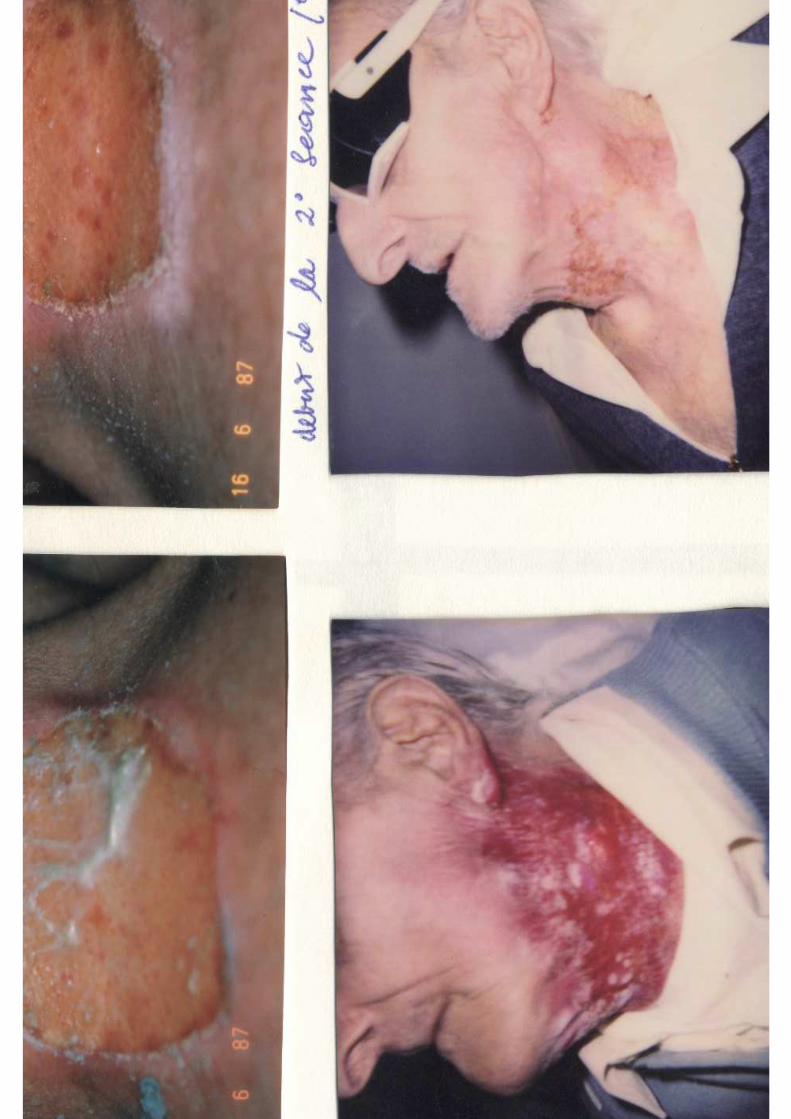
Epithélite Grade 3 (4 : 1 bras B)Bras A : 27 % (22/82)Bras B : 38% (30/81)(53/163 : 32,5% pour les 2 bras)
Neutropénie G 3 et 4Bras A : 2% (2/82)Bras B : 33% (27/81) dont 74,1% grade 3 (20/27), 25, 9% grade 4 (7/27)(29/163 = 29% pour les 2 bras)
Tox digestive (nausées, vomissements, diarrhée) grade 3Bras A : 0Bras B : 5/81 (6%)(5/163 = 3% pour les 2 bras)
NOTION DE«QUALITE de SOINS» :
� OBTENIR UNE EFFICACITE MAXIMALE (DOSE, ADMINISTRATION, et CHOIX du TRAITEMENT), avec :
– une BONNE COMPLIANCE du PATIENT au traitement ;
– le MOINS POSSIBLE D’’’’EFFETS SECONDAIRES.
«Doing the right thing right»
MISE EN OEUVRE des protocoles de RADIO-CHIMIOTHERAPIE (K ORL)
� Notion d'intensité de dose optimale .� Prise en charge des effets secondaires
précoces, � Support nutritionnel :
("Supportive care")
=> Notion de rapport "coût fonctionnel"/efficacité,
=> et FAISABILITE ou non du protocole.

TRAITEMENTS ASSOCIES
� SUPPORT NUTRITIONNEL ++
� ANTALGIQUES (et AINS)
� ANTIBIOTIQUES
� ANTINAUSEEUX
� SOINS LOCAUX / LASER DE BASSE ÉNERGIE
� FACTEURS DE CROISSANCE HEMATOPOIETIQUES
� RADIOPROTECTEURS, CHIMIOPROTECTEURS ??

LIMITES
� HOSPITALISATION ? Alternatives ++� Compliance au traitement?� Support logistique ++� Qualité de vie ?� Séquelles des réactions locales
précoces ?� Efficacité à long terme ?� Coût …
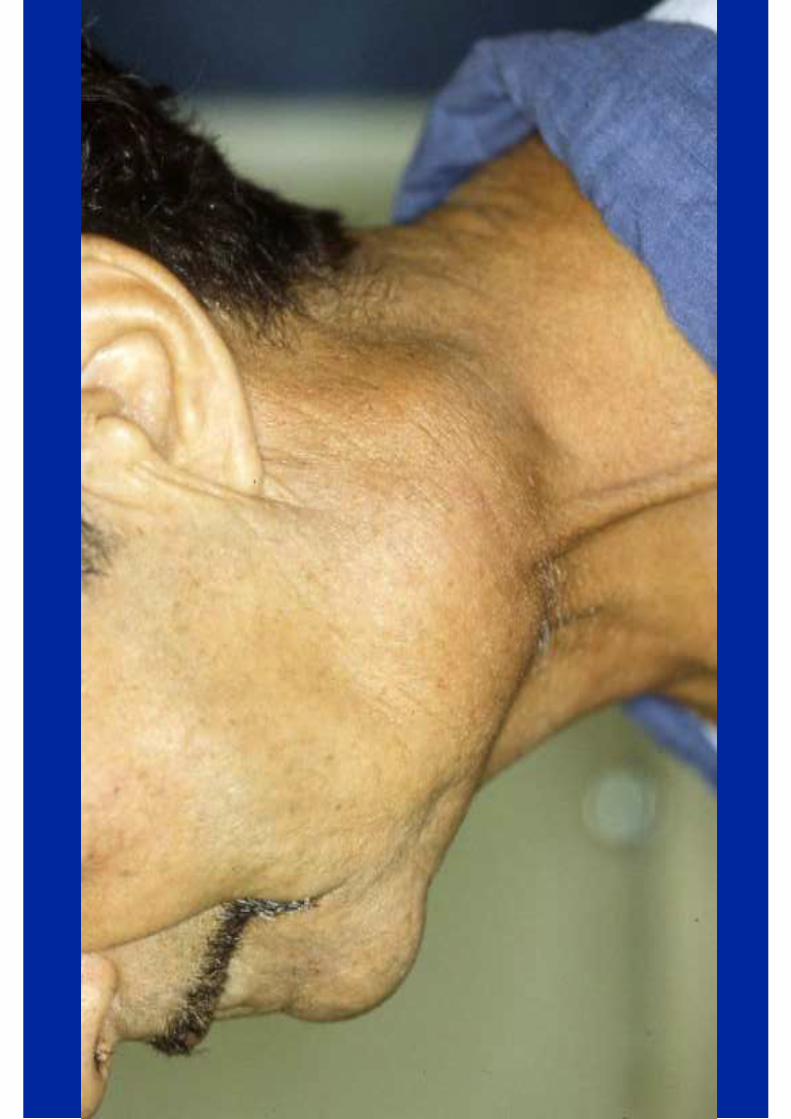
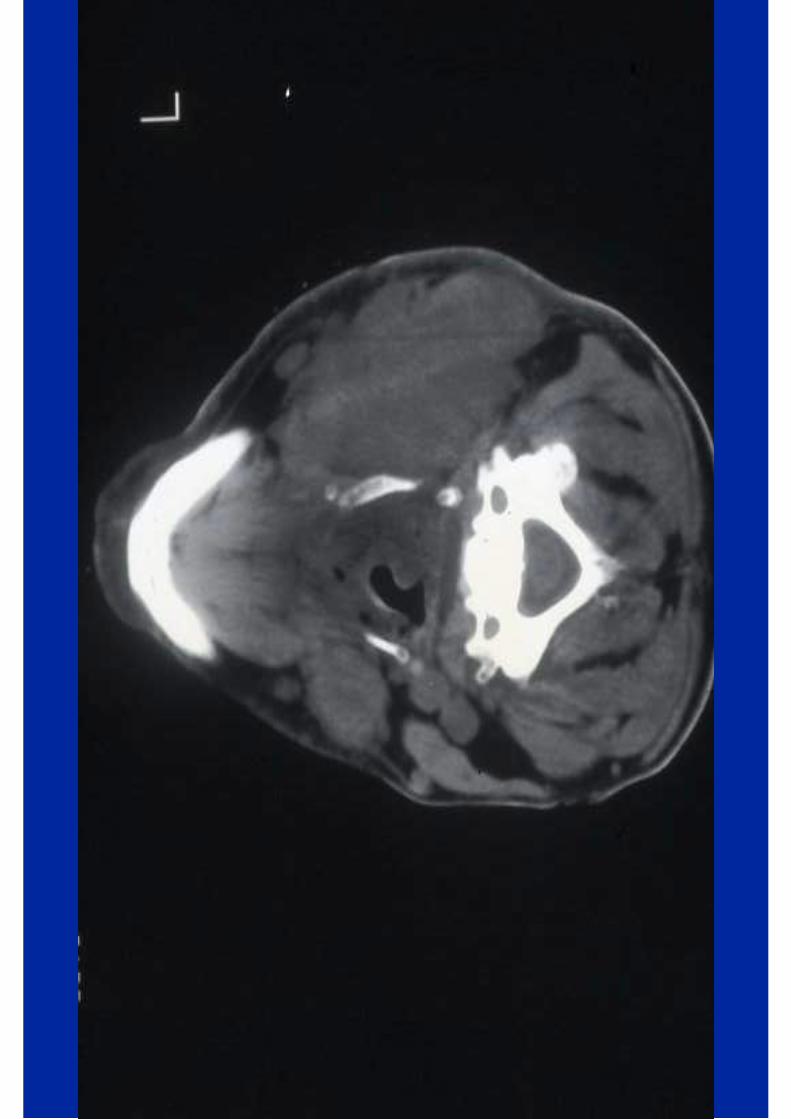
Exemple de la Radio -chimiothérapie des Cancers ORL:
EFFETS SECONDAIRES PRECOCES
� Perte de poids� Mucite� Epithélite� Neutropénie fébrile� Surinfections� Insuffisance rénale et troubles
métaboliques� Troubles digestifs� Oedème laryngé.

