(Official Publication of Delhi Psychiatric Society) Delhi ... · Jyoti Dubey, Shweta Singh, Adarsh...
242
Vol. 22 No. 2 October, 2019 Hon. Editor M.S. Bhatia Assoc. Editor Shruti Srivastava Journal Committee Aparna Goyal Ankit Saxena N.C. Priyadarshini Editorial Advisory Board A.Q. Siddiqui Ajay Kohli Ajit Avasthi Ashwani Kumar B.S. Chavan E. Mohan Das Indira Sharma M.L. Agarwal Maqbool Dar Mushaq A. Margoob N.K. Bohra Neena Bohra R.C. Jiloha R.K. Gaur R.K. Solanki Rajesh Nagpal Rajesh Rastogi Rajiv Gupta Rakesh K. Chadda Roy Kallivayalil S.A. Azmi S.C. Malik S.C. Tiwari S.K. Khandelwal Smita Deshpande Sunil Mittal T.B. Singh T.P. Jindal T.S.S. Rao Tushar Jagawat Editorial Committee: Ajit Sidana Rajesh Sagar Avinash Desousa Ramesh Chandra Anubhav Rathi Rashmita Saha Anurag Jhanjee Ravi Gupta Dinesh Kataria Rupesh Chaudhary Gaurav Rajendra S.K. Verma Jaswinder Kaur Sandeep Choudhary Jyoti Prakash Savita Jagawat K.K. Verma Shahzadi Malhotra Lalit Batra Shalini Malhotra Maryam Safara Sonali Jhanjee N.K. Aggarwal Sujata Sethi Nimisha Doval Uday K. Sinha Nirmaljit Kaur Vibha Sharma Pankaj Kumar Vikas Gaur Priyanka Gautam Vishal Chabbra Delhi Psychiatry Journal is Published by Dr. M.S. Bhatia on behalf of Delhi Psychiatric Society (Regd.), University College of Medical Sciences & G.T.B. Hospital, Dilshad Garden, Delhi- 110095 (India). Layout Designing and Printing by AAR Computers, 5-C, Pocket B-7, Mayur Vihar Phase-III, Delhi-110096. Correspondence to: D-1, Naraina Vihar, New Delhi-110028 (India). Editorial Office : Department of Psychiatry, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi-110095 Tel.: 22586262 Extn. 2127 Fax : 0091-11-22590495 E-mail : [email protected] : [email protected] Copyright © The Association of Delhi Psychiatric Society of Delhi. The views expressed by authors in publications of Delhi Psychiatry Journal are their own, Editor and Editorial Board do not hold any responsibility for their views. The Publishers are not responsible for any error or omission of fact. Delhi Psychiatric Society www.delhipsychiatricsociety.com Executive Council (2018-2019) Office Bearers President : Deepak Raheja Vice President : Vishal Chhabra General Secretary : Pankaj Kumar Patron : N.K. Bohra Joint Secretary : Manushree Gupta Treasurer : Shruti Srivastava Hon. Editor : M.S. Bhatia Immediate Past President : Rajesh Goyal Executive Council Members Manish S. Kansal Deepak Gupta Dinesh Kumar Kataria Nikhil Raheja Shobhana Mittal Delhi Psychiatry Journal 2019; 22:(1) © Delhi Psychiatric Society (Official Publication of Delhi Psychiatric Society)
Transcript of (Official Publication of Delhi Psychiatric Society) Delhi ... · Jyoti Dubey, Shweta Singh, Adarsh...

Vol. 22 No. 2 October, 2019Hon. EditorM.S. BhatiaAssoc. EditorShruti SrivastavaJournal CommitteeAparna GoyalAnkit SaxenaN.C. PriyadarshiniEditorial Advisory BoardA.Q. SiddiquiAjay KohliAjit AvasthiAshwani KumarB.S. ChavanE. Mohan DasIndira SharmaM.L. AgarwalMaqbool DarMushaq A. MargoobN.K. BohraNeena BohraR.C. JilohaR.K. GaurR.K. SolankiRajesh NagpalRajesh RastogiRajiv GuptaRakesh K. ChaddaRoy KallivayalilS.A. AzmiS.C. MalikS.C. TiwariS.K. KhandelwalSmita DeshpandeSunil MittalT.B. SinghT.P. JindalT.S.S. RaoTushar JagawatEditorial Committee:Ajit Sidana Rajesh SagarAvinash Desousa Ramesh ChandraAnubhav Rathi Rashmita SahaAnurag Jhanjee Ravi GuptaDinesh Kataria Rupesh ChaudharyGaurav Rajendra S.K. VermaJaswinder Kaur Sandeep ChoudharyJyoti Prakash Savita JagawatK.K. Verma Shahzadi MalhotraLalit Batra Shalini MalhotraMaryam Safara Sonali JhanjeeN.K. Aggarwal Sujata SethiNimisha Doval Uday K. SinhaNirmaljit Kaur Vibha SharmaPankaj Kumar Vikas GaurPriyanka Gautam Vishal Chabbra
Delhi Psychiatry Journal is Published by Dr.M.S. Bhatia on behalf of Delhi PsychiatricSociety (Regd.), University College of MedicalSciences & G.T.B. Hospital, Dilshad Garden, Delhi-110095 (India). Layout Designing and Printingby AAR Computers, 5-C, Pocket B-7, MayurVihar Phase-III, Delhi-110096. Correspondenceto: D-1, Naraina Vihar, New Delhi-110028 (India).
Editorial Office :Department of Psychiatry,
University College of Medical Sciencesand Guru Teg Bahadur Hospital,Dilshad Garden, Delhi-110095
Tel.: 22586262 Extn. 2127 Fax : 0091-11-22590495E-mail : [email protected]
Copyright © The Association of Delhi Psychiatric Society of Delhi.The views expressed by authors in publications of Delhi PsychiatryJournal are their own, Editor and Editorial Board do not hold anyresponsibility for their views. The Publishers are not responsiblefor any error or omission of fact.
DelhiPsychiatric Society
www.delhipsychiatricsociety.com
Executive Council (2018-2019)Office Bearers
President : Deepak RahejaVice President : Vishal ChhabraGeneral Secretary : Pankaj KumarPatron : N.K. BohraJoint Secretary : Manushree GuptaTreasurer : Shruti SrivastavaHon. Editor : M.S. BhatiaImmediate Past President : Rajesh Goyal
Executive Council Members
Manish S. Kansal
Deepak Gupta
Dinesh Kumar Kataria
Nikhil Raheja
Shobhana Mittal
Delhi Psychiatry Journal 2019; 22:(1) © Delhi Psychiatric Society
(Official Publication of Delhi Psychiatric Society)

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society196
DELHI PSYCHIATRIC SOCIETY(Regd. No. S/ 25490 /94)
MEMBERSHIIP FORM
NAME : ……………………………………………..........
AGE : ……………………………………………..........
SEX : ……………………………………………..........
QUALIFICATION : ……………………………………………..........
CURRENT PROFESSIOINAL AFFILIATION & ADDRESS (with Telephone numbers)
.................................................................................................... ...........................................................
.................................................................................................... ...........................................................
.................................................................................................... ...........................................................
.................................................................................................... ...........................................................
RESIDENTIAL ADDRESS (With telephone numbers, E-mail address)
.................................................................................................... ...........................................................
.................................................................................................... ...........................................................
CATEGORY OF MEMBERSHIHP APPLIED FOR : (LIFE FULL MEMBER)
CURRENT MEMBERSHIP FEE :• Mental Health Professionals/Non-mental Health Professionals: Life member: Rs. 10,000/-
Proposed By:Name:……………………………………....................................Signature…………………………....
Seconded By:Name……………………………………......................................Signature……………………………
Gen. SecretaryDR. PANKAJ KUMARTHE HEALERS PSYCHIATRY & DENTAL CENTRED-215 (Basement), Vivek Vihar Phase-I, (Below South Indian Bank), New Delhi-110095Mobile : 9999959044 E-mail: [email protected]
For any further query please do not hesitate to call General Secretary
DECLARATION
I hereby declare that I agree to abide by the rules and regulations of DELHI PSYCHIATRIC SOCIETY
Name:……………………………… Signature……………………….............
Date………………………………..

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 197
Contents
EditorialMicrobiome and Mental health – 199a new Gateway to ResearchM.S. Bhatia, Nirmaljit Kaur
Review ArticlesSomatization and conversion disorders in 201children and adolescentsBheemsain Tekkalaki, S.K. Kar, Adarsh Tripathi
Personality Theories: A Brief Overview 213Sushma Rathee
Preclinical Concepts of Depression 222Bhumija Sharma, Preeti Sharma,Pradeep Kumar, Anil Sharma
Original ArticlesA Study to Assess the Magnitude of Various 232Minor Physical Anomalies in Schizophrenia andto compare them between Schizophrenic Patientsand their First-degree RelativesAbhinav Pandey, Haseeb Khan, D.M.S. Rathore
A study of burden of care among mothers of 238mentally retarded children and adolescentsattending child and adolescent psychiatryOPD in a tertiary care center in North IndiaAmit Arya, Savita Verma, Deblina Roy,Pawan Kumar Gupta, Fauzia Jawaid
Relevance of Patterns of Use and Preferred 244Contents in Problematic Internet Use amongUndergraduate StudentsManoj Kumar Pandey, Prabha Mishra
To study the prevalence, pattern and 250psychopathology of Internet Addiction amongUndergraduate students of different streamsSrishti Detha, Manju Bhaskar, Abhishek Charan,Aditya Soni
Metacognitions in patients with Generalized 256Anxiety Disorder (GAD) in a tertiary carecenter of North IndiaJyoti Dubey, Shweta Singh, Adarsh Tripathi,P.K. Dalal, Seema Rani Sarraf
Co-Morbidity of Attention Deficit Hyperactivity 264Disorder in Dyslexic School going Childrenin JaipurRajinder Pal Singh, Manju Bhaskar
Management of different domains of Aggressive 271Behaviour of Persons with Mental Illness(PMI) by Caregivers in both hospital andhome settingsNibedita Banerjee, Sandhya Ghai,Renu Sharma, D. Basu
Assessment of hostility, suicidality and 276co-morbid psychiatric disorders in patientspresenting with deliberate self-harmPoonam Bharti, Navkiran S. Mahajan,Ranjive Mahajan, Anshu Gupta
A Study of Suicidal Ideation and Suicidal 288Attempt in Patients with ObsessiveCompulsive DisorderShah Karan Kiritkumar, Tushar Jagawat,Krishna Kanwal, Bajrang Dhaka,Ritu Meena, Pankaj Kumar
The pattern of behavioural and psychological 296symptoms in patients with Major NeurocognitiveDisorder attending Psychogeriatric OPD in atertiary care teaching hospitalShravan Kumar, Rakesh Kumar GaurYasir Alvi, Suhail Ahmad Azmi
Impact of Mindfulness Meditation on 303Caregivers of Epilepsy and IntellectualDisabilityDeoshree Akhouri
Factors affecting Rehospitalization in 312psychiatric patients – an exploratory studySushma Sonavane, Reetika Dikshit,Amresh Shrivastava, Nilesh Shah,Avinash De Sousa
Knowledge, awareness and utilization of 318telepsychiatry services among health careprofessionalsRenu Sharma, Karobi Das, Ruchita Shah,Afroz, Isha Kumari, Prahalad Singh,Sarita Kumari, Suman
Prevalence of Internet addiction and psychiatric 325distress among young adults: A gender-basedcross-sectional comparative studyShiv Prakash, Jai Singh Yadav
Cognitive advantage of second-generation 331anti-psychotics against combination of first-generation anti-psychotic and anti-cholinergic

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society198
drugsSunny Chattopadhyay, Om Prakash Singh,Debanjan Saha
A study of Socio-demographic and Psycho- 337sexual dysfunctions in female patients withDepression and Anxiety disorderRitu Meena, Tushar Jagawat, Krishna Kanwal,Bajrang Lal, Pankaj Tondon
Sexual Health Related Issues among Indian 341Unmarried Undergraduate Male Students:A SurveyVivek Kumar, Apoorv Yadav, Surendra Pal Bharti
Quality of Life and Caregiver burden in Chronic 349Kidney Disease — Case for a paradigm shiftin holistic managementShagufta Khanam, Shahbaz A. Khan,A.W. Waheed, D.S. Ray, Aruna Deshpande,Swetanka Prasad, V.V. Gantait, P. Patra
Correlates of Dyadic Adjustment in 357SchizophreniaShipra Singh, Deoraj Sinha, Nitin B. Raut
Depression among elderly people living 363separately from their children: a cross-sectionalcomparative studyShiv Prakash, Adya Shanker Srivastava,Jai Singh Yadav
Impact of Cannabis Use on Executive 371Functions in Male Patients with BipolarDisorder: A Comparative StudyPushpanjali Vishwakarma, Anshul Kumar,Neetee Mehata
PsychophysiotherapyPsychophysiotherapy in Management of 379Cervical DystoniaJaswinder Kaur, Shweta Sharma, M.S. Bhatia
Postpartum Depression – A Psychophysio- 386therapeutic ApproachJaswinder Kaur, Mansi Gupta,Megha Masaun, M.S. Bhatia
View PointHistorical Development of Rights and Care 391of Differently Abled Persons: Are we cruisingtowards an ideal framework in India?Navya Gupta, Vimal Joshi
Invited ArticleWorld Mental Health Day 397Shruti Srivastava
Drug ReviewBremelanotide 399Aparna Goyal, M.S.Bhatia
Forensic PsychiatryTestamentary Capacity – a clinical framework 401Nilesh Shah, Sagar Karia, Avinash De Sousa
An overview of Organ Transplant Act: 408Role of Psychiatrist and Forensic expertN.S. Sonwani, N.K. Aggarwal, M.S. Bhatia
Case ReportsKleine-Levin Syndrome 412Reena Jambulkar, Sagar Karia, Nilesh Shah,Avinash De Sousa
Capgras Syndrome: She’s Not My Wife !! 414P. Patra, Rajiv K. Saini, D. Bhattacharya,B. Patra, SA Khan, Kartikeya R. Singh
Disulfiram-induced delirium: Diagnostic dilemma 417Ravi Parkash, Priti Singh, Ripu Daman, Sakshi,Neharika Saini, Rajiv Gupta
Pyromania like behavior in a case of Dementia 420Avinash De Sousa
Auto erythrocyte sensitization syndrome 422in a young girlAbhishek Singh Chauhan, Deepak Gupta
First Episode Mania after Traumatic 425Brain InjurySheetal Tripathi, Anju Agarwal,A.Q. Jilani, Shantanu Bharti
Acceptance and Commitment Therapy in 428Reappraisal of Past Events?Report of Two CasesAarzoo, Archana Kashyap, Ajeet Sidana
Interesting Articles 431
Forthcoming Events 432
Instructions to authors 434

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 199
Microbiome and Mental health –a new Gateway to Research
M.S. Bhatia1, Nirmaljit Kaur2
Department of Psychiatry1, UCMS & GTB Hospital, Dilshad Garden, Delhi andDepartment of Microbiology2, ABVIMS & Dr. RML Hospital, New Delhi
Editorial
The connection between microbiome andmental health has recently come to the attention.The human gastrointestinal tract alone contains adelicately balanced ecosystem of 100 trillionmicroorganisms, nearly ten times the number of cellsin the entire human body.1 These gut bacteria ormicrobiome play many physiological roles in the bodye.g. synthesizing vitamins, developing the immunesystem, aiding digestion, and managing the stressresponse.1 The human genome represents about23,000 genes, whereas our microbiome representsover 3,000,000 genes, producing thousands ofmetabolites that may replace many of the functionsof the host.2
Bacteria begin to form an inextricable linkshortly before birth when they colonize our gutswithin the womb.1 By the age of 3-5 years, theydevelop a full adult microbiome and a gut-brain axis.The microbiome remains relatively stable throughoutlife, but can be altered as a result of bacterialinfections, antibiotic treatment, lifestyle, surgical, anda long-term change in diet.3 Shifts in this complexmicrobial system have been reported to increasethe risk of disease.3
The gut-brain axis (GBA) is a set of mechanismsthrough which the gut and brain communicatebidirectionally. Three of the main communicationroutes are the immune system, the nervous system,and the endocrine system.4 One study found thatwhen the gut bacteria from two different mice wereswapped, stress-prone mice became calm and calmmice became stress-prone.1
The first mechanism through which bacteria inthe gut interact with our brain is through inflamma-
tion. In a mentally and physically healthy person,anti-inflammatory cytokines are in equilibrium withpro-inflammatory cytokines.5 Research has foundthat increased levels of pro-inflammatory cytokineactivity in the brain lowers metabolism of neurotrans-mitters, specifically that of GABA; GABA, whenin lower levels, causes depressive symptoms.6
The enteric nervous system is connectedbidirectionally with the central nervous system.Normally, information is sent from the heart, lungs,pancreas, liver, stomach, and intestines to the brain(including the cerebral cortex, medulla oblongata,limbic system, etc.) via sensory fibers in the vagusnerve.5 Elevated stress and anxiety have been shownto deplete one’s microbiome of bacteria that produceanti-inflammatory cytokines, thus resulting in thebiological effects inherent in inflammatory responseand subsequent depression.4
Research shows that stress-induced neuroendo-crine hormones can influence bacterial growth7 andthat endocrine effects of gut microbiota mayinfluence host responses ranging from behavior tometabolism and appetite, and even immuneresponses.8
For many years, research has been underwayto uncover the relationships between microbiomedysfunction and conditions such as colorectal cancer,inflammatory bowel disease, celiac disease, psoriaticarthritis, atopic eczema, childhood-onset asthma,rheumatoid arthritis, Type 1 and 2 diabetes andobesity.4,9 Research has shown a link between gutand psychiatric disorders. Depression is known tobe closely related to elevations in C-reactiveproteins, inflammatory cytokines, and oxidative

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society200
stress.10 There is a relationship between fecalbacteria (which served as a proxy to analyze thegut microbes) and symptoms of depression.11
Previous studies have demonstrated that bothschizophrenia and bipolar disorder are associatedwith alterations of the systemic immune systemincluding low-grade chronic inflammation (increasedplasma cytokines, soluble cytokine receptors,chemokines, acute phase reactants) and T-cellactivation features.11,12 In addition, elevated anti-bodies to S. cerevisiae were also found in individualswith schizophrenia and bipolar disorder.13 Linksbetween particular bacteria (Clostridium orDesulfovibrio) and phenotypes relevant to AutisticSpectrum Disorder (ASD) raise the question ofwhether microbial dysbiosis plays a role in thedevelopment or presentation of ASD symptoms.14
Psychobiotics are beneficial bacteria (probiotics) orsupport for such bacteria (prebiotics) that influencebacteria–brain relationships.15 Two bacterial genera,Lactobacillus and Bifidobacteria, and also Campy-lobacteria, Citrobacter, and Trichuris are commonanti-inflammatory probiotics that have been shownto reduce anxiety and behavioral signs of distress inboth human and rodent studies.4,16 Probioticsdecrease ruminative, negative thoughts in humans,and that the introduction of prebiotics (or fibers) thatpromote the growth of beneficial bacteria decreaseanxiety.4,16 It is challenging to find ways (recentlyfecal transplant and crapsules) to deliver desirablebiota in a way where they can thrive in a new body.4
The human microbiome and its relationship todisease is a new and rapidly evolving field ofstudy.1,4,9 Understanding the links between the gutmicrobiome and disease may provide therapeuticor prophylactic tools to improve human health.9
References1. Kramer P, Bressan P. Humans as Super-
organisms. Persp Psychol Sci 2015; 10 (4) : 464–481.
2. Valdes AM, Walter J, Segal E, Spector TD. Roleof the gut microbiota in nutrition and health. BMJ2018; 361 : k2179.
3. Rodríguez JM, Murphy K, Stanton C, et al. Thecomposition of the gut microbiota throughout life,with an emphasis on early life (in en). MicrobEcol Health Dis 2015; 26 : 26050.
4. https://en.wikiversity.org/wiki/Microbiome_
and_Mental_Health#cite_ref-:0_5-4. Accessedon 05/20/2019.
5. Forsythe P, Bienestock J. Immunomodulationby Commensal and Probiotic Bacteria. ImmunolInvest 2010; 39 : 429-438.
6. Dantzer R, O’Connor J C, Freund GG; JohnsonRW, Kelley KW. From inflammation to sicknessand depression: when the immune systemsubjugates the brain. Nat Rev Neurosci 2008;9 (1) : 46–56.
7. Hegde M, Wood TK, Jayaraman A. The neuro-endocrine hormone norepinephrine increasesPseudomonas aeruginosa PA14 virulencethrough the las quorum-sensing pathway. ApplMicrobiol Biotechnology 2009; 84 (4) : 763–776.
8. Neuman H, Debelius JW, Knight R, Koren O.Microbial endocrinology: the interplay betweenthe microbiota and the endocrine system. FEMSMicrobiol Rev 2015; 39(4) : 509-521.
9. Cho I, Blaser MJ. The Human Microbiome: atthe interface of health and disease. Nat RevGenet 2012; 13(4) : 260–270.
10. Naseribafrouei A, Hestad, K, Avershina, E, etal. Correlation between the human fecal micro-biota and depression. Neurogastroenterol Motil2014; 26(8) : 1155–1162.
11. Rosenblat JD, Cha DS, Mansur RB.; McIntyreRS. Inflamed moods: A review of the inter-actions between inflammation and mooddisorders. Prog Neuro-Psychopharmacol BiolPsychiatry 2014; 53 : 23–34.
12. Anderson G, Maes M. Bipolar Disorder: Roleof Immune-Inflammatory Cytokines, Oxidativeand Nitrosative Stress and Tryptophan Cata-bolites. Curr Psychiatry Rep 2015; 17(2) : 8.
13. Severance EG, Alaedini A; Yang S, et al. Gastro-intestinal inflammation and associated immuneactivation in schizophrenia. Schizophr Res 2012;138(1) : 48–53.
14. Vuong HE, Hsiao EY. Emerging Roles for theGut Microbiome in Autism Spectrum Disorder.Biol Psychiatry 2016; 81(5) : 411–423.
15. Sarkar A, Lehto SM, Harty S, et al. Psycho-biotics and the manipulation of Bacteria–Gut–Brain Signals. Trends Neurosci 2016; 39(11) :763–781.
16. Deans E. Microbiome and mental health in themodern environment. J Physiol Anthropol 2017;36 : 1.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 201
Somatization and conversion disorders in childrenand adolescents
Bheemsain Tekkalaki1, S.K. Kar2, Adarsh Tripathi3
Department of Psychiatry, J.N. Medical College, Belagavi, Karnataka 1Department of Psychiatry, King George’s Medical University, Lucknow, U.P.2,3
Contact: AdarshTripathi, E-mail:[email protected]
Review Article
Introduction
Medically unexplained physical symptoms(somatic symptoms) are common in children andadolescents1 (Referred simply as children here afterin this article). The severity of such symptoms variesfrom being transient, mild and self-limiting to beingchronic and impairing. Various disorders comprisingsuch impairing somatic symptoms are grouped intothe category of somatization disorders. The word“Somatization” means the tendency to experienceand communicate somatic distress and symptoms,unexplained by pathological findings.2
Children with somatization disorders often arefirst seen by general practitioner or a paediatrician.They are referred to mental health professionals latein the course of illness, often leading to excessive,unnecessary investigations and overuse of medicalservices. If not identified and managed early, thesedisorders are known to cause long term psychiatriccomplications, poor quality of life for the childrenand significant burden of care for families.3 Thisarticle aims to help the reader to understand theetiological factors and clinical features of somatiza-tion disorder and also basic management principles.
Epidemiology
Though somatic symptoms are reported to becommon in children, the epidemiological data aboutthe somatization disorders in children is sparse. Thereis no data specific to the DSM-5 somatic symptomdisorder in children. In his classical study, Apleyreported that about 10% of school children had atleast thrice experienced the severe pain abdomenover a period of three months.4 Different populationbased studies have reported the different prevalencerates of somatic symptoms ranging from 2 to 10 %
to 25 to 80%. Whereas a clinic based study reporteda prevalence of 1.3 to 5%. Recurrent abdominalpain accounts for around 5% of the paediatric clinicvisits. Headaches have been reported to affect 20%to 55% of all children, with 10% of teenagersreporting frequent headaches, chest pain, nausea,and fatigue.5, 6 Higher prevalence of somatization isseen in girls (10.7%) than boys (4.5%)6-8 Bodydysmorphic disorder, another variant of somatoformdisorder, has prevalence of approximately 1% (0.7to 1%).9,10 However, Dyl et al, in their study foundthat 6.7 % of adolescents have either definite orprobable body dysmorphic disorder.11
Some differences in the prevalence of somatiza-tion in different cultures in observed in adults.Kleinman found the difference between prevalenceof somatization higher in population of East incomparison to population of West12 and study byWeiss et al, also found higher prevalence of somati-sation in the psychiatric clinics in response to stressin the East in comparison to West. 13 Theseevidences favour the belief that, as a stress response,population from East tend to somatize, whereaspopulation from West present with depressivesymptoms, which again indicates the possible culturalattribution to variation in stress responses.12,13
However, there is no definite evidence to say thatthe same trend is observed in children.
Nosological AspectsThere are some differences in how these
disorders are described and classified by Inter-national Classification of Diseases (ICD) and theDiagnostic and Statistical Manual of Mental disorders(DSM). Further there are differences between therecently released DSM-5 and its predecessor DSMIV–TR.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society202
ICD-10 describes somatoform disorders ashaving:
(i) Repeated presentations of physicalsymptoms,
(ii) Persistent requests for investigations despitenegative findings and reassurance, and
(iii) The resistance for the attempts to discussthe possibility of psychological causation.ICD-10 subdivides these disorders intosomatization disorder, undifferentiatedsomatoform disorder, hypochondriacaldisorder, somatoform autonomic dysfunc-tion, persistent somatoform pain disorder,and other somatoform disorders.14
DSM-IV describes these disorders as having:(i) Physical symptoms suggesting a medical
condition; however, no medical disease,substance misuse or another mentaldisorder can be found to account for thesesymptoms
(ii) The symptoms cause significant distress orimpairment in social, occupational or otherareas of functioning
(iii) The physical symptoms are not intentionallyproduced. DSM-IV subdivides somatoformdisorders into somatization disorder, undiffe-rentiated somatoform disorder, conversiondisorder, pain disorder, hypochondriasis,body dysmorphic disorder and somatoformdisorder not otherwise specified (includesunexplained physical complaints, e.g.,fatigue).15
As one can observe, conversion disorders aregrouped together with somatoform disorders inDSM where as they are part of dissociative
disorders in ICD. Neurasthenia is also a separatediagnostic category in ICD, whereas, Bodydysmorphic disorder is not a separate diagnosticentity, it is considered under the category ofhypochondriacal disorder.
DSM-5 has brought several changes. The term“somatoform disorder” is replaced by “somaticsymptom disorder”. Diagnosis is not based on“absence of any identifiable physical cause”, rathera positive diagnosis based on the presence ofmaladaptive cognitive and behavioural patternsassociated with the somatic symptoms like excessivepreoccupation, exaggerated importance attached tosymptoms and disproportionate impairmentassociated with the symptoms. 16 DSM-5 hasachieved simplicity to some extent by removingsome overlapping diagnostic entities. It has alsoemphasised the concept that presence of a medicalillness do not rule out somatoform disorders, andthey can coexist.17 By discarding the mind bodydualism, it has made some efforts to reduce stigma.Table No. 1 compares the different disordersincluded under the heading of somatoform disordersin ICD-10, DSM-IV TR and DSM-5.
Application of the above ready made diagnosticcriteria to children poses some problems. Childrenrarely present with the classic syndromes describedabove, they rather present with discrete symptoms.It is difficult to find cognitive symptoms likeexaggerated importance, excessive preoccupationwith symptoms in children. For the latter problem,DSM-5 has given a provision to consider the parents’reaction to the symptoms.16 Research focusing onformulating the specific diagnostic guidelines forchildren is needed. We have followed DSM-5 inthis article.
Table-1: Comparison of the different disorders included under the heading of somatoformdisorders in ICD-10, DSM-IV TR and DSM-5
ICD 10 DSM-IV TR DSM-5
Somatization disorder Somatization disorderPersistent Somatoform pain disorder Somatoform pain disorder Somatic symptom disorderUndifferentiated somatoform disorder Undifferentiated somatoform disorderHypochondriacal disorder Hypochondriasis Somatic symptom disorder
Illness anxiety disorderNo category Conversion disorder Conversion disorderSomatic autonomic dysfunction No category No categoryNo category Body dysmorphic disorder No categoryOther somatoform disorders Somatoform disorder NOS No categorySomatoform disorder NOS

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 203
Etiology
The definite etiology of somatoform disordersis not known. Nevertheless, many bio-psycho-socialfactors are identified, which possibly play role.Thorough understanding of this model is also essen-tial for complete assessment and holistic manage-ment of the disorder.
Biological factorsChildren with somatic symptoms are more likely
to have family members with higher levels ofsomatic symptoms.18 Recent evidences suggest astrong genetic component in the form of polymor-phism of catecholamine-O-methyl Transferase(COMT), related to pain sensitivity. The promoterregion of serotonin transporter gene is associatedwith traits like neuroticism and anxiety, which arecommonly found in children with frequent somaticsymptoms.18
Other than the genetic factors, some otherbiological factors explain the generation of somaticsymptoms in somatoform disorders. Patients withconversion disorders may have – prolonged motorreaction time, activation of prefrontal, orbitofrontal,and anterior cingulate areas and decreased bloodflow to certain brain areas (basal ganglia andthalamus).19-22
Child related factorsChildren who are conscientious, perfectionistic
(obsessive), sensitive, insecure and anxious are moreprone to develop frequent somatic symptoms understress. Children with high levels of functional somaticsymptoms have fewer adaptive coping skills. Theyuse poor coping skills like disengagement, ruminationover pain, avoidance, anger, cognitive interferenceor combination of them.3,23 Preoccupied and fearfulattachment styles also are associated with faultysymptom perception and service utilization.24 Otherpsychological factors that may contribute to soma-tization is increased anxiety sensitivity and tendencyfor catastrophizing the physical symptoms. Highanxiety sensitivity also influences the catastrophizingbeliefs about physical symptoms by making themstronger.25
Family related issuesChildren with somatic symptoms are more likely
to have anxious mothers than healthy children.
Somatization can also be a learnt behaviour. Further,parental reaction to the child’s symptoms alsodetermines the clinical picture. Over protective andanxious parents are more likely to have somatisingchildren. Somatization can also be an indicator ofunderlying family disputes.3,23,24,26,27
Environmental factorsNegative and adverse events at home and
school increase somatic symptoms in children. Highacademic expectations from parents, child-teacherrelationship, bullying in peer group are commonlyassociated with stress and somatic symptoms.Sexual abuse is one important factor to be consi-dered, as children who have undergone sexual abuseare more likely to have psychiatric consequences,including somatization.26,27 It was also found thatchildhood abuse and neglect (both physical andemotional) may play causative rolein bodydysmorphic disorder.28
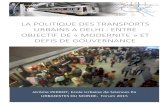
Biological factors• Family h/o somatization,
anxiety
• Genetic studies
• COMT polymorphism
• 5HT gene
Psychologicalfactors• Consientiousness,
perfectionistic,anxious traits
• Poor coping skills
• Faulty attachmentstyles
Social factors• Role models in family
Overprotective andanxious parents
• Family disputes
• School relatedproblems
• H/O abuse
Fig. 1: Etiological factors for the children’s somaticsymptoms
Individual SyndromesWe have followed the DSM-5 classificatory
system while describing the different somatizationand conversion disorder in this chapter. In DSM-5,the term used is somatic symptom and relateddisorder with five subtypes which have beenexplained here (Table 2, 3, 4, 6, 7).
Somatic Symptom DisorderThe DSM-5 Somatic symptom disorder has
replaced somatization disorder, undifferentiatedsomatoform disorder and somatoform pain disorder.The classic features of somatic symptom disorderare, multiple somatic symptoms and associated setof maladaptive thinking, feelings and behaviour thatleads to exaggerated importance given to thesymptoms and disproportionately high impairment.However, if impairing, single symptom is also

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society204
sufficient to make a diagnosis. Requirement forpresence of a specific number of symptoms involvingdifferent systems like neurological, urogenital,gastrointestinal systems is eliminated in DSM-5,which was difficult to apply in children. Patients withDSM-IV TR diagnosis of hypochondriasis can begiven this diagnosis if significant somatic symptomsaccompany the hypochondriacal preoccupation.Patients with isolated chronic pain symptom shouldbe given a specifier- “with predominant pain”.16 Thediagnostic criteria for DSM-5 somatic symptomdisorder are given in Table 2.
Table-2: Diagnostic guidelines for somaticsymptom disorder as per DSM-5
DSM-5 Diagnostic guidelines for somaticsymptom disorder
A. One or more somatic symptoms that are distressing andresult in significant disruption of daily life.
B. Excessive thoughts, feelings, or behaviour related to thesomatic symptoms or associated health concernsmanifested by at least one of the following:1. Disproportionate and persistent thoughts about the
seriousness of one’s symptoms.2. Persistently high level of anxiety about health or
symptoms3. Excessive time and energy devoted to these symptoms
or health concerns.C. Although any one somatic symptom may not be
continuously present, the state of being symptomatic ispersistent (typically more than 6 months)Specify if:With predominant painSpecify if:PersistentSpecify current severity :MildModerateSevere
Source: DSM-5, American Psychiatric Association
Somatic symptoms are equally common in bothboys and girls before adolescence, whereas girlsexpress more somatic symptoms after adolescence.Most common somatic symptoms are head ache,pain abdomen, fatigue, nausea, vomiting etc. DSM-IV TR undifferentiated somatoform disorder is themost common diagnosis in children.5,18
Children rarely present with multiple somaticsymptoms. Often, they present with a singlesymptom, commonly pain symptom. Typically painabdomen is located to the peri-umbilical region,
worsens during day time and absent during nightand on holidays. It can sometimes be associatedwith altered bowel habit, nausea, vomiting, and pallor.Persistent severe pain abdomen is often associatedwith significant stressor.
Head ache often presents with the character-istics of tension type headache, described as a dull,constant pain in frontal region. It can also co-occurwith migraine, hence a detailed assessment iswarranted. Fatigue, muscle-ache, neurologicalsymptoms often begin at adolescence.
Illness anxiety disorderIllness anxiety disorder has replaced the
diagnosis of hypo-chondriasis of DSM-IV TRanxiety disorder. It is characterised by the fear ofhaving a dreaded illness. Repeated negative medicalinvestigations and reassurance do not solve theproblem, rather strengthen the patient’s preoccupa-tion. There is no literature specifically on illnessanxiety disorder in children, literature on hypochon-driasis is also poor. A proxy form has been describedwhere caretakers excessively worry over theirchildren with normal phenomena or minor symptoms.The hypochondriasis is believed to begin in lateadolescence and early adulthood, and it leads tosignificant health care utilization. Depression, anxietyand obsessive-compulsive disorder (OCD) are thecommon co-morbidities of hypochondriasis.1,18
Conversion disorderConversion disorder is characterized by single
or multiple deficits or symptoms suggestive ofneurological or general medical conditions, but arenot corroborating with any anatomical or patho-physiological explanations.
Conversion disorders are common in Indian setup than in western population.Usually onset is abruptand in most commonly preceded by any stressfulevent. Presence of several factors like – personalityrelated (anankastic personality traits), other axis Ico-morbidities (anxiety or depression), grief, abuse,perceived parental rejection, stress at home or schoolsettings are commonly associated with conversiondisorder in children and adolescents.19
Common presentations include pseudo seizures,syncope, abnormal movements of limbs, paraes-thesia, and impaired vision etc. Children can alsopresent with symptoms mimicking the illness of

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 205
elders in the family. General physical examination,neurological examination and relevant investigationsare always non-contributory. La belle indifference,once thought as pathognomonic symptom ofconversion disorder is uncommon in children.1,18
Table 5 shows difference between true seizure andpseudo seizure.29
Table 3: Diagnostic features of illnessanxiety disorder as per DSM-5
DSM-5 Diagnostic guidelines for Illness anxietydisorder
A. Preoccupation with having or acquiring a serious illnessB. Somatic symptoms are not persistent or, if present, are
only mild in intensity. If another medical illness is presentor there is high risk for developing a medical condition(e.g. Strong family history is present), the preoccupationis clearly excessive or disproportionate.
C. There is a high level of anxiety about health, and theindividual is easily alarmed about personal health status.
D. The individual performs excessive health relatedbehaviours (e.g., repeatedly checks his or her body forsigns of illness) or exhibits maladaptive avoidance (e.g.,avoids doctor or appointments and hospitals)
E. Illness preoccupation has been persistent for at least 6months, but the specific illness that is feared may changeover period of time.
F. The illness-related preoccupation is not better explainedby another mental disorder, such as somatic symptomdisorder, panic disorder, generalized anxiety disorder,body dysmorphic disorder, obsessive compulsive disorder,or delusional disorder, somatic type.Specify if:Care seeking typeCare avoiding type
Psychodynamic theories postulate that patientsunconsciously “convert” their underlyingpsychological conflicts into the physical symptoms,and the relief obtained by doing so is called primarygain. Secondary gain is term used for the ‘gains’the patients obtain from outside because of thesymptoms for example excessive sympathy andprotection from the family and friends, concessionfrom work or school etc. Secondary gains act aspositive reinforcements and play significant role inmaintenance of symptoms.18
Factitious disorderFactitious disorder is characterised by inten-
tional production of physical/ psychiatric symptoms.
Unlike conversion disorder the symptoms of facti-tious disorder appear to be produced intentionallywith anintent of deception. Factitious disorder differsfrom malingering in that the former the benefits areemotional and not materialistic. In children, two typesof factitious disorder are identified. One where childhimself produces the symptoms and the other onewhere symptoms in child are produced by a caretaker, called as factitious disorder by proxy. The laterone is commonly known as Munchausen syndrome,and was described for the first time by Meadow.30
Table-4: Diagnostic features of conversiondisorder as per DSM-5
DSM-5 Diagnostic guidelines for conversiondisorder (Functional neurological symptom
disorder)
A. One or more symptoms of altered voluntary motor orsensory function.
B. Clinical findings provide evidences of incompatibilitybetween the symptoms and recognized neurological ormedical conditions.
C. The symptom or deficit is not better explained by anymedical or mental disorder
D. The symptom or deficit causes clinically significantdistress or impairment in social, occupational, or otherimportant areas of functioning or warrants medicalevaluation.Specify symptom typeWith weakness or paralysisWith abnormal movementWith swallowing symptomsWith speech symptomWith attacks or seizureWith anaesthesia or sensory lossWith special sensory systemWith mixed symptomsSpecify if:Acute episodePersistentSpecify if:With psychological stressorWithout psychological stressor
Source: DSM-5, American Psychiatric Association
A review of factitious disorder in youth overpast 30 years described 42 cases with the ageranging from 8 to 18 years old. The majority of

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society206
children were females, and were above 15 years ofage. Frequently reported conditions were fever,ketoacidosis, purpura, and infections. The meanduration of falsification of symptoms was around16 months before discovery. When confronted, allyounger children accepted their behaviour, whereasonly 55% of the older children did so. The patientswere found to be bland, flat and indifferent.Dysthymia, oppositional defiant disorder, adjustmentdisorder, anorexia nervosa, passive dependantpersonality disorder and hysterical disorder werecommon comorbidities. Many of them beganfabricating the symptoms after some experiencewith medical set up. Strained family relationshipsand family history of psychiatric illness were commonfindings.31
In the proxy form, the caretaker, often a parentdeliberately produces symptoms in children. Themotives are said to be assuming a sick role,enhancing self-identity by acting as a selflesscaregiver or main-taining a relationship with medicalprofessionals, where caretaker controls doctor’sattention. Care-takers initially are perceived asconcerned and caring. They are considered as modelcare givers by the health care staff. Majority ofperpetrators are mothers. Assessment of mothers,revealed frequent histories of self-harm, factitiousdisorder, personality disorder and drug abusers. Childmay or may not be part of deception, either activelyor passively. Common presentations are gastro-
Table 5: Difference between true seizure and pseudo seizure
Sl. No Clinical features Epileptic seizures Dissociative seizures
1 Clinical pattern Stereotyped and know clinical pattern No established pattern. Movementsappear purposeful.
2 Place of occurrence Anywhere Usually indoors, at safe places.3 Occurrence during sleep Yes No4 Sustaining injury Common Uncommon5 Speech No verbalization during seizure Verbalization may occur and may be
Stereotyped sounds may be produced emotionally charged.6 Facial expression Trismus in tonic phase, symmetrical Emotional expressions may be seen
twitching in clinic phase7 Duration Usually short (for about 70 sec) Can occur for minutes8 Eye gaze Staring/ up rolled Avoidant gaze.9 Pupillary reaction light Absent, usually dilated pupils Present10 Corneal reflex Absent Present11 Plantar reflex Up-going Absent12 Post ictal confusion Present Absent13 EEG May be abnormal Usually normal14 Serum prolactin Increased to more than 1000 IU/ml Normal or less than 500 IU/ml
15-20 minutes after seizure.Returns to normal levels within 1 hour.
Table 6: Diagnostic features of factitious disorderDiagnostic guidelines for Factitious disorder
Factitious disorder imposed by selfA. Falsification of physical or psychological signs or
symptoms, induction of injury or disease, associated withidentified deception.
B. The individual presents himself or herself to others as ill,impaired or injured.
C. The deceptive behaviour is evident even in the absence ofobvious external rewards.
D. The behaviour is not better explained by another mentaldisorder such as delusional disorder or another psychoticdisorder.Specify :Single episodeRecurrent episode
Factitious disorder imposed on an another(Previously Factitious Disorder by Proxy)A. Falsification of physical or psychological signs or
symptoms, induction of injury or disease, in another,associated with identified deception.
B. The individual presents another individual (victim) toothers as ill, impaired or injured.
C. The deceptive behaviour is evident even in the absence ofobvious external rewards.
D. The behaviour is not better explained by another mentaldisorder such as delusional disorder or another psychoticdisorder.Note: The perpetrator, not the victim, receives thisdiagnosisSpecify :Single episodeRecurrent episode
Source: DSM-5, American Psychiatric Association

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 207
intestinal, cardiopulmonary, neurologic, infections,dermatologic symptoms.
A review of literature of 451 cases of factitiousdisorder by proxy had revealed that majority ofchildren were diagnosed before the age of 6. Mostfrequent methods were suffocation, drug admini-stration and poisoning. Most frequent presentationswere apnoea, anorexia, diarrhoea, seizures, cyanosis,asthma, fever etc. about 7% of the patients had longterm disabilities and 6% were dead. Among thesiblings, about 25% were dead and 60% had similarsuspicious symptoms. Around 30% of the perpetra-tors had employment or training in health and relatedprofession. About one fourth of them had psychiatricdiagnosis, commonest being depression andpersonality disorders. About 22% had a history ofchild abuse.32
Psychological factors affecting medical illnessThis is a newly introduced diagnostic entity in
DSM-5. It is well known fact that psychologicalproblems often coexist with medical illness andaffect their course and outcome, for examplerelationship between asthma and anxiety, pepticulcer and stress, cardiovascular illness anddepression etc. Many patient related factors likecoping skills, personality traits, and adherence tomedical advice affect the medical illness.
Body dysmorphic disorderBody dysmorphic disorder has been moved from
somatoform disorder to obsessive compulsivespectrum disorder in DSM-5. This clinical entity isdescribed here as it continues to be a part of somato-form disorders (hypochondriasis) in ICD and alsofor the sake of comparison with other somatizationdisorders.
In Body dysmorphic disorder, there occursexaggerated concern towards ones appearance andsome perceived bodily defects, which usually startsduring the period of adolescence and follows achronic course.33,34 Individuals with body dysmorphicdisorder, usually engage in activities like –
• Repeated self-checking of body morphology(mirror gazing, grooming)
• Repeated assurance seeking• Repeated consultation and doctor shoppingPerceived body image distortion produces
significant psycho-social distress and may lead to
depression and suicidal behaviour.11 A series ofgender specific morphological changes occursduring adolescence which may be the targetsymptom in adolescents affected with bodydysmorphic disorder.11 However, this disorder is notextensively studied in paediatric population andresearch is needed to understand this entity inchildren and adolescents.11,34 Body dysmorphicdisorder in paediatric population is mostly related toskin and hair, producing significant decline inperformance at school and social situations.11,34
Table-7: Diagnostic features of Psychologicalfactors affecting medical illness
DSM-5 Diagnostic guidelines for Psychologicalfactors affecting medical illness
A. A medical symptom or condition, (other than mentaldisorder) is present.
B. Psychological or behavioural factors adversely affect themedical condition in one of the following ways:1. The factors have influenced the course of the medical
condition as shown by a close temporal associationbetween the psychological factors and thedevelopment or exacerbation of, or delayed recoveryfrom, the medical condition.
2. The factors interfere with the treatment of medicalcondition (e.g., poor adherence)
3. The factors constitute the additional well-establishedhealth risks for the individual.
4. The factors establish the underlying pathophysiology,precipitating or exacerbating symptoms ornecessitating medical attention.
C. The psychological and behavioural factors in criterion Bare not better explained by an another mental disorder(e.g.,panic disorder, major depressive disorder, posttraumaticstress disorder)Specify current severity:MildModerateSevereExtreme
Source: DSM-5, American Psychiatric Association
Assessment and ManagementChildren with somatic symptoms are often
referred to psychiatry either by a paediatrician or ageneral practitioner. It is not uncommon that child islabelled as “mental” or told that “all in your mind”before referring to a psychiatrist, for the dismal of

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society208
the parents and child. Hence the first step in thepsychiatric management is taking parents and childinto confidence and building a rapport.
A detailed history and physical examination isimportant not only to rule out any organic conditionbut also to make a positive diagnosis of somaticsymptom disorder. Points that are helpful in makinga diagnosis are - symptoms not fitting into anyphysical diagnosis, disproportionate disability,stressors which are temporally correlating, previoushistory of somatic symptoms, “role model” in familyetc.26,35 Child should be encouraged to express hisfeelings. Methods like asking the child to write on arelated neutral topic or to paint can sometimes helpin identifying the stressors. Assessment of tempera-ment of child is essential. Response to the placebo,suggestion and psychological treatment should beassessed. Parents should also be assessed to under-stand the parent child relationships, family dynamics,family conflicts and their understanding and attitudetowards child’s symptoms. Information from schoolis also important to know any adjustment problemsat school that would have led to symptoms.35
Diagnosing somatoform disorders, particularlyconversion disorder in paediatric population is oftena challenge.36 One should think about the long termimplications of such diagnosis. The diagnosis ofsomatoform disorder in children and adolescentsneeds to be reviewed time to time as many medicalconditions may present in the early days as vague,unexplained symptoms with normal investigationfindings.
Some tools have been developed for thestructured assessment of the somatic symptoms inchildren. The children’s somatization inventory (CSI-35) is a 35 item scale to assess the medicallyunexplained symptoms. It is the most widely usedscale for this purpose and is well validated forcommunity and clinical sample. A revised versionwith 24 items has been introduced to make the toolconcise and to improve the validity.37 The somaticcomplaint list is a self-report questionnaire, whichhas been found suitable in children between 8 to 12years of age in the initial validation study.38 Somaassessment interview (SAI) is a parent interviewquestionnaire.39 Functional disability index (FDI) andChalder Fatigue Self-Report Scale are also usefultools.40
Management of a child with somatic symptom
disorder is individualized, however the generalprinciples are same. The goals of management areenlisted in Table 7. It is important on the part ofpsychiatrist to convey the message that, he acceptsthat, child’s symptoms and suffering are real and isgenuinely concerned towards them. Psychia-tristshould team up with paediatrician, child psycho-logist, and psychiatric social worker for a compre-hensive management. Psychoeducation shouldaddress the issues like mind body relationships,physical manifestation of stress but one should avoidtoo much psychologizing the symptoms. Child shouldbe handled with empathy. Focus should be onreducing the symptoms and improving the function-ing. Pain diaries are helpful in delineating theconditions that exuberate the pain. Appropriate useof positive and negative reinforcements should bemade to enhance the functioning. Secondary gainsshould be identified and cut. Age appropriatefunctioning should be encouraged and initiated assoon as possible. Face saving methods like physio-therapy, aerobic exercise, and hot fomentation canbe useful.
Table-8: Treatment goals for somaticsymptoms and related disorders in children
Goals Issues addressed
Immediate goals Involvement of family in treatmentCessation of unnecessary medicalinvestigation Ensuring the safety ofchild
Short term goals Maintaining reasonable medicalcareSymptom reductionTo initiate age appropriate activities
Long term goals Appropriate (not excessive)medical careResolution of symptomsTo develop appropriate copingskillsTo address environmental andpsychological stressorsResumption of age appropriateactivities
There is limited literature on usefulness ofvarious non-pharmacological treatments in childrenwith somatic symptoms. School based relaxationexercise administered by a nurse was helpful inreducing tension type headache in a study by Larssonand Carlsson (1996).41 Guided imagery was superiorto routine paediatric care in a small study on children

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 209
with recurrent abdominal pain.42 Efficacy of CBTin somatization disorders especially in recurrentabdominal pain is promising. A randomised controltrail by Robins et al concluded that cognitivebehavioural family therapy was superior to standardmedical care and improvement persisted even afterone year.43 Cochrane systematic review on psycho-logical therapies for recurrent abdominal pain inchildren concluded that, psychological treatments areeffective in reducing pain intensity for children andadolescents with headache and benefits from therapyappear to be maintained. Psychological treatmentsalso improve pain and disability for children withnon-headache pain. There is limited evidenceavailable to estimate the effects of psychologicaltherapies on mood for children and adolescents withheadache and non-headache pain.44
There is no convincing evidence for pharmaco-therapy for somatic symptoms in children. Amulticentre randomised control trial (RCT) compar-ing Amitriptyline and placebo in children withfunctional gastrointestinal symptoms found thatamitriptyline was no better than placebo.45 Cochranereview on the antidepressants for the treatment ofabdominal pain related functional gastrointestinaldisorders in children and adolescents found only twoRCTs eligible for inclusion (one of them is describedabove). Both studies failed to establish superiorityof amitriptyline over placebo.46
Despite the lack of evidence for pharmaco-therapy, drugs are sometimes used in children withsomatic symptoms. SSRIs are have shown possiblebenefits in adults with somatoform disorder, and aresometimes also used in children. Low dose tricyclicantidepressants are often used by for functionalgastrointestinal symptoms and headache. Anti-depressants are advised only in case of significantcomorbidities of anxiety and depression.
There are no standard guidelines for manage-ment of factitious disorder. Once the diagnosis isconfirmed, the members of the treatment team withbest therapeutic alliance with the parent should tryconfronting the behaviour. The aim of confrontationis to educate the parent about the health hazards tothe child. Occasionally, perpetrators may confesswhen confronted. If otherwise, it is not useful tocontinue to confront even after multiple failedattempts. Before confronting, arrangements shouldbe made to ensure child’s safety. Sometimes child
needs to be separated from the parent, in that case,child’s psychological problems should be promptlyaddressed. Relapse is a common phenomenon infactitious disorder, hence a continued relationshipwith the child and the family is essential.18,47
Psychiatrist should be an integral part of treat-ing team for management of psychiatric factorsaffecting medical illness. Proper Psychoeducation,family education, supportive psychotherapy, cognitivebehavioural therapy and judicial use of antidepre-ssants and anxiolytics may be needed.Propositions in ICD 11
Propositions has been made for somatoformdisorder in ICD 11 and the beta draft of ICD 11 hasbeen released recently in the public domain.48 Theterm “Bodily distress disorder” is proposed to replacesomatoform disorder in ICD-11 and it will includeall the diagnostic subcategories mentioned undersomatoform disorder in ICD-10, except the entity“Hypochondriasis”.49 Bodily distress disorder (BDD)has been categorised according to the severity asmild, moderate and severe BDD. A new terminology“Body integrity dysphoria” has been introduced,which refers to an entity characterized by – intenseand persistent desire to become physicallydisabled in a significant way.48 It usually has itsonset in the adolescence.Conclusion
Somatic symptoms are common in children.They cause significant morbidity, long term psychia-tric consequences and significant healthcare utiliza-tion. Recurrent functional pain symptoms, non-epileptic seizures, motor and sensory conversiondisorder are common presentations. Specificdiagnostic guidelines for children are lacking.Management principles include cessation ofunnecessary medical investigations, proper psychoeducation, and use of appropriate positive andnegative rewards to reinforce age appropriatefunctioning, avoidance of secondary gains,addressing family and scholastic problems andimproving functioning. There is good evidence forusefulness of CBT in children. Pharmacotherapy isto be used only in case of significant psychiatric co-morbidities.
References1. Dingle AD. Disorders with physical symptoms.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society210
In: Sexson SB editor. Child and AdolescentPsychiatry. 2nd ed. Blackwell Publishing Ltd2005.
2. Lipowski ZJ. Somatization: the concept and itsclinical application. Am J Psychiatry 1988; 145: 1358–1368.
3. Beck JE. A Developmental Perspective onFunctional Somatic Symptoms. J Pediatr Psychol2008; 33(5) : 547–562.
4. Apley J. The Child with Abdominal Pains, 2ndedition. Oxford: Blackwell Scientific 1975.
5. Mohapatra S, Deo SJK, Satapathy A, Rath N.Somatoform Disorder in Children andAdolescents. German J Psychiatry 2014; 17(1): 19-24.
6. Postilnik I, Eisman HD, Price R, Fogel J. Analgorithm for defining somatization in children.J Can Acad Child Adolesc Psychiatry 2006;15(2) : 64-74.
7. Garber J, Walker LS, Zeman J. Somatizationsymptoms in a community sample of childrenand adolescents: Further validation of theChildren’s Somatization Inventory. PsycholAssess 1991; 3 : 588–595.
8. Offord DR, Boyle MH, Szatmari P, Rae-GrantNI, Links PS, Cadman DT, Byles JA, CrawfordJW, Blum HM, Byrne C, et al. Ontario ChildHealth Study. II. Six-month prevalence ofdisorder and rates of service utilization. ArchGen Psychiatry 1987; 44(9) : 832-6.
9. Bienvenu OJ, Samuels JF, Riddle MA, Hoehn-Saric R, Liang KY, Cullen BA, Grados MA,Nestadt G. The relationship of obsessive–compulsive disorder to possible spectrumdisorders: results from a family study. BiolPsychiatry 2000; 48(4) : 287-93.
10. Otto MW, Wilhelm S, Cohen LS, Harlow BL.Prevalence of body dysmorphic disorder in acommunity sample of women. Am J Psychiatry2001; 158 : 2061–2063.
11. Dyl J, Kittler J, Phillips KA, Hunt JI. Bodydysmorphic disorder and other clinicallysignificant body image concerns in adolescentpsychiatric inpatients: prevalence and clinicalcharacteristics.Child Psychiatry Hum Dev2006; 36(4) : 369-82.
12. Kleinman A. Depression, somatization, andthe”new cross-cultural psychiatry”. Soc SciMed 1977; 11 : 3–10.
13. Weiss B, Tram JM, Weisz JR, Rescorla L,Achenbach TM. Differential symptomexpression and somatization in Thai versus U.S.children. J Consult Clin Psychol 2009; 77(5) :987-92.
14. World health organization (WHO). InternationalClassification of Disorders 10th edition: clinicaldescription and diagnostic guidelines. Geneva:WHO 1992.
15. American Psychiatric Association. Diagnosticand Statistical Manual IV Text Revision (DSMIV TR) Washington DC: American PsychiatricAssociation 2000.
16. American Psychiatric Association. Diagnosticand Statistical Manual of Mental HealthDisorders. 5th (ed.) Washington DC: AmericanPsychiatric Association 2013.
17. Ghanizadeh A, Firoozabadi A. A review ofsomatoform disorders in DSM-IV and somaticsymptom disorders in proposed DSM-V.Psychiatria Danubina 2012; 24 : 353–358.
18. Dell ML, Campo JV. Somatoform Disorders inChildren and Adolescents. Psychiatr Clin N Am2011; 34 : 643–660.
19. Leary PM. Conversion disorder in childhood—diagnosed too late, investigated too much? JRSoc Med 2003; 96(9) : 436-8.
20. Roelofs K, Van Gallen G, Keÿers G, HoogduimC. Motor initiation and execution in patients withconversion paralysis. Acta Psychol 2002; 110 :21-34.
21. Marshall JC, Halligan PW, Fink GR, Wade DT.Frackowiak RSJ. The functional anatomy of ahysterical paralysis. Cognition 1997; 64 : B1-8
22. Vuilleumier P, Chicherio C, Assal F, SchwartzS, Slosman D, Landis T. Functional neuro-anatomical correlates of hysterical sensori-motor loss. Brain 2001; 124 : 1077-90.
23. Thomsen AT, Compass BE, Colletti RB, StangerC, Boyer MC, Konik BS. Parent reports ofcoping and stress response in children withrecurrent abdominal pain. J Pediatr Psychol2002; 27(3) : 215-226.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 211
24. Ciechanowski PS, Walker EA, Katon WJ,Russo JE. Attachment Theory: A Model forHealth Care Utilization and Somatization.Psychosom Med 2002; 64 : 660–667.
25. Tsao JC, Allen LB, Evans S, Lu Q, Myers CD,Zeltzer LK. Anxiety sensitivity and catastro-phizing: associations with pain and somatizationin non-clinical children. J Health Psychol 2009;14(8) : 1085-94.
26. Fiertag O, Taylor S, Tareen A, Garralda E.Somatoform disorders. In Rey JM (ed),IACAPAP e-Textbook of Child and AdolescentMental Health. Geneva: International Associa-tion for Child and Adolescent Psychiatry andAllied Professions 2012.
27. Garralda E. Somatization and SomatoformDisorders. In: Skuse D, Bruce H, Dowdney L,Mrazek D, editors. Child Psychology andPsychiatry Frameworks for Practice. 2ndEdition. New Jersey: John Wiley & Sons Ltd;2011.
28. Didie ER, Tortolani CC, Pope CG, Menard W,Fay C, Phillips KA. Childhood abuse and neglectin body dysmorphic disorder. Child Abuse Negl2006; 30(10) : 1105-15.
29. Ahuja N, Hebbar S. Dissociative Disorders. In:Vyas JN, Ahuja N, editors. Textbook of post-graduate psychiatry, 2nd edition. Delhi: JaypeePublications 2008.
30. Meadow R. Munchausen syndrome by proxy:Hinterland of child abuse. Lancet 1977; 2 : 343–345.
31. Libow JA. Child and adolescent illness falsifi-cation. Pediatrics 2000; 105 : 336–342.
32. Sheridan MS. The deceit continues: an updatedliterature review of Munchausen syndrome byproxy. Child Abuse Negl 2003; 27 : 431–451.
33. Grau K, Fegert JM, Allroggen M. Body dysmor-phic disorder. Z Kinder Jugend PsychiatrPsychother 2015; 43(1) : 29-35; quiz 36-7.
34. Albertini RS, Phillips KA. Thirty-three casesof body dysmorphic disorder in children andadolescents. J Am Acad Child Psychiatry 1999;38 : 453–459.
35. Sitholey P, Agarwal V. Clinical practice guide-lines for the management of pediatric somato-
form disorders. Indian J Psychiatry 2008; 157-67.
36. Barnum R. Problems with diagnosing Conver-sion Disorder in response to variable and unusualsymptoms. Adolesc Health Med Ther 2014; 5 :67-71.
37. Walker LS, Beck JE, Garber J, Lambert W.Children’s Somatization Inventory: psychometricproperties of the revised form (CSI-24). JPediatr Psychol 2008; 34(4) : 430-40.
38. Jellesma FC, Rieffe C, Terwogt MM. TheSomatic Complaint List: Validation of a self-report questionnaire assessing somaticcomplaints in children. J Psychosoma Res 2007;63 : 399– 401.
39. Rask CU, Christensen MF, Borg C et al. Thesoma assessment interview: new parentinterview on functional somatic symptoms inchildren. J Psychosom Res 2009; 66(5) : 455-64.
40. Chalder T, Berelowitz G, Pawlikowska T, et al.Development of a fatigue scale. J PsychosomRes 1993; 37 : 147-153.
41. Larsson B, Carlsson J. School based, nurseadministered relaxation training forchildren withchronic tension type headache. J PediatrPsychol 1996; 21(5) : 603-614.
42. Weydert JA, Shapiro DE, Acra SA, MonheimCJ, Chambers AS, Ball TM. Evaluation ofguided imagery as treatment for recurrentabdominal pain in children: a randomizedcontrolled trial. BMC Pediatrics 2006; 6(29) :1–10.
43. Robins PM, Smith SM, Glutting JJ, Bishop CT.Randomized Controlled Trial of a Cognitive-Behavioral Family Intervention for PediatricRecurrent Abdominal Pain. J Pediatr Psychol2005; 30(5) : 397-408.
44. Eccleston C, Palremo TM, Williams AC,Lewandowski A, Morley S, Fisher E et al.Psychological therapies for the management ofchronic and recurrent pain in children andadolescents. Cochrane Database Syst Rev2014; 5 : CD003968. doi:10.1002/14651858.CD003968.pub3.
45. Saps M, Youssef N, Miranda A, Nurko S,

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society212
Hyman P, Cocjin J, et al. Multicenter, rando-mized, placebo controlled trial of amitriptylinein children with functional gastrointestinaldisorders. Gastroenterology 2009; 137(4) :1261–9.
46. Kaminski A, Kamper A, Thaler K, ChapmanA, Gartlehner G. Antidepressants for thetreatment of abdominal pain-related functionalgastrointestinal disorders in children andadolescents. Cochrane Database of SystematicReviews 2011; 7 : CD008013. DOI: 10.1002/14651858.CD008013.pub2
47. Sandberg S, Stevenson J. Psychiatric Aspectsof Somatic Disease. In: Rutter M, Bishop DVM,Pine DS, Scott S, Stevenson J, Taylor E, ThaparA, editors. Rutter’s child and adolescentpsychiatry. 5th edition. Oxford: BlackwellPublishing Limited; 2008.
48. ICD-11 for Mortality and Morbidity Statistics(2018). https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f334423054[ Last accessed on 17-08-2018].
49. Gureje O, Reed GM. Bodily distress disorder inICD 11: problems and prospects. WorldPsychiatry. 2016;15(3):291-2.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 213
Personality Theories: A Brief OverviewSushma Rathee
Assistant Clinical Psychologist, PGIMER, Chandigarh, IndiaContact: [email protected]
Review Article
IntroductionThe term personality comes from the Latin word
persona, which means mask. Those definingpersonality as a mask view personality as one’spublic self. We select to display to the world. Thisdefinition of personality implies that important aspectsof a person remain concealed for some reason. Thedescription of the personality word has been startedwith the famous definition given by Allport.1 Hestated that “Personality is a dynamic organization,within the person, of those psychophysical systemsthat determine his unique adjustment to theenvironment”. Personality is generally defined asindividual unique and relatively stable pattern ofbehaviour, thoughts and emotion. More or less stable,
Types of personality Symptoms
a) Vata: is produced by an interaction of Dry, cold, light, subtle, clear and roughakasha (ether) and vayu (air)
b) Pitta emerges out of an interaction of Unctuous, hot, acute, fluid, acid, mobile, and poignantvayu and agni (fire)
c) Kapha is produced by the joint action Cold, soft, unctuous, sweet, stable and viscidof jala (water) and prithvi (earth)
comparable situations.2
Theories of Personalitya) Type Theories: The personality types are
used to communicate certain expectedbehaviours based on similarities. Suchefforts have been made since ancient times.
i) Charak Samhita of Ayurveda or the Indianscience of medicine, the original treatiseclassifies people on the basis of threeelements called doshas i.e., (a) vata, (b) pittaand (c) kapha.
Each of these refers to a type of temperamentreferred to as prakriti (nature) of the person.
ii) Hippocrates,3 a Greek physician, whoproposed a typology based on the fluid or
Four temperament categories Dominance CharacteristicSanguine blood Highly talkative, enthusiastic, active, and socialCholeric yellow bile Extroverted, independent, decisive, and goal-oriented, and ambitiousMelancholy black bile Analytical and detail-oriented, and they are deep thinkers and feelersPhlegmatic phlegm Relaxed, peaceful, quiet, and easy-going
Three temperament categories Body Structure TemperamentEndomorphic Fat, soft and round Relaxed and sociableMesomorphic Strong musculature, are rectangular Energetic and courageousEctomorphic Thin, long, and fragile Brainy, artistic, and introverts
internal factors make one person’s behaviourconsistent from one time to another, and differentfrom the behaviour other people would manifest in
humour.iii) Sheldon was proposed his personality theory
on the basis of body structure.4

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society214
b) Trait Theory of Personality1. In the trait theories the first name is Allport.5
Heconducted idiographic research thatfocused on conscious motivation andpersonal traits.
He proposed his theory at three levels of traits:a) Cardinal trait: These are defining
characteristic, in a small number of us, thatdominates and shapes all of our behavior.Mother Theresa is the most cited exampleof a person whose life focused on altruism— benefiting others, even to her owndetriment.
b) Central trait: These are general character-istic, between 5 and 10 of which shape muchof our behavior. For example, cheerfulnessand shyness can be central traits.
c) Secondary trait: These are those chara-cteristic, which apparent in only certainsituations. For example, being uncomfor-table in confined spaces can be a secondarytrait. Our unique pattern of traits determinesour behavior.
2. Second prominent trait theory is given byRaymond B. Cattell.6 He has developed adifferent approach to the description andanalysis of personality. He relies on datacollected from three sources: a) person’slife record, b) self-ratings, and c) objectivetests. Drawing from people’s life recordsand self-ratings, Cattell identified majorpersonality factors both within individualsand across people in general.
He proposed two major types of traits:A) Surface traits: These are those personality
characteristics which are easily seen byother people (one’s outward actions).
B) Source traits: In the opposite of surfacetraits, source traits are more basic traits thatunderlie the surface traits
Cattell6 distinguishes between surface traits,which are observable patterns of behavior, andsource traits, which he viewed as underlying, internaltraits responsible for our overt behavior. He viewedthe source traits as more important. Source traitscan be identified only by means of computer analysisof all the collected data.
3. Hans Eysenck7, proposed a theory that istrait as well as type in nature. He was tried
to reduce description of personality to threemajor genetically influenced dimensions,which everyone possesses to varyingdegrees. He was also used factor analysis,a statistical procedure that identifiescommon factors among groups of items, tosimplify a long list of traits into his threedimensions:a) Extroversion measures our sociability
and tendency to pay attention to theexternal environment, as opposed to ourprivate mental experiences.
b) Neuroticism measures our level ofinstability — howmoody, anxious, andunreliable we are — as opposed tostability — how calm, even-tempered,and reliable we are.
c) Psychoticism measures our level oftough-mindedness — how hostile,ruthless, and insensitive we are — asopposed to tender-mindedness — howfriendly, empathetic, and cooperativewe are.
4. Paul Costa and Robert McCrae8 proposeda latest theory in the area of personality.They have developed a five-factor modelof personality, nicknamed, “The Big Five.”In cross-cultural studies, the same fivefactors have been identified in trait ratings.The Big Five Theory includes the traits ofopenness, conscientiousness, extraversion,agreeableness, and neuroticism. (AcronymOCEAN).i) Openness-Person’s willingness to try
new things/experiencesii) Conscientiousness- Person’s
organization and motivationiii) Extraversion- Outgoing and socialiv) Agreeableness-Basic emotional style of
a person (easygoing, friendly, andpleasant)
v) Neuroticism-A person’s emotionalinstability or stability (excessiveworriers, overanxious, and moody).
Trait theories basically describe the personalityin terms of different different traits.
c) Psychoanalytic based theoriesSigmund Freud9 developed a numberofhypothetical models to show how the mind

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 215
(or what he called the psyche) works: (a)Topographic model of the psyche: how themind is organized. (b) Structural model: howpersonality works. (c) Psychogenetic modelof development: how personality develops.
Consciousa) Topographic model:-In the topographic
model the mind is divided into three sub-parts.
Sub-consciousi) Conscious: It is the part of the mind that
holds everything you are currently aware.ii) Preconscious: It contains everything you
could become aware of but are not
Unconscious currently thinking about.iii) Unconscious: It is the part of the mind that
we cannot usually become aware of.This is the deepest part of the mind.According to Sigmund Freud10 our all typeof repressed and disturbing memoriesstored in the unconscious level.
c) Structural model: According to Freud,structure of the mind divided into threeparts:i) Id: It functions in the unconscious level
and it is closely tied to instinctual andbiological processes. It is the primitivecore from which the ego and thesuperego develop. It is basedon‘pleasure principle’ the idea that allneeds have to be satisfied immediately,avoiding pain and seeking pleasure,regardless of external conditions.
ii) Ego: It focuses on ensuring the id’simpulses are expressed effectively inthe context of the real world.The ego,as a source of rationality, conforms tothe ‘reality principle’ – delaying thedischarge of energy from the id untilan appropriate object or activity can befound.
iii) Superego: Third structure, thesuperego, which provides moralguidance, embodying parental andsocietal values. It has two sub-systems:
(a) conscience: It consist images ofwhat is right and what deservespunishment – this is the basis for guilt.(b) Ego ideal: It consist imagesof whatis rewarded or approved of this is thebasis for pride.
Sigmund Freud9 describes two types of instinct:a) Life instinct or Eros: A drive for life, love,
growth, self-preservation, constructiveworks and human propagation. Libido –energy force for sexual activities.
b) Death instinct or Thanatos: A drive foraggression and death and destructiveness.Death instinct If external, leads to a persontoward homicide and if internal leads to theperson toward suicide or self-harm.
Types of anxietyHe defines anxiety in terms of an affective and
unpleasant feeling which alerts ego to the impendingdanger so that person can behave in an adaptiveway.
i) Realistic anxiety: It occurs when theemotional response to real danger.
ii) Neurotic anxiety: It occurs when anxietyregarding the ability of control of ego on idwishes, particularly sexual and aggressiveimpulse.
iii) Moral anxiety: It occurs when ego isthreatened by superego.
c) Psychogenetic model: In the psychogenicmodel he emphasize on stages of personalitydevelopment. Freudgave emphasis on thechildhood traumas as key to neuroticdisorder during adulthood.He believed thatpeople normally progress through fivestages of psychosexual development.
i) Oral stage (0 to18 months): The newbornbaby is completely dependent on others forthe satisfaction of all needs. During thisstage body pleasure is centered on themouth. The baby gets satisfaction fromsucking, eating, and biting in the course offeeding.
ii) Anal stage (18 to 3 years): It is characte-rized by a shift in body pleasure to the anus.It is reflected by a concern with the retentionand expulsion of faces. This is why Freudfelt that it is during toilet training a child has

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society216
the first experience with externally imposedcontrol. The pattern of toilet training,therefore, may influence later personalqualities and conflicts experienced by theperson.
iii) Phallic stage (3 to 6 years): In this stagethe child observes the difference betweenmale and female and experiences whatFreud called the Oedipus complex. This kindof attraction leads to serious conflict, whichhe termed as Oedipus and ElectraComplexes in boys and girls, respectively.
iv) Latency stage (7 to puberty): This stagefollows the phallicstage; there is very littleexplicit or overt concern with sexuality. Thechild represses his or her memories ofinfantile sexuality and forbidden sexualactivity.
v) Genital stage (puberty and above):During this stage the personattains maturityin psychosexual development. The personbecomes capable of genuine love for otherpeople and can achieve adult sexualsatisfaction. He or she may relate to othersin a heterosexual fashion. However, ifjourney towards this stage is marked byexcessive stress or overindulgence, it maycause fixation to an earlier stage ofdevelopment.
Carl Gustav Jung Analytical PsychologyDefinition of personality: Personality as
wholeness or unity which helps to adapt with physicalenvironment and society bythought, feelings,behavior and conscious and unconscious process.Jung believed that personality is shaped by thecumulative experiences of past generationsextending back to our evolutionary past.
a) Ego: It is the conscious mind, responsiblefor our feeling of identity and continuity.Structure of personality: According toJung’s10 analytic theory of personality, thepsyche—or whole personality—consists ofinteracting systems including the ego; thepersonal unconsciouswith its complexes; thecollective unconscious with its archetypes,attitudes, and functions; and the self.
b) Personal unconscious: it is similar to Freud’spreconscious and unconscious, a storehouse
of all our own past memories, hiddeninstincts, and urges unique to us. It containscomplexes, which are groups of associated,emotional, unconscious thoughts thatsignificantly influence our attitudes, andassociations that act as driving forces.
c) Collective unconscious is the powerful andinfluential system of the psyche thatcontains universal memories and ideas thatall people have inherited from our ancestorsover the course of evolution. The inheritedmemories are archetypes or commonthemes found in all cultures, religions, andliterature, both ancient and modern.
Four especially important archetypes in Jung’stheory are known as persona, shadow, animus&anima and self.
i) Persona – It is named after the mask wornby ancient Greek actors, or publicpersonality, mediates between the ego andthe real world.
ii) Shadow – A reverse image of the personacontains traits that are unacceptable to thepersona, whether they are positive ornegative.
iii) Animus – It is the masculine side of femaleswhile the anima is the feminine side ofmales.
iv) Self - It is the innate potential for wholeness,an unconscious ordering principle directingoverall psychic life that gives rise to the ego,which compromises with and is partlyshaped by external reality.
Psychic energy – the energy by which thework of personality is performed is called psychicenergy. Principle of opposite- aspolarity in physicalenergy like polarity is in the wish, affect of theperson. i.e. affect of pleasant and unpleasant.Principle of equivalence-if energy is expended inbringing about a certain condition, the amountexpended will appear elsewhere in the system.Principle of entropy-states when two bodies ofdifferent temperatures are placed in contact withanother heat will pass from the hotter to the colderbody.
Alfred Adler Individual PsychologyWhile Freud emphasized sex, and Jung empha-
sized ancestral thought patterns, Adler emphasized

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 217
social interest as the primary determinant ofbehavior. He made consciousness the center ofpersonality in his individual or ego theory ofpersonality.11
Personality – Adler saw individual as unique.He also postulated a principle of dynamism, whichin every individual is future directed and movestoward a goal. Once the goal is established, thepsychic apparatus shapes itself toward attainment.
Subjectivity of perception – Humans aremotivated by their expectation of the future than byexperiences of the past. Personality is not determinedby external cause rather by subjectivity perception.Human behavior are determined by the futureexpectation
Fictional Finalism – Adler called this fictionalfinalism. Many people behave as if there were aheaven or a hell in their personal future. Of course,there may be a heaven or a hell, but most of usdon’t think of this as a proven fact. That makes it a“fiction” in Vaihinger’s and Adler’s sense of theword. And finalism refers to the teleology of it: Thefiction lies in the future, and yet influences ourbehavior today
Style of life: Adler’s self is a personalized,subjective system that interprets and makes meaningfrom our experiences, trying to fulfill our unique styleof life, the system principle by which the individualpersonality functions.Striving for success:Ourcreative self-constructs our personality out of theraw material of heredity and experience. Adlerbelieved that people strive for superiority to bealtruistic, cooperative, creative, unique, aware, andinterested in social welfare. He thought that we alltry to compensate for inferiority complexes basedon what we see as physical, intellectual, or socialinadequacies. Social interest:Social interest is theinevitable compensation for all of our naturalweaknesses. Adler thought that birth order was animportant factor controlling personality. Birth order:He hypothesized that the oldest child (who isprepared for the appearance of a rival) is likely todevelop into a responsible, protective person; themiddle child is likely to be ambitious and welladjusted; and the youngest child is likely to bespoiled.
Erik Erikson’s Psychosocial TheoryErikson12 developed a theory of personality
development with a focus on social adaptation. Hecalls attention to the problems of social adaptation.With advancing age we face a wider range of humanrelationships. The solution of problems faced duringthe eight psycho-social stages determines adultdevelopment. His emphasis on social and culturalforces is crucial as it distinguishes him from Freud.He also viewed development as a life-long process.In this process ego identity is central. His conceptof identity crisis of adolescent has drawnconsiderable attention. Erikson believed that “humanpersonality in principle develops according to stepspre-determined in the growing person’s readinessto be driven toward, to be aware of, and to interactwith, a widening social radius”. On the other hand,the society “in principle, tends to be so constitutedas to meet and invite this succession of potentialitiesfor interaction and attempts to safeguard and toencourage the proper rate and the proper sequenceof their enfolding.” Thus young people must generatefor themselves some central perspective anddirection that gives them a meaningful sense of unityand purpose. Favorable outcomes of each stage aresometimes known as “virtues”, a term used in thecontext of Erikson’s work as it is applied to medicine,meaning “potencies.”
The Erikson life-stage virtues, in order of theeight stages in which they may be acquired, are:
I. Basic trust vs. basic mistrust: This stagecovers the period of infancy. 0-1 year ofage. - Whether or not the baby developsbasic trust or basic mistrust is not merely amatter of nurture. It is multi-faceted andhas strong social components. It dependson the quality of the maternal relationship.The mother carries out and reflects theirinner perceptions of trustworthiness, asense of personal meaning, etc. on the child.If successful in this, the baby develops asense of trust, and virtue named ‘hope’ isdeveloped which “forms the basis in thechild for a sense of identity”.
II. Autonomy vs. Shame – It around earlychildhood around 1–3 years old- Introducesthe concept of autonomy vs. shame anddoubt. During this stage the child is tryingto master toilet training.
III. Initiative vs. Guilt - Preschool / 3–6 years- Does the child have the ability to or do

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society218
things on their own, such as dress him orherself? If “guilty” about making his or herown choices, the child will not function well.Erikson has a positive outlook on this stage,saying that most guilt is quickly compen-sated by a sense of accomplishment. Aftersuccessful completion of this stage child hasdeveloped ‘purpose’ virtue.
IV. Industry vs. Inferiority: School-age / 6-11. Child comparing self-worth to others(such as in a classroom environment). Childcan recognize major disparities in personalabilities relative to other children. Eriksonplaces some emphasis on the teacher, whoshould ensure that children do not feelinferior. In the successful completion of thisstage the virtue is competence has beendeveloped.
V. Identity vs. Role Confusion: - Adolescent/ 12 years till 18. Questioning of self. Whoam I, how do I fit in? Where am I going inlife? Erikson believes, that if the parentsallow the child to explore, they will concludetheir own identity. However, if the parentscontinually push him/her to conform to theirviews, the teen will face identity confusion.Fidelity virtue has been developed.
VI. Intimacy vs. isolation: - This is the firststage of adult development. This develop-ment usually happens during young adult-hood, which is between the ages of 18 to35. Dating, marriage, family and friendshipsare important during the stage in their life.By successfully forming loving relationshipswith other people, individuals are able toexperience love and intimacy. Those whofail to form lasting relationships may feelisolated and alone.
VII. Generativity vs. stagnation: - It is thesecond stage of adulthood and happensbetween the ages of 35-64. During this timepeople are normally settled in their life andknow what is important to them. A personis either making progress in their career ortreading lightly in their career and unsure ifthis is what they want to do for the rest oftheir working lives. Also during this time, aperson is enjoying raising their children andparticipating in activities, that gives them a
sense of purpose. If a person is notcomfortable with the way their life isprogressing, they’re usually regretful aboutthe decisions and feel a sense ofuselessness.
VIII. Ego integrity vs. despair: - This stageaffects the age group of 65 and on. Duringthis time an individual has reached the lastchapter in their life and retirement isapproaching or has already taken place.Many people, who have achieved what wasimportant to them, look back on their livesand feel great accomplishment and a senseof integrity. Conversely, those who had adifficult time during middle adulthood maylook back and feel a sense of despair.Wisdom virtue is emerging in this stage.
Erikson’s research suggests that each individualmust learn how to hold both extremes of eachspecific life-stage challenge in tension with oneanother, not rejecting one end of the tension or theother.
Karen HorneyHorney brought a feminist perspective to
psychoanalytic theory and sharply attacked the malebias, she saw in Freud’s work. Her counterpart toFreud’s penis envy in females was the male’s wombenvy or desire to procreate. She thought that malesand females both are envious of attributes of theother sex, but that women were more envious ofmen’s societal status than their penises. Horneyproposed that youngsters feel helpless andthreatened, and learn to cope by showing affectionor hostility toward others, or by withdrawing fromrelationships.Adults who use all three strategies arehealthy, whereas according to her theory, using onlyone strategy leads to mental illness.13
Needs of child hood: Horney believed thatthere are two needs are important in childhood:satisfaction need and safety need.
Basic anxiety: these are the feelings ofloneliness and helplessness which is connected tothe repression of hostility.
Neurotic needs: recurrent failure becomesparts of personality which leads to neurotic needs.
These 10 neurotic needs can be classedinto three broad categories:
1. Needs that move you towards others:

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 219
These neurotic needs cause individuals toseek affirmation and acceptance fromothers and are often described as needy orclingy as they seek out approval and love.The need under this category areNeed forAffection and Approval, Need for a Partner,and Need for Personal Admiration.
2. Needs that move you away from others:These neurotic needs create hostility andantisocial behavior. These individuals areoften described as cold, indifferent, andaloof.The neurotic needs under this categoryareNeed to Restrict One’s Life, Need forSelf-Sufficiency and Independence.
3. Needs that move you against others:These neurotic needs result in hostility anda need to control other people. Theseindividuals are often described as difficult,domineering, and unkind. The needs underthis category are Need for Power, Need toExploit Others, Need for Prestige, Need forPersonal Achievement, and Need forPerfection and Unassailability.
d) Humanistic Theories of PersonalityAbraham Maslow’s Holistic Dynamic Theory14:
Trained as a behaviorist in the 1920s, Maslowthought that behaviorism could not account for hisobservations of developing children. He asserted thatwe are born good and move toward self-actuali-zation as our goal.
i) The physiological needs. These includethe needs people have for oxygen, water,protein, salt, sugar, calcium, and otherminerals and vitamins. Also, there’s theneeds to be active, to rest, to sleep, to getrid of wastes (CO2, sweat, urine, and feces),to avoid pain, and to have sex.
ii) The safety and security needs. When thephysiological needs are largely taken careof, this second layer of needs comes intoplay. One will become increasingly interes-ted in finding safe circumstances, stability,and protection.
iii) The love and belonging needs. Whenphysiological needs and safety needs are,by and large, taken care of, a third layerstarts to show up. One begin to feel theneed for friends, a sweetheart, children,
affectionate relationships in general, evena sense of community.
iv) The esteem needs Maslow noted twoversions of esteem needs, a lower one anda higher one. The lower one is the needfor the respect of others, the need for status,fame, glory, recognition, attention, reputa-tion, appreciation, dignity, even dominance.The higher form involves the need for self-respect, including such feelings as confi-dence, competence, achievement, mastery,independence, and freedom.
v) Self-actualization: is reaching toward thebest person one can be.
Rogers’ self-theoryHe proposed the self-theory,15 an organized,
consistent set of beliefs andperceptions about us,which develops in response to our life experiences.Experiences that are inconsistent with our self-concept cause us to feel threatened and anxious. Ifwe are well adjusted, we can adapt by modifyingour self-concept. Rogers believed that we are allborn with a need for unconditional positive regard,for acceptance and love from others independentof how we behave, and positive self-regard fromourselves. When positive regard is not unconditional,conditions of worth dictate behaviors that cause usto approve or disapprove of ourselves. Thedifference between our real self, and what Rogerscalls the ideal self, or what we think society wants,is called incongruence. To become fully functioning(Rogers’ term for self-actualization), we must learnto accept ourselves (unconditional positive self-regard) and unite the real and ideal selves into oneagain.
e) Behavioral Theory of Personalityi) Skinner was an influential behavioral
psychologist of the last half century. As aresult of his observations of experimentalstudies with pigeons, rats, people, and avariety of other organisms, Skinner deve-loped his operant conditioning theory.Skinner maintained that behavior ispersonality. The environment shapes whowe become, and who we become isdetermined by the contingencies ofreinforcement we have experienced. If we

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society220
change someone’s environment, we changehis/her personality.16
ii) George Kelly’s Personal Construct Theory.The primarily cognitive theories ofpersonality, the personal-construct theory ofengineer and psychologist George Kelly17
is the best known. He thought that, likescientists, we all try to make sense of ourworld by generating, testing, and revisinghypotheses about our social reality, calledpersonal constructs. We develop personalconstructs, for example, when we considerhow someone is similar to or different fromsomeone else. Our personal constructs area set of bipolar categories we use as labelsto help us categorize and interpret theworld.For example, our personal constructscan include happy/unhappy, energetic/inactive, selfish / generous, etc. We applyour personal constructs to all of the situationswe are in, and revise them when they arenot accurate. Our pattern of personalconstructs determines our personality.People who use few constructs tend tostereotype others. People who use too manytend to have difficulty predicting otherpeople’s behavior.
iii) Bandura18 thinks that we learn more byobservational learning than by operantconditioning.He explains behavior using hisconcept of reciprocal determinism, whichstates that the characteristics of the person,the person’s behavior, and the environmentall affect one another in two-way causalrelationships. The person includes persona-lity characteristics, cognitive processes, andself-regulation skills. The person’s behaviorincludes the nature, frequency, and intensityof actions. The environment includes stimulifrom the social or physical environment andreinforcement contingencies.According toBandura, self-efficacy is the major factorin how we regulate our lives. Self-efficacyis our belief that we can perform behaviorsthat are necessary to accomplish tasks, andthat we are competent. Bandura hasextended his theory to behavior of theindividual in groups. Collective efficacy isour perception that with collaborative effort,
our group will obtain its desired outcome.iv) Julian Rotter’s sociallearning theory is
focused on locus of control, the degree towhich we expect that a reinforcement oroutcome of our behavior is contingent onour own behavior or personal character-istics, is under the control of others, or isunpredictable. Those with an internal locusof control think they control and areresponsible for what happens to them—forexample, their hard work gets rewarded19.
ConclusionAll personality theories stress the importance
of experiences, particularly childhood experiences,in shaping and influencing personality. They differ,of course, in the precise dynamics of howexperiences contribute to personality developmentand change. Whereas the effects of experience takecenter stage in personality theories, physiologicalfactors are normally given only a secondary role.Though some theories mention heredity and otherbiological factors (Eysenck’s theory in particular),the classic theories have mostly ignored biologicalsources as contributors to personality. Thepersonality theorist attempts to describe what allhumans have in common (human nature), whatsome have in common, and the uniqueness of eachindividual (individual differences). A comprehensiveexplanation of personality would specify the relativeimportance of genetics, traits, socioculturaldeterminants, learning, existential– humanisticconsiderations, unconscious mechanisms, andcognitive processes.
References1. Allport GW. Personality: a psychological
interpretation. New York: Holt 1937.2. Child IL. Personality in Culture. In EF Borgatta,
WW Lambert (Eds.), Handbook of personalitytheory and research. Chicago: Rand McNally1968.
3. Merenda PF. ”Toward a Four-Factor Theoryof Temperament and/or Personality”. J PersAssess 1987; 51 : 367–374.
4. Sheldon H. The Varieties of Temperament.New York; London: Harper & Brothers.Archived from the original on 2012-02-24via University of Delhi 1942.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 221
5. Allport GW. Patterns and growth in personality.New York: Holt, Rinehart, Winston 1961.
6. Cattell RB. The scientific analysis of personality.Baltimore: Penguin Books 1965.
7. Eysenck HJ. Dimensions of personality: 16, 5or 3? Criteria for a taxonomic paradigm.Personality Indiv Diff 1991; 12 : 773–790.
8. Costa PT, McCrae RR. Six approaches to theexplication of facet-level traits: Examples fromconscientiousness. Eur J Psychol 1998; 12 : 117–134.
9. Freud S. The resistances to psycho-analysis. Inthe Standard Edition of the Complete Psycho-logical Works of Sigmund Freud, VolumeXIX (1923-1925): The Ego and the Id and otherworks 1961; 211-224
10. Jung CG. On the nature of psychology.Princeton: Princeton University Press 1960.
11. Adler A. The practice and theory of individualpsychology. London: Routledge, Kegan Paul1923.
12. Erikson EH. The life cycle completed. NewYork, NY: Norton 1982.
13. Horney K. Feminine psychology. New York:Norton 1967.
14. Maslow AH. Toward a psychology of being,New York: Van Nostrand 1968.
15. Rogers CR. A theory of therapy, personality,and interpersonal relationships as developed inthe client-centered framework. In S. Koch (ed.)Psychology: a study of a science, 3. New York:McGraw-Hill 1959; 184-256.
16. Skinner BF. Science and human behavior. NewYork: Macmillan 1953.
17. Hall CS, Lindzey G. Theories of personality. NewYork: John Wiley & Sons, Inc 1970.
18. Bandura A. A social learning interpretation ofpsychological dysfunction. In: P. London &D.Rosenhan (Eds.), Foundations of abnormalpsychology. New York: Holt, Rinehart &Winston 1968.
19. Rotter JB. Level of aspiration as a method ofstudying personality. II. Development andevaluation of a controlled method. J Exp Psychol1942; 31 : 410-422.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society222
Preclinical Concepts of DepressionBhumija Sharma,1 Preeti Sharma,2 Pradeep Kumar,3 Anil Sharma4
Department of Biochemistry, 1FH Medical College and Hospital, Etmadpur, Agra, UP;2,3Santosh Medical College and Hospital, Ghaziabad, UP;
4Department of Medicine, FH Medical College and Hospital, Etmadpur, Agra, UP.Contact: Preeti Sharma, Email: [email protected]
Review Article
IntroductionHealth is pivotal for the growth, development
of every individual and is vital for a happy and healthylife anywhere in the world. The World HealthOrganization [WHO] definition of health includesphysical, social, spiritual and mental health, and notmerely the absence of disease.1 The maxim, “thereis no health without mental health” underlines thefact that mental health is an integral and essentialcomponent of health.2 Due to outcome of techno-logical advancement, changing lifestyles, biologicalclock variations etc. diseases like, common mentaldisorders (CMDs), depression, alcohol use, suicidalbehaviors, anxiety, drug use, sleep disorders andseveral others are on the rise.3 Disorders related tobrain affect everyone, irrespective of age, gender,residence and lifestyles, even though some of themare at a higher risk for certain illnesses. These CMDsare neglected by individuals and families and ignoredtill they become severe. According to NationalMental Health Survey (NMHS) 2015 the prevalenceof depression for current, life time was 2.7% and5.2%. This indicated that, nearly 1 in 40 and 1 in 20suffer from past and current depression, respectively.It was reported to be more in females, in the age-group of 40-49 years and among people in urbanmetros, also high rates were reported among theelderly (3.5%).2 WHO defines depression as aCMD which, is characterized by persistent sadness,lack of interest and pleasure, fluctuations betweenfeelings of guilt and low self-esteem, as well as sleepand/or appetite disorders that affect activities of dailyliving? These manifestations occur in the differenttypes of depression and are distinguished in termsof intensity, duration and mode of presentation(WHO, 2017).4 “WHO ranks depression as the
fourth leading cause of disability worldwideandestimates that by 2020, it will be the secondleading cause.5 Indians are among the world’s oneof the most depressed people. The average age ofdepression is 31.9 years, 18.8 years, 22.7 years inIndia, China and US respectively.5 Aim of thisreview is to assemble all possible information relatedto depression including definition, types,symptoms,causes, mostly concentrating upon preclinical areasanatomy, physiology and biochemistry ofdepression.
Types of depressionMajor depression disorders (MDD) not a single
disorder but has many differing phenotypicpresentations that have features of many forms, justlike other illnesses, such as heart disease anddiabetes. However, important is that within each ofthese types, there is variety in the number, timing,severity and persistence of symptoms and alsodifferences in how individuals experience depressiondepending on age, gender etc. (Table 1)
Depression not only causes great mental agonybut also intrudes upon elementary biologicalprocesses that regulate inflammation, coagulation,metabolism, autonomic function, neuroendocrineregulation, sleep, and appetite.9-12 These distur-bances are likely to contribute to the prematurecoronary artery disease premature osteoporosis andthe doubling of mortality in patients with majordepression at any age independent of suicide,smoking, or significant physical illness.13-17
Etiology18-20
• Stressful environment• Inheritance - Some types of depression run
in families, indicating that a biological

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 223
(divorce), financial problem, or anyunwelcome change in life patterns cantrigger a depressive episode.
• A combination of all above (genetic,psychological and environmental factors).
• Regardless of ethnicity, men appear to beparticularly sensitive to the depressiveeffects of unemployment, divorce, lowsocioeconomic status.
• Physical, emotional or sexual abuse- eitheras a child or in females.
• Specific medications- used in treatment ofhigh blood pressure, cancer, seizures,extreme pain and to achieve contraceptioncan result in depression.
Individuals with anxiety, attention deficithyperactivity disorder (ADHD), substance abuse(Alcohol or drug abuse), and developmentaldisabilities are more prone.
Clinical features of major depressive disorderare mentioned in Table No. 223-27
Anatomical changes in depressionStructural and functional changes in MDD have
been reported especially in the brain structuresrelated to emotionalprocessing and mood regula-tion.28 In MDD patients, morphological abnormalitieshave been reported including volume reduction inseveral brain structures such as the hippocampus,basal ganglia, anterior cingulate cortex (ACC),orbitofrontal cortex (OFC), and dorsolateral pre-frontal cortex (DLPC), decreased cortical thick-ness, decrease in gray matter volume, and deterio-ration in white matter integrity.29,30 These volumechanges in regions are thought to be part of thenetwork and pathways of neurons involved indepression. Meta-analyses show that the volumesof both the left and right hippocampus decrease evenin the first episode of depression.31 There are alsoreports of reversal in decreased hippocampalvolume with treatment of antidepressants or ECTin the patients with depression.32,33 Volume changesin the hippocampus therefore may be a potentialdiagnostic marker in depression. Patients withdepression exhibit activity changes in areas such asthe OFC, DLPC, ventromedial prefrontal cortex(VMPC), insula, amygdala, and ACC, all are foundto be associated with functions such as the regulationof emotions, cognitive control, and reward
Table-1: Types of Depression
1. Melancholic: hyper arousal, anxiety, feelings ofworthlessness and hopelessness, deficiency of self forfuture satisfaction in relationships or work. Preventsexperience of pleasure in one’s achievement.6 Alterationsin a multiple system affecting inflammation andmetabolism. A diurnal variation in the severity ofdepressed mood, which is most severe early in themorning.7 Melancholic’s marks evidence of an activatedstress system. Signs of hyperarousal: hypercortisolism,suppression of the reproductive and growth hormones,insomnia.
2. Atypical depression: Patients often seem to shut offfrom themselves. Associated with a disturbing sense ofdisconnectedness and emptiness, usually complains of acognitive and mental tiredness and avoids others.Neurovegetative symptoms - lethargy, fatigue, excessivesleepiness, increased food intake, weight gain.8Both atypical and melancholic depressions haveAnhedonia (inability to feel pleasure in normallypleasurable activities). Dysphoria (state of unease orgeneralized dissatisfaction with life)
3. Major depression (MD): characterized by a combinationof symptoms that last for at least two weeks, with sadand/or irritable mood. Interfering with the ability to work,sleep, eat and enjoy other delightful activities. Disablingepisodes of depression can occur once, twice, or severaltimes in a lifetime.5
4. Dysthymia: Involves long-term (chronic) symptoms thatprevent the affected person from functioning at “fullsteam” or from feeling good but do not disable him/her5.Less severe but usually longer lasting type of depression
5. Bipolar disorder (manic depression): Group of mooddisorders that were formerly called manic-depressiveillness or manic depression, involve cycles of mood thatinclude at least one episode of mania or hypomania andmay include episodes of depression. Mania affectsthinking, judgment, and social behavior that cause seriousproblems and embarrassment in society. Shows aparticular pattern of inheritance. Mostly chronic andrecurring.
6. Postpartum depression (PPD): State that describesphysical and emotional changes occurring in women afterdelivery of a child. Can happen after the birth of anychild, not just the first child. Often keeps a woman fromdoing the things she needs to do every day. PPD are ofdifferent kinds - “BABY BLUES” - sudden mood swings,crying for no reason, feeling impatient, irritable, restless,anxious and lonely. May last for few hours or up to oneto two weeks after delivery.5 Postpartum psychosis is avery serious mental illness, it happens quickly, oftenwithin the first three months after childbirth. Depressioncauses them to lose touch with reality, have auditoryhallucinations, delusions as well.
vulnerability to depression can be inherited.• An external event- A serious loss (death),
chronic illness, difficult relationship

