Prescription antifongique et émergence de la … · Prescription antifongique et émergence de la...
35
Prescription antifongique et émergence de la résistance Olivier Lortholary M.D.; Ph.D Centre National de Référence Mycoses Invasives & Antifongiques, Unité de Mycologie Moléculaire, CNRS URA3012 Institut Pasteur, & Centre d’Infectiologie Necker-Pasteur Université Paris Descartes, Hôpital Necker Enfants malades, IHU Imagine Paris, France. Impossible d’afficher l’image. Impossible d’afficher l’image.
Transcript of Prescription antifongique et émergence de la … · Prescription antifongique et émergence de la...

Prescription antifongique et émergence de la résistance
Olivier Lortholary M.D.; Ph.D
Centre National de Référence Mycoses Invasives & Antifongiques,
Unité de Mycologie Moléculaire, CNRS URA3012 Institut Pasteur,
& Centre d’Infectiologie Necker-Pasteur Université Paris Descartes, Hôpital Necker Enfants malades,
IHU Imagine Paris, France. Impossible d’afficher l’image.
Impossible d’afficher l’image.
Polling Question
Which of the following infectious organisms have increased in resistance at your institution over the past several years? Select all that apply.
1. Aspergillus
2. Candida
3. Coccidioides
4. Fusarium
5. Mucorales
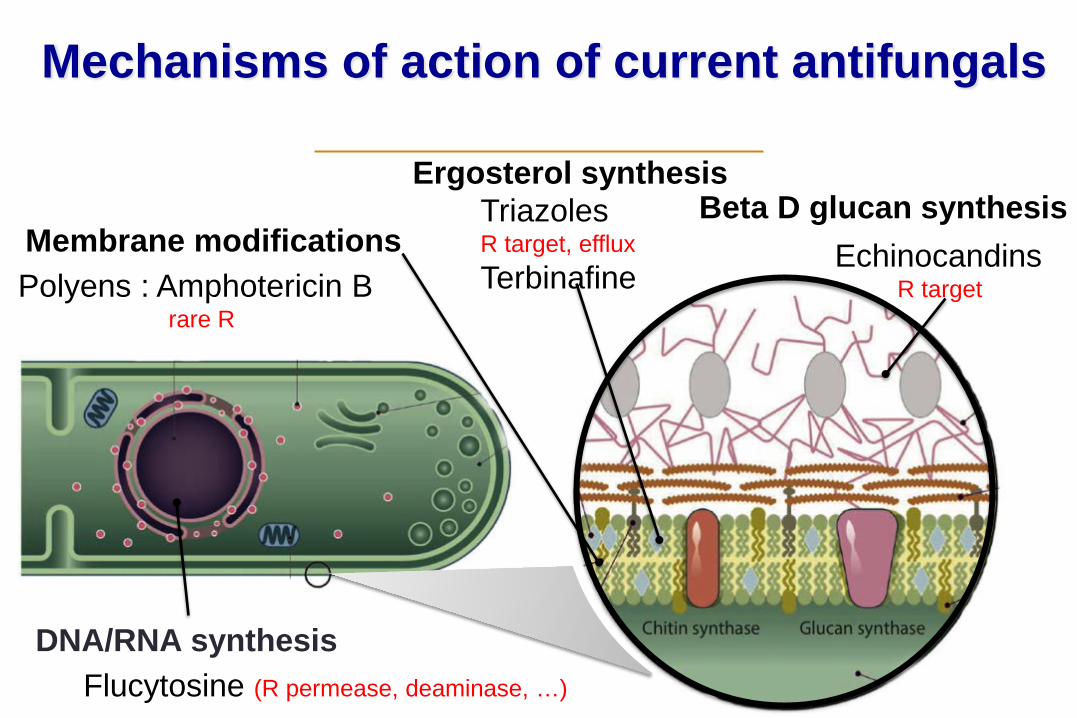
DNA/RNA synthesis Flucytosine (R permease, deaminase, …)
Ergosterol synthesis
Polyens : Amphotericin B rare R
Membrane modifications Triazoles R target, efflux Terbinafine
Beta D glucan synthesis Echinocandins
R target
Mechanisms of action of current antifungals
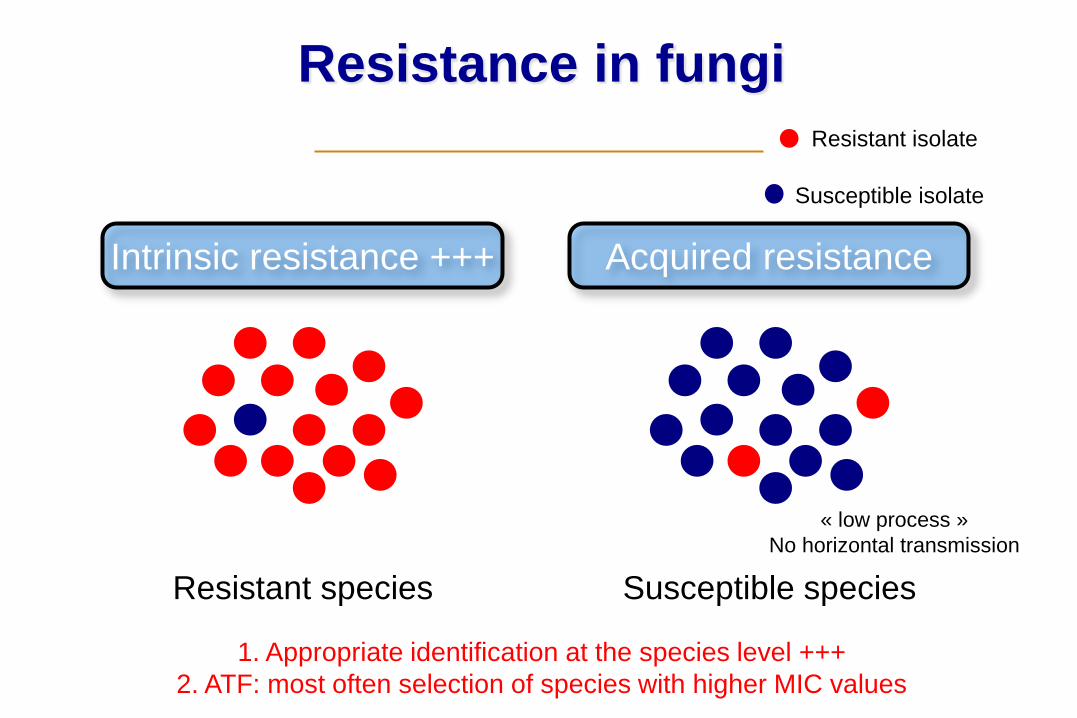
Resistance in fungi