A différencier des EFFETS SECONDAIRES TARDIFS :
� atteintes muqueuses� atteintes cutanées, sous-cutanées, et
musculaires� atteintes neurologiques� atteintes osseuses� fonctions de déglutition, de phonation
=> qualité de vie=> vie de relation=> réinsertion sociale .
Optimisation de la Prise en Charge Globale
du patient traité pour cancer ORL :
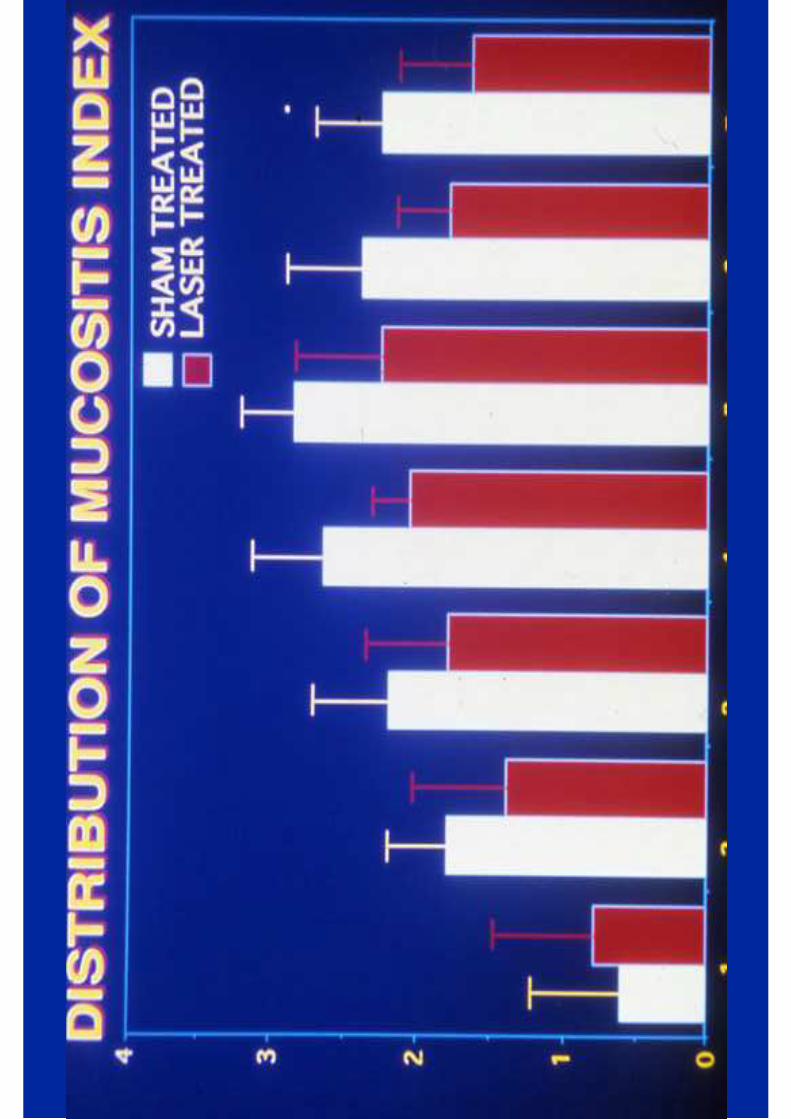
� Prise en charge de la Mucite, et de l’Epithélite, notamment par Laser de basse énergie (essais de phase III concluants)
� Soins locaux, antalgiques opiacés de niveau III, AINS, anti-fongiques locaux
� Renutrition entérale par Gastrostomie
(essais de phase II et phase III).

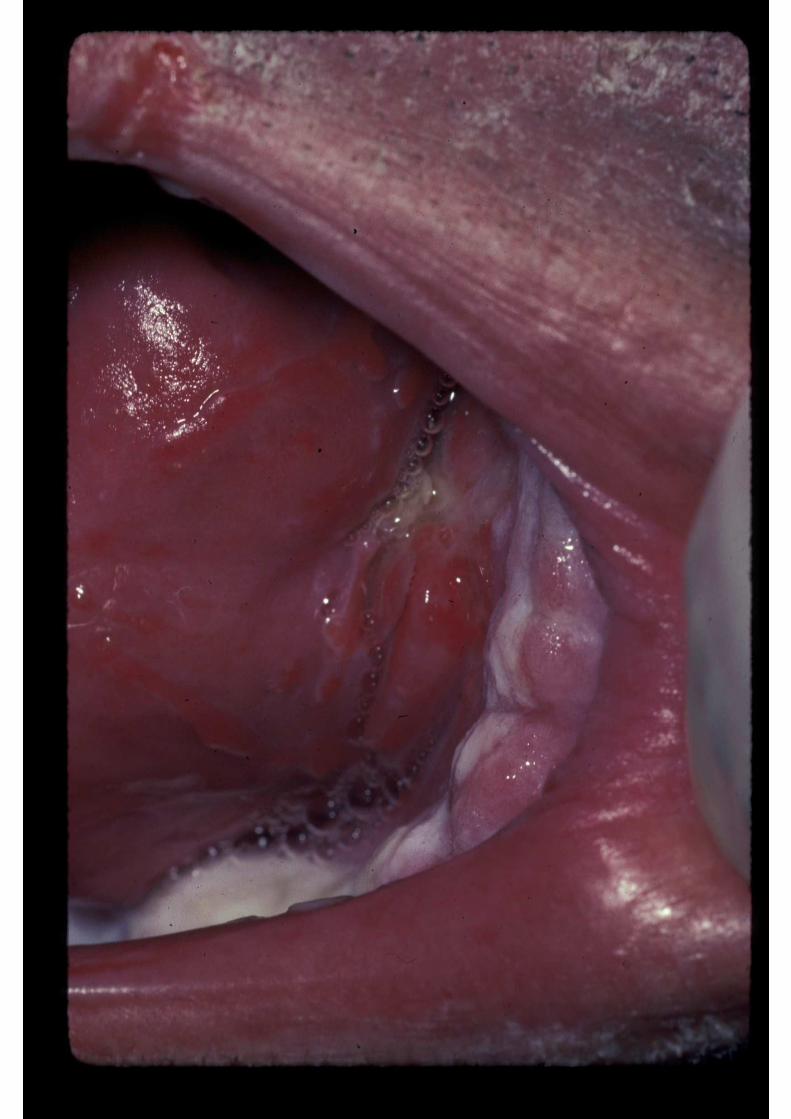
Mucite Chimio-Induite de grade 3:
Mucite Radio-Induite de grade 3:
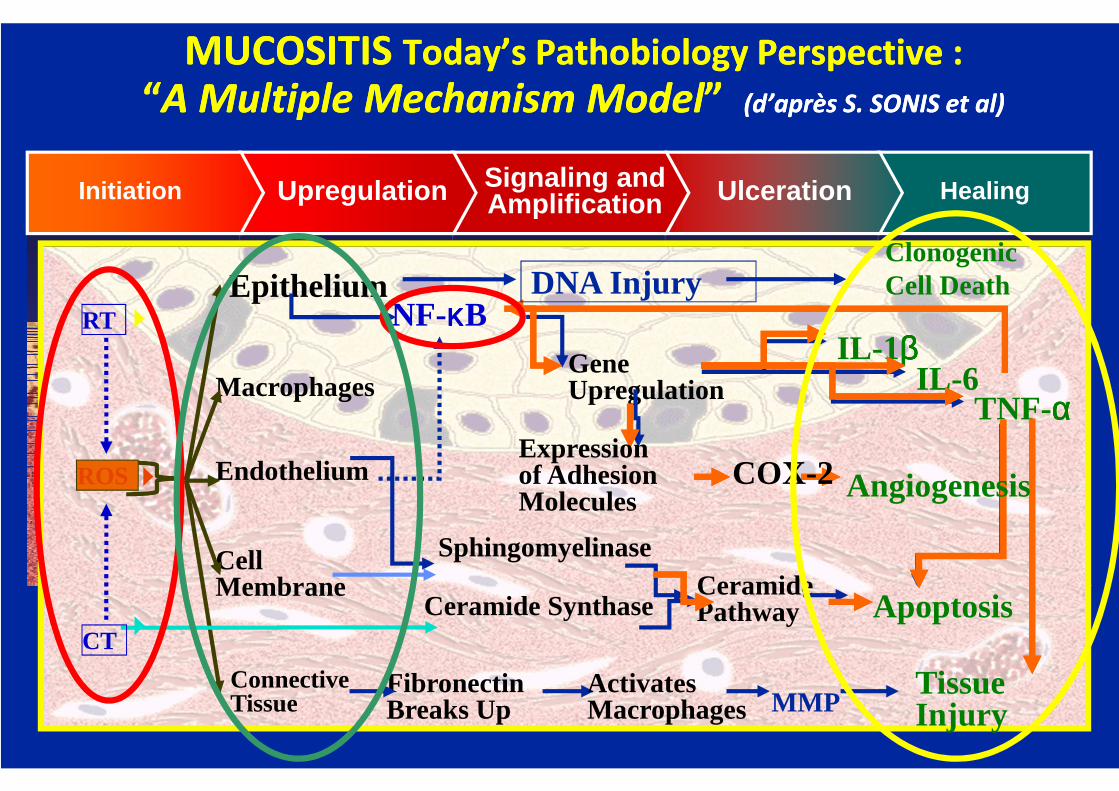
HealingUlcerationSignaling andAmplificationUpregulationInitiation
Apoptosis
FibronectinBreaks Up
ActivatesMacrophages MMP
IL -1ββββ
TNF-ααααIL -6Gene
Upregulation
NF-κκκκB
Cell Membrane
Epithelium
Endothelium
ConnectiveTissue
Macrophages
SphingomyelinaseCeramidePathwayCeramide Synthase
ClonogenicCell Death
ROS
MUCOSITIS Today’s Pathobiology Perspective :
“A Multiple Mechanism Model” (d’après S. SONIS et al)
MUCOSITIS Today’s Pathobiology Perspective :
“A Multiple Mechanism Model” (d’après S. SONIS et al)
CT
