
Occurrence of Tertiary Lymphoid Tissue Is Associated with T ......Giuseppe Di Caro 1, Francesca...
13
Imaging, Diagnosis, Prognosis See related article by Taube, p. 2023 Occurrence of Tertiary Lymphoid Tissue Is Associated with T-Cell Infiltration and Predicts Better Prognosis in Early-Stage Colorectal Cancers Giuseppe Di Caro 1 , Francesca Bergomas 1 , Fabio Grizzi 1 , Andrea Doni 1 , Paolo Bianchi 3 , Alberto Malesci 2 , Luigi Laghi 2,3 , Paola Allavena 1 , Alberto Mantovani 1,4 , and Federica Marchesi 1,4 Abstract Purpose: Tumor-infiltrating T lymphocytes (TIL) play a key role in the clinical outcome of human colorectal cancer; however, the dynamics of their recruitment along colorectal cancer clinical progression have not been fully elucidated. Tertiary lymphoid tissue (TLT) is an ectopic organized lymph node–like structure that typically forms at sites of chronic inflammation and is involved in adaptive immune responses. Its occurrence in cancer is sporadically documented and its role and clinical relevance is largely unknown. Experimental Design: The occurrence of TLT, the correlation with TILs, and the clinical relevance were evaluated retrospectively, in a cohort study involving a consecutive series of 351 patients with stage II and III colorectal cancer. The role of TLT in lymphocyte recruitment was assessed in a preclinical model of colorectal cancer. Results: In both human colorectal cancer and in a murine model of colorectal cancer, we identified organized TLT, highly vascularized (including high endothelial venules), and correlated with the density of CD3 þ TILs. Intravenous injection in mice of GFP splenocytes resulted in homing of lymphocytes to TLT, suggesting an active role of TLT in the recruitment of lymphocytes to tumor areas. Accordingly, TLT density and TIL infiltration correlated and were coordinated in predicting better patient’s outcome among patients with stage II colorectal cancer. Conclusions: We provide evidence that TLT is associated with lymphocyte infiltration in colorectal cancer, providing a pathway of recruitment for TILs. TLT cooperates with TILs in a coordinated antitumor immune response, when identifying patients with low-risk early-stage colorectal cancer, thus, representing a novel prognostic biomarker for colorectal cancer. Clin Cancer Res; 20(8); 2147–58. Ó2014 AACR. Introduction Immune infiltration is a fundamental component of solid tumors (1), its involvement in cancer progression being documented by preclinical and clinical studies. The adaptive immune response plays an active role in control- ling cancer growth and dissemination. In fact, T-cell infil- tration correlates with favorable prognosis in various common neoplastic diseases, including colorectal cancer (2–5), emerging as a potential immune biomarker of out- come and promising therapeutic target. In colorectal cancer, tumor-infiltrating lymphocytes (TILs) are associated with favorable prognosis (2–4, 6–8), independently by tumor–node–metastasis (TNM) stage (3, 6, 8), or only in stage II colorectal cancer (4). Surprisingly, despite the documented association between TILs and the clinical outcome, the dynamics of T-cell recruitment and activation along colorectal cancer progression have not been fully elucidated. Tertiary (or ectopic) lymphoid tissue (TLT) is a vascular- ized immune compartment that forms at sites of exacerbat- ed inflammatory reactions and is potentially involved in the promotion of adaptive immune responses (9, 10). Similarly to secondary lymphoid organs, the function of TLT is dependent on its structural organization, with Authors' Affiliations: Departments of 1 Immunology and Inflammation; and 2 Gastroenterology; 3 Laboratory of Molecular Gastroenterology, Humanitas Clinical and Research Center, Rozzano; and 4 Department of Biotechnologies and Translational Medicine, University of Milan, Milan, Italy Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). G. Di Caro and F. Bergomas contributed equally to this work. Corresponding Author: Federica Marchesi, Department of Biotech- nologies and Translational Medicine, University of Milan—Humanitas Clinical and Research Center, Via Manzoni 56 20089 Rozzano, MI. Phone: 39-028-224-5113; Fax: 39-028-224-5101; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-13-2590 Ó2014 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org 2147 on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590
Transcript of Occurrence of Tertiary Lymphoid Tissue Is Associated with T ......Giuseppe Di Caro 1, Francesca...

Imaging, Diagnosis, PrognosisSee related article by Taube, p. 2023
Occurrence of Tertiary Lymphoid Tissue Is Associatedwith T-Cell Infiltration and Predicts Better Prognosis inEarly-Stage Colorectal Cancers
Giuseppe Di Caro1, Francesca Bergomas1, Fabio Grizzi1, Andrea Doni1, Paolo Bianchi3,Alberto Malesci2, Luigi Laghi2,3, Paola Allavena1, Alberto Mantovani1,4, and Federica Marchesi1,4
AbstractPurpose: Tumor-infiltrating T lymphocytes (TIL) play a key role in the clinical outcome of human
colorectal cancer; however, the dynamics of their recruitment along colorectal cancer clinical progression
have not been fully elucidated. Tertiary lymphoid tissue (TLT) is an ectopic organized lymph node–like
structure that typically forms at sites of chronic inflammation and is involved in adaptive immune
responses. Its occurrence in cancer is sporadically documented and its role and clinical relevance is largely
unknown.
Experimental Design: The occurrence of TLT, the correlation with TILs, and the clinical relevance were
evaluated retrospectively, in a cohort study involving a consecutive series of 351 patients with stage II and III
colorectal cancer. The role of TLT in lymphocyte recruitmentwas assessed in a preclinicalmodel of colorectal
cancer.
Results: In both human colorectal cancer and in a murine model of colorectal cancer, we identified
organized TLT, highly vascularized (including high endothelial venules), and correlated with the density of
CD3þ TILs. Intravenous injection in mice of GFP splenocytes resulted in homing of lymphocytes to TLT,
suggesting an active role of TLT in the recruitment of lymphocytes to tumor areas. Accordingly, TLT density
and TIL infiltration correlated and were coordinated in predicting better patient’s outcome among patients
with stage II colorectal cancer.
Conclusions: We provide evidence that TLT is associated with lymphocyte infiltration in colorectal
cancer, providing a pathway of recruitment for TILs. TLT cooperates with TILs in a coordinated
antitumor immune response, when identifying patients with low-risk early-stage colorectal cancer,
thus, representing a novel prognostic biomarker for colorectal cancer. Clin Cancer Res; 20(8); 2147–58.
�2014 AACR.
IntroductionImmune infiltration is a fundamental component of
solid tumors (1), its involvement in cancer progressionbeing documented by preclinical and clinical studies. The
adaptive immune response plays an active role in control-ling cancer growth and dissemination. In fact, T-cell infil-tration correlates with favorable prognosis in variouscommon neoplastic diseases, including colorectal cancer(2–5), emerging as a potential immune biomarker of out-come and promising therapeutic target. In colorectalcancer, tumor-infiltrating lymphocytes (TILs) are associatedwith favorable prognosis (2–4, 6–8), independently bytumor–node–metastasis (TNM) stage (3, 6, 8), or only instage II colorectal cancer (4). Surprisingly, despite thedocumented association between TILs and the clinicaloutcome, the dynamics of T-cell recruitment and activationalong colorectal cancer progression have not been fullyelucidated.
