Pulmonary hypertension associated with veno-occlusive ... · A 55-year-old female with severe...
4
Journal of Cardiology Cases (2012) 5, e44—e47 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/jccase Case Report Pulmonary hypertension associated with veno-occlusive disease in systemic sclerosis: Insight into the mechanism of resistance to vasodilator Hayato Tada (MD) a,∗ , Tetsuo Konno (MD, FJCC) a , Motohiko Aizu (MD) b , Junichiro Yokawa (MD) a , Toshinari Tsubokawa (MD) a , Hiroshi Fujii (MD) b , Kenshi Hayashi (MD, FJCC) a , Katsuharu Uchiyama (MD) a , Masami Matsumura (MD) b , Mitsuhiro Kawano (MD) b , Masa-aki Kawashiri (MD) a , Masakazu Yamagishi (MD, FJCC) a a Division of Cardiovascular Medicine, Kanazawa University Graduate School of Medicine, Kanazawa, Japan b Division of Rheumatology, Department of Internal Medicine, Kanazawa University Graduate School of Medicine, Kanazawa, Japan Received 20 September 2011; received in revised form 1 November 2011; accepted 6 November 2011 KEYWORDS Pulmonary veno-occlusive disease; Pulmonary hypertension; Pulmonary arterial hypertension; Epoprostenol Summary We report a case with pulmonary veno-occlusive disease (PVOD) associated with systemic sclerosis which exhibits strong resistance to pulmonary vasodilator. A 55-year-old female with severe pulmonary hypertension was admitted to our hospital to be introduced to epoprostenol infusion therapy. She was diagnosed as having pulmonary arterial hypertension (PAH) associated with systemic sclerosis at the age of 51. Several aggres- sive treatments with pulmonary vasodilators, including oral prostaglandin, endothelin receptor antagonists, and phosphodiesterase 5 inhibitors, failed to improve her symptoms. We introduced continuous intravenous epoprostenol therapy from 2 g/kg/min for her. However, pulmonary edema appeared and worsened in a dose-dependent manner. We made a diagnosis of PVOD clinically at that time. Thereafter, pulmonary edema gradually disappeared consistent with the reduction of the dose of epoprostenol infusion. She died of renal failure and infection 4 months after the introduction of epoprostenol infusion therapy. A histological examination revealed severe stenosis and occlusions of pulmonary veins as well as pulmonary arteries over a wide area. We suggest that prevalence of veno-occlusive type of disease could be one of the major mechanisms of less responsive or even refractory to pulmonary vasodilator therapies in patients with PAH associated with connective tissue disease. © 2011 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved. ∗ Corresponding author at: Division of Cardiovascular Medicine, Kanazawa University Graduate School of Medicine, 13-1 Takara-machi, Kanazawa 920-8641, Japan. Tel.: +81 76 265 2000/2251; fax: +81 76 234 4251. E-mail address: [email protected] (H. Tada). 1878-5409/$ — see front matter © 2011 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jccase.2011.11.001
Transcript of Pulmonary hypertension associated with veno-occlusive ... · A 55-year-old female with severe...

J
C
Pvi
HJKMM
a
b
J
R
K
1d
ournal of Cardiology Cases (2012) 5, e44—e47
Available online at www.sciencedirect.com
journa l homepage: www.e lsev ier .com/ locate / j ccase
ase Report
ulmonary hypertension associated witheno-occlusive disease in systemic sclerosis: Insightnto the mechanism of resistance to vasodilator
ayato Tada (MD)a,∗, Tetsuo Konno (MD, FJCC)a, Motohiko Aizu (MD)b,unichiro Yokawa (MD)a, Toshinari Tsubokawa (MD)a, Hiroshi Fujii (MD)b,enshi Hayashi (MD, FJCC)a, Katsuharu Uchiyama (MD)a,asami Matsumura (MD)b, Mitsuhiro Kawano (MD)b,asa-aki Kawashiri (MD)a, Masakazu Yamagishi (MD, FJCC)a
Division of Cardiovascular Medicine, Kanazawa University Graduate School of Medicine, Kanazawa, JapanDivision of Rheumatology, Department of Internal Medicine, Kanazawa University Graduate School of Medicine, Kanazawa,apan
eceived 20 September 2011; received in revised form 1 November 2011; accepted 6 November 2011
KEYWORDSPulmonaryveno-occlusivedisease;Pulmonaryhypertension;Pulmonary arterialhypertension;Epoprostenol
Summary We report a case with pulmonary veno-occlusive disease (PVOD) associated withsystemic sclerosis which exhibits strong resistance to pulmonary vasodilator.