RT
Tissue Injury
AngiogenesisExpressionof AdhesionMolecules
COX-2
DNA Injury

Le Laser de basse énergie (LLLT) dans la prise en charge des Mucites et Epithélites
radio- et chimio-induites
A - MUCITES
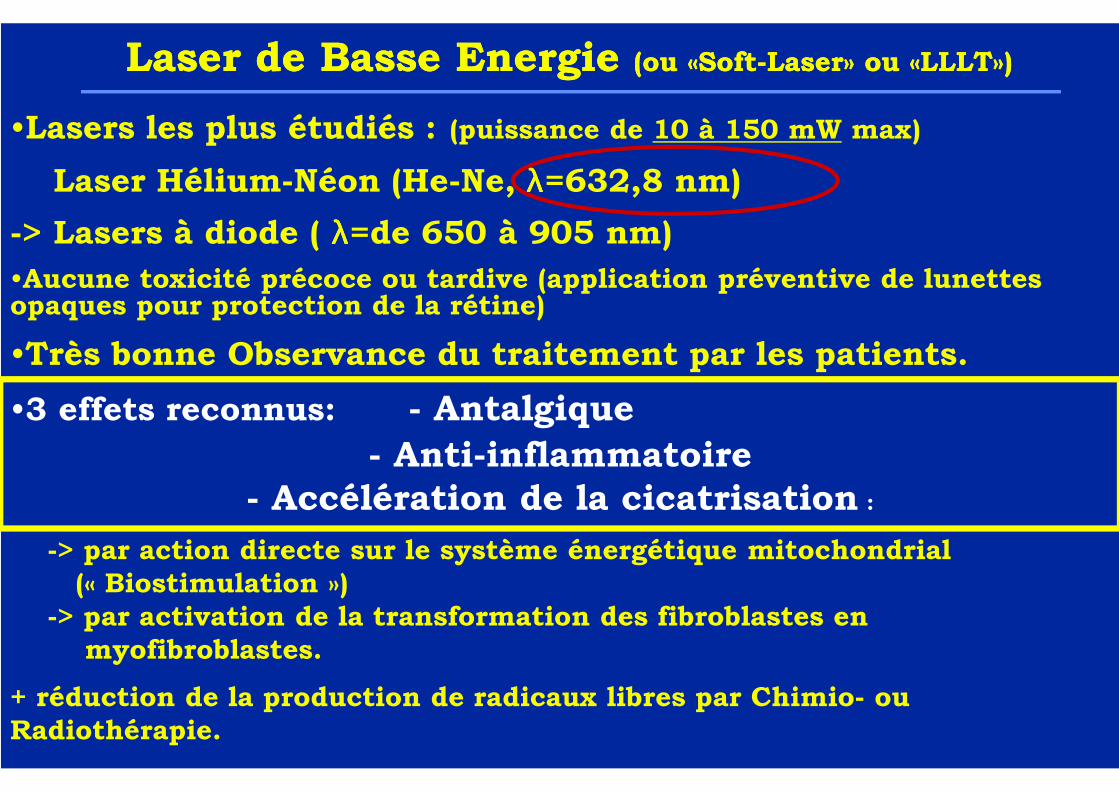
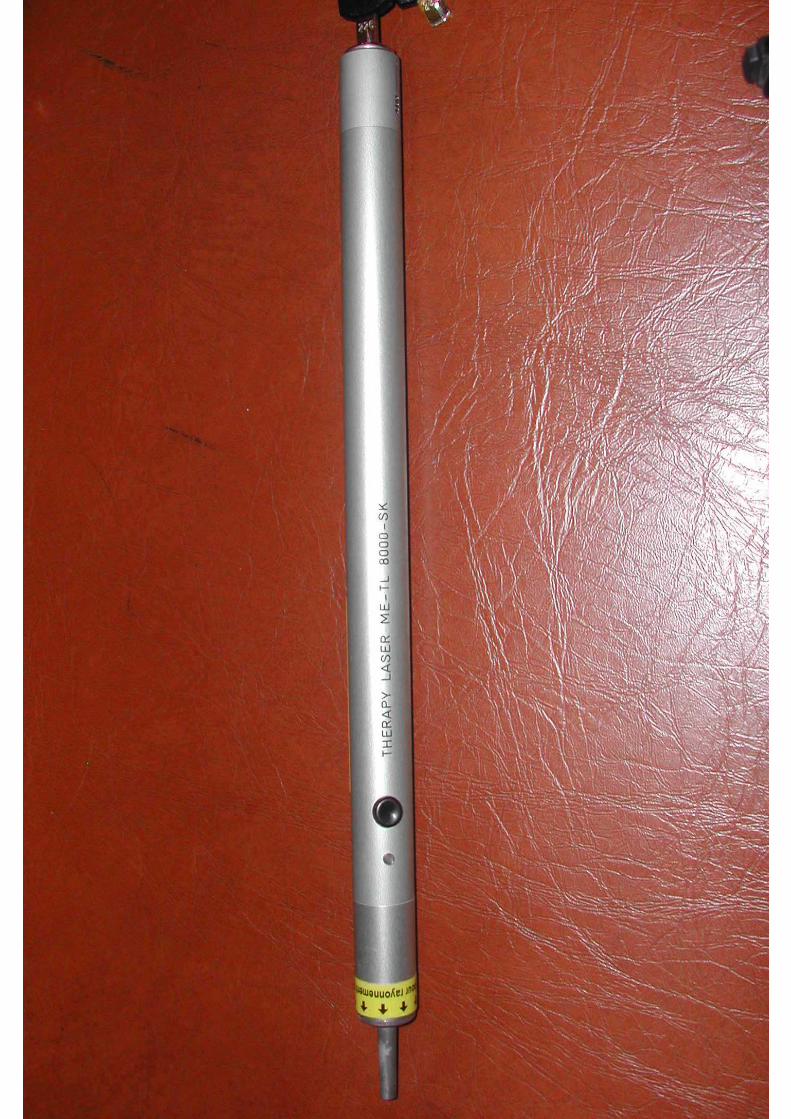
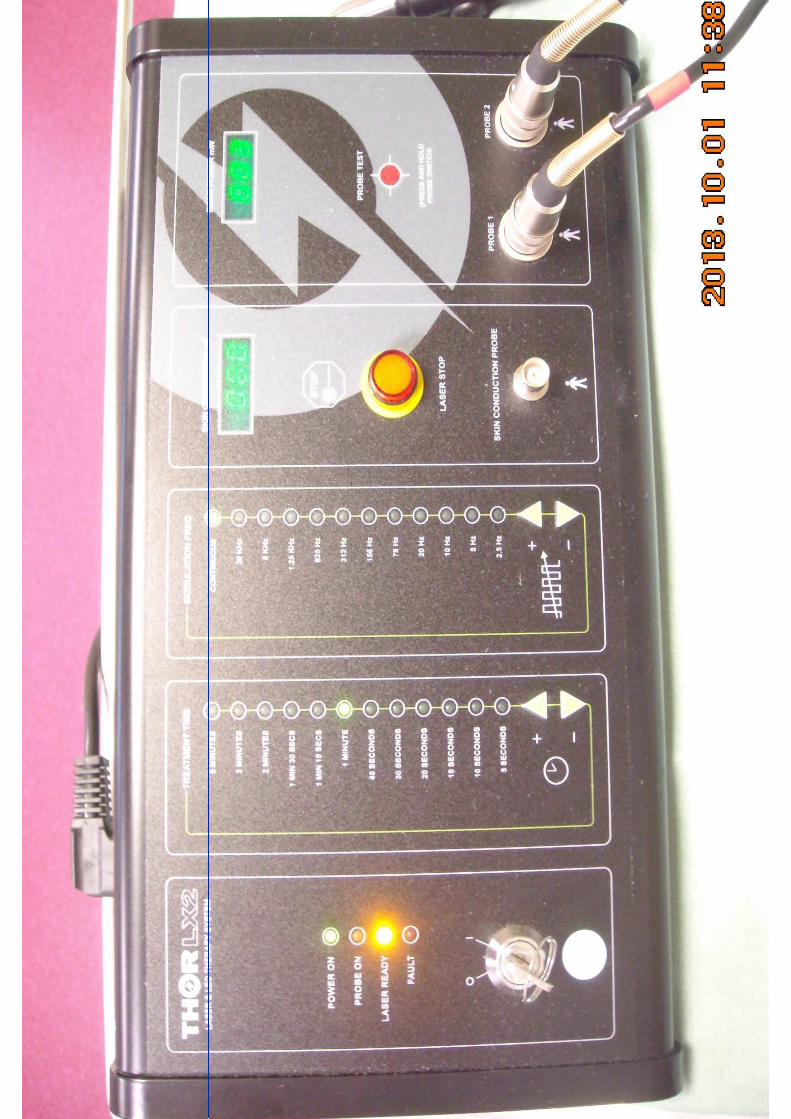
•Lasers les plus étudiés : (puissance de 10 à 150 mW max)
-> Laser Hélium-Néon (He-Ne, λλλλ=632,8 nm)
-> Lasers à diode ( λλλλ=de 650 à 905 nm)
•Aucune toxicité précoce ou tardive (application préventive de lunettes opaques pour protection de la rétine)
•Très bonne Observance du traitement par les patients.
•3 effets reconnus: - Antalgique
- Anti-inflammatoire- Accélération de la cicatrisation :
-> par action directe sur le système énergétique mitochondrial(« Biostimulation »)
-> par activation de la transformation des fibroblastes en myofibroblastes.
+ réduction de la production de radicaux libres par Chimio- ou Radiothérapie.
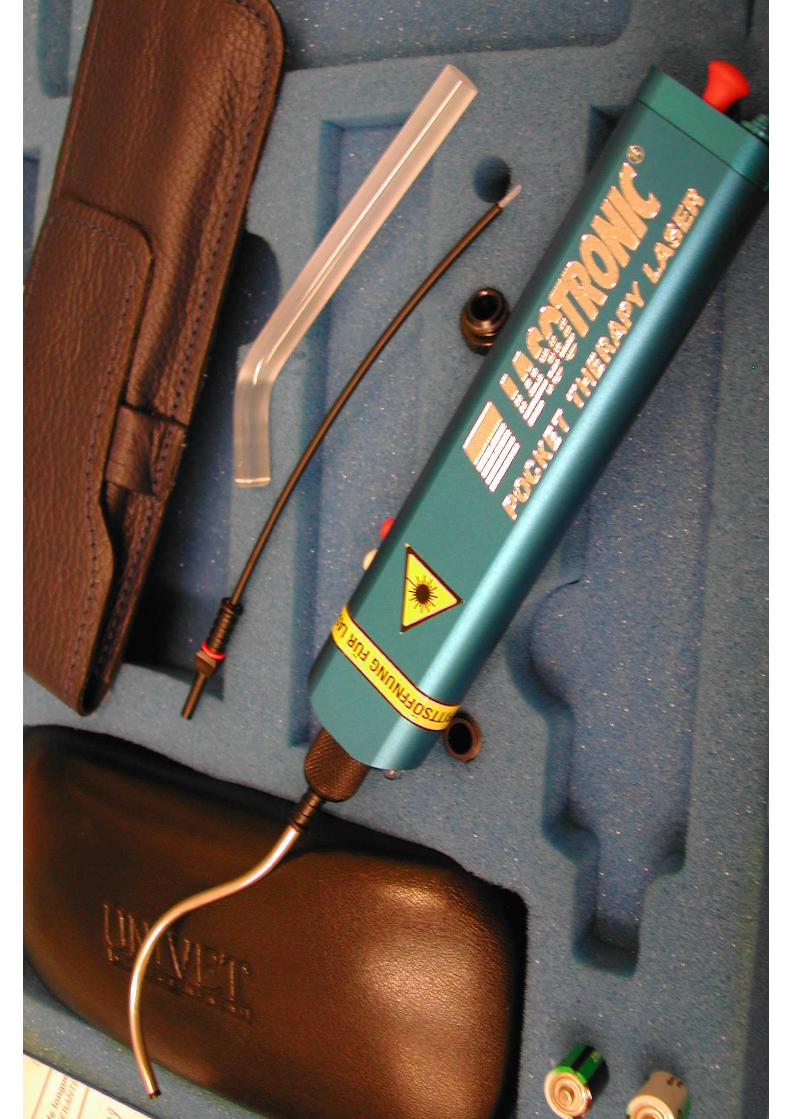
Laser de Basse Energie (ou «Soft-Laser» ou «LLLT»)Laser de Basse Energie (ou «Soft-Laser» ou «LLLT»)
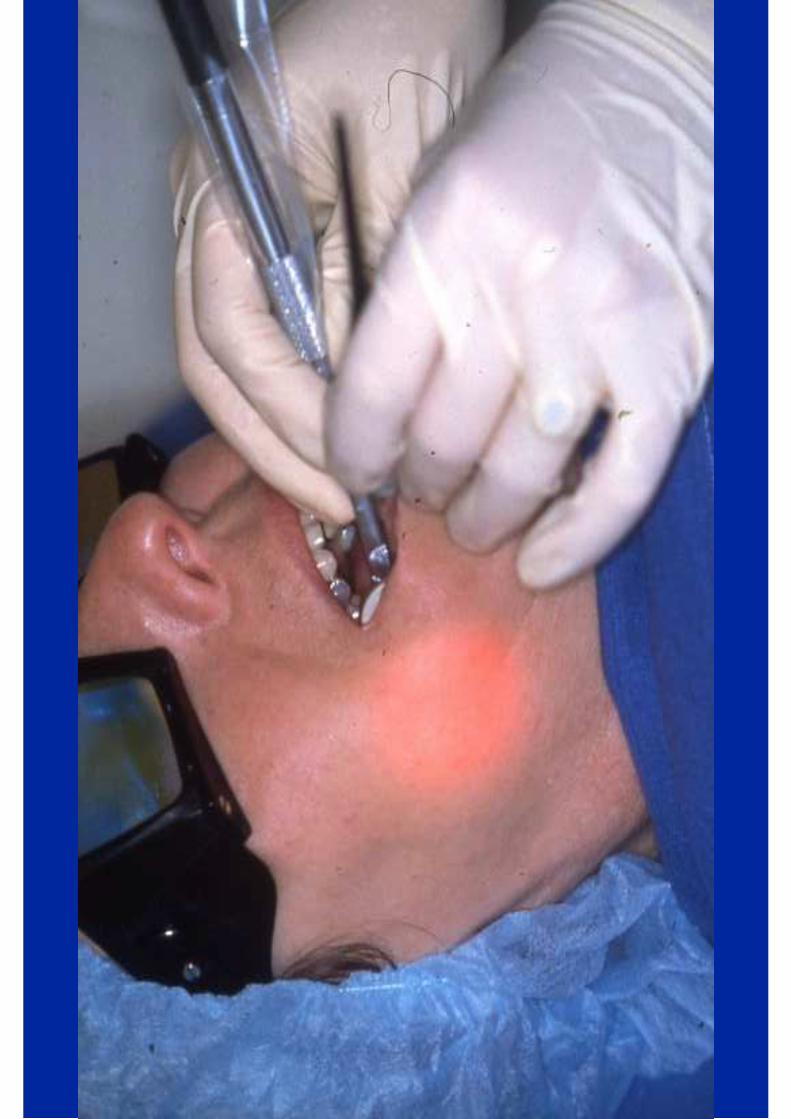


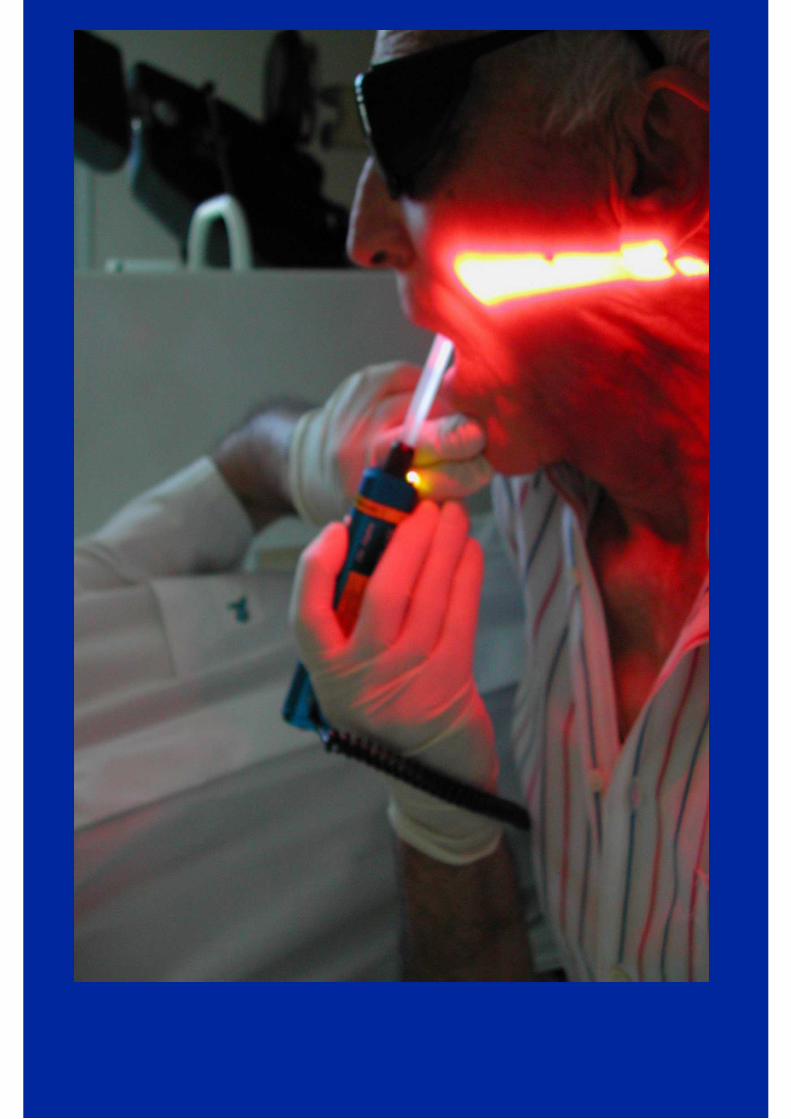
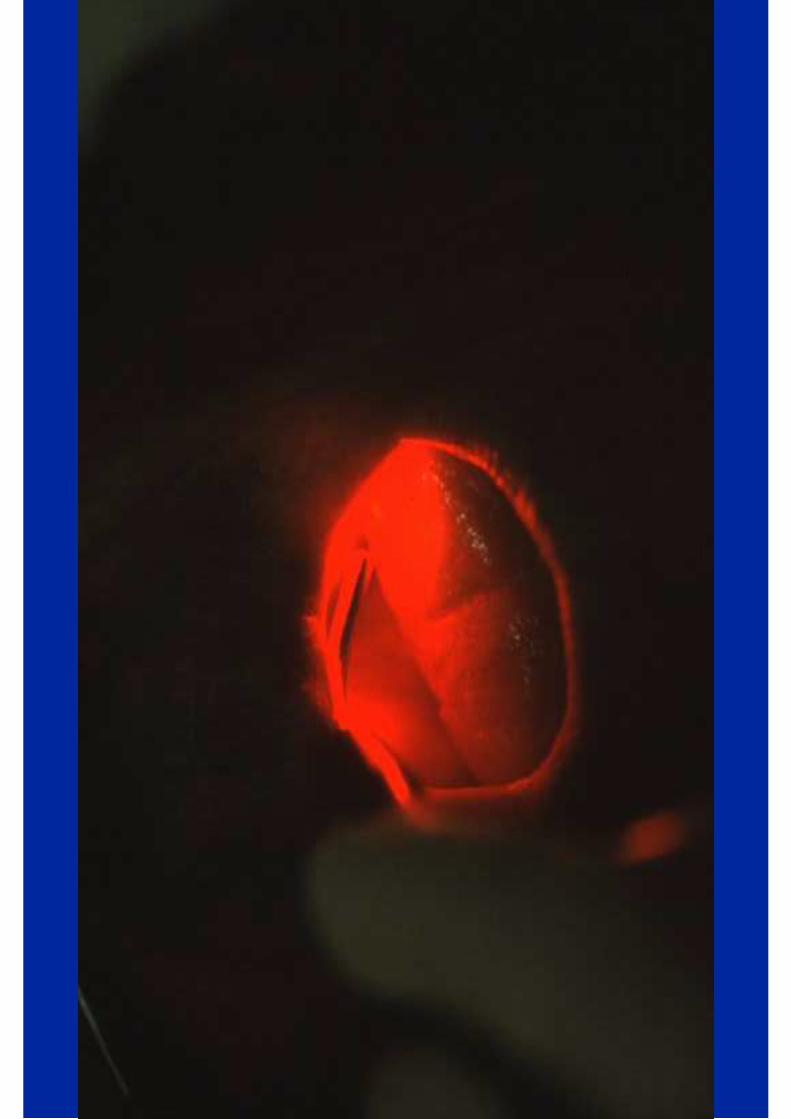

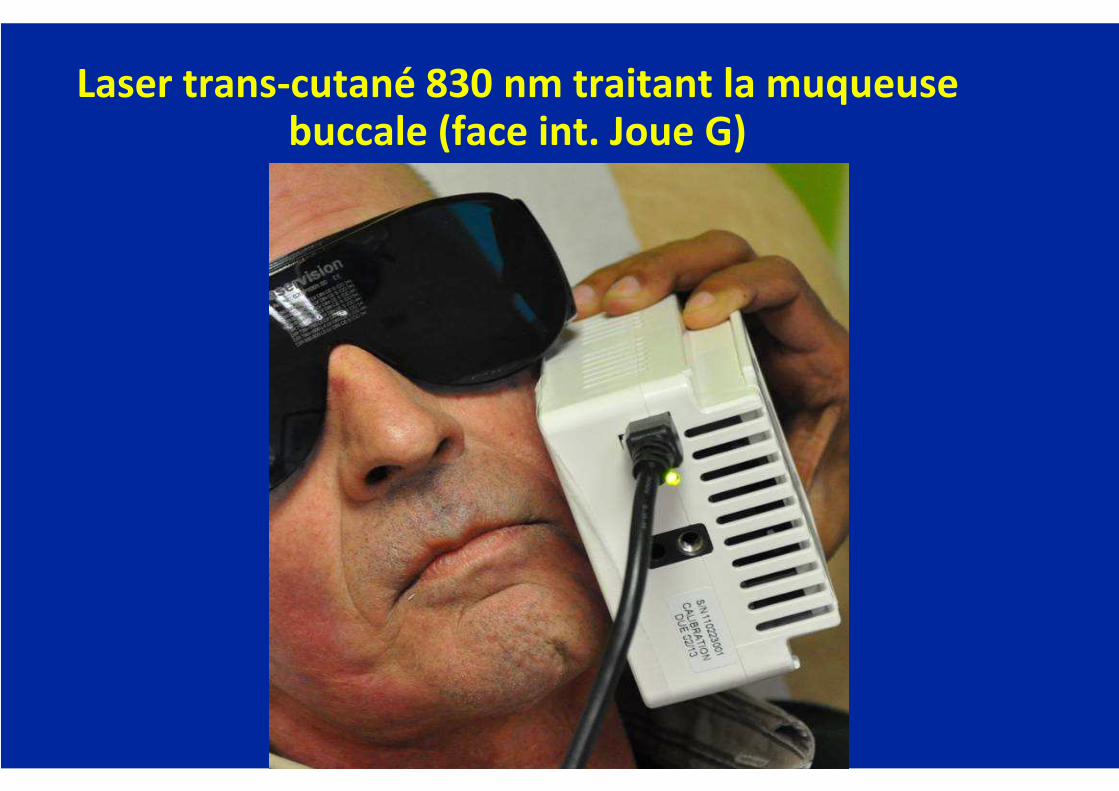
Laser trans-cutané 830 nm traitant la muqueuse buccale (face int. Joue G)