Tertiary (or ectopic) lymphoid tissue (TLT) is a vascular-ized immune compartment that forms at sites of exacerbat-ed inflammatory reactions and is potentially involved inthe promotion of adaptive immune responses (9, 10).Similarly to secondary lymphoid organs, the function ofTLT is dependent on its structural organization, with
Authors' Affiliations: Departments of 1Immunology and Inflammation;and 2Gastroenterology; 3Laboratory of Molecular Gastroenterology,Humanitas Clinical and Research Center, Rozzano; and 4Departmentof Biotechnologies and Translational Medicine, University of Milan,Milan, Italy
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
G. Di Caro and F. Bergomas contributed equally to this work.
Corresponding Author: Federica Marchesi, Department of Biotech-nologies and Translational Medicine, University of Milan—HumanitasClinical and Research Center, Via Manzoni 56 20089 Rozzano, MI. Phone:39-028-224-5113; Fax: 39-028-224-5101; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-13-2590
�2014 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 2147
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

B-cell follicles, T-cell areas, and specialized hematic andlymphatic vessels, suggesting the possibility that it behavesas a functional immune site (11, 12). TLT is found in theinflamed area of several autoimmune diseases (13), chronicinflammatory conditions (14–16), and some tumor types(17–21). In these clinical settings, TLT improves the adap-tive immune response to persisting antigens expressed inthe target organ (9, 10). In solid tumors, a role for TLTin the organization of the local immune response and inlymphocyte recruitment has been suggested (22), but solidevidence has not been provided yet (23, 24). In humancolorectal cancer, discrete aggregates of lymphocytes at thetumor invasivemargins have been described and referred toas Crohn’s-like reaction (25–27); however, its functionalrole and the connection with the dispersed lymphocyticinfiltrate with prognostic value, also in regard to the type ofgenetic instability, is surprisingly unexplored. Being a par-adigm for the complex relationship between chronicinflammation, T-cell–mediated immunity, and cancer pro-gression (28, 29), colorectal cancer, represents an idealclinical setting to define the association between ectopiclymphoid tissue, a frequent manifestation of chronicinflammatory conditions, and infiltration of T cells withantitumor properties.
As in secondary lymphoid organs, the formation ofTLT relies on few molecular mediators released by resi-dent stromal cells, including members of the lympho-toxin family (30) and lymphorganogenic chemokines(CXCL13 and CCL21), responsible for lymphoid cellrecruitment (30–33). During the process of adult lym-phoid neogenesis, similar molecular mediators and cel-lular interactions induce formation of specialized vessels,including high endothelial venules (HEV) and lympha-tics, which support traffic of lymphocytes from the blood
to lymphoid tissues and lymph nodes (34). The pre-sence of HEV in ectopic tissues indicates the pos-sibility for na€�ve and central memory T lymphocytes tobe recruited, thanks to their expression of L-selectin(CD62L) and its specific binding to peripheral nodeaddressin (PNAd), selectively expressed on HEV (35).In fact, the formation of HEV has been suggested to med-iate rapid recruitment of lymphocytes into chronicallyinflamed tissues, including some tumor tissues (36).
In the present study, we investigated the contribution ofTLT to CD3þ T-cell infiltration in colorectal cancer. In aretrospective cohort study, we identified highly organizedlymphocyte aggregates representing bona fide TLT and wedefined its prognostic relevance with respect to CD3þ T-cellinfiltration and demographics, clinical, and histopatholog-ic variables and their interactions. In a preclinical model ofcolitis-associated colorectal cancer, we functionallyaddressed the question whether TLT is involved in therecruitment of T lymphocytes into colon cancer tissue. Aquantitative analysis, not subjected to estimation of pathol-ogist has not been performed to date for lymphoid tissue incolorectal cancer. Thus, a clinically relevant definition ofTLT in human colorectal cancer is expected to have impor-tant implications in the standardized assessment of lym-phocyte infiltration in human colorectal cancer and in thedesign of clinical trials aimed to test novel immunothera-peutic approaches.
Patients and MethodsPatients
Tissue specimens from 351 stage II and III patientswithout any sign of metastatic disease at diagnosis whoconsecutively underwent radical surgical resection for pT3or pT4 colorectal cancer, were retrieved from the previousseries (4). Patients’ demographics, clinical, and histopath-ologic data were available and obtained from the Institu-tional Intranet; please refer to Supplementary Table S1 forthe list of the variables assessed. The absence ofmetastasis atdiagnosis was assessed in all patients by combining histo-pathologic findings, surgical records, and perioperativeimaging. To study the prediction of disease recurrencesaccording to the state of immune infiltration, patients withpT1 or pT2 colorectal cancer, who have a very low risk ofprogression at diagnosis, and patients with perioperativelydetected metastases were excluded. To exclude potentialconfounders in the study design, stage I patients were notenrolled in the cohort studied for their unlikely occurrenceof disease recurrence, whereas patients with stage IV colo-rectal cancer were not included because they are character-ized by the presence of distant metastasis, which is anoutcome event of our analysis. Patients who underwentneoadjuvant radiotherapy for rectal cancer were excludedfrom the study, because of the possibility of interferencewith the assessment of the local immune response. Che-motherapy treatment was administered and allocated by anonrandom assignment according to adjuvant protocols inuse at the time of surgery.
Translational RelevanceOur findings reveal that tertiary lymphoid tissue
(TLT) is associated with lymphocyte infiltration incolorectal cancer, contributing to tumor-infiltratinglymphocyte (TIL) recruitment; TLT cooperates withTILs in a coordinated antitumor immune responseand in predicting better outcome in patient, thus,representing a novel prognostic biomarker for humancolorectal cancer. Improved understanding of thecomplexity of immune infiltration along the progres-sion of colorectal cancer and the identification ofimmune biomarkers might help in the design of tai-lored immune-based therapeutic approaches, targetingthe immune system according to the stage of disease.The organized accumulation of lymphocytes intoectopic lymphoid tissue in colorectal cancer is a pos-itive prognostic factor and may then represent a targetfor therapeutic intervention in stage II colorectal can-cer, with the aim to stimulate the immune systemagainst tumor progression.
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2148
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

Study designTissue specimens of patients with colorectal cancer
who consecutively underwent radical surgical resectionfor pT3 or pT4 colorectal cancer at the Humanitas Clini-cal and Research Center (Rozzano, Milan, Italy) fromJanuary 1997 to November 2005 were retrospectivelystudied. Investigators who were blinded to the results ofthe morphologic analysis assembled a clinical retrospec-tive database by collecting demographics, clinical, andhistopathologic data from the institutional intranet (Sup-plementary Table S1). These variables, together withthe median values of TLT and TIL IRA (immunoreactivearea), were tested as predictors of the outcome of patient.The outcome of patients who undergo radical resectionof colorectal cancer is a variable affected by an eventdefined as any local tumor recurrences or any metachro-nous distant organ metastases and named disease-freesurvival (DFS). To detect or exclude any postsurgicaltumor recurrences, patients underwent thoracoabdom-inal computed tomography, abdominal ultrasonography,and chest radiography, which were done according tocommon protocols for surveillance. The observation peri-od started immediately after the surgical procedure. Themean follow-up period of the cohort studied was 4.71years (SD ¼ 2.63 years) for DFS. The detection of tumorrecurrence or death was computed from diagnosis untildata were censored on May 30, 2010. To further assessany possible biases, interaction analyses in predicting theprognosis of patient were performed for all the variablesassessed to detect any effect modifier (P < 0.10).