Susceptible species Resistant species
Intrinsic resistance +++ Acquired resistance
Resistant isolate
Susceptible isolate
1. Appropriate identification at the species level +++ 2. ATF: most often selection of species with higher MIC values
« low process » No horizontal transmission
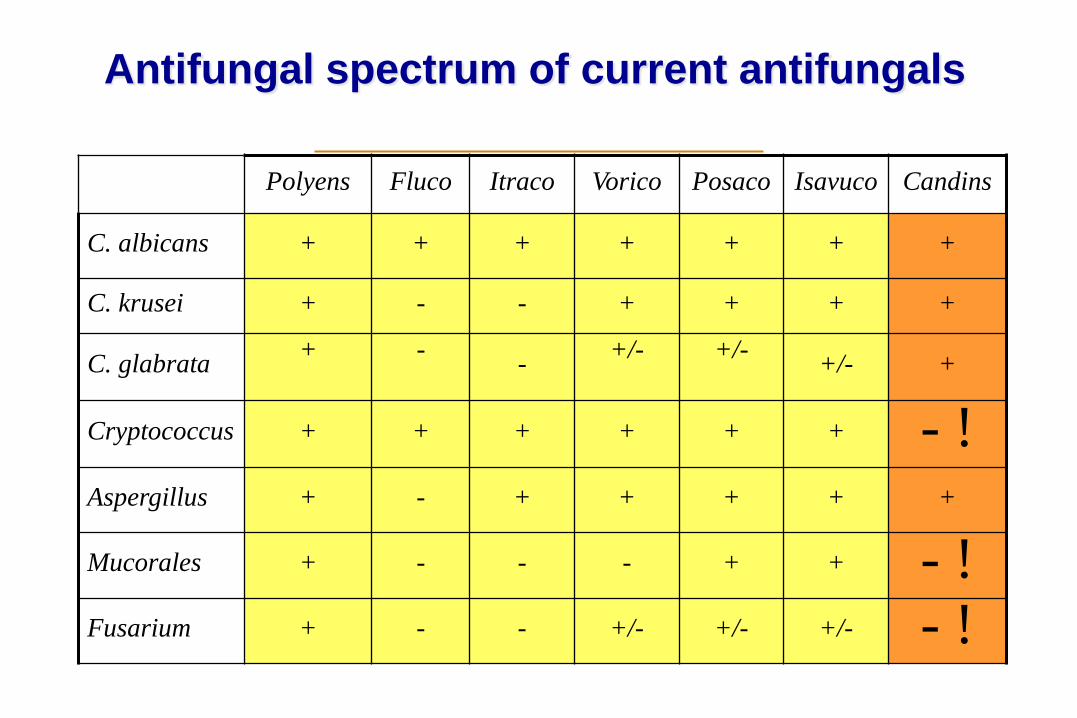
Antifungal spectrum of current antifungals
Polyens Fluco Itraco Vorico Posaco Isavuco Candins
C. albicans + + + + + + +
C. krusei + - - + + + +
C. glabrata +
- - +/-
+/-
+/- +
Cryptococcus + + + + + + - ! Aspergillus + - + + + + +
Mucorales + - - - + + - ! Fusarium + - - +/- +/- +/- - !

C A N D I D A
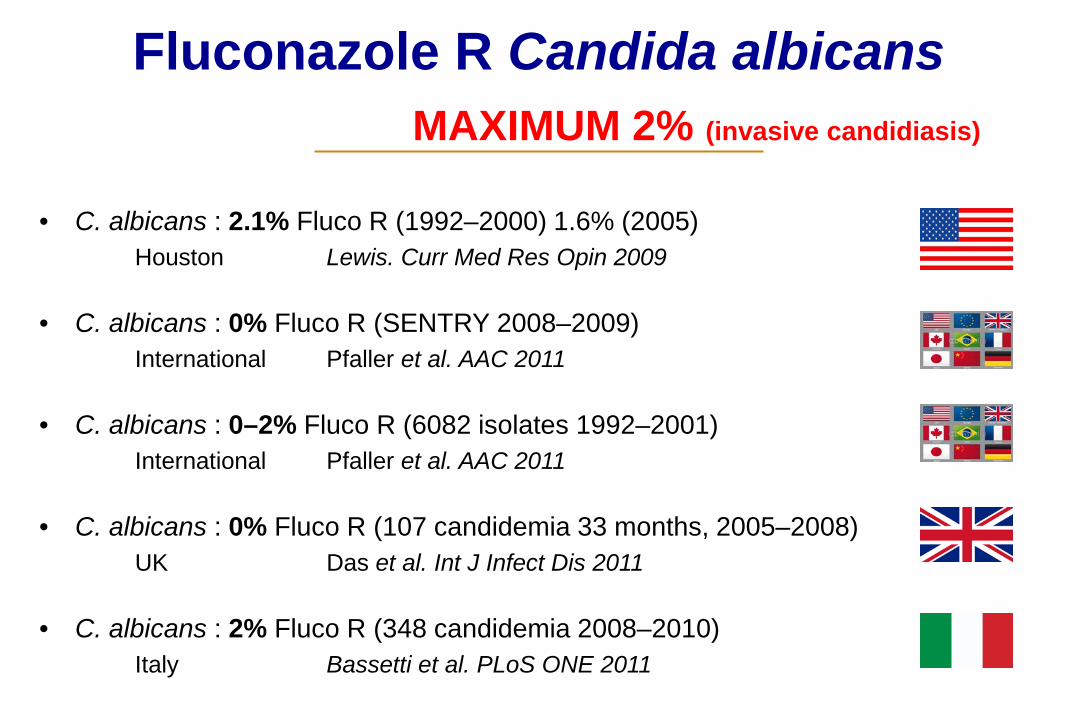
Fluconazole R Candida albicans
• C. albicans : 2.1% Fluco R (1992–2000) 1.6% (2005) Houston Lewis. Curr Med Res Opin 2009 • C. albicans : 0% Fluco R (SENTRY 2008–2009) International Pfaller et al. AAC 2011 • C. albicans : 0–2% Fluco R (6082 isolates 1992–2001) International Pfaller et al. AAC 2011 • C. albicans : 0% Fluco R (107 candidemia 33 months, 2005–2008) UK Das et al. Int J Infect Dis 2011 • C. albicans : 2% Fluco R (348 candidemia 2008–2010) Italy Bassetti et al. PLoS ONE 2011
MAXIMUM 2% (invasive candidiasis)

No increased resistance to azoles among susceptible Candida species during fungemia in
Paris area
Unpublished data, provided by the NRCMA (French National Reference Center for Mycoses and Antifungals), Institut Pasteur Paris.
MICs; EUCAST Fcz > 4 µg/ml Vcz > 0.12 µg/ml
0.2% FCZ R
Similar conclusion by US CDC [Cleveland, CID 2012]
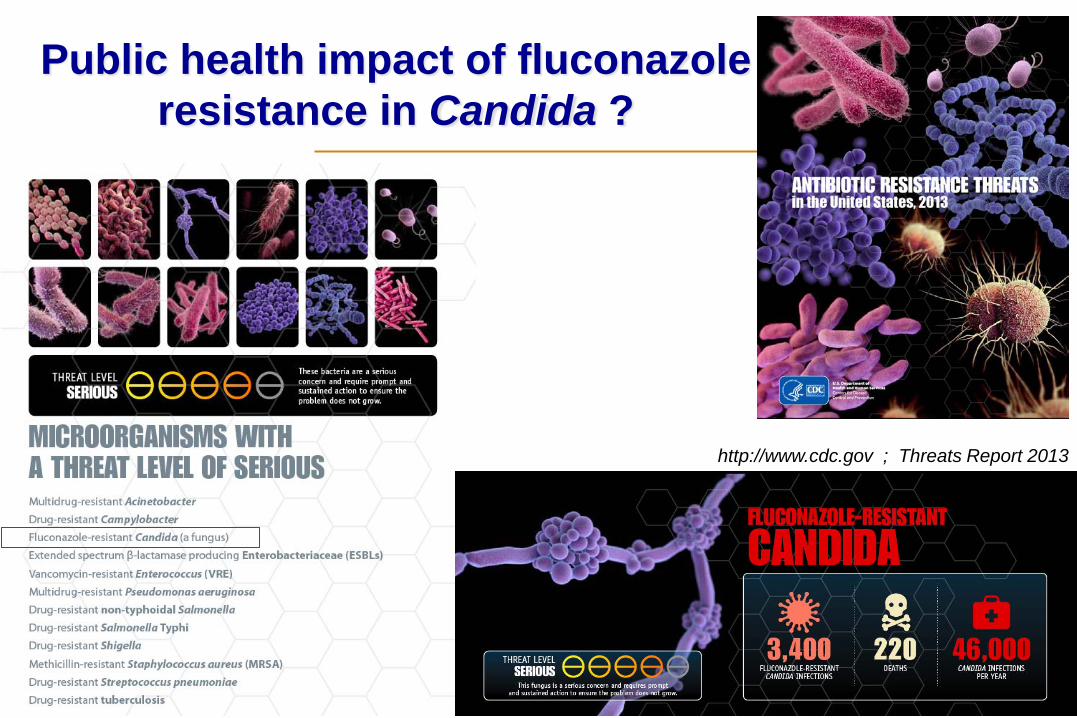
Public health impact of fluconazole resistance in Candida ?