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society224
Table-2: Clinical features of major depressive disorder
Symptoms General Children Teenagers Elder
Sadness/ mood swings present present present presentIrritability/anger present present present presentChanges in appetite decreased Not common Present/higher risk may be caused by
of obesity other illnessesInsomnia / excessive sleeping Both Not common common With other disorderIndecisiveness/lack of concentration present present present Present due to age alsoMemory loss present Schoolwork suffers Work suffers Present due to age alsoFatigue/ tiredness present present present presentSuicidal thoughts/attempts May be — — Males at high riskSexual drive reduced — — —Special features — behavior problems Antisocial behaviour Antisocial behaviour
(ADHD)
processing.34,35 Patients with MDD exhibit hypo-active responses to emotional stimuli in the frontalregions and hyperactive responses in the limbicregions.30 For example, depressed patients show anincreased activity in the amygdala, ventral striatumand medial prefrontal cortex and decreased activityin the dorsal prefrontal cortex when looking atfrightened or sad face images.36-38 In earlier studies,frontal hypo-metabolism was found before treatmentand the reversal with treatment could possibly bethe best predictor of treatment response to bothantidepressants and cognitive behavioral therapy.39
Physiological changes in depressionHypothalamus-pituitary-adrenal (HPA) axis
system - Depressive disorders resemble thephysiology of chronic stress. Disorders of the HPAaxis are observed in 50–75% of patients withdiagnosed depression.40 The following status isfound: increased concentration of glucocorticoids inplasma, urine and cerebrospinal fluid, changes in thedaily profile of glucocorticoid secretion with morefrequent and longer periods of secretion, increasedsecretion of glucocorticoids in response to ACTH,an increase in the volume of hypophysis and adrenalglands.41,42 In the patients with a tendency to dwellingupon unpleasant events the level of cortisol is higherthan in a comparative group of healthy subjects.43
The hippocampus is a structure of the brain whichis particularly susceptible to stress-induced func-tional changes and dysregulation of the HPA axis.In such cases, a drop in the expression of the brain-derived neurotrophic factor (BDNF), deteriorationof long-term potentiation (LTP), and inhibition ofneurogenesis in the dentate gyrus (DG) are
observed.42 The series of physiological andbehavioral programs are responding in acute danger.These will enhance chances of survival during lifethreatening situations which includes tachycardia,increase in blood pressure and blood flow to thebrain and to the stressed body site, breakdown oftissue and the mobilization of fuel. Inhibition offunctions like feeding, sleep, sexual behavior, growthand reproduction are done, which are likely todiminish the possibility of surviving any emergency.Fear-related behaviors predominate during stressfulsituations and are crucial for survival during emer-gencies. There is rapid use of simple, well-rehearsedbehavioral and cognitive responses which are simpleand speedy. More complex, new or untestedresponses are inhibited that require considerable timeto assemble.44 Morale is maintained by stimulatingthe mesolimbic dopaminergic reward system duringthe acute crisis.
Inflammatory and prothrombotic status-During exposure to stressmultiple systems are setto produce an acute inflammatory response,representing a premonitory readying of the immunesystem in case of possible acute injury during athreatening situation. Acute phase response isactivated by Nor-Epinephrine (NE) and othermediators, of the innate immune system. Multipleinflammatory mediators stored in visceral fat arealso released, including interleukin-6 (IL- 6). C-reactive protein (CRP) and serum amyloid A (SAA)are among the two best-known proinflammatorymediators of the acute phase response,45 whilefibrinogen is an important procoagulant compound.Duringthe stress, a prothrombotic state is deve-loped; a promontory procoagulant state is established

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 225
so as to prevent a possible hemorrhage. Plasminogenactivator inhibitor-1 (PAI-1), is released by visceralfat, in the acute stress response. Insulin is also aproinflammatory compound.7
Insulin Resistance - Acute insulin resistanceis also an intrinsic element of the stress response.Insulin resistance is caused by stress mediators suchas cortisoland cytokines. Ininsulin resistance, insulindependent cells, such as muscle and fat, have lessglucose transferred across their cell membranesaccording to circulating insulin, so that plasmaglucose levels increase. This is beneficial to thecritical cells (brain, immune system and the breast)that do not depend upon insulin for glucose transport.Thus, during various emotional stress and/orinfections, increased glucose need is initiated andsustained in insulin-independent structures of thebrain and immune system.7
Biochemical Pathways in depressionCorticotrophin and Cortisol pathway in
Depression – Corticotropin-releasing hormone(CRH) is responsible for the regulation of ACTHrelease, which is related to the HPA axis andassociated with neurotransmission and autonomic,immunological, neuroendocrine and cardiovascularresponses.46 In anterior pituitary; CRH stimulatesACTH release which acts on the adrenal cortexpromoting the release of cortisol (involved with stressand adrenaline release), estrogen and mineralo-corticoids into the bloodstream. The CRH systemcontributes to the transduction of many of thecomponents of the stress response. Two maincomponents of the CRH system are the amygdalaand hypothalamic CRH systems. The amygdalaCRH system is largely responsible for the activationof anxiety and fear related behaviors and CRHantagonists block fear conditioning. The hypo-thalamic CRH system is responsible for theregulation of the HPA axis and contributes to theactivation of the LC-NE system. The hypothalamicCRH systems consist of three descending pathwaysas depicted in Figure 1. The pathophysiology ofstress is similar to that of major depression, wherein both cases there is decreased appetite, sleepdisturbances and hypervigilance. Reduced libido andpsychomotor changes in depression are associatedwith the release of CRH. MDD is associated withabnormal release of CRH and deregulation of the
HPA axis, consequently, increased release of ACTH,in addition to excessive secretion of cortisol(hypercortisolemia).47
Fig. 1: Descending pathways of CRH system
Locus Ceruleus-Norepinephrine (LC-NE)Systems -The LC-NE system is a general alarmsystem for the brain and increases the signal-to-noise ratio in key areas that regulate the stressresponse. It has many effects similar to those ofCRH system, such as the intense arousal, inhibitionof neurovegetative functions, and it reciprocallyactivates the amygdala and hypothalamic CRHsystems. The amygdala CRH system also contri-butes to the activation of the hypothalamic CRHsystem and the LC-NE system.7
The kynurenine pathway - Hyperactivity ofthe HPA axis and dysregulation of the immunesystem are the source of irregularities in the activityof the kynurenine pathway (transform tryptophaninto two essential compounds engaged in moodregulation, i.e., serotonin and melatonin).48 Basedon the kynurenine pathway hypothesis of depressionetiology, inflammatory factors cause excessiveactivation of indoleamine-2,3-dioxygenase (IDO), anenzyme present in microglia, astrocytes andneurons.49 This enzyme catabolizes tryptophan, intokynurenine (KYN) which is then converted toneurotoxic quinolinic acid in the brain, whichincreases the risk of neurodegenerative processes.In this way, IDO reduces the amount of tryptophanavailable for the production of serotonin,49 which isdirectly linked with the etiology of depression.Quinolinic acid binds to N-methyl D-aspartate(NMDA) receptors. Thus, because of the pro-inflammatory cytokines inducing IDO, depressionmay develop as a result of the decrease in serotoninlevels due to reduced tryptophan on the one handand glutamatergic neurotoxicity on the other as

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society226
shown in Figure 2. through some regions of the blood-brain barrier orby the active reuptake mechanism and also affectbehavioral responses.51 It is suggested thatinflammatory variables may lead to depression by(i) affecting neurotransmitters, (ii) decreasingserotonin and inducing glutamate toxicity bystimulating IDO in glial cells, (iii) suppressingneurogenesis by decreasing BDNF activity, or (iv)increasing HPA axis activity.50,51,52 Stress andinflammatory cytokine activation have beenreported to adversely affect neurogenesis andneuroplasticity.53,54 Cytokines such as TNF andIL-6 exert a direct suppressive effect onhippocampal neurogenesis.55,56 Increased levels ofcytokines stimulate the HPA axis. The effect ofcytokines on the HPA axis may be through directthrough stimulation of the CRH or through alteringthe GR expression to induce GR resistance.57 Mostchanges in depression are found in proinflammatorycytokines such as IL-1, IL-6 and TNF, and C -reactive protein (CRP).58 It has been reported thatserum levels of IL-1, IL-6, and TNF and themessenger ribonucleic acid (mRNA) expressionsof these in peripheral cells are increased in patientswith MDD.59,60
Neurotransmitter systems - The disturbanceof the three mono-amine neurotransmitter systems,serotonin (5-HT), NE, and dopamine (DA) systemsmay be present in diverse neural circuits in differentbrain regions. Also, the disturbance of thesemonoamine neurotransmitters may even affect thefunction of their receptors and the downstreamreceptors.
5-HT (Serotonin) system - The reduction andexcess of 5-HT in the brain may play an importantrole in the regulation of the emotional condition ofthe disease. Disturbances in the synthesis, release,transport, and retake of 5-HT may aggravatedepression. It is found that reserpine interferes withsynaptic vesicle of serotonin, it depletes brain storesof 5-HT, and increases the urine concentrations of5-HT major metabolite 5-hydroxyindoleacetic acid(5-HIAA), therefore producing depression inhumans.61 These findings support that 5-HT systemsare a biochemical basis for MDD. 5-HT deficiencyin the brain may augment negative emotions inMDD, including depressive mood, self-accusationand criticism, disgust, fear, anxiety, aggression,irritability and loneliness. Previous studies found that
Fig. 2: Biochemistry of Depression
Enzymes of inflammation - ManganeseSuperoxide Dismutase (MnSOD), Myeloperoxidase(MPO), and inducible Nitric Oxide superoxidesynthase (iNOS) are among most popular enzymesof inflammation which take part in the etiology ofrecurrent depressive disorders (RDD). Theseenzymes actively engage in the production of freeradicals, as well as damaging proteins, fatty acidsand cellular DNA leading to brain damage throughneurogenesis weakening as well as amplification ofneurodegenerative processes.
Cytokines and inflammatory markers - Theneuroendocrine and immune systems play animportant role in stress response. Therefore,inflammatory markers have been extensivelyinvestigated in stress-related disorders anddepression. Inflammatory mediators have beenfound to affect many factors (monoamine andglutamate neurotransmission, glucocorticoidreceptors (GRs) resistance, and hippocampalneurogenesis) that are thought to be important inthe etiopathogenesis of MDD. This suggests thatinflammatory markers may be used as a marker forthe diagnosis and treatment response of depression.Cytokines are members of the interleukin (IL) family.They are produced by macrophages, natural killercells, and T lymphocytes. Cytokines are classifiedas pro-inflammatory or anti-inflammatory. IL-1, IL-6, and tumor necrosis factor (TNF) are knownas pro-inflammatory cytokines, and IL-4, IL-10, andIL-13 are known as anti-inflammatory cytokines.50
Cytokines play a role in the maintenance of normalbrain function and development by supportingneuronal integrity, neurogenesis, and synapticremodeling. It has been reported that the cytokinesreleased by peripheral immune cells and adiposetissue enter the central nervous system (CNS)

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 227
serum 5-HT concentrations in patients with MDDwere significantly lower than those in healthycontrols.62,63 Long-term reduction of serotoninsynthesis may contribute to high susceptibility ofMDD. 5-HT produces its physiological functionsthrough the binding and interaction with multiple 5-HT receptors. Seven families of 5-HT receptors,including 5-HT1 to 5-HT7 receptors with theirsubtypes, have been identified.64,65 Numerous studieshave found that abnormalities of 5-HT1 (5-HT1A,5-HT1D) and 5-HT2 (5-HT2A, 5-HT2C) receptorsin the CNS may be responsible for the manifestationof MDD. Postmortem and neuroimaging studiesinformed that patients with MDD exhibited elevateddensity and/or activity of 5-HT1A auto receptorscompared with healthy controls.66,67 Studies haveproven sensitivity of postsynaptic 5-HT1D receptorsand a distinctly higher distribution of 5-HT1Dreceptors in the globus pallidus in patients with MDDand/or suicide victims.68,69 A meta-analysis reportedreduction in 5-HT1A receptor binding in the insula,raphe nuclei, hippocampus, occipital cortex, andanterior cingulate cortex in patients with MDD.70
NE (Norepinephrine) system - Precursors oftyrosine and NE ingest NE into the noradrenergicnerve endings by tyrosine transporters. In 1979, Ziset al proposed that depressive symptoms werecaused by the decrease of NE in the CNS.71 NEreduction in the CNS is associated with reductionof positive emotions in patients with MDD,(decrease in pleasure, interest, happiness, alertness,energy and loss of confidence). On the contrary,the symptoms of anxiety were assumed to be causedby hyperactivity of NE in theCNS. During stress,CRH can activate the NE pathway in the locuscoeruleus-temporal hippocampal area, whichreleases NE and induces alertness and anxietysymptoms.72
DA (Dopamine) system - DA is a neurotrans-mitter in the hypothalamus and pituitary which is akey neurobiological substrate for reward, concen-tration, motivation, psychomotor speed, and theability to experience pleasure, and also play a rolein the modification of emotional behavior. 64
Dopamine activity has been verified to be involvedin depressive73 or anxious processes. A study haslinked reward-related, motivated behaviors with themesolimbic DA system.74 Injuries of these functionsare all well-known characteristics of MDD.
Immediate bidirectional control (inhibition orexcitation) of specified midbrain DA neuronsmodifies multiple independent depressive symptoms.This process affects depressive symptoms whichfurther alter the DA neural encoding of action inthe limbic circuits. Moreover, poor functioning ofDA neurons may cause depressive symptoms.Patients of MDD were found with lower level ofDA metabolites in the CSF compared with healthycontrols.75 Deficiency in DA receptor functions maylead to the failure in inhibition from the prefrontalcortex to the amygdala, and induce over excitabilityof the amygdala, resulting in induction of fear andanxiety behavior.
Circuits between 5-HT, NE and DA - TheNE and 5-HT neurotransmitter systems are mutuallyconnected in the CNS. NE plays a role in theregulation of the release of 5-HT. Stimulation of the2 receptor on the axon terminals can inhibit therelease of 5-HT, and that of 1 receptors on neuronalcell bodies or dendrites may cause positive feedbackon the release of 5-HT. 5-HT systems also can exertnegative influence on NE systems and DA systemthrough the 5-HT2A and 5-HT2C receptor-mediated mechanisms.76 Both NE and 5-HT nervefibers project signaling in the frontal cortex andhippocampus, this results in an important regulatoryrole in cognition and behaviors, especially in mentaland emotional regulation in the CNS.77 There aremultiple interactions between the 5-HT and DAsystems. Increased or reduced neurotransmissionof serotonergic or noradrenergic systems can affectdopamine function and induce similar changes indopamine signaling. Acute stimulation of the basal5-HT2A receptor in the basal area may inhibit DAfunction and causes acute motor changes and, inthe midbrain, may inhibit DA activity, causing lossof libido.
ConclusionThe present review succeeded to achieve its
targets regarding major depressive disorders[MDD].1. Neuroimaging data suggested vital information
regarding pre and post treatments of depression,anatomical picture of depression is clear.
2. Physiological pathways of depression arenoticeable on its hormonal disbalances of HPAaxis.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society228
3. Serotonin-kynurenine hypothesis of depressionhas improved our understanding of pathogenesisof depression and of possible links betweendepression and medical conditions associatedwith chronic inflammation.
4. KYN pathway of tryptophan metabolism couldbe measured as a new target for prevention andtreatment of depression.
5. Cytokines, are strong potentials both in termsof being markers of depression and in providingimportant information about the etiology ofMDD. DA, NE and 5-HT systems are clear ontheir grounds. More researches are required fordifferentiating MDD and set of biochemicalmarkers, which probably could constitute anefficient panel for supporting the diagnosis andprognosis of the same.
References1. Preamble to the Constitution of WHO as adopted
by the International Health Conference, NewYork, 19 June - 22 July 1946; signed on 22 July1946 by the representatives of 61 States(Official Records of WHO, No. 2, 100) andentered into force on 7 April 1948.
2. Murthy RS. National mental health survey ofIndia 2015–2016. Indian J Psychiatry 2017; 59: 1.
3. World Health Organization. The world healthreport 2001 — Mental health: newunderstanding, new hope. Geneva: World HealthOrganization 2001.
4. de Souza Duarte N, de Almeida LM, AssuncaoLR, et al. Relation between Depression andHormonal Dysregulation. Open J Depression2017; 6 : 69-78.
5. Bhowmik D, Sampath KP, Srivastava S, et. al.Depression - Symptoms, Causes, Medicationsand Therapies. Pharma Innovation 2012; 1(3) :37-51.
6. Gold PW, Goodwin FK, Chrousos GP. Clinicaland biochemical manifestations of depression.Relation to the neurobiology of stress. New EnglJ Med 1988; 319(6) : 348–353.
7. Gold PW, Vieira RM, Pavlatou MG. Clinical andBiochemical Manifestations of Depression:Relation to the Neurobiology of Stress. NeuralPlasticity. [Internet]. 2015 [cited 30 apr 2019].https:// doi.org/10.1155/2015/581976 PMID:
258789038. American Psychiatric Association, Diagnostic
and Statistical Manual of Mental Disorders:DSM-IV-TR, APA Press 2000.
9. Gold PW, Chrousos GP. Organization of thestress system and its dysregulation inmelancholic and atypical depression: high vs lowCRH/NE states. Mol Psychiatry 2002; 7( 3) :254–275.
10. Chrousos GP, Gold PW. The concepts of stressand stress system disorders: overview ofphysical and behavioural homeostasis. JAMA1992; 267(9) : 1244-1252.
11. Gold PW, Goodwin FK,Chrousos GP. Clinicaland biochemical manifestations of depression.Relation to the neurobiology of stress. N EnglJ Med 1988; 319(6) : 348-353.
12. Gold PW, Goodwin FW, Chrousos GP. Clinicaland biochemical manifestations of depression.Relation to the neurobiology of stress (2). NEngl J Med 1988; 319(7) : 413-20.
13. Anda R, Williamson D, Jones D, et al.Depressed affect, hopelessness, and the risk ofischemic heart disease in a cohort of U.S.adults. Epidemiology 1993; 4(4) : 285–294.
14. Barefoot JC, Schroll M. Symptoms ofdepression, acute myocardial infarction, and totalmortality in a community sample. Circulation1996; 93(11) : 1976–1980.
15. Penninx BWJH,Guralnik JM, Mendes de LeonCF, et al, Cardiovascular events and mortalityin newly and chronically depressed persons >70 years of age. Am J Cardiology 1998; 81(8): 988–994.
16. Penninx BWJH, Geerlings SW, Deeg DJH, etal Minor and major depression and the risk ofdeath in older persons. Arch GenPsychiatry 1999; 56(10) : 889-895.
17. Shapiro PA, Lidagoster L, Glassman AH.Depression and heart disease. Psychiatr Ann1997; 27(5) : 347–352.
18. Langreth Robert (2010-01-05). StudyUndermines Case for Antidepressants. Forbes.Retrieved 2010-07-02.
19. Lund C, Breen A, Flisher AJ, et al. Poverty andcommon mental disorders in low and middleincome countries: A systematic review. Soc SciMed 1982; 71(3) : 517-528.
20. Palmer B, Gates J, Lader M. Causes and

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 229
Management of Hyponatremia. AnnPharmacotherapy 2003; 37(11) : 1694–702.
21. Guaiana G, Barbui C, Hotopf M. Amitriptylinefor depression. Cochrane Database Syst Review2007; 18(3) : 11–7.
22. Anderson IM. Selective serotonin reuptakeinhibitors versus tricyclic antidepressants: Ameta-analysis of efficacy and tolerability. JAffect Disord 2000; 58(1) : 19–36.
23. Fava M,Cassano P. Mood disorders: Majordepressive disorder and dysthymic disorder. In:Stern TA, Rosenbaum JF, Fava M, BiedermanJ, Rauch SL, eds. Massachusette GeneralHospital Comprehensive Clinical Psychiatry. 1sted. Philadelphia, Pa: Mosby Elsevier, 2008.
24. American Psychiatric Association. Practiceguidelines for the treatment of patients withmajor depressive disorder. 2nd ed. September2007.
25. Little A. Treatment-resistant depression. AmFam Physician 2009; 80 : 167-172.
26. Patel V, Pereira J, Mann AH. Somatic andpsychological models of common mentaldisorder in primary care in India. Psychol Med1998; 28 : 135-14.
27. Murray D, Cox JL. Screening for depressionduring pregnancy with the EdinburghDepression Scale. J Reproduction InfantPsychol 1990; 8 : 99-107.
28. Wise T, CleareAJ, Herane A, et al. Diagnosticand therapeutic utility of neuroimaging indepression: an overview. Neuropsychiatr DisTreat 2014; 10 : 1509–1522.
29. Dunlop BW, Mayberg HS. Neuroimaging-basedbiomarkers for treatment selection in majordepressive disorder. Dialogues Clin Neurosci2014; 16 : 479–490.
30. Lener MS, Iosifescu DV. In pursuit ofneuroimaging biomarkers to guide treatmentselection in major depressive disorder: a reviewof the literature. Ann NY Acad Sci 2015; 1344: 50–65.
31. Cole J, Costafreda SG, McGuffin P, et. al.Hippocampal atrophy in first episode depression:a meta-analysis of magnetic resonance imagingstudies. J Affect Disord 2011; 134 : 483–487.
32. Arnone D, McKie S, Elliott R, et al. State-dependent changes in hippocampal grey matterin depression. Mol Psychiatry 2013; 18 : 1265–
1272.33. Tendolkar I, Vanbeek M, Van oostrom I, et. al.
Electroconvulsive therapy increaseshippocampal and amygdala volume in therapyrefractory depression: a longitudinal pilot study.Psychiatry Res 2013; 214 : 197–203.
34. Phillips ML, Chase HW, Sheline YI, et al.Identifying predictors, moderators, andmediators of antidepressant response in majordepressive disorder: neuroimaging approaches.Am J Psychiatry 2015; 172 : 124–138.
35. Echelle M, Kula MA, MT Turan, Reyhanc M,Hold on, Gonul AS, M. Baþtürk unipolar andbipolar depression changes in regional cerebralkanakým patients: a study of Tc-HMPAO 99M.Psychiatry, Psychology Psychopharmacology(3P) Journal 2001; 9 : 369–376.
36. Arnone D, McKie S, Elliott R, Thomas EJ, etal. Increased amygdala responses to sad butnot fearful faces in major depression: relationto mood state and pharmacological treatment.Am J Psychiatry 2012; 169 : 841–850.
37. Fales CL, Barch DM, Rundle MM, et al.Altered emotional interference processing inaffective and cognitive-control brain circuitryin major depression. Biol Psychiatry 2008; 63 :377–384.
38. Ruhe HG, Booij J, Veltman DJ, Michel MC,Schene AH. Successful pharmacologictreatment of major depressive disorderattenuates amygdale activation to negative facialexpressions: a functional magnetic resonanceimaging study. J Clin Psychiatry 2012; 73 : 451–459.
39. Mayberg HS. Modulating limbic-cortical circuitsin depression: targets of antidepressanttreatments. Semin Clin Neuropsychiatry 2002;7 : 255–268.
40. Ga³ecki P, Talarowska M. Inflammatory theoryof depression. Psychiatr Pol 2018; 52(3) : 437–447.
41. Hansson PB, Murison R, Lund A, Hammar Å.Cognitive functioning and cortisol profiles in firstepisode major depression. Scand J Psychol2015; 56(4) : 379–383.
42. Milne AM, MacQueen GM, Hall GB. Abnormalhippocampal activation in patients with extensivehistory of major depression: An fMRI study. JPsychiatry Neurosci 2012; 37(1) : 28–36.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society230
43. Stewart JG, Mazurka R, Bond L, Wynne-Edwards KE, Harkness KL. Rumination andimpaired cortisol recovery following a socialstressor in adolescent depression. J AbnormChild Psychol 2013; 41(7) : 1015–1026.
44. L. Cahill, RJ. Haier, J. Fallon et al. Amygdalaactivity at encoding correlated with long-term,free recall of emotional information. Proc NatlAcad Sci (USA) 1996; 93(15) : 8016–8021.
45. M.A. Kling, S. Alesci G. Csako et. al. Sustainedlow-grade pro-inflammatory state inunmedicated, remitted women with majordepressive disorder as evidenced by elevatedserum levels of the acute phase protein C-reactive protein and serum amyloid A. BiolPsychiatry 2007; 62(4) : 309–313.
46. GRAEFF, Frederico G. Anxiety, panic and thehypothalamic-pituitary-adrenal axis. Rev. Bras.Psiquiatr. [online] 2007; 29 (suppl 1) [cited 2019-04-30], pp.s3-s6. Available from: <http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-44462007000500002&lng=en&nrm=iso>.ISSN15164446. http://dx.doi.org/10.1590/S1516-44462007000500002.
47. Juruena M, Claire A, Pariante C. The Hypo-thalamic-Pituitary-Adrenal Axis, the Role ofGlucocorticoid Receptors and Their Importancein Depression. Brazilian J Psychiatry 2004;26(3) : 189-201.
48. Kanchanatawan B, Sirivichayakul S, Thika S,Ruxrungtham K, Carvalho AF, Geffard M etal. Physio-somatic symptoms in schizophrenia:Association with depression, anxiety,neurocognitive deficits and the tryptophancatabolite pathway. Metab Brain Dis 2017;32(4):1003-1016 Doi: 10.1007/s11011-017-9982-7. [Epub 2017 march 3].
49. Anderson G. Editorial: The kynurenine andmelatonergic pathways in psychiatric and CNSdisorders. Curr Pharm Des 2016; 22(8) : 947–948.
50. Han QQ, Yu J. Inflammation: a mechanism ofdepression? Neurosci Bull 2014; 30 : 515–523.
51. Felger JC, Lotrich FE. Inflammatory cytokinesin depression: neurobiological mechanisms andtherapeutic implications. Neuroscience 2013;246 : 199–229.
52. Young JJ, Bruno D, Pomara N. A review of therelationship between proinflammatory cytokines
and major depressive disorder. J Affect Disord2014; 169 : 15–20.
53. Peng CH, Chiou SH, Chen SJ, Chou YC, KuHH, Cheng CK, Yen CJ, Tsai TH, Chang YL,Kao CL. Neuroprotection by Imipramine againstlipopolysaccharide induced apoptosis inhippocampus-derived neural stem cellsmediated by activation of BDNF and the MAPKpathway. Eur Neuropsychopharmacol 2008; 18: 128–140.
54. Koo JW, Russo SJ, Ferguson D, Nestler EJ,Duman RS. Nuclear factor-kappa B is a criticalmediator of stress-impaired neurogenesis anddepressive behavior. Proc Natl Acad Sci U S A2010; 107 : 2669–2674.
55. Iosif RE, Ekdahl CT, Ahlenius H, Pronk CJ,Bonde S, Kokaia Z, Jacobsen SE, Lindvall O.Tumor necrosis factor receptor 1 is a negativeregulator of progenitor proliferation in adulthippocampal neurogenesis. J Neurosci 2006; 26: 9703–9712.
56. Monje ML, Toda H, Palmer TD. Inflammatoryblockade restores adult hippocampal neuro-genesis. Science 2003; 302 : 1760–1765.
57. Pace TW, Hu F, Miller AH. Cytokine-effectson glucocorticoid receptor function: relevanceto glucocorticoid resistance and thepathophysiology and treatment of majordepression. Brain Behav Immun 2007; 21 : 9–19.
58. Valkanova V, Ebmeier KP, Allan CL. CRP, IL-6 and depression: a systematic review andmeta-analysis of longitudinal studies. J AffectDisord 2013; 150 : 736–744.
59. Kahl KG, Bens S, Ziegler K, Rudolf S, DibbeltL, Kordon A, Schweiger U. Cortisol, thecortisol-dehydroepiandrosterone ratio, and pro-inflammatory cytokines in patients with currentmajor depressive disorder comorbid withborderline personality disorder. Biol Psychiatry2006; 59 : 667–671.
60. Cattaneo A, Gennarelli M, Uher R, Breen G,Farmer A, Aitchison KJ, Craig IW, Anacker C,Zunsztain PA, McGuffin P, Pariante CM.Candidate genes expression profile associatedwith antidepressants response in the GENDEPstudy: differentiating between baseline‘predictors’ and longitudinal ‘targets’.Neuropsychopharmacology 2013; 38 : 377–385.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 231
61. Shore PA, Silver SL, Brodie BB. Interaction ofreserpine, serotonin, and lysergic aciddiethylamide in brain. Science 1955; 122 : 284–285. doi:10.1126/science.122.3163.284-a
62. Bot M, Chan MK, Jansen R, Lamers F,Vogelzangs N, Steiner J, et al. Serum proteomicprofiling of major depressive disorder. TranslPsychiatry 5:e599.2015. doi: 10.1038/tp.2015.88
63. Phillips C. Physical activity modulates commonneuroplasticity substrates in major depressiveand bipolar disorder. Neural Plast 2017. 7014146.doi:10.1155/2017/7014146
64. Hoyer D, Clarke DE, Fozard JR, Hartig PR,Martin GR, Mylecharane EJ, et al. InternationalUnion of Pharmacology classification ofreceptors for 5-hydroxytryptamine (Serotonin).Pharmacol Rev 1994; 46 : 157–203.
65. Barnes NM, Sharp T. A review of central 5-HT receptors and their function. Neuropharma-cology 1999; 38 : 1083–1152.
66. Boldrini M, Underwood MD, Mann JJ, ArangoV. Serotonin-1A autoreceptor binding in thedorsal raphe nucleus of depressed suicides. JPsychiatr Res 2008; 42 : 433–442.
67. Andrade R, Huereca D, Lyons JG, Andrade EM,Mcgregor KM. 5-HT1A receptor-mediatedautoinhibition and the control of serotonergic cellfiring. ACS Chem Neurosci 6, 1110–1115.2015.
68. Lowther S, Katona CL, Crompton MR, HortonRW. 5-HT1D and 5-HT1E/1F binding sites indepressed suicides: increased 5-HT1D bindingin Globus pallidus but not cortex. Mol Psychiatry1997; 2 : 314–321.
69. Whale R, Clifford EM, Bhagwagar Z, CowenPJ. Decreased sensitivity of 5-HT(1D)receptors in melancholic depression. Br JPsychiatry 2001; 178 : 454–457.
70. Wang L, Zhou C, Zhu D, Wang X, Fang L,Zhong J, et al. Serotonin-1 A receptor alterationsin depression: a meta-analysis of molecularimaging studies. BMC Psychiatry 2016;16:319.doi: 10.1186/s12888-016-1025-0
71. Zis AP, Goodwin FK. Novel antidepressants andthe biogenic amine hypothesis of depression.The case for iprindole and mianserin. Arch GenPsychiatry 1979; 36 : 1097–1107.
72. Muntner IBN. Stahl’s essential psychopharma-cology. Mens Sana Monogr 2010; 8 : 417.
73. Ryan JP, Sheu LK, Critchley HD, Gianaros PJ.A neural circuitry linking insulin resistance todepressed mood. Psychosom Med 2012; 74 :476–482.
74. Cabib S, Puglisi-Allegra, S. Stress, depressionand the mesolimbic dopamine system.Psycho-pharmacology 1996; 128 : 331342.
75. Jokinen J, Nordström AL, Nordström P. Therelationship between CSF HVA/5-HIAA ratioand suicide intent in suicide attempters. ArchSuicide Res 2007; 11 : 187–192.
76. Clausius N, Born C, Grunze H. The relevanceof dopamine agonists in the treatment ofdepression. Neuropsychiatrie 2009; 23 : 15–25.
77. Graeff FG, Guimarães FS, De Andrade TG,Deakin JF. Role of 5-HT in stress, anxiety, anddepression. Pharmacol Biochem Behav 1996;54 : 129–141.1996.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society232
A Study to Assess the Magnitude of Various MinorPhysical Anomalies in Schizophrenia and to
compare them between Schizophrenic Patients andtheir First-degree Relatives
1Abhinav Pandey, 2Haseeb Khan, 3D.M.S. RathoreDepartment of Psychiatry, 1,2 Hind Institute of Medical Sciences. Safedabad, Barabanki, U.P. and
3IMHH Agra, U.P. IndiaContact: Haseeb Khan, E-mail: [email protected]
Original Article
IntroductionMinor Physical Anomalies (MPA) are mild,
clinically and cosmetically insignificant errors ofmorphogenesis which have a prenatal origin and maybear major informational value for diagnostic,prognostic and epidemiological purposes.1
MPAs are subtle morphologic signs that are oflittle or no consequence but which represent fixedmarkers of gestational developmental abnormality.
MPAs evolved into a construct of interest toschizophrenia researchers as well as those studyinga variety of other neurodevelopmental andbehavioral disorders, including but not limited toattentional disorders, autism, fetal alcohol syndrome,learning disabilities, and sensory impairments.
The presence of MPAs is a sensitive physicalindicator of embryonic development and serves asindicators of altered morphogenesis that occurred
Abstract
Introduction: Minor Physical Anomalies(MPA) are mild, clinically and cosmeticallyinsignificant errors of morphogenesis which have a prenatal origin and may bear majorinformational value for diagnostic, prognostic and epidemiological purposes. Materialand methods: It was a cross-sectional comparative hospital based study. The subjectswere recruited for the study by the purposive sampling technique.The study was conductedat the Institute of mental health and hospital Mathura Road Agra.The study sample consistedof 20 schizophrenia patients diagnosed as per ICD-10 DCR (WHO, 1992) criteria, 20first degree relatives, one for each patient. Total sample size is 40. Results: It is observedthat in schizophrenic patients’ maximum anomalies were present in eyes (0.55 ± 0.88),mouth (0.45 ± 0.60) followed by anomalies of head (0.35 ± 0.81), feet (0.30 ± 0.47) andear (0.20 ± 0.52). The lowest anomalies were present in hand region (0.05 ± 0.22). It isobserved that in schizophrenic FDRs maximum anomalies were present in eyes (0.40 ±0.52) feet (0.20 ± 0.52) and ear (0.10 ± 0.30) and then equal anomalies in head and hand(0.05 ± 0.22). High Waldrop mean score of mouth in schizophrenics (0.45) compared totheir FDRs(0.00) is statistically significant. Conclusion: It seems worthwhile to combinemultiple markers of abnormal neurodevelopment to answer such questions. Future studiesshould be carried out on a larger sample size with equal socio-demographic representationsincluding female population to enhance the significance.
Keywords: Minor Physical Anomalies, Schizophrenia, PANSS scale, Waldrop scale.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 233
early in gestation.2 These may be minor abnormalitiesof the head, feet, hands, and face (e.g., high-steepledpalate, large or small distance between tear ducts).As both skin and central nervous system developfrom the same ectodermal tissue in utero, MPAsmay be external markers of abnormal braindevelopment. High rates of MPAs are associatedwith disorders that have known prenatal CNSinvolvement, such as down’s syndrome.3 Hence,MPAs are believed to reflect some event related toCNS development.
Minor Physical Anomalies (MPA) has beenreported to be more frequent in persons withschizophrenia.4 The Waldrop scores were higher inpatients (48%) followed by relatives (28%) andcontrols (10%), with more anomalies in the head,eyes, ears, and feet.5 It is not yet clear whetherMPAs are specific for schizophrenia or they holdground for psychosis in general. Another funda-mental question is whether MPAs reflect somegenetic vulnerability or any defect in embryogenesisbecause studies with siblings of these groups ofpatients did not come out with any definitivestatement.
To the best of one’s knowledge, previous studieshave only looked for frequency of minor physicalanomalies in schizophrenia but have not exploredthe socio-demographic correlates or the possiblerelationship with symptom severity, neither have theyattempted to assess the first degree relatives of thepatients thus providing and insight into the geneticbasis of MPAs.
The present study aims at evaluating thecomparison between prevalence of minor physicalanomalies in patients diagnosed with schizophreniaand their first degree relatives thus attempting toexplore the relevance of neurodevelopmentalhypothesis regarding schizophrenia.
Material and MethodsStudy design: It was a cross-sectional compa-
rative hospital based study. The subjects wererecruited for the study by the purposive samplingtechnique.
Study place and population:The study wasconducted at the Institute of mental health andhospital Mathura Road, Agra. It is a tertiary referralcenter with bed strength of 800, and a postgraduateteaching hospital, which imparts training in
psychiatry, clinical psychology, psychiatric socialwork and psychiatric nursing. The hospital has awide catchments area which includes the states ofUttar Pradesh, Madhya Pradesh, Rajasthan,Haryana andUttarakhand admitted as inpatients anddiagnosed with schizophrenia.
Study period: Data was collected over a periodof 12 months from 15th march 2009-15th March2010.
Sample sizeThe study sample consisted of 20 schizophrenia
patients diagnosed as per ICD-10 DCR (WHO,1992)4 criteria, 20 first degree relatives, one for eachpatient. Total sample size is 40.
Inclusion criteriaPatients
1. Inpatients/ Outpatients, male, 18-50 yearsof age.
2. Diagnosis of Schizophrenia according toICD10.6
3. At least two episodes of illness includingthe present episode.
4. Patients accompanied by first degreerelatives.
5. Only those patients were included in thestudy who gave informed consent.
First Degree RelativesIf more than one FDR are available, then the
one nearer to patient by age would be taken up forstudy. Preference – sibling > son > father
Exclusion criteriaPatients
1. History of head trauma, major neurologicaldisorder, or seizure disorder.
2. Psychoactive substance dependence(except nicotine).
3. Mental retardation.
First Degree RelativesHistory suggestive of1. Psychotic or affective disorder,2. Head trauma,3. Major neurological disorder or4. Seizure disorder.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society234
Procedure: After obtaining informed consent,all the patients, their first degree relatives (FDRs)meeting their respective exclusion and inclusioncriteria were taken up for the study. Detailed datawas collected on the sociodemographic and clinicaldata sheet designed for the purpose. All patientsand their respective FDRs were assessed for minorphysical anomalies with the Waldrop scale andforschizophrenia PANSS scale was used.
Positive and negative symptoms of schizo-phrenia7
The tools used for schizophrenia in this studywere PANSS (Positive and negative symptoms ofschizophrenia). The PANSS is a widely usedresearch tool to measure psychopathology inschizophrenia. It is a 30 item, seven point (1-7, fromabsent to extremely severe) scale, rated with thehelp of a semi-structured interview. It has threesubscales to measure specifically (1) the severityof the positive (7-items) symptoms, (2) the severityof the negative (7 items) symptoms and (3) evaluatessymptoms, which cannot be linked decisively toeither the positive or negative syndrome (16 items).composite scale. The difference between positiveand negative scores indicates whether positive ornegative symptoms prevail.Waldrop scale8
The scale used to assess minor physicalanomalies is the Waldrop scale used in majority ofthe earlier studies. It is a simple 5-10-minuteexamination for the assessment of 17 anomalousfeatures and therefore provides an opportunity formuch more extensive assessment of minor physicalanomalies. Seventeen morphological abnormalitieswere assessed in six body regions: head, eyes, ears,mouth, hands, and feet. Most of the abnormalitieswere scored qualitatively as present (1) or absent(0).General Health Questionnaire (GHQ12)9
The GHQ is a good screening instrument forpsychiatric illnesses. The original version consistedof 140 items which was later reduced to brieferversions. The one consisting of 12 items has beenused widely and effectively to screen out psychiatricillnesses. It is a self-reported scale. To screen anypsychiatric morbidity in normal controls, GeneralHealth Questionnaire-12 was administered.
Analysis of dataData was analyzed using standard statistical
software package, SPSS 10.1. Descriptive statisticsand inferential statistics, such as students ‘t’ test,independent t test was used. The level of significance(alpha) of 0.05 and 0.01 were adopted in the study.Chi-square test was used to ascertain groupdifference between categorical variables, students‘t’ test was used in case of determining groupdifference of dimensional variables.
ResultsPresent study includes 20 schizophrenia patients
and 20 their first degree relatives.Schizophreniapatients had a mean age of 30.45 ± 1.58 their firstdegree relatives had a mean age of 38.53 years (±14.99).
Table-1: Mean and S.D. of Various MinorPhysical Anomalies (MPA) Across Group
Schizophrenia Schizophrenia FDR
MPA Head 0.35 ± 0.81 0.05 ± 0.22MPA Eye 0.55 ± 0.88 0.40 ± 0.82MPA Ear 0.20 ± 0.52 0.10 ± 0.30MPA Mouth 0.45 ± 0.60 0.00 ± 0.00MPA Hand 0.05 ± 0.22 0.05 ± 0.22MPA Feet 0.30 ± 0.47 0.20 ± 0.52
Total 1.80 ± 1.64 0.75 ± 0.91
Table 1 depicts the mean scores of variousMPAs in patients of schizophrenia. It is observedthat in schizophrenic patients’ maximum anomalieswere present in eyes (0.55 ± 0.88), mouth (0.45 ±0.60) followed by anomalies of head (0.35 ± 0.81),feet (0.30 ± 0.47) and ear (0.20 ± 0.52). The lowestanomalies were present in hand region (0.05 ± 0.22).It is observed that in schizophrenic FDRs maximumanomalies were present in eyes (0.40 ± 0.52) feet(0.20 ± 0.52) and ear (0.10 ± 0.30) and then equalanomalies in head and hand (0.05 ± 0.22)
Table 2 shows mean, standard deviation and tvalue computed through independent t test showingmore anomalies in head region in schizophrenia(0.35) compared to FDRs of schizophrenia (0.05)though the difference is not large enough to be calledstatically significant, high Waldrop mean scores ofeye region in schizophrenic patients(0.55) comparedto their FDRs(0.40) though not to the level ofstatistical significance.Waldrop score of ear in

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 235
Table-2: Comparison of MPA in schizophrenia and their FDRsComparison of MPA in schizophrenia and their FDRs
MPA Patients and Controls N Mean Std. Deviation t-value
Minor physical anomalies of head Schizophrenia pt 20 .3500 .81273 0.12Walrdrop score Schizophrenia control 20 .0500 .22361Minor physical anomalies of eye Schizophrenia pt 20 .5500 .88704 0.58Walrdrop score Schizophrenia control 20 .4000 .82078Minor physical anomalies of ear Schizophrenia pt 20 .2000 .52315 0.46Walrdrop score Schizophrenia control 20 .1000 .30779Minor physical anomalies of mouth Schizophrenia pt 20 .4500 .60481 0.002**Walrdrop score Schizophrenia control 20 .0000 .00000Minor physical anomalies of hand Schizophrenia pt 20 .0500 .22361 1.00Walrdrop score Schizophrenia control 20 .0500 .22361Minor physical anomalies of feet Schizophrenia pt 20 .3000 .47016 0.529Walrdrop score Schizophrenia control 20 .2000 .52315Minor physical anomalies total Schizophrenia pt 20 1.8000 1.64157 0.017**Walrdrop score Schizophrenia control 20 .7500 .91047
schizophrenic patients (0.20) greater than theirFDRs(0.10). High Waldrop mean score of mouth inschizophrenics (0.45) compared to their FDRs (0.00)which is statistically significant.
DiscussionThe main objective of this study was to deter-
mine the prevalence of minor physical anomalies inschizophrenia and compare the same withprevalence in first degree relatives of the patientsin order to explore whether the neurodevelopmentalhypothesis holds true for schizophrenia. First degreerelatives were included in the study to see if there isany genetic explanation of occurrence of minorphysical anomalies as has been suggested by earlierstudies (Ismail et al, 1998; Gourion et al, 2004).10,11
Our results in schizophrenic patients showmaximum number of anomalies in eye regionfollowed by mouth and hand region similar to studydone by Ismail et al, McGrath et al in (2002).10,12
Our study also reports increased MPAs ofmouth region compared to FDRs in Schizophreniawhich is statically significant. similar to the resultsof past studies who report topographical distributionof MPAs in schizophrenic individuals are highlyvariable, although it is generally held that the greatestnumber of MPAs occur within the oral cavity.13
Importantly, information about which regionsare most susceptible to MPAs can provide clues tothe temporal origins of the dysmorphology and itsunderlying relationship to brain development.
Our results are supported by study of Ismail et
al10 about the frequency of MPAs in schizophrenicpatients and their normal siblings. Patient hadsignificantly more minor physical anomalies thancomparison subjects in all body areas tested andalso more minor physical anomalies than theirsiblings. Siblings had more minor physical anomaliesthan control group. Our study showed higher numberof anomalies in eye, head and mouth similar to Ismailet al study which had increased hand, eye and mouthminor physical anomalies compared to controls.10
Our study is also supported by a recent studyby Trixler et al who suggested that specific anomaliesof the mouth and head may have more relevance toneurodevelopmental abnormalities than does thecumulative prevalence of MPAs. This is alsosupported by hypothesis by MPAs of the craniofacialregion may form concurrently with the in uterostructural brain changes that ultimately areassociated with schizophrenia.14,15
Our study when seen in context of Weinbergerstudy et al posited that information about bodyregions are most susceptible to MPAs in the contextof schizophrenia can provide clues to the temporalorigins of the dysmorphology and its relationship toneurodevelopment.16
Results of our study is also supported by studyof Murphy and Owen, 1996 who found that there isgeneral agreement that schizophrenic cases possessmore MPAs than healthy controls. It is also clear,however, that the magnitude of the disparity in MPAscores between cases and controls varies widelyacross studies.17 Currently, there is no clear explana-

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society236
tion for this outcome variability.Similarly, Green et al18 assessed minor physical
anomalies in schizophrenia and their siblings, andfound significantly more MPAs in schizophrenicpatients than normal controls. In Trixler’s studyschizophrenic group MPAs were significantly higherthan controls while Alexander’s study in1992 didn’tfind any difference.14,18,19
Our study concluded that schizophrenic patientshad significantly more anomalies than their FDRsThese findings seems to support the neurodevelop-mental hypothesis to be true in schizophrenia whichis supported by study of Lohr and Flynn whoassessed using Waldrop Scale that Schizophreniagroup had significantly higher levels of MPA thanthe controls.20
ConclusionAlthough assessment of MPAs offers a conve-
nient way to bridge the gap between the time ofdata collection and the time of interest (prenatal andperinatal), this method offers only sketchy informa-tion regarding the specific time period (e.g., whichmonth of development)involved. It seems worthwhileto combine multiple markers of abnormalneurodevelopment to answer such questions.
There were few limitations of this study as thesample size was modest, which makes it difficult togeneralize the result.The female population wasunder-represented in the study. Similarly there wasno representation of urban population. Future studiesshould be carried out on a larger sample size withequal socio-demographic representations includingfemale population to enhance the significance.
References1. Pinsky L: Informative morphogenesis variants.
Minor congenital anomalies revisited. Iss RevTeratol 1985; 3 : 135-170.
2. Trixler M, Tenyi T, Csabi G, Szabo R: Minorphysical anomalies in schizophrenia and bipolaraffective disorder. Schizophr Res 2001; 52 : 195-201.
3. Krouse JP, Kauffman JM: Minor physicalanomalies in exceptional children: a review andcritique of research. J Ab Child Psychol 1982;10 : 247-264.
4. John JP, Arunachalam V, Ratnam B, Isaac MK:Expanding the schizophrenia phenotype: a
composite evaluation of neurodevelopmentalmarkers. Compr Psychiatry 2008; 49(1) : 78–86.
5. Mulky P, Poornachandrika P, Anandan H.Comparative Study of Minor Physical Anoma-lies in Schizophrenia. Int J Sci Stud 2017; 4(12): 46-49.
6. World Health Organization: The ICD-10 classi-fication of mental and behavioural disorders:diagnostic criteria for research. World HealthOrganization, Geneva, 1992.
7. Opler MG, Yang LH, Caleo S, Alberti P.Statistical validation of the criteria for symptomremission in schizophrenia: preliminaryfindings. BMC Psychiatry 2007; 7 : 35.Published 2007 Jul 24. doi:10.1186/1471-244X-7-35.
8. Waldrop MF, Pedersen FA, Bell RQ: Minorphysical anomalies and behaviorin preschoolchildren. Child Development 1968; 39 : 391-400.
9. Hankins, Matthew. The reliability of the twelve-item general health questionnaire (GHQ-12)under realistic assumptions. BMC Public Health2008; 8. p. 355. ISSN 1471-2458.
10. Ismail B, Cantor-Graae E, McNeil TF: Minorphysical anomalies in schizophrenic patients andtheir siblings. Am J Psychiatry 1998; 155 : 1695–1702.
11. Gourion D, Goldberger C, Bourdel MC, BayleFJ, Loo H, Krebs MO. Minor physical anomaliesin patients with schizophrenia and their parents:prevalence and pattern of craniofacialabnormalities. Psychiatry Res 2004a; 125(1) :21–28.
12. McGrath J, El-Saadi O, Grim V, Cardy S,Chapple B, Chant D, Lieberman D, Mowry B:Minorphysical anomalies and quantitativemeasures of the head and face in patients withpsychosis. Arch Gen Psychiatry 2002; 59 : 458-464.
13. Tarrant CJ, Jones PB. Precursors to schizo-phrenia: do biological markers have specificity?Can J Psychiatry 1999; 44(4) : 335-49.
14. Trixler M, Tenyi T, Csabi G, Szabo R: Minorphysical anomalies in schizophrenia and bipolaraffective disorder. Schizphr Res 2001; 52 : 195-201.
15. Steg J.P., Rapoport J.L. Minor physicalanomalies in normal, neurotic, learning disabled

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 237
and severely disturbed children. J Autism ChildSchizophr 1975; 5 : 299-307.
16. Marenco S, Weinberger DR. The neurodevelop-mental hypothesis of schizophrenia: following atrail of evidence from cradle to grave. DevPsychopathol 2000; 12(3) : 501-27.
17. Murphy KC, Owen M.J. Minor physicalanomalies and their relationship to the aetiologyof schizophrenia. Br J Psychiatry 1996; 168 :139-142.
18. Green MF, Satz P, Christenson B: Minorphysical anomalies in schizophrenia patients,bipolar patients and their siblings. Schizphr Bull1994; 20 : 433-440.
19. Alexander R.C., Reddy R, Mukherjee S. Minorphysical anomalies in schizophrenia. BiologicalPsychiatry, 1992; 31 : 209.
20. Lohr JB. FLynn K. Minor physical anomaliesin schizophrenia and mood disorder. SchizophrBull 1993; 19 : 551-556.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society238
A study of burden of care among mothers ofmentally retarded children and adolescents
attending child and adolescent psychiatry OPD in atertiary care center in North India
Amit Arya,1 Savita Verma,2 Deblina Roy,3 Pawan Kumar Gupta,4 Fauzia Jawaid5
1,3,4Department of Psychiatry, KGMU, Lucknow, U.P., India2 Baba Institute of Nursing, Lucknow
5All India Institute of Medical Sciences, PatnaContact: Pawan Kumar Gupta, E-mail: [email protected]
Original Article
Introdution
Mental retardation (MR) is a developmentaldisability in which the intellectual ability and adaptivebehavior of an individual becomes deficient to a sub-average level. According to this definition, for anindividual to be called mentally retarded, he or shemust fulfill at least the following three character-istics. First, the individual must have below averageintellectual ability i.e. individual’s IQ must be below70 on the standard tests. Secondly, there must be asignificant impairment in the adaptive behavior ofthe individual. The individual must demonstrate an
inability to meet the standard of personal and socialresponsibilities appropriate to his/her age group.Thirdly, these deficiencies in intellectual functioningand adaptive behavior must occur during thedevelopmental period of the individual.1
Recent mental health survey in India showsstate wide prevalence for MR to be 0.5% in UttarPradesh.2 Western studies also shows parentalburden due to disabilities in children.3-4 It has beenseen that a diagnosis of MR in the child brings abouta psychological, financial and social stress amongthe family. It primarily effects the parents of thesechildren. Most of the stress is often borne by the
Abstract
Background: Mothers are the most important caregivers of children. When a child withdisability is born a mother’s responsibilities increase by leaps and bounds. Caring for achild with mental retardation (MR) challenges the role of mother and may lead to excessiveburden of care. Method: A non-experimental descriptive cross sectional assessment ofburden of care among mothers of mentally retarded children and adolescents attendingchild and adolescent psychiatry OPD was done using burden assessment schedule. Resultsand conclusion: The mean age of children with mental retardation was 9.09 ± 3.07 years.The mean age mothers of children with mental retardation was 32.97 ± 6.25 years. Maximumburden of care was found in physical and mental health domains (14.33 ± 2.81) followedbyexternal support domain (10.79± 2.24), taking responsibility (9.3 ± 1.06)and Caregiversroutine (8.77 ± 1.67). In this study, it was found that mother of mentally retarded childrenand adolescent experience burden of care which increases as the financial status of thefamily decreases. The burden of care is higher in severe to profound MR than mild tomoderate MR. The burden of care in the domain of physical and mental health was highest.
KEYWORDS: Mothers, Burden Assessment Schedule, Mental Retardation.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 239
mothers in the family as they are the most importantcaregivers in such families. Burden of care refersto the physical burden and emotional reactions ofcaregivers including the perception of strain, reducedmorale, anxiety and depression. A family who has achild with mental retardation will experience manychallenges such as physical problems, emotionalstress, psychological disturbances, family problems,and additional financial burden.5 Some caregiversadapt well to these situations of caring for a childwith a disability but others may not. The attitudesand emotional reaction of caregivers of disabledchildren are of crucial importance in planning fortheir treatment and rehabilitation. It is found that71% of the mothers felt scared when they realizedthat their child is retarded. Some caregivers do notadmit that they have a child with retardation andkeep the child behind closed doors for fear of criticismfrom others. Lack of understanding about the natureof this condition and stigma associated with it mayworsen caregiver stress.6
Mothers of mentally disabled children undergomore stressful experience than mothers of normallydeveloping children.7 Social problems within thefamily reveal that parental feelings stronglyexpressed anxiety about future effecting the siblingsnegatively, psychological stress of var iouskinds,social isolation of the family and economicburden.8 Parents of children with disabilities facemany stresses like little opportunity to explore theirown needs and depression.9 The quality of life ofthe mothers was found to be below average. It wasseen that the mothers experienced the most difficultyin the domains of perception of inadequacy andemotional burden.10 With the scope of helping themothers cope up with these stressful situations, thereis a dire need for conducting more studies in gaininginsight of their burden as caregivers. The main aimof this study is to assess the burden of care amongmothers of mentally retarded children andadolescents and to find the association betweenburden of care with the severity of MR.
Material and MethodsNon experimental, cross-sectional descriptive
design was used for the present study. The studywas conducted in the Child Psychiatry OPD of thePsychiatry Department of King George’s MedicalUniversity, Lucknow, UP. The study was conducted
from November 2016 till April 2017. The study wasapproved from the institutional ethics committee. Inthis study 74 mothers of children diagnosed withMR as per DSM-IV-TR were screened for theselection criteria. 61 mothers were included in thestudy who brought their children for the variousservices in the department of psychiatry KGMU.13 mothers were excluded and reasons of exclusionwere unwillingness of the mother due to requirementof priority management of their child and presenceof any other member of the family with chronicdisabling illness. Informed consent was taken fromall the study participants. Socio-demographic andclinical details were recorded on semi-structuredproforma. Burden of care was assessed by usingBurden assessment schedule (Thara et al. 1998)5.Descriptive statistics (frequency distribution andpercentage, mean and standard deviation) was usedto analyse the socio-demographic, clinical data.Inferential Statistics t-test, one-way analysis ofvariance were used to find the relationship of burdenof care with selected demographic and clinicalvariables.
ResultsThe mean age of mothers of mentally retarded
children and adolescents was 32.97 ± 6.25 years.Almost half of the mothers belonged to Urban(50.82%) and other half (49.18%) belonged to ruralhouseholds. Majority of the mothers were (70%)were Hindu. 42.62% mothers were illiterate, 40.98%mothers lived in households earning between 5000-10,000/- per month and 32.79% belong to <5000monthly income group. Majority of mothers (65.5%)lived in nuclear families and 72.13% were housewife,and majority (80.33%) were living with their partners(Table-1). The mean age of children with mentalretardation was 9.09 ± 3.07 years.
The burden of care was assessed under 8domains, the burden in the physical and mental healthdomain was found to be highest (14.33 ± 2.81)followed by external support domain (10.79 ± 2.24),taking responsibility (9.3 ± 1.06), caregiver’s routine(8.77 ± 1.67), and patient’s behavior (7.6 ± 1.42).(Table 2).
On comparing the burden of care as per theseverity of mental retardation it was found thatburden was significantly higher in severe MR in theexternal support domain (p value = 0.004) (Table

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society240
Table-1: Socio-demographic profile of mothers n=61
Sl. No. Variables Frequency Percentage %
1 Age (in years) (32.98 ± 6.25)20-30 years 19 31.15%31-40 years 39 63.93%Above 40 years 03 4.92%
2 DomicileUrban 31 50.82%Rural 30 49.18
3 ReligionHindu 43 70%Muslim 18 30%
4 EducationIlliterate (speak and understand Hindi) 26 42.62%Junior high school 15 24.69%High school 06 9.84%Inter mediate 03 4.91%Graduation and above 11 18.03%
5 Type of familyNuclear 40 65.57%Joint 21 34.43%
6 family income<5000 20 32.79%5000-10000 25 40.98%>10000 16 26.23%
7 Total number of family member2 member 01 0.64%3 member 04 6.56%4 member 14 22.95%Above 4 member 42 68.85%
8 OccupationWorking 17 27.87%Housewife 44 72.13%
7 Are you living with your partnerYes 49 80.33%No 12 9.67%
7(a) If no then give reasonSeparated 07 58.33%Divorced 01 8.33%Widow 04 33.33%
Table-2: Distribution of total burden of care on various domains of burden assessmentschedule (n=61)
Sl. no. Subgroup Score range Mean ± SD
1 Physical and mental health 6-18 14.33 ± 2.812 External support 5-15 10.79 ± 2.243 Taking responsibility 4-12 9.3 ± 1.064 Patient’s behavior 3-9 7.6 ± 1.425 Caregivers routine 4-12 8.77 ± 1.676 Caregiver’s strategy 3-9 7.3 ± 1.277 Support of patient 4-12 6.54 ± 1.348 Other relations 4-12 6.23 ± 1.81
3). While in all other domains the difference is notsignificant on the basis of severity. The total burdenscore was also not significantly different.
The burden of care among mothers accordingto family income (Table 4), shows that lower incomegroups has statistically significant higher burden

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 241
Table-3: Domain wise burden of care according to severity of mental retardation (n=61)
Burden of care SeverityMild Moderate Severe & Profound p-value(n=23) (n=20) (n=18)
Physical and mental health 13.61 ± 3.17 14.75 ± 2.27 14.78 ± 2.28 0.30External support 10.26 ± 2.2 12.1 ± 2.22 10 ± 1.68 0.004Caregivers routine 8.57 ± 1.84 8.75 ± 1.37 9.05 ± 1.77 0.65Support of patient 6.26 ± 1.51 6.85 ± 1.35 6.56 ± 1,04 0.36Taking responsibility 9.43 ± 0.95 9.15 ± 1.18 9.33 ± 1.09 0.68Other relations 5.96 ± 1.89 6.1 ± 1.188 6.72 ± 1.60 0.38Patient’s behavior 8,91 ± 2,53 8.85 ± 3.06 9.28 ± 2.21 0.87Caregiver’s strategy 8.17 ± 1.33 8.2 ± 1.06 8.83 ± 1.46 0.21Total adjusted burden score 71.17 ± 11.25 74.75 ± 9.27 74.56 ± 8.21 0.41
(One-way ANOVA). Level of significance p = <0.05
Table-4: Domain wise burden of care according to family income (n=61)
Burden of care Family income< 5000 (n=20) 5000-10000 (n=25) >10000 (n=16) P value
Physical and mental health 14.7 ± 2.43 15.32 ± 2.08 12.31 ± 3.34 0.001External support 11.7 ± 1.87 11.08 ± 2.14 2.07 ± 2.07 0.001Caregivers routine 8.75 ± 1,62 9.44 ± 1.66 7.75 ± 1.24 0.005Support of patient 6.9 ± 1.29 6.76 ± 1.36 5.75 ± 1.07 0.01Taking responsibility 9.3 ± 1.13 9.29 ± 1.08 9.31 ± 1.01 0.10Other relations 6.5 ± 1.96 6.72 ± 1.51 5.13 ± 1.67 0.01Patient’s behaviour 9.8 ± 1.85 9.52 ± 2.69 7.16 ± 2.51 0.003Caregiver’s strategy 8.25 ± 1.16 8.48 ± 1.45 8.38 ± 1.31 0.85Total adjusted burden score 75.9 ± 9.30 76.64 ± 7.56 65 ± 8.97 0.0001
(One way ANOVA). Level of significance p= <0.05
scores in the domains of Physical and mental health(P=0.001), external support (P=0.001), caregiversroutine (P=0.005), Support of patient (P=0.01), otherrelations (P=0.01), patient’s behaviour (P=0.003) andtotal adjusted burden score (P=0.0001).
DiscussionThe present study was done using a cross
sectional research design in the department ofpsychiatry of King George’s Medical University inthe child psychiatry out-patient department. Inmajority of the cases, mothers accompanied theirchildren for diagnosis, treatment and follow up. Inthis study we found that there was moderate tosevere burden among the mothers of mentallyretarded children which was seen in previous studiesas well. Vijesh and Sukuraman11 in their studyrevealed that that mothers who had children withdisabilities had considerable burden of care. SimilarlyGosch8 and Tisbosch9 reported that parents ofchildren with lower levels of cognitive functioning
perceived more burden.On analyzing the burden of care on mothers in
various domain using burden assessment, it wasfound that maximum burden of care was found inphysical and mental health domains (14.33 ± 2.81)followed by external support domain (10.79 ± 2.24),taking responsibility (9.3 ± 1.06) and Caregiversroutine (8.77 ± 1.67). These findings are congruentwith the study by Pal T et al. which shows the highburden in the domain of physical and mental health,external support domain, taking responsibility andCaregivers routine.12 The reasons could be thatthese mothers had to persistently engage with suchchildren ignoring her own care. Mother of thesechildren also has to bear the critical comments andstigma associated with the condition of her childwhich could be the reason for lack of externalsupport and sharing responsibility of the child as wellas caregiving which increases the burden in thesedomains.
The present study shows that there is signifi-

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society242
cantly higher burden in the following domains.Physical and mental health (P=0.001), externalsupport (P=0.001), Caregivers routine (P=0.005),Support of patient (P=0.01), other relations (0.01),Patient’s behavior (0.003) among mother with lowfamily income. Total adjusted burden score was alsosignificantly higher (P=0.0001). (Table 4) Similarlysignificant relationship between the levels of parent’sburdens and their monthly income was reported inprevious study.13 This means that the burdenperceived by caregivers increases as the financialstatus decreases.
In the present study we also found that there isinverse relation of burden with education of mother.This finding is in congruence with studies byMajumdar et al.14 which shows that parentaleducation had an inverse relationship with theburden. It can be elaborated that educatedcaregivers had a chance to clarify their doubts andexpand their horizons with internet, TV, posters, andhandouts. Illiterates lack such exposure. This wasalso emphasized by Narmada et al.15 who mentionedthat educated mothers have good interaction andtolerance towards their child’s behavior, have betterunderstanding of nature of the illness and how tomanage mentally retarded children there byexperience lesser burden.
When we assessed burden of care as per theseverity of MR, it was found that burden was signifi-cantly higher in severe MR in the external supportdomain (p value = 0.004). It can be understood asthe patients having severe disability require morecare. Upadhyay and Havalappanavar16 found thatthe parents of moderately retarded children notedmore of psychological problems than those of mildlyretarded. Sethi also reported parents of childrenwith severe to profound mental perceive moreburden.17 A similar finding was also found in previousstudy by Pal T et al.,13 where burden of careincreased as severity of mental retardationincreased.
Strengths and LimitationsStrengths of our study are firstly the study has
been done with standardized tools and methodology.Secondly, in this study the cases who have any otherfamily member with chronic physical or mentaldisability requiring constant carewere excluded. Thenumber of siblings of children with MR were not
analysed. Generalization of finding is not possiblebecause it is a clinic based study with small samplesize.
ConclusionIn this study, the burden of care in the domain
of physical and mental health was highest. Mothersof mentally retarded children and adolescentexperience burden of care which increases inexternal support domain as the severity of MRincreases. There is significantly higher burden ofcare among mothers with low family income andilliteracy. Similar studies should be conducted foridentifying the scope of improving quality of life ofmothers of mentally retarded children. Measureshould be taken in our country to cater the mentalhealth need of mothers who care for children withmental retardation. More studies specially multi-centric needs to be conducted in the specializedcenters. In our country now District EarlyIntervention Centers have been started undergovernment programs in various parts of the countryfor early diagnosis and management of variousdisabilities including mental retardation. Furtherstudies on these centers on the very topic will addmore insight in the area of burden of care as well asmay suggest measures to decrease the burden ofcare on parents of disabled children and adolescents.
References1. Diagnostic and statistical manual - text revision
(DSM-IV-TR, 2000). Washington, DC:American Psychiatric Association 2000.
2. Gururaj G, Varghese M, Benegal V, Rao GN,Pathak K, Singh LK, et al. National mentalhealth survey of India, 2015-2016: Mental healthsystems. NIMHANS Publication No. 130.Bengaluru: National Institute of Mental Healthand Neuro Sciences 2016.
3. Weiss JA, Sullivan A, Diamond T. Parent stressadaptive functioning of individuals with develop-mental disabilities. J Dev Disabil 2003; 10(1) :29–35.
4. Pelchat D, Lefebvre H, Perreault M. Diffe-rences and similarities between mothers’ andfathers’ experiences of parenting a child with adisability. J Child Health Care 2003; 7(2) : 31–47.
5. Thara R, Padmavati R, Kumar S, Srinivasan

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 243
L. Burden assessment schedule: instrument toassess burden on caregivers of chronic mentallyill. Indian J Psychiatry 1998; 40(1) : 21-29.
6. Khare SD. Mental retardation affects qualityof life in families of disabled children and roleof nursing practices. Int J Nurs Res 2015; 1(1): 100-109.
7. Burnett SA, Meares PA. Infants and toddlerswith disabilities: Relationship-Based Appro-aches. Social Work 2000; 45 : 371-380.
8. Gosch A. Maternal stress among mothers ofchildren with Williams-Beuren syndrome, Downsyndrome and mental retardation of non-syndromaletiology in comparison to non-disabledchildren. Zeitschift Fuer Kinder und Jugendpsychiatrieund Psychotherapie 2001; 29(4) : 285-295.
9. Tisbosch M. Family Stress in Dutch Familieswith Motor Impaired Toddlers. J Early Child Res2008, 6(3) : 233-246.
10. Farber B. Family organization and crisis:Maintenance of integration in families with aseverely retarded child. Monographs of theSociety for Research in Child Development1960; 25(4) : 2-9.
11. Vijesh PV and Sukurnaram PS. Stress amongthe Mothers of Children with Cerebral PalsyAttending Special Schools. Asia Pacific DisabilRehabil J 2007; 18(1) : 76-91.
12. Pal T, Agrawal V, Arya A, Gupta PK, MahourP. A Study of Burden of Care on Key Relativesof Children and Adolescents with MentalRetardation. Indian J Public Health Res Dev2017; 8(2) : 24-28.
13. Bhatia MS, Srivastava S, Gautam P, Saha R,Kaur J. Burden assessment, psychiatricmorbidity and their correlates in caregivers ofpatients with intellectual disability. East AsianArch Psychiatry 2015; 25 : 159-63.
14. Majumdar M, Da Silva Pereira Y, Fernandes J.Stress and anxiety in parents of mentallyretarded children. Indian J Psychiatry 2005;47(3) : 144-147.
15. Narmada H, Pushpa BK. A study to assess thestress level among mother of intellectualdisability children. University of Agriculturalsciences, PhD (dissertation) Dharwad 2007; 24-36.
16. Upadhyay GR, Havalappanavar NB. Grandparental Support for Parents of MentallyRetarded Children, J Indian Acad Appl Psychol2008; 34(1) : 137-141.
17. Sethi S, Bhargava SC, Dhiman V. Study ofLevel of Stress and Burden in the Caregiversof Children with Mental Retardation. East J Med2007, 12 : 21-24.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society244
Relevance of Patterns of Use and PreferredContents in Problematic Internet Use among
Undergraduate StudentsManoj Kumar Pandey, Prabha Mishra
Department of Clinical Psychology, Post Graduate Institute of Behavioural & Medical Sciences,Raipur, Chattisgarh - 492001
Contact: Manoj Kumar Pandey, Email: [email protected]
Original Article
IntroductionIn India, prevalence of problematic internet use
(PIU) is estimated around 19.85% among under-graduate population, which is quite alarming. Lowlife satisfaction, psychological distress, poor emo-tional control etc. were also found to be associatedwith it.1
Researchers report that the undergraduatestudents experience pressure due to differentacademic demands on them and this pressure hasan adverse impact upon their life-satisfaction and
adjustment. They try to cope with such pressure indifferent ways (either solving problems or usingdifferent sorts of defenses to protect themselves).Internet has become an easy way to escapeproblems (postponing the academic tasks by texting,chatting, or using different entertainment means)similar to substance use.2 It is a matter of worrythat PIU has become a form of coping mechanism.Undergraduate students remain in process ofenhancing or growing their identity by findingmeaning and achievement in different spheres of
Abstract
Background: Problematic internet use (PIU) has diverse adverse impact on different spheresof life of undergraduate students, who are in process of identity exploration throughfinding direction in world views, work and love. Internet use is a widely studied phenomenonworldwide. In Indian set-up, there are fewer attempts to study the impact of patterns ofinternet use on PIU, and variations in preferred contents and purposes of internet useamong problematic and normal internet users. Aim: The current study was aimed to explorewhether the patterns of use of internet, preferred contents in internet and purposes ofinternet use lay their impact on problematic internet use. Methods: This study was conductedin a sample of 480 undergraduate students (equal male and female participants) agedbetween 18 to 25 years. They were selected in equal numbers (f=120) from medical,engineering, management and non-professional streams of education with convenientsampling. Semi-structured data sheet was used to obtain information about demographics,patterns of use, preferred contents and purposes of use of internet. Online cognitionscale was used to assess PIU. Data were analyzed by descriptive statistics, ANOVA and t-test. Results and conclusion: In current study, it was found that more than two years of useand higher than two hours daily use of internet has significant impact on the severity ofPIU. Further, it was observed that individuals with PIU are more inclined to contents andpurposes related to entertainment, gaming, social networking, pornography, and romancethan normal internet users.
Key Words: Patterns, Contents, Problematic internet use, Undergraduate students

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 245
their life.3,4 PIU may deviate them from these goals.Therefore, it is important to find out the factorsassociated with PIU.
In a study in young population, it was observedthat average time spent on internet (in generalpopulation) was 2.13 hours (SD 1.98) every day.The common reasons for using internet reportedwere urge to use internet and using it to over comenegative mood. Quite high numbers of participantswere found with inability to control use hours andusing it simultaneously while accomplishing crucialtasks such as eating etc. It was observed that theirphysical activity had gone down since they startedusing it.5 These findings are indicating that usinginternet in these patterns are either replacing otherconventional methods of mood modification orreducing physical activity, which might result invarious life-style related medical conditions amongthe young individuals with PIU.
It is reported in studies that intra-individualfactors are more appealing in PIU than inter-individual factors. Self-avoidance, poor regulatoryfunction, addictive traits, anger, and poor coping areprominently found associated with PIU with largereffect sizes across the studies.6 However, there arefewer attempts by researchers to explore whetherusing patterns of internetand preferred contents init are more vulnerable factors leading to PIU. Onlyfew researches were sought, which found that moreduration of use in terms of frequency and hours arelikely to lead addiction to internet.7 Hence, thecurrent study was aimed at:
1. to explore whether the patterns of use ofinternet, such as years of use and daily usehours of internet, and;
2. preferred contents in it and purposes ofusing internet lay their impact on severityof PIU.
In the line of above study,6 these factors areprimarily intra-individual factors, which need to beexplored so that if something meaning is found inthe results, might be helpful in the treatment ofundergraduate students with PIU.
Material and MethodsPurposive sampling method was considered
convenient seeing the nature of study. A sample of480 (240 problematic and 240 normal internet userswith equal numbers of male and female students),
aged 18 to 25 years served as the participants forthe study. One hundred and twenty students (30males with problematic and 30 males with normalinternet use and 30 females with problematic and30 females with normal internet use) were selectedfrom each streams of education, i.e., medical,engineering, management, and non-professionalfrom different colleges and institutions in Raipur,C.G., India. Classification of participants asproblematic and normal internet users in sample wasdone in order to know the difference betweenpreferred contents and purposes of internet usebetween them. Classification was done based onthe mean score on online cognition scale.
Online Cognition Scale (OCS) is a question-naire about the thoughts related to the internet. Itemphasizes more on the assessment of cognitionthan behaviour related to problematic internet use.It was developed by Davis, Flett, and Besser.8 TheOCS is a 36-item questionnaire that measuresproblematic Internet use. Respondents rate theagreeableness on a seven-point Likert scale for eachitem. The scale has high internal consistency as atotal measure of problematic Internet use (=0.94)and for each of the four OCS dimensions: socialcomfort (=0.87), loneliness/depression (=0.77),diminished impulse control (=0.84), and distraction(=0.81). Item-total correlations were highlysignificant, ranging from 0.47 to 0.77 for socialcomfort, 0.49 to 0.81 for loneliness/depression, 0.50to 0.76 for diminished impulse control, and 0.55 to0.80 for distraction.
Another tool used in the study was a semi-structured purposefully prepared data sheet to gatherinformation about demographic variables, patternsof internet use i.e., daily use (in hours) etc. andcontents usually surfed or watched (websites) ininternet platform by participants and the differentpurposes for which they had been using internet.
Data was analyzed using descriptive statistics,one way ANOVA and t-test through StatisticalPackage for Social Sciences (SPSS 20.0) version.
ResultsTable 1 reveals that mean scores on OCS of
the participants in relation to years of use of internet(for how many years they have been using internet).It can be seen from the table that those who havebeen using internet since 2 years or more, have

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society246
higher OSC scores. However, the mean score (M= 111.61, SD = 27.63) of participants who have beenusing internet less than 6 months is higher than thosewith 6 months to 1 years of use (M = 108.37, SD =28.21). But the participants in that group arerelatively less in number (f = 26). Otherwise, it isobserved from ANOVA in Table 2 that there is asignificant F (4,475) = 3.17, p < .05 impact of yearsof use of internet on the severity of PIU, whichwas assessed by OCS.
Table-1: Mean and SD on OCS of internetusers in relation to years of use
(beginning of using internet)
Different years Mean Std. Nof Internet use Deviation
< .5 year 111.61 27.63 26.5 to 1 year 108.37 28.21 371 to 2 years 120.51 30.27 1352 to 5 years 124.25 29.79 162>5 years 122.85 24.78 120
480
Note: OCS = Online Cognition Scale
Table-2: ANOVA showing impact of years ofuse of interneton severity on OCS
Sources Sum of Df MeanSquare Square F
Different 10345.62 4 2586.40 3.17*years ofInternetuseError 386622.97 475Total 7418358.00 480
*p<0.05Note: OCS=Online Cognition Scale
Table 3 represents that those individuals whohave been using internet since last two years or moreare having significantly higher (p < .05 & p < 0.01)PIU in comparison to those individuals who havebeen using it for lesser years than two years.Moreover, there is no significant (p > 0.05)difference between participants using internet for 2years or more on the severity of PIU as assessedby OCS.
It is revealed from Table 4 that PIU isincreasing in severity with increasing daily use hoursof internet with an exception of those individualswho use it more than 8 hours daily (M = 127.36, SD
= 26.78). There are relatively less (f = 30)participants in more than 8 hours and 6 to 8 hourscategories of internet use. Although, their meanscoresare higher than those who use internet 1 hour(M = 110.34, SD = 24.30), 1 to 2 hours (M = 113.42,SD = 25.66) and 2 to 4 hours of daily (M = 123.34,SD = 32.37). Further, ANOVA (Table 5) revealedthat there is a prominent significant impact F (5,474) = 7.19, p < 0.01 of daily use hours on theseverity of PIU.
Table-3: t-tests showing significance ofdifference between different categories of
years of use of internet on severity of PIU asassessed by OCS
Different years of internet use Df t-test
< .5 year and .5 to 1 year 61 .452< .5 year and 1 to 2 years 159 1.39< .5 year and 2 to 5 years 186 2.028*< .5 year and >5 years 144 2.05*.5 to 1 year and 1 to 2 years 170 2.19*.5 to 1 year and 2 to 5 years 197 2.95**.5 to 1 year and >5 years 155 3.00**1 to 2 years and 2 to 5 years 295 1.0691 to 2 years and >5 years 253 .6682 to 5 years and >5 years 280 .421
*p < 0.05;**p < 0.01Note: PIU = Problematic Internet Use; OCS = Online Cognition
Scale
Table-4: Mean and SD on OCS of internetusers in relation to daily use (in hours) of
internet
Different daily use Mean Std. Nhours of internet Deviation
1 110.34 24.30 581 to 2 113.42 25.66 1382 to 4 123.34 32.37 1464 to 6 130.43 24.01 786 to 8 133.26 30.98 30>8 127.36 26.78 30
480
Note: OCS=Online Cognition Scale
Following the ANOVA in Table 5, it is seen intable 6 (t-test) that more than 2 hours of daily useof internet appeared a kind of cut-off point todetermine the PIU. Those participants who havebeen using internet for more than 2 hours daily aresignificantly higher (p < 0.01) than those who use itfor lesser than 2 hours. Moreover, there is no

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 247
significant difference (p > 0.05) between differentcategories of more than 2 hours of daily use ofinternet, such as 2 to 4 and 4 to 6 hours and/or 4 to6 and more than 8 hours of use of internet etc.
Table-5: ANOVA showing the impact of dailyuse of internet (in hours) on the severity on
OCS
Sources Sum of Df Mean FSquare Square
Different daily 27992.66 5 5598.53 7.19**use hours ofinternetError 368975.92 474Total 7418358.00 480
**p < 0.01Note: OCS=Online Cognition Scale
Table-6: t-tests showing significance ofdifference between different categories of
daily use of internet (in hours) on severity ofPIU as assessed by OCS
Different daily use Df t-testhours of internet
1 and 1 to 2 194 .7781 and 2 to 4 202 2.76**1 and 4 to 6 134 4.80**1 and 6 to 8 86 3.88**1 and >8 86 3.00**1 to 2 and 2 to 4 282 2.85**1 to 2 and 4 to 6 214 4.78**1 to 2 and 6 to 8 166 3.69**1 to 2 and > 8 166 2.67**2 to 4 and 4 to 6 222 1.692 to 4 and 6 to 8 174 1.532 to 4 and > 8 174 .6364 to 6 and 6 to 8 106 .5054 to 6 and > 8 106 .5766 to 8 and > 8 58 .789**p < 0.01Note: PIU = Problematic Internet Use; OCS=Online Cognition
Scale
Table-7: Comparison of internet users for preferred contentsNormal users (n=240) Problematic users (n=240)f % f %
Preferred content (Websites) Facebook 120 50* 178 74.2*Google 218 90.8 221 92.1YouTube 150 62.5* 204 85*Chat sites 46 19.2* 103 42.9*Pornography sites 20 8.3* 48 20*Game sites 38 15.8* 54 22.5*Romantic sites 3 1.3* 20 8.3*
*Indicating problematic internet users are higher in % for corresponding contents
Table 7 and 8 reveal the qualitative analysis ofdifference in percentage for different contents andpurposes the internet being used by problematic andnormal internet users (who were classified basedon score on OCS). Table 7 indicates that higherpercentage of participants in problematic internetusers group have been observed to use contents ininternet which are related to social networking,entertainment, gaming, pornography and romance.Whereas, there is a slight (negligible) differencebetween normal (90.8%) and problematic users(92.1%) for the use of Google platform, which isthe platform for different sorts of information,knowledge, ect.
Similarly, table 8 suggests that in terms ofpurposes of use of internet, seeking information isone variable, in which the difference in percentageof participants between problematic (90.4%) andnormal (87.5%) users is least. Otherwise, for allother purposes i.e., entertainment, communicating,online marketing, online games, pornography,establishing and maintaining online relationship,problematic internet users are sufficiently higher inpercentage than normal users.
Discussion and ConclusionThis study was aimed at exploring two objec-
tives. First, whether patterns (years of use and dailyuse hours of internet) of internet use influence theseverity of PIU and second, to find out whether thepreferred contents and purposes of internet use laytheir impact on severity of PIU.
It was found in the current study that both thepatterns of use and, preferred content and purposesof internet use influenced the severity of PIU asassessed by OCS. Findings (Tables 1, 2 and 3)revealed that morethan two years of internet useand higher than two hours of daily use of internet

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society248
psychological treatment had large and durable effectas compared to medium-to-large short term effectsof pharmacotherapy.9 It is indicative from thesestudies that both form of treatment should bepreferred for the treatment of PIU, yet, psycho-logical treatment must be included and emphasized.
The findings of this study specially provideinputs for the management of PIU in affectedundergraduates. It is advised that clinicians canemphasize (by modifying) upon the patterns, andcontents and purposes of use of internet in order toreduce the severity of PIU. To reduce the severityof PIU,daily hour use of internet should be targetedin management plan. In addition, the content andpurpose of use of internet should be graduallytransferred from entertainment, leisure time, andmood modification to need based (searching infor-mation, education, banking, communication etc.) useof internet. Other authors also suggested thattreatment goals for PIU should be targeted to gradualabstinence from excessive online activities or toencourage regulated use of internet than totalabstinence from internet.10
Like other studies, with its strengths, it hasshortcoming too. First, the participants could not berandomly selected and second, there were unequalparticipants in the categories of different years ofinternet use and daily hours of internet use.
Overall, patterns of internet use, preferredcontents and purposes of using internet are quiterelevant to be assessed in order to know the levelsof severity of PIU. These issues further can helpthe clinicians in designing proper management planfor the undergraduate students with PIU.
References1. Gedam RS, Ghosh S, Modi L, Doyal A,
Table-8: Comparison of internet users for the purposes of useNormal users(n=240) Problematic users (n=240)
F % F %
Purposes of using internet Entertainment 162 67.5* 193 80.4*Information 210 87.5 217 90.4Communicating 152 63.3* 173 72.1*Online marketing 70 29.2* 111 46.3*Online Relationship 42 17.5* 74 30.8*Pornography 20 8.3* 47 19.6*Online games 36 15* 49 20.4*Online romance 6 2.5* 11 4.6*
* Indicating problematic internet users are higher in % for corresponding purposes of internet use
(Tables 4, 5, and 6) significantly increased PIU inundergraduate students. Therefore, undergraduatestudents, who have been using internet for morethan two years and those who use it daily more thantwo hours, must be screened for PIU. Although,there is a dearth of studies in this line of research,one study reported that more duration of use in termsof frequency and hours are likely to lead addictionto internet.7
In addition, one other interesting phenomenonwas observedin the current study that problematicinternet users (undergraduate students) are moreinclined towards the contents and purposesof useof internet, which are related to entertainment,gaming, social networking, pornography andromance as compared to normal internet users.These findings suggest that contents and purposesof use of internet can be important factors leadingto problematic internet use. However, for theexploration of impact of contents and purposes ofinternet use on severity of PIU, current studyemployed only qualitative analysis using percentage.It needs to be further explored using more robustquantitative methods such as random control trialsto reach to a confident and reliable prediction aboutthe impact of preferred contents and purposes onseverity of PIU.
Moreover, it is a common understanding thatindividuals with PIU would be using internet morefrequently than normal users. But this study is aunique effort to find out the impact of patterns ofuse on the severity of PIU and on other hand to findout the difference in contents and purposes ofinternet use between normal and problematic users.
Meta-analytic reviews report that for thetreatment of PIU, pharmacological and psycho-logical treatments are effective. It is seen that

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 249
Mansharamani H. Study of internet addiction:prevalence, patterns, and psychopathologyamong health professional undergraduates.Indian J Soc Psychiatry 2017; 33 : 305-11.
2. Kuss, DJ, Griffiths, MD, Karila, L, Billieux, J.Internet addiction: A systematic review ofepidemiological research for the last decade.Curr Pharm Design 2014; 20 : 1-26.
3. Arnett, JJ. Are College Students Adults? TheirConceptions of the Transition to Adulthood. JAdult Devel 1994; 1 : 154-168.
4. Arnett, JJ. Young People’s Conceptions of theTransition to Adulthood. Youth Soc 1997; 29 :1-23.
5. Grover S, Chakraborty K, Basu D. Pattern ofinternet use among profession in India: Criticallook at a surprising survey result. Indian JPsychiatry 2010; 19,2. 94-100. doi:10.4103/0972-6748.90338
6. Koo JH, Kwon J. Risk and Protective Factorof Internet Addiction: A Meta-Analysis ofEmpirical Studies in Korea. Yonsei Med J 2014;55 : 6. 1691-1711.
7. Wu CC, Pu KC. Does mobile internet affectlearning achievement? J Mo Com 2017; (4) 1 :1-9.
8. Davis RA, Flett GL, Besser A. Validation of aNew Scale for Measuring Problematic InternetUse: Implications for Pre-Employment Screen-ing. Cyberpsy Behav 2002; (5) 4 : 331345.
9. Winkler A, Dörsing B, Rief W, Shen Y,Glombiewski JA. Treatment of Internetaddiction: a meta-analysis. Clin Psychol Rev2013; 33(2) : 317–329.
10. Pontes MH, Kuss JD, Griffiths DM. Clinicalpsychology of internet addiction: a review of itsconceptualization, prevalence, neuronalprocesses, and implications for treatment.Neurosci Neuroeco 2015; (4) 11-23.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society250
To study the prevalence, pattern andpsychopathology of Internet Addiction among
Undergraduate students of different streamsSrishti Detha1, Manju Bhaskar2, Abhishek Charan3, Aditya Soni4
Departmentsof Psychiatry1,2,4 and Medicine3, Mahatma Gandhi Medical College and Hospital, JaipurContact: Manju Bhaskar, E-mail: [email protected]
Original Article
IntroductionThe turn of the century was marked by the
development of the World Wide Web. The internet,while proving itself as an unparalleled tool ofinformation exchange, has also invaded the lives ofmillions as an addictive menace. Affecting socio-demographic strata ranging from the urban to therural, there is no denying that internet addiction hasevolved into a serious threat.
Much like any other addiction, youth andadolescents are the most vulnerable group forinternet addiction, being influenced by the surround-
ings and its psychosocial impact. Currently theworld’s population comprises of about 1.2 billionadolescents of which 243 million are in India.Indiaboasts the second highest number of mobilesubscribers of any country worldwide – testamentto the technological transformation that has spreadacross Indian society over the past decade. Thecountry is also now the world’s second largestsmartphone market, having overtaken the US in thefirst half of 2016.2 It comes as no surprise that mostof our internet users consist of the youth, theirincreasing numbers being attributed to many reasons
Abstract
Introduction - In this 21st century, internet has worked as a boon to develop our society.But with the vast advantages, internet has also brought some dangers and internet addictionis one of those. The youngsters who are the prime users of the internet are its major victim.India having the highest number of young populations in the world is more prone for sucha disorder. Material and methods - It is a cross-sectional study conducted in the metrocity. The study included 1000 students from different streams and colleges. They wereasked to fill three questionnaires that included Duke’s General Health Questionnaire,Young’s Internet Addiction Test and a semi structured proforma. The presence of internetaddiction was assessed by the Young’s Internet Addiction Test. Results - In this study, outof 1000 participants, 981 completed all the questionnaires. Out of these 981, 499 weremales (50.8%) and 482 were females (49.1%). The data were analyzed based on Young’sinternet addiction test and respondents were distributed in 4 groups with 40.4% beingaverage users,31.4% mild addicts, 27.01% as moderate addicts and 1.1% as true addictswhose life got affected due to this addiction. The addicts were mostly male and thisrelationship was statistically significant (P value < 0.0001). Conclusions - This is a publichealth issue which still hasn’t caught the attention of our society, including family andpolicy making bodies, health institutions and the education sector. It is very important todevelop strategies to bring internet usage and dependence under check.
Keywords: Internet addiction, Prevalence, Psychopathology, Undergraduate students

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 251
like free internet access, cheap smart phones, widerange of entertainment options available and so on.These factors lead to unorganized and excess useof the internet.
Owing to the increasing dependence on internet,Dr. Ivan Goldberg coined the term ‘InternetAddiction’ in 1996 where he defined it as pathologicalcompulsive internet use.3 Later in 1996, a psycho-logist – Miss Kimberly Young described it as animpulse control disorder, dividing it into 5 subtypes,
1. Cyber relationship addiction2. Cyber-sex addiction3. Net compulsions4. Information overload5. Computer addiction4
She also developed an internet addictionquestionnaire with 8 questions which was laterformulated to Internet addiction test with 20questions. This is the most commonly used test,accepted by Mc Murran. There are several studiestargeting internet addiction, but a formal consensusremains to be achieved; a common ground for itsdiagnostic criteria has eluded researchers world-wide.
When it comes to undergraduates undertakingvarious professional courses, the scenario may bedifferent as these students may not have excessfree hours. This study aims at contributing to theinternet addiction prevalence, pattern and its psycho-pathology in college going students.
Aims and ObjectivesTo study the prevalence, pattern and psycho-
pathology of Internet Addiction among under-graduate students pursuing various professionalcourses.
Materials and Methods• Study design: This cross-sectional study
was conducted in 4 different faculties ofcolleges between May and July (2018).
• Sample size: The sample students wereselected randomly; sample size wasrestricted to 1000 students: 250 studentsfrom 4 different streams each, who havebeen using internet for last 10 months atleast. A tentative lower bound for the samplesize can be calculated using Cochran’sformula:
where Z is the Z value (=1.96 at 95% confi-dence),p is the prevalence of internet addiction, q is simply1-p, and d is the absolute allowable error.
• Measurement tools and data collection:Three questionnaires in straightforward andcomprehensive English were used in thestudy. It was distributed in classrooms tostudents who volunteered and were given20 minutes to fill it.
1. A Semi structured proforma: designed toseek details of educational course pursued, purposeof internet usage, device and time of the daypreferred for internet access and the duration ofuse.
2. Duke’s General Health Questionnaire(GHQ): which was used to screen for anypsychiatric illnesses in non-clinical environment; itcovered general aspects of the respondents suchas stress, insomnia and depression in last one week.5
It consists of 11 scales ranging from 0 to 100. Outof these 11 scales, 6 scales consist of physical health,mental health, general health, self-esteem, social andperceived health. These were used to define generalfunctioning of an individual: high scores suggestiveof good health. The remaining 5 scales consisted ofanxiety, pain, disability and depression whichprovided measures of dysfunction (higher scoresindicative of poor health).
3. Young’s Internet Addiction Test (IAT):which is the most used test for gauging internetaddiction and has been approved time and again forits psychometric properties. It consists of 20questions with responses based on a 5-point Likert-like scale. At the end, results were grouped basedon level of addictions corresponding to final scores,where 0-30 is normal, 31-49 is mild addiction, 50-79is moderate and 80-100 was severe addiction. Forour study group, this tool fits best because of itsvalidity and reliability.6 The presence and severityof Internet Addiction was assessed using this test,as it has not been included as a disorder in any ofthe currently used classification systems namely –ICD 10, DSM 5. Though the inclusion of GamingDisorder in the ICD 11 marks the possibility of anupcoming disorder of Internet Addiction in futureowing to increasing dependence of people on internet

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society252
usage.• Institutional ethical committee (IEC) - IEC
approval was sought for this study.• Data analysis- descriptive statistics were
used to analyze data and to bring out anassociation of various factors involved withinternet addiction. Chi square values werecalculated in all variables with significant pvalue between these variables.
ResultsIn this study, out of 1000 participants, 981
completed both the questionnaires. Out of these 981,499 were males (50.8%) and 482 were females(49.1%). The data were analyzed based on Young’sinternet addiction test and respondents weredistributed in 4 groups with 40.4% being averageusers, 31.4% mild addicts, 27.01% as moderateaddicts and 1.1% as true addicts whose life gotaffected due to this addiction. There was clear malepreponderance for the moderate and severe addicts.
Table-1: Distribution of internet users basedon the age group –
Age group Number of Percentagestudents wise age distribution
16-19 203 20.6%20-22 409 41.6%23-26 369 37.6%
The mean age of the student was 20.82 years.Most of these students fell in the 19-22 age group.
Table-2: Distribution of the users based onthe gender
Sex Normal Mild Moderate Severe Total
Male 181 123 186 9 499Female 216 186 79 1 482
Chi-square value - 65.2591P value < 0.0001 significant
Male gender had a greater number of internetaddicts as compared to female gender.
Table-3: Preferred time of the day forinternet access by the users–
Time of the day Normal Mild Moderate Severe
Morning 237 151 102 1Night 160 158 163 9Total 397 309 265 10
Chi-square value – 35.5336p value - < 0.00001 ’! significant
Users preferred night-time over the daytime asthe severity of addiction increased.
Table-4: Association between InternetAddiction and various Internet Usage
Options –
Usage options Normal Mild Moderate Severe
Gaming 70 56 88 6Social networking 145 106 72 2Web surfing 112 83 67 2Education 70 64 38 0
Chi-square value – 36.784P value - < 0.0003 ’! significant
Table-5: Prevalence of Internet Addiction in different Professional Courses –
Professional course Normal Mild Moderate Severe
Medical 124 60 45 1Physiotherapy 93 86 108 2Engineering - Information Technology 82 98 50 2Engineering – Civil 93 65 62 5
Chi-square value– 51.52P value<0.0001 ’! significant
Table-6: Significant scores on Duke’s GHQ among the Internet Addicts assessed –
Variables Mild Moderate Severe F-ratio P- value Significance
Physical health score 75 74 54 3508.33 0.00001 SignificantMental health score 70 70 60 313.73 0.00001 SignificantSelf-esteem score 74 70 65 101.66 0.00001 SignificantAnxiety score 82 76 60 68.695 0.0001 SignificantDepression score 75 70 45 51.666 0.0001 SignificantAnxiety depression score 80 75 48 68.914 0.0001 Significant