Immunohistochemistry and microsatellite statusFrom each patient enrolled in the study, 2-mm thick
tissue slided from formalin-processed and paraffin-embedded tumor sections were processed for immuno-histochemistry. After deparaffinization and rehydration,sections were immersed in an antigen retrieval bath,incubated with 3% H2O2 for 15 minutes. Slides wereautostained (IntelliPATH FLX; Biocare Medical) with pri-mary antibodies raised against CD3 (clone F7.2.38;Dako), CD20 (clone L26; Dako), PNAd (MECA-79; BDPharmingen), Lyve-1 (ab14917; Abcam), CD21 (cloneEP3093; Abcam), a-smooth muscle actin (a-SMA) (clone1A4; R&D Systems), and CXCL13 and CCL21 (AF801 andAF457; R&D Systems). A 30-minute incubation with theDAKO Envision system (Dako) or the Anti-Goat PolymerKit (BioCare) followed. Diaminobenzidine tetrahy-drochloride (Dako) was used as chromogen. Nuclei werelightly counterstained with a freshly made hematoxylinsolution (Medite). Presence of fibrosis was assessed on 2-mm thick sections stained for 20 minutes with 0.1% Siriusred in saturated picric acid (Sigma-Aldrich). The sectionswere further washed in water, mounted, and analyzedunder an optical microscopy. Microsatellite status wasscreened preliminarily for all cancers included in thestudy by testing instability at mononucleotide repeats,as previously described (37, 38). The Ethics Committee ofthe Humanitas Clinical and Research Center approved
the study, and written informed consent was obtained bythe referring physician, at the time of surgery by eachpatient. Slides were digitized using a computer-aidedimage analysis system (Olympus dotSlide).
TLT exhibited a distinct structural organization in colo-rectal cancer, outlined by an area composed of CD3þ cellsand a compartment of CD3-negative lymphoid cells (Bcells). To quantify TLT, an expert pathologist, who wasblinded to any patient clinical data, randomly selected threenoncontiguous microscopic areas located at the tumorinvasive front occupied by TLT. Computer-assisted mea-surement of the selected areas was obtained as the percent-age ratio between TLT area and the total digitized tissuesurface. For each histologic section, the mean valuesobtained in three different regions were calculated and usedfor the subsequent statistical analysis. CD3þ TIL IRA wasquantified as previously described (4).Median values of theoverall distribution of TLT and TIL IRA (2.68% and 2.06%,respectively) were chosen as representative cutoff to per-form statistical analyses.
Statistical analysisThe association between the extent of TLT density and
CD3þ TILs, baseline characteristics and tumor features ofpatient was estimated by Pearson simple linear regressionanalysis. A Cox proportional hazards model was devel-oped to assess the role of TLT density and other demo-graphic, clinical, and histopathologic features, in predict-ing the occurrence of disease-free–specific survival. Timeto follow-up was stopped at the time of the death ofpatient for any case unrelated to colorectal cancer disease,and this case was not considered an event of outcome. Toassess for confounders, COX multivariate analysis wasperformed by entering only variables and their significantinteractions with a P value less than 0.20 at univariateanalysis. Interactions between variables were calculatedby analyzing their multiplicative term in the Cox model.By a backward stepwise elimination approach, nonsig-nificant variables, and their nonsignificant interactions,were removed from the model. Interacting variables atmultivariate analysis (P < 0.10) were then tested forsubgroups analysis accordingly. Differences in medianvalues of TLT density between subsets of colorectal cancerand DFS were tested by the Mann–Whitney U test and bythe Cuzick trend test. Kaplan–Meier curves of DFS wereplotted, whereas the log-rank test was used to comparethe curves of each subgroup of patients with colorectalcancer. For each test, only two-sided P values lower than0.05 were considered statistically significant. All the anal-yses were done using Epi Info (Version 3.4.3), StatsDirectStatistical software (Version 2.5), and GraphPad Prismsoftware (Version 4.1).
Quantification of HEV in human colorectal cancerConsecutive tumor slides from 20 patients with colo-
rectal cancer were stained with antibodies raised againstPNAd. For each tumor slide, the absolute numbers ofPNAd-positive vessels within each intratumoral follicle
Tertiary Lymphoid Tissue in Colorectal Cancer
www.aacrjournals.org Clin Cancer Res; 20(8) April 15, 2014 2149
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

and follicles associated with the normal mucosa werequantified.
Mice and murine models of colorectal cancerEight-week-old C57BL/6J and mice were purchased
from Charles River Laboratories; eGFP/C57Bl/6 mice fromThe Jackson Laboratory. Procedures involving animalsand their care were conformed to institutional guidelinesin compliance with national and international laws andpolicies. Mice were housed in a specific pathogen-free ani-mal facility of the IRCCS Humanitas Clinical and ResearchCenter in individually ventilated cages. In the AOM/DSS(azoxymethane/dextran sodium sulphate) model, micedeveloped adenomas as a result of the combined treat-ment with the carcinogen AOM (10 mg/kg; Sigma-Aldrich)and sequential administration of the mucosal irritantDSS [3 rounds of 2% DSS (MW ¼ 36,000–50,000; MPBiomedicals)] in the drinking water. Adenomas developin the distal colon overtime during the different treatmentsand are evaluated after 10 weeks.
Additional details are included in the SupplementaryMethods.
ResultsHuman colorectal cancer contains aggregates ofT cells with features of TLT
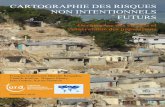
The lymphocytic reaction in colorectal cancer tissuesincludes dispersed TILs and discrete lymphoid aggregates,the latter referred to as Crohn-like reaction (25–27), whichhas not been characterized yet. By staining colon cancerspecimens with an anti-CD3 antibody, we identified aggre-gates of lymphocytes displaying a distinct structural orga-nization, compared with generic clusters of TILs (Fig. 1A).These organized structures had features of TLT, with com-partmentalizedT (Fig. 1B, left) andB (Fig. 1B,middle) areas,sometimes with germinal centers, and a network of CD21þ
follicular dendritic cells (FDC; Fig. 1B, right). Notably, TLTwas often localized at the invasive front of the tumor, instromal regions containing a considerable amount of cellsexpressing a-SMA (Fig. 1C, left), a marker of activatedfibroblast cells usually associated with local inflammato-ry/fibrotic response. The lymphorganogenic chemokinesCCL21 (Fig. 1C, middle) and CXCL13 (Fig. 1C, right) werealso found inside lymphoid tissue, suggesting an activerecruitment of T andB cells andplasticity of these structures.Staining of collagen fibers confirmed the fibrosis surround-ing TLT (Fig. 1D, left). TLT contained PNAdþHEV (Fig. 1D,middle) and Lyve-1–positive lymphatic vessels (Fig. 1D,right), thus, confirming that lymphoid aggregates in humancolorectal cancer have features of TLT.
Density of TLT in human colorectal cancer correlateswith increased density of TILs and associates withincreased number of HEVs
To analyze the relationship between TLT and TILs inhuman colorectal cancer, we systematically evaluated thedensity of TLT in 351 tissue specimens from deeply invad-ing (pT3/pT4) patients with colorectal cancer without
evidence of distant organ metastasis at diagnosis, by stain-ing with an anti-CD3–specific antibody and quantifyingthe area of TLT by computer-assisted image analysis. Wequantified TLT at the invasive front of the tumor, whichrepresents the tumor–host interface (Fig. 1A). Notably, inthe cohort of 351 patients with colorectal cancer, whole-tissue visualization of CD3 infiltration showed a higherdensity of TLT in tumors containing high density of CD3þ
TILs (Fig. 2A, left), compared with tumors containing lowdensity of CD3þ TILs (Fig. 2A, right). In fact, the density ofTLT linearly correlated with the density of dispersed tumor-infiltrating CD3þ T cells (R ¼ 0.32; P < 0.001; Supplemen-tary Table S2; Fig. 2B).
Because lymphoid tissue contained PNAdþ HEVs, spe-cialized vessels with a key role in the traffic of T cells (Fig.1D), we aimed to explain the correlation of TLT and TILs inhuman colorectal cancer, by quantifying the distribution ofHEV in colorectal cancer specimens. HEVs were presentmostly in the context of TLT and very rarely found in thesurrounding tumor tissue. Comparison between lymphoidtissue associated with the normalmucosa (Fig. 2C, left) andTLT at the invasive front of the tumor (Fig. 2C, right)showed an increased number of HEV associated with lym-phoid follicles in the tumor compartment (P < 0.05; Fig.2D), indicating that the process of lymphoid neogenesis inhuman colorectal cancer includes formation of HEV, whichmight allow recruitment of T cells.