http://www.cdc.gov ; Threats Report 2013

Echinocandin resistant Candida isolates
• 5% Caspofungin R (168 Candida sp 2001–2007) Houston Sipsas et al. Cancer 2009
• 0–1% MIC >2 Caspofungin (13147 Candida sp 1992–2006) International database Lewis et al. Curr Med Res Opin 2009 • 0–2% Caspofungin R (238 bloodstream isolates 2005–2006) Sweden Axner-Elings et al. JCM 2011 • 0.4% (6/1643) Caspofungin R among C. albicans, C. glabrata and C. krusei isolates (1643 isolates, 2002–2009) Paris
Dannaoui et al. Emerg Infect Dis 2012 • 1% Echinocandin R (2329 Candida spp. 65% C. glabrata 2008–2011) Atlanta & Baltimore Cleveland et al. CID 2012 Recent increase: 1.2 to 2.9% (+ 147%) and 2.0 to 3.5% (+ 77%) from
2008 to 2013 in Atlanta and Baltimore Cleveland et al. PLoS ONE 2015
Historically rare in the absence of prior exposure !
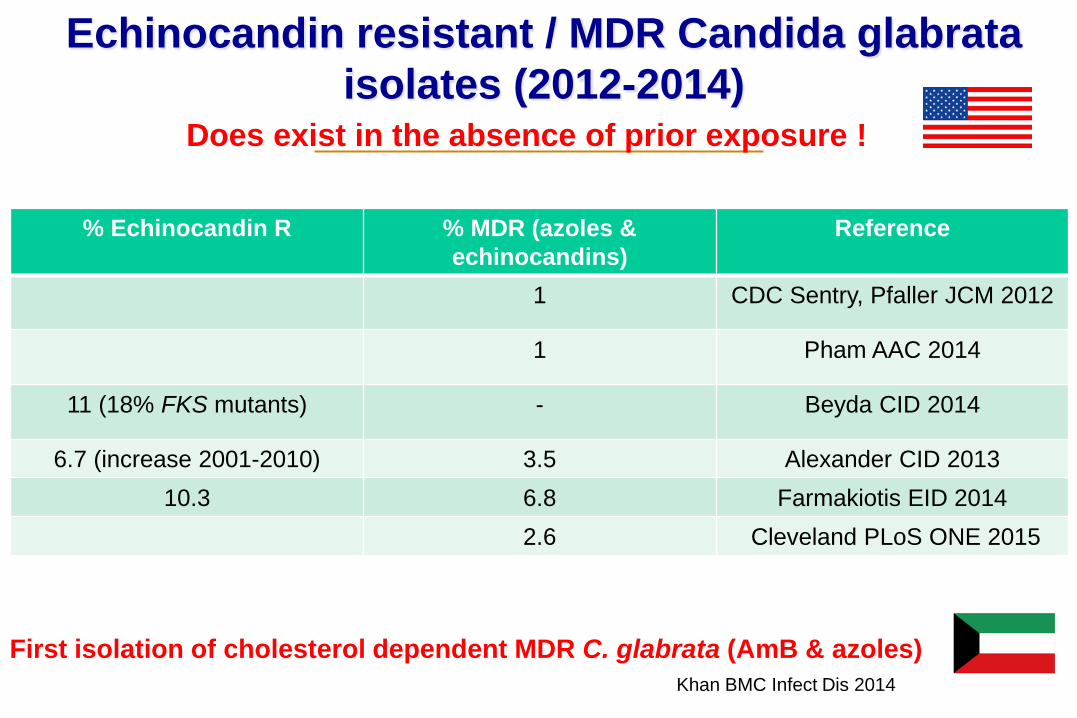
% Echinocandin R % MDR (azoles & echinocandins)
Reference
1 CDC Sentry, Pfaller JCM 2012
1 Pham AAC 2014
11 (18% FKS mutants) - Beyda CID 2014
6.7 (increase 2001-2010) 3.5 Alexander CID 2013 10.3 6.8 Farmakiotis EID 2014
2.6 Cleveland PLoS ONE 2015
Echinocandin resistant / MDR Candida glabrata isolates (2012-2014)
Does exist in the absence of prior exposure !
First isolation of cholesterol dependent MDR C. glabrata (AmB & azoles) Khan BMC Infect Dis 2014
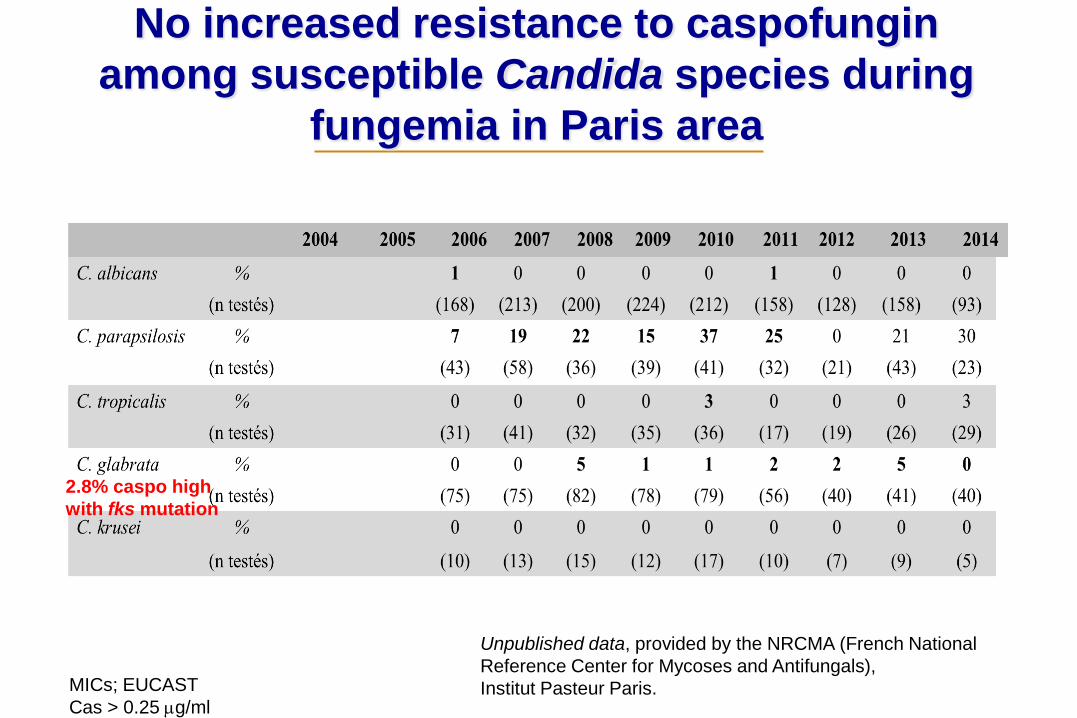
No increased resistance to caspofungin among susceptible Candida species during
fungemia in Paris area
