Les nouveaux anti-diabétiques oraux: comment faire le …€¦ · Les nouveaux anti-diabétiques...
36
Les nouveaux anti-diabétiques oraux: comment faire le bon choix ? Pr Nicolas PAQUOT Département de Médecine Interne Service de Diabétologie, Nutrition et Maladies métaboliques 3 ème Journée Liégeoise de Diabétologie Samedi 15 novembre 2014
Transcript of Les nouveaux anti-diabétiques oraux: comment faire le …€¦ · Les nouveaux anti-diabétiques...
Les nouveaux anti-diabétiques oraux: comment faire le bon choix ?
Pr Nicolas PAQUOT
Département de Médecine Interne Service de Diabétologie, Nutrition et
Maladies métaboliques
3ème Journée Liégeoise de Diabétologie Samedi 15 novembre 2014

Sources: American Diabetes Association, 2008, www.diabetes.org; Centers for Disease Control, 2008, www.cdc.gov
Prévalence du diabète de type 2 en Belgique: + 33% en 6 ans
Germany 10.2%
6.3 million
Sweden 7.3%
460,000
Italy 6.6%
2.9 million
Netherlands 3.7%
432,000
Belgium 20031
4.2% (315,000) 20092
5.6% (420.000)
France 6.2%
2.7 million
Spain 9.9%
3.0 million
Adapted from IDF E-Atlas. Available at www.eatlas.idf.org. Accessed 9 March 2007. 1: Prevalence data, 2003 2: Thalès data 2009
ME
422H
Q09
PM06
5(6)
- N
S 1
883-
06-1
0
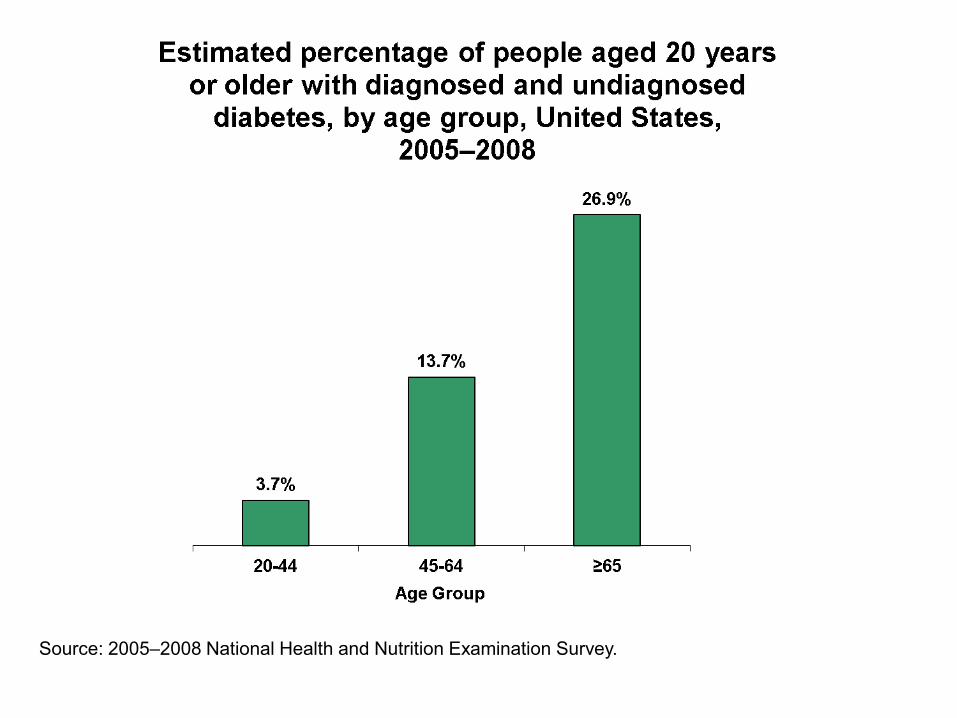
Source: 2005–2008 National Health and Nutrition Examination Survey.
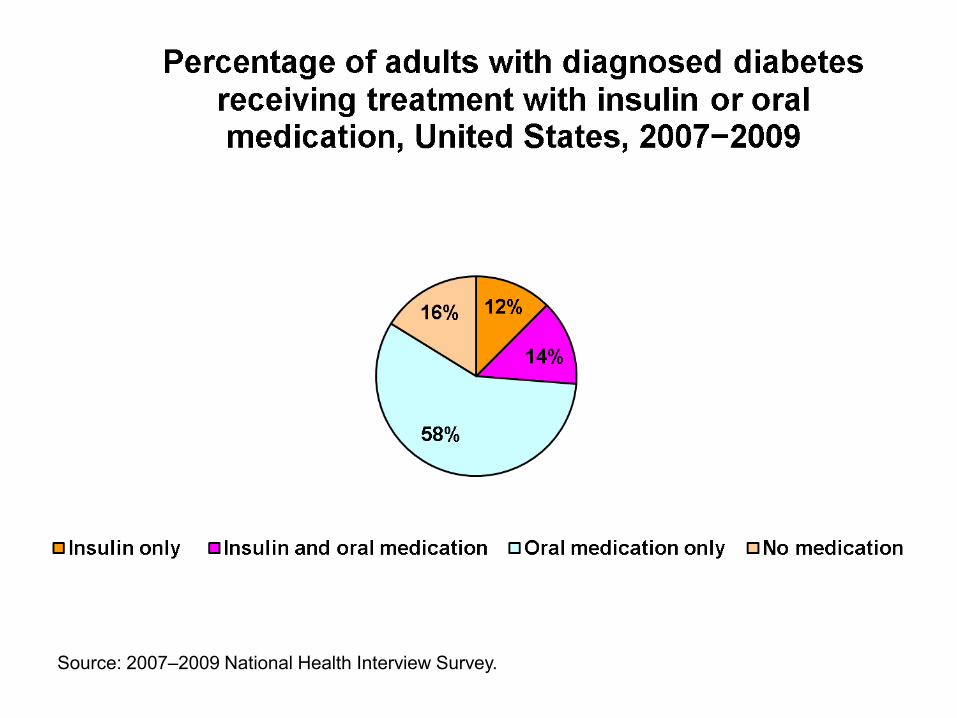
Source: 2007–2009 National Health Interview Survey.
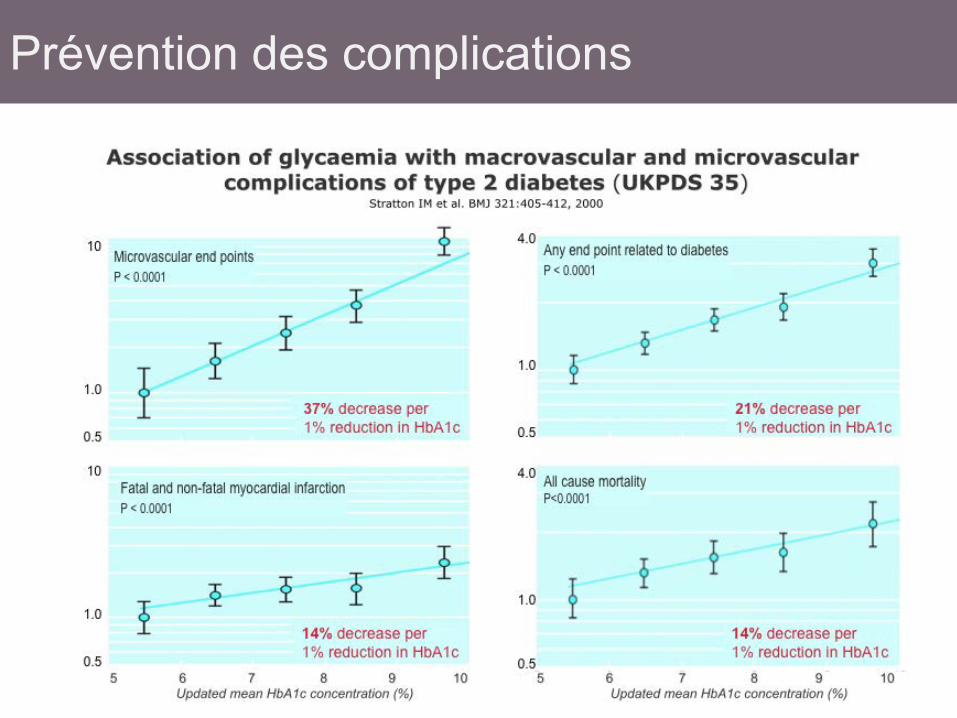
Prévention des complications
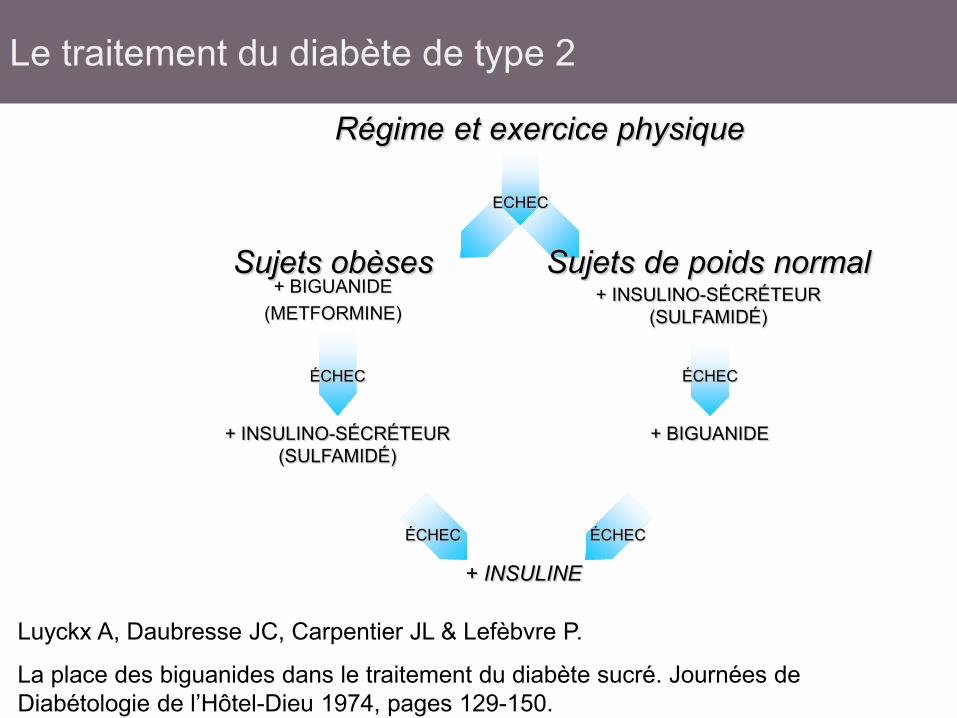
Régime et exercice physique
ECHEC
Sujets obèses Sujets de poids normal
ÉCHEC ÉCHEC
+ BIGUANIDE (METFORMINE)
+ INSULINO-SÉCRÉTEUR (SULFAMIDÉ)
+ BIGUANIDE
ÉCHEC ÉCHEC
+ INSULINE
+ INSULINO-SÉCRÉTEUR (SULFAMIDÉ)
Luyckx A, Daubresse JC, Carpentier JL & Lefèbvre P.