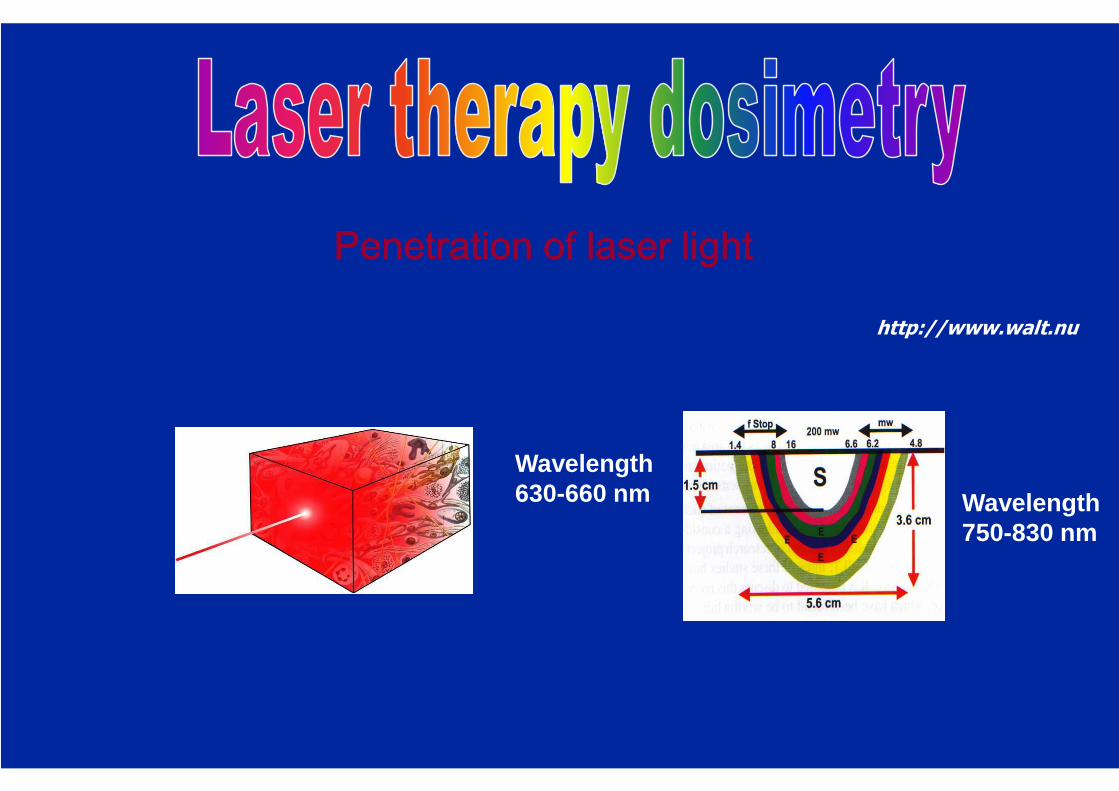
Penetration of laser lightPenetration of laser lightPenetration of laser lightPenetration of laser light
http://www.walt.nu
Wavelength630-660 nm Wavelength
750-830 nm
B - Epithélites

Laser cutané


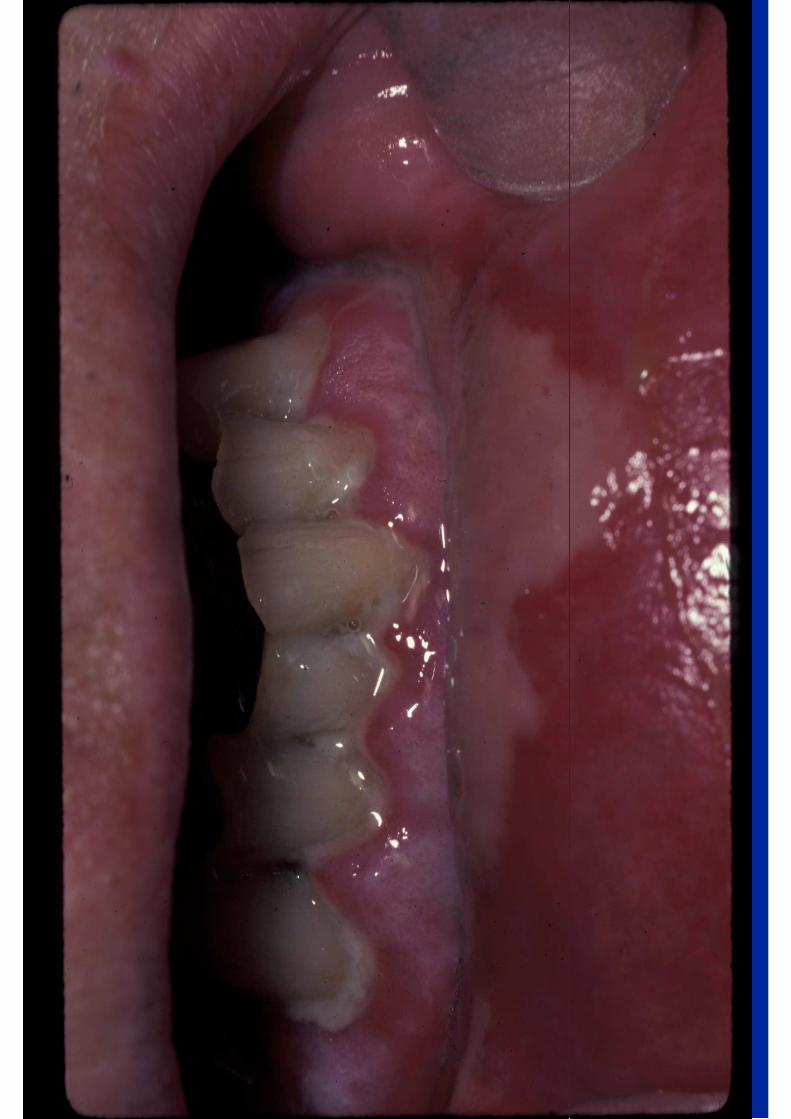
Oral Mucositis
Joel Epstein DMD, MSD, FRCD(C), FDS RCS(Ed)Diplomate American Board of Oral Medicine
Samuel Oschin Comprehensive Cancer InstituteCedars-Sinai Medical Center, Los Angeles, CA
Department of SurgeryCity of Hope National Medical Center,Duarte, CA
Oralmedicinepacific.com
Oral/Dental Complications � Oral and dental care:
– prevention and intervention – before, during and following cancer therapy:
� Acute complications: – mucositis, stomatitis, saliva (quantity, quality), taste, pain,
infection
� Chronic complications: – Mucositis/stomatitis, pain, saliva (quantity, quali ty),
infection, taste, tissue necrosis, caries, periodon tal disease, oral function, rehabilitation
� Impact: cost of care, hospitalization, diet/nutriti on, speech, esthetics, infection risk, pain, systemic health, activity of daily living, quality of life
Why does mucositis matter in the treatment of potentially fatal disease:
� Common & debilitating� Pain, functional impact:
� Oral intake, dysphagia, dehydration, weight loss, ( need for nutritional support), speech, infection risk