Unpublished data, provided by the NRCMA (French National Reference Center for Mycoses and Antifungals), Institut Pasteur Paris. MICs; EUCAST
Cas > 0.25 µg/ml
2.8% caspo high with fks mutation
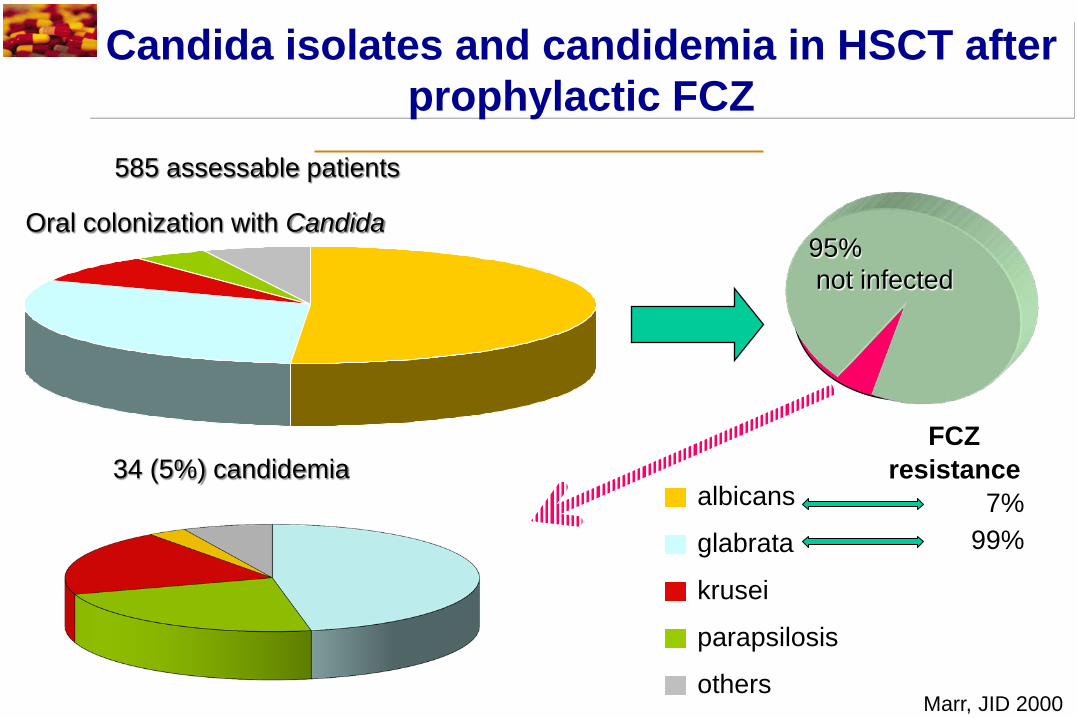
Candida isolates and candidemia in HSCT after prophylactic FCZ
albicans
glabrata
krusei
parapsilosis
others
FCZ resistance
7% 99%
585 assessable patients
Oral colonization with Candida
34 (5%) candidemia
95% not infected
Marr, JID 2000
Risk of candidemia due to fluconazole non-susceptible isolates
Candipop study, 29 hospitals, Spain 2010-2011: 617 patients (21.7% FCZ non-susceptible) Independent factors with FCZ-NS:
Transplant recipient (AOR 2.13; 95% CI 1.01-4.55) Hospitalization in a unit with high prevalence (≥ 15%) of FCZ-NS strains
(7.53; 4.68-12.10) Previous azole therapy (≥ 3d, within 30 d) (2.04; 1.16-3.62)
Definition and validation of a predictive score
Cuervo et al. CMI 2015
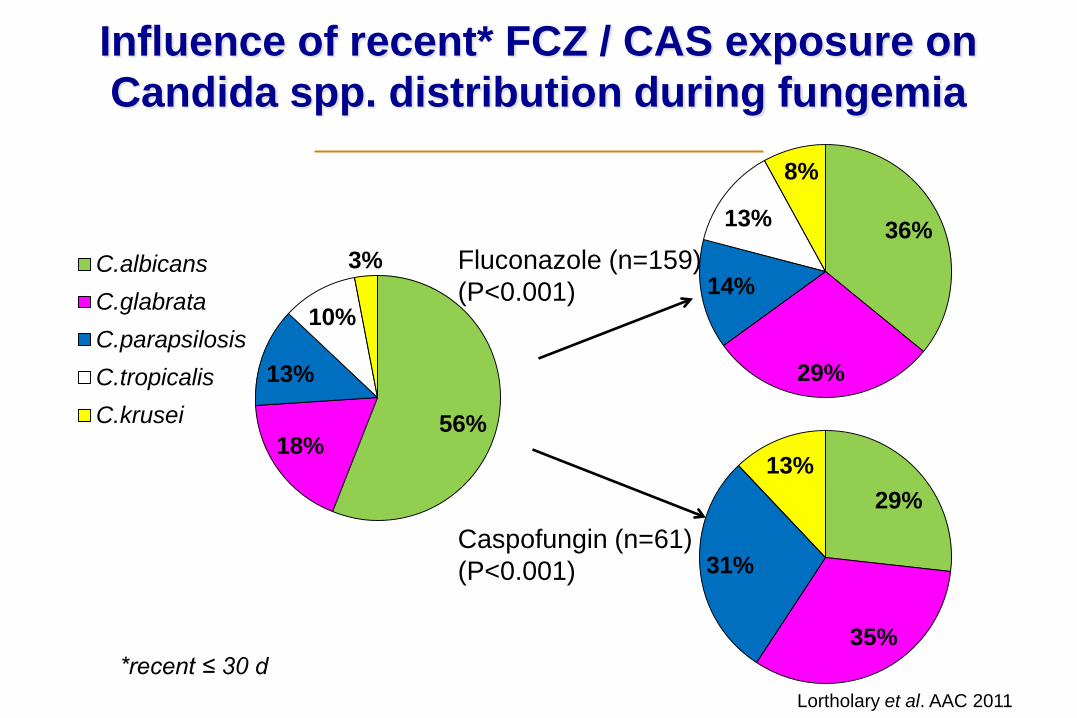
Influence of recent* FCZ / CAS exposure on Candida spp. distribution during fungemia
56% 18%
13%
10%
3% C.albicansC.glabrataC.parapsilosisC.tropicalisC.krusei
36%
29%
14%
13%
8%
29%
35%
31%
13%
Fluconazole (n=159) (P<0.001)
Caspofungin (n=61) (P<0.001)
Lortholary et al. AAC 2011
*recent ≤ 30 d
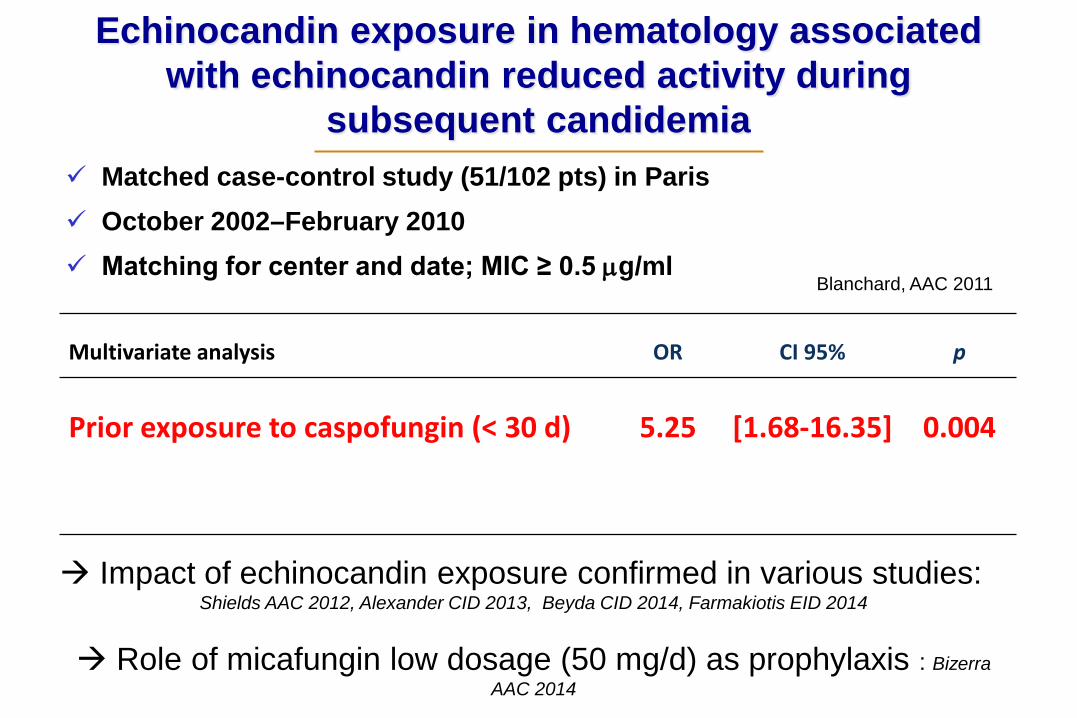
Echinocandin exposure in hematology associated with echinocandin reduced activity during
subsequent candidemia
Multivariate analysis OR CI 95% p