La place des biguanides dans le traitement du diabète sucré. Journées de Diabétologie de l’Hôtel-Dieu 1974, pages 129-150.
Le traitement du diabète de type 2
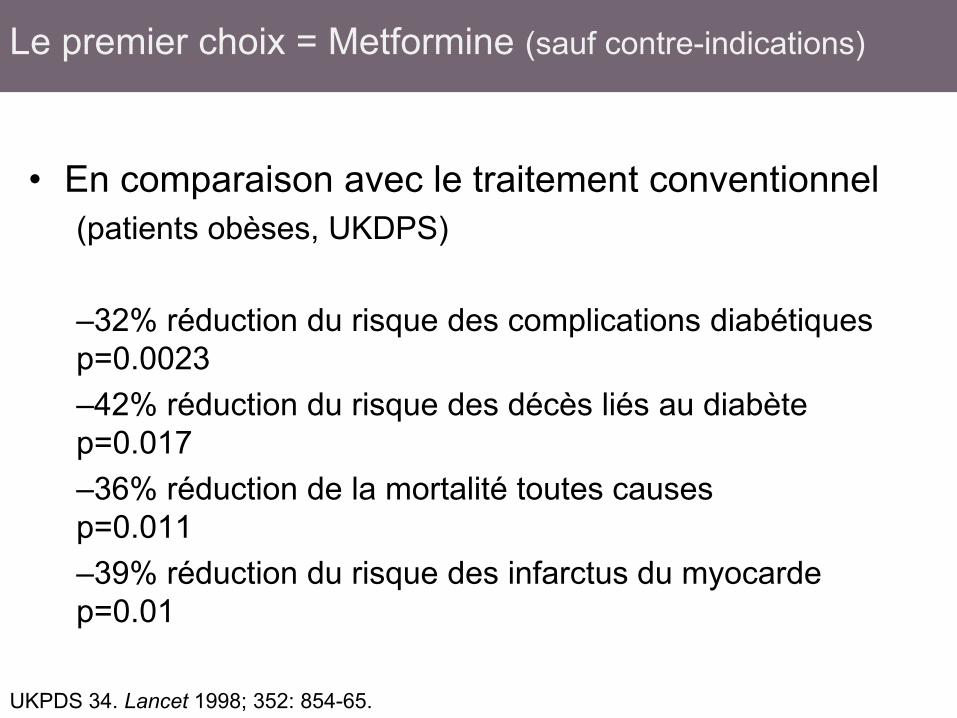
• En comparaison avec le traitement conventionnel
(patients obèses, UKDPS) –32% réduction du risque des complications diabétiques p=0.0023 –42% réduction du risque des décès liés au diabète p=0.017 –36% réduction de la mortalité toutes causes p=0.011 –39% réduction du risque des infarctus du myocarde p=0.01
UKPDS 34. Lancet 1998; 352: 854-65.
Le premier choix = Metformine (sauf contre-indications)
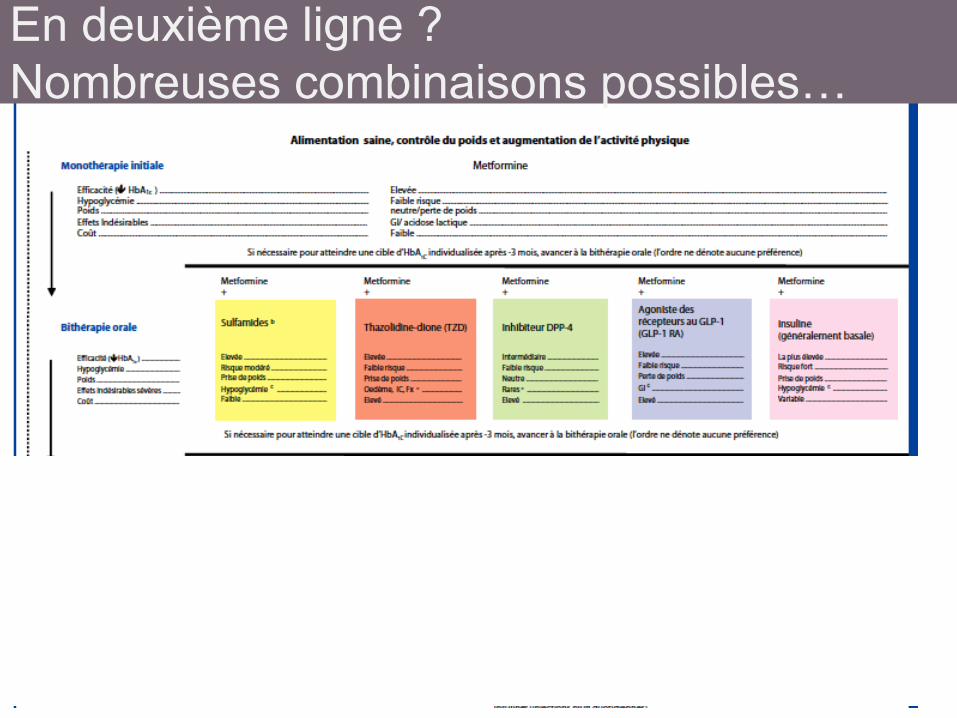
En deuxième ligne ? Nombreuses combinaisons possibles…
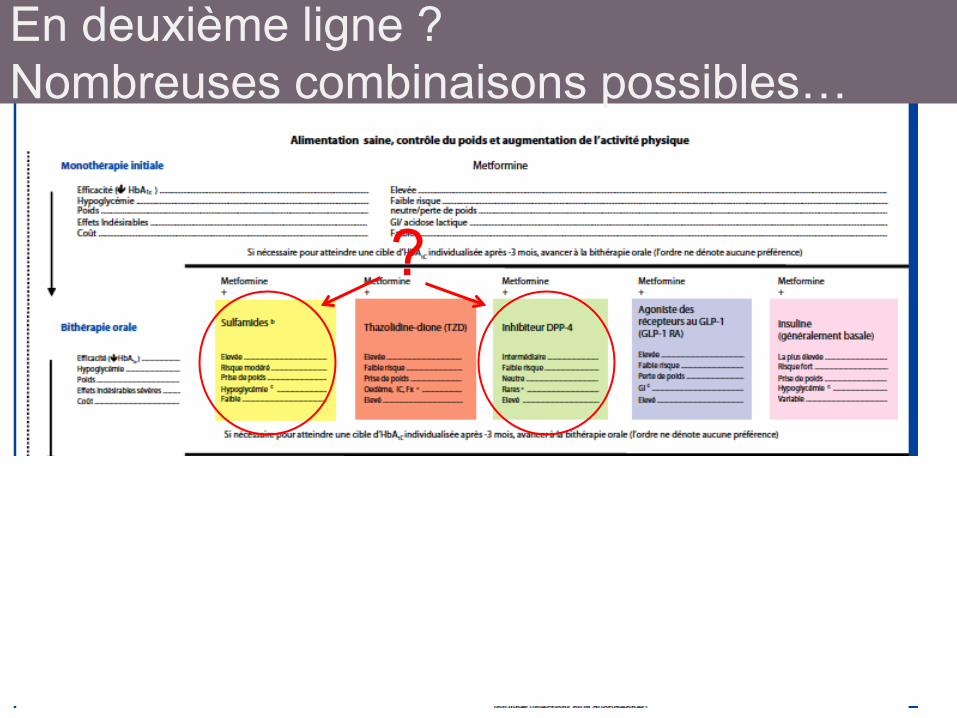
En deuxième ligne ? Nombreuses combinaisons possibles…
?