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 253
As per the data collected, the initial levels ofinternet addiction were inclined to social networkingand web surfing. As the severity of addictionincreased it was found that gaming is the mostaddictive usage of internet while educational purposebeing the least.
Data showed clear preponderance ofengineering students over students from medical line.
Duke’s GHQ suggested that severe addicts hadmental and physical health problems like poorconcentration, lack of sleep,anxiety,depression,lowself-esteem. This observation was statisticallysignificant.
Those students who got the significant scoreson the items used here, were psycho-educated abouttheir situation and were advised to consult the OPDservices where they were considered forpharmacotherapy, psychotherapy or both.
DiscussionMany studies conducted worldwide show
different trends of internet addiction. This variationwas attributed to the local factors such as socio-demographics, education status, internet availability,etc. Our study was focused on learning the internetaddiction trend in our city among different age groupsand streams of undergraduate students. This studyshowed clear predilection in male students forinternet addiction. This observation was statisticallysignificant. This finding was also seen in manystudies such as Nalwa and Anand7 whereinvestigators observed that male school goingstudents had more internet addiction than theirfemale peers. Similar observation was made byArvind et al.8 This increased vulnerability of malestudents towards internet addiction may be becauseof their likely interest in gaming, pornography andgambling activities.9 Mean age of the participantswas 20.82 years. Some studies found that late 20sand early 30s have more internet addiction.10,11 Ourstudy showed that most users were in 19-22 agegroup. Similar study conducted by Surwase12 showed60.63% in 19-20 age group.
In our study most of the internet users put smartphone as their most preferred device, placing themabove computer/laptops, may be because of theimmense ease of access facilitated by smart-phonesand the portability are unparalleled. This observationis like the results in studies conducted by Paul et
al,13 Surwase,12 Krishnamurthy et al14 and Dhoketal.15
In our study we found that engineering studentshave statistically proven to be more addicted ascompared to other fields of study. Our study showedthat 40.4% were average users while 31.4% hadmild addiction,27.01% were moderate addicts whichwere prone to become true addicts and 1.01% weretrue addicts. Similar study showed 0.3 % true addictsin study conducted by Arvind et al.8 Another studyconducted by Vidya et al16 in south India on MBBSstudents showed 18.88% prevalence of internetaddiction including moderate and severe addiction.Wide prevalence rate was observed in the rest ofthe world such as 6.3% in Iran17 and 16.25% inChina.18 The prevalence range was 0.9% to 38%in various studies involving different standards.19 Thiswide variation can be due to the different standardsused in different studies across the globe. It is ofcrucial importance that a consensus be reached anda universally accepted standard diagnostic scale forinternet addiction be created. Variation can also bedue to the different social structure of the populationstudied.
Our study also observed that most of the usersand almost all addicts preferred night-time forinternet usage. This may lead to the adverserepercussions on user’s health, leading to less sleepand decline in physical and mental health. Thisfinding corroborates with study conducted by Goelet al.20
In our study, the internet usage was found tobe mainly directed to social networking and websurfing with few students involving in educationaland gaming purposes at initial levels of internetaddiction. As the severity of addiction increased itwas found that gaming is the most addictive ofinternet, web surfing and social networking at equalprevalence while educational purpose being the leastamong the severe addicts. Our study thus clearly isfollowing the importance gaming addiction is givenin ICD-11 recently that it has been added as anindependent disorder recently, as Gaming disorder.Other studies by Kormas et al,21 Morrison and Gore22
and Durkee et al,23 on patterns of usage show socialnetworking as the highest ranked online activity.Though our study found gaming as the mostaddictive online activity amongst students.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society254
students.• Use of self-reporting tests is inferior to in-
person interviews but it would have beentedious at this sample size so could not bedone.
• Recall bias – as students were asked abouttheir past usage of internet.
• Social- desirability bias – as the studentsmay have attempted the questionnaires topresent himself/herself as a normal user.
References1. United Nations, Department of Economic and
Social Affairs, Population Division, WorldPopulation Prospects: The 2008 revision,<www.esa.un.org/unpd/wpp2008/index.htm>,accessed October 2010; and UNICEF globaldatabases, accessed October 2010.Adolescence - An Age of Opportunity. UNICEF.2015 : 1-12.
2. The Mobile Economy: India. 2015: 1-56 GSMA.Source: Cyber Media Research. These latestunique mobile subscriber statistics are based onthe results of an extensive global consumersurvey conducted by GSMA Intelligence in 2015
3. New Yorker Magazine. Just Click No. TalkStory about Dr. Ivan K. Goldberg and theInternet Addiction Disorder. [Last accessed on2015 Dec 14]. Availablefrom: http://www.newyorker.com/magazine/1997/01/13/just-click-no.
4. Young K, Pistner M, O Mara J, Buchanan J.Cyber-disorders: the mental health concern forthe new millennium. Cyberpsychol Behav 2000;3 : 475-9.
5. Hu Y, Stewart-brown S, Twigg LIZ, et al. Canthe 12 item General Health Questionnaire beused to measure positive mental health? PsycholMed 2007; 37 : 1005–13.
6. Widyanto L, McMurran. The psychometricproperties of the internet addiction test.Cyberpsychol Behav 2004; 7 : 443-50.
7. Nalwa K, Anand A. Internet addiction instudents A cause of concern. Cyber psycholBehav 2003; 6 : 653-656.
8. Sharma A, Sahu R, Sharma R, et al. Internetaddiction among professional courses students:A study from central India. Int J Med Sci PublicHealth 2014; 3 : 1069-1073.
Several studies demonstrated significantcorrelation between stress, anxiety, depression andinternet addiction. Carli et al24 conducted a studywhich showed an association between depressionand internet addiction. Some studies such as Fischeret al25 and Yen et al26 showed depression as anindependent predictor for internet addiction.However, in this study the depression was animpelled action of internet addiction. The bi-directional association shows that these phenomenashould not be viewed separately. Low self-esteemand loneliness may push a depressed person towardsinternet addiction. Sometimes, internet may workas a “therapeutic healer” in socially isolated peopleby providing an interactive platform online. Ourstudy showed that internet addiction causessignificant mental and physical health problems. Onestudy conducted by Alpaslan et al27 on Turkishmedical students found that internet addicts had poormental health that involved loneliness and increasechances of suicide.
ConclusionInternet addiction is spreading and affecting an
ever-increasing number of people. The main victimof this addiction is the youth. This has led to anegative impact on their mental and physical healthand has thus declined their overall efficiency in eachfield. This is a public health issue which still hasn’tcaught the desired attention of our society, includingfamily-policy making bodies, health institutions andthe education sector. It is very important to developstrategies to bring internet usage and dependenceunder check. Spreading awareness is of paramountimportance for students and their families; this canbe effectively achieved by creative projects suchas advertisements, dramas, short-films etc. Seminarsand sessions should be considered and held invarious colleges to inform the students regardingthis addiction. Psychiatrists and physicians shouldalso keep a lookout for internet addiction in casesof anxiety and depression. To ensure a healthy andproductive future for the Indian youth, we need toaddress this issue with all the seriousness andurgency it deserves.
Limitations· A matched control population was absent,
making it difficult to compare the results with healthy

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 255
9. Morahan-Martin J, Schumacher P. Incidenceand correlates of pathological Internet useamong college students. Comput Human Behav2000; 16 : 13-29.
10. Marahatta S, Adhikari B, Aryal N, Regmi R.Internet Addiction and Associated Factorsamong Health Sciences Students in Nepal. JCommunity Med Health Educ 2015; 5(4) : 6–10.
11. Osada H. Internet addiction in Japanese collegestudents: Is Japanese version of InternetAddiction Test (JIAT) useful as a screening tool?Bull Senshu Univ Sch Hum Sci 2013; 3(1) : 71–80.
12. Surwase K, Adikane H, Narlawar U, et al. ACross Sectional Study on the Prevalence ofInternet Addiction and its Association withMental Health Among College Going Studentsin Nanded City. Int J Community Med PublicHealth 2017; 5(2) : 385–90.
13. Paul AV, Chellavel Ganapthi R. DuraimuruganK, Abirami M, Elizabeth Reji V. InternetAddiction and Associated Factors: A StudyAmong College Students in South India. InnovJ Med Heal Sci 2015; 5(3) : 121–5.
14. Krishnamurthy S, Chetlapalli SK. Internetaddiction: Prevalence and risk factors: A cross-sectional study among college students inBengaluru, the Silicon Valley of India. Indian JPublic Health 2015; 59(2) : 115–21.
15. Dhok RS, Kadarkar KS, Doibale MK. Exploringlevels of Internet addiction among medicalinterns: a cross-sectional study. Int J Med SciPublic Heal 2016; 5(11) : 1–5.
16. Chathoth VM, Kodavanji B, Arunkumar N, PaiSR.Internet behavior pattern in undergraduatemedical students in Mangalore. IJIRSET 2013;2.
17. Mashaei N, Mohammad A, Ahmad PB, et al.The Prevalence of Internet Addiction Amongthe Students of Rafsanjan University of MedicalSciences. ASEAN J Psychiatry 2013; 14 : 109-16.
18. Liu X, Bao Z, Wang Z. Internet Use and InternetAddiction Disorder Among Medical Students:
A Case from China. Asian Soc Sci 2010; 6 : 1.19. Jang KS, Hwang SY, Choi JY. Internet addiction
and psychiatric symptoms among Koreanadolescents. J Sch Health 2008; 78 : 16571.
20. Goel D, Subramanyam A, Kamath R. A studyon the prevalence of internet addiction and itsassociation with psychopathology in Indianadolescents. Indian J Psychiatry 2013; 55 : 140-3.
21. Kormas G, Critselis E, Janikian M, Kafetzis D,Tsitsikacorresponding A. Risk factors andpsychosocial characteristics of potentialproblematic and problematic internet use amongadolescents: A cross-sectional Study. BMCPublic Health 2011; 11 : 595.
22. Morrison CM, Gore H. The Relationshipbetween excessive Internet Use anddepression: a questionnaire-based Study of 1319young people and adults. Psychopathology 2010;43 (2) 121–126.
23. Durkee T, Kaess M, Carli V, Parzer P, et al.Prevalence of pathological Internet Use amongAdolescents in Europe: demographic and Socialfactors. Addiction 2012; 107 (12) : 2210–2222.
24. Carli V, Durkee T, Wasserman D, et al. Theassociation between pathological internet useand comorbid psychopathology: a systematicreview. Psychopathology 2013; 46 : 1-13.
25. Fischer G, Brunner R, Parzer P, et al. Depression,Deliberate self-harm and suicidal Behavior inAdolescent Engaging in Risky and PathologicalInternet use. Praxis Der Kinderpsychologie UndKinderpsychiatrie 2012; 61(1) : 16–31.
26. Yen JY, Ko CH, Yen CF, Wu HY, Yang MJ.The Comorbid Psychiatric symptoms of Internetaddiction: Attention deûcit And Hyperactivitydisorder (ADHD), depression, Social phobia,And hostility. J Adolesc Health 2007; 41(1) :93–98.
27. Alpaslan AH, Avci K, Soylu N, Guzel HI. TheAssociation between Problematic Internet Use,Suicide Probability, Alexithymia and Lonelinessamong Turkish Medical Students. J Psychiatry2015; 18(1) : 1–8.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society256
Metacognitions in patients with GeneralizedAnxiety Disorder (GAD) in a tertiary care center
of North IndiaJyoti Dubey,1 Shweta Singh,2 AdarshTripathi,3 P.K. Dalal,4 Seema Rani Sarraf5
1Department of Psychiatry, Balrampur Hospital, Lucknow;2,3,4 Department of Psychiatry, KGMU, Lucknow and
5Department of Psychology, M.G. Kashi Vidyapeeth, VaranasiContact: Shweta Singh, Email: [email protected]
Original Article
IntroductionCommonly characterized by ‘free floating
anxiety’, Generalized Anxiety Disorder (GAD) isone of the most commonly occurring mentaldisorders in community and in the primary healthcare setting.1,2 According to the major diagnosticclassification schemes including the Diagnostic andStatistical Manual of Mental Disorders, 5th Edition(DSM-5) the essential feature of GAD is excessiveanxiety and worry (apprehensive expectation) abouta number of event or activities. Intensity, duration,or frequency of the anxiety and worry in individualsare out of proportion to the actual likelihood orimpact of the anticipated events.3
Meta cognition refers to “psychological struc-
tures, knowledge, events, and processes that areinvolved in the control, modification, and inter-pretation of thinking”.4 The maintenance ofpathological worrying in GAD can be linked toparticular meta cognitions about worry5 which havebeen indicated in Metacognitive models ofpsychological disorder and their treatments.6,7 In hismodel, Wells8 proposes that the perception ofworrying as “uncontrollable” is a central theme thatis causally involved in the maintenance of GAD.
The Metacognitive model given by Wells5
views worry to be a relatively normal cognitiveprocess, however in individuals with GAD, worryis viewed to be pathological. This pathological,repetitive and uncontrollable worry in GAD is
Abstract
Background and Objective: Involvement of the Metacognitions as the a vulnerability factorhas a role in predicting development and maintenance of various psychological disordersincluding GAD. This study aimed to examine the metacognitions in patients with GAD incomparison to healthy controls. Methods: This was a cross- sectional study on 25 Subjects ofGAD and equal number of healthy controls, assessed on Mini International NeuropsychiatricInterview (MINI), General Health Questionnaire (GHQ) and Metacognition Questionnaire(MCQ). Purposive sampling method was used and t-tests were conducted to determine thesignificant difference between metacognition of the GAD patient to the healthy controls. Results:Results revealed metacognitions of the GAD to be significantly different from the healthy controlson all sub domains of MCQ i.e positive belief about worry, negative beliefs about uncontrollabilityof thoughts and danger, beliefs about cognitive confidence, general negative beliefs aboutworry and cognitive self-consciousness. Conclusion: Finding of the study corroborate withthe metacognitive model of anxiety disorder . The GAD patients have higher dysfunctionalmetacognition then the healthy controls.
Keywords : Metacognition, Worry, Generalized Anxiety Disorder.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 257
accompanying individual’s metacognitive beliefsaround worrying. The individuals with GAD areprone to have rigid beliefs about the advantages ofusing worry as a coping strategy. According toWells7 it was suggested that while people generallybelieve that worrying can be beneficial, adults withgeneralized anxiety disorder (GAD) tend to believethat worrying is “uncontrollable and dangerous”.8,9
In a study by Leredana10 worry is a cognitiveprocess characterized by repetitive uncontrollablethought that anticipated negative outcomes andcause distress in individuals. Wells and Carte11
found that compared to Type1 worry, the Type 2worry is a stronger predictor of pathologicalworrying. Nassif12 suggested the causal role ofnegative metacognitions in the development ofGAD,13 and found that negative ‘beliefs aboutuncontrollability and danger ’ predicted thedevelopment of GAD 12–15 weeks later in non-patients. Purdon14 examined the effects of in-vivoappraisals of worrying in non-patients. The modelsuggests that the use of worrying as a copingstrategy can have problematic consequences forself-regulation, and these effects can contribute tothe development of negative Metacognitions. Astudy also showed that participants with high levelsof ‘positive and negative metacognitive beliefs’about worry have higher psychopathology; andthose with higher scores in ‘positive beliefs’ hadthe highest worry.15
In a recent study16 the comparison of metacog-nitive beliefs and worry in depressed, anxiouspatients and controls was done. The results of thestudy indicated that compared to depressed patientsand non-patient subjects, anxious patients hadsignificantly higher levels of meta-cognitive beliefsand worry. Moreover, there was a positive signi-ficant correlation between meta-cognitive beliefsand worry in anxious patients and healthy subjects.
The existing body of research gives evidencefor the involvement of the Metacognitions as thevulnerability factors in predicting development andmaintenance of psychological worry in GAD. Therole of metacognition in GAD has been studied inthe west, there is scarcity of the research data inIndian population. The metacognitive parametersvary across the globe in due to cultural factors; andit have a role in the belief system. Hence there is aneed to study metacognitions of GAD in Indian
population. By identifying and understanding ofdifferent metacognitive beliefs and worries ofpatients with GAD in our population it will help usin planning better management of this condition.This project was set out to study Metacognitions inpatients with Generalized Anxiety Disorder (GAD)in a tertiary care center of North India. It washypothesized that the Metacognitions of GADwould be different from the healthy controls.
Material and MethodsDesign and Sample
This is a cross sectional case control studyconducted on 25 patients diagnosed with GAD andequal number of healthy controls. Purposivesampling was used for sample selection. weincluded the GAD diagnosed by the Psychiatristmeeting the selection criteria of our study,presenting to the Adult Psychiatry OPD,Department of Psychiatry, K.G. Medical University,UP, Lucknow.
Healthy individuals meeting the selectioncriteria, matched on (age, sex, education) wererecruited from staff employees and healthyvolunteer who were not first degree relatives of anyother patient with psychiatric disorder.
Inclusion criteria for case group• Willing to give informed consent.• Patients aged between 18-60 years.• Diagnosis of GAD as per ICD-10 DCR
criteria.• Minimum education of 5th std.• Patients who were not receiving any
psychotropic medications from at least past2 days
Exclusion criteria for case group• Those fulfilling ICD 10 DCR criteria of any
other psychiatric disorder (except GAD).• Those with a severe or chronic physical/
medical disorder or condition that requireprior medical management.
• Those with family history (first degreerelatives) of any psychiatric disorder as perICD 10 DCR.
Inclusion criteria for healthy controls• Willing to give informed consent.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society258
• Patients aged between 18-60 years.• Minimum education of 5th std.• GHQ score less than or equal to 3.
Exclusion criteria for healthy controls• Those fulfilling current or lifetime criteria
of any psychiatric disorder on MINI• Those with family history (first degree
relatives) of any psychiatric disorder as perICD 10 DCR criteria
Description of the tools:The International Statistical Classification of
Diseases and Related Health Problems 10thRevision (ICD-10): This is a coding system ofdiseases and signs, symptoms, abnormal findings,complaints, social circumstances and externalcauses of injury or diseases, as classified by theWorld Health Organization.17 The DiagnosticCriteria for Research accompanying the ICD-10(DCR-10) are designed for use in research by WHOin 1992.
MINI International NeuropsychiatricInterview (M.I.N.I. 6.0): The M.I.N.I. InternationalNeuropsychiatric Interview (M.I.N.I. 6.0) is a short,structured diagnostic interview developed bySheehan et al.18 MINI provides diagnoses accordingto DSM-IV and ICD-10 criteria psychiatricdisorders.
General Health Questionnaire (GHQ): TheGHQ19,20 was designed to assess psychiatric distressrelated to general medical illness. The GHQ deve-loped to evaluate the psychological component ofill health. GHQ-12 is a measure of current mentalhealth. Transitory symptoms of that last less than 2weeks are viewed as psychologically significant onGHQ. Hindi version is available.21
Metacognition Questionnaire (MCQ): TheMetacognitions Questionnaire, developed byCartwright and Wells9 concerned with the beliefspeople have about thinking. The MCQ is a 65-itemquestionnaire. It assesses individual differences inmetacognitive beliefs, The Questionnaire has 5subscales, measuring the following dimensions ofmetacognition:
1) Positive worry beliefs,2) Beliefs about uncontrollability and danger
of worry, 3) Meta-cognitive efficiency,
4) General negative beliefs, and5) Cognitive self-consciousness.
Statistical analysis:Statistical analyses were performed on SPSS
version 20, Graph Pad InStat software. Discretevariables data were expressed in percentages,frequencies, and test of significance werecalculated. Categorical data were compared by Chi-square test . For continuous variable t-test(independent samples Student t-test) was used forcomparison between two group.
ResultsTotal number of the patients screened in the
case group were 40 out of which 25 could beincluded in case group. Whereas in the controlgroup total no of subjects screened were 28 out ofwhich 25 could be included in the study as per theselection criteria. Most common exclusion criteriawere presence of comorbid psychiatric illness andmedications use from past 2 days in the case group.
Table 1: shows the means age of the case groupwas 30.28 ± 7.02 and range was 19-47 years, andthe controls mean age and range was 32.61 ± 10.23and 19-56 years. In terms of age , sex, gendereducation, employment status and family incomethere is no significant difference
As depicted in the table 2 clinical parametersrevealed 76% of the study group had duration ofillness between 0-5 years. Mean years of durationof illness was 3.35 years. The mean age of onset ofillness was 25.52 years. 56% of the cases were inthe 20-29 year-group.
Table 3 Shows Mean, S.D and t-test analysiscomputed to see the differences between cases andcontrols, it was seen that the Metacognition of thecase group, was significantly different at the levelof confidence (p=<0.001 and 0.01) from controlgroup on total scores and all five sub domains ofmetacognition.
DiscussionThe present study was conducted to examine
metacognitions in patients with GAD in comparisonto healthy controls in a tertiary care center of NorthIndia. The subjects were matched on age, sex andeducation. Moreover, the selection criteria of thestudy sample were made stringent to reduce the

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 259
Table-1: Socio demographic characteristics of the case and the control groups
Characteristics Case group n=25 (%) Control group n=25 (%) Test of significanceX², df, P-value
Age in year18-30 18 (72%) 18 (72%)31-45 5 (20%) 4 (16%) 0.31(2)46-60 2 (8%) 3 (12%) 0.85Mean age ± SD 30.28 ± 7.02 32.61 ± 10.23
Sex
Male 17 (68%) 15 (60%) 0.86 (1)Female 8 (32%) 10 (40%) 0.076
Level of education
Secondary level 6 (24%) 5 (20%)High school 3 (12%) 3 (12%)Intermediate 4 (16%) 5 (20%) 0.202(4)Graduation 7 (28%) 7 (28%) 0.995Post-graduation 5 (20%) 5 (20%)
Employment Status Case group n=25 (%) Control group n=25 (%) Test of significanceX², df,P-value
Unemployed 3 (12%) 1 (4%) 3.16 (4), 0.53Skilled 7 (28%) 6 (24%)Semi-skilled 2 (8%) 6 (24%)Student 7 (28%) 7 (28%)Housewife 6 (24%) 5 (20%)
Marital Status
Married 18 (72%) 13 (52%) 1.35 (1),024Unmarried 7 (28%) 12 (48%)Muslim 9 (36%) 5 (20%)
Family type
Nuclear 7 (28%) 18 (72%) 8.0, (1), 0.0047**Joint 18 (72%) 7 (28%)
Family Income in Rupees/Months
<5,000 9 (36%) 9 (36%) 4.50(2) 0.1055,000-10,000 11 (44%) 5 (20%)>10,000 5 (20%) 11 (44%)
Domicile
Rural 15 (60%) 7 (28%) 3.97 (1) 0.046*Urban 10 (40%) 18 (72%)
* significant at < 0.05 level** significant at < 0.001 leveleffects of confounding variables on the metacogni-tions of subjects It has been emphasized by literaturethat it is essential to consider these aspects whilestudying metacognition.22-24
Our study results indicate higher totaldysfunctional metacognitions in GAD compared tohealthy controls on all five sub-domains of
metacognition assessed on MCQ i.e. positive beliefabout worry, negative beliefs about uncontroll-ability of thoughts and danger, cognitive efficiency,general negative beliefs about worry and cognitiveself-consciousness. These findings are consistentwith conceptualization of GAD according tometacognitive theory and therapy models of anxiety

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society260
Table-2: Clinical Characteristics of the casegroup
Characteristics (n=25) (%)
Duration of illness (in yrs.)0-5 19 (76%)6-10 4 (16%)11-15 2 (8%)Mean ± SD 3.35 ± 3.54Age of onset in (yrs.)10-19 3 (12%)20-29 14 (56%)30-39 8 (32%)Mean ± SD 25.52 ± 6.35
Table-3 Comparision of Metacognitions (MCQ) between case group and control group
MCQ domains Case group Control groupMean ± SD(n=25) Mean ± SD(n=25) t-valuedf=48 P-value
1. Positive worry beliefs 40.44 ±10.71 33.64 ± 8.07 4.01 0.0002**2. Belief aboutUncontrollability and Danger 50.4 ± 6.22 32.72 ± 9.01 8.07 0.0001**3. Meta cognitive efficiency 23.56 ± 8.09 17.92 ± 4.93 2.97 0.0046*4. Gen negative belief 37.92 ± 8.20 26.56 ± 6.49 5.43 0.0001**5. Cognitive self-consciousness 19.92 ± 2.81 17.24 ± 3.75 2.86 0.0063*Total (Mean ± SD) 172.2 ± 22.41 127.68 ± 22.78 6.97 0.0001**
* significant at <0.05 level** significant at <0.001 level
Figure-1
disorders.25 According to which, worry becomesproblematic when individual develops negativebelief about worry at which point ‘worry about
worry’ develops as worrying itself is appraised asdangerous and uncontrollable.
People with GAD share contradictory thoughtsabout worrying (i.e. both positive and negativebeliefs co-exist) a manner to resolve this conflict isto attempt not to think about these thoughts.Unfortunately thought suppression strategies of thiskind are rarely successful as indicated bysuppression research26,27 and their failure reinforcesbelief in uncontrollability.
Positive metacognitive beliefs refer toinformation individuals hold about coping strategies
that impact on cognition and internal states. Thesemay include beliefs such as “Worrying will helpme get things sorted out in my mind”9 or

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 261
“Rumination will help me solve the problem”28.Such beliefs are understood as antecedent to thebeginning of maladaptive coping and central to itsstrategic selection. Negative metacognitive beliefsrelate to the meaning and consequences of engagingin a given form of coping and related intrusivethoughts and feelings. These may include beliefssuch as “My worry is uncontrollable”9 or“Ruminating will damage my mind”.28 Such beliefsare associated with an escalation of negative verbalactivity that contributes to fixing attention on threatso that individuals have difficulty switching tonormal threat-free condition.7 The model postulatesa sequential process with positive meta cognitions(i.e., “Worry helps me cope.”), initiating Type 1worries (worries about internal or external cues;),which in turn trigger negative metacognitions (i.e.,“Worry is dangerous for me.”), leading to Type 2worry (meta-worry; i.e., “If I keep worrying, I willbe mad.”). Importantly, Type 2 worries aresuggested to trigger negative emotions and futileefforts to stop worrying (i.e. thought suppression,reassurance-seeking or avoidance), both conditionscontribute to worry being maintained.29 This viciouscircle of negative metacognitions is continuous andworry is then viewed by the individual as assertionfor the belief that worry is uncontrollable.
Studies which assessed the relationshipbetween metacognition and anxiety disorder showthat GAD is characterized by negative beliefs aboutuncontrollability and danger and negative beliefsIndividuals meeting criteria for GAD on DSMIII-R, DSM-5 report positive reasons for worrying30,as do non-patients.31 Proneness to pathologicalworry characteristic of GAD is positively associatedwith both negative and positive beliefs aboutworry.9,32 An earlier study done by, Wells andCarter11 demonstrated that patients meeting criteriafor GAD in DSM-III-R33 could be significantlydistinguished from patients with panic disorder,social phobia, or non-patients by their elevatedlevels of negative beliefs about worry and meta-worry. Nassif (1999) examined the causal role ofnegative metacognitions in the development ofGAD in DSM-III-R,13 and found that negativebeliefs about uncontrollability and danger predictedthe development of GAD, 12–15 weeks later in non-patients. Other researchers34 have reported similarfindings. It was shown that GAD is characterized
by beliefs about cognitive competence, negativebeliefs about uncontrollability and danger andnegative, while OCD was characterized byincreased cognitive self-consciousness.35
The limitations of the study are that due to smallsample size generalizability of the finding becomeslimited, therefore studies need to be done on largesamples, The biggest strength of this study is thattill date only western data has been found toexploring the role of metacognition in patients withGAD. Although in Indian setting we could not findstudy on the role of metacognition patients withGAD and compare with that of healthy controls.Implications of comparing metacognitions withother anxiety disorders and compulsion relateddisorders. Negative metacognition should betargeted in the therapy before the positive belief,since these are closely linked to acute anxiety.
References1. Kessler RC, Wittchen HU. Patterns and
correlates of generalized anxiety disorder incommunity samples. J Clin Psychiatry 2002;63 Suppl 8 : 4-10.
2. World Health Organization. The ICD-10.Classification of mental and behavioraldisorders-clinical descriptions and diagnosticguidelines. New Delhi: Oxford University Press1992.
3. American Psychiatric Association (APA).Diagnostic and Statistical Manual of MentalDisorders, 5th edition. (DSM-5). Washington:APA 2013.
4. Fisher R. Thinking About Thinking: Develop-ing Metacognition in Children. Early ChildDevelopment Care 1998; 141(1) : 1-15.
5. Wells A. Cognitive therapy of anxiety disorders:a practice manual and conceptual guide.Chichester, UK: Wiley 1997.
6. Wells A, Matthews G. Attention and emotion:a clinical perspective. Hove, UK: Erlbaum,1994.
7. Wells A. Emotional disorder and metacogni-tion: innovation cognitive therapy, Chichester.UK: Wiley 2000.
8. Wells A. Meta-Cognition and Worry: A Cogni-tive Model of Generalized Anxiety Disorder.Behav Cogn Psychother 1995; 23(3) : 301-320.
9. Cartwright-Hatton S, Wells A. Beliefs about

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society262
Worry and Intrusions: The Meta-CognitionsQuestionnaire and its Correlates. J AnxietyDisord 1997; 11(3) : 279-296.
10. Benedetto L, Di Blasi D, Pacicca P. Worry andmeta-cognitive beliefs in childhood anxietydisorders. Mediterranean J Clin Psychol 2013;1(3).
11. Wells A, Carter K. Preliminary tests of a cogni-tive model of generalized anxiety disorder.Behav Res Ther 1999; 37(6) : 585-594.
12. Nassif Y. Predictors of pathological worry.Unpublished M.Phil. Thesis. University ofManchester, UK 1999.
13. American Psychiatric Association. Diagnosticand statistical manual of mental disorders (3rded., rev.). Washington, DC: Author 1987.
14. Purdon C. Metacognition and the persistenceof worry. Paper presented at the Annual Con-ference of the British Association of Beha-vioural and Cognitive Psychotherapy, Instituteof Education, London: UK 2000.
15. Davey GCL, Jubb M, Cameron C. Catastrophicworrying as a function of change in problem-solving confidence. Cogn Ther Res 1996; 20 :333–344.
16. Sheikh M, Saadat SH, Sarabandi H, TabatabaeeSM, Karimian A. Comparing metacognitivebeliefs and worry in patients with anxiety,depression and non-patients. Der PharmaciaSinica 2013; 4(6) : 59-65.
17. World Health Organization. The ICD-10classification of mental and behaviouraldisorders: diagnostic criteria for research.Geneva: World Health Organization 1993.
18. Sheehan DV, Lecrubier Y, Sheehan KH,Amorim P, Janavs J, Weiller E, HerguetaT, Baker R, Dunbar GC. The Mini-InternationalNeuropsychiatric Interview (M.I.N.I.): thedevelopment and validation of a structureddiagnostic psychiatric interview for DSM-IVand ICD-10. J Clin Psychiatry 1998; 59 Suppl20 : 22-33; quiz 34-57.
19. Goldberg D. The detection of psychiatric illnessby questionnaire: A technique for the identifi-cation and assessment of non-psychoticpsychiatric illness. London, New York: OxfordUniversity Press 1972.
20. Goldberg D, Williams P. A user’s guide to theGeneral Health Questionnaire. National
Foundation for Educational Research (NFer)Nelson: Windsor 1988.
21. Gautam S, Nijhawan M, Kamal P. Standardi-zation of Hindi version of Goldberg’s GeneralHealth Questionnaire, Indian J Psychiatry.1987; 29(1) : 63-6.
22. Varkal M, Yalvac D, Tufan F, Turan S, CengizM, Emul M. Metacognitive differences betweenelderly and adult outpatients with generalizedanxiety disorder. Eur Geriatr Med 2013; 4(3) :150-153.
23. Ellis D, Hudson J. The Metacognitive Modelof Generalized Anxiety Disorder in Childrenand Adolescents. Clin Child Fam Psychol Rev2010; 13(2) : 151-163.
24. Bahrami F, Yousefi N. (2011). Females are moreanxious than Males: A Metacognitive Perspec-tive. Iran J Psychiatr Behav Sci 2011; 83-90.
25. Wells A, Welford M, King P, Papageorgiou C,Wisely J, Mendel E. A pilot randomized trialof metacognitive therapy vs applied relaxationin the treatment of adults with generalizedanxiety disorder. Behav Res Ther 2010; 48(5) :429-434.
26. Wegner D, Schneider D, Carter S, White T.Paradoxical effects of thought suppression. JPers Soc Psychol 1987;53(1):5-13.
27. Purdon C. Thought suppression and psycho-pathology. Behav Res Ther 1999; 37(11) : 1029-1054.
28. Papageorgiou C, Wells A. Metacognitive beliefsabout rumination in recurrent major depression.Cogn Behav Pract 2001; 8(2) : 160-164.
29. Andor T, Gerlach A, Rist F. Superior perceptionof phasic physiological arousal and the detri-mental consequences of the conviction to bearoused on worrying and metacognitions inGAD. J Abnorm Psychology 2008; 117(1) :193-205.
30. Borkovec TD, Roemer L. Perceived functionsof worry among generalized anxiety disordersubjects: Distraction from more emotionallydistressing topics? J Behav Ther Exp Psychiatr1995; 26(1) : 25-30.
31. Tallis F, Davey GCL, Capuzzo N. The pheno-menology of non-pathological worry: a preli-minary investigation. In: G.C.L. Davey & F.Tallis (Eds.), Worrying: Perspectives on Theory,Assessment and Treatment. Chichester, UK:

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 263
Wiley 1994.32. Wells A, Papageorgiou C. Social phobia:
Effects of external attention on anxiety, nega-tive beliefs, and perspective taking. Behav Ther1998; 29(3) : 357-370.
33. Wells A, Carter K. Further tests of a cognitivemodel of generalized anxiety disorder: Meta-cognitions and worry in GAD, panic disorder,social phobia, depression, and nonpatients.
Behav Ther 2001; 32(1) : 85-102.34. Gwilliam P, Wells A, Cartwright-Hatton S. Does
meta-cognition or responsibility predictobsessive–compulsive symptoms: a test of themetacognitive model. Clin Psychol Psychother2004; 11 : 137-144.
35. Barahmand U. Metacognitive Profile in anxietydisorder. Psychiatr Res 2007; 240-243.
Errata
The authors have updated the list of contributors in the following articlepublished in 2018 issue and must be referenced as – “Shweta Singh, FauziaJawaid Kazi, Amit, Arya, Pawan Kumar Gupta, Suyash Dwivedi. A study ofparenting style and coping strategies in mothers of children and adolescentwith ADHD, 2018; 21(2) : 386–390.”

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society264
Co-Morbidity of Attention Deficit HyperactivityDisorder in Dyslexic School going
Children in JaipurRajinder Pal Singh,1 Manju Bhaskar2
Department of Psychiatry, 1Global Hospital, Bhatinda, Punjab and 2 MGMCH, Jaipur, RajasthanContact: Manju Bhaskar, E-mail: [email protected]
Original Article
IntroductionDyslexia is defined as difficulty in learning to
read despite conventional instruction, adequateintelligence, and socio-cultural opportunity.1 It is oneof the common learning disability with a prevalenceranging from 5 to 17.5% among school agechildren.2 Dyslexic people often have a natural talentfor any of the arts (such as music, dance, drawing,or acting). They often possess capability to seepatterns in noise, which helps them to producemundane into something more interesting andexciting.3
The most common childhood psychiatric
disorders reported in dyslexia is Attention-DeficitHyperactivity Disorder (ADHD); Up to 25% ofchildren with dyslexia also have ADHD; 15-30%children with ADHD have reading disorder.4
Attention Deficit Hyperactivity Disorder(ADHD) and Reading Disorder (RD) are two ofthe most frequent childhood developmentaldisorders. Each of them affects between 6-9% ofschool going children, although these percentagesdecline to 5% when the DSM-IV-TR (2000) criteriais applied. Attention Deficit Hyperactivity Disorder(ADHD) is a common neurodevelopment disorderof childhood associated with substantial cognitive,
Abstract
Introduction: Attention Deficit Hyperactivity Disorder (ADHD) and Reading Disorder(RD) are two of the most frequent childhood developmental disorders. Dyslexia and ADHDco-occur more frequently than expected by chance, with 25–40% of children with onedisorder meeting criteria for the other. Material and methods: This cross-sectional studyincluded total of 800 children from a CBSE affiliated coeducational public school atJaipur from the period between April 2013 to August 2014. Research tools used were -Specific Learning Disability -Screening Questionnaire (SLD-SQ), Malin’s Intelligence Scalefor Indian Children (MISIC), Diagnostic Test for Reading Disorder. (DTRD), ADHD Scale,Diagnostic criteria for Attention-Deficit/Hyperactivity Disorder (DSM-4 TR).All thestatistical analysis was done with the help of MS excel and Premier of biostatistics. Results:The prevalence of dyslexia was 7.43% in the present study, being higher in male children.The study found statistically significant relation of dyslexia with family type, family historyof psychiatric illness.14.52% of dyslexic children in the sample were found to have co-morbid ADHD. Conclusions: Children suffering from Dyslexia should be thoroughlyassessed for Attention-Deficit/Hyperactivity Disorder and managed accordingly for betteroutcome.
Keywords : Dyslexia, Attention-Deficit/Hyperactivity Disorder, Malin’s Intelligence Scalefor Indian Children

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 265
family, social, behavioral, and academic impairment.ADHD in childhood occurs in an estimated 3%–7% of school-aged children.5 It is characterized bypersistence of hyperactivity, impulsivity and attentiondeficit.6 The worldwide prevalence rate of childhoodADHD has been estimated to 3.40–5.29% in meta-analyses.7,8
The co-morbidity between dyslexia and ADHDhas been well established. Dyslexia and ADHD co-occur more frequently than expected by chance,with 25–40% of children with one disorder meetingcriteria for the other.9
The causes of co-morbidity between ReadingDisorder (RD) and ADHD remain uncertain. Somelongitudinal studies suggest that attention deficits leadto reading problems later because they interfere withreading instruction10 whereas others suggest thatearly reading difficulties also predict later attentionproblems.11 A third possibility is that RD and ADHDmay be due to a shared risk factor that increasesrisk for both disorders.
Aim and Objectives• To find out the prevalence of dyslexia in
school going children.• To find out the relationship of socio-
demographic factors with dyslexia.• To find out the prevalence of ADHD as a
co-morbidity, if any, with dyslexia.
Material and MethodsThis study was carried out in Department of
Psychiatry, Mahatma Gandhi Medical College andHospital, Jaipur from April 2013 to August 2014.The study protocol was approved by the EthicsCommittee of Mahatma Gandhi Medical Collegeand Hospital. Permission from the Principal of theschool and a written informed consent was takenfrom the parents before starting the study.
Sample size: A total of 800 children; 500students from class 3rd and 4th and 300 in class 5th
from a CBSE affiliated coeducational public schoolat Jaipur were enrolled in this study. The pre-tested,structured dyslexia screening questionnaire wasused.
Methodology:Various research tools wereused to conduct the study are –
A. Specific Learning Disability – ScreeningQuestionnaire (SLD-SQ)12
It is a 12 item brief screening instrument inwhich answers are to be given in either ‘yes’or ‘no’ with cut of score 4 and any totalscore above the cut off score indicatespossibility of SLD.
B. Malin’s Intelligence Scale for IndianChildren (MISIC)13
It is an Indian adaptation of WISC(Wechsler’s Intelligence Scale for children).The test consists of 11 subtest divided intoverbal and performance group. Thesesubtests maybe administered in any orderconvenient for rapport. Only 10 tests -5 fromeach group are required for completescoring.
C. Diagnostic Test for Reading Disorder(DTRD)14
It is an individually administered instrumentfor diagnosing the reading disorders inchildren aged 8 through 11 years. A child’sperformance on the items indicate theadequacy/inadequacy with regard to thefunctioning of his/her cognitive processes.The scored on individual items are inter-preted in combination with the scores onthe other items. It aims at measuringthrough 8 items at two levels.
D. ADHD Scale.15
This scale has been developed on the basisof APA DSM IV. It has 3 subscales whichreflect a conceptualization of relationshipamong three categories, namely, inattention,hyperactivity & impulsivity.
E. Diagnostic criteria for Attention-Deficit/Hyperactivity Disorder (DSM-IV TR).
The study was conducted in three phases. Thephase 1, which was a specially designed Performa,was given to the parents and data on SpecificLearning Disability, a Screening Questionnaire(SLD-SQ) was obtained from the parents with thehelp of clinical psychologist. In phase 2, the childrenwho scored four and above on SLD-SQ were furtherevaluated for Intelligence Quotient using Malin’sIntelligence Scale (MISIC) by taking help of clinicalpsychologist and then they were assessed onDiagnostic Test for Reading Disorder (DTRD) tomake a diagnosis of reading disorder. In Phase 3,those children who were found to have readingdisorder were screened for co-morbidity of ADHD

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society266
through ADHD scale. Simultaneously, a confirmdiagnosis of ADHD was made by DSM-4 TRcriteria for children who were positive on ADHDscale.
Statistical analysisAnalysis of the result was done by calculating
the frequencies and percentages of the variablesrelating to socio-demographic factors of the totalsample. Data obtained with the help of screeningquestionnaires, IQ assessment, Diagnostic tests andco-morbidity were analyzed by calculating Chi-square, Mean and Standard Deviation. In order tofind out the significance of difference on variousscores in the two groups, student t-test was used.All the statistical analysis was done with the help ofMS excel and Premier of biostatistics.
ResultsOut of 800 children, parents of 42 children did
not give their consent to participate in the study and18 children in 3rd standard were found to be belowthe age of 8 years, so they were excluded from thisstudy. Thus, the total sample consisted of 740children out of which 478(63%) were males and262(37%) females. The prevalence of readingdisorder, i.e., Dyslexia was 7.43% in the presentstudy. The prevalence of Dyslexia was higher inmale children, i.e., 81% while only 19% femalechildren were dyslexic. Out of 740 children 402(59%) in non-dyslexic group were in the age groupof 10-11 years, whereas in dyslexic group subjectswere approximately equally distributed in all the fourage groups (22%, 27%, 27% and 24% respectively).
Table-1: Distribution of the children in thenon-dyslexic and dyslexic group according to
their age
Age Non-Dyslexic Dyslexic(N=685) (N=55)
8 years 165 (24%) 12 (22%)9 years 118 (17%) 15 (27%)10 years 282 (41%) 15 (27%)11 years 120 (18%) 13 (24%)
Table 1 shows that majority of the subjects i.e.402 (59%) in Non-Dyslexic group were in the agegroup of 10-11 years, whereas in Dyslexic group,subjects were approximately equally distributed inall the four age groups (22%, 27%,27% and 24%
respectively). It was found to be statistically non-significant.
Table-2 : Comparison of birth order innon-dyslexic and dyslexic children
Birth Order Non-Dyslexic Dyslexic(N=685) (N=55)
Only child 64 (9%) 2 (3.6%)First child 289 (42%) 33 (60%)Last child 255 (37%) 15 (27.4%)Other 77 (12%) 5 (9%)
It is evident from table 2 that 64 (9%) childrenin Non-Dyslexic group were only child of theirparents followed by 289 (42%) first born, 255 (37%)were last born and 77 (12%) other in Non-Dyslexicgroup. In the Dyslexic group, 2 (3.6%) were onlychild followed by 33 (60%) first order, 15 (27.4%)last born and 5 (9%) other order children. Thedifference between the two groups was notstatistically significant.
Table-3: Comparison of family type in non-dyslexic and dyslexic children
Family Type Non-Dyslexic Dyslexic(N=685) (N=55)
Joint family 461 (67%) 45 (82%)Nuclear family 224 (33%) 10 (18%)

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 267
Table 3 shows comparison between the twogroups with respect to family type. 461 (67%)children in non-dyslexic group belonged to joint familyand 224 (33%) belonged to nuclear family whereasin dyslexic group 45 (82%) children were from jointfamilies and 10 (18%) belonged to nuclear family.The difference was statistically significant betweenthe two groups.
Table-5: Significance of difference in SLD-SQscores in dyslexic children by parents and
teachers
Screening Total Score Mean S DPerson
Parents 317 5.76 2.134Teachers 411 7.47 1.73
Table 5 shows that there exists a highly signi-ficant difference in reporting of learning disabilities(which includes dyslexia) on SLD-SQ by parentsand teachers as t-ratio is significant at 0.000 level.Mean scores indicate that teachers showed moreaccuracy in reporting reading disorder in comparisonto parents. This indicates that reporting of teachersis more reliable.
Table-4 : Comparison of family history ofpsychiatric illness in non-dyslexic and
dyslexic childrenH/O Psychiatric Non-Dyslexic DyslexicIllness in Family (N=685) (N=55)
Absent 683 (99.7%) 52 (94.5%)Present 2 (0.3%) 3 (5.5%)
Table 4 shows that in 683 (99.7%) Non-Dyslexicand 52 (94.5%) Dyslexic children, there was nofamily history of psychiatric illness whereas 2(0.3%) Non-Dyslexic and 3 (5.5%) Dyslexicchildren had positive family history of psychiatricillness. The difference between the two groups wasstatistically highly significant.
Table-6: Significance of difference in verbaland performance IQ on MISIC of dyslexic
children
Intelligence Total Score Mean S DQuotient
Verbal IQ 4731 86.02 4.9Performance IQ 6330 115.09 3.85
Table 6 shows that there is highly significantdifference in verbal and performance IQ on MISICas t-ratio is significant at 0.000 level. Mean scoresindicate that performance IQ is much higher thanverbal IQ in dyslexic children.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society268
child followed by 33 (60%) first order, 15 (27.4%)last born and 5 (9%) other order children. Thedifference between the two groups was notstatistically significant. Our findings are consistentwith several other studies.19,22,27 However Dhandaand Jagawathave reported a significant differencein birth order of dyslexia and their total samplestudied.21 Therefore, these results are in contradictionto the present ones.
In this study we also did a comparison betweenthe two groups with respect to family type. 461(67%) children in Non-Dyslexic group belonged toJoint family and 224 (33%) belonged to Nuclearfamily; whereas in Dyslexic group 45 (82%) childrenwere from Joint families and 10 (18%) belonged toNuclear family. The difference was statisticallysignificant between the two groups. This indicatesthat dyslexia and type of family are related. Ourfindings are in the accordance with the findings ofstudy done by Saviour and Ramachandra who havealso reported a preponderance of extended / jointfamily in their sample.23 On the contrary, Dhandaand Jagawat21 and Choudhary et al19 have reportedmore number of dyslexia/ SpLD children in nuclearfamilies.
We also found that in 683 (99.7%) Non-Dyslexic and 52 (94.5%) Dyslexic children, therewas no family history of psychiatric illness whereas2 (0.3%) Non-Dyslexic and 3 (5.5%) Dyslexicchildren had positive family history of psychiatricillness. The difference between the two groups wasstatistically highly significant. These results aresupported by the results of the study done byChoudhary et al who has also reported presence ofpsychiatric illness in the families of SpLD children.19
These findings have the indirect support (though inthe present study family history of dyslexia has notbeen included) of the studies done by others whohave reported impact of family history of dyslexia/SpLD on development of dyslexia/SpLD inchildren.23,35
We observed that there is a highly significantdifference in reporting of learning disabilities (whichincludes dyslexia) on SLD-SQ by parents andteachers as t-ratio is significant at 0.000 levels. Meanscores indicate that teachers showed more accuracyin reporting reading disorder (dyslexia) in comparisonto parents. This indicates that reporting of teachersis more dependable. This proves the hypothesis
Table-7: Co-morbidity of ADHD in dyslexicchildren
Dyslexia Positive Cases ADHD PercentageCo–Morbidity
55 8 14.52%
Data from above table revealed that ADHDco-morbidity prevalence was found to be 14.52%in dyslexic children in the present study.
DiscussionChildren have varied reading ages. Some read
at their real age while others read far above theirreal ages and some will read lower than their realages. In the present study, among the school childrenin Jaipur, the prevalence of dyslexia is found to be7.43%. These findings are supported by the studiesdone by Shayawitzet al, 17 Mogasale et al,18
Choudharyet al,19 and Berger et al20 who havereported the prevalence of dyslexia 11.2%, 7.47%,from 6.9% to 9.0%, 6.3%, around 7% and 9.9%respectively. However various other authors havereported a prevalence of dyslexia 2.26% in Englishmedium schools and 3.36% in Hindi medium schools,2.7%, 28.07%, 27.8% and 33% respectively.21-25
These differences may be due to the difference inmethods and tools used or sample taken fromdifferent geographical areas that varied with respectto age, language and size of the sample.
In this study, prevalence of dyslexia wasobserved more among males being 81% and only19% females were dyslexic which is in consistentwith other studies.26-32 However Tomblin et al33 andCecila et al34 reported a little difference in theprevalence of Dyslexia / SpLD (Specific LearningDifficulty) in boys and girls, there by indicatecontradiction.
We found that dyslexic group were approxi-mately equally distributed in the age groups of 8, 9,10 and 11 years and there was no significantdifference among different ages and presence ofreading disorder which is in consistent with variousauthors who all have reported the prevalence oflearning disabilities in age group of 8-11 years.19,21,24
We also found that 64 (9%) children in Non-Dyslexic group were the only child of their parentsfollowed by 289 (42%) who were first born, 255(37%) were last born and 77 (12%) were others,whereas in the Dyslexic group 2 (3.6%) were only

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 269
2(R).Our findings are strongly supported by thestudies done by other authors who has also reportedthat sensitivity of the teachers in screening ofdyslexia/ SpLD is more useful than parents inscreening children for dyslexia/SpLD though onecannot solely rely on them.17,36 This can be consideredas a caution. Use of diagnostic tool should be stronglyrecommended after screening.
In this study, the significance of difference inverbal and performance IQ on MISIC was found.The t-ratio indicates significance at 0.000 levels.Mean scores indicate that performance IQ is muchhigher than verbal IQ in dyslexic children. Hencehypothesis 2 (S) is proved and correlates with thestudies done by other authors who have alsoindicated a difference in verbal and performanceIQ.23,36
Our study reveals ADHD co-morbidity indyslexic children. Prevalence of ADHD co-morbidity was found to be 14.52% in dyslexicchildren in the present study. Therefore, thehypothesis 3 stating ADHD will be present as co-morbid illness with dyslexia is proved. These findingsare supported by majority of the studies Gilger et al.(1992) done in past in which prevalence of ADHDco-morbidity is reported to be between 11-40%.4,27
ConclusionReading disorder and ADHD are chronic
conditions that have a significant impact on academicdevelopment and educational outcome. Becausemost of the children with these difficulties spend asignificant proportion of time in both specialeducation and regular classroom environment,educators in both settings should receive specifictraining on the characteristics and causes of bothdisorders their long term implications and theinterventions most likely to be effective.
Limitations• The sample was taken from only one school;
therefore, the findings cannot be genera-lized.
• The study would have been more informa-tive if it was extended to secondary andsenior secondary levels.
References1. Critchley M, Critchley E. Dyslexia Defined.
London: Heinemann 1978.2. DeFries JC, Fulker DW, LaBuda MC. Evidence
for a genetic aetiology in reading disability oftwins. Nature 1987; 329(6139) : 537.
3. Sherman G. Can neuroscience help to demystifydyslexia, Schwats learning; 2007. <http://world.schwablearning.org/articles>.
4. Sadock BJ, Sadock VA. Synopsis of Psychiatry,10th Ed. Philadelphia: Lippincott Williams &Wilkins 2007; 1158-69.
5. Bird HR, Yager TJ, Staghezza B, Gould MS,Canino G, Rubio-Stipec M. Impairment in theepidemiological measurement of childhoodpsychopathology in the community. J Am AcadChild Adolesc Psychiatry 1990; 29(5) : 796-803.
6. Riglin L, Collishaw S, Thapar AK, DalsgaardS, Langley K, Smith GD, Stergiakouli E,Maughan B, O’donovan MC, Thapar A. Asso-ciation of genetic risk variants with attention-deficit/hyperactivity disorder trajectories in thegeneral population. JAMA Psychiatry 2016;73(12) : 1285-92.
7. Polanczyk G, de Lima MS, Horta BL,Biederman J, Rohde LA 2007. The worldwideprevalence of ADHD: a systematic review andmeta-regression analysis. Am J Psychiatry164(6) : 942–8.
8. Polanczyk GV, Salum GA, Sugaya LS, Caye A,Rohde LA. Annual Research Review: A metaanalysis of the worldwide prevalence of mentaldisorders in children and adolescents. J ChildPsychol Psychiatry 2015; 56(3) : 345-65.
9. August GJ, Garfinkel BD. Comorbidity ofADHD and reading disability among clinic-referred children. J Abnorm Child Psychol 1990;18(1) : 29-45.
10. Fergusson DM, Horwood LJ. Attention deficitand reading achievement. J Child PsycholPsychiatry 1992; 33(2) : 375-85.
11. McGee R, Prior M, Williams S, Smart D, SansonA. The long term significance of teacher ratedhyperactivity and reading ability in childhood:Findings from two longitudinal studies. J ChildPsychol Psychiatry 2002; 43(8) : 1004-17.
12. Sinha Uday K. Specific Learning DisabilityScreening Questionnaire (SLD-SQ), New Delhi:Psychomatrix 2012.
13. Malin AJ. Manual for Malin’s intelligence scale

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society270
for Indian children (MISIC). Lucknow: IndianPsychological Corporation 1969.
14. Mehta DH, Swarup S. The Diagnostic Test ofReading Disorders (DTRD). Asia PacificDisabilit Rehabilit J 2004; 15(1) : 50-8.
15. Jain N, Gunthey Ravi K. Attention DeficitHyperactivity Disorder. New Delhi: PrasadPsycho Corporation 2013.
16. Shaywitz SE, Shaywitz BA, Fletcher JM,Escobar MD. Prevalence of reading disabilityin boys and girls: Results of the ConnecticutLongitudinal Study. JAMA 1990; 264(8) : 998-1002.
17. Shaywitz SE, Shaywitz BA, Pugh KR, FulbrightRK, Constable RT, Mencl WE, Shankweiler DP,Liberman AM, Skudlarski P, Fletcher JM, KatzL. Functional disruption in the organization ofthe brain for reading in dyslexia. Proc Natl AcadSci 1998; 95(5) : 2636-41.
18. Mogasale VV, Patil VD, Patil NM, MogasaleV. Prevalence of specific learning disabilitiesamong primary school children in a South Indiancity. Indian J Pediatr 2012; 79(3) : 342-7.
19. Choudhary MG, Jain A, Chahar CK, Singhal AK.A case control study on specific learningdisorders in school going children in Bikaner city.Indian J Pediatr 2012; 79(11) : 1477-81.
20. Berger M, Yule W, Rutter M. Attainment andAdjustment in Two Geographical Areas: II—The Prevalence of Specific Reading Retarda-tion. Br J Psychiatry 1975; 126(6) : 510-9.
21. Dhanda A, Jagawat T. Prevalence and patternof learning disabilities in school children. DelhiPsychiatr J 2013; 16(2) : 386-90.
22. Donfrancesco R, Iozzino R, Caruso B, FerranteL, Mugnaini D, Talamo A, Miano S, Dimitri A,Masi G. Is season of birth related todevelopmental dyslexia?. Ann Dyslexia 2010;60(2) : 175-82.
23. Saviour P, Ramachandra NB. Modes of genetictransmission of dyslexia in south Indian families.Indian J Human Genet 2005; 11(3) : 135-139.
24. Siddqui S, Tripathi N. Identification and Assess-ment of Children with Dyslexia in AllahabadCity. Universal J Psychol 2014; 2(6) : 205-11
25. Williams S, McGee R. Reading attainment andjuvenile delinquency. J Child Psychol Psychiatry1994; 35(3) : 441-59.
26. Roongpraiwan R, Ruangdaraganon N,Visudhiphan P, Santikul K. Prevalence andclinical characteristics of dyslexia in primaryschool students. J Med Assoc Thailand 2002;85 : S1097-103.
27. Karande S, Venkataraman R. Self-perceivedhealth-related quality of life of Indian childrenwith specific learning disability. J Postgrad Med2012; 58(4) : 246.
28. St. Sauver JL, Katusic SK, Barbaresi WJ,Colligan RC, Jacobsen SJ. Boy/girl differencesin risk for reading disability: potential clues?. AmJ Epidemiol 2001; 154(9) : 787-94.
29. Shifrer D, Muller C, Callahan R. Disproportion-ality and learning disabilities: Parsing apart race,socioeconomic status, and language. J LearningDisabil 2011; 44(3) : 246-57.
30. Flannery KA, Liederman J, DALY L,SCHULTZ J. Male prevalence for readingdisability is found in a large sample of black andwhite children free from ascertainment bias. JInt Neuropsychol Soc 2000; 6(4) : 433-42.
31. Lewis C, Hitch GJ, Walker P. The prevalenceof specific arithmetic difficulties and specificreading difficulties in 9 to 10 year old boys andgirls. J Child Psychol Psychiatry 1994; 35(2) :283-92.
32. Rutter M, Yule W. The concept of specificreading retardation. J Child Psychol Psychiatry1975; 16(3) : 181-97.
33. Tomblin JB, Records NL, Buckwalter P, ZhangX, Smith E, O’Brien M. Prevalence of specificlanguage impairment in kindergarten children.J Speech language Hearing Res 1997; 40(6) :1245-60.
34. Cecilia MR, Vittorini P, Cofini V, di Orio F. ThePrevalence of Reading Difficulties amongChildren in Scholar Age. Styles Communication2014; 6(1) : 18-30.
35. Fisher SE, Smith SD. Progress towards theidentification of genes influencing developmentaldyslexia. In: Dyslexia: Theory and GoodPractice. London: Whurr Publishers 2001; 39-64.
36. Arun P, Chavan BS, Bhargava R, Sharma A,Kaur J. Prevalence of specific developmentaldisorder of scholastic skill in school students inChandigarh, India. Indian J Med Res 2013;138(1) : 89.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 271
Management of different domains of AggressiveBehaviour of Persons with Mental Illness (PMI)by Caregivers in both hospital and home settings
Nibedita Banerjee,1 SandhyaGhai,2 Renu Sharma,3 D. Basu4
NINE, PGIMER1,2,3 Department of Psychiatry, PGIMER, Chandigarh-1600124
Contact: Nibedita Banerjee, E-mail: [email protected]
Original Article
IntroductionAggression means a feeling of anger or
antipathy which can result in hostile or violentbehaviour.1 Aggressive behaviour is most commonamong psychiatric patients because they are havingaggressive personality trait as well as inability tocontrol anger because of illness.2 Aggression isbroadly divided into two aspects-affective (or
reactive aggression) and instrumental aggression.Affective or reactive aggression means a kind ofaggression which is associated with doing orshowing some negative affect (like anger). Instru-mental aggression means aggressive behaviourwhich are intended to achieve goal.3 In most of thecases patient himself,care givers and health careprofessionals becomes victim of patient’s
Abstract
Background : Anger is a normal human emotion which, if handled appropriately and expressedassertively, can provide an individual with a positive strength to solve problems and take decisionsconcerning life situations. Anger becomes aggression when it is not expressed appropriately.Aggressive behaviour can lead to so many harmful behaviour including violence thus representsmost challenging phenomenon in psychiatric in-patient care. It also further intensifies stigmatowards patient with mental illness.So it is important to reduce the impact of aggression andhelp the person with mental illness to live a better and productive life. Aim: To assess theeffectiveness of brief intervention package among caregivers in reducing aggressive episodesof Person with mental illness (PMI) in psychiatric unit of a tertiary care hospital, Chandigarh.Material and Methods: The research approach used was quantitative and design was preexperimental. Total enumeration sampling technique was used for this study. Total 48 caregiverswho were willing to participate were registered for this study. The tool used for data collectionwas interview schedule. Data collected was analyzed by using descriptive and inferentialstatistics. Results:Out of 48 caregivers, 50% samples were from the age group of 41-60 yearswith mean ± SD= 44.35 ± 13.737 and range 20-79. Among them 58.3% were female and 87.5%were married. Modified Overt Aggression Scale (MOAS) was applied to assess changes inaggression score after intervention. The result showed that there was significant improvementin post interventional MOAS score (p<0.05). 18.7% patients had severe aggression in preintervention assessment but in post test no one reported of having severe aggression. Conclusion:Findings revealed that improving knowledge and skills of caregivers can reduce the episodesof aggressive behaviour among person with mental illness. It is recommended that study needto be conducted on large scale among persons with mental illness to know the current incidenceof aggressive episodes.
Keywords : Aggressive behaviour, Persons with mental illness (PMI), Caregivers.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society272
aggressive behaviour.Aggressive behaviour in the hospitals can
occurin any form like using physical strengthdeliberately, doing verbal and physical abuse tocaregivers and other staff which sometimes canresults in physical or psychological harm towardsself or others. Literature on causes of aggressivebehaviour among psychiatric patients showed someconflicting information where few factors aremostly associated with patient’s aggressivepersonality trait or innate tendency for aggression.and others showed that socio-demographicfactorssuch as age, sex, marital status, diagnosis,psychopathologyassociated with crime behaviourare linked with patient’s aggressive behaviour.4
Aggression if not resolved it can turn intoviolence. Aggression can be in different forms likeverbal aggression, aggression against property, autoaggression and physical aggression. Though verbalaggression is milder form of aggression, it isimportant to mention that emotional impact ofcontinuous exposure to verbal aggression is equallydistressing as a single exposure to physicalaggression.5
Loughland et al revealed in their study thatalmost 80% caregivers of psychiatric patient hadexperienced moderate and severe level ofaggressive behaviour from their patient withpsychosis. And most of the time it was in verbalaggression form. It has also been reported that onein five psychiatric patients have fear for their ownlives and became concern about re occurring ofviolence again.6
Caregivers have very little knowledge andawareness about how to manage violent behaviourof psychiatric patient. Mental illness has becomestigmatized in most of the countries. In maximumcases, people with this illness are often subjectedto be tortured. Sometimes, the caregivers feelburdened because of their patient’s behaviour. Theyfeel afraid too. A study was conducted oncaregiver’s attitude towards patient with mentalillness and their perceived stigma. It reported thatinterventions targeting for these high-riskpopulations/communities might be beneficial as ithelps to build a positive attitude and overcomeperceived social stigma.7
The consequences of aggressive incident havesome negative impact on caregivers and other
family members and it also further intensifies stigmatowards patient with mental illness. Sometimes evenit can compromise care required and available forthose patients. So it is important to analyze factorsresponsible for origin of violent behaviour and toteach care givers regarding necessary skills andstrategies to reduce the impact of violent behaviourand help the persons with mental illness to live abetter and productive life.
Material and MethodsResearch approach used in this study was
quantitative and design was pre experimental. Totalenumeration sampling technique was used. Thesample population was caregivers of person withmental illness registered in psychiatry unit (bothward and OPD) of Tertiary care hospital ofChandigarh. Sample size were 48. Inclusivesampling criterion of the study was participants whowere willing to take part in study. Exclusion criteriawere caregivers who had previous psychotic illness.Tools used for study were prepared after extensiveliterature review and validation from experts. Toolsselected and used for data collection were (1)Subject’s socio demographic profile (2) Clinicalprofile of patients 3) Modified Overt AggressionScale (MOAS) for assessing severity of aggression.All subjects in the study were explained aboutresearch protocol. Permission was taken fromInstitutes ethics committee and written informedconsent was taken from each subject.Confidentiality and privacy of each subject wasmaintained. Full autonomy was given to participantto be withdrawn from study at any time. Preinterventional assessment was done for 15-20minutes for each participant. Intervention was giventhrough “brief intervention package” prepared byextensive literature review. One protocol was madewhich contained definition of violent behaviour,causes of aggressive behaviour, sign and symptomsof aggressive behaviour, management andprevention of aggressive incident in both hospitaland home settings. And intervention was given byinformation booklet in both Punjabi and Hindilanguage. After 15 days of intervention, again posttest was conducted by using same criteria of preintervention assessment. Scoring was doneaccording to selected criteria. The analysis was doneby using SPSS version 20.0.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 273
ResultsTable 1 depicts that half of the subjects were
in age group of 41- 60 years (50%). Mean age ofparticipants was 44.35 ± 13.7 37.5 8.3% subjectswere female. Out of 48 participants 33.3% weremothers, 41.7% were having high school educationfollowed by 27% having graduation and above and41.7% participants were house wives. Per capitaincome of subjects were within range Rs 500-3000with mean per capita income 7671.94 ± 7339.38.50% subjects had 1-5 year of duration of stay withthe patient.
Table-1: Socio-demographic variables ofcare-givers
N= 48
S. Variable n (%)No.
1. Age (in years)*a) 21-40 20 (41.7)b) 41-60 24 (50.0)c) 61-80 4 (08.3)
2. Sexa) Male 20 (41.7)b) Female 28 (58.3)
3. Relationship statusa) Mother 16 (33.3)b) Spouse 10(20.8)c) Siblings 9 (18.8)d) Father 7 (14.6)e) Son 4 (08.3)f) Uncle 2 (04.2)
4. Educational statusa) No formal education 2 (04.2)b) Primary school 6 (12.5)c) Middle school 13 (27.1)d) High school 20 (41.7)e) Graduation and above 13 (27.0)
5. Occupational statusa) Professional 03 (06.3)b) Skilled worker 06 (12.5)c) Unskilled worker 13 (27.1)d) Housewife 20 (41.7)e) Unemployed 04 (08.3)f) Others (Retired) 02 (04.1)
9. Per capita income**a) <985 3 (06.2)b) 986-1971 8 (16.7)c) 1972-3286 6 (12.6)d) 3287-6573 10 (20.7)e) >6574 21 (43.8)
10. Duration of stay with the patient (year)***a) < 1 12 (25.0)b) 1-5 24 (50.0)c) 6-10 8 (16.7)d) 11-15 2 (04.2)e) >16 2 (04.1)
* Mean ± SD = 44.35 ± 13.737, Range: 20-79** Mean ± SD= 7671.94 ± 7339.38, Range: 500-30000***Mean ± SD= 48.85± 56.173
Table No 2 describes the clinical profile ofpatients. According to care givers, patients were inthe age group of 20-80 years with mean age 34.17± 12.72. Most of the patients were in the age groupof 20-40 years (68.7%). In case of gender (sex),54.2% were female. According to diagnosis ofpatient, neurosis and psychosis found equal as 50%for each. Caregivers reported that 33% patients hadoccurrence of violent behaviour almost every dayfollowed by 20.8% had several times a week. Onasking about reasons related to violence, 50%caregivers reported that there were other reasons(altercation between family members, discordfamily relationship, not obeying command) forviolence.
Table -2: Clinical variable of patients
N=48S. Variables n (%)No.
1. Age (in years)*a) 20-40 33 (68.7)b) 41-60 13 (27.1)c) 61-80 2 (04.2)
2. Sexa) Female 26 (54.2)b) Male 22 (45.8)
3. Diagnosis of patienta) Psychotic 24 (50.0)b) Neurotic 24 (50.0)
4. Frequency of occurring violent behavioura) Everyday 16 (33.3)b) Several times a week 10 (20.8)c) Once a week 9 (18.8)d) Once a month 5 (10.4)e) 15 days a month 8 (16.7)
5. Duration of violent behaviour**a) 1- 5 min 46 (95.8)b) 6-10 min 2 (04.2)
6. Reason for violent behaviour:a) Auditory hallucination 04 (08.3)b) Panic attack 03 (06.3)c) Generalized anxiety disorder 09 (18.7)d) Phobia 08 (16.7)e) Others# 24 (50.0)
*Mean ± SD = 34.17 ± 12.72, Range: 19-67** Mean ± SD = 2.77±1.859, Range: 1-10# Altercation between family members, discord familyrelationship, not obeying command
Table No 3 depicts changes in pre and postintervention assessment of the Modified OvertAggression Scale (MOAS) among the patients. TheMOAS scale is divided into four domains verbal

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society274
aggression, aggression against property, auto aggre-ssion and physical aggression. The comparisons ofthe pre test and post intervention test scores of thesefour domains were done using pared t test. Theresult showed that total MOAS mean score in thepre test was 14.15 ± 13.381 and after interventionit was 5.83 ± 6.663 at <0.001 level of significance.It shows significant improvement in the MOASscore of the subjects after intervention. Further invarious domains of MOAS, in verbal aggressiondomain mean pre test score and range was 2.40 ±2.36 and 0-10 respectively. And after interventionmean post test score and range was 1.42 ± 1.127and 0-5 at 0.006 level of significance which showssignificant improvement after intervention. In caseof second domain aggression against property, meanpre test score and range was 2.96 ± 4.063 and 0-12and after intervention mean post test score and rangewas 2.10 ± 2.595 and 0-12 at 0.153 level of signi-ficance which shows there was no such differencein score of before and after intervention. In the thirddomain auto aggression, pre test mean score andrange was 5.69 ± 6.926 and 0-24 respectively andin post test the mean score and range became 1.81± 3.20 and 0-9 at <.001 level of significance whichshows significant improvement was seen before andafter giving intervention. In case of physicalaggression domain, pre test mean score and rangewas 3.25 ± 5.452 and 0-24 respectively and afterintervention post test mean score and range was.50 ± 1.571 and 0-8. So there is also significantimprovement seen in pre intervention and postintervention score with level of significance .001.
As per MAOS score 1-13 refers to mildaggression, 14-26 refers to moderate aggression and> 26 refers to severe aggression. Majority of theparticipants (58.3%) had score between 1-13 in pretest and 83.3% had same score in post test. 22.9%patients had moderate aggression in pre test andin post test 16.7% patient had moderate aggression.Only 18.7% participants had severe aggression inpre test. And in post test no one had severeaggression. So after intervention severity ofaggressive episodes were reduced.
DiscussionPresent study was undertaken with an objective
to find out impact of brief intervention package onaggression for caregivers to reduce the episodes of
aggression among persons with mental illness (PMI)of psychiatry unit, PGIMER, Chandigarh and toassess knowledge, practice and incidence regardingaggression and violent behaviour of psychiatricpatient.
Present study showed that 50% individuals hadpsychosis and 50% individuals had neurosis as adiagnosis and reason for their violent behaviourwere mainly altercation between family members,discord family relationship etc. But episodes ofviolent behaviour were same in both psychosis andneurosis. A similar study was conducted in Chicagoto observe relationship between psychoticsymptoms and subsequent physically aggressive
Table-3: Pre and post interventional ModifiedOvert Aggression Score (MOAS) among
subjectsDomain Pre test Post test #Paired t
Mean ± SD Mean ± SD dfrange range p value
Verbal aggression 2.40±2.32 1.42 ± 1.127 2.8680-10 0-5 47
0.006*Aggression 2.96 ± 4.063 2.10 ± 2.595 1.451against property 0-12 0-12 47
0.153Auto aggression 5.69± 6.926 1.81 ± 3.20 4.137
0-24 0-9 47<0.001*
Physical 3.25 ± 5.452 .50 ± 1.571 3.556aggression 0-24 0-8 47
0.001*Total 14.15±13.381 5.83 ± 6.663 4.806
0-51 0-26 47<0.001*
*p value= <0.05#paired t test
Figure-1: Pre intervention and post interventionMAOS score

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 275
Aggression&oldid=8963693012. A.S. Subathra Harikrishnan. Effectiveness of
Structured Teaching Program on Managementof Aggressive Patients among Staff Nurses atselected Psychiatric Hospitals, Hyderabad,Andhra Pradesh. Narayana Nurs J 2016; 5(1) :31–4.
3. Benjamin James Arlin. Aggression. Researchgate. [cited 2016 Jan 16]
4. Barling J1, Dupré KE, Kelloway EK. Predictingworkplace aggression and violence. Annu RevPsychol 2009; 60 : 671-92.
5. Bock TM. Assessment of attitudes related tothe management of aggression and violence infour psychiatric hospitals. Thesis presented infulfilment of the requirements for the degreeM Cur. (Nursing), Department of Interdisci-plinary Health Sciences, StellenboschUniversity. South Africa, March 2011 [cited2019 Jul 7].
6. Loughland C, Lawrence G, Allen J, et al.Aggression and trauma experiences amongcarer-relatives of people with psychosis. SocPsychiatry Psychiatr Epidemiol 2009; 44(12) :1031–1040.
7. Iseselo MK, Kajula L, Yahya-Malima KI. Thepsychosocial problems of families caring forrelatives with mental illnesses and their copingstrategies: a qualitative urban based study inDar es Salaam, Tanzania. BMC Psychiatry;2016 May 14 : 16. [cited 2018 Dec 26]
8. Gilley DW, Wilson RS, Beckett LA, Evans DA.Psychotic Symptoms and Physically AggressiveBehavior in Alzheimer’s Disease. J Am GeriatrSoc 1997; 45(9) : 1074–9.
9. Mehta JR, Mehta R, Singh N. A case controlstudy of aggressive behaviour in stable patientsof schizophrenia who have improved ontreatment and in normal and its effect on qualityof life. Int J Med Sci Clin Invent 2016; 3 : 1565-1574.
10. Iversen VC, Aasen OHF, Cüneyt Güzey I,Helvik A-S. Incidence of violent behavioramong patients in Psychiatric Intensive CareUnits. Eur J Psychiatry 2016; 30(1) : 67–78.
11. Sim MG1, Wain T, Khong E. Aggressivebehaviour - prevention and management in thegeneral practice environment. Aust FamPhysician 2011; 40(11) : 866-72.
behaviourfound that Disease condition foroccurring aggressive behaviour among psychiatricpatients may be psychosis or neurosis. Psychosisconditions like schizophrenia, delusional disorder.Neurosis conditions like OCD, phobia, panicanxiety disorder, generalized anxiety disorder etc.Precipitating factors may be impaired family rela-tionship, aggressive personality trait, environmentalproblem, existing condition etc.8
The present study revealed that among totalpatient 81% patient showed verbal aggression, 56%patient showed auto aggression and 37.5% patientshowed physical aggression. So numbers of patientswith verbal aggression were more than othercategory. Similar study was conducted whichreported that prevalence of mild aggression incontrol group (91.66%) was more than that ofpatient with experimental group (schizophrenia)(85%). Prevalence of physical aggression againstself was 18.33%, aggression towards object was48.33% and others were 63.33%.9
In present study 87.5% patient had no earlierhospitalization because of violence and 6.5% hadsingle hospitalization due to violence. A Same studywas conducted by Iversen C et al on incidence ofviolent behaviour among in patients of psychiatricintensive care unit in 2016 reported that patientswho have single hospitalization history become lessviolent than who had history of two hospitalizationepisodes.10
ConclusionIn the present study brief intervention package
for management of aggression was found effectivein reducing the episodes of aggression amongpersons with mental illness (PMI) as there wasstatistically significant difference in MOAS score(p<0.05) between pre intervention and postintervention assessment.Aggressive behaviourmainly occurs in that time, when a person is nottreated fairly by others. So if the caregivers can betaught about skills to manage aggressive behaviourof person with mental illness, episodes of aggressionand stigma would be less.11
References1. Aggression. In: Wikipedia [Internet]. 2019
[cited 2019 May 28]. Available from: https://en . wikip edia .org / w/ index . p hp ? t i t l e=

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society276
Assessment of hostility, suicidality and co-morbidpsychiatric disorders in patients presenting with
deliberate self-harmPoonam Bharti,1 Navkiran S. Mahajan,2 Ranjive Mahajan,3 Anshu Gupta4
Departments of Psychiatry1 and Pharmacology,4 Maharishi Markandeshwar Institute ofMedical Sciences and Research, Mullana, Ambala;
Department of Psychiatry,2,3 Dayanand Medical College and Hospital, LudhianaContact: Poonam Bharti, E-mail : [email protected]
Original Article
IntroductionDelibrate self-harm is ‘An act with non-fatal
outcome in which an individual deliberatelyinitiates a non-habitual behaviour, that withoutintervention from others will cause self-harm, ordeliberately ingest a substance in excess of theprescribed or generally recognized dosage, andwhich is aimed at realizing changes that the persondesires via the actual or expected physical
consequences.1 About 8,00,000 people die bysuicide worldwide every year, of these 1,35,000(17%) are residents of India, a nation with 17.5%of world population. Between 1987 and 2007, thesuicide rate increased from 7.9 to 10.3 per 100,000,with higher suicide rates in southern and easternstates of India.2-4 Deliberate self-harm is one of thetop five causes of acute medical admissions for bothmen and women.5
Abstract
Background: Deliberate self-harm (DSH) is one of the top five causes of acute medicaladmissions for men and women. In India, every minute there is a suicide attempt and completedsuicide every 7th minute with a suicide rate of 12 per lakh. In view of which the study wasplanned to explore the various factors and associated comorbid illness with the suicidal attempts.Materials and methods: The study included 125 patients presenting with DSH in D.M.C. andHospital, Ludhiana. Cases were drawn from psychiatry, casualty and referred inter departments.Excluding those who didn’t give consent and those who were too seriously ill. Cases wereevaluated by using Buss Durkee Hostility Inventory (BDHI), Overt aggression scale – modified(OSA-M), Pierce suicide intent scale (PSSI). Chi square test and correlation coefficient wasused to calculate and compute the results. Aims and Objectives: To assess the hostility andsuicidality in patients presenting with deliberate self-harm and its association with any co-morbid psychiatric illness and various other factors. Results: Majority of subjects were from20-29 years of age group which was found to be statistically significant. Majority of subjects(70.4%) presented with OPC ingestion which was found to be statistically significant. Majorityof the subjects (84.0%) presented with 1st attempt which was found to be significant. Irritability,verbal hostility (BDHI), irritability, aggression and suicidality (PSISS) were significantlyassociated with severity of intent of suicide. Conclusion: Early identification of suicidality,hostility among adolescents could be one of the preventive measures of DSH and treating theco morbid psychiatry illness associated with DSH will improve overall quality of the life of thesubjects.
Key Words: Co morbid illness, Deliberate self-harm, Hostility, Suicidality.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 277
Hostility in DSHSeveral studies have reported a relationship
between violence and suicide. In one study6 byMann et. al. the persons who attempted suicide hadsignificantly higher scores for lifetime aggressionthan those who did not. Longitudinal investigationshave demonstrated associations between suicideand self-reported aggression and between suicideand hostility. However, in the developmentalliterature, suicidal and violent behaviours have oftenbeen associated with two different types of under-lying psychopathology: internalizing problems andexternalizing behaviours. Internalizing problems,such as anxiety, depressions, and somatization, arestrongly associated with suicide. These actionsstand in contrast to externalizing behaviours, whichinclude violent and antisocial behaviours.
Risk Factors and EtiologyPotential risk factors for suicide attempts in
adolescents include female gender, psychopatho-logy especially a major depressive disorder,previous suicide attempts, hopelessness, recentstressful life events, suicide attempts by the familymembers or friends, chronic physical illness, familyviolence and dysfunction and lower academicachievement. west.6 There may be many risk factorsbehind deliberate self-harm, which may includemany psychiatric co-morbidities in form ofdepression, alcoholism, generalized anxietydisorders and adjustment disorders. Commonlyfemales present morewith deliberateself-harmthanmales. The relationships of younger adults aregenerally less stable and more prone to violencethan those of older adults and this may be vulnerablefactor for deliberate self-harm. The probable reasonbehind this may be due to academic relatedproblems and family issues.7 The most commonmethod of intentional self-harm in children andadolescents is by consumption of insecticidesusually precipitated by familial interpersonalproblems.8 Poisoning (36.6%), hanging (32.1%),and self-immolation (7.9%) were the commonmethods used to commit suicide and poisoning isthe commonest mode of attempt by the Indianpopulation.9
Violence in women appears to confer greaterrisk for suicide than violence in men. Roy reporteda similar phenomenon with respect to alcohol use
disorders in women. In a meta-analysis, theycalculated higher relative risks for suicideassociated with alcohol use disorders in women thanmen.10
Homicide and Suicide in DSHA homicide/suicide cluster was defined as one
or more homicides with the subsequent suicide ofthe perpetrator that occurred in Allen study from1985 through 1990. Of 67 homicide/suicide clustersidentified 63 (94%) were found through matchingdeath certificates by the last name of the homicidevictim(s) and the perpetrator or by county ofoccurrence for homicides and suicides that occurredon the same day (n=53) or through computersearches of two newspapers with state widecoverage (n=40); 30 homicide/suicide clusters werefrom both sources.11
It seems that many studies had compareddeliberate self-harm with hostile and impulsivebehaviour. Many studies had favoured directcorrelation of deliberate self-harm with impulsiveand violent episodes in DSH patients.Moreover,seriousness of DSH is also associated positivelywith hostile and violence incidences. In India, thereis hardly any study to compare hostility and violencein Deliberate self-harm patients and theirsignificance in future DSH. Hence, we planned thisstudy as initial attempt to explore further on theseareas in Indian set up. We also tried to assess recentsocio demographic factors effecting deliberate self-harm.
Aims and Objectives• To assess the hostility and suicidality in
patients presenting with deliberate self-harm.
• To study the association between hostilityand suicidality and any co morbidpsychiatric disorder in patients presentingwith DSH.
• To assess correlation between hostility andsuicidality.
Material and Methods
Sample:The study included 125 patients presented with
deliberating self-harm in multispecialty hospital inurban region (D.M.C. & Hospital, Ludhiana). The

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society278
study period was from November 2006 toNovember 2008 after obtaining the ethicalclearance.
Inclusion CriteriaCases of deliberate self-harm drawn from
psychiatry, casualty department and referred fromother departments in the hospital.
Exclusion CriteriaThose who were not willing to give the consent
and those who were too physically ill to undergodetailed interview. Statistical Analysis was done byusing Chi square test and correlation coefficientbetween hostility and suicidality was calculated.
Scales1. Socio-Demographic Proforma:
Included the name, age, gender, maritalstatus, education, locality status of thesubject as well as any co morbid psychiatricillness.
2. Buss Durkee Hospitality Inventory(BDHI):12
The BDHI developed by AH Buss and ADurkee in 1957. It is perhaps the bestknown inventory with 75 item anger andhostility questionnaire with a true falseformat. It is self-rated scale with eightsubscales assault, indirect hostility, irrita-bility, negativity, resentment, suspicion,verbal hostility and guilt. The BDHI wasdeveloped as a tool for clinical assessmentand to help in clinical research in the areaof anger and hostility.
3. Overt Aggression Scale - Modified(OAS-M):13
It was developed by Coccaro and colla-borators in 1991 to assess aggressivebehaviour in the patients including 25 itemssemi structured interview with ninesubscales. It is an observer rated scale.Aggression (verbal aggression, aggressionobject, aggression against others, autoaggression)Irritability (global irritability, subjectiveirritability), Suicidality (suicidal tendencies(ideation and behaviour), intent of attempt,lethality of attempt. Two different ways of
scoring are used in this scale, each one ofthe aggression subscales has 7 differentbehaviour which are listed in order ofseverity Scored separately by frequencyand multiplied by weight assigned (1 forverbal aggression, 2 aggression againstobjects, 3 aggression against others). OAS-M is short instrument relatively easy toadminister, and was developed from workwith aggressive patients.
4. Pierce Suicide Intent Scale (PSISS)14:This scale devised by Pierce in 1971, isclinician rated scale, to assess the intent forsuicide. The scale was designed, bearingin mind the need to be as objective aspossible. Item 1-6 are same as on Beckrating scale of suicidal intent and are scoredin a way as recommended by Beck. Item 7-10 are more of subjective in character and8 is included the beck. Item 10 was differentin than other, dealing not with self-injuryitself but with the patient reaction to it atthe time interview. It will clearly beinfluenced by the event occurring after theself-injury. But this was minimized byinterviewing the patient as soon as possibleafter the admission. Item 11-12 deal withthe medical risk assessing self-injury.Variables are rated as 3- point scale, 0- lowintent and less severity, 1- moderate intentand moderate severity and 2 severe intentand severity. Scoring is done as, low (0-3),moderate (4-10) and high (>11).
ResultsTable 1 Majority of subjects belongs to age
group of 20-29, which was found to be statisticallysignificant with age parameter (p value < 0.01highly significant). Out of 125 cases 72 (57.6%)were males and 53 (42.4%) were females.According to the marital status of the sample 46were married and 26 unmarried among malepopulation, 37 were married and 16 were unmarriedamong female population. Among males 27.8%businessmen presented with DSH which washighest among all other occupation and similarlyamong females homeworkers presented with DSHmore frequently than any other occupation (p value(> 0.001) highly significant. The distribution of

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 279
Table-1. Socio-demographic profile of the subjects
Character Category Males Females P valueN(%) N(%)
Age 10-19 7 (9.7) 8 (15.1) 0.00220-29 37( 51.4) 27 (50.9)30-39 16 (22.2) 10 (18.9)40-49 8 (11.1) 6 (11.3)50-59 3 (4.2) 1 (1.9)60-69 1 (1.4) 1 (1.9)
Gender 72 (57.6) 53 (42.4) 0.293Marital Status Married 46 (63.9) 37 (69.8) 0.488
Unmarried 26 (36.1) 16 (30.2)Occupation Business 20 (27.8) 1 (1.9)
Student 9 (12.50 13 (24.5)Household 0 (0) 30 (56.6)Skilled 15 (20.8) 5 (9.4)Unemployed 10 (13.9) 1 (1.9)Others 18 (25) 3 (5.7)
Education Postgraduate 1 (1.4) 1 (1.9) 0.548Graduate 6 (8.3) 6 (11.3)Higher Secondary 26 (36.1) 13 (24.5)Matric 27 (37.5) 19 (35.8)Below Matric 12 (16.7) 14 (26.4)
Locality Rural 48 (66.7) 25 (58.4) 0.29Urban 24 (33.3) 28 (41.6)
vTable-2: Various methods used for DSH by thesubjects
Method used for DSH N (%)OPC (organophosphate) 88 (70.4*)Celphos 6 (4.8)Wrist slashing 1 (0.8)Benzodiazepines 9 (7.2)Head Banging 10 (8)Other 11 (8.8)
Table 3. Showing distribution of casesaccording to the no. of attempts (total
subjects)No. of Attempt N %age
Single Attempt 105 84.0*Two Attempts 14 11.2Multiple Attempt 6 4.8
Total 125 100.0
Table-4: shows the distribution of casesaccording to the severity of intent on PSISS
PSISS N(%) P value
0.897Mild 23 (18.4)Moderate 78 (62.4)Severe 24 (19.2)Total 125 (100)
subjects as per their education status did not reveala significant result. As more number of subjectsfrom rural were found to be more prone to DSHbut the finding was not significant.
Table 2 shows methods used by subjects forDSH. OPC ingestion being significant and mostfrequently used method for deliberate self harm thanany other methods.
Table 3 shows distribution of cases accordingto the no. of attempts made. Majority presented with1st attempt which was significantly more commonthan 2nd or multiple attempts.
Table 4 shows the distribution of the subjectsaccording to the severity of suicidal intent. Out ofwhole population, majority had moderate intent(62.4%). About 18.4 % had mild intent and 19.2%had severe intent. It was found statisticallyinsignificant.
Table 5 The distribution of the subjectsaccording to the psychiatric disorders was done.The psychiatric co morbidity commonly seen in thepatients presenting with DSH were depression,bipolar mood disorder, substance dependence,adjustment disorder and many more psychiatricdisorders. None of the females presented withsubstance dependence. It was found that majority

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society280
of the subjects presenting with DSH were sufferingfrom depression followed by adjustment disorder,bipolar disorder and alcohol dependence.Statisticalsignificant association was seen with depression,alcohol dependence and bipolar disorder.
Table 6 the analysis of the results betweendifferent parameters of BDHI and with co morbidpsychiatric illness in patients presenting with DSHwas done. The mean score between the differentparameters of BDHI (assault, indirect hostility,irritability, negativism, resentment, suspicion,verbal) and different psychiatric co morbidity(depression, bipolar mood disorder, alcohol, opioiddependence, adjustment disorders and many more)was calculated. The p value was calculated (p>0.05)
Table-5: Distribution of cases according to thedifferent psychiatric disorders
Disorders Total p valueN (%)
Depression 45 (36) 0.002*Alcohol dependence 18 (14.4) 0.004*Opioid dependence 15 (12.0) 0.74Adjustment disorder 22 (17.6) 0.63Bipolar mood disorder 21 (16.8) 0.008*Others 4 (3.2) 0.24
Table-6: Analysis between different parameters on BDHI and psychiatric disorders in patientspresenting with DSH.
Disorders Assault Indirect hostility Irritability Negativism Resentment Suspicion Verbal
Mean ± SD Mean ± SD Mean ± SD Mean ± SD Mean ± SD Mean ± SD Mean ± SD
Depression 4.26 ± 1.38 5.13 ± 0.87 4.74 ± 1.81 2.11 ± 0.72 2.03 ± 0.91 3.13 ± 1.77 2.44 ± 1.09Alcohol dependence 3.77 ± 1.23 5.00 ± 1.08 5.69 ± 2.35 2.69 ± 0.94 2.15 ± 1.34 2.92 ± 1.65 2.36 ± 0.67Opioid dependence 4.50 ± 1.06 5.2 ± 0.70 4.38 ± 1.18 2.31 ± 1.18 2.38 ± 0.74 3.75 ± 1.28 2.41 ± 0.76Adjustment disorder 3.83 ± 1.58 5.11 ± 1.13 4.83 ± 1.82 2.44 ± 1.09 2.06 ± 1.05 3.28 ± 1.90 2.34 ± 0.85Bipolar mood disorder 4.09 ± 0.70 5.00 ± 1.26 4.73 ± 2.49 2.36 ± 0.67 1.91 ± 0.83 3.36 ± 1.80 2.03 ± .91Others 3.92 ± 1.01 5.11 ± 1.09 4.78 ± 1.37 2.41 ± 0.76 2.41 ± 1.09 3.24 ± 1.34 2.15 ± 1.34p value 0.57 0.99 0.60 0.35 0.55 0.91 0.84
Table-7: Analysis between different parameters on OAS and psychiatric disorders inpatients presenting with DSH
Disorders Aggression Irritability Suicidality
Mean ± SD Mean ± SD Mean ± SD
Depression 80.26 ± 16.14 6.00 ± 1.37 5.58 ± 1.26Alcohol dependence 74.38 ± 12.99 6.31 ± 1.31 5.00 ± 1.68Opioid dependence 72.88 ± 15.74 6.25 ± 1.28 5.75 ± 1.66Adjustment disorder 73.56 ± 14.79 6.44 ± 1.24 5.22 ± 1.26Bipolar mood disorder 78.64 ± 12.16 6.00 ± 1.54 5.45 ± 1.36Others 70.11 ± 11.23 6.16 ± 1.25 5.21 ± 1.32p value 0.50 0.87 0.77
which reflects that the patients can even presentwith DSH without having any co morbid psychiatricillness.
Table 7 The analysis of the results betweendifferent parameters (aggression, irritability andsuicidality) of OAS-M with the subjects presentingwith DSH having co morbid psychiatric illness wasdone. The mean score between the differentparameters of OAS-M and different psychiatric comorbidity (depression, bipolar mood disorder,alcohol, opioid dependence, adjustment disordersand many more) was calculated. The p value wascalculated (p>0.05) was not found to be statisticallysignificant. This reflects that the patients presentingwith DSH who scores high on aggression, irrita-bility parameter of OAS-m might not be sufferingfrom psychiatric disorder.
Table 8 the distribution of the subjectspresenting with DSH having co morbid psychiatricillness were done according to the severity ofsuicidal intent (PSISS) was done. It was found thatamong the subjects having mild intent, 26.08% weresuffering from depression. 13.4%, 4.34% presentedwith alcohol and opioid dependence respectively.17.39 had adjustment problem, 13.04% had bipolar

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 281
mood disorder. 4.34% were categorized in the grouphaving other psychiatric diagnosis. 21.73% werenot having any active psychiatric illness. Amongthe subjects with moderate intent, majority of thesubjects (32.5%) were suffering from depressivedisorder. 8.97%, 6.41% presented with alcohol,opioid dependence respectively. 11.53% had adjust-ment disorder. 7.69% were suffering from bipolarmood disorder. 1.28 % were categorized in thegroup of others. 32.05 % subjects presented withno active psychiatric illness. Among the subjectswith severe suicidal intent, majority of the subjects29.26% were suffering from depressive disorder and12.5% from bipolar mood disorder. 12.5%, 8.3%were cases of alcohol, opioid dependence respecti-vely. 4.16% were cases of adjustment disorder. 25%
Table-8: Distribution of subjects with psychiatric diagnosis on PSISS scale according tothe severity of intent
Psychiatric Disorders PSISS
Mild Intent Moderate intent Severe intentN (%) N (%) N (%)
Depression 6 (26.08) 25 (32.05) 7 (29.16)Alcohol dependence 3 (13.04) 7 (8.97) 3 (12.5)Opioid dependence 1 (4.34) 5 (6.41) 2 (8.33)Adjustment disorder 4 (17.39) 9 (11.53) 1 (4.16)Bipolar mood disorder 3 (13.04) 6 (7.69) 3 (12.5)Others 1 (4.34) 1 (1.28) 2 (8.33)Total 23 (100) 78 (100) 24 (100)
Table-9: Association among parameters of BDHI and PSISS
BDHI PSISS N Mean ± SD p-value
Assault Mild 23 3.29 ± 1.27 0.626Moderate 78 4.03 ± 1.21Severe 24 4.25 ± 1.26
Indirect Mild 23 5.14 ± 1.28 .055Moderate 78 5.23 ± .911Severe 24 4.67 ± .963
Irritability Mild 23 4.17 ± 1.23 .014*Moderate 78 4.78 ± 1.92Severe 24 5.67 ± 1.49
Negativism Mild 23 2.48 ± .947 .453Moderate 78 2.27 ± .893Severe 24 2.46 ± .588
Resentment Mild 23 1.74 ± .915 .071Moderate 78 2.29 ± 1.05Severe 24 2.17 ± .917
Suspicion Mild 23 3.96 ± 1.79 .054Moderate 78 3.05 ± 1.57Severe 24 3.08 ± 1.41
Verbal Mild 23 5.91 ± 1.23 .768Moderate 78 7.15 ± 9.27Severe 24 7.25 ± .989
of the subjects with severe suicidal intent were notdiagnosed to have any active psychiatric disorder.
This reflects that the majority of the subjectswho presented with DSH were suffering fromdepressive disorder. Followed by the subjectshaving no active psychiatric illness. The p valuecalculated was p>0.05 found to be statistically non-significant reflects that the severity of intent doesnot vary significantly with co morbid psychiatricdisorders. Majority of subjects have moderateintent.
Table 9 shows relationship between thedifferent parameters on Buss Durke Hostility Index(BDHI) (assault, indirect, irritability, negativism,resentment, suspicion and verbal) with severity ofsuicidal intent on Pierce Suicide Intent Scale. The