� Impact on cancer therapy: � Dose delay, dose reduction, change in CT, treatment breaks, hospitalization,
discontinuing treatment
� Increased costs.
Barasch A, Epstein JB. Dermatol Ther 2011;24:424-31Murphy BA, Beaumont JL, Isitt J,et al.. J Pain Symp Ma nage 2009; 38:522-32.Scully C, Epstein JB, Sonis S. Head Neck 2003;25:105 7-70.; Head Neck 2004;26:77-84Gabriel DA, Shea T, Olajida O, Serody JS, Comeau T. Sem in Oncol 2003;30:76-83Rose-Ped AM, Bellm LA, Epstein JB, et al. Cancer Nurs ing 2002:25:461-467Bellm LA, Epstein JB, Rose-Ped A, et al. Supp Care Ca ncer. 2000; 8:33-39. 59
Impact of Mucositis
� Impact QOL & completion of Cancer TX� Symptom clusters: shared pathobiology 1,2
� True incidence under-estimated� Most clinical trials toxicity not primary endpoint� Most clinical trails report based on PRO, NCI CTCAE 3
� Health professionals assessment of incidence & seve rity less than patient report 4
� Pain, swallowing, speech, eating, feeling ill, wght loss, overall QoL (all p<0.01) 5
� ↑ toxicity in elderly (p=0.04) 5
1 Aprile G, Ramoni M, Keefe D. Curr Opin Supp Palliat Ca re 2009;3:50-42 Nishimura N, , Nakano K, Ueda K. Support Care Can cer 2011
3. Saed ED. Ind J Med Res 2011;134:413-84. Bateman E, Keefe D. Semin Oncol 2011;38:358-61