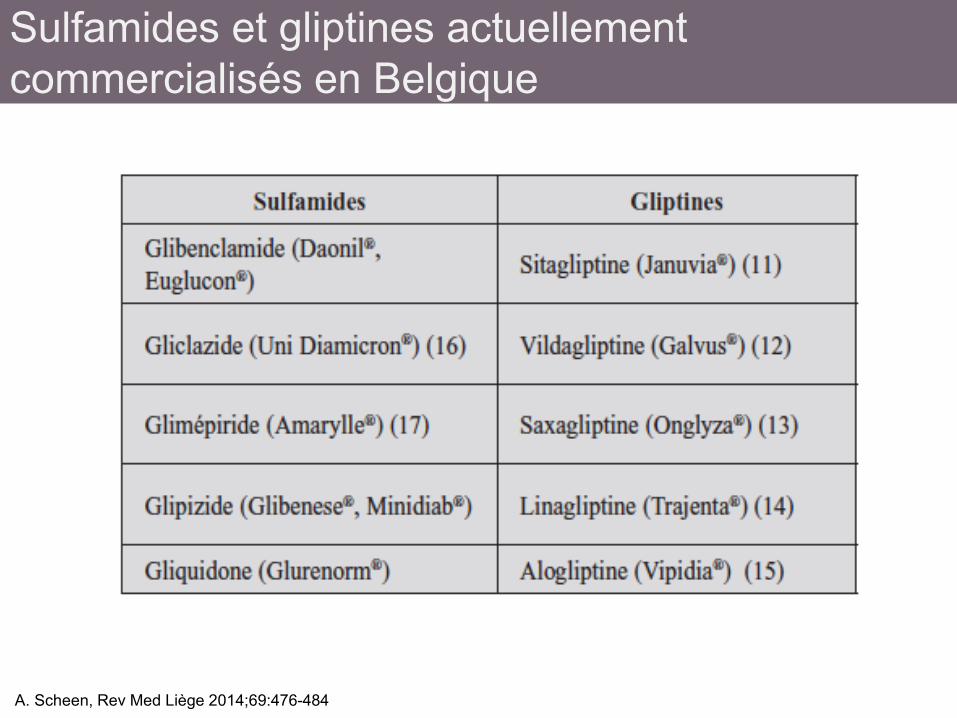
Sulfamides et gliptines actuellement commercialisés en Belgique
A. Scheen, Rev Med Liège 2014;69:476-484
• Preuves scientifiques (EBM) • Mécanisme d’action • Efficacité • Tolérance et sécurité • Coût • Aspects individuels
Comment faire son choix ?
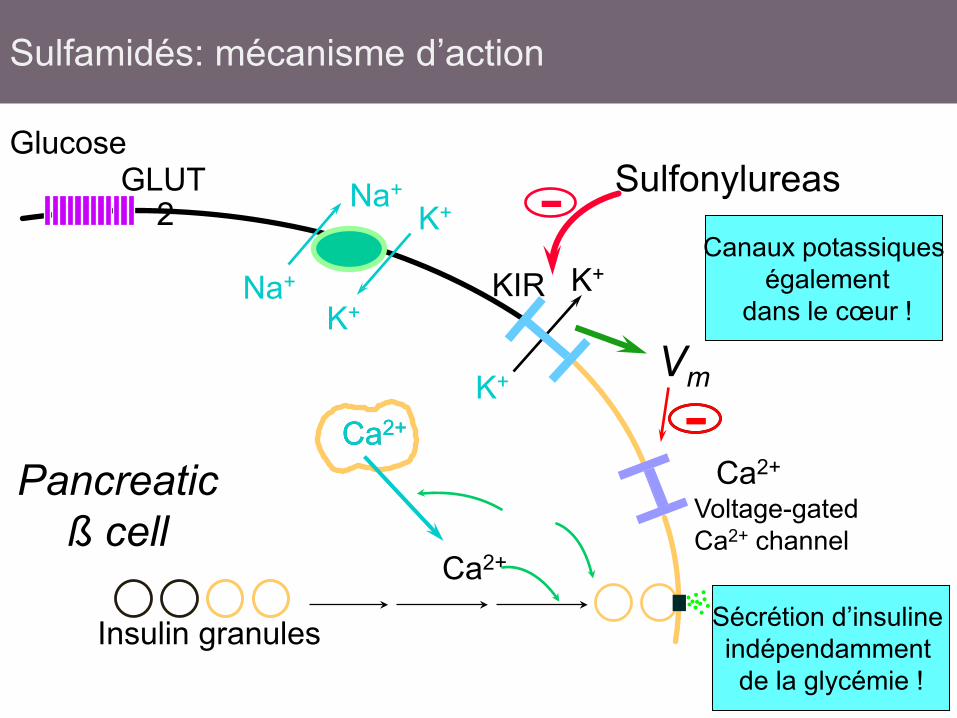
Na+
Na+ K+
K+
K+
K+
GLUT2
Ca2+
Voltage-gated Ca2+ channel
KIR
Pancreatic ß cell
Insulin granules
Ca2+
Ca2+ Ca2+ -
Sulfonylureas -
Vm
Sécrétion d’insuline indépendamment de la glycémie !
Glucose
Canaux potassiques également
dans le cœur !
Sulfamidés: mécanisme d’action
Sulfamidés Quelques questions non (ou imparfaitement) résolues
• Epuisement de la cellule B (UKPDS, ADOPT)
• Sécurité cardio-vasculaire (UGDP, méta-analyses mais UKPDS, ADVANCE, ADOPT rassurants)
• Risque hypoglycémique (sujets à risque) • …
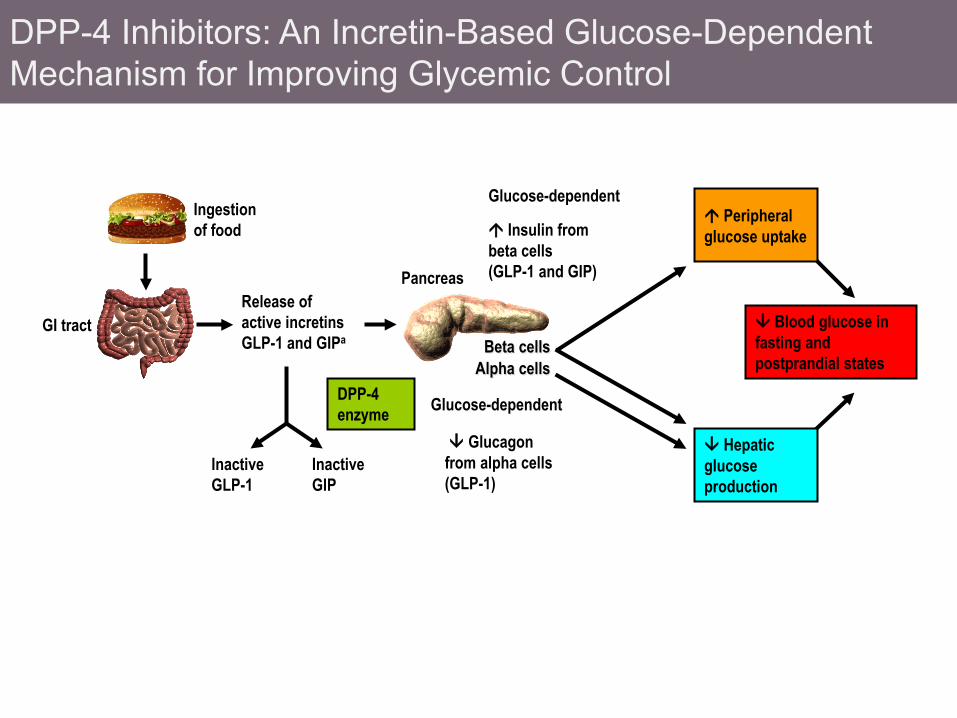
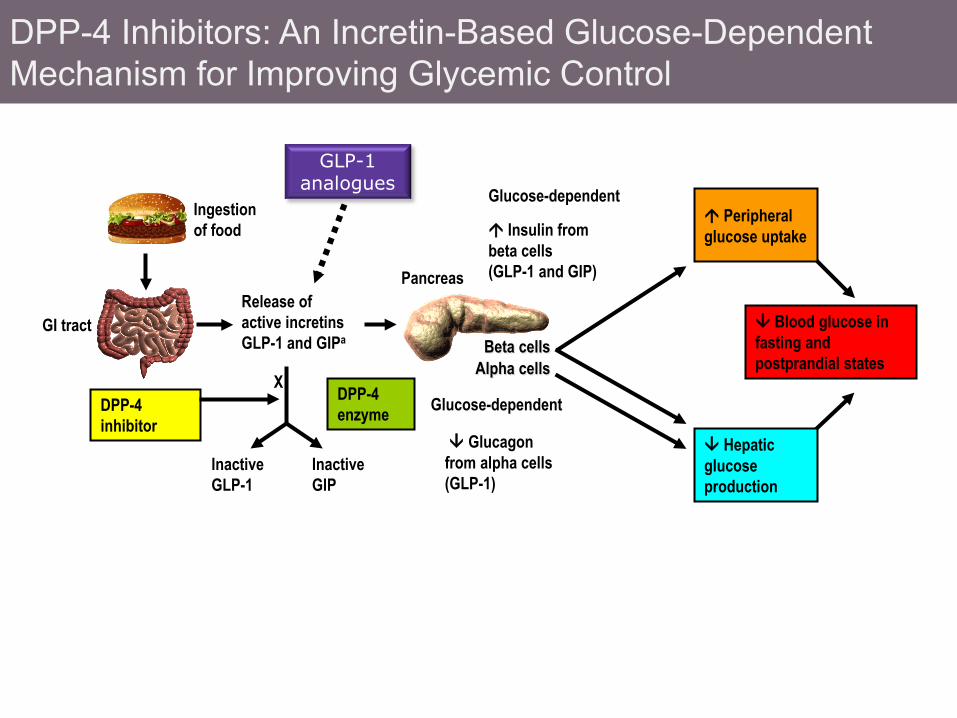
DPP-4 Inhibitors: An Incretin-Based Glucose-Dependent Mechanism for Improving Glycemic Control
Release of active incretins GLP-1 and GIPa
Blood glucose in fasting and postprandial states
Ingestion of food
Glucagon from alpha cells (GLP-1)
Hepatic glucose production
GI tract
DPP-4 enzyme
Inactive GLP-1
Insulin from beta cells (GLP-1 and GIP)
Glucose-dependent
Glucose-dependent
Pancreas
Inactive GIP
Beta cells Alpha cells
Peripheral glucose uptake
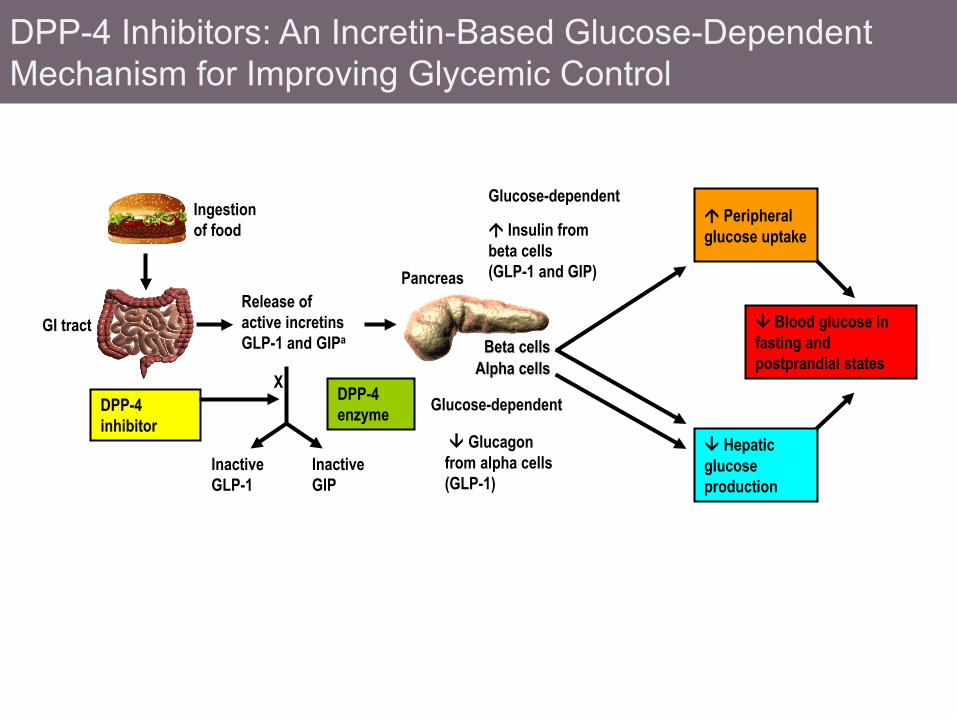
DPP-4 Inhibitors: An Incretin-Based Glucose-Dependent Mechanism for Improving Glycemic Control
Release of active incretins GLP-1 and GIPa
Blood glucose in fasting and postprandial states
Ingestion of food
Glucagon from alpha cells (GLP-1)
Hepatic glucose production
GI tract
DPP-4 enzyme