Prior exposure to caspofungin (< 30 d) 5.25 [1.68-16.35] 0.004
Age at fungemia (≤ 65 yrs vs > 65 yrs) 3.27 [1.26-8.50] 0.015
Matched case-control study (51/102 pts) in Paris October 2002–February 2010 Matching for center and date; MIC ≥ 0.5 µg/ml
Blanchard, AAC 2011
Impact of echinocandin exposure confirmed in various studies: Shields AAC 2012, Alexander CID 2013, Beyda CID 2014, Farmakiotis EID 2014
Role of micafungin low dosage (50 mg/d) as prophylaxis : Bizerra
AAC 2014
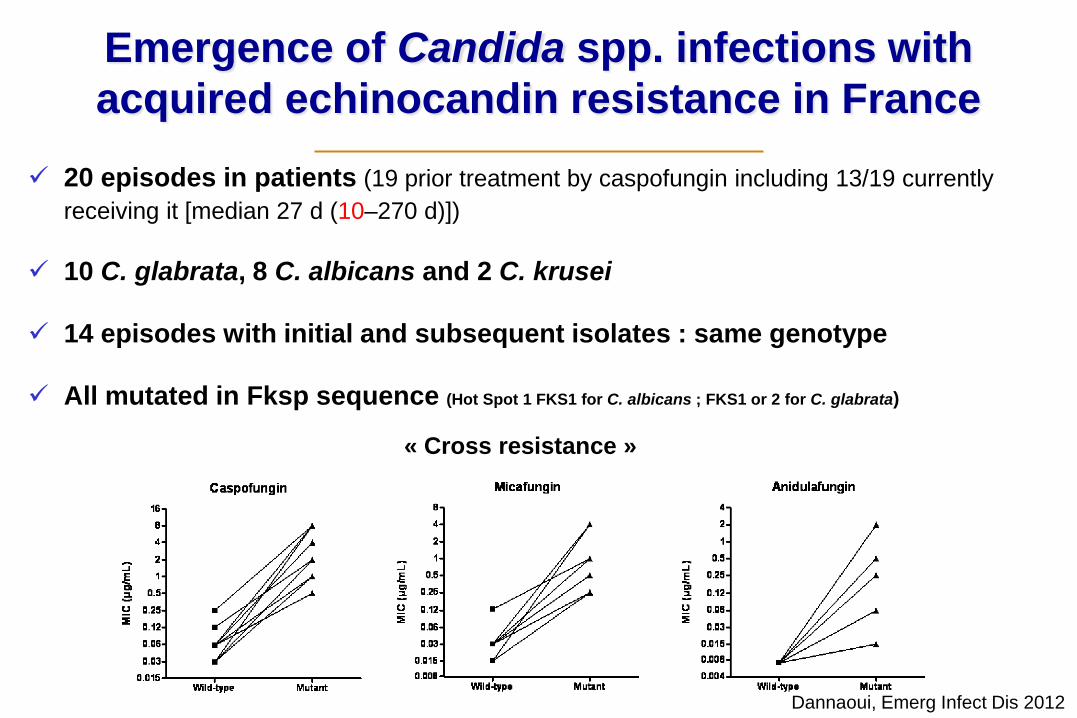
Emergence of Candida spp. infections with acquired echinocandin resistance in France
20 episodes in patients (19 prior treatment by caspofungin including 13/19 currently receiving it [median 27 d (10–270 d)])
10 C. glabrata, 8 C. albicans and 2 C. krusei
14 episodes with initial and subsequent isolates : same genotype
All mutated in Fksp sequence (Hot Spot 1 FKS1 for C. albicans ; FKS1 or 2 for C. glabrata)
Dannaoui, Emerg Infect Dis 2012
« Cross resistance »
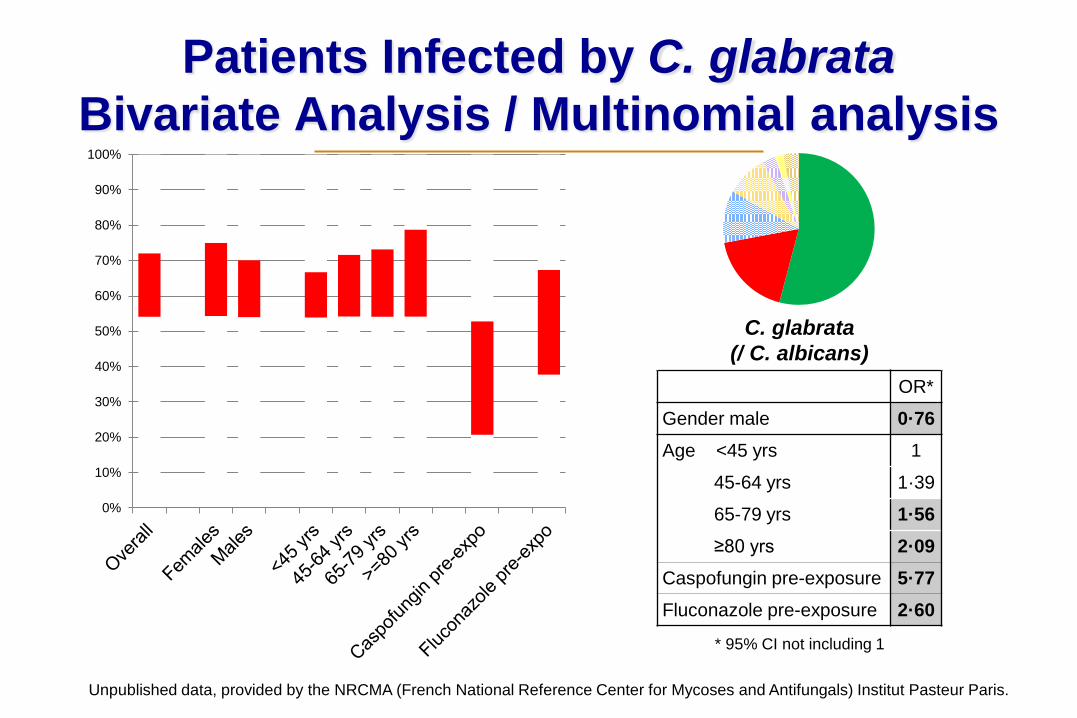
C. glabrata (/ C. albicans)
OR*
Gender male 0·76 Age <45 yrs 1
45-64 yrs 1·39
65-79 yrs 1·56 ≥80 yrs 2·09 Caspofungin pre-exposure 5·77 Fluconazole pre-exposure 2·60
* 95% CI not including 1
Patients Infected by C. glabrata Bivariate Analysis / Multinomial analysis
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Unpublished data, provided by the NRCMA (French National Reference Center for Mycoses and Antifungals) Institut Pasteur Paris.