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society282
relationship between the parameter irritability on(BDHI) and severity of suicidal intent was foundthat irritability was statistically significantly relatedwith the severity of suicidal intent in patientspresenting with DSH.
Table 10 show relationship between the para-meters aggression, Irritability and suicidality onOvert Aggression Scale (OAS-M) and severity ofsuicidal intent. It was found that all three parameterswere highly statistically significantly related withthe severity of suicidal intent in patients presentingwith DSH.
Table 11 the analysis of the correlation wasdone between the different parameters of BussDurkee hostility scale, Overt aggression scale modi-fied and pierce suicide intent scale. Multiplepositive and negative correlations are seen betweendifferent parameters. The positive correlation wasalso seen between irritability (BDHI) and suicidalintent. (r value – 0.257) and similarly the verbaldomain (BDHI) was also seen directly related withthe suicide intent (r value – 0.303). The aggressiondomain of overt aggression was positively relatedto the suicide intent seen on pierce suicide intent
Table-10: Association among parameters of OAS-M and PSISS
OAS-M PSISS N Mean ± SD p-value
Aggression Mild 23 70.13 ± 10.81 0.000Moderate 78 76.82 ± 15.39Severe 24 87.13 ± 8.93
Irritability Mild 23 5.22 ± 1.23 0.000Moderate 78 6.03 ± 1.21Severe 24 7.17 ± 0.917
Sucidality Mild 23 4.61 ± 0.988 0.000Moderate 78 5.14 ± 1.24Severe 24 7.04 ± 0.75
Table-11: Shows correlation coefficient (r) among different parameters on BDHI, OAS-M, PSISS
OAS-M aggression OAS-M irritability OAS-M suicidality PSISS
BDHI (Assault) -.002 -.035 .102 .085BDHI (indirect) -.079 .000 -.273(**) -.145BDHI (irritability) .191(*) .216(*) -.055 257(**)BDHI (negativism) -.129 -.130 .010 -.005BDHI (resentment) -.109 .172 -.288(**) .126BDHI (suspicion ) -.132 -.091 .132 -.164BDHI (verbal) .031 .149 -.013 .303(**)PSISS .361(**) .399(**) .544(**) 1
scale (r value -0.361), Similarly seen with irritabilityand suicidality domain of overt aggression was alsofound to be directly related with suicide intent. Theanalysis showed direct (weak) correlation betweenirritability (BDHI) and aggression on (OAS-M) (rvalue 0.191) and similarly seen with irritability(BDHI) and irritability (OAS-M) (r value – 0.216).The inverse correlation was seen between theindirect and suspicion parameters of (BDHI) (rvalue- -0.198) and similarly inverse correlation wasseen in the indirect (BDHI) and suicidality of (OAS-M) (r value- -0.273) and too with resentment(BDHI) and suicidality (OAS-M) (r value- -0.288).
DiscussionThe present study was carried out to assess the
hostility and suicidality in patients presenting withdeliberate self-harm, while analysing the sociodemographic profile of the 125 cases who presentedwith DSH out of which 53.6% were males and46.4% were females, as in this study more no. ofmales presented with DSH than females which isin concordance with other Indian studies, In onestudy of attempted suicide5 in Madurai, found male

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 283
predominance of 108 males as compared to 90females who presented with deliberate self-harm.Similarly Ponnudurai15 reported in the studyconducted, in which male to female predominancewas 2.3:1 in a sample of 208 patients presentingwith DSH. In Indian set up, the reason for greaterproneness of males to deliberate self-harm couldbe easy access to poisonous chemicals due to theirincreasing household use, unemployment among theyoung, increasing social and financial burden andincreasing substance use. Other reasons could bethat due to male dominance in Indian families, morestress on males, with more responsibilities towardsfamily and hence they are more prone to stress anddeliberate self-harm.
In our study, prominent age group of deliberateself-harm was 20 -29.Venkoba Rao et. al.5 studiedin India and found male dominance in their studies.General consensus is that 50% of the attemptersare under 30 years of age and reported an increasein male attempters of this age group. There is a gooddeal of research showing that suicidal behaviourincreases markedly during adolescence.
In our study 58.4 patients belong to ruralcommunity and 41.6% belongs to urban community.This is in contrast to the study by Hegde et.al.16
who found no significant difference in DSH in ruralcommunity as compared to the urban. The reasonfor more number of rural subjects could be easyaccess to poisonous substances. As our study alsoreported poisoning as most common cause of DSHso this could be the best explanation for morenumber of rural predominance in our sample.
Our study has shown that more number ofhousehold 24.8%) and students (17.6%) presentedwith deliberate self-harm. This is in concordancewith the study conducted by Venkoba Rao et.al.5,who found that students accounted for majority ofsuicide attempters. The reason could be morestressful life events and more competitive approachwith high aspirations and easy accessibility tosubstance of abuse. As women are not socialized toexpress violence externally and when confrontedwith the vast rage, women tend to vent onthemselves and many present with deliberate harmself. Banerjee et. al.17 Out of 58 who committedsuicide there were 46 (79.3%) women. Thecommonest cause of suicides was quarrel withhusband and commonest method used was
poisoning with insecticides.In our study among the cases, (89.8%) of
subjects to present with DSH had educational statusup to tenth and below. The possible reason mightbe higher level of stress of low education in thismore competitive world and their keen desire forgrowth that lead to higher level of stress and theypresent with deliberate self-harm. This was seen inaccordance with the study conducted by Shukla etal.18 in which 46% males and 42% females whopresented with deliberate self-harm were educatedup to matriculation but this is opposite with thestudy by Lal and Sethi et al19 that had 42% subjectswith education level above matriculation, Gupta andSingh et al20 had 47% of subjects were educatedabove higher secondary. This reflects that deliberateself-harm is more common in these subjects as thisis the period of increasing stress as it is the stage ofcompetition and struggle in life in academics to setup a career.
Our results show, that majority of patients(70%) belong to high socio economic group andonly 4% belongs to low socio economic group. Thisis in contrast with study by Lal and Sethi et al,19
who observed 38.3% subjects falling into low socioeconomic group. The reason could be tertiary careand private set up of our hospital as more of subjectsbelonging to high socio-economic status can affordto come to this private set up for care.
In present study 52% patient were married and48% were unmarried. This is in contrast to otherstudies where predominance of unmarried subjectswas observed for deliberate self-harm, 66% ofunmarried presented with suicidal attempt byVenkoba et al,5 65.3% by Sethi et al21 62% ofsubjects were unmarried who presented withdeliberate self-harm by Gupta and Singh et al,20 ascompared to married persons predominance 51.9%by Lal and Sethi et al.19 The reason could be moresocial support available to married people to presentin hospital. More over disturbed interpersonalrelationships and adjustment problems may be oneof the precipitating factor which can lead to morenumber of subjects to present with deliberate self-harm.
We have found that, most common method ofdeliberate self-harm was poisoning (42%),including 30% OPC, 12% Celphos. Out of thismajority were males (30%) as compared to females

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society284
(12%). Other studies vary in their results as regardattempted suicide by poisoning as 47% poisoningwas found by Badrinaraynan et al,22 33% of subjectspresented with the ingestion of OPC, in the studyconducted by Hegde et al,16 similar results were seenin the study conducted by 20.0% males and 20.5%females by Shukla et al.18 77.70% males and 76.99%females too presented with the self-harm with thepoisoning seen in the study conducted by, Sudhiret al.23 The reasons for more number of cases bypoisoning are that there is easy access to thesechemicals due to their wider and common use inhomes and other places and they can be procuredwithout any prescription from retail outlets.
Our results on BDHI scale showed that para-meter like irritability was found to be significantlyrelated with the intent on PSISS. But assault,indirect, negativism, resentment, suspicion was notfound to be statistically significantly related withthe intent to harm self-harm. Similarly, Silver etal24 studied the relation of impulsive behaviour andviolence to attempted suicide. Results showed that30% of the attempted suicide showed moderateimpulsivity scores on Buss Durkee inventory. Onemore study by Hull et al25 studied positive relation-ship between suicidal ideations/or attempts inpatients with substance abuse, impulsivity andaggression. In our study the different parameters(aggression, irritability, suicidality) of OvertAggression Scale-Modified were also correlatedwith the severity of intent on PSISS. Statisticallysignificant relation was seen between aggression,irritability, suicidality, as it was found that all thethree parameters were significantly positivelyrelated with high suicidal intent.
In past Hull et al25 studied positive relationshipbetween suicidal ideations/or attempts in patientswith substance abuse, impulsivity, aggression, andirritability Stanley et al26 studied Trait impulsivityand hostility assessed among 52 DSM-IV bipolarsubjects with and without histories of suicideattempts. Impulsivity and hostility were correlatedamong attempters but not non-attempters. Ascompared to non-attempters, attempters hadsignificantly higher levels of overall hostility, moreextensive subcomponents of hostility, and a trendtoward higher overall impulsivity. Accordingly,Doihara et al27 investigated aggression in medicallyserious suicide attempters at an emergency
department. Trait aggression was evaluated in 55suicide attempters and 71 healthy individuals as acontrol group using the Japanese version of theBuss-Perry Aggression Questionnaire (BAQ). TotalBAQ scores (t = 2.782, P = 0.006) and the hostilityscores (t = 3.735, P < 0.001) were significantlyhigher in the suicide attempters than the controls.In one more study, Brittlebank et al28 examinedsixty-one consecutive patients who presentedfollowing an episode of deliberate self-harm (DSH)were assessed on a number of variables, includingmeasures of hopelessness and hostility. Those whowere known to have had a further episode of DSHhad significantly higher levels of hopelessness andintropunitive hostility after the index episode thanthose who did not repeat.
In this present study it was seen that amongthe subjects, 33.9% females presented withadjustment disorder which was significant morethan in males. This reflects that females withadjustment disorder were found to be vulnerable toDSH but no significant difference among males andfemales for other psychiatric disorders. 26.4% ofmales presenting with deliberate self-harm weresubstance dependence which was found to bestatistically significant among males and females.As in our culture less number of females presentwith substance dependence. Though majority of thesubjects (36%) presented with depressive disorder,followed by (28.8%) of subjects presented withDSH but no active psychiatric illness.
Our results show that there is no significantrelation between the patients of deliberate self-harmwith and without psychiatric illness on theparameters of violence and assault as assessed onBDHI. Similar results were seen in the studyconducted by Krakowski et al.29
In the present study females who were sufferingfrom adjustment disorder were found to more proneto DSH. Similar results were quoted by Portzky etal30 of 19 suicide victims’ by means of a semi-structured interview schedule which showed thatthe suicidal attempts was significantly more infemales (48%) diagnosed with adjustment disordercompared with suicide cases diagnosed with otherdisorders.
The findings were in contrast with the studyconducted by Takaoet et al31 which revealed thatschizoaffective and depressive disorder in

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 285
psychiatric patients with completed suicide andschizophrenia, depressive disorder and adjustmentdisorders in patients with attempted suicide weresignificantly more frequent than in 312 controls. Inthe end it appears important that early identificationof hostility in patients presenting with variouspsychiatric disorders could be one of the preventivemeasure for deliberate self-harm.
Hence from the study it can be seen significantthat most of the hostile behaviour including irrita-bility, aggression and violence vary significantlyin direct proportion with the severity of suicideintent. More over among psychiatric disorders,adjustment disorder appears to be significant riskfactor in females as compared to males as far asrisk for DSH is concerned. However hostilebehaviour in different psychiatric does not seem tovary significantly. In the end it appears importantthat early identification of hostility in patientspresenting with various psychiatric disorders couldbe one of the preventive measure for deliberate self-harm.
Haw et al,32 studied 150 patients presentingwith DSH at a general hospital. Out of which 40patients of alcohol dependence were compared withthe remaining sample. Compared with other DSHpatients, those with an alcohol diagnosis were olderand more often male, living alone, unemployed,sick, disabled, or with a past history of DSH. Theyalso had higher scores on measures of anger,aggression, and impulsivity. Depression as acomorbid psychiatric disorder was present in 37(92.5%) patients In our study it was observed thatout of 125 cases, 18 (14.4%) were of alcoholdependent syndrome. Irritability on BDHI Scalewas seen high among them as compared with otherco morbid disorders but on OAS Scale, aggressionwas high in mood disorder cases.
The common method employed to execute self-harm was corrosive poisoning and insecticidepoisoning. Similar findings have been reported fromelsewhere in India and other low- and middle-income countries.33,34
Hayashi et al33 studied 155 suicidal patientsadmitted consecutively during a 20-month periodin psychiatry center. In this study 68 were malesand 87 were females and their average age (SD)was 36.5 (11.9) years old. 49 subjects (31.6%)
started to exhibit SB at an age of 20 years oryounger. The common diagnoses among suicidalpatients were affective disorders 62%, anxietydisorders 56% and substance-related disorders 38%.56% of the subjects were diagnosed as havingborderline PD. Commonly used suicidal behaviourprior to admission were self-cutting 41%,overdosing 32%, self-strangulation 15%, jumpingfrom a height 12% and attempting traffic death 10%.The studied sample showed the high prevalence ofaffective disorders, anxiety disorders and borderlinePD, a variety of SB methods used prior to admissionand frequent SB repetition in the lifetime history.Gender and age appeared to have an influence onSB method selection and SB-preceding processes.The findings have important implications forassessment and treatment of psychiatric suicidalpatients.
As mood largely plays major role in suicidalintent so usually individuals suffering from affectivesymptoms may present with suicidal attempts. Evenunder the effect of the substance too, individualsthey do deliberate harm to themselves. Commonlyused method for deliberate self-harm was OPC,probable reason is the easily availability of thischemical as maximum cases were from ruralbackground.
Ghimire et al35 did retrospective observationalstudy on 200 cases of deliberate self-harm in thetertiary centre in Eastern Nepal, data collected fromthe medical records of these patients. Various socio-demographic data and any psychiatric comorbiditiesin them were studied. Majority (77%)of casespresented with deliberate self-harm were less than35 years of age. Majority (73.5%) were married.72.5% of cases had consumed organophosphates/-chlorides. 37% of cases had psychiatric disordersand 20 % had premorbid personality problems Themost common was adjustment disorder (13.5%)followed by mood disorder (11%). In our studymajority (51.2%) of the cases were from age groupof 20 – 29 years. Majority (66.4 %) were married.70.4% consumed OPC, which was most commonmethod used for deliberate self-harm. The mostcommon comorbidity seen among our cases wasmood disorder (36%) followed by adjustmentdisorder (17.6%). So almost similar results wereobserved.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society286
ConclusionMore number of males presented with
deliberate self-harm than females. Majority of thesubjects presented with DSH were from age groupof 20-29 years of age. Most common method ofDSH used was poisoning (Organophosphorus).Majority of the subjects presented with DSHattempted once. Females suffering from adjustmentdisorder presented with DSH more than males. OnBDHI scale irritability parameter was found tostatistically significant in relation with severity ofsuicide intent on PSISS. On BDHI males expressmore verbal hostility than females which wasstatistically significant. On OAS-M all the threeparameters (irritability, aggression and suicidality)were significantly associated with severity of intentof suicide on PSISS.
LimitationsAs patients presenting with the deliberate self-
harm in the emergency were shifted to medicinedepartment for maintaining medical stability, somany of them were missed and follow up inpsychiatry OPD was not done. Due to fear of hustlesin their future life refused to participate.
References1. Harrington JA, Cross KW. Cases of attempted
suicide admitted in general hospital. Br Med J1959; 2 : 463.
2. Using the phrase ‘commit suicide’ is offensiveto survivors and fr ightening to anyonecontemplating taking his/her life. It’s not thesame as ‘being committed’ to a relationship orany other use of it as a verb. Suicide prevention(SUPRE) World Health Organization 2012.
3. Suicides in India Archived 2014-05-13 at theWayback Machine. The Registrar General ofIndia, Government of India 2012.
4. Polgreen, Lydia. “Suicides, Some for SeparatistCause, Jolt India”. The New York Times 2010.
5. Venkoba Rao A, Rawlin CR. Attempted suicideand suicide among students in Madurai. IndianJ Psychiatry 1972; 14 : 389-97.
6. Mann JJ. A current perspective on suicide andattempted suicide. Ann Intern Med 2002; 136 :302.
7. Kumar S, Mohan R, Gopinath R. Genderdifference in suicide attempts. A Study from
South India 2006; 144 : 79-86.8. Grover S, Sarkar S, Chakrabarti S, Malhotra S,
Avasthi A. Intentional Self-harm in Childrenand Adolescents: A Study from PsychiatryConsultation Liaison Services of a Tertiary CareHospital. Indian J Psychol Med 2015; 37(1) :12–6.
9. Vijayakumar L, Rajkumar S. Are risk factorsfor suicide universal? A case-control study inIndia. Acta Psychiatr Scand 1999; 99 : 407 :11- 17.
10. Roy A, Linnoila M. Alcohol and suicide.Suicide Life-Threatening Behav 1986; 16 : 244-273.
11. Allen NH. Homicide followed by suicide.SuicideLife ThreatBehav 1983; 13 : 155-65.
12. Alfred Lange, Bahman Dehghani, Edwin deBeurs. Validation of the dutch adaptation of thebuss-durkee hostility inventory. Behav Res Ther1995; 33(2) : 229-33.
13. Silver Jonathan C, Yudofsky S. The OvertAggression Scale: Overview and guidingprinciples. J Neuropsychiatry Clin Neurosci1991; 3(2) : 22.
14. Keegan, Richard & Chan, Derwin King Chung& Lonsdale, Chris. Development and validationof the Perceived Social Influences in SportScale-2 (PSISS-2): A cross cultural study. J SciMed Sport 2013; 16(5) : 50.
15. Ponnudurai R, Patnaik KA, Sathianathan R,Kumudinisubhan. A study on the venues ofsuicide. Indian J Psychiatry 1997; 39 : 34-36.
16. Hegde RS. Suicide in rural community. IndianJ Psychiatry1980; 22 : 368-70.
17. Banerjee G, Nandi DN, Nandi S, Sarkar S, BoralGC, Ghosh A. The vulnerability of Indianwomen to suicide- a field studies. Indian JPsychiatry 1990; 32 : 305-8.
18. Shukla GD, Verma BL, Mishra DN. Suicide inJhansi city Indian J Psychiatry 1990; 32 : 44-51.
19. Lal N, Sethi BB. Demographic and socio-economic variables in attempted suicide bypoisoning Indian J Psychiatry 1975; 17 : 100-7.
20. Gupta SC, Singh H. Psychiatric illness insuicide attempters. Indian J Psychiatry 1981;23 : 69-74.
21. Sethi BB, Gupta SC, Singh H. Psychological

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 287
factors and personality characteristics in casesof attempted suicide. Indian J Psychiatry 1978;20 : 25-30.
22. Badrinarayanan A. Suicide attempt inGulbergha. Ind J Psychiatry 1977; 19 : 69-70.
23. Sudhir Kumar CT, Chandrasekaran R. A studyof psychosocial and clinical factors associatedwith adolescent suicide attempts. Indian JPsychiatry 2000; 42(3) : 237-42.
24. Silver MA, Bohnert M, Beck AT, Marcus D.Relation of depression and attempted suicideand seriousness of intent. Arch J Psychiatry1971; 25 : 573.
25. Hull EE, Kerr BA, Robinson. Risk factors ofsuicidal ideations and attempts in talented, atrisk girls. Suicide Life Threat Behav 2004;34(3) : 267-76.
26. Stanley B, Gameroff MJ, Michalson V. Aresuicides attempters who self mutilates areunique population. Am J Psychiatry 2001;158(3) : 427-32.
27. Doihara C, Kawanishi C, Yamada T, Traitaggression in suicide attempters: a pilot study.Psychiatr Clin Neurosci 2008; 352-4.
28. Brittlebank AD, Cole A, Hassanyeh F, KennyM, Simpson D, Scott J. Hostility, hopelessnessand deliberate self-harm: a prospective follow-up study Acta Psychiatr Scand 1990; 81(3) :280-3.
29. Krakowski M, Czobor P. Suicide and violencein patients with major psychiatric disorders JPsychiatr Pract 2004; 10(4) : 233-8.
30. Portzky G, Audenaert K, Heeringen. Adjust-ment disorder and the course of the suicidalprocess in adolescents. J Affect Disord 2003;87 : 265 – 70.
31. Takao Hattori, Kazuo TaketaniI. Suicide andsuicide attempts in general hospital psychiatry:Clinical and statistical study. Psychiatr ClinNeurosci 2008; 49 : 43-8.
32. Haw C, Houston K, Townsend E, Hawton K.Deliberate self-harm patients with alcoholdisorders: characteristics, treatment, andoutcome. Crisis 2001; 22(3) : 93-101.
33. Hayashi N, Igarashi M, Imai A. Psychiatricdisorders and clinical correlates of suicidalpatients admitted to a psychiatric hospital inTokyo. BMC Psychiatry 2010; 10 : 109.
34. Rodham K, Hawton K, Evans E. Reasons fordeliberate self-harm: Comparison of self-poisoners and self-cutters in a communitysample of adolescents. J Am Acad ChildAdolesc Psychiatry 2004; 43 : 80–7.
35. Ghimire S, Devkota S, Budhathoki R, SapkotaN, Thakur A. Psychiatric Comorbidities inPatients with Deliberate Self-Harm in a TertiaryCare Center. J Nepal Med Assoc 2014; 52(193): 697-701.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society288
A Study of Suicidal Ideation and Suicidal Attemptin Patients with Obsessive Compulsive Disorder
Shah Karan Kiritkumar, Tushar Jagawat, Krishna Kanwal, Bajrang Dhaka, Ritu Meena, Pankaj KumarDepartment of Psychiatry, National Institute of Medical Sciences & Research, Jaipur, Rajasthan, India
Contact: Tushar Jagawat, E-mail: [email protected]
Original Article
IntroductionSuicide is among the top three causes of death
among youth worldwide. According to the WHO,every year, almost one million people die fromsuicide and 20 times more people attempt suicide;a global mortality rate of 16 per 1,00,000 or onedeath every 40 seconds and one attempt every 3seconds, on average. Suicide worldwide wasestimated to represent 1.8% of the total globalburden of disease in 1998; in 2020, this figure isprojected to be 2.4% in countries with market andformer socialist economies. According to the mostrecent World Health Organization (WHO) data thatwas available as of 2011,1 India ranks 43rd in
descending order of rates of suicide with a rate of10.6/100,000.1
Suicidal ideation and suicide attempts (suicida-lity) are important indicators of extreme emotionaldistress2 Attempted suicide is one of the strongestrisk factors for death by suicide, and 60% of plannedfirst attempts occur within the first year of ideationonset.3-5 Mental disorders are strongly associatedwith completed suicides, with studies mainly fromWestern populations showing that approximately 9out of every 10 individuals appear to have had apsychiatric disorder at the time of their death.6
Serious Suicidal ideation is not uncommon in thegeneral population, with studies consistently noting
Abstract
Background: Suicide is among the top three causes of death among youth worldwide. Suicidalideation and suicide attempts (suicidality) are important indicators of extreme emotional distress.Obsessive-compulsive disorder (OCD) is a chronic, distressing, disorder associated with asignificant functional impairment. This present study aims to understand the prevalence ofsuicidal ideation and attempts in patients of Obsessive-Compulsive Disorder and their sociodemographic characteristics. Methodology: Patient who fulfilled the selection criteria wereenrolled in the study. A total of 50 patients participated in study.Diagnosis of OCD was doneusing ICD 10. Sociodemographic data was evaluated using structured proforma designedespecially for the study. The severity of OCD was measured using YBOCS scale. Suicidalideations were evaluated using Beck’s Scale for Suicidal Ideation. Past history of suicide attemptwas noted. All the data was evaluated using appropriate statistical methods. Results: SuicidalIdeations were present in 46% of the OCD patients while 12% of patients had attempted suicide.Conclusion: This study concludes that patient of OCD can have significant suicidal ideationsand attempts. Early identification of suicidal ideations in OCD patients can potentially belifesaving.
Keywords: Obsessive compulsive disorder, Suicidal ideation, Suicidal attempt

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 289
lifetime prevalence rates of up to 16.5%.3,7,8,9,10
Suicidal behavior – suicidal ideation, suicideattempt and completed suicide – probablyrepresents a continuum of self-harming behaviors.Suicidal behavior as a concept includes thetendency, thoughts or acts of self-harming behavioror life-threatening risks. Suicidal behavior can bedirect – suicidal ideation, suicide attempt orcompleted suicide, or indirect – such as riskydriving, high-risk hobbies, hazardous alcoholdrinking, drug misuse or neglecting the managementof physical illness.8
Obsessive-compulsive disorder (OCD) is achronic, distressing, anxiety disorder associatedwith a significant functional impairment. OCD hasemerged to be one of the most prominent anddisabling mental disorders. OCD is an anxietydisorder characterized by recurrent obsession orcompulsions that are recognized as excessive orunreasonable causing a marked distress, are time-consuming (>1 h/day), interfere with normalfunction, and are ego dystonic. It is the fourth mostcommon psychiatric disorder. 11-14 There is areasonable probability that the patients of OCDhave suicidal thoughts, plans, or actually attemptsuicide. Suicidal behavior is the result of a complexinteraction of biological, genetic, psychological,sociological, and environmental factors.15-21
This present study aims to understand theprevalence of suicidal ideation and attempts inpatients of Obsessive-Compulsive Disorder andtheir socio demographic characteristics.
Materials and MethodsStudy Design:
It is cross-sectional type of study.
Study Area:The Study was conducted in Tertiary Hospital,
Jaipur, Rajasthan.
Study Period:1st January 2018 to 30th June 2018
Selection Criteria of PatientsInclusion Criteria:
1. All patients diagnosed as Obsessive-Compulsive Disorder as per ICD 10
classification in the age group of 18-45years attending psychiatry outpatientdepartment.
2. Patients who gave written informed consentto participate in the study.
Exclusion Criteria:1. Patients who were aged below 18 years or
above 45 years were not included in thestudy.
2. Patients who did not give written consentwere not included in the study.
3. Patients having other psychiatric illnessthan Obsessive Compulsive Disorder.
4. Patients having any significant medical orsurgical co-morbidity.
MethodologyAfter taking permission from Scientific and
Ethical committee of Institute and on the basis ofinclusion and exclusion criteria patients wereincluded in the study. A total number of 50 patientsparticipated in the study. Diagnosis of ObsessiveCompulsive Disorder was made according to ICD-10 Classification.22 A written consent from thepatient was obtained after explaining the study tothe patient. Patient was given a Semi StructuredProforma designed especially for the study. Patient’ssocio-economic status was evaluated using B.G.Prasad’s Socio Economic Scale.23 Suicidal Ideationswere evaluated using Beck’s Scale for SuicidalIdeation.24 Patients past history of suicidal attemptwas taken. The severity of Obsessive-CompulsiveDisorder was measured using Yale-BrownObsessive Compulsive Scale (Y-BOCS).25 Aftercollecting all the data proper statistical methodswere applied under supervision of statistician.
Technique1. All Psychiatric diagnosis were made
according to ICD-10 criteria.2. Semi Structured Proforma designed
especially for the study.3. B. G. Prasad’s socioeconomic scale.23
4. Becks Scale for Suicidal Ideation.24
5. Yale-Brown Obsessive CompulsiveScale(Y- BOCS) for severity of Obsessive-Compulsive disorder.25

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society290
ResultsTable-1: Socio-demography of Patients having
OCD enrolled in the study
Age Group Number of Patients Percentage (%)with OCD
18-30 yrs 43 86%31-45 yrs 7 14%Total 50 100%SexMale 33 66%Female 17 34%Total 50 100%Marital StatusMarried 29 58%Single 21 42%Total 50 100%DomicileRural 35 70%Urban 15 30%Total 50 100%ReligionHindu 41 82%Muslim 9 18%Total 50 100%Socioeconomic StatusUpper 0 0%Upper Middle 7 14%Middle 4 8%Lower Middle 26 52%Lower 13 26%Total 50 100%EducationIlliterate 16 32%Primary 10 20%Secondary 8 16%Higher Secondary 6 12%Graduate/Post Graduate 10 20%Total 50 100%OccupationUnemployed 9 18%Unskilled 5 10%Skilled 7 14%Service 9 18%Student 10 20%Housewife 10 20%Total 50 100%
Table 1 shows the socio-demography of thepatients having OCD enrolled in our study. A totalnumber of 50 patients were enrolled in the study.Majority of our patients (86%) were below the ageof 31 years. Most of the patients enrolled were males(66%). Majority of the patients were single (62%).Patients were mostly from the rural area (70%).Majority of the patients followed Hindu religion(82%). Most of patients belonged to lower middle
class (52%). Most of the patients were illiterate(32%) followed by primary educated (20%).Students, Housewife and Unemployed made themajority of the sample.
Table-2: Patient Distribution on the basis ofseverity of OCD (Y-BOCS scale)
Parameter(Y-BOCS) No. of Patients Percentage
Subclinical (0-7) 20 40%Mild (8-15) 9 18%Moderate (16-23) 12 24%Severe (24-31) 5 10%Extreme (32-40) 4 8%Total 50 100%
Table 2 shows the patient distribution accordingto the severity of OCD as measured by the YBOCSscale. Most of the patients were subclinicalcases(40%).
Table-3: Distribution of Compulsion &Obsession in enrolled patients
Variables Number of Patients (N=50)
ObsessionsContamination 28 (56%)Pathological doubt 12 (24%)Sexual 5 (10%)Religious 2 (4%)Aggressive 2 (4%)Symmetry 1 (2%)CompulsionsCleaning 28 (56%)Checking 12 (24%)Arranging 1 (2%)Repeating 1 (2%)No compulsion 8 (16%)
Table 3 shows the common presentations ofthe obsessions and compulsions in the enrolledpatients. Most of the patients showed obsessivethoughts of contamination which was followed bycompulsion of cleaning. Second most commonobsession was pathological doubt followed bycompulsion of checking.
Table-4: Distribution of Suicidal Ideators andAttempters in total number of patients
Total Number Patients Patients with Patientsof Patients without Suicidal with
Suicidal Ideation SuicidalIdeation Attempt
50 27 (54%) 23 (46%) 6(12%)

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 291
Table 4: shows that out of total sample enrolledin the study 46% of the patients with OCD hadcurrent suicidal ideations while 12% had a previoussuicide attempt.
Table-5: Correlation between Age group andSuicidal Ideations and Attempts
Age Group Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
18-30(N=43) 19 (82.60%) 24 (88.88%) 5 (83.33%)31-45 (N=7) 4 (17.39%) 3 (11.11%) 1 (16.66%)Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 1.6695. The p-value is .43399. Theresult is not significant at p < .05
Table 5 shows Majority of patients havingsuicidal ideation (82.60%) belonged to age groupof 18-30 years, similarly suicidal attempt (83.33%)was mostly seen in 18-30 years age group.
Table-6: Correlation between Sex andSuicidal Ideations and Attempts
Gender Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Male (N=33) 16 (69.56%) 17 (62.96%) 5 (83.33%)Female (N=17) 7 (30.43%) 10 (37.03%) 1 (16.66%)Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 1.1809. The p-value is .554074. Theresult is not significant at p < .05.
Table 6 shows Suicidal ideations and attemptswere more common in male gender with 69.56% &83.33% respectively.
Table-7: Correlation of Marital Status andSuicidal Ideations and Attempt
Marital Sucidal Sucidal SucidalStatus Ideation Ideation Attempt
Present Absent
Married 16 (69.56%) 13 (48.14%) 4 (66.66%)(N=29)Single (N=21) 7 (30.43%) 14 (51.85%) 2 (33.33%)Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 7.4519. The p-value is .02409. Theresult is significant at p < .05.
Table 7 shows majority of patients with suicidalideations (69.56%) were married and majority ofsuicide attempters (66.66%) were also married.
Table-8: Correlation of Domicile and SuicidalIdeations and Attempt
Domicile Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Rural (N=35) 15 (65.21%) 20 (74.07%) 2 (33.33%)Urban (N=15) 8 (34.78%) 7 (25.92%) 4 (66.66%)Total ( N=50) 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 3.6475. The p-value is .16142. Theresult is not significant at p < .05.
Table 8 shows that patient having more suicidalideations (65.21%) belonged to the rural area whilepatient having more suicide attempt (66.66%)belonged to urban area.
Table 9: Correlation between Religion andSuicidal Ideations and Attempt
Religion Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Hindu (N=41) 20 (86.95%) 21 (77.77%) 5 (83.33%)Muslim(N=9) 3 (23.04%) 6 (22.22%) 1 (16.66%)Total N =50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 0.7198. The p-value is .697729. Theresult is not significant at p < .05
Table 9 shows majority of patients with suicidalideations (86.95%) and suicide attempts (83.33%)were Hindu.
Table-10: Correlation between socioeconomicclass and suicidal ideations and attempts
Socio- Sucidal Sucidal SucidalEconomic Ideation Ideation AttemptStatus Present Absent
Upper Middle 4 (17.39%) 3 (11.11%) 2 (33.33%)(N=7)Middle (N=4) 2 (8.69%) 2 (7.40%) 1 (16.66%)Lower Middle 8 (34.78%) 18 (66.66%) 2 (33.33%)(N=26)Lower (N=13) 9 (39.13%) 4 (14.81%) 1 (16.66%)Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 19.7577. The p-value is .003058.The result is significant at p < .05.
Table 10 shows majority of suicidal ideationswere present in lower (39.13%) and lower middle(34.78%) class. While suicide attempt was morecommon in lower middle and upper middle classwith 33.33% respectively.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society292
Table-11: Correlation between Education andSuicidal Ideations and Attempt
Education Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Illiterate (N=16) 8 (34.78%) 8 (29.62%) 0Primary (N=20) 3 (13.04%) 17 (62.96%) 0Secondary (N=8) 4 (17.39%) 4 (14.81%) 0Higher Secondary 4 (17.39%) 2 (7.40%) 3 (50%)(N=6)Graduate/Post 4 (17.39%) 6 (22.22%) 3 (50%)Graduate (N=10)Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 8.0376. The p-value is .09021. Theresult is not significant at p < .05.
Table 11 shows that suicidal ideations are morecommon in illiterate with 34.78% while suicideattempts are common in educated patients.
Table-12: Correlation Between Occupationand Suicidal Ideations and Attempt
Occupation Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Unemployed (N=9) 3 (13.04%) 6 (22.22%) 0Unskilled (N=5) 1 (4.34%) 4 (14.81%) 0Skilled (N=7) 6 (26.08%) 1 (4.34%) 2 (33.33%)Service (N=9) 3 (13.04%) 6 (22.22%) 1 (16.66%)Student (N=10) 4 (17.39%) 6 (22.22%) 3 (50%)Housewife (N=10) 6 (26.08%) 4 (14.81%) 0Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 7.672. The p-value is .104361. Theresult is not significant at p < .05.
Table 12 shows suicidal ideations are commonin Housewife (26.08%) and students (26.08%)while suicide attempts are more common in students(50%)
Table-13: Correlation between Severity ofOCD and Suicidal Ideations
Correlation between Pearson CorrelationCoefficient (r)
Y-BOCS & SSI 0.9301
Table 13 shows a strong positive correlationbetween the Y-BOCS and SSI
Y-BOCS & SSI score P-Value is < .00001. Theresult is significant at p < .05.
Table-14: Correlation between Type ofObsession and Suicidal Ideations and Attempt
Type of Obsession Sucidal Sucidal SucidalIdeation Ideation AttemptPresent Absent
Contamination 9 (39.13%) 19 (70.37%) 3 (50%)(N=28)Pathological 7 (30.43%) 5 (18.51%) 3 (50%)doubt (N=12)Sexual (N=5) 4 (17.39%) 1 (3.70%) 0Misc (N=5) 3 (13.04%) 2 (7.40%) 0Total N=50 23 (46%) 27 (54%) 6 (12%)
The chi-square statistic is 5.6207. The p-value is .131593. Theresult is not significant at p < .05.
Table 14 shows majority of suicidal ideationswere present in patients having obsession ofContamination (39.13%) which was closelyfollowed by Obsession of Pathological doubt(30.43%) while suicide attempts were equallydivided between patients with Obsession ofContamination and Doubt.
DiscussionA total of 50 patients diagnosed with OCD were
enrolled in the study. Out of our total sample 23patients that is 46% of the patients had currentsuicidal ideations. 6 of the patients had a past historyof suicide attempt that is 12% of the patients hadattempted suicide. This finding is comparable toother study conducted by Chaudhary et al18 thatfound 56% of the patients with OCD had suicidalideations while 16% had actual attempt of suicide.Dhyani et al17 found 55.76% suicidal ideations inOCD patients while 19.23% had history of theattempt. This data suggests that OCD possess asignificant risk of developing suicidal ideations dueto distress and finally may lead to suicide. Earlydiagnosis and intervention can therefore belifesaving for the patient.
In present study we found majority of patientshaving suicidal ideation (82.60%) belonged to agegroup of 18-30 years, similarly suicidal attempt(83.33%) was mostly seen in 18-30 years agegroup.This is a relevant finding since the onset ofthis disorder is in young population. These findingsare similar to the study done by Maina et al26 andDhyani et al17 in which mean age of patients was31.8 years and age group of 26-35years respectively.These studies had also shown similar age strati-

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 293
fication. While comparing the age groups andsuicidal ideations and attempt we found nostatistically significant relation.
In our study we found Suicidal ideations andattempts were more common in male gender with69.56% & 83.33% respectively. A contrary findingto our study was reported by Gupta et al.27 andChaudhary et al.18 who observed higher proportionof patients with OCD with current Suicidal ideationswere females 66.7% and 70% respectively. Theyhave indicated a female predominance. Manyreasons can be possible for male majority ofpatients. One of them can be rural background hasa male dominance and females having psychiatricsymptoms are not seen at the hospital due to stigma.Overall the outpatients seen in our department isalso male dominated. On running the statisticalanalysis, we did not find statistical significancebetween gender and suicidal ideations and attempts.
In current study majority of patients withsuicidal ideations (69.56%) were married andmajority of suicide attempters (66.66%) were alsomarried. In our study most of the patients belongedto rural population and it is cultural to get marriedin younger age. Radhakrishnan et al. who reportedthat Marriage is not a strong protective factor forsuicide attempts in developing countries. 70.4% ofall suicide victims in India were married and 21.9%were unmarried.28 The data was also statisticallysignificant. This means that Marital status caninfluence the suicidal ideations and attempts. Sincemarried people put distress on their spouse andfamily which in turn puts more distress on thepatient. This vicious cycle may be the reason forhigher suicidal ideations.
In our study majority of patients with suicidalideations (86.95%) and suicide attempts (83.33%)were Hindu. Other study by Gupta et al. reportedmost of the patients who attempted suicide wereHindus.29 This can be a result of the local populationsurrounding the hospital region where majority ofthe people follow Hindu religion. StatisticallyReligion is not significant factor that influences thesuicidal ideations and attempts.
In present study majority of suicidal ideationswere present in lower (39.13%) and lower middle(34.78%) class. While suicide attempt was morecommon in lower middle and upper middle classwith 33.33% respectively. Kodali et almade
observation that maximum number of suicideattempters belonged to low socioeconomic status(62%).30 This data is statistically significant mean-ing that a person’s socio-economic class caninfluence the suicidal ideations and lead to attemptof suicide. Poverty in itself is distressing while thedisease adding to the distress only adds up tosuicidal ideations.
Our study shows that suicidal ideations aremore common in illiterate with 34.78% whilesuicide attempts are common in educated patients.Gupta et al showed that according to years ofeducation, the results of their study shows that bothlow and high educational status confers risk ofsuicide.29 Since many of these patients belonged tolower and lower middle socioeconomic class, theyhad no sufficient financial support to further study.Education was not statistically significant to havesuicidal ideations and attempts.
The present study shows suicidal ideations arecommon in Housewife (26.08%) and students(26.08%) while suicide attempts are more commonin students (50%). Kodali reported majority (61%)of the subjects were employed, working in theagricultural sector.30 Different results were shownin study done by Dhyani et al 2013, reportedmajority of patients were unemployed (50%).17
Since most of our patients are young, they are eitherstudying or married. Statistically the Employmentstatus is also not significant to induce suicidalideations and attempts.
In our study, we used Pearson’s correlation toexamine the relationship between the severity ofOCD and Suicidal ideations and we found a positiveand strong correlation between them. It was alsostatistically significant which means that as theseverity of OCD increase the suicidal ideations alsoincreases.
In our current study majority of suicidalideations were present in patients having obsessionof Contamination (39.13%) which was closelyfollowed by Obsession of Pathological doubt(30.43%) while suicide attempts were equallydivided between patients with Obsession ofContamination and Doubt. Literature is in line withthese findings. Similar findings are reported byDhyani et al.17 However the type of obsession orcompulsion is not statistically related to the suicidalideations and attempt.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society294
Limitations1. Hospital based study.2. Small sample size.3. Only Out patients were selected.4. Psychiatric co-morbidity was not accounted.
ConclusionThis study concludes that Obsessive Compul-
sive Disorder patients do have significant suicidalideations and if not treated can lead to suicideattempt. Early recognition of suicidal ideations andmanagement can potentially be lifesaving for thepatient.
Referrences1. World Health Organization. Suicide rates per
1,00,000 by country, year and sex. Availablefrom:http:/ /www.who.int/mental_health/prevention/suicide_rates/en/index.html.
2. Kessler RC, Berglund P, Borges G et al. Trendsin suicide ideation, plans, gestures, and attemptsin the United States, 1990 –1992 to 2001–2003.JAMA 2005; 293 : 2487–2495.
3. Kessler RC, Borges G, Walters EE. Prevalenceof and risk factors for lifetime suicide attemptsin the National Comorbidity Survey. Arch GenPsychiatry 1999; 56 : 617– 626.
4. Suominen K, Isometsä E, Suokas J. Completedsuicide after a suicide attempt: a 37-year follow-up study. Am J Psychiatry 2004; 161 : 562–563.
5. Wang AG, Mortensen G. Core features ofrepeated suicidal behaviour. A long-termfollow-up after suicide attempts in a low-suicide-incidence population. Soc PsychiatryEpidemiol 2006; 41 : 103–107.
6. Cavanagh JTO, Carson AJ, Sharpe M, LawrieSM. Psychological autopsy studies of suicide:a systematic review. Psychol Med 2003; 33 :395-405.
7. Schwab JJ, Warheit GJ, Holzer CE 3rd. Suicidalideation and behavior in a general population.Dis Nerv Syst 1972; 33(11) : 745–748.
8. Sokero TP, Melartin TK, Rytsala HJ. Suicidalideation and attempts among psychiatricpatients with major depressive disorder. J ClinPsychiatry 2003; 64(9) : 1094–1100.
9. Weissman MM, Bland RC, Canino GJ, et al.Prevalence of suicide ideation and suicide
attempts in nine countries. Psychol Med 1999;29(1) : 9–17.
10. Hintikka J, Pesonen T, Saarinen P. Suicidalideation in the Finnish general population. A12-month follow-up study. Soc PsychiatryPsychiatr Epidemiol 2001; 36(12) : 590–594.
11. Reddy VM, Chandrashekar CR. Prevalence ofmental and behavioural disorders in India: ameta-analysis. Indian J Psychiatry 1998; 40 :149-57.
12. Nandi DN, Banerjee G, Mukherjee SP, GhoshA, Nandi PS, Nandi S. Psychiatric morbidityof a rural Indian community. Changes over a20 year interval. Br J Psychiatry 2000; 176 :351-6.
13. Kaplan A, Hollander E. A review of pharmaco-logic treatments for obsessive-compulsivedisorder. Psychiatr Serv 2003; 54 : 1111–8.
14. Karno M, Golding JM, Sorenson SB, BurnamMA. The epidemiology of obsessive-compul-sive disorder in five US communities. Arch GenPsychiatry 1988; 45 : 1094-9.
15. Srivastava AS, Kumar R. Suicidal ideation andattempts in patients with major depression:Sociodemographic and clinical variables.Indian J Psychiatry 2005; 47(4) : 225–228.
16. Trivedi MH, Morris DW. Clinical and Socio-demographic Characteristics Associated WithSuicidal Ideation in Depressed Outpatients. CanJ Psychiatry 2013; 58(2) : 113–122.
17. Dhyani M, Trivedi JK, Nischal A, et al. Suicidalbehaviour of Indian patients with obsessivecompulsive disorder. Indian J Psychiatry 2013;55(2) : 161–166.
18. Chaudhary RK, Kumar P, Mishra BP.Depression and risk of suicide in patients withobsessive-compulsive disorder: A hospital-based study. Ind Psychiatry J 2016; 25 : 166-70.
19. Pavan Kumar K, Girish M. & Saritha G.Suicidal Behaviour in Obsessive CompulsiveDisorder Patients. Int J Curr Med Appl Sci2015; 6(2) : 149-154.
20. Subramaniam M, Abdin E. Suicidal Ideation,Suicidal Plan and Suicidal Attempts AmongThose with Major Depressive Disorder. AnnAcad Med Singapore 2014; 43 : 412-421.
21. Hamilton M. Development of a rating scale forprimary depressive illness. Br J Soc Clin

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 295
Psychol 1967; 6 : 278-296.22. WHO. The ICD-10 classification of mental and
behavioural disorders: Clinical descriptions anddiagnostic guidelines. Geneva: World HealthOrganization 1992.
23. Prasad BG. Social classification of Indianfamilies. J Indian Med Assoc 1961; 37 : 250-251.
24. Beck AT, Kovacs M. Assessment of SuicidalIntention: The Scale for Suicide Ideation. JConsult Clin Psychol 1979, Vol. 47, No. 2, 343-352.
25. Goodman WK, Price LH, Rasmussen SA, etal.: The Yale-Brown Obsessive CompulsiveScale (YBOCS): Arch Gen Psychiatry 1989;46 : 1012-1016.
26. Maina G, Salvi V, Tiezzi MN, Albert U, BogettoF. Is OCD at risk for suicide? A case-control
study. Clin Neuropsychiatr 2007; 4(3) : 117-121.
27. Gupta G, Avasthi A, Grover S, Singh SM.Factors associated with suicidal ideations andsuicidal attempts in patients with obsessivecompulsive disorder. Asian J Psychiatry 2014;12 : 140–6.
28. Radhakrishnan R, Andrade C. Suicide: AnIndian perspective. Indian J Psychiatry 2012;54 : 304-319.
29. Gupta B, Choudhary P, Tripathi A, Nischal A,Agarwal M. Correlates of suicide and temporalvariations in subjects with suicide attempt.Indian J Health Sci Biomed Res 2019; 12(1) :62.
30. Kodali M. Psychiatric Morbidity of AttemptedSuicide Patients Admitted To A GeneralHospital In Rural Area of South India. IOSR-JDMS 2013; 4(3) : 46–50.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society296
The pattern of behavioral and psychologicalsymptoms in patients with Major Neurocognitive
Disorder attending Psychogeriatric OPD in atertiary care teaching hospital
Shravan Kumar,1 Rakesh Kumar Gaur,2 Yasir Alvi,3 Suhail Ahmad Azmi4
Departments of Psychiatry1,2,4 and Community Medicine,3 Jawaharlal Nehru Medical College & Hospital,Aligarh Muslim University (AMU), Aligarh, India
Contact: Shravan Kumar, Email: [email protected]
Original Article
IntroductionThe term “Major Neurocognitive Disorder”
was used in DSM 5 for the first time and thissubsumes the previously popular term “dementia”.1
This refers to an acquired disorder of the brain,designating an impairment of established mentalfunctions due to various etiologies, representing adecline from the premorbid level which is severeenough to impair normal daily functioning.Dementias are a growing public health problem thatresults from population aging.The hallmarks of
dementia are cognitive, functional, and behavioralmanifestations. Among the first manifestations ofdementing disorders are behavioral symptomswhich might appear before cognitive alterations, atsome time during the course of the illness and varyaccording to dementia severity.2 Behavioral andPsychological symptoms of dementia (BPSD) arenon-cognitive symptoms associated with MajorNCDs.3 Early detection of BPSD is extremelyimportant because these symptoms not only inducenoticeable disability in demented patients but also
Abstract
Background: Major Neurocognitive Disorder is a growing public health problem that resultsfrom population aging. While behavioral disturbances are a distressing problem in these patientsand their attendants, the lifetime risk of behavioral disturbances are nearly 100%. So weconducted this study to know the demographic and behavioral disturbances pattern in patientswith Major Neurocognitive Disorder. Methods: A cross-sectional study was conducted at thepsycho-geriatric OPD, Jawaharlal Nehru Medical College, AMU Aligarh. A total of 93 patientswith Major Neurocognitive Disorder were included in the study. A semi-structured proformacontaining patient’s particulars and BEHAVE-AD scale was used for measuring behavioraldisturbances. Data were analyzed using the SPSS version 20.0., keeping significance at p<0.05.Results: Major Neurocognitive Disorder is common among the patients who are divorced,illiterate, belonging to low and middle-income groups, and living in an urban area. Among thetotal 93 patients, the majority were having Major Neurocognitive Disorder due to Alzheimer’sdisease (71%) while Major Vascular Neurocognitive Disorder was seen in 29%. Behavioraldisturbances were seen in every patient and activity disturbance was the most common problemon BEHAVE-AD assessment. Conclusion: We concluded that all the patients with MajorNeurocognitive Disorder have behavioral disturbances in the course of illness. These findingsstress the need for evaluation of behavioral and psychological symptoms in every patient withMajor Neurocognitive Disorder.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 297
increase the caregivers’ stress and they arepotentially treatable.4 BPSD increases impairmentin daily living activities, accelerates cognitivedecline and worsens patient’s quality of life.Behavioral disturbances are one of the main reasonfor increasing cost of dementia care and lead to earlypatient institutionalization, therefore, increasing theoverall financial cost.5 In cross-sectional studies,the reported prevalence of BPSD ranges from 50%to 100%.6–8 The lifetime risk of behavioraldisturbances is nearly 100%.9 In a study assessingseverity, BPSD were severe in 36.6% of the patients,moderate in 49.3%, and mild in 14.1% of patients.10
Different types of BPSD have been reported invarying frequencies considering the type and degreeof dementia , number of BPSD studiedenvironmental parameters and the instruments used.As per best of our knowledge, there is no study donein India so far, in which BPSD pattern has beenevaluated in the clinical sample of dementia. Tobridge this gap in literature we planned this studywith the objective of studying the pattern ofbehavioral and psychological symptoms among thepatients with Major Neurocognitive Disorderattending Psychogeriatric OPD.
Material and MethodsWe conducted a cross-sectional study over a
period of 12 months from January to December2016. The study population included all the patientswith Major Neurocognitive Disorder who visitedthe Psychogeriatric OPD of Department ofPsychiatry, Jawaharlal Nehru Medical College andHospital, Aligarh Muslim University, Aligarh, UttarPradesh, India. The study was approved byInstitutional Ethics and Research Advisory Committee,Jawaharlal Nehru Medical College, AMU, Aligarh.Written informed consent was taken from all of thepatient or their caregiver. Before the start of theinterview, individual rapport-building sessionswere held explaining the purpose of the researchand its implications and ensuring confidentiality.
All the patients aged more than 60 years andof either sex, who fulfilled DSM 5 criteria ofMajor Neurocognitive Disorder, were eligible forthe study. Patients with delirium, with intellectualdisability and patients’ caregivers who did notgave consent for the study, are excluded from the
study. All the eligible population during the entirestudy period was taken for the study.
We recorded the socio-demographic andclinical factors using the semi-structured pro-forma. For the assessment of cognitive functions,we used Hindi Mental State Examination.11 Thisscale is used for an objective assessment ofcognitive deficits and is a modified version of theMini-mental State Examination,12 which has beenstandardized for the Indian population. It is a briefassessment of an individual’s orientation to timeand place, recall ability, arithmetic ability, language,and praxis. For the assessment of behavioral andpsychological symptoms, Behavioural Pathologyin Alzheimer’s disease Rating Scale (BEHAVE-AD) was employed. This scale is specificallydesigned to assess the presence and rate the severityof BPSD in AD patient.13The first part of scaleconcentrates on sympto-matology and the secondrequires a global rating of symptoms on a 4 pointscale of severity. It focuses on 7 behavioral domains;(1) Paranoid and delusional ideation, (2)Hallucinations, (3) Activity disturbances (4)Aggressiveness (5) Diurnal rhythm disturbances (6)Affective disturbances (7) Anxieties and phobias.Each point is scored on a 4 point scale of severitywhere 0= not present, 1=present, 2=present withan emotional component and 3=present, generallywith an emotional and physical component.
The data was entered and analysed inStatistical Package for Social Sciences14 Version 20.Descriptive statistics (Mean, SD); was used for anoverall measure of Major Neurocognitive Disorderscale. Group differences between two variableswere analysed with student sample independent t-test. All p-values were two-tailed and values of p<0.05 were considered statistically significant. Allconfidence interval were calculated at the 95%level.
ResultsDuring the study period, a total of 96 patients
with Major Neurocognitive Disorder who visitedPsychogeriatric OPD, were recruited for the study.Out of these, 3 patients were excluded from thestudy owing to multiple diagnoses. Finally, 93patients with Major Neurocognitive Disorder werestudied.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society298
Table-1: Socio-demographic characteristics ofthe patients
Demographic Frequency Percentagecharacteristics
Age 60-70 55 59.171-80 27 29.0>80 11 11.8
Sex Male 43 46.2Female 50 53.8
Religion Hindu 53 57.0Muslim 39 41.9Others 1 1.1
Residence Urban 57 61.3Rural 36 38.7
Marital Status Married 55 59.1Divorced 1 1.1Widower 37 39.8
Education Illiterate 46 49.5Primary 32 34.4Secondary 10 10.8Graduation 5 5.4and above
Present Unemployed 54 58.1occupation
Employed 39 41.9Type of family Nuclear 22 77.3
Joint 71 23.7Family income <5000 09 9.7
5001-10000 42 45.210001-15000 16 17.2>15000 26 28.0
Socio-demographic and clinical characteristicsAmong the total of 93 patients, 46.2% were
males and remaining 53.8% females. Majority ofthem were in 60-70 year age group. About three-fifths were married, two-fifth were widow and avery small percentage of the patients wereseparated. The literacy rate was quite low with justhalf being literate, and rates of higher educationbeing about 5% of total patients studied. Majorityof them were resident of the urban area andbelonging to joint family and were Hindu byreligion. 58.1 % of the total patients were currentlyunemployed. Major chunk (77.3%) of the patients
was living in a nuclear family and rest were livingin joint family. The total income of the family was<5000 in 9.7%, 5001-10000 in 45.2%, 10001-15000in 17.2% and >15000 in 28% of the patients (Table1).
Clinical characteristicsAmong the total 93 patients, 66 patients were
diagnosed as Major Neurocognitive Disorder dueto Alzheimer’s disease while 27 as Major VascularNeurocognitive Disorder (Table 2). Sixty-eightpercent of the patients with Major NeurocognitiveDisorder scored below 17 on the HMSE scale whilethe remaining 32% scored between 17 to 23. Ourdata suggest that mean HMSE scores of the totalstudy population was found to be 15.06±4.88, whilethe mean of HMSE score among AD and VD was15.48±4.62 and 14.03±5.40 respectively. Thisrelationship was not found to be statisticallysignificant in independent t-test analysis (Table 2).
Among the patients; paranoid and delusionalideations were present in 18.27% of the patients,hallucinations were present in 11.82% of thepatients, activity disturbances were present in60.21%, aggressiveness was present in 38.70% ofpatients, diurnal rhythm disturbance was presentin 52.68% of the patients, affective disturbanceswere found in 21.50%, and 11.82% of the MNCDpatients had anxiety and phobias. Among the ADpatients, paranoid and delusional ideations werepresent in 13.63% of the patients. Hallucinationswere present in 7.57%; Activity disturbances,aggressiveness, diurnal rhythm disturbances,affective disturbances, anxiety and phobias werepresent in 59.09%, 42.42%, 45.45%, 18.18%, and12.12% of the total AD patients respectively. In VDpatients, 29.62% had paranoid and delusionalideations, 22.22% had hallucinations. Activitydisturbances, aggressiveness, diurnal rhythmdisturbances, affective disturbances and anxietiesand phobias were present in 62.96%, 29.62%,70.37%, 29.62% and 11.11% of the total VDpatients respectively (Figure 1).
Table 2: Relationship between cognitive status and clinical diagnosis
Diagnosis Frequency Mean SD t P
AD 66 (71%) 15.48 4.62 1.30 0.196VD 27 (29%) 14.03 5.40Total 93 15.06 4.88

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 299
Figure 1: Distribution of patients according tobehavioral domains
DiscussionWe conducted this study with the objective of
studying the pattern of behavioral and psycholo-gical symptoms in patients with Major Neuro-cognitive Disorder attending Psychogeriatric OPDin a tertiary care hospital
In the socio-demographic variables of oursample, we found that most of the patients withMajor NCD (59.1%) were aged between 60 to 70years, consistent with many studies in India andother developing countries,15–20 but it is youngerthan that reported from the developed countries.This may be related to the socio-demographicprofile of India characterized by lower lifeexpectancy and a larger proportion of patients withVD due to a high prevalence of cardiovasculardisease burden.21 We also found that MajorNeurocognitive Disorder was more common inwomen than men (53.8% in women vs 46.2% inmen). Our finding is supported by a study whichconcluded that in India, Latin America, and Chinaare at the greater risk of having Major NCD.22
Similar rates were reported in studies conducted inEurope.23,24 A number of reasons may becontributing to this result in developing countries,like the women’s limited access to primary care and
their low educational level. The lack of primaryhealth care can predispose these individuals tosuffer from dementia caused by controllablediseases, such as hypertension or diabetes mellitus.The study concludes that most of the patients(59.1%) were married. Our findings are in contrastto the previous study results from western countries,showing a beneficial effect of marriage ondementia.25–28 Our study reveals a negativerelationship between educational status andprevalence of Major NCD. A major proportion ofour sample consisted of illiterate subjects (49.5%).The predominant finding reported in earlier studiesexamining the relationship between education anddementia is that education appears to protect againstdementia. These results have been typicallyexplained in the context of how early life advantagesconferred by schooling contribute to cognitivereserve.29–33 In the Indian context, anepidemiological study from rural and urban areasin the state of Uttar Pradesh observed a continuouspattern of decrease in dementia prevalence withincrease in educational level.34 Low educationallevels have been consistently linked to highdementia rates, whereas individuals with highereducational levels tend to have a cognitive reservethat delays the emergence of clinical signs ofdementia.35
In our study sample, 53.8% of the cases werehousewives. Our finding is in unison with asystemic review of scientific publications datedbetween 1990 and 2014 which concluded that thosewho have a predominantly manual occupationthroughout life have an increased risk of cognitiveimpairment and/or dementia than those withoccupations with higher intellectual requirement.36
Moreover, our sample consists of more number ofwomen and hence this finding is justifiable owingto the cultural background of the patients.
In the context of religion distribution, the studysample consisted of the maximum percentage ofHindus (57%) followed by Muslims (41.9%). Thisfinding attributes to the religious distribution of thelocal community visiting our center. 61.3% of thetotal patients with Major NCD were the residentsof the urban area and rest 38.7% were from ruralareas. Our findings are supported by a study in northIndia by Tripathi et al in 2012 which found similarresults and concluded that 65% of people with

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society300
dementia were residing in urban areas. As per thatstudy diabetes, depression, hyperhomo-cysteinemia, hyperlipidemia, APOE 4 gene, bodymass index (BMI), use of saturated fatty acids,pickles in diet, urban living, and lack of exercisewere associated with independent risk ofdementia.37 A population-based, cross-sectionalsurvey conducted in Latin America, India, andChina have arrived at crude prevalence rate rangingfrom 0.8% in rural India to 4.6% in urban LatinAmerica.38
Our finding is supported by one sociologicalstudy suggesting that overall educational status andhealth of the members of the joint family are poorerthan that of nuclear families.39 However, our resultis opposed by a study of Letenneur L and Gilleronet al., 1999 which suggested that traditional jointfamilies allow for diffusion of burden in familiescaring for the mentally ill and could be responsiblefor mediating the good course and outcome of majormental disorders.40 In India, the number of jointfamilies and the dependency ratio in such familiesis still high and this explains the poor health of themembers.
Our data suggest that mean HMSE scores were15.48 ± 4.62. According to the mean scores inHMSE, the severity of dementia might beconsidered moderate, which might also haveinfluenced the results since moderate AD patientsmight exhibit global cognitive impairment.
We also found that mean of HMSE score amongAD (15.48 ± 4.62) was higher than the means ofHMSE score among VD (14.03 ± 5.40) suggestingbetter cognitive function among the AD patients inour study population. However, this relationshipwas not found to be statistically significant.
In regard to behavioral disturbance as assessedby the BEHAVE-AD scale, every patient of oursample had one or more kind of behavioraldisturbance. This finding is consistent with theprevious study by Lyketsos et al., which concludedthat the lifetime risk of neuropsychiatric distur-bances is nearly 100%.41 Our study demonstratedthat behavioral disturbances are very common,regardless of the dementia type. After analysis ofBPSD on BEHAVE-AD subscales we found thatactivity disturbances were the most prevalentsymptom, present in 60.21% of patients with MajorNCD; followed by diurnal rhythm disturbance
(52.68%). Aggressiveness was the third mostcommon symptom present in 38.70% of patients.Different affective disturbances were found in21.50% of patients. In the previous study alsoactivity disturbances, diurnal rhythm distur-bance,and aggression were among the most commonlyseen BPSD, and it has been suggested that patientswith AD have a higher frequency of aggression.42
Likewise, in our study too, activity disturbance wasthe most commonly seen BPSD symptom in bothAD and VD patients, followed by diurnal rhythmdisturbance and aggression. We found no significantdifference in the rates of activity disturbances,diurnal rhythm disturbances, and aggressionbetween two types of dementia.
Our study has some limitations. Firstly, it wasa cross-sectional study done in a hospital setting,restricting its generalizability. Secondly, theselection bias may have occurred as we recruitedonly the patients who reported to the OPD.BEHAVE-AD has its own limitation of being scoredby the examiner based only upon the impressionsgathered during a single interview with the patientand caregiver; thus the examiner might beinfluenced by his or her snapshot impression of thepatient at the time of the interview, which may notbe a representative of the patient’s behavior duringhis or her typical daily routine.
ConclusionWe concluded that the Major Neurocognitive
Disorder is common among patients who weredivorced, illiterate, belonging to low and middle-income groups, and living in an urban area. Therewas some kind of behavioral disturbance in everypatient we studied. These findings stress the needfor evaluation of behavioral and psychologicalsymptoms in every patient with Major Neuro-cognitive Disorder.Conflict of interest
None declaredReferences1. American Psychiatric Association. Diagnostic
and Statistical Manual of Mental Disorders(DSM-5). American Psychiatric Association2013.
2. Chiu M-J, Chen T-F, Yip P-K, Hua M-S, TangL-Y. Behavioral and psychologic symptoms in

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 301
different types of Dementia. J Formos MedAssoc 2006; 105(7) : 556–62.
3. International Psychogeriatric Association. IPAComplete Guides to Behavioral and Psycho-logical Symptoms of Dementia (BPSD).Milwaukee, WI: International PsychogeriatricAssociation 2010.
4. Tible OP, Riese F, Savaskan E, von Gunten A.Best practice in the management of behaviouraland psychological symptoms of dementia. TherAdv Neurol Disord [Internet]. 2017 Aug [cited2019 May 14]; 10(8) : 297–309.
5. Torrisi M, De Cola MC, Marra A, De Luca R,Bramanti P, Calabrò RS. Neuropsychiatricsymptoms in dementia may predict caregiverburden: a Sicilian exploratory study. Psycho-geriatrics 2017; 17(2) : 103–7.
6. Makimoto K, Kang Y, Kobayashi S, et al.Prevalence of behavioural and psychologicalsymptoms of dementia in cognitively impairedelderly residents of long term care facilities inEast Asia: a cross sectional study.Psychogeriatrics [Internet]. 2019 Mar 4 [cited2019 May 14]; 19(2) : 171–80.
7. Parnetti L, Amici S, Lanari A, Gallai V. Pharma-cological treatment of non-cognitive distur-bances in dementia disorders. Mech AgeingDev 2001; 122(16) : 2063–9.
8. Neil W, Bowie P. Carer burden in dementia—assessing the impact of behavioural andpsychological symptoms via self-reportquestionnaire. Int J Geriatr Psychiatry 2008;23(1) : 60–4.
9. Lyketsos CG, Hoover DR, Guccione M, et al.Depressive symptoms as predictors of medicaloutcomes in HIV infection. Multicenter AIDSCohort Study. JAMA 1993; 270 : 2563-7.
10. Cohen-Mansfield J. Nonpharmacologic inter-ventions for inappropriate behaviors indementia: a review, summary, and critique. AmJ Geriatr Psychiatry 2001; 9(4) : 361–81.
11. Ganguli M, Ratcliff G, Chandra V, et al. A hindiversion of the MMSE: The development of acognitive screening instrument for a largelyilliterate rural elderly population in india. Int JGeriatr Psychiatry [Internet]. 1995 May [cited2019 May 2]; 10(5) : 367–77.
12. Folstein MF, Folstein SE, Mchugh PR. “Mini-Mental State” A practical method for gradingthe cognitive state of patients for the clinician*.
J Psychiat Res 1975; 12(1) : 189–98.13. Sclan SG, Saillon A, Franssen E, et al. The
Behaviour in Alzheimer’s Disease Rating Scale(Behave-AD): Reliability and Analysis ofSymptom Category Scores. Int J GeriatrPsychiatry [Internet]. 1996 Sep 1 [cited 2019Jun 7]; 11(9) : 819–30.
14. IBM SPSS Statistics for Windows. Armonk,NY: IBM Corp 2011.
15. Iyer GK, Alladi S, Bak TH, et al. Dementia indeveloping countries: Does education play thesame role in India as in the West? DementNeuropsychol 2014; 8(2) : 132–40.
16. Shelley BP, Al Khabouri J. The Spectrum ofDementia: Frequency, Causes and ClinicalProfile. Dement Geriatr Cogn Disord 2007;24(4) : 280–7.
17. Aarsland D, Cummings JL, Larsen JP. Neuro-psychiatric differences between Parkinson’sdisease with dementia and Alzheimer’s disease.Int J Geriatr Psychiatry 2001; 16(2) : 184–91.
18. Yokota O, Sasaki K, Fujisawa Y, et al.Frequency of early and late-onset dementias ina Japanese memory disorders clinic. Eur JNeurol 2005; 12(10) : 782–90.
19. Sheng B, Law CB, Yeung KM. Characteristicsand diagnostic profile of patients seekingdementia care in a memory clinic in HongKong. Int Psychogeriatrics 2009; 21(02) : 392.
20. Zhang Z-X, Zahner GEP, Román GC, et al.Dementia Subtypes in China. Arch Neurol2005; 62(3) : 447.
21. Yusuf S, Reddy S, Ounpuu S, Anand S. Globalburden of cardiovascular diseases: part I:general considerations, the epidemiologictransition, risk factors, and impact of urbaniza-tion. Circulation 2001; 104(22) : 2746–53.
22. Prince M, Bryce R, Albanese E, Wimo A,Ribeiro W, Ferri CP. The global prevalence ofdementia: A systematic review and metaanalysis. Alzheimer’s Dement 2013; 9(1) : 63-75.e2.
23. Winblad B, Amouyel P, Andrieu S, et al.Defeating Alzheimer’s disease and otherdementias: a priority for European science andsociety. Lancet Neurol 2016; 15(5) : 455–532.
24. Lobo A, Launer LJ, Fratiglioni L, et al.Prevalence of dementia and major subtypes inEurope: A collaborative study of population-based cohorts. Neurologic Diseases in the

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society302
Elderly Research Group. Neurology 2000; 54(11 Suppl 5) : S4-9.
25. Hakansson K, Rovio S, Helkala E-L, et al.Association between mid-life marital status andcognitive function in later life: population basedcohort study. BMJ 2009; 339(jul02 2) : b2462–b2462.
26. Sundström A, Westerlund O, Mousavi-NasabH, Adolfsson R, Nilsson L-G. The relationshipbetween marital and parental status and the riskof dementia. Int Psychogeriatrics 2014; 26(5) :749–57.
27. Khan R, Pai K, Kulkarni V, Ramapuram J.Depression, anxiety, stress and stigma ininformal caregivers of People Living with HIV(PLHIV). AIDS Care 2017; 0(0) : 1–5.
28. Fratiglioni L, Wang H-X, Ericsson K, MaytanM, Winblad B. Influence of social network onoccurrence of dementia: a community-basedlongitudinal study. Lancet 2000; 355(9212) :1315–9.
29. Stern Y. What is cognitive reserve? Theory andresearch application of the reserve concept. JInt Neuropsychol Soc 2002; 8(3) : 448–60.
30. Mortimer JA, Snowdon DA, Markesbery WR.Head Circumference, Education and Risk ofDementia: Findings from the Nun Study. J ClinExp Neuropsychol 2003; 25(5) : 671–9.
31. Karp A, Kåreholt I, Qiu C, et al. Relation ofeducation and occupation-based socioeconomicstatus to incident Alzheimer’s disease. Am JEpidemiol 2004; 159(2) : 175–83.
32. Chaves ML, Camozzato AL, Köhler C, KayeJ. Predictors of the Progression of DementiaSeverity in Brazilian Patients with Alzheimer’sDisease and Vascular Dementia. Int JAlzheimers Dis 2010; 2010 : 1–7.
33. Prince M, Acosta D, Ferri CP, et al. Dementiaincidence and mortality in middle-incomecountries, and associations with indicators ofcognitive reserve: a 10/66 Dementia Research
Group population-based cohort study. Lancet(London, England) 2012; 380(9836) : 50–8.
34. Poddar K, Kant S, Singh A, Singh TB. Anepidemiological study of dementia among thehabitants of Eastern Uttar Pradesh, India. AnnIndian Acad Neurol 2011; 14(3) : 164.
35. Fratiglioni L, Wang H-X. Brain reservehypothesis in dementia. J Alzheimers Dis 2007;12(1) : 11–22.
36. Gracia Rebled AC, Santabárbara Serrano J,López Antón RLA, Aragüés G. Occupation andRisk of Cognitive Impairment and Dementiain People in over 55 Years: A SystematicReview, Spain. Rev Esp Salud Publica 2016;90 : e1–15.
37. Tripathi M, Vibha D, Gupta P, et al. Risk factorsof dementia in North India: a case–controlstudy. Aging Ment Health 2012; 16(2) : 228–35.
38. Rodriguez JJL, Ferri CP, Acosta D, et al.Prevalence of dementia in Latin America, India,and China: a population-based cross-sectionalsurvey. Lancet 2008; 372(9637) : 464–74.
39. Desai I. A note on the family research.Explorations in the family and other essays. 1sted. Thacker and Company Limited. New Delhi:Thacker and Company Limited 1975; 63–68 p.
40. Letenneur L, Gilleron V, Commenges D,Helmer C, Orgogozo JM, Dartigues JF. Are sexand educational level independent predictorsof dementia and Alzheimer’s disease? Incidencedata from the PAQUID project. J NeurolNeurosurg Psychiatry 1999; 66(2) : 177–83.
41. Lyketsos CG, Steinberg M, Tschanz JT, et al.Mental and Behavioral Disturbances inDementia: Findings From the Cache CountyStudy on Memory in Aging. Am J Psychiatry2000; 157(5) : 708–14.
42. Wragg RE, Jeste D V. Overview of depressionand psychosis in Alzheimer’s disease. Am JPsychiatry 1989; 146(5) : 577–87.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 303
Impact of Mindfulness Meditation on Caregiversof Epilepsy and Intellectual Disability
Deoshree AkhouriAssistant Professor (Clinical Psychology), Department of Psychiatry, Jawaharlal Nehru Medical College,
Aligarh Muslim University, Aligarh, Uttar Pradesh, IndiaE-mail:[email protected]
Original Article
IntroductionBirthing and raising a child is considered one
of the most important jobs of an individual. Butcaring for a sick child, mental or physical, couldnot only be challenging but it could also prove toput strain on individuals. If a child is diagnosedwith any form of disability, parent’s world turnsupside down, especially in cases of epilepsy andintellectual disability.
According to The American Association onIntellectual and Developmental Disability,intellectual disability is characterized by significantlimitations in both intellectual functioning(reasoning, problem solving) and adaptivebehaviour (conceptual, social) that manifests beforethe age of 18 years.1 AAIDD views intellectualdisability as a functional interaction betweenindividual and environment.
In the Diagnosis and Statistical Manual ofMental Disorders, Fifth Edition level of severity ofintellectual disability are determined by adaptivebehaviour and not just on level of IQ (intelligencequotient).2 Assessment of functioning involvesconceptual areas (academic skills), social areas(relationships) and practical areas (personalhygiene).
According to International League AgainstEpilepsy,3 epilepsy is a disease of brain characte-rized by an enduring predisposition to generateepileptic seizures and by the neurobiological,cognitive, psychological and social consequencesof this condition.In diagnosis of epilepsy, EEG helpsin distinguishing type of seizure or syndromepresent in an individual. Caregiver of patients withsuch conditions goes through a lot of difficulty inbringing up their children, especially for mothers
Abstract
Introduction: Mindfulness meditation is an emerging therapeutic technique that intends toprevent various psychosocial problems while focusing on the present-moment. Aim: The presentstudy aims to see the impact of mindfulness meditation on family burden, anxiety, aggressionand quality of life among caregivers of patients with epilepsy and intellectual disability.Objectives: The main objective of present study is to assess the level of family burden, anxiety,aggression and quality of life among the caregivers and to see the impact of mindfulnessmeditation on the said aspects. Procedure: Through purposive sampling method60 femalecaregivers were selected from Psychiatry OPD of JNMCH, AMU in which 30 caregivers wereof epilepsy and 30 caregivers of intellectually disabled. Tools used: The study used GeneralHealth Questionnaire-12, Family Burden Interview Schedule, Hamilton Anxiety Rating Scale,Aggression Scale, WHO Quality of Life andFive Facet Mindfulness Questionnaire. Result:Result of the study explains that mindfulness has positive effect in improving psychosocialfactors of caregivers.
Keyword: Mindfulness meditation; Family burden; Anxiety; Aggression; Quality of life;Caregivers

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society304
who have to look after them all the time. Anxietyand aggression are common reactions in such cases.The quality of life of caregivers also reducesbecause of the burden faced by parents in the formof child’s disability.
Family burden usually refers to psychological,social and financial burden faced by family/caregivers whilst caring for patients. Family burdencan put strains on interpersonal relationships,careers, social life, etc. Family members/caregiversconsider psychiatric and behavioural problems tobe an extra burden and find it difficult to managesuch children, compelling them to seek help outside(rehab centres). The burden of caring fora family member across the lifespan has a largelynegative and pervasive impact. In order to reducethe anxiety and aggression levels among caregivers,and increasing their quality of life, mindfulnessmeditation is considered to be quite useful.
According to the World Health Organisation,4
in pyramid of mental health services, caregivers(informal care) occupies second position as the mostimportant care, self-care being the first one. A studyconducted in Kenya 2011, it was found that about79% of caregivers were at risk for developingclinical depression.5
Mindfulness meditation has been proven to bequite an effective technique to address the issuesrelated to caregiving and its burden. In a systematicreview conducted in 2016, mindfulness meditationhas been seen as an attempt to treat the problemsassociated with caregivers of patients with variousconditions.6
Various mindfulness-based interventiontechniques are in use these days but the mostprominent one is mindfulness-based stress reductiontechnique.Mindfulness meditation has beenconsidered quite effective in reducing the levels ofanxiety, depression and providing good quality oflife to different individuals. The aim of present studywas to see the efficacy of mindfulness-based stressreduction (MBSR) program on caregivers ofpatients with epilepsy and intellectual disability.
Objectives1. To assess and compare family burden,
anxiety, aggression and quality of life andlevel of mindfulness of caregivers ofpatients withepilepsy and intellectual
disability along with people belonging fromnormal population.
2. To asses and compare the effect ofmindfulness meditation on psychosocialfactors ofcaregivers of patients withepilepsy and intellectual disability
MethodologySample - 30 female caregivers of epilepsy
patients and 30 female caregivers of intellectualdisability patients were randomly selected from thePsychiatry OPD of JNMCH, AMU. Patients fallingunder inclusion criteria were taken.Caregiversfalling under inclusion and exclusion criteria wereselected. 30 people from normal population werealso selected.
Inclusion Criteria for Epilepsy Patients1. On the basis of ICD-10, abnormal EEG
report2. Age 8-16 years
Inclusion Criteria for Intellectually DisabledPatients
1. According to ICD-10, IQ moderate-to-severe level
2. Age 8-16 years
Inclusion Criteria for Caregivers• Age 30-50 years• Caregivers with no psychiatric illness or
severe medical condition• Caregivers showing mild-to-moderate
levels of family burden anxiety, aggressionand reduced quality of life
• Caregivers showing low level of mind-fulness
• Caregivers having no physical disability
Exclusion Criteria for Caregivers• Caregivers not falling under age range• Having psychiatric illness or severe
medical condition• Caregivers who showed no family burden,
anxiety, aggression and increased qualityof life
• Caregivers showing high level of mind-fulness
• Caregivers having physical disability

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 305
Inclusion Criteria for Normal Population• Age 30-50 years (Caregivers)• Children of 8-16 years of age• Children with IQ more than 90
Exclusion Criteria for Normal Population• Caregivers not falling under age range• Children not of 8-16 years of age• Children with IQ less than 90
Tools Used1. General Health Questionnaire-12- is used
to assess the general mental health ofindividuals.7
2. Raven’s Coloured Progressive Matrices:It is a nonverbal group test of intelligenceconsisting of 36-items. Designed forchildren aged 5 through 11 years-of-age,the elderly, and mentally and physicallyimpaired individuals.8
3. Vineland Social Maturity Scale: This scalewas adapted to the Indian scenario byMalin.It is a semi-structured assessmentbased on an interview of the caregiver andevaluates the social ability of the child.9
4. Family Burden Interview Schedule- is asemi-structured interview schedulecomprising of 24 items, grouped under 6dimensions, i.e. financial burden, disrup-tion of routine family activities, familyleisure and family interaction, effect onphysical and mental health of others.Burden is rated on 3-point, i.e. severeburden, moderate burden and no burden.10
5. Hamilton Anxiety Rating Scale (HAM-A)-is a 14 item scale rated on 5-points. Eachitem is scored on a scale of 0 (not present)to 4 (severe), with a total score range of 0–56, where <17 indicates mild severity, 18–24 mild to moderate severity and 25–30moderate to severe.11
6. Aggression Scale- It consists of 55statements, describing different forms ofhuman aggression. 30 statements are inpositive form while 25 are in negative form.It is a Likert type 5-point scale. Maximumscore is 275 and minimum is 55. Below 154indicates low aggression, 155-204 indicatesaverage aggression and 205 and above
indicates high level of aggression.12
7. WHO Quality of Life-BREF-consists of26 items among them 24 items are basedon a 4 domain structure that is Physical,health, Psychological, Social Relationshipsand Environment, in addition 2 items arefrom the Overall Quality of Life andGeneral Health facet. The items are basedon 5 point Likert Scale ranging from verypoor, poor, neither poor nor good, good andvery good. The higher the score, the higheris the quality of life.13
8. Five Facet Mindfulness Questionnaire(FFMQ)- is a 24 item scale, with 5-pointrating. The higher the score, the higher isthe mindfulness.14
Table 1 indicates that most of the caregiversbelonged within the age-range 30-40, epilepsy(60%) and intellectual disability (50%) and ofnormal population (50%). More than 87% of theparticipants were married and about 13% werewidows.Majority of the female caregivers ofepilepsy and of intellectually disabled belonged torural area (60%) and were housewives (approx.92%). Most of the caregivers came from joint/extended family, epilepsy (66.6%) and intellectualdisability (33.34%). Almost all the participants ofthe study belonged from 10,000-25,000 incomebracket, i.e. approximately 70%. No significantdifference was among the three groups (analysisnot shown). The socio-demographic details are alsoexplained by the following graph (Graph 1)
The graph (Graph 1) illustrates the socio-demographic details of all the participants of thestudy. The graph shows that maximum number ofcaregivers is housewives, belonging from rural areaand middle income bracket.
Procedure-77caregivers of patients withepilepsy and intellectual disability were selectedfrom Psychiatry OPD of JNMCH, AMU, 30 femalescaregivers of epilepsy patients and 30 of intellectualdisability were retained on the basis of inclusion-exclusion criteria.
For the selection of patients, Raven’s ColouredProgressive Matrices was used to assess the levelof intellectual disability. Those showing moderate-to-severe levels of IQ were included in the study.Patients with mild IQ level were excluded asprevious studies showed that caregivers of such

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society306
Table-1: showing socio-demographic details of Caregivers of Epilepsy, Intellectual Disability andNormal Population
Variables Characteristics Caregivers of Caregivers of Normal PopulationEpilepsy (n=30), % Intellectual (n=30), %
Disability (n=30), %
Age 30-40 (18) 60 (15) 50 (15) 5040-50 (12) 40 (15) 50 (15) 50
Marital status Married (25) 83.33 (27) 90 (27) 90Widow (5) 16.66 (3) 10 (3) 10
Occupation Housewife (28) 93.33 (27) 90 (27) 90Working (2) 6.66 (3) 10 (3) 10
Residence Rural (18) 60 (18) 60 (18) 60Urban (12) 40 (12) 40 (12) 40
Family Type Nuclear (10) 33.34 (12) 40 (11) 36.66Joint/Extended (20) 66.66 (18) 60 (19) 63.34
Socio-economic status >10,000 (9) 30 (9) 30 (9) 3010,000-25,000 (20) 67 (20) 67 (20) 67< 25,000 (1) 3 (1) 3 (1) 3
Figure 1 shows socio-demographic details oftheparticipants
Table-2: shows the content of intervention for caregivers
Sessions Mindfulness Meditation Content of Intervention
1 Detailed Assessment; Pre Intervention Psycho-education given, rapport was build, purpose of interventionwas explained, Assessment of psychosocial factors done
2 Mindfulness Body Scan Psycho-education given, Mindfulness Body Scan was introduced,daily practice as part of Homework was given
3 Mindfulness Breathing Psycho-education given, previous session discussed, MindfulnessBreathing was introduced, Homework for daily practice was given
4 Mindfulness Acceptance Psycho-education given, previous session discussed, MindfulnessAcceptance was introduced, daily practice as part of Homework wasgiven
5 Mindfulness Sleeping Psycho-education given, previous session discussed, MindfulnessSleeping was explained, daily practice as part of Homework
6 Mindfulness Sitting Psycho-education given, previous session discussed, MindfulnessSitting was introduced, daily practice as part of Homework
7 Mindfulness Eating Psycho-education given, previous session discussed, MindfulnessEating was explained, daily practice as part of Homework
8 Assessment Post Intervention Psycho-education given, previous session discussed, assessment wasdone, daily practice without supervision of therapist was emphasized
patients have low family burden, anxiety, etc. Thepatients of epilepsy were selected on the basis ofabnormal presentation from EEG report.
The caregivers were administered with GHQ-12, Family Burden Scale, HAM-A, AggressionScale, WHO-QOL and FFMQ.The level ofmindfulness was assessed on all the three groups.For normal population, their level of family burden,anxiety, aggression was low and quality of life wasgood,and on FFMQ their mindfulness level wasfound high, therefore no mindfulness interventionwas given. Only pre and post assessment was done.
Intervention - Caregivers meeting the inclusionand exclusion criteria were retain and explained

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 307
about the therapy i.e. mindfulness meditation. Theywere given training once a week, up to 8 sessionsfor 2 months. After the completion of therapy, theywere asked to daily practice at home, park, garden,etc. After the 2 months of therapy, the abovementioned scales were applied again on caregiversof epilepsy and intellectual disability to see whethermindfulness has effect on reduction of familyburden, anxiety and aggression, and increment inquality of life among the caregivers. The level ofmindfulness was also assessed after every session.The mindfulness package included mindfulnessbody scan, breathing, sitting, eating, sleepingandacceptance.
Statistical AnalysisUsing Statistical Package for Social Sciences
(SPSS) version 20, t-test was used to see the effectof mindfulness meditation from pre-to-post-intervention. Column graph was used to show thesocio-demographic details of the caregivers andnormal population and bar graphs were to representtheeffect of mindfulness meditation from pre-to-post-intervention among caregivers of epilepsy andintellectual disability patients and of normalpopulation. To represent the level of mindfulnessafter each intervention, column graph was used.
ResultsTable 1 shows sociodemographic profile
whereas Table 2 shows the content of interventionfor caregivers.
patients, as well as it increases their quality of life.The t-test was used for comparing the effect ofmindfulness meditation (pre-post-follow-up) ondifferent psychological domains. The table showsMean, SD and t-values. The results indicated thatthere has been a significant reduction of familyburden from pre-intervention (M=1.06, SD=0.81)to post-intervention (M=0.26, SD=0.44), indicatingthe significant difference (t=10.29, sig. <0.05).Anxiety reduced from M=15.68, SD=6.63 (pre-intervention) to M=7.08, SD=1.49 (post-intervention), explaining the significant difference,i.e. t=13.36, sig. <0.05. Reduction in aggression wasnoticed, M=148.09, SD=43.65 (pre-intervention) toM=127.48, SD=11.34 (post-intervention). t-value(4.61) is found significant at <0.05 level.Qualityof life has also improved from pre-intervention(M=218.91, SD=97.08) to post-intervention(M=333.87, SD=19.34). It is found significant at<0.05 level with t=11.94. The obtained result isexplained through following graphicalrepresentation (Graph 2).
Table 4 shows M, SD and t-scores of caregiversof intellectually disabled patients. Table indicatesthat mindfulness meditation reduces family burden,anxiety and aggression of the caregivers ofintellectually disabled patients as well as it increasestheir quality of life. The t-test was used forcomparing the effect of mindfulness meditation(pre-post-follow-up) on different psychologicaldomains. The table shows Mean, SD and t-values.The results indicated that there has been a
Table-3: shows effect of mindfulness meditation on psychosocial factors of Caregivers of Epilepsy
Assessment Variable M SD t Sig.
Pre Intervention Family Burden 1.06 0.81 10.29 <0.05*Post Intervention 0.26 0.44Pre Intervention Anxiety 15.6 6.63 13.36 <0.05*Post Intervention 7.08 1.49Pre Intervention Aggression 149.09 43.65 4.61 <0.05*Post Intervention 127.48 11.34Pre Intervention Quality of Life 218.91 97.08 11.94 <0.05*Post Intervention 338.87 19.34
*sig. at 0.05 level
Table 3 shows M, SD and t-scores of caregiversof epilepsy patients. Table indicates thatmindfulness meditation reduces family burden,anxiety and aggression ofthe caregivers of epilepsy
significant reduction of family burden from pre-intervention (M=1.50, SD=0.57) to post-intervention (M=0.40, SD=0.49), indicating thesignificant difference (t=11, sig. <0.05). Anxiety

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society308
Table-4: shows effect of mindfulness meditation on psychosocial factors of Caregivers ofIntellectually Disabled
Assessment Variable M SD T Sig.
Pre Intervention Family Burden 1.50 0.57 11 <0.05*Post Intervention 0.40 0.49Pre Intervention Anxiety 20.33 1.89 28.13 <0.05*Post Intervention 7.40 1.75Pre Intervention Aggression 208.87 3.04 47.77 <0.05*Post Intervention 131.8 8.63Pre Intervention Quality of Life 131.77 39.23 24.25 <0.05*Post Intervention 331.1 21.43*sig. at 0.05 level
Table-5: shows level of mindfulness after every intervention of caregivers of epilepsy andintellectual disability patients
Group Intervention Epilepsy Caregivers Intellectual Disability Caregivers
Pre Intervention t 0.46SD 1.71 1.62M 13.4 13.2
First Intervention t 2.15SD 1.96 1.86M 15.16 14.1
Second Intervention t 1.57SD 1.9 2.47M 17.46 16.56
Third Intervention t 4.32SD 2.04 1.82M 19.5 17.33
Fourth Intervention t 3.56SD 2.26 2M 21.3 19.33
Fifth Intervention t 4.55SD 2.17 3.32M 24.03 20.73
Sixth Intervention t 3.23SD 1.85 3.49M 25.83 23.5
Seventh Intervention t 4.5SD 1.74 3.34M 27.73 24.63
Post Intervention t 4.85SD 2.26 3.55M 28.7 24.96
reduced from M=20.33, SD=1.89 (pre-intervention)to M=7.40, SD=1.75 (post-intervention), explainingthe significant difference, i.e. t= 28.13, sig. <0.05.Reduction in aggression was noticed, M=208.87,SD=3.04 (pre-intervention) to M=131.8, SD=8.63(post-intervention). t-value (47.77) is foundsignificant at <0.05 level. Quality of life has alsoimproved from pre-intervention (M=131.77,
SD=39.23) to post-intervention (M=331.1,SD=21.43). It is found significant at <0.05 levelwith t=24.25. The results are explained throughgraphical representation (Graph 3), explaining thatmindfulness meditation helps in improving variouspsychosocial factors of female caregivers.
Table 5 explainsthe level of mindfulness amongthe caregivers of epilepsy and intellectual disability.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 309
Figure 2 showscaregiver’s level of mindfulness
The level of mindfulness at baseline level (pre-intervention) showed no significant differencebetween both groups of caregivers. From the pre-intervention to post-intervention, the mean valuesof epilepsy caregivers changed, i.e. M=13.4 toM=28.7. Similar result was obtained for caregiversof intellectual disability from pre-interventionM=13.2 to post-intervention M=24.96, indicatinghow level of mindfulness increased gradually forboth groups. Both the groups differsignificantlypost-intervention, which could beattributed to intellectual disability caregivers andtheir everyday challenge with their child’s disability.
Graph 2 shows how with every intervention,
caregivers level of mindfulness is increasing. Thegraphical representation also explains that amongthe caregivers, epilepsy caregivers showedincreased level of mindfulness in comparison tocaregivers of intellectual disability.
Table 6 indicates effect of mindfulnessmeditation on the level of mindfulness on caregiversof epilepsy and intellectually disabled patients. Thelevel of mindfulness of epilepsy caregiversincreased from pre-intervention (M=13.4, SD=1.71)to post-intervention (M=28.7, SD=2.26) significantat <0.05 level. The level of mindfulness ofcaregivers of intellectually disabled enhanced fromM=13.2, SD=1.62 (pre-intervention) to M=24.96,SD=3.55 (post-intervention).It is also depicted howfor normal population, level of mindfulnessremained static, whatever the difference was found(not significant enough) could be attributed toenvironmental factor. Graphical representation(Graph 4) also shows the effect of mindfulnessmeditation on level of mindfulness on caregiversboth of epilepsy and intellectual disability.
Graph 3 indicates how level of mindfulnesshas increased after the intervention of mindfulnessmeditation. Bar graph also shows comparison
Table-6: shows level of mindfulness of caregivers of epilepsy and intellectual disability patientsand of normal population (pre-post)
Caregivers Intervention M SD t Sig.
Epilepsy(n=30) Pre-Mindfulness 13.4 1.71 36.56 <0.05Post-Mindfulness 28.7 2.26
Intellectual Disability(n=30) Pre-Mindfulness 13.2 1.62 19.6 <0.05Post-Mindfulness 24.96 3.55
Normal Population (n=30) Pre-Mindfulness 28.3 1.95 2.45 No differencePost-Mindfulness 28.63 1.81
Figure 3 shows level of mindfulness from pre-intervention-to-post-intervention

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society310
between the caregivers and normal population.
DiscussionDiagnosed intellectual disability and epilepsy
affects not only the patient but also the members offamily, community and society. Caregiver’s qualityof life and life satisfactionis often negativelyaffected by frequent seizures, co-morbidbehavioural and sleep disorders. Furthermore, thenegative effects can be magnified by individualcoping styles and resources available to them. Mostof the literature views family burden in negativemanner, directly or indirectly influencingcaregiver’s life, may also be causing anxiety,depression, decreased life satisfaction and qualityof life. Low level of social support provided tocaregivers also accounts for anxiety, burden and lowquality of life.Present study indicates positiveinfluence of mindfulness meditation on reductionof family burden, anxiety, aggression and increasingquality of life of caregivers.
The results of present study show thatmindfulness has positive effect in reducing familyburden, anxiety, aggression and increases qualityof life, which further supports the previous studyconducted by Minor et al15 to evaluate mindfulnessbased stress reduction (MBSR) for caregivers ofchildren with chronic conditions. Caregivers of suchchildren often experience high levels of chronicstress and MBSR was found to be quite effectivereducing the substantial amount of stress symptomsand mood disturbances in caregivers of chronicallyill children.The present study also indicates thesame result, i.e. mindfulness meditation has positiveeffect on caregivers of children with variousconditions.
In 2017, Tkatch et al16 also conducted a studyusing mindfulness to reduce perceived stress,caregiver burden, anxiety and loneliness and foundsignificant effect of mindfulness on variouspsychological factors. Present study supportsprevious finding that mindfulness has positiveimpact on various psychosocial domains of life(anxiety, family burden, aggression etc.).
ConclusionThe results of the present study makes us
conclude that mindfulness meditation is one of theeffective methods of treatment that helps in
reducing family burden, anxiety and aggression ofcaregivers and increasing their quality of life. Theresult of the study also indicates that aftermindfulness intervention the level of mindfulnessincreases gradually (after each session) in anindividual.
Limitations1. Since the sample size of present study is
small, result cannot be generalized to alarger population.
2. Male caregivers were not included in thestudy.
3. Patients of profound level of intellectualdisability were avoided.
4. Patients showing co-morbidity withepilepsy and intellectual disability werealso avoided.
Future Plans1. There is a need to conduct this study on
larger sample.2. Effect of mindfulness meditation could also
be seen on caregivers of other disorders.3. Mindfulness could also be used to assess
psychological variables other than the onesused here.
References1. American Association on Intellectual and
Developmental Disabilities. Overview ofintellectual disability: Definition, classificationsand systems of support, 2010.
2. American Psychiatric Association. Diagnosticand statistical manual of mental disorders (5thed.). Arlington, VA: American PsychiatricPublishing 2013.
3. https://www.ilae.org/guidelines/definition-and-classification/the-2014-definition-of-epilepsy-a-perspective-for-patients-and-caregivers(accessed on 06/03/2018)
4. World Health Organisation. Mental HealthAction Plan (2013-2020). Geneva, Switzerland:World Health Organisation, 2013.
5. Mbugua MN, Kuria MW, Ndetei DM. ThePrevalence of Depression among FamilyCaregivers of Children with IntellectualDisability in a Rural Setting in Kenya, Int J FamiMed 2011, Article ID 534513, 5 pages. http://