Inactive GLP-1
X DPP-4 inhibitor
Insulin from beta cells (GLP-1 and GIP)
Glucose-dependent
Glucose-dependent
Pancreas
Inactive GIP
Beta cells Alpha cells
Peripheral glucose uptake
DPP-4 Inhibitors: An Incretin-Based Glucose-Dependent Mechanism for Improving Glycemic Control
Release of active incretins GLP-1 and GIPa
Blood glucose in fasting and postprandial states
Ingestion of food
Glucagon from alpha cells (GLP-1)
Hepatic glucose production
GI tract
DPP-4 enzyme
Inactive GLP-1
X DPP-4 inhibitor
Insulin from beta cells (GLP-1 and GIP)
Glucose-dependent
Glucose-dependent
Pancreas
Inactive GIP
Beta cells Alpha cells
Peripheral glucose uptake
GLP-1 analogues
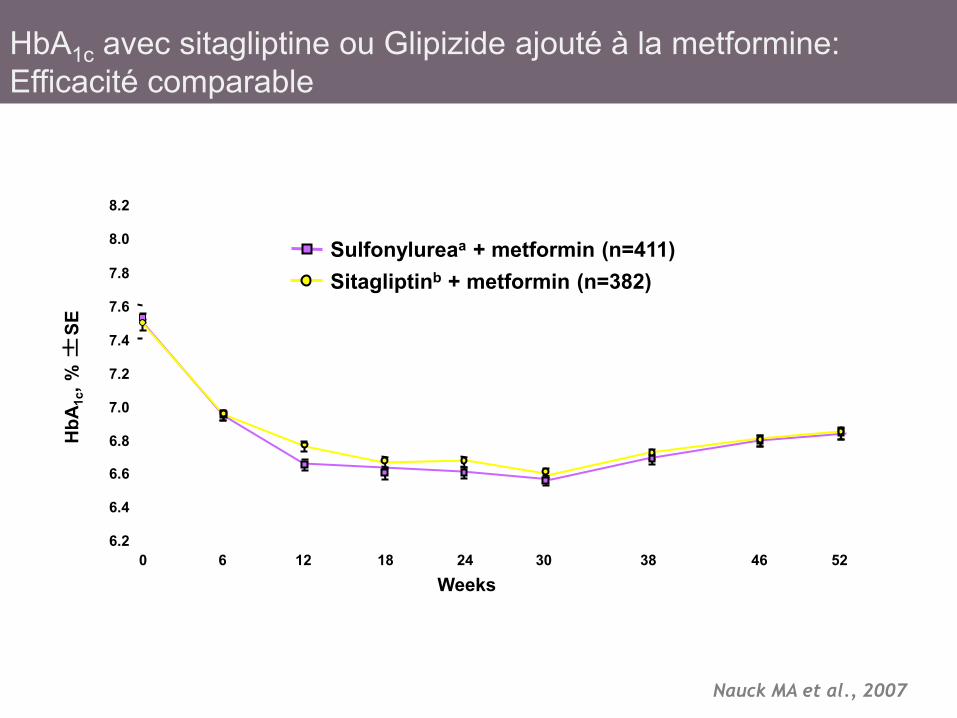
Sulfonylureaa + metformin (n=411) Sitagliptinb + metformin (n=382)
HbA
1c, %
±SE
Weeks
6.2
6.4
6.6
6.8
7.0
7.2
7.4
7.6
7.8
0 6 12 18 24 30 38 46 52
8.0
8.2
HbA1c avec sitagliptine ou Glipizide ajouté à la metformine: Efficacité comparable
Nauck MA et al., 2007
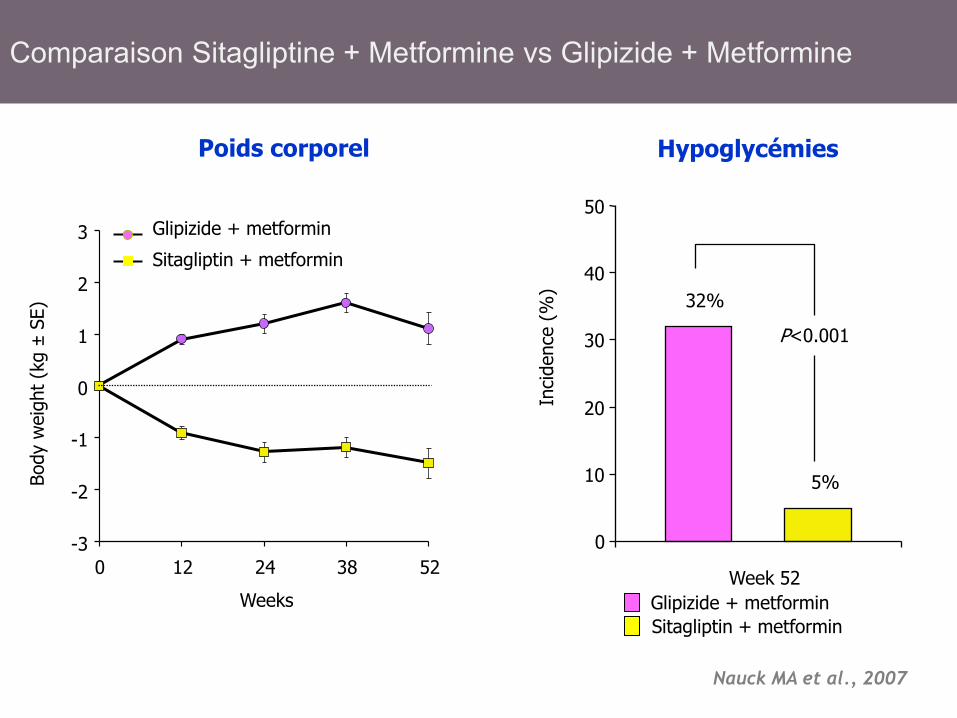
Glipizide + metformin Sitagliptin + metformin
Hypoglycémies
P<0.001
32%
5%
0
10
20
30
40
50
Week 52
Inci
denc
e (%
)
Poids corporel
Body
wei
ght (
kg ±
SE)
Glipizide + metformin
Sitagliptin + metformin
-3
-2
-1
0
1
2
3
0 12 24 38 52
Weeks
Nauck MA et al., 2007
Comparaison Sitagliptine + Metformine vs Glipizide + Metformine
19
Gliptines et affections pancréatiques Pancreatic Safety of Incretin-Based Drugs — FDA and EMA
Assessment N Engl J Med 2014;379:794-97
Both agencies agree that assertions concerning a causal association between incretin-based drugs and pancreatitis or pancreatic cancer, as expressed recently in the scientific literature and in the media, are inconsistent with the current data.