A 55-year-old female with severe pulmonary hypertension was admitted to our hospitalto be introduced to epoprostenol infusion therapy. She was diagnosed as having pulmonaryarterial hypertension (PAH) associated with systemic sclerosis at the age of 51. Several aggres-sive treatments with pulmonary vasodilators, including oral prostaglandin, endothelin receptorantagonists, and phosphodiesterase 5 inhibitors, failed to improve her symptoms. We introducedcontinuous intravenous epoprostenol therapy from 2 �g/kg/min for her. However, pulmonaryedema appeared and worsened in a dose-dependent manner. We made a diagnosis of PVODclinically at that time. Thereafter, pulmonary edema gradually disappeared consistent with thereduction of the dose of epoprostenol infusion. She died of renal failure and infection 4 monthsafter the introduction of epoprostenol infusion therapy. A histological examination revealed
severe stenosis and occlusions of pulmonary veins as well as pulmonary arteries over a widearea. We suggest that prevalence of veno-occlusive type of disease could be one of the majormechanisms of less responsive owith PAH associated with conne© 2011 Japanese College of Car∗ Corresponding author at: Division of Cardiovascular Medicine, Kanazaanazawa 920-8641, Japan. Tel.: +81 76 265 2000/2251; fax: +81 76 234
E-mail address: [email protected] (H. Tada).
878-5409/$ — see front matter © 2011 Japanese College of Cardiology.oi:10.1016/j.jccase.2011.11.001
r even refractory to pulmonary vasodilator therapies in patients
ctive tissue disease.diology. Published by Elsevier Ltd. All rights reserved.wa University Graduate School of Medicine, 13-1 Takara-machi,4251.
Published by Elsevier Ltd. All rights reserved.

ase
vt
C
AinTmwdotd
Pulmonary hypertension associated with veno-occlusive dise
Introduction
Recent advances regarding the treatment for pulmonaryhypertension, especially, for pulmonary arterial hyperten-sion (PAH) have improved the prognosis of patients withPAH [1,2]. Several reports have described that connec-tive tissue diseases such as systemic sclerosis and systemiclupus erythematosus could be complicated by severe PAHwhich worsens their prognosis [3,4]. Pulmonary hyperten-sion associated with connective tissue disease has beencategorized into PAH. Pulmonary veno-occlusive disease(PVOD) has been described as a relatively rare cause ofpulmonary hypertension that affects predominantly post-capillary pulmonary vessels. A major concern with PVOD isthe poor responsiveness to available pulmonary vasodilators,
especially, the risk of pulmonary edema with continu-ous intravenous epoprostenol therapy [5,6]. We recentlyexperienced a case with PVOD associated with systemicsclerosis which exhibited strong resistance to pulmonarynb2a
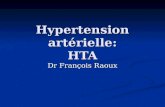
Figure 1 Imaging of the case. Electrocardiogram at admission reveaprecordial leads with right ventricular strain pattern (A). Chest X-rayarch and pulmonary artery trunk (B). Echocardiography revealed dilwith flattening of ventricular septum (C). High-resolution computedopacities and septal thickness (D, arrow).
in systemic sclerosis e45
asodilators, including continuous intravenous epoprostenolherapy.