5.Liu Y, Guan X, Zhu G. Oral Oncol 2012
61
Outcomes of Oral Mucositis in HNC
� 103 consecutive HNC, chart review� 81% males; 80% Caucasian; average 66 Gy� Mucosal ulcers associated with:
• ↑↑↑↑ topical & opioid analgesics (p<0.001) •↑ weight loss (p=0.02) •↑ feeding tubes (p=0.07) • RT delay 6% vs 0% without ulcers
Elting L, Cookelsy C, Garden A. Supp care Cancer 2005; 13:443
Outcomes of Oral Mucositis in HNC
� Retrospective review 204 consecutive pts treated 20 02, single center
� Mucositis 91% � 66% severe (gr 3-4); severity & duration ↑ with RT+CT
� OM more common: � combined CT/RT (OR 7.8) p=0.02), � altered fractionation RT (OR 6.3, p=0.03)
� Severe mucositis:� associated with severe pain (54% v 6%, p<0.001) � weight loss >5% (60% v 17%, P<0.001)
� OM associated with ↑cost: $1,700 (mild mucositis) to $6,000 (severe mucositis)
Elting LS, Cooksley CD, Chambers MS, Garden AS. Int J Radiat Oncol Biol Phys 2007;68:1110-20
62
Mucositis in HNC: morbidity & resource utilization
� 75 pts, 6 centers; RT+CT 67%, 33% RT alone� 76% mouth/throat soreness, opioids in 85%� Mucositis pain affects function despite opioids� Resource utilization:
� tube feeding 51% � hospitalization 31% (30% recorded due to mucositis), average LOS 4.9 days
Murphy BA, Beaumont JL, Isitt J, Garden AS, Gwede CK, et aly. J Pain Symp Manage 2009;38(4):522-32.