20
Sitagliptin TECOS
Start: Dec 2008 Projected completion: Dec 2014 N=14,000
Trial Evaluating Cardiovascular Outcomes With Sitagliptin Primary Outcome: Time to first confirmed occurrence of CV event , a composite defined as CV-related death, nonfatal MI, nonfatal stroke, or unstable angina requiring hospitalization
Alogliptin EXAMINE
Start: Sept 2009 Projected completion: May 2015 N=5,400
Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome Primary Outcome: Time from randomization to the occurrence of the primary major adverse cardiac events, a composite of CV death, nonfatal MI, and nonfatal stroke
Saxagliptin SAVOR
Start: May 2010 Projected completion: June 2014 N=16,500
Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus Trial Primary Outcome: The primary efficacy outcome variable of the study is defined as the composite end point of CV death, nonfatal MI, or nonfatal ischemic stroke
Linagliptin CAROLINA
Start: Oct 2010 Projected completion: Sept 2018 N=6,000
Cardiovascular Outcome Study of Linagliptin vs Glimepiride in Patients With Type 2 Diabetes Primary Outcome: Time to first occurrence of any component of the composite end point: CV death, nonfatal MI, nonfatal stroke, and hospitalization for unstable angina pectoris
Vildagliptin •Vildagliptin does not have an ongoing cardiovascular outcomes trial.
Etudes en cours
Etudes à visée cardiovasculaire actuellement en cours avec les gliptines (inhibiteurs de la DPP-4)
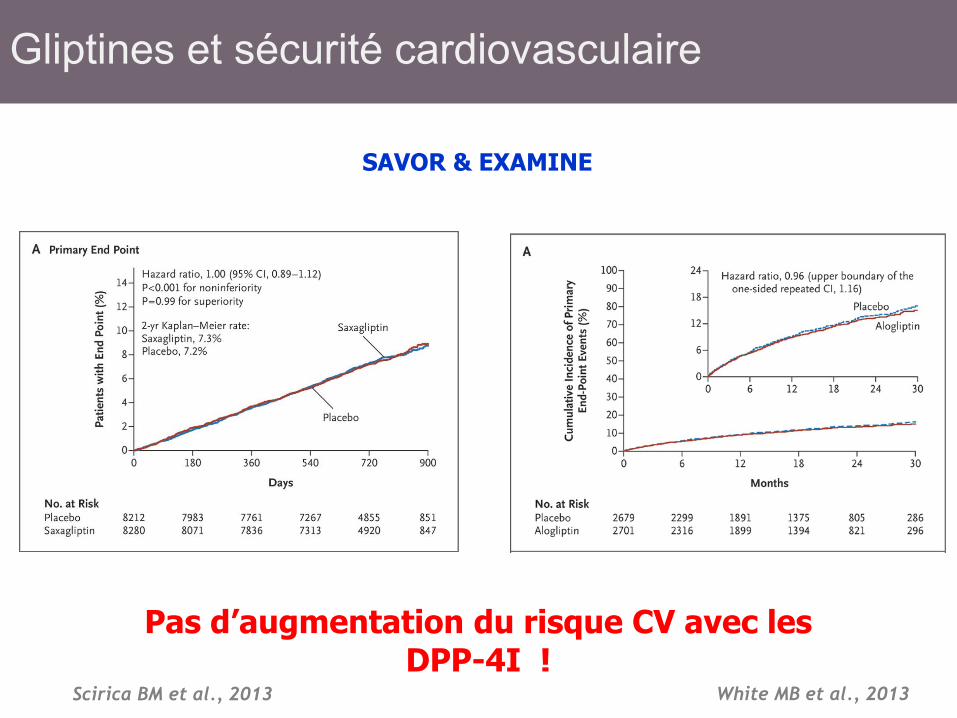
SAVOR & EXAMINE
Scirica BM et al., 2013 White MB et al., 2013
Pas d’augmentation du risque CV avec les DPP-4I !
Gliptines et sécurité cardiovasculaire
• Plus âgés • Plus longue durée du diabète • Repas régulièrement manqué • Activité physique • Prise d’une posologie de médicament plus
importante que celle prescrite
1. Henderson JN et al. Diabet Med. 2003;20:1016–1021. 2. Miller CD et al. Arch Intern Med. 2001;161:1653–1659.
Caractéristiques des patients à risque accru d’hypoglycémies
• Coût • Qualité de vie • Observance • Morbi-mortalité cardiovasculaire très
accrue si atcd hypo sévère – ACCORD (+ 59 %) – ADVANCE ( X 4) – ORIGIN (+ 71 à 74 %)