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 311
dx.doi.org/10.1155/2011/5345136. Li G, Yuan H, Zhang W(2015 Aug 28),Arch
Psychiatr Nurs 2016; 30(2) : 292-9.7. Goldberg D, Williams P. A user’s guide to the
General Health Questionnaire. Windsor : Nfer-Nelson 1988.
8. Raven J, Raven JC, Court J.H. Manual forRaven’s progressive matrices and vocabularyscales. Section 2: The coloured progressivematrices. Oxford, UK: Oxford PsychologistsPress; San Antonio, TX: The PsychologicalCorporation 1998b.
9. Doll EA. Vineland social maturity scale.Oxford, England: Educational Test Bureau1947.
10. Pai S, Kapur RL. The burden on the family ofa psychiatric patient: development of aninterview schedule, Br J Psychiatry 1981;138(4) : 332–334.
11. Hamilton M. The assessment of anxiety states
by rating. Br J Med Psychol 1959; 32 : 50–55.12. Mathur GP, R. Bhatnagar. Aggression Scale.
Agra: Rakhi Prakashan 2004.13. WHO. The World Health Organisation Quality
of Life assessment (WHO QOL, position paperfrom The World Health Organisation. Soc SciMed 1995; 41(10) : 1403-9.
14. Baer RA, Smith GT, Hopkins J, Krietemeyer J,Toney L. Using self-report assessment methodsto explore facets of mindfulness. Assessment2006; 13 : 27- 45.
15. Minor HG, Carlson LE, Mackenzie MJ,Zernicke K, Jones L. Soc Work Health Care2006; 43(1) : 91-109.
16. Tkatch R, Bazarko D, Musich S, et al. A pilotonline mindfulness intervention to decreasecaregiver burden and improve psychologicalwell-being. J Evidence-based Integ Med 2017.https://doi.org/10.1177/2156587217737204.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society312
Factors affecting Rehospitalization inpsychiatric patients – an exploratory study
Sushma Sonavane,1 Reetika Dikshit,2 Amresh Shrivastava,3 Nilesh Shah,4 Avinash De Sousa5
1,2,4,5Department of Psychiatry, Lokmanya Tilak Municipal Medical College, Mumbai3Professor Emeritus, Department of Psychiatry, University of Western Ontario, Canada
Contact: Avinash De Sousa, E-mail – [email protected]
Original Article
IntroductionDespite revolutionary advances in under-
standing and treatment of mental disorders,treatment outcome of patients is far fromsatisfactory. The reason for poor outcome has beencited as the number of repeated hospitalizationsamongst other causes which continues to happenas patient’s relapse.1 Psychiatric rehospitalizationcontinues to be most challenging area of mentalhealth with repeated hospitalization leading to pooroutcome, high cost of treatment and a major part ofhealth resources.2
It has been demonstrated across studies thatmore than 50% of patients with severe mentaldisorder recover poorly and about 40% arehospitalized again within 6 months of discharge.3
The causes of rehospitalization can be classifiedinto 4 different groups viz. (1) those related toindividual patient characteristics, e.g. personalitytraits, acceptance of treatment, attitude towardsmanagement, stigma and discrimination, resilienceand coping ability; (2) those that are illness relatede.g. early onset of illness, prolonged duration ofuntreated illness, severe psychopathology and
Abstract
Background: Resilience is the ability to bounce back to normal after adversity and has been amarker of recovery and prognosis for psychiatric disorders. It is in fact a personality factorand a psychobiological construct as well. The following study aims to look at the associationbetween key factors and rehospitalization in a group of patients admitted to a psychiatric facility.Methodology: 78 patients admitted to a psychiatric facility were assessed usingsociodemographic proforma and rating scales like the Brief Psychiatric Rating Scale (BPRS),Hamilton Depression Rating Scale (HDRS), Connor-Davidson Resilience Scale (CD-RISC)and the Scale for impact of Suicidality – Management, Assessment and Planning (SISMAP).The data was analyzed statistically. The data was compared on the basis of resilience scoresand number of rehospitalizations. Results: The mean age of the sample was 42.8 ± 15.2 years.The mean duration of illness of the sample was 12.6 ± 12.7 years. 33 (42.3%) had more thanone hospitalization in the past. Significantly greater patients with lower resilience scores hadhigher scores on the SISMAP scale while depression scores on the HDRS and BPRS scoreswere unaffected by resilience scores.When patients were compared on the basis of 1 or morerehospitalizations it was noted that significantly greater patients with male gender hadrehospitalizations and higher resilience scores indicated fewer rehospitalizations. Conclusion:Resilience is a protective factor against development of mental disorder and a risk factor for anumber of clinical conditions, e.g. suicide. Early identification of vulnerable candidates andeffectiveness of resilience based intervention may offer more clarity in possibility of preventionof relapse and rehospitalization.
Key words: Resilience, Rehospitalization, Suicidality, Psychiatric disorders

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 313
treatment resistance, comorbidities and suicideattempt or frequent episodes with deterioratingcourse; (3) those that are treatment related, e.g.delayed intervention, poor access to care,inadequate and lack of maintenance treatment,presence of side effects and lack of specializedtreatments and (4) systemic factors e.g. lack ofhuman resource, modern treatment facilities,training and competency of professional staff.4-5
Other common factors which have beendescribed leading to relapse and rehospitalizationare non-compliance, comorbidity, history of pasthesitation, duration of illness, severity age at onsetof illness.6-7 The nature and quality of treatmentaccess to care and availability for inpatients as wellas community care has also contributed to repeatedhospitalization.8 Local conditions, manpowerresources, clinical practices and effectivenetworking with a range of mental healthprofessionals that can influence the way we treat.9
Identifying the potential risk factors for repeatedhospitalization, interrelationships between riskfactors, and vulnerability will help us take theappropriate measures to prevent hospitalization andpromote care in the community.10
Resilience is a term used to describe thepersonal characteristics that enable one to adapt toenvironmental challenges and to overcomeadversities or stressors. It comprises the ability tocope with stress as well as other protective factors,and has been shown to protect development ofpsychopathology. A number of psychiatric disordershave been linked to resilience.11-12
There are specific patient related factors whichcan prevent rehospitalization such individualcharacteristics like resilience and its constituentfactors are closely linked with prevention of goodoutcome and a state of wellness. Since there are anumber of other factors responsible for hospita-lization, level of resilience does not indicate overallcause of rehospitalization. However, it doesrepresent a major patientrelated factor which canbe targeted for treatment.13
Keeping these factors in mind, the primaryobjective of this study is to find out differencesamong the clinical characteristics of patients whohave been hospitalized more than once in past oneyear and those who have been hospitalized onlyonce during previous one year. The study also looks
at resilience as a probable factor in preventingrehospitalization in patients.
MethodologyThis study was carried out at the regional
mental health care facility, Canada. The sampleconsisted of 78 patients who have been recentlydischarged from assessment program which admitsacute psychiatric patients in a tertiary psychiatricfacility. The patients discharged from the ward foracutely ill patients were screened for presence ofat least one hospitalization during immediateprevious one year. The patients who gave consentwere recruited for the study as per inclusion andexclusion criteria.A total of 117 patients werescreened and 78 that met criteria were selected forthe study.
The inclusion criteria were age between 20-60years, history of hospitalization within the previousone year from the time of assessment and thepresence of an Axis I and/or Axis II diagnosis asper DSM IV-TR criteria.14 The exclusion criteriawere presence of ser ious medical and orneurological conditions, any recent head traumawithin previous one year, absence of any of theinclusion criteria, pregnancy and acutely ill patientswith current risk of suicide or harm to self, harm toothers or serious physical impairment.
Assessment ToolsDemographic and clinical information was
collected from the history available using a semi-structured proforma. of the illness. We usedstandard assessment tools in the evaluation ofpatients like
1. Brief Psychiatric rating scale (BPRS):The 18-item BPRS was used to evaluatedisorganized speech and other psychiatricsymptoms in the subjects. All the BPRSitems were scored on a 7-point scale from‘not present’ to ‘very severe’. Many studieshave confirmed its psychometric propertiesincluding reliability, validity and sensiti-vity. As mentioned earlier, the conceptualitems of the BPRS have been previouslyused to evaluate disorganized speech orformal thought disorder in patients withschizophrenia.15-16
2. Hamilton Depression rating scale

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society314
(HDRS): The HDRS (also known as theHam-D) is the most widely used clinician-administered depression assessment scale.The original version contains 17 items(HDRS-17) pertaining to symptoms ofdepression experienced over the past week.Although the scale was designed forcompletion after an unstructured clinicalinterview, there are now semi-structuredinterview guides available. The HDRS wasoriginally developed for hospital inpatients,thus the emphasis on melancholic andphysical symptoms of depression. A later21-item version (HDRS-21) included 4items intended to subtype the depression,but which are sometimes, incorrectly, usedto rate severity.17-18
3. Connor-Davidson Resilience Scale (CD-RISC): The Connor-Davidson ResilienceScale (CD-RISC) is a 25-item scale usinga 5-point likert type response scale fromnot true at all (0) to true nearly all of thetime (4). Participants rated each item withreference to the past month. Total scoresrange from 0 to 100, with higher scorescorresponding to higher levels ofresilience.19-20
4. Scale for impact of Suicidality – Manage-ment, Assessment and Planning(SISMAP): This scale was used for theassessment of the risk of suicide inpsychiatric patients. The scale is based onconcept of ‘trait’ and ‘state’ risk. The scalehas been assessed in studies anddemonstrates a specificity of 78.1% whilethe sensitivity of the scale has been shownas 66.7%.21-22
Primary outcome criteria were presence ofstatistically significant difference on clinical andpsychopathological parameters between the groupsof patients admitted only once and the group ofpatients admitted more than once during immedi-ately preceding duration measured from the timeof assessment.The secondary outcome criteria wasconsidered as presence of statistically significantdifference in parameters measured by individualitems of the scale of resilience (assessed by CD-RISC) and suicidality (assessed by SISMAP)between the patients group of those (1) admitted
only once and more than once and (2) those scoringCD-RISC more and less than 60 (cut-off point forsignificance of adequate resilience).
Assessment was carried out within 3 weeks ofdischarge from the hospital, either at the time ofbeing discharge or at the time of first follow up, therecruited patients were assessed by trained researchassistants. Assessment was carried out in one to twosessions. Data was collected on semi structuredproforma which contained demographic, clinicaland structured assessment tools. Data was enteredin the computer database within the hospital system.The data was analyzed using the Graph Padcomputerized statistical software. The entire studywas approved by the Institutional Ethics Committee.Written informed valid consent was taken from eachpatient.Results
The mean age of the sample was 42.8 ± 15.2years. 20 (25.64%) of the sample was married and48 (61.53%) were male. All subjects had completedhigh school education and 32 (41.02%) weregraduates. The mean duration of illness of thesample was 12.6 ± 12.7 years. 33 (42.3%) had morethan one hospitalization in the past. The length ofthe current hospitalization of the sample was 11.3± 28.3 days. The mean score on the CD-RISC scalefor the sample was 52.7 ± 17.7 and 56 (71.79%)had a score of > 60. When the sample was assessedon the SISMAP scale, 44 (56.41%) had score ofsevere suicidal risk. 55 (70.51%) patients had morethan one psychiatric disorder. The commonest diag-nosis was schizophrenia (n=29), major depressivedisorder (n=21) and personality disorders (n=17).
The sample was divided into two groups basedon the CD-RISC scores of 60 or more. Significantlygreater patients with lower resilience scores hadhigher scores on the SISMAP scale (p=0.0001)while depression scores on the HDRS and BPRSscores were unaffected by resilience scores (Table1).
When patients were compared on the basis of1 or more rehospitalizations it was noted thatsignificantly greater patients with male gender hadrehospitalizations (p=0.0015) as were scores on theCD-RISC scale (p=0.004) (Table 2).Discussion
Resilience is an important psychobiological

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 315
of mental disorder and a risk factor for a number ofclinical conditions, e.g. suicide. Available infor-mation from scientific studies points out thatresilience is modifiable factor which opens upavenues for a numberof newer psychosocial as wellas biological therapies.In our study patients withsevere psychopathology were excluded and this isa limitation of the study. Resilience and suicidalitywere the main factors considered while duration ofpsychiatric illness was not taken into considerationwhich is also a limitation of the study. Earlyidentification of vulnerable candidates andeffectiveness of resilience based intervention mayoffer more clarity in possibility of prevention.26
There is a need for resilience building as an inter-vention in in-patient psychiatric programs to preventrelapse and rehospitalization of psychiatric patients.Future research in this arena is warranted.
References1. Corrigan PW, Druss BG, Perlick DA. The
impact of mental illness stigma on seeking andparticipating in mental health care. Psychol SciPub Int 2014; 15(2) : 37-70.
2. Irmiter C, McCarthy JF, Barry KL, Soliman S,Blow FC. Reinstitutionalization followingpsychiatric discharge among VA patients withserious mental illness: a national longitudinalstudy. Psychiatr Quart 2007; 78(4) : 279-86.
marker for psychiatric illness and has beenelucidated vividly in many reviews on the subject.It is the inherent tendency of an individual to bounceback to normalcy after adversity and is a marker ofprognosis and recovery in psychiatric disorders.23
The level of resilience in our study had a directimpact on suicidality scores on the SISMAP.Suicidal behavior and resilience have been studiedand resilience acts as a buffering agent in preventinga suicidal act. In a study where 77 studies werereviewed, it has been demonstrated that a range ofpsychological factors may confer resilience tosuicidality including resilience as a personality trait.The identification of moderators may improveestimates of suicide risk and that the developmentof buffering factors could be a key focus of suicideprevention interventions.24 Higher resilience scoresin our study has been linked to low suicide risk.Resilience is also a marker for the re-emergence ofpsychopathology after recovery and probably therisk for re-admission of patients. In our studyresilience was a protective factor againsthospitalization. Of late, there has been a paradigmshift in the understanding of resilience in contextof stress risk vulnerability dimension. It is aneurobiological construct with significantneurobehavioral and emotional features whichplaysimportant role in deconstructing mechanismof biopsychosocial model of mental disorders.25
Resilience is a protectivefactor against development
Table-1: Resilienceand Suicidality
Psychopathology Scales CD-RISC scores
> 60 (n=56) < 60 (n=22) Chi square / t value p value
SISMAP Severe scores 7 (31.8%) 15 (68.18%) 21.1 0.0001*a
HDRS 18.6 ± 6.1 20.2 ± 6.9 1.0044 0.318b
BPRS 53.9 ± 13.5 57.1 ± 20.7 0.8024 0.424b
*significant (p < 0.05), aChi square test, bUnpaired t test
Table-2: Parameters based on hospitalizations
Parameter studied 1st hospitalisation Rehospitalisation(n=45) (n=33) X2 value p value
Married 11 (24.44%) 4 (12.12%) 1.153 0.283a
Male gender 18 (40%) 26 (78.78%) 10.13 0.0015*a
CD–RISC (< 60) 23 (51.12%) 28 (84.82%) 8.142 0.004*a
BPRS scores 59.6 ± 16.9 51.6 ± 19.1 1.9545 0.054b
*significant (p < 0.05), aChi square test, bUnpaired t test

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society316
3. Ralph RO, Corrigan PW. Recovery in mentalillness: Broadening our understanding ofwellness. American Psychological Association:New York 2005.
4. Davydow DS, Ribe AR, Pedersen HS, Fenger-Grøn M, Cerimele JM, Vedsted P, VestergaardM. Serious mental illness and risk forhospitalizations and rehospitalizations forambulatory care-sensitive conditions inDenmark. Medical Care 2016; 54(1) : 90-7.
5. Marom S, Munitz H, Jones PB, Weizman A,Hermesh H. Expressed emotion: relevance torehospitalization in schizophrenia over 7 years.Schizophr Bull 2005; 31(3) : 751-8.
6. Prince JD. Practices preventing rehospitali-zation of individuals with schizophrenia. J NervMent Dis 2006; 194(6) : 397-403.
7. Fakhoury WK, White I, Priebe S, PLAO StudyGroup. Be good to your patient: how thetherapeutic relationship in the treatment ofpatients admitted to assertive outreach affectsrehospitalization. J Nerv Ment Dis 2007; 195(9): 789-91.
8. Golden AG, Tewary S, Dang S, Roos BA. Caremanagement’s challenges and opportunities toreduce the rapid rehospitalization of frailcommunity-dwelling older adults. Gerontol2010; 50(4) : 451-8.
9. Schmidt-Kraepelin C, Janssen B, Gaebel W.Prevention of rehospitalization in schizo-phrenia: results of an integrated care project inGermany. Eur Arch Psychiatr Clin Neurosci2009; 259(2) : 205-10.
10. Harrow M, Grossman LS, Jobe TH, HerbenerES. Do patients with schizophrenia ever showperiods of recovery? A 15-year multi-follow-up study. Schizophr Bull 2005; 31(3) : 723-34.
11. Fletcher D, Sarkar M. Psychological resilience:A review and critique of definitions, concepts,and theory. Eur Psychol 2013; 18(1) : 12-23.
12. Black K, Lobo M. A conceptual review offamily resilience factors. J Fam Nurs 2008;14(1) : 33-55.
13. Lysaker PH, Roe D, Buck KD. Recovery andwellness amidst schizophrenia: definitions,evidence, and the implications for clinicalpractice. J Am Psychiatr Nurs Assoc 2010;
16(1) : 36-42.14. American Psychiatric Association. Diagnostic
and Statistical Manual for the Classification ofPsychiatric Disorders – Text Revised. (DSM-IV TR). American Psychiatric Publishing: NewYork 2001.
15. Leucht S, Kane JM, Kissling W, Hamann J,Etschel EV, Engel R. Clinical implications ofbrief psychiatric rating scale scores. Br JPsychiatry 2005; 187(4) : 366-71.
16. Kopelowicz A, Ventura J, Liberman RP, MintzJ. Consistency of Brief Psychiatric Rating Scalefactor structure across a broad spectrum ofschizophrenia patients. Psychopathology 2008;41(2) : 77-84.
17. Zimmerman M, Martinez JH, Young D,Chelminski I, Dalrymple K. Severity classifi-cation on the Hamilton depression rating scale.J Affect Disord 2013; 150(2) : 384-8.
18. Trajkoviæ G, Starèeviæ V, Latas M, LeštareviæM, Ille T, Bukumiriæ Z, Marinkoviæ J.Reliability of the Hamilton Rating Scale forDepression: a meta-analysis over a period of49 years. Psychiatr Res 2011; 189(1) : 1-9.
19. Campbell Sills L, Stein MB. Psychometricanalysis and refinement of the connor–davidsonresilience scale (CD RISC): Validation of a 10item measure of resilience. J Traum Stress2007; 20(6) : 1019-28.
20. Scali J, Gandubert C, Ritchie K, Soulier M,Ancelin ML, Chaudieu I. Measuring resiliencein adult women using the 10-items Connor-Davidson Resilience Scale (CD-RISC). Role oftrauma exposure and anxiety disorders.PloSOne 2012; 7(6) : e39879.
21. Johnston ME, Nelson C, Shrivastava A.Dimensions of suicidality: Analyzing thedomains of the SIS-MAP suicide risk assess-ment instrument and the development of a briefscreener. Arch Suicide Res 2013; 17(3) : 212-22.
22. Nelson C, Johnston M, Shrivastava A. Improv-ing Risk Assessment with Suicidal Patients: APreliminary Evaluation of the Clinical Utilityof The Scale for Impact of Suicidality - Manage-ment, Assessment and Planning of Care (SIS-MAP). J Clin Psychol Pract 2010; 1 : 19-26.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 317
23. Shrivastava A, Desousa A. Resilience: Apsychobiological construct for psychiatricdisorders. Indian J Psychiatry 2016; 58(1) : 38-43.
24. Johnson J, Wood AM, Gooding P, Taylor PJ,Tarrier N. Resilience to suicidality: Thebuffering hypothesis. Clin Psychol Rev 2011;31(4) : 563-91.
25. Agaibi CE, Wilson JP. Trauma, PTSD, andresilience: A review of the literature. TraumViol Abuse 2005; 6(3) : 195-216.
26. Samani S, Jokar B, Sahragard N. Effects ofresilience on mental health and life satisfaction.Iran J Psychiatr Clin Psychol 2007; 13(3) : 290-5.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society318
Knowledge, awareness and utilization oftelepsychiatry services among health care
professionalsRenu Sharma, Karobi Das, Ruchita Shah, Afroz, Isha Kumari, Prahalad Singh,
Sarita Kumari, SumanNational Institute of Nursing Education (NINE), PGIMER, Chandigarh, Punjab
Contact: Renu Sharma, E-mail: [email protected]
Original Article
IntroductionTelemedicine is the delivery of health care
services in far away places like preventive, curative,health assessments or consultations, over the telecommunications infrastructure. It allows health careproviders to examine, diagnose and treat patientsusing communication technology, such as videoconferencing and smartphones, without the need foran in person visit.1
In same way, telepsychiatry is known as“telemental health or e –health”. First timetelepsychiatry services were used during 1950 for
group therapy, long term treatment, consultation andtraining of students in Norfolk.2
For providing telepsychiatry services video-conferencing is the main tool. Videoconferencingis examined as the real time transmission of digitalvideo images between multiple sites.3 There are twomain types of telepsychiatry services, first issynchronous and other one is asynchronous.
Synchronous telepsychiatry services canprovide real time consultation, monitoring, assess-ment and interactions through video connectionswhich transmit information in both directions
Abstract
Background and objectives: Telepsychiatry is the application of telemedicine to the specialtyfield of psychiatry. It also termed as “tele-mental health” or “e-health”. Videoconferencing isthe main tool for providing telepsychiatry services through video-calling. The main objectivesof this study is to assess the awareness utilization and barriers related to use of telepsychiatryservices among health care professionals and caregivers of patients attending psychiatry unitof tertiary hospital of Chandigarh. Material and Method: A descriptive study was conductedon 50 health care professionals who work in Department of Psychiatry between April 10th,2019-April 26th, 2019. The data was collected by interview method and through questionnaires.Questions related to the knowledge, attitude, perception, benefits, limitation and barriers oftelepsychiatry were asked. The data was encoded and analyzed by using SPSS version: 20.Result: The mean age of health care professionals was 33.40 ± 8.07. The study revealed that70% health care professionalknew about the telepsychiatry services. 72% health careprofessionals (HCP) agreed that it also improves the access to care. 78% health careprofessionalsbelieved firmly that telepsychiatry services required the understanding of softwareprograms. 95% health care professionals revealed that it reduces the trips to the emergencyroom and 96% health care professional felt that it reduces delay in patient’s care. The mainbarrier among health care professionals reported that patients are not satisfied through videocalling treatment.
Keywords: Telepsychiatry, Videoconferencing, Health care professionals, Caregivers, Barriers.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 319
during the same time period.An asychronous telepsychiatry services does
not require presence of both parties at same time. Itsends data from one site to another through the useof a camera or similar device that records and storesan image that is sent (forword) via telecommuni-cation to another site for consultation. It is alsoknown as “Store and Forward” technique.
Video based telepsychiatry make consultationswithin reach, cheap and attainable to all.4 It hasnumber of advantages for the patients and the healthcare providers and many problems for proper useof telepsychiatry services but there are many otherimportant benefits for health system being timesaving and less expensive.
The utilization of telepsychiatry for patientsruns the risks of leaving a “Digital Paper trail”,allowing unwanted people access personalinformation and also hackers who can break thesecurity of transcribed medical information.Although, many issues for effective use of tele-psychiatry services are present that could save time,save expenses which occurred on traveling and curbdaily issues of the client. Thus, telepsychiatryservices can be greatest promise to remote areasand removing geographical disparities in providingmental health care services.
Telepsychiatry services are implementabledirectly in counseling, control, prevention and alsoin follow-up. There is lack of awareness andknowledge which prevents implementation oftelepsychiatry services in remote rural areas. Thisstudy would improve awareness regarding tele-psychiatry services among caregivers and HealthCare Professionals. It assessed their attitude andperception regarding telepsychiatry services. Thestudy would be helpful in exploring the otherbarriers and implementing telepsychiatry services.
A study was conducted by Myers et al toexamine the utilization and satisfaction of tele-psychiatry among children and adolescent inWashington on March, 2008. Telepsychiatryprovides opportunity to give needed services tochild and youth by using interactive video-teleconferencing. 387 telepsychiatry visits weregiven to 172 youth between the age of 2-21 years.Parents supported high gratification among theirschool aged children’s telepsychiatric care andlower pleasure with their adolescents. Tele-
psychiatry services was used appropriately andparents were highly pleased with their children’scare which was offered by Regional childrenhospital.5
A randomized clinical trial study by Cuevas etal was conducted in Canary Island, Spain whichexamined the efficacy in the treatment of mentaldisorders that was provided through telepsychiatryby means of video-conferencing and also comparedthe video-conferencing with face-to-face conven-tional treatment.Results revealed that the effective-ness of telepsychiatry treatment through video-conference was parallel to face to face interactions.Telepsychiatry proved to be a productive way togive psychiatric consultation and mental healthservices to outpatients who are living in far awayareas with limited resources.6
A pilot study was conducted by Yeung et al inBoston to assess the viability and productivenessof telepsychiatry services provided to Chineseimmigrants and their families in the nursing home.This study enrolled 8 Chinese immigrants betweenthe age of 54 to 88 years who had mood andbehavioral problems. Out of the 8 subjects, 6 weretransferred for psychiatric intervention, 01 fordifferential diagnosis and 01 for suicidalassessment. This study showed that the nursingstaffs were greatly pleased with the telepsychiatryservices and appreciable improvement among theparticipants and other families who were givenintervention.7
Yellowlees et al (2008) reviewed a study toassess acceptability of telepsychiatry for managingpsychiatrist consultations. 60 consultations weredone among English speaking adults’ patientsthrough asynchronous telepsychiatry. Psychiatristsrecommended short term medication changes for95% of the patients and they recommended that itshould not replace face to face interview but it maybe very helpful additional process that improvesaccess to care and expertise.8
Ye et al did a pilot study in Atlanta to explorethe cultural and language barriers in Asian Americanpopulation who were seeking mental health treat-ment. All of them were from Korea. They were 26in number. They completed a questionnaire whichassessed their acceptability of telepsychiatryservices. Result showed that high level ofacceptance of telepsychiatry services among Korean

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society320
clients. They also faced technical issues anddifficulty in establishing rapport which affected thequality of clinical interaction.9
An experimental study was done by Parekh etal in 2005 in district of Pudukottai which pioneeredthe delivery of telepsychiatry services on a mobileplatform. The mobile service covers 156 villageswith a population of about 30000 and servicesfocused only on those with serious mental disorder.Results obtained and showed mobile services hasbeen extremely positiveand it encourages us tobroaden the reach of the program.10
A retrospective study was done by Gowda etal in the year 2013 to 2017 on collaborative tele-psychiatric consultations to outpatients of districthospitals of Karnataka, India. Total 139 consulta-tions were provided at the telemedicine center,NIMHANS over 4 years and 6 months. It was seenthat consultation to district Hospitals from tertiarycare Hospitals were feasible and beneficial for ruralareas.11
Advances in technology and research areexpected to overcome many of the current obstacles.Increased awareness and a more realistic apprecia-tion of telepsychiatry potential as well as limitationmay contribute to better acceptance among users.
ObjectiveTo assess the awareness, utilization and barriers
related to use of telepsychiatry services amongHealth Care Professionals of psychiatry unit ofPGIMER, Chandigarh.
MethodologyIt was a descriptive study with quantitative
approach. Study was conducted at Department ofPsychiatry in tertiary care hospital of Chandigarh.A total of 50 health care professionalswere enrolledin the study using total enumeration technique. Thestudy was approved by the ethics committee of theinstitute. The written informed consent wasobtained from each subject and the purpose of studywas explained to them. Questionnaire and interviewmethod was used to collect the data from healthcare professionals. Questionnaires contain know-ledge, attitude, perception, benefits, limitations andbarriers regarding telepsychiatry services amonghealth care professionals.The subjects were dulyexplained about the purpose of study and they were
given liberty to clarify any doubts before rating theitems on scale. The data was collected in psychiatrysettings. The analysis was done using SPSS version20. The frequencies, means and standard deviationswere computed. The findings of the study arepresented in the forms of tables.
ResultsTable 1 depicts the distribution of subjects as
per their socio demographic profile. About 46% ofthe subjects were in the age group of 28-36 yearswith mean ± SD as 33.40 ± 8.08 years and range
Table-1: Socio demographic variables ofhealth care professionals
N=50
Sr. No. Variables n (%)
1. Age (in year)18-27 13 (26)28-36 23 (46)37-45 08 (16)46-54 01(02)55-64 05(10)
2. SexMale 24 (48)Female 26 (52)
3. Marital statusMarried 32 (64)Unmarried 18 (36)
4. DesignationConsultant 04 (08)Senior resident 08 (16)Junior resident 13 (26)Senior nursing officer 08 (16)Nursing officer 09 (18)Social worker 01 (02)Technician 01 (02)Play therapist 01 (02)Therapist 02 (04)M.Sc. Nursing student 03 (06)
5. EducationMBBS 11 (22)MD 13 (26)Ph.D. 02 (04)M.Sc Nursing 05 (10)M.A. Sociology 01 (02)M.A. Psychology 03 (06)B.Sc. Nursing 15 (30)
6. Working experience in psychiatry (in years)1-10 41 (82)11-20 06 (12)Above 21 03 (06)
7. Duration of working in PGIMER (in years)1-5 33 (66)6-10 05 (10)>10 years 12 (24)

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 321
Table-2: Knowledge of telepsychiatry services among health care professionalsN= 50
Sr. No. Variables Yes n (%) No n (%)
1. Knowledge about telepsychiatry 35 (70) 15 (30.0)2. If yes, source of information
• Interaction 15 (30)• Seminar 08 (16)• Workshop 03 (6)• Self Study 04 (8)• Journals 05 (10)• Other specify —
3. Telepsychiatry is• Consultation through Internet 15 (30)• Report communication 05 (10)• Management with drugs 06 (12)• Electronic medical and mental records 04 (8)• Follow up 05 (10)
4. Knowledge of telepsychiatry guidelines 09 (18) 41 (82)5. Knowledge about Health data security and privacy and in 14 (28) 36 (72)
telepsychiatry services
23-65 years. Half of the subjects (52%) werefemales and majority of the subjects (64%) weremarried. About 26% of the subjects were juniorresidents. Almost 30% of the subjects were havingeducational qualification of B.Sc. Nursing. Majorityof the subjects 82% were having workingexperience within 1-10 years with mean ± SD as1.46 ± 1.82 years and range 1-24 years. Most of thesubjects 66% had 1-5 years duration of working inpsychiatry unit with mean ± SD as 6.52 ± 5.06 yearsand range as 1-20 years.
Table 2 depicts the knowledge of health careprofessionals related to telepsychiatry services.Majority of the subjects 70% had knowledge abouttelepsychiatry services, about 30% of the subjectswere getting information from interaction with
Table-3: Attitude of the health care professionals towards telepsychiatry servicesN=50
Sr. No. Variables Strongly Agree Neutral Disagree StronglyAgree n (%) n (%) n (%) Disagreen (%) n (%)
1. Improve access to care 36 (72) 11 (22) 03 (6) — —2. Improve the continuity of care 38 (76) 10 (20) 02 (4) — —3. Reduce the travel time 17 (34) 16 (32) 17 (34) — —4. Patients prefer to see their psychiatrist in real 01 (2) 17 (34) 17 (34) 03 (6) 01 (2)5. Health care providers are likely to be sued for malpractice 27 (54) 18 (36) 05 (10) —6. More research on the telepsychiatry is needed 7 (14) 19 (38) 09 (18) 11 (22) 04 (8)7. Psychiatrist uses it for practice for initial follow-up care 7 (14) 22 (44) 16 (32) 5 (10) 01 (2) 8. Improve interpersonal relations 11 (22) 20 (40) 08 (16) 11 (22) 01 (2) 9. Less time consuming 16 (32) 22 (44) 09 (18) 03 (6) —10. Help in monitoring of therapy and treatment 15 (30) 13 (26) 37 (74) 19 (38) 15 (30)
others HCP and about 16% of the subjects weregetting information from seminars and about 10%of the subjects were getting information fromjournals. Only 8% and 6% of subjects were gettinginformation from self study and workshops respecti-vely. Almost 30% of the subjects knew thattelepsychiatry is consultation of patients throughinternet. Majority of the subject 82% did not haveany knowledge about telepsychiatry guidelines.Most of the subject 72% did not have knowledgeabout health data security and privacy act fortelepsychiatry services.
Table 3 delineates the attitude of the healthcareprofessionals towards telepsychiatry services.Majority of the subjects (72%) strongly agreed thattelepsychiatry services improved access to care of

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society322
the patient. Majority of the subject (76%) stronglyagreed with that telepsychiatry services improvedthe continuity of care of the patient. About 34% ofthe subjects strongly agreed that with telepsychiatryservices reduced the amount of time of patienttraveling to receive care. Among 34% of thesubjects agreed that patients preferred to see theirpsychiatrist in real not in telecommunicationdevices. Most of the subjects (54%) strongly agreedthat healthcare professionals were likely to be suedfor malpractice if they provide poor telepsychiatryservices. About 38% of the subjects agreed thatmore researches on the telepsychiatry are needed.Almost 44% of the subjects agreed that psychiatristused telepsychiatry for initial follow-up care. About40% of the subjects agreed that telepsychiatryservices would improve interpersonal relations withpatients. About 44% of the subjects agreed thattelepsychiatry services are less time consuming.Majority of the subject (74%) had neutral point ofview that telepsychiatry services would help in themonitoring of therapy and treatment.
Table 4 delineates the perception of thehealthcare professionals towards telepsychiatryservices. Nearly 52% of the subjects perceived that
telepsychiatry services required a “formulated andclear framework to access psychiatry information”.Majority of the subjects (78%) perceived thatunderstanding of software programs made it easyfor clinicians to use telepsychiatry services. Mostof the subjects (66%) perceived that thetelepsychiatry must be strictly secured. About 56%of the subjects perceived that telepsychiatry servicesrequired legal clarification for patients. About 36%of the subjects perceived that national standardswere essential for telepsyciatry technologyimplementation. Nearly 42% of the subjectsperceived that telepsychiatry services can assistthe psychiatrist for diagnosing the patient’s disease.Majority of the subjects (80%) perceived thattelepsychiatry services did not help to providespecialised care to the patients.
Table 5 is showing the barriers of telepsychiatryservices in health care professionals. Most of thesubjects that is 40% agreed about the health careprofessional need formal training in computer.Almost 36 % subjects were agreeing with thatlanguage was a barrier in telepsychiatry servicesbecause it is difficult to understand by the healthcare professionals. Nearly 44% subjects were
Table-4: Perception of the health care professionals towards telepsyhiatry services
N=50
S. No. Variables None Some Quite a Extermelyn (%) n (%) bit n (%) n (%)
1. Requires a formulated and clear framework — 07 (14) 17 (34) 26 (52)2. Understanding of software programs — 04 (8) 7 (14) 39 (78)3. Security policies and guidelines necessary for 01 (2) 05 (10) 11 (22) 33 (66)
the use of telepsychiatry4. Legal clarification for patients — 6 (12) 16 (32) 28 (56)5. National standard are essential 08 (16) 18 (36) 15 (30) 9 (18)6. Assist the psychiatrist for diagnosing the patient’s disease 05 (10) 13 (26) 21 (42) 11 (22)7. Help to provide specialized care to the patients 40 (80) 04 (8) 04 (8) 02 (4)
Table-5: Barriers related to telepsychiatry services in health care professionals
N= 50
S. No. Barriers Agree Neutral Disagreen (%) n (%) n (%)
1. Need a formal training 20 (40) 18 (36) 12 (24)2. Difficulty to understand the language 18 (36) 25 (50) 07 (14)3. Patient is not satisfied with video-calling treatment 22 (44) 20 (40) 08 (16)4. Quality of care will be affected by telepsychiatry 30 (60) 17 (34) 03 (6)5. Battery backup will affect the services 40 (80) 09 (18) 01 (2)6. Technical barriers affect the services 36 (72) 11 (22) 03 (6)7. Ethical and legal issues obstacles in service 03 (6) 42 (84) 05 (10)

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 323
agreeing that patient did not feel satisfied withvideo-calling treatment. Mostly 60% subjects wereagreeing about the quality of care affected bytelepsychiatry services. Majority of the subjects(80%) agreed that battery backup affectedtelepsychiatry services. Most of the subjects (72%)agreed that the technical barriers affect thetelepsychiatry services. Majority of the subjects(84%) were neutral about the ethical and legal issuesbeing obstacles in telepsychiatry services.
DiscussionTelepsychiatry services are contemporary
healthcare innovation which addresses patientsatisfaction, care quality and cost effectiveness. Incontrast to other delivery methods of psychiatryservices telepsychiatry services is blessing for thepatients in remote access area. Althoughtelepsychiatry services provides many benefits butits application is not an easy work. There are manyobstacles in its application e.g. less knowledgeregarding use of computer/Smartphone/anytelecommunication devices which operate intelepsychiatry services among patient and theircaregivers, ethical and legal issues are obstacles inservices among health care professionals. Henceeffective utilization of telepsychiatry servicesdramatically changes care of the remote areaspatients.
The present study showed that only 35 out of50 health care professionals had knowledge towardstelepsychiatry services and 41 healthcareprofessionals did not know its guidelines.
Present study showed that 15 out of 50 healthcare professional considered that telepsychiatryservices in monitoring of therapy and treatment.Another study done by Munezenmaier et al(2018)which assessed 143 physician’s belief , attitude anduse of telepsychiatry services found that tele-psychiatry use was most common among (62%) ofemergency physicians and (61.5%) of psychiatrists.(82.3%) physicians felt that it improved access tocare and (50.8%) felt that it reduced patients traveltime. (71.4%) reported concern regarding potentialloss of personal contact associated with tele-psychiatry.12
Our study showed results of the perception oftelepsychiatry services among health careprofessionals. 52% health care professionals
showed that telepsychiatry services required aformulated and clear framework.78% felt thatimplementation of software program will make iteasy. 66% felt that it required security policies.56%perceived that legal clarification for patients wasrequired. 18% felt that national standards areessential. 22% perceived that it assisted thepsychiatrist for diagnosing the patients and 24%perceived that it provided specialist care to thepatients.
The present study identified the barriers oftelepsychiatry services among Health Care Profe-ssionals. Barriers of telepsychiatry services among50 healthcare professionals were as follows: 40%of health care professional felt that there was a needfor formal training, 36% felt that there was adifficulty to understanding language of patients.44% felt that patients did not feel satisfied withvideo-calling treatment. A study done by Hailey etal 2016 which reported that difficulties incorpo-rating telepsychiatry into their practice includedifficulty in assessing training for telepsychiatry andlack of resources.13 Similarly McGinty et alconducted a study on potential for improving accessto mental health care via telepsychiatry and e-mentalhealth services. This study showed that the potentialbarriers for implementation of telepsychiatryservices for reimbursement, license, impactingpractice behavior, privacy and security and mainbarriers are cost associated with infrastructuredevelopment and maintenance.14
ConclusionTelepsychiatry is the implementation of
psychiatric evaluation and care by video calling todistant people. It is a boon for the health careprofessionals. Although telepsychiatry services areuseful to provide preventive and promotive mentalhealth services and education of care providers inremote area and it also saves the time of patientand as well as of care providers. Patient satisfactiondepends upon the quality and regularity of careprovided by the psychiatrists.
The recommendation of the study can bereproduced on a large number of sample to proveand generalize its result, a chapter on telepsychiatryshould be incorporated in medical professionalscurriculum.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society324
References1. American Telemedicine Association. ‘‘Tele-
medicine Defined.’’ Available at http://searchhealthit.techtarget.com/definit ion/telemedicine. (Accessed on Dec 2018).
2. INSIGHT about telepsychiatry. “What is Tele-psychiatry” Available on http://insight tele-psychia try.com/partners/learn/what-is-telepsychiatry/ (Accessed on Dec 17, 2018).
3. Jsahealth Telepsychiatry. “The History of Tele-mental Health” Available at http://jsahealthmd.com/the-history-of-telemental-health/ .Accessed on: (2 Dec 2018).
4. Elder L, Clarke M. Past, present and future:experiences and lessons from telehealthprojects. Open Medicine 2007; 1(3) : e166.
5. Myers KM, Valentine JM, Melzer SM. Childand adolescent telepsychiatry: utilization andsatisfaction. Telemed J E-Health 2008; 14(2) :131-7.
6. Cuevas CD, Arredondo MT, Cabrera MF,Sulzenbacher H, Meise U. Randomized clinicaltrial of telepsychiatry through videoconferenceversus face-to-face conventional psychiatrictreatment. Telemed J E-Health 2006; 12(3) :341-50.
7. Yeung A, Johnson DP, Trinh NH, Weng WC,Kvedar J, Fava M. Feasibility and effectivenessof telepsychiatry services for Chineseimmigrants in a nursing home. Telemed E-Health 2009; 15(4) : 336-41.
8. Yellowlees PM, Odor A, Parish MB, Iosif AM,Haught K, Hilty D. A feasibility study of theuse of asynchronous telepsychiatry forpsychiatric consultations. Psychiatr Serv 2010;61(8) : 838-40.
9. Ye J, Shim R, Lukaszewski T, Yun K, Kim SH,Rust G. Telepsychiatry services for Koreanimmigrants. Telemed E-Health 2012; 18(10) :797-802.
10. Parekh A. “Reaching the Unreachable: ThePromise of Telepsychiatry in India.” ColumbiaSocial Work Review 2015; 6(1) : 1-7. Doi: http://doi.org/10.7916/D82Z Accessed on: 28|11|2018.
11. Gowda GS, Kulkarni K, Bagewadi V, et al. Astudy on collaborative telepsychiatricconsultations to outpatients of district hospitalsof Karnataka, India. Asian J Psychiatry 2018;37 : 161-6.
12. Munezenmaier K, Martin KB, Norris ER.Physicians’ Beliefs, attitude and use oftelepsychiatry services. J Psych Beahv 2018;4(1) : 021.
13. Hailey D, Ohinmaa A, Roine R. Limitations inthe routine use of telepsychiatry. J TelemedTelecare 2009; 15(1) : 28-31.
14. McGinty KL, Saeed SA, Simmons SC, YildirimY. Telepsychiatry and e-mental health services:potential for improving access to mental healthcare. Psychiatr Quart 2006; 77(4) : 335-42.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 325
Prevalence of Internet addiction and psychiatricdistress among young adults: A gender-based
cross-sectional comparative studyShiv Prakash, Jai Singh Yadav
Department of Psychiatry, Institute of Medical Sciences, Banaras Hindu University,Varanasi, Uttar Pradesh, India
Contact: Shiv Prakash, E-mail: [email protected]
Original Article
IntroductionIn the recent few decades, technology has been
more developed all over the world. Especially afterthe discovery of the internet, it has broughtrevolutionary changes in every area not only incommunication but in business, education, research,and health, etc. There are about 4.31 billion internetusers all over the world, only in India; there areabout 700 million internet users. India stood thirdafter China and America in the ranking of internetusers.1-2 And the number of internet users is very
high especially in young age groups not only inIndia but all over the world.
Internet Addiction (IA) can be defined asexcessive or poorly-controlled preoccupations,urges or behavior related to internet use that increasedistress or impairment.3 It is associated with mentalhealth issues such as anxiety, depression, andsuicidal behaviors.4 It affects both men and womenin all age groups.5 It has become a globalphenomenon especially among adolescents andyoung adults, which has brought a serious negative
AbstractBackground: Young adults are at the increased risk of Internet Addiction (IA) and psychiatricdistress. Objective: To assess and compare the prevalence of IA and Psychiatric distress betweenmale and female young adult college going students. Methods: A cross-sectional comparativestudy was conducted in Varanasi District in Uttar Pradesh, in the period between June 2019 toJuly 2019. Total 150 (75 male and 75 female) college going students were interviewed using asemi-structured questionnaire including socio-demographic variables, Internet Addiction Test(IAT) and GHQ-12. The data was entered in MS Excel and statistical analysis was done in IBMSPSS 20 version. Result: Findings revealed that 57.3% male and 40% female respondents werefound with psychiatric distress (GHQ-12 Score>3). Majority of the male respondents (36%)were found with moderate internet addiction. On the other hands, in female respondents majorityof them (28%) were found with mild addiction. Gender of the respondent was found significantlyassociated with IA (P<0.01) and psychiatric distress (P<0.05). Prevalence of IA and psychiatricdistress was found significantly higher among male compared to female respondents. The meanof daily internet use (in hours) among respondents was found 4.77 ± 2.63 hours. There was asignificant positive correlation found between daily internet use (in hour), IA, and psychiatricdistress. Conclusion: The prevalence of IA and psychiatric distress was found more commonamong male compared to female. Awareness program related to Internet Addiction andpsychiatric distress are needed in college and universities.
Keywords: Young adults, Gender differences, Internet addiction, Psychiatric distress, Mentalhealth.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society326
effect on their physical-mental health, socialbehavior, and academic performance. According toa recently done Meta-analysis in South East-Asiathe prevalence of IA ranged from 7.4% to 46.4%among students.6 In another Meta-analysis ongender differences in the prevalence of IA had beenreported that males have a relatively highertendency to experience internet addiction than dofemales.7
In India, according to previously done studies,the prevalence of IA has been found very highamong young adults compared to other age groups.8
But very few studies have focused on the genderdifferences in the prevalence of IA and thecorrelation between IA and psychiatric distress inyoung adults. The objective of the present studywas to assess and compare the prevalence of internetaddiction and psychiatric distress among male andfemale young adults.
Material and MethodsA cross-sectional comparative study was
carried out to assess the prevalence of internetaddiction and it’s correlation with psychiatricdistress among college-going students in Varanasidistrict in Uttar Pradesh during the period of May2019 to June 2019. A total of 150 (75 males and 75females) college going students aged between 18-29 years from Banaras Hindu University wereselected through convenient sampling for thepresent study.
Inclusion Criteria• University students.• Aged 18-29 years.• Both female and male.• Knowing Hindi & English language.• Using internet from past 1 year or more.• Willing to participate and giving consent.
Exclusion Criteria• Not using internet or a history of using
internet less than 1 year.• Neither willing to participate nor giving
consent.Tools
• A semi-structured questionnaire consistingof socio-demographic characteristics; age,gender, marital status, education, religion,
category, family income, family type, andresidence.
• Internet Addiction Test (IAT): It is areliable and the most frequently used scaleto assess the IA.9 It was developed byKimberly Young in 1998.10 It consists of20 items based on the five-point Likertscale with scores ranging 0 to 5 for eachitems. The respondents are expected tochoose one of the best responses from thegiven options that determine the degree towhich the internet uses affects their dailylife. The total score of IAT was calculatedby adding the responses of all 20 itemsranging from 0 to 100. A score of 0-19 wasconsidered as normal user, 20-49 as averageuser or mild addiction, 50-79 as moderateaddiction and 80-100 as severe addiction.13, 16
• General Health Questionnaire (GHQ) 12:It was used for the determination of thepresence or absence of psychologicaldistress among respondents. It wasdeveloped by Goldberg et al (1978).11 Itconsists of 12 items in which six questionsare positively phrased and six negativelyphrased. Each item was rated on a four-point scale including less than usual, nomore than usual, rather more than usual, ormuch more than usual. The binary scoringmethod (0-0-1-1) was used in the presentstudy; a higher score indicates a higherdegree of psychological distress.
ProcedureThe respondents who fulfilled the inclusion and
exclusion criteria were selected from the selectedstudy area. They were informed about the purposeof the presents study by the interviewer. They wereinterviewed using the prepared questionnaire; first,they were asked about their socio-demographicprofile and interviewed for internet addiction(through IAT). Then were screened using the GHQ-12 questionnaire, the respondent who scored morethan 3 was taken as with psychiatric distress. Theeach interview was done in approximately 30minutes.Statistical Analysis
The data collected from the respondents wasentered in MS Excel sheet and then exported to the

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 327
software IBM SPSS version 20 for analysis. Thedescriptive analysis was done using frequency,percentage, mean and standard deviation (SD). Theassociation was assessed using the chi-squire test.The student’s independent t-test was applied tocompare the study groups. The correlation betweenvariables was assessed using Pearson Correlationtest. The significant value for the study results hasbeen set at P<0.05.
ResultsOut of the total 150 respondents, 75
respondents were male and 75 respondents werefemale. The mean age of the respondents wasapproximately 23 years in both study groups andmajority of them were belong to age group 22-25years. Most of the respondents among male 42
Table: 1 Socio-demographic characteristics of the respondents
Male N=75, F (%) Female N=75, F (%) Total N=150, F (%)
Age (years)18-21 16 (21.3) 20 (26.7) 36 (24.0)22-25 51 (68.0) 45 (60.0) 96 (64.0)26-29 8 (10.7) 10 (13.3) 18 (12.0)Mean and SD 23.4 ± 2.41 22.9 ± 2.42 23.1 ± 2.45EducationGraduation 42 (56.0) 35 (46.7) 77 (51.3)Post Graduation 27 (36.0) 33 (44.0) 60 (40.0)Ph.D. 6 (8.0) 7 (9.3) 13 (8.7)Family TypeJoint 27 (36.0) 33 (44.0) 60 (40.0)Nuclear 48 (64.0) 42 (56.0) 90 (60.0)Socioeconomic StatusLower 6 (8.0) 16 (21.3) 22 (14.7)Lower middle 9 (12.0) 12 (16.0) 21 (14.0)Upper middle 22 (29.3) 28 (37.3) 50 (33.3)Upper 38 (50.7) 19 (25.3) 57 (38.0)ResidenceRural 15 (20.0) 23 (30.7) 38 (25.3)Urban 60 (80.0) 52 (69.3) 112 (74.7)
Table: 2 Distribution of psychiatric distress and internet addiction among the respondents
Male Female Total Chi squire df P ValueN=75, F (%) N=75, F (%) N=150, F (%) Value
Psychiatric DistressAbsent 32 (42.7) 45 (60.0) 77 (51.3) 4.510 1 0.034*
Present 43 (57.3) 30 (40.0) 74 (48.7)Internet AddictionNot present 18 (24.0) 41 (54.7) 59 (39.3) 21.061 3 0.000**
Mild 20 (26.7) 21 (28.0) 41 (27.3)Moderate 27 (36.0) 11 (14.7) 38 (25.3)Severe 10 (13.3) 2 (2.7) 12 (8.0)
Significant at: *0.05, **0.01
(56%) and in female 35 (46.7%) were graduatestudents. Majority of them (60%) were belong tonuclear family and total 57 (38%) of the respondentsbelong to high socioeconomic status. Most of therespondents about 75% were from urban area.(Table 1)
In screening (GHQ-12 score >3); 43 (57.3%)male and 30 (40%) female respondents were foundwith psychiatric distress. Majority of the malerespondents 27 (36%) were found with a moderatelevel of internet addiction. But in femalerespondents, most of them 41(54.7%) were foundwithout internet addiction. Result also indicates thatgender was associated with psychiatric distress andinternet addiction. (Table 2)
The mean of daily use of internet (inhours)among the respondents especially male was

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society328
5.25 hours that is higher than female 4.28 hours.Majority of the respondents about 45% (both maleand female) use internet about 4-6 hours daily.Majority of the male respondents 33 (44%) useinternet for social networking. In other hands mostof the female respondents 31 (41.3%) use internetfor academic purpose. (Table 3)
Table-3: Internet uses among the respondents
Male Female TotalN=75, F (%) N=75, F (%) N=150, F (%)
Daily Uses (in hours) 1-3 26 (34.7) 26 (34.7) 52 (34.7)4-6 38 (50.7) 29 (38.7) 67 (44.7)>7 11 (14.7) 20 (26.7) 31 (20.7)
Mean and SD 5.25 ± 1.94 4.28 ± 3.1 4.77 ± 2.63Purpose Academic 12 (16.0) 31 (41.3) 43 (28.7)
Media 13 (17.3) 14 (18.7) 27 (18.0)Online games 17 (22.7) 7 (9.3) 24 (16.0)
Social Networking 33 (44.0) 23 (30.7) 56 (37.3)
Table-4: Gender differences in IAT and GHQ-12
N Mean SD t value P
IATMale 75 50.16 19.52 5.043 0.000**
Female 75 32.71 22.75GHQ-12
Male 75 4.87 3.43 3.159 0.002*
Female 75 3.27 2.73
Significant at: *0.05, **0.01
Table-5: Pearson Correlation between Internet use daily in hours, IAT and GHQ-12
Internet use (in hours) IAT GHQ-12
Internet use (in hours) 1 .754** .358**
IAT .754** 1 .465**
GHQ-12 .358** .465** 1
** Correlation is significant at the 0.01 level (2-tailed).
On applying student independent t-test, therewas a significant difference found in the score ofInternet Addiction Test (P < 0.01) between maleand female respondents. Internet addiction wasfound more prevalent among male respondentscompared to female respondents. There was also asignificant difference in GHQ-12 score (P <0.05)between male and female respondents. Psychiatricdistress was found more prevalent among malerespondents compared to female respondents,(Table 4)
Pearson correlation was applied to assess thecorrelation among time spent (in hours) in daily
internet uses, internet addiction and psychiatricdistress. There was a significant positive correlationfound among internet use daily (in hours), internetaddiction and psychiatric distress. (Table 5)
DiscussionThe present study was conducted to assess and
compare the prevalence of internet addiction andpsychiatric distress among male and female college-going students in Varanasi district in Uttar Pradeshand the correlation between psychiatric distress andinternet addiction. In the present study, findingsindicate that the prevalence of psychiatric distress(P<0.05) and internet addiction (P<0.01) werefound significantly associated with the gender ofthe respondents. These findings were similar to aprevious study conducted in south India and Iran.11-
14In contrast the present finding, a study conductedby Gupta et al in Delhi, they found no significantrelationship between internet addiction and

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 329
gender.15
And the average time of daily internet use (inhours) among male was found comparatively higherthan female respondents. And the majority of therespondents were using the internet for socialnetworking in both genders, but the majority of thegirls were using the internet for academic purpose.In another study conducted by Srijampana et alconducted in Andhra Pradesh reported a similarfinding to the present study.16
Findings of the presents study indicate that therewas a significant difference in the prevalence ofpsychiatric distress and internet addiction betweenmale and female young adults. Psychiatric distress andinternet addiction were found more prevalent amongmale compared to female. The studies conducted bySrijampana et al,17 Kawa and Shafi,18 Subhashini andPraveen,19 and Alhajjar20 had reported similar findingsin their studies.16-19
Findings of the present study also indicate thattime spent on internet use, psychiatric distress andinternet addiction have a significant positivecorrelation. More time spent in using the internetdaily (in hours) will increase the prevalence rate ofinternet addiction and psychiatric distress amongstudents. Similar to the present findings a studyconducted by Alhajjar B. in Gaza-Palestine foundthat internet addiction and psychiatric distress arepositively correlated to each other. In another studyconducted in Jordan found that internet addictionwas significantly associated with the mentaldistressamong the students.21 ElSalhy et al foundtheir study that internet addiction was significantlypositively associated with time serpent in theinternet use, social networking and psychiatricdistress among students and had a significantnegative correlation with using internet foracademic purpose.22
LimitationsThere are some limitations in the present study;• The sample size was too small.• The data collected from only a small study
area.• There was a lack of randomization in
sampling methods.• Uneducated young adults were not included
in the present study.Therefore the results of the present study may
not be generalized for the whole population.
ConclusionDespite the noted limitations, the present study
has provided some important information regardingthe prevalence of internet addiction (IA) andpsychiatric distress among Indian college goingyoung adults. Findings indicate that IA andpsychiatric distress has a significant associationwith the gender of the students. Male students havemore risk of getting affected by IA and psychiatricdistress compared to female students. The study alsoindicates that daily time spent (in hours) has apositive relationship with IA and psychiatricdistress. And IA and psychiatric distress alsopositively correlated with each other. Therefore,there should some awareness programs beconducted to aware them about IA and psychiatricdistress to prevent them from other majorpsychiatric disorders.
AcknowledgementsWe are very thankful to the volunteers named
Mr. Ved Prakash Tiwari, Mr. Rameshwar Kumar,Miss Samiksha and Miss Jyoti Joanna Kisku(Students of MA in Social Work, Banaras HinduUniversity, Varanasi), who helped us in the datacollection, And all the respondents who participatedin the present study.
References1. Sulania A, Sachdeva S, Dwivedi N. Risk of
internet addiction among undergraduatemedical, nursing, and lab technology studentsof a health institution from Delhi, India. DigitMed 2015; 1 : 72-82.
2. Internet Live Stats. Available from: http://www.internetlivestats.com.[Last accessed on2019 June 5].
3. Shaw M, Black DW. Internet addiction. CNSDrugs 2008; 22(5) : 353-65.
4. Cheng YS, Tseng PT, Lin PY, Chen TY, StubbsB, Carvalho AF, Wu CK, Chen YW, Wu MK.Internet Addiction and Its Relationship WithSuicidal Behaviors: A Meta-Analysis ofMultinational Observational Studies. J ClinPsychiatry 2018; 79(4):pii: 17r11761. doi:10.4088/JCP.17r11761.
5. Anderson EL, Steen E, Stavropoulos V. Internet

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society330
use and Problematic Internet Use: A systematicreview of longitudinal research trends inadolescence and emergent adulthood. Int JAdolesce Youth 2017; 22(4) : 430-54.
6. Balhara YP, Mahapatra A, Sharma P, BhargavaR. Problematic internet use among students inSouth-East Asia: Current state of evidence.Indian J Public Health 2018; 62(3) : 197.
7. Su W, Han X, Jin C, Yan Y, Potenza MN. Aremales more likely to be addicted to the internetthan females? A meta-analysis involving 34global jurisdictions. Computer Human Behav2019; 99 : 86-100.
8. Anand N, Jain PA, Prabhu S, et al. Prevalenceof excessive internet use and its association withpsychological distress among universitystudents in South India. Ind Psychiatry J 2018;27(1) : 131.
9. Frangos CC, Frangos CC, Sotiropoulos I. Ameta-analysis of the reliabilty of young’sinternet addiction test. In: Proceedings of theWorld Congress on Engineering. London,United Kingdom: World Congress onEngineering 2012; 1 : 368-371.
10. Young K. Internet addiction test (IAT). Stoelting2016. Accessed from https://www.stoeltingco.com/media/wysiwyg/IAT_web_sample.pdf
11. Goldberg D. Manual of General HealthQuestionnaire. Windsor: NFER PublishingCompany 1978.
12. Jain T, Mohan Y, Surekha S, et al. Prevalenceof internet over use among undergraduatestudents of a private university in South India.Int J Recent Trends Sci Technology 2014; 11 :301-4.
13. Sushma J, Ahmed M, Amrutha AM. A study toassess internet addiction among undergraduatemedical students of MMC & RI, Mysore. Int JCommunity Med Public Health 2018; 5(7) :2984-8.
14. Poorolajal J, Ghaleiha A, Darvishi N, Daryaei
S, Panahi S. The prevalence of psychiatricdistress and associated risk factors amongcollege students using GHQ-28 questionnaire.Iran JPublic Health 2017; 46(7) : 957.
15. Subhaprada C, Kalyani P. A cross-sectionalstudy on internet addiction among medicalstudents. Int J Community Med Public Health2017; 4(3) : 670-4.
16. Gupta A, Khan AM, Rajoura OP, Srivastava S.Internet addiction and its mental healthcorrelates among undergraduate collegestudents of a university in North India. J FamMed Prim Care 2018; 7(4) : 721.
17. Srijampana VV, Endreddy AR, Prabhath K,Rajana B. Prevalence and patterns of internetaddiction among medical students. Med J Dr.DY Patil University 2014; 7(6) : 709.
18. Kawa MH, Shafi H. Evaluation of internetaddiction and psychological distress amonguniversity students. International Journal ofModern Social Sciences 2015; 4(1) : 29-41.
19. Subhashini KJ, Praveen G. An era of digitalslavery: a study on internet addiction amongprofessional college students of Hassan,Karnataka. Int J Community Med PublicHealth. 2018; 5(7) : 2977-83.
20. Alhajjar B. Internet addiction and psychologicalmorbidity among nursing students in Gaza-Palestine. Internet addiction and psychologicalmorbidity among nursing students in Gaza-Palestine. Am J Appl Psychol 2014; 3(4).
21. Al Gamal E, Alzayyat A, Ahmad MM.Prevalence of Internet Addiction and Its Asso-ciation With Psychological Distress and CopingStrategies Among University Students inJordan. Persp Psychiatr Care 2016; 52(1) : 49-61.
22. El Salhy M, Miyazaki T, Noda Y, et al. relation-ships between internet addiction and clinico-demographic and behavioral factors. Neuro-psychiatr Dis Treat 2019; 15 : 739.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 331
Cognitive advantage of second-generation anti-psychotics against combination of first-generation
anti-psychotic and anti-cholinergic drugsSunny Chattopadhyay,1 Om Prakash Singh,2 Debanjan Saha3
1,3Psychiatrist, NRSMC, Kolkatta2Psychiatrist, Department of Health & FW, Govt of W.B.
Contact: Sunny Chattopadhyay, E-mail: [email protected]
Original Article
IntroductionCognition is the sum total of mental processes
that makes us acquire knowledge and keeps usaware of our surroundings and thus enables us toarrive at appropriate judgments.1 Cognitive deficitsare core features of schizophrenia. Cognitivedeficits are the key factors determining functionaloutcome and quality of life.2 Bleuler explaineddelusions and hallucinations were secondary tocognitive changes. There is an increased need for aprecognitive drug with robust improvement inneurocognitive biomarkers for improved functionaloutcome. Improved understanding of the pharmaco-dynamics shall help in drug development.
In meta-analytic studies, Antipsychotics notonly showed improvement of improve positive and
negative symptoms, but improvements in cognitivedeficits have also been noted, though varying.3
Typical antipsychotics otherwise known as first-generation antipsychotic medications reducehallucinations, delusions, behavior problems andrisk for relapse. Predominantly acting on D2receptors, they also bind to histamine H1 receptors,muscarinic M1 receptors, and adrenergic NE1receptors.4-5 These fail to adequately amelioratenegative and cognitive symptoms. 5,6 Second-generation antipsychotics or atypicals benefitnegative and cognitive symptoms.7 A possibleexplanation for this could be a blockade of 5-HT2aand a weaker blockade of D2 relative to typical.8,9
Speed of processing has been noted to be mostsignificantly impaired in patients of schizo-
Abstract
Introduction: Cognitive deficits are core features of schizophrenia and determine functionaloutcome and quality of life. The cognitive benefit a drug produces becomes important in choosingthe antipsychotic. Objective: To compare the cognitive benefits of typical and atypicalantipsychotics in stable patients of schizophrenia. Method: On obtaining ethical clearance weenrolled stable patients of schizophrenia into two groups based on the medication they weretaking. It was a case control design. Only one antipsychotic must have been used throughmajority of the course of treatment. After screening by GHQ and assessing remission by PANSS,different tests of neurocognition were applied. Information obtained was analyzed by appropriatestatistical methods. Mann-Whitney U test was applied to compare the significance of differenceof means between groups. Results: Patients on atypical antipsychotics performed better in alldomains of neuro-cognition except executive function. Conclusion: Atypical antipsychotics asa class offer distinct neuro-cognitive advantages which should be considered in choice of drugfor schizophrenia.
Key Words: Schizophrenia, Dopaminergic, Prefrontal, Working memory, Attention.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society332
phrenia.10 It is determined by visual scanning, motorscanning, and co-ordination. The variation in thepharmacokinetics of different anti-psychoticscauses a varying impact on the speed of processing.
Cognitive deficits as a principle feature ofschizophrenia render individuals deficient inacquiring a new skill and making them sociallyisolated even in remission.11 This raises the searchfor measures to address cognitive impairments.Substantial cognitive improvement was reported tobe produced by atypical antipsychotics in a meta-analysis of 12 studies.12 In a study patients treatedwith typicals continued to show low p50 suppre-ssion, while those on a typicals had improved.13 Inrodents, learning and memory impairments thatwere produced by stress and neurotoxin wereattenuated by atypical antipsychotic drugs.14 Thesehave been explained by augmented synapticplasticity in hippocampal-prefrontal pathway andmodulation of muscarinic and glutaminergictransmission.15 Olanzapine has produced improvedmemory relative to haloperidol and risperidone.16
Again, risperidone was found to improve workingmemory.17,18 Clozapine impaired working memorybut improved semantic memory.19,20 Clozapine is apartial agonist at D1 and potent antagonist of D4,both of which are present in the prefrontal cortex,the area implicated in neurocognition. In anothermeta-analysis, it was shown that except for largedoses benefit produced by haloperidol was similarto others. This raises the need for comparing theneuro-cognitive benefits of typical and atypical.,proceeding with the hypothesis that atypicalantipsychotics have a cognitive advantage overtypical antipsychotics.The null hypothesis that nosignificant difference exists between groups wasformulated.
MethodologyIt was a cross-sectional tertiary hospital-based
study by purposive sampling. Subjects wereassigned to groups based on their history of drugused. Each group had 30 patients.
SamplingWe enrolled all successive patients as per
inclusion and exclusion criteria who consented toparticipate. The study was conducted at NilratanSircar Medical College, Kolkata. Ethical clearance
was provided by the institutional ethical clearancecommittee. All patients of schizophrenia inremission (stable) attending Psychiatry OPD andpatients admitted in the psychiatry ward wereincluded in the study.Inclusion and Exclusion criteria
Samples included people between 18-50 years,who were educated in English up to at least 10th
and consented to participate in the study. We usedtests standardized on Indian Population, that wereavailable in English, hence only subjects educatedin English were chosen.20 As use of multipleantipsychotic may interfere with the objective ofthe study, so subjects whose treatment recordsshowed use of only one antipsychotic through themajority of the course of treatment were included.Patients who had co-morbid conditions such as drugabuse except for nicotine dependence, affectivedisorders, dementia, mental retardation, history ofhead injury and seizure within one-year durationwere excluded. Those receiving benzodiazepineswithin one month and ECT within the last 6 monthswere also excluded. Any patient who was onatypical antipsychotic along with anticholinergicwere also excluded.Screening and Assessment
A specially prepared proforma was used tocollect the patient’s socio-demographic data whichincluded age, gender, educational status, residentialstatus, socio-economic status, past history, familyhistory, personal history, general physical examina-tion, systemic examination, and mental statusexamination. The International Classification ofDiseases(ICD-10 DCR) 10th edition diagnosticcriteria for Psychiatric Illnesses by WHO was usedto diagnose each patient (World HealthOrganization, 1993). Mental retardation was ruledout by screening all subjects by Raven’s ColoredProgressive Matrices. All subjects were screenedby the Positive and Negative Syndrome Scale(PANSS) for assessing the severity of illness inschizophrenia.22 The accepted criteria for remissionas in literature was PANSS score of < 3 for all itemsin the last 6 months.22 GHQ-28 was used forchecking the presence of any psychiatric comorbi-dity.
Speed of Processing was accessed by digitsymbol substitution test.21 In it the time taken to

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 333
perform the task was measured. Verbal workingmemory was tested by N-Back test and visualworking by Visual N-Back.21 Verbal learning wastested by the paired association test. In it the numberof pairs correctly reproduced forms the score.23
Visual learning was tested by PGI-visualrecognition test.24 In it a correctly identified andnaming of the object is given 1 mark while a correctidentification but wrongly naming fetched ½ mark.Attention and concentration were tested by digitforward, digit backward and serial subtraction test.25
Animal name and design fluency tests were usedfor assessment of executive function. In it thenumber of items generated is the score.21
Data Analysis Data obtained weretabulated, means, standard
deviation, and percentages were calculated. Mann-Whitney U test was applied to compare the signi-ficance of the difference of means between groups.The critical value of U was calculated to be 119.P<0.05 was considered significant. The nullhypothesis that no significant difference existsbetween groups was formulated.We used Epi Info7 for analysis of data.
Results
Table-1: Demographic Variables
Variable Typicals + Atypicals PAnti-cholinergic n=30
n=30
Sex (Male) 20 (67%) 18 (59%) 0.01Age (years) 30.28 ± 7.24 30.27 ± 7.17 0.50Education School 11(35.5%) 6 (21.6%) 0.76
High School 5(17.6%) 4 (13.5%)Graduate 6 (20.6%) 7 (24.3%)Post Grad 2 (5.9%) 2 (5.4%)
Professional 6(20.6%) 11 (35.1%)GHQ Score 6.03 ± 1.14 2.00 ± 0.81 < 0.001
the two groups as criteria for remission is based oneach individual item, where the score in each shouldbe less than three.22
In most cases, patients on typical antipsychoticsrequire the administration of a centrally actinganticholinergic while atypical drugs are known bythe rarity of such side effects. Anticholinergic drugsare known to affect muscarinic transmission andimpact cognitive pathways. In practical circum-stances as typical drugs are combined with anti-cholinergic drugs studying the effect of this drug,the combination would be of clinical relevance. Itcreated a real-life scenario in a naturalistic study.
Reduced speed of processing is enduringfeatures in schizophrenia.23 Speed of processing wasmeasured by the digit symbol substitution test thatmeasures the amount of work done in the fixed time.Patients on atypicals fared better significantly.Improvements with large effect size have beenreported to be produced by atypical drugs in variousmeta-analysis.26 Digit symbol substitution isdetermined by visual scanning, motor scanning, andco-ordination. The greater propensity of extra-pyramidal effects of typical antipsychotics has beenhypothesized by many for this difference. Theeffects on motor system like extrapyramidal
DiscussionThe present study intended to compare the
cognitive functions of patients with respect to drugsused. Patients on atypical antipsychotics fared betterin all domains of neuro-cognition except forexecutive function. Comparison of the demographiccharacteristics shows samples were matched withrespect to age and duration of illness. There is asignificant difference in the total PANSS scores of
syndrome that typical antipsychotics often producehas been suggested as the reason for this difference.Dickinson had observed a direct relationshipbetween the dose of anti-psychotic and the amountof impairment inspeed of processing.12
Working memory includes verbal memory andvisual memory. N-Back test was used for verbalworking memory assessment. Visual N-Back issimilar to verbal N-Back test where unlike in the

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society334
Table-2: Comparison between two groups of patients in remission
Typicals + Anti-cholinergic Atypicals pn=30 n=30
Age of Patients 31.67 (6.46) 30.70 (7.81) 0.68Duration of Illness 3.85 (2.43) 4.11 (1.93) 0.70GHQ Score 0.7 (0.67) 0.61 (0.0) 0.69PANSS Total 18.36 (1.30) 15.95 (1.23) <0.001
Speed of Processing
Digit Symbol Substitution Test 240.79 (19.7) 261.75 (19.33) 0.001
Working Memory
N-Back-1-Hit - Verbal 5.4 (1.21) 7.1 (1.04) <0.001N-Back-1-Eror - Verbal 4.74 (1.48) 3.00 (0.92) <0.001N-Back-2-Hit - Verbal 4.6 (2.11) 4.27 (1.17) 0.98N-Back-2-Eror - Verbal 7.37 (1.54) 5.25 (1.74) <0.001N-Back-1-Hit - Visual 5.37 (1.21) 7.10 (1.02) <0.05N-Back-1-Eror - Visual 6.16 (1.21) 4.50 (0.69) <0.05N-Back-2-Hit - Visual 2.68 (0.48) 4.75 (0.44) <0.001N-Back-2-Eror - Visual 6.63 (1.42) 4.70 (0.92) <0.001
Verbal Learning -
Paired Assoc -Similar Pair 3.68 (067) 5.54 (1.43) <0.001Paired Assoc Dis-Similar Pair 3.00 (0.82) 4.8 (1.51) <0.001
Visual Learning
PGI- Visual repetitive Card 5.21 (0.98) 6.35 (0.75) <0.001
Attention & Vigilance
Digit Forward 3.16 (1.12) 5.25 (1.77) <0.001Digit Backward 2.79 (0.63) 4.75 (1.16) <0.001Serial Subtraction– 7 1.16 (0.37) 1.45 (0.51) 0.04
Executive Function Tests
Animal Name Test 11.42 (0.69) 11.50 (0.61) 0.70Design Fluency- Free 8.32 (1.06) 8.25 (0.97) 0.65Design Fluency- Fixed 3.37 (0.96) 3.45 (0.60) 0.75
previous one in which the task is to identify wordsheard, here the subject has to identify the positionof a dot in a card and compare it with the previousone. Patients on atypical had significantly betterworking memory.21 Deficiency of dopamine inprefrontal cortex is postulated to cause deficits ofworking memory.27 Atypicals improve workingmemory by increasing dopamine in frontal cortex.28
Risperidone has been reported to improve workingmemory as a whole.28,29
Learning involves obtaining information andretrieving it later. Dopamine has an important effecton learning from experiences. The improvedmemory by atypicals may be explained by better
availability of dopamine that atypicals produce.Atypical antipsychotics improve the availability ofdopamine, which in turn may improve learning.Moreover, typicals tend to affect cholinergicsystems through their muscarinic effects. Clozapineand olanzapine have been reported to produceimprovement in verbal learning.28,2927,28
Patients on atypicals showed significant betterattention span. In studies, 5-HT2 antagonists havebeen found to benefit attention. Atypical anti-psychotics exhibit 5-HT2 antagonistic actions.
Patients on atypicals did not exhibit any advan-tage with respect to typical on executive function.Executive function involves multiple networks like

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 335
prefrontal-striate-thalamic, prefrontal-parietal, andprefrontal-temporal neural networks, hence thedifference. The effects that the drugs might haveon these pathways would be a complicated one topredict. Probably executive function would involvepathways different from other domains.30
This study shows atypical antipsychotics to behaving distinct cognitive advantages over typicalexcept for executive functions.
Strengths: 1. Tests standardized for Indianpopulation was applied.21
2. Groups were matched with respect toeducation, age, and IQ which affect cognition.
3. Criteria of remission were PANSS score of< 3 each individual item.
Weakness: In general hospital-based studysample size remained a constraint.
References1. Sadock BJ, Sadock VA. Kaplan & Sadock’s
Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. 10th ed. Philadelphia (PA):Lippincott Williams & Wilkins 2007 : 275.
2. Sharma T, Antonova L. Cognitive function inschizophrenia. Deficits, functional consequen-ces, and future treatment. Psychiatr Clin NorthAm 2003; 26 : 25-40.
3. Keefe RSE, Silva SG, Perkins DO, LiebermanJA. The effects of atypical antipsychotic drugson neurocognitive impairment in schizophrenia:a review and meta-analysis. Schizophr Bull1999; 25(2) : 201–222.
4. Blyler CR, Gold JM. Cognitive effects oftypical antipsychotic treatment: another look.In: Sharma T, Harvey PD; editors. Cognitionin Schizophrenia. NY, USA: Oxford UniversityPress 2000; 241-265.
5. Spohn HE, Strauss ME. Relation of neurolepticand anticholinergic medication to cognitivefunctions in schizophrenia. J Abnorm Psychol1989; 98 : 367–380.
6. Honey GD, Bullmore ET, Soni W, VaratheesanM, Williams SCR, Sharma T. Differences infrontal cortical activation by a working memorytask after substitution of risperidone for typicalantipsychotic drugs in patients with schizo-phrenia. Pro Natl Acad Sc USA 1999; 96 :13432–7.
7. Kane J, Honigfeld G, Singer J, Meltzer H.
Clozapine for the treatment-resistant schizo-phrenic. A double-blind comparison with chlor-promazine. Arch Gen Psychiatry 1988; 45(9) :789–796.
8. Altar CA, Wasley AM, Neale RF, & Stone GA.Typical and atypical antipsychotic occupancyof D-2 and S-2 receptors: an autoradiographicanalysis in rat brain. Brain Res Bull 1986; 16 :517–525.
9. Meltzer HY, Matsubara S, Lee MJ. The ratiosof serotonin-2 and dopamine-2 affinitiesdifferentiate atypical and typical antipsychoticdrugs. Pharmacol Exp Ther 1989; 251 : 238–246.
10. Dickinson D, Ramsey ME, Gold JM. Over-looking the obvious: a meta-analytic compari-son of digit symbol coding tasks and othercognitive measures in schizophrenia. Arch GenPsychiatry 2007; 64(5) : 532–542.
11. Green MF: What are the functional conse-quences of neurocognitive deficits in schizo-phrenia? Am J Psychiatry 1996; 153 : 321–330.
12. Keefe RSE, Silva SG, Perkins DO, LiebermanJA. The effects of atypical antipsychotic drugson neurocognitive impairment in schizophrenia:a review and meta-analysis. Schizophr Bull1999; 25(2) : 201–222.
13. Keedy SK, Rosen C, Khine T, Rajarethinam R,Janicak PG, Sweeney JA. An fMRI study ofvisual attention and sensorimotor functionbefore and after antipsychotic treatment in first-episodeschizophrenia. Psychiatr Res 2009;172(1) : 16–23.
14. Luo C, Xu H, Li XM. Quetiapine reverses thesuppression of hippocampal neurogenesiscaused by repeated restraint stress. Brain Res2005; 1063(1) : 32–89.
15. Spohn HE, Strauss ME. Relation of neurolepticand anticholinergic medication to cognitivefunctions in schizophrenia. J Abnorm Psychol1989; 98 : 367–380.
16. Cassens G, Inglis AK, Appelbaum PS, GutheilTG. Neuroleptics: effects on neuropsycho-logical function in chronic schizophrenicpatients. Schizophr Bull 1990; 16(3) : 477–499.
17. Meltzer HY, McGurk SR. The effects ofclozapine, risperidone, and olanzapine oncognitive function in schizophrenia. SchizophBull 1999; 25 : 233–256.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society336
18. Gray JA, Feldon J, Rawlins JNP, HemsleyDR,Smith AD. The neuropsychology of schizo-phrenia. Behav Brain Sci 1999; 14 : 1–84.
19. Heaton R, Paulsen JS, McAdams LA, Kuck J,Zisook S, Braff D, et. al. Neuropsychologicaldeficits in schizophrenics. Relationship to age,chronicity, and dementia. Arch Gen Psychiatry1994; 51 : 469–476.
20. Palmer BW, Heaton RK, Paulsen JS, Kuck J,Braff D, Harris MJ, et al. Is it possible to beschizophrenic yet neuropsychologicallynormal? Neuropsychology 1997; 11 : 437–446.
21. Rao SL, Subbakrishna DK, Gopukumar K.NIMHANS Neuropsychology Battery-2004Manual. Bangalore: National Institute ofMental Health and Neurosciences (DeemedUniversity) 2004.
22. Keshavan MS. Cognitive impairment,especially executive dysfunction and memoryloss, is a key diagnostic component ofschizophrenia. J Clin Psychiatry 2009; 70(suppl1) : 13-16.
23. Pogue-Geile MF, Harrow M. Negative andpositive symptoms in schizophrenia anddepression: A follow up. Schizophr Bull 1984;10 : 371-87.
24. Pershad D, Verma SK. Handbook of PGIBattery of Brain Dysfunction (PGI-BBD). Agra:National Psychological Corporation 1990; 70-111.
25. Chapman LJ, Chapman JP. The measurementof differential deficit. J. Psychiatry Res 1978;14 : 303–311.
26. Woodward ND, Purdon SE, Meltzer HY, ZaldDH. A metaanalysis of neuropsychologicalchange to clozapine, olanzapine, quetiapine,and risperidone in schizophrenia. Int JNeuropsychopharmacol 2005; 8 : 457-472.
27. Carpenter WT, Gold JM. Another view oftherapy for cognition in schizophrenia. BiolPsychiatry 2002; 51(12) : 969–971.
28. Perlick D, Stastny P, Katz I, Mayer M, MattisS. Memory deficits and anticholinergic levelsin chronic schizophrenia. Am J Psychiatry1986; 143(2) : 230–232.
29. Blomqvist AG, Leger PT, Hoch JS. The cost ofschizophrenia: lessons from an internationalcomparison. J Ment Health Policy Econ 2006;9(4) : 177–183.
30. Cassens G, Inglis AK, Appelbaum PS, GutheilTG. Neuroleptics: effects on neuropsycho-logical function in chronic schizophrenicpatients. Schizophr Bull 1990; 16(3) : 477–499.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 337
A study of Socio-demographic andPsychosexual dysfunctions in female patients with
Depression and Anxiety disorderRitu Meena,1 Tushar Jagawat,2 Krishna Kanwal,3 Bajrang Lal,4 Pankaj Tondon5
1,2,4,5Department of Psychiatry, National Institute of Medical Sciences & Research, Jaipur, Rajasthan, IndiaProfessor and HOD3 at Jaipur National University, Jaipur, Rajasthan, India
Contact: Tushar Jagawat, Email: [email protected]
Original Article
IntroductionWomen’s sexual problems were cast as techni-
cal problems to be understood in terms of socialphenomena and resolved through educationregarding the profound physical, emotional andspiritual differences between men and women.1
Normal sexual behavior brings pleasure to his or
her along with partner that involves in stimulationof the primary sex organs including coitus; it is freefrom the feeling of anxiety or guilt and is notcompulsive.2 So the disturbance in normal sexualresponse cycle is related with many psychosexualdisorder.3 As the female sexual dysfunctions aretaboo subject for the discussion in many places
Abstract
Background: Psychosexual disorders are common all over the world, but very few studies aredone which are related with female sexual dysfunctions. Most of the studies are done on malesexual dysfunctions. It is very important to understand that how sexual beliefs, values andattitudes act and effect these problems. Aim and Objectives: To find out the pattern of sexualproblems among female patients with Anxiety and Depression. Material and Methods: Thestudy conducted in department of psychiatry of National Institute of Medical Sciences Researchand Hospital, Jaipur. The duration of the study was for 6 months.The Study consisted of 147consecutive female subject with diagnosis of anxiety and depression according toICD10.Hamilton rating scale for anxiety (HAM-A) used in study on subject to know the severityof anxiety , Hamilton rating scale for depression (HAM-D) applied for measuring the severitydepression and Arizona Sexual Experience Scale (ASEX) for assessing the sexual dysfunctions.Subjects were assessed by using ICD-10 criteria. Results: Total 147 female subjects were takenout of which 78 were of anxiety and 69 were of depression. Total 46 female subjects werehaving sexual dysfunctions out of 147 subjects .Out of 46 subjects 26 were having depressionand remaining 20 were having anxiety. Most common age group of depressive subjects withsexual dysfunction were 18-28 years 46.2% , 50.1% subjects were illiterate and 53.8% werehaving loss of sexual desire and 46.2%% were complaint of orgasmic dysfunction. And mostcommon age groupof subjects with anxiety disorder associated with sexual dysfunctions were18-28 years 55%and. while60% of patients belongs to nuclear family while 45% patients wereHindu and 50% subjects were illiterate and lack of sexual desire was 50 %, sexual aversion35%, lack of sexual enjoyment 15%. Conclusion: The study focusses on the psychosexualdysfunctions associated with psychiatric disorders and need for careful identification of sexualdysfunctions.Key words: Depression, Anxiety and Female sexual dysfunctions.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society338
which ultimately creates the negative effects whichmay include familial conflict and even divorce.4 Soit is very important to create awareness aboutfemale sexual dysfunctions which may help in earlydiagnosis and management of sexual dysfunctions.5
The epidemiological studies done on female sexualdysfunctions are very less due to which there areless data available on prevalence of sexual problemsassociated with female.6 So it is difficult to knowthe exact number of patients suffering from sexualproblems.7 It may be due negligence of medicalpractitioner or hesitancy of female patients indiscussing sexual problems.8 So there is a need forresearch on female sexual dysfunctions.9
Female Sexual Response Cycle2
Normal sexual response cycle was firstdescribed by Master and Johnson in 1966 andconsists of phases: Desire, Excitement, Plateau,Orgasm, Resolution.3
Psychosexual Dysfunctions According to ICD -10:10
F 52.0 Lack or Loss of Sexual DesireF 52.1 Sexual Aversion and Lack of Sexual
EnjoymentF 52.1 -0 Sexual AversionF 52.1 -1 Lack of Sexual EnjoymentF 52.2 Failure of Genital ResponseF 52.3 Orgasmic DysfunctionF 52.5 Nonorganic VaginismusF 52.6 Nonorganic DyspareuniaF 52.8 Other Sexual Dysfunctions, not caused
by organic disorder or diseaseF 52.9 Unspecified sexual dysfunction, not
caused by organic disorder
Aims & ObjectivesThe specific objectives of study were to study:1. The pattern of psychosexual problems
among female patients.2. The socio-demographic correlates of
various psychosexual disorders.3. The clinical correlates of various psycho-
sexual disorders.
Material and Methods This study was done in out-patient department
(OPD) of psychiatry in National Institute of MedicalSciences and Research, Medical College and
Hospital, Jaipur. Study population consisted of thesubjects who have fulfilled the inclusion andexclusion criteria. The privacy and confidentialityof the subjects were ensured and maintained. Theduration of study was for 6 months. The Studyconsisted of 147 female subjects with depressionand anxiety disorder diagnosed on the basis of ICD10 criteria out of which 46 female subjects werehaving sexual dysfunctions along with depressionand anxiety disorder. The Severity was assessed byHamilton rating scale for anxiety (HAM-A),Hamilton rating scale for depression (HAM-D)applied for measuring the severity of depressionand Arizona Sexual Experience Scale (ASEX) forassessing the sexual dysfunctions.
Inclusion Criteria1. All female patients with age group of 18
years to 50 years who attended psychiatryOPD of NIMS Hospital, Jaipur.
2. Healthy, married and sexually activefemales.
3. Who gave a written informed consent forparticipating in the study.
4. Meeting the criteria for Depression andAnxiety disorder according to ICD-10.
Exclusion Criteria1. The cases below 18 years and above 50
years of age.2. Women who were not living with their
husbands in the previous six months.3. The cases with preexisting significant
medical, gynecology, genitourinary,surgical, organic brain disorders and mentalretardation, psychosis, bipolar disorder andsubstance use disorder.
4. Postmenopausal women were excluded.
ResultsThe sample comprised of 147 female subjects
with diagnosis of depression and anxiety disorder.Out of 147 female subjects 46 were having sexualdysfunction associated with depression and ofanxiety disorder and out of 46 subjects 26 (56.5%)subjects were of depression and 20 (43.5%) wereof anxiety disorder.
The Table 1 shows that most common agegroup of depression with sexual dysfunctions wereof 18-28 years 46.2% and most of the subjects were

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 339
illiterate 50.1%,muslim 36.8% were living innuclear family 42.4%.
Table-1: Socio-demographic profile of patientswith Depression
Age group Patient with depression N=26 (%)
18-28 year 12 46.229-39 year 9 34.640-50 year 5 19.2Family typeNuclear 11 42.4Joint 15 57.6ReligionHindu 8 30.7Muslim 10 38.6Sikh 8 30.7EducationIlliterate 13 50.1Primary 6 23.1Middle 3 11.6Secondary 2 7.6College 2 7.6
Table-2: Clinical profile of Depression patients
Referred Patient with depression N=26 (%)
Direct 12 46.2Medicine 9 34.6Skin 5 19.2Years of marriage (%)0-5 years 15 57.66-10 years 11 42.4No of sexual dysfunctionsOne 8 30.7Two 10 38.6Three or more 8 30.7Psychosexual Number of dysfunction N=26 (%)dysfunction (Depression)According toICD-10F 52.0 14 53.8F 52.3 12 46.2
The Table 2 shows that most of the subjectscame directly to the psychiatry OPD were 46.2%while 34.6% were referred by medicine department.Most of the subjects complains of lack of sexualdesire 53.8% and years of marriage (0-5) associatedwith sexual dysfunctions were 57.6%
The Table 3 shows that most common agegroup of Anxiety disorder with sexual dysfunctionswere of 18-28 years 55% and most of the subjectswere illiterate 50%, Hindu 45 % were living in jointfamily 60%.
Table-3: Socio-demographic profile of patientswith Anxiety disorder
Age group Patient with Anxiety disorder (%)N=20
18-28 year 11 5529-39 year 6 3040-50 year 3 15Family type (%)Nuclear 8 40Joint 12 60Religion (%)Hindu 9 45Sikh 4 20Muslim 7 35Education (%)Illitrate 10 50Primary 6 30Middle 3 15Secondary 1 5College
Table-4: Clinical profile of patients withAnxiety disorder
Reference Patient with Anxiety disorder (%)N=20
Direct 15 75Medicine 5 25Year of marriage (%)0-5 years 8 406-10 years 12 60No of sexual dysfunctionsSingle 13 65Two 7 35Three or more 0Psychosexual dysfunction (%)According to ICD-10F52.0 10 50F52.1 7 35F52.1-1 3 15
The Table 4 shows that most of the subjectscame directly to the psychiatry OPD were 75%while 25% were referred by medicine department.Most of the subjects complains of lack of sexualdesire 50% and years of marriage (6-10) associatedwith sexual dysfunctions were 60%.
DiscussionThe current study was done in department of
psychiatry, National Institute of Medical Sciencesand Research Hospital and Medical College, Jaipur.The sample comprised of 147 female subjects withdiagnosis of Depression and anxiety disorder. Out

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society340
of 147 female subjects 46 were having sexualdysfunction associated with Depression and ofanxiety disorder. And out of 46 subjects 26 (56.5%)subjects were of depression and 20 (43.5%) wereof anxiety disorder. In current study, we founddifferent sexual dysfunctions associated withdepression and anxiety. 53.8% were having lack ofsexual desire and 46.2% were having orgasmicdysfunction was found in patients with depression.While in study doneon 904 female subjects byFabreetal., 17.7% female subjects were having lackof sexual desire, sexual aversion 3.2% and orgasmicdysfunction was 7.5%.11 The reason for higherpercentage of sexual dysfunction in our study mayto due difference in sample size as compare to otherstudies. And study done by Pereria et al, 2013, on155 female subjects of both anxiety and depressionand found that anxiety was 36.1%, depression was21.9% and lack of sexual desire 52.9%, orgasmicdysfunction was 39.4%.8
ConclusionThe psychosexual dysfunctions are commonly
associated with psychiatric disorders in women andthere is a need for careful identification of sexualdysfunctions comorbid in patients with depressionand anxiety disorders.
Limitations1. Hospital based study.2. Small sample size.3. Only took females with active menstrual
cycle.
References1. Om Prakash, Rao T. Sexuality research in India:
An update. Indian J Psychiatry 2010; 52 : 260-263.
2. Sadock VA. Normal human sexuality andsexual dysfunctions. In: Sadock BJ, Sadock VA,Kaplan HI, editors. Kaplan and Sadock’s
Comprehensive Textbook of Psychiatry. 9th ed.Philadelphia: Lippincott Williams and Wilkins,2009; 2027-2060.
3. Master WH & Johnson VE: Human SexualInadequacy. Boston: Little, Brown 1970.
4. Safarinejad MR. Female sexual dysfunction ina population-based study in Iran: prevalenceand associated risk factors. Int J Impot Res2006; 18(4) : 382-395.
5. Viswanathan S, Prasad J, Jacob KS, KuruvillaA. Sexual function in women in rural TamilNadu: disease, dysfunction, distress and norms.Natl Med J India 2014; 27(1) : 4-8.
6. Rao TS, MS Darshan, Tandon A. An epidemio-logical study of sexual disorders in south Indianrural population. Indian J Psychiatry 2015; 57: 150-157.
7. Kendurkar A, Kaur B. Major DepressiveDisorder, Obsessive-Compulsive Disorder, andGeneralized Anxiety Disorder: Do the SexualDysfunctions Differ? Prim Care Companion JClin Psychiatry 2008; 10(4) : 299–305.
8. Pereria MV, Nardi EA, Silva CA. Sexualdysfunction, depression, and anxiety in youngwomen according to relationship status: anonline survey. Trends Psychiatry Psychother2013; 35(1) Porto Alegre. http://dx.doi.org/10.1590/S2237-60892013000100007
9. Avasthi A, Kaur R, Prakash O, Banerjee A,Kumar L, Kulhara P. Sexual behavior ofmarried young women: a preliminary studyfrom north India. Indian J Community Med2008; 33(3) : 163-7.
10. World Health Organization. The ICD-10Classification of Mental and BehavioralDisorders; Clinical Description and DiagnosticGuidelines. Geneva: WHO 1992.
11. Fabre LF, Smith LC. The effect of majordepression on sexual function in women. J SexMed 2012; 9 : 231-239.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 341
Sexual Health Related Issues among IndianUnmarried Undergraduate Male Students:
A SurveyVivek Kumar, Apoorv Yadav, Surendra Pal Bharti
Department of Psychiatry, NSCB Subharti Medical College, SVSU, Meerut, 250005Contact: Vivek Kumar, [email protected]
Original Article
IntroductionSex is a widely discussed topic everywhere in
the world. Since the beginning ofour education anduntil we become young adults, the knowledge ofsex are very restricted, particularly in young males.The lack of formal sex education predisposes us tofalling into the trap of various myths regarding sexand sexuality which has shown a high prevalencein studies.1-5 Instead of true facts what we’re taughtis an amalgamation of falsities and other culturebound myths especially regarding topics such asmasturbation, penis size, importance of semen, andphenomenon such as nightfall, premature ejacula-tion, impotence and erectile dysfunction. A goodscientific knowledge about these topics is important
so that actual medical issues don’t get dismissed aspersonal problems.6
This is a bigger issue among educated youngadult males in society. It is of utmost importancefor this specific population group as they are in theage where they will be/are sexually active, for theirsexual health and mental well being of them andtheir partners. Young males have been found tobelieve that masturbation or excessive sex isharmful and can lead to mental/physical illness.7
Researchers suggest that the person having thesemyths and misconceptions is typically more likelyto be married or recently married, of average orlow socioeconomic status, of a more rural back-ground and belonging to a family with conservative
Abstract
Introduction: In a psychosexual clinic patients do not merely turn up with problems describedin classificatory systems in psychiatry. Rather, they also present with numerous issues regardinga variety of aspects of sexual life. Aims and Objectives: The issues regarding sexual life aremostly raised by young unmarried patients hence the survey was designed to be carried outamong undergraduate youngsters. Materials and Method: A questionnaire was formulatedwith 30 items which were written to correspond with recurrent themes in sexual issues andmyths regarding various aspects of it. The format of the items was a conventional questionnairewith items presented as brief descriptive elements to which the respondents rate their level ofagreement/disagreement on a 3-point rating scale. The sample population for this survey wassexually inexperienced undergraduate male included after stratified random sampling thosewho were studying in the various colleges of the University. Results: 32.0% and 48.9%participants were opted incorrect (myth) and correct (truth) responses regarding sex life issues,respectively. 19.1% of the participants were not sure of the sex life issues. Conclusions: Youngand sexually inexperienced males are highly vulnerable to have psycho-sexual problems intheir future due to lack of factual knowledge regarding the sex life related issues.
Keywords: Sexual myths, Undergraduate, Unmarried male.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society342
ideas about sex, which can in part be attributed toexposure (or lack thereof) to Western literature.1,8
One of the most culture bound of these is thecomplaint of dhat also known as Dhat syndrome. Atypical patient presents with complaints likeimpotence, premature ejaculation and loss of sementhrough urine (whitish discharge in the urine) andat night. This loss of semen is accompanied bysymptoms like feelings of guilt, anxiety, loss ofappetite and physical weakness.2,9,10 According to astudy done on Dhat syndrome, it was noted that themost common psychiatric comorbidities associatedwere neurotic depression and anxiety neurosis, anda third of them did not have an associated psychia-tric diagnosable problem.11
Rather than reading from scientific sources,most young males have heard it from their eldersand friends that semen is a vital fluid in the humanbody and it needs to be preserved. Loss of semenby activities such as excessive masturbation andsex will lead to the afore mentioned complaints.3,12
These people are of the view that there is only afinite quantity of semen in the human body and thatit cannot be wasted. These beliefs are compoundedby the omnipresence of quacks who swear by thefact that they can make all sexual problems so away.A phenomenon like nocturnal discharge of semenwhich is absolutely normal has been made out tobe this huge sexual disorder called nightfall whichneeds immediate treatment.13,14
In a culture like ours where open discussionabout sex is taboo, fears are bound to creep in. Theurogenital system is always a focus of preoccupa-tion. Thus under stressful conditions, people arelikely to misdirect their somatic symptoms andhealth anxieties into symptoms of sexualdysfunction like turbidity of urine and tiredness dueto loss of semen.15 Other myths prevalent are thatsize of penis is important during sexual intercourse.In an internet survey, it was found that 12% menrated their penis as small while 66% men rated it asaverage and 22% large.16
Such misconceptions among men aremultiplied manifold when the topic is the female.Myths regarding pregnancy, virginity, menstrualblood being impure, female masturbation, orgasmand oral sex are extremely common. Prevalentmyths are regarding the hymen, namely that it’spresence is the proof of virginity, it should be intact
until marriage and that the first sexual encountershould be painful for a woman.17 Misconceptionslike a man need to have sex very often to be regardedas macho, female virginity is more important thanmale virginity and activities like kissing can leadto pregnancy or AIDS are still prevalent amongyoungsters.18,19
Hence, in the view of above discussion weconducted a survey to find out the understandingof the sex life issues among sexually inexperiencedyoung males and discussed the evidence based facts.
Methodology1. Questionnaire development: A questionnaire
had been formulated with the consensus ofpsychiatrists and clinical psychologist as pertheir clinical experience and informationgathered from unstructured interviews of fewundergraduate students. In this questionnaire30 items were written to correspond withrecurrent themes in sexual education and mythsregarding various aspects of it e.g. related tomasturbation, semen, pregnancy, sex positions,STD, etc., including few questions pertainingto demography. (Table -1 and 2) The format ofthe items was a conventional questionnaire withitems presented as brief descriptive elementsto which the respondents rate their level ofagreement/disagreement on a 3-point ratingscale. Scale interval anchors were ‘Yes’, ‘No’and ‘I Don’t Know’ or ‘True’, ‘False’ and ‘IDon’t Know’. Prior to conducting the surveythis questionnaire was tested on 10 randomlyselected students to rectify its applicability.
2. Sample selection: The population for thissurvey was undergraduate students studying inthe various colleges of Swami VivekanandSubharti University, Meerut. Target populationwas sexually inexperienced unmarried maleundergraduate students. Stratified randomsampling was done to select sample of thesurvey. Subjects fulfilling the inclusion criteriawere included in the study. The includedsubjects were screened for exclusion criteriaand those who were not befitted were excluded.
3. Survey conduction: After sample selection, onthe basis of the size of classrooms of theirrespective colleges, 10-15 students were handedover the questionnaire for their response.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 343
Adequate space was provided to eachparticipant to maximize privacy.Participants were informed that if they
experience discomfort during the study, they canwithdraw their participation which will not incurany academic penalty or loss of credit.
Results:In this study the total number of participants
was 205. The average age of participants was 20years. Majority of participants were belonged toBachelor of Physiotherapy (BPT) followed byBachelor of Medicine and Bachelor of Surgery(MBBS), Bachelor of Naturopathy and YogicScience (BNYS) and Bachelor of Technology (B-TECH). (Table - 1)
The response of participants on questionnaire
regarding sex life issues can be observed in Table –2.
Table-1: Demographic details of the sampleAge 20.0 ± 2.2 years
Course N (205)
BNYS 49BPT 66B-TECH 41MBBS 49
Table-3: Average of the responses byparticipants for myths, truths and neutral
responses regarding sexual life issues
Myths (n%) Truths (n%) Unaware of the issues (n%)
65.5 (32.0) 100.3 (48.9) 39.2 (19.1)
Table-2: Response of the participants for sexual life issuesS.No. Issue Yes / No / I do not
True False KnowN (n%) N (n%) N (n%)
1. Is masturbation harmful for health? 107 (52.2) 73 (35.6) 25 (12.2)2. Is the stock of semen in the body limited and if you waste it 45 (22) 129 (63.9) 31 (15.1)
by masturbating, you will soon run out of it?3. Loss of semen through masturbation/night-fall causes physical 118 (57.5) 60 (29.3) 27 (13.2)
weakness or harm to the body?4. Too much masturbation may make the penis shrink in size? 45 (22) 105 (51.2) 55 (26.8)5. Pre-cum coming out through penis during sexual arousal is a 136 (66.3) 29 (14.1) 40 (19.6)
normal biological phenomenon?6. Pre-cum coming out through penis during sexual arousal is semen? 116 (56.6) 61 (29.8) 28 (13.6)7. Is this possible that semen can come along with urine during urination? 67 (32.7) 111 (54.1) 27 (13.2)8. In your opinion dhat may be a cause of physical weakness? 122 (59.5) 21 (10.2) 62 (30.3)9. Every drop of semen is formed out of forty and more drops of blood? 87 (42.4) 44 (21.5) 74 (36.1)10. Less viscosity of semen has an adverse affect on sexual pleasure? 87 (42.4) 66 (32.2) 52 (25.4)11. A female cannot get pregnant if semen of her partner is less viscose? 75 (36.6) 81 (39.5) 49 (23.9)12. Vasectomycan lead to impotence? 90 (43.9) 85 (41.5) 30 (14.6)13. A man should be able to achieve an erection whenever he wants to? 129 (62.9) 56 (27.3) 20 (9.8)14. Wet dreams/Nightfall is actually a type of biological disease? 96 (46.8) 88 (42.9) 21 (10.3)15. Some special foods/drugs and exercise can increase the size of the penis? 101 (49.3) 62 (30.2) 42 (20.5)16. A female cannot get pregnant if her partner has small length and width of penis? 28 (13.7) 147 (71.7) 30 (14.6)17. A woman becomes ‘impure’ during menstruation and bad blood is 110 (53.7) 56 (27.3) 39 (19)
thrown out through the menstrual flow?18. Woman ejaculates during orgasm as man does? 127 (62) 21 (10.2) 57 (27.8)19. Females don’t ever masturbate? 30 (14.6) 148 (72.2) 27 (13.2)20. Can a female get pregnant the first time she has sex? 128 (62.4) 50 (24.4) 27 (13.2)21. Only males have medical issues with sexual dysfunction? 19 (9.3) 172 (83.9) 14 (6.8)22. Menopause is the end of a woman’s sex life? 41 (20) 122 (59.5) 42 (20.5)23. Females can only orgasm through penetrative sex? 57 (27.8) 77 (37.6) 71 (34.6)24. Can a female only get pregnant having sex lying down? 41 (20) 115 (56.1) 48 (23.9)25. Can a female get pregnant through oral sex? 13 (6.3) 167 (81.4) 25 (12.3)26. Does the ‘withdrawal method’ work to prevent pregnancy? 120 (58.5) 53 (25.9) 32 (15.6)27. A female cannot get pregnant when she is on her period/menstruating? 84 (41) 79 (38.5) 42 (20.5)28. A woman can’t get pregnant if the intercourse is done in a standing position? 51 (24.9) 106 (51.7) 48 (23.4)29. Whether a specific kind of sex position can ascertain gender of the expected child? 26 (12.7) 140 (68.3) 39 (19)30. Having intercourse with a virgin will cure a man of his venereal disease 27 (13.2) 127 (61.9) 51 (24.9)
(sexually transmitted disease/infection)?