63
Oral Mucositis: Resource utilization in HNC
� Prospective study: 69 pts; 75% OSCC or OPC; 49% IMRT with chemo; 72% male
� 90% mouth & throat soreness (MTS) > 2; only 6% no MTS
� Patients with MTS: – non-prophylactic G-tubes 25% – unplanned office visits 37%– hospitalization 18%
Keefe D et al. Supp Care Cancer 2007:395
64
Survey of Professional Burden of Mucositis in HNSCC
• 50 Rad Onc & 51 Oncol Nurses, tx average of 6-12 HNC pts/mo
• Mean target RT 72 Gy; 92% developing mucositis, 71% Gr 2 or 3 (WHO), 16% Gr 4
• Rad Onc spend 7.2hrs, nurses 12.1 hrs managing mucositis, increasing time as mucositis increased
Xiao X, Barron RL, Mautner B et al. J Support Care C ancer 2010
Targeted Agents, immunotherapy & oral complications
� EGFRi (cetuximab): erythema , pain; ↑mucositis with cytotoxicTX, anterior mucositis, in field/ out of field muco sitis/dermatitis; taste change
� Anti-VEGF (bevacizumab): bleeding, delayed healing, osteonecrosis; taste
� Tki (sunitinib/sorafinib): osteonecrosis, lichenoid m ucositis; taste
� mTORi (tacro-, siro-, evero-, ridaforo-limus): stoma titis (aphthous-like), pain; lichenoid; taste
� Immunotherapy� Different pathobiology, different management
MASCC/ISOO Evidence -Based Clinical Practice Guidelines for Oral Mucositis (2014)
� Recommend for prevention:– Cryotherapy 30 mins bolus 5-FU CT (level evidence II ) – KGF-1-palifermin for high-dose CT + TBI in auto-HSC T (level evidence II)– LLLT (2J/cm 2; 2 secs/point) for HSCT with high dose CT, with or without TBI
(level evidence II)– Benzydamine HNC for standard dose RT (level evidence I)
� Recommend for Treatment: – PCA for oral pain in HSCT (level evidence II)
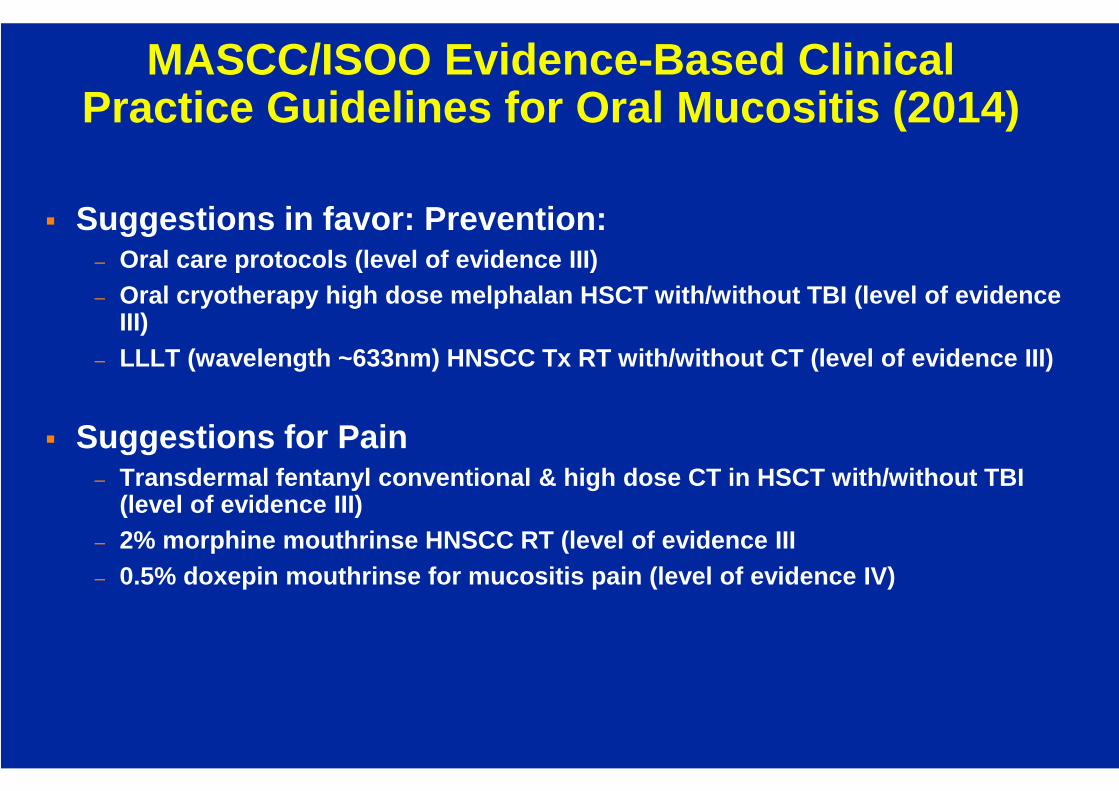
MASCC/ISOO Evidence -Based Clinical Practice Guidelines for Oral Mucositis (2014)
� Suggestions in favor: Prevention: – Oral care protocols (level of evidence III)– Oral cryotherapy high dose melphalan HSCT with/witho ut TBI (level of evidence
III)– LLLT (wavelength ~633nm) HNSCC Tx RT with/without CT (level of evidence III)
� Suggestions for Pain– Transdermal fentanyl conventional & high dose CT in HSCT with/without TBI
(level of evidence III)– 2% morphine mouthrinse HNSCC RT (level of evidence I II– 0.5% doxepin mouthrinse for mucositis pain (level of evidence IV)
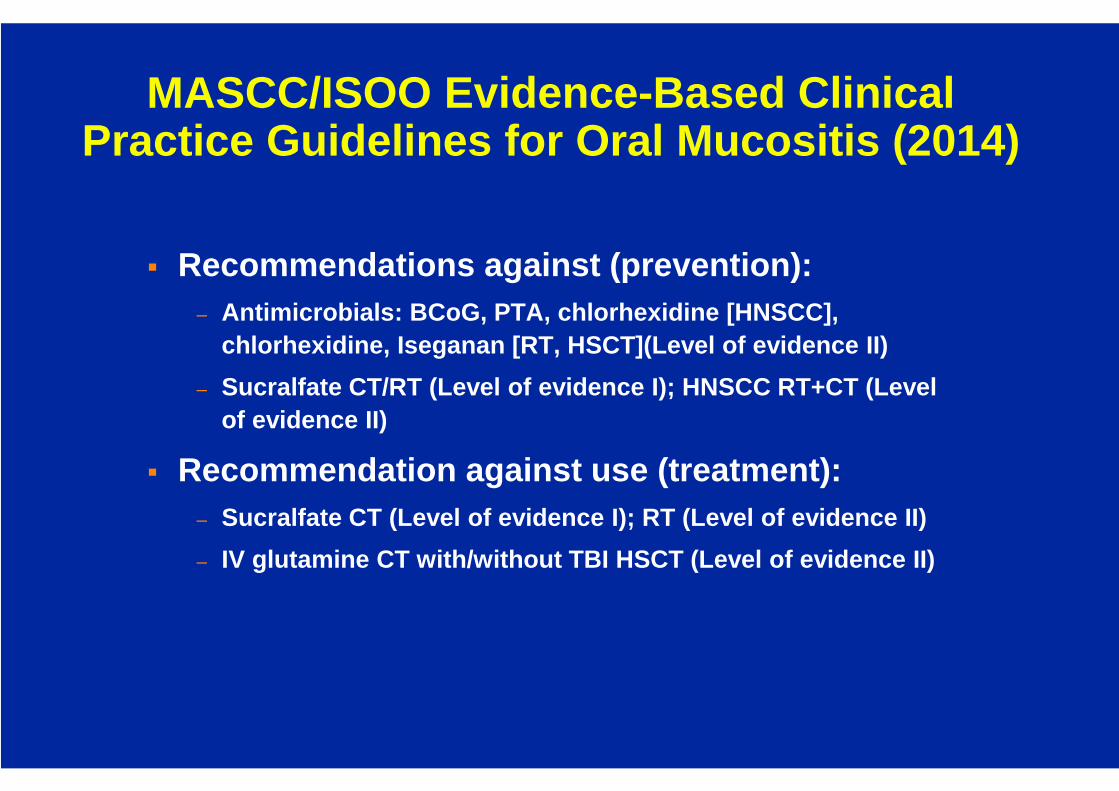
MASCC/ISOO Evidence -Based Clinical Practice Guidelines for Oral Mucositis (2014)
� Recommendations against (prevention): – Antimicrobials: BCoG, PTA, chlorhexidine [HNSCC],
chlorhexidine, Iseganan [RT, HSCT](Level of evidence II)