Density of TLT associates with a better prognosis inpatients with colorectal cancer
We then investigated the clinical significance of TLT inrelationship with TILs in a retrospective cohort study. Con-sidering the overall cohort, TLT IRA% at the invasive tumorfront ranged from 0% to 23.98%, with a median value of2.68% (second–third quartiles, 0.75%–5.99%). TLT waspresent in 276 (78.6%) of 351 tumors and the distributionwas skewed toward low values. Distributions of TLT accord-ing to the patient histopathologic characteristics aredescribed in Supplementary Table S2. We recorded 84events of colorectal cancer disease relapse (DFS) in 351patients with stage II and III colorectal cancer.
Unadjusted univariate analysis showed that high TLTdensity (�median) significantly correlated with better out-come [HR, 0.62; 95% confidence interval (CI), 0.40–0.97;Supplementary Table S3]. Importantly, to control for con-founders, we performed multivariate Cox analysis thatrevealed an interaction between higher densities(�median) of both TLT and TILs with nodal status inpredicting patients relapse (P ¼ 0.07 and P ¼ 0.03, respec-tively), which suggests that the ability of TLT and TILs topredict patients relapse may change according to nodalstatus (Supplementary Table S3). Therefore, we performeda subgroup analysis revealing that in patients with node-negative colorectal cancer (n ¼ 185), a high density of TLT(�median, 2.68%) and of TILs (�median, 2.06%) wasassociated with better prognosis compared with patientswith a low density of TLT and TILs (log-rank test; P ¼ 0.02and P ¼ 0.02, respectively; Fig. 3A and B, left); conversely,
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2150
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

TLT and TIL densities were irrelevant to predict the prog-nosis of patients with node-positive colorectal cancer (n ¼166; log-rank test; P ¼ 0.46 and P ¼ 0.64, respectively; Fig.3A and B, right). Moreover, we further confirmed that theprognostic behavior of TLT and TILs varies with diseaseextent in a different analysis, performed with continuousvalues. Similarly to TILs (Fig. 3C, right), among patientswith node-negative colorectal cancer, TLT density was sig-nificantly lower in patients who relapsed (n ¼ 26) than inpatientswith no evidence of disease recurrence [n¼159;N0(no relapse) vs. N0 (relapse; P ¼ 0.03; Fig. 3C, left)].Conversely, TLT density did not differ in nodal-positivepatients (N1 andN2)with orwithout tumor recurrence [N1
(no relapse) vs. N1 (relapse; P ¼ 0.43); N2 (no relapse) vs.N2 (relapse; P ¼ 0.15)], thus, behaving as a prognosticbiomarker only in early-stage patients (Fig. 3C, left).
To address the question whether the immune responsecomprising of TLT and TILs has no impact at all in stage IIIcolorectal cancer, we performed a stage-by-stage analysis,showing the ability of nodal status to identify relapses ofpatient with colorectal cancer among subgroups of TLTdensity (Table 1). Similarly to TILs, nodal involvement wasassociated with worst outcome in subgroups of patientswith colorectal cancer with intermediate TLT density(0.1%–4.2%, P ¼ 0.001; 4.2%–8.4%, P ¼ 0.05) but not inpatients with colorectal cancer with very low or very high
Figure 1. Characterization ofaggregates of Tcellswith featuresof TLT in human colorectalcancer. A, a representative imageobtained fromavirtual digital slideof a colorectal tumor specimen.Staining with anti-CD3 antibodyallows identification of the T-lymphocytic reaction, includingthe presence of lymphoidaggregates at the invasive front(asterisks). On the right aremagnifications of the lymphoidaggregates. B, lymph node–likefollicles (dotted lines) in humancolorectal cancer specimens arecomposed of CD3þ T cells (left),CD20þ B cells (middle), andnetworks of CD21þ FDCs (right).Sections in left and middle areconsecutive sections and showthe compartmentalizationbetween B and T cells in thefollicle. C, intratumor lymphoidtissue is prevalently associatedwith tumor stroma, containing–-a-SMA-positive cells (left). Thelymphoid chemokines CCL21(middle) and CXCL13 (right) arepresent inside lymphoid follicles.D, staining with Sirius redevidenced the presence ofcollagen fibers closed to vascularstructures (asterisks; left).Vessels within lymphoid tissueinclude PNAdþ HEV (middle) aswell as Lyve-1þ lymphatic vessels(right), suggesting traffic of naïveand memory lymphocytes.Sections in D middle and rightare consecutive sections,showing HEV and lymphaticvessels in the same follicle. Dotlines indicate follicle contour.Scale bars, 1 mm (A); 200 mm (Band C, left; D, left and right); and100 mm (C, middle and right; D,middle).
Tertiary Lymphoid Tissue in Colorectal Cancer
www.aacrjournals.org Clin Cancer Res; 20(8) April 15, 2014 2151
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

immune values (0%, P¼ 0.16;�8.32%, P¼ 0.33; Table 1).Consequently, only very low and very high TLT densities(0%;�8.32%) were associated with better outcome in bothstage II (P ¼ 0.04) or stage III (P ¼ 0.02) colorectal cancerand might, therefore, operate as stage-independent predic-tors of survival (Table 1).
These results suggest that the prognostic behavior of TLTis similar to that of TILs and prompted us to test which onewas the best prognostic marker. However, because thesebiomarkers identified overlapping populations, whichweremutually dependent in predicting prognosis (data notshown), we developed two stepwise, backward Cox multi-variate analysis models (model A and model B), to testthe independency of their prognostic performance, withrespect to other demographics, clinical, histopathologicfeatures, and microsatellite status in stage II colorectalcancer (Table 2). Model A andmodel B revealed that higherdensities of TLT and TILs are both independent prognosticmarkers of better prognosis in stage II colorectal cancer,compared with other tumor features (Table 2). Resultsobtained so far prompted us to hypothesize that TLT andTILs have a comparable prognostic impact. To better under-stand their prognostic function, we analyzed the correla-tion of TLT and TILs distribution according to disease
progression. Figure 3D showed that TLT correlates withTILs density (�median) only in patients who did notexperience relapse (P ¼ 0.001), but not in those whorelapsed (P ¼ 0.28; Fig. 3D), thus, suggesting that the twobiomarkers are coordinated in mediating the antitumorresponse only among patients with a good prognosis.
Our data have shown that microsatellite instable (MSI)patients with colorectal cancer had a tendency to betterprognosis compared with those with microsatellite stable(MSS) phenotype, althoughnot statistically significant (HR,0.56; 95% CI, 0.27–1.16; P ¼ 0.12; Supplementary TableS3). To further address whether the prognostic value of MSImight differ according to the density of TLT, we performedKaplan–Meier curveswith subgroups analyses (Supplemen-tary Fig. S1). The analysis showed thatMSI colorectal cancerwas not significantly associated with prognosis in bothpatientswith TLTdensity low (<median)or high (�median;P ¼ 0.27; P ¼ 0.36, respectively), thus, being independentvariables in predicting prognosis (Supplementary Fig. S1).