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society344
DiscussionIn a true sense psychosexual behavior of an
individual is a complex phenomenon. The problemsrelated to sexual behavior go beyond the boundariesof psychosexual factors such as sexual identity,gender identity, gender role and sexual orientation,particularly in young inexperienced males. In apsychosexual clinic a young inexperienced malemay turn up with a lot of curiosity and queriesregarding sexual aspects in which the majority ofthemes revolve around dhat (a fear of leakage ofsemen), quality and quantity of semen, nocturnalemesis (nightfall), size and shape of externalgenitalia, vague somatic associations, etc.Youngmales who recently became sexually active mayblame their in competence to perform sexualactivity to these misconceptions and may developanxiety/depressive features. To the extent suchmisconceptions are inculcate through misleadinghoardings, internet, and hearsay information. Forthe longest time, problems like passage of semenin urine,20 anticipatory anxiety about potency,21 guiltassociated with masturbation,19,22 harmful concernsof loss of semen,22 anxiety due to nocturnalemission,23,26 small size of penis,19 abnormalsensation in the genitals,19 conversion of semenfrom blood and its loss during sexual activity23 havebeen reported. In the recent studies which evaluatedthe pattern of psychosexual disorders in hospitalsetting reveals that dhat syndrome is consistentlytops the list e.g. 39.2%,4 62%5 and 32.39%.24 In thepresent study, if the issues related to masturbation,semen and dhat (point No. 1 to 11, Table-2) areclubbed together, the percentage of students gaveresponse in favor of myths were 39.8%. 20.8% wereunsure of the fact and 39.4% responded in favor oftruth. This means, quite a good number of students(i.e. 60.6%) in the sample required to be psycho-educated regarding the concerned facts. Similarly,when average of total responses was calculate fordifferent responses then it was observed that almosthalf of the participants (51.9%) were eithermisinformed or unaware of the factual position ofthe concerned issue. (Table-3) Further, the notionregarding the pre-ejaculatory fluid which isconsidered as semen is the secretion of Cowper’sgland has physiological explanations, which aredescribed as it functions as lubricant for semen andpenis and also neutralizes the acidity in urethra and
vagina.25 In this way the pre-ejaculatory fluid isuseful against the notion.
Similarly, nocturnal emission (NE) is thebody’s way of relieving sexual tension, whichbecomes particularly high at the adolescent age.26
These emissions characteristically begin when a boyis 11 to 16 years of age.26 A high percentage of allmales do experience nocturnal emissions at sometime in their lives. Ultimately, about 83% of allmales have wet dreams.27 Despite of high preva-lence of nocturnal emission we don’t know the exactmechanism of it. The speculations regardingfunctionality of nocturnal emission are that it occursto either relieve sexual tension, misuse of inhibitoryneural control system during drowsiness and sleep,related to higher testosteronergic activity, it isrelated to low frequency of masturbatory/sexualactivity or it improves the quality of next freshsemen naturally.28 A study done sampling standardXI and XII students were found that 67% of theboys were had a notion that NE is a naturalphenomenon. Weakness and tiredness were reportedas physical symptoms by 18.6% and 16.6% of theboys and rest problems were more of psychologicalin nature.29 A study shown that after 10 days of dailyejaculates when the 11th sample of semen werestudied after 3-5 days of abstinence showedincrement in progressive and total spermatozoamotility30 which may have role in achievingfatherhood as shown in the study done on patientshaving low sperm counts.31
Further, a common misconception regardingvasectomy is that it causes impotence later in thelife. A study done to seek the fact of impotenceimposed by vasectomy concluded that amotivationto undergo the procedure and female dominancebetween the couples may be the probable cause ofsexual dysfunction, after excluding somatic erectiledysfunctions.32 Another study found that there isno change in frequency of sexual activity betweenvasectomized and non-vasectomized samples.33
For a long time, masculinity has been equatedwith size, shape and appearance of the penis whichis also the concern in young males attending thepsychosexual clinic. Frequently, it has also beenobserved in clinics that the patients turn up withtheir guess or comparative observation of peniseswith their colleague or porn actors. When they hadbeen asked that ever they had measured their penis

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 345
length or girth accurately with measuring scale, theanswer come up to be “NO”. As far as penis lengthand circumference are concerned in India it cameout to be mean flaccid length 8.21 cm (3.23 inches),mean stretched length 10.88 cm (4.28 inches) andcircumference 9.14 cm (3.60 inches) in a group of301 physically normal men. Out of 301, in 93 ofthe subjects erected length and circumference werefound to be 13.01 cm (5.12 inches) and 11.46 cm(4.51 inches), respectively.34 When women’spreferences for penis size and circumference werestudied, a few interesting facts surfaced. It is notalways that a female gives preference for penis sizeeither for one-time or long-term partners as 15women indicated ‘No’ in their answer’ and alsoneither does a woman always end a relationshipdue to small penis but sometimes does so due totoo large a penis as well, as 5 out of 75 were endedrelationship due to too large penis.35 In comparisonof long term relationship slightly larger size andcircumference were preferred in one-time partners.35
In many males negative correlates such as shorterheight, obesity and older age also play role inreporting smaller/average penis size by self.16 In thesimilar study despite of 55% of men satisfied withtheir penis size 84% women satisfied with the penissize of their partner’s.16 Further, most of the patientsseeking penile lengthening procedures also foundto be having normal penile length.36
As far as the female’s ejaculation duringorgasm is concerned an anatomically, histo-chemically and histo-pathologically similar tissueshas been found located in paraurethral part infemales.37 These tissues containing prostatic glands,ducts and smooth muscles officially termed as‘Skene’s paraurethral glands and ducts’ which iscommonly referred as “female prostate”. Now thequestion arises whether these tissues contribute tofemale ejaculate and whether females do ejaculateduring orgasm? The suggestions has been made onbasis of positivity of acid phosphatase test on femalesecretions that these secretions are present via anejaculatory mechanism and also in restingsecretions. The urethral expulsion in females hasbeen reported during sexual arousal with or withoutorgasm.37 Apart from the ejaculation and expulsiondescribed in context of females there are two morephenomenon i.e. vaginal lubrication and coitalincontinence which should be discussed here.
Vaginal lubrication consists of plasma transudateactivated by peptides and thought to be dischargedby contraction of perivaginal muscles and it isdescribed as discharge rather than a gush.38,39
Regarding female masturbation contrary to thebelief that females do not masturbate, the literaturereported that masturbation in females is a commonpractice.40,41
“Coitus interruptus, or withdrawal, requiresthat the penis be removed from the vagina anddirected away from the external genitalia of thewoman before ejaculation to prevent sperm fromentering the upper reproductive tract and fertilizingan ovum.”42 Coitus interruptus/withdrawalsometimes considered as preferred method ofcontraception for various reasons like havingconfidence in the success of this method, fear ofinfertility with medical practices, husbandunwillingness to use other methods.43 Although thismethod has been proven successful in preventingpregnancy to considerable extent with failure rateapproximately 4%42 Curiosity regarding failure ofthis method lead to the idea that pre-ejaculatoryfluid may contain spermatozoa leading to studieswhich showed mixed results. Killick et al. reportedthat 11 of 27 subjects (41%) produced pre-ejaculatewith spermatozoa and 10 of the cases had somemotile spermatozoa44 while Zukerman et al. reportedthat none of the pre-ejaculatory samples containedsperm, all patients had sperm in routine spermanalysis.45 Further, the fact regarding failure of anytype of contraceptive cannot be ignored as in thecase of withdrawal method also.
There are reports that 70-90% of femalescannot achieve orgasm through penetrative sexualplay. It has also been said that the distance betweena woman’s clitoris and her urinary opening hasmajor role in achieving orgasm during peno-vaginalsex. 90% of those who achieves orgasm viapenetrative sex say that the position of femalepartner used to be on top in that condition.46 Theresearcher also does not rule out the role of penissize, skill and intensity of desire to achieve orgasmin females.47
In short, on the issue of post-menopausal sexlife, researcher concluded that “……….. Thefindings suggest that framing sex aroundmenopausal changes misses important cultural andsocial issues. ……….. Instead, women emphasize

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society346
issues such as status and quality of relationships,health, and sexual history, which are social factorsrelevant for all women.
An important finding of this study is theconnection between sexual orientation, relationshipquality, and cultural ideas about sex. ………. Manyheterosexual and lesbian women similarly describesatisfying sexual relationships as well as no sex witha partner.” 47
Hence, there are lot many misconception thatprevail in the mind of young males which can beexplained on the basis of the evidences as thediscussion above.
ConclusionsIn this study we had observed that quite a good
number of participants were unaware or mis-informed regarding facts of sexual life issues.Participants were also chosen the incorrect optionfor the issues which are the known facts for obviousreasons such as role of sexual position in conceptionand intercourse with virgin female can cure STDs.From this survey it may be concluded that youngstermales are highly vulnerable to have psycho-sexualproblems in their future due to lack of factualknowledge regarding the sex life related issues.They are highly in need of to be psycho-educatedregarding the same.
AcknowledgementWe are thankful to Dr. A.K. Srivastava,
Principal, NSCB Subharti Medical College, SVSU,Meerut, Mr. Manoj Kapil, Principal, CS SubhartiInstitute of Technology and Engineering, SVSU,Meerut, Dr R.K. Meena, Principal, Jyoti Rao PhulePhysiotherapy College, SVSU, Meerut, and Dr.Abhay M. Shankaregowda, Principal, M.A.Subharti Institute of Naturopathy and YogicScience, SVSU, Meerut for their support inconduction of the survey.
DisclaimerNone
Conflicts of InterestNone
References1. Akhtar S. Four culture-bound psychiatric
syndromes in India. Int J Soc Psychiatry 1988;
34 : 70-74. 2. Balhara YPS. Culture-bound Syndrome: Has it
Found its Right Niche? Indian J Psychol Med2011; 33(2) : 210-215.
3. Bhatia MS. An analysis of 60 cases of culturebound syndromes. Indian J Med Sci 1999; 93 :149-192.
4. Jagawat T, Dhanda A, Gaur V, Parakh P,Jagawat S. A study of pattern of psychosexualdisorders and the role of pharmacotherapy intreating comorbid anxiety symptoms. DelhiPsychiatr J 2013; 16(2) : 350-54.
5. Bhatia MS, Jhanjee A, Srivastava S. Pattern ofPsychosexual Disorders among males attendingPsychiatry OPD of a Tertiary Care Hospital.Delhi Psychiatr J 2011; 14(2) : 266-69.
6. Malhotra HK and Wig NN. Dhat syndrome: aculture-bound sex neurosis of the Orient. ArchSex Behav 1975; 4 : 519-628.
7. Singh G. Dhat syndrome revisited Indian JPsychiatr 1985; 27 : 119-122.
8. Behere PB, Natraj GS. Dhat syndrome: Thephenomenology of a culture bound sex neurosisof the orient. Indian J Psychiatr 1984; 26 : 76-78.
9. Mehta V, De A, Balachandran C. DhatSyndrome: A Reappraisal. Indian J Dermatol2009; 54(1) : 89-90.
10. Bhatia MS, Malik SC. Dhat Syndrome A UsefulDiagnostic Entity in Indian Culture. Br JPsychiatr 1991; 159 : 691-695.
11. Neki JS. Psychiatry in South-east Asia. Br JPsychiatr 1973; 123 : 256-269.
12. Dewaraja R, Sasaki Y. Semen loss syndrome Acomparison between Sri Lanka and Japan. AmJ Psychotherapy 1991; 45 : 14-20.
13. Prakash O, Kar SK, Sathyanarayana Rao TS.Indian story on semen loss and related Dhatsyndrome. Indian J Psychiatr 2014; 56(4) : 377–382.
14. Gerressu M, Mercer CH, Graham CA, WellingsK, Johnson AM. Prevalence of masturbationand associated factors in a British nationalprobability survey. Arch Sex Behav 2008; 37(2): 266-78.
15. Ranjith C, Mohan R. Dhat syndrome: afunctional somatic syndrome? Br J Psychiatr2001; 1852-77.
16. Lever J, Frederick DA, Peplau LA. Does Size

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 347
Matter? Men’s and Women’s Views on PenisSize Across the Lifespan. Psychol MenMasculinity 2006; 7(3) : 129-143.
17. Dhall A. Adolescence: myths and miscon-ceptions. Health Millions 1999; 21(3) : 35-38.
18. Chadda RK, Ahuja N. Dhat syndrome: A sexneurosis of the Indian subcontinent. Br JPsychiatr 1990; 196 : 977-979.
19. Verma KK, Khaitan BK, Singh OP. Thefrequency of sexual dysfunctions in patientsattending a sex therapy clinic in North India.Arch Sex Behav 1998; 27 : 309-14.
20. Bagadia VN, Dave KP, Pradhan PV, Shah LP.Study of 258 male patients with sexualproblems. Indian J Psychiatr 1972; 14 : 143-51.
21. Nakra BR, Wig NN, Varma VK. A study of malepotency disorders. Indian J Psychiatr 1977; 19: 13-8.
22. Nakra BR, Wig NN, Varma VK. Sexualbehavior in the adult north Indian patients ofmale potency disorders. Indian J Psychiatr1978; 20 : 178- 82.
23. Prakash O, Meena K. Association between Dhatand loss of energy - A possible psychopathologyand psychotherapy. Med Hypotheses 2008; 70: 898-9.
24. Singh BK, Sinha V. Treatment seeking patternin patient with psychosexual dysfunction.Indian J Behav Sci 2011; 21(2) : 48-54.
25. Chughtai B, Sawas A, O’Malley RL, Naik RR,Khan SA, Pentyala S. A neglected gland: reviewof Cowper’s gland. Int J Androl 2005; 28 : 74-77.
26. Masland RP, Rigg CA, Shochet BR, WestmanJC, Lopez R1. What should boys be told aboutnocturnal emissions? Med Aspects HumanSexuality 1980; 22 : 26-29.
27. Kinsey AC, Pomeroy WB, Martin CE. Sexualbehavior in the human male. Philadelphia: W.B.Saunders Co., 1948.
28. Meng X, Fan L, Liu J, Wang T, Yang J, WangJ, Wang S, Ye Z. Fresh semen quality inejaculates produced by nocturnal emission inmen with idiopathic anejaculation. Fertil Steril2013; 100(5) : 1248-52.
29. Sathe AG, Sathe S. Knowledge and behaviorand attitudes about adolescent sexualityamongst adolescents in Pune: A situational
analysis. J Fam Welfare 2005; 51 : 49–59.30. Valsa J, Skandhan KP, Gusani P, Khan PS,
Amith S, Gondalia M. Effect of dailyejaculation on semen quality and calcium andmagnesium in semen. Rev Int Androl 2013;11(3) : 94-99.
31. Van Zyl JA, Mankveld R, Relief AE, VanNiekerk MA. In: Hafez ESE, editor.Oligozoospermia in human semen and fertilityregulation in men. Saint Louis: CV MosbyCompany; 1976. p. 363.
32. Buchholz NP, Weuste R, Mattarelli G, et al.Post-vasectomy erectile dysfunction. JPsychosom Res 1994; 38 : 759-762.
33. Guo DP, Lamberts RW, Eisenberg ML. TheRelationship Between Vasectomy and SexualFrequency. J Sex Med 2015; 12(9) : 1905-10.
34. Promodu KV, Shanmughadas K, Bhat SR, NairK. Penile length and circumference: An Indianstudy. Int J Impot Res 2007; 19 : 558-63.
35. Prause N, Park J, Leung S, Miller G. Women’sPreferences for Penis Size: A New ResearchMethod Using Selection among 3D Models.PLoS One. 2015 Sep 2; 10(9) : e0133079.doi:10.1371/ journal.pone.0133079.
36. Mondaini N, Ponchietti R, Gontero P, Muir GH,Natali A, Di Loro F, Caldarera E, Biscioni S,Rizzo M. Penile length is normal in most menseeking penile lengthening procedures. Int JImpot Res 2002; 14 : 283–286.
37. Zaviacic M, Whipple B. Update on the femaleprostate and the Phenomenon of femaleejaculation. J Sex Res 1993; 30(2) : 148-51.
38. Kinsey AC, Pomeroy WB, Martin CE. Sexualbehaviour in the human female. Sanders:Oxford; 1953.
39. Levin RJ. The ins and outs of vaginallubrication. Sex Relation Ther 2003; 18 : 509–13.
40. Sathyanarana Rao TS, Nagaraj AM. Femalesexuality. Indian J Psychiatr 2015; 57 : 296-302.
41. Sharma V, Sharma A The guilt and pleasure ofmasturbation: A study of college girls inGujarat, India. Sex Marit Ther 1998; 13 : 1, 63-70.
42. Russo JA, Nelson AL. Behavioral Methods ofContraception. In: Shoupe D, Kjos SL (eds).The Handbook of Contraception. Current

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society348
Clinical Practice. Humana Press 2006. https://doi.org/10.1007/978-1-59745-150-5_11
43. Azari S, Shahnazi M, Farshbafkhalili A,Abbasnezhad O. Reasons for Choosing theTraditional Method (Withdrawal) as Contra-ception among Women in Tabriz/Iran. Int JWomen’s Health Reproduction Sci Autumn2014; 2(5) : 297–300.
44. Killick SR, Leary C, Trussell J, Guthrie KA.Sperm content of pre-ejaculatory fluid. HumFertil 2011; 14 : 48-52.
45. Zukerman Z, Weiss DB, Orvieto R. Does pre-
ejaculatory penile secretion originating fromCowper’s gland contain sperm? J Assist ReprodGenet 2003; 20 : 157-159.
46. HealthyWomen. What’s the Key to FemaleOrgasm During Sex? 2019; | Healthy Women.[online] Available at: https://www.healthywomen.org/content/article/whats-key-female-orgasm-during-sex [Accessed 3 Jul. 2019].
47. Winterich JA. Sex, Menopause, And CultureSexual Orientation and the Meaning ofMenopause for Women’s Sex Lives. Gender &Society 2003; 17(4) : 627–642.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 349
Quality of Life and Caregiver burden in ChronicKidney Disease – Case for a paradigm shift in
holistic managementShagufta Khanam,1 Shahbaz A. Khan,2 A.W. Waheed,3 D.S. Ray,4 Aruna Deshpande,5
Swetanka Prasad,6 V.V. Gantait,7 P. Patra8
1VKS University, Patna, Bihar; 2,8Department of Psychiatry, Command Hospital Kolkata;3,4,6Department of Nephrology, Brahmananda Narayana Hridayalaya, Jamshedpur;
5Senior Research Advisor, Public health;7Department of Psychiatry, Base Hospital Barrackpur, West Bengal
Contact: Shahbaz A. Khan, E-mail:[email protected]
Original Article
IntroductionAmong the various chronic illnesses, chronic
kidney disease (CKD) is a big culprit and everincreasing. Unfortunately, from India there is nolongitudinal study and limited data on theprevalence of CKD. Of the few studies available,a prevalence of CKD upto 17.2% has been found.1
Even in apparently healthy adult population a
prevalence of CKD is reported as high as 13–15%.2
Western research indicates that there has been30% increase in prevalence of chronic kidneydisease (CKD) over last 10 years3-5 and there isreason to believe that actual Indian figures are notonly similar but continuously increasing due tolifestyle diseases and increased longevity.4 End-stage renal disease (ESRD) represents the final stage
AbstractIntroduction:End-stage renal disease (ESRD) represents the final stage of chronic kidney disease(CKD). Quality of Life and as well as Caregiver burden are important determinants of treatmentoutcome in a complex manner. Objectives: to study Quality of Life in patients of ESRD andcorrelate with caregiver burden with respect to the type of dialysis being given-hemodialysis orperitoneal dialysis. Methodology: Between January 2018 and June 2018, all patients withESRD reporting to the nephrology OPD of a tertiary care hospital of eastern India with aspecialized nephrology unit were offered to be included in the study. Of these 56 patients onhemodialysis, 50 patients on peritoneal dialysis and 32 patients of ESRD not on dialysis wereenrolled. The study assessed patients’ demographic characteristics and noted biochemical andhematological variables from the medical record. We diagnosed ESRD based on CKD-EPIformula and a GFR of < 15ml/min/1.78 m2 BSA was diagnosed as ESRD. We used the briefversion of the WHO’s QOL scale (WHOQOL-BREF) in this study. For CG burden assessmentFamily Scale for Caregiver Burden, a well validated scale in this population was used. Results:The significant difference in mean scores between HD and PD group Mean QOL was significantlyhigher for PD. Conclusion: The study brought out the advantages in QoL as well as caregiverburden in the peritoneal dialysis group as compared to the hemodialysis group, even thoughmajority of ESRD patients in India are on hemodialysis. There appears to be a direct correlationbetween all domains of quality of life and caregiver burden in this group of patients. In theIndian context, certain modifiable sociodemographic factors are also at play. Close cooperationbetween nephrologist and psychiatrist is called for in holistic management of these patients.Key words: Hemodialysis, Peritoneal dialysis, Caregiver burden, Quality of Life

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society350
of chronic kidney disease (CKD). While, CKD ispresent in as many as 20 million Americans andthis number is likely to increase with the growingburden of diabetes mellitus and hypertension, ESRDaffects approximately 500,000 patients in the UnitedStates.5
In the Indian context, a rough estimate of themagnitude of the problem can be had from theresults of an Indian study which found incidenceof ESRD to be 229/million population.6
There are 2 major modalities of treatment forESRD patients - hemodialysis and peritonealdialysis. Among the ESRD patients on dialysis,majority (upto 90%) are on hemodialysis and therest on Peritoneal dialysis.7 As per US CDC controldata, by 2013, 63.7 percent of all prevalent ESRDcases were receiving hemodialysis therapy and 6.8percent were being treated with peritoneal dialysis.8
A key determinant in assessment of CKDpatients is the quality of life (QoL). According tothe WHO, QoL is defined as “individual’s percep-tion of their position in life in the context of theculture and value systems in which they live and inrelation to their goals, expectations, standards andconcerns”. It is a broad ranging concept affectedby the person’s complex physical health, psycho-logical state, level of independence, social relation-ships, personal beliefs and their relationship tosalient features of their environment.9 The corecomponents of QOL are physical, functional,psychological/emotional, and work/occupational.10
Patients with end-stage renal disease (ESRD)whether or not on maintenance dialysis experiencesignificant impairments in quality of life (QOL).11
The question arises as to what causes thisdeterioration in the quality of Life in patients ofCKD? The obvious sources appear to be problemswith physical health, psychological state, level ofindependence, social support, personal beliefs andtheir relationship to salient features of their environ-ment.12 Findings have shown that lower scores onQoL were strongly associated with higher risk ofdeath and hospitalization, than clinical parametersin cases of ESRD patients.13,14 There are very fewstudies looking at this domain in Indian context andeven fewer studies of QoL in CKD patients whoare on peritoneal dialysis15 and we could find norecent attempts at comparing these physical andpsychological burden in PD and HD population.
Caregiver Burden - Caregiver burden (CG) is“the physical, financial, and psycho-socialhardships of caring for a loved one, usually a familymember, struggling with a medical condition”.16
Family care-givers are those individuals whoprovide the majo-rity of the patient’s physical,emotional, financial, and social care needsthroughout the continuum of care, from beinghospitalized to providing care at home, withoutreceiving any remuneration.17
Family caregivers may develop caregiverburden, when the stress of care exceeds theresources available to cope with the demands ofcare.18 The substantial amount of caregivingrequired by patients with ESRD may increasefamily caregiver’s vulnerability to emotional,physical and psychological consequences.19,20
As family caregivers often bear the burden ofcaregiving alone, their physical, social, emotional,and financial life are negatively impacted, leadingto caregiver burden21 there is a stark paucity ofresearch regarding caregiver burden among familycaregivers of ESRD patients and this also meansthat there appears to be a lack of support for thesefamily members. Any management plan which doesnot take into consideration the caregiver dimension,is incomplete to say the least and completely missesthe understanding of such chronic illnesses and sucha misunderstanding is bound to negatively impactthe overall outcome of treatment.22
Apart from being an important determinant ofoutcome in CKD patient on maintenance dialysis(hemodialysis (HD) or peritoneal dialysis (PD)–23
considerably less is known about these health-related domains in caregivers of patients with ESRDwho are not on dialysis. Understanding the degreeto which impaired QOL and the Caregiver burdenaffect this group of patients is also important inappreciating how such health-related domains maychange when advanced CKD progresses to ESRDand onto renal replacement modality (hemodialysis)as well as help in planning effective and compre-hensive long-term management plan for thesepatients. In this background we decided to studythe prevalence of QOL in ESRD patients on dialysis(HD as well as PD) and we also used a comparativecontrol arm of patients of ESRD who are not ondialysis. We looked at Caregiver burden in thefamily caregivers of these patients and compared

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 351
the same between these 3 groups (ESRD on HD,ESRD on PD and a control ESRD not on dialysis).To our knowledge this is a one of its kind of studyon Indian population which compares thesedomains together in these 3 groups of patientsamples.
Material and MethodsThis study was a part of a larger study of mental
health and kidney disease by the authors where westudied depression and QoL in patients withadvanced CKD and subjects undergoing chronicperitoneal dialysis and twice/thrice-weekly in-center hemodialysis. Institutional ethical committeeclearance was taken and all participants providedinformed consent.
Between Jan 2018 and June 2018, all patientswith ESRD reporting to the nephrology OPD of atertiary care hospital of eastern India with aspecialized nephrology unit were offered to beincluded in the study. Of these 56 pts on hemo-dialysis, 50 pts on peritoneal dialysis and 32 pts ofESRD not on dialysis were enrolled after dueconsent. Exclusion criteria included age <18 yr or>70 year, active malignancy, active infection(pneumonia), active coronary artery disease (e.g.,unstable angina, myocardial infarction) within thelast 6 months, bed bound patients, advancedcirrhosis, advanced dementia, substance usedisorder, presence of schizophrenia, bipolar mooddisorder, past history for treatment for anysyndromal psychiatric illness, past h/o head injury,stroke in the last 6 months, Patients withoutexclusion criteria were approached at the time oftheir initial or routine CKD clinic visit. This studywas conducted in accordance with the principlesof the Declaration of Helsinki. We assessed patients’demographic characteristics and noted biochemicaland hematological variables from the medicalrecord. We diagnosed ESRD based on CKD-EPIformula and a GFR of < 15ml/min/1.78 m2 BSAwas diagnosed as ESRD. We used the brief versionof the WHO’s QOL scale (WHOQOL-BREF) in thisstudy. This instrument derived from the WHOQOL-100. The WHOQOL-BREF questionnaire containstwo items from the Overall QoL and General Healthand 24 items of satisfaction that divided into fourdomains: Physical health with 7 items (DOM1),psychological health with 6 items (DOM2), social
relationships with 3 items (DOM3) and environ-mental health with 8 items (DOM4)24 Domainscores are scaled in a positive direction (i.e., higherscores denote higher QoL). The mean score of itemswithin each domain is used to calculate the domainscore. For CG burden assessment we used theFamily Scale for Caregiver Burden which is a wellvalidated scale in this population.25
For our analyses, we first took hemodialysisand peritoneal dialysis patients as one group(referred to as the dialysis group). These patientswere compared with ESRD patients who were noton dialysis (controls). Then an intra group compari-son was done between HD and PD patients.Differences between the groups in demographiccharacteristics, clinical variables, QoL scores andCG Burden score were assessed using ANOVA forcontinuous variables, and the 2 statistic or Fisher’sexact test for categorical variables.
To assess the impact of demographic andclinical variables on group differences we usedlinear regression, logistic regression, or theWilcoxon-Mann-Whitney rank sum test , asappropriate. Variables included in these analyseswere those that demonstrated statisticallysignificant differences between the study groups inunivariate analyses. We assessed correlations ineach patient group using Spearman’s correlationcoefficient, and evaluated the internal consistencyreliability using Cronbach’s coefficient alpha. A p-value of <0.05 was considered to representstatistical significance in all analysis. All datahandling and in-depth analyses was done by one ofthe authors who is a qualified statistician too, usingthe SPSS version 20.
ResultsAmong the samples there are 3 subgroups -
Hemodialysis (HD), Peritoneal dialysis (PD) andcontrols (CKD patients not on dialysis). Wecompared the following parameters between these3 major groups.
1. Sociodemographic variables2. Quality of Life of the patients3. Caregiver burdenSociodemographic variables: We found that
there was significant difference in mean age of threegroups. HD cases were younger than PD samplesand control. There was no difference with respect

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society352
to gender, education or socioeconomic statusbetween the 3 groups. Mean duration of dialysis inHD group was 38.18 months. For PD, this avg was27.5 months (p< 0.05).
QoL score: there is significant difference inmean scores between HD and PD group. Mean QoLis significantly higher for PD. (Table 1 and Table2)
Satisfaction score: there is significantdifference in mean scores between HD and PD
group as well as between Control and HD - HD hassignificantly lower mean values compared tocontrol and PD (Table 2)
CG Burden: The caregiver burden score wassignificantly higher in hemodialysis group ascompared to the peritoneal dialysis and controlgroup which did not differ significantly betweenthemselves. The QoL domains are significantlycorrelated with caregiver burden on family (Table3)
Table-1: Comparison of mean scores between the groups
N Mean Std. Deviation
QOL score ( Q 1) Control 19 3.32 1.003HD 50 2.90 .931PD 53 3.85 1.199Total 122 3.38 1.145
Satisfaction score (Q 2) Control 19 3.89 .809HD 50 3.16 .866PD 53 3.81 .982Total 122 3.56 .963
DOM 1 ( PHYSICAL HLTH) Control 19 3.34 .676HD 50 3.72 .648PD 52 3.48 .840Total 121 3.56 .749
DOM 2( PSY HLTH) Control 19 3.39 .838HD 50 3.22 .777PD 52 3.33 .776Total 121 3.29 .783
DOM 3 ( SOCIAL HLTH) Control 19 3.47 .630HD 50 3.65 .622PD 52 3.73 .735Total 121 3.66 .675
DOM 4 (ENV HLTH) Control 19 3.66 .661HD 50 3.63 .814PD 52 3.67 .835Total 121 3.65 .795
CAREGIVER BURDEN SCORE Control 19 9.63 8.275HD 50 26.60 17.299PD 53 11.91 9.676Total 122 17.57 15.141
Table 2: Statistical Comparison of means between the 3 groups
p-value for the comparison betweenParameter Control & HD Control & PD HD & PDQoL score (Q 1) 0.321 0.152 0.000*Satisfaction score (Q 2) 0.009 0.937 0.001*DOM 1 (PHYSICAL HLTH) 0.140 0.757 0.235DOM 2 (PSY HLTH) 0.693 0.962 0.732DOM 3 (SOCIAL HLTH) 0.568 0.317 0.829DOM 4 (ENV HLTH) 0.991 0.997 0.963Caregiver Burden Score 0.000* 0.796 0.000*
* statistically significant p value

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 353
DiscussionPrevious studies have found poorer QoL in
CKD patients in general and ESRD patients ondialysis in particular.26 In our study in Indianpopulation we found that even though the scoreson the 4 different various domains of QoL was notstatistically different between the 3 groups, therewas significant difference in the overall perceptionof QoL (assessed by Q1) as well as overallsatisfaction levels (assessed by Q2). The satisfactionlevels and the overall QoL perception by patientswas found to be better in the peritoneal dialysis andnon dialysis patients as compared to the hemo-dialysis group. In other words those on hemodialysiswere less satisfied and felt that they had poor qualityof life than those on peritoneal dialysis and in acomplex manner because when we compare the 3groups in terms of the 4 specific domains of QoL(physical health, psychological health, social andenvironmental health) they appeared to becomparable. At the same time, we also found thatthe CG burden was significantly more in thehemodialysis group as compared to peritonealdialysis group which was similar to the non dialysisgroup. This assumes importance given that only10% of ESRD are on PD and the majority are onHD.27
It perhaps can be understood in terms of thefact that that PD patients stay home and are in morecontrol of their illness/treatment as compared to HDpatients who have to come 2-3 times a week forhemodialysis to the hospital. Apart from any
inherent effect of the hemodialysis process itself,In Indian and rural/semi urban context we also needto consider psychosocial factors like travel, poormodes of communication, stay, need for anattendant caregiver to accompany, financial burdenas well as mental and physical labor involved.28
The most important difference between the PD(and control) on one side and the HD group on theother is the frequent visits to the hospital(dependency) in the latter and its attendant socialand psychological factors. From a biopsychosocialpoint of view, it appears that when a patient has tovisit the hospital 2-3 times a week for hemodialysisthen the gains of therapy (in the form of tight controlof renal pathology/parameters) is offset or fritteredaway by the psychological impact of dependencyand other socioeconomic factors like stay, finances,need for an accompanying person, difficulties inconveyance and communication, disruption ofsocial commitments/involvement etc. This is alsoindirectly inferred from the finding that HD grouphas significantly higher caregiver burden than thePD and control group. It can be argued that perhapsthere is a selection bias in the beginning in thatpatients with less severe illness or less comorbidconditions are prescribed peritoneal dialysis andhence they have better QoL as well as lessercaregiver burden in the peritoneal dialysis patient.However, in terms of potency and efficacy both PDand HD are comparable.27 the KDIGO guidelinesdo recommend that PD should be started first innon-oliguric young ESRD pts but only if other
Table-3: Correlation coefficients are significant between all the pairs of parameters except for thepair Caregiver burden and physical health (DOM 1)
Caregiver Burden Score
QOL score (Q 1) Correlation Coeff -.499**
p-value .000satisf score (Q 2) Correlation Coeff -.454**
p-value .000DOM 1 (PHYSICAL HLTH) Correlation Coeff -.109
p-value .233DOM 2 (PSY HLTH) Correlation Coeff -.430**
p-value .000DOM 3 (SOCIAL HLTH) Correlation Coeff -.269**
p-value .003DOM 4 (ENV HLTH) Correlation Coeff -.301**
p-value .001

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society354
clinical factors are favorable like for e.g. thosepatients where vascular access is not possible orAV fistula fails (usually happens in pts with othersystemic comorbid conditions), those with severecardiac compromise, vascular risk factors likerecent ICH etc. other bleeding disorders etc. Theseare all poor risk factors and these patients areassigned peritoneal dialysis. So it cannot be inferredreadily that it is the good prognosis patients whoare assigned peritoneal dialysis in the first place.This is also bailed out by the fact that at 5 yearssurvival rate for both PD and HD were found to becomparable.27 In the light of the present findings,nephrologists will do well to involve the patientmore in their treatment regimen. After all what is atreatment if our patients are not happy and satisfiedat the end of it. Afterall we are not treating thediseased kidney but the person with the diseasedkidney. There is evidence to show that psycho-logical distress, depression29 and psychosocialfactors including poor social support30 appears toinfluence QoL in CKD as seen in our study too andpoor QoL has direct impact on outcome morbidityand morbidity independent of physical parameters.31
In fact, differences in social support between groupshas been suggested to underlie differences inmortality of dialysis patients between units.32
Coming to the other important parametermeasured in the study, we found high caregiverburden on family caregivers across the spectrum.Again, we found that caregivers of peritonealdialysis patients as well as of those who were notyet on any dialysis, were less burdened than thoseof pts on hemodialysis. There also appears to be asignificant relationship in the negative directionbetween all the domains of the QoL with thecaregiver burden except domain 1 (physical health)– poorer QoL correlated with higher caregiverburden across physical, social, psychological andhealth related domains of QoL. We infer thatperhaps the family caregivers are less burdened bythe physical health of their patients than thepsychological health, social constraints, financialissues and the logistics of taking the patient forhemodialysis 2-3 times a week to the centre.Expectedly, that is quite understandable and logicalinference – a patient who has poor social support,is low on confidence and money and is far awayfrom the dialysis centre/hospital is likely to have
less subjective satisfaction and is likely to rate hisQoL as poor. On the other hand, the reverse is alsotrue – a patient with good psychological health andgood social support etc will have higher subjectivewellbeing and higher QoL when we talk of burdenon the caregivers, evidence suggests that even thehealthcare workers attending these chronically illpatients get burdened enough to get their QoLaffected.33
ConclusionBased on our finding from this study, we
recommend that a holistic approach to patients ofCKD with/without dialysis, would entail assessmentof detailed psychosocial factors which affect overall outcome. Management approach should takethese into account as well. Care of the caregiversalso should be a part of the management protocol.Addressing the social factors, environmentalfactors, psychological issues through our counselingand psychoeducation (of the patient and thecaregivers alike) is as important as physical healthin these patients. Perhaps there is a need for theservices of mental health professionals in closeliaison with the nephrology team, as underlined bythe findings of our study.
Limitations of the studyOne of the major limitations is the fact that this
is a cross sectional design study and despite it’sstrength of adequate sample size, strict inclusioncriteria and inclusion of controls (in the form ofend stage renal disease patients not yet on dialysis),a cross sectional design in itself is handicapped tocomment on causality.
Future directionsIn future we recommend a similar study with
prospective follow up cohort design and preferablyto include the domains of severity of renal illnessas well as psychopathology and its correlation, ifany, in the patients being cared for. Such a studydesign has been planned by the authors and the studyis underway.
References1. Singh AK, Farag YM, Mittal BV, et al.
Epidemiology and risk factors of chronic kidneydisease in India - results from the SEEK(Screening and Early Evaluation of Kidney

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 355
Disease) study. BMC Nephrol 2013; 14 : 114.2. Varma PP, Raman DK, Ramakrishnan TS,
Singh P, Varma A. Prevalence of early stagesof chronic kidney disease in apparently healthycentral government employees in India.Nephrol Dial Transplant 2010; 25 : 3011–7.
3. Coresh J, Selvin E, Stevens LA, et al.Prevalence of chronic kidney disease in theUnited States. JAMA 2007; 298 : 2038–47.
4. Verma PP. Prevalence of chronic kidney diseasein India - Where are we heading. Indian JNephrol 2015; 25(3) : 133–135.
5. Murphy D, McCulloch CE, Lin F, et al. Trendsin prevalence of chronic kidney disease in theUnited States. Ann Intern Med 2016; 165(7):473–481.
6. Modi GK, Jha V. The incidence of end-stagerenal disease in India: A population-based study.Kidney Int. 2006; 70 : 2131–3.
7. US Renal Data System. USRDS 2010 AnnualData Report: Atlas of End-Stage Renal Diseasein the United States. Bethesda: NationalInstitutes of Health, National Institute ofDiabetes and Digestive and Kidney Diseases2010.
8. Xu JQ, Murphy SL, Kochanek KD, Bastian BA.Deaths: final data for 2013. www.cdc.gov .Published February 16, 2016.
9. WHOQOL. Measuring Quality of Life,Program on Mental Health. World HealthOrganization 1997. Available from: URL:http://www.who.int/mental_health/media/68.pdf
10. Fellowfield L. What is Quality of Life. 2nd ed.2009. Available from: URL: http://www.medicine.ox .ac .uk/ bandolier /pa inres /download/whatis/WhatisQoL.pdf
11. Spiegel BM, Melmed G, Robbins S, EsrailianE. Biomarkers and health-related quality of lifein end-stage renal disease: a systematicreview. Clin J Am Soc Nephrol 2008; 3 : 1759–1768.
12. Abraham S, Ramachandran A. Estimation ofquality of life in haemodialysis patients. IndianJ Pharm Sci 2012; 74 : 583–587.
13. Schatell D, Witten B. Measuring DialysisPatients’ Health-Related Quality of Life withthe KDQOL-36TM. Medical EducationInstitute, Inc. (608) 833-8033, KDQoLComplete 2012. Available from: URL: ttp://
www.kdqol-complete.org814. Mapes DL, Bragg-Gresham JL, Bommer J, et
al. Health-related quality of life in the DialysisOutcomes and Practice Patterns Study(DOPPS). Am J Kidney Dis 2004; 44 : 54-60.
15. Kim JA, Lee YK, Huh W, et al. Analysis ofdepression in continuous ambulatory peritonealdialysis patients. J Korean Med Sci 2002; 17(6): 790-794.
16. Garlo K, O’Leary JR, van Ness PH, Fried TR.Burden in caregivers of older adults withadvanced illness. J Am Geriatr Soc 2010; 58 :2315–2323.
17. Collins L G, Swartz K. Caregiver care. Am FamPhysician 2011; 83 : 1311–1319.
18. Northouse L, Katapodi M, Schafenacker AM,Weiss D. The impact of caregiving on thepsychological well-being of family caregiversand cancer patients Sem Oncology Nurs 2012;28 : 236–245.
19. Bastawrous, M. Caregiver burden—A criticaldiscussion. Int J Nurs Stud 2013; 50 : 431–441.
20. Khosravan S, Mazlom B, Abdollahzade N,Jamali Z, Mansoorian MR. Family participationin the nursing care of the hospitalized patients.Iran Red Crescent Med J 2014; 16 : 1–6.
21. Given BA, Given CW, Sherwood P. Caregiverburden. Philadelphia: Saunders 2012.
22. Oyegbile YO, Brysiewicz P. Exploring care-giver burden experienced by family caregiversof patients with End-Stage Renal Disease inNigeria. Int J Africa Nurs Sci 2017; 7 : 136-143.
23. Boulware LE, Liu Y, Fink NE, Coresh J, FordDE, Klag MJ, Powe NR: Temporal relationamong depression symptoms, cardiovasculardisease events, and mortality in end-stage renaldisease: Contribution of reverse causality. ClinJ Am Soc Nephrol 2006; 1 : 496–504.
24. World Health Organization. WHOQOL-BREF.Introduction, Administration, Scoring andGeneric Version of the assessment. Geneva:WHO, 1996.
25. Fukahori H, Yamamoto-Mitani N, Sugiyama T,et al. Psychometric properties of the CaregivingBurden Scale for Family Caregivers withRelatives in Nursing Homes: scaledevelopment. Jpn J Nurs Sci 2010; 7(2) : 136-47.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society356
26. Kalender B, Ozdemir AC, Dervisoglu E,Ozdemir O. Quality of life in chronic kidneydisease: effects of treatment modality,depression, malnutrition and inflammation. IntJ Clin Pract 2007; 61 : 569–76.
27. US Renal Data System. USRDS 2016 AnnualData Report: Atlas of End-Stage Renal Diseasein the United States. Bethesda: NationalInstitutes of Health, National Institute ofDiabetes and Digestive and Kidney Diseases.2016.
28. Daniel Cukor, Scott D. Cohen, Rolf A.Peterson, and Paul L. Kimmel PsychosocialAspects of Chronic Disease: ESRD as aParadigmatic Illness. JASN 2007; (18) No 12: 3042-3055.
29. Varma PP, Raman DK, Ramakrishnan TS,
Singh P, Varma A. Prevalence of early stagesof chronic kidney disease in apparently healthycentral government employees in India.Nephrol Dial Transplant 2010; 25 : 3011–7.
30. Kimmel PL: Psychosocial factors in dialysispatients. Kidney Int. 2001; 59 : 1599–1613.
31. House JS, Landis KR, Umberson D: Socialrelationships and health. Science 1988; 241 :540–545.
32. Kimmel PL, Peterson RA: Depression in end-stage renal disease patients treated withhemodialysis: Tools, correlates, outcomes, andneeds. Sem Dialysis 2005; 8 : 91–97.
33. Gholami A, Jahromi LM, Zarei E, Dehghan A.Application of WHOQOL-BREF in MeasuringQuality of Life in Health-Care Staff. - Int J PrevMed 2013; 4(7) : 809–817.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 357
Correlates of Dyadic Adjustment inSchizophrenia
Shipra Singh,1 Deoraj Sinha,2 Nitin B. Raut3
Department of Psychiatry, 1PGIMS, Rohtak, 2Dr. R.N. Cooper Hospital & HBT Medical College, Mumbai;3Lady Hardinge Medical College, Delhi
Contact: Deoraj Sinha, E-mail:[email protected]
Original Article
IntroductionSchizophrenia is a severe mental disorder that
is often referred to as loss of contact from reality. Itincludes cognitive, emotional, and perceptualdisturbances, that distort reality, and can result intransformation of a person’s self.1 The expressionof these manifestations varies across patients andover time, but the effect of illness is always severeand is usually long-lasting. Schizophrenia manifestsas a relapsing and remitting illness. More than 50%have a poor outcome, with repeated exacerbationsand hospitalizations.2
With the deinstitutionalization process andgovernment policies for rehabilitation of mentallyill, the responsibility of care shifted to the familyand society. Parents and spouses are the people mostlikely taking up the caregiving role. During this
course, the caregivers experience considerablefinancial, emotional, and practical burdens.
Studies have reported lower rates of marriageor stable partnership in patients with schizo-phrenia.3-5 However, a few Indian studies have foundfairy high rates of the same.6,7 Marriage is essen-tially a social process in which two individualsrelate on a personal and intimate basis, pledging toshare a life together. In several societies includingIndia, it is sanctified and glorified and is still largelya commitment for life. Marital responsibilitiesrequire certain social abilities for it to be successful.Schizophrenia is associated with a number ofbehaviouralchanges andimpairment of social andcognitive abilities, probably leading to a low maritalrate and maladjustments in the marriage.7
Marriage has a bearing on mental health and
Abstract
Introduction: Mental illness and marriage are interconnected. Various factors related to thementally ill spouse, the demographics and illness related factors have been found to have abearing on the marital relations. Objective: This study aims at assessing marital adjustment inthe spouses of patients with schizophrenia and its relation with different contributory factors.Method: It was a cross-sectional study, including 100 consecutive participants, 20-60 years ofage, who were spouse of patients diagnosed with Schizophrenia(according to DSM-5) and hadminimum illness duration of 5 years and spouses are the primary caregivers. A sociodemographicproforma, Dyadic adjustment scale (DAS)and Positive and negative syndrome scale (PANSS)were used to assess different variables. Results: Of the subscales, mean score of the subscale‘consensus on matters of importance to marital functioning’ (3.07) was the highest and that of‘affection expression’ was the lowest (1.66). Onset of illness before marriage, multiple numberof relapses and hospital admissions and poor compliance was associated with poor dyadicadjustment. Conclusion: Spouses, as caregivers, have some distinct issues and concerns, whichon discussion and exploration in routine clinical practice may help in identifying caregiver’sstress.
Keywords: Marriage, Schizophrenia, Dyadic adjustment.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society358
mental illness; and the reverse is also true.7 How-ever, it is noted that patients with mental illnesspermanently living with a spouse have better socialoutcome and prognosis.8 Earlier research has founddifferences in perceived burden and caregivingbetween spouse and other caregivers. 9 Theexperience of objective burden may be similar forboth parents and spouses, but they differed in theirexperience of subjective emotional burden.10
Various factors including those related to thementally ill spouse, the demographics and illnessrelated factors have been found to have a bearingon the marital relations. This study aims at assessingmarital adjustment in the spouses of patients withschizophrenia along with its relationship withdifferent contributory factors.
MethodsStudy participants
Hundred consecutive participants, who werespouse of patients diagnosed with Schizophrenia,according to DSM-5 and had minimum illnessduration of 5 years were included in the study.Participants were required to be between 20-60years of age, primary caregiver of the patient andwilling to give informed consent. Those spouseswho had any chronic physical or mental illness andthose whose schizophrenic spouse had anyassociated mental or chronic physical illnesses,were excluded from the study. The diagnosis wasalso based on MINI (Mini International Neuro-psychiatric Interview), a structured interview toolwith a high validity and reliability, and it was alsoused to rule out other coexistent psychiatric disorderin both spouse and the patient.11
Study designIt was a cross-sectional study done in the
psychiatry department of a tertiary care teachinghospital after approval from Institutional EthicsCommittee. A written informed consent wasobtained from the participants before theirenrollment in the study.
Assessment MeasuresA semi-structured proforma was used to gather
socio-demographic and illness related details. Inaddition, following scales were used:
Dyadic adjustment scale (DAS) – It was created
by Spanier in 1976. It is a 32 item scale in Likertform which encompasses different dimensions ofmarital adjustment. These are: (a) consensus onmatters of importance to marital functioning, (b)dyadic satisfaction, (c) dyadic cohesion, and (d)affection expression.Coefficient alpha r for totalscore of Dyadic Adjustment Scale is 0.93.Convergent validity was established with LockeWallis marital adjustment Scale (r is 0.87) anddivergent validity by evidence of an inverserelationship with the Marital Dissatisfaction scale(r is -0.79). Internal consistency of DAS score ishigh. Traditionally, a total score of 102 or morewould indicate that the couple is non-distressed,however as outlined in recent revisions, a cut-offof 97 was indicated for the above, and same cut-offis used in our study.12-14
Positive and Negative Syndrome Scale(PANSS) - The PANSS by Stanley R. Kay andcolleagues is a 30-item symptom rating scale thatwas designed to measure core positive and negativesymptoms of schizophrenia. Symptoms are ratedalong a seven-point continuum of severity on thebasis of a semi-structured interview with the patientas well as observations of the patient’s behaviour,during the past seven days by informants. Each ofthe items making up the Positive and NegativeScales correlated very strongly with the scale total(p <.001), and the mean item total correlations of0.62 and 0.70, respectively.15-16
Statistical analysis:It was done by SPSS version 20. Results
obtained for quantitative data was presented usingmean, range and standard deviation. Data wasnormally distributed. Chi-square test was done forcategorical variables, and t-test for continuousvariables.
ResultsDemographic profile
Out of the 100 spouses included in the study,72 were male and rest female. Their mean age was47 years (standard deviation SD = 9.25 years).Range was 25 years minimum age to maximum 59years. 61% lived in nuclear family and others injoint family system. Considering their education,2% were illiterate, 22% had primary education and76% had education of higher secondary and above.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 359
The mean age of spouse at the time of marriagewas 25.97 years (SD = 5.8 years), ranging from 9to 41 years.
Illness related variablesAmong illness related variables, mean duration
of illness of the patients was 14 years, minimumbeing 5 years (as per the inclusion criteria) andmaximum 38 years. In 89% of the cases, patienthad developed the illness (schizophrenia) aftermarriage, and in 11% before the marriage. Patient’scurrent symptoms were assessed using PANSS(Positive and negative syndrome scale), whichshowed mean positive subscale score 17.02 (SD =7.075), negative subscale score 15.35 (SD = 4.998),general psychopathology subscale score 32.26 (SD= 10.072) and total score 64.63 (SD = 19.209). Outof the 100 patients, 57% had minimal or residualsymptoms while 43% were actively symptomaticat the time of interview. The number of hospitaladmissions ranged from minimum of 0 to amaximum of 7 admissions. Based on subjectivequestioning about adherence to treatment, 59%were adherent to treatment.
Dyadic AdjustmentThe assessment tool for studying marital
adjustment in this study was DAS (DyadicAdjustment Scale). It has a minimum score of 31and maximum of 146 and a cut-off score of 97.Based on this, 56% couples in our study had scoresabove 97 suggesting good marital adjustment andrest 44% had poor marital adjustment. Among its 4subscales, mean average score on scale ‘consensuson matters of importance to marital functioning’was highest i.e. 3.307, for ‘dyadic satisfaction’ was3.171, for ‘dyadic cohesion’ was 3.188, and for‘affect expression’ was 1.66, the lowest.
Correlates of dyadic adjustmentBased on DAS scores, two groups emerged-
one with good and the other with poor maritaladjustment. The difference in the two groups basedon age, gender, education and family type was notstatistically significant.Illness related variables werealso studied in context of dyadic adjustment (Table1 and 2). Analysing the onset of illness, we found94.6% of patients in the well-adjusted group and81.8% in the poorly adjusted group had their illness
Table-1: Comparison of various variables in good and poor adjustment groups
Poor marital adjustment Good marital adjustment Unpaired T-test
Mean SD Mean SD p-value
Age 46.18 8.822 47.77 9.595 0.397Duration of illness 14.59 8.136 13.55 8.104 0.527Number of hospitalizations 2.23 1.52 1.41 0.96 0.002*
PANSS Total score 79.57 14.598 52.89 13.373 0.000*
* - Significant
Table-2: Comparison of variables in the good and poor adjustment groups
Poor marital Good marital Pearson’s chiadjustment N (%) adjustment N (%) square (p-value)
ONSET OF ILLNESS 0.042*
Before marriage 8 (18.2) 3 (5.4)After marriage 36 (81.8) 53 (94.6)RELAPSE 0.000*
More than 5 17 (38.6) 5 (8.9)Less than 5 27 (61.4) 51 (91.1)COMPLIANCE 0.000*
Poor 35 (79.5) 6 (10.7)Good 9 (20.5) 50 (89.3)ACTIVE SYMPTOMS 0.000*
Present 36 (81.8) 7 (12.5)Absent 8 (18.2) 49 (87.5)
* - Significant

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society360
onset after the marriage, and the difference wassignificant (p=0.042). The difference in durationof illness in the two groups was not significant.Enquiry about the patient’s current illness statusand PANSS assessment revealed that there wassignificant difference in the symptom profile of thepatients in the two groups; having more number ofrelatively asymptomatic patients and having lowerscores on PANSS in the well-adjusted group ascompared to the poorly adjusted group. Number ofrelapses and hospitalizations was significantlyhigher in the poorly adjusted group as well as pooradherence to treatment, when subjectively enquiredfrom the patient’s spouses.
DiscussionOn DAS, mean average score of ‘consensus
on matters of importance to marital functioning’sub-scale was highest (3.307) and affect expressionwas the lowest (1.66), which suggests that most ofthe patients and their spouses agreed on routine lifeissues like handling family finances, ways ofdealing with parents or in-laws, making majordecisions or household tasks. However, the affectexpression of patients was less, probably due toeffect of illness on patients’ social cognition,negative symptoms and due to effect ofantipsychotics reducing the emotional expressivity,which can thereby reduce the same in spouse. Also,the spouse in most cases, were taking on some extraresponsibilities, due to which they were mostlybusy, tired and fatigued.
Dividing the entire subjects, on the basis ofDAS, two groups were identified - one having goodadjustment and other, poor. There was no significantdifference between the mean age of spouses havingpoor adjustment and good marital adjustment,which is in keeping with the findings of an Indianbased study.17 Difference on gender, education andfamily structure in two groups was also notsignificant. However, certain studies showed thatfemale caregiver spouses had more problematicadjustment.13
Considering the onset of illness, dyadic adjust-ment was better in cases where illness developedafter marriage compared to ones before marriage.According to a study, this was a factor responsiblefor better marital outcome, in a 10-years follow-upstudy.7 This might be because firstly, if there was a
period after marriage, where the person wasnormally carrying out the responsibilities expectedof a marriage, the emotional bond between the twogets strengthened and more of positive appraisal isfound in caregiving. For the same reason, thereseems to be more consensus between them even inthe later phases. Secondly, Indians have more of afatalistic attitude, and for them, marriage is a one-time event. So, anything that happens after marriageis considered as destiny by the spouse and caringfor their ill spouse becomes a duty for them, whichhas its social recognition and reinforcement.However, when illness is present before marriage,in most cases, spouse is not aware of it, probablydue to fear of disengagement and also stigma relatedto illness. In such cases, there is often an elementof being cheated in the spouse’s mind and may notnecessarily be aware of the risk of a renewed acuteillness phase and cannot anticipate the burdensconnected with it. It is found in previous studiesthat caregiver appraisal and functioning is betterwhen the choice of being a caregiver is made bythe spouse himself.18 Further, the impaired socialperception and cognition of the schizophrenicspouse makes it difficult to establish the intimacyand attachment at any point of time in therelationship, and thus leads to a comparatively pooradjustment even in the later years of life.
There was no significant difference betweenthe duration of illness of the patients in the twogroups, which is consistent with findings of Kumarand Mohanty.19 In our study, the results could bedue to the fact that we included only those spouseswhere the duration of illness is minimum 5 years.Generally, the initial years after onset of illness arecrucial when spouse as a caregiver, has to face lotof changes in terms of their role transition,responsibilities, expectations from the ill spouse andother family members and difficult and unexpectedbehaviour of the patient. They even have to under-stand the nature and course of the illness andmanage with the upcoming alterations in theirmarital relations. During this time, they learn tocope with the situations, and therefore have frequentadjustment issues. But with passing years, theyprobably become more perceptive and developacceptance to it, and the illness also stabilizes withtime.
In this study, it was evident that presence and

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 361
severity of symptoms is related to marital adjust-ment. PANSS scores (suggesting the currentseverity of symptoms of the patient), were higherin poorly adjusted group. A study by Kate et al20
found that caregivers report more positiveexperience when the caregiver had fewer dailyhours of responsibility towards the ill relative,whichis possible only when the behaviour (in terms ofpositive symptoms) of the patient is manageableand the emotional expressivity, attachment andsocial cognition is not much affected (due tonegative symptomatology). However another studyindicated that it is not the patient’s symptoms butability to perform expected roles that matters.21
We also found that the number of relapses andhospital admissions were significantly more in thegroup having poor adjustment, which is consistentwith findings of an Indian study,7who found theseas predictors of poor marital outcome at 10 yearsfollow-up.With every relapse, the entire functioningof the spouse gets disrupted, starting from house-hold routine to care of children, from caring of thepatient to safety responsibilities, and taking care ofself. Hospitalizing the patient brings uponadditional financial burden to the spouse. Andusually, every relapse takes a toll over the patientand the spouse in form of leaving some residualsymptoms, thereby worsening their overallfunctioning and leading to a worse outcome.According to another study, more symptomatic thepatient and more number of relapses was related tonegative caregiving experiences as well in thespouses.22
Considering compliance, it was found to begood in the well-adjusted group, which seems quiteobvious, as the spouses who are having good maritaladjustment would be having more positive care-giving and thus would take more care of their illrelative in all respect, including compliance, whichis an important factor responsible for health andgood outcome.
ConclusionThis study shows that onset of illness after
marriage and less severe symptoms were related togood marital adjustment and onset of illness beforemarriage, more number of relapses and hospitaliza-tions were related to poor adjustment. Gender andeducation of spouse and duration of illness did not
appear to have any significant effect.As mental health professionals, the spouses of
the patients with schizophrenia can be encouragedto discuss various aspects of marriage and relatedissues like change in the roles and responsibilitiesof the carer spouse, parenting issues, and concernsregarding intimacy and sexuality, which are rarelyput forth, especially in Indian settings.
The cross-sectional nature and smallsample size were the limitations of this study. Alarger sample size which is community based wouldprovide more generalizable results. In addition,qualitative approach would have yielded moremeaningful and probably some untouched factorsin the subject.
References
1. Estroff S. Self, Identity, and SubjectiveExperiences of Schizophrenia: In Search of theSubject. Schizophr Bull 1989; 15(2) : 189–196.
2. Lippincott Williams & Wilkins. Schizophrenia.Sadock Benjamin J., Sadock Virginia A.,editors. Kaplan and Sadock’s Synopsis ofPsychiatry: Behavioral Sciences/ClinicalPsychiatry, tenth North American edition 2010;467.
3. Li XJ, Wu JH, Liu JB, Li KP, Wang F, SunXH, et al. The influence of marital status onthe social dysfunction of schizophrenia patientsin community. Int J Nurs Sci 2015; 2 : 149-52.
4. Lane A, Byrne M, Mulvany F, Kinsella A,Waddington JL, Wash D, Larkin C,O’Callaghan E. Reproductive behaviour inschizophrenia relative to other mentaldisorders; evidence for increased fertility inmen despite reduced marita l rate. ActaPsychiatr Scand 1995; 91 : 222-228.
5. Lee PWH, Lieh-Mak F, Yu KK, Spinks JA.Patterns of outcome in schizophrenia in HongKong. Acta Psychiatr Scand 1991; 84 : 346-352.
6. Deshmukh V, Bhagat A, Shah N, Sonavane S,Desousa AA. Factors affecting marriage inschizophrenia: A cross-sectional study. J MentalHealth Hum Behav 2016; 21(2) : 122.
7. Thara R, Srinivasan TN. Outcome of marriagein schizophrenia, Soc Psychiatry PsychiatrEpidemiol 1997; 32 : 416-420.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society362
8. Salokangas RKR. Living situation, socialnetwork and outcome in schizophrenia: A five-year prospective follow-up study. ActaPsychiatr Scand 1997; 96 : 459-468.
9. Szmukler G. From family ‘burden’ tocaregiving. Psychiatr Bull1996; 20 : 449-451.
10. Jungbauer J, Angermeyer M. Living with aSchizophrenic Patient: A Comparative Study ofBurden as It Affects Parents and Spouses.Psychiatry 2002; 65 : 110-123.
11. Sheehan DV, Lecrubier Y, Sheehan KH, et al.The Mini-International Neuropsychiatric Inter-view (M.I.N.I.): the development and validationof a structured diagnostic psychiatric interviewfor DSM-IV and ICD-10. J Clin Psychiatry1998; 59 Suppl 20: 22–33.
12. Spanier GB. Measuring dyadic adjustment:New scales for assessing the quality of marriageand similar dyads. J Marriage Fam 1976; 38 :15-28.
13. Busby DM, Christensen C, Crane DR. LarsonJH. A revision of the Dyadic Adjustment Scalefor use with distressed and non-distressedcouples: Construct hierarchy and multidimen-sional scales. J Marital Fam Ther 1995; 21 :289-308.
14. Eiseberg SD, Peluso PR, Schindler RA. Impactof brief marriage and relationship educationclasses on dyadic adjustment. [Monograph onthe Internet]. PAIRS Foundation EvaluationReport. 2011.Available from http://www.pairs.com/PDF/MRE_Dyadic_Adjustment.pdf
15. Kay SR, Opler LA, Fiszbein A. Significance
of positive and negative syndromes in chronicschizophrenia. Br J Psychiatry1986; 149 : 439-448.
16. Thara R, Srinivasan TN. How stigmatizing isschizophrenia in India? Int J Soc Psychiatry2000; 46(2) : 135-141.
17. Kumari S, Singh AR, Verma AN, Verma PK,Chaudhary S. Subjective burden on spouses ofschizophrenia patients. Ind Psychiatry J 2009;18(2) : 97.
18. Mo FY, Chung WS, Wong SW, Chun DYY,Wong KS, Chan SSM. Experience of caregivingin caregivers of patients with first-episodepsychosis. Hong Kong J Psychiatry 2008; 18 :101.
19. Kumar S, Mohanty S. Spousal burden of carein schizophrenia. J Indian Acad Appl Psych2007; 33 : 189-94.
20. Kate N, Grover S, Kulhara P, Nehra R. Positiveaspects of caregiving and its correlates incaregivers of schizophrenia: A study from northIndia. East Asian Arch Psychiatry 2013; 23 :45-55.
21. Harvey K, Burns T, Fahy T, Manley C, TattanT. Relatives of patients with severe psychoticillness: factors that influence appraisal ofcaregiving and psychological distress. SocPsychiatry Psychiatr Epidemiol 2001; 36 : 456-461.
22. Singh S, Sinha D, Raut NB. Caregiving experi-ence and marital adjustment inspouses ofpatients with schizophrenia. Indian J SocPsychiatry 2019; 35 : 125-130.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 363
Depression among elderly people livingseparately from their children: a cross-sectional
comparative studyShiv Prakash,1 Adya Shanker Srivastava,2 Jai Singh Yadav2
Department of Psychiatry, Institute of Medical Sciences, Banaras Hindu University,Varanasi-221005, Uttar Pradesh, India
Contact: Shiv Prakash, Email: [email protected]
Original Article
IntroductionPopulation of older adults or elderly people is
increasing day by day in all over the world and thisincrease in the population of older adults has beenseen between the years 2001 to 2011.1 According toPopulation Census 2011, there are about 104 millionelderly people (aged 60 years or above) in India.2,3
And there are about 15 million of the elderly peopleliving alone or with spouse only in India, and mostof them are females.4 In National Family HealthSurvey (NFHS) 2005-06, it was found that livingarrangement of the elderly in India is getting
changed day by day. There are about three fourthsof elderly people living either alone or with theirspouse in India.5 Due to this change in livingarrangement most the elderly people are being leftbehind at their own home without any proper careand support especially in developing countries likeIndia.
World Health Organization (WHO) hasdescribed that elderly living alone in their late lifeincrease the risk of the decline in their quality oflife. When elderly living alone or separately in theirlate life is often taken as an undesirable state of
Abstract
Background: Prevalence of depression is increasing day by day today especially among elderlypeople. It has been observed a large amount of decline in joint family system in India. Due tothis decline in family system most of the elderly people have to live separately from their childrenwithout any proper support and care at home. Objective: this study was to assess the level ofdepression among elderly people living with their children and elderly people living separatelyfrom their children. Materials and Methods: A cross sectional study was conducted in someselected area in Varanasi district in Uttar Pradesh. Total sixty (30 elderly people living separatelyfrom their children and 30 elderly people living with their children) were selected throughpurposive sampling method. All of them assessed by a semi structured questionnaire includingsocio-demographic variables and Hamilton Depression Rating Scale (HDRS). Result: The meanage of respondent was 68.20 (±7.14) years. Out of 60 respondents 34(56.7%) were female and33(55%) were widow/widower. Majority of the respondent were illiterate and belonged to OtherBackward Class and Hindu religion. Marital status, education, religion, and living conditionwere found significantly associated with depression. Depression was found significantly moreprevalent among elderly people living separately from their children compared to elderly peopleliving with their children or other family members. Conclusion: Findings of the present studyrevealed that elderly people living separately from their children without any proper care andsupport at their home, used to easily become target of depression.
Keywords: Aging, Older Adults, Mental Health, Left Behind, Living Arrangement

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society364
risk for their health and require a specialattention.5,6,8 Depression has become a major issuein all over the world today. In the various typespsychiatric disorders, depression is the mostcommon type of disorder found worldwide, withmore than 300 million people affected. 7 Theprevalence of depressive disorder is very high inthe elderly people. According to an estimation doneby the WHO the prevalence of depression in olderadults generally varies between 10% and 20%depending upon social and cultural situations.9,10
According to a previous study, the medianprevalence rate of depression in elderly populationin the world was determined to be 10.3%. But inIndia the median prevalence of depressive disorderin elderly people was determined to be 21.9% (IQR,11.6%–31.1%).11
Some previous studies have found significantrelationship between mental health and livingarrangement of elderly people. But very fewresearchers have studied about the prevalence ofdepression among elderly people living separatelyfrom their children or family members without anyproper care and support at their home in thecommunity. Hence, the present study was plannedto assess and compare the prevalence of depressionamong elderly people living separately from theirchildren and elderly people living with theirchildren or other family members in the community.
Objectives:• To assess and compare the level of depre-
ssion among elderly people living with theirchildren and elderly people livingseparately from their children.
• To assess the relationship between socio-demographic variables and level ofdepression.
Hypothesis:• There will be no significant difference
between the level of the depression amongelderly people living separately from theirchildren and elderly living with theirchildren or other family members.
• There will be no significant relationshipbetween the socio-demographic variablesand depression.
Materials and MethodsStudy Design: A Cross Sectional Study was
carried out in some selected areas. Study Area: Thestudy was conducted in some selected areas inVaranasi district in Uttar Pradesh. Period of thestudy: The study was conducted for period of 3months (October 2017 to December 2017). Thefield data collection was carried twice (everyThursday and Saturday) in a week. Ethical clearancefor the present study was taken from the ethicalcommittee of Institute of Medical Sciences (IMS),Banaras Hindu University, Varanasi, Uttar Pradesh.
Sample size calculation: For the calculationof sample size, first we take average of prevalenceof depression among elderly people from findingsof some previous studies =11.25 (approximately11).11,14,21,22,28 Considering this, the sample size ofthe present study was calculated. Hence, Z=95%confidence Interval=1.96. The prevalence was takenp=11, the allowed error (d) is taken 8%.
The sample size was calculated with theformula:
=
= 58.76 (Approximately 60)Sample Size and Sampling Method: Total 60
elderly person (30 elderly people living separatelyfrom their children and 30 elderly people living withtheir children) aged 60 or above were selectedthrough random sampling method for the study.
Inclusion criteria:• Elderly people aged 60 years and above.• Those who gave the informed consent.• Elderly people living with their children
and family members and Elderly livingseparately from their children.
Exclusion criteria:• Having any hearing or visual impairment
and other physical or mental illness.
Tools used:Semi Structured Interview Schedule (SSIS):
A semi structured interview schedule incorporating

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 365
socio demographic variables like age, sex, maritalstatus, occupation, education, religion, category,family income, residential area, etc. and psychiatrichistory and mental status examination was preparedby the research scholar.
Hamilton depression Rating Scale (HDRS):It is a gold standard clinical rating scale to assessthe severity of, and change in symptoms ofdepression. It is also named as HAM-D, the mostwidely used tool by the clinician and in the researcharea. It was developed by Max Hamilton in 1960.12
The original version of HDRS scale contains 17items, later a 21 items version was developed. Alimitation of this scale is that atypical symptoms ofdepression (Hypomania and Hyperphagia) are notassessed. A score between 0-7 accepted as normal(or clinical remission), 8-17 indicate milddepression; 18-23 indicate moderate depression andscore 24 or above indicate severe depression. Thevalidity of the scale has been reported between 0.65to 0.90 and test retest value has been reported ashigh as 0.81.
Sampling Procedure: First a list of elderlypeople living in selected study area was preparedwith help of regional booth level officer (BLO) andParshad. Then the respondents who fulfilled theinclusion and exclusion criteria were selected. Theyinterviewed individually using the semi structuredquestionnaire by the research scholar. Therespondents who have any depressive symptomsthey referred to department of psychiatry for theassessment. They were assessed and diagnosed(Using diagnostic criteria of International StatisticalClassification of Diseases and Related HealthProblems (ICD-10) for depression) by thepsychiatrist and then the severity of depression wasassessed using Hamilton Depression Rating Scale.
Statistical Analysis: The data were entered inthe MS Excel after the competition of datacollection. The qualitative data were presented inthe form of frequency and percentage. The analysiswas performed using IBM SPSS Statistics software(Version-20). The significant association of socio-demographic variables with depression was testedby Chi squire test or Fisher’s exact test at a 5%level of significance. Significance difference ofdepression was assessed using students indepen-dent-samples t-test.
ResultsTable-1 Presents the distribution of the
respondents by socio-demographic characteristicsand other study variables. Majority of the respon-dents 42 (70%) were between age group 60-75 witha mean age of 68.20 (±7.14) years and rest of them18 (30%) were between age group 76-85 years. Outof the 60 respondents 34 (56.7%) were female and26 (43.3%) were male. Majority of the respondents33 (55%) were widow or widower and 27 (45%)were married. Most of the respondents (56.7) wereLiterate and other (43.3%) were illiterate. Therewere majority 49 (81.7) of the respondents belongedto Hindu religion. Approximately (45%) half ofthe respondents were belong to Other BackwardClass (OBC) category followed by (28.3%)General, (16.7%) Scheduled Class (SC) and (10%)Scheduled Tribes (ST). Most of the respondents 38(76.7) were living in urban area. Out of the 60respondents, majority of the respondents 46 (76.7%)were unemployed/house wife/retired. Most of them(58.3%) were belong to low socio economic statusdue to low family income below Rs 5000. Out ofthe 60 the respondents 30 (50%) were living withtheir children and 30 (50%) were living separatelyfrom their children without any proper support andcare.
Table-2 Shows the association of the socio-demographic characteristics with depression.Majority of the respondents 31 (73.8%) betweenage group 60-75 years found suffering withdepression. Female were found highly 27 (79.4%)affected with depression. A significantly higherprevalence of depression was found in therespondents who were widow or widower 29(87.9%) than the respondent who were married 14(51.9%). The prevalence of depression was highamong illiterate 28 (82.4%) than literate 15(57.7%),this difference was statistically significant. Thedepression status among Hindu respondent was high32 (65.3%) than Muslim respondents which wasfound statistically significant. The prevalence ofdepression was higher among the respondent whobelonged to scheduled caste. Most of therespondents 17 (77.3%) were found affected withdepression than rural area. The prevalence ofdepression found higher among unemployed/housewife/retired 35(76.1%) than employed/business/

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society366
shop owner 8(57.1%). Majority of the respondents29 (82.9%) who were economically poor founddepressed. The respondents who were livingseparately from their children found more 25(83.3%) depressed than the respondents living withtheir children 18 (60%).There was statisticallysignificant association found between livingcondition and depression.
Table-3 Shows that 43 (71.67%) out of the 60respondents were found with depression. Most ofthe (40%) elderly people living with their childrenwere found normal followed by 23.3% found withmild depression, 30% with moderate depression and6.7% with severe depression. In other hand mostof the 10 (33.3%) elderly people living separatelyfrom their children were found with moderatedepression followed by 26.7% with severedepression, 6.7% with very severe depression,16.7% with mild depression, and 16.7% were foundnormal.
Table-4 This table presented that there was astatistically significant difference between the meanof HAM-D score of elderly people living with theirchildren (10.87 ± 5.18) and elderly people livingseparately from their children (15.27 ± 5.56).
DiscussionThe present study aimed to assess the presence
and the severity of the depression among elderlypeople living with their children and elderly peopleliving separately from their children without anyproper support and care in the community. In thepresent study the prevalence of depression amongelderly people was found 71.67 % almost consistentwith other studies.13-20 Depression was found highamong elderly belonging to age group 60-75 yearsthan aged group 76-85 years or above, similar resultwas found in a previous study.21 In contrast to resultof present study some studies have found rate ofdepression increased with increase age ofindividuals.22-25
The severity of the depressionwas found to behighamong females in study consistent with someother studies conducted India and other developingcountries.18,23,24,27-31 Present study found a highersignificant relationship with marital status anddepression among elderly people, and severity ofthe depression were found high among elderly whowere widow or widower.18,19,24,25,27 The presentsstudy revealed that there is a significant relationship
Table-1: Socio-Demographic Characteristics of the Respondents
Variables Frequency Percentage (%)
Age (years) 60-75 42 70.076-85 18 30.0
Gender Male 26 43.3Female 34 56.7
Marital status Married 27 45.0Widow/widower 33 55.0
Eduacation Literate 34 56.7Illiterate 26 43.3
Religion Hindu 49 81.7Muslim 11 18.3
Category General 17 28.3Other Backward Class 27 45.0Scheduled Class 10 16.7Scheduled Tribes 6 10.0
Residence Rural 22 36.7Urban 38 63.3
Occupation Employed/business/shop owner 14 23.3Unemployed/housewife/retired 46 76.7
Monthly income Below 5000 35 58.35001-15000 11 18.315001-25000 7 11.725001-35000 33 5.0Above 35000 4 6.7
Living with Living with their children 30 50.0Living separately from children 30 50.0

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 367
Table-2: Association of Socio-Demographic Variables with DepressionSocio Demographic STATUS OF DEPRESIONVariables Depression Depression Total Chi-square df p-value
Present Absent N=60 valuef (%) f (%) f (%)
Age (Years)60-75 31 (73.8) 11 (26.2) 42 (70.0) 0.317 1 0.57476-85 12 (66.7) 6 (33.3) 18 (30.0)
GenderMale 16 (61.5) 10 (38.5) 26 (43.3) 2.318 0.128
Female 27 (79.4) 7 (20.6) 34 (56.7)Marital Status
Married 14 (51.9) 13 (48.1) 27 (45.0) 9.492 1 0.002Widow/widower 29 (87.9) 4 (12.1) 33 (55.0)
EducationLiterate 15 (57.7) 11 (42.3) 26 (43.3) 4.413 1 0.036Illiterate 28 (82.4) 6 (17.6) 34 (56.7)
ReligionHindu 32 (65.3) 17 (34.7) 49 (81.7) 5.325 1 0.021
Muslim 11(100) 0 (0) 11 (18.3)Category
General 12 (70.6) 5 (29.4) 17 (28.3) 5.044 3 0.169Other backward class 17 (63.0) 10 (37.0) 27 (45.0)
Scheduled class 10 (100.0) 0 (0) 10 (16.7)Scheduled tribes 4 (66.7) 2 (33.3) 6 (10.0)
ResidenceRural 17 (77.3) 5 (22.7) 22 (36.7) 0.538 1 0.463Urban 26 (68.4) 12 (31.6) 38 (63.3)
OccupationEmployed/business/shop owner 8 (57.1) 6 (42.9) 14 (23.3) 1.897 1 0.168Unemployed/housewife/retired 35 (76.1) 11 (23.9) 46(76.7)
Monthly IncomeBelow 5000 29 (82.9) 6 (17.1) 35 (58.3) 6.667 4 0.1555001-15000 6 (54.5) 5 (45.5) 11 (18.3)
15001-25000 3 (42.9) 4 (57.1) 7 (11.7)25001-35000 2 (66.7) 1 (33.3) 3 (5.0)Above 35000 3 (75.0) 1 (25.0) 4 (6.7)
Living WithLiving with their Children 18 (60.0) 12 (40.0) 30 (50.0) 4.022 1 0.045
Living Separately from their children 25 (83.3) 5 (16.7) 30 (50.0)p < 0.05=Statistically significant
Table-3: Severity of the Depression found among elderly peopleGroups Severity of Depression n (%)
Normal Mild Moderate Severe Very Severe Totalf (%) f (%) f (%) f (%) f (%) N=60
f (%)
Living with their Children 12 (40.0) 7 (23.3) 9 (30.0) 2 (6.7) 0 (0) 30 (50.0)Living Separately from their children 5 (16.7) 5 (16.7) 10 (33.3) 8 (26.7) 2 (6.7) 30 (50.0)
Table-4: Comparison of HDRS Score among elderly people living in different conditions
Variable N=60 Mean SD P value Significance
Living with their Children 30 10.87 5.18 .002 SignificantLiving Separately from their children 30 15.27 5.56
p < 0.05=Statistically significant

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society368
with education and depression, there prevalenceof the depression was found high among illiterateas compare to literate respondent, consistent withsome previous studies.17-19,23,32
The depression status among Hindu respondentwas high (65.3%) than Muslim respondents whichwas found statistically significant, this finding issimilar to a previous study conducted in India.29 ThePrevalence of depression was found high amongelderly living in urban area than elderly peopleliving in rural area. Similar findings were alsoreported in other studies.19,20,23,28,29,33
Depression was found common in thoserespondents who were unemployed, housewife, andretired as compared to those respondents who wereemployed. Some previous studies also found similarresult to the present study.21,23And the prevalenceof depression was found higher among respondentbelonging to low or poor socioeconomic status thanthose belonging to middle or upper socioeconomicstatus consistent to some previous studies.21,24,25-27
In the present study the most of elderly peoplewere found normal (more than one third) and otherswere found mild to very severe depression. Theseverity of the depression was found high in elderlypeople living separately from their children, andsimilar findings were found in some previousstudies.30,31
There was significant association foundbetween living arrangement of elderly people anddepression. Also there was a significant differencefound between the mean of HDRS score of elderlypeople living separately and elderly people livingwith their children. In the present study theprevalence of depression was high among elderlyliving separately from their children than thoseliving with their children. This might have occurreddue to lack proper social and financial support andcare of the family members. Similarly someprevious studies conducted in India, China andKorea have revealed that elderly people livingseparately from their children or left behind havehigh prevalence of depression than those living withtheir children or grandchildren or other familymembers.32-34 In contrast to present findings a studyconducted by Sharma et al35, in which the resultwas found that the prevalence of depression washigh among elderly people living with their spouseand children than those living with spouse or alone.
LimitationsThe generalization of the findings of the present
study is limited due to the less number of samplesize. It was a cross sectional study and therespondent were not followed up. It was alsodifficult to find the related study sample. Therespondent may not have been representative forthe study.
ConclusionThe present study was conducted to assess the
comparison of the status of the depression amongelderly people living separately from their children.The present study revealed that depression wassignificantly associated with marital status,education, religion, and living condition of elderlypeople. And depression was found more prevalentamong elderly those are living separately from theirchildren without any proper emotion, social andfinancial support than those living with theirchildren and other family members. Findings of thepresent study suggests that elderly people needemotional, financial and social support and carefrom their family members especially their son ordaughter and grandchildren. There is also need ofsome further studies in this area to find out the otherphysical and mental health related problems amongelderly people in India.
References1. United Nations. Report of the Second World
Assembly on Ageing: Madrid, 8–12 April 2002.United Nations, 2002. [cited 2018 Feb 16].Available from Netlibrary: http://mospi.nic.in/sit es/default /files/publica tion_repor ts/ElderlyinIndia_2016.pdf
2. Sathyanarayana KM, Kumar S, James KS.Living arrangements of elderly in India: policyand programmatic implications. PopulationAgeing in India 2014; 74.
3. Situational analysis of elderly in India. 2011.(accessed on 2014 May 14th ). Available from:http://mospinew/upload/elderly in India.pdf.
4. Nagrajan R. 15 million elderly Indians live allalone: Census. The Times of India. [cited 2018Feb 16]. Available from Netlibrary:https://timesofindia.indiatimes.com/india/15-million-elder ly-Indians- l ive-a ll-alone-Census /articleshow/43948392.cms

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 369
5. IIPS O. National Family Health Survey (NFHS-3), 2005-06: India. Mumbai: InternationalInstitute of Population Sciences 2007.
6. Kharicha K, Iliffe S, Harari D, Swift C,Gillmann G, Stuck AE. Health risk appraisal inolder people 1: are older people living alonean ‘at-risk’group?. Br J Gen Pract 2007;57(537) : 271-6.
7. World Health Organization (WHO). Preventionof Mental Disorders in the Elderly. WHO;Copenhagen: 1977.
8. Iliffe S, Tai SS, Haines A, Gallivan S,Goldenberg E, Booroff A, Morgan P. Areelderly people living alone an at risk group?.BMJ 1992; 305(6860) : 1001-4.
9. World Health Organization [homepage on theInternet] Mental health, depression: let’s talk.Available from hhttp://www.who.int/mental_health/management/depression/en/[Accessed15th Jan 2018]
10. World Health Organization (WHO). Preventionof Mental Disorders in the Elderly. WHO;Copenhagen: 1977.
11. Barua A, Ghosh MK, Kar N, Basilio MA.Prevalence of depressive disorders in theelderly. Ann Saudi Med 2011; 31(6) : 620-4.
12. Hamilton M. A rating scale for depression. JNeurol Neurosurg Psychiatry 1960; 23(1) : 56-62.
13. Tiwari SC, Srivastava G, Tripathi RK, PandeyNM, Agarwal GG, Pandey S, Tiwari S.Prevalence of psychiatric morbidity amongstthe community dwelling rural older adults innorthern India. Indian J Med Res 2013; 138(4): 504-14.
14. Rathod MS, Dixit JV, Goel AD, Yadav V.Prevalence of depression in an urban geriatricpopulation in Marathwada region of WesternIndia. Indian J Psychol Med 2019; 41(1) : 32-37.
15. Jain RK, Aras RY. Depression in geriatricpopulation in urban slums of Mumbai. IndianJPublic Health. 2007; 51(2) : 112-13.
16. Swarnalatha N. The prevalence of depressionamong the rural elderly in Chittoor District,Andhra Pradesh. Journal of clinical anddiagnostic research: JCDR. 2013; 7(7) : 1356-60.
17. Amonkar PS, Mankar MJ. Geriatric Depression
and Associated Risk Factors: A Cross-sectionalStudy in an Urban Setting. MGM J Med Sci2015; 2 : 179-83.
18. Gupta S, Singh AK, Kurupath A. ComparativeStudy of Depressive disorders in Elderly fromRural and Semi urban Areas of Varanasi. IndianJ Psychiatry 2015; 57(5) : S45-S45.
19. Naik PR, Nirgude AS. Depression among theelderly: A cross sectional study in a ruralcommunity of South India. Natl J CommunityMed 2015; 6 : 394-7.
20. Zhao KX, Huang CQ, Xiao Q, Gao Y, Liu QX,Wang ZR, et al. Age and risk for depressionamong the elderly: A meta-analysis of thepublished literature. CNS Spectr 2012; 17 :142–54.
21. Sengupta P, Benjamin AI. Prevalence ofdepression and associated risk factors amongthe elderly in urban and rural field practice areasof a tertiary care institution in Ludhiana. IndianJ Public Health 2015; 59 : 3–8.
22. Chauhan P, Kokiwar PR, Shridevi K, KatkuriS. A study on prevalence and correlates ofdepression among elderly population of ruralSouth India. Int J Community Med PublicHealth 2017; 3(1) : 236-9.
23. Abas M, Tangchonlatip K, Punpuing S,Jirapramukpitak T, Darawuttimaprakorn N,Prince M, Flach C. Migration of children andimpact on depression in older parents in ruralThailand, Southeast Asia. JAMA Psychiatry2013; 70(2) : 226-33.
24. Ravindra NR, Rashmi MR, Maheswaran R.Risk factors for depression among elderly inBangalore urban district: a case control study.Int J Community Med Public Health 2017; 4(8): 2696-700.
25. Sanjay T, Jahnavi R, Gangaboraiah B, LakshmiP, Jayanthi S. Prevalence and factors influenc-ing depression among elderly living in the urbanpoor locality of Bengaluru city. Int J HealthAllied Sci 2014; 3(2) : 105-.
26. Chalise HN, Rai SL. Prevalence and correlatesof depression among Nepalese Rai older adults.J Gerontol Geriatr Res 2013; 2(4) : 1-5.
27. D’souza L, Ranganath TS, Thangaraj S.Prevalence of depression among elderly in anurban slum of Bangalore, a cross sectionalstudy. Int J Interdiscip Multidiscip Stud 2015;

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society370
2(3) : 1-4.28. Pilania M, Bairwa M, Khurana H, Kumar N.
Prevalence and predictors of depression incommunity-dwelling elderly in rural Haryana,India. Indian J Community Med 2017; 42(1) :13-18.
29. Soni S, Shukla S, Kumar M. Prevalence ofdepression and associated risk factors amongthe elderly in rural field practice areas of atertiary care institution in Katihar, Bihar. Int JAdv Med 2016; 3(4) : 1016-19.
30. Radhakrishnan S, Nayeem A. Prevalence ofdepression among geriatric population in a ruralarea in Tamilnadu. Int J Nutr Pharmacol NeurolDis 2013; 3(3) : 309-3012.
31. Pawar RD, Kale KM ,Aswar NR, Solanke S. Across sectional study on prevalence of depre-
ssion and its socio-demographic correlatesamong elderly in rural India. IJFCM 2018; 5(4): 210-214.
32. Khamu S, Langstieh BT. Living Arrangementsamong the Chakhesang Elders. IOSR JHSS2015; 20(4): 54-60.
33. Lee YM, Holm K. Family relationships anddepression among elderly Korean immigrants.ISRN Nursing 2011; 1-7.
34. He G, Xie JF, Zhou JD, Zhong ZQ, Qin CX,Ding SQ. Depression in left behind elderly inrural China: Prevalence and associated factors.Geriatrics Gerontol Int 2016; 16(5) : 638-43.
35. Sharma R, Dey AB, Chadha NK. Functionalityand Depression in Late Life. DU J UndergradRes Innovation 2015; 1(3) : 153-168.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 371
Impact of Cannabis Use on Executive Functionsin Male Patients with Bipolar Disorder: A
Comparative StudyPushpanjali Vishwakarma,1 Anshul Kumar,2 Neetee Mehata3
1,3Department of Psychology, Bhagwant University, Ajmer;2Department of Psychiatry, DDU Hospital, Delhi;
Contact: Anshul Kumar, E-mail: [email protected]
Original Article
IntroductionBipolar Disorder (BD) is a severe psychiatric
disorder characterized by recurrent episodes ofmania and/or hypomania, as well as depressiveepisodes. It represents the sixth leading worldwidecause of psychosocial disability, morbidity, andsuicide.1 Decreased concentration and attention arecommon complaints among bipolar patients. Suchcognitive impairment can be objectively measuredwith neuropsychological tests.2 Meta-analyses ofneuropsychological studies has confirmed that there
is cognitive deficits in patients with bipolar disorderthat persist in euthymia and during periods ofremission3,4,5,6 with verbal memory and executivefunction being the most commonly encounteredareas of cognitive impairment.
Cannabis is the most widely used illicitsubstance in the world. The National HouseholdSurvey of Drug Use in India reported that cannabisis the third most widely used substance in Indiaafter tobacco and alcohol7.
The impact of cannabis use disorders (CUDs)
Abstract
Introduction: Decreased concentration and attention are common complaints among Bipolarpatients. Compared to the general population, patients with Bipolar disorder have a two tothree-fold increase in Cannabis use rates. Cognitive deficits in patients with Bipolar disorderpersist in euthymia and during periods of remission with verbal memory and executive functionmost commonly affected. Only few studies have evaluated the relationship between cannabisuse and cognition in patients with Bipolar disorder and shown conflicting results. Aim: Tostudy the impact of cannabis use on executive functions in patients with Bipolar disorder.Materials and Methods: Patients with Bipolar mood disorder having YMRS score < 6 andHDRS score < 7 meetingexclusion and inclusion criteria were divided in two groups. CannabisUse Disorder Identification Test (CUDIT) was administered to both groups: Group 1: Thirtypatients with Bipolar disorder with cannabis use disorder (CUDIT score >8) Group 2: Thirtypatients with Bipolar disorder without cannabis use disorder. Both groups were administeredWisconsin card sorting test (WCST)for evaluation of executive functions. Data Collected wastabulated and analysed using SPSS version 16. Results: On measures of WCST variables Bipolarpatients with cannabis use disorder performed significantly worse than Bipolar patients withoutcannabis use disorder on Number of Total Responses, Percent errors, Percent PerseverativeResponses, Percent Perseverative Error, Percent Conceptual Level responses and Learning tolearn.Conclusions: Present study supports the hypothesis that Bipolar patients who use cannabishave greater cognitive deficits, in particular executive dysfunction.
Key word: Executive Function, Cognitive Function, Cannabis Use Disorder, Bipolar Disorder.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society372
is particularly pertinent among subjects with majorpsychiatric disorders. Compared to the generalpopulation, patients with bipolar disorder have atwo to three fold increase in CUD rates.8, 9,10,11,12
Several studies reported that cannabis affectcognition in healthy individuals13, 14 but only fewstudies had evaluated the relationship betweencannabis use and cognition in patients with bipolardisorder and shown conflicting results. Some hadreported cognitive dysfunctions in BD with co-morbid CUD,15 while others had reported superiorcognitive performance in bipolar patients with co-morbid CUD when compared to patients with nocannabis use history.16,17
In spite of high prevalence of cannabis usedisorder in India there is scarcity of systemic studiesfrom India assessing the cognitive functions amongbipolar patients. One may expect cannabis to havea detrimental effect on cognitive performance.However, the literature provides inconsistentevidence of the effects of cannabis on cognitivefunction in bipolar disorder. Given that thesepatients already suffer from compromisedcognition, it is necessary to determine whethercannabis use causes added impairments, remediescore deficits, or whether the effects areinconsequential. So this study was done to comparethe cognitive outcome in bipolar patients withcannabis use disorder with bipolar patients withoutcannabis use disorder.
AimTo study the impact of cannabis use on
executive functions in patients with bipolardisorder.
Materials and MethodsThe study was conducted in the psychiatry
department of tertiary care hospital. Male Patientsaged between 18-55 yrs, educated up to 10th grade,with Diagnosis of Bipolar affective disorder,currently in remission (as per ICD 10- Diagnosticcriteria) were screened for study. Sociodemographicand clinical profile depicting detailed history ofselected patients were collected in a semi structuredproforma. The patients who passed above screeningwere further administered Hamilton Rating Scalefor Depression (HAM-D) (Hamilton M, 1967) and
Young Mania Rating Scale (YMRS) (Young RC etal, 1978). Patient having either YMRS score of < 6or HDRS score of < 7were further selected for study.
All the selected patients were administeredCannabis Use Disorders Identification Test(CUDIT) (Adamson S. and Sellman J.D. 2003).First thirty of those with score more than 8 onCUDIT scale were assigned to Group 1 named BDwith CUD group. First thirty of those who had nohistory of cannabis use were placed in Group 2named BD without CUD group.
Group 1: Thirty patients with bipolar disorderwith cannabis use disorder (BD with CUD)
Group 2: Thirty patients with bipolar disorderwithout cannabis use disorder (BD without CUD).
The study subjects were given full informationabout the nature of study and informed consent wastaken from the subjects and their guardians present.Institutional ethics committee approval was takenprior to the study. Both groups were administeredWisconsin card sorting test (WCST) (WCST; 1981)for evaluation of executive functions. The selectedneuropsychological test Wisconsin Card SortingTest (WCST) was administered to assess executivefunctions on each subject in a quiet room, withminimal disturbance. Any queries regarding thetests were addressed without giving them any clueabout the possible solutions. Total time taken tofinish the cognitive assessment in a subject variedfrom one to three hours. The test was conducted ina single sitting for all patients.
Data Collected was tabulated and analysedusing SPSS version 16. Chi square test was used todetermine any significance between categoricalsociodemographic variables (marital status,religion, education, occupation, socioeconomicstatus, habitat) and categorical clinical profilevariables (Family history of bipolar disorder, natureof latest mood episode, history of psychotic featuresand medication). For continuous variables (age inyears, age of onset, duration of illness, total numberof episodes, number of manic episodes, number ofdepressive episodes, duration of treatment) pairedt test was used to evaluate significance. Similarly,paired T Test was used to test significance betweenWCST test variables for two groups.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 373

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society374
ResultsThe present study was a cross sectional study
of sixty subjects, out of which thirty were patientswith bipolar disorder without cannabis use disorderas per ICD 10-DCR (BD without CUD), and thirtywere patients with bipolar disorder with cannabisuse disorder (BD with CUD).
Table 1 and 2 shows the comparison of socio-demographic and clinical variables among the twogroups using Chi square test.It yielded significantdifference in education level and occupationbetween the two groups. Bipolar patients withcannabis use disorder are less qualified then theother group (BD without CUD) as majority of
Table-1: Sociodemographic Data of Sample
Demographic Variable BD without CUD BD with CUD Analysis(n=30) (n=30)
N % N % X2 df P
Marital status Married 18 60% 19 63.3% .001 1 1.0Unmarried 12 40% 11 36.7%
Religion Hindu 26 86.7% 26 86.7% .001 1 1.0Muslim 4 13.3% 4 13.3%
Education High school 12 40% 23 76.7% 9.03 3 .029Intermediate 10 33.3% 5 16.7%Graduate 6 20% 1 3.3%Postgraduate 2 6.7% 1 3.3%
Occupation* Unemployed 7 23.3% 13 43.3% 8.79 3 .032Unskilled worker 9 30% 13 43.3%Skilled worker 11 36.7% 4 13.3%Professional 3 10% 0 0
Socioeconomic status*Lower 20 66.7% 21 70% 3.27 2 .195Upper lower 7 23.3% 9 30%Middle 3 10% 0 0
Habitat* Rural 15 50% 18 60% 1.55 2 .922Semiurban 10 33.3% 10 33.3%Urban 5 16.7% 2 6.7%
Table-2: Clinical Profile of sample (Categorical Variables)
Demographic Variable BD without CUD BD with CUD Analysis(n=30) (n=30)
N % N % X2 df P
Family history of Present 8 26.7% 5 16.7% .393 1 .531bipolar disorder Absent 22 73.3% 25 83.3%Latest episode Mania 10 33.3% 4 13.3% 7.45 3 .059
Mania with PF 17 56.7% 26 86.7%Depression 1 3.3% 0 0Depression with PF 2 6.7% 0 0
History of psychotic Present 26 86.7% 30 100% 2.41 1 .12features Absent 4 13.3% 0 0Medication Mood stabilizer (MS) 4 13.3% 3 10% .163 2 .92
Antipsychotics (AP) 2 6.7% 2 6.7%MS+AP 24 80% 25 83.3%
patients we found are educated up to high schooland intermediate (highschool-76.7%, intermediate-16.7%) where as very few are having graduate orpostgraduate degree (graduate-3.3%, pg- 3.3%).Also, unemployment is more in group usingcannabis (43%) when compared to group not usingcannabis (23%). Apart from these two variables chisquare test yielded no significant difference amongother sociodemographic and clinical profilevariables.
Table 3 shows comparison of clinical profileof patients among the two groups. Paired t test wasapplied to compare the variables. Test yieldedsignificant difference in number of depressive

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 375
Table-3: Clinical Profile of sample (continues variables)
Variables BD without CUD BD with CUDMean ± SD (n=30) Mean ± SD (n=30) T P
1. Age in years 30.1 ± 5.41 31.1 ± 5.19 -0.73 0.4682. Age of Onset of Illness in years 23.3 ± 4.86 23.4 ± 3.41 -0.123 0.9033. Duration of Illness in years 7.2 ± 4.05 7.3 ± 3.59 -0.067 0.9464. Number of Depressive Episodes 0.76 ± 0.93 0.2 ± 0.48 2.947 0.005*5. Number of Manic Episodes 3.73 ± 1.55 4.23 ± 1.94 -1.102 0.2756. Total Number of Episodes 4.46 ± 1.75 4.33 ± 2.0 0.274 0.7857. Duration of Treatment in Months 4.13 ± 0.77 4.2 ± 0.71 -0.346 0.73
*Significant at .05 level;** Significant at .01 level
Table-4: Comparison of WCST Variables
Variables BD without CUD BD with CUDMean ± SD (n=30) Mean ± SD (n=30) T P
1. No. of Trials Administered 117.43 ± 15.42 124.2 ± 8.04 -2.13 0.037*2. No. of Correct Responses 79.46 ± 11.5 73.5 ± 17.92 -1.53 0.1313. No. of Errors 37.96 ± 16.2 51.7 ± 22 -2.75 0.008**4. % Errors 31.66 ± 10.98 40.4 ± 15.89 2.475 0.016*5. % Perseverative Responses 22.53 ± 9.41 30.8 ± 16.76 -2.355 0.022*6. % Perseverative Errors 20.2 ± 8.47 27.7 ± 15.23 -2.356 0.022*7. % Non Perseverative Errors 13.03 ± 5.10 13.33 ± 4.88 -0.233 0.8178. % Conceptual Level Responses 58.86 ± 13.64 48.9 ± 18.18 2.401 0.02*9. No. of Categories Completed 4.73 ± 1.48 3.56 ± 1.67 2.855 0.006**10.No. of Trials to Complete 1st Category 20.63 ± 12.27 16.06 ± 9.99 1.58 0.11911.Failure to Maintain Set 1.06 ± 1.04 1.53 ± 1.96 -1.15 0.25512.Learning to Learn -3.43 ± 5.67 -9.54 ± 8.56 3.26 0.002**
*Significant at .05 level;** Significant at .01 level
episodes between the two groups. Bipolar patientswith CUD have less number of depressive episodes(0.2 ± 0.48) then BD patients without CUD (0.76 ±0.93). Apart from this no significant difference wasfound in continuous clinical profile variablesbetween two groups like age in years, age of onset,duration of illness, total number of episodes,number of manic episodes, duration of treatmentetc.
Table 4 shows comparison of WCST variablesbetween two groups of patients.
Total Number of trial administered: Itrepresents the total number of trials that the subjectrequires to complete the task of WCST. On thisvariableBD patient with CUD had the higher meanscore (124.2 ± 8.04) than the other group withoutCUD (117.43 ± 15.42). This result is alsostatistically significant (p=0.037*). It indicatesmarkedly poor performance of the BD patients withcomorbid CUD.
Number of Correct Responses: they represent
the total number of responses which match thesorting principle of WCST. BD Patients with CUDhad low correct responses (73.5 ± 17.92) then theother group without CUD (79.46 ± 11.5). But theresult failed to reach statistical significance(p=0.131)
Number of Errors and Percent Error: thisvariable represents the total number of responseswhich did not match the sorting principle of theWCST. BD Patients with CUD made more errors(51.7 ± 22) then BD patients without CUD (37.96± 16.2). The result is also statistically significant(p=0.008**) and indicates poor performance ofpatients with CUD.
Perseverative Responses: it representsresponses of the subject which match the sortingprinciple of the category (i.e. correct responses) andalso match the sorting principle of the previouscategory (i.e. perseveration). BD patients with CUDgave more perseverative responses (30.8 ± 16.76)then the patients without CUD (22.53 ± 9.41).