– Sucralfate CT/RT (Level of evidence I); HNSCC RT+CT (Level of evidence II)
� Recommendation against use (treatment): – Sucralfate CT (Level of evidence I); RT (Level of ev idence II)
– IV glutamine CT with/without TBI HSCT (Level of evi dence II)
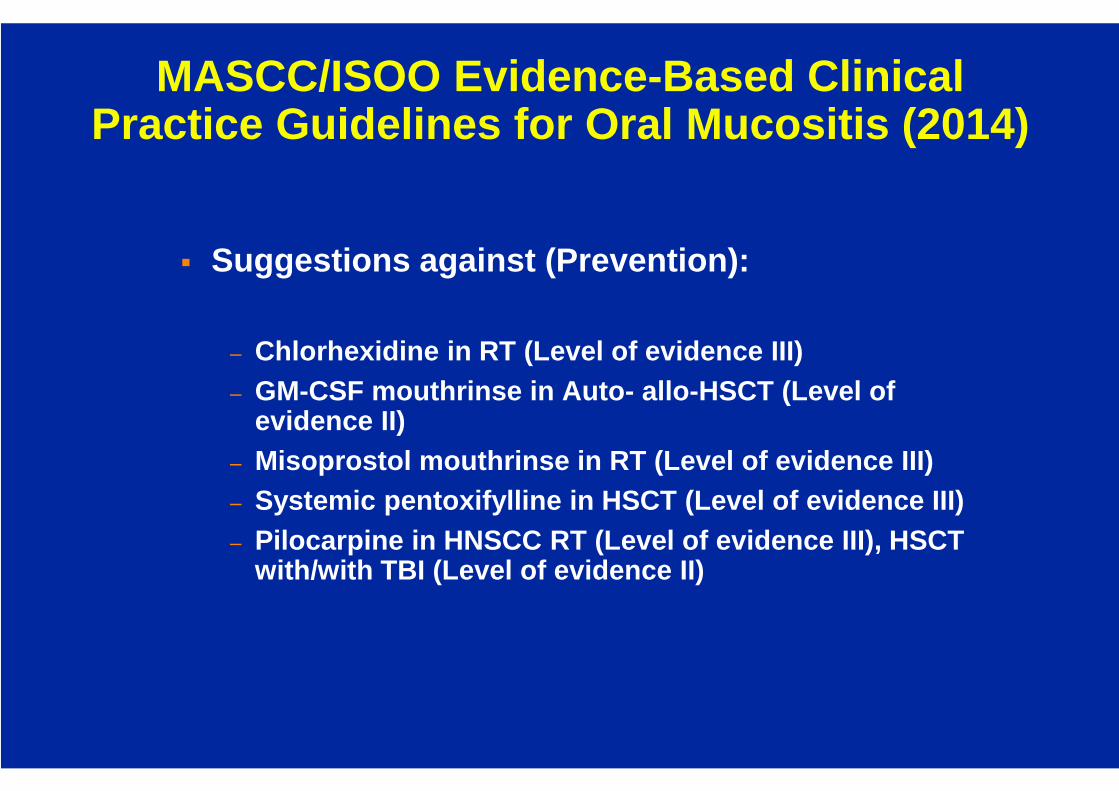
MASCC/ISOO Evidence -Based Clinical Practice Guidelines for Oral Mucositis (2014)
� Suggestions against (Prevention):
– Chlorhexidine in RT (Level of evidence III)– GM-CSF mouthrinse in Auto- allo-HSCT (Level of
evidence II)– Misoprostol mouthrinse in RT (Level of evidence III)– Systemic pentoxifylline in HSCT (Level of evidence I II)– Pilocarpine in HNSCC RT (Level of evidence III), HSC T
with/with TBI (Level of evidence II)
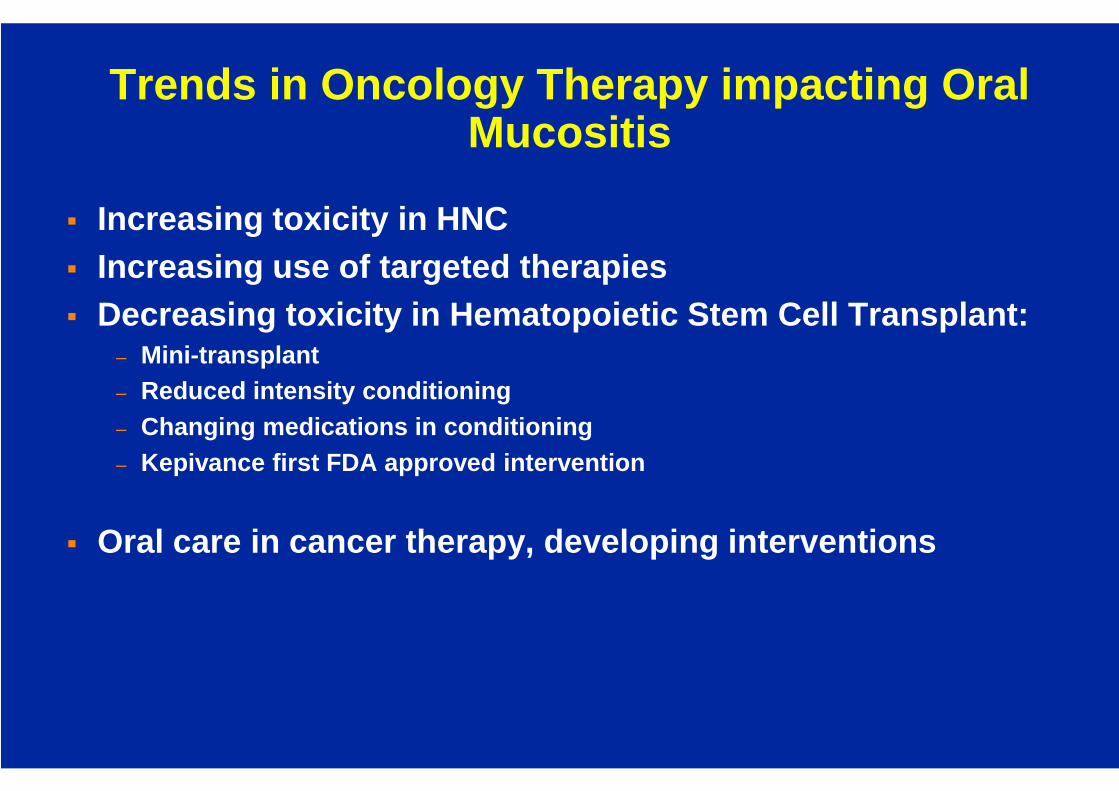
Trends in Oncology Therapy impacting Oral Mucositis
� Increasing toxicity in HNC� Increasing use of targeted therapies� Decreasing toxicity in Hematopoietic Stem Cell Tran splant:
– Mini-transplant– Reduced intensity conditioning– Changing medications in conditioning– Kepivance first FDA approved intervention
� Oral care in cancer therapy, developing interventio ns
Mucositis and QOL
� Impact QOL & completion of Cancer TX� Symptom clusters: shared pathobiology 1,2
� True incidence under-estimated– Most clinical trials toxicity is not primary endpoi nt, report based on PRO, NCI
CTCAE 3
– Health professionals assessment of incidence and se verity lower than patient report 4
1 Aprile G, Ramoni M, Keefe D. Curr Opin Supp Palliat Ca re 2009;3:50-42 Nishimura N, , Nakano K, Ueda K. Support Care Can cer 20113. Saed ED. Ind J Med Res 2011;134:413-84. Bateman E, Keefe D. Semin Oncol 2011;38:358-61
Advances in Cancer Therapy: Targeted Therapy/Immunotherapy
Personalized Medicine
� New drug or TX presents new toxicity(s)� Understanding mechanism of action is key to managem ent� Multimodality TX� Symptoms clusters� Toxicity assessment: validated PROs, scales� Antitumor effect must not be compromised by TX of t oxicity� Risk prediction (personalized medicine).
MucositisA fish hook lodges in my throat.
Splittle, kindergarten paste, thickens everything-e ven vision.Mouth packed with sores and blisters, swollen ulcer ated tongue.Topside sandpapered with number 7 coarsest grade.Taste buds, saliva glands seared.Cool water, corrosive acid now.The tongue rests; the teeth become enemies now.Coiled steel razored wire stop dentate prison walls.Only moans escape my lips. I cannot eat or speak.
Inside a howl festers.
Pain lengthens time.
-Anita Hart Balter…