TLT is involved in lymphocyte infiltration in apreclinical model of colorectal cancer
Despite CD3þ T-cell density is recognized as a prog-nostic marker for patients with colorectal cancer (3, 4),
CD3 CD3
PNAd PNAd
A B
C D
P < 0.001r = 0.32
30
20
10
0
0 10 20 30
60
50
40
30
20
10
0Normal Tumor
CD3+ TIL density (%)
HE
V n
umbe
r/T
LTT
LT d
ensi
ty (
%)
*
Figure 2. Correlation of tumor-associated TLT with increased density of T cells and formation of HEVs in human colorectal cancer. A, representativeimages obtained from virtual digital slides of two colorectal tumor specimens with a low (left) and high (right) density of infiltrating T cells and TLT.Staining with anti-CD3 antibody allows identification of lymphoid tissue and infiltrating lymphocytes. Asterisks, lymphoid tissue. B, correlationbetween CD3þ TILs (% IRA) and TLT density (% IRA) in 351 patients with colorectal cancer. A P value by Pearson simple linear regression analysis.C, increased number of HEV associated with TLT in the tumor compartment. Comparison between lymphoid tissue associated with the normalmucosa (left) and TLT at the invasive front of the tumor (right). Quantification of HEV in tumor lymphoid tissue compared with lymphoid folliclesassociated with normal mucosa. HEV were quantified by computer-assisted image quantitative analysis on slides from 20 paraffin-embedded cancertissue specimens stained with anti-PNAd antibody. Bars, number of HEV in each follicle (D). Two-tailed P values by the t test. �, P < 0.05. Scale bars,1 mm (A); and 200 mm (C).
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2152
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

the dynamics of CD3þ T-cell recruitment and activationat the tumor site have not been clarified. The coordina-tion between TLT and TILs in predicting prognosis inhuman colorectal cancer prompted us to better clarifythe association of TLT and T-cell infiltration. We tookadvantage of a preclinical model of inflammation-drivencarcinogenesis (AOM/DSS; ref. 39), which would reca-pitulate the formation of TLT associated with chronicinflammatory conditions (23). Organized accumulationsof lymphoid cells are present in murine colon mucosaof AOM/DSS mice, both adjacent to the normal crypts(Supplementary Fig. S2A, left) and in the tumor region(Supplementary Fig. S2A, right). The aggregates are com-prised of mostly B lymphocytes and include an area ofT cells (Supplementary Fig. S2B) and a network of FDCs(Supplementary Fig. S2C, left). The lymphoid chemokineCXCL13 is expressed at high levels in the aggregates(Supplementary Fig. S2C, right), consistent with thepredominant presence of B cells. During inflammation-
driven colon carcinogenesis, lymphoid tissue signi-ficantly increased compared with control mice (Sup-plementary Fig. S2D), consistently with the local induc-tion of TLT in chronically inflamed tissues. To define theassociation of TLT with T lymphocytes in colorectalcancer, we compared CD3þ T cells within TLT of con-trol and AOM/DSS mice (Fig. 4A, left and middle).Quantification of the T-cell infiltrate indicated thatthe number of CD3þ T cells in lymphoid tissue signi-ficantly increased in AOM/DSS mice (Fig. 4A, right).Thus, as evidenced by our previous clinical analysis, thisresult further confirmed in a preclinical model thatTLT associates with increased T-cell infiltration in colo-rectal cancer.
To test the hypothesis that TLT is actively involvedin the recruitment of lymphocytes, we intravenouslyinjected GFPþ splenocytes into control mice and micesubjected to the AOM/DSS protocol. After 24 hours,GFPþ cells localized in TLT of AOM/DSS mice, whereas
Figure 3. Clinical relevance of TLT in 351 patients with colorectal cancer. A and B, Kaplan–Meier curves showing DFS, according to TLT and TIL density.A high density of TLT (�median, 2.68%) and of TILs (�median, 2,06%) is associated with better outcome in patients with node-negativecolorectal cancer (P ¼ 0.02 and P ¼ 0.02, respectively, n ¼ 185; A and B, left), but not in those with node-positive colorectal cancer (P ¼ 0.46 andP ¼ 0.64, respectively, n ¼ 166; A and B, right). C and D, coordination of TLT and TIL immune infiltration. The prognostic behavior of TLT (C, left) andTILs (C, right) varies with disease extent. Among patients with node-negative colorectal cancer, TLT density is significantly lower in patients whorelapsed (n ¼ 26) than in patients with no evidence of disease recurrence (n ¼ 159; P ¼ 0.03), whereas it does not differ in nodal-positivepatients with or without tumor recurrence. Distribution of TLT IRA% according to the CD3þ density (�median) in relapsing and not relapsing patientswith stage II colorectal cancer. TLT and TILs correlate only among patients that do not relapse (D). P (C, left): N0 (no relapse) versus N0 (relapse)P ¼ 0.03; N1 (no relapse) versus N1 (relapse) P ¼ 0.43; N2 (no relapse) versus N2 (relapse) P ¼ 0.15. P (C, right): N0 (no relapse) versus N0 (relapse)P ¼ 0.01; N1 (no relapse) versus N1 (relapse) P ¼ 0.74; N2 (no relapse) versus N2 (relapse) P ¼ 0.51.
Tertiary Lymphoid Tissue in Colorectal Cancer
www.aacrjournals.org Clin Cancer Res; 20(8) April 15, 2014 2153
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

very few or none were observed in lymphoid tissue ofcontrol mice (Fig. 4B, left and middle). Whole-tissueanalysis evidenced a significant increase in the density
of GFPþ cells in colorectal cancer–associated lymphoidtissue (Fig. 4B, right), thus, confirming that TLT in thetumor mediates recruitment of lymphocytes.
Table 1. Prediction of risk for disease relapse by nodal status in 351 pT3/pT4 colorectal cancer
Relapse Cox hazards model
No Yes(n ¼ 267) (n ¼ 84) HR (95% CI) P
CD3 TILs density <1% N0 32 11 1.00 ref.N1–N2 33 17 1.39 (0.65–2.97) 0.39
1%–5% N0 77 11 1.00 ref.N1–N2 52 25 2.91 (1.43–5.91) 0.003
5%–10% N0 32 2 1.00 ref.N1–N2 15 15 12.12 (2.75–53.38) 0.001
�10% N0 18 2 1.00 ref.N1–N2 8 1 1.12 (0.10–12.36) 0.92
TLT density No TLT N0 25 8 1.00 ref.N1–N2 25 17 1.81 (0.78–4.20) 0.16
0%–4.16% N0 62 12 1.00 ref.N1–N2 45 31 2.90 (1.48–5.65) 0.001
4.16%–8.32% N0 42 4 1.00 ref.N1–N2 20 7 3.27 (0.95–11.17) 0.05
�8.32% N0 30 2 1.00 ref.N1–N2 18 3 2.41 (0.40–14.45) 0.33
NOTE: Colorectal cancer were subgrouped according to the density of CD3þ TILs and TLT at the tumor invasive front.Abbreviations: N0, no lymph node involvement; N1, one to three nodes involved; N2, more than or equal to four nodes involved.
Table 2. Themultivariate Cox hazardmodel for predictive factors of disease relapse in 185 stage II pT3/pT4colorectal cancer
Multivariate analysis
Relapse Model A Model B
No Yes(n ¼ 159) (n ¼ 26) HR (95% CI) P HR (95% CI) P
TLT density<Median 71 18 1.00 (reference) — —
�Median 88 8 0.42 (0.18–0.99) 0.05 — —
TIL density<Median 76 19 — — 1.00 (reference)�Median 83 7 — — 0.35 (0.15–0.83) 0.02
Local invasiona
pT3 149 20 1.00 (reference) 1.00 (reference)pT4 10 6 3.78 (1.47–9.76) 0.006 4.76 (1.86–12.17) 0.001
Tumor cell typeb
Adenocarcinoma 153 23 1.00 (reference) 1.00 (reference)Variants 6 3 3.94 (1.15–13.50) 0.03 4.27 (1.24–14.67) 0.02
NOTE:Multivariate analysis was performedby introducing TLT density (�median) inmodel A and TIL density (�median) inmodel B andby entering all other variables with a P value less than 0.20 at univariate analysis. By a backward stepwise elimination approach,nonsignificant variables, and their nonsignificant interactions, were removed from the model.apT3, invading through the muscularis propria into subserosa or into nonperitonealized pericolic or perirectal tissues. pT4, directlyinvading adjacent organs or perforating visceral peritoneum.bVariants mucinous or medullary.