ase report
55-year-old female was admitted to our hospital for thentroduction of epoprostenol infusion therapy. She was diag-osed as having systemic sclerosis at the age of 39 years.he initial diagnosis of her pulmonary hypertension wasade when she was 51 years old. She had been treatedith beraprost since then. Thereafter, her symptoms ofyspnea gradually worsened associated with the increasef pulmonary artery pressure in spite of the introduc-ion of sildenafil, ambrisentan, and home oxygen therapyuring four years of the clinical course. Physical exami-
ation at admission revealed a heart rate of 80 bpm, alood pressure of 90/52 mmHg, and a respiratory rate of0 breaths/min. She had some signs of fluid overload suchs jugular vein distension and lower extremity edema andled right ventricular hypertrophy findings of tall R waves in rightdemonstrated bilateral hilar enlargement, a prominent medialatation of right ventricle, and normal left ventricular function
tomography of her chest revealed centrilobular ground-glass

e
wAPerr(etruwflti(m
9mt13leohBcTsi
Flhtaoe
46
as in functional New York Heart Association class III.rterial blood gas analysis revealed hypoxemia (pH 7.41,aCO2 35 mmHg, PaO2 79 mmHg under O2 2 L/min). Thelectrocardiogram revealed a sinus rhythm of 80 bpm, andight ventricular hypertrophy findings of tall R waves inight precordial leads with right ventricular strain patternFig. 1A). Chest X-ray (Fig. 1B) demonstrated bilateral hilarnlargement, a prominent medial arch and pulmonary arteryrunk. Echocardiography confirmed dilatation of both theight atrium and right ventricle, and normal left ventric-lar function (left ventricular ejection fraction of 62%)ith flattening of ventricular septum (Fig. 1C). Trans-mitralow velocity pattern revealed abnormal relaxation, andhe ratio of mitral inflow and mitral annular tissue Doppler
maging velocities (E/e′) was within the normal range8.3). Right heart catheterization demonstrated severe pul-onary hypertension (pulmonary arterial systolic pressureoap
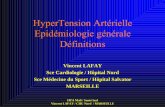
igure 2 Histopathological findings. Macroscopic finding of heart; Teft and right ventricles (A). Small pulmonary artery revealed pronoypertension (B, Elastica van Gieson stain, ×200). Small pulmonarhickening characteristics of pulmonary veno-occlusive disease (C, Erea showed dilatation like angioma (D, hematoxylin and eosin stainbserved (E, arrow). Intra-alveolar macrophages were observed (F, axistence of iron in the alveoli (G, arrow, Fe-stain, ×200). LV, left v
H. Tada et al.
4 mmHg, pulmonary arterial diastolic pressure 27 mmHg,ean pulmonary arterial pressure 48 mmHg) in contrast to
he normal range of pulmonary capillary wedge pressure4 mmHg. Other important parameters were cardiac output.9 L/min, (thermo dilution method) and pulmonary vascu-ar resistance 540 dynes s cm−5. After these examinations,poprostenol infusion therapy was introduced from the dosef 2 �g/kg/min. However, pulmonary edema appeared ander oxygenation worsened in a dose-dependent manner.ased on this clinical course, we made a diagnosis of PVODlinically and the dose of epoprostenol was 12 �g/kg/min.hereafter, pulmonary edema gradually recovered con-istent with the reduction of the dose of epoprostenolnfusion. A high-resolution computed tomography (HRCT)
f her chest revealed centrilobular ground-glass opacitiesnd septal thickness (Fig. 1D). Lung transplantation wasroposed as the sole treatment option to prolong her life,ransverse section of the heart showing hypertrophy of both theunced intimal fibrosis, as typically seen in pulmonary arterialy vein showed fibrotic occlusive lesions with marked intimallastica van Gieson stain, ×200). The capillaries in the alveolar, ×200). Macroscopic findings of lung; alveolar hemorrhage wasrrow, hematoxylin and eosin stain, ×40). Fe-stain revealed theentricle; RV, right ventricle.

ase
tmd
A
WYt
R
[
[
[
[
[
[
[
[
Pulmonary hypertension associated with veno-occlusive dise
but she declined. The patient died of renal failure andinfection 4 months after the introduction of epoprostenolinfusion therapy. Histopathological examination of her heartrevealed hypertrophy of both ventricles without any appar-ent pathological interstitial fibrotic change (Fig. 2A). Inaddition to the findings of small pulmonary arteries thatrevealed pronounced intimal fibrosis as typically seen in PAH(Fig. 2B), small pulmonary vein also showed fibrotic occlu-sive lesions with marked intimal thickening characteristicsof PVOD (Fig. 2C). The capillaries in the alveolar area showeddilatation like angioma (Fig. 2D) as well as the findings ofintra-alveolar hemorrhage (Fig. 2E—G). On the basis of thesepathological findings and clinical features, the patient wasdiagnosed as having PVOD.