1. Henderson JN et al. Diabet Med. 2003;20:1016–1021. 2. Miller CD et al. Arch Intern Med. 2001;161:1653–1659.
Conséquences des hypoglycémies chez le sujet diabétique
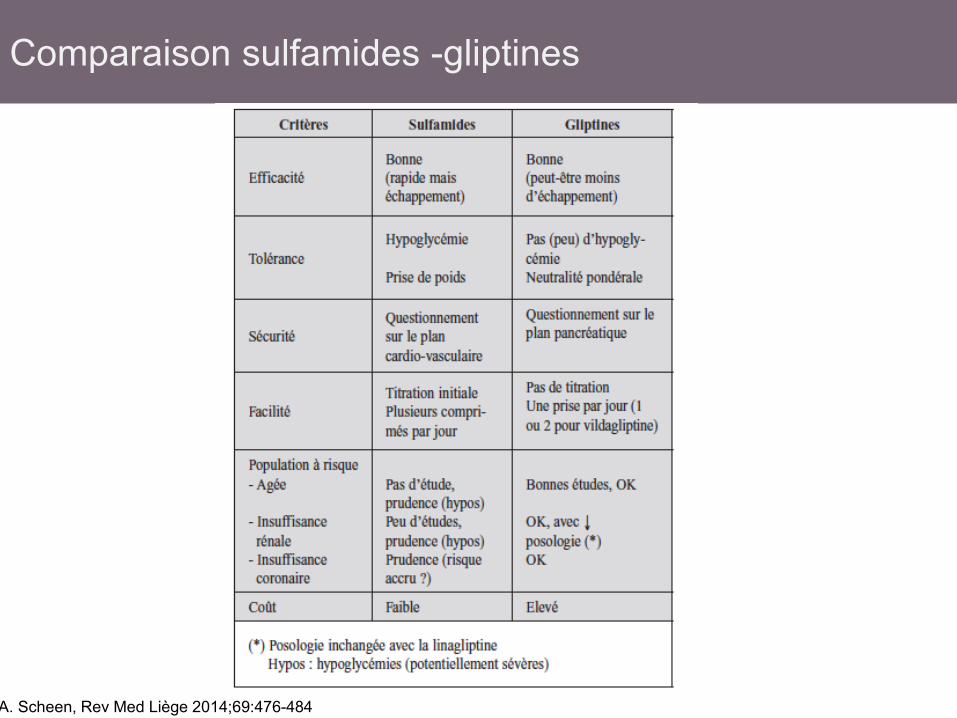
Comparaison sulfamides -gliptines
A. Scheen, Rev Med Liège 2014;69:476-484
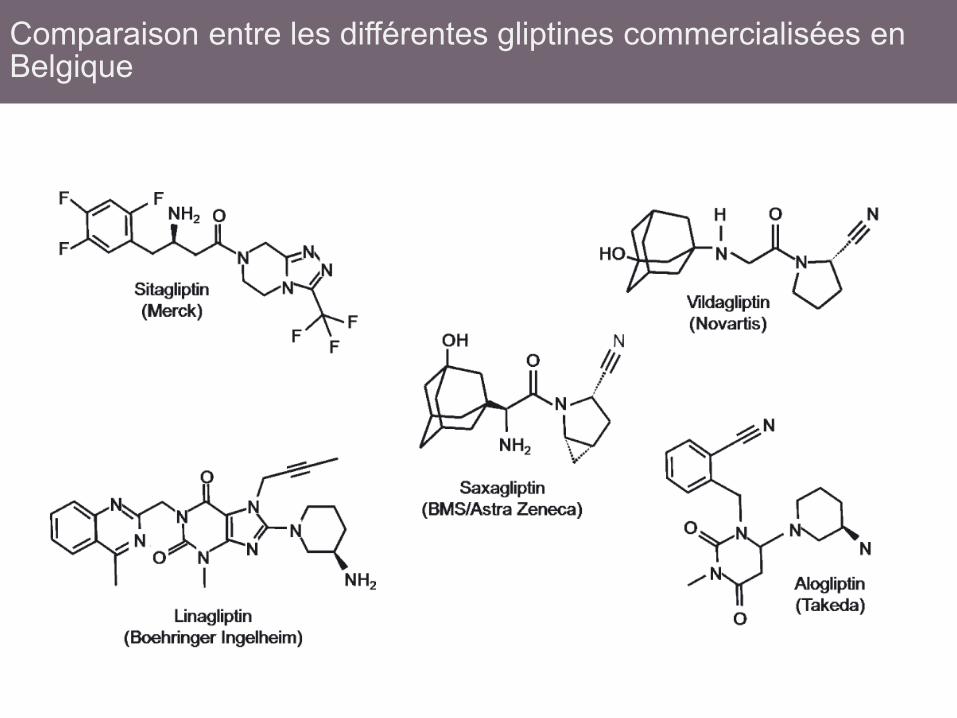
Comparaison entre les différentes gliptines commercialisées en Belgique
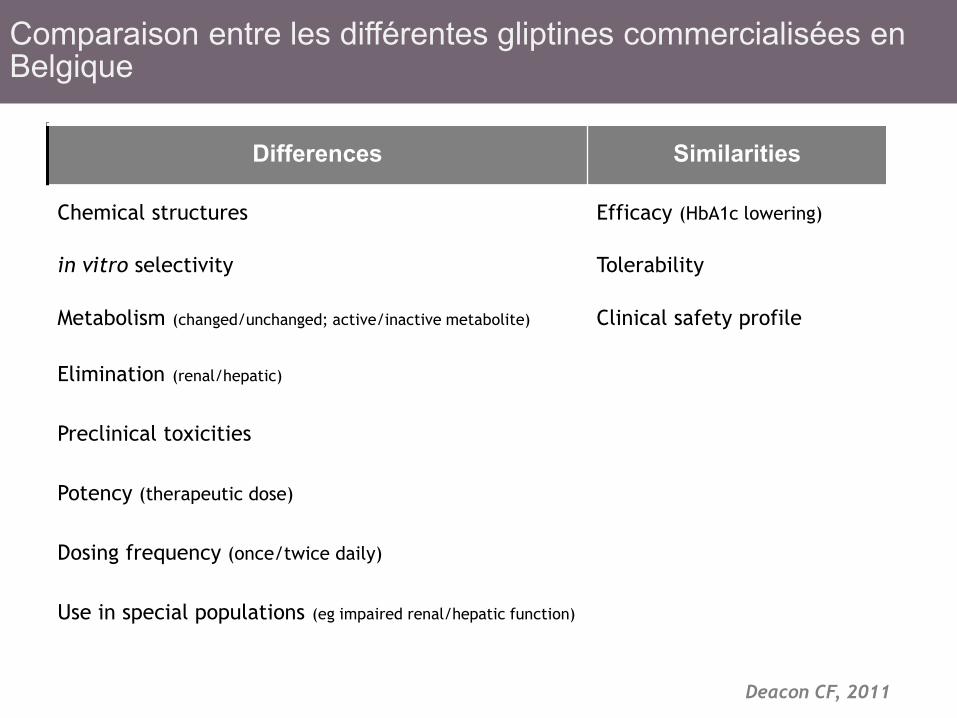
Deacon CF, 2011
Differences Similarities
Chemical structures Efficacy (HbA1c lowering)
in vitro selectivity Tolerability
Metabolism (changed/unchanged; active/inactive metabolite) Clinical safety profile
Elimination (renal/hepatic)
Preclinical toxicities
Potency (therapeutic dose)
Dosing frequency (once/twice daily)
Use in special populations (eg impaired renal/hepatic function)
Comparaison entre les différentes gliptines commercialisées en Belgique
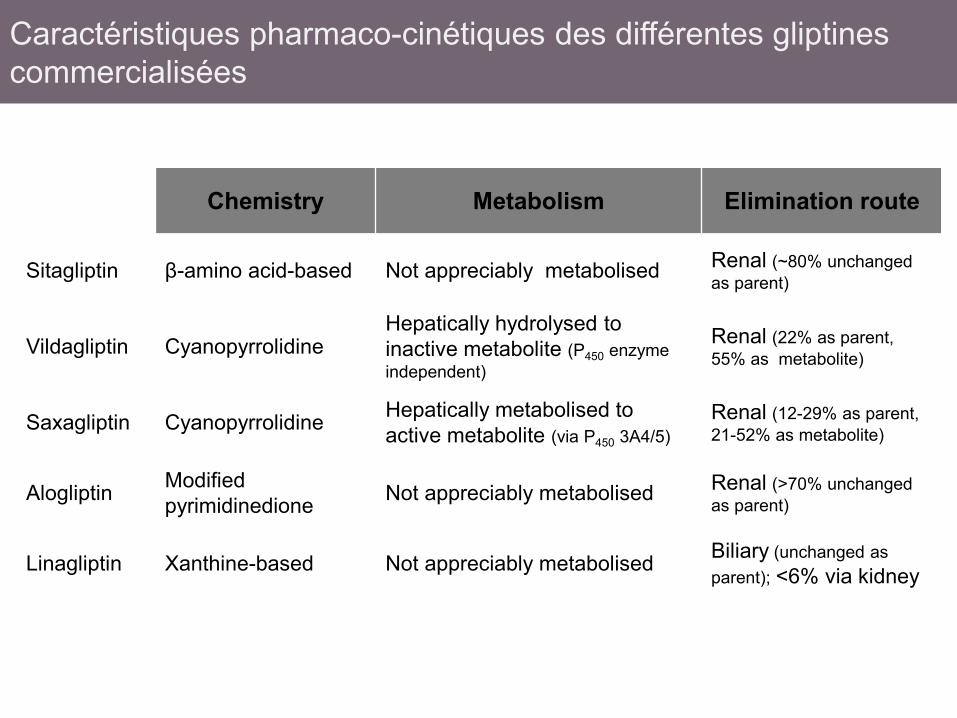
Chemistry Metabolism Elimination route
Sitagliptin β-amino acid-based Not appreciably metabolised Renal (~80% unchanged as parent)
Vildagliptin Cyanopyrrolidine Hepatically hydrolysed to inactive metabolite (P450 enzyme independent)
Renal (22% as parent, 55% as metabolite)
Saxagliptin Cyanopyrrolidine Hepatically metabolised to active metabolite (via P450 3A4/5)
Renal (12-29% as parent, 21-52% as metabolite)
Alogliptin Modified pyrimidinedione Not appreciably metabolised Renal (>70% unchanged
as parent)
Linagliptin Xanthine-based Not appreciably metabolised Biliary (unchanged as parent); <6% via kidney
Caractéristiques pharmaco-cinétiques des différentes gliptines commercialisées
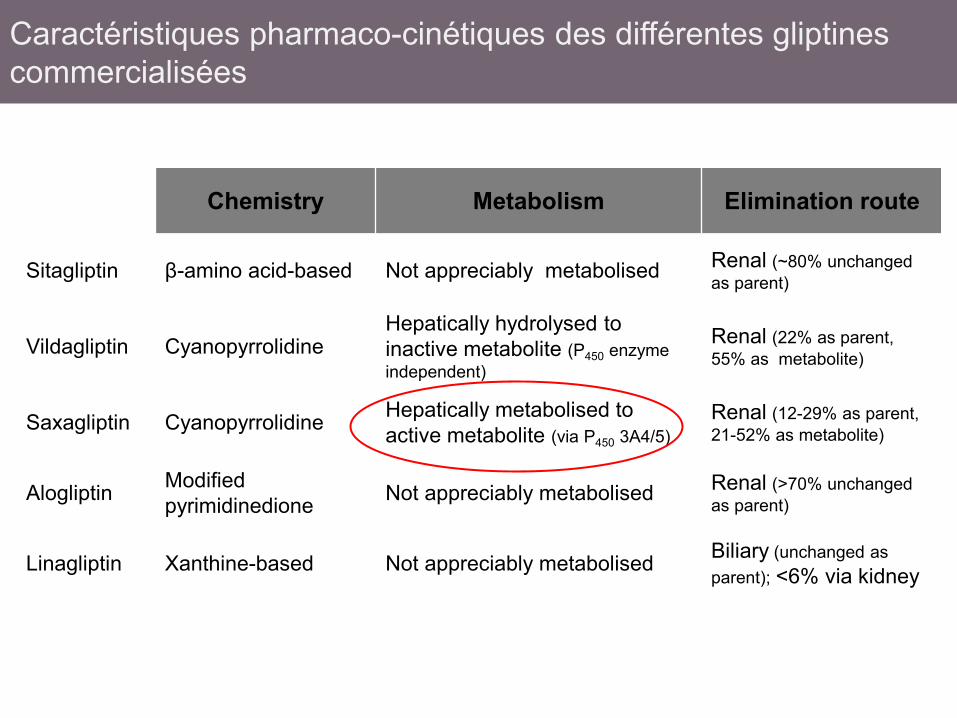
Chemistry Metabolism Elimination route
Sitagliptin β-amino acid-based Not appreciably metabolised Renal (~80% unchanged as parent)
Vildagliptin Cyanopyrrolidine Hepatically hydrolysed to inactive metabolite (P450 enzyme independent)
Renal (22% as parent, 55% as metabolite)