Impact of echinocandin exposure on C. glabrata
Multiply resistant C. glabrata: 78 FCZ R isolates => 14.1% with resistance to ≥ 1 echinocandin
Failure of echinocandin therapy during invasive candidiasis Relationship with prior echinocandin exposure
Impact of FKS mutations and elevated MICs
Failure rate : 60-91%
Alexander, CID 2013 ; Shields AAC 2012, 2013 ; Beyda CID 2014

Echinocandin exposure and C. parapsilosis experience in Grenoble, France
Fournier JAC 2011

C. parapsilosis (// C. albicans)
OR* Gender male 1·36
Age < 45 yrs 1
45-64 yrs 0·67
65-79 yrs 0·50
≥ 80 yrs 0·46
Intensive Care Unit 0·60
Caspofungin pre-exposure 5·92
Patients infected by C. parapsilosis Bivariate analysis Multinomial analysis
* 95% IC not including 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NRCMA unpublished data
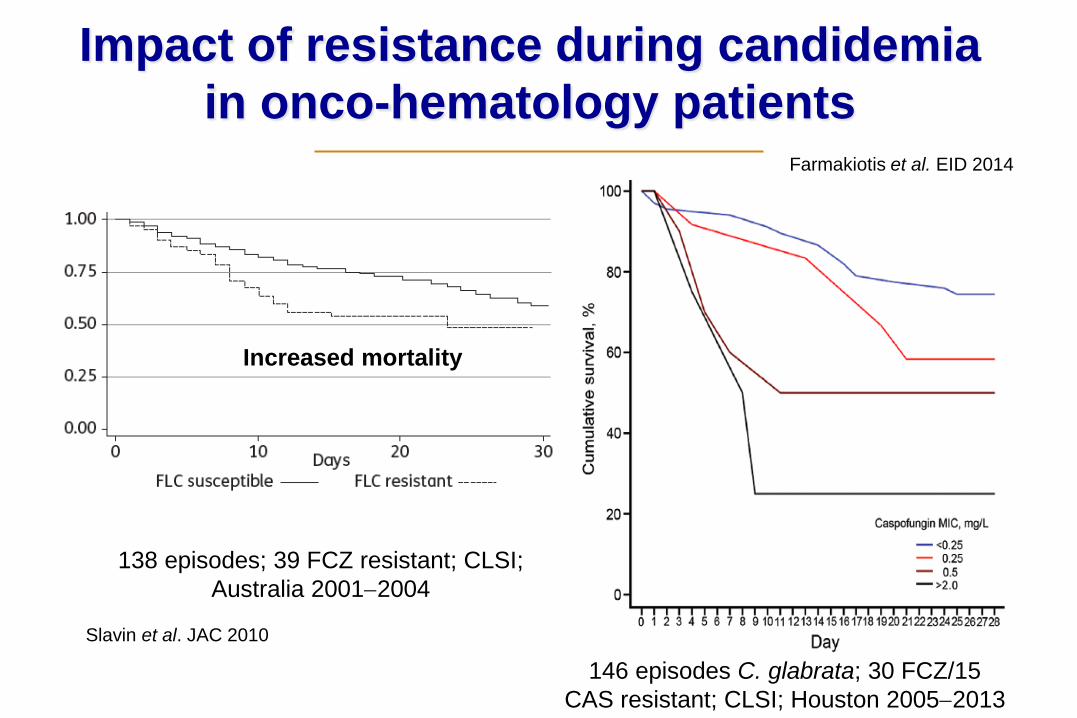
Impact of resistance during candidemia in onco-hematology patients
138 episodes; 39 FCZ resistant; CLSI; Australia 2001−2004
Increased mortality
146 episodes C. glabrata; 30 FCZ/15 CAS resistant; CLSI; Houston 2005−2013
Slavin et al. JAC 2010
Farmakiotis et al. EID 2014
Early acquired flucytosine resistance during combination with caspofungin
for C. glabrata cystitis
2 episodes of cystitis with rapid acquired resistance to flucytosine due to nonsense mutations in the FUR1 gene
Identical MLST profile before and after flucytosine Observed as early as d6 and d10 of combination
therapy Combination does not protect against resistance if
single therapy at infectious site (… echinocandin in urine)
Charlier AAC 2015

Why so few Candida spp. amphotericin B resistant ?
Amphotericin B resistant mutants : hypersensitive to oxidative stress, febrile temperatures, killing by neutrophils defects in filamentation and tissue invasion avirulent in a murine model
Oct 2013

ASPERGILLUS

Triazole resistant Aspergillus spp.