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2154
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

Whole-mount tissue analysis of TLT in murine colonsallowed to visualize a dense network of vessels surround-ing TLT, which included CD31þ blood vessels and Lyve-
1þ lymphatic vessels (Fig. 4C, left and middle). Quanti-fication of the volume of vessels draining TLT evidenced asignificant increase in AOM/DSS mice compared with
Figure 4. TLT mediates increased lymphocyte infiltration in a preclinical model of colorectal cancer. A, expansion of TLT associates with increased number ofCD3þTcells. Stainingwithanti-CD3antibody in lymphoid tissue (dottedcircle) of controlmice (left) andAOMDSSmice (middle).QuantificationofCD3þ cells in colontissues of mice was performed by computer-assisted image analysis and indicates increased number of CD3þ T cells in the TLT of AOMDSS mice,comparedwith controlmice (right). B, TLT is actively involved in the recruitment of lymphocytes. GFPþ splenocyteswere intravenously injected in control andAOM/DSSmiceandwhole colonsanalyzedby immunofluorescenceafter 24hours.Representative imagesofGFPþ cells in a lymphoid follicle (dottedcircle) of control (left)and AOM/DSS (middle) mice. Quantification of GFPþ cells was performed on 20-mm thick sections from the whole colon; Each dot represents the density of GFPþ
cells in theTLTanalyzed (right). One representative of twoexperimentsperformed (n¼ 3mice;Ctrl;n¼ 5miceAOM/DSS;bars, SEM).C, the vessel networkdraininglymphoid tissue (B220þ B cells) in the colonmucosa of control (left) and tumor-bearingmice (middle) includesCD31þ blood vessels and Lyve1þ lymphatic vessels.Morphometric analysis on colon wholemounts indicates vessel expansion around and inside lymphoid tissue of AOMDSSmice (right; n¼ 6mice; Ctrl; n¼ 6miceAOM/DSS; bars, SEM). D, TLT contains functional HEVs. Staining with and anti-PNAd antibody indicates presence of HEV in lymphoid tissue (left). CD3þ Tlymphocytescirculate intoPNAdþHEV,and localize incloseproximity to thevesselwall (asterisks;middle).ThenumberofHEV increases in lymphoid tissueof tumor-bearing mice (right). Scale bar, 200 mm (A–C); 100 mm (D, left); 50 mm (D, middle). Two-tailed P values by the t test. ��, P < 0.005; ���, P < 0.001.
Tertiary Lymphoid Tissue in Colorectal Cancer
www.aacrjournals.org Clin Cancer Res; 20(8) April 15, 2014 2155
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

control mice (Fig. 4C, right). Among CD31þ vessels,lymphoid tissue contained PNAdþ HEVs (Fig. 4D, left);CD3þ T cells were localized inside HEV and in closeproximity to the vessel wall (Fig. 4D, middle). The num-ber of PNAdþ HEV within lymphoid tissue of AOM/DSSmice was higher compared with control mice (Fig. 4D,right), thus, confirming that TLT formation in coloncancer associates with expansion of a vascular networkand can sustain lymphocyte recruitment.
DiscussionThe recognition of the key role of tumor-infiltrating
leukocytes in cancer has triggered the efforts toward a betterdefinition of the complexity of the immune response intumors, with the relevant clinical perspective to identifynovel prognostic biomarkers, which might help in thedesign of immune-based therapeutic approaches. In thisscenario, CD3þ lymphocytes have recently emerged as arobust immune biomarker in several solid tumors, includ-ing colorectal cancer. In our study, we show that CD3þ T-infiltrating lymphocytes at the tumor invasive front ofcolorectal cancer can localize in organized aggregates, com-prised of T- and B-cell areas and a network of FDCs, thuswith features of TLT, in which clinical relevance in relation-ship to TILs has been so far unexplored.
Intratumor TLT was associated with an increased densityof TILs and to a dense vascular network, including HEV andlymphatic vessels, required to ensure proper traffic of lym-phocytes within lymphoid organs, and thus, suggesting thatTLT has the capability to sustain traffic of T cells. Thepresence of the chemokines CCL19 and CXCL13 withinTLT strongly supports the hypothesis that lymphoid tissue isrelevant to mediate active recruitment of lymphocytes intothe tumor, which was then confirmed by intravenous injec-tion of GFP splenocytes in mice.
The clinical relevance of tumor-infiltrating T cells inhuman colorectal cancer has been extensively documented(2–6, 8, 26, 27). Previous analyses of T-cell infiltration inpatients with colorectal cancer claimed CD3þ TILs as betterindicator of prognosis than TNM tumor staging (3). How-ever, on accurate analysis, CD3þ TILs retained prognosticsignificance only in patients with nodal-negative colorectalcancer (4), thus, identifying CD3þ TILS as a prognosticbiomarker for stage II colorectal cancer and suggesting thepossibility to implement the TNM-based system with onedeveloped upon the densities of CD3þ TILs. About TLT,here, we took advantage of a computer-assisted imageanalysis, which is objective and statistically more relevant,providing continuous distributions of immune cell densi-ties. By these means, we showed for the first time that, inaccordance with TILs, TLT are not predominant over tumorstaging in predicting patient outcome and their prognosticrelevance varies with the state of disease progression atdiagnosis. Thus, they may contribute to tumor control atthe early stages of the disease, while they progressively loosethis capability along with tumor progression and occur-rence of lymph node metastasis.
Our stage-by-stage analysis showed that only very highor very low TLT densities have prognostic impact in stageIII and behave as independent predictors of survival.Essentially, although the antitumor impact of immuneinfiltration is more relevant in stage II colorectal cancer,only the strongest immune responses have an impact onthe prognosis in stage III. However, the number ofpatients with colorectal cancer identified by very highcutoff values is proportionally scarce and thus, limits itsclinical impact. The generation of threshold values andcombined immune values is a critical issue in the assess-ment of the prognostic abilities of immune cells andshould be carefully managed. In previous studies, theuse of these cutoffs together with combined valuesobtained from markers identifying overlapping immunecell populations has led to claim the futility of pathologicstaging (3, 8). This strategy fostered statistical analysis butidentified a very small benchmarking population ofpatients with colorectal cancer devoid of TILs and witha dismal prognosis (3, 8), with limited clinical prognosticrelevance when addressing surveillance strategies in theoverall population of colorectal cancer.
The type of genomic instability has been proposed as animportant variable to be included in the design of studies onimmune cells and prognosis (40). MSI patients with colo-rectal cancer have a better prognosis over MSS (41, 42)together with a higher lymphocytic reaction at the tumorsite (4, 6, 26, 37). Our data further addressed this issue byshowing that the prognostic value of TLT density is inde-pendent by MSI, thus, not being influenced by their lowermetastatic potential.
Protocol variability for quantification of immune cells,together with inconsistent statistical design is a criticalfactor contributing to discrepancy of results among studies.Importantly, although the assessment of TILs, irregularlyand heterogeneously dispersed within the tissue is chal-lenging, TLT are easy to detect under an optical microscopeand by image analysis, being organized as cellular aggre-gates. A worldwide concerted action (Immunoscore) isongoing, aimed at assessing the actual clinical usefulnessof a standardized methodologic assessment of T-cell infil-tration (43, 44). The results presented here further suggestthat the quantification of organized TLT is a feasible andeasy approach to this issue in the context of TNM stagingand that TLT and TILs are coordinated in their clinicalrelevance in early-stage human colorectal cancer. Thus, TLTassessment should also be considered when the prognosticvalue of TILs is investigated.