Saxagliptin Cyanopyrrolidine Hepatically metabolised to active metabolite (via P450 3A4/5)
Renal (12-29% as parent, 21-52% as metabolite)
Alogliptin Modified pyrimidinedione Not appreciably metabolised Renal (>70% unchanged
as parent)
Linagliptin Xanthine-based Not appreciably metabolised Biliary (unchanged as parent); <6% via kidney
Caractéristiques pharmaco-cinétiques des différentes gliptines commercialisées

Chemistry Metabolism Elimination route
Sitagliptin β-amino acid-based Not appreciably metabolised Renal (~80% unchanged as parent)
Vildagliptin Cyanopyrrolidine Hepatically hydrolysed to inactive metabolite (P450 enzyme independent)
Renal (22% as parent, 55% as metabolite)
Saxagliptin Cyanopyrrolidine Hepatically metabolised to active metabolite (via P450 3A4/5)
Renal (12-29% as parent, 21-52% as metabolite)
Alogliptin Modified pyrimidinedione Not appreciably metabolised Renal (>70% unchanged
as parent)
Linagliptin Xanthine-based Not appreciably metabolised Biliary (unchanged as parent); <6% via kidney
Caractéristiques pharmaco-cinétiques des différentes gliptines commercialisées
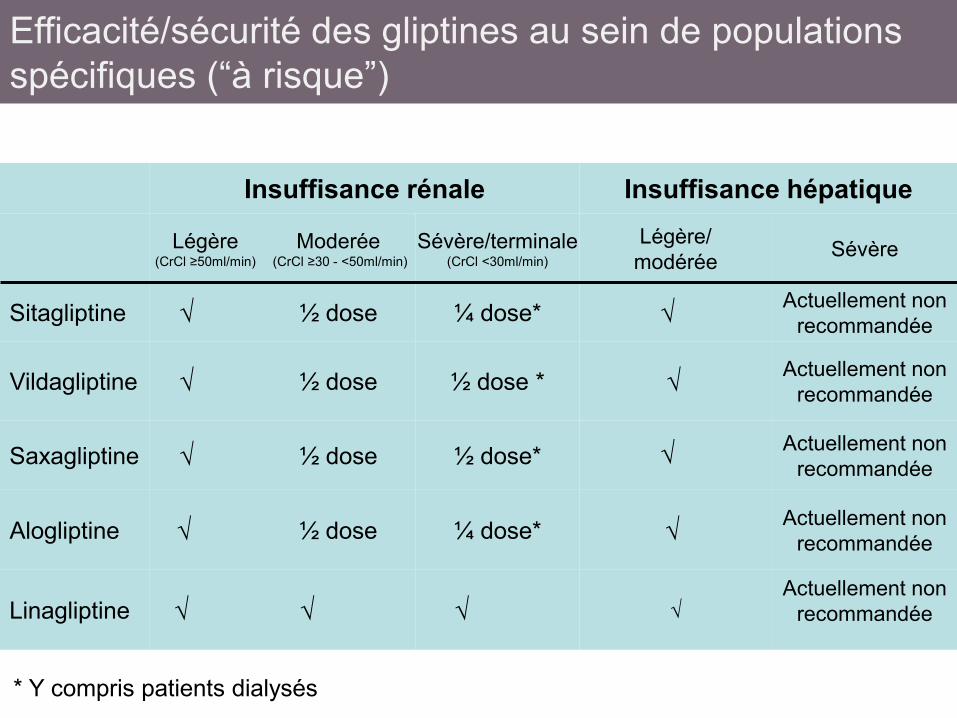
Efficacité/sécurité des gliptines au sein de populations spécifiques (“à risque”)
Insuffisance rénale Insuffisance hépatique
Légère (CrCl ≥50ml/min)
Moderée (CrCl ≥30 - <50ml/min)
Sévère/terminale (CrCl <30ml/min)
Légère/ modérée Sévère
Sitagliptine √ ½ dose ¼ dose* √ Actuellement non recommandée
Vildagliptine √ ½ dose ½ dose * √ Actuellement non recommandée
Saxagliptine √ ½ dose ½ dose* √ Actuellement non
recommandée
Alogliptine √ ½ dose ¼ dose* √ Actuellement non recommandée
Linagliptine √ √ √ √ Actuellement non
recommandée
* Y compris patients dialysés
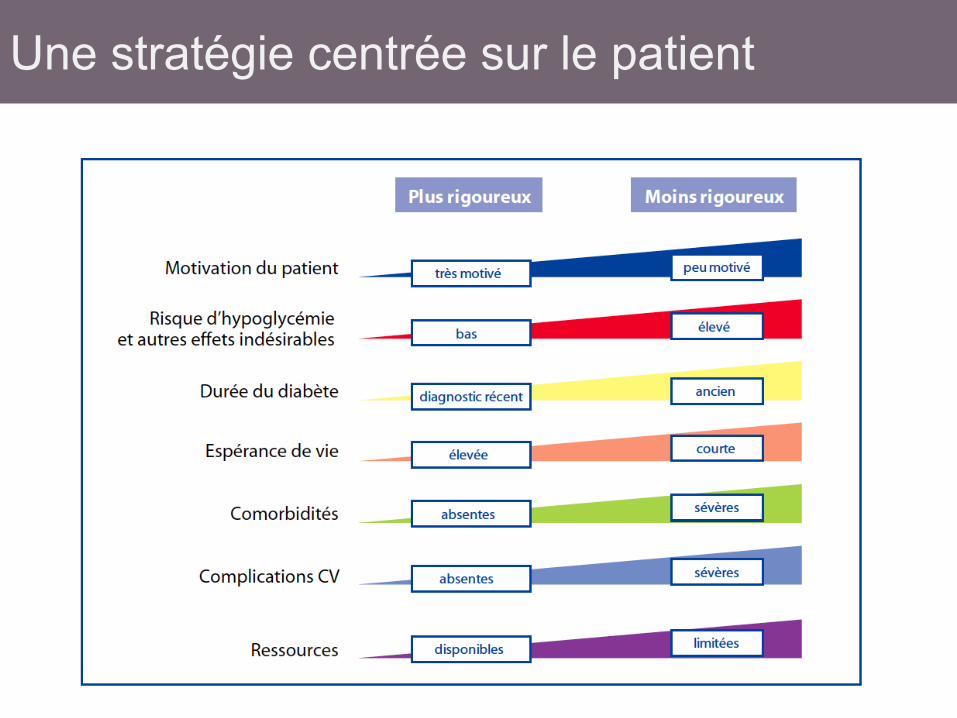
Une stratégie centrée sur le patient
• Individualiser • Toutes les options: grande sécurité si
utilisation appropriée – Gliptines
• Excellente tolérance (et observance) • prise de poids • risque d’hypoglycémie • Protection cardiovasculaire ?