How to get a resistant infection “Primary” resistance in antifungal naïve Pts
• Intrinsically resistant species • Isolate with acquired resistance (environment)
“Acquired” resistance in the AF-treated patient • long term treatment in the individual patient (chronic infection)
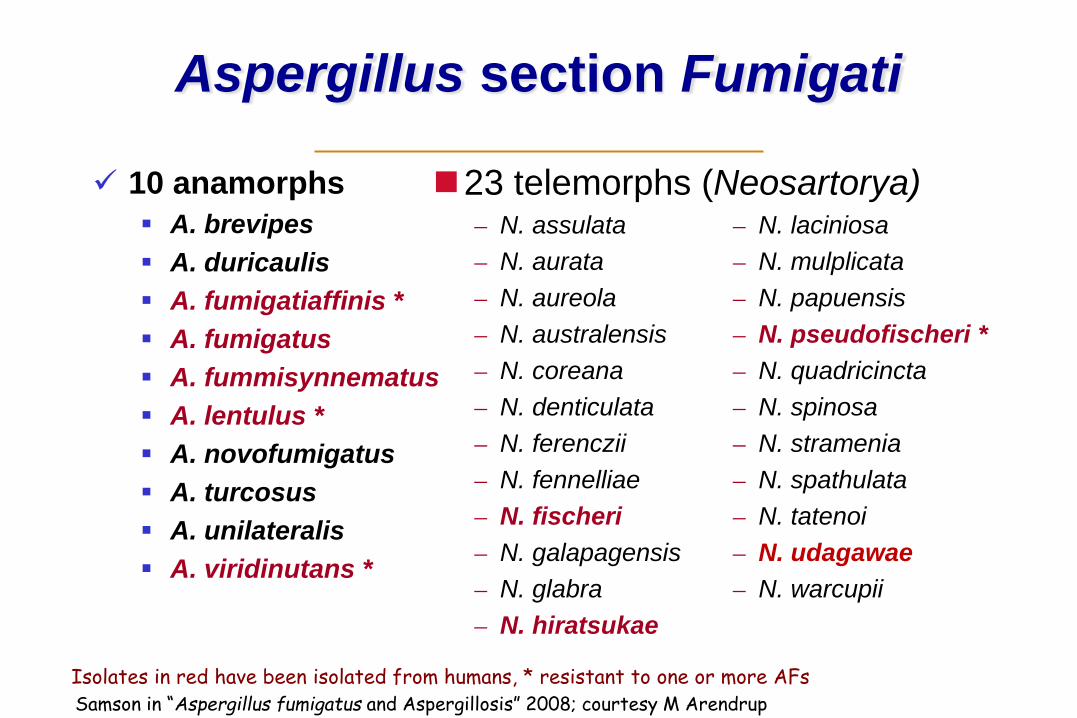
Aspergillus section Fumigati
10 anamorphs A. brevipes A. duricaulis A. fumigatiaffinis * A. fumigatus A. fummisynnematus A. lentulus * A. novofumigatus A. turcosus A. unilateralis A. viridinutans *
23 telemorphs (Neosartorya) – N. assulata – N. aurata – N. aureola – N. australensis – N. coreana – N. denticulata – N. ferenczii – N. fennelliae – N. fischeri – N. galapagensis – N. glabra – N. hiratsukae
– N. laciniosa – N. mulplicata – N. papuensis – N. pseudofischeri * – N. quadricincta – N. spinosa – N. stramenia – N. spathulata – N. tatenoi – N. udagawae – N. warcupii
Samson in “Aspergillus fumigatus and Aspergillosis” 2008; courtesy M Arendrup Isolates in red have been isolated from humans, * resistant to one or more AFs
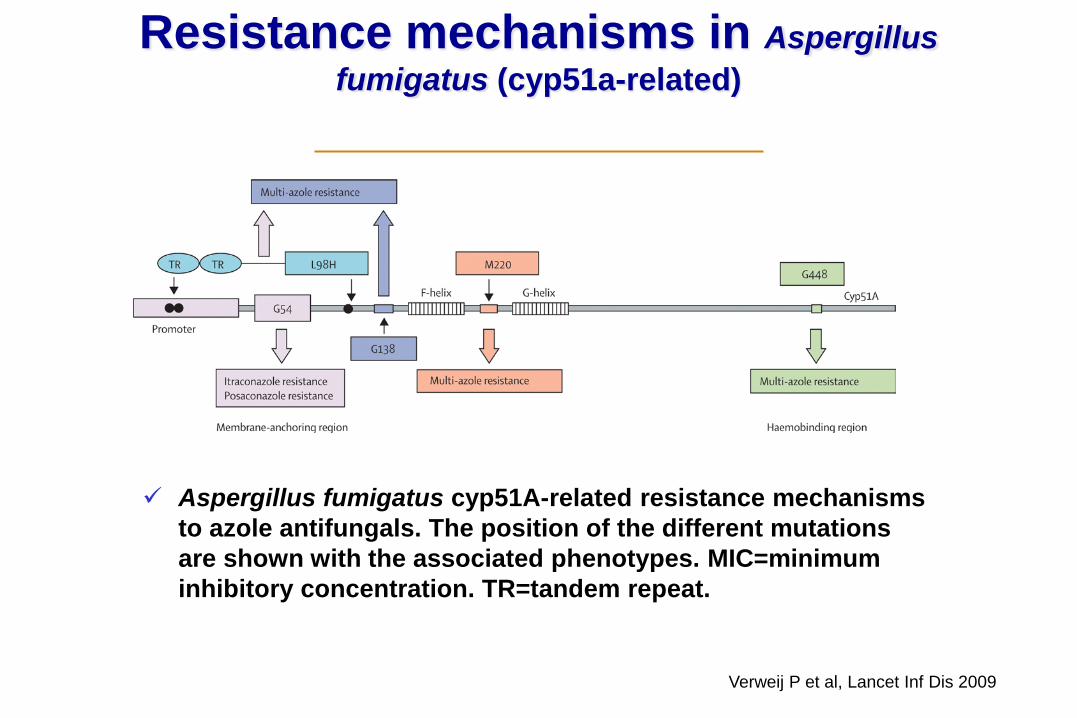
Resistance mechanisms in Aspergillus fumigatus (cyp51a-related)
Aspergillus fumigatus cyp51A-related resistance mechanisms to azole antifungals. The position of the different mutations are shown with the associated phenotypes. MIC=minimum inhibitory concentration. TR=tandem repeat.
Verweij P et al, Lancet Inf Dis 2009
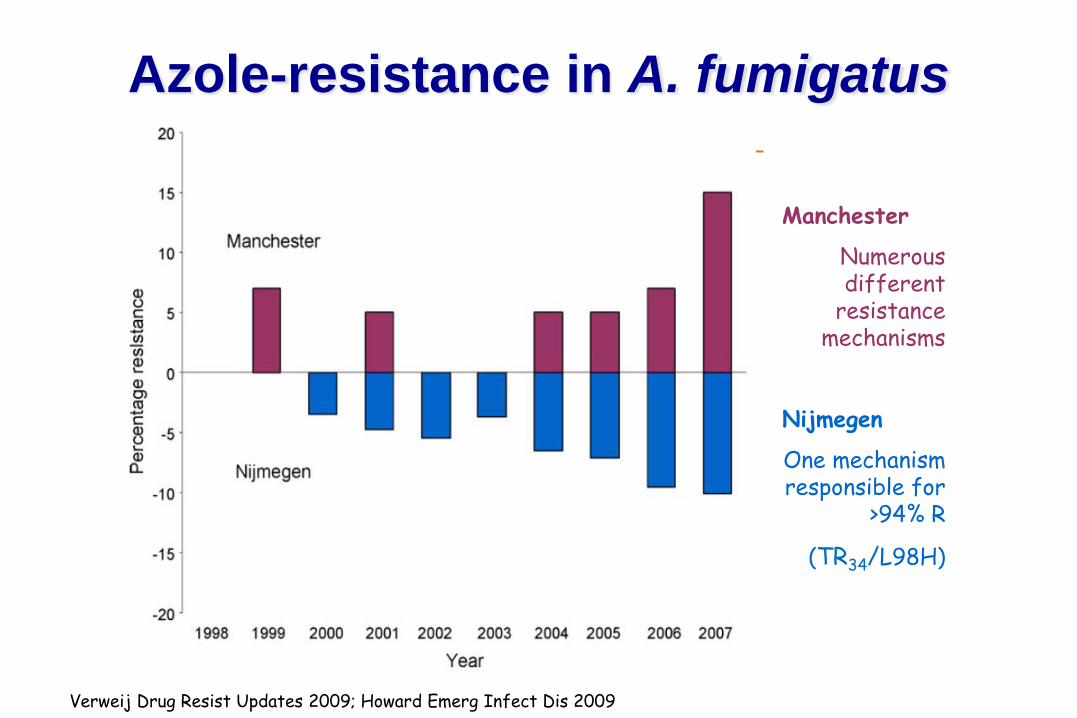
Azole-resistance in A. fumigatus
Verweij Drug Resist Updates 2009; Howard Emerg Infect Dis 2009
Manchester
Numerous different
resistance mechanisms
Nijmegen
One mechanism responsible for
>94% R
(TR34/L98H)
TR34/L98H TR53
TR46/Y121F/T289A G54?