We found that TLT and TILs populations are highlyoverlapping in their extent and prognostic abilitiesbecause these biomarkers were mutually dependent inpredicting the prognosis of patient. However, we provid-ed phenomenologic evidence that the antitumor algo-rithm represented by TLT and TIL densities is coordinatedonly when identifying colorectal cancer patients whowere not relapsing. Thus, it is conceivable to hypothesizethat T-cell recruitment and the mounting of an efficientT-cell antitumor immune reaction is favored by the
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2156
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

presence of a local immune environment like TLT at thetumor site, whereas the pathways of activation of thesetwo immune players seem to differ among colorectalcancers with an aggressive behavior. According to theircellular composition, rich in T and B cells, their structuralorganization and their intratumor localization, it is rea-sonable to hypothesize that TLT at the invasive front inhuman colorectal cancer might collect T cells in closeproximity to cancer cells, potentially improving the effi-ciency of the antitumor response.B cells are a relevant component of TLT. In human cancer,
B cells are known to promote tumor immunity by severalmechanisms, including production of antibodies directedto tumor-specific antigens, antigen presentation, andenhancement of T-cell antitumor activity (45, 46) all func-tions being highly favored by the presence of an immunesite. In this regard, our data suggest that also a humoralimmune response organized at the tumor site, within TLT,might be a player in the generationof an antitumor immuneresponse with prognostic relevance.Overall, the occurrence and modulation of TLT may be
particularly significant in the development and the respon-siveness of novel immunotherapeutic approaches. In thisscenario, we also provided further phenomenologic evi-dence to the idea that nodal invasion is crucial in deter-mining the efficiency and the coordination of adaptiveantitumor responses (47). Nevertheless, the lack of murinemodels properly reproducing the progression of colorectalcancer across its stages of disease might explain at least inpart recent failures in translating immunotherapeuticapproaches to clinical practice. Therefore, we suggest thatTNM stage of disease should be a critical variable in thedesign and the assessment of clinical trials aimed to test the
responsiveness of novel immunotherapeutic strategies incolorectal cancer.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
DisclaimerThe funders had no role in the study design, data collection and analysis,
decision to publish, or preparation of the article.
Authors' ContributionsConception and design: A. Malesci, L. Laghi, F. MarchesiDevelopment of methodology:G. Di Caro, F. Bergomas, F. Grizzi, A. DoniAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): G. Di Caro, F. Bergomas, F. Grizzi, A. MalesciAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis):G.Di Caro, F. Grizzi, P. Bianchi, L. Laghi,F. MarchesiWriting, review, and/or revision of themanuscript:G.Di Caro, F. Grizzi,P. Bianchi, L. Laghi, P. Allavena, A. Mantovani, F. MarchesiAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): A. MalesciStudy supervision: A. Malesci, A. Mantovani, F. Marchesi
AcknowledgmentsThe authors thank Chiara Rossi.
Grant SupportThis work was supported by the Italian Association for Cancer Research
(AIRC) Italy (grant numberMFAG-11677; to F.Marchesi and IG-12051; to P.Allavena) and the Italian Ministry of University and Research, FIRB grant(RBAP11H2R9; to A. Mantovani). G. Di Caro is supported by a fellowshipfrom Fondazione Umberto Veronesi.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received September 24, 2013; revised December 17, 2013; acceptedJanuary 12, 2014; published OnlineFirst February 12, 2014.
References1. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflamma-
tion. Nature 2008;454:436–44.2. Pages F, Berger A, Camus M, Sanchez-Cabo F, Costes A, Molidor R,
et al. Effector memory T cells, early metastasis, and survival in colo-rectal cancer. N Engl J Med 2005;353:2654–66.
3. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A,Mlecnik B, Lagorce-Pages C, et al. Type, density, and location of immune cells withinhuman colorectal tumors predict clinical outcome. Science 2006;313:1960–4.
4. Laghi L, Bianchi P, Miranda E, Balladore E, Pacetti V, Grizzi F, et al.CD3þ cells at the invasive margin of deeply invading (pT3-T4) colo-rectal cancer and risk of post-surgicalmetastasis: a longitudinal study.Lancet Oncol 2009;10:877–84.
5. Fridman WH, Pages F, Sautes-Fridman C, Galon J. The immunecontexture in human tumours: impact on clinical outcome. Nat RevCancer 2012;12:298–306.
6. NoshoK, Baba Y, TanakaN, ShimaK,HayashiM,Meyerhardt JA, et al.Tumour-infiltrating T-cell subsets, molecular changes in colorectalcancer, and prognosis: cohort study and literature review. J Pathol2010;222:350–66.
7. Dahlin AM, Henriksson ML, Van Guelpen B, Stenling R, Oberg A,Rutegard J, et al. Colorectal cancer prognosis depends on T-cellinfiltration and molecular characteristics of the tumor. Mod Pathol2011;24:671–82.
8. MlecnikB, TosoliniM,KirilovskyA,BergerA,BindeaG,Meatchi T, et al.Histopathologic-based prognostic factors of colorectal cancers are
associated with the state of the local immune reaction. J Clin Oncol2011;29:610–8.
9. Aloisi F, Pujol-Borrell R. Lymphoid neogenesis in chronic inflammatorydiseases. Nat Rev Immunol 2006;6:205–17.
10. Carragher DM, Rangel-Moreno J, Randall TD. Ectopic lymphoid tis-sues and local immunity. Semin Immunol 2008;20:26–42.
11. Moyron-Quiroz JE, Rangel-Moreno J, Hartson L, Kusser K, Tighe MP,Klonowski KD, et al. Persistence and responsiveness of immunologicmemory in the absence of secondary lymphoid organs. Immunity2006;25:643–54.
12. Lee Y, Chin RK, Christiansen P, Sun Y, Tumanov AV, Wang J, et al.Recruitment and activation of naive T cells in the islets by lymphotoxinbeta receptor-dependent tertiary lymphoid structure. Immunity 2006;25:499–509.
13. Armengol MP, Cardoso-Schmidt CB, Fernandez M, Ferrer X, Pujol-Borrell R, Juan M. Chemokines determine local lymphoneogenesisand a reduction of circulating CXCR4þ T and CCR7 B and T lympho-cytes in thyroid autoimmune diseases. J Immunol 2003;170:6320–8.
14. Carlsen HS, Baekkevold ES, Johansen FE, Haraldsen G, BrandtzaegP. B cell attracting chemokine 1 (CXCL13) and its receptor CXCR5 areexpressed in normal and aberrant gut associated lymphoid tissue. Gut2002;51:364–71.
15. Grabner R, Lotzer K, Dopping S, Hildner M, Radke D, Beer M, et al.Lymphotoxin beta receptor signaling promotes tertiary lymphoidorganogenesis in the aorta adventitia of aged ApoE�/� mice. J ExpMed 2009;206:233–48.
Tertiary Lymphoid Tissue in Colorectal Cancer
www.aacrjournals.org Clin Cancer Res; 20(8) April 15, 2014 2157
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

16. Thaunat O, Patey N, Caligiuri G, Gautreau C, Mamani-Matsuda M,Mekki Y, et al. Chronic rejection triggers the development of anaggressive intragraft immune response through recapitulation of lym-phoid organogenesis. J Immunol 2010;185:717–28.
17. Coronella JA, Spier C, Welch M, Trevor KT, Stopeck AT, Villar H,et al. Antigen-driven oligoclonal expansion of tumor-infiltrating Bcells in infiltrating ductal carcinoma of the breast. J Immunol 2002;169:1829–36.
18. Dieu-Nosjean MC, Antoine M, Danel C, Heudes D, Wislez M, PoulotV, et al. Long-term survival for patients with non–small cell lungcancer with intratumoral lymphoid structures. J Clin Oncol 2008;26:4410–7.
19. Coppola D, Nebozhyn M, Khalil F, Dai H, Yeatman T, Loboda A, et al.Unique ectopic lymph node-like structures present in human primarycolorectal carcinoma are identified by immune gene array profiling. AmJ Pathol 2011;179:37–45.
20. Cipponi A, Mercier M, Seremet T, Baurain JF, Theate I, van denOord J, et al. Neogenesis of lymphoid structures and antibodyresponses occur in human melanoma metastases. Cancer Res2012;72:3997–4007.
21. Messina JL, Fenstermacher DA, Eschrich S, Qu X, Berglund AE, LloydMC, et al. 12-Chemokine gene signature identifies lymph node-likestructures in melanoma: potential for patient selection forimmunotherapy? Sci Rep 2012;2:765.
22. Yu P, Lee Y, Liu W, Chin RK, Wang J, Wang Y, et al. Priming of naive Tcells inside tumors leads to eradication of established tumors. NatImmunol 2004;5:141–9.
23. Bergomas F, Grizzi F, Doni A, Pesce S, Laghi L, Allavena P, et al.Tertiary intratumor lymphoid tissue in colorectal cancer. Cancers2012;4:1–10.
24. Gajewski TF, Schreiber H, Fu YX. Innate and adaptive immune cells inthe tumor microenvironment. Nat Immunol 2013;14:1014–22.
25. Graham DM, Appelman HD. Crohn's-like lymphoid reaction and colo-rectal carcinoma: a potential histologic prognosticator. Mod Pathol1990;3:332–5.
26. Ogino S, Nosho K, Irahara N, Meyerhardt JA, Baba Y, Shima K, et al.Lymphocytic reaction to colorectal cancer is associated with longersurvival, independent of lymph node count, microsatellite instability,and CpG island methylator phenotype. Clin Cancer Res 2009;15:6412–20.
27. Roxburgh CS, McMillan DC. The role of the in situ local inflammatoryresponse in predicting recurrence and survival in patients with primaryoperable colorectal cancer. Cancer Treat Rev 2012;38:451–66.
28. Clevers H. At the crossroads of inflammation and cancer. Cell2004;118:671–4.
29. Terzic J, Grivennikov S, Karin E, Karin M. Inflammation and coloncancer. Gastroenterology 2010;138:2101–14.
30. Kratz A, Campos-Neto A, Hanson MS, Ruddle NH. Chronic inflam-mation caused by lymphotoxin is lymphoid neogenesis. J Exp Med1996;183:1461–72.
31. Peduto L, Dulauroy S, Lochner M, Spath GF, Morales MA, Cumano A,et al. Inflammation recapitulates the ontogeny of lymphoid stromalcells. J Immunol 2009;182:5789–99.
32. de Chaisemartin L, Goc J, Damotte D, Validire P, Magdeleinat P,Alifano M, et al. Characterization of chemokines and adhesion mole-cules associated with T cell presence in tertiary lymphoid structures inhuman lung cancer. Cancer Res 2011;71:6391–9.
33. Marchesi F, Martin AP, Thirunarayanan N, Devany E, Mayer L, GrisottoMG, et al. CXCL13 expression in the gut promotes accumulation of IL-22-producing lymphoid tissue-inducer cells, and formation of isolatedlymphoid follicles. Mucosal Immunol 2009;2:486–94.
34. Drayton DL, Liao S, Mounzer RH, Ruddle NH. Lymphoid organ devel-opment: from ontogeny to neogenesis. Nat Immunol 2006;7:344–53.
35. Liao S, Ruddle NH. Synchrony of high endothelial venules andlymphatic vessels revealed by immunization. J Immunol 2006;177:3369–79.
36. Martinet L,Garrido I, Filleron T, LeGuellecS,Bellard E, Fournie JJ, et al.Human solid tumors contain high endothelial venules: associationwithT- and B-lymphocyte infiltration and favorable prognosis in breastcancer. Cancer Res 2011;71:5678–87.
37. Laghi L, Bianchi P, Delconte G, Celesti G, Di Caro G, Pedroni M, et al.MSH3 protein expression and nodal status in MLH1-deficient colo-rectal cancers. Clin Cancer Res 2012;18:3142–53.
38. Laghi L, Beghelli S, Spinelli A, Bianchi P, Basso G, Di Caro G, et al.Irrelevance of microsatellite instability in the epidemiology of sporadicpancreatic ductal adenocarcinoma. PLoS ONE 2012;7:e46002.
39. Neufert C, Becker C, Neurath MF. An inducible mouse model of coloncarcinogenesis for the analysis of sporadic and inflammation-driventumor progression. Nat Protoc 2007;2:1998–2004.
40. Ogino S, Galon J, Fuchs CS, Dranoff G. Cancer immunology–analysisof host and tumor factors for personalized medicine. Nat Rev ClinOncol 2011;8:711–9.
41. Popat S, Hubner R, Houlston RS. Systematic review of microsat-ellite instability and colorectal cancer prognosis. J Clin Oncol 2005;23:609–18.
42. Malesci A, Laghi L, Bianchi P, Delconte G, Randolph A, Torri V, et al.Reduced likelihood of metastases in patients with microsatellite-unstable colorectal cancer. Clin Cancer Res 2007;13:3831–9.
43. Galon J, Mlecnik B, Bindea G, Angell HK, Berger A, Lagorce C, et al.Towards the introduction of the Immunoscore in the classification ofmalignant tumors. J Pathol 2014;232:199–209.
44. Galon J, Pages F, Marincola FM, Angell HK, Thurin M, Lugli A, et al.Cancer classification using the Immunoscore: a worldwide task force.J Transl Med 2012;10:205.
45. Whiteside TL. Immune responses to cancer: are they potential bio-markers of prognosis? Front Oncol 2013;3:107.
46. Nelson BH. CD20þ B cells: the other tumor-infiltrating lymphocytes.J Immunol 2010;185:4977–82.
47. Di Caro G, Marchesi F, Laghi L, Grizzi F. Immune cells: plastic playersalong colorectal cancer progression. JCellMolMed2013;17:1088–95.
Di Caro et al.
Clin Cancer Res; 20(8) April 15, 2014 Clinical Cancer Research2158
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590

2014;20:2147-2158. Published OnlineFirst February 12, 2014.Clin Cancer Res Giuseppe Di Caro, Francesca Bergomas, Fabio Grizzi, et al. CancersInfiltration and Predicts Better Prognosis in Early-Stage Colorectal Occurrence of Tertiary Lymphoid Tissue Is Associated with T-Cell
Updated version
10.1158/1078-0432.CCR-13-2590doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/02/12/1078-0432.CCR-13-2590.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/8/2147.full#ref-list-1
This article cites 47 articles, 19 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/8/2147.full#related-urls
This article has been cited by 23 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/8/2147To request permission to re-use all or part of this article, use this link
on September 3, 2021. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2014; DOI: 10.1158/1078-0432.CCR-13-2590














![Occurrence of Clinostomum Metacercariae in mossambicus …downloads.hindawi.com/journals/scientifica/2018/9565049.pdf · parasite [13]. Clinostomum metacercariae species have zoonotic](https://static.fdocuments.fr/doc/165x107/60743858b0822a62721d00c0/occurrence-of-clinostomum-metacercariae-in-mossambicus-parasite-13-clinostomum.jpg)