Conclusions
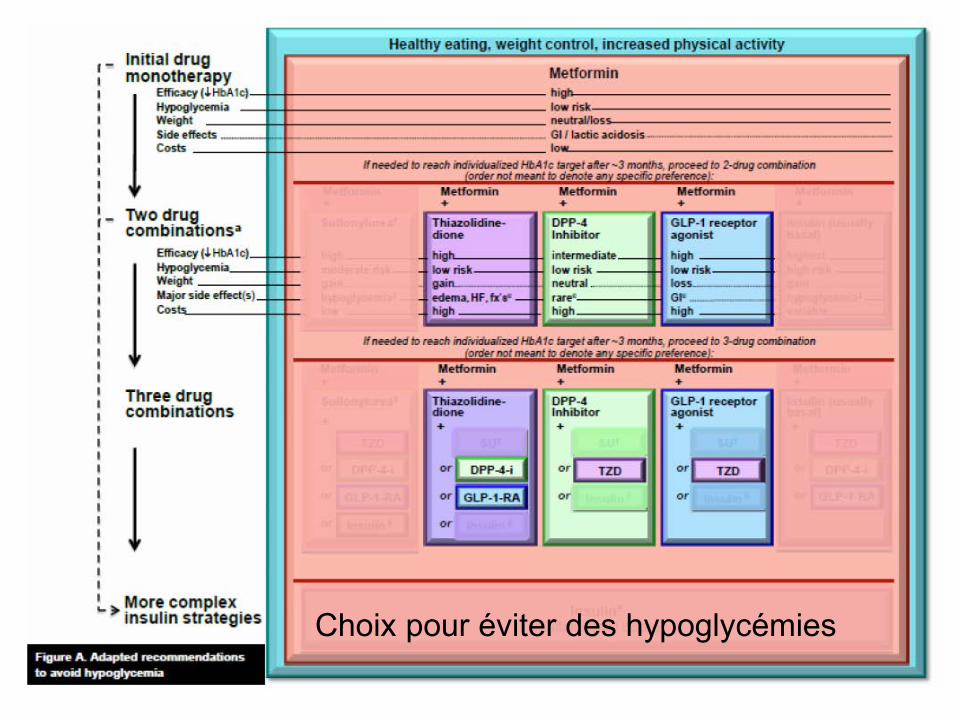
Choix pour éviter des hypoglycémies
Choix pour éviter des hypoglycémies
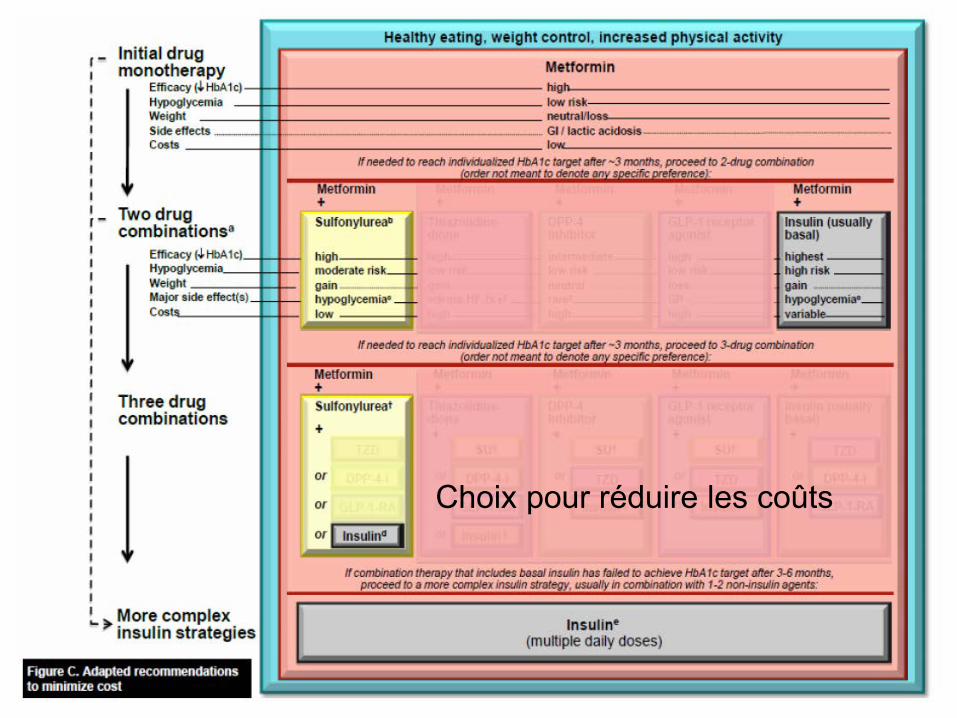
Choix pour réduire les coûts
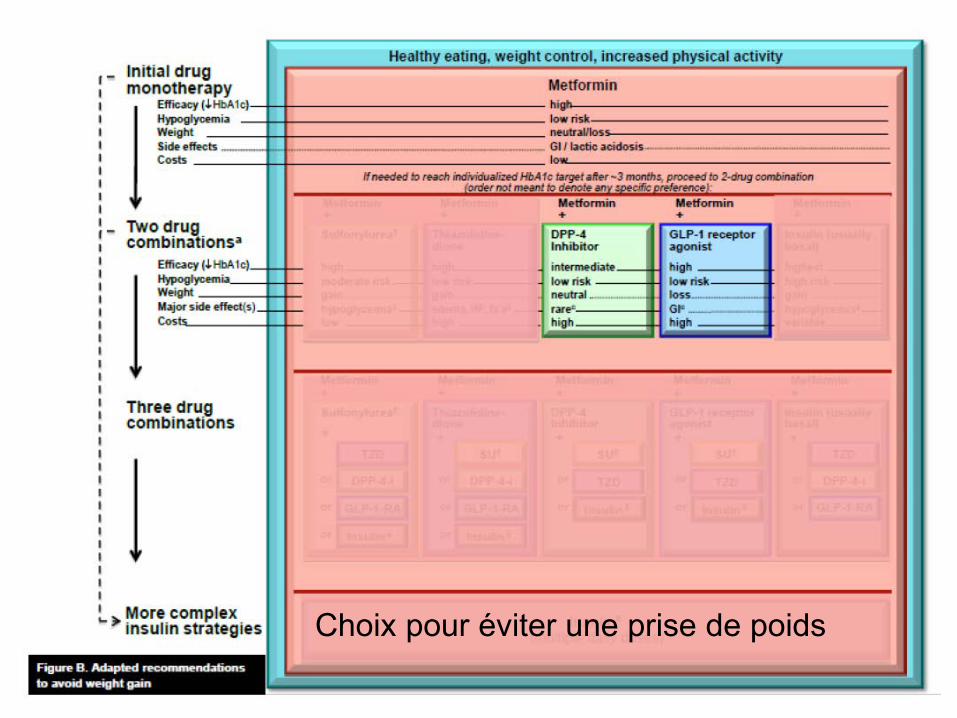
Choix pour éviter une prise de poids
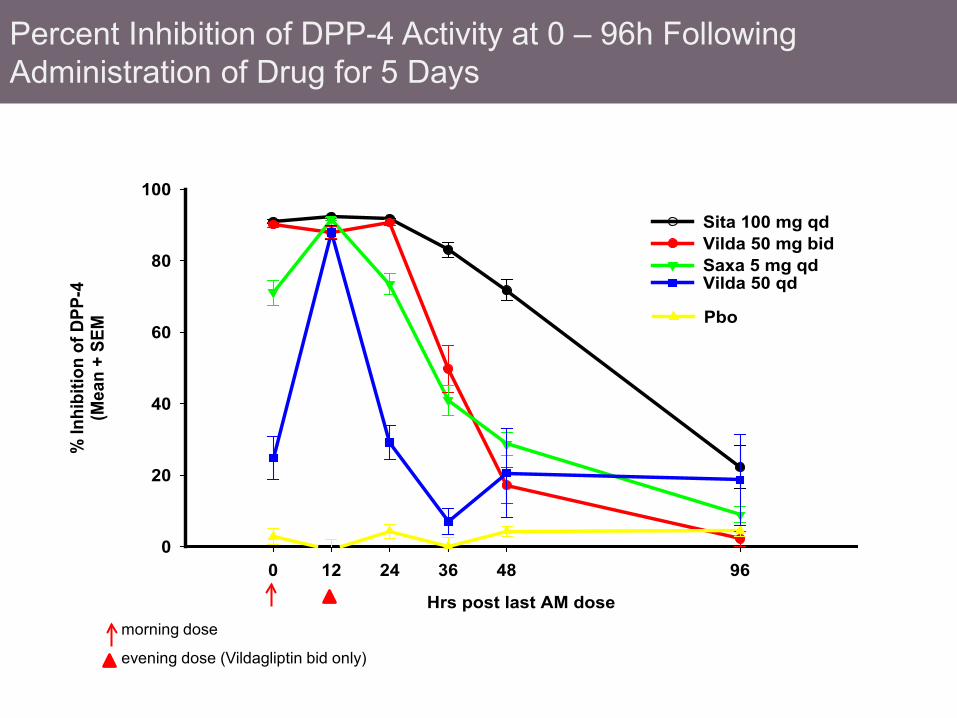
morning dose
evening dose (Vildagliptin bid only)
Hrs post last AM dose
0 12 24 36 48 96
% In
hibi
tion
of D
PP-4
(Mea
n +
SEM
0
20
40
60
80
100
Sita 100 mg qdVilda 50 mg bidSaxa 5 mg qd
Pbo
Vilda 50 qd
Percent Inhibition of DPP-4 Activity at 0 – 96h Following Administration of Drug for 5 Days