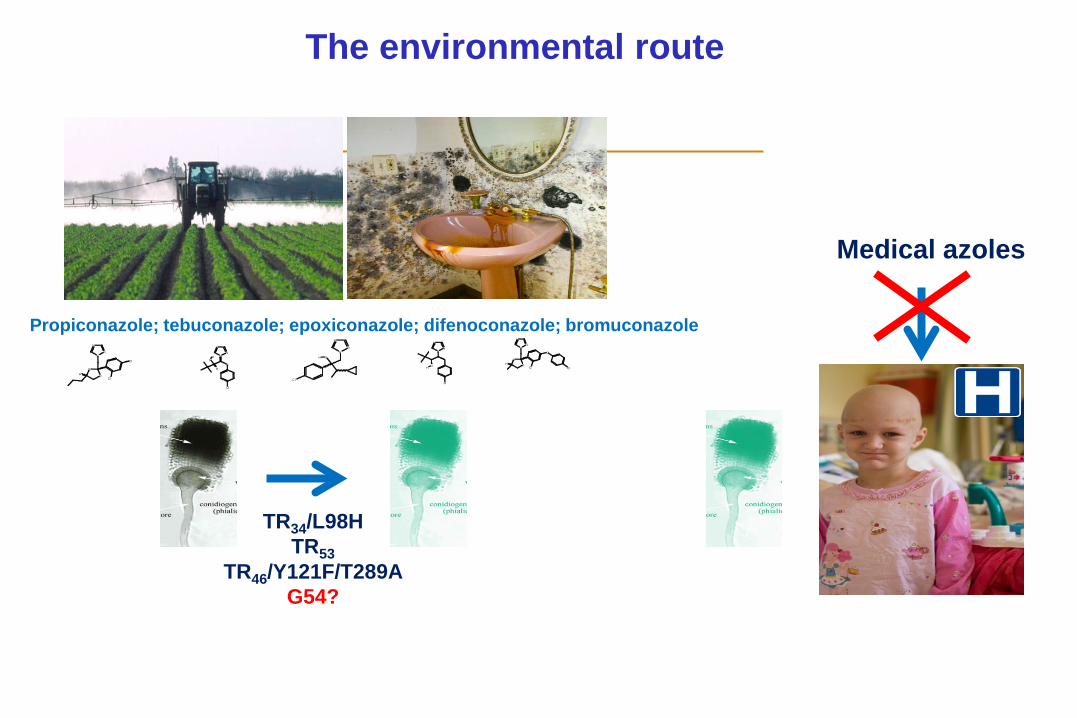
Medical azoles
The environmental route
C l
C l
O
O
N N
N
H
C l
O O
N N
N
H
H
C l
O N
N
N
H
C l
O
N N
N
H C l C l
O
O
O N
N
N
H
Propiconazole; tebuconazole; epoxiconazole; difenoconazole; bromuconazole

37% W-Eur.
24% Asia- Pacific
22% S- & Latin America
9% N-America
5% E-Eur.
Fungicide use & TR34/L98H reports Global market share of fungicide use in agriculture TR34/L98H
Stensvold Curr Fungal Inf Reports 2012, Rath AAC 2012
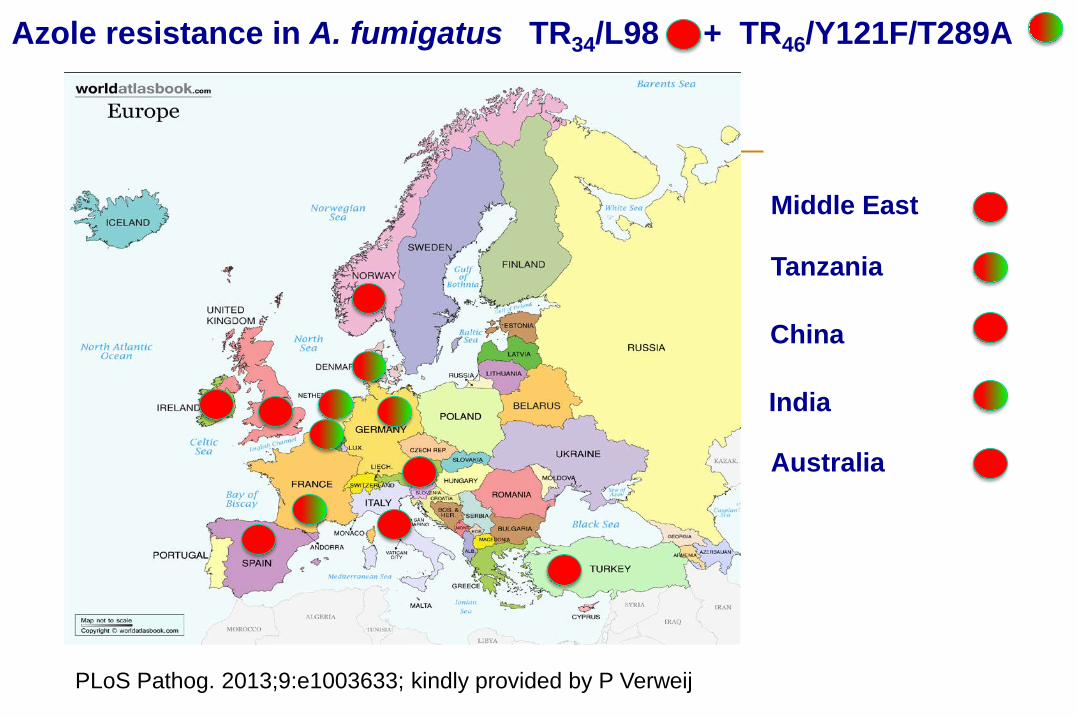
Middle East
Tanzania
China
India
Australia
Azole resistance in A. fumigatus TR34/L98 + TR46/Y121F/T289A
PLoS Pathog. 2013;9:e1003633; kindly provided by P Verweij
Yeast Fungemia due to Uncommon Species (<2%, ODL 2002-2013)
7.4% (306/4136); stable incidence 33 different species: 26 ascomycetes, 7 basidiomycetes 10 had CAS MIC >0.5 mg/L, 13 had FCZ MIC >8 mg/L
Prior exposure to CAS, but not to FCZ: Predisposing factor for uncommon species with high MICs for
both CAS and FCZ (ORs=13.8 and 11.4, respectively, p<0.001)
Bretagne S, et al. ECCMID 2015. Abstract O181.

Multidisciplinary antifungal stewardship programs: Madrid experience
Knowledge survey: room for improvement. Valerio, Enf Infecc Microbiol Clin 2014
Antifungal use audit : identifies how AF are used and targets for intervention. Valerio, JAC 2014
Non restrictive bed-side
intervention: safe and very cost-effective. Valerio, JAC 2015
Combination of Candida biomarkers : help for stopping antifungals. Martinez-Jimenez, JAC 2015
Courtesy: P Munoz
Antifungal failure may be multifactorial Resistance in fungi: +++ intrinsic but may be acquired Prevention of acquired resistance: Adequate ATF indications Limited duration of exposure (stop/switch) Good tissue penetration & drug monitoring Combination therapy if flucytosine Improve host status (HIV+)
Documentation of acquired resistance: Appropriate methodology Comparison with initial isolate Molecular characterization ± therapeutic failure
Conclusions