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society376
Result is also statistically significant (p=0.022*)and shows poor performance of patients with CUD.
Percent Perseverative Error: they representresponses of the subject which do not match thesorting principle of the category (i.e. error) andmatch the sorting principle of the previous category(i.e. perseveration). On percent perseverative errorBD patients with CUD made more errors as shownby higher mean score (27.7 ± 15.23) then werepatients without CUD (20.2 ± 8.47). Results is alsostatistically significant (p=0.022*) and indicatespoor performance of CUD group.
Percent Non-Perseverative error: Thisvariable represents responses which do not matchthe sorting principle (i.e. error) and also do notmatch the sorting principle of the previous category(i.e. non perseveration). As shown in the table wecan see that both the groups have similar meanscores (Table-4). The results did not reveal anysignificant group differences indicating both groupshave more or less equal performance on thisvariable.
Percent Conceptual Level Responses: whenthree or more responses match the sorting principlein succession they are called as conceptualresponses. BD patients without CUD had moreconceptual level responses (58.86 ± 13.64) then thegroup with CUD (48.9 ± 18.18) and statisticallysignificant difference is seen between two groups(p=0.02*).
Number of Categories Completed: theyrepresent successive ten responses which match thesorting principle (i.e. category). Six such categoriesneed to be completed to finish the task of WCST.The analysis revealed that BD patients without CUDhad completed more categories (4.73 ± 1.48) thenthe BD patients with CUD (3.56 ± 1.67). The resultis statistically highly significant (p=0.006**). BDpatients with CUD performed poorly in thisvariable.
Trials to Complete First Category: theyrepresent total number of responses taken to achievefirst ten consecutive correct responses (i.e. firstcategory). BD patients with CUD performedslightly better in this variable (16.06 ± 9.99) thenthe other group (20.63 ± 12.27). But the result isnot statistically significant.
Failure to Maintain Set: this variablerepresents the situation when the patient
accomplishes five consecutive correct responses butis not able to get ten successive correct responses.On this variable of WCST the BD patient with CUDslightly higher mean score (1.53 ± 1.96) then theother group (1.06 ± 1.04) (Table-4). The result wasnot statistically significant.
Learning to Learn: reflects the client’s averagechange in conceptual efficiency across theconsecutive categories of WCST. BD Patient withCUD had lowest score (-9.54 ± 8.56) then the otherpatient group without CUD (-3.43 ± 5.67). Negativescore indicates poor performance in the test (Table-4). Result was highly statistically significant(0.002**) and suggests markedly poor performanceof patients with CUD as comparison to BD patientwithout CUD.
DiscussionSeveral studies have demonstrated the validity
of the WCST in assessing executive functions, aswell as its applicability in neuropsychologicalassessments in general.18 The ability to measureabstraction and cognitive flexibility is one of theWCST’s advantages.19,20
Our findings are consistent with the views ofCahill et al15 who reviewed the interactions betweenchronic cannabis use and cognitive compromise inbipolar disorder. They highlighted the inherentdifficulties in researching this area including smallsample sizes, differences in clinical presentation orphases of illness, and the confounding effects ofmedication. Baseline neuropsychological deficitshave been found in people with bipolar disorder;these include executive functioning deficits,attentional difficulties and deficits in memory andverbal learning. There are also neuropsychologicaldeficits associated with chronic cannabis usenotably in executive functioning and impulsecontrol. When looking at cognitive functioning incannabis users with bipolar disorder, the deficitsseem to lie mostly in the domain of executivedysfunction. Cahill et al.15 suggest that thesefindings in bipolar disorder represent difficultieswith encoding, concentration and memory, and havesome overlap with cannabis use where the primarydeficits are in decision making, response inhibition,cognitive flexibility and abstraction, in addition toimpaired memory and learning abilities.
Results of our study are also supported by Dixit

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 377
et al.21 While comparing the two groups of bipolarpatients with and without cannabis use disorder theyfound that the patients who are using cannabisshowed more neuropsychological dysfunction thenthose BD patients who are not using cannabis onmost of the scales of AIIMS comprehensiveneuropsychological battery. The result wasstatistically significant in domains of motorfunctions and receptive speech of the battery.
In a different kind of study which partiallysupport our argument of more executive dysfunctionamong cannabis using bipolar patients is done byliraud et al.22 They studied on 119 patients of which77 patients had non affective psychosis and 42patients had mood disorder. Among these patients23.4% presented with a lifetime historyof cannabis abuse/dependence. To assess neuro-psychological performance they used Batteried’Efficience Mnésique 84 to test memoryperformance, WCST and STROOP test to assessexecutive abilities. They found that subjectswith cannabis use disorder performed poorly on theStroop test. This finding remains statisticallysignificant even after adjustment for confoundingfactors. No other significant difference in executiveand memory performance was found afteradjustment for confounding factors (age, gender,educational level, age at onset, diagnosis, andcurrent versus past addictive behaviour).
Surprisingly two recent studies are in contrastto our findings, and reported better cognitivefunctioning in cannabis using bipolar patients.Ringen et al16studied on 273 patients of which 133patients with bipolar disorder and 140 patients withschizophrenia. They found that in bipolar disordersubjects, cannabis use was associated with bettercognitive function. In the bipolar disorder group,the neuropsychological test performance reachedstatistical significance only for executivefunctioning. Braga et al17studied on 200 bipolarpatients of whom 50 had CUD. They found thatbipolar patients with cannabis use disorder (CUD)performed better on measures of attention,processing speed, and working memory than otherbipolar patients. Major limitations of these studiesare that they have not taken euthymic bipolarpatients and percent of symptomatic subjects aremore in group without the history of cannabis use.Thus group differences regarding cognitive function
might be explained by differences in sympto-matology.
The result of present study indicates towards agreater deficit in bipolar patients with CUD whencompared with bipolar patients without CUD inexecutive functioning.
Summary and ConclusionsOn measures of WCST variables bipolar
patients with cannabis use disorder performedsignificantly worse than bipolar patients withoutcannabis use disorder on number of total responses,Percent errors, Percent Perseverative Responses,Percent Perseverative Error, Percent ConceptualLevel responses and learning to learn.
Present study supports the hypothesis thatbipolar patients who use cannabis have greatercognitive deficits, in particular executivedysfunction.
References1. Harvey PD, Wingo AP, Burdick KE,
Baldessarini RJ. Cognition and disability inbipolar disorder: lessons from schizophreniaresearch. Bipolar Disord 2010; 12(4) : 364-375.
2. Martinez-Aran A, Vieta E, Colom F, Torrent C,Reinares M, Goikolea JM, Benabarre A, ComesM, Sanchez-Moreno J: Do cognitive complaintsineuthymic bipolar patients reflect objectivecognitive impairment? Psychother Psychosom2005; 74(5) : 295–302.
3. Robinson LJ, Thompson JM, Gallagher P,Goswami U, Young AH, Ferrier IN, Moore PB:A meta-analysis of cognitive deficits ineuthymic patients withbipolar disorder. J AffectDisord 2006; 93(1–3) : 105–115.
4. Kurtz MM, Gerraty RT. A meta-analyticinvestigation of neurocognitive deficits inbipolar illness: profile and effects of clinicalstate. Neuropsychology 2009; 23 : 551-62.
5. Bora E, Yucel M, Pantelis C: Cognitiveendophenotypes of bipolar disorder: a meta-analysis of neuropsychological deficits ineuthymic patients and their first-degreerelatives. J Affect Disord 2009; 113(1–2) : 1–20.
6. Torres IJ, Boudreau VG, Yatham LN. Neuro-psychological functioning in euthymic bipolardisorder: a metaanalysis. Acta Psychiatr Scand

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society378
Suppl. 2007; 434 : 17-26.7. Ray R. The Extent, Pattern and Trends of Drug
Abuse In India, National Survey, Ministry OfSocial Justice and Empowerment, GovernmentOf India and United Nations Office on Drugsand Crime, Regional Office for South Asia2004.
8. Stinson FS, Ruan WJ, Pickering R, Grant BF.Cannabis use disorders in the USA: prevalence,correlates and co-morbidity. Psychol Med 2006;33 : 1447–1460.
9. Zuardi AW, Crippa JAS, Guimarães FS.Cannabis e Saúde Mental. Uma revisão sobrea Droga de Abuso e o Medicamento. São Paulo:FUNPEC Editora 2008.
10. Leweke FM, Koethe D. Cannabis and psychia-tric disorders: it is not only addiction. AddictBiol 2008; 13(2) : 264-75.
11. Castle D, Murray R. Marijuana and Madness.First edition. United Kingdom: CambridgeUniversity Press 2004.
12. Koskinen J, Lohonen J, Koponen H, IsohanniM, Miettunen J. Rate of cannabis use disordersin clinical samples of patients with schizo-phrenia: a meta-analysis. Schizophr Bull 2010;36 : 1115–1130.
13. Ilan AB, Smith ME, Gevins A. Effects ofmarijuana on neurophysiological signals ofworking and episodic memory. Psychopharma-cology (Berlin) 2004; 176 : 214–222.
14. Ranganathan M, D’Souza DC. The acute effectsof cannabinoids on memory in humans: areview. Psychopharmacology (Berlin) 2006;188 : 425–444.
15. Cahill CM, Malhi GS, Ivanovski B, LagopoulosJ, Cohen M. Cognitive compromise in bipolardisorder with chronic cannabis use: cause orconsequence? Expert Rev Neurother 2006; 6 :591–598.
16. Ringen PA, Vaskinn A, Sundet K et al. Oppositerelationships between cannabis use andneurocognitive functioning in bipolar disorderand schizophrenia. Psychol Med 2009; 6 : 1–11.
17. Braga RJ, Burdick KE, Derosse P, MalhotraAK. Cognitive and clinical outcomes associatedwith Cannabis use in patients with bipolar Idisorder. Psychiatr Res 2012; 200 : 242–245.
18. Demakis GJ. A meta-analytic review of thesensitivity of the Wisconsin Card Sorting Testto frontal and lateralized frontal brain damage.Neuropsychology 2003; 17 : 255-264.
19. Heaton HK. A manual for the Wisconsin CardSorting Test.Odessa (FL): PsychologicalAssessment Resources 1981.
20. Heaton HK, Cheloune GJ, Tally JL, Kay GG,Curtiss G. Wisconsin Card Sorting Test manualrevised and expanded. Odessa (FL): Psycho-logical Assessment Resources 1993.
21. Dixit V, Kenswar DK, Singh AR, ChoudhuryS. Neuropsychological dysfunctions in bipolarmanic patients with and without cannabisdependence. RINPAS J 2011; 3(1) : 62-66.
22. Liraud F, Verdoux H. Effect of comorbidsubstance use on neuropsychological perfor-mance in subjects with psychotic or mooddisorders. Encephale 2002; 28 : 160–168.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 379
Psychophysiotherapy in Management ofCervical Dystonia
Jaswinder Kaur,1 Shweta Sharma,1 M.S. Bhatia2
Department of Physiotherapy,1 Dr. R.M.L. Hospital & ABVIMS, New DelhiDepartment of Psychiatry,2 UCMS & GTB Hospital, Delhi
Contact: Jaswinder Kaur, [email protected]
Psychophysiotherapy
Cervical Dystonia (CD) is a common form ofadult onset, focal dystonia characterized byanomalous and involuntary contraction of cervicalmuscles leading to awkward posture of head andneck and impaired motor control with concurrentactivation of both antagonist and agonist muscles.1,2
Along with motor manifestations, somatosensoryperception deficits and debilitating symptoms likepain, abnormal head posture and tremors are alsoseen.3,4 Mental stress may also contribute to highlevel of dysfunction and affect ADL’s and socialactivities.5
It has a prevalence rate ranged from 20–4,100cases/million.An epidemiological study showed theprevalence rate of the nine cases per 100,000inhabitants in Rochester, USA.1 In 70-90% of thecases, the onset of symptoms occurs around thethird or fourth decade of life. Women are 1.5-1.9times more affected than men. The pathophysiologystill remains unclear, a recent review by Berardelliet al. suggests that dystonia may result fromfunctional disturbance of the basal ganglia, possiblyinvolving striatal control of the globus pallidus andconsequently thalamic control of cortical motorplanning and execution.6
Pain is one of the most common and disablingcomplaint. Study suggest the prevalence of painranging from 65 to 75%.7,8 Pain is often experiencedin head, neck and down the ipsilateral arm on theside to which the head is rotated. 9 Thesternocleidomastoid and trapezius muscles arefrequently involved.10 Chronic pain, emotional andphysical limitations and social exclusions arecommon symptoms.11 Symptoms of CD usually getworse over the period of 3-5 years.12 Common
factor leading to worsening are physical activities,fatigue and emotional stress. It is often defined as“spasmodic torticollis” and it is not only linked withperipheral or central nervous system alterations, butcan also be due to bone, joint, or muscle pathology.Early in the 1900s, physicians realized that thisbizarre condition was linked to brain disease.13
Abnormalities of cortical and basal ganglia functionshave been described in functional imaging andneurophysiology studies of patients with dystonia.6
CD can be considered an important healthproblem with a devastating impact on all level offunctioning like working capacity and sleepingquality. Due to awkward postures dystonia oftengives sufferers a disfigured appearance which isthen associated with embarrassment and can leadto isolation and social avoidance.14 High prevalenceof depression and anxiety disorder have also beendemonstrated in patients with CD.15
Psychiatric Illness and DystoniaIn addition to more visually apparent and well
defined motor symptoms, there is emerging evidencefor the presence of non-motor symptoms likealteration in mood, cognition, sleep, autonomicfunction in CD.16, 17 Subjects with dystonia also havehigher rates of depression, anxiety, social phobiasand emotional processing deficits and have aprofound effect on quality of life. Psychiatric distur-bances often precede onset of motor symptoms indystonic patients suggesting that the pathophysiologyof dystonia itself contributes to the genesis ofpsychiatric disturbances.18 Scheidt et. al. reportedthat cervical dystonia patients were more likely tohave psychopathology if symptoms were triggered

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society380
by a stressful life event. Self-esteem, body concept,and QoL have also contributed to the variance ofdepression.19 Functional imaging shows disorderedstriatofrontal circuits among the CD patients whichregulates the mood and behavior.20 Dysfunctionalmood is an important predictor of patients QoL.Along with QoL, self-esteem and body concept alsocontribute to variance of depression.19 Neuropsy-chological cognition testing shows statisticallysignificant executive deficits including verballearning, set shifting deficits and performance of dualtask.21
A prevalence of 71% of social phobia wasfound in 116 patients with spasmodic torticollis byusing the Social Phobia and Social InteractionAnxiety scales.22 Using the Pittsburgh Sleep QualityIndex, it has been reported that specific polysomno-graphic abnormalities like sleep initiation, mainte-nance and reduced REM sleep are reported inpatients with CD.23 Diagnostic prevalence ofpsychiatric illness is 91.4% in cervical dystoniapopulation as compared to 35% in the generalpopulation. The lifetime risk for patients with CDmeeting diagnostic criteria for depression rangesfrom 15%11 to 53.4%.24 The rates of anxietydisorders are also increased ranging from 26.4%7
to an 83.3%12 lifetime risk. 19.7% of patients withfocal dystonia meet DSM-IV criteria for OCD.25
InterventionsPrior to the current era where dystonia was
understood as a physical illness, approaches wereused to alleviate motor symptomatology. Currentlya more holistic approach is used for the treatmentand are more symptom based, time-limited, and haveestablished efficacy in treating mood and anxietydisorders.26
Physiotherapy ManagementThe overarching goal of the Physiotherapy is
to improve quality of life by reducing neck pain,improving awareness of postural orientation,increasing muscle strength, and reducing movementenergy.
1. Electrotherapya) Functional electrical stimulation (FES) on
antagonists’ muscles with frequency 50 Hz;1:3 on-off ratio, pulse 200µs, is applied as
follows:• Torticollis: the ipsilateral SCM, contralateral
splenius and trapezius were stimulated• Laterocollis: the contralateral trapezius,
SCM and splenius were stimulated• Retrocollis: bilateral SCM• Anterocollis: trapezius and splenius were
stimulated (physical therapy pro. Forcervtort) (R)
• Each FES treatment session lasts for 30minutes27
b) Foley-Nolan et al has found significantdecrease in pain in cervical dystonia afterwhiplash injury with the help of TENS.28
c) A 6 week programme of manual therapyand TENS shows significant decrease ofrotational deviation of the head andimproved fine motor hand functions in CDpatients.29
2. EMG biofeedback trainingEMG-biofeedback is a self-control training of
muscle activity, based on a constant feedbackof EMG signal registered in a certain muscle, withthe goal of modifying it. Korein et al demonstratedthe use of integrated EMG equipment in CDpatients.30 Patients were trained in volitional controlof spasmodic activity. Both auditory and visualfeedback were used once patient had learned tocontrol the activity of their spasmodic neck musclesmore complex type of motor exercises wereproposed with ongoing feedback. Studies haveshowed that EMG biofeedback is a widely usedtechnique to train patients with unwanted musclecontraction.31
3. Relaxation trainingA major aspect of CD is deficient muscle
relaxation leading to a fixed dystonic posture andlimited range of motion. Impaired muscle relaxationmay be caused by increased activity of agonist andantagonist muscles (co-contraction) and reducedvoluntary and sequential movements. Followingmeasures can be used:
meditation visualization relaxation breathing soft tissue mobilisationSpencer et al. has seen significant increasein

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 381
cervical ROM, improved head position, decreasedmuscle tension in SCM by using Relaxation training,strengthening the antagonists muscles and correctionof the head position with mirror with 7 supervisedsessions for 20 weeks of treatment.32 Zetterberg etal in his 4 weeks physiotherapy programme ofrelaxation conjunct with balance and coordinationtraining and body perception has shown decreasepain and disability and improved quality of life inCD patients.33
4. Kinesiotherapy exercisesa. Active exercises to enhance muscular
strength and posture:Active exercises involve conditioning,strengthening, flexibility and functionaltraining. Boyce et al study performedindividualized exercise program of activeexercises to increase muscle strength ofantagonist muscles and induce normal headposition. Patients were able to perform anactive exercise program and has shownbetter score on TWSTR and decreaseddepression.34
b. Active and passive stretching exercises;streching elongates the dystonic musclesand helps to relax it due to golgi tendonreflex.35
c. Passive mobilization of neck; This techniquecreates stress relaxation in the collagenfiber of the cervical facet joints thus helpsto increase ROM.35
Tassorelli et al reported significant improvementin activities of daily living and subjective pain ofcervical dystonia in subjects receiving kinesio-therapy.36
5. Myofascial ReleaseMyofascial Release is a safe and very effective
hands-on technique that involves applying gentlesustained pressure into the Myofascial connectivetissue restrictions to eliminate pain and restoremotion. This essential “time element” has to do withthe viscous flow and the piezoelectric phenomenon:a low load (gentle pressure) applied slowly will allowa viscoelastic medium (fascia) to elongate. Treatmentfor cervical dystonia is focused on release of myo-fascial bands with restoration of range of motion.37
Bienfait demonstrated 20 minutes of passive
myofascial elongation maneuvers on targetedmuscles sternocleidomastoid, scalene complex,levator scapulae, and upper trapezius.38
6. Postural re-education techniquesExercises carried out following Souchard’s
principles of “global postural reeducation” aimed atimproving postural control while maintaining correcthead-trunk alignment.39
7. Vestibular stimulationVestibular stimulation is the input that your body
receives when you experience movement or gravity.It can be acoustic or galvanic. It has been showedthat vestibular acoustic stimulation reduced neckmuscle activity between 16% and 44% andgalvanic stimulation reduced head acceleration by22.5% in cervical dystonia. Vestibular stimula-tion can reduce neck muscle activity in cervicaldystonia and give symptomatic relief.40
8. Motor Learning ProgramIt is designed to help patients recover a positive
body image. A 20 minute of exercise sessionconsisting of repeated movements in the oppositedirection to the dystonic pattern are performed. Oncethey are able to correctly perform, in the next PTsession they would compatibly with their complianceand learning ability and thus begin to learn a newmore difficult exercise.41 Mirror is used as a tool inmirror imaging therapeutic approach in CD for thecorrection of head posture which is tilted to 20°.
Psychiatric Management1. Somatic treatment
It includes drugs, electroconvulsive therapy, andother therapies that stimulate the brain (such astranscranial magnetic stimulation and vagus nervestimulation).
Drug therapya. Antidepressant drugs:
• Selective serotonin reuptake inhibitors(SSRIs), such as fluoxetine, sertraline
• Serotonin-norepinephrine reuptakeinhibitors (SNRIs), such as venlafaxine,duloxetine
• Norepinephrine-dopamine reuptakeinhibitors, such as bupropion

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society382
• Tricyclic antidepressants are seldomused if people have chronic paindisorder that interferes with theirADL’s.
b. New antipsychotic drugs such as risperi-done, olanzapine, quetiapine, ziprasidonearenow commonly used as initial treatment.
c. Mood stabilizers, such as lithium,carbamazepine, valproate are used to treatbipolar disorder.
Electroconvulsive therapyWith electroconvulsive therapy, electrodes areplaced on the head, and while the person is underanesthesia, a series of electrical shocks aredelivered to the brain to induce a brief seizure.This therapy has consistently been shown to bethe most effective treatment for severe depre-ssion. Many people treated with electro-convulsive therapy experience temporarymemory loss. However, contrary to its portrayalin the media, electroconvulsive therapy is safeand rarely causes any other complications. Themodern use of anesthetics and muscle relaxantshas greatly reduced any risk.
Other brain stimulation therapiesa. Repetitive transcranial magnetic stimulationb. Vagus nerve stimulation, involves activation
of brain directly with magnets or implantsthat stimulate the vagus nerve. The stimula-ted cells are thought to release chemicalmessengers (neurotransmitters), which helpregulate mood and may thus relieve symp-toms of depression. These procedures aretypically used for people who do not respondto drugs or psychotherapy.
2. Psychotherapy Psychotherapy is appropriate and effective in awide range of conditions. such as employmentdifficulties, bereavement, or chronic illness inthe family. It comprises of following therapies:• Cognitive Behavioral therapy (CBT):
Cognitive therapy helps people identifydistortions in thinking and understanding.Behavioral therapy involves a number ofinterventions that are designed to help theperson unlearn maladaptive behaviors.CBThas been successfully used to treat
psychiatric conditions like mood, psychosis,anxiety, personality and eating disorders42,43.It is associated with activation of pre frontalcortex, decreased metabolism in dorso-ventral and medial frontal cortex andincreased metabolism in the hippocampusand dorsal singulated cortex.44 Treatmentof psychiatric symptoms with CBT in move-ment disorders has shown changes in thebrain areas with underlying pathophysio-logy.45 Spencer J et al showed improvementin behavioral and physiological symptoms(depression and anxiety) continued to besignificant at the 2 year follow up withCBT.46
• Interpersonal therapy was initiallyconceived as a brief psychologic treatmentfor depression and is designed to improvethe quality of a depressed person’s relation-ships. It focuses on the following:i. Unresolved griefii. Conflicts that arise when people have
to fill roles that differ from theirexpectations (such as when a womanenters a relationship expecting to be astay-at-home mother and finds that shemust also be the major provider for thefamily)
iii. Transitions in social roles (such as goingfrom being an active worker to beingretired)
iv. Difficulty communicating with othersThe therapist teaches the person to improve
aspects of interpersonal relationships, such asovercoming social isolation and responding in a lesshabitual way to others.
• Psychoanalysis and psychodynamics: Itwas developed by is Sigmund Freud. Itfocuson understanding how past patternsof relationships repeat themselves in thepresent. The relationship between theperson and the therapist is a key part ofthis focus. An understanding of how the pastaffects the present helps the person developnew and more adaptive ways of functioningin relationships and in work settings whilepsychodynamics, emphasizes the identifi-cation of unconscious patterns in currentthoughts, feelings, and behaviors

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 383
• Supportive psychotherapy, which is mostcommonly used, relies on the empatheticand supportive relationship between theperson and the therapist. It encouragesexpression of feelings, and the therapistprovides help with problem solving. Problem-focused psychotherapy, a form of suppor-tive therapy, may be used successfully byprimary care doctors.
Other Interventions1. Neurofeedback: It is an electroencepha-
lography-based biofeedback used foroptimization of physical and mental training.N. Pandria et al has used neurofeedbackintervention for cervical dystonia and foundsuccessful results in treating anxiety,depression, epilepsy and ADHD.47
2. Deep brain stimulation (DBS): DBS ofinternus globuspallidus in dystonic patientsdeserves special attention for its effect onmood.Studies suggests that DBS helps inimprovement in non-motor manifestation ofdystonia like depression, worsened moodand suicide.48
ConclusionThe presence of non-motor manifestations in
CD such as fatigue, anxiety and pain support theuse of an integrated approach to treat chronic painand functional movement disorder.49 Understandingof dystonia as motor disorder with abnormal plasticitysuggests the possibility of retraining the dystonicbrain to a normal automatic movement using mind-fulness, motor imagery and visualization.50 Multi-modal physiotherapy programme consisting ofmyofascial release, active ROM and stretchingexercise and relaxation techniques is incooperatedalong with psychotherapeutic intervention for thetreatment of cervical dystonia.
References1. Nutt JG, Muenter MD, Aronson A, Kurland LT,
Melton LJ 3rd. Epidemiology of focal andgeneralized dystonia in Rochester, Minnesota.Mov Disord 1988; 3 : 188-194.
2. Fahn S, Marsden CD, Calne DB. Classificationand investigation of dystonia. In: MovementDisorders 2. London; Butterworths, 1987.
3. Tarsy D, Simon DK. Dystonia. N Eng JMed 2006; 355 : 818–829.
4. Bogey RA, Elovic EP, Bryant PR, Géis CC,Moroz A, O’Neill BJ. Rehabilitation ofmovement disorders. Arch Phys Med Rehabil2004; 85(Suppl 1) : S41–S45.
5. Ramdharry G. Case report: physiotherapy cutsthe dose of botulinum toxin. Physiother ResInt 2006; 11 : 117–122.
6. Berardelli A, Rothwell JC, Hallett M, et al. Thepathophysiology of primary dystonia. Brain1998; 121(Pt 7) : 1195–1212.
7. Jankovic J, Leder S, Warner D, Schwartz K.Cervical dystonia: clinical findings andassociated movement disorders. Neurology.1991; 41(7) : 1088–1091.
8. Lowenstein DH, Aminoff MJ. The clinicalcourse of spasmodic torticollis. Neurology 1988;38(4) : 530–532.
9. Kutvonen O, Dastidar P, Nurmikko T. Pain inspasmodic torticollis. Pain 1997; 69(3) : 279–286.
10. Duane DD. Spasmodic torticollis. In: JankovicJ, Tolosa E, editors. Advances in Neurology.New York: Raven Press 1988; 135–150.
11. Camargo CHF, Teive HAG, Becker N, et al.Cervical dystonia: clinical and therapeuticfeatures in 85 patients. Arquivos deNeuropsiquiatria 2008; 66 : 15-21.
12. Dauer WT, Burke RE, Greene P, Fahn S.Current concepts on the clinical features,aetiology and management of idiopathic cervicaldystonia. Brain 1998; 121 : 547- 560.
13. Oppenheim H. Uber eineeigener tigeKampfrankheit des kindlichen undjugenlichenAletrs (Dysbasia LordoticaProgressiva, Dystonia musculorum deformans).Neurol Zentbl 1911; 30 : 1090-1107.
14. Jahanshahi M, Marsden CD. Depression intorticollis: a controlled study. Psychol Med 1988;18 : 925–933.
15. Fabbrini G, Berardelli I, Moretti G, et al. Psychia-tric disorders in adult-onset focal dystonia: acase-control study. Mov Disord 2010; 25 : 459–465.
16. Miller KM, Okun MS, Fernandez HF, et al.Depression symptoms in movement disorders:Comparing Parkinson’s disease, dystonia, and

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society384
essential tremor. Mov Disord 2007; 22(5) : 666–672.
17. Soeder A, Kluger BM, Okun MS, et al. Moodand energy determinants of quality of life indystonia. J Neurol 2009; 256(6) : 996–1001.
18. Jahanshahi M. Behavioural and psychiatricmanifestations in Dystonia. In: Anderson K,Weiner W, Lang A, editors. BehaviouralNeurology of Movement Disorders. 2.Lippincott: Williams & Wilkins 2005; 291–319.
19. Scheidt CE, Heinen F, Nickel T et al. Spasmodictorticollis – a multicentre study on behaviouralaspects IV: psychopathology. Behav Neurol1996; 9(97–103) : 97.
20. Carbon M, Ghilardi MF, Argyelan M, et al.Increased cerebellar activation during sequencelearning in DYT1 carriers: an equiperformancestudy. Brain 2008; 131(Pt 1) : 146–154.
21. Lewis L, Butler A, Jahanshahi M. Depressionin focal, segmental and generalized dystonia. JNeurol 2008; 255(11) : 1750–1755.
22. Gundel H, Wolf A, Xidara V, et al. Social phobiain spasmodic torticollis. J Neurol NeurosurgPsychiatry 2001; 71(4) : 499–504.
23. Sforza E, Montagna P, Defazio G, Lugaresi E.Sleep and cranial dystonia. ElectroencephalogrClin Neurophysiol 1991; 79(3) : 166–169.
24. Fabbrini G, Berardelli I, Moretti G, et al.Psychiatric disorders in adult onset focaldystonia: A case control study. Mov Disord2010; 25 : 459-465.
25. Cavallaro R, Galardi G, Cavallini MC, et al.Obsessive compulsive disorder among idiopathicfocal dystonia patients: an epidemiological andfamily study. Biol Psychiatry 2002; 52(4) : 356–361.
26. Zurowski M, McDonald WM, Fox S, Marsh L.Psychiatric comorbidities in dystonia: emergingconcepts. Mov Dis 2013; 28(7) : 914–920.
27. Queiroz MA, Chien HF, Sekeff-Sallem FA,Barbosa ER. Physical therapy program forcervical dystonia: a study of 20 cases. FunctNeurol 2012; 27(3) : 187–192.
28. Foley-Nolan D, Kinirons M, Coughlan RJ,O’Connor P. Post whiplash dystonia wellcontrolled by Transcutaneous Electrical NervousStimulation (TENS): case report. J Trauma1990; 30 : 909-910.
29. El-bahrawy MN, El-tamawy MS, Shalaby NM,
Abdel-alim AM. Cervical Dystonia: abnormalhead posture and its relation to hand function.Egypt J Neurol Psychiatry Neurosurg 2009; 46: 203–208.
30. Korein J, Brudny J, Grynbaum B, Sachs-FrankelG, Weisinger M, Levidow L. Sensory feedbacktherapy of spasmodic torticollis: results intreatment of 55 patients. In: Dystonia. Advancesin Neurology. Vol. 14. New York; Raven Press1976.
31. Health and Public Policy Committee, AmericanCollege of Physicians. Biofeedback for neuro-muscular disorders. Ann Intern Med 1985; 102: 854-858.
32. John Spencer, Goetsch Virginia L, BrugnoliRobert J, Herman S. Behavior therapy forspasmodic torticollis: a case study suggesting acausal role for anxiety. J Behav Ther ExpPsychiatry 1991; 22 : 305–311.
33. Zetterberg L, Halvorsen K, Fa¨rnstrand C, etal. Physiotherapy in cervical dystonia: sixexperimental single-case studies. PhysiotherTheory Pract 2008; 24 : 275–290.
34. Boyce MJ, Canning CG, Mahant N, et al. Activeexercise for individuals with cervical dystonia:a pilot randomized controlled trial. Clin Rehabil2013; 27 : 226–235.
35. Fung YC. Biomechanics. Mechanical propertiesof living tissues. New York: Springer Verlag1993.
36. Tassorelli C, Mancini F, Balloni L, et al.Botulinum toxin and neuromotor rehabilitation:an integrated approach to idiopathic cervicaldystonia. Mov Disord 2006; 21 : 2240–2243.
37. Joke De Pauw et al. The effectiveness ofPhysiotherapy for Cervical Dystonia: A systemicliterature review. J Neurol, 2014; 415(13) : 7220-8.
38. Bienfait M. Il trattamentodellefasce “LesPompages”. Milan; Quaderni AITR 1987.
39. Souchard PE. Le champ clos. Bases de laméthode de Rééducation Posturale Globale.2ème edition. Saint-Mont; Le Pousoe Publ 1993.
40. Rosengren SM, Colebatch JG. Cervical dystoniaresponsive to acoustic and Galvanic VestibularStimulation. Mov Dis 2006; 21(9).
41. Hauptmann B, Karni A. From primed to learn:the saturation of repetition priming and theinduction of long-term memory. Brain Res Cogn

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 385
Brain Res 2002; 13 : 313–322.42. Cuijpers P, Berking M, Andersson G, Quigley
L, Kleiboer A, Dobson KS. A meta analysis ofcognitive behavioural therapy for adultdepression, alone and in comparison with othertreatments. Can J Psychiatry 2013; 58 : 376–385.
43. Hay P. A systematic review of evidence forpsychological treatments in eating disorders:2005-2012. Int J Eat Disord 2013; 46 : 462–469.
44. Goldapple K, Segal Z, Garson C, et al.Modulation of cortical-limbic pathways in majordepression: treatment-specific effects ofcognitive behavior therapy. Arch GenPsychiatry 2004; 61 : 34–41.
45. Etkin A, Pittenger C, Polan HJ, KandelER. Toward a neurobiology of psychotherapy:basic science and clinical applications. JNeuropsychiatry Clin Neurosci 2005; 17 : 145–158.
46. Spencer J, Goetsch VL, Brugnoli RJ, HermanS. Behavior therapy for spasmodic torticollis: acase study suggesting a causal role for anxiety. JBehav Ther Exp Psychiatry 1991; 22 : 305–311.
47. Pandria N, Spachos D, Bamidis PD. Evaluationof neurofeedback on ADHD using mobile healthtechnologies, IFMBE Proc 2015; 57 : 1292-1296.
48. Dressler D, Altenmueller E, Bhidayasiri R, etal. Strategies for treatment of dystonia. J NeuralTransm (Vienna) 2016; 123 : 251–8.
49. Zetterberg L, Lindmark B, Soderland G, etal. Self-perceived non-motor aspects of cervicaldystonia and their association with disability. JRehabil Med 2012; 44(11) : 950–4.
50. Pierre Burbaud (2012). Dystonia Pathophysio-logy: A Critical Review, Dystonia – The ManyFacets, Prof. Raymond Rosales (Ed.), ISBN:978-953-51-0329-5.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society386
Postpartum Depression –A Psychophysiotherapeutic Approach
Jaswinder Kaur,1 Mansi Gupta,1 Megha Masaun,1 M.S. Bhatia2
Department of Physiotherapy,1Dr. R.M.L. Hospital & ABVIMS, New DelhiDepartment of Psychiatry,2 UCMS & GTB Hospital, Delhi
Contact: Jaswinder Kaur, [email protected]
Psychophysiotherapy
Postpartum Depression (PPD) is a major healthissue affecting up to 13% - 15 % of all new mothersthroughout the world, with most cases beginning inthe first 3 months of the postnatal period.1,2 The WorldHealth Organization (WHO) describes the postnatalperiod as the most critical and yet the most neglectedphase in the lives of mothers and babies.3 Thepostpartum period begins an hour following the birthof the fetus and expulsion of the placenta andreflects the approximate time required for uterineinvolution and return of most maternal body systemsto a non-pregnant state. Post-partum period isdivided into the early postpartum period, the firstthree weeks after childbirth, and the late postpartumperiod, four to six weeks after childbirth.4
Giving birth involves many changes in awoman’s physical, emotional and social health.Major changes of both hormonal and social originoccur with pregnancy and continue into the postnatalperiod. Increased levels of sex hormones causelaxity of ligaments and muscles to prepare awoman’s body for the growing baby and birthprocess which makes women prone to injury andvarious kinds of pains.4 Despite the normality ofchildbirth, complications may arise that will havedetrimental effects on the postpartum woman.These include postpartum hemorrhage, thrombo-phlebitis, infections including mastitis, endometritisand urinary tract infections, wound infections,endocrine disorders as postpartum thyroditis, andpsychiatric disorders such as postpartum blues,postpartum depression (PPD), and postpartumpsychosis.2
Depression in the postpartum period causesadverse effects, both physiological and behavioralto mothers and can have a substantial impact on the
child and family as a whole.5 Postpartum Depressionis poorly understood in terms of pathophysiology.6
Although its duration varies among mothers, it isthought to be determined by sociocultural factors,such as self-esteem of the mother, the childbirthexperience, relationship with partner, the availabilityof support from friends and family and localservices.1 Decisions regarding career as well assleep deprivation, perception of herself as a newmother affects a woman’s self-esteem whichinfluences her parenting ability.4 Risk factors forpostpartum depression include lower socioeconomicstatus, multiparty, disappointment with the sex ofthe child, female sex of the child, congenital malfor-mations of the child, antenatal depression, lack ofsocial support, marital status, child-care stress,adolescent pregnancy, poor relationship satisfaction,infant temperament and low self-esteem.7
Postpartum Depression (PPD) can be linkedto mental symptoms like sadness, irritability, anxietyor worrying and crying more than usual for noreason, feeling of worthlessness, depression,exhaustion, insomnia or over sleeping, inability tocope up with her situation along with a sense offutility and hopelessness, loss of interest in activitiesthat are usually enjoyable, loss of libido,8 physicalaches and pains including frequent headaches,stomach problems, and muscle pain, eating disorders,withdrawing from friends and family, difficultybonding with the baby, persistently doubting herability to care for her baby, thoughts of self harmand/or harming the baby etc. Frequently exacerbatingthese symptoms are low self-esteem, lack ofconfidence, and unrealist ic expectations ofmotherhood. Women who have PPD are twice aslikely to experience subsequent episodes of

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 387
depression in later life.9 PPD can cause impairedmaternal-infant interactions and negative perceptionsof infant behavior.10 Marital difficulties are notuncommon and the partner may also becomedepressed.11 Suicide is a rare but devastatingconsequence of PPD.
PathophysiologyPostnatal depression is thought to evolve from
neuroendocrine changes, such as pregnancy stress,and personality predisposition, as well as acombination of many other factors.12 Stress andprevious adverse life events are risk factors fordepression. Further, neuroendocrine disruptions areassociated with Post-Partum Depression. Thehypothalamic-pituitary-adrenal (HPA) axis, whichmediates the body’s neuroendocrine response tostress, is tightly controlled by GABAergic signalingand there is evidence that GABAergic dysfunctioncontributes to the impact of stress on depression.GABAergic signaling plays a critical role in theneurobiological effects of stress, not only by tightlycontrolling the activity of the HPA axis, but alsomediating stress effects in stress-related brainregions. Deficits in neuroactive steroids andneurosteroids, some of which are positive allostericmodulators of GABA, have also been implicated inPPD, further supporting a role for GABAergicsignaling in depression. Alterations in neurosteroidlevels and GABAergic signaling are implicated aspotential contributing factors to neuroendocrinedysfunction and vulnerability to PPD.13
TreatmentDepression after childbirth is particularly
problematic because of the social role adjustmentsrequired of women during this time. Women areexpected to provide immediate and constant carefor their infants. Women also face challenges in theirrelationships with spouses or partners and often findthat they must redefine their relationships with theirfamily members and friends. Finally, womenfrequently need to make adjustments in their workroles to accommodate the care required by theirinfants. Effective treatment of postpartum depressionis needed to prevent these problems.
Antidepressant medications, cognitivebehavioral therapy, and interpersonal psychotherapy(IPT) have been validated as effective treatments
for major depression. Concerns about the possibleeffects of antidepressant medications on thebreastfed infant have often led to the exclusion ofpregnant and breastfeeding postpartum women fromdepression treatment trials. American Academy ofPediatrics classifies most antidepressants as drugswhose effect on nursing infants is unknown but maybe of concern. Given these considerations, it isimportant that nonpharmacologic interventionsshould be preferred with postpartum women.14
Research has shown several types of psycho-therapy to be effective specific to the treatment ofpostpartum depression: Individual interpersonalpsychotherapy, Cognitive Behavioral Therapy andgroup or family therapy.15 Interpersonal Psycho-therapy is a time-limited, dynamically informedpsychotherapy that aims to alleviate patients’symptoms and improve their interpersonalfunctioning. Interpersonal psychotherapy for PPDis based on the premise that interpersonal distressis connected to the symptoms of depression. Thus,the threefold targets of treatment are biopsycho-social: psychiatric symptoms, Interpersonal ProblemAreas (i.e., the conflicts, transitions and lossexperiences in the patient’s relationships) and socialsupport.16 Michael suggested that IPT is anefficacious treatment for postpartum depression. Itreduces depressive symptoms and improve socialadjustments representing an alternative topharmacotherapy, particularly for women who arebreastfeeding.14
Cognitive Behavioral Therapy (CBT) is a shortterm, goal oriented psychotherapy treatment thattakes a hands on, practical approach to problemsolving. Huang concluded that cognitive behavioraltherapy is sufficient to relieve the psychologicalsymptoms of postpartum depression and effectivelyimprove the quality of life in new mothers, resultingin a reduced prevalence of postnatal depression.17
Family therapy where members of the familyhelp the mother to gain confidence and improve herself-esteem to tackle with the situation by strategiesfor making changes in her life. Other strategies likestress management, learning practices like deepbreathing, meditation or staying present in themoment along with coping strategies like activeproblem solving can also be beneficial for themother.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society388
Physiotherapy TreatmentA tailored exercise intervention can effectively
alleviate postnatal depressive symptoms, benefittingwomen both physically and psychologically. Socialsupport experienced by participants in relation tothe exercise intervention has also shown to have apositive impact on women.18 Physical activity has asignificant impact on both the physical and mentalstate of pregnant women.19 The American Collegeof Obstetricians and Gynecologists recommends aminimum of 150 min of moderate physical activitywithin a week for pregnant women and afterchildbirth.20 Exercise during pregnancy minimizesthe risk of postpartum depression,21 as well asreduces the symptoms of depression.22 Benefits ofExercise in postpartum period23 include improvementin blood circulation, Strengthening of the abdominaland spine muscles, Stimulation of lactation, Accelera-tion the constriction of the uterus, preventionurogynecological dysfunction and Improvement ofmental and physical condition of mothers. Regularphysical activities also eliminate the risk of developingdepression during pregnancy and is a safe form ofpreventative treatment.
Mechanism of action of exercisesThe positive influence of regular physical
activities on eliminating depressive disorders wasexplained using several mechanisms.24 Exercisesincrease the concentration of neurotransmitters suchas 5HT, dopamine, and noradrenaline.25 In addition,physical activity increases the secretion of BDNF(neurotic factor produced in the brain)26theconcentration of which is low in people withdepression.27The BDNF factor plays a veryimportant role in the human body because it isresponsible for neuroprotection, neurogenesis, andsynaptic plasticity.28 Exercise also stimulates theproduction of GH (growth hormone) and IGF-1(insulin-like growth hormone). GH and IGF-1 areresponsible for the regulation of sleep, cognitivefunction, and mood.29
Physical therapy program aims to address painand the physical changes the body goes through,prescribe safe and specific exercise, teach properbody mechanics and posture care etc. Physiotherapycan be given in form of electrotherapy for lowerpelvic pain, perineal pain, musculoskeletal discomfortand incontinence, Manual therapy for musculo-
skeletal dysfunction, pelvic floor exercises for stressincontinence and to alleviate lower pelvic pain,Abdominal exercises to improve muscle tone,educating about breast feeding posture, advice withregard to everyday functional activities such as babybathing, lifting or carrying etc., posture correctionand ergonomic advice, relaxation exercises to reducetension and maternal fatigue and psychologicalcounselling.
Relaxation exercises including Deep Breathingexercises: Relaxation techniques are often employedas one element of a wider stress managementprogram and can decrease muscle tension, lowerthe blood pressure and slow heart and breath rates.30
Progressive Muscle Relaxation (PMR) therapyinvolves sequential tensing and relaxation of majorskeletal muscle groups and aims to reduce feelingsof tension, to lower perceived stress, and to inducerelaxation. It is purported to decrease the arousalof the autonomic and central nervous system and toincrease parasympathetic activity.31
ROM exercises are indicated for maintainingjoint range of motion and for maintaining the muscleflexibility and to maintain the length tensionrelationship of the muscles.
Strengthening and toning exercises for laxabdominal muscles: Core strengthening forabdominals and back extensors help prevent lowerback injuries, prevent abdominal organs fromdropping forward and help in maintaining properposture thereby curing and preventing variousmechanical pains.
Aerobic exercise has a range of benefits includ-ing reduction in severity of depressive symptoms.Asystematic review by Rethorst et al reported thataerobic exercise at a dose of at least 30 minutes ofmoderate intensity physical activity on most,preferably all, days of the week is an effectivemonotherapy for symptoms of depression.32
Kegels exercises are beneficial as strong pelvicfloor muscles decrease the chances of urinaryincontinence and uterine prolapse which are thecomplications of delivery and major causes ofpostpartum depression. It also helps in preventingweakness of pelvic floor muscles, maintain muscletone and improve pelvic control. Pelvic floor muscleexercises, also called as Kegels exercises includetightening levator ani muscles of pelvic floor, holdingthe contraction for a while and relaxing, repeating

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 389
the same at least 100 to 200 times a day (10 – 15repetitions every hourly).
Berger et al concluded that a single session ofexercise can result in both an increase in positivemood states (e.g., feeling positive, more energetic,happy and more refreshed) and a decrease innegative moodstates (e.g., tension, anxiety, confu-sion).33
ConclusionAwareness program regarding postpartum
depression can be conducted. Healthcare providersmust integrate depression screening into antenatalassessment throughout pregnancy and through thefirst 3 months postpartum or later. Physical therapyshould be incorporated in antenatal and postnatalperiod to address physical and mental changes ofthe body and to provide subsequent preventive andtherapeutic management for PostpartumDepression.
References1. Norman E, Sherburn M, Osborne RH, Galea
MP. An Exercise and Education ProgramImproves Well-Being of New Mothers: ARandomized Controlled Trial. Phys Ther 2010;Mar; 90(3) : 348-55.
2. Dennis C. Psychosocial and psychological inter-ventions for prevention of Postnatal depression:a systematic review. BMJ 2005; 331 : 1–8.
3. Song J. Predictors of Postpartum FatigueBetween Early and Late Postpartum Period inParturient Women: Divided by 3/4 Weeks ofPostpartum Period, Korean J Women HealthNurs 2007; 13(4) : 299-309.
4. Milgrom J, Martin PR, Negri LM. TreatingPostnatal Depression: A PsychologicalApproach for Treating Health Care Practi-tioners. London, United Kingdom: John Wiley& Sons Ltd, 1999.
5. Amanda J Daley, Kate Jolly, Debbie J Sharp,Katrina M Turner, Ruth V Blamey, Theeffectiveness of exercise as a treatment forpostnatal depression: study protocol BMCPregnancy Childbirth 2012; 12 : 45.
6. Nemeroff CB. Understanding the pathophysio-logy of postpartum depression: implications forthe development of novel treatments.Neuron 2008; 3159(2) : 185-6.
7. Deepika Goyal, Caryl Gay, Kathryn A Lee. Howmuch does low socioeconomic status increasethe risk of prenatal and postpartum depressivesymptoms in First time mothers? Women HealthIssues 2010; 20(2) : 96-104.
8. Sidhpura DK, PimpaleS, Kumar A. Comparisonof post-natal depression among women ofUpper, middle and lower socioeconomic status.Int J Physiother Res 2018; 6(2) : 2643-47.
9. Cooper PJ, Murray L. Course and recurrenceof postnatal depression. Evidence for thespecificity of the diagnostic concept. Br JPsychiatry 1995; 166 : 191–195.
10. Murray L.The impact of postnatal depressionon infant development. J Child PsycholPsychiatry 1992, 33 : 543–561.
11. O’Hara MW. Depression and marital adjust-ment during pregnancy and after delivery. AmJ Fam Ther 1985; 4 : 49–55.
12. Rice MJ, Records K, Williams M. Postpartumdepression: Identification, treatment, andprevention in primary care. Clin Letter NursPract 2001; 5 : 1-4.
13. Maguire J. Neuroactive steroids andGABAergic involvement in the neuroendocrinedysfunction associated with major depressivedisorder and postpartum depression, Front CellNeurosci 2019; 13 : 83.
14. O’Hara MW, Stuart S, Gorman LL, Wenzel A.Efficacy of Interpersonal Psychotherapy forPostpartum Depression. Arch Gen Psychiatry.2000; 57(11) : 1039–1045.
15. Perfetti J, Clark R, Fillmore CM. PostpartumDepression: Identification, Screening andtreatment. WMJ 2004; 103 : 56-63.
16. Stuart S. Interpersonal psychotherapy forpostpartum depression. Clin PsycholPsychother 2012; 19(2) : 134–140.
17. Huang L, Zhao Y, Qiang C, Fan B. Is cognitivebehavioral therapy a better choice for womenwith postnatal depression? A systematic reviewand meta-analysis. PLoS One. 2018; 13(10) :e0205243.
18. Daley AJ, Blamey RV, Jolly K et al. A pragmaticrandomized controlled trial to evaluate theeffectiveness of a facilitated exercise interven-tion as a treatment for postnatal depression: thePAM-PeRS trial. Psychol Med 2015; 45 : 2413-25.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society390
19. Poudevinge MS, O’Connor PJ. A review ofphysical activity patterns in pregnant women andtheir relationship to psychological health. SportsMed 2006; 36 : 19–38.
20. The American College of Obstetricians andGynecologists. Physical Activity and ExercisesDuring Pregnancy and the Postpartum Period.Available online: https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Physical-Activity-and-Exercise-During-Pregnancy-and-the-Postpartum-Period? IsMobile Set = false (accessed on 24 May 2019.
21. Blum JW, Beaudoin CM, Caton-Lemos L.Physical activity patterns and maternal well-being in postpartum women. Matern ChildHealth J 2004; 8 : 163–169.
22. Carter T, Bastounis A, Guo B, Morrell CJ. Theeffectiveness of exercise-based interventions forpreventing or treating postpartum depression:A systematic review and meta-analysis. Arch.Womens Ment Health 2019; 22 : 37–53.
23. Juøíková J, Havelka R. Physical Activity inPuerperium Period. EpSBS. Available online:https://dx.doi.org/10.15405/epsbs.2019.02.37(accessed on 20/10/2019)
24. Al-Qahtani AM, Shaikh MAK, Shaikh IA.Exercise as a treatment modality for depression:A narrative review. Alex J Med. 2018; 54 : 429–435.
25. Lin TW, Kuo YM. Exercise Benefits BrainFunction: The monoamine connection. Brain Sci2013; 3 : 39–53.
26. Hung CL, Tseng JW, Chao HH, Hung TM,Wang HS. Effect of acute exercise mode onserum Brain-Derived Neurotrophic Factor(BDNF) and task switching performance. J ClinMed 2018; 7 : 301.
27. Phillips C. Brain-Derived Neurotrophic Factor,Depression, and Physical Activity: Making theneuroplastic connection. Neural Plast 2017;2017, 7260130.doi: 10.1155/2017/7260130.
28. Mattson MP, Maudsley S, Martin B. BDNF and5-HT: A dynamic duo in age-related neuronalplasticity and neurodegenerative disorders.Trends Neurosci 2004; 27 : 589–594.
29. Frystyk J. Exercise and the Growth Hormone-Insulin-Like Growth Factor Axis. Med SciSports Exerc 2010; 42 : 58–66.
30. Seaward B. Managing Stress: Principles andStrategies for Health and Well-Being. 6th ed.Sudbury, Mass.: Jones & Bartlett Publishers,2009; 512.
31. Kwekkeboom K, Wanta B and Bompus M.Individual difference variables and effects ofprogressive muscle relaxation and analgesicimagery interventions on cancer pain. J PainSymptom Manage 2008; 36(6) : 604-615.
32. Rethorst CD, Wipfli BM, Landers DM. Theantidepressive effects of exercise: a meta-analysis of randomized trials. Sports Med 2009;39 : 491–511.
33. Berger BG, Motl RW. Exercise and mood: aselective review and synthesis of researchemploying the profile of mood states. J App SportPsychol 2000; 12 : 69 –92.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 391
Historical Development of Rights and Care ofDifferently Abled Persons: Are we cruising towards
an ideal framework in India?Navya Gupta,1 Vimal Joshi2
Faculty of Law, BPSMV, Khanpur, SonepatContact: Navya Gupta, E-mail: [email protected]
View Point
IntroductionThe disabled have been experiencing wide-
ranging human rights violations worldwide and areoppressed, marginalized and stigmatized in almostall societies. The Romans and Ancient Greeks havelooked upon the disabled as a burden on the societyand hence were treated atrociously. The conceptof differently abled persons can be traced back evenin the 4th and 5th BC where in the Maurya Dynasty,Kautilya passed an edict stating ban on both verbaland behavioral abuse of persons with disability(PWD) and also recognized their right to propertyand employment. “The Panchatantra”, the ancientIndian collection of animal fables dating around 1000BC is considered to be the first book on specialeducation having collection of animal stories relatedto diplomacy and values honoured universally.1
The ancient Greeks and Romans usually killedinfants believed to be defective or were sold forentertainment. Since God’s wrath or demonicpossession was thought to be the cause, theseindividuals were treated as less than humans. Theyconstituted a section of the population, which wasconsidered burden, least served and willfullyneglected. Individuals with disability have beensocially, educationally and economically disadvan-taged. In 1980, the World Health Organization laidthe international classification of impairment,disability and handicap, which defined concepts suchas: Impairment as the loss or abnormality of physical,anatomical structure or psychological, or dysfunctionat the system or organ level that may or may not be
permanent and that may or may not result in disability.Disability refers to an individual with limitation orrestriction of an activity as the result of impairment.Handicap refers to the disadvantage to the individualresulting from an impairment or disability thatpresents a barrier to fulfilling a role or reaching agoal2. Disability is a relative term in so far asdifferent cultures define their norms of being anddoing differently. Hence, genesis of disability is highlycontextual and subjective.
Disability in Ancient EraAncient cultures presumed that demon
possession caused disability whereas some culturesthought disability was a punishment by God. Theancient Greeks and Romans felt that children withIntellectual Disability (ID) were born because thegods had been angered. Often children with severeID would be allowed to die of exposure as infantsrather than permitted to grow up. However, theRomans did provide some form of protection tochildren with intellectual disability (ID) who wereborn to the rich, by allowing people with ID propertyrights and allowing them to have guardians.3
Ayurveda has stated, learning or acquisition ofknowledge as a result of successive and complexinteraction and coordination of Indriyas (cognitiveand motor organs), Indriyartha (sense organs),Mana (psyche), Atma, and Buddhi (intellect).Primarily, the functioning of these factors is governedby Tridosha (Vata, Pitta and Kapha) and Triguna(Sattva, Raja and Tama) in a specific balance and

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society392
coordination. Any disturbance in these Tridosha andTriguna will cause disordered functioning ofIndriya, Mana and Buddhi leading to impairedlearning or Dyslexia.3 The description of variousmental illnesses in ancient Indian texts is consideredto be the oldest account. Two well-known Ayurvedicmanuscripts, the Charaka Samhita by Charaka, andthe Sushruta Samhita by Sushruta, have establishedthe roots of modern Indian medicine. The ancientIndian scripture, Atharva-Veda, states that mentalillnesses may rise from divine curses. Othertraditional medical systems such as Siddha, havealso recognized various types of mental disordersleading to various incapacities and disabilities,prevalent in southern India.4-6
Great epics such as the Ramayana and theMahabharata made several references to disorderedstates of mind and body leading to disabilities andtheir peculiar means of coping with them.7 In theIndian society there exists the custom of joint familysystem with certain values and principles. Theseniors or elders in the family were respected; theaged, sick persons or any handicapped persons allwere well taken care of in the family. Such traditionsfind ample descriptions in the Dharmashastras.8 Inthe Indian context, the epics of Ramayana andMahabharata have popular characters havingcertain disability or deformity which was associatedwith some peculiar coping style or behaviouralattributes. For example, character of Manthra, themaid servant with a hunchback in the epicRamayana was a woman having shrewd andrevengeful attitude. It was due to her interferencethat Ram was sent to exile. In Mahabharata, theKing Dhritarastra was completely blind and thenarration goes, he was solely responsible for thewar of Kurukshetra as he couldn’t perform his dutyas a King. Even the character of Shakuni inMahabharata who instigated the war also had alimping leg. Thus, any kind of deformity, ugliness ordisability was thought to be incarnation of somethingbad or evil. In the Mahabharata it was said thatblindness or any form of disability can disqualify anyheir from inheriting the throne.
The difficulties of individuals with developmentaldisabilities have been influenced by the customs andbeliefs of that era, culture or locale. In ancient Romeand Greece, infanticide was a prevalent practice.In Sparta, for example, neonates were usually
examined by the inspectors of State Council and ifthey suspected that the infant was defective, it wasthrown from a cliff to die. In the second centuryA.D. individuals with disabilities, including children,who lived in Rome were frequently sold for enter-tainment or amusement. The rise of Christianity ledto a decline in these barbaric practices; in fact, allthe dominant leaders, Jesus, Buddha, Mohammed,and Confucius, advocated human treatment for thementally retarded, developmentally disabled, orinfirmed.9
This change of attitude emphasized the impor-tance of all persons having worth and resulted in amore compassionate approach towards persons withdisability. In the fourth century, the first protectorof those considered mentally retarded was theBishop of Myra, better known as St. Nicholas whobecame the prototype for the modern Santa Claus.The Bishop of Myra showed a strong compassionfor the mentally retarded and advocated tender careto them. Further, charity towards people withdisabilities and illnesses was preached and theChurch set up orphanages for abandoned childrenin the 3rd and 4th centuries and one of the earliesthospitals was founded by St. Fabiola in Rome wayback in 399 A.D.10
Disability in Middle EraDuring the middle era the status and care of
individuals with mental retardation varied greatly.Although a lot of humane practices emerged in themiddle era (i.e., decreases in infanticide and theestablishment of foundling homes), many childrenwere still sold into slavery or were abandoned. Inthe 16th century, Christians such as Luther and JohnCalvin believed that the mentally retarded and PWDwere possessed by demonic spirits. Therefore,religious leaders of those times usually subjectedpeople with disabilities to mental and/or physical painas a way of exorcising the spirits.11
With the rise of the colonial rule in India, includ-ing the Mughal Dynasty, the rulers exemplifiedthemselves as protectors, established charity homesfor feeding and taking care of the destitute andPWD. The community along with its governanceand local elected bodies, the Panchayati system,collected sufficient data on persons with disabilitiesfor providing services, based on the philosophy ofcharity. With the rise of the colonial rule in India,

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 393
changes became evident on the type of care andmanagement received by the PWD.
Disability in Modern EraThe landmark work by Edward Seguin who
developed a comprehensive approach to the educa-tion of children with mental retardation, known asthe ‘physiological method’ was an importantbeginning.9
Assuming a direct link between the senses andcognition, his approach emphasized sensory trainingincluding smell, vision, hearing, taste and eye-handcoordination. The curriculum included basic self-careskills to vocational education with an equal emphasison coordination, imitation, perception, memory,positive reinforcement and generalization. In 1850,Seguin relocated to the United States and becamea pioneer in the education of individuals with mentalretardation. In 1876, he founded what would becomethe American Association on Mental Retardation.Many of Seguin’s techniques have been modifiedand are still in use today.11
During this period, two key developmentsoccurred in the United States; residential trainingschools were established in most states (19 statesoperated and 9 privately operated) by 1892, and thedevelopment of a new intelligence test by Binetwhich was translated in 1908 by Henry Goddard.The training schools, which were initially educationalin nature, later became custodial living centers.Disappointment with residential treatment led toformation of advocacy and support groups like theNational Association of Retarded Citizens and thePresident’s Commission on Mental Retardation in1950’s. In 1970’s the Wyatt-Stickney federal courtaction, gave a landmark class action suit in Alabamaby laying the right to treatment of disabled individualsliving in residential facilities, thus making custodialcare no longer acceptable. In consonance, theUnited States Congress passed the Education forthe Handicapped Act in 1975, now known as theIndividuals with Disabilities Education Act. This Actensured appropriate education of all children withmental retardation and developmental disabilities,from school age through 21 years of age. In 1986this law was amended to guarantee educationalservices to children with disabilities age 3 through21 and provided incentives for states to developinfant and toddler service delivery systems.12
Contemporary Changes in Legal and SocialContext of Disability in India
Changes in attitudes towards persons withmental retardation also came to consideration in citylife and many schools for persons with mentalretardation were established including an integratedschool in Mumbai.13 The Constitution of India(1950),14 Article, 41 states the ‘Right to Educationand Work’ and Article 45 on ‘Free CompulsoryEducation for All Children up to the Age of 14 years’,both Articles are inclusive of children with mentalretardation. Inclusive education (IE) is a newapproach towards educating the children withdisability and learning difficulties with that of normalones in the same setting. There is now a consensusamong Indian intellectuals and pedagogues foradopting inclusive education in mainstream schools.The term “Special Need Education” (SNE) hasreplaced the term “Special Education”, as it wasmainly understood to refer the education of all thosechildren and youth whose needs arise fromdisabilities or learning difficulties. The Statementaffirms: “those with special educational needs musthave access to regular schools which shouldaccommodate them within child centered pedagogycapable of meeting these needs”.15
The government is committed to provideeducation through mainstream schools for childrenwith disabilities in accordance with PWD Act, 1995which is now amended into The Rights of Personswith Disability Act, 201616 and all the schools in thecountry will be made disabled friendly by 2020.Enrolment and retention of all children withdisabilities in the mainstream education systemshould be ensured providing need based educationaland other support to these children in order todevelop their learning and abilities. The specialinterventions and strategies like pedagogic improve-ment and adoption of child centered practices arefocused on the children with disabilities.15
Article 15(1) enjoins on the Government not todiscriminate against any citizen of India (includingdisabled) on the ground of religion, race, caste, sexor place of birth. Article 15(2) States that no citizen(including the disabled) shall be subjected to anydisability, liability, restriction or condition on any ofthe above grounds in the matter of their access toshops, public restaurants, hotels and places of publicentertainment or in the use of wells, tanks, bathing

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society394
ghats, roads and places of public resort maintainedwholly or partly out of government funds or dedicatedto the use of the general public. No person includingthe differently abled irrespective of his belongingcan be treated as an untouchable. It would be anoffence punishable in accordance with law asprovided by Article 17 of the Constitution. Everyperson including the differently abled has his lifeand liberty guaranteed under Article 21 of theConstitution. There can be no traffic in human beings(including the disabled), and beggar and other formsof forced labour is prohibited and the same is madepunishable in accordance with law (Article 23).Article 24 prohibits employment of children (includ-ing the disabled) below the age of 14 years to workin any factory or mine or to be engaged in any otherhazardous employment. Article 25 guarantees toevery citizen (including the disabled) the right tofreedom of religion. Every differently abled person(like the non-disabled) has the freedom ofconscience to practice and propagate his religionsubject to proper order, morality and health. Everydifferently abled person can move the SupremeCourt of India to enforce his fundamental rights andthe rights to move the Supreme Court is itselfguaranteed by Article 32. The right to education isavailable to all citizens including the disabled. Article29(2) of the Constitution provides that no citizen shallbe denied admission into any educational institutionmaintained by the State or receiving aid out of Statefunds on the ground of religion, race, caste orlanguage.17
Article 41 of the Constitution of India (1950)has stated in its clause the “Right to Free andCompulsory Education for all children up to Age 14years. The National policy on Education (1986) putemphasis on mainstreaming the handicapped childrenwith general community.18 The major three Actsnamely, Rehabilitation Council of India Act, 1992,19
Persons with Disabilities (Equal opportunities,protection of rights, and full participation) Act, 199516
and National Trust for welfare of persons withAutism, Cerebral Palsy, Mental Retardation andMultiple Disabilities Act, 199920 in India have resultedin number of action plans, developments of researchprojects, service delivery system and well regulatedhuman resource development in the field ofrehabilitation passed and the policies touching thelives of the differently abled persons in India.
National Policy for Persons with Disabilities,2006
The National Policy, released in February 2006recognizes that PWD are valuable human resourcefor the country and seeks to create an environmentthat provides them equal opportunities, protectionof their rights and full participation in society. Itsaim is to ensure better coordination between variouswings of the State and Central Governments. Thefocus of the policy is on the following: Preventionof Disabilities, Rehabilitation Measures, PhysicalRehabilitation Strategies, Early Detection and Inter-vention, Counseling and Medical Rehabilitation. Inaddition to the legal framework, extensive infra-structure has been developed in India for differentlyabled persons under this Act and includes theestablishment of the following institutions: Institutefor the Physically Handicapped, New Delhi, NationalInstitute of Visually Handicapped, Dehradun,National Institute for Orthopedically Handicapped,Kolkata, National Institute for Mentally Handi-capped, Secunderabad, National Institute forHearing Handicapped, Mumbai, National Instituteof Rehabilitation Training and Research, Cuttack,National Institute for Empowerment of Persons withMultiple Disabilities, Chennai.21
The rights, type and category of PWD has beenmodified presently and some more disabilities havebeen added. On the 13th day of December, 2006The United Nations Convention on the Rights ofPWD has laid down the following principles forempowerment of PWD; (a) Non-discrimination; (b)Full and effective participation and inclusion insociety (c) Respect for natural worthiness, individualautonomy including the freedom to make one’s ownchoices, and independence of persons; (d) Respectuniqueness and acceptance of Divyangjan as a partof human diversity and humanity; (e) Equality ofopportunity; (f) Accessibility; (g) Equality betweenmen and women; (h) Respecting the evolvingcapacities of children with disabilities and respectingtheir right of preserving their identities. India signedthe said Convention on the 1st day of October, 2007and considered necessary to implement it. The Actcame into force during December 2016 and included17 chapters.
There is unique geographical area, limitedrecourses, utilization of available infrastructure,available negative attitude and social stigma pull the

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 395
CBR (Community-Based-Relation) for themainstreaming and welfare of PWD as well asreduce the burden of their family members/caregivers in India. CBR aims to encourage thecommunity to create awareness about negativeattitudes and behaviours towards PWD and theirfamilies, that the community is supportive of them,and that disability is mainstreamed across alldevelopment sectors. There is right time to worktogether and also needed strong liaisons betweenvarious stock holders those are working in the areaof disability. Collaborative approaches are alsoessential between various central / state governmentpolicy (like National rural heath mission, nationalmental health policy, district mental healthprogramme, primary health centre, district disabledrehabilitation centre, etc.), school teacher, faithhealers, NGOs, police personal, judiciary, local leader,health professional, policy makers, researchers etc.for the betterment and rehabilitation of person withdisability.22
In India, the numbers of differently abled areso large, their problems are complex, availableresources also scarce, social stigma still attachedand people attitudes so damaging. Attitudinal barriershave been engrained as part of India’s historicalresponse to disability need to be changed througheducative programs for both teachers and thegeneral population. These programs would requireresources both financial and administrative along withcollaborative commitment from key national andstate education stakeholders, and tie ups withuniversities to support research-based initiatives. Itis only legislation that can eventually bring about asubstantial change in a uniform manner in this regard.However, legislation alone cannot change the attitudeof society in a short span of time, though it canincrease accessibility of the differently abled toeducation and employment, to public buildings andshopping centres, to means of transport andcommunication. Therefore, in country like Indiamainstreaming of these people is challenging issue.For achieving this task it is necessary to changepublic attitudes, remove social stigma, providebarrier free environment and needs reformation inthe area of policy and institutional level.23
ConclusionThis historical journey reviews psychosocial
attention and legal factors which influence the originof perceptions towards differently abled. It is clearthat perception of the society towards the differentlyabled is full of neglect. But it is encouraging thatafter India got independence the national govern-ment began to pay serious attention towardsdifferently abled and took various administrative andlegislative measurers for the upliftment of thecondition of differently abled persons. However, thechallenge lies in reaching a threshold of implemen-tation to what our law theoretically envisions. Therecent legal push in the area of disability throughMental Health Care Act,24 Rights of persons withDisability and Deendayal Disabled RehabilitationScheme25 etc. have created an optimum environ-ment and if this momentum is maintained and thelaws and policies are implemented in the true letterand spirit then we will be able to achieve and createperfect environment for differently abled persons.
References1. Balasundraram P. The Journey towards inclusion
education in India. Presented at Seisa Uni.Hokkaido, Japan. Retrieved from http://www.jldd.jp/gtid/global_trend/4
2. World Health Organization. InternationalClassification of Impairments, Disabilities, andHandicaps: A manual of classification relatingto the consequences of disease. Geneva: WHO1980.
3. Harris JC. Mental disorder: Understanding itsdevelopment, causes, classification, evaluation,and treatment. NY: Oxford University Press2006; 42-98.
4. Nizamie SH. Goyal N. History of psychiatry inIndia. Ind J Psych 2010; 52(1) : S7-S12.
5. Weiss M. History of psychiatry in India. Samiksa1986; 11 : 31–45.
6. Bhugra D. Psychiatry in ancient Indian texts: Areview. Hist Psych 1992; 3 : 167–186.
7. Reynolds T. Zupanick CE. Dombeck M.Historical and contemporary perspectives onintellectual disabilities. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/36652.
8. Kane PV. History of Dharmasastra, Vol. II, PartI, Poona: Bhandarkar Oriental ResearchInstitute 1941; 297-298.
9. Scheerenberger RC. A history of mentalretardation. Baltimore, PH. Brookes Pub Co.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society396
1983. https://www.ncbi.nlm.nih.gov/books/ citedon 23.07.2019.
10. Slater C. Cantab MA. Idiots , inbleciles andintellectual impairment. Retrieved from https://langdondownmuseum.org.uk/the-history-of-learning-disability/idiots-imbeciles-and-intellectual-impairment cited on 27/7/2019.
11. Heinz EB. Mental retardation researchadvances. NY: Nova Science Publishers Inc.2007; 35-44.
12. Ainsworth P. Baker C. Understanding MentalRetardation: A resource for parents, caregiversand counselors. US: University Press ofMississippi 2004; 1-50.
13. Walker S. Issues and Trends in the Educationof the Severely Handicapped. Review ofResearch in Education, 1984. Retrieved fromhttps://www.jstor.org/stable/1167233.
14. Basu DD. Commentary on the Constitution ofIndia by Justice Subramani. Article 15-19(contd.) 9th ed. New Delhi: Lexis Nexis, 2014.
15. Kumar S, Kumar K. Inclusive Education inIndia. Elec J Incl Edu 2007; 2 : 1-15.
16. Act No. 49 of 2016.17. Singh MP. VN Shukla’s Constitution of India
(13th ed). New Delhi: Eastern Book Co. 2017.18. Ministry of Human Resource Development,
Govt. of India. Right to Education. Retrievedfrom mhrd.gov.in/rte
19. Act No. 34 of 1992.20. Act No. 44 of 1999.21. National Health Portal, India. National Policy
for Persons with Disabilities 2006. Retrievedfrom nhp.gov.in/national-policy-for persons-with-disabilities 2006; pg
22. Kumar P, Sushma, Raj A. Emergence ofcommunity based rehabilitation for person withdisability in India. Delhi Psychiatr J 2018; 21, 2: 7-12.
23. Srivastava P. Kumar P. Disability, its issues andconsquences: psychosocial and legal conse-quences in Indian scenario. Delhi Psychiatr J2015; 18(1) : 195-205.
24. Act No. 10 of 2017.25. Department of Empowerment of Persons with
Disabilities (Divyangjan), Ministry of SocialJustice and Empowerment, Government ofIndia, Deendayal Disabled RehabilitationScheme (DDRS) (2018). Retrieved from http://disabilityaffairs.gov.in/content/page/ddrs.php.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 397
World Mental Health Day (10th October, 2019)Theme: Mental Health Promotion and Suicide Prevention
Shruti SrivastavaDepartment of Psychiatry, Guru Tegh Bahadur Hospital, University College of Medical Sciences,
Dilshad Garden, New Delhi-110 095, IndiaE mail: srivastava_shruti@ hotmail.com
Invited Article
World Federation for Mental Health(WFMH) has given the theme for 10th October,2019 as of Mental Health Promotion and SuicidePrevention.1 The theme focuses on two importantaspects mental health promotion for making aperson resilient to common mental health problemsand ways for suicide prevention.
Suicide can be defined as “ the intentional actof self destruction committed by someone whoknows what he is doing and knowing probableconsequences of his actions.” One person dies ofsuicide every 40 seconds globally. Suicide is aglobal epidemic that affects all age groups, allnations. The prevalence figures as reflected by agestandardized graphs show high suicide rates inEastern European countries like Russia, includingIndia. Low middle income country, like India wheretotal Suicide Rateis 16.3, male suicide rate is 17.8,female suicide rate is 14.7per lac population. Totalsuicide per year is 220,481.2
India’s contribution to global suicide deaths(2016) increased from 25·3% in 1990 to 36·6%among women, and from 18·7% to 24·3% amongmen. Suicide Death Rates (SDR) in women was2·1 times higher in India than the global average in2016.2 Women in the age group of 15-29 years, 75years and older have higher age specificStandardized death rates, while men in the age groupof 75 years and older are affected most.3 If suchalarming rates of suicide persist , sustainabledevelopment goal of suicide death rate reductiontarget of India by the year 2030 will be zero.
In India a lot of situational factors such as job
loss, examination stress, deaths, divorce, propertydispute, and family history of suicide, substanceuse, past history of psychiatric illness, physicalillness, sexual or physical abuse contribute tosuicide. The history suggestive of depression likelow mood state, crying spells, lack of interest inpleasurable activities, declined work performance,avoiding social contacts, friends or families,preference to stay alone, reduced appetite ,sleepdisturbances are impending signs, and also,expressions in words as well as letters areimpending signs that should alert or aise alarm.Thoughts of helplessness, hopelessness, worthless-ness, changes in behavior to irritability, agitation,unprovoked violence, dejected, crying spells areoften noted with suicide notes discovered after thecalamity. Withdrawn behavior is first to be observedand we need to make our society aware of how toidentify the risk, seek timely professional help andprevent suicide.
On 10th October, 2019 , Department of Psychia-try at University College of Medical Sciences andaffiliated Guru Teg Bahadur Hospital, Delhiorganized the workshop widely attended by medicaland nursing students, faculty, neighboring residents,public and media to make people aware of thesuicide and its alarming rates, how to identify theimpending risks, how to prevent using simple meansof empathy, seeking timely psychological help,keeping away lethal items, extending one’s handas a human being , not letting the individual feellonely, giving emotional warmth and support so thatthe individual can come out of the crisis.4

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society398
Empathy is defined in simple terms by under-standing the client by giving unconditioned positiveregard , narration of client’s problems from theclient’s perspective as if one has inserted the feet
in client’s shoes. The theme as well as manual onWorld Health Organization website aims to promotepositive mental health and prevent suicide bycreating awareness, through empathy, empower-ingpeople to act and prevent suicide by giving hand toperson feeling helpless on the verge of death.5 We,all the people of India as per the theme thereforeshould focus and empower ourselves to bring abouta change and reduction in this alarming suicide rateworldwide through action by instilling hope ineveryone’s life to nurture and not to perish.Decriminalization of suicide by Government ofIndia, through new Mental Health Care Act andremoving the clause of imprisonment of one yearis going to help in reducing stigma in our countryand bring the people who feel miserable to seekhelp from mental health services for betterment oftheir lives.
References1. https://wfmh.global › world-mental-health-day-
2019.2. http://worldpopulationreview.com/countries/
suicide-rate-by-country/ last accessed on 10th
October, 2019.3. India State-Level Disease Burden Initiative
Suicide Collaborators. Gender differentials andstate variations in suicide deaths in India: theGlobal Burden of Disease Study 1990-2016. Lancet Public Health 2018; 3(10) : e478–e489. doi:10.1016/S2468-2667(18)30138-5
4. http://www.jagran.com. last accessed on 16th
October, 20195. http://www.who.int.last accessed on 10th
October, 2019.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 399
BremelanotideAparna Goyal, M.S.Bhatia
Department of Psychiatry, UCMS & GTB Hospital, Delhi 110095
Drug Review
IntroductionOne of the few entities which have been under
explored in psychiatry are sexual disorders andmore so when it relates to women. The subject ofsex in itself specially in women has beenconstructed as taboo to discuss leading tounexplored issues but is a cause of great distress.Female sexual disorders (FSD) is one such areawhich remains hidden both in nosological as wellas treatment significance. Lack of adequate andeffective treatment strategies makes it difficult forthe physician to counter the issue. Newer develop-ments help address these disorders and here we arereviewing one of the recently FDA approved drugfor female sexual interest/ arousal disorder (asdefined in DSM-5) in premenopausal women isbremelanotide (BMT) trade name Vyelesi.1
Mechanism of actionBMT is a melanocortin receptor agonist and a
novel cyclic heptapeptide analog of the endogenousneuropeptide alpha melanocyte stimulatinghormone. Exact mechanism is not clear but BMThas shown high affinity for type 4 receptor. It hasbeen reported that BMT acts on physiological andneurobiologcal components of female sexualfunction by modulating neurotransmitter pathwaysinvolved in sexual desire and arousal in women.2
Chemical structure3
BMT has a molecular formula of C50H68N14O10and weight of 1025.2 g/mol. The 2 D chemicalstructure of BMT is given in Figure 1.
Pharmacokinetics3
AbsorptionBremelanotide has a Tmax or 1.0 hour (0.5-
1.0 hours) and is 100% bioavailable. The Cmax is
72.8 ng/mL and the AUC is 276hr\*g/mL. Halflife of BMT is 2.7 hours.
Route of Elimination64.8% of a radiolabelled dose is excreted in
the urine and 22.8% of the dose is recovered in thefeces.
Volume of DistributionThe mean volume of distr ibution of
bremelanotide is 25.0 ± 5.8L. It is 21% proteinbound in serum.
ClearanceThe mean clearance of bremelanotide is 6.5 ±
1.0L/hr.
Clinical StudiesRandomised clinical trial by Clayton et al4 on
327 premenopausal women with FSD with BMTvs placebo reported significant increase in thenumber of satisfying sexual events/month with 1.25mg and 1.75 mg of BMT as compared to patientstreated with placebo. BMT 0.75 mg did not differfrom placebo. Women with a primary or solediagnosis of hypoactive sexual desire disorder
Fig-1: Chemical Structure of BMT

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society400
showed responses to BMT similar to those in thestudy population.RECONNECT study5,6
Two phased trialIn the core phase there were two identically
designed, phase 3, randomized, double blind,placebo controlled, multicenter trials with 1.75 mgsc dose of BMT for a 24 week randomized doubleblind treatment period. In the open label extensionwomen who completed the core phase were enrolledin a 52 week study if they had not experienced anyserious side effects in the core phase.RECONNECT study concluded that premenopausalwomen treatment with BMT was safe and alsoshowed improvement in hypoactive sexual desiredisorder symptoms and even sustained them infollow up during open label extension.
Responder analysis by Althof et al7 for phase2b of bremelanotide reported that for all 7 endpointsresponder rates at the 1.75 mg dose achievedstatistical significance in comparison to placebo andconcluded that it is a safe and well tolerated drug .
Dosage and mode of administration0.75, 1.25, 1.75 mg subcutaneous injections
with as desired dosing. Bremelanotide is meant tobe used as needed, 45 minutes before sexual activity.It can be used as an autoinjector though reservationsto problems in learning mode of administration hasbeen proposed.
Side effectsMost common side effects seen are nausea,
headache, flushing with no marked dosagedependence. There can also be pain at the site ofinjection, upper respiratory tract infection andpruritis.
Special precautionsThe effects of BMT on blood pressure has been
reported in many studies but has consistentlyrevealed only a small transient rise within 4 hoursof intake and return to baseline within 8 to 10 hours.Also, it has been advocated that since BMT usageis a limited, as need based, no long term adverse
cardiovascular effects are expected. Overdose withBMT has not been reported but higher doses arereported with side effects like nausea, focalhyperpigmentation and increases in blood pressure.
ConclusionFemale sexual response is a complex interplay
of neurobiological, physiological and psychosocialfactors. Bremelanotide with its capability inmodulating these pathways can prove to be a goodchoice in treating those with hypoactive sexualdisorder when compared to other availablealternatives like flibanserin, testosterone, bupropionetc.
References1. Dhillon S, Keam SJ. Bremelanotide: First
Approval. Drugs 2019; 79(14) : 1599-1606.2. Pfaus JG, Giuliano F, Gelez H. Bremelanotide
: an overview of preclinical CNS effects onfemale sexual function. J Sex Med 2007; 4(suppl 4) : 269-79.
3. Bremelanotide. Pubchem open chemistrydatabase. US national library of medicine.National centre for biotechnology information.Avlbl from: https://pubchem.ncbi.nlm.nih.gov/compound/bremelanotide.
4. Clayton AH. Althof SE, Kingsberg S, et al.Bremalonatide for sexual dysfunctions inpremenopausal women: a randomized, placebocontrolled dose finding trial. Womens Health(Lond) 2016; 12(3) : 325-337.
5. Kingsberg SA, Clayton AH, Portman D, et al.Bremalontide for the treatment of hypoactivesexual desire disorder : two randomized phase3 trials. Obstet Gynecol 2019; 134 : 899-908.
6. Simon JA, Kingsberg SA, Portman D, et al.Long term safety and efficacy for bremelanotidefor hypoactive sexual desire disorder. ObstetGynecol 2019, 134(5) : 909-917.
7. Althof S, Derogatis LR, Greenberg S, et al.Responder Analyses from a Phase 2b Dose-Ranging Study of Bremelanotide. J Sex Med2019; 16(8) : 1226-1235.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 401
Testamentary Capacity – a clinical frameworkNilesh Shah, Sagar Karia, Avinash De Sousa
Department of Psychiatry, Lokmanya Tilak Municipal Medical College, MumbaiContact:Avinash De Sousa, E-mail – [email protected]
Forensic Psychiatry
IntroductionThe number of aging populations in India is
increasing and the number of elderly in India shalltriple by 2030.1 There has also been an increase inproperty disputes and fights for their parents wealthamongst people and the number of court casesrelated to the same has also been substantiallyincreasing.2 Demographic data in India reveals agrave increase in the number of older adults(especially the very old), who have a highprevalence of dementia, cognitive impairment, andassociated behavioral and psychiatric disorders.3
There has also been an exponential rise inblended and fractured families where there aremultiple marital and extra-marital relationships,later-life partnerships, same-sex marriages andchildren including step-children, adopted childrenand thus the list of people claiming the property ofthe person is growing. Families are no longer closeand tight-knit units as they once were in the past.These relatively recent developments in our currentdemographic trends shall inevitably result incomplicated distributions of proper distributionsand transfer of wealth along with issues that mayarise in wills that are mad and the need to changethe will time and again.4
Testamentary Capacity (TC) is the legal termused to describe a complex capacity that representsthe required decisional understanding to make avalid Will.5 It is important to note that while“competency” and “capacity” are often usedinterchangeably, the term “capacity” is common toboth clinical and estate contexts. All mentalcapacities are based on two underlying principles:the understanding of relevant facts and theappreciation of the reasonably foreseeableconsequence of a decision.6
Patients in old age may be referred to
psychiatrists for a clinical opinion of testamentarycapacity which may or may not be upheld by thecourts. Yet the patient may be referred for a clinicalopinion and the psychiatrist may be called to thecourt as a witness whenever the property matterarises. The judicial opinion may include input frommore than one clinical expert, evidence from laywitnesses, as well as the influence of legalprecedent/common law, statute, and other equitableprinciples.7 TC can be assessed contemporaneously(at the time instructions are given for a Will) orjust before making a will.
Elder abuse i.e. the exploitation of an olderadult by strangers, family members, or friends isbecoming common in India and being is reported.8
The Elder Abuse law is now in place in India aswell.9 It is thus inevitable that physicians who dealextensively with the elderly, including geriatriciansand geriatric psychiatrists, will increasingly beasked to provide an opinion on these matters. Themedical profession at large and geriatric specialistsin particular must prepare to assist and help informthe court in such cases. The current paper providesa clinical framework for the evaluation of TC sothat a consistent, uniform assessment process maybe followed.
Concept of a willAccording to Section 2(h) of the Indian
Succession Act 1925, a Will is defined as follows:“A Will is a legal declaration of the intention
of the testator, with respect to his property whichhedesires to be carried into effect after his death.”10
Important postulates of the Will are as follows-• A Will is a legal declaration. It must be
signed and attested as required.• The declaration should relate to disposition
of the person making the Will.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society402
• A Will becomes enforceable only after thedeath of the testator.It has no effect duringthe lifetime of the testator.
• It is revocable and the testator can changethe Will at any time during his life-time.
Persons capable and competent to make a Will –According to Section 59 of Indian Succession
Act 1925, Any person of sound mind can make aWill and a person who has reached the age ofmajority can make a Will.
However, as per Section 60 of the Act, a fatherwhatever his age may be, may by Will may appointa guardian or guardians for his child duringminority. Also a married woman may make a Willof her property which she could alienate by her ownactduring her life-time.
The following persons cannot make a Will –• Lunatic, insane persons• Minor i.e. below 18 years of age.• Corporate bodies by their very nature are
incapable of making a Will, though theymay benefit under the Will of an individualpartner.
Other persons who can make a Will –• Persons who are deaf or dumb or blind are
not thereby, incapable in making a Will, ifthey are of sound mind
• Persons, who are ordinarily insane, maymake a Will during an interval while theyare of sound mind.
Concept of CodicilA codicil is a supplement to a Will when a
testator intends to make any minor alterations inhis Will e.gchange in the number of trustees.According to the Section 2(b) of the IndianSuccession Act 1925, codicil means an instrumentmade in relation to a Will and explaining, alteringor adding to its disposition and shall be deemed toform the part of the Will. Accordingly, a codicilhas to be executed and attested just as a Will(Section 64, Indian Succession Act 1925).
A codicil may be endorsed on the original Willitself, or it may be a separate document. Its natureis not substantive but adjective. A codicil may standeven though the Will to which it is supplementaryis revoked. However, a codicil cannot be anindependent document.When alterations areconsiderable, a fresh Will revoking the earlier Will
should be executed.
Definition of Testamentary CapacityTestamentary capacity refers to person’s full
sense and mental sanity to have confirmed andsignedthe Will after understanding what his assetscomprised and what he is doing by making a Will.Heunderstands in full mental capacity who he isnaming the assets to and how are they related tohimand what repercussions it may have later.Testamentary capacity is the legal status of beingcapable of executing a Will.
Testamentary capacity is defined in commonlaw and U.S., Canada and English jurisdictions,addresses its task-specific nature as opposed to theglobal status of the mental illness. It means thataperson suffering from mental disorder can make aWill provided he is capable of required competencyfor making a Will. In Banks v. Good fellow, acommonly cited English case, John Banks, thetestator clearly suffered from a chronic and seriousmental disorder but was deemed capable withrespect tothe execution of his Will because hisdelusions did not affect the distribution of his assets.This judgment remains the test in most commonlaw jurisdictions today.
According to Indian Succession Act 1925, aperson is said to have testamentary capacity only ifhe isin a sound disposing state of mind. It is essentialthat the testator should have sufficient capacitytocomprehend perfectly the conditions of hisproperty, his relations to the persons who were orshouldor might have been object of his be questand the scope or the bearing of the provisions ofhis Will.
Banks Versus Goodfellow Criteria forTestamentary Capacity11
• Understanding of the nature of the act (Willmaking) and its effects
• Knowledge of the nature and extent ofone’s assets.
• Knowledge of persons who have areasonable claim to be beneficiaries.
• Understanding of the impact of the distribu-tion of the assets of the estate.
• A confirmation that the testator is free ofany delusions that influence the dispositionof the assets.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 403
• Ability to express wishes clearly andconsistently in an orderly plan of disposi-tion.
Clinical Framework to Assess TestamentaryCapacity
Part A – Prior to the Clinical Interview
The Setting• The assessment may be carried out at any
quiet and comfortable place. It may be doneat a psychiatrist’s clinic, at the client’shome, in the hospital or at a rehabilitationcentre where client is admitted etc….
• It is preferable to have bare minimumnumber of people in the room and norelatives should be present in the roomunless it is necessary.
The Doctor Carrying Out the Assessment• The assessment is preferably carried out by
a qualified Psychiatrist holding a validallopathic post-graduation in psychiatry.
• If a psychiatrist is not available, then it maybe carried out by any qualified mentalhealth professional (psychologist orpsychotherapist) or even another healthprofessional (family physician or generalphysician with proper qualifications).
Documentation that is needed• It is preferable to video record theinterview
for medico-legal purposes.• The assessor may request his colleague to
video record the interview.• One may also note down the interview on
a letterhead or a hospital paper.
Assessment and Certification Fees• A psychiatrist may charge a reasonable fee
based on the time spent on the assessmentand certification.
• An additional fee for video recording maybe charged.
Language to be used• The interview should be preferably
conducted in a language preferred by theperson making a will.
• It should be conducted in a simple language
using day-to-day words and phrases andwithout much of a legal or technical jargon.
Part B – The Assessment of TestamentaryCapacity
Introduction**Assessor Good morning, I am Dr.............; I
am a psychiatrist and I am here toassess your testamentary capacity;i.e. capacity to make a will. For thispurpose I would be asking yousome questions and I request youto answer them to the best of yourknowledge and capacity. I may alsocarry out some tests to check yourcognitive abilities (memory) ifnecessary.
Assessor For maintaining the record of thisinterview for medico-legalpurposes, I would also like toinform you that the wholeinterview is being video recordedby a colleague mine. This shallserve as good documentaryevidence of the interview for bothof us in the future.
**The client must wear his glasses or hearingaids if he uses the same during the interview
Verification of Identity of the ClientAssessor May I request you to introduce
yourself ?Client I am Mr ..............; I am 76 years
old; I am staying at ........ with my.....................
Assessor I need to check your photo-identitycard (election card / PAN card /passport/Aadhar Card); would youplease show me your photo-identify card? (Verify the identityof the client).
It is essential to keep a copy of the self-attestedphoto identity card and a passport size photo of theclient in your file.
Awareness about the Intent to make a WillAssessor Do you wish to make a willClient YesAssessor Is it for the 1st time that you are

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society404
making a will or you have madeany will in the past?
Client Yes. It is the first time that I ammaking a will(If it is not the first time then thereason for changing the will mustbe asked and if additions are beingmade, the reasons for making thesame must be asked and documen-ted in the file.)
Assessor Are you making this will volun-tarily and without any unduepressure or influence?
Client Yes.
Assessment of Cognitive AbilitiesAssessor What time of the day is it now
(Morning, Afternoon or Evening)The client must answer the samecorrectly
Assessor Can you please repeat these threewords – Apple, Walk and SevenThe client must repeat all threewords correctly
Assessor Can you draw a circle, a triangleand a square? Let the client drawthese three figures on a plain paper.The client must be able to draw thesame correctly
If on preliminary examination one suspectsdementia then a detailed assessment using MiniMental Status Examination (MMSE) and/orMontreal Objective Cognitive Assessment Test(MOCA) and/or Clock Drawing Test may be carriedout.
Assessing for the physical and mental disordersAssessor Are you suffering from any
physical or mental disorder atpresent or did you have any majorphysical or mental disorder in thepast?May I have a look at your medicalrecord.The details of the client’s medicalcondition with the treatment beingtaken must be noted and a xeroxof the current prescription and casedetails for the file.
Client Yes, at present I am suffering fromhypertension and taking treatmentfor the same. I do not have anypsychiatric disorder at present andI have not suffered from any mentaldisorder in the past.
• If on preliminary examination one suspectsany psychiatric disorder then one mayobtain objective data from a close relativeabout client’s illness and carry out mentalstatus examination.
• Please make detailed notes of the mentalstatus examination with date and time foryour record.
• If there is an evidence of mental disorderthen try to find out if it in any way affectsthe individual’s capacity to make a will.Clients having mental disorders can makea will provided the mental disorder doesnot affect client’s capacity to make a will.
Awareness of the Extent of PropertyAssessor Are you aware about the extent of
your property for which you aremaking a will.
Client Yes. I have a flat at ......, a shop at......., some money in my bankaccounts and some jewellery.These facts may be confirmed bythe relatives or advocate if neededand documented with name andsignature of the person confirmingthe same
Awareness of their Legal HeirsAssessor Are you aware about the legal heirs
of your property ?Client Yes. I have a son and two daughters
who are the legal heirs of myproperty.These facts may be confirmed bythe relatives or advocate if neededand documented with name andsignature of the person confirmingthe same.
Clarity about Distribution of PropertyAssessor Are you planning to distribute your
property equally amongst yourlegal heirs ?