Discussion
Even though PAH and PVOD share many similarities, theclinical classification was modified to separate PVOD fromother forms of PAH following the Fourth World Symposiumon PAH held in 2008 at Dana Point, CA, USA [7]. It is cur-rently well established that PAH associated with connectivetissue disease such as systemic sclerosis is frequently lessresponsive or even refractory to pulmonary vasodilator ther-apies. The likely mechanism is a selective dilatation of thesmall pulmonary arteries without associated pulmonary ven-odilatation which could cause an increase in trans-capillaryhydrostatic pressure. Several papers have described the use-fulness of HRCT to predict the presence of PVOD [8,9]. Ourcase also showed centrilobular ground-glass opacities andseptal thickness; however, the findings of HRCT suggestingthe presence of PVOD were obtained after the introduc-tion of epoprostenol infusion therapy. Thus, we could notsuspect PVOD until then. Several studies suggested thatthe frequencies of veno-occlusive types of disease in thepatients with PAH associated with connective tissue diseasemight be larger than expected, and there is some evidencefrom histopathological reports to support this hypothesis[5]. However, the current definite diagnosis of PVOD can bemade histopathologically, thus, limiting the estimation forthe accurate involvements of this type of disease.
In conclusion, we report a case with PVOD associated
with systemic sclerosis which exhibits strong resistanceto pulmonary vasodilator. We suggest that prevalenceof veno-occlusive type of disease could be one of themajor mechanisms of less responsive or even refractory[
in systemic sclerosis e47
o pulmonary vasodilator therapies to patients with pul-onary hypertension associated with connective tissueisease.
cknowledgments
e express our special thanks to Kazuko Honda and Sachioamamoto (staff of Kanazawa University) for their assis-ance.
eferences
1] Lourenco AP, Fontoura D, Henriques-Coello T, Leite-Moreira AF.Current pathophysiological concepts and management of pul-monary hypertension. Int J Cardiol June 2011 [Epub ahead ofprint].
2] Gomberg-Maitland M, Dufton C, Oudiz RJ, Benza RL. Compellingevidence of long-term outcomes in pulmonary arterial hyperten-sion? A clinical perspective. J Am Coll Cardiol 2011;57:1053—61.
3] Koh ET, Lee P, Gladman DD, Abu-Shakra M. Pulmonary hyper-tension in systemic sclerosis: an analysis of 17 patients. Br JRheumatol 1996;35:989—93.
4] Mathai SC, Hummers LK, Champion HC, Wigley FM, ZaimanA, Hassoun PM, Girgis RE. Survival in pulmonary hyperten-sion associated with the sceroderma spectrum of diseases:impact of interstitial lung disease. Arthritis Rheum 2009;60:569—77.
5] Montani D, Achouh L, Dorfmüller P, Le Pavec J, Sztrymf B,Tchérakian C, Rabiller A, Haque R, Sitbon O, Jaïs X, Dartev-elle P, Maître S, Capron F, Musset D, Simonneau G, et al.Pulmonary venoocclusive disease: clinical, functional, radio-logic, and hemodynamic characteristics and outcome of 24cases confirmed by histology. Medicine (Baltimore) 2008;87:220—33.
6] Montani D, Price LC, Dorfmuller P, Achouh L, Jaïs X, Yaïci A,Sitbon O, Musset D, Simonneau G, Humbert M. Pulmonary veno-occlusive disease. Eur Respir J 2009;33:189—200.
7] Simonneau G, Robbins IM, Beghetti M, Channick RN, DelcroixM, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC,Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clin-ical classification of pulmonary hypertension. J Am Coll Cardiol2009;54:S43—54.
8] Iwaki M, Imaizumi K, Yokoi T, Kondo M, Kawaguchi K, HasegawaY. Idiopathic pulmonary veno-occlusive disease. Intern Med2009;48:1289—92.
9] Montani D, Kemp K, Dorfmuller P, Simonneau G, Humbert M.Idiopathic pulmonary arterial and pulmonary veno-occlusive dis-ease: similarities and differences. Semin Respir Crit Care Med2009;30:411—20.