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 405
Client Yes.If the answer is ‘No’ then one mayhave to find out the reason for thesame; one may have to take thedetails and find out the logicalreasoning behind uneven distribu-tion. It is necessary to rule outundue pressure and influence onclient. Document all this in the file.
After the complete assessment the certificateis made out and handed over like mentioned inAppendix.
The video recording is preserved on a harddrive for future use and one copy may be handedover to the relatives if needed.
Certain terms used in the assessment of TCTestamentary capacity: It refers to person’s
full sense and mental sanity to have confirmed andsigned the Will after understanding what his assetscomprised and what he is doing by making a Will.He understands in full mental capacity who he isnaming the assets to and how are they related tohim and what repercussions it may have later.Testamentary capacity is the legal status of beingcapable of executing a Will.
Capacity : Medical determination made by adoctor indicating that an individual understandsrelevant facts and appreciates potential outcomes.
Codicil: Amendment to an existing will.Testator: Historically referred to a man who
made a will (became a gender-free term).Testatrix: Historically referred to a woman
who made a will.Holographic will: A Handwritten will.
Important Points to be noted at the time ofexaminationVoluntary act on the part of the testator
• There is no compulsion or force on thetestator to make the Will and it is his owndecision to dispose off his property.
The testator should have a sound disposing mind• The testator should not be suffering from
any mental disorder which could possiblyinterfere in his decision making.
• He should not be in a state of intoxicationdue to alcohol, drugs or disease.
• Testamentary capacity is task-specific, aperson suffering from mental illness canmake a will provided his psychopathologyis not interfering in his decision making.
• Testamentary capacity is also situation-specific. Clinician should explore thecircumstances under which the testator ismaking the Will.
The testator should know the nature of the acthe is doing
• The testator should be in full senses toappreciate the nature of the act an.
The testator should have sufficient capacity toknow the extent of his property
• The testator should know the nature andextent of his assets which he is going todistribute
• Testator should also know the approximatevalue of his property.
The testator should be aware of the potentialbeneficiary
• The testator should have the knowledgeabout the legal heirs of his property.
• He should also know the potentialbeneficiaries whom he is likely to distributehis property as well as relationship withthem.
• He should be able to rationalize hisdecision.
The testator should be aware of the consequencesof his decision
• Testator should be aware of the possibleconsequences of the distribution of hisassets.
The testator should be free from undueinfluence//fraud/coercion
• Under Section 61 of Indian Succession Act1925, a Will or any part of a Will, themaking of which has been caused by fraudor coercion or by such importunity as takesaway the free agency of the testator is void.
• However sound mind the testator may behaving, if it has been the subject of undueinfluence, the soundness of mind will nothelp the will to be declared valid.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society406
The testator must have the knowledge of thecontents of the Will
• If the testator does not know the contentsof his Will it can’t be said to be a validWill.
• However, such knowledge and approval ofthe testator may be presumed on the proofof signature of the testator.
Neuropsychological Factors in Assessing TCA neuropsychological model for testamentary
capacity includes an assessment of cognitive skillsand knowledge related to the specific capacity beingassessed.10-11
Some of the neuropsychological factors wouldinclude12-13
1. The capable of understanding the act ofmaking a Will and its effects viz. Semanticknowledge with regards to terms such asdeath, property, and inheritance.
2. Capable of understanding the nature andextent of their property relevant to thedisposition - Long-term semantic andautobiographical memory related to assets.
3. Short-term episodic and working memoryare necessary for more recently acquiredassets and property, or if there have beenchanges to the estate.
4. Ability to form working estimates of assets,and comprehension of the approximatevalue attached to one’s estate.
5. Capable of evaluating the claims of thosewho might be expected to benefit from hisestate, and able to demonstrate an apprecia-tion of the nature of any significant conflictand/or complexity in the context of thetestator’s life situation. This would enticehistorical and short-term episodic personalmemory are required to recall nature ofrelationships with testator.
6. Executive functions including planning andreasoning are required for distributing one’sestate.
7. Capable of communicating a clear, consis-tent rationale for the distribution of theirproperty, especially if there has been asignificant departure from previouslyexpressed wishes or prior Wills.
8. The person must be free of a mental
disorder, including delusions, thatinfluences the dispositive provisions of aWill.
9. Language (or, broadly speaking, the abilityto communicate) is an important cognitivefunction for all legal criteria.
ConclusionsThe rapidly growing aging population,
suffering from age associated cognitive impairmentwould always be making transfer of wealthincreasingly complex and fragmented families inthe years to come with a number of legal problemsthat would ensue. There would be marked increasesin wills being legally challenged and much neededinput / evaluation from medical practitioners.Clinicians must be adept in the assessment anddocumentation for TC. Training programs on TCevaluation need to be conducted for cliniciansdealing with the elderly. This shall be a burningissue for geriatric medicine in the years to come.
References1. Mahal A, McPake B. Health systems for aging
societies in Asia and the Pacific. Health SystReform 2017; 3(3) : 149-53.
2. Kumar SV. Challenges Before the Elderly: AnIndian Scenrio. MD Publications Pvt. Ltd.;1995.
3. Bloom DE, Canning D, Lubet A. Global popula-tion aging: Facts, challenges, solutions andperspectives. Daedalus 2015; 144(2) : 80-92.
4. Sonawat R. Understanding families in India: Areflection of societal changes. Psicologia:Teoria e Pesquisa 2001; 17(2) : 177-86.
5. Kennedy KM. Testamentary capacity: apractical guide to assessment of ability to makea valid will. J Forensic Legal Med 2012; 19(4): 191-5.
6. Sousa LB, Simoes MR, Firmino H, Peisah C.Financial and testamentary capacity evalua-tions: procedures and assessment instrumentsunderneath a functional approach. IntPsychogeriatr 2014; 26(2) : 217-28.
7. Shulman KI, Peisah C, Jacoby R, Heinik J,Finkel S. Contemporaneous assessment oftestamentary capacity. Int Psychogeriatr 2009;21(3) : 433-9.
8. Chokkanathan S, Lee AE. Elder mistreatment

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 407
in urban India: A community based study. JElder Abuse Negl 2006; 17(2) : 45-61.
9. Skirbekk V, James KS. Abuse against elderlyin India–The role of education. BMC PubHealth 2014; 14(1) : 336.
10. Paruck PL. The Indian Succession Act, 1925(Act XXXIX of 1925). Georg Thieme Verlag;1988.
11. Jiloha RC. Mental capacity/testamentarycapacity. Clinical Practice Guidelines of theIndian Psychiatric Society – ForensicPsychiatry. Indian Psychiatric Society, 2009;29-34.
12. Voskou P, Douzenis A, Economou A,Papageorgiou SG. Testamentary capacityassessment: legal, medical, and neuropsycho-logical issues. J Geriatr Psychiatr Neurol 2018;31(1) : 3-12.
13. Sullivan K. Neuropsychological assessment ofmental capacity. Neuropsychol Rev 2004;14(3) : 131-42.
APPENDIX:CERTIFICATE FOR TESTAMENTARY
CAPACITY(To be issued on the letter head of the Doctor
or Institution / Department / Hospital)
This is to certify that I, Dr. ..........................have assessed the testamentary capacity of Mr....................................../ on (date), at (venue), time.
I have to state as follows:Mr ...................................................... is of / not
of sound mind; he is not / is suffering from anymajor mental disorder that mayinterfere with hiscapacity to make a will.
Mr ................................................. knows / doesnot know that he is making a will and he is makingit voluntarily without any pressure or influence fromanyone.
Mr ........................................ is aware / unawareabout the extent of his asset and about the legalheirs of his assets.
Impression:Mr ........................... is fit / unfit to make a will.
Signature(with seal of the doctor)
Medical Registration No.Date and Time:Place:

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society408
An overview of Organ Transplant Act:Role of Psychiatrist and Forensic expert
N.S. Sonwani,1 N.K. Aggarwal,2 M.S. Bhatia3
Departments of Forensic Medicine1,2 and Psychiatry,3 University College of Medical Science,Dilshad Garden, Delhi-110095
Contact: NS Sonwani, Email: [email protected]
Forensic Psychiatry
IntroductionOrgan transplantation (OT) is defined as the
transfer of a living tissue or organ to an injured orill person to restore health or reduce disability. Itwas first started in the 1930s. Earlier this conceptgave new hopes and new life to ailing patients whenseveral kidney transplants were successfullyperformed in the 1950s. Following that, transplanta-tion of other organs was done successfully, henceimproving quality of life and reducing morbidityand mortality.1 In India, primary legislation relatedto organ donation and transplantation was passedin 1994 as Transplantation of Human Organs Act(THOA).2 It was aimed at regulation of removal,storage, and transplantation of human organs fortherapeutic purposes and for prevention of commer-cial dealings in human organs. Despite a regulatoryframework, cases of commercial dealings in humanorgans were reported in the media. An amendmentto the act was proposed by the states of Goa,Himachal Pradesh and West Bengal in 2009 toaddress inadequacies in the efficacy, relevance andimpact of the act.3The amendment to the act waspassed by the parliament in 2011 and the rules werenotified in 2014.4
Apart from living donors, deceased donors arealso important source of organs. Deceased donationcan be done either after brain death (brain stemdeath) or after cardiac death. Deceased donationshould be done altruistically. It is necessary thatdeceased donation should be governed bytransparency to ensure that the sentiments of thedonor’s relatives are adequately respected.
Important features of Transplantation of
Human Organs Act(1994) and some majordifferences from Transplantation of Human Organand Tissue Act (2014) have been explained in TableI.
Present Scenario of Organ Transplantation inIndia
The shortage of organs is virtually a universalproblem and there is a wide gap between patientswho need transplants and the organs available inIndia. An estimated around 1.8 lakh persons sufferfrom renal failure every year, however the numberof renal transplants done is around 6000 only. Anestimated 2 lac patients die of liver failure or livercancer annually in India, about 10-15% of whichcan be saved with a timely liver transplant. Henceabout 25-30 thousand liver transplants are neededannually in India but only about one thousand fivehundred are being performed.Similarly about 50000persons suffer from Heart failures annually but onlyabout 10 to 15 heart transplants are performed everyyear in India.(Figure 1) In case of Cornea, about25000 transplants are done every year against arequirement of 1 lakh.5
Opt-out and Opt- in system: Comparisonbetween India and Spain
There are two main methods for determiningvoluntary consent, “opt in” (only those who havegiven explicit consent are donors) and “opt out”(anyone who has not refused consent to donate is adonor). In terms of an opt-out or presumedconsent system, it is assumed that individuals dointend to donate their organs to medical use whenthey expire.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 409
Table-1: Features and differences in Transplantation of Human Organs Act (THOA) 1994 andTransplantation of Human Organ and Tissue Act (THOTA) 2014
Features THOA (1994)2 THOTA (2014)3
Advisory Not mentioned Central and state govt. constitute advisorycommittee committee for a period of two years to aid and advise the
appropriate authority to discharge its functionAppropriate Appointed by state and central Govt.to AA is a national organs and tissue removal and storageauthority grant, suspend and cancel registration, network at one or more place to perform function as AP.
and inspect, investigate any complaint AA can issue summons and search warrant for unauthorizedremoval, procurement or transplantation of human organ.
Authorization Appointed by central and state government Additional Authorization Committees in the districts orcommittee Institutions or hospitals (if the number of transplants is
twenty five or more in a year at the respectivetransplantation centers)
Brain death By board of medical experts consisting the Added physician, anesthetist, intensivist.declaration team registered medical practitioner and neurologist
and neurosurgeon.Who is donor Near relative: spouse, son, daughter, father, Near relative: grandmother, grandfather, mother, father,
mother, brother or sister; brother, sister, son, daughter, grandson and granddaughter,above the age of eighteen years,
Numbers of forms 13 21Video No Applicant should be personally interviewed by the
Authorization Committee which shall be video graphed andminutes of the interview shall be recorded.
Penalties Punishment for commercial dealings in Five years but which may extend to ten yearsand shall behuman organs which shall not be less than liable to fine which shall not be less than twenty lakhtwo years but which may extend to seven rupees but may extend to one crore rupees” shall beyears and shall be liable to fine which shall substituted;not be less than ten thousand rupees but mayextend to twenty thousand rupees.Punishment for contravention of any other Five years or with fine which may extend to twenty lakhprovision of this Act shall be punishable rupees” shall be substitutedwith imprisonment for a term which mayextend to three years or with fine whichmay extend to five thousand rupees
India and USA follow opt-in system whereascountries like Spain, Austria, Israel, France, Greece,Norway, Sweden and Turkey follow opt-out system.
India - Human organ and tissue transplantationwas started in India in 1962. Initially, the organtransplant was unregulated, and organ traffickingwas rampant. The act governing the transplantationwas passed in 1994. This has been subsequentlyamended in 2011, and new rules came into force in2014. India follows opt- in method and the finalauthority over the matter lies with the deceased nextof kin. If the family refuses, the organs of thedeceased person cannot be harvested.5
Spain - The first legislation of organ transplan-tation in Spain was established in 1979, and in 1989,the Organization National De Transplants (ONT),as the national transplant organization in Spain, wasestablished with the aim to promote transplantation.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society410
With the highest donor rates in the world for24 years running, Spain is considered the goldstandard for organ donations. In 2015 with 39.7donors per million, 4,769 transplants wereperformed in Spain.Working on a system of“presumed consent”, the Spanish model considersall citizens as potential donors unless theyspecifically choose to opt-out.6
Role of PsychiatristOrgan transplantation (OT) is a complex and
major surgical procedure. It carries tremendousexpectations from the OT candidates and caregiversfor saving life and improving the quality of life(QOL).Thus, starting from the onset of the end stageorgan disease (ESOD), undergoing evaluation forcandidacy, surgical procedure and relatedcomplications, and ending with death, all throughthese phases, OT and organ donation are inherentlyenormously distressing.7
Psychiatrists play an important role not onlyin selecting the best suitable candidate for theprocedure by psychosocial screening but also totackle post-operation psychological issues thattrouble patients as well as caretakers. Issues likeselection of patients with psychiatric disorders andsubstance abuse for transplantation process andtheir treatment both pre- and post- operation, riskyhealth behaviors, treatment adherence for immuno-suppressant’s and psychological support forcaretakers can be better addressed by a psychiatristwho is sensitive towards these issues.Organ transplant: A high distressing process
1. Waiting for organ donation is the mostdistressing phase. Continued deteriorationof health and critical medical care likedialysis is associated with 10-18 per centpatients dying, and 5 per cent becomingmedically unsuitable; another 2 per centrefuse OT.8
2. Transplantation and after, means dealingwith a complex OT procedure, periopera-tive complications and a post-OT life withconstant threat to survival, and inevitableand often distressing dependence oncaregivers for help on various counts.
Pre-transplant Psychosocial EvaluationHelps to get a more complete understanding of
mutual and sometimes contradictory, expectationsand needs of transplant candidates, donors,caretakers and the transplant team. The psychiatristplays a unique dual role in serving both the needsof the transplant team as well as the transplantpatient, donor and the carers.9
Psychiatric Disorders in OT casesOT cases are higher risk for psychiatric
disorders. It may be due to either the exacerbationof a pre-existing disorder or the development ofnew-onset disorder.
Mainly it includes, mood and anxiety disorder,personality disorders, cognitive disorder, immuno-suppressant drug acquired neuropsychiatricmanifestation.
Burden over CaregiversDependency of transplant recipients on care-
givers for everything including self-care, treatmentadherence, finance, transportation, and emotionalsupport, put them under stress. Heavy burden oncaregivers and negative coping styles are shown tobe associated with higher levels of depression.10
Management of Psychiatric DisordersThe risk for psychiatric disorders rises during
organ transplantation and it adversely affects theOT outcome, compliance, morbidity, and mortality.Hence, there is need for early recognition andmanaged by psychotropic’s and psychotherapy.
Indian ScenarioThere is very little study from India on psychia-
tric issues related to OT. An early study reportednegative emotions among kidney recipients anddonors. Among the recipients the common emotionsincluded anxiety-depression and resentment duringdialysis and perioperative period, and anxiety,dependency-frustration, body image change anddecreased libido on a long term basis.11 In a sixmonth to six year follow up of 50 male kidneyrecipients psychiatric illness was noted in 46 percent of recipients and it was more common amongunmarried, high education group and high socio-economic status.12
Role of Forensic Expert in Organ DonationIn India the donation (cadaveric and brain dead)
and transplantation of human organs is governed

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 411
by Transplantation of Human Organs Act 1994. Theforensic expert plays a significant role in facilitatingorgan donation (brain dead and cadaveric) bycoordinating between relations, legal agencies,organ banks and transplant surgeons.Further,forensic expert can also contribute in investigationin cases of illegal removal of organs from the bodyof persons.13
Future of organ transplantationThe future of transplantation is one full of
miracles of modern medicine. New option includevascularized composite allograft (like face andhand) transplant, protocols permitted the successfulminimization or even discontinuation of immuno-suppressive medication, and the use of stem cellsfor organ regeneration.
The fulfillment of this promise will depend onmany factors. Primary among these is the fundingof clinical and basic science research that will allowthe development of these new therapies.
Progress continues to be made in xenotrans-plantation (organ taken from other species intohumans). New biochemical device to replace organfunction are under development.
Also the fields of pharmacogenomics willaccurate individualization in the selection anddosing of medication, including transplant medica-tion.References1. Linden PK. History of solid organ transplan-
tation and organ donation. Crit Care Clin 2009;25(1) : 165-84.
2. Government of India. Transplantation ofHuman Organs Act, 1994. Central Act 42 of1994. The Gazette of India, part II; section 3;sub section (I); Feb 4, 1995.
3. Transplantation of Human Organs(Amendment) Act, 2011. Available from:https://www.india.gov.in/transplantation humanorgans amendmentact 2011.
4. Extraordinary Transplantation of HumanOrgans and Tissues Rules (THOTA). Ministryof Health and Family Welfare Notification. Part2. Sec 3. New Delhi: The Gazette of India, 2014.
5. Sahay M. Transplantation of human organs andtissues act- “Simplified”. Indian J Transplant2018; 12 : 84-9.
6. Kobayashi M, Usui J, Yamagata K. SituationSurrounding Organ Transplantation: A Com-parison between Spain and Japan. J Clin CaseRep 2015; 5 : 589.
7. United Network of Organ Sharing andScientific Registry of Transplant Recipients.Available from: http://www.unos.org/data,accessed on December 21, 2014.
8. Dimartini AF, Dew MA, Crone CC. Organtransplantation. In: Sadock BJ, Sadock V A,Ruiz P, editors. Kaplan & Sadock’s compre-hensive textbook of psychiatry. 9th ed.Philadelphia: Lippincott Williams and Wilkins,2009; 2441-55.
9. Goetzinger AM, Blumenthal JA, O’Hayer CV,Babyak MA, Hoffman BM, Ong L, et al. Stressand coping in caregivers of patients awaitingsolid organ transplantation. Clin Transplant2012; 26 : 97-104.
10. Kuruvilla K, Mohan Rao M, Johny KV.Psychiatric aspects of renal transplantation -some observations on recipients. Indian JPsychiatry 1976; 17 : 26-32.
11. Chaturvedi SK, Pant VLN. Psychiatric aspectsof renal transplantation. Indian J Psychiatry1985; 27 : 77-81.
12. National Organ and Tissue Transplant Organi-zation (NOTTO). Directorate General of HealthServices, Ministry of Health and FamilyWelfare, Government of India.
13. Dogra TD, Lalwani S, Vij A, Vyas M,Venugopal P. Organ retrieval in medicolegalcases. J Acad Hosp Admin 2004; 16(2) : 7-12.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society412
Kleine-Levin SyndromeReena Jambulkar, Sagar Karia, Nilesh Shah, Avinash De Sousa
Department of Psychiatry, Lokmanya Tilak Municipal Medical College, MumbaiContact: Sagar Karia, E-mail: [email protected]
Case Report
IntroductionKleine-Levin syndrome (KLS) is a syndrome
characterized by hypersomnolence, hyperphagiaand hypersexuality.1 Hypersomnolence is the keyfeature while the two other may be absent.Cognitive disturbances, hallucinations, delusions,psychosis and mood abnormalities have beendescribed in relation to the disorder.2 The disorderhas shown a male preponderance while cases infemales have been reported.3 The treatment optionsare many and have been documented in anecdotalcase reports and include Lithium,4 antidepressants,5
antipsychotics,6 benzodiazepines7 and evenelectroconvulsive therapy.8 We describe herewitha case of 30 year old that developed male andpresented to our outpatient department.
Case ReportA 30-year-old married Hindu male shopkeeper,
educated till the 12th standard, presented to ouroutpatient department accompanied by his fatherwith chief complaints of episodes of headache andexcessive sleep since the past 3 years. The patientwas apparently alright 3 years back when hesuddenly developed irritability and headache in bothfrontal regions. The headache would be intermittentand last for 15-20 minutes, subsiding for a few hoursand recurring again. The patient had depressivefeatures during these episodes where he would notfeel like going out and mixing with people, lowmood, not feel like working, feeling of weaknessand fatigue and loss of appetite. These symptomswould last for a 2-3 days and would culminate inhim sleeping for 20- 22 hours at a stretch. After
sleeping for 20-22 hours, he would wake up, usethe washroom and would eat in large quantities andagain go to sleep. The sleeping episodes wouldcontinue for 4-6 days. He would remain absolutelynormal for the next 15 days and again would getsimilar episodes of sleep. This pattern was prevalentsince the past 3 years.
During the symptom free days, he had nohistory of sadness of mood, irritability or sleep andappetite disturbances. The patient’s birth andchildhood developmental history was uneventful asper the information given by his father. He had apast medical history of seizures at age of 12 yearsand was started on antiepileptic medication whichhe took for a period of 5 years and it was taperedoff by the treating neurologist. He was maintainedon Sodium Valproate 800mg per day in divideddoses and was seizure free currently. There was nohistory of head injury and significant medicalillnesses and there was no family history suggestiveof psychiatric illness or epilepsy. On mental statusexamination, no significant psychiatric findingswere present as the patient was symptom free atthe time of presentation. The patient was subjectedto routine blood investigations like blood counts,liver and kidney function, serum lipids andelectrolytes which were within normal limits. Hewas also investigated for serum vitamin B12 levels,vitamin D levels, calcium levels, serum testosteroneand serum uric acid which were all normal. He wasasked to get an electroencephalogram (EEG) donein view of his past history of seizures and the EEGwas within normal limits. A magnetic resonanceimaging (MRI) study of his brain was done which

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 413
patient responded very well to a combination ofmedication and more systematic studies are neededfor coming up with treatment guidelines for themanagement of KLS.
References1. Ramdurg S. Kleine–Levin syndrome: etiology,
diagnosis, and treatment. Ann Indian AcadNeurol 2010; 13(4) : 241-6.
2. Arnulf I, Zeitzer JM, File J, Farber N, MignotE. Kleine–Levin syndrome: a systematic reviewof 186 cases in the literature. Brain 2005;128(12) : 2763-76.
3. Arnulf I. Kleine-Levin syndrome. Sleep MedClin 2015; 10(2) : 151-61.
4. Loganathan S, Manjunath S, Jhirwal OP,Varghese M, Srinath S. Lithium prophylaxis inKleine-Levin syndrome. J Neuropsychiatr ClinNeurosci 2009; 21(1) : 107-8.
5. Huang YS, Arnulf I. The kleine-Levinsyndrome. Sleep Med Clin 2006; 1(1) : 89-103.
6. Oliveira MM, Conti C, Saconato H, Prado GF.Pharmacological treatment for Kleine Levinsyndrome. Cochrane Database Syst Rev 2009;(2) : CD006685.
7. Arnulf I, Lin L, Gadoth N, File J, LecendreuxM, Franco P, Zeitzer J, Lo B, Faraco JH, MignotE. Kleine–Levin syndrome: a systematic studyof 108 patients. Ann Neurol 2008; 63(4) : 482-93.
8. Moise FN, Petrides G. Case study: electrocon-vulsive therapy in adolescents. J Am Acad ChildAdolesc Psychiatry 1996; 35(3) : 312-8.
9. Das S, Gupta R, Dhyani M, Raghuvanshi S.Kleine-Levin syndrome: a case report andreview of literature. Pediatr Neurol 2014; 50(4): 411-6.
10. Aggarwal A, Garg A, Jiloha RC. Kleine-Levinesyndrome in an adolescent female and responseto modafinil. Ann Indian Acad Neurol 2011;14(1) : 50-2.
did not reveal any abnormality. A neurological andendocrinological consultation was done which inconsultation liaison with psychiatry led to adiagnosis of KLS.
He was started on tablets Lithium sustainedrelease 400 mg and Fluoxetine 20 mg per day inview of his symptoms. On follow up after 15 days,he reported 20% improvement in the sense that nowhe used to sleep for 16-20 hours instead of 20-22hours. We further increased the dose of Lithium to800mg and Fluoxetine to 40 mg while addingModafinil 200 mg per day. In the next 15 days hereported around 70-80% improvement with sleepepisodes being 8-10 hours which was manageableand no other symptoms during the episode. He iscurrently maintained on the same.
DiscussionThe diagnosis in most cases of KLS is a clinical
one and there is no single of group of laboratorytests that may be diagnostic for the condition. Hencewe did all the routine investigations which werewithin normal limits and diagnosed clinically withhelp from our neurology and endocrinologycolleagues. In our case, hypersexuality was absent,but studies have shown that hypersomnia is the solemain requirement for the diagnosis of KLS.3
Limited literature is available on the managementof KLS with Lithium being used in a large numberof cases.4 We thought of restarting the patient onValproate in view of it being a mood stabilizer andit being used in the past by the patient without sideeffects. The patient refused to be on an antiepilepticand hence we chose Lithium. In view of thedepressive features seen in the episode we startedthe patient on Fluoxetine as SSRIs have been usedin the management of KLS.9 The disorder usuallyhas a good prognosis and can be managed well withmedications. In our patient we also startedModafinil which has been used in many cases tomanage excessive sleepiness with success.10. Our

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society414
Capgras Syndrome: She’s Not My Wife !!P. Patra,1 Rajiv K. Saini,2 D. Bhattacharya,3 B. Patra,4 SA Khan,5 Kartikeya R. Singh6
1,2,3,5,6Department of Psychiatry, Command Hospital Kolkata4 Department of Psychiatry, Katihar Medical College, Bihar.
Contact: Priyadarshee Patra, E-mail: [email protected]
Case Report
IntroductionCapgras syndrome was originally described by
Capgras and Reboul-Lachaux. It is a delusion thata person or persons have been replaced by“doubles” or imposter.1 It is a type of a misidenti-fication syndrome, the others being: FregoliSyndrome, the syndrome of intermetamorphosisand the syndrome of subjective doubles. Clearaetiology of Capgras syndrome is not known andboth organic and psychodynamic theories attemptto explain it. The psychodynamic theory emphasizesthe role of primitive ego defence mechanisms ofprojection, denial, and splitting. It explains that thisdelusion is the result of how a patient deals withthe ambivalent emotions that he feels toward theclose family members. Denying anger at the closerelative and instead claiming that the anger is beingexpressed at an impostor. 2,3 Organic theorypostulates “identification without recognition” i.e.the ability to identify a person is intact but a brainlesion affects the ability to recognise/sense afamiliarity.4 Capgras syndrome has been reportedin neurogenerative conditions like dementia or brainlesions affecting the right frontal or left temporalregion,5.6 dementia with Lewy bodies,7 multiplesclerosis,8 and Parkinson’s disease.9 Also, it hasbeen associated with psychiatric disorders likeschizophrenia.10,11 The prevalence of Capgrassyndrome is two times higher in females thanmales.12 It has been treated with mostly anti-psychotic drugs and in at least one case withantidepressant but without achieving completeresolution of symptoms.13,14
Case reportA 65 year old retired clerk was brought to the
psychiatry OPD by his wife and children withcomplaints of, increased irritability and angeroutburst since last one year and suspiciousnessdirected towards wife since last 4 months. Thecomplaints were insidious in onset and graduallyprogressive in course. Detailed history revealed thatthat individual was apparently asymptomatic till 1year back when his family members noticed thathe is easily getting irritated over trivial things, moreso with activities related to his wife. He would scoldher over minor issues like food being served a bitlate, plates and utensils not being clean as per hissatisfaction, the bathroom lights being left on. Hisbehaviour was a clear departure from his usualaffable and loving self. Gradually his behaviourworsened and he would offer no clear cut reasonfor his anger outbursts but preferred to stay alone.During this time his wife and sons left town for aweek to attend a marriage ceremony of a relative.When they returned, they found that the individualwas refusing to talk to his wife. He did not allowher to sleep on the same bed. He accused his wifeto be someone else in disguise. No amount ofexplanation and rationalization by his wife and sonscould convince him otherwise. He explained to hissons that the woman who had returned with themthough looked exactly like their mother, was in factan imposter who has come to their house to stealmoney and property documents. He took back thealmirah key which was with his wife and accusedher of being a thief. He made his wife shift out of

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 415
DiscussionIn this case report we have discussed the
clinical presentation and management of Capgrassyndrome in an elderly man. Though many casesof Capgras syndrome have an organic aetiology, thisone did not. Capgras syndrome has been called asa mirror image of prosopagnosia12 albeit withsignificant differences between the two. In Proso-pagnosia though facial recognition is affected butauditory perception and recognition is not. Patientscan identify and recognise persons by their voices.15
Also in prosopagnosia, the ventral pathway facialrecognition is affected and the dorsal pathwaywhich contributes to emotional processing,remained unaffected. While the exact oppositeoccurs in Capgras syndrome, which may explainthe abnormal emotional reactions.12 Remaining trueto the nature and course of Capgras syndrome,13
our case too did not achieve full remission. Manage-ment in such cases first involves ruling outorganicity. Patients must be handled with empathy,reassurance. Risk assessment is important, as thereis a higher incidence of violence in patients withdelusional disorders.16 Treatment modality includedboth pharmacotherapy and psychotherapy. Patientand family members need to be adequately psycho-educated about the nature and course of the disorder,the signs and risk factors of relapse, expected sideeffects of the medications, necessity of drugcompliance and regular follow up.
References1. Sinkman A. The syndrome of Capgras.
Psychiatry 2008; 71(4) : 371-8.2. Silva JA, Jalali B, Leong GB: Delusion of
exchanged doubles in an immigrant: a new |Capgras variant? Int J Soc Psychiatry 1987; 33: 299-302.
3. Berson RJ. Capgras’ syndrome. Am JPsychiatry 1983; 140 : 969–78.
4. Feinberg TE, Roane DM. Delusional Misidenti-fication. Psychiatry Clin N Am 2005; 28 : 665–83.
5. Josephs KA: Capgras syndrome and its relation-ship to neurodegerative disease. Arch Neurol2007; 64 : 1762-1766.
6. Signer SF: Localization and lateralization in thedelusion of substitution. Capgras symptom and
their bedroom and restricted her entrance in thekitchen accusing her of hatching a plan to kill himby strangulating him or poisoning his food. Theindividual continued to be adequately functional inother spheres of his life. He continued his regularwalks, visits to the market, maintained self care andhad normal interactions with others. Around a weekback, individual made a will and left out his wifefrom it and also complained to the police about thisimposter. These events led to his psychiatricconsultation. Evaluation revealed a well kemptindividual with normal pace and gait. A full neuro-logical workup was done (Physical examination,MRI, MMSE, bedside tests for parietal lobe,temporal lobe and occipital lobe), which wasnormal. Also relevant investigations (FBC, ESR,CRP, T4 and TSH, biochemical screen, urea andcreatinine, glucose, B12 and folate ) were WNL.Psychomotor activity was normal. Speech wasnormal in rate, tone and volume. It was coherentand relevant with prosody maintained. Nodisarticulation or neologism. Affect was anxiouswith normal range and reactivity, congruent to thisthought process. Mood was objectively andsubjectively dysphoric, stable, adequate controlwith no diurnal variation. Thinking was normal instream and form. Content revealed Delusion ofmisidentification and delusion of persecution. Therewere no syndromal depressive features, no percep-tual anomalies. Individual had intact cognition andclear sensorium. Test and social judgement wereimpaired and he lacked insight into his conditionand behavioural oddities. Biodrives were stable.Individual was diagnosed as a per ICD 10 as a caseof Delusional disorder (F22.0) – Delusion ofmisinterpretation (Capgras syndrome) and delusionof persecution. He was started on Tab Risperidone2 mg HS which was gradually built upto 6 mg perday in divided doses, as per the response of thepatient. Additionally, he was exposed to Cognitivebehaviour therapy and insight oriented psycho-therapy. Over the next two months, there wasencapsulation of the delusions with correspondingreduction in their emotional valence. Individualstarted cohabitating with his spouse. Thoughoccasionally he expressed doubts about her identitybut now was amenable to advices of his familymembers.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society416
its variants. Psychopathology 1994; 27 : 168-176.
7. Thaipisuttikul P, Lobach I, Zweig Y, GurnaniA, Galvin JE. Capgras syndrome in Dementiawith Lewy Bodies. Int Psychogeriatr 2013;25(5) : 843-9.
8. Sharma A, Garuba M, Egbert M. Capgrassyndrome in a patient with multiple sclerosis:a case report. Prim Care Companion J ClinPsychiatry 2009; 11(5) : 274. | 15
9. Moro A, Munhoz RP, Moscovich M, ArrudaWO, Teive HA. Delusional misidentificationsyndrome and other unusual delusions inadvanced Parkinson’s disease. ParkinsonismRelat Disord 2013; 19(8) : 751-
10. Armando M, Girardi P, Vicari S, Menghini D,Digilo MC et al. Adolescents at ultra high riskfor psychosis with and without 22q11 deletionsyndrome: a comparison of prodromalpsychotic symptoms and general functioning.
Schizophr Res 2012; 139 : 151-156.11. Feinberg TE, Roane DM: Delusinal misidenti-
fication. Psychiatr Clin North Am 2005; 28 :665-683.
12. Edelstyn NM, Oyebode F: A review of thephenomenology and cognitive neuropsycho-logical origins of the Capgras syndrome. Int JGeriatr Psychiatry 1999; 14 : 48-59.
13. Sinkman A: The syndrome of Capgras.Psychiatry 2008; 71 : 371-378.
14. Khouzam HR: Capgras syndrome respondingto the antidepressant mirtazapine Compr Ther2002; 28 : 238-240.
15. Barton JJ. Disorders of face perception andrecognition. Neurol Clin 2003; 21 : 521-548.
16. Sadock BJ, Sadock VA. Kaplan and Sadock’sSynopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Philadelphia: LippincottWilliams & Wilkins; 2003; 511-520.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 417
Disulfiram-induced delirium: Diagnostic dilemmaRavi Parkash,1 Priti Singh,2 Ripu Daman,3 Sakshi,4
Neharika Saini,5 Rajiv Gupta6
Departments of Psychiatry1,2,3,4,6 and Medicine5 Pt. B.D. Sharma PGIMS, RohtakContact: Priti Singh, E-mail: [email protected]
Case Report
IntroductionDisulfiram (Antabuse), an inhibitor of acetal-
dehyde dehydrogenase, is a drug used extensivelyin the treatmentof alcohol addiction.1 It wassynthesized for the first time in 1881 and was usedin industry as a catalytic accelerator for the vulcani-zation of rubber. Hald and Jacobson, two Danishphysicians, in 1940, became ill while takingdisulfiram as an anthelminthic,2 after alcoholconsumption and since 1948 it is being used foralcohol dependence management. Neuropsychiatricmanifestations of disulfiram use have been reportedin both the neurology and psychiatry literature andhave been characterized by symptoms such asparanoia, impaired memory and concentration,ataxia, dysarthria,and frontal release signs.3 Disul-firam induced delirium alone is very rare in theabsence of an ongoing psychotic process ordisulfiram-ethanol reaction. In our knowledge, acase of disulfiram-induced delirium at a deterrentdose in the absence of disulfiram-ethanol reactionis very rare which may lead to a diagnostic dilemma.
Case reportMr. R 43-year-old, a graduate, currently work-
ing as an inspector in food and supply, belongingto a middle socioeconomic nuclear family, Haryana.Presented to state drug deaddiction center withhistory of drinking Indian made foreign liquor sincelast 20 years and in dependent pattern from last 10years (meeting both ICD-10 and DSM 5-criteria),patient had prior history of two-time relapse aftertreatment. Patient had no past history of comorbid
psychiatric and medical illness. Patient wasadmitted in deaddiction center PGIMS Rohtak incontemplation stage of motivation for themanagement of alcohol dependence. Patient’sdetoxification was done with tablet lorazepam andtablet thiamine was started in view of chronic useof alcohol. During ward stay, motivation wasassessed and motivational enhancement therapywas started. After 15 days of ward stay, he wasstarted on tablet disulfiram after informed consentand was discharge on tablet disulfiram 250 mg oncedaily. While he was compliant with his medicationswith regular weekly follow up and with strictalcohol abstinence (corroboratedby familymembers), 4 weeks after his hospital discharge thepatient was again brought by his family memberswith 2 days history of forgetfulness, insomnia,irritability, increased psychomotor activity,irrelevant speech fluctuating course of orientationand confused behavior. There was no history ofalcohol consumption in any form during that wholemonth after being discharged from the hospital. Onadmission, his blood investigations revealedhemoglobin of 10.5 g/dl, total white cell count of5900/cubic mm with 83% neutrophils, 9% lympho-cytes, 8% monocytes, and normal platelets counts.His baseline biochemical parameters were withinnormal limit. urea, creatinine, serum electrolytessodium, potassium, chloride, hepatic transaminases,blood sugar, urinalysis, thyroid function, and uricacid levels were all within normal limits. MRI brainwas done which was found within the normal limit.As no other differential diagnosis could be establi-

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society418
similar to those of the schizophrenic spectrum ofillness, which has also been partially attributed toincrease in dopamine.7
Disulfiram encephalopathy usually occurswithin the first few months of disulfiram therapy.This complication of disulfiram therapy hasoccurred largely independent of disulfiram dosageand, to our knowledge, exclusively in the absenceof concomitant ethanol intake the incidence ofdisulfiram encephalopathy has been reported veryrarely.8 Although delirium usually accompaniespsychotic reactions, psychosis in clear conscious-ness has also been known to occur. But deliriumalone without psychosis, disulfiram-ethanolreaction and other medical complications is veryrare. If a patient having any psychiatric illness orhaving any serious medical illness, any brain lesionmay increase the risk of development of toxic effectof disulfiram. Hence, the above-mentioned riskfactors should be evaluated before prescribingdisulfiram to any individual.9 In the index patient,delirium occurred within 4 weeks of startingdisulfiram. He had no past history of alcohol-induced psychotic disorder and withdrawal seizure;hence the diagnostic dilemma. However, hisdelirium resolved within 3 days of stopping thedisulfiram and no other psychiatric or physicalcause or disulfiram-ethanol reaction could beidentified.
References1. Mohapatra S, Rath NR. Disulfiram Induced
Psychosis. Clin Psychopharmacol Neurosci2017; 15(1) : 68–9.
2. Jacobsen E. The Sensitizing Effect ofTetraethylthiuram disulphide (Antabuse) toEthylalcohol. Acta pharmacol 1948; 4(1) : 286–96.
3. Melo RC De, Lopes R, Alves JC. Case ReportA Case of Psychosis in Disulfiram Treatmentfor Alcoholism. Adv Psychiatr Treat 2014; 2(1): 25–9.
4. Wood PL, Alexander RS, Felty CC. Disulfi ramneurotoxicity/ : Decrements in ethanolamine,serine and inositol glycerophospholipids. J MolPathophysiol 2014; 3(3) : 33–7.
5. Singh HMRR, Radha A, Thyloth M. DisulfiramInduced Psychosis. J Addict Depend 2017; 3(2): 2–4.
shed for the delirious condition of the patient, tabletdisulfiram was stopped along with supportivemanagement and low dose benzodiazepine werestartedwith close monitoring for the managementof delirium.
He recovered completely in 72 hours andthereafter. Motivation enhancement and relapseprevention counseling were done. Tab disulfiramwas excluded from further treatment option. Patientwas discharged in fair condition was advise toregular follow up in our center.
DiscussionDisulfiram is an important drug in the treatment
of alcohol abuse and is under clinical evaluationsin a number of other addictions. Disulfiram(tetraethylthiuram disulfide) is a quaternaryammonium compound, it has been used for morethan 60 years as an aversion therapeutic agent inthe treatment of alcohol dependence.4 Disulfiramacts as a deterrent agent against drinking alcohol.Neuropsychiatric adverse effects of disulfiramaccount for 4-13% of total adverse drug reactions.3
In this case, patient was abstinence for almost amonth and was taking tablet disulfiram when hedeveloped symptoms of delirious state withoutconcomitant use of ethanol.
When there is concomitant alcohol consump-tion, it produces sensitivity to alcohol, leading toan unpleasant reaction, ethanol-disulfiram reaction,caused by the accumulation of acetaldehyde throughthe inhibition of the enzyme acetaldehyde dehydro-genase with histamine release. Disulfiram can alsocause adverse symptoms, when used alone, such asdrowsiness, fatigue, impotence, headaches, skineruptions, neurological toxicity, and psychosis.5
Positive psychotic symptoms such as delusions,hallucinations, bizarre behavior, and disorganiza-tion of thought process, as well as classic catatoniacharacterized by negativism, catalepsy, mutism, andstereotypes, have been reported in patientscompliant with alcohol abstinence during disulfiramtherapy.6 These cases have been at least partiallyattributed to disulfiram being a known inhibitor ofdopamine beta-hydroxylase, the enzyme thatconverts dopamine to norepinephrine. Excessdopamine contentand perhaps increased dopami-nergic tone, in the limbic and frontal regions of thebrain are thought to cause symptoms that would be

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 419
6. Dixit V, Karia S, Kalra G, Dixit V, Karia S,Kalra G. Catatonia due to surreptitiousadministration of disulfiram/ : a case report. JSubst Use ISSN 2016; 9891(3) : 181–3.
7. Tartara E, Fanucchi S, Errico ID, Farina LM,Casoni F, Sinforiani E, et al. A Case of WernickeEncephalopathy Combined With DisulfiramIntoxication. Cogn Behav Neurol 2013; 26(2) :93–8.
8. Park CW, Riggio S. Disulfiram–EthanolInduced Delirium. Ann Pharmacother 2001;35(1) : 32–5.
9. Basu D, Sharma A, Nebhinani N. Disulfiram-induced delirium/ : Diagnostic dilemmaDisulfiram-induced delirium/ : diagnosticdilemma. J Ment Heal Hum Behav 2014; 1(January 2009) : 103–7.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society420
Pyromania like behavior in a case of DementiaAvinash De Sousa
Department of Psychiatry, Lokmanya Tilak Municipal Medical College, MumbaiContact: Avinash De Sousa, E-mail – [email protected]
Case Report
IntroductionPyromania is an impulse control disorder which
is characterised by repetitive fire setting behaviourpreceded by anxious urges to set useful and non-useful objects or property on fire.1 It has beendocumented as a disorder on its own seen in youngeradults and may also be seen as a symptom havingdocumented under the context of antisocialpersonality disorder and schizophrenia.2 We presentherewith the case of a 73 year old male withdementia that presented with pyromania likebehaviour.
Case ReportA 73 years old married retired teacher was
brought by his wife to the outpatient clinic withchief complaints of setting things on fire at homeand enjoying the process by laughing and smilingas the things would burn. The wife mentioned thatthis behaviour started around 2 months prior topresentation when the patient suddenly startedplaying with matchboxes and matchsticks andwould set all the matches on fire at one go and wouldlaugh and enjoy the process. He also started settingsmall objects made of plastic, newspapers and otherthings on fire and would enjoy the process. He oncetried to set some clothes and the curtains on fire.He was taken to his family physician in view ofthisand was then referred to the psychiatry depart-ment. When the patient presented to the psychiatrydepartment a detailed clinical history and evaluationwas conducted which yielded a history of forget-fulness and behavioural issues in the form of
aggressive abusive behaviour once or twice a week.The patient had gone for a complete health
check-up prior to presentation and all his bloodreports were normal with no medical disordersexcept hypertension for which he was prescribedAmlodipine 5 mg twice a day. The patientcomplained of forgetfulness and his wife mentionedthe abusive aggressive behaviour and hence he wasadvised a magnetic resonance study of the brain.The imaging study revealed generalised corticalatrophy more in the temporal and frontal regionswith microvascular infarcts in bilateralhemispheres. A diagnosis of combined Alzheimer’sand Vascular Dementia was given and the patientwas started on Donepezil 5mg at night andPiracetam 800 mg thrice a day with Citicholine 500mg once a day by the family physician. His MMSEscore was 22. When we saw the patient we startedhim on Escitalopram 10 mg at night and Risperidone1mg twice a day with Trihexyphenydyl 2 mg at nightin view of the behavioural problems and fire setting.We attributed the same to his dementia and thoughtthe medication would help. The patient did not thinkfire setting behaviour was a problem and said thathe enjoyed the same. On follow up within 3 weeksof starting the medicine the patient was much calmerand completely stopped the behaviour. The familywas psycho-educated about dementia and thepatient has been following up regularly.
DiscussionThere have been anecdotal reports and case
series on pyromania in young adults.3-4 There has

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 421
been to the best of our knowledge no report ofpyromania like behaviour with an onset after theage of 70 years seen in dementia. Treatmentguidelines and management issues are not welldefined for pyromania like behaviour due tolack ofa large number of cases.5 The patient in our studyhad symptoms for a few months and also haddementia with behavioural issues. This case reportaims to make clinicians aware of this rare yetpossible occurrence of pyromania like behaviourin patients with dementia where the behaviour maypresent as a part of behavioural and psychologicalsymptoms of dementia.
References1. Lindberg N, Holi MM, Tani P, Virkkunen M.
Looking for pyromania: Characteristics of a
consecutive sample of Finnish male criminalswith histories of recidivist fire-setting between1973 and 1993. BMC Psychiatry 2005; 5(1) :47.
2. Burton PR, McNiel DE, Binder RL. Firesetting,arson, pyromania, and the forensic mentalhealth expert. J Am Acad Psychiatry LawOnline 2012; 40(3) : 355-65.
3. Soltys SM. Pyromania and fire settingbehaviors. Psychiatr Ann 1992; 22(2) : 79-83.
4. Kolko DJ. Fire setting and pyromania. JohnWiley & Sons 1989.
5. Kirsch JL, Simeon D, Berlin H, Hollander E.Disruptive, impulse control, and conductdisorders: Intermittent explosive disorder,kleptomania, and pyromania. Psychiatry 2015;1 : 1367-93.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society422
Auto erythrocyte sensitization syndrome ina young girl
Abhishek Singh Chauhan, Deepak GuptaDepartment of Child Psychiatry, Sir Ganga Ram Hospital, New Delhi
Contact: Abhishek Singh Chauhan, [email protected]
Case Report
IntroductionAuto erythrocyte syndrome also k/a painful
bruising syndrome is a rare but well-recognisedcondition, which is almost entirely confined towomen, exquisitely tender bruises arises afterminimal trauma or emotional stress.1 This syndromewas first described by Gardner and Diamond whopostulated it as an auto erythrocyte sensitizationsyndrome.2 The patient describes a wide range ofboth haemorrhagic and non-haemorrhagic com-plaints, including severe headaches, paraesthesias,repeated syncope, diplopia (sometimes monocular)and nervousness. Psychiatric studies indicated thatpatients had overt depression, anxiety disorders,sexual problems, feelings of hostility, and obsessivecompulsive disorder.3 Typical ecchymosis can beproduced by the intradermal injection of the patientsown RBC’s. Some feel that this response differen-tiates the condition from the psychogenic purpura.1
Case presentationA 16 year old girl studying in class 11th belong-
ing to the hindu nuclear family urban backgroundfrom a higher socioeconomic status, came to ourhospital with complaints of spontaneous painfulbruise over the right index finger associated withsevere anxiety and restlessness (Fig. 1). She cameto the paediatrics OPD where her routine investi-gations in the form of Complete blood count,erythrocyte sedimentation rate, C-reactive protein,and other haematological test were carried out, allinvestigations came to be normal except ESR whichwas found to be 45 mm/h. Patient was prescribed
some anti-inflammatory drug and was asked toreview after seven days. Two weeks later patientpresented with spontaneous painful reddishswelling of both knee joints (Fig. 2,3). All theseepisodes occurred day before her examinations.
Her physical examination revealed tendernesson all the affected joints, and laboratory reports,ESR-45 mm/h, CRP- 11.2, CBC- 11,200 rest allother haematological and rheumatological testswere normal. Intralesional injection of steroid wasgiven in both the knee joint along with that tabprednisolone in the low dose of 20 mg/day wasstarted, ecchymosis and swelling resolved over theperiod of 1 week. Paediatrician suspecting thepsychogenic cause referred the patient to the childand adolescent psychiatry OPD. Detailed work upwas done and found that girl was a high achieverthroughout her school life with traits of avoidantpersonality. In order to confirm the diagnosis of autoerythrocyte sensitization syndrome, an intradermalskin test was performed in which 0.1 ml of washederythrocyte and normal saline was injected ascontrol, test came to be positive with ecchymoticlesion was observed over the area injected withwashed erythrocyte. Although negative test resultdoes not rules out the diagnosis.9 On the basis ofthis test and clinical history diagnosis of ASS wasmade. Treatment was started in the form ofpsychotherapy and pharmacotherapy. Cognitivebehaviour therapy and SSRI was started in the formof escitalopram 10 mg/ daily, with mild anxiolyticclonazepam 0.25 mg on SOS basis.
One month later patient again came to the OPD

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 423
with sharp cut lesions over her left ankle, as per thepatient they appeared by themselves (Fig. 4). Onquestioning from the mother she said “I do not knowhow they appeared, although she does mentionedthat she found a broken glass in her room nextmorning”. These lesions appeared overnightwithout any previous history of such lesions. Sametreatment was continued and in the last 6 monthspatient had no such episodes.
Patient was having history of polycystic ovariandisease, diagnosed 1 year back. On further inter-viewing history of panic attacks, mild depressionwas found in the last one year. Traits of avoidantpersonality were also found in the patient.
age group also.3,4 Bruises can develop anywhere onthe body but are usually located on extremities.There is usually a prodrome of warmth and pain atthe bruising site, or systemic symptoms such asheadache, nausea or vomiting. Organic factors areseldom identified. Skin biopsy has never beenconclusive and is considered an unreliable methodfor the diagnosis of psychogenic purpura. However,biopsies have revealed extravascular erythrocytesin the dermis, edema, and nonspecific lympho-histiocytic infiltration around the blood vessels.Macrophages may also show pigment deposition,predominantly hemosiderin.5
The pathogenesis of ASS remains unknown.Groch et al.6 tried to identify a single biochemicalagent that could be responsible for the characteristicskin lesions. Groch et al proposed phosphatidyl-serine, which could be isolated from the erythrocytemembrane, to the substance causing the disease.However, patients who were injected withphosphatidylserine showed no reaction. Thereafter,most investigators proposed psychosomatic compo-nents to be one of the important contributors
Figure-1
Figure-2
Figure-3
Figure-4
DiscussionAuto erythrocyte sensitization syndrome also
known as Gardner-Diamond syndrome is a rareclinical syndrome of recurrent bruising or bleeding,usually following a physical or psychosocial stress.It most commonly affects women but certain caseshas been reported in the children and adolescent

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society424
eventually leading to the outbreak of the disease.Agle and Ratnoff suggested that ASS might be apsychophysiological entity, in which the reactionsto psychosomatic instabilities involve the autono-mic nervous system, and is a way of relievinganxiety.7 Such psychosomatic instabilities includeemotional stress, hysteria, and masochism, whichtended to erupt and become more severe during thecourse of disease, while antipsychotic drugs, anti-depressants or psychotherapy often helpful.
In this patient along with the ASS, we werealso suspecting the diagnosis of Dermatitis arte-facta, Because of the typical “hollow history”sudden appearance of complete lesions with littleor no prodrome. “la belle indifference” patient wasnot at all worried upon the appearance of newlesions over her sole, she did not reported anyanxiety, pain, or apprehension associated with thelesion.1
TreatmentThere is no specific treatment for ASS, several
approaches including antihistamines, cortico-steroids, antidepressants, hormones, and vitaminuse have met with variable success.8 We have optedfor the combined approach psychotherapy andpsychopharmacological.
Psychotherapy on the principles of cognitivebehaviour therapy was started. Psychoeducationabout the relationship between her symptoms andher thoughts and emotions. Introducing thecognitive emotional model. Helping her trackingher negative thoughts (NATs). Neuro linguisticprogramme (NLP) for eliminating/rationalising thisbelief.
Antidepressant in the form of escitalopram 10mg daily dosing, with mild benzodiazepine in theform of clonazepam 0.25 mg SOS basis. Patientperforming very well on this dual mode of therapy.Currently asymptomatic since 6 months without anysimilar episodes.
ConclusionAuto erythrocyte sensitization syndrome is a
rare condition that should be considered in a
differential diagnosis of conditions in whichunexplained ecchymosis or purpuric lesions arenoticed and no apparent identifiable cause is known.ASS could produce a diagnostic dilemma and thusrequires thorough investigation. Proper diagnosisof ASS could save many unnecessary procedures.The role of stress in ASS should not be ignored.Complete psychodermatologic evaluation and theliaison between dermatology, primary care, andpsychiatry are of vital importance for the manage-ment of these conditions.
References1. Rook/Wilkinson/Ebling Text book of Derma-
tology, UK: Wiley-Blackwell 1998; 4(6) : 2800-2804.
2. Gardner EH and Diamond LK: auto erythrocytesensitization a form of purpura producingpainful bruising following autosensitization tored blood cells in certain women. Blood 1955;10 : 675-690.
3. Ratnoff OD. Psychogenic purpura (autoerythrocyte sensitization): an unsolveddilemma. Am J Med Sep 1, 1989
4. Campbell AN, Freedman MH, McClure PD.Autoerythrocyte sensitization. J Pediatr 1983;103 : 157-60.
5. Meeder R, Bannister S. Gardner-Diamondsyndrome: difficulties in the management ofpatients with unexplained medical symptoms.Paediatr Child Health 2006 Sep; 11(7) : 416-419.
6. Groch GS, Finch SC, Royoway W, et. al.Studies in the pathogenesis of auto erythrocytesensitization syndrome. Blood 1966; 28 : 19-33.
7. Agle DP, Ratnoff OD. Purpura as a psycho-somatic entity. Arch Intern Med 1962; 109 :89-98.
8. Settle EC. Jr Auto erythrocyte sensitizationsuccessfully treated with antidepressants.JAMA 1983; 250(130) : 1749-1750.
9. Stocker WW, McIntyre OR, Clendenning WE.Psychogenic purpura. Arch Dermatol 1977;113(5) : 606-609.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 425
First Episode Mania after Traumatic Brain InjurySheetal Tripathi, Anju Agarwal, A.Q. Jilani, Shantanu Bharti
Department of psychiatry, Era’s Lucknow Medical College & Hospital, Lucknow-226003Contact: Anju Agarwal, E-mail: [email protected]
Case Report
IntroductionMood disorders are the common outcome of
Traumatic Brain Injury (TBI), among which maniais the most problematic consequence accounting for1-9%.1 Despite the common occurrence, there ispaucity of literature supporting the diagnosis andpharmacological management of psychiatricsequelae of TBI. Even the neurobehavioral guide-line working group members has not establishedthe definitive treatment standards.2 Various casereports, and studies on mania post-TBI havedemonstrated successful treatment with moodstabilizers such as valproate, lithium, carba-mazepine, and antipsychotics like haloperidol,olanzapine, and quetiapine.1 Despite the fact thatthese agents improve the post traumatic manicsymptoms, such patients are at risk of early sideeffects and also may not recover completely.Hereby, we are reporting a case of 54-year-old male,who had first episode of mania post TBI.
Case ReportOur patient Mr. A, 54-year-old man with no
previous history of psychiatric or neurologicaldisease was involved in a road traffic accident andunderwent traumatic brain injury.
The patient was admitted to intensive care unitof a tertiary hospital. The immediately done CT scanrevealed hemorrhagic contusion in both frontallobes, more in right side with linear undisplacedfracture of right parietal bone. He recovered con-sciousness after 2 days followed by a delirious statefor next 7 days. Patient was discharged after 2 weeks
of hospitalization in satisfactory condition onPhenytoin 300 mg per day. During the recoveryperiod patient was oriented, but had memoryproblems in the form of no recall of his accidentand impaired immediate memory. Within 6 weekspost trauma, Patient’s family members observed thathe had become over-talkative, excessively irritableand suspicious towards family members withdisturbed sleep. There were frequent episodes ofaggression and assaultivness. He was referred toneuropsychiatry outpatient department (OPD) ofEra’s Lucknow medical college and hospital, forfurther evaluation of these psychiatric symptoms.
At the initial psychiatric evaluation patient hadincreased psychomotor activity and pressuredspeech. His mood was markedly irritable. He hadbig questionable plans with delusion of grandiosityand delusion of persecution towards family alongwith decreased need for sleep. There was noperceptual abnormality. His immediate and recentmemory was impaired together with impairedabstract thinking and judgment abilities. His insightwas absent regarding his symptoms.Young maniarating scale (YMRS) and Mini mental stateexamination (MMSE) scores were 48 and 21respectively. His investigations, including completeblood counts, kidney function tests, liver functiontests, blood sugar, serum electrolytes, thyroidfunction tests, and serum vitamin B12 were carriedout and all were within normal range. Magneticresonance imaging of the brain (MRI) performed 6weeks after head trauma, revealed chronic bleed inright frontal region with gliosis, chronic contusion

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society426
in bilateral temporal regions, mild cerebral atrophywith ischemic demyelination.
On admission the patient was started ondivalproex 500 mg per day, olanzapine 7.5 mg perday with Lorazepam 1mg per day. Dose ofdivalproex and olanzapine was gradually titratedup to 1500 mg per day and 15 mg per dayrespectively with Lorazepam 2 mg per day. Thepatient showed improvement in his symptoms overa period of next 3 weeks, he became co-operative,and was no longer aggressive or violent. His psycho-motor activity improved, mood was elevated andthere was improvement in delusion of persecutionagainst family members. However, patient stillharbored delusion of grandiosity with big plans andhad disturbed sleep. Patient developed severehyperphagia and fine tremors on the treatment;hence he was shifted from olanzapine to quetipainewith starting dose of 50 mg per day which wasgradually increased up to 300 mg per day. Patientresponded on this treatment and at the time ofdischarge, his YMRS was 18 and MMSE scoreimproved to 23. After 2 weeks of discharge, on hisfollow up patient had shown further improvementin his manic symptoms. He is being followed upfor management in subsequent OPD visits.
DiscussionIn our case, TBI had temporal co-relation with
emergence of manic symptoms. There was absenceof evidence to suggest an alternative cause of mentalsyndrome such as strong family history, past historyof psychiatric illness or any substance abuse.Furthermore these symptoms persisted throughoutthe day without any fluctuation and absence of anyclouding of consciousness. Therefore the diagnosisof “other mental disorders due to brain damage anddysfunction and to physical disease – organic mooddisorder” as per ICD-10 DCR was established inthis case.3
TBI attributes to heterogeneous pathology suchas cerebral contusion, hemorrhage, and diffuseaxonal injury. Our case had lesion in right frontaland bi-temporal region with diffuse cerebral atrophyleading to emergence of mania and cognitivedecline. A number of neuroimaging-basedresearches signified that manic symptoms arecorrelated with greater right than left hemisphereprefrontal and subcortical impairment.4 Study done
by Starkstein et al revealed that patients with maniahave significantly higher frequency of corticallesions mainly involving right orbitofrontal andright inferior temporal cortex. 5 In addition,Structural lesions in frontal temporal lobe alsosupports the finding of impaired attention andanterograde amnesia, as diffuse lesion in thesecortex effects the long-term storage of memory.6
These reports are in concordance with the findingsof our case and therefore explain the developmentof psychiatric consequences in the form of maniaand cognitive deficit after TBI in this patient.
In the management of Mania secondary to TBI,Valproate and Olanzapine has been used as first lineof treatment in various case studies.7,8 Hence westarted our patient on divalproex and olanzapine.Over the course of treatment, patient improved butside effects were reported on increment ofolanzapine and patient was switched toquetiapine.The drug was chosen as it has antimanic action withlow frequency of motor side effects and welltolerated efficacy. Oster et al reported improvementin post-traumatic mania with quetiapine mono-therapy without producing adverse cognitive, motoror functional impairments.9 Similarly, Kim andBijlani in their open label study support the use ofquetipaine for both mania and cognition.10
In conclusion, trauma induced mania isassociated with injuries to the right cerebral hemi-sphere. Even though standard anti manic treatmentscan be beneficial for the management of posttraumatic mania, these agents may producetreatment limiting motor and cognitive side effectsamong patients of TBI. Therefore, this reflects theneed for a gradual increase in dose and carefulmonitoring of adverse effects of drugs in patientswith TBI.
References1. Cittolin-Santos GF, Fredeen JC, Cotes RO. A
Case report of Mania and Psychosis FiveMonths after Traumatic Brain InjurySuccessfully Treated Using Olanzapine. CaseRep Psychiatry 2017; Article ID 7541307.https://doi.org/10.1155/2017/7541307.
2. Warden DL, Gordon B, McAllister TW, et al.Guidelines for the Pharmacologic Treatment ofNeurobehavioral Sequelae of Traumatic BrainInjury. J Neurotrauma 2006; 23 : 1468-1501.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 427
3. The ICD-10 classification of mental andbehavioral disorders = ICD-10: diagnosticcriteria for research Geneva: World HealthOrganization 1993.
4. Blumberg HP, Stern E, Martinez D, et al:Increased anterior cingulate and caudateactivity in bipolar mania. Biol Psychiatry 2000;48 : 1045–1052.
5. Starkstein SE, Fedoroff P, Berthier ML, et al:Manic–depressive and pure manic states afterbrain lesions. Biol Psychiatry 1991; 29 : 149–158.
6. W moyra OL, Zangwill. Memory defects afterhead injury. J Neurol Neurosurg Psychiatry1952; 15 : 54-58.
7. Masodkar K, Khan S, Traumatic brain injury–induced mania. Prim Care Companion CNSDisord 2015; 17 : 10.4088/PCC.14l01749.
8. Zincir SB, Izci F, Acar G. Mania secondary totraumatic brain injury: A case report. JNeuropsychiatr Clin Neurosci 2014; 26 : E31.
9. Oster TJ, Anderson CA, Filley CM, et al.Quetiapine for mania due to traumatic braininjury, CNS Spectrums 2007; 12 : 764–769.
10. Kim E, Bijlani M. A pilot study of quetiapinetreatment of aggression due to traumatic braininjury. J Neuropsychiatry Clin Neurosci 2006;18 : 547-549.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society428
Acceptance and Commitment Therapy inReappraisal of Past Events?
Report of Two CasesAarzoo, Archana Kashyap, Ajeet Sidana
Department of Psychiatry, Government Medical College & Hospital (GMCH),Sector- 32, Chandigarh (UT)-160030
Contact: Aarzoo, E-mail: [email protected]
Case Report
IntroductionPost Traumatic Stress Disorder (PTSD) asso-
ciated with sexual assault or abuse makes the victiminternalise a sense of shame and guilt.1 The distressfrom the trauma may be accompanied by conditionslike depression, anxiety, suicidality or obsessivecompulsive disorder.2 Insecure attachments inchildhood also impact the perception of sexualtrauma as it activates withdrawn and avoidant styleof attachment.3 Acceptance and CommitmentTherapy (ACT) is found to be an effective treatmentfor trauma4 and its associated consequences as itdesensitizes the individual by reducing experientialavoidance5 and increasing acceptance;6 conse-quently, improving one’s functioning and qualityof life. The presented cases revealed how processesof acceptance and commitment therapy (ACT) werehelpful in alleviation of manifested symptoms,underlying sense of self-responsibility associatedwith the traumatic event. In addition, mindfulnessand acceptance enhanced interpersonal effective-ness by altering the discrimination perceived in thefamily relations. This resulted in enhancing copingresources as patients started seeking emotionalsupport in family relations that helped in sustainingthe treatment outcome as well as preventing furtherrelapse, as highlighted in the presented cases.
Case No. 1S, 19 years old unmarried female student of
Nursing presented with features of PTSD compris-ing difficulty in falling asleep, decreased concentra-tion, discomfort being touched, fearful in public
transport and interpersonal difficulties for 8 years.The clinical interview revealed history of sexualabuse in 4 years of age on 3-4 occasions by a youngadolescent boy of neighbourhood in the village. Shebecame aware of it during a sex-education programcampaign in school in 5th class. Then onwards shestarted getting flashbacks in the form of nightmares.She was sent to live with her maternal-grandmotherin the City for education at 5 years of age. Sheexcelled in academics but she did not mingle withpeers or family members and mostly stayed aloof.This social withdrawal continued and her flashbacksincreased manifold when she entered course inNursing. The curriculum including anatomy classes,exposure to blood stains, dressing the wounds inprivate parts of patients etc acted as triggers andintensified the flashbacks even during the daycausing significant occupational dysfunction, henceshe sought consultation. The aassessment furtherrevealed that she had anger against parents, stateof helplessness and significant anxiety resulted intointerpersonal avoidance. Cognitive BehaviorTherapy7 was initiated but discontinued as dailythought record worsened the flashbacks anddistress. Then Inter Personal Therapy wasattempted, the formulation8 helped her identify theavoidant attachment style. She discontinued butreturned to the treatment after 6 months with similarcomplaints. She was now more aware and she couldrationalize her thoughts but continued to struggleemotionally. At this point, therapy was resumed andACT was planned. Creative hopelessness andexperiential avoidance in ACT benefitted her to

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 429
understand her anxiety and fear reactions. This wasfollowed by fusion-diffusion, it facilitatedreattribution and reprocessing of the past event.Thereafter, values and committed action was usedalong with the figure-background concept whichimproved her socio-occupational functioning.Lastly, mindfulness practice reduced nightmaresand it enhanced quality of sleep. After a total of 7sessions, she reported significant alleviation insymptoms and improved interpersonalrelationships. She started mingling with friends, herparticipation and interaction with family membersincreased. She also started attending her clinicalposting regularly without anxiety and avoidance.
Case No. 2A, 23 years old unmarried female, Graduate,
employed, hailing from Sikh religion presented withrepetitive thoughts of hands being dirty and hair-
anxiety leading to full blown mental disorders. TheACT processes such as fusion, experientialavoidance and creative hopelessness were used; andthe belief system operating behind these wasexplained. She was made to view the victim andperpetrator objectively through observing self ratherthan thinking and critical self, this significantly ledto decreased self-blame. Her beliefs were addressedusing processes of diffusion and self as a context.Use of committed actions decreased avoidantbehavior, she started dressing-up well with make-up on and participated in group outings atworkplace. By the 8th session, she reported beingopen to the idea of being in love and she wasconfident to manage new challenges in a foreignland. Therapy was terminated9 educating her aboutrelapse prevention and emphasizing acceptance; theblue print of skills acquired in therapy was revisedand given for practical use.
Table-1: Pre and post assessment scores on measures of symptoms and functioning
Measures Case No. 1 Case No. 2
Pre-ACT Post-ACT Pre-ACT Post-ACT
PCL-C 65 21 75 20High severity Little to no severity High severity Little to no severity
GAF 56 84 50 88Moderate symptoms Absent or minimal Serious symptoms Absent or minimal
symptoms symptoms
Note: PCL-C: PTSD Checklist-civilian version,11 GAF: Global Assessment of Functioning scale.12
ends having mouths leading to repetitive hand-washing and trimming of skull-hair; soughtconsultation due to interpersonal difficulties inconnecting with the opposite sex. Assessmentrevealed two episodes of molestation four yearsback in a span of 2 months, one by her room-mate’smale friend in a movie hall and second by a teacherin the College. This caused disturbance in the formof nightmares and images during the daytime. Herinteraction with family members and peersdecreased, she stayed aloof and wore a shabbyappearance. She was given diagnosis of Post-Traumatic Stress Disorder (PTSD) and Obsessive-Compulsive Disorder (OCD) as per The ICD-10Classification of Mental and Behavioural Disorder:clinical descriptions and diagnostic guidelines2.Treatment comprised of medicines along with 9sessions of ACT. Formulation laid link betweenemotional difficulties and molestation causing fear,
DiscussionIn case No. 1 ACT was a 3rd option of therapy
adopted after 2 models (CBT and IPT) ofpsychotherapy failure, ACT was effective inbringing the outcome in 7 sessions. This knowledgeand experience was used while dealing with asecond case that authors came across and outcomewas evident in 9 sessions. This implies that ACTmight be preferred when talking about trauma intherapy triggers symptoms in patients. This kind ofworsening resulting from treatment may cause drop-out. Thus, ACT might be chosen as an option whenfaced with similar challenges.
The common factor in both cases wasinterpersonal difficulties resulting from unwantedsexual experiences in the past. Also, emotionalneglect was reported in both the cases, case # 1perceived when she was sent to live with thegrandmother whereas case No. 2 perceived sibling

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society430
rivalry, where she was given clothes, books,stationary of her sister to use making her feelunwanted. ACT through ‘self as a context’ providedunderstanding of the role of contextual factors bycreating new perceptions using principle of hereand now. The past childhood experiences werereappraised and viewed as a safety measure solutionin case No. 1 and way to deal with financialconstraints in family in case No. 2.
The age at which of sexual abuse or assaulttakes place might also determine the degree of itsimpact on the victim. This is to be explored if typeof trauma and psychological symptoms areinfluenced by cognitive maturation of the victim10.ACT altered cognitive processing frameworkresulting in improvement in symptoms andinterpersonal relationships. It facilitated in dealingwith the abuse and its consequences in later life aswell as neglect perceived in interpersonalrelationships. Early attachments, if regained, canbe a protective factor1 for one’s mental health. Thereprocessing and desensitization that appearedfollowing experiential avoidance and creativehopelessness decreased the autonomic symptomsand self-blame3. Improvement sustained up to 28months and 18 months follow-up in both casesrespectively. The objective outcome measures usedalso showed decreased disturbance and improvedlevel of functioning, shown in table1.
ConclusionThe processes of ACT resulted in reprocessing
of past experiences by altering cognitions associatedwith perceived discrimination and traumatic eventin both the cases. The increased cordiality in familyrelations, a protective factor, which enhancedcoping and; social and emotional support byimproving mental health and well-being.
References1. Ginzburg K, Butler L, Davis J G, Cavanaugh
CE, Neri E, Koopman C, Classen CC, SpiegelD. Shame, Guilt, and Posttraumatic StressDisorder in Adult Survivors of ChildhoodSexual Abuse at Risk for Human Immuno-
deficiency Virus. J Nerv Men Dis 2009; 197 :536-42.
2. World Health Organization. The ICD 10 Classi-fication of Mental and Behavioural Disorder:clinical descriptions and diagnostic guidelines:tenth revision, 2nd ed. Geneva: World HealthOrganization 2004.
3. Boykina DM, Himmericha SJ, Pinciottia CM,Miller LM, Lynsey R, Miron LR, Orcutt HK.Barr iers to self-compassion for femalesurvivors of childhood maltreatment: The rolesof fear of self-compassion and psychologicalinflexibility. Child Abuse Negl 2018; 76 : 216-224.
4. Hayes SC, Follette VM, Linehan M. Mindful-ness and acceptance: Expanding the cognitive-behavioral tradition. New York, NY: GuilfordPress 2004.
5. Orsillo SM, Batten SV. Acceptance andcommitment therapy in the treatment of posttraumatic stress disorder. Behav Modif 2005;29 : 95-121.
6. Follette V, Palm KM, Pearson AN. Mindfulnessand trauma: implications for treatment. J RatEmo Cogn Behav Therap 2006; 24(1) : 45-61.
7. Freeman A, Pretzer J, Fleming B, Simon KMClinical applications of cognitive therapy. NewYork and London: Plenum Press 1990.
8. Stuart S, Robertson M. Interpersonal psycho-therapy a clinician’s guide. London: Arnold2003.
9. Wolberg LR. The technique of psychotherapy.New York: Grune & Stratton 1977.
10. Bremner JD. Traumatic stress: effects on thebrain. Dialogues Clin Neurosci 2006; 8 : 445-461.
11. Holliday R, Smith J, North C, Surís A. Develop-ing the PTSD Checklist-I/F for the DSM-IV(PCL-I/F): Assessing PTSD SymptomFrequency and Intensity in a Pilot Study of MaleVeterans with Combat-Related PTSD. BehavSci 2015; 5 : 59–69.
12. American Psychiatric Association Diagnosticand statistical manual of mental disorders. (4thed., Text Revision). Washington, DC 2000.

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 431
Interesting ArticlesBritish Journal of Psychiatry
• Dietary intake of people with severe mental illness: systematic review and meta-analysis.Teasdale SB, et al. May 2014; 251-259.
• Self-management interventions for people with severe mental illness: systematic review andmeta-analysis. Melanie Lean M, et al, Mat 2014; 260-268.
• The neuroscience of attachment: implications for psychological therapies. Holmes J, SladeA. 2019 June 214; 318-319.
• Mood stabilisers and risk of stroke in bipolar disorder. Pao-Huan Chen, et al. July 2019; 215: 409-414.
• Repetitive transcranial magnetic stimulation in non-treatment-resistant depression.Maximilian Kiebs, et al. 2019 August; 215 : 415-416.
• Off-label use of ketamine for treatment-resistant depression in clinical practice: Europeanperspective. López-Díaz A, et al. 2019 August; 215 : 447-448.
• Association between particulate matter air pollution and risk of depression and suicide:systematic review and meta-analysis. Xuelin Gu, et al. 2019 August; 215 : 456-467.
• Sodium valproate in psychiatric practice: time for a change in perception. Owens DC. 2019September; 516-518.
Journal of Clinical Psychiatry• The Prevalence of Anxiety Disorders During Pregnancy and the Postpartum Period: A
Multivariate Bayesian Meta-Analysis. Fawcett EJ, et al. J Clin Psychiatry 2019; 80(4) : 18r12527.• Treatment-Resistant Schizophrenia: A Brief Overview of Treatment Options. Faden J. J Clin
Psychiatry 2019; 80(4) : 18ac12394.• The Effect of Antipsychotic Treatment on Recurrent Venous Thromboembolic Disease: A
Cohort Study. Ferraris A, et al. J Clin Psychiatry 2019; 80(5) : 18m12656.• Medical Marijuana: What Physicians Need to Know. Rajiv Radhakrishnan R, et al. J Clin
Psychiatry 2019; 80(5) : 18ac12537.American Journal of Psychiatry
• A Word to the Wise About Intranasal Esketamine. Schatzberg AF. 2019 June;176 : 422–424.• Correlates of Future Violence in People Being Treated for Schizophrenia. Buchanan A, et al.
2019 September; 176 : 694–701.Asian Journal of Psychiatry
• Gaming- a bane or a boon-a systematic review. John N, et al. 2019 April; 42 : 12-17.• Metabolic syndrome and substance use: A narrative review. Kuppili PP, et al. 2019 May; 43 :
111-120.• Mindfulness and hemodynamics in Asians: a literature review. Choo CC, et al. 2019 August;
44 : 112-118.Indian Journal of Psychiatry
• Measuring reliability and validity of “Stressometer®”: A computer-based mass screeningand assessment tool for evaluation of stress level and sources of stressors. Vohra S, et al,2019; 61 : 218.
• The extent and nature of coverage of mental health issues in printed media in India. MohandassB, et al. 2019; 61 : 496.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society432
Forthcoming Events
• Delhi Psychiatric Society 29th Annual Conference 2019, December 22, 2019, Roseate House, Aerocity,New Delhi-110037.
• Autism Spectrum Condition Masterclass 2020, January 9, 2020 - Handforth, wilmslow, United Kingdom
• 18th Annual Mild Cognitive Impairment Symposium, Special Topic Workshop & Alzheimer’s PublicForum 2020, January 18, 2020 - January 19, 2020, North Miami, United States
• RAC2020 — 1st Regional Autism Conference, 24 January 2020 - 26 January 2020 • Muscat, Oman
• Indian Psychiatric Society 72nd Annual National Conference 2020, January 22, 2020 - January 25,2020, Kolkata, India
• American College of Psychiatrists Annual Meeting 2020, February 19, 2020 - February 23, 2020, FortLauderdale, Florida, United States.
• Mayo Clinic Psychiatry Clinical Updates 2020, February 25, 2020 - February 28, 2020, Koloa, Hawaii,United States
• Young Adults with Chronic Conditions: Optimizing Treatment and Transition from Pediatric to AdultCare 2020, March 2, 2020 - March 4, 2020, Cambridge, MA, United States.
• Drugs for Medical Conditions: The Annual Practical Update for the Psychiatrist 2020, March 5, 2020- March 5, 2020, London, United Kingdom.
• British Neuropsychiatry Association 33rd Annual General Meeting 2020, March 5, 2020 - March 6,2020, London, United Kingdom
• American Psychosomatic Society 78th Annual Scientific Meeting 2020, March 11, 2020 - March 14,2020, Long Beach, United States.
• International Family Therapy Association World Family Therapy Congress 2020, March 12, 2020 -March 14, 2020, Basel, Switzerland.
• American Association for Geriatric Psychiatry 33rd Annual Meeting 2020, 13 March 2020 - 16 March2020 • San Antonio, United States.
• American Neuropsychiatric Association 31st Annual Meeting 2020, March 18, 2020 - March 21, 2020Philadelphia, Pennsylvania, United States.
• 3rd International Congress on Evidence Based Mental Health: From Research to Clinical Practice2020, March 18, 2020 - March 22, 2020, Ioannina, Greece.
• Anxiety and Depression Association of America 40th Annual Conference 2020, March 19, 2020 -March 22, 2020, San Antonio, United States.
• Current Psychiatry / American Academy of Clinical Psychiatrists Psychiatry Update 2020, March 26,2020 - March 28, 2020, Chicago, United States.
• 28th European Congress of Psychiatry 2020, March 28, 2020 - March 31, 2020, Madrid, Spain thePyschiatry Talks — the Talks on Psychiatry and Mental Health, 02 April 2020 - 03 April 2020 • SanAntonio, Texas, Usa, United States

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 433
• Schizophrenia International Research Society Conference 2020, April 4, 2020 - April 8, 2020, Florence,Italy.
• 12th International Congress on Psychopharmacology & 8th International Symposium on Child andAdolescent Psychopharmacology 2020, April 15, 2020 - April 18, 2020, Antalya, Turkey
• American Academy of Psychodynamic Psychiatry and Psychoanalysis 64th Annual Meeting 2020,April 23, 2020 - April 25, 2020, Philadelphia, Pennsylvania, United States
• American Academy of Psychoanalysis & Dynamic Psychiatry 64th Annual Meeting 2020, April 23,2020 - April 25, 2020, Philadelphia, United States.
• American Psychiatric Association Annual Meeting 2020, April 25, 2020 - April 29, 2020, Philadelphia,United States
• Association for Death Education and Counselling 42nd Annual Conference 2020, April 28, 2020 -May 2, 2020, Columbus, United States
• World Psychiatric Association Regional Meeting 2020, May 5, 2020 - May 7, 2020, ST Petersburg,Russia
• 27th International Symposium on Controversies in Psychiatry 2020, May 14, 2020 - May 16, 2020,Barcelona, Spain.
• Royal Australian and New Zealand College of Psychiatrists Annual Meeting 2020, May 17, 2020 -May 21, 2020, Hobart, Australia.
• 19th Congress of the WPA Epidemiology & Public Health Section 2020, May 27, 2020 - May 30,2020, Marrakech, Morocco
• West Coast Symposium on Addictive Disorders 2020, May 28, 2020 - May 31, 2020, La Quinta, Ca,United States.
• Gordon Research Seminar — Neurobiology of Drug Addiction, 15 Aug 2020 - 16 Aug 2020 • Newry,Me, United States.
• ECNP — 33rd ECNP Congress, 12 September 2020 - 15 September 2020 • Vienna, Austria
• 12th International Conference on Early Intervention in Mental Health 2020, September 20, 2020 -September 23, 2020, RIO De Janeiro, Brazil.

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society434
Instructions to AuthorsGuidelines
Aims and Scope of the Journal
This journal is aimed to help in the academicdevelopment of its readers. To accomplish theobjectives we publish following sections in thejournal: Original articles, reviews, view points, shortreports, case reports letters and newer developments.
Prior Publication
All the articles are published in this journal withthe understanding that they have never beenpublished or accepted in any journal previously orsubmitted to any other journal simultaneously.However, publication of abstracts in conference’sabstract book will not be considered as priorpublication if such abstracts are limited to 300 words.It includes all kind of printed material (whetherscientific or not), symposia, panel discussion, paper/poster presentation, workshops etc. If author/s aresubmitting any other paper with overlapping contentto any other journal, they must inform the editor withthe explanation of the differences in the paper.
Submission of the manuscriptManuscripts should preferably be submitted
online at the journal’s account: [email protected] or [email protected] of the manuscript will be acknowledgedwithin no more than ten working days, failing whichauthors are free to submit it elsewhere. However, itis advisable that they make sure that the mail hasnot returned and recipient mail-id is filled correctly.Authors who want to submit hard copy ofmanuscripts must send 2 copies along with CD toeditorial office – Department of Psychiatry UCMSand GTB Hospital, Dilshad Garden, Delhi-110095(India).
AuthorshipAll persons designated as authors must qualify
authorship criteria. It implies that all the authors haveparticipated sufficiently to take the publicresponsibility of the content. Authorship credit shouldbe based on substantial contributions to (1)conception and design or analysis and interpretationof data, (2) drafting the article or revising it criticallyfor important intellectual content, and on (3) finalapproval of the version to be published. Conditions1, 2, and 3 must all be met. Participation solely inthe acquisition of funding or the collection of datadoes not justify authorship. Other persons involvedin the study may be acknowledged at the end of themanuscript.
It is the responsibility of the principal author orauthor who is submitting the manuscript to informall the co-authors regarding submission and revisionof manuscript. Editor or society is not responsiblefor any conflict of interest arising out of manuscript.
Conflict of Interest disclosure
While submitting the manuscript authors shouldprovide details regarding conflict of interests in thecovering letter. It involves financial grant for thestudy, paid consultancies, stock ownership or otherequity interests, patent ownership, royalties fromrating scales, inventions, therapy methods, and fundsfor travel. At the Editor’s discretion, this informationmay be shared with reviewers. Such involvementswill not be grounds for automatic rejection of themanuscript.
Copyright transfer
After the receiving of the article is acknow-ledged, authors are expected to submit copyrighttransfer form via regular mail or scanned e-mailwithin next seven working days, failing whichmanuscript could not be processed further. It mayresult in delay in review and hence final decision onthe article. Copyright transfer form is provided and

OCTOBER 2019 DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society 435
it should be signed by all authors. Signature of theco-authors will be responsibility of correspon-dingauthor.
Review ProcessAll the articles will be peer reviewed, and name
of the reviewers and authors will be kept confiden-tial. Authors will be supplied comments of thereviewers along with the decision on the manu-script.
Type of articles and word limit
We publish review articles, original articles, casereports in the field of psychiatry and allied branchese.g., neuropsychiatry, adult psychiatry, childpsychiatry, geriatric psychiatry, psychosomatics,addiction, forensic psychiatry, newer developmentsetc.
Review articles are invited from the experts ofthe fields only and authors wish to send the reviewarticle must take the written permission of the editorbeforehand. Word limit for review article is 5000words with maximum of 50 references.
Original articles must not exceed 3000 words withmaximum 30 references and should contain originalunpublished research.
Care reports should not exceed 1000 words anda maximum of 10 references.
Setting of ManuscriptsAll the pages must be numbered starting from
title page. The manuscript should be typed on A4size paper with 1 inches margin and should bedouble-spaced. All abbreviations should bementioned when they first appear in the text as wellas on the abstract page below key words.
Title Page
Title page must contain type of article, title andrunning title not exceeding 40 characters on the topof it. In the byline authors name (last name, firstname followed by initials of middle name) and highestacademic qualifications must be mentioned.Department and institution to which the work shouldbe attributed should be mentioned below authorsname.
Following it, name, address, telephone numberand e-mail address of the corresponding author mustbe mentioned.
Total number of words in the text (excluding
abstract and references), total number of tables,figures should be mentioned thereafter.
Any acknowledgement (if any) must be cited atthe bottom of this page.
It must be made sure that following pages doesnot have any information that may disclose theidentity of the authors/institution to which the workis attributed.
Second pageIt should contain title of the manuscript, abstract
and at least three key words. Abstract should bestructured in following sections: introduction;objectives, method, results and conclusions.
Start each of following section on a separate page.Introduction: State the object of research with
reference to previous work.Methods: Describe methods in sufficient detail
so that the work can be duplicated, or cite previousdescriptions if they are reality available.
Results: Describe results clearly, concisely, andin logical order. We possible give the range, standarddeviation, or mean error, and significance ofdifferences between numerical values.
Discussion: Interpret the result and relate themto previous work in the field.
Tables : All tables must be created using thetable function in a word processor program and alsomust conform to a one - (3.25”) or two-column(6.5”) format. Prepare each table with a title aboveand and any description below the table. Tablesshould be self-explanatory and should not duplicatetextual material. They must be numbered and citedin consecutive order in the text, and must have ashort title. Tables consisting of more than 10 columnsare not acceptable. Previously published tables musthave a signed permission from the publisher andcomplete reference data so that appropriate creditcan be given. Tables must be given after referenceswhile sending the manuscript.
Figure : As far as possible, figures should beblack and white. They should contain title and shouldbe numbered. They should be mentioned in textaccording to their number.
References: Delhi Psychiatry Journal complieswith the reference style given in “UniformRequirements for Manuscripts Submitted toBiomedical Journals” (see Ann Intern Med 1997;126 : 36-47 or online at http://www.acponline.org).

DELHI PSYCHIATRY JOURNAL Vol. 22 No. 2 OCTOBER 2019
Delhi Psychiatry Journal 2019; 22:(2) © Delhi Psychiatric Society436
References should be cited in Vancouver style inthe manuscript. In the text they should be cited bysuperscript Arabic numerals and in references theyshould be cited in the order of their appearance inthe text. First 3 authors should be cited (followedby et al. if more than 3 authors and their nameshould be in following sequence: Last namefollowed by initials of first and middle names. Eachauthor’s name should be separated by comma. Itshould be followed by title of manuscript, journal’sname as cited in index medicus, year of publication,volume, issue and page number.
For clarification see following reference styles.
Sample citationsAccording to our previous work,1,3-8,19
The Patient’s were studied as follows.3,4
Sample References• Articles
1. Roest AM, Zuidersma M, de Jonge P. Myo-cardial infarction and generalised anxietydisorder : 10-year follow up. Br J Psychiatry2012; 200 : 324–329.
2. Bremner JD, Shearer KD, McCaffery PJ.Retinoic acid and affective disorders: Theevidence for an association. J Clin Psychiatry2012; 73 : 37–50.
• Book1. Stahl SM. The Prescriber’s Guide (Stahl’s
Essential Psychopharmacology, 4th ed. Cam-bridge, U.K.: Cambridge University Press,2011.
• Chapter of a book1. Blacker D. Psychiatric Rating Scales In:
Sadock BJ, Sadock VA, editors. Kaplan andSadock’s Comprehensive Text Book ofPsychiatry. Vol. I. Philadelphia: LippincottWilliams and Williams; 2000. pp 755-782.
Personal communication and unpublished datashould not be used for the reference.
ProofingAfter acceptance, paper will be sent to authors
for proof reading. It is the responsibility of the authorsto check the proof and return them within threeworking days. At this stage content of the manuscriptcan not be changed. Failure to send proofs in duetime may result in delay in the publication ofmanuscript.
The Journal Can be accessed from :
Website:http://www.medIND.nic.in
http://www.delhipsychiatricsociety.com
Kindly send your submissions by :E-mail to : [email protected]
Journal (2007 onwards) is indexed by :
medIND.nic.in(Biographic Informatics Division)
National Informatics Centre(Department of Information Technology)
A-Block, CGO Complex, Lodhi Road,New Delhi-110003, India
Journal is lndexed in• Google Scholar• medIND (Indian Medlar by National
Informatic Centre; a project of ICMR, Govt.of India)
• Index Medicus (by WHO for South EastAsia Region)
• Indian Science Abstracts• k-hub.in• UGC List of Periodicals
Journal is indexed in
INDEX COPERNICUS(ICV 2016 = 70.93)(ICV 2017 = 84.45)(ICV 2018 = 